Submitted:
13 April 2023
Posted:
13 April 2023
You are already at the latest version
Abstract
Alcohol and substance addiction is a type of brain disease that damages many areas of life of the individual and has psychological components. Since questioning alcohol use alone is not sufficient in the diagnostic evaluation process, self-awareness and the individual's long-term psychological well-being are important in the rehabilitation process. Since investigating alcohol use alone is not sufficient in the diagnostic evaluation process, self-awareness and the individual’s long-term psychological well-being are important in the rehabilitation process. Primary prevention is used to prevent disease in healthy people, and secondary prevention is used for early diagnosis to people at risk. Tertiary prevention is important to prevent recurrence of the disease in the treated person. In addiction, which is a chronic problem, a need has emerged for tertiary prevention, that is, rehabilitation standards. If people are uncertain about the harm perception and the natural result of their behavior, they easily slip into the substance. Therefore, as a positive psychotherapy technique, harm perception and result awareness levels should be clarified. For this reason, scales were developed. The inclusion of new psychology perspectives and therapy techniques, such as positive psychology, in the treatment process requires setting new standards. In this study, it was aimed to develop result awareness and harm perception scales to determine the awareness levels and rehabilitation standards of alcohol and substance addicted individuals, and to compare awareness in normal and addicted groups. The study group consisted of 1134 participants, 41 of whom were addicts. Among the two scales developed in the study, the Uskudar Result Awareness Scale (USRAS) consisting of 25 items and 6 factor, explained 58.4% of the total variance. The Uskudar Harm Perception Scale (USHPS), consisting of 36 items and 10 factors, explained 56.3% of the total variance. Confirmatory factor analysis of the two scales resulted in acceptable goodness-of-fit values. (X2/df<3; RMSEA<.08; NFI>.90; NNFI>.95; CFI>.95; GFI>.90; AGFI>.85). In the comparisons made, the result awareness of the normal group was moderate (X=3,81); whereas the addicted group had a low result awareness (X=3,20); The effect size of the difference between the two groups was found to be high (d=1,45; >0,8). In the other measure, the harm perception of the normal group was found in the low-risk group (X=3,78); the harm perception of the addicted group was found in the moderate-risk group (X=3,43). According to Cohen d calculations, the effect size of the difference between the two groups is high (d=1,43; >0,8). It has been concluded that the two scales that emerged in the research are valid and safe, can be included in the rehabilitation studies and the creation of self-awareness, and their effectiveness should be tested.
Keywords:
Alcohol addiction
; substance addiction
; self-awareness
; rehabilitation
; scale development
; tertiary prevention
; dangerous and harmful use
; positive psychotherapy in addiction
1. Introduction
Alcohol and substance use is one of the important issues in psychiatry. Alcohol can create relief by allowing individuals to experience a certain level of pleasure. It has negative effects on the central nervous system and is the most addictive substance in the world after tobacco and caffeine [1]. Alcohol and substance use disorders are evaluated in a wide range. Investigating alcohol use alone is quite insufficient for diagnostic evaluation, and it is necessary to identify the problems that accompany people’s use of these substances.
In order for the substance use to cause a problem for the individual and his/her environment, he/she must experience problems, uneasiness or have impaired functionality in his/her social and/or professional life to a certain extent. Substance use is basically evaluated in three categories such as risky use, abuse and substance addiction [2,3,4]. Risky use is the use of alcohol and substances that can lead to harmful consequences. This use can cause both physical and mental problems and social negativities. Abuse is the result of not being able to take the main responsibilities that should be taken or expected at work, school or at home within the 12-month period in the fourth edition of the Diagnostic and Statistical Manual of Mental Disorders [DSM-IV]. It is defined as an inappropriate use of behavior pattern characterized by repetitive social or interpersonal problems and the emergence of negative experiences at the clinical level. Substance addiction, on the other hand, can be defined as a disease characterized by the desire to take a substance continuously or to reach the substance at an intense level, in order to feel the pleasurable effects of a substance with a drug quality and to avoid the discomfort caused by its absence. It is considered as a brain disease that has psychological components such as epilepsy, Parkinson’s and Alzheimer’s diseases and that significantly inhibits the functionality of the individual [5,6,7,8]. Within the framework of this study, the subject will be discussed through the concept of addiction, as awareness levels of alcohol and substance addicted individuals and the development of result awareness and harm perception scales to determine rehabilitation standards will be made by making awareness comparison in normal and addicted groups.
In order to diagnose a person as an addict, at least three of the following diagnostic criteria must be present in a way that causes clinically significant discomfort and problems for a minimum of 12 months [9]:
-Tolerance: Due to the decreased effect of the substance, increasing the amount of substance taken to achieve the desired effect.
-Withdrawal: Appearance of substance-specific withdrawal symptoms as substance intake is reduced or discontinued.
-Loss of control over substance use: Taking the substance in larger amounts and for longer periods than intended, unable to be stopped once started.
-Inability to quit the substance despite the desire and efforts to quit or reduce it.
-Spending a lot of time on substance use-related activities (for finding the substance, while using or under the influence).
-Inability to spare time for social, professional obligations, other activities, neglecting responsibilities, delaying.
-Continuing substance use despite the presence of social and legal problems, physical and mental health problems.
It is not obligatory for a person to have tolerance and/or withdrawal symptoms to be considered addicted. Meeting at least three of the other diagnostic criteria is sufficient for the diagnosis of substance addiction. However, it is observed that there is an accompanying internal problem in most of the alcohol and substance addicts who apply to hospitals for treatment. Therefore, it should not be overlooked that there are many factors accompanying addiction and that addiction should be handled multidimensionally. In order to ensure standardization in awareness and rehabilitation studies to be carried out, model studies developed considering the biopsychosocial perspective should be updated by adding new perspectives such as positive psychology-based rehabilitation and current measurement tools developed for this purpose. This is also the subject of this study.
1.1. Factors Affecting Alcohol and Substance Addiction
There are many factors that affect alcohol and substance addiction. For example; family is considered both an etiological factor in terms of alcohol and substance addiction and a basic protective factor that is effectively used in the fight against addiction [1]. Accordingly, in addition to the preventive effect of positive family dynamics in alcohol and substance addiction, familial factors such as secure attachment within the family and close and empathic behavioral relationships are the main psychotherapeutic elements that are actively studied in the psychotherapy of addicted individuals. In order for the treatment of substance addiction to be completed successfully, family members and relatives who are valuable to the addicted person should be involved in the necessary stages of the treatment. It is very important to include family members in therapy in order to prevent the emergence of a possible childhood regression in case any of the family members of the treated cases suddenly leaves the life of the case [10,11,12]. Thus, the family plays a fundamental role in strategies and techniques developed against alcohol and substance abuse.
On the other hand, anger level, addiction profile, depression and anxiety levels are associated in patients with substance addiction [13]. As the anger level increases, it is seen that substance use has a greater effect on life and the desire for substance use increases. For this reason, it is thought that anger is an important factor that should be evaluated in the substance addiction process. Again, appetite, nutritional status and quality of life are associated with individuals with alcohol and substance addiction [14]. In a study conducted on 213 male individuals aged between 20-60 years, 167 of whom are addicted to substances and 46 alcohol, a questionnaire was applied by face-to-face interview technique, general information, dietary habits, 24-hour food consumption status were determined. Simplified Nutritional Appetite Questionnaire (SNAQ), Dietery Diversity Score (DDS), Short Form of Quality of Life Scale (SF-36) were administered and anthropometric measurements were taken. As a result of the research, it was determined that 71.3% of substance users and 93.5% of alcohol users have a significant risk of weight loss in the next 6 months due to impaired appetite. In the general evaluation, it was found that individuals generally consume a single meal (57.7%), and this situation is more common in alcohol addicts (76.1%) than in individuals using substance (57.7%) [14].
Another aspect of the studies was to examine the sociodemographic and clinical characteristics of patients with alcohol and substance use disorders who applied to an AMATEM (Alcohol and Substance Abuse Treatment Center) unit. In studies, it is noteworthy that the rate of seeking treatment due to alcohol and substance use in men is higher than women, they use alcohol and substances at a level that may cause problems for their families, and there is a very high rate of job loss in particular [15]. In the in-depth interview study conducted with 9 patients receiving drug addiction treatment, when asked about their addiction and treatment experiences, they were exposed to labeling during the process of using substances, they faced medical, psychological, social, legal and economic problems, and their motivation to seek treatment mostly stemmed from these problems [16].
1.2. Rehabilitation Process in Alcohol and Substance Addiction
Treatment of individuals with alcohol and non-alcoholic substance addiction; consists of medical treatment, psycho-social treatment and social rehabilitation programs. Drug treatment of addicts is carried out in two stages: short-term and long-term. Short-term drug therapy is used to control the withdrawal symptoms that occur during the withdrawal of the addictive substance or in the physical and mental disorders that develop due to substance intoxication. Long-term drug therapy is called replacement or maintenance therapy. In this treatment, those who are addicted to addictive substances such as alcohol and heroin are included in continuous and versatile treatment programs. The main purpose of social rehabilitation programs is to reintegrate substance-addicted individuals into society and to ensure their social functionality [17,18]. Psychosocial treatments, on the other hand, are treatments in which individual therapies and group therapies are applied in which the skills are gained to prevent the substance addicted individual from starting to use drugs again, the behavior patterns brought by addiction are replaced by the new behavioral patterns, and his/her relations with his/her family and environment are regulated [19].
Addiction rehabilitation has promoted treatment models that address addiction as a chronic rather than an acute illness. The biopsychosocial model is important in the treatment process of alcohol and substance addiction [20]. This model does not reduce the disease to a medical focus only; It predicts that the factors causing the disease may be related to the psychological and social contexts. This perspective, which considers the psychological and social aspects of the person, suggests that psycho-social characteristics may be related to substance use, and thus the medical perspective that blames the person and claims that the source of the problems is himself/herself alone is rejected.
The number of applications made due to substance use to AMATEM (Alcohol and Substance Abuse Treatment Center), which has been the institution with the highest number of applications related to alcohol and non-alcoholic psychoactive substance use in Turkey since 1983, was 78 in 1983, this figure was 2917 in 1996. Since repeated applications are included in these numbers, when the number of drug users who applied for the first time is investigated, it is seen that it was 665 in 1993, 882 in 1994, 984 in 1995 and 955 in 1996. During the first 10 months of 2006, this number reached 1742. This situation can be considered as an indicator of the increasing problem of substance use [21].
On the other hand, it has been reported that 50-60% or more of patients with alcohol and substance use disorders started drinking again within a few months after detoxification due to negative emotional states, interpersonal conflicts, and social pressure [22,23,24,25,26,27,28,29]. Thus, while determining awareness and rehabilitation standards, it is important to structure these standards to protect the addict as much as possible from relapse. At this stage, it is useful to include the perspective of positive psychology in the rehabilitation processes. Positive psychology distinguishes itself from known psychology teachings. The purpose of positive psychology is not to replace conventional psychology, but to become an important complement to it. Positive psychotherapy, on the other hand, takes its source from positive psychology [30].
It is known that more than half of physical diseases are caused by living without nutrition, not exercising and not paying attention to hygiene, that is, they are related to the consequences of lifestyle. It would not be wrong to say that more than half of mental illnesses are caused by not being able to live right and wrong life philosophy, that is, mental well-being is directly proportional to positive life philosophy. At this point, positive psychology suggests using core values and developing some skills. The science of positive psychology tries to understand and intervene in order to increase the life satisfaction and happiness of both healthy individuals and the clinical population [31,32,33,34,35]. “Positive Activity Interventions” (PAI) encourage positive emotions, positive thoughts, and/or positive behaviors rather than directly aiming to correct negative or pathological feelings, thoughts, and behaviors. It is also defined as a relatively short, self-administered and non-stigmatizing activity or exercise.
Results of a pilot study of 8 sessions of positive intervention with a group of adolescents with substance use problems in the UK showed that groups at greater risk were more likely to benefit from positive interventions. The results of this study provided support for investigating the value of such interventions among people being treated for substance use disorders. A more detailed description of positive psychology’s contributions sheds light on its potential for addiction research in general and rehabilitation in particular. The conceptual map drawn by the founding positive psychologists is in three areas: positive emotion, personality strength, and positive knowledge. These three domains are associated with three “types of happiness”. “Pleasant life” is filled with positive emotion, “good life” represents the strength of character required for full commitment, and “meaningful life” represents positive institutions that allow individuals to develop and contribute.
1.3. Self-Awareness in Substance Use
Self-awareness of the addicted individual is an important factor affecting the treatment process. Mindfulness is a mind and body practice that involves focusing attention on momentary experiences and observing inner experiences [36,37]. Mindfulness is defined as accepting and evaluating the positive and negative situations as they are and being aware of them [38]. In the literature, it is known that mindfulness can create positive mood, decrease in depressive relapses, increase in empathy, decrease in substance use, increase in motivation, increase in students’ academic success, decrease in stress level, awareness of emotions and decrease in anxiety level [39]. The existence of three pillars of addiction can be questioned as a support for awareness studies. The first pillar is matter itself. The second is the addiction subculture the person is in. The third pillar is the personality structure of the individual. Here, subculture is the culture that develops without breaking its connection with the dominant culture, but by separating at various important points (different purpose, expectation, behavior, attitude, action, clothing style, language, value and lifestyle) [40]. When dealing with addiction, it is necessary to evaluate these three dimensions together and to plan together in treatment.
When the literature is examined, scales for addiction awareness and studies using scales are found [41,42,43]. One of these scales is The Substance Addiction Awareness Scale, developed by Özay Köse and Gül in 2018, to measure substance addiction awareness. It was developed by applying to 230 secondary school students. It consists of 4 factors (Support and legal regulations, Symptoms and effects of substance use, Personal attitudes and opinions, Factors causing addiction) and 27 items. The explained variance rate of the scale was 4,.9%, and the internal consistency coefficient was found to be ,88 [42]. It is important to know the risk factors in the addiction treatment process. It is important for the person to be self-aware, that is, to know himself [44]. For example; Mindful Awareness is used in the treatment of substance use disorder in body-focused therapy. The treatment results of 61 women who received this body-focused therapy for 8 sessions per week showed moderate to large effects [45]. It is also stated that mindfulness and regulating emotions are predictive of substance addiction and other non-substance-related behavioral addictions [46]. Studies conducted with students in which awareness and level of knowledge are determined [47] are important as well as it is essential that current perspectives on mindfulness be included in the measurement tools used. It is stated that there is a need for awareness scales that can be applied especially to addicted individuals [48]. In this study, it was aimed to develop two scales suitable for a positive psychology-focused biopsychosocial perspective and to establish rehabilitation standards by determining awareness in normal individuals and addicted individuals.
2. Materials and Methods
2.1. Ethical Approval
This study received ethical approval from the Uskudar University Non-Interventional Research Ethics Committee report number of 61351342/December 2022-47 (28 December 2022). This study was performed according to the principles set out by the Declaration of Helsinki for the use of humans in experimental research.
2.2. Participants
In the study, the sample consisted of 1134 people over the age of 18, including the normal group (n=1091) and the addicted group (n=43). The validity and reliability studies of the Uskudar Result Awareness Scale (USRAS) and the Uskudar Harm Perception Scale (USHPS) were conducted on a sample consisting of two groups. Subsequently, psychometric properties of the scales and group comparisons were made and some rehabilitation standards were determined.
Considering the genders of the participants in the study, there were 80,8% female (n=882) and 17.7% male (n=193) in the normal group; 14% women (n=6) and 86% men (n=37) were in the addicted group. The addicted group consists of alcohol addicts and substance addicts who are hospitalized in the clinic with a mean age of 29,5 years. On the other hand, the normal group consists of volunteers over the age of 18, whose mean age is 34,6 and whom were reached via the internet. In general, the ages of the participants in the study group ranged from 18 to 67.
2.3. Data Collection Tools
A questionnaire including two scales developed in the study and a demographic information form were used as data collection tools in the research.
2.3.1. Demographic Information Form
In the demographic information form, the participants were asked questions such as gender, age, educational status, marital status, having a child, and daily use of social media, as well as whether they used harmful substances and the frequency of sleep disorders.
2.3.2. Uskudar Result Awareness Scale (USRAS) ve Uskudar Harm Perception Scale (USHPS)
For the validity and reliability studies of Uskudar Result Awareness Scale (USRAS) and Uskudar Harm Perception Scale (USHPS) developed in this study, content validity, factor analysis, construct validity, discriminant validity and internal consistency reliability were performed. Firstly, the researchers searched the literature for both scales and created an item pool by considering the principles of positive psychology in the study. Six experts were consulted for their opinions. With the expert evaluation inventory, questions in each candidate scale were evaluated as “It is appropriate for the item to remain on the scale”, “The item may remain on the scale, but unnecessary” and “It is not appropriate for the item to remain on the scale”. A pool of experts was formed with two academicians from each of the fields of psychology, psychiatry, and communication in order to include interdisciplinary views. Inventories were sent to the experts via e-mail. Subsequently, the compatibility ratios of the items were calculated with the help of the formula proposed by Miles and Huberman [49].
Compliance rates were calculated for each item using the ratings in the inventory. Accordingly, care was taken to ensure that the relevant item was scored between 0 and 1 and not below ,80. In addition, each item was revised and arranged in terms of spelling and grammar, taking into account the section in which the experts expressed their opinions. Thus, the 35-item Uskudar Result Awareness Scale (USRAS) and the 44-item Uskudar Harm Perception Scale (USHPS) candidate scale forms were prepared in a five-point Likert type (from Strongly Disagree to Totally Agree), and the data collection phase was started for factor analysis.
Explanatory Factor Analysis is one of the statistical calculation techniques performed in accordance with a large number of variables and is frequently applied within the scope of construct validity of scale development. Before performing EFA, it is necessary to test whether the data set is suitable for factor analysis [50]. For this, Bartlett Test of Sphericity and Kaiser-Meyer-Olkin (KMO) test were applied to the obtained data. A KMO value of ,90 and above is “excellent”, between ,80-,89 is “very good”, between ,70-,79 is “good”, between ,60-,69 is “moderate”, between ,50-,59 is “weak”, and below is considered “unacceptable”. Furthermore, the Bartlett Sphericity value is expected to be significant [51,52].
When the construct validity phase of the scales is proceeded, the number of factors can be determined with the EFA. For this, the Eigenvalues is used. According to the Eigenvalues, factors with this value equal to or greater than 1 are considered significant, and when it is less than 1, they are not taken into account [53]. Again, when the explained variance rate revealed by factor analysis varies between 40% and 60% it is ideal in social sciences. On the other hand, in the criterion validity studies of each scale, correlation values are examined in the relations of the scales with each other. It is stated that when interpreting the correlation values, the correlation value between 0,30-0,70 is “medium”; values above 0,70 indicate a “high” relationship, and values below 0,30 indicate a “weak” relationship [51].
The Confirmatory Factor Analysis is carried out to determine whether the parameters revealed by factor analysis confirm the scale structure, and the goodness-of-fit values are calculated with the structural equation modeling. Goodness-of-fit values are expected to be within acceptable ranges in the literature. During the reliability studies, internal consistency analysis for items is performed according to the item variances of the scales and Cronbach’s Alpha coefficients were calculated.
2.4. Criteria for Inclusion/Exclusion
While creating two groups in the study, patients who were diagnosed with alcohol use disorder and substance use disorder (American Psychiatric Association DSM-5 diagnostic criteria manual) and who received inpatient treatment in the clinic were included in the Addicted group in the study. The diagnostic criteria for the Normal group were ignored. Persons under 18 years of age were not included in the study for the groups.
2.5. Procedures
Pilot Application: The comprehensibility of the questions was tested by applying the online questionnaire, which was prepared as a data collection tool in the research, to 15 people for trial purposes. After the questionnaire was administered to the undiagnosed participants, a trial application was made to two patients who were treated under the supervision of a psychologist in consultation with a psychiatrist in the AMATEM unit. It was determined that no problem was encountered during the pilot application, and then the field application was started.
Application of Scales: The online questionnaire including Demographic Information Form, USRAS and USHPS scales was applied to both groups on a voluntary basis for a month on 1-30 January 2023, after the approval of the Ethics Committee dated 30 December 2022. For the participants in the normal group, the questionnaire was shared on digital platforms, via e-mail and sms. For the addicted group, data were collected by applying the online survey on a PC under the supervision of a psychologist, on a voluntary basis.
2.6. Data Processings and Statistical Analysis
Exploratory factor analysis (EFA) was applied in the USRAS and USHPS construct validity studies. The correlation coefficient of the Pearson product of moments was calculated for the relationship between the dimensions of the scales and the sum of the scales. Pearson Correlation Coefficient test was applied in criterion validity studies. The internal consistency reliability coefficient of the scales was determined by the Cronbach Alpha value. In the confirmatory factor analysis study, goodness-of-fit values (X2/df, RMSEA, NFI, NNFI, CFI, GFI, AGFI) were evaluated in the presence of structural equation model on a 400-person data set, which consists of groups classified as Normal and Addicted. While comparing the Normal group and Addicted group, the normal distribution was checked in the data set. In the case of normal distribution, the differentiation of independent variables according to the dependent variable was examined by parametric tests (independent group t-test, one-way analysis of variance). SPSS 26.0 and AMOS statistical program were used for all validity and reliability analyzes and comparison tests.
3. Results
3.1. The Validity and Realibility Studies of Uskudar Result Awareness Scale (USRAS)
At the beginning of the validity and reliability studies, whether the data were suitable for factor analysis was examined with the Kaiser Meyer Olkin (KMO) sampling coefficient and the Bartlett Test of Sphericity. Accordingly, the KMO coefficient value was found to be ,85. The result of the Bartlett Test of Sphericity was found to be significant (X2=9271,572; df: 300; p=0,000). Thus, the results showed that the data were suitable for factor analysis (52). Exploratory factor analysis (EFA) was performed with 35-item candidate scale data created after the expert opinion phase. During EFA, values with Eigenvalue greater than 1 formed a factor and a 6-factor structure emerged for USRAS [53].

Table 1.
USRAS Factor Structure and Explained Variance Ratio.
| USRAS | Eigenvalue | Variance | Cummulative Varience |
|---|---|---|---|
| Factor 1 | 5,38 | 21,54 | 21,54 |
| Factor 2 | 3,59 | 14,36 | 35,90 |
| Factor 3 | 1,68 | 6,72 | 42,62 |
| Factor 4 | 1,53 | 6,12 | 48,74 |
| Factor 5 | 1,29 | 5,16 | 53,90 |
| Factor 6 | 1,14 | 4,58 | 58,49 |
As seen in Table 1, the Eigenvalues of the factors vary between 5,38 and 1,14. The explained variance rate in the total scale was 58,49%. After determining the number of factors, item factor loads were examined, and when the factor load of each item was ,50, a suitable structure with 6 factors and 25 items emerged. Thus, 10 items (7,9,10,13,14,17,20,21,22,32) in the scale were eliminated from the scale due to their presence in more than one factor or low factor load. The factor loading values of the items are given in Table 2.
As seen in Table 2, the factor and item distributions in the scale were determined, and the items were renumbered. Subsequently, each of the factors to which the new numbered items belong was given a name. Accordingly, Factor 1 (Items 1-7) is “Medium and Long-Term Plan”; Factor 2 (Items 8-11) “Action”; Factor 3 (Items 12-15) “Decision”; Factor 4 (Items 16-18) “Short-Term Plan”; Factor 5 (Items 19-22) “Emotion/Intention”; Factor 6 (Items 23-25) is named as “Philosophy of Life”. Item-total correlations were found to be within the acceptable range for each item and correlated with the scale (r>,30). Within the scope of reliability studies, Cronbach Alpha values, which are the internal consistency coefficients of the factors and the scale total, were calculated. The Cronbach Alpha values of the factors were found to be between ,67 and ,82; and the total scale was found to be ,72.
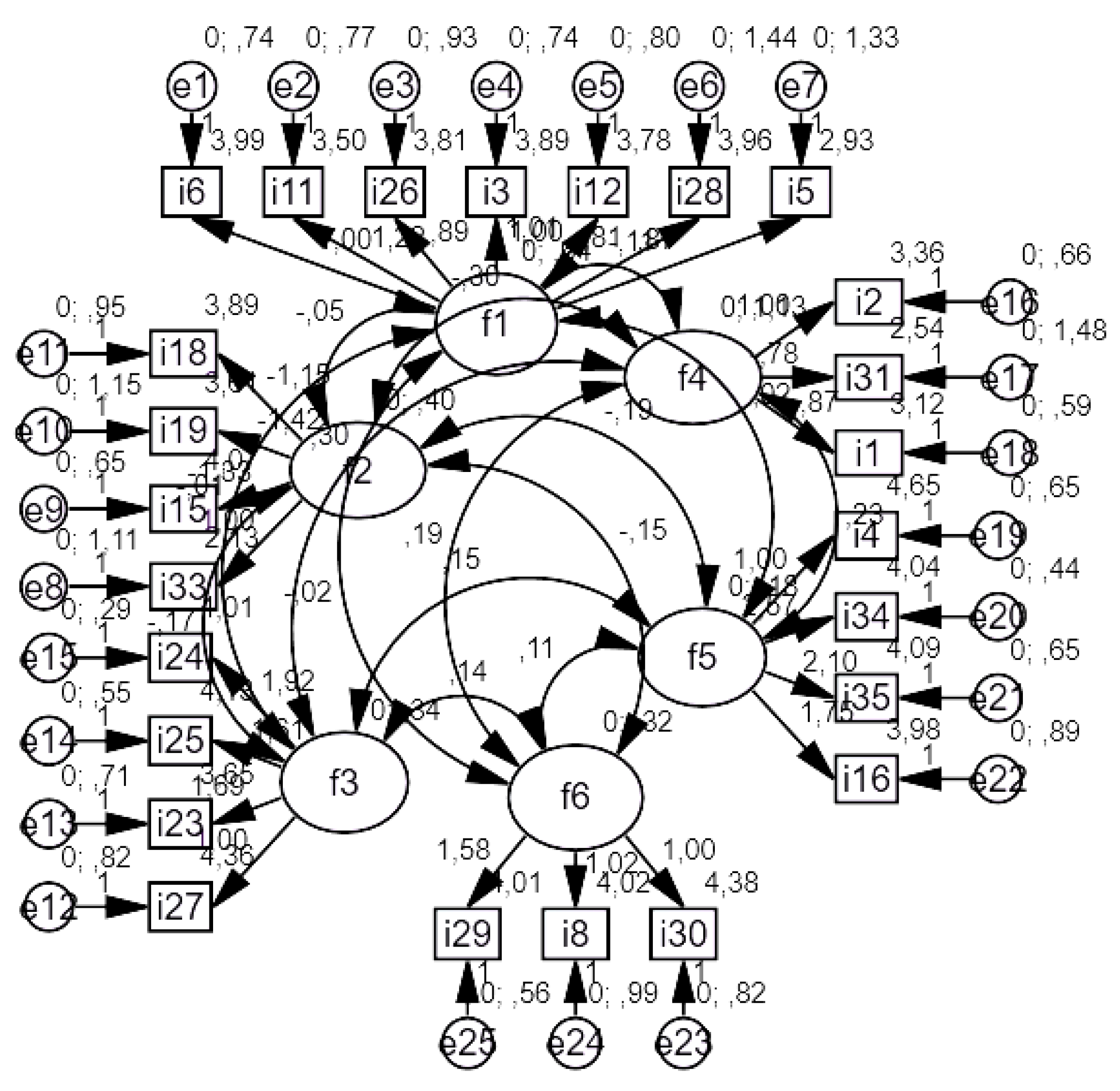
After the USRAS factor structure was formed, a scale model was drawn using the AMOS program with the data set consisting of 400 people, and confirmatory factor analysis was applied. Whether the model was validated or not was tested with goodness-of-fit values. When the model was run by creating covariance among the factors in the model, the goodness-of-fit values were found to be in the acceptable range and the model was validated (X2/sd=2.47<3; RMSEA=.06<.08; NFI=.92>.90; NNFI=.96>.95; CFI=.97>.95; GFI=.91>.90; AGFI=.87>.85).
Figure 1.
USRAS Scale Standardized Model.
3.2. Intergroup Awareness Scores of Uskudar Result Awareness Scale (USRAS)
As a result of the validity and reliability studies, the average scores of the participants from the scale were calculated by adding each item and dividing it by 25. The mean scores of the normal and addicted groups in the study were also obtained, using the Effect Size (d) calculation developed by Cohen (1988) [54]. The effect size of the groups was revealed as in Table 3.
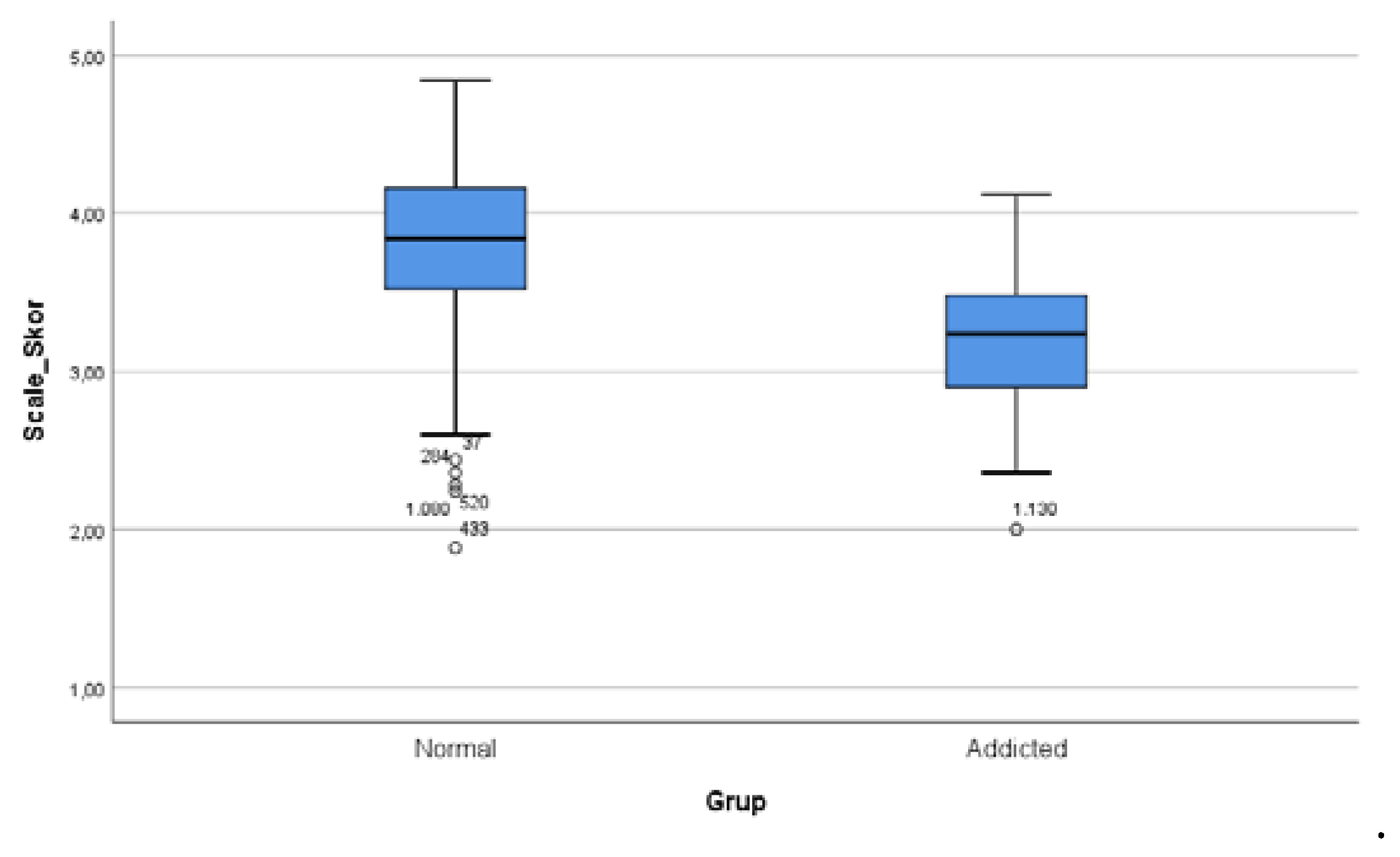
The normal and addicted groups were taken as reference while performing the statistical analysis. In the first stage, the scale scores of the total of the normal group and the total of the addicted group were compared with the independent group t-test, and the result was found to be significant (t=9,17; p<,001). It was revealed that the addicted group’s result awareness was lower than the normal group (X=3,20). The effect size of the difference between the addicted group and the normal group was evaluated with Cohen’s D effect size calculation, taking into account the scale scores. Accordingly, the normal group was found to be in a higher impact area in terms of result awareness compared to the addicted group (d=1,45; >0,8).
When evaluating the effect size of Cohen, it is stated that if the d value is less than 0,2, the effect size can be defined as “weak”; if it is 0,5, it can be defined as “medium” and if it is greater than 0,8, it can be defined as “strong” [54]. In addition, when the difference between the two groups according to gender was examined, the number of men and women was found to be suitable for the normal group statistically. In the independent group t-test calculations, there was no difference according to gender (t=1,93; p>,005). In the addicted group, no comparison was made since the number of women was less than 30.
Figure 2.
USRAS Scale Scores of the groups (The cut-off value was accepted as 2.5.).
The difference between the groups and the effect size were analyzed in the comparison of the scale scores of the normal and addicted groups for harmful substance use (Table 4).
First, the normal group was compared with one-way Anova analysis according to the three categories within itself, and the difference between the groups was found to be significant (p<0.001). When the difference between the groups was examined by LSD analysis, the result awareness of the group that replied “never use” was found to be the highest compared to the other groups. The result awareness score of the group with “tobacco, alcohol and substance use” was found to be the lowest compared to the other two groups (X=3,47). The difference in the three categories within the normal group was also examined by Cohen's d effect size calculation. The group that never used harmful substances was found to be in a higher effect area compared to the group that “uses tobacco, alcohol and substance” (d=0,82; >0,8). The group that never used was slightly above the weak effect area and at the border of the medium effect area compared to the “only tobacco use” group (d=0,24; >0,2<0,5). The “only tobacco use” group included in the normal group was found to be in the medium effect area compared to the “tobacco, alcohol and substance use” group (d=0,59; >0,5). Lastly, the “tobacco, alcohol and substance use” group in the normal group and the addicted group (tobacco, alcohol and substance use) were compared with the independent group t-test, and the difference was found at the border (p=0.05). According to the effect size calculation, the effect area of the group using more harmful substances in the normal group was found to be moderate compared to the addicted group using the same type of harmful substances” (d=0,57; >0,5). The scale score of the addicted group was found to be the lowest in all categories in the normal group (X=3,20). In other words, the result awareness level was observed to be the lowest.
3.3. The Validity and Realibility Studies of Uskudar Harm Perception Scale (USHPS)
At the beginning of the validity and reliability studies, whether the data were suitable for factor analysis was examined with the Kaiser Meyer Olkin (KMO) sampling coefficient and the Bartlett Test of Sphericity. Accordingly, the KMO coefficient value was found to be ,85. The result of the Bartlett Test of Sphericity was found to be significant (X2=10198,805; df: 630; p=0,000). Thus, the results showed that the data were suitable for factor analysis. After receiving expert opinions for the scale, exploratory factor analysis (EFA) was applied to the data collected with the 44-item candidate scale. During EFA, values with Eigenvalue greater than 1 formed a factor and a 10-factor structure emerged for USHPS [53].
Table 5.
USHPS Factor Structure and Explained Variance Ratio.
| USHPS | Eigenvalue | Variance | Cummulative Variance |
|---|---|---|---|
| Factor 1 | 6,37 | 17,70 | 17,70 |
| Factor 2 | 2,78 | 7,72 | 25,43 |
| Factor 3 | 2,14 | 5,95 | 34,38 |
| Factor 4 | 1,89 | 5,25 | 36,64 |
| Factor 5 | 1,44 | 4,01 | 40,65 |
| Factor 6 | 1,27 | 3,54 | 44,19 |
| Factor 7 | 1,17 | 3,26 | 47,46 |
| Factor 8 | 1,11 | 3,09 | 50,55 |
| Factor 9 | 1,06 | 2,94 | 53,50 |
| Factor 10 | 1,02 | 2,85 | 56,36 |
As seen in Table 5, the Eigenvalues of the factors vary between 6,37 and 1,02. The explained variance rate in the total scale was 56,36%. After determining the number of factors, item factor loads were examined, and when the factor load of each item was ,50, a suitable structure with 10 factors and 36 items emerged. Thus, 8 items (3,13,19,21,22,33,35,38) in the scale were eliminated from the scale due to their presence in more than one factor or low factor load. The factor loading values of the items are given in Table 6.
As seen in Table 6, the factor and item distributions in the scale were determined, and the items were renumbered. Subsequently, each of the factors to which the new numbered items belong was given a name. Accordingly, Factor 1 (Items 1-6) is “Objectivity and Long-Term Perceptual Blindness”; Factor 2 (Items 7-11) “Stress Relief”; Factor 3 (Items 12-156 “Impulsivity and Subjective Reality Blindness”; Factor 4 (Items 17-19) “Curiosity”; Factor 5 (Items 20-22) “Harm Avoidance”; Factor 6 (Items 23-24) “Sensation-seeking”; Factor 7 (Items 25-27) “Perception of Narcissism”; Factor 8 (Items 28-31) “Perception of Hedonism;” Factor 9 (Items 32-33) “Control”; Factor 10 (Items 34-36) is named as “Intention”. Item-total correlations for USHPS were within the acceptable range for each item and correlated with the scale (r>,30). Within the scope of reliability studies, Cronbach Alpha values, which are the internal consistency coefficients of the factors and the scale total, were calculated. The Cronbach Alpha values of the factors were found to be between ,68 and ,86; and the total scale was found to be ,83.
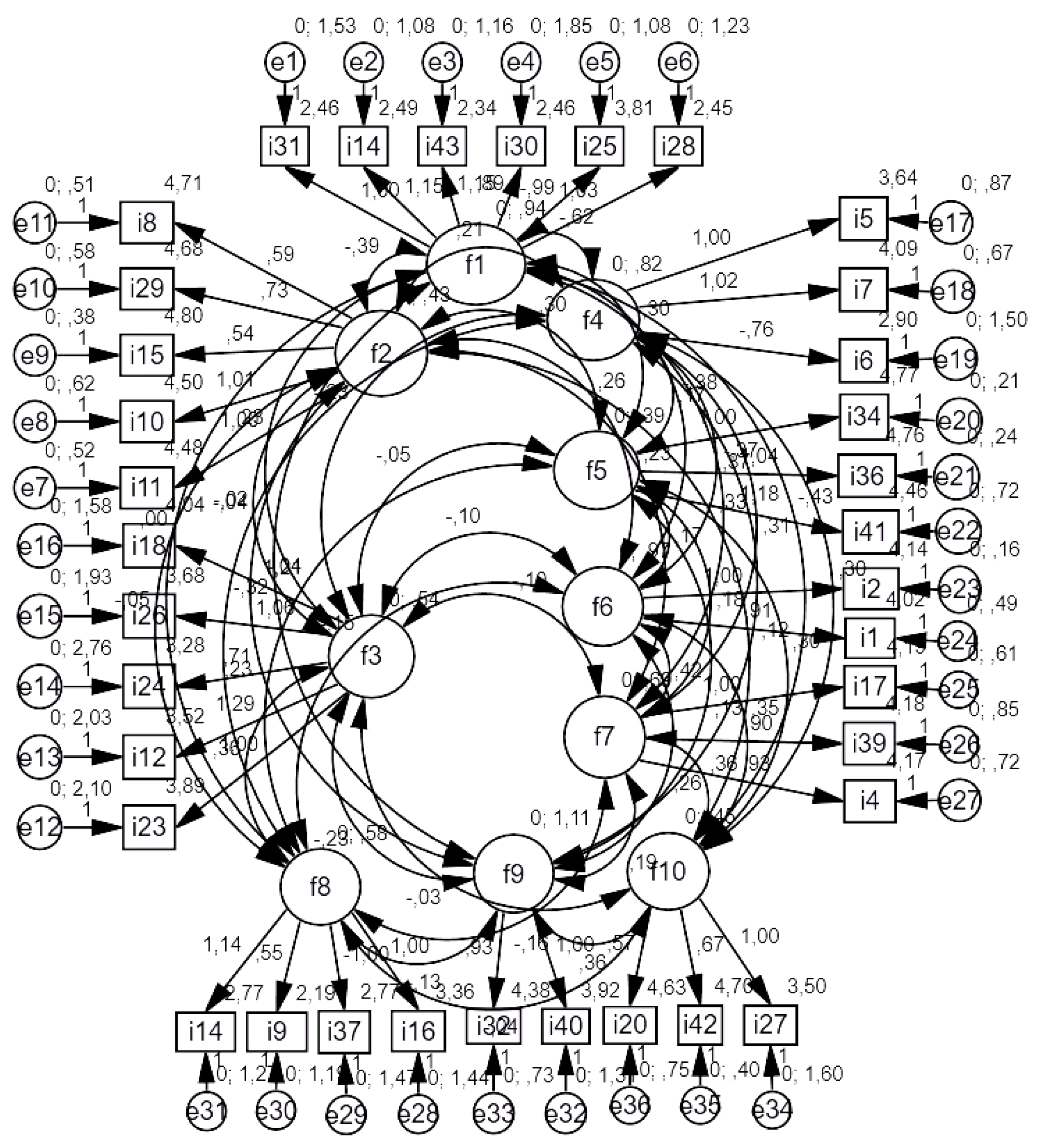
After the USHPS factor structure was formed, a scale model was drawn using the AMOS program with the data set consisting of 400 people, and confirmatory factor analysis was applied. Whether the model was validated or not was tested with goodness-of-fit values. When the model was run by creating covariance among the factors in the model, the goodness-of-fit values were found to be in the acceptable range and the model was validated (X2/df=2.01<3; RMSEA=.05<.08; NFI=.93>.90; NNFI=.97>.95; CFI=.96>.95; GFI=.92>.90; AGFI=.86>.85).
Figure 3.
USHPS Scale Standardized Model.
3.4. Intergroup Awareness Scores of Uskudar Harm Perception Scale (USHPS)
As a result of the validity and reliability studies, the average scores of the participants from the scale were calculated by adding each item and dividing it by 36. By using the Effect Size (d) calculation developed by Cohen (1988) [54], the effect size of the groups was revealed as in Table 7.
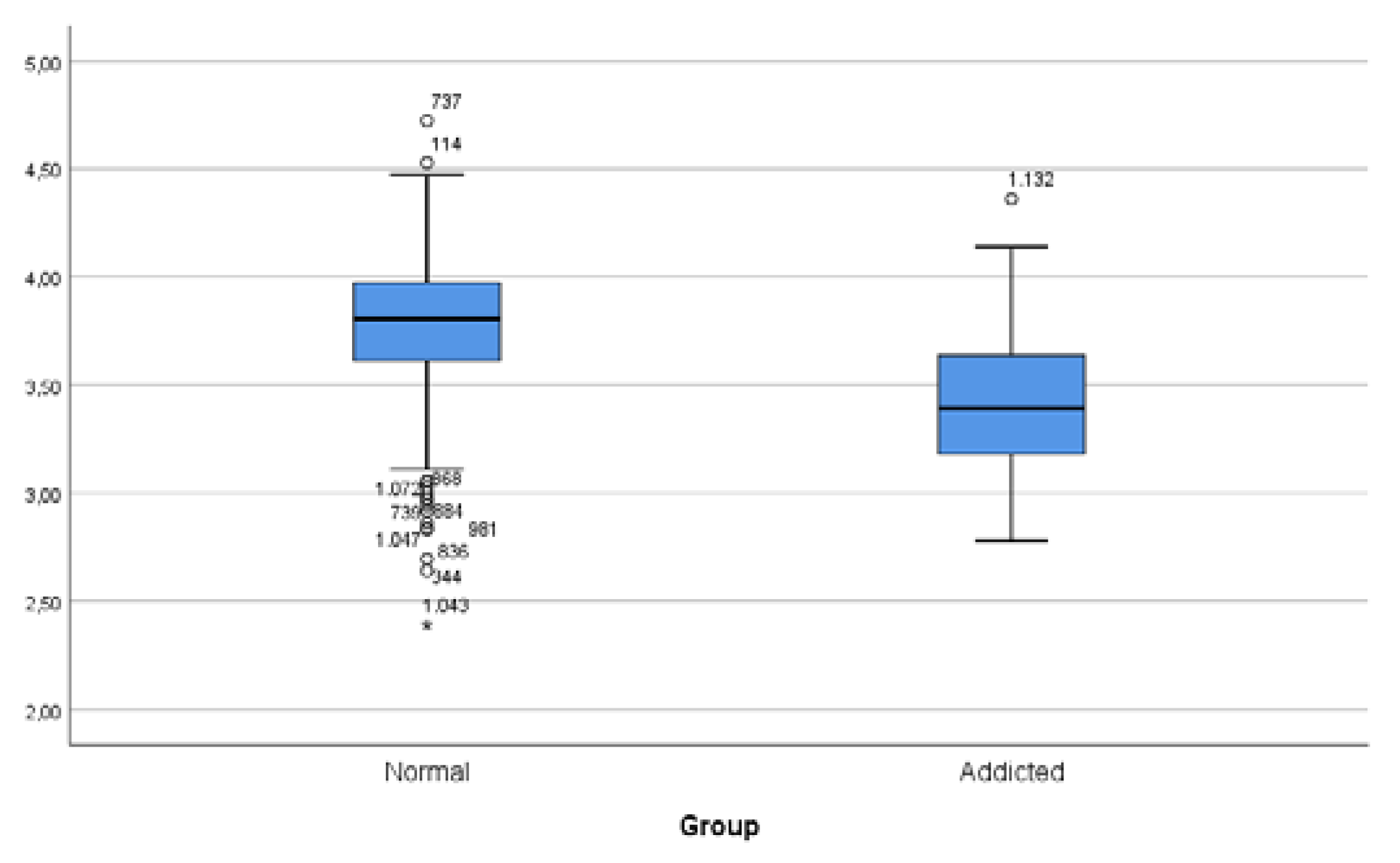
The normal and addicted groups were taken as reference while performing the statistical analysis. In the first stage, the scale scores of the total of the normal group and the total of the addicted group were compared with the independent group t-test, and the result was found to be significant (t=7,81; p<,001). It was revealed that the addicted group’s harm perception was lower than the normal group (X=3,43). The effect size of the difference between the addicted group and the normal group was evaluated with Cohen’s d effect size calculation, taking into account the scale scores. Accordingly, the normal group was found to be in a higher impact area in terms of harm perception compared to the addicted group (d=1,43; >0,8). In addition, when the difference between the two groups according to gender was examined, the number of men and women was found to be suitable for the normal group statistically. In the independent group t-test calculations, there was no difference according to gender (t=1,55; p>,005). In the addicted group, no comparison was made since the number of women was less than 30.
Figure 4.
USHPS Scale Scores of the groups (The cut-off value was accepted as 2.5.).
The difference between the groups and the effect size were analyzed in the comparison of the USHPS scale scores of the normal and addicted groups for harmful substance use (Table 8).
For USHPS score comparisons, three categories within the normal group were compared with one-way Anova analysis and the difference between groups was found to be significant (p<0.001). When the difference between the groups was examined by LSD analysis, the harm perception of the group that replied “never use” was found to be the highest compared to the other groups. The harm perception score of the group with “tobacco, alcohol and substance use” was found to be the lowest compared to the other two groups (X=3,51). The difference in the three categories within the normal group was also examined by Cohen's d effect size calculation. The group that never used harmful substances was found to be in a higher effect area compared to the group that “uses tobacco, alcohol and substance” (d=1,02; >0,8). The group that never used was slightly above the weak effect area and at the border of the medium effect area compared to the “only tobacco use” group (d=0,28; >0,2<0,5). The “only tobacco use” group included in the normal group was found to be in the medium effect area compared to the “tobacco, alcohol and substance use” group (d=0,69; >0,5). Lastly, the “tobacco, alcohol and substance use” group in the normal group and the addicted group (tobacco, alcohol and substance use) were compared with the independent group t-test, and no difference was found (p>0.05). According to the effect size calculation, the effect area of the group using more harmful substances in the normal group was slightly above the low effect compared to the addicted group using the same type of harmful substances” (d=0,24; >0,2<0,5). This shows that there is not much difference in the harm perception between the normal and addicted groups, where the use of harmful substances is most intense.
3.5. Criterion Validity of Scales
Since the USRAS and USHPS scales were thought to be related, the Pearson Correlation (r) correlation coefficient of these two scales was calculated for criterion validity. As expected, a relationship was found between the USRAS scale and the USHPS scale. As in Table 9, it is seen that this relationship is of medium strength and this relationship is significant (r=,54; p<0,001).
4. Conclusions
The prevalence of alcohol and substance addiction in Turkey as well as all over the world necessitated the review of current rehabilitation studies on the subject and the discovery of new standards. It is very important to include new perspectives, including self-awareness in the treatment process for addicted individuals to stay away from harmful substances for life. Psychometric scales constitute a part of these processes based on concrete data. Since the scales developed according to the biopsychosocial model perspective are multidimensional, they are used in the addiction treatment process, thus, the self-awareness of the person is also activated.
In this study, two psychometric scales named “Uskudar Result Awareness Scale” (USRAS) and “Uskudar Harm Perception Scale” (USHPS) were developed using a data set of 1134 people, consisting of normal and addicted individuals aged 18 and over. In addition, for both scales, a model was created from factor structures using the AMOS program in the data set of 400 people (normal group + addicted group), and acceptable goodness-of-fit values were obtained by confirming the model with confirmatory factor analysis. Accordingly, USRAS, consisting of 25 items and 6 factors, explained 58,49% of the total variance. The internal consistency reliability Cronbach Alpha value was found to be ,72 in the total scale. The USHPS scale consisted of 36 items and 10 factors and explained 56,36% of the total variance. The internal consistency reliability Cronbach Alpha value was found to be ,83 in the total scale.
In the first measurement performed in the study, the USRAS scale score of the sample of 1134 people was found to be 3,81 points for the normal group and 3,20 points for the addicted group. Evaluation score ranges of the scale were calculated using the equal spacing technique, taking into account that at least 1 and maximum 5 for each item (paying attention to the items to be reverse coded). According to this; between 25-58 points is evaluated as “Low Result Awareness”; between 59-89 points is evaluated as “Medium Result Awareness”; between 90-125 points is evaluated as “High Result Awareness”. As a result of multiplying the scores obtained by dividing 25 by 25 in the study, the result awareness of the normal group was moderate (X=95,25). It was found that the addicted group had a low result awareness (X=80,00). According to Cohen d calculations, the effect size of the difference between the two groups was found to be high (d=1,45; >0,8). Since the addicted group consisted mostly of men and the total number was not high (n=43) in the study, the difference between men and women could not be analyzed statistically. However, there was no difference between men and women in the normal group.
In USHPS measurements, the score of the normal group was found to be 3.,8, and the score of the addicted group was found to be 3,43. Evaluation score ranges of the scale were calculated using the equal spacing technique, taking into account that at least 1 and maximum 5 for each item (paying attention to the items to be reverse coded). According to this; between 36-83 points is evaluated as “Low harm perception/very high risk”; between 84-132 points is evaluated as “Moderate harm perception/moderate risk”; between 133-180 points is evaluated as “High harm perception/low risk”. As a result of multiplying the scores obtained by dividing 36 by 36 in the study, the harm perception of the normal group was found high and inthe low-risk group (X=136,08); the harm perception of the addicted group was found in the moderate risk group (X=123,48). According to Cohen d calculations, the effect size of the difference between the two groups was found to be high (d=1,43; >0,8).
Finally, according to the results obtained for the normal group in the triple category (1: Never use, 2: Only tobacco use, 3: Tobacco, alcohol and substance use), the result awareness and harm perception decreased as the use of harmful substances increased. The group that does not use any of them has the highest awareness of consequences and perception of harm, followed by the group that only use tobacco. The group that uses tobacco, alcohol and substances has the lowest levels of result awareness and harm perception. The addicted group is comprised of the group that currently uses tobacco, alcohol, and substances, and is in any case at a low level in terms of result awareness and harm perception compared to the normal group. Validity and reliability studies and fit index values of the two scales developed in the study were found acceptable. The strengths of the study are that the scales were developed in a study group that included normal and addicted groups and that their usability was tested by giving functional results in the first comparisons. On the other hand, there is a need to expand the study by ensuring the proportionality of the number of men and women among addicted groups and with larger samples where the number of alcohol addicts and substance addicts is also higher. The potential of testing the effectiveness of the scales by including the scales in the process and creating new standardizations in rehabilitation studies and creating self-awareness should not be ignored.
In summary, this study proved that these scales are capable of measuring and evaluating whether people “know the natural consequences of their actions or whether they realize that they are living harmful and dangerous” with their sub-dimensions, by comparison with healthy control in this study. Thus, it determines the low-medium-high risk sub-dimensions and offers a target-determining feature in personalized treatment and rehabilitation. When the treatment or rehabilitation is finished, measuring the level again will give us the treatment output.
References
- Derin, G.; Okudan, M.; Aşıcıoğlu, F., Family Risk Factors in Alcohol and Substance Use Disorders. In Family Psychopathology, 1 ed.; Öztürk, E., Ed. Türkiye Clinics: Ankara, Turkey, 2021; pp 118-126.
- Coşkunol, H., Addictive Substances and Substance Use Patterns. In Basic and Clinical Psychiatry, Karamustafalıoğlu, K., Ed. Gunes Medical Bookstores: Ankara, Turkey, 2018; pp 581-4.
- Jaffe, j.; Anthony, j., Substance-related disorders: Introduction and overview. In Kaplan and Sadock's Comprehensive Texbook of Psychiatry, 8 ed.; Sadock, B.; Ruiz, P.; VA., S., Eds. Lippincott Williams and Wilkins: 2015; pp 1137-67.
- Asicioglu, F., New Psycho-Active Substances: The Legal Procedure Used in European Union Countries and Turkey. Klin Psikofarmakol B 2010, 20 (4), 334-339. [CrossRef]
- Bahadır, E.; Güneş, F.; Noyan, C., The Effect of Distress Tolerance to the Process on Substance Use in Individuals with Substance Use Disorders Journal of Dependence 2019, 20 (4), 214-223.
- Koçak, D.; Hotun Şahin, N.; Büyükkayacı Duman, N., Alcohol and Smoking Addiction, Its Effects on Women's Health and Nursing Interventions. Journal of literature symposium 2015, 1 (5), 43-7.
- Öztürk, Y.; Kırlıoğlu, M.; Kıraç, R., Risk Factors in Alcoholism and Substance Abuse. Journal of Selcuk University Vocational School of Social Sciences 2015, 18 (2), 97-118.
- Akfert, S.; Çakıcı, E.; Çakıcı, M., Cigarette and alcohol use among university students and its relationship with family problems Anatolian Journal of Psychiatry 2019, 10 (40), 40-7.
- Tarhan, N.; Nurmedov, S., Addiction: Coping with virtual or real addiction. Timaş Publishing: Istanbul, Turkey, 2019.
- Neger, E. N.; Prinz, R. J., Interventions to address parenting and parental substance abuse: Conceptual and methodological considerations. Clin Psychol Rev 2015, 39, 71-82. [CrossRef]
- Hernandez, L.; Rodriguez, A. M.; Spirito, A., Brief Family-Based Intervention for Substance Abusing Adolescents. Child Adol Psych Cl 2015, 24 (3), 585-99. [CrossRef]
- Hogue, A.; Liddle, H. A., Family-based preventive intervention: An approach to preventing substance use and antisocial behavior. Am J Orthopsychiat 1999, 69 (3), 278-293. [CrossRef]
- Ekinci, S.; Kural, H.; Yalçınay, M., The level of anger in patients with substance dependence; Its relationship with addiction profile, depression and anxiety level. Journal of Dependence 2016, 17 (1), 12-17.
- Küçükerdönmez, Ö.; Urhan, M.; Köksal, E., Association of appetite, nutritional status and quality of life in alcohol and substance abusers. Journal of Nutrition and Diet 2018, 46 (2), 147-156.
- Asan, Ö.; Tıkır, B.; Okay, İ.; Göka, E., Sociodemographic and clinical features of patients with alcohol and substance use disorders in a specialized unit. Journal of Dependence 2015, 16 (1), 1-8.
- Arıkan, Z.; Genç, Y.; Etik, Ç.; Aslan, S.; Parlak, İ., Labeling of patients and their relatives in alcohol and other substance addictions. Journal of Dependence 2004, 5 (2), 3-7.
- Erükçü Akbaş, G.; Mutlu, E., Addiction and treatment experiences of people receiving substance abuse treatment. Journal of community and social work 2016, 27 (1), 101-122.
- Köknel, Ö., Addiction. Altın Kitaplar Publishing: Istanbul, Turkey, 1998.
- Ögel, K., Approach and Treatment of Substance Abuses. IQ Culture Art Publishing: Istanbul, Turkey, 2001.
- Sevin, Ç.; Erbay, E., Problems of substance addicts in social life after treatment and social work practices. journal of Dependence 2008, 9 (1), 36-41.
- Saatçioğlu, Ö.; Evren, E.; Çakmak, D., Evaluation of alcohol and substance use cases receiving inpatient treatment between 1998-2002. Journal of Dependence 2003, 4 (3), 109-117.
- Yılmaz, A.; Can, Y.; Bozkurt, M.; Evren, C., Remission and relapse in alcohol and substance addiction. Current Approaches in Psychiatry 2014, 6 (3), 243-256. [CrossRef]
- Gordon, A. J.; Zrull, M., Social networks and recovery: one year after inpatient treatment. J Subst Abuse Treat 1991, 8 (3), 143-152. [CrossRef]
- Walton, M. A.; Castro, F. G.; Barrington, E. H., The role of attributions in abstinence, lapse, and relapse following substance abuse treatment. Addict Behav 1994, 19 (3), 319-331. [CrossRef]
- Irvin, J. E.; Bowers, C. A.; Dunn, M. E.; Wang, M. C., Efficacy of relapse prevention: a meta-analytic review. J Consult Clin Psychol 1999, 67 (4), 563-570.
- Schuckit, M., Goals of Treatment. In Textbook of Substance Abuse Treatment, Galanter, M.; Kleber, H., Eds. American Psychiatric Press: 1994; pp 3-10.
- Evren, C.; Durkaya, M.; Dalbudak, E.; Çelik, S.; Çetin, R.; Çakmak, D., Factors related with relapse in male alcohol dependents: 12 months follow-up study. Dusunen Adam The Journal of Psychiatry and Neurological Sciences 2010, 23 (2), 92-99. [CrossRef]
- Donovan, D., Assesment issues and domains in the prediction of relapse. Addiction 1996, 91 (suppl), 29-36.
- Brownell, K. D.; Marlatt, G. A.; Lichtenstein, E.; Wilson, G. T., Understanding and preventing relapse. Am Psychol 1986, 41 (7), 765-782.
- Tarhan, N., Positive psychology and psychotherapy in addiction. In Addiction diagnosis and treatment essential book, Dilbaz, N.; Göğcegöz, I.; Noyan, C. O.; Kazan Kızılkurt, Ö., Eds. Nobel Medical Bookstores: 2021; p 419.
- Seligman, M. E. P.; Peterson, C., Positive clinical psychology. In A psychology of human strengths: Fundamental questions and future directions for a positive psychology Aspinwall, L. G.; Staudinger, U. M., Eds. American Psychological Association: 2003; pp 305-317.
- Donaldson, S. I.; Dollwet, M.; Rao, M. A., Happiness, excellence, and optimal human functioning revisited: Examining the peer-reviewed literature linked to positive psychology. The Journal of Positive Psychology 2015, 10, 185-195. [CrossRef]
- Kern, M. L.; Williams, P.; Spong, C.; Colla, R.; Sharma, K.; Downie, A.; Taylor, J. A.; Sharp, S.; Siokou, C.; Oades, L. G., Systems informed positive psychology. The Journal of Positive Psychology 2019, 15 (4), 1-11.
- Seligman, M. E., Positive psychology: A personal history. Annual review of clinical psychology 2019, 15, 1-23.
- Seligman, M. E., Flourish. Simon & Schuster: 2011.
- Çatak, P. D.; Ögel, K., Mindfulness as a Therapy Method. Neuropsychiatry Archive 2010a, 47, 69-73.
- Çatak, P. D.; Ögel, K., Mindfulness-based therapies and therapeutic processes. Clinical Psychiatry 2010b, 13, 85-91.
- Brown, K. W.; Ryan, R. M., The benefits of being present: mindfulness and its role in psychological well-being. Journal of personality and social psychology 2003, 84 (4), 822. [CrossRef]
- Tırışkan, M.; Onnar, N.; Çetin, Y. A.; Cömert, I. T., The importance of conscious awareness in preventing relapse in substance abuse: A review study. Addicta: The Turkish Journal on Addictions 2015, 2 (2), 123-142.
- Köknel, Ö., Alcohol and substance abuse subculture. Journal of Dependence 2001, 2 (2), 71-76.
- Yurtsever, B.; Arabacı Baysan, L., Validity and reliability of the substance awareness scale and the substance addiction knowledge test among adults. Fenerbahce University Journal of Health Sciences 2021, 1 (3), 206-225.
- Özay Köse, E.; Gül, Ş., The substance addiction awareness scale: A study of the validity and reliability. Inonu University Journal of the Faculty of Education 2018, 19 (3), 41-56.
- Ünal Demir, F.; Akpınar Aslan, E.; Batmaz, S.; Çelikbaş, Z.; Hızlı Sayar, G.; Ünübol, H., Levels of awareness, negative attitudes and stigma towards addictions of university students using smoking, alcohol, or substances Journal of Dependence 2022, 23 (1), 86-94.
- Verdejo-García, A.; Pérez-García, M., Substance abusers' self-awareness of the neurobehavioral consequences of addiction. Psychiatry Research 2008, 158 (2), 172-180. [CrossRef]
- Price, C. J.; Wells, E. A.; Donovan, D. M.; Rue, T., Mindful awareness in body-oriented therapy as an adjunct to women's substance use disorder treatment: A pilot feasibility study. J Subst Abuse Treat. 2012, 43 (1), 94-107.
- Estévez, A.; Jáureguı, P.; Sánchez-Marcos, I.; López-González, H.; Griffiths, M. D., Attachment and emotion regulation in substance addictions and behavioral addictions Journal of Behavioral Addictions 2017, 6 (4), 534-544.
- Pragnesh, P., Knowledge and Awareness Regarding Substance Addiction Among Medical Students of Valsad, Gujarat. Forensic Sci Add Res. 2018, 4 (1), 305-307.
- Valdés-Sánchez, N.; Díaz, R.; Quevedo, Y.; Arriagada, L.; Borzutzky, A.; Schilkrut, R., Construction and Validation of the Inventory of Addiction Awareness (ICE-A) International Journal of Mental Health and Addiction 2020, 18, 314-327.
- Tavşancıl, E.; Aslan, A. E., Content analysis and application examples for oral, written and other materials. Epsilon 2001.
- Büyüköztürk, Ş., Manual of data analysis for social sciences. Pegem Citation Index: 2018.
- Kalaycı, Ş., SPSS applied multivariate statistical techniques (Vol. 5). Asil Publishing: Istanbul, Turkey, 2010.
- Sharma, S., Applied Multivariate Techniques. John Wiley&Sons Inc: 1996.
- Tinsley, H.; Tinsley, D., Uses of factor analysis in counseling psychology research. J Couns Psychol. 1987, 34 (4), 414-424.
- Cohen, J., Statistical power analysis fort he behavioral sciences 2ed.; Erlbaum: 1988.
Table 2.
USRAS Item Factor Loads, Item Total Correlations and Cronbach Alpha Values.
|
Factor |
New Item Nu. |
Items | Factor Load | Item Total Correlation |
Cronbach Alpha |
|---|---|---|---|---|---|
|
F1 |
1 | Q6: I like the saying “Learn from the past, live in the present, look to the future”. | ,76 | ,44 | ,82 |
| 2 | Q11: It is good to think long term and I try to do that. | ,75 | ,48 | ||
| 3 | Q26: When I make a wrong decision, I go back and reevaluate. | ,73 | ,40 | ||
| 4 | Q3: It is always necessary to wait and be patient in order to reach a goal. | ,73 | ,38 | ||
| 5 | Q12: It is very important to be disciplined and to provide standards in life. | ,70 | ,41 | ||
| 6 | Q28: The most important thing that gives meaning to my life is the true meaning of death and the belief in eternity. | ,62 | ,33 | ||
| 7 | Q5: When I make a decision, I think 5-10 years ahead. | ,56 | ,30 | ||
| F2 | 8 | Q18: It is good to do hard work, but it is not for me. | ,80 | ,38 | ,80 |
| 9 | Q19: I am the type who cannot be bothered. | ,69 | ,43 | ||
| 10 | Q15: Getting pleasure is the important thing for me, hard work is not for me. | ,65 | ,42 | ||
| 11 | Q23: It is good to be principled and systematic, but it is not for me. | ,63 | ,30 | ||
| F3 | 12 | Q24: If there is an adventure, I forget almost everything. | ,86 | ,63 | ,82 |
| 13 | Q25: If there is a surprise, I will do it without thinking about the end. | ,82 | ,53 | ||
| 14 | Q23: If there is something different and attractive, I do it without thinking. | ,80 | ,51 | ||
| 15 | Q27: The purpose of life is to live in my own way. | ,50 | ,34 | ||
| F4 | 16 | Q2: People usually say I am in a hurry. | ,86 | ,47 | ,70 |
| 17 | Q31: I am known to be hasty and impatient, but I do not like this situation. | ,75 | ,36 | ||
| 18 | Q1: Getting what I want right away is very important to me. | ,71 | ,40 | ||
| F5 | 19 | Q4: If the problem is not resolved at home or in any case; alcohol, substance, or anything that gives pleasure suits me. | ,74 | ,30 | ,73 |
| 20 | Q34: When I cannot solve problems, I immediately turn to something that gives pleasure. | ,66 | ,51 | ||
| 21 | Q35: Hedonism does not end well, but I cannot give up on pleasurable things. | ,58 | ,43 | ||
| 22 | Q16: I find it difficult to express my feelings and turn to something that gives me pleasure. | ,52 | ,39 | ||
| F6 | 23 | Q29: My happiness is important instead of someone else’s happiness. | ,76 | ,31 | ,67 |
| 24 | Q8: My well-being and my own future come before the well-being of my family. | ,68 | ,30 | ||
| 25 | Q30: Those who say “The meaning of life; you have to be selfish to be happy after all.” are right. | ,65 | ,30 | ||
| Total | ,72 |
* As a result of the EFA, the USRAS scale form, consisting of 25 items and 6 factors, was rated in a 5-point Likert type as “Strongly disagree”, “Disagree”, “Neither/Nor Agree”, “Agree” and “Strongly agree”. A minimum of “1” and a maximum of “5” points can be taken from each item, and there are items that need to be scored in reverse. (According to “New Item Number”: 8,9,10,12,13,14,15,16,18,19,20,21,22,23,24,25).
Table 3.
USRAS Average Scale Scores of the Groups.
| Groups | X | SS | d |
|---|---|---|---|
| Normal Female (n=882) | 3,83 | ,42 | |
| Normal Male (n=193) | 3,76 | ,45 | |
| Normal Total (n=1075) | 3,81 | ,42 |
1,45ab |
| Addicted Female (n=6) | 3,07 | ,41 | |
| Addicted Male (n=37) | 3,22 | ,43 | |
| Addicted Total (n=43) | 3,20 | ,42 |
The range of points that can be obtained is between 1 and 5.aNormal reference group is calculated as total X1-X2/SDNormal bAddicted reference group is calculated as total X1-X2/SDAddicted.
Table 4.
USRAS Scale Scores by Harmful Substance Use.
| Groups | X | SS | d |
|---|---|---|---|
| Normala “Never Use” (n=767) | 3,85 | ,41 | 0,82ac; 0,24ab; 0,59bc 0,57cd |
| Normalb “Only Tobacco Use” (n=214) | 3,75 | ,42 | |
| Normalc “Tobacco +Alcohol + Substance Use” (n=53) | 3,47 | ,51 | |
| Normal Total (n=1034) | 3,81 | ,42 | |
| Addictedd “Tobacco +Alcohol + Substance Use” (n=43) | 3,20 | ,42 | |
| Addicted Total (n=43) | 3,20 | ,42 |
The range of points that can be obtained is between 1 and 5.cNormal reference group is calculated as “Tobacco+ Alcohol + Substance Use” X1-X2/SDNormal cAddicted reference group is calculated as “Tobacco+ Alcohol + Substance Use” X1-X2/SDAddicted.
Table 6.
USHPS Item Factor Loads, Item Total Correlations and Cronbach Alpha Values.
|
Factor |
New Item Nu. |
Items | Factor Load | Item Total Correlation |
Cronbach Alpha |
|---|---|---|---|---|---|
|
F1 |
1 | Q31: My habits take up most of my time and my thoughts, but I am determined to complete them. | ,68 | ,34 | ,74 |
| 2 | Q44: I want to be careful, planned and act with the end in mind, but I cannot. | ,68 | ,44 | ||
| 3 | Q43: I do something that is harmful to me, and then I regret it. | ,68 | ,32 | ||
| 4 | Q30: My bad habits affect my health from time to time, I try to curb them. | ,67 | ,40 | ||
| 5 | Q25: I cannot plan; I got into a lot of trouble because of being hasty and impatient. | ,55 | ,41 | ||
| 6 | Q28: People say that I make a quick decision and act without thinking about the end, but I try hard to fix this. | ,55 | ,35 | ||
| F2 | 7 | Q8: Alcohol or drugs can be used for curiosity. | ,66 | ,33 | ,68 |
| 8 | Q29: I think pleasurable substances such as alcohol and drugs are harmless when taken in small amounts. | ,63 | ,43 | ||
| 9 | Q15: I think life is empty if there is no excitement, pleasure, and enjoyable alcohol substance. | ,58 | ,33 | ||
| 10 | Q10: When I feel troubled and distressed, the first thing that comes to my mind is to drink or seek something pleasant. | ,58 | ,57 | ||
| 11 | Q11: I do not think about the end when I am in a bad mood, I turn to whatever gives me pleasure. | ,55 | ,73 | ||
| F3 | 12 | Q18: It is very wrong to say that “Using tobacco and alcohol is a symbol of masculinity”. | ,65 | ,35 | ,82 |
| 13 | Q26: It is necessary not to drive in traffic, if it is very dangerous. I mostly achieve this. | ,63 | ,37 | ||
| 14 | Q24: I find social activities related to bad habits correct. | ,61 | ,62 | ||
| 15 | Q12: I think it is harmful to relax by drinking or taking something at that moment. | ,55 | ,71 | ||
| 16 | Q23: I do not want my children to use alcohol even if I use it. | ,54 | ,63 | ||
| F4 | 17 | Q5: Being curious often got me in trouble. | ,74 | ,33 | ,77 |
| 18 | Q7: I cannot control my curiosity, it has become a habit, it is harmful. | ,70 | ,65 | ||
| 19 | Q6: Curiosity is what drives me the most. | ,70 | ,63 | ||
| F5 | 20 | Q34: I get very bad if I do not drink alcohol or use substance. | ,83 | ,84 | ,70 |
| 21 | Q36: I cannot sleep if I do not drink alcohol or use substance. | ,81 | ,44 | ||
| 22 | Q41: Even though I know that it hurts me, I cannot get away from exciting and pleasurable substances. | ,53 | ,36 | ||
| F6 | 23 | Q2: For me, the more excitement, the more success. I do not think it does any harm. | ,83 | ,61 | ,82 |
| 24 | Q1: I think, “Life has no meaning, if there is no excitement”. | ,82 | ,53 | ||
| F7 | 25 | Q17: The rule of “First my interest, then my close circle.” is always valid. | ,78 | ,60 | ,76 |
| 26 | Q39: I think a person who does not think of his/her own interest first is an idiot. | ,76 | ,42 | ||
| 27 | Q4: I say “First me, then others”. I live by my mind. | ,60 | ,39 | ||
| F8 | 28 | Q14: When I am not happy, I do not feel incomplete, I can somehow relax myself. | ,74 | ,40 | ,86 |
| 29 | Q9: There are not many times in my life when I feel troubled and sad. | ,69 | ,80 | ||
| 30 | Q37: No matter what anyone says, I am a special and important person, I like myself. | ,50 | ,70 | ||
| 31 | Q16: It is very pleasant to do things that satisfy me, but I think you have to put up with the trouble. | ,50 | ,32 | ||
| F9 | 32 | Q32: I adjust the dose of alcohol or substance, I use it in a controlled manner. | ,77 | ,62 | ,80 |
| 33 | Q40: I am not addicted, I quit whenever I want. | ,76 | ,40 | ||
| F10 | 34 | Q20: I do not think it is harmful to eat a lot, drive dangerously or live fast. | ,65 | ,33 | ,78 |
| 35 | Q42: No need to think about harmful or dangerous situations, nothing will happen to me. | ,54 | ,65 | ||
| 36 | Q27: I cannot read or work for a long time. | ,50 | ,32 | ||
| Total | ,83 |
* * As a result of the EFA, the USHPS scale form, consisting of 36 items and 10 factors, was rated in a 5-point Likert type as “Strongly disagree”, “Disagree”, “Neither/Nor Agree”, “Agree” and “Strongly agree”. A minimum of “1” and a maximum of “5” points can be taken from each item, and there are items that need to be scored in reverse. (According to “New Item Number”: 5,7,8,9,10,11,17,18,20,21,22,23,24,25,26,27,30,32,33,34,35,36).
Table 7.
USHPS Average Scale Scores of the Groups.
| Groups | X | SS | d |
|---|---|---|---|
| Normal Female (n=882) | 3,78 | ,27 | |
| Normal Male (n=193) | 3,75 | ,30 | |
| Normal Total (n=1075) | 3,78 | ,28 |
1,43ab |
| Addicted Female (n=6) | 3,34 | ,38 | |
| Addicted Male (n=37) | 3,45 | ,33 | |
| Addicted Total (n=43) | 3,43 | ,33 |
The range of points that can be obtained is between 1 and 5.aNormal reference group is calculated as total X1-X2/SDNormal bAddicted reference group is calculated as total X1-X2/SDAddicted.
Table 8.
USHPS Scale Scores by Harmful Substance Use.
| Groups | X | SS | d |
|---|---|---|---|
| Normala “Never Use” (n=767) | 3,81 | ,25 | 1,02ac; 0,28ab; 0,69bc 0,24cd |
| Normalb “Only Tobacco Use” (n=214) | 3,73 | ,30 | |
| Normalc “Tobacco + Alcohol + Substance Use” (n=53) | 3,51 | ,33 | |
| Normal Total (n=1034) | 3,78 | ,28 | |
| Addictedd “Tobacco+ Alcohol + Substance Use” (n=43) | 3,43 | ,33 | |
| Addicted Total (n=43) | 3,43 | ,33 |
The range of points that can be obtained is between 1 and 5.cNormal reference group is calculated as “Tobacco+ Alcohol + Substance Use” X1-X2/SDNormal cAddicted reference group is calculated as “Tobacco+ Alcohol + Substance Use” X1-X2/SDAddicted.
Table 9.
Pearson Correlation Values of Scales.
| Scales | N | X | r | p |
|---|---|---|---|---|
| USRAS &USHPS | 1134 | 3,79 | ,54 | ,000 |
| 1134 | 3,76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



