
Submitted:
12 April 2023
Posted:
13 April 2023
You are already at the latest version
Abstract
Abstract: (1) Background: existing treatment methods for neglect are concentrated on egocentric neglect and lead to various problems, such as cost/space constraints and portability. Therefore, this study seeks to determine how treatment (a.k.a., Twins Therapy, TT) can improve an existing problem in relation to neglect in stroke patients; (2) Method: The research design was a pre-post test control group design and both groups maintained existing rehabilitation treatment and added TT intervention only to the experimental group. TT intervention was conducted for a total of 20 sessions (1 session 30 min/day, 5 days/week for 4 weeks); (3) Result: as a result of comparison be-fore and after the TT intervention, there was no significant difference in MFT and MBI items (p>.05). However, the score and execution time of the Apple Cancellation Test showed significant reduction only in the experimental group (p<.05); (4) Conclusion: as a result of the study, TT im-proved not only egocentric neglect, but also allocentric neglect symptoms in stroke patients
Keywords:
Egocentric neglect
; Allocentric neglect
; Stroke
; Rehabilitation
; Twins Therapy
1. Introduction
Neglect is described as a lack of spatial attention and is a symptom of impaired perception, attention and behavior in the opposite space of the damaged cerebral hemisphere despite no sensory damage [1,2,3]. Neglect is caused by various pathological conditions, especially after cerebral infarction or cerebral hemorrhage [2]. The incidence of neglect is more common in stroke patients in the right cerebral hemisphere than in stroke patients in the left cerebral hemisphere [3]. Symptoms of neglect caused by right cerebral hemisphere lesions mainly include neglect of the left space, impaired concentration and restriction of behavior on the transverse plane [4]. Limitation of response to the neglect aspect negatively affects body balance, functional ability such as walkin and activities of daily living [5].
Neglect is classified into two types, depending on how objects are recognized: egocentric neglect (or viewer-centered neglect) and allocentric neglect (or object-centered neglect). Egocentric neglect is associated with dorsal visual pathways [7] and shows a defect in the ability to recognize objects or body parts, such as the head, trunk and arms, on the left side of the patient's midline [1]. In contrast, allocentric neglect is associated with ventral visual pathways [7] and has a defect in the ability to perceive the left side as the center of an object, regardless of the location of the object [1].
Various methods have been introduced to treat such various symptoms and types of neglect [8,9,10,11,12,13]. First, Pierce et al (2002) classified the treatment methods for neglect into three main categories as follows [8]: 1) treatments targeting arousal deficits; 2) treatments targeting deficient visual attention; and 3) treatments targeting spatial representation deficits. The treatments targeting arousal deficits approach is a method of using drugs, such as anti-dopamine, to treat neglect [8]. The treatments targeting deficient visual attention approach uses a computer-based scanning program to increase attention to the patient's space and the treatments targeting spatial representation deficits approach uses prism and trunk rotation to help reconstruct the neglected space that the patient is seeing [8]. On the other hand, Barrett et al (2006) classified the treatment methods into two main categories [9]. The first classification includes the top-down and bottom-up approaches [9]. Top-down approach is scanning training, which uses tactile and visual assist devices to urge patients to turn their bodies around and look at the left-hand space [9]. The bottom-up approach is a method that is attempted to enhance or rearrange the characteristics of perceived information by stimulating the negated hemispace by frequently viewing it [9]. The second classification includes the endogenous and exogenous approaches. The endogenous approach is a method to increase the tendency to view the left space without special equipment, such as limb activation therapy and the exogenous approach is a method of inducing dynamic remapping by using special equipment such as prism lenses [9]. Finally, a treatment method by using virtual reality has been announced recently [10]. Virtual reality therapy has no spatial constraints and can improve activities of daily living and spatial attention concentration even in chronic patients [11]. However, majority of treatment methods are concentrated on egocentric neglect and studies separating egocentric neglect and allocentric neglect are insufficient [12].
On the other hand, neglect evaluation is mainly divided into a pencil-paper test, behavioral assessment, clinical observation and virtual reality assessment [13]. However, existing evaluation methods are mainly targeting egocentric neglect and it is insufficient to address other types of neglect [14]. For this reason, existing treatment methods are concentrated in the treatment for egocentric neglect, like prism treatment, transcutaneous electrical nerve stimulation (TENS), optokinetic stimulation (OKS), etc. [15,16,17]. Moreover, the study of Turgut et al (2018) mentioned the need to distinguish between egocentric neglect and allocentric neglect treatments because existing treatments, such as prism treatment and cueing paradigm training, have only been verified to improve egocentric neglect [18]. Accordingly, as a result of previous studies on differential diagnosis, the evaluation method mainly used an apple cancellation test that can distinguish between egocentric neglect and allocentric neglect [19], and the treatment method mainly used a virtual reality navigation task (VRNT) [20] and repetitive transcranial magnetic stimulation (rTMS) [21]. Research shows that treatment using VR helps re-identify space and improves concentration, and rTMS is effective not only for egocentric neglect, but also for allocentric neglect [21,22]. However, existing treatment methods lead to cost problems due to the use of expensive equipment [23]. In addition, it has both spatial constraints and portability problems due to the size of the equipment [23].
Therefore, in this study, through a new treatment (Twins Therapy, TT) that improved existing problems, we attempted to find out how it affects the improvement of symptoms of egocentric neglect and allocentric neglect, upper extremity function and activities of daily living in stroke patients.
2. Materials and Methods
2.1. Participants
This study included 15 people with both egocentric and allocentric neglect due to stroke, and used the Edinburgh Handless Inventory (EHI) to target 15 people with right dominant hands [24]. The participants heard enough explanation about the study and conducted the study after receiving a written consent. The participants were randomly divided into 7 in the experimental group and 8 in the control group through the SPSS 21.0 Version. The research design was based on a pre/post test control group design and the selection criteria for all research participants are as follows: 1) Those who are more than 3 months after the stroke lesion; 2) Those with symptoms of neglect; 3) Those with a score of 24 or higher in MMSE-K; and 4) Those who understand and agree with the purpose of this study. This study was approved by the Kangwon National University Institutional Review Board (KWNUIRB-2021-05-011-003) prior to commencement.
2.2. Materials
2.2.1. Korean version of the Mini-Mental Status Examination (MMSE-K)
MMSE-K is an evaluation tool standardized by Kwon and Park (1989) to use the existing MMSE for the elderly in consideration of educational background [25]. MMSE-K consists of seven items. Out of a total of 30 points, 24 points or more are classified as definite normal, 23~20 points are classified as suspected dementia and 19 points or less are classified as definite dementia. The inter-inspector reliability is .99 [25].
2.2.2. Apple cancellation test
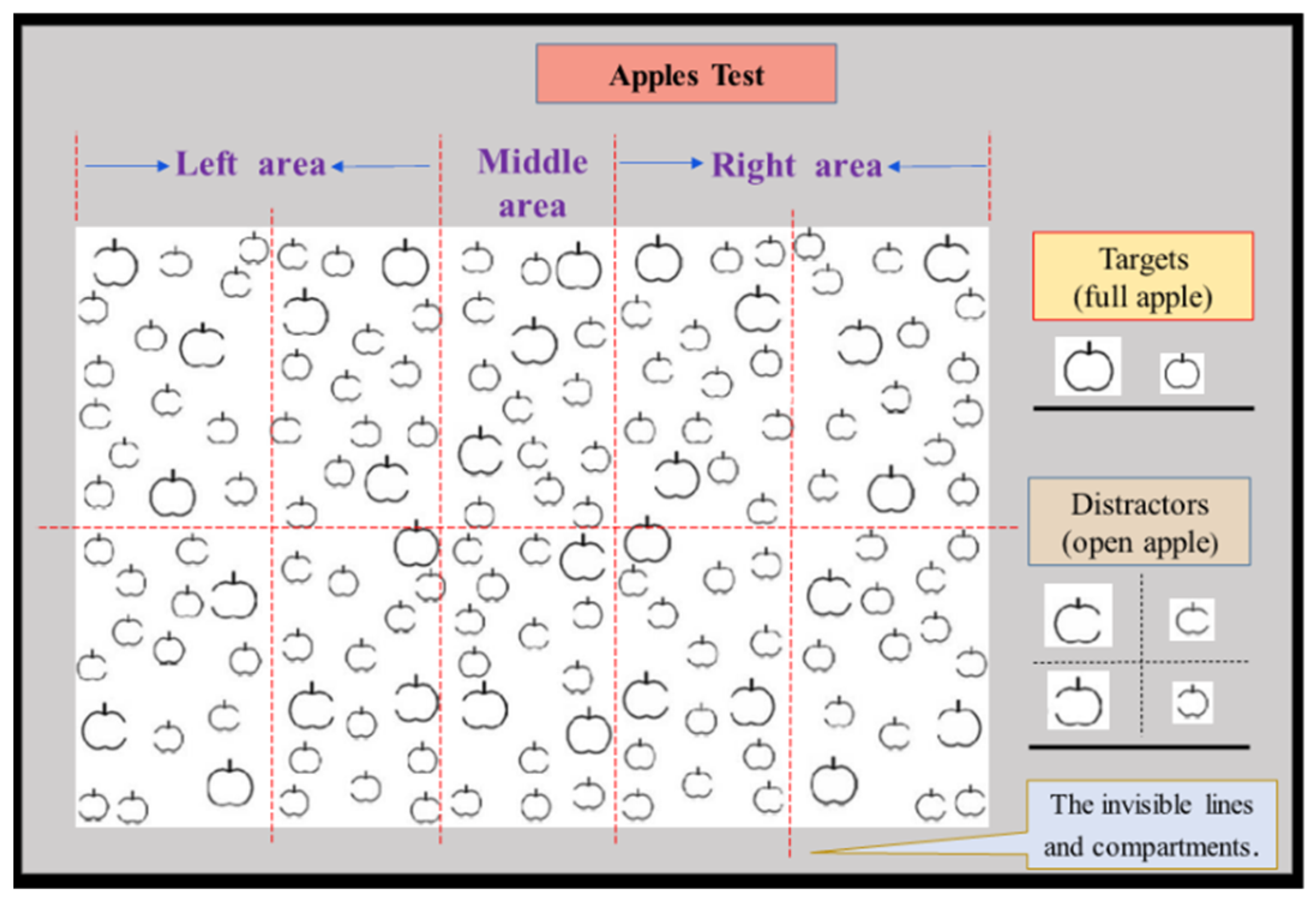
The apple cancellation test was developed by Bickerton et al (2011) to differentiate between egocentric and allocentric neglect. A total of 150 apples are randomly scattered on the test paper. One third of the apples are intact and two-thirds are left or right side open. The test paper is divided into 10 zones (4 on the left, 2 in the middle and 4 on the right) due to two invisible rows and five columns. The participant proceeds by marking only intact apples, regardless of size. Each section contains 15 apples (3 large apples and 12 small apples), of which 5 are correct (1 large apple and 4 small apples). The test lasts up to 5 minutes and has a total score of 50 points. The result of the analysis is that egocentric neglect is divided into left-side egocentric neglect if it is a positive integer and right-side egocentric neglect if it is a negative integer when subtracting the number of intact apples selected from the four areas on the left from the number of intact apples selected in the four areas on the right. Allocentric neglect counts the number of wrong answers (apples with left or right open) in the entire domain (including the middle 2 zones) and when the number of apples with the left open is subtracted from the number of apples with the right open, it is divided into left-side allocentric neglect if it is a positive integer and right-side egocentric neglect if it is a negative integer [19,26]. The cut-off scores are ±2 for egocentric neglect and ±1 for allocentric neglect [23]. In this study, we used separate score and execution time for egocentric and allocentric neglect, and the decrease in score means improvement of symptoms.
Figure 1.
Composition of apple cancellation test.
2.2.3. Manual Function Test
MFT was developed by the Myeongja branch of the Faculty of Medicine, Tohoku University, Japan and is a tool for assessing upper limb function and mobility ability in stroke patients [27]. The MFT consists of 4 items of upper limb movement, 2 items of grip, 2 items of finger manipulation and out of a total of 32 points, each sub-item is awarded 1 point when performed, and 0 points if it is impossible [27].
2.2.4. Korean version of the Modified Barthel Index (K-MBI)
K-MBI is an evaluation tool that was translated and standardized by Jung et al (2007) in 2007 from the MBI (5th edition), published by Shah et al in 1989 [28]. The questions consist of 10 assessment items, can be divided into 7 self-care activities and 3 mobility activities [29]. The scores are divided into 5 levels, with a total of 100 points, with 100 points being completely independent, 99~91 points being minimally dependent, 90~75 points being slightly dependent, 74~50 points being partially dependent, 49~25 points being maximum dependent and 24~0 points being completely dependent [30]
2.3. Procedure
The intervention used in this study was called Twins Therapy (TT), which consists of 7 sheets of A4 paper, each with 45 different pairs of stimuli (pictures, numbers, letters). The training procedure was to position the paper directly in the center of the patient, and then ask to find 15 complete pairs of stimuli (twins) out of 45 pairs of stimuli. Each sheet of paper means one step, consists of a total of seven steps and various stimuli are presented as the level increases. Interventions were conducted for a total of 20 sessions (1 session 30 mins/day, 5 days/week for 4 weeks) (Figure 2). All tests were performed twice, before and after TT training.
2.4. Data Analyses
In this study, the general characteristics of the subjects, such as sex, educational background and injury type were analyzed by using the chi-square test, and the age and duration of onset were analyzed by using the Mann-Whitney U test to determine the mean value and significance level. We used the Mann-Whitney U test for homogeneity between the two groups and the Mann-Whitney U test for the comparison of the amount of change between the two groups, and the Wilcoxon's signed-ranked test for the pre-post comparisons.
3. Results
3.1. General characteristics of the participants
The participants in each group in this study showed no significant differences and the general characteristics were as follows (p>.05) (Table 1).
3.2. Homogeneity test between two groups before training
There was no significant difference in all tests, including the Apple Cancellation Test (p>.05) (Table 2).
3.3. Comparison of test scores between experimental and control groups
In the experimental group, the Apple score (Ego) and Apple score (Allo) were significant (p<.05). However, in the control group, there was no significant difference in all tests (p>.05) (Table 3).
3.4. Comparison of test score variations between experimental and control groups
The comparison of the test score variations showed no significant difference in all items, but there was a greater improvement in the mean value of the experimental group in all items (p>.05) (Table 4).
4. Discussion
Treatment methods for neglect have been combined with cutting-edge technologies, such as virtual reality (VR), transcranial magnetic simulation (TMS) and optic simulation (OKS) [15,16,17]. However, these studies failed to consider various types of neglect and there are spatial constraints due to the size and the high cost of equipment [17,18,19,20,21,22,23,25,26]. Accordingly, this study was conducted to determine how the newly developed therapy, Twins Therapy (TT), affects stroke patients with neglect by improving these shortcomings.
First, the 15 participants in this study showed no significant differences in general characteristics, such as gender, educational background and duration of onset. The homogeneity test also showed no significant difference in all the Apple Cancellation tests, including the egocentric neglect and allocentric neglect tests. Therefore, the two groups are judged to be homogeneous groups with no differences.
Next, pre-post comparisons within the group showed significant differences in both egocentric and allocentric outcomes of the Apple Cancellation Test only in the experimental group. This means that Twins Therapy is effective not only in the treatment of egocentric neglect, but also in the treatment of allocentric neglect. There was no significant difference between the execution time of the Apple Cancellation Test, manual function test (MFT) and the Korean version of the Modified Barthel Index (MBI). However, the execution time of the Apple Cancellation Test, in which about 12 seconds were reduced in the control group, while about 60 seconds were reduced in the experimental group, confirming smoother performance.
Comparisons of the variation of test score for each test item between groups showed no significant difference in all items. However, the variation of test score of all items was higher in the experimental group compared to the control group. In particular, the Apple score (ego), Apple score (allo) and Apple time (sec) showed more changes in the experimental group (ego: 2.85±2.26 points, allo: 4.57±2.29 points), compared to the control group (ego: 2.62±1.76 points, allo: 2.75±2.05 points). Also, the variation of test score in allocentric is higher than in egocentric within the experimental group. This means that TT has a positive effect on neglect, especially in patients with relative allocentric neglect. In addition, in the Korean version of Modified Barthel Index (MBI) category, the experimental group (1.13±1.21points) showed more change than in the control group (0.37±0.74 points). This suggests that TT also has a positive effect on the function of activities of daily living and is expected to result in significant differences in future studies with more participants.
The limitations of this study are as follows. First, it is difficult to generalize due to the small number of participants. Second, the patient's own functional recovery and training effectiveness are not sufficiently distinguished due to the verification of homogeneity before training only once. Third, there is no additional comparison of MBI subdomains or a more detailed comparison analysis of proximal and distal extremity of MFT. Future studies are likely required to improve on these limitations. Nevertheless, this study is significant because the newly developed Twins Therapy provides an opportunity to break free from the limitations of cost and space, which are limitations of conventional therapies. It is also worth noting that it is the world's first pencil & paper training that can simultaneously improve the symptoms of egocentric neglect and the improvement of allocentric neglect, which is still lacking in training methods.
5. Conclusions
This study sought to find out how Twins Therapy affects neglect in stroke patients. As a result, there was a significant difference in improving symptoms of egocentric neglect and allocentric neglect in the experimental group, but there was no significant difference in the MBI and MFT tests. Furthermore, as a result of comparing changes between groups, there was no significant difference in all items, but the experimental group showed higher changes than the control group. Therefore, through this study, we hope that Twins Therapy will be used in more studies in patients with unilateral neglect in actual clinical practice.
Author Contributions
Conceptualization, W-H.J.; Methodology, W-H.J. and H-M.K.; Formal analysis, W-H.J. and H-M.K. and J-Y.K.; Data curation, H-M.K.; Writing, J-Y.K.; Review and editing, W-H.J. and J-Y.K. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the National Research Foundation of Korea, grant No.2021R1G1A1093494.
Institutional Review Board Statement
This study was approved by the Kangwon National University Institutional Review Board (KWNUIRB-2021-05-011-003) prior to commencement.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data used for the study are private but can be made available upon reasonable request.
Acknowledgments
None.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kerkhoff, G. (2001). Spatial hemineglect in humans. Progress in neurobiology, 63(1), 1-27. [CrossRef]
- Parton, A., Malhotra, P., & Husain, M. (2004). Hemispatial neglect. Journal of Neurology, Neurosurgery & Psychiatry, 75(1), 13-21.
- Azouvi, P., Jacquin-Courtois, S., & Luauté, J. (2017). Rehabilitation of unilateral neglect: Evidence-based medicine. Annals of physical and rehabilitation medicine, 60(3), 191-197.
- Lafitte, R., Jeager, M., Piscicelli, C., Dai, S., Lemaire, C., Chrispin, A., ... & Pérennou, D. (2022). Spatial neglect encompasses impaired verticality representation after right hemisphere stroke. Annals of the New York Academy of Sciences.
- van Nes, I. J., van Kessel, M. E., Schils, F., Fasotti, L., Geurts, A. C., & Kwakkel, G. (2009). Is visuospatial hemineglect longitudinally associated with postural imbalance in the postacute phase of stroke?. Neurorehabilitation and Neural Repair, 23(8), 819-824. [CrossRef]
- Jang, S. H., & Jang, W. H. (2018). The different association of allocentric and egocentric neglect with dorsal and ventral pathways: a case report. Medicine, 97(37). [CrossRef]
- Neggers, S. F., der Lubbe, R. H., Ramsey, N. F., & Postma, A. (2006). Interactions between ego-and allocentric neuronal representations of space. Neuroimage, 31(1), 320-331. [CrossRef]
- Pierce, S. R., & Buxbaum, L. J. (2002). Treatments of unilateral neglect: a review. Archives of physical medicine and rehabilitation, 83(2), 256-268. [CrossRef]
- Barrett, A. M., Buxbaum, L. J., Coslett, H. B., Edwards, E., Heilman, K. M., Hillis, A. E., ... & Robertson, I. H. (2006). Cognitive rehabilitation interventions for neglect and related disorders: moving from bench to bedside in stroke patients. Journal of cognitive neuroscience, 18(7), 1223-1236. [CrossRef]
- Moon, H.-S., & Chung, S.-T. (2020). Quantitative Evaluation Method of Unilateral Neglect based on K-CBS using Virtual Reality. The Journal of The Institute of Internet, Broadcasting and Communication, 20(1), 141–148. [CrossRef]
- Ogourtsova, T., Archambault, P. S., & Lamontagne, A. (2018). Post-stroke unilateral spatial neglect: virtual reality-based navigation and detection tasks reveal lateralized and non-lateralized deficits in tasks of varying perceptual and cognitive demands. Journal of neuroengineering and rehabilitation, 15, 1-16. [CrossRef]
- Tanaka, T., Ifukube, T., Sugihara, S., and Izumi, T. (2010). A case study of new assessment and training of unilateral spatial neglect in stroke patients: effect of visual image transformation and visual stimulation by using a head mounted display system (HMD). J. Neuroeng. Rehabil. 7:20. [CrossRef]
- Ting, D. S., Pollock, A., Dutton, G. N., Doubal, F. N., Ting, D. S., Thompson, M., & Dhillon, B. (2011). Visual neglect following stroke: current concepts and future focus. Survey of ophthalmology, 56(2), 114-13. [CrossRef]
- Bowen, A., Hazelton, C., Pollock, A., & Lincoln, N. B. (2013). Cognitive rehabilitation for spatial neglect following stroke. Cochrane database of systematic reviews, (7). [CrossRef]
- Ko, Seok-Beom, Kim, Ju-Hee, Park, Hae Yean. (2017). Intervention of Neglect for Stroke Patients: A Systematic Review. The Journal of Korean Society of Occupational Therapy, 25(1), 85-104. [CrossRef]
- Gossmann, A., Kastrup, A., Kerkhoff, G., López-Herrero, C., & Hildebrandt, H. (2013). Prism adaptation improves ego-centered but not allocentric neglect in early rehabilitation patients. Neurorehabilitation and neural repair, 27(6), 534-541. [CrossRef]
- Moon, S. Y., Lee, B. H., & Na, D. L. (2006). Therapeutic effects of caloric stimulation and optokinetic stimulation on hemispatial neglect. Journal of Clinical Neurology, 2(1), 12-28. [CrossRef]
- Turgut, N., Möller, L., Dengler, K., Steinberg, K., Sprenger, A., Eling, P., ... & Hildebrandt, H. (2018). Adaptive cueing treatment of neglect in stroke patients leads to improvements in activities of daily living: a randomized controlled, crossover trial. Neurorehabilitation and neural repair, 32(11), 988-998. [CrossRef]
- Bickerton, W. L., Samson, D., Williamson, J., & Humphreys, G. W. (2011). Separating forms of neglect using the Apples Test: validation and functional prediction in chronic and acute stroke. Neuropsychology, 25(5), 567. [CrossRef]
- Mohammadi, A., Hesami, E., Kargar, M., & Shams, J. (2018). Detecting allocentric and egocentric navigation deficits in patients with schizophrenia and bipolar disorder using virtual reality. Neuropsychological rehabilitation, 28(3), 398-415. [CrossRef]
- Kim, Y. K., Jung, J. H., & Shin, S. H. (2015). A comparison of the effects of repetitive transcranial magnetic stimulation (rTMS) by number of stimulation sessions on hemispatial neglect in chronic stroke patients. Experimental brain research, 233(1), 283-289. [CrossRef]
- Ansuini, C., Pierno, A. C., Lusher, D., & Castiello, U. (2006). Virtual reality applications for the remapping of space in neglect patients. Restorative neurology and neuroscience, 24(4-6), 431-441.
- Lee, S. H., Lim, B. C., Jeong, C. Y., Kim, J. H., & Jang, W. H. (2022). Assessment tools for differential diagnosis of neglect: Focusing on egocentric neglect and allocentric neglect. World Journal of Clinical Cases, 10(24), 8625-8633. [CrossRef]
- Oldfield, R. C. (1971). The assessment and analysis of handedness: the Edinburgh inventory. Neuropsychologia, 9(1), 97-113. [CrossRef]
- ] Park, J. H. (1989). Standardization of Korean of the mini-mental state examination (mmse-k) for use in the elderly. Part II. Diagnostic validity. J Korean Neuropsychiatr Assoc, 28, 508-513.
- Mancuso, M., Rosadoni, S., Capitani, D., Bickerton, W. L., Humphreys, G. W., De Tanti, A., ... & Antonucci, G. (2015). Italian standardization of the apple cancellation test. Neurological Sciences, 36(7), 1233-1240. [CrossRef]
- Kim, Mi-Young. (1994). A Study of Manual Functional Test for C.V.A. The Journal of Korean Society of Occupational Therapy, 2(1), 19-26.
- Shah, S., Vanclay, F., & Cooper, B. (1989). Improving the sensitivity of the Barthel Index for stroke rehabilitation. Journal of clinical epidemiology, 42(8), 703-709. [CrossRef]
- Mi Hyun Yong, Deok Ju Kim. (2014). Analysis of Correlation among Upper Extremity Function and Activities of Daily Living With Stroke Patients: Focused on FMA, MFT, K-MBI. The Journal of Korea Aging Friendly Industry Association, 6(1), 35-41.
- Hwang, Ho-Sung, Yoo, Doo-Han, Kim, Hee, Kim, Su-Kyoung. (2020). Effects of Virtual Reality-Based Upper Limb Rehabilitation Training on Upper Limb Function, Muscle Activation, Activities of Daily Living, and Quality of Life in Stroke Patients. The Journal of Korean Society of Occupational Therapy, 28(2), 115-129. [CrossRef]
Figure 2.
Steps and composition of Twins Therapy.
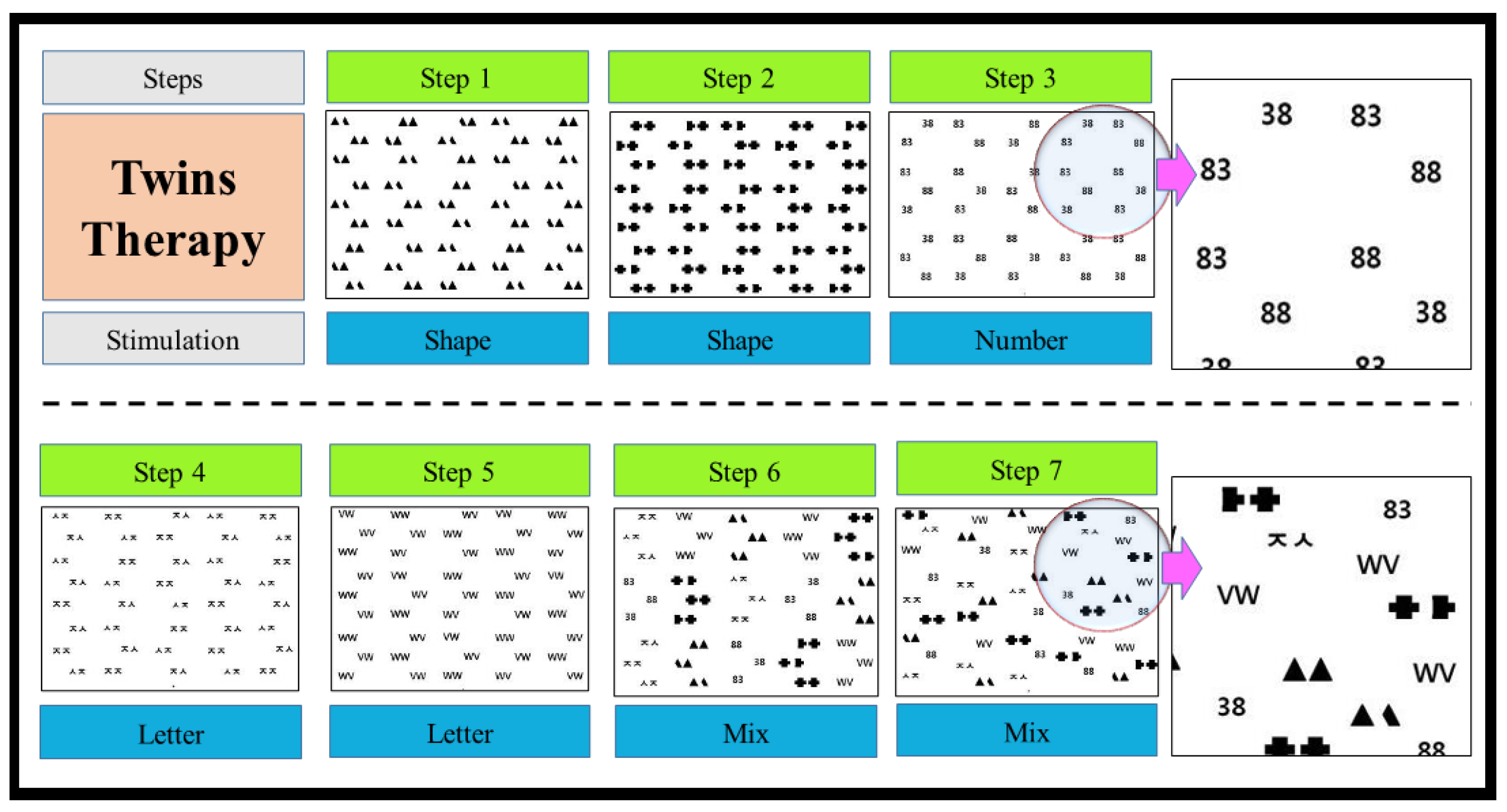

Table 1.
General Characteristics.
| Characteristic | Classification | Experimental (n=7) Mean ± SD |
Control (n=8) Mean ± SD |
P |
| Age (year) |
Average age | 61.57±16.33 | 62.37±12.99 | 1.00 |
| Gender | Male | 3 | 5 | .447 |
| Female | 4 | 3 | ||
| Education Level |
None | 0 | 1 | .635 |
| Elementary | 1 | 2 | ||
| Middle school | 1 | 1 | ||
| High school | 4 | 3 | ||
| College | 0 | 1 | ||
| University or higher | 1 | 0 | ||
| Damage type | Cerebral hemorrhage | 5 | 5 | .714 |
| Cerebral infarction | 2 | 3 | ||
| Duration of Onset (day) |
121.71±41.70 | 119.12±76.59 | .867 | |
(N=15). *SD= standard deviation. *P<.05
Table 2.
Homogeneity test between experimental and control groups (N=15).
| Assessment type | Experimental (n=7) Mean ± SD |
Control (n=8) Mean ± SD |
P |
| Apple score (Ego) | 6.00±3.36 | 9.00±4.47 | .336 |
| Apple score (Allo) | 9.42±4.42 | 7.12±2.58 | .336 |
| Apple_time (sec) | 555.14±137.85 | 542.00±131.83 | .694 |
| MFT_Rt | 29.57±1.39 | 28.25±1.48 | .094 |
| MFT_Lt | 5.28±6.89 | 4.62±6.67 | .867 |
| MBI | 31.57±12.35 | 38.75±9.60 | .152 |
*SD= standard deviation, Ego= egocentric neglect, Allo= allocentric neglect, sec= second, MFT = Manual Function Test, Rt= right, Lt= left, MBI= Korean version of Modified Barthel Index.*P<.05.
Table 3.
Comparison of test scores between experimental and control groups (N=15).
| Assessment type | Experimental (n=7) Mean ± SD |
Control (n=8) Mean ± SD |
||||||
| Pre | Post | P | Pre | Post | P | |||
| Apple score (Ego) | 6.00±3.36 | 3.14±1.21 | .039* | 9.00±4.47 | 7.62±5.50 | .139 | ||
| Apple score (Allo) | 9.42±4.42 | 4.85±2.67 | .017* | 7.12±5.58 | 5.62.85±1.50 | .231 | ||
| Apple_time (sec) | 555.14±137.85 | 494.28±181.91 | .063 | 542.00±131.83 | 529.25±118.22 | .575 | ||
| MFT_Rt | 29.57±1.39 | 29.85±1.46 | .317 | 28.25±1.48 | 28.25±1.48 | 1.00 | ||
| MFT_Lt | 5.28±6.89 | 5.71±7.13 | .180 | 4.62±6.67 | 4.87±6.89 | .157 | ||
| MBI | 31.57±12.35 | 32.71±11.71 | .066 | 38.75±9.60 | 39.12±9.47 | .180 | ||
*SD= standard deviation, Ego= egocentric neglect, Allo= allocentric neglect, sec= second, MFT = Manual Function Test, Rt= right, Lt= left, MBI= Korean version of Modified Barthel Index.*P<.05
Table 4.
Comparison of test score variations between experimental and control groups (N=15).
| Assessment type | Experimental(n=7) Mean ± SD |
Control(n=8) Mean ± SD |
P |
| Apple score (Ego) | 2.85±2.26 | 2.62±1.76 | .867 |
| Apple score (Allo) | 4.57±2.29 | 2.75±2.05 | .189 |
| Apple_time (sec) | 71.42±56.73 | 44.75±27.57 | .397 |
| MFT_Rt | 0.28±0.75 | 0.25±0.46 | .867 |
| MFT_Lt | 0.42±0.78 | 0.25±0.46 | .867 |
| MBI | 1.14±1.21 | 0.37±0.74 | .232 |
*SD= standard deviation, Ego= egocentric neglect, Allo= allocentric neglect, sec= second, MFT = Manual Function Test, Rt= right, Lt= left, MBI= Korean version of Modified Barthel Index. *P<.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



