
Submitted:
17 April 2023
Posted:
18 April 2023
You are already at the latest version
Abstract
Introduction Prostate Cancer (PCa) exhibits one of the widest racial and socioeconomic disparities. PCa disparities have also been widely linked to location as living in more deprived regions was associated with lower healthcare access and worse outcomes. This study aims to examine PCa survival across various US counties in function of different socioeconomic profiles and discuss the role of potential intermediary factors.
Methods The SEER database linked to county-level SES was utilized. Five-year PCa-specific survival using the Kaplan Meier method was performed for 5 racial/ethnic categories in function of SES quintiles. Multilevel Cox proportional hazards regression was performed to assess the relationship between county-level SES and PCa survival. Multivariate regression analysis was performed to examine the role of healthcare utilization and severity.
Results 279,000 PCa records were extracted, 5-year PCa-specific survival was 94%. Overall, living in counties with worst poverty/income quintile and highest proportions of foreign-born/language-isolated increased PCa mortality by 23% each. No association was observed with county-level High-School education, while Bachelor’s-level education decreased mortality risk by 23%. Associations varied considerably upon racial/ethnic stratification. Multilevel analyses showed varying contributions of individual and area-level factors to survival within minorities. The relationship between SES and PCa survival appeared to be influenced by healthcare utilization and disease stage/grade.
Discussion Racial/ethnic categories responded differently under similar county-level SES and individual-level factors to the point where disparities reversed in Hispanics. The inclusion of Healthcare utilization and severity factors may provide partial early support for their role as intermediaries. Healthcare access (insurance) might not necessarily be associated with better PCa survival, through performing biopsy and or/surgery. County-level education plays an important role in PCa decision-making as it might elucidate discussions of other non-invasive management options.
Conclusion Findings of this study demonstrate that interventions need to be tailored according to each group's needs. This potentially informs the focus of public health efforts in terms of planning and prioritizing. This study could also direct further research delving into pathways between area-level characteristics with PCa survival.
Keywords:
Prostate Cancer
; Survival
; Disparities
; Geographic
; Multilevel
; Healthcare Access
Introduction
Prostate cancer (PCa) is the second leading cause of death and the most common cancer in men residing in the U.S. [1]. Although survival from PCa is relatively very high to other malignancies, remarkable disparities in PCa outcomes have been reported across multiple settings and series. For example, Non-Hispanic Blacks (NHB), on average, have a 78% higher incidence of PCa as compared to Non-Hispanic Whites (NHW) in their lifetimes [1,2,3,4]. Furthermore, PCa is more aggressive and occurs at a younger age in AA men resulting in a 2.3-fold increase in mortality rate (vs. NHW) [3,4,5]. Additionally, Hispanics and some populations of individuals of Asian descent have lower PCa incidence, however, suffer from more advanced disease at diagnosis [4,5,6].
PCa outcomes are sensitive to geographic locations [7], as disparities vary based on area-level characteristics at multiple geographic scales [7,8,9]. Hispanics living in Mexico have a lower incidence than Hispanics living in the Caribbean [10] while Puerto Ricans living in Puerto Rico have a lower incidence than Puerto Ricans living in the mainland U.S. [11] suggesting that geographical elements may help to explain PCa disparities.
Existing literature supports the view that disparities emerge, in part, due to inequalities in access to adequate healthcare (HC) that vary across race and socioeconomic status [12,13]. As an example, NHBs with PCa experienced delays in care and were less likely to undergo definitive management such as surgery [2,14]. Most importantly, advances in imaging and procedures, and surgical access are critical in PCa [15] as they appear to interfere with disparities in outcomes. For example, NHBs, lower socioeconomic status, and older age were found to be associated with underutilization of PCa diagnostic imaging (Deville). More importantly, Multiparametric Magnetic Resonance Imaging (mpMRI) fusion-guided biopsy, a revolutionary technique in accurately diagnosing and staging PCa was less likely to be performed by NHBs even though it has been found to possess better performance indicators in that group as compared to NHW [16,17]. Disparities in PCa outcomes after treatment were noted as worse bowel and urinary functions were reported by men from racial/ethnic minorities suggesting receipt of lower-quality treatment [18]. Additionally, disparities decreased in magnitude in equal-access samples like the Veterans Health Administration, indicating non-clinical causal pathways for PCa disparities [19].
To date, area-level PCa disparities in survival have been mostly studied across NHW and NHB and in relatively smaller geographical scales such as neighborhoods or zip codes [20,21,22]. Some evidence suggests that associations between area-level SES and PCa measure highly rely on the geographical scale chosen [23,24,25]. The goal of the present study was to describe differences in PCa outcomes across an expanded category of racial/ethnic groups, to examine whether county-level SES helped to explain disparities in PCa survival, and understand how potential factors influence any established association between county-level SES and PCa survival.
Methods
Data sources and study population
Disparities in five-year PCa survival were estimated by race/ethnicity and SES. The study cohort was derived from the SEER cancer database. The SEER (NCI) program provides valuable information on various cancer statistics as it’s a population-based cohort that covers around one-third of the US population and contains a larger proportion of foreign-born, thereby facilitating studies of racial and ethnic disparities [26].
Outcome definition
The primary outcome of this study is 5-year PCa survival. Cancer-specific mortality was utilized to ascertain net survival and; probability of surviving PCa in the absence of other causes of death. We included biopsy-confirmed diagnoses among men aged 18 years and older. Analyses focused on diagnoses initiated from January 1st, 2007, to December 31st, 2011, followed up for at least five years through December 31st, 2016. Participants who had missing information on survival follow-up were excluded (11.4%), however, this did not result in a selection bias as no significant differences in racial composition and SES status were found in the excluded sample. Disease severity was also described through a later SEER summary stage at diagnosis (distant) and a more aggressive Gleason Score (GS = 8–10).
Race/Ethnicity and Risk Factors
Groups included all five races/ethnicities within the SEER registry: NHW, NHB, Non-Hispanic Asian or Pacific Islander (NHAPI), Non-Hispanic American Indian or Alaska Native (NHAI/AN), and Hispanics (HISP). Individual characteristics selected were factors that are known to be associated with PCa survival such as age, marital status, stage at diagnosis, and GS [27,28]. Healthcare (HC) access was ascertained through individual-level insurance status, while HC utilization was through having a GS done and PCa-directed surgery.
Socioeconomic Status (SES)
Area-based SES was derived from the SEER linkage with the American Community Survey (ACS). County-level 5-year ACS were collected for each case enclosed in its corresponding county. The 2007–2011 5-year ACS linkage was selected as it would reflect the SES of the selected PCa cohort diagnosed between 2007–2011. County-level SES represented income (median household income), material deprivation (percentage of individuals 150% below poverty level, percentage of family below poverty level, unemployment rates), social class levels (percentage of individuals with less than high-school education, percentage of individuals with at least a bachelor-level education) and population composition (percentage of foreign-born, percentage of language isolation). Such variables are often included in health outcomes research relating poorer SES status with poorer health outcomes such as higher mortality [29,30]. SES characteristics were classified into quintiles, ranging from worse to best. Because some variables tend to explain very similar constructs, composite indices have been created. “Percentage of individuals 150% below poverty level”, “percentage of family below poverty level”, and “median household income” have been grouped into a single index named “Poverty/Income”. “Percentage of foreign-born”, “percentage of language isolation” have also been grouped into a single index called “Foreign-born/language-isolation”.
Statistical Analysis
Overall baseline characteristics were examined for significance using the chi-square test. 5-year prostate cancer-specific survival was determined using the official software for the SEER database, SEERStat. The end of follow-up status was either "dead" or "alive" and intervals were in months, totaling 60 months. Kaplan-Meier curves were used to examine 5-year survival for racial/ethnic groups in the lowest and highest SES quintiles and log-rank test to examine equality for survival functions.
Cox-proportional hazard models assessed relationships between county-level SES and PCa survival [31]. The model was adjusted for established and independent risk factors for poorer PCa survival; age, and marital status, and stratified by races/ethnicities to assess in-between groups disparities. We used the variance inflation factor (VIF) to verify the absence of multicollinearity [32]. Because worse PCa can often be predicted by poorer access to care and more severe disease [12], individual-level factors measuring those were also included in subsequent modeling to compare results with and without them.
Because observations are located within the county of residence, geographical clustering was plausible and a multilevel survival cox proportional hazards model with mixed effects incorporating cluster-specific random effects that could potentially modify the baseline hazard function was performed and an exponential distribution was specified. A multivariate logistic regression examining the relationship between SES and advanced disease (i.e.: Distant stage and GS 8–10) and healthcare utilization (having a GS and undergoing PCa-directed surgery) was performed. Stata v.16 was utilized for statistical analyses and a p-value of less than 0.05 was considered statistically significant.
Results
Table 1 represents the baseline characteristics of participants stratified by race/ethnicity. The total number of participants was 279,000. NHB expectedly exhibited the youngest age at diagnosis at 63.6 years. Five-year PCa survival ranged between 93% and 94% in all groups except NHAI/AN which had the lowest survival (88%). NHB, NHAPI, and Hispanics had the most advanced stage at diagnosis and were also found to have the highest proportion of GS ≥ 8. Although PCa-directed surgery was present in slightly less than half of the patients, NHAI/AN and NHB were the least to undergo one. More than half of the groups had medical insurance at diagnosis while NHAI/AN, HISP, and NHAPI had the highest percentage of Medicaid-insured patients. NHW had the lowest rates of uninsured while NHB had the highest (Table 1).
Hispanics resided in counties with the worst education where almost half (42.2%) had the highest percentage of less than high school education (<HS) and only 12.6% achieved at least a bachelor’s-level education (≥BL). More than one-third of NHAPI and NHB resided in counties with the highest poverty/income. Almost half of NHAPIs (45%) and HISP (41%) resided in counties with the highest concentrations of foreign-born/language isolated (Table 1).
Figure 1 provided Kaplan Meier survival curves for individuals in the lowest and highest quintiles of SES variables stratified by racial/ethnic groups throughout the five-year follow-up. Log-rank test was statistically significant for all the plots included. For each graph, observations were restricted to the most and the least deprived quintiles to illustrate racial/ethnic comparisons in survival throughout extreme SES variations. Lowest survival was observed within the worst quintiles of “Poverty/Income” as well as “<HS” education. NHAI/AN exhibited the poorest survival rates within all five most deprived SES quintiles. NHW kept having the highest survival even in counties with the worst unemployment and poverty/income rates. NHAPI had the highest survival in counties with the lowest foreign/born-language isolation rates while HISP had the highest survival in counties with the best HS education (Q1 of <HS) (Figure 1).
Table 2 represents the cox-proportional hazard model in function of SES for the overall population and then stratified into racial/ethnic groups. For every SES variable, worst SES quintile is compared to the best SES quintile. Overall, living in a county with the worst poverty/income rates and highest proportions of foreign-born/language-isolated had a significant 23% increase in the risk of PCa mortality (p < 0.01). On the contrary, living in a county with the highest rates of ≥BL education and unemployment had a significant protective effect on PCa survival (HR 0.77, 95%CI 0.70–0.85) and HR 0.89, 95%CI 0.83–0.95 respectively). County-level HS education did not have a significant effect on PCa survival except in HISP where <HS education doubled the risk of PCa mortality. Upon stratification, same statistically significant directions remained in NHW while they almost completely disappeared in the remaining groups, however, the higher mortality risk associated with worst poverty/income remained. Highest rates of “≥BL” had a considerate and significant protective effect in NHAI/AN (HR 0.17, 0.05–0.97, p < 0.05), however, their survival was extensively affected by highest proportions of foreign-born/language-isolated (HR 6.6, 1.17–35.76, p < 0.05). PCa survival in NHAPI men was not statistically affected by any SES factor included.
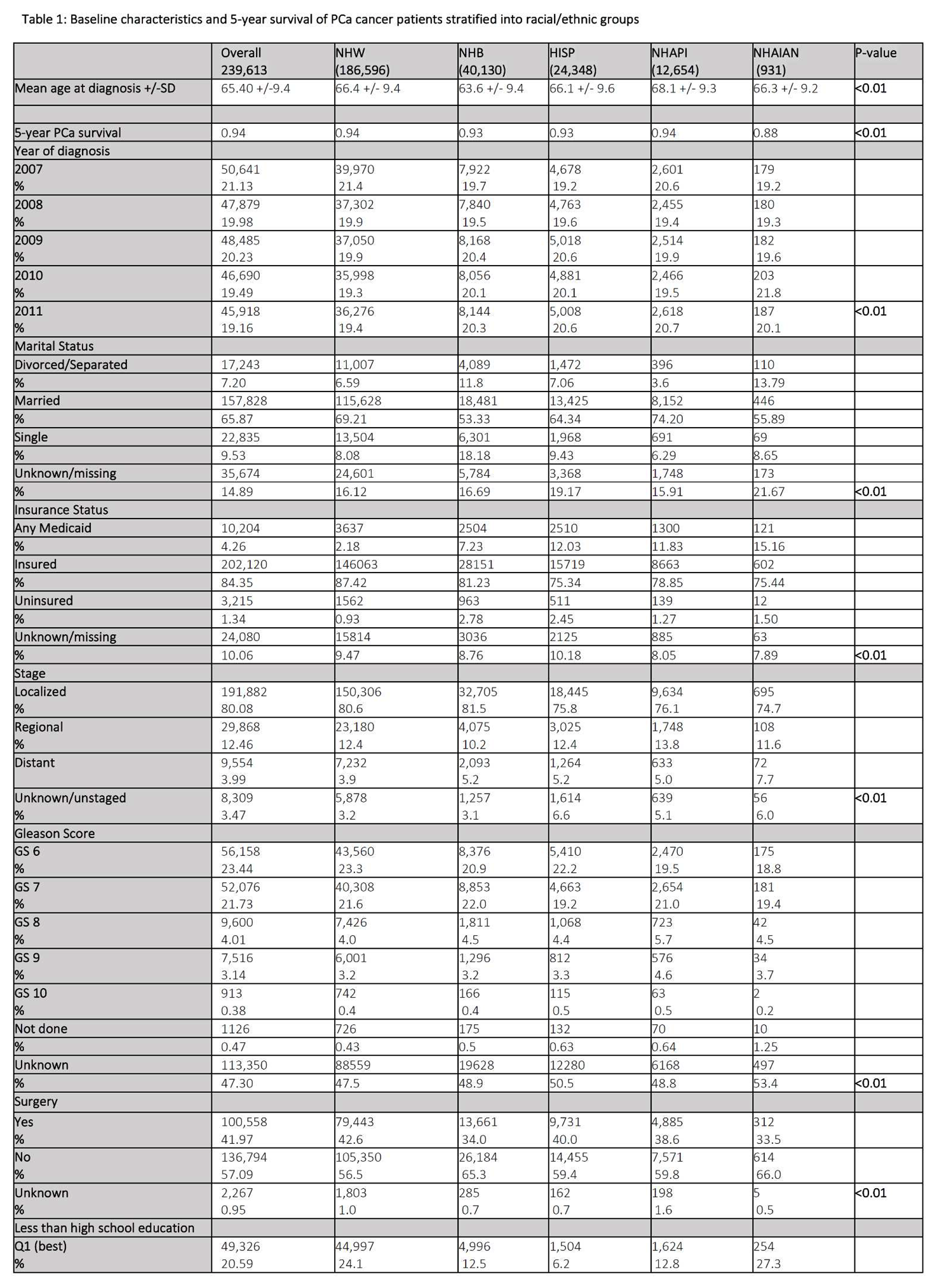
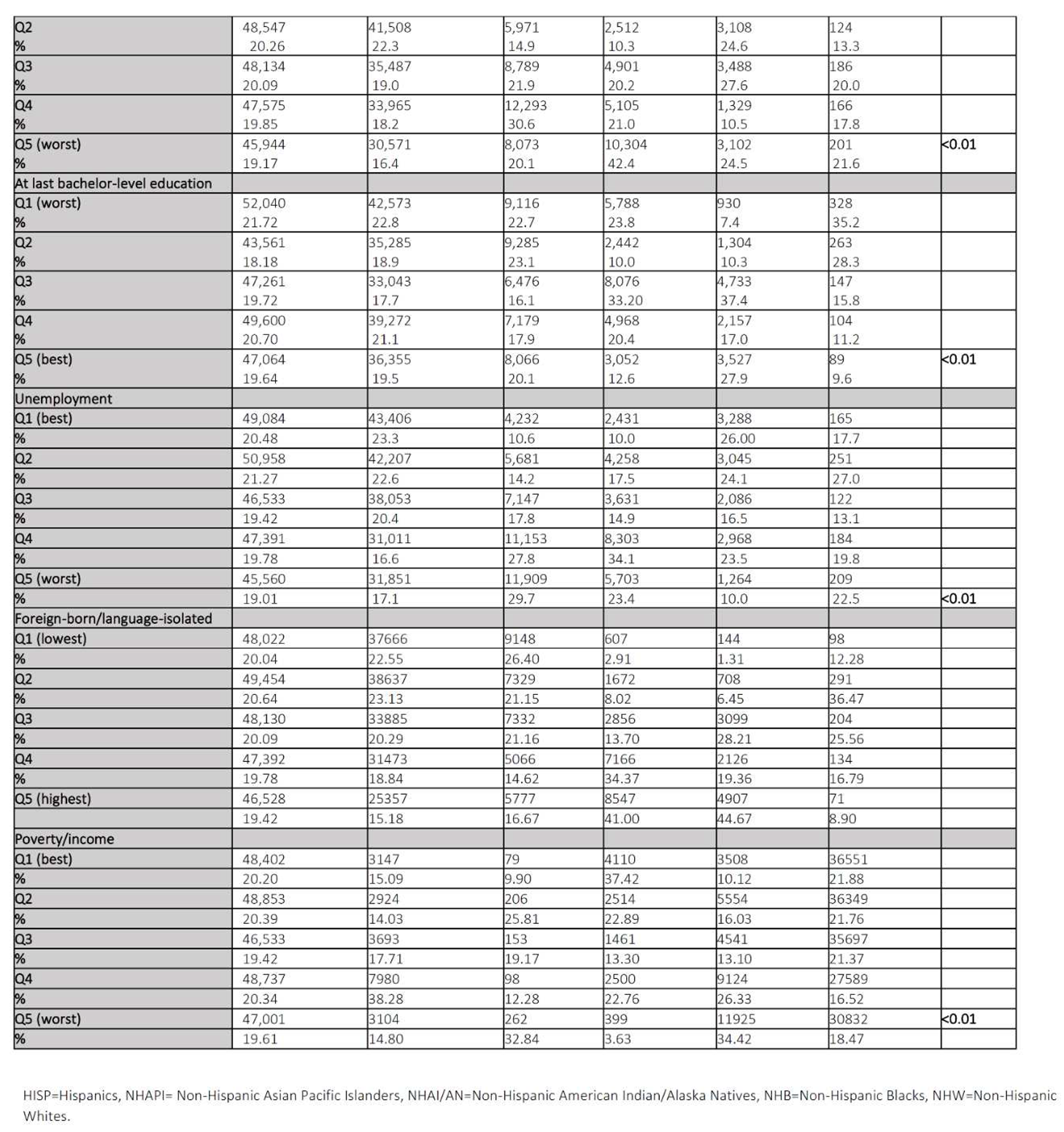
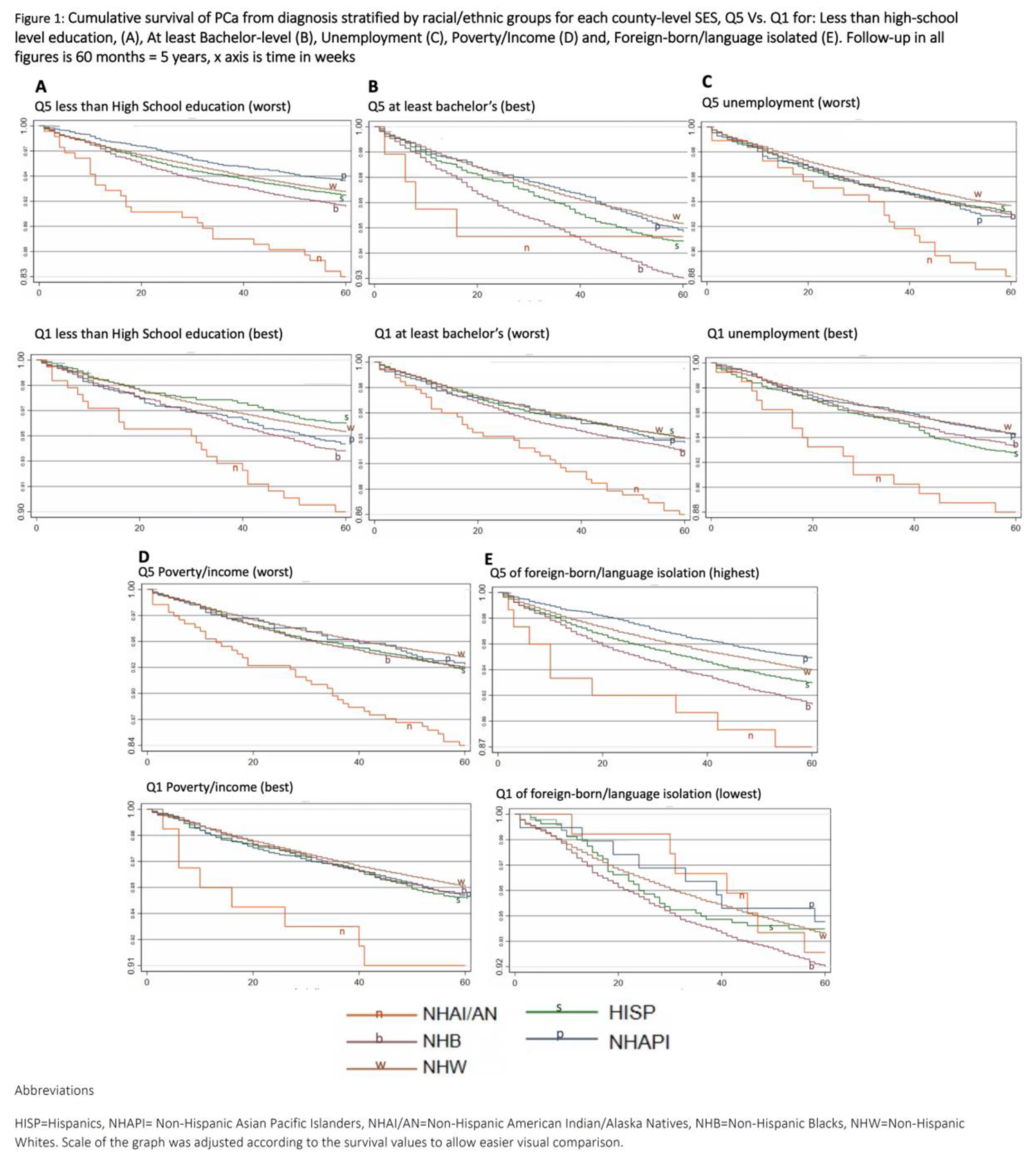
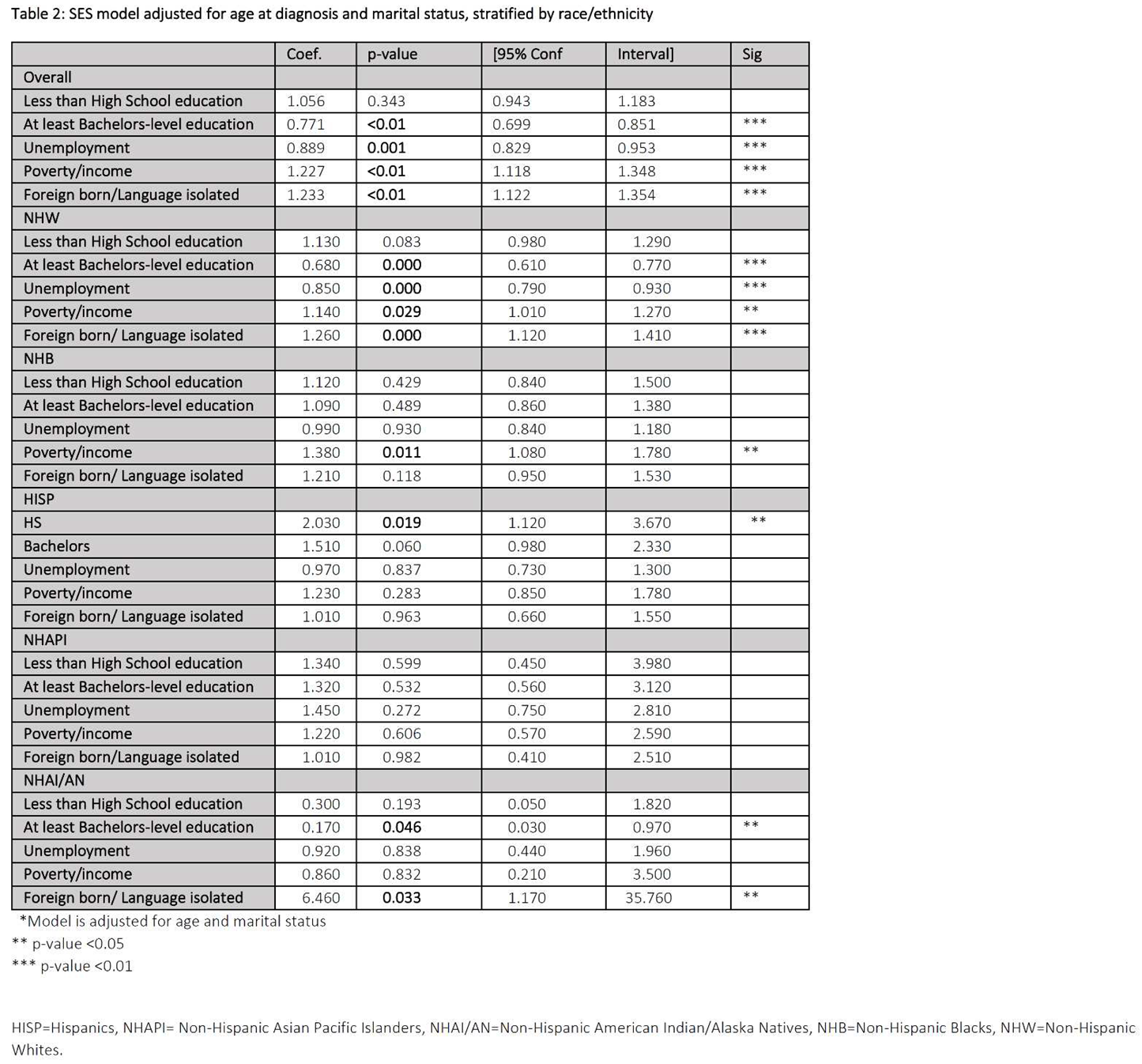
Table 3 illustrates our multilevel analysis, which accounts for county-level clustering effects. Model 1 represents group-level cox proportional HR with NHW as the reference, adjusted for marital status and age. Model 2: adjusted for model 1 covariates and county-level SES covariates. Model 3: adjusted for model 2 covariates and individual-level covariates. HISP men were at higher risk of PCa mortality in models 1 and 2, however, upon adjusting for county-and individual-level covariates, HISP exhibited lower mortality than NHW (0.89, 95%CI 0.85–0.95, p < 0.01). NHAI/AN had twice the mortality of NHW in both models 1 and 2. This disparity was attenuated in model 3 when accounting for individual-level factors such as insurance and cancer severity and treatment (surgery). NHB (vs. NHW) were 1.6 times more likely to die from PCa in models 1 and 2, however, such disparity decreased to 1.2 (95%CI 1.07–1.6, p = 0.01) in model 3. The protective effect in NHAPIs was further increased in model 3 (0.68, 95%CI 0.62–0.74).
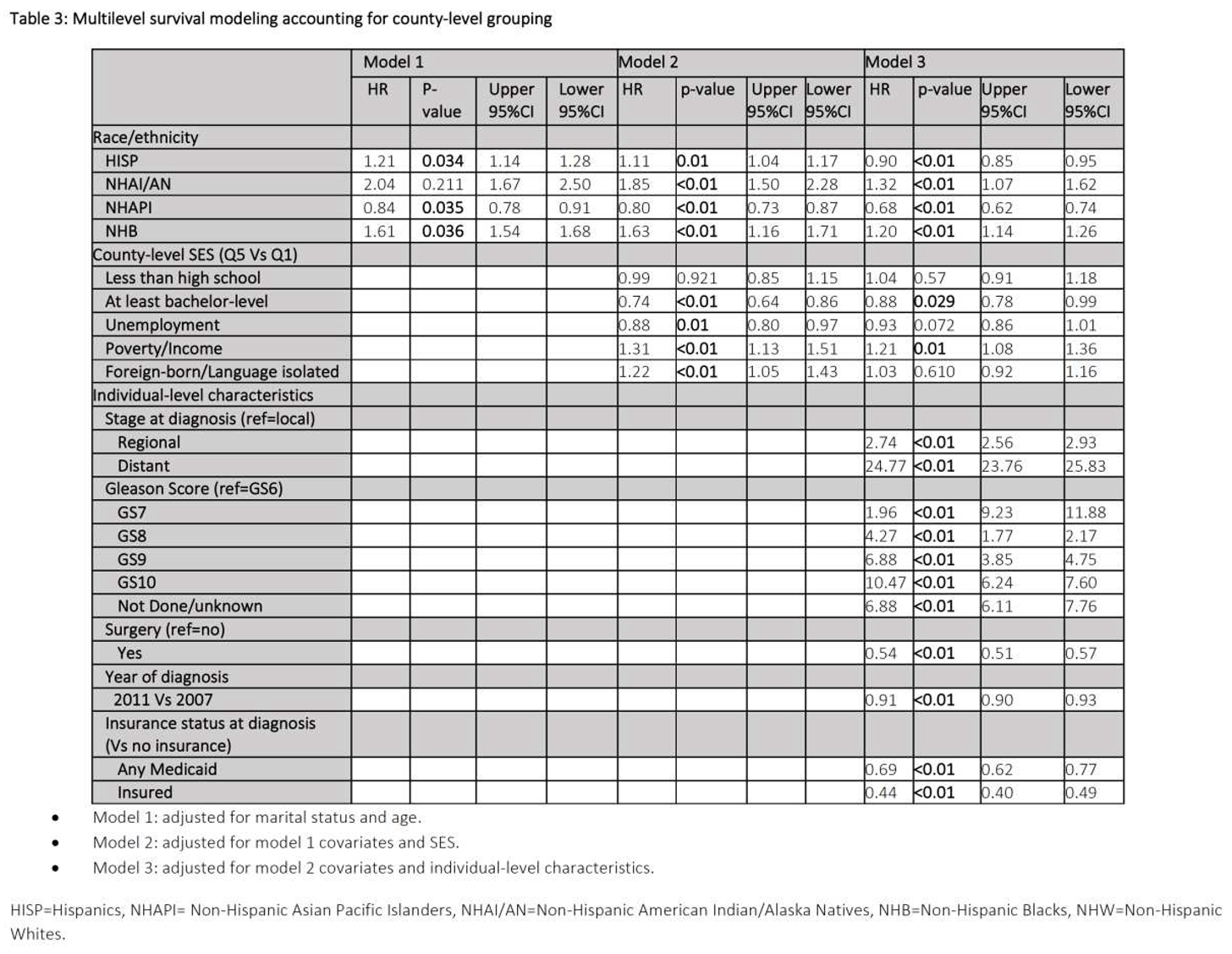
All county-level SES (except “<HS”) were significantly associated with 5-year PCa survival in all races/ethnic groups in model 2. Upon adjusting for disease severity and surgery in model 3, the significant association only remained for ≥BL and poverty/income. Having a distant stage and advanced GS was significantly associated with the worst survival while undergoing a PCa-directed surgery and having insurance were the most protective covariates. As “diagnosis year” advanced, risk of PCa-specific mortality decreased (0.72, 95%CI 0.68–0.77).
Table 4 examines the relationship between SES and disease severity (“Stage” and “GS”) and HC access/utilization (“GS not done” and “surgery”). The risk of having a distant stage significantly increased by around 30% and 20% with worst “<HS” (RR 1.27 95%CI 1.19–1.36) and poverty/income (RR 1.2 95%CI 1.13–1.23). The risk of having a worse GS (GS = 8–10) significantly decreased with highest proportion of “≥BL” (RR 0.9 95%CI 0.86–0.95). Highest rates of foreign-born/language-isolated rates significantly protected against the highest GS (RR 0.91 95%CI 0.86–0.95).
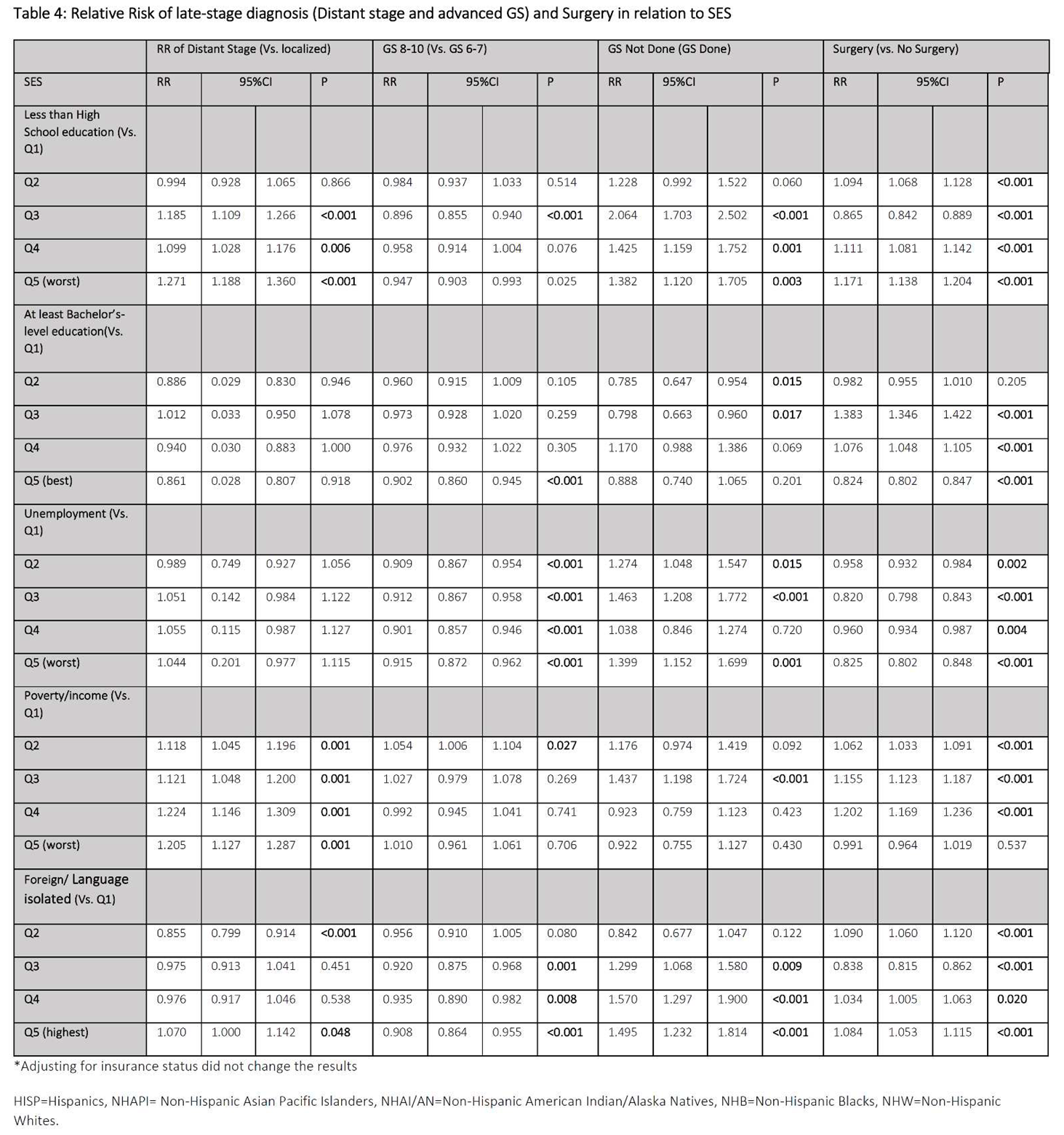
The risk of “GS not done” significantly decreased with better education (both “<HS” and “≥BL”). Residing in a county with the highest unemployment rate significantly increased the risk of having a “GS not done” by 40% (1.40 95%CI 1.52–1.69). The highest percentage of foreign-born/language-isolated increased the risk of not doing a GS by half (RR 1.50 95%CI 1.23–184). The risk of having surgery varied according to education level; where it increased with lower HS and decreased with higher “≥BL” education rates. Finally, residing in a county with the worst unemployment and poverty rates significantly decreased the risk of surgery while foreign-born/language-isolation significantly increased it (Table 4).
Discussion
The goal of the present study was to describe the degree to which county-level SES explained PCa survival in U.S. residents across a wide group of races and ethnicities. To our knowledge, this is the first study to examine the association between county-level SES and PCa-specific survival across five different racial/ethnic categories. In addition to other studies in the literature, our study included five racial/ethnic categories and examined how survival changes specifically in response to county-level SES profile in each racial/ethnic category included. Additionally, this study examined the potential pathway leading to worse PCa survival by demonstrating the influence of late-stage diagnosis and poorer healthcare utilization. Such analysis highlights how PCa survival behaves in the function of race/ethnicity under different SES profiles and informs public health policies on potential county-level interventions to decrease the disparity gaps in PCa.
Overall, lower area-level SES was associated with reduced PCa survival, which was in agreement with the literature examining a similar relationship, however, on a neighborhood level [20,21,22]. For example, a systematic review of 169 international publications established that men living in disadvantaged and/or rural areas face a greater PCa burden [33]. They also had consistently lower prostate-specific antigen (PSA) testing and PCa incidence, poorer survival, more advanced disease, and higher mortality [33]. DeRouen et al. also established a relationship between poorer neighborhood SES and poor PCa survival. Similarly, to our study, they found that although NHB had worse survival than NHW, the relationship was attenuated when accounting for neighborhood-level SES [21]. Our positive associations between county-level education and PCa stage/grade were also similarly found on the neighborhood level [22]. When adjusting for county-level SES (model 2, Table 3), PCa survival disparities between groups only slightly attenuated, suggesting other factors may have contributed to survival disparities between groups. Those could have been related to rural/urban status, commuting and traffic patterns, residential mobility, and/or food environment [21,22].
Racially stratified findings illustrated within-group disparities in 5-year prostate-specific survival suggesting varying county-level SES associations across race/ethnicity. NHW were more sensitive to changes in county-level SES while remaining minorities were not. In fact, education (≥BL), unemployment, and foreign-born/language-isolation did not impact PCa survival in NHB, suggesting that interventions on those factors might not turn out as beneficial on minorities as when applied to NHW. Such findings could also support the diminishing returns hypothesis where minorities might not achieve the same health gains at higher SES as do their nonminority counterparts (NHW) at the same SES levels [34,35,36]. For example, Kish et al identified that mortality risk for NHB increased with higher neighborhood SES compared with NHW in the same SES quintile [20]. Further, higher education was also found to be protective for advanced PCa among men residing in low SES, but not for men residing in high SES California neighborhoods [21] which suggests a varying effect on PCa survival even under similar area-level characteristics.
When adjusting for individual-level factors representing disease severity and HC access/utilization, disparities were diminished further until they even reversed in Hispanics (model 3, Table 3). Additionally, the magnitude of change was the highest in NAHI/AN and NHB as risk of PCa-specific mortality decreased from almost 2 to 1.3 and 1.6 to 1.2 respectively from model 2 to 3 (Table 3). This could suggest that some minority groups might be more sensitive to area-level SES while others more to individual-level SES. Hence, no single method of intervention would be closing all disparity gaps, as those should be carefully crafted and tailored based on each group’s needs. One could even argue that in some minority groups individual-level factors could be driving poorer PCa survival in a way that better county-level SES cannot overcome. As an example, Du Xl et al., found individual-level SES to be accounting for disparities in PCa survival [37].
Analysis demonstrating the association between poorer SES and severity (stage and grade) as well as HC utilization (“GS not done” and “surgery”) may provide partial early support for the view that these factors could play an intermediary role. Since worse stage/grade and poorer HC utilization (surgery/GS not done) were associated with county-level SES and increased the risk of PCa mortality, the inclusion of those factors appeared to strengthen the relationship between SES and PCa survival. More importantly, being insured was significantly protective against PCa mortality, however, adjusting for insurance, did not change the results between SES and HC utilization and disease severity in Table 4. This could show that insurance might not necessarily affect PCa survival by performing biopsy/surgery or by having a better stage at diagnosis, contrary to some findings. Also, men residing in counties with the worst HS education rates were more likely to undergo PCa-directed surgery. Both of these findings could demonstrate how better education in PCa patients leads to more in-depth discussions with healthcare providers about additional less invasive options such as watchful waiting [38]. Other studies suggested that while guaranteeing universal adequate health insurance is important, additional measures are needed to address persisting survival disparities [39,40]. Thus, interventions aiming at enhancing insurance status alone, will likely not improve healthcare utilization for men residing in SES-deprived counties.
On the other hand, protective effect of “year” could be explained by advances in PCa management or could further backup recommendations against routine screening [41] since no increase in mortality was observed. It was surprising that unemployment showed a protective effect in NHW, which became non-significant in subsequent models adjusted for individual-level covariates. Since employment is tied with health insurance in the US, we would normally expect lower HC access (and hence lower survival) caused by higher unemployment rates. However, PCa patients have a mean age between 63–64, where most of those patients would be retired. Thus, detrimental effects of unemployment might not be as pronounced in this sample of elderly patients. Still, this variable was included to test whether unemployment on a county level would show any effect on individual-level survival.
Last, NHAPI men often experienced better cancer survival than the remaining minority groups while NHAI/AN men showed to suffer from worse PCa survival disparities (Figure 1 and Table 3). Also, the six-fold mortality increase in NHAI/AN men residing in counties with the largest proportions of foreign-born/language may suggest that this group faces the strongest health burden when situated within heavily-dense foreign-born population which could be creating even more isolation for this minority group. Such findings illustrate a minority group that is relatively rarely discussed in the literature which warrants further attention and thus more public health, and clinical efforts should be focused on them. Alternatively, men residing in counties with the highest foreign-born/language-isolated proportions tend to be protected against a more aggressive GS which could be explained by the social support phenomenon where minorities exhibit better outcomes when socially surrounded and supported [42,43].
Strengths and limitations
This study has several strengths including its population-based design that covers almost one-third of the American population and its linkage to SES characteristics. To our knowledge, this study is the first study to relate county-level SES with PCa survival. Additionally, this study described how PCa survival varies across five racial/ethnic groups under different county-level SES profiles and the role of HC utilization and disease severity.
Although some suggest that census tract-level analyses might detect more accurate relationships between area-level factors and individual health outcomes [23,25], our adoption of the county-level might have been beneficial for delving deeper into disparities pathways. Meliker et al observed disappearing survival disparities in PCa between NHBs and NHWs when moving their spatial analysis from larger scales (Federal/State Legislative Districts) to neighborhoods [44] suggesting that smaller scales often mimic “SES adjustment” as smaller entities tend to be more homogenous. This likely demonstrates the advantage of adopting relatively larger geographical boundaries to capture racial/ethnic variation of survival and the crucial importance of area-level SES in PCa survival analyses. Further, as a multilevel regression was performed within our analysis, clustering of observations has been accounted for, where findings demonstrate robustness independent of geographical cluster effects.
Despite its strengths, this study has also some limitations. Although missing data was kept at minimum in almost all covariates included (1% to 11.4%), the only exception was the large proportion of “unknown” values in GS. Despite this large percentage, “unknown” proportions remained the same across all racial/ethnic groups suggesting that missing results are not related to one group or another. Nonetheless, the absence of time-varying covariates could have also affected the estimate as, for instance, some patients could have migrated to another geographical location just after diagnosis. Furthermore, the absence of chemotherapy/radiation therapy data would have been informative in the context of individual-level variables' impact on PCa survival. Still, access to those would have been also linked to insurance status, a variable that was accounted for. Lastly, the smaller sample of NHAI/AN as compared to remaining groups could have impacted group comparability. Due to the small NHAI/AN population, a longer period for incident cases could be adopted in the future to better represent variability within that group.
Conclusions
Overall, this study provides insight into the impact of county-level SES on 5-year PCa survival as risk of PCa-specific mortality for five ethnic/racial groups in the US. Using findings of this study could potentially inform the focus of public health efforts. As such, this study provides insight into the rising need to tailor interventions based on race/ethnicity and SES so that the benefit can be provided equitably. Future studies could benefit from performing mediation analysis for factors influencing the relationship between SES and PCa outcomes in order to more deeply understand pathways leading to PCa disparities.
Funding
This research received no external funding.
Disclosures
Dr. Christiane El Khoury: no disclosures exist. Dr. Sean Clouston: no disclosures exist.
Data Availability Statement
The SEER database is publicly available, with free access. In case additional information is needed regarding data analysis, we are happy to share STATA files.
References
- American Cancer Society. Cancer Facts and Figures 2021. American Cancer Society, 2021. Available online: https://www.cancer.org/con-tent/dam/cancer-org/research/cancer-facts-and-statistics/annual-can-cer-facts-and-figures/2021/cancer-facts-and-figures-2021.pdfTaggedEnd. (accessed on 17 February 2021).
- Zavala, V.A.; Bracci, P.M.; Carethers, J.M.; Carvajal-Carmona, L.; Coggins, N.B.; Cruz-Correa, M.R.; Davis, M.; de Smith, A.J.; Dutil, J.; Figueiredo, J.C.; et al. Cancer health disparities in racial/ethnic minorities in the United States. Br. J. Cancer 2021, 124, 315–332. [Google Scholar] [CrossRef] [PubMed]
- Siegel, R.L.; Miller, K.D.; Jemal, A. Cancer statistics, 2020. CA Cancer J. Clin. 2020, 70, 7–30. [Google Scholar] [CrossRef] [PubMed]
- DeSantis, C.E.; Miller, K.D.; Goding Sauer, A.; Jemal, A.; Siegel, R.L.; Msph, A.G.S.; Dvm, A.J. Cancer statistics for African Americans, 2019. CA: A Cancer J. Clin. 2019, 69, 211–233. [Google Scholar] [CrossRef] [PubMed]
- Chornokur, G.; Dalton, K.; Borysova, M.E.; Kumar, N.B. Disparities at presentation, diagnosis, treatment, and survival in African American men, affected by prostate cancer. Prostate 2011, 71, 985–997. [Google Scholar] [CrossRef] [PubMed]
- Tyson, M.D., 2nd; Castle, E.P. Racial disparities in survival for patients with clinically localized prostate cancer adjusted for treatment effects. Mayo Clin. Proc. 2014, 89, 300–307. [Google Scholar] [CrossRef]
- Coughlin, S.S. A review of social determinants of prostate cancer risk, stage, and survival. Prostate Int. 2020, 8, 49–54. [Google Scholar] [CrossRef]
- Freeman, V.L.; Ricardo, A.C.; Campbell, R.T.; Barrett, R.E.; Warnecke, R.B. Association of census tract-level socioeconomic status with disparities in prostate cancer-specific survival. Cancer Epidemiology Biomarkers Prev. 2011, 20, 2150–2159. [Google Scholar] [CrossRef]
- Gomez, S.L.; Shariff-Marco, S.; DeRouen, M.; Keegan, T.H.; Yen, I.H.; Mujahid, M.; Satariano, W.A.; Glaser, S.L. The impact of neighborhood social and built environment factors across the cancer continuum: Current research, methodological considerations, and future directions. Cancer 2015, 121, 2314–2330. [Google Scholar] [CrossRef]
- Pinheiro, P.S.; Sherman, R.L.; Trapido, E.J.; Fleming, L.E.; Huang, Y.; Gomez-Marin, O.; Lee, D. Cancer incidence in first generation U.S. Hispanics: Cubans, Mexicans, Puerto Ricans, and new Latinos. Cancer Epidemiology Biomarkers Prev. 2009, 18, 2162–2169. [Google Scholar] [CrossRef]
- Ho, G.Y.; Figueroa-Vallés, N.R.; De La Torre-Feliciano, T.; Tucker, K.L.; Tortolero-Luna, G.; Rivera, W.T.; Jiménez-Velázquez, I.Z.; Ortiz-Martínez, A.P.; Rohan, T.E. Cancer disparities between mainland and island Puerto Ricans. Rev Panam Salud Publica 2009, 25, 394–400. [Google Scholar] [CrossRef]
- Clouston, S.A.P.; Link, B.G. A retrospective on fundamental cause theory: State of the literature, and goals for the future. Annu. Rev. Sociol. 2021, 47, 131–156. [Google Scholar] [CrossRef] [PubMed]
- Ward, E.; Jemal, A.; Cokkinides, V.; Singh, G.K.; Cardinez, C.; Ghafoor, A.; Thun, M. Cancer disparities by race/ethnicity and socioeconomic status. CA: A Cancer J. Clin. 2004, 54, 78–93. [Google Scholar] [CrossRef] [PubMed]
- Mahal, B.A.; Aizer, A.A.; Ziehr, D.R.; Hyatt, A.S.; Lago-Hernandez, C.; Chen, Y.W.; Choueiri, T.K.; Hu, J.C.; Sweeney, C.J.; Beard, C.J.; et al. The association between insurance status and prostate cancer outcomes: implications for the Affordable Care Act. Prostate Cancer Prostatic Dis. 2014, 17, 273–279. [Google Scholar] [CrossRef] [PubMed]
- Washington, C.; Deville, C., Jr. Health disparities and inequities in the utilization of diagnostic imaging for prostate cancer. Abdom Radiol 2020, 45, 4090–4096. [Google Scholar] [CrossRef] [PubMed]
- El Khoury, C.J.; Ros, P.R. A Systematic Review for Health Disparities and Inequities in Multiparametric Magnetic Resonance Imaging for Prostate Cancer Diagnosis. Acad. Radiol. 2021, 28, 953–962. [Google Scholar] [CrossRef] [PubMed]
- Ajayi, A.; Hwang, W.T.; Vapiwala, N.; Rosen, M.; Chapman, C.H.; Both, S.; Shah, M.; Wang, X.; Agawu, A.; Gabriel, P.; et al. Disparities in staging prostate magnetic resonance imaging utilization for nonmetastatic prostate cancer patients undergoing definitive radiation therapy. Adv. Radiat. Oncol. 2016, 1, 325–332. [Google Scholar] [CrossRef]
- Orom, H.; Biddle, C.; Underwood, W., 3rd; Homish, G.G.; Olsson, C.A. Racial or Ethnic and Socioeconomic Disparities in Prostate Cancer Survivors' Prostate-specific Quality of Life. Urology 2018, 112, 132–137. [Google Scholar] [CrossRef]
- Dess, R.T.; Hartman, H.E.; Mahal, B.A.; Soni, P.D.; Jackson, W.C.; Cooperberg, M.R.; Amling, C.L.; Aronson, W.J.; Kane, C.J.; Terris, M.K.; et al. Association of Black Race With Prostate Cancer–Specific and Other-Cause Mortality. JAMA Oncol. 2019, 5, 975–983. [Google Scholar] [CrossRef]
- Kish, J.K.; Yu, M.; Percy-Laurry, A.; Altekruse, S.F. Racial and ethnic disparities in cancer survival by neighborhood socioeconomic status in Surveillance, Epidemiology, and End Results (SEER) Registries. JNCI Monogr. 2014, 2014, 236–243. [Google Scholar] [CrossRef]
- DeRouen, M.C.; Schupp, C.W.; Koo, J.; Yang, J.; Hertz, A.; Shariff-Marco, S.; Cockburn, M.; Nelson, D.O.; Ingles, S.A.; John, E.M.; et al. Impact of individual and neighborhood factors on disparities in prostate cancer survival. Cancer Epidemiology 2018, 53, 1–11. [Google Scholar] [CrossRef]
- DeRouen, M.C.; Yang, J.; Jain, J.; Weden, M.M.; Gomez, S.L.; Shariff-Marco, S. Disparities in Prostate Cancer Survival According to Neighborhood Archetypes, A Population-Based Study. Urology 2021. epub ahead of print. [Google Scholar] [CrossRef] [PubMed]
- Oliver, M.N.; Smith, E.; Siadaty, M.; Hauck, F.R.; Pickle, L.W. Spatial analysis of prostate cancer incidence and race in Virginia, 1990–1999. Am. J. Prev. Med. 2006, 30 (Suppl. 2), S67–S76. [Google Scholar] [CrossRef] [PubMed]
- Thornton, L.E.; Pearce, J.R.; Kavanagh, A.M. Using Geographic Information Systems (GIS) to assess the role of the built environment in influencing obesity: a glossary. Int. J. Behav. Nutr. Phys. Act. 2011, 8, 71. [Google Scholar] [CrossRef] [PubMed]
- Krieger, N.; Chen, J.T.; Waterman, P.D.; Soobader, M.J.; Subramanian, S.V.; Carson, R. Geocoding and monitoring of US socioeconomic inequalities in mortality and cancer incidence: does the choice of area-based measure and geographic level matter?: the Public Health Disparities Geocoding Project. Am. J. Epidemiology 2002, 156, 471–482. [Google Scholar] [CrossRef] [PubMed]
- SEER. Available online: https://seer.cancer.gov/registries/characteristics.html.
- Tyson, M.D.; Andrews, P.E.; Etzioni, D.A.; Ferrigni, R.G.; Humphreys, M.R.; Swanson, S.K.; Castle, E.K. Marital status and prostate cancer outcomes. Can. J. Urol. 2013, 20, 6702–6706. [Google Scholar] [CrossRef]
- Gomez, S.L.; Hurley, S.; Canchola, A.J.; Keegan, T.H.; Cheng, I.; Murphy, J.D.; Clarke, C.A.; Glaser, S.L.; Martínez, M.E. Effects of marital status and economic resources on survival after cancer: A population-based study. Cancer 2016, 122, 1618–1625. [Google Scholar] [CrossRef] [PubMed]
- Singh, G.K.; Siahpush, M. Increasing inequalities in all-cause and cardiovascular mortality among US adults aged 25–64 years by area socioeconomic status, 1969–1998. Int J Epidemiol. 2002, 31, 600–613. [Google Scholar] [CrossRef]
- Census.gov. Available online: https://www.census.gov/topics/population/foreign-born/data/tables/acs-tables.html.
- Hashim, D.; Weiderpass, E. Cancer Survival and Survivorship. In Encyclopedia of Cancer (Third Edition); Academic Press: Cambridge, MA, USA, 2019; pp. 250–259. ISBN 9780128124857. Available online: https://www.sciencedirect.com/science/article/pii/B9780128012383651024. [CrossRef]
- Kim, J.H. Multicollinearity and misleading statistical results. Korean J. Anesthesiol. 2019, 72, 558–569. [Google Scholar] [CrossRef]
- Dasgupta, P.; Baade, P.D.; Aitken, J.F.; Ralph, N.; Chambers, S.K.; Dunn, J. Geographical Variations in Prostate Cancer Outcomes: A Systematic Review of International Evidence. Front. Oncol. 2019, 9, 238. [Google Scholar] [CrossRef]
- Braveman, P.A.; Cubbin, C.; Egerter, S.; Williams, D.R.; Pamuk, E. Socioeconomic disparities in health in the United States: what the patterns tell us. Am. J. Public Health 2010, 100 (Suppl. 1), S186–S196. [Google Scholar] [CrossRef]
- Farmer, M.M.; Ferraro, K.F. Are racial disparities in health conditional on socioeconomic status? Soc. Sci. Med. 2005, 60, 191–204. [Google Scholar] [CrossRef]
- Schoendorf, K.C.; Hogue, C.J.; Kleinman, J.C.; Rowley, D. Mortality among infants of black as compared with white college-educated parents. N. Engl. J. Med. 1992, 326, 1522–1526. [Google Scholar] [CrossRef] [PubMed]
- Du, X.L.; Lin, C.C.; Johnson, N.J.; Altekruse, S. Effects of individual-level socioeconomic factors on racial disparities in cancer treatment and survival: findings from the National Longitudinal Mortality Study, 1979-2003. Cancer 2011, 117, 3242–3251. [Google Scholar] [CrossRef] [PubMed]
- Nierengarten, M.B. Health literacy may determine treatment choice for favorable-risk prostate cancer: Results from a new trial show that men with low health literacy are less likely to choose active surveillance for prostate cancer after genomic testing. Cancer 2021, 127, 2825–2826. [Google Scholar] [CrossRef] [PubMed]
- Niu, X.; Roche, L.M.; Pawlish, K.S.; Henry, K.A. Cancer survival disparities by health insurance status. Cancer Med. 2013, 2, 403–411. [Google Scholar] [CrossRef] [PubMed]
- Chang, C.M.; Su, Y.C.; Lai, N.S.; Huang, K.Y.; Chien, S.H.; Chang, Y.H.; Lian, W.C.; Hsu, T.W.; Lee, C.C. The combined effect of individual and neighborhood socioeconomic status on cancer survival rates. PLOS ONE 2012, 7, e44325. [Google Scholar] [CrossRef] [PubMed]
- PSA guidelines: V.A. Moyer, Force USPSTF Screening for prostate cancer: U.S. Preventive Services Task Force recommendation statement. Ann Intern Med 2012, 157, 120–134.
- Ruiz-Rodríguez, I.; Hombrados-Mendieta, I.; Melguizo-Garín, A.; Martos-Méndez, M.J. The Importance of Social Support, Optimism and Resilience on the Quality of Life of Cancer Patients. Front. Psychol. 2022, 13, 833176. [Google Scholar] [CrossRef]
- Taylor, S.E.; Repetti, R.L.; Seeman, T. Health psychology: what is an unhealthy environment and how does it get under the skin? Annu. Rev. Psychol. 1997, 48, 411–447. [Google Scholar] [CrossRef]
- Meliker, J.R.; Goovaerts, P.; Jacquez, G.M.; AvRuskin, G.A.; Copeland, G. Breast and prostate cancer survival in Michigan: can geographic analyses assist in understanding racial disparities? Cancer 2009, 115, 2212–2221. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



