
Submitted:
14 April 2023
Posted:
17 April 2023
You are already at the latest version
Abstract
Growing evidence indicates the involvement of a genetic component for CaP susceptibility and clinical severity. Somatic mutations of TP53 have been associated with 50% of diverse human cancers. Studies have also reported the role of germ line mutations and single nucleotide poly-morphisms (SNPs) of TP53 as possible risk factors for cancer development. In this single De-partment of Defense institutional retrospective study, we identified common SNPs in the TP53 gene in AA and CA men and performed association analyses for functional TP53 SNPs with clinico-pathological features of CaP. The CPDR Oncoarray database on blood derived genomic DNA from 321 men treated by radical prostatectomy at WRNMMC were used to examine clini-co-pathological associations with TP53 SNPs. The SNP genotyping analysis on the final cohort of 308 patients (212 AA; 95 CA) identified 74 SNPs in the TP53 gene region with a minor allele fre-quency (MAF) of at least 1%. Two SNPs were non-synonymous in the exonic region of TP53: rs1800371 (Pro47Ser) and rs1042522 (Arg72Pro). The Pro47Ser variant, had a minor allele frequency of 0.01 in AA, however, was not detected in CA. Arg72Pro was the most common SNP with a minor allele frequency of 0.50 (0.41 in AA; 0.68 in CA). Additionally, Arg72Pro was associated with time to biochemical recurrence (BCR) after statistical adjustment for patient age at diagnosis, self-reported race, and Gleason score (p= 0.046; HR = 1.52).
The present study demonstrated ancestral differences in allele frequencies of TP53 Arg72Pro and Pro47Ser SNPs in AA and CA CaP, providing a valuable framework for the interrogating CaP disparity among AA and CA men.
Keywords:
prostate cancer
; SNP
; TP53
; Pro47Ser
; Arg72Pro
; African American
1. Introduction
Prostate cancer (CaP) is the most common non-skin cancer and is the second leading cause of cancer death in American men [1], with an unequal burden of disease incidence and mortality among men of different ancestries [2]. Prostate cancer is a clinically heterogenous disease comprising of diverse clinico-pathologic and progression features and is characterized by a large subset of the indolent cancer type. Therefore, it is critical to identify molecular and genetic markers with diagnostic, predictive and prognostic potential in addition to the standard of care (SOC) variables [3]. A significant proportion of CaP susceptibility has been attributed to inherited predisposition. Genome wide association studies (GWAS) have identified 269 low penetrance single nucleotide polymorphisms (SNPs) associating with CaP risk or aggressiveness [4]. The TP53 gene, also referred to as the guardian of the genome, is a key tumor suppressor gene involved in DNA repair, cell cycle arrest, apoptosis, cell metabolism and genomic stability [5,6]. The TP53 is the most commonly mutated gene in human cancers and malfunction of the TP53 pathway is a key feature of human tumors [7]. Germline mutations in TP53 predisposes to Li-Fraumeni syndrome (LFS) which is characterized by early onset of cancers including breast cancer, sarcomas, brain tumors, leukemia and adrenocortical carcinomas [8,9,10]. However, the role of germline mutations in TP53 is not completely understood in CaP. Some studies point to the role of specific TP53 SNPs as a possible risk factor for CaP [11,12]. Polymorphisms in codons 47 and 72 in the TP53 tumor suppressor gene have been shown to affect phosphorylation and the expression of pro-apoptotic genes, respectively, both of which could increase cancer risk [13]. A more recent study found heterozygosity at codon 72 SNP (rs1042522, GC), and either of the two intron 4 SNPs (rs9895829, TC and rs2909430, AG) are associated with up to 5-fold greater CaP risk, greater tumor-promoting inflammation, and shorter patient survival [14].
Racial disparities in CaP incidence and mortality rates remain significant even after adjusting for socio-economic status and access to healthcare, suggestive of a greater contribution from genetic factors [15]. However, several Veterans Affairs studies revealed conflicting results in CaP outcomes for Black and White men within a single, equal access health care system [16,17]. Black men have an increased risk for CaP, especially clinically aggressive CaP, and elevated PSA levels at the time of diagnosis compared to White men in similar cohorts. Genetic associations between such clinical findings and SNPs have been described earlier, however with inconsistent results. Thus, further understanding and additional confirmation of such genetic factors may be beneficial in understanding the clinical outcomes which influence screening and treatment guidelines across AA and CA men in an equal access military healthcare system.
We hypothesize that the germline variants in TP53 could contribute to distinct clinical phenotype of CaP. Thus, the goals of this study were to identify the common SNPs in the TP53 gene in AA and CA men and to perform an association analysis for functional variants in TP53 with clinico-pathological features of CaP including biochemical recurrence-free survival and metastasis-free survival.
2. Materials and Methods
2.1. Study Population
This study is based on a retrospective cohort design utilizing germline blood DNA derived Oncoarray data from 321 men (AA = 216 and CA = 105) who were treated with radical prostatectomy at Walter Reed National Military Medical Center (WRNMMC). Only those patients were included who consented to enrollment in the CPDR biospecimen databank and multicenter national clinical database. The databases have been approved by the Institutional Review Boards (IRBs) at the WRNMMC and the Uniformed Services University of the Health Sciences (USUHS) in Bethesda, Maryland. All subjects provided written informed consent and agreed to participate for present study under IRB approved protocols. These patients are under the equal access DoD healthcare system and were clinically followed up to 25 years. Demographics, clinical characteristics, pathology information, and all treatment data were obtained from the CPDR multicenter national clinical database. Patient characteristics included patient age at CaP diagnosis (years), self-reported race (AA, CA), diagnostic PSA (ng/ml), pathologic T Stage (pT2,T3, T4) , biopsy and pathology Gleason (≤6, 3 + 4, 4 + 3, and 8–10), biochemical recurrence (BCR), time to BCR and metastasis outcome. A BCR event was defined as either two successive post-RP PSAs of ≥0.2 ng/mL, or initiation of salvage therapy after a rising PSA of ≥0.1 ng/mL. The clinical characteristics of the patients are shown in Table 1.
2.2. SNP Analysis and Validation
Genotype analysis for common SNPs with minor allele frequency (MAF) of at least 0.01, was performed using Eagle [18] for phasing and for imputation TOPMed (v R2 on GRCh38) was used as a reference comprising of 194,512 haplotypes [19]. Genotype data were split into 20MB regions with an overlap of 5MB. Experimental validation for the imputed SNPs (rs1800371/Pro47Ser and rs1042522/Arg72Pro) was performed using droplet digital polymerase chain (ddPCR) approach using a QX200 (BioRad). Briefly, a ddPCR mastermix was prepared containing 11 μl 2X ddPCR Supermix (BioRad), 1.1 μl 20X TaqMan SNP Genotyping Assay (BioRad, ThermoFisher Scientific; Supplementary Table 6), and 7.9 μl nuclease-free water (Qiagen) per sample. The mastermix was prepared at room temperature and 20 μl was added to 2 μl (=5 ng) of each DNA sample. Samples were loaded into individual wells of DG8TM cartridges (BioRad), and droplets were generated using a QX200 Droplet Generator (BioRad). For each sample, 40 μl of droplet mix was then transferred to a 96-well plate, and PCR was performed in a thermal cycler using the following cycling conditions: 95 °C × 10 min; 40 cycles of [94 °C × 30 s, 60 °C × 60 s]; 98 °C × 10 s; 40 C × 10 min. The BioRad QX200 Droplet Reader was then used to assess droplets as positive or negative based on fluorescence amplitude. The QuantaSoft software (BioRad) was used to analyze droplet data.
2.3. Statistical Analysis:
Descriptive distributions for clinico-pathological variables in the overall cohort stratified by exonic SNP genotypes was examined. The chi-square test or Fisher's exact test was used to compare categorical variables and the Mann-Whitney U test was used to compare continuous variables. Time to biochemical recurrence (BCR) or metastasis was evaluated using Cox proportional hazards (PH) modeling adjusting for age at diagnosis, race, and Gleason score to examine SNP effects. Unadjusted Kaplan-Meier survival analysis and log-rank testing were used to show the probability of BCR-free survival stratified by genotypes. All statistical analysis was performed using SAS version 9.4 (SAS Institute Inc., Cary, NC) and statistical significance was set at p < 0.05.
3. Results
Clinical and pathological features of the patient cohort is summarized in Table 1. The cohort had higher proportion of AA patients compared to CA patients (69% vs 31%), were over-represented by subjects with serum PSA in range 4-9ng/ml (63%), T2 clinical stage (74%) and pathological Gleason ≤ 7 (83%). The post-prostatectomy follow-up data showed that 15% of the subjects had biochemical recurrence, with 3% having metastasis.
The SNP analysis on the final cohort of 308 patients with available clinical data identified 74 SNPs in the TP53 gene region with MAF of at least 1%. The description of the 74 SNPs is included in Supplementary Table 1. Two imputed SNPs (rs1800371/Pro47Ser and rs1042522/Arg72Pro) of the 74 SNPs are non-synonymous, functional SNPs located in exon 4 of TP53 (Figure 1). MAF for Pro47Ser and Arg72Pro was 0.01 and 0.50 respectively. Both these imputed SNPs were experimentally validated by ddPCR approach (Figure 2). Concordance between TaqMan genotypes and imputed genotypes was 99%.
Race stratified analysis for the SNPs demonstrated and confirmed ancestry-dependent differences in allele frequencies of TP53 Arg72Pro and TP53 Pro47Ser SNPs in AA and CA CaP (Table 2; Supplementary Tables 2 and 3). The Pro47Ser variant has an MAF of 0.01 in AA, however, was not detected in CA men. While Arg72Pro was the most common SNP with an MAF of 0.50 (AA, 0.41; CA, 0.68) (Supplementary Table 4). The MAF distribution in our dataset was in concordance with publicly available databases Pro47Ser variant (A=0.005591/28 (1000Genomes), A=0.02439/8 (HapMap); Arg72Pro G=0.457069/2289 (1000Genomes), G=0.43865/143 (HapMap).
An association analysis of the TP53 Pro47Ser and Arg72Pro SNPs with respect to clinico-pathologic features of CaP is shown in Table 2. Except for race, there were no observed statistically significant associations between the Arg72Pro or Pro47Ser SNPs and age of onset of prostate cancer, CaP aggressiveness (Grade, Clinical Stage), tumor upgrading from biopsy to RP (Supplementary table 5) and disease outcome (BCR, Metastasis). However, Arg72Pro SNP was the only exonic SNP significantly (p= 0.046; HR = 1.52) associated with shorter time to BCR following radical prostatectomy after adjusting for patient age at diagnosis, race, and Gleason score (Table 3). Additionally, we found that 3 non-exonic SNPs were significantly associated with shorter time to BCR (rs4968186, intergenic; p 0.004; HR 1.75; rs9894227, intronic, p 0.007; HR 1.72 and rs8079544 , intronic, p 0.02; HR 1.63).
4. Discussion
The present study investigates the association of common functional germline variants in the TP53 gene with CaP in a racially diverse cohort of men with longitudinal clinical follow up. We confirmed ancestry-dependent differences for MAF across AA and CA men and found that Arg72Pro was associated with shorter time to BCR. Arg72Pro and Pro47Ser SNPs have been well characterized for their function and for association with cancer [12,20,21,22,23,24]; however, there is no consistent conclusion for CaP risk or clinico-pathological features [25,26,27,28,29]. This variability may be attributed to small sample size, study design and mixed ancestry.
Additionally, the prognostic role of the SNP in relation to disease and treatment outcome has been found in many cancers including CaP [30], lung cancer [31], gastric cancer [32], breast cancer [33], acute lymphoblastic leukemia. Common variant, Arg72Pro, leads to altered activities for TP53 protein. The C to G base change results in a proline (Pro) to arginine (Arg) amino acid alteration in the proline-rich domain impacting the programmed cell death or cell cycle arrest. Additionally, TP53 arginine has increased affinity for MDM-2, resulting in destabilization of the protein, lower levels of the TP53 protein, and ultimately earlier onset of TP53 associated tumors [14]. On the other hand, less frequent and AA centric Pro47Ser variant exhibits functional consequences by attenuating p53 transcriptional activation and pro-apoptotic functions [34]. The inactivation of p53 via somatic and germline TP53 mutations have been documented for both aggressive disease and poor outcomes in many cancer types [35]. The somatic mutations of TP53 have also been reported with variable frequencies in primary CaP and consistently with higher frequencies in metastatic disease [36]. Several studies from our center over the years including, a recent study show that focal alterations of TP53 protein in prostatectomy specimens associate with BCR and metastatic progression [37].
In a recent multi-institutional retrospective study by Maxwell et al. on CaP incidence in a cohort of patients with Li-Fraumeni syndrome (LFS) showed men with LFS had a 25-fold increased risk of CaP compared to the population controls and the rate of inherited deleterious TP53 variants was 9-times higher than men with no CaP [38]. Our current findings on the association of TP53 SNPs with aggressive disease further support the role of germline TP53 functional alterations in prostate tumorigenesis and suggests a potential clinical benefit to include evaluation of germline TP53 variants (SNPs identified in this study and pathogenic SNVs) for CaP susceptibility testing, especially in context of high risk men [39,40].
In addition to the genetic influence on CaP, studies described differences in such associations as they pertained to patient ancestry [41]. While associations between AA race, TP53 SNPs, and CaP incidence, mortality, and post-treatment BCR have been made in the past, the three primary guideline tools – National Comprehensive Cancer Network (NCCN), United States Preventive Services Task Force (USPSTF), and American Urological Association (AUA) Clinical Guidelines - used by physicians to guide patient screening and treatment - do not suggest its use in treatment decision-making recommendations, despite their clinical relevance [42,43,44].
The findings in our study not only further confirm previous research, but also improve the understanding of the association between TP53 SNPs, race/ancestry, and poor disease outcome. The present study provides important data that could influence medical providers to improve screening tools, germline CaP susceptibility testing for high-risk men, and treatment approaches for patients. Future directions include comprehensive analysis of germline variants in TP53 pathway in high-risk men, investigation of TP53 mutation profile to predict response to treatment, and functional understanding of the biology of these SNPs in relation to aggressive CaP.
5. Conclusions
Comprehensive analysis of common germline variants in TP53 confirms genetic heterogeneity across AA and CA men for Arg72Pro and Pro47Ser variants and suggests TP53 Arg72Pro predisposes men to clinically significant prostate cancer. Therefore, TP53 should be included in CaP germline screening panel for high-risk men representing different ancestries.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Table S1: Description of SNPs in TP53 gene region with MAF of at least 1%; Table S2: Literature review table for Pro47Ser; Table S3: Literature review table for Arg72Pro; Table S4: Allele frequency of rs1042522 and rs1800371 SNPs in TP53 gene region; Table S5: Association of TP53 SNPs with pathological upgrading from Diagnostic Biopsy to Radical Prostatectomy
Author Contributions
Conceptualization, Indu Kohaar and Shiv Srivastava; methodology, Indu Kohaar; software, Darryl Nousome, Indu Kohaar, Jennifer Cullen; validation, Indu Kohaar, Randy Ricks, Lakshmi Ravindranath and Allison Duncan; formal analysis, Jennifer Cullen, Darryl Nousome, Huai-Ching Kuo and Randy Ricks; investigation, Randy Ricks; resources, Gregory Chesnut; data curation, Jennifer Cullen and Huai-Ching Kuo; writing—original draft preparation, Indu Kohaar, Allison Duncan; writing—review and editing, Indu Kohaar, Allison Duncan, Jennifer Cullen, Gyorgy Petrovics and Albert Dobi; funding acquisition, Gregory Chesnut and Gyorgy Petrovics. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by a Center for Prostate Disease Research, Uniformed Services University Grant, HU0001-10-2-0002 (G.C.) and the DoD/PCRP Health Disparity Award; W81XWH-13-2-0096 (GP).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board of the Walter Reed National Military Medical Center and the Uniformed Services University of the Health Sciences in Bethesda, Maryland (WRNMMC IRB Protocols #392143, #393738 and #385525).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data supporting reported results can be found in Table 1, Table 2 and Table 3 and Supplementary Tables 1–5.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Siegel, R.L.; Miller, K.D.; Fuchs, H.E.; Jemal, A. Cancer statistics, 2022. CA Cancer J Clin 2022, 72, 7–33. [Google Scholar] [CrossRef]
- McHugh, J.; Saunders, E. J.; Dadaev, T.; McGrowder, E.; Bancroft, E.; Kote-Jarai, Z.; Eeles, R. Prostate cancer risk in men of differing genetic ancestry and approaches to disease screening and management in these groups. British journal of cancer 2022, 126, 1366–1373. [Google Scholar] [CrossRef] [PubMed]
- Kohaar, I.; Petrovics, G.; Srivastava, S. A Rich Array of Prostate Cancer Molecular Biomarkers: Opportunities and Challenges. Int J Mol Sci 2019, 20, 1813. [Google Scholar] [CrossRef] [PubMed]
- Conti, D.V.; Darst, B.F.; Moss, L.C.; Saunders, E.J.; Sheng, X.; Chou, A.; Schumacher, F.R.; Olama, A.A.A.; Benlloch, S.; Dadaev, T. Trans-ancestry genome-wide association meta-analysis of prostate cancer identifies new susceptibility loci and informs genetic risk prediction. Nat Genet 2021, 53, 65–75. [Google Scholar] [CrossRef]
- Lane, D.P. Cancer. p53, guardian of the genome. Nature 1992, 358, 15–16. [Google Scholar] [CrossRef]
- Vogelstein, B.; Lane, D.; Levine, A.J. Surfing the p53 network. Nature 2000, 408, 10. [Google Scholar] [CrossRef] [PubMed]
- Brosh, R.; Rotter, V. When mutants gain new powers: news from the mutant p53 field. Nat Rev Cancer 2009, 9, 13. [Google Scholar] [CrossRef]
- Li, F.P.; Fraumeni, J.F.; Mulvihill, J.J.; Blattner, W.A.; Dreyfus, M.G.; Tucker, M.A.; Miller, R.W. A cancer family syndrome in twenty-four kindreds. Cancer Res 1988, 48, 5358–5362. [Google Scholar]
- Malkin, D.; Li, F.P.; Strong, L.C.; Fraumeni, J.F., Jr.; Nelson, C.E.; Kim, D.H.; Kassel, J.; Gryka, M.A.; Bischoff, F.Z.; Tainsky, M.A.; Friend, S.H. Germ line p53 mutation in a familial syndrome of breast cancer. Science 1990, 250, 1233–1238. [Google Scholar] [CrossRef]
- Srivastava, S.; Zou, Z.; Pirollo, K.; Blattner, W.; Chang, E.H. Germ-line transmission of a mutated p53 gene in a cancer prone family with Li-Fraumeni syndrome. Nature 1990, 348, 747–749. [Google Scholar] [CrossRef]
- Zawacka-Pankau, J.E. The Role of p53 Family in Cancer. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Whibley, C.; Pharoah, P.D.; Hollstein, M. p53 polymorphisms: cancer implications. Nat Rev Cancer 2009, 9, 95–107. [Google Scholar] [CrossRef] [PubMed]
- Barnoud, T.; Parris, J.L.D.; Murphy, M.E. Common genetic variants in the TP53 pathway and their impact on cancer. J Mol Cell Biol 2019, 11, 578–585. [Google Scholar] [CrossRef] [PubMed]
- Eiholzer, R.A.; Mehta, S.; Kazantseva, M.; Drummond, C.J.; McKinney, C.; Young, K.; Slater, D.; Morten, B.C.; Avery-Kiejda, K.A.; Lasham, A. et al. Intronic TP53 Polymorphisms Are Associated with Increased Delta133TP53 Transcript, Immune Infiltration and Cancer Risk. Cancers (Basel) 2020, 12. [Google Scholar] [CrossRef] [PubMed]
- Freedland, S.J.; Isaacs, W.B. Explaining racial differences in prostate cancer in the United States: sociology or biology? Prostate 2005, 62, 243–252. [Google Scholar] [CrossRef]
- Riviere, P.; Luterstein, E.; Kumar, A.; Vitzthum, L.K.; Deka, R.; Sarkar, R.R.; Bryant, A.K.; Bruggeman, A.; Einck, J.P.; Murphy, J.D. et al. Survival of African American and non-Hispanic white men with prostate cancer in an equal-access health care system. Cancer 2020, 126, 1683–1690. [Google Scholar] [CrossRef]
- Yamoah, K.; Lee, K.M.; Awasthi, S.; Alba, P.R.; Perez, C.; Anglin-Foote, T.R.; Robison, B.; Gao, A.; DuVall, S.L.; Katsoulakis, E. et al. Racial and Ethnic Disparities in Prostate Cancer Outcomes in the Veterans Affairs Health Care System. JAMA Netw Open 2022, 5. Erratum in: JAMA Netw Open 2022, 5. [Google Scholar] [CrossRef]
- Loh, P.R.; Danecek, P.; Palamara, P.F.; Fuchsberger, C.A.; Reshef, Y.K.; Finucane, H.; Schoenherr, S.; Forer, L.; McCarthy, S.; Abecasis, G.R.; et al. Reference-based phasing using the haplotype reference consortium panel. Nat. Genet. 2016, 48, 1443–1448. [Google Scholar] [CrossRef]
- Taliun, D.; Harris, D.N.; Kessler, M.D.; Carlson, J.; Szpiech, Z.A.; Torres, R.; Taliun, S.A.G.; Corvelo, A.; Gogarten, S.M.; Kang, H.M.; et al. Sequencing of 53,831 diverse genomes from the NHLBI TOPMed Program. Nature 2021, 590, 290–299. [Google Scholar] [CrossRef]
- Dumont, P.; Leu, J.I.; Della Pietra, A.C.; George, D.L.; Murphy, M. The codon 72 polymorphic variants of p53 have markedly different apoptotic potential. Nat Genet 2003, 33, 357–365. [Google Scholar] [CrossRef]
- Hrstka, R.; Coates, P.J.; Vojtesek, B. Polymorphisms in p53 and the p53 pathway: roles in cancer susceptibility and response to treatment. J Cell Mol Med. 2009, 13, 440–453. [Google Scholar] [CrossRef]
- Hu, W.; Feng, Z.; Atwal, G.S.; Levine, A.J. p53: a new player in reproduction. Cell Cycle 2008, 7, 848–852. [Google Scholar] [CrossRef] [PubMed]
- Bond, G.L.; Levine, A.J. A single nucleotide polymorphism in the p53 pathway interacts with gender, environmental stresses and tumor genetics to influence cancer in humans. Oncogene 2007, 26, 1317–1323. [Google Scholar] [CrossRef] [PubMed]
- Khan, M.; Khalil, A.; Rashid, H. Evaluation of the p53 Arg72Pro polymorphism and its association with cancer risk: A HuGE review and meta-analysis. Genetics Research 2015, 97, e7. [Google Scholar] [CrossRef]
- Huang, S.P.; Huang, C.Y.; Wang, J.S.; Liu, C.C.; Pu, Y.S.; Yu, H.J.; Yu, C.C.; Wu, T.T.; Huang, C.H.; Wu, W.J.; et al. Prognostic significance of p53 and X-ray repair cross-complementing group 1 polymorphisms on prostate-specific antigen recurrence in prostate cancer post radical prostatectomy. Clin Cancer Res 2007, 13, 6632–6638. [Google Scholar] [CrossRef]
- Quiñones, L.A.; Irarrázabal, C.E.; Rojas, C.R.; Orellana, C.E.; Acevedo, C.; Huidobro, C.; Varela, N.E.; Cáceres, D.D. Joint effect among p53, CYP1A1, GSTM1 polymorphism combinations and smoking on prostate cancer risk: an exploratory genotype-environment interaction study. Asian J Androl 2006, 8, 349–355. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, K.; Matsui, H.; Ohtake, N.; Nakata, S.; Takei, T.; Nakazato, H.; Okugi, H.; Koike, H.; Ono, Y.; Ito, K.; et al. A p53 codon 72 polymorphism associated with prostate cancer development and progression in Japanese. J Biomed Sci 2003, 10, 430–435. [Google Scholar] [CrossRef]
- Huang, S.P.; Wu, W.J.; Chang, W.S.; Wu, M.T.; Chen, Y.Y.; Chen, Y.J.; Yu, C.C.; Wu, T.T.; Lee, Y.H.; Huang, J.K.; et al. p53 Codon 72 and p21 codon 31 polymorphisms in prostate cancer. Cancer Epidemiol Biomarkers Prev 2004, 13, 2217–2224. [Google Scholar] [CrossRef]
- Henner, W.D.; Evans, A.J.; Hough, K.M.; Harris, E.L.; Lowe, B.A.; Beer, T.M. Association of codon 72 polymorphism of p53 with lower prostate cancer risk. Prostate 2001, 49, 263–266. [Google Scholar] [CrossRef]
- Cintra, H.S.; Pinezi, J.C.; Machado, G.D.; de Carvalho, G.M.; Carvalho, A.T.; dos Santos, T.E.; Marciano, R.D.; Soares Rde, B. Investigation of genetic polymorphisms related to the outcome of radiotherapy for prostate cancer patients. Dis Markers 2013, 35, 701–710. [Google Scholar] [CrossRef]
- Han, J.Y.; Lee, G.K.; Jang, D.H.; Lee, S.Y.; Lee, J.S. Association of p53 codon 72 polymorphism and MDM2 SNP309 with clinical outcome of advanced nonsmall cell lung cancer. Cancer 2008, 113, 799–807. [Google Scholar] [CrossRef] [PubMed]
- Kim, J.G.; Sohn, S.K.; Chae, Y.S.; Song, H.S.; Kwon, K.Y.; Do, Y.R.; Kim, M.K.; Lee, K.H.; Hyun, M.S.; Lee, W.S.; et al. TP53 codon 72 polymorphism associated with prognosis in patients with advanced gastric cancer treated with paclitaxel and cisplatin. Cancer Chemother Pharmacol 2009, 64, 355–360. [Google Scholar] [CrossRef] [PubMed]
- Toyama, T.; Zhang, Z.; Nishio, M.; Hamaguchi, M.; Kondo, N.; Iwase, H.; Iwata, H.; Takahashi, S.; Yamashita, H.; Fujii, Y. Association of TP53codon 72 polymorphism and the outcome of adjuvant therapy in breast cancer patients. Breast Cancer Res 2007, 9, R34. [Google Scholar] [CrossRef] [PubMed]
- Kohaar, I.; Li, Q.; Chen, Y.; Ravindranath, L.; Young, D.; Ali, A.; Sesterhenn, I.A.; Rosner, I.L.; Cullen, J.; Srivastava, S. Association of germline genetic variants with TMPRSS2-ERG fusion status in prostate cancer. Oncotarget 2020, 11, 1321–1333. [Google Scholar] [CrossRef]
- Teroerde, M.; Nientiedt, C.; Duensing, A.; Hohenfellner, M.; Stenzinger, A.; Duensing, S. Revisiting the Role of p53 in Prostate Cancer. In Prostate Cancer; Bott, S.R.J., Ng, K.L., Eds.; Exon Publications: Brisbane, Australia, 2021; Volume 1, pp. 116–117. ISBN 978-0-6450017-5-4. [Google Scholar] [CrossRef]
- Robinson, D.; Van Allen, E.M.; Wu, Y.M.; Schultz, N.; Lonigro, R.J.; Mosquera, J.M.; Montgomery, B.; Taplin, M.E.; Pritchard, C.C.; Attard, G.; et al. Integrative clinical genomics of advanced prostate cancer. Cell 2015, 161, 1215–1228. [Google Scholar] [CrossRef]
- Gesztes, W.; Schafer, C.; Young, D.; Fox, J.; Jiang, J.; Chen, Y.; Kuo, H.C.; Mwamukonda, K.B.; Dobi, A.; Burke, A.P.; et al. Focal p53 protein expression and lymphovascular invasion in primary prostate tumors predict metastatic progression. Sci Rep 2022, 12, 5404. [Google Scholar] [CrossRef]
- Levine, A.J. Spontaneous and inherited TP53 genetic alterations. Oncogene 2021, 40, 5975–5983. [Google Scholar] [CrossRef]
- Maxwell, K.N.; Cheng, H.H.; Powers, J.; Gulati, R.; Ledet, E.M.; Morrison, C.; Le, A.; Hausler, R.; Stopfer, J.; Hyman, S. et al. Inherited TP53 Variants and Risk of Prostate Cancer. Eur Urol 2022, 81, 243–250. [Google Scholar] [CrossRef]
- Nicolosi, P.; Ledet, E.; Yang, S.; Michalski, S.; Freschi, B.; O'Leary, E.; Esplin, E.D.; Nussbaum, R.L.; Sartor, O. Prevalence of Germline Variants in Prostate Cancer and Implications for Current Genetic Testing Guidelines. JAMA Oncol 2019, 5, 523–528. [Google Scholar] [CrossRef]
- Doffe, F.; Carbonnier, V.; Tissier, M.; Leroy, B.; Martins, I.; Mattsson, J.S.M.; Micke, P.; Pavlova, S.; Pospisilova, S.; Smardova, J. et al. Identification and functional characterization of new missense SNPs in the coding region of the TP53 gene. Cell Death Differ 2021, 28, 1477–1492. [Google Scholar] [CrossRef]
- Schaeffer, E.M.; Srinivas, S.; Adra, N.; An, Y.; Barocas, D.; Bitting, R.; Bryce, A.; Chapin, B.; Cheng, H.H.; D'Amico, A.V.; et al. NCCN Guidelines® Insights: Prostate Cancer, Version 1.2023. Journal of the National Comprehensive Cancer Network : JNCCN 2022, 20, 1288–1298. [Google Scholar] [PubMed]
- US Preventive Services Task Force; Grossman, D.C.; Curry, S.J.; Owens, D.K.; Bibbins-Domingo, K.; Caughey, A.B.; Davidson, K.W.; Doubeni, C.A.; Ebell, M.; Epling, J.W.; et al. Screening for Prostate Cancer: US Preventive Services Task Force Recommendation Statement. JAMA 2018, 319, 1901–1913. [Google Scholar] [CrossRef] [PubMed]
- Carter, H.B.; Albertsen, P.C.; Barry, M.J.; Etzioni, R.; Freedland, S.J.; Greene, K.L.; Holmberg, L.; Kantoff, P.; Konety, B.R.; Murad, M.H.; et al. Early detection of prostate cancer: AUA Guideline. The Journal of urology 2013, 190, 419–426. [Google Scholar] [CrossRef] [PubMed]
- Gnanapradeepan, K.; Leu, J.I.; Basu, S.; Barnoud, T.; Good, M.; Lee, J.V.; Quinn, W.J.; Kung, C.P.; Ahima, R.; Baur, J.A.; et al. Increased mTOR activity and metabolic efficiency in mouse and human cells containing the African-centric tumor-predisposing p53 variant Pro47Ser. Elife 2020, 9, 55994. [Google Scholar] [CrossRef]
- Tutton, S.; Deng, Z.; Gulve, N.; Vladimirova, O.; Beishline, K.; Wiedmer, A.; Murphy, M.; Lieberman, P.M. Elevated telomere dysfunction in cells containing the African-centric Pro47Ser cancer-risk variant of TP53. Oncotarget 2019, 10, 3581–3591. [Google Scholar] [CrossRef] [PubMed]
- Pinto, G.R.; Yoshioka, F.K.; Silva, R.L.; Clara, C.A.; Santos, M.J.; Almeida, J.R.; Burbano, R.R.; Rey, J.A.; Casartelli, C. Prognostic value of TP53 Pro47Ser and Arg72Pro single nucleotide polymorphisms and the susceptibility to gliomas in individuals from Southeast Brazil. Genet Mol Res 2008, 7, 207–216. [Google Scholar] [CrossRef]
- Murphy, M.E.; Liu, S.; Yao, S.; Huo, D.; Liu, Q.; Dolfi, SC.; Hirshfield, K.M.; Hong, C.C.; Hu, Q.; Olshan, A.F.; et al. A functionally significant SNP in TP53 and breast cancer risk in African-American women. NPJ Breast Cancer 2017, 3. [Google Scholar] [CrossRef]
- Almeida, L.O.; Custódio, A.C.; Pinto, G.R.; Santos, M.J.; Almeida, J.R.; Clara, C.A.; Rey, J.A.; Casartelli, C. Polymorphisms and DNA methylation of gene TP53 associated with extra-axial brain tumors. Genet Mol Res 2009, 8, 8–18. [Google Scholar] [CrossRef]
- Jaiswal, P.K.; Goel, A.; Mittal, R.D. Association of p53 codon 248 (exon7) with urinary bladder cancer risk in the North Indian population. Biosci Trend 2011, 5, 205–210. [Google Scholar] [CrossRef]
- Siraj, A.K.; Al-Rasheed, M.; Ibrahim, M.; Siddiqui, K.; Al-Dayel, F.; Al-Sanea, O.; Uddin, S.; Al-Kuraya, K. RAD52 polymorphisms contribute to the development of papillary thyroid cancer susceptibility in Middle Eastern population. J Endocrinol Invest 2008, 31, 893–899. [Google Scholar] [CrossRef]
- Daugherty, C.L.; Curtis, H.; Realini, T.; Charlton, J.F.; Zareparsi, S. Primary open angle glaucoma in a Caucasian population is associated with the p53 codon 72 polymorphism. Mol Vis 2009, 15, 1939–1944. [Google Scholar] [PubMed]
- Ruggeri, R.M.; Vicchio, T.M.; Giovinazzo, S.; Certo, R.; Alibrandi, A.; Trimarchi, F.; Benvenga, S.; Trovato, M. TP53 polymorphism may contribute to genetic susceptibility to develop Hashimoto's thyroiditis. J Endocrinol Invest 2015, 38, 1175–1182. [Google Scholar] [CrossRef] [PubMed]
- Elsaid, A.; Zahran, R.; Elshazli, R.; El-Sayed, A.; Abou Samra, M.; El-Tarapely, F.; Abdel-Malak, C. Genetic polymorphisms of TP53 Arg72Pro and Pro47Ser among Egyptian patients with colorectal carcinoma. Arch Physiol Biochem 2019, 125, 255–262. [Google Scholar] [CrossRef] [PubMed]
- Sameer, A.S.; Shah, Z.A.; Syeed, N.; Banday, M.Z.; Bashir, S.M.; Bhat, B.A.; Siddiqi, M.A. TP53 Pro47Ser and Arg72Pro polymorphisms and colorectal cancer predisposition in an ethnic Kashmiri population. Genet Mol Res 2010, 9, 651–660. [Google Scholar] [CrossRef]
- Santos, L.E.; Guilhen, A.C.; de Andrade, R.A.; Sumi, L.G.; Ward, L.S. The role of TP53 PRO47SER and ARG72PRO single nucleotide polymorphisms in the susceptibility to bladder cancer. Urol Oncol 2011, 29, 291–294. [Google Scholar] [CrossRef]
- Alawadi, S.; Ghabreau, L.; Alsaleh, M.; Abdulaziz, Z.; Rafeek, M.; Akil, N.; Alkhalaf, M. P53 gene polymorphisms and breast cancer risk in Arab women. Med Oncol 2011, 28, 709–715. [Google Scholar] [CrossRef]
- Mostaid, M.S.; Ahmed, M.U.; Islam, M.S.; Bin Sayeed, M.S.; Hasnat, A. Lung cancer risk in relation to TP53 codon 47 and codon 72 polymorphism in Bangladeshi population. Tumour Biol 2014, 35, 10309–10317. [Google Scholar] [CrossRef]
- Nairuz, T.; Rahman, M.; Bushra, M.U.; Kabir, Y. TP53 Arg72Pro and XPD Lys751Gln Gene Polymorphisms and Risk of Lung Cancer in Bangladeshi Patients. Asian Pac J Cancer Prev 2020, 21, 2091–2098. [Google Scholar] [CrossRef]
- Diakite, B.; Kassogue, Y.; Dolo, G.; Wang, J.; Neuschler, E.; Kassogue, O.; Keita, M.L.; Traore, C.B.; Kamate, B.; Dembele, E.; et al. p.Arg72Pro polymorphism of P53 and breast cancer risk: a meta-analysis of case-control studies. BMC Med Genet 2020, 21, 206. [Google Scholar] [CrossRef]
- Fang, Y.; Wu, X.; Li, L.; Zhu, J.; Wu, H.; Zhou, H.; He, J.; Wang, Y. TP53 Arg72Pro polymorphism and neuroblastoma susceptibility in eastern Chinese children: a three-center case-control study. Biosci Rep 2020, 40. [Google Scholar] [CrossRef]
- Drokow, E.K.; Chen, Y.; Waqas Ahmed, H.A.; Oppong, T.B.; Akpabla, G.S.; Pei, Y.; Kumah, M.A.; Neku, E.A.; Sun, K. The relationship between leukemia and TP53 gene codon Arg72Pro polymorphism: analysis in a multi-ethnic population. Future Oncol 2020, 16, 923–937. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Lollipop plot for single nucleotide polymorphisms in TP53. Variant in the coding region of the TP53 gene is indicated by green. Exon and UTR is shown in blue.
Figure 1.
Lollipop plot for single nucleotide polymorphisms in TP53. Variant in the coding region of the TP53 gene is indicated by green. Exon and UTR is shown in blue.
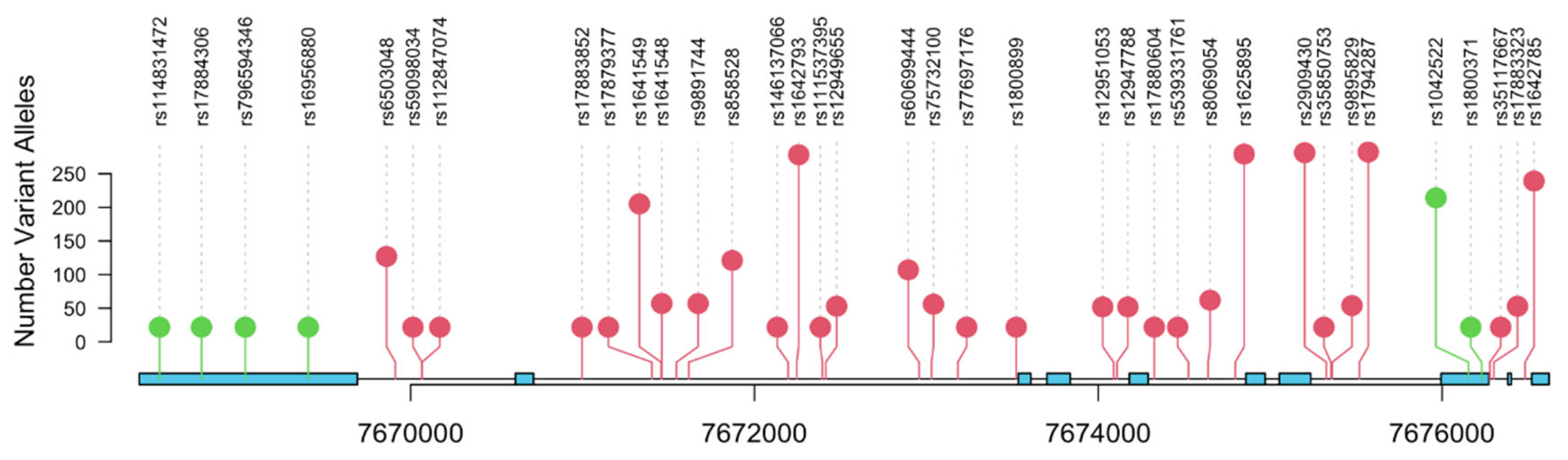
Figure 2.
Representative graph of SNP genotyping for rs1800371 (C/G) using digital droplet PCR (ddPCR) approach. 2-D Amplitude view where each axis represents the amplitude of fluorescence for either FAM (vertical axis) or VIC (horizontal axis). The FAM probe can hybridize only to the alternate allele (G allele), while VIC probe hybridizes only to reference allele (C allele).
Figure 2.
Representative graph of SNP genotyping for rs1800371 (C/G) using digital droplet PCR (ddPCR) approach. 2-D Amplitude view where each axis represents the amplitude of fluorescence for either FAM (vertical axis) or VIC (horizontal axis). The FAM probe can hybridize only to the alternate allele (G allele), while VIC probe hybridizes only to reference allele (C allele).
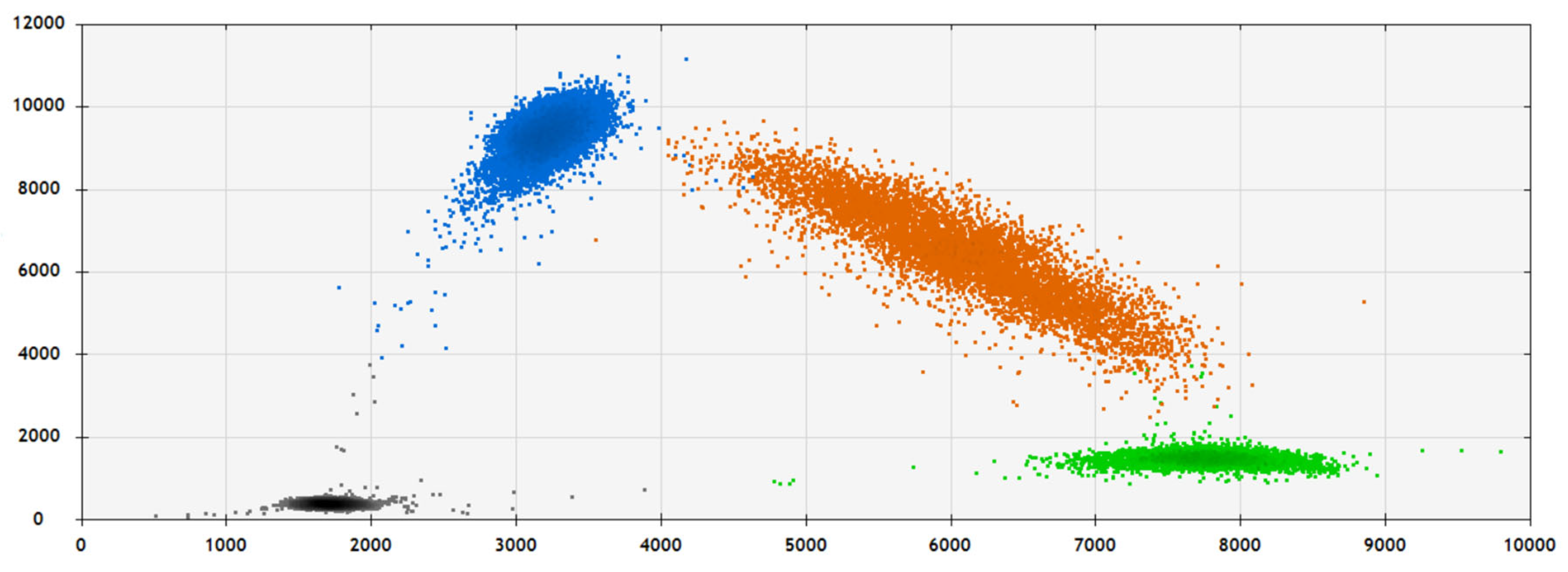

Table 1.
Descriptive statistics of the patient cohort (N=308).
| Characteristic | N = 308 (%) |
|---|---|
| Diagnosis Age (in years) | 57 (9) |
| Unknown | 1 |
| Race | |
| African American | 212 (69%) |
| Caucasian | 95 (31%) |
| Unknown | 1 |
| Diagnosis PSA (ng/ml) | |
| 1:<4 | 72 (24%) |
| 2:4-9 | 193 (63%) |
| 3:10-20 | 31 (10%) |
| 4:>20 | 10 (3.3%) |
| Unknown | 2 |
| Pathologic T Stage | |
| T2 | 228 (74%) |
| T3-4 | 80 (26%) |
| Biopsy Gleason | |
| ≤6 | 204 (70%) |
| 7 | 69 (24%) |
| 8-10 | 17 (5.9%) |
| Unknown | 18 |
| Pathologic Gleason | |
| 3+3 | 169 (57%) |
| 3+4 | 76 (26%) |
| 4+3 | 24 (8.2%) |
| 8-10 | 25 (8.5%) |
| Unknown | 14 |
| BCR | 47 (15%) |
| Unknown | 3 |
| Metastasis | 9 (2.9%) |
Table 2.
TP53 rs1800371 and rs1042522 SNP association analysis.
| SNP | TP53 rs1800371 SNP | TP53 rs1042522 SNP | |||||
|---|---|---|---|---|---|---|---|
| Patient Characteristics | GG, N = 302 |
GA, N = 6 |
p-value | GG, N=87 | GC, N=137 | CC, N=84 | p-value |
| Diagnosis Age | 57 (9) | 56 (12) | 0.6 | 58 (9) | 57 (8) | 57 (9) | 0.8 |
| Unknown | 1 | 0 | 0 | 1 | 0 | ||
| Race | 0.2 | <0.001 | |||||
| African American | 206 (68%) | 6 (100%) | 81 (93%) | 87 (64%) | 44 (52%) | ||
| Caucasian | 95 (32%) | 0 (0%) |
6 (6.9%) | 49 (36%) | 40 (48%) | ||
| Unknown | 1 | 0 | 0 | 1 | 0 | ||
| Diagnosis PSA | 0.085 | 0.8 | |||||
| 1: <4 | 70 (23%) | 2 (33%) |
22 (25%) | 28 (21%) | 22 (26%) | ||
| 2: 4-9 | 191 (64%) | 2 (33%) |
55 (63%) | 87 (64%) | 51 (61%) | ||
| 3: 10-20 | 30 (10%) | 1 (17%) |
9 (10%) | 14 (10%) | 8 (9.5%) | ||
| 4: >20 | 9 (3.0%) |
1 (17%) |
1 (1.1%) | 6 (4.4%) | 3 (3.6%) | ||
| Unknown | 2 | 0 | 0 | 2 | 0 | ||
| Pathologic T Stage | >0.9 | 0.6 | |||||
| T2 | 223 (74%) | 5 (83%) |
57 (68%) | 104 (76%) | 59 (70%) | ||
| T3-4 | 79 (26%) | 1 (17%) |
22 (25%) | 33 (24%) | 25 (30%) | ||
| Biopsy Gleason | 0.2 | 0.8 | |||||
| ≤6 | 199 (70%) | 5 (83%) |
57 (68%) | 93 (73%) | 54 (69%) | ||
| 7 | 69 (24%) | 0 (0%) |
21 (25%) | 27 (21%) | 21 (27%) | ||
| 8-10 | 16 (5.6%) | 1 (17%) |
6 (7.1%) | 8 (6.2%) | 3 (3.8%) | ||
| Unknown | 18 | 0 | 3 | 9 | 6 | ||
| Pathologic Gleason | 0.6 | >0.9 | |||||
| 3+3 | 164 (57%) | 5 (100%) | 46 (55%) | 74 (57%) | 49 (60%) | ||
| 3+4 | 76 (26%) | 0 (0%) |
22 (26%) | 35 (27%) | 19 (23%) | ||
| 4+3 | 24 (8.3%) | 0 (0%) |
7 (8.3%) | 10 (7.8%) | 7 (8.6%) | ||
| 8-10 | 25 (8.7%) | 0 (0%) |
9 (11%) | 10 (7.8%) | 6 (7.4%) | ||
| Unknown | 13 | 1 | 3 | 8 | 3 | ||
| BCR | 47 (16%) | 0 (0%) |
0.6 | 13 (15%) | 20 (15%) | 14 (17%) | >0.9 |
| Unknown | 3 | 0 | 1 | 1 | 1 | ||
| Metastasis | 8 (2.6%) |
1 (17%) |
0.2 | 3 (3.4%) | 6 (4.4%) | 0 (0%) |
0.2 |
Table 3.
Association of TP53 SNPs with time to biochemical recurrence.
| Position | SNP | Location | HR | P |
|---|---|---|---|---|
| chr17:7667612:A:G | rs4968186 | downstream | 1.753 | 0.004 |
| chr17:7676963:G:A | rs9894227 | intronic | 1.720 | 0.007 |
| chr17:7676734:C:T | rs8079544 | intronic | 1.632 | 0.020 |
| chr17:7676154:G:C | rs1042522 | exonic | 1.523 | 0.046 |
| chr17:7664197:C:T | rs35119871 | intergenic | 1.461 | 0.046 |
| chr17:7675519:A:G | rs1794287 | intronic | 1.508 | 0.058 |
| chr17:7676230:G:A | rs1800371 | exonic | 1.473 | 0.067 |
Time to events (BCR) were included in a Cox PH model adjusting for age at diagnosis, race, and Gleason score to examine SNP effects.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



