
Submitted:
18 April 2023
Posted:
19 April 2023
You are already at the latest version
Abstract
Background and aim: Human Papillomavirus (HPV) is sexually transmitted, one of the three most common sexually transmitted infections (STIs) in both males and females, and the most common viral STI. A crucial public health strategy to protect people against HPV is through vaccination, which has shown its effectiveness in preventing HPV related diseases. Presently three types of vaccines are available (bivalent, quadrivalent, and nonavalent) and they all target at least the two most oncogenic virus genotypes (HPV 16, 18). In the past few years, the need to implement vaccination programmes that include all genders has been discussed in order to achieve herd immunity against HPV. To date, only a few countries have included young males in their vaccination programmes, so we aim through this review to provide an overview of the epidemiology of HPV and prevention strategies to prevent it, reporting the latest findings from the scientific literature.
Keywords:
Human papillomavirus
; Epidemiology
; Prevention Strategies
; Vaccination
; Screening
; Cervical Cancer
; Gender Gap
1. Introduction
Human papillomaviruses HPVs infections are the most common sexually transmitted infections worldwide [1], they are prevalent in young women, but infections may also occur in sexually active adults [2].
HPVs are icosahedral viruses with a double-stranded DNA genome belonging to the Papillomaviridae family, which is divided into 39 genera [3,4]. Particularly, HPVs are divided into 5 genera (alpha, beta, gamma, mu, and nu) based on the L1 protein containing more than 200 types, differently distributed across geographic areas [5]. The Alpha papillomavirus genus is, in turn, divided into two categories based on its power to develop benign or malignant tumors [6]. HPVs infect the under-differentiated deeper layer cells of the skin and/or mucous membranes called basal epithelial cells [1]. The viral genome is characterized by 8 ORFs (open reading frames) divided into seven early (E) and two late (L) genes. The L region encodes the two viral capsid proteins. The oncogenic E5, E6, and E7 proteins encoding by the high-risk types can transform and stimulate cell growth in the basal and parabasal layers [5,6]. The E6 and E7 genes inhibit tumor suppressors like p53 and pRb respectively, that regulate the cell cycle and apoptosis, leading to an elevated risk of cancer development [7]. Globally, 4.5% of all cancers are attributable to HPVs: 8.6% of cancer cases in women (the third most prevalent, with a high mortality), and 0.8% in men [8]. The low- risk genotypes are usually associated with genital warts and respiratory tract papilloma, while the high-risk ones are associated with a malignant transformation of cells, as in oropharyngeal and anogenital cancer [3]. The association between high-risk (HR)-HPVs and some types of cancer is well-established [2;9], not only with the most common HR-HPV types 16 and 18, but also the less prevalent 31, 33, 45, 52, and 58 ones [8]. The 16 and 18 types are strongly associated with cervical and penis cancer, but also with anal and oropharyngeal cancer [3; 10-11]. Most of HR-HPV infections do not develop into external lesions and remain asymptomatic, being immunologically cleared. [12,13]. The first vaccine against HPV has been available since 2006. To date there are three types of vaccines against HPVs available, and they have been progressively introduced into many national vaccination programs. Unfortunately, however, several studies and international agencies have reported that both the introduction of the vaccine and the coverage achieved are still suboptimal [14,15]. The purpose of this overview is to summarize recent studies in order to highlight how epidemiology and prevention strategies have developed in recent years.
2. Epidemiology
HPVs infection and related diseases affect both women and men. In fact, it is estimated that about 80% of sexually active women and men will be infected with HPVs at least once during their lifetime [16]. HPV infection is the second-most common cause of cancer, after gastric cancer which is caused by Helicobacter pylori [17,18]. However, the epidemiology of HPVs among the male and female populations is different [19]. Worldwide, in the female population 26.8% of the cases afflict the genital organs (highest in Sub-Saharan Africa) and 14% afflict the anus, whereas in the male population 45.2% of the cases afflict the genital organs and 16% the anus [20,21].
Figure 1 [22] shows the age-standardized incidence rates of cervical cancer, of these the HPV is responsible for 97% all cases. HPV-16 and 18 cause the 90% of HPV related cancer [14], although cases linked to HPV 45, 33, and 35 have been increasing [23,24]. Figure 1 [22] also shows that the incidence of cervical cancer is very high in many states in Africa and in some South-East Asian and Latin American states. In women, persistent infection increases the risk of developing intraepithelial lesions or cervical cancer, which represent about 80% of HPV-related cancer. Usually, the prevalence of cervical infection decreases after the age of 30 [14; 25]. It has also been observed that cervical infection results in a higher prevalence of HPVs anal diseases [25]. Seventy percent of vulva cancer and 75% of vaginal cancer cases are HPV-related [26].
HPV infections are higher in men who are sexually active with other men, and men who are HIV positive [27]. Globally, HPVs are responsible for 50.8% cases of penile cancers, 79.8% of penile intraepithelial neoplasia (PeIN), and 90% of genital warts. Furthermore, HPV 16 is the most common cause of these lesions with a pooled prevalence of 68.3% of penile cancer and 69.8% of PeIN cases [18]. Additionally, HPVs cause around 26-30% of head-neck cancers [25].
The incidence of HPV (up to 90% HPV-16 positive) associated oropharyngeal squamous cell carcinoma (OPSCC) cases are rising nowadays in developed countries [27,28]. Globally, 33% of HPV+ OPSCC cases were reported in 2021; however, prevalence varies considerably depending on country, with estimates ranging from 0% in southern India to 85% in Lebanon [29]. In addition, HPV+ is more prevalent than HPV– in OPSCC in people who do not consume tobacco or alcohol [30]. The prevalence of HPV+ OPSCC was previously reported to decrease with increasing age, and historically most HPV+ OPSCCs occur in men. [30,31]. HPV+ OPSCC incidence has greatly increased over the last two decades in some European countries [30; 32-33], while in lower middle-income South Asia and sub-Saharan Africa epidemiological reports are scarce, so it is consequently unclear whether similar upward trends are absent or simply undetected in these regions [34]. A 26% incidence of HPV is found in conjunctival intraepithelial neoplasia and to conjunctival squamous cell carcinoma (with a high rate of genotypes 16, 18 and 33); HPV infection increases the likelihood of developing these two neoplasms eight-fold [35].
3. Transmission
Worldwide the best-known route of HPV transmission is sexually, principally causing the high incidence of HPV in anogenital warts and cervical cancer. However, HPVs are also diagnosed in children and adolescents who are not sexually exposed, so other ways of transmission are considered in studies.
HPV has been found in infants' mouths, breast milk, amniotic fluid, placenta, umbilical blood, spermatozoa, and sperm fluid [36]. However, since the papillomavirus has historically been associated with intercourse, the increasing incidence of anogenital warts in infants would lead one to suspect sexual violence. Fortunately, this hypothesis has been abandoned [13]. The virus can be transmitted from the mother to the embryo, fetus, or child during pregnancy or delivery, although the mechanism is still not understood. A study by Mastora et al. showed that mouse sperm can internalize HR-HPV genes [37]. Therefore, the infection can also occur at the time of fertilization [12]. The presence of the same HPV type in mothers and newborn children suggests perinatal transmission [38].
HPV-related warts have also been found in virgins, so several routes of horizontal HPV transmission have been highlighted [13]: autoinoculation, heteroinoculation, or via fomites. At the genital level, HPV infection not transmitted through sexual acts can be spread by contact between infected fingers and genitals. For children this incidence is associated with a parent or caretaker who has hand warts who could transmit infection to the infant during diaper changing and cleaning of the anogenital area [12].
We know there is a risk of transmission through endovaginal ultrasound probes that have been inadequately disinfected, and thus ineffective in preventing HR-HPV contamination. This represents a risk of nosocomial HR-HPV transmission during an ultrasound procedure [39]. In a different set of circumstances, the HPV virus appears to transmit through surgical smoke generated in laser ablation procedures. This risk of infection has so far been documented in animal models: bovine papillomavirus collected from CO2 laser smoke during wart treatment in cattle induced cutaneous fibropapillomas when re-inoculated into the skin of calves. However, this risk of infection remains controversial in humans [40,41,42].
Lastly, waterborne transmission has never been proven, even though we know that HPV type 16 remains infectious for seven days on wet surfaces [43,44,45], and HPV samples have been detected in raw sewage and sewage sludge [46,47,48,49]. HPV was detected in 50% of the samples of domestic bathing water [50].
4. Clinical Manifestation
4.1. Benign
Anogenital warts and recurrent respiratory papillomatosis are mainly caused by HPV 6 and 11. Almost all the of anogenital warts (90%) are caused by low-risk HPVs which do not have oncogenic potential, even if occasional high- risk types are detected as co-infections with HPV 6 and 11 [51]. Despite most anogenital warts are considered benign lesions, in some cases they are associated with an increased risk of developing grade 2 or worse cervical intraepithelial neoplasia (CIN), intraepithelial neoplasia, and anogenital cancer [52].
Recurrent respiratory papillomatosis (RRP) is usually a benign condition affecting the upper aerodigestive tract following HPV-6 and HPV-11 infection. Two forms are recognized and distinguished according to the age of onset of symptoms: JoRRP (juvenile-onset RRP) and AoRRP (adult-onset RRP). The former, probably related to perinatal infections, is very frequent especially in sub-Saharan Africa and is present in individuals younger than 12 years of age. The adult form, frequent in Europe and South America, is generally related to the practice of oral sex. Papillomatosis is most prevalent in the larynx, but sometimes involves the trachea, oropharynx, nasopharynx, nose, oral cavity, and lung parenchyma. Clinical manifestation is characterized by progressive hoarseness that may evolve into a “cauliflower-like” lesion which could potentially develop to a point of obstructing the airway, consequently requiring clinical intervention, and sometimes even tracheostomy [53,54].
Cutaneous Warts (CWs), also known as verrucae, generally affect children and young adults, and peak between 10 and 14 years. CWs are mainly caused by the genera beta and gamma (HPV 4 and 65) and rarely by the other strains. HPVs are detected in the commensal cutaneous flora of healthy individuals but can evolve into CWs due to viral multiplication. Most lesions, however, resolve with no treatment within two years [13]. Infections occur through skin-to-skin contact with infected individuals (often without clinical manifestations) and could possibly be transmitted from inanimate objects [55]. CW infection is higher in males than females, young people, and immunocompromised individuals. Individuals who are immunocompromised could later develop squamous cell carcinoma, probably related to latent HPV reactivation [56].
HPV 6 and 11 are also the major culprits of condyloma acuminata (CA), which are warts located in the anogenital region or on the tongue and lips. CA occurs in both sexes with a symptomatology that varies from asymptomatic to painful. Their morphology is likewise variable, they can be flat or take on a cauliflower-like shape [57,58]. In some cases, they resolve spontaneously, but others require removal by an immunomodulatory approach or physical intervention, in some cases surgery is recommended to prevent progression to cancer. When (CA) location is intravaginal or intra anal surgery is the only form of intervention available [57].
4.2. Malignant
The persistence of HR-HPV genotypes added to other common risk factors such as cigarette smoking, use of oral contraceptives, alcohol, etc. can result in non-silent mutations in onco-suppressor genes (such as p 53) and/or proto-oncogenes that lead to cell over proliferation and initiate the carcinogenesis process. It has been observed that the triggering event for the development of HPV-related, malignant lesions is the integration of viral oncoproteins E5, E6 and E7 within human genome. Genotypes 16 and 18 are most responsible for carcinoma of the cervix, anogenital area (vulva, vagina, penis, anus) and head and neck carcinoma (mouth, tonsils, pharynx, and larynx) [36; 59]. The most clinically encountered cervical cancers (CC) are squamous cell carcinoma (SCC) and adenocarcinoma (AC), with a higher incidence of the former than the latter, while the most common histological types of cervical cancer are keratinized squamous cell carcinoma and non-keratinized squamous cell carcinoma, adenocarcinoma, and adenosquamous carcinoma [60,61].
In a low percentage of women permanent HR-HPV, in conjunction with other risk factors, can induce low-grade squamous intraepithelial lesions (L- SIL) which include a mild dysplasia known as CIN 1 (cervical intraepithelial neoplasia grade 1) which can then evolve into high-grade squamous intraepithelial lesions (H- SIL). H- SIL is a progressive lesion that evolves into moderate (CIN 2) and then severe dysplasia (CIN 3). Epithelial involvement goes from being minimal and limited (less than one-third of the epithelium) in CIN 1, to two-thirds involvement in CIN 2, to total in CIN 3. When the whole thickness of the epithelium of the cervix is involved, it can be defined as in situ cervical carcinoma (ISCC) [60]. A correlation between vaginal microbiome and tumor progression has also been observed in some studies. Specifically, it appears that the severity of cervical lesions is promoted by a decrease in lactobacilli that can be observed following infection by high-risk papilloma genotypes [62].
Penile cancer is an aggressive disease that, like all cancers, implicates several risk factors, including phimosis, lichen sclerosis and inflammatory conditions (balanitis xerotica obliterans), premalignant lesions (Bowen's disease, erythroplasia Queyrat), high numbers of sexual partners, socioeconomic status, and HPV infections (especially by high-risk genotypes such as 16 and 18). Papillomavirus is found most in basaloid squamous carcinoma, warty carcinoma, clean-cell carcinoma, and lymphoepithelioma-like carcinoma [63,64]. An over expression or down expression of miRNAs have diagnostic and prognostic value. A down expression of hsa- miR-218 and miRNA- 246a and over expression of EFGR has been observed in HPV-related penile cancers. In the case of penile cancer, clinical intervention is a total or partial penectomy, therefore precancerous lesions, when identified, should be treated immediately [65].
Head and neck squamous cell carcinoma (HNSCC) are tumors arising from the mucosal epithelium of the oral cavity, pharynx, and larynx. High incidence is mainly determined by personal habits, but HR-HPV involvement is increasingly considered. HNSCC are therefore distinguished into HPV-related HNSCC and HPV-unrelated HNSCC (HPV- negative HNSCC), with the former generally having better prognosis than the latter [66]. HPV + HNSCC carcinomas usually occur following infection at the deep crypts of the palatine and lingual tonsils and demonstrate a different gene expression, mutational, and immune profile than HPV-negative HNSCC, which is most related to the use of tobacco or alcohol [66,67].
5. Prevention
5.1. Primary prevention
Despite HPV infections usually regress spontaneously within 1 to 2 years, and not all genotypes are implicated in cancer [9; 43; 68-70]; HPV infections and related diseases should be taken seriously, and to date vaccines provide the best and most cost-effective option for prevention. All the vaccines currently in use are based on virus-like particles (VLPs) of the L1 protein, considered a strong immunogen protein, which spontaneously self-assemble from pentamers. [13; 36; 71-72]. Gardasil (4vHPV) is the first vaccine to be approved in 2006 by the Food and Drug Administration which targeted 4 types of HPV (6, 11, 16, and 18) [3]. The bivalent vaccine Cervarix (2vHPV) which targets HPV 16 and 18 was approved in 2007. It has been proven that 2vHPV also protects against HPV 31, 33, and 45, and reduces genital warts caused by HPV 6 and 11 [3; 43]. Both vaccines contain different adjuvants and while proteins of Cervarix are produced in baculovirus-infected insect cell, Gardasil’s in Saccharomyces cerevisiae [70]. The nine-valent Gardasil (9vHPV) adds five L1 VLPs, particularly the oncogenic HPV types 31, 33, 45, 52, and 58, and when compared to the 4vHPV demonstrates the best rate of prevention for low and high-risk human papillomavirus infection. Approved by the FDA (Food and Drug Administration) in 2014, it is considered the best way to prevent CIN I, II, and III and 90% of HPV- related diseases compared to its predecessors [3; 73], and in 2020 received an indication for prevention of some head and neck cancer caused by HPV [70]. According to CDC (Centers for Disease Control and Prevention) and ACIP (Advisory Committee on Immunization Practices) recommendation, two or three doses of 9vHPV are recommended for both males and females ages 9 to 45 years. [73,74]. Both the Gardasil and Cervarix vaccines induce cross-protection against nonvaccine types like HPV 31 and HPV 45, but with a lower antibody titer than the epitopes included in the vaccines [75,76]. Vaccination can be provided from 9 years of age, however since 2006 catch-up vaccination has been recommended for females up to the age of 26, and for males up to the age of 21 since 2011, in addition to some special populations up to the age of 26. Furthermore, since HPV infection incidence in adults is increasing, vaccination is currently recommended for women and men aged 45 years [2].
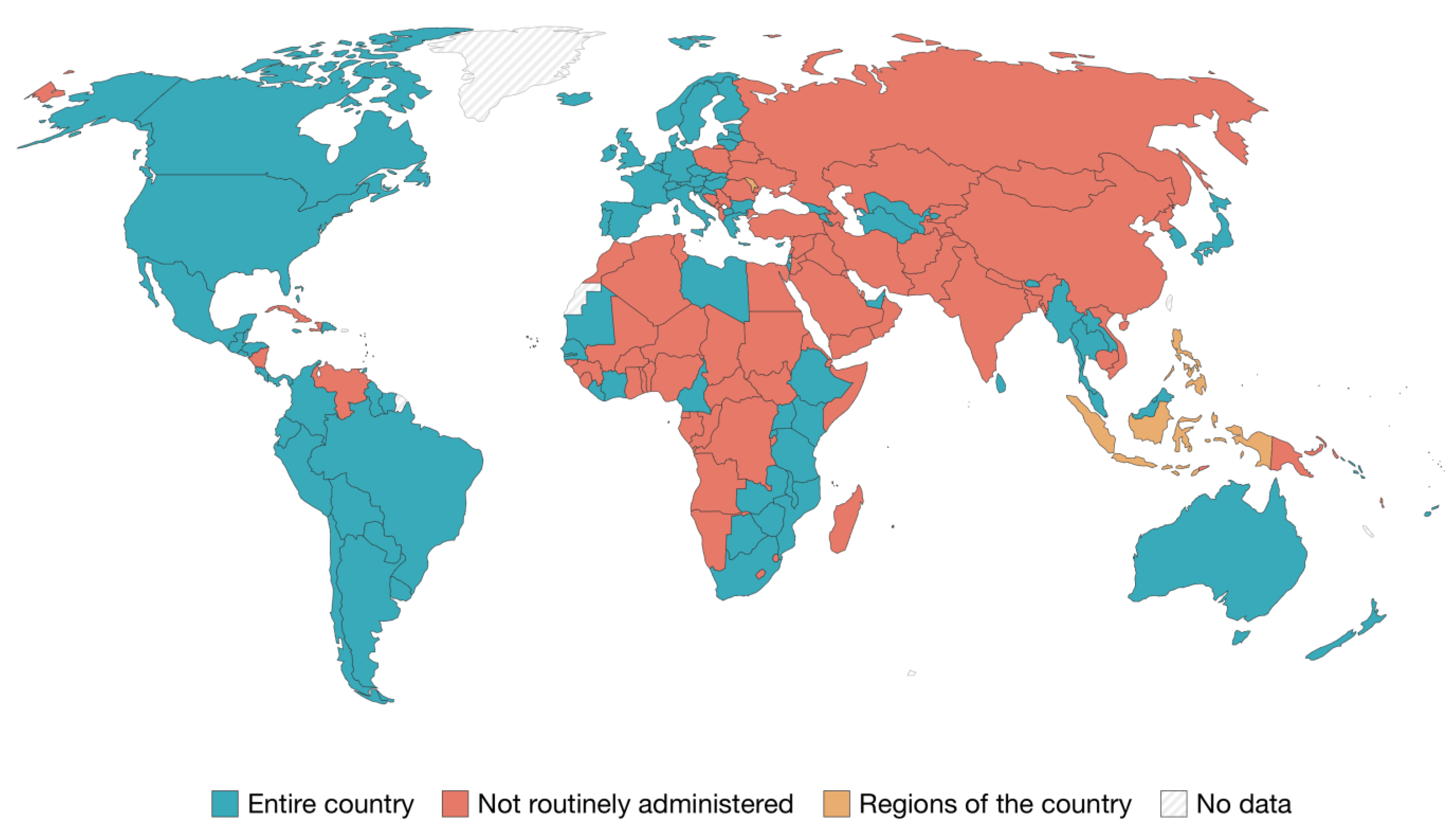
Figure 2 [77] shows which countries provide and recommend HPV vaccines through routine services. Australia was one of the first countries to introduce a publicly funded national HPV vaccination program in 2007. This not only resulted in a 70% decrease in the incidence of HPV 6, 11, 16 and 18 infections, but also achieved high vaccination coverage for both gender groups [24; 36; 70; 78]. Primary prevention against HPV is available due to the presence of vaccines targeting high-risk genotypes; in fact, since 2006 more than 110 countries have implemented a vaccination campaign against HPV, but only about 40 countries have introduced a gender- neutral HPV vaccination program; Australia and the United States were among the first to take this step, in 2011 and 2013, respectively [63; 65; 79].
Herd immunity is impossible to achieve if males are not included in vaccination programs. In fact, adopting gender-neutral HPV vaccination schedules will reduce population-transmitted infections, combat misinformation, minimize vaccine-related stigma and promote gender equity [80,81]. To date, only a few countries have achieved 70% vaccination coverage [81] with a marked discrepancy between continents, ranging from 20% in sub-Saharan Africa to 77% in New Zealand. In a few African countries the bivalent and quadrivalent vaccine was made available free of charge (only for females), several years after the first one was approved in 2008 [82]. As in Africa, vaccination coverage is also very low in several Asian countries. In some countries, such as China, coverage is not very clear and the vaccine is not approved for use in males, and it is not included in the national vaccination program and vaccination is at one's own expense [83]. In Japan, female coverage reached 70% but following reports of adverse events, which were widely covered in the media and turned out to be unrelated to vaccination, vaccination coverage fell to less than 1% and has remained this low to date [84]. In 2021, the South-Eastern Asian country of Bhutan was the first country to adopt a gender-neutral vaccination strategy [80,81]. In the United States, vaccination has been recommended for females since 2006 and for males since 2011, furthermore, since 2016 only 9vHPV has been distributed [85]. In South America data on vaccination coverage is not available for all countries; Mexico is the only one that has reached the target of 90% for females fully vaccinated by the age of 15. Moreover, not all countries have yet introduced the vaccine as a public health policy [86]. In Europe, coverage varies between about 14% and 86%, with highest values in the UK and lowest values in Bulgaria. The availability of vaccines and vaccination policies varies from country to country [87,88,89]. In Italy the national vaccine program provides universal vaccination for the target populations, utilizing the nine-valent vaccine for both males and females from the age of 11 [90]. Poland, instead, requires citizens to pay for the HPV vaccine and in France national health insurance reimburses 65% of the cost [89].
Finally, some evidence shows that male circumcision reduces the risk of certain sexually transmitted viral infections in men and consequently for their female partners. Specifically, male circumcision is associated with slight reductions in high-risk HPV, whereas licensed HPV vaccines only protect with high efficacy against a limited number of HPV types. It is therefore likely that the two interventions have important synergistic effects [91].
5.2. Secondary prevention
Primary prevention is not a substitute for secondary prevention. Indeed, women should adhere to national screening programs to prevent cervical cancer [68]. The WHO recommends screening for cervical cancer from the age of 30 onwards [92]. Unequal access to screening is a major reason for the dramatic disparities in cervical cancer incidence, and mortality between low- and high-income countries. In 2020, in order to reduce the circulation of HPV and eliminate cervical cancer, WHO, launched the "Global Strategy to Accelerate the Elimination of Cervical Cancer as a Public Health Problem," to be achieved by 2030, which includes intensifying vaccination, screening, and treatment of women with cervical cancer [80; 92]. Eliminating the incidence of cervical cancer does not mean eliminating the circulation of HPV, so gender-based primary prevention is the best weapon to invest in [80]. There are many ways to check cancer progression such as VIA (visual inspection with acetic acid), a procedure used to identify CIN through a solution of acetic acid with a concentration ranging from 3 to 5 percent. Interpretation of the results is crucial to determine positivity and negativity to decide on clinical treatment in case of positivity. Since 1990, some countries have used EIA as the primary screening [93]. To assess the squamocolumnar junction, which is the area that has the highest risk of going to dysplasia, the Papanicolau test (Pap test) or the thin-layer liquid-based cytology method is performed [94]. Colposcopy is a diagnostic procedure used to examine the cervix, vagina, and vulva of women who have previously undergone VIA or who have tested positive for Papanicolau (Pap) or HPV DNA testing for high-risk oncogenic genotypes. It is also a test used after treatment of intraepithelial and invasive carcinoma [95]. Viral genome identification can be done by the HPV DNA test, a multiplex test capable of detecting the high risk- HPV genome by PCR [96]. Currently, the Roche Cobas® test is the only HPV test approved by the FDA as an independent screening test for women 25 years of age and older [96,97]. Genome amplification should not only involve the L1 protein, as this may be unexpressed after viral infection, but through HPV mRNA testing the expression of oncoproteins E6 and E7, which are markers of integration of the viral genome with that of the host, is detected [96]. Because cancer is a multifactorial disease, a positive HPV DNA test does not necessarily mean that one has cancer, but further investigation with colposcopy is necessary; moreover, in some cases, HPV DNA testing may be negative in women with high-grade precancer due to low viral load [97]. An additional marker of HPV oncogenic activity is the tumor suppressor protein p16, which is overexpressed following demethylation of its promoter at oncoprotein E7 [98]. The use of immunohistochemical techniques to mark p16 could reduce overtreatment and conization, which could result in preterm delivery [98,99]. In men and for other HPV+ cancers, there is still no validated method of diagnosis or screening, but papillomavirus has been detected in several samples: seminal fluid, phenocopy with acetic acid, urethral specimen, penile scrapings (taken from the crown of the glans of the penis, from the inner layer of the foreskin, from the body of the penis). Among the detection methods, Polymerase Chain Reaction (PCR) is the most widely used [100,101,102,103,104].
5.3. Tertiary prevention
Tertiary prevention targets both the clinical and outcome phases of a disease. It is implemented in symptomatic patients and aims to reduce the severity of the disease and any associated sequelae [105]. For HPV induced cancers, some retrospective studies show a significant protective effect of HPV vaccine in women and men surgically treated for HPV disease [106,107,108]. Indeed, in males who have sex with males, adjuvant vaccination, post treatment of high-grade squamous intraepithelial lesions, is potentially the most effective approach to reduce the incidence of invasive anal cancer. Specifically, vaccination should be considered for all HIV-infected individuals aged 27 years or older undergoing treatment for high-grade squamous intraepithelial lesions [107]. In women, on the other hand, adjuvant vaccination reduces the risk of recurrence by about 80% for women treated surgically for CIN II lesions and FIGO stage 1A1 cervical cancer [108]. However, it is still under discussion whether vaccination is more effective first as a neo-adjuvant or adjuvant to conization, although it would appear to be within 30 days of standard treatment. [109,110]. Moreover, the reduction of recurrences after treatment in vaccinated patients is also confirmed for benign lesions [111,112]. In fact, for respiratory papillomatosis the substantial benefit is known for HPV vaccination used as adjunctive therapy in combination with surgery [113]. In contrast, vaccination does not seem to provide a significantly secondary benefit in patients with previous ano-genital warts, also this cannot be generalized due to the few randomized controlled trials performed [114]. Several methods have been studied for the tertiary prevention of oropharyngeal squamous cell carcinoma, although they have not yet been prospectively validated through a rigorous study [115]. These methods include oral fluid biomarkers and blood biomarkers [115]. In the former, the presence of HR-HPV DNA seems to be correlated with a risk of recurrence [116]. While for blood biomarkers it has been observed that higher E6 antibody levels are associated with an increased risk of recurrence [117]. Furthermore, the role of circulating HPV DNA will need further investigation. It has already been observed that in more advanced stages of disease higher levels of circulating DNA are present [118]: whether, as in other virus-induced carcinomas, the level of circulating DNA is indicative of disease persistence or recurrence still needs to be studied [119,120].
6. Conclusions
The epidemiology of HPV has been heterogeneous between the sexes, with a higher prevalence of infection in ano-genital areas among males, which is even higher in some subgroups. To date, the only way to block the chain of transmission is vaccination, but HPV vaccination programs are still in their infancy in many countries, particularly in less developed countries [81]. This makes it difficult to achieve herd immunity, especially in males who were only invited to vaccinate in the years after the first vaccine was introduced. There is growing evidence that only gender-neutral vaccination will lead to substantial control of HPV-related diseases in both women and men, as well as maximize cervical cancer prevention, especially if vaccination coverage for girls in a particular program is not high [121]. Given the current situation, it is logical to assume that cervical cancer prevention will still rely on secondary prevention methods in the years to come. Finally, another global public health goal will be to propose scientific evidence to establish the optimal timing of vaccination in preventing the greatest number of cancer recurrences in order to improve the outcome of proposed treatments.
Author Contributions
Conceptualization, I.M. and E.M.; methodology, G.M. and I.M..; investigation, G.M. and G.G.; resources, N.N. and E.M.; writing—original draft preparation, G.M. and G.G.; writing—review and editing, G.M., G.G., I.M.; visualization, G.M. and G.G.; supervision, N.N., E.M. and I.M.; project administration, E.M. and I.M.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Nøhr, B.; Kjaer, S.K.; Soylu, L.; Jensen, A. High-risk human papillomavirus infection in female and subsequent risk of infertility: a population-based cohort study. Fertil Steril. 2019, 111, 1236–1242. [Google Scholar] [CrossRef] [PubMed]
- Meites, E.; Szilagyi, P.G.; Chesson, H.W.; Unger, E.R.; Romero, J.R.; Markowitz, L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep. 2019, 16, 698–702. [Google Scholar] [CrossRef] [PubMed]
- Rosalik, K.; Tarney, C.; Han, J. Human Papilloma Virus Vaccination. Viruses 2021, 13, 1091. [Google Scholar] [CrossRef] [PubMed]
- Harden, M.E.; Munger, K. Human papillomavirus molecular biology. Mutat Res Rev Mutat Res. 2017, 772, 3–12. [Google Scholar] [CrossRef] [PubMed]
- Soheili, M.; Keyvani, H.; Soheili, M.; Nasseri, S. Human papilloma virus: A review study of epidemiology, carcinogenesis, diagnostic methods, and treatment of all HPV-related cancers. Med J Islam Repub Iran 2021, 22, 65. [Google Scholar] [CrossRef] [PubMed]
- Egawa, N.; Doorbar, J. The low-risk papillomaviruses. Virus Res. 2017, 2, 119–127. [Google Scholar] [CrossRef] [PubMed]
- Goodman, A. HPV testing as a screen for cervical cancer. BMJ. 2015, 30, h2372. [Google Scholar] [CrossRef]
- Roman, B.R.; Aragones, A. Epidemiology and incidence of HPV-related cancers of the head and neck. J Surg Oncol. 2021, 124, 920–922. [Google Scholar] [CrossRef]
- Ryndock, E.J.; Meyers, C. A risk for non-sexual transmission of human papillomavirus? Expert Rev Anti Infect Ther. 2014, 12, 1165–70. [Google Scholar] [CrossRef]
- Iorga, L.; Dragos, Marcu, R.; Cristina Diaconu, C.; et al. Penile carcinoma and HPV infection (Review). Exp Ther Med. 2020, 20, 91–96. [Google Scholar] [CrossRef]
- Manini, I.; Montomoli, E. Epidemiology and prevention of Human Papillomavirus. Ann Ig. 2018, 30, 28–32. [Google Scholar] [PubMed]
- Sabeena, S.; Bhat, P.; Kamath, V.; Arunkumar, G. Possible non-sexual modes of transmission of human papilloma virus. J Obstet Gynaecol Res. 2017, 43, 429–435. [Google Scholar] [CrossRef] [PubMed]
- Kombe Kombe, A.J.; Li, B.; Zahid, A.; Mengist, H.M.; Bounda, G.A.; Zhou, Y.; Jin, T. Epidemiology and Burden of Human Papillomavirus and Related Diseases, Molecular Pathogenesis, and Vaccine Evaluation. Front Public Health. 2021, 20, 552028. [Google Scholar] [CrossRef] [PubMed]
- Di Donato, V.; Caruso, G.; Petrillo, M.; Kontopantelis, E.; Palaia, I.; Perniola, G.; Plotti, F.; Angioli, R.; Muzii, L.; Benedetti Panici, P.; Bogani, G. Adjuvant HPV Vaccination to Prevent Recurrent Cervical Dysplasia after Surgical Treatment: A Meta-Analysis. Vaccines 2021, 9, 410. [Google Scholar] [CrossRef] [PubMed]
- Bruni, L.; Saura-Lázaro, A.; Montoliu, A.; Brotons, M.; Alemany, L.; Diallo, MS.; Afsar, O.Z.; LaMontagne, D.S.; Mosina, L.; Contreras, M.; Velandia-González, M.; Pastore, R.; Gacic-Dobo, M.; Bloem, P. HPV vaccination introduction worldwide and WHO and UNICEF estimates of national HPV immunization coverage 2010-2019. Prev Med. 202, 144, 106399. [Google Scholar] [CrossRef] [PubMed]
- Tao, Y.; Shao, H.; Zhang, T.; Pu, J.; Tang, C. Factors Influencing Men’s Attitudes toward HPV Vaccination in Males Included in the Chinese National Immunization Program. Vaccines 2022, 10, 1054. [Google Scholar] [CrossRef]
- Elst, L.; Albersen, M. HPV Vaccination: Does It Have a Role in Preventing Penile Cancer and Other Preneoplastic Lesions? Semin Oncol Nurs. 2022, 38, 151284. [Google Scholar] [CrossRef]
- de Martel, C.; Georges, D.; Bray, F.; Ferlay, J.; Clifford, GM. Global burden of cancer attributable to infections in 2018: a worldwide incidence analysis. Lancet Glob Health. 2020, 8, e180–e190. [Google Scholar] [CrossRef]
- Yousefi, Z.; Aria, H.; Ghaedrahmati, F.; Bakhtiari, T.; Azizi, M.; Bastan, R.; Hosseini, R.; Eskandari, N. An Update on Human Papilloma Virus Vaccines: History, Types, Protection, and Efficacy. Front Immunol. 2022, 27, 805695. [Google Scholar] [CrossRef]
- Shen, J.; Zhou, H.; Liu, J.; Zhang, Z.; Fang, W.; Yang, Y.; Hong, S.; Xian, W.; Ma, Y.; Zhou, T.; Zhang, Y.; Zhao, H.; Huang, Y.; Zhang, L. Incidence and risk factors of second primary cancer after the initial primary human papillomavirus related neoplasms. MedComm 2020, 1, 400–409. [Google Scholar] [CrossRef]
- Bhatla, N.; Aoki, D.; Sharma, D.N.; Sankaranarayanan, R. Cancer of the cervix uteri: 2021 update. Int J Gynaecol Obstet. 2021, 155 (Suppl 1), 28–44. [Google Scholar] [CrossRef] [PubMed]
- International Agency for Research on Cancer, World Health Organization. Incidence, prevalence and mortality rates (World) in 2020. Available online: https://gco.iarc.fr/today/online-analysis-map?v=2020&mode=population&mode_population=continents&population=900&populations=900&key=asr&sex=2&cancer=23&type=0&statistic=5&prevalence=0&population_group=0&ages_group%5B%5D=0&ages_group%5B%5D=17&nb_items=10&group_cancer=1&include_nmsc=0&include_nmsc_other=0&projection=natural-earth&color_palette=default&map_scale=quantile&map_nb_colors=5&continent=0&show_ranking=0&rotate=%255B10%252C0%255D (accessed on 11/02/23).
- Santella, B.; Schettino, M.T.; Franci, G.; De Franciscis, P.; Colacurci, N.; Schiattarella, A.; Galdiero, M. Microbiota and HPV: The role of viral infection on vaginal microbiota. J Med Virol. 2022, 94, 4478–4484. [Google Scholar] [CrossRef] [PubMed]
- Calabrò, G.E.; Ricciardi, W. Verso un mondo HPV free: strategie internazionali, da implementare a livello nazionale, per l’eliminazione del cancro cervicale: il valore della prevenzione e della vaccinazione anti-HPV negli adolescenti Da: I Numeri del Cancro in Italia. AIOM-AIRTUM,2022. Available online: https://www.aiom.it/wp-content/uploads/2022/12/2022_AIOM_NDC-web.pdf.
- Pimple, S.; Mishra, G. Cancer cervix: Epidemiology and disease burden. Cytojournal. 2022, 29, 21. [Google Scholar] [CrossRef] [PubMed]
- Efua Sackey, M.; Markey, K.; Grealish, A. Healthcare professional's promotional strategies in improving Human papillomavirus (HPV) vaccination uptake in adolescents: A systematic review. Vaccine. 2022, 26, 2656–2666. [Google Scholar] [CrossRef] [PubMed]
- Sasidharanpillai, S.; Ravishankar, N.; Kamath, V.; Bhat, P.V.; Bhatt, P.; Arunkumar, G. Prevalence of Human Papillomavirus (HPV) DNA among Men with Oropharyngeal and Anogenital Cancers: A Systematic Review and Meta-Analysis. Asian Pac J Cancer Prev. 2021, 22, 1351–1364. [Google Scholar] [CrossRef] [PubMed]
- Lehtinen, M.; Gray, P.; Louvanto, K.; Vänskä, S. In 30 years, gender-neutral vaccination eradicates oncogenic human papillomavirus (HPV) types while screening eliminates HPV-associated cancers. Expert Rev Vaccines. 2022, 21, 735–738. [Google Scholar] [CrossRef] [PubMed]
- Carlander, A.F.; et al. A contemporary systematic review on repartition of HPV-positivity in oropharyngeal cancer worldwide. Viruses. 2021, 13, 1326. [Google Scholar] [CrossRef]
- Lechner, M.; Liu, J.; Masterson, L.; Fenton, T.R. HPV-associated oropharyngeal cancer: epidemiology, molecular biology and clinical management. Nat Rev Clin Oncol. 2022, 19, 306–327. [Google Scholar] [CrossRef]
- Gabutti, G.; d'Anchera, E.; De Motoli, F.; Savio, M.; Stefanati, A. Human Papilloma Virus Vaccination: Focus on the Italian Situation. Vaccines (Basel). 2021, 9, 1374. [Google Scholar] [CrossRef]
- Zamani, M.; et al. The current epidemic of HPV-associated oropharyngeal cancer: an 18-year Danish population-based study with 2,169 patients. Eur. J. Cancer. 2020, 134, 52–59. [Google Scholar] [CrossRef]
- Del Mistro, A.; et al. Age-independent increasing prevalence of human papillomavirus-driven oropharyngeal carcinomas in North-East Italy. Sci. Rep. 2020, 10, 1–10. [Google Scholar]
- De Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide burden of cancer attributable to HPV by site, country and HPV type. Int. J. Cancer. 2017, 141, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Seedat, R.Y. Juvenile-Onset Recurrent Respiratory Papillomatosis Diagnosis and Management - A Developing Country Review. Pediatric Health Med Ther. 2020, 11, 39–46. [Google Scholar] [CrossRef] [PubMed]
- Araldi, R.P.; Sant'Ana, T.A.; Módolo, D.G.; de Melo, T.C.; Spadacci-Morena, D.D.; de Cassia Stocco, R.; Cerutti, J.M.; de Souza, E.B. The human papillomavirus (HPV)-related cancer biology: An overview. Biomed Pharmacother. 2018, 106, 1537–1556. [Google Scholar] [CrossRef]
- Mastora, E.; Kitsou, C.; Evangelou, T.; Zikopoulos, A.; Zagorianakou, N.; Georgiou, I. Presence of HPV 16 and HPV 18 in Spermatozoa and Embryos of Mice. In Vivo. 2021, 35, 3203–3209. [Google Scholar] [CrossRef]
- Rombaldi, R.L.; Serafini, E.P.; Mandelli, J.; Zimmermann, E.; Losquiavo, K.P. Perinatal transmission of human papilomavirus DNA. Virol J. 2009, 21, 83. [Google Scholar] [CrossRef]
- Casalegno, J.S.; Le Bail Carval, K.; Eibach, D.; Valdeyron, M.L.; Lamblin, G.; Jacquemoud, H.; Mellier, G.; Lina, B.; Gaucherand, P.; Mathevet, P.; Mekki, Y. High risk HPV contamination of endocavity vaginal ultrasound probes: an underestimated route of nosocomial infection? PLoS One. 2012, 7, e48137. [Google Scholar] [CrossRef]
- Palma, S.; Gnambs, T.; Crevenna, R.; Jordakieva, G. Airborne human papillomavirus (HPV) transmission risk during ablation procedures: A systematic review and meta-analysis. Environ Res. 2021, 192, 110437. [Google Scholar] [CrossRef]
- Sawchuk, W.S.; Weber, P.J.; Lowy, D.R.; Dzubow, L.M. Infectious papillomavirus in the vapor of warts treated with carbon dioxide laser or electrocoagulation: detection and protection. Journal of the American Academy of Dermatology. 1989, 21, 41–9. [Google Scholar] [CrossRef]
- Garden, J.M.; O'Banion, M.K.; Bakus, A.D.; Olson, C. Viral disease transmitted by laser-generated plume (aerosol). Archives of dermatology 2002, 138, 1303–1307. [Google Scholar] [CrossRef]
- Petca, A.; Borislavschi, A.; Zvanca, M.E.; Petca, R.C.; Sandru, F.; Dumitrascu, M.C. Non-sexual HPV transmission and role of vaccination for a better future (Review). Exp Ther Med. 2020, 20, 186. [Google Scholar] [CrossRef] [PubMed]
- Ding, D.C.; Chang, Y.C.; Liu, H.W.; Chu, T.Y. Long-term persistence of human papillomavirus in environments. Gynecol Oncol. 2011, 121, 148–151. [Google Scholar] [CrossRef] [PubMed]
- La Rosa, G. Papillomavirus. In: Global Water Pathogen Project. Rose JB and Jiménez-Cisneros B (eds) (Meschke JS and Girones R (eds) Part 3 Viruses). Michigan State University, E. Lansing, MI, Unesco, 2016.
- Symonds, E.M. Viruses in raw sewage and their potential to indicate fecal pollution in coastal environments. Graduate School Theses and Dissertations 2008.
- Cantalupo, P.G.; Calgua, B.; Zhao, G.; Hundesa, A.; Wier, A.D.; Katz, J.P.; et al. Raw sewage harbors diverse viral populations. mBio 2021, 2, e00180–11. [Google Scholar] [CrossRef] [PubMed]
- Bibby, K.; Peccia, J. Identification of viral pathogen diversity in sewage sludge by metagenome analysis. Environ- mental Science and Technology 2013, 47, 1945–1951. [Google Scholar] [CrossRef]
- Fratini, M.; Di Bonito, P.; La Rosa, G. Oncogenic papillomavirus and polyomavirus in water environments: Is there a potential for waterborne transmission? Food Environ Virol. 2014, 6, 1–12. [Google Scholar] [CrossRef] [PubMed]
- Di Bonito, P.; Della Libera, S.; Petricca, S.; Iaconelli, M.; Sanguinetti, M.; Graffeo, R.; Accardi, L.; La Rosa, G. A large spectrum of alpha and beta papillomaviruses are detected in human stool samples. J Gen Virol. 2015, 96, 607–613. [Google Scholar] [CrossRef]
- Dediol, I.; Buljan, M.; Vurnek-A Ivkoviä, M.; Bulat, V.; A Itum, M.; A Ubriloviä, A. Psychological burden of anogenital warts. J Eur Acad Dermatol Venereol. 2009, 23, 1035–8. [Google Scholar] [CrossRef]
- Tyros, G.; Mastraftsi, S.; Gregoriou, S.; Nicolaidou, E. Incidence of anogenital warts: epidemiological risk factors and real-life impact of human papillomavirus vaccination. Int J STD AIDS. 2021, 32, 4–13. [Google Scholar] [CrossRef]
- Fortes, H.R.; von Ranke, F.M.; Escuissato, D.L.; Araujo Neto, C.A.; Zanetti, G.; Hochhegger, B.; Souza, C.A.; Marchiori, E. Recurrent respiratory papillomatosis: A state-of-the-art review. Respir Med. 2017, 126, 116–121. [Google Scholar] [CrossRef]
- Seedat, R.Y.; Dikkers, F.G. Global epidemiology of HPV-associated recurrent respiratory papillomatosis and effect of vaccination. Future Virology 2022, 17, 265–268. [Google Scholar]
- McLaughlin-Drubin, M.E.; Crum, C.P.; Münger, K. Human papillomavirus E7 oncoprotein induces KDM6A and KDM6B histone demethylase expression and causes epigenetic reprogramming. Proc Natl Acad Sci U S A. 2011, 108, 2130–5. [Google Scholar] [CrossRef]
- Singh, R.K. Diffuse Non-Genital Cutaneous Warts. The American journal of tropical medicine and hygiene 2021, 106, 378–379. [Google Scholar] [CrossRef] [PubMed]
- El Moussaoui, S.; Fernández-Campos, F.; Alonso, C.; Limón, D.; Halbaut, L.; Garduño-Ramirez, M.L.; Calpena, A.C.; Mallandrich, M. Topical Mucoadhesive Alginate-Based Hydrogel Loading Ketorolac for Pain Management after Pharmacotherapy, Ablation, or Surgical Removal in Condyloma Acuminata. Gels 2021, 7, 8. [Google Scholar] [CrossRef] [PubMed]
- Pennycook, K.B.; McCready, T.A. Condyloma Acuminata. In: StatPearls. StatPearls Publishing, Treasure Island (FL); 2022.
- Oyervides-Muñoz, M.A.; Pérez-Maya, A.A.; Rodríguez-Gutiérrez, H.F.; Gómez-Macias, G.S.; Fajardo-Ramírez, O.R.; Treviño, V.; Barrera-Saldaña, H.A.; Garza-Rodríguez, M.L. Understanding the HPV integration and its progression to cervical cancer. Infect Genet Evol. 2018, 61, 134–144. [Google Scholar] [CrossRef]
- Bañuelos-Villegas, E.G.; Pérez-yPérez, M.F.; Alvarez-Salas, LM. Cervical Cancer, Papillomavirus, and miRNA Dysfunction. Front Mol Biosci. 2021, 8, 758337. [Google Scholar] [CrossRef]
- Merz, J.; Bossart, M.; Bamberg, F.; Eisenblaetter, M. Revised FIGO Staging for Cervical Cancer - A New Role for MRI. Rofo. 2020, 192, 937–944. [Google Scholar] [CrossRef] [PubMed]
- Castanheira, C.P.; Sallas, M.L.; Nunes, R.A.L.; Lorenzi, N.P.C.; Termini, L. Microbiome and Cervical Cancer. Pathobiology. 2021, 88, 187–197. [Google Scholar] [CrossRef]
- Schlenker, B.; Schneede, P. The Role of Human Papilloma Virus in Penile Cancer Prevention and New Therapeutic Agents. Eur Urol Focus. 2019, 5, 42–45. [Google Scholar] [CrossRef]
- Iorga, L.; Dragos Marcu, R.; Cristina Diaconu, C.; Maria Alexandra Stanescu, A.; Pantea Stoian, A.; Liviu Dorel Mischianu, D.; Surcel, M.; Bungau, S.; Constantin, T.; Boda, D.; Fekete, L.; Gabriel Bratu, O. Penile carcinoma and HPV infection (Review). Exp Ther Med. 2020, 20, 91–96. [Google Scholar] [CrossRef]
- Kuasne, H.; Barros-Filho, M.C.; Busso-Lopes, A.; Marchi, F.A.; Pinheiro, M.; Muñoz, J.J.; Scapulatempo-Neto, C.; et al. Integrative miRNA and mRNA analysis in penile carcinomas reveals markers and pathways with potential clinical impact. Oncotarget 2017, 8, 15294–15306. [Google Scholar] [CrossRef] [PubMed]
- Johnson, D.E.; Burtness, B.; Leemans, C.R.; Lui, V.W.Y.; Bauman, J.E.; Grandis, J.R. Head and neck squamous cell carcinoma. Nat Rev Dis Primers. 2020, 6, 92. [Google Scholar] [CrossRef] [PubMed]
- Chen, Y.H.; Chien, C.Y.; Huang, T.L.; Chiu, T.J.; Wang, Y.M.; Fang, F.M.; Li, S.H. Low p16 Cytoplasmic Staining Predicts Poor Treatment Outcome in Patients with p16-Negative Locally Advanced Head and Neck Squamous Cell Carcinoma Receiving TPF Induction Chemotherapy. Biomedicines 2023, 11, 339. [Google Scholar] [CrossRef] [PubMed]
- Bik, E.M.; Bird, S.W.; Bustamante, J.P.; Leon, L.E.; Nieto, P.A.; Addae, K.; et al. A novel sequencing-based vaginal health assay combining self-sampling, HPV detection and genotyping, STI detection, and vaginal microbiome analysis. PLoS One 2019, 14, e0215945. [Google Scholar] [CrossRef] [PubMed]
- Eun, T.J.; Perkins, R.B. Screening for Cervical Cancer. The Medical clinics of North America 2020, 104, 1063–1078. [Google Scholar] [CrossRef] [PubMed]
- Markowitz, L.E.; Schiller, J.T. Human Papillomavirus Vaccines. The Journal of infectious diseases 2021, 224, S367–S378. [Google Scholar] [CrossRef] [PubMed]
- Gualano, M.R.; Bert, F.; Voglino, G.; Buttinelli, E.; D'Errico, M.M.; De Waure, C.; Di Giovanni, P.; Fantini, M.P.; Giuliani, A.R.; Marranzano, M.; Masanotti, G.; Massimi, A.; Nante, N.; Pennino, F.; Squeri, R.; Stefanati, A.; Signorelli, C.; Siliquini, R.; Collaborating Group. Attitudes towards compulsory vaccination in Italy: Results from the NAVIDAD multicentre study. Vaccine 2018, 36, 3368–3374. [Google Scholar] [CrossRef] [PubMed]
- Yazdani, Z.; Rafiei, A.; Valadan, R.; Ashrafi, H.; Pasandi, M.; Kardan, M. Designing a potent L1 protein-based HPV peptide vaccine: a bioinformatics approach. Computational biology and chemistry. 2020, 85, 107209. [Google Scholar] [CrossRef]
- Soca Gallego, L.; Dominguez, A.; Parmar, M. Human Papilloma Virus Vaccine. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Harden, M.E.; Munger, K. Human papillomavirus molecular biology. Mutat Res Rev Mutat Res. 2017, 772, 3–12. [Google Scholar] [CrossRef]
- Panwar, K.; Godi, A.; Cocuzza, C.E.; Andrews, N.; Southern, J.; Turner, P.; Miller, E.; Beddows, S. Multiplex Human Papillomavirus L1L2 virus-like particle antibody binding assay. MethodsX. 2022, 9, 101776. [Google Scholar] [CrossRef]
- Godi, A.; Panwar, K.; Haque, M.; Cocuzza, C.E.; Andrews, N.; Southern, J.; Turner, P.; Miller, E.; Beddows, S. Durability of the neutralizing antibody response to vaccine and non-vaccine HPV types 7 years following immunization with either Cervarix® or Gardasil® vaccine. Vaccine. 2019, 37, 2455–2462. [Google Scholar] [CrossRef]
- Roser, M.; Ortiz-Ospina, E.-. "Which countries include human papillomavirus (HPV) vaccines in their vaccination schedules?, 2021". (accessed on: 02/03/23). Available online: https://ourworldindata.org/grapher/human-papillomavirus-vaccine-immunization-schedule?country=BFA~ROU~ARM.
- Brotherton, J.M.; Malloy, M.; Budd, A.C.; Saville, M.; Drennan, K.T.; Gertig, D.M. Effectiveness of less than three doses of quadrivalent human papillomavirus vaccine against cervical intraepithelial neoplasia when administered using a standard dose spacing schedule: observational cohort of young women in Australia. Papillomavirus Research 2015, 1, 59–72. [Google Scholar] [CrossRef]
- Wang, W.V.; Kothari, S.; Khoury, H.; Niccolai, L.; Garland, S.M.; Sundström, K.; de Pouvourville, G.; Bonanni, P.; Chen, Y.T.; Franco, E.L. A review of data systems for assessing the impact of HPV vaccination in selected high-income countries. Expert Rev Vaccines. 2023, 22, 161–179. [Google Scholar] [CrossRef] [PubMed]
- Dorji, T.; Tshomo, U.; Gyamtsho, S.; Tamang, S.T.; Wangmo, S.; Pongpirul, K. Gender-neutral HPV elimination, cervical cancer screening, and treatment: Experience from Bhutan. Int J Gynecol Obstet 2022, 156, 425–429. [Google Scholar] [CrossRef]
- Dykens, J.A.; Peterson, C.E.; Holt, H.K.; Harper, D.M. Gender neutral HPV vaccination programs: Reconsidering policies to expand cancer prevention globally. Front Public Health. 2023, 11, 1067299. [Google Scholar] [CrossRef] [PubMed]
- Amponsah-Dacosta, E.; Blose, N.; Nkwinika, V.V.; Chepkurui, V. Human Papillomavirus Vaccination in South Africa: Programmatic Challenges and Opportunities for Integration With Other Adolescent Health Services? Front Public Health. 2022, 10, 799984. [Google Scholar] [CrossRef]
- Ma, Y.; Wang, C.; Liu, F.; Lian, G.; Li, S.; He, Q.; Li, T. Human papillomavirus vaccination coverage and knowledge, perceptions and influencing factors among university students in Guangzhou, China. Hum Vaccin Immunother. 2021, 17, 3603–3612. [Google Scholar] [CrossRef]
- Simms, K.T.; Hanley, S.J.B.; Smith, M.A.; Keane, A.; Canfell, K. Impact of HPV vaccine hesitancy on cervical cancer in Japan: a modelling study. Lancet Public Health. 2020, 5, e223–e234. [Google Scholar] [CrossRef]
- Meites, E.; Szilagyi, P.G.; Chesson, H.W.; Unger, E.R.; Romero, J.R.; Markowitz, L.E. Human Papillomavirus Vaccination for Adults: Updated Recommendations of the Advisory Committee on Immunization Practices. MMWR Morb Mortal Wkly Rep 2019, 68, 698–702. [Google Scholar] [CrossRef]
- Nogueira-Rodrigues, A.; Flores, M.G.; Macedo Neto, A.O.; Braga, L.A.C.; Vieira, C.M.; de Sousa-Lima, R.M.; de Andrade, D.A.P.; Machado, K.K.; Guimarães, A.P.G. HPV vaccination in Latin America: Coverage status, implementation challenges and strategies to overcome it. Front Oncol. 2022, 12, 984449. [Google Scholar] [CrossRef]
- Athanasiou, A.; Bowden, S.; Paraskevaidi, M.; Fotopoulou, C.; Martin-Hirsch, P.; Paraskevaidis, E.; Kyrgiou, M. HPV vaccination and cancer prevention. Best Pract Res Clin Obstet Gynaecol. 2020, 65, 109–124. [Google Scholar] [CrossRef] [PubMed]
- Sheikh, S.; Biundo, E.; Courcier, S.; Damm, O.; Launay, O.; Maes, E.; Marcos, C.; Matthews, S.; Meijer, C.; Poscia, A.; Postma, M.; Saka, O.; Szucs, T.; Begg, N. A report on the status of vaccination in Europe. Vaccine. 2018, 36, 4979–4992. [Google Scholar] [CrossRef]
- Nguyen-Huu, N.H.; Thilly, N.; Derrough, T.; Sdona, E.; Claudot, F.; Pulcini, C.; Agrinier, N. ; HPV Policy working group. Human papillomavirus vaccination coverage, policies, and practical implementation across Europe. Vaccine. 2020, 38, 1315–1331. [Google Scholar] [PubMed]
- Italian Communication campaign on HPV vaccination. Available at: [https://www.salute.gov.it/portale/vaccinazioni/dettaglioCampagneVaccinazioni.jsp?lingua=italiano& menu=campagne&p=dacampagne&id=167] (Accessed on: 28/03/23).
- Giuliano, A.R.; Nyitray, A.G.; Albero, G. Male circumcision and HPV transmission to female partners. Lancet. 2011, 377, 183–4. [Google Scholar] [CrossRef] [PubMed]
- Global strategy to accelerate the elimination of cervical cancer as a public health problem. Geneva: World Health Organization; 2020. Available at: https://www.who.int/publications/i/item/9789240014107 (Accessed on 29/03/23).
- Sami, J.; Lemoupa Makajio, S.; Jeannot, E.; et al. Smartphone-Based Visual Inspection with Acetic Acid: An Innovative Tool to Improve Cervical Cancer Screening in Low-Resource Setting. Healthcare (Basel). 2022, 10, 391. [Google Scholar] [CrossRef] [PubMed]
- Khairkhah, N.; Bolhassani, A.; Najafipour, R. Current and future direction in treatment of HPV-related cervical disease. J Mol Med (Berl). 2022, 100, 829–845. [Google Scholar] [CrossRef]
- Cooper, D.B.; Dunton, C.J. Colposcopy. 2022 Jul 16. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2023.
- Bhatla, N.; Singhal, S. Primary HPV screening for cervical cancer. Best Pract Res Clin Obstet Gynaecol. 2020, 65, 98–108. [Google Scholar] [CrossRef]
- Tota, J.E.; Bentley, J.; Blake, J.; Coutlée, F.; Duggan, M.A.; Ferenczy, A.; et al. Introduction of molecular HPV testing as the primary technology in cervical cancer screening: Acting on evidence to change the current paradigm. Preventive medicine 2017, 98, 5–14. [Google Scholar] [CrossRef]
- Ebisch, R.M.F.; Rijstenberg, L.L.; Soltani, G.G.; et al. Adjunctive use of p16 immunohistochemistry for optimizing management of CIN lesions in a high-risk human papillomavirus-positive population. Acta Obstet Gynecol Scand. 2022, 101, 1328–1336. [Google Scholar] [CrossRef]
- Stoler, M.H.; Wright, T.C. Jr.; Ferenczy, A.; Ranger-Moore, J.; Fang, Q.; Kapadia, M.; Ridder, R. Routine Use of Adjunctive p16 Immunohistochemistry Improves Diagnostic Agreement of Cervical Biopsy Interpretation: Results From the CERTAIN Study. Am J Surg Pathol. 2018, 42, 1001–1009. [Google Scholar] [CrossRef]
- Profozić, Z.; Meštrović, T.; Savić, I.; Profozić, V. Prevalence of HPV Infection in Croatian Men during a 12-year Period: a Comparative Study of External Genital and Urethral Swabs. Cent Eur J Public Health. 2016, 24, 321–325. [Google Scholar] [CrossRef] [PubMed]
- Pan, L.J.; Ma, J.H.; Zhang, F.L.; Pan, F.; Zhao, D.; Zhang, X.Y. [HPV infection of the external genitalia in men whose female partners have cervical HPV infection]. Zhonghua Nan Ke Xue. 2018, 24, 516–519. [Google Scholar] [PubMed]
- Luttmer, R.; Dijkstra, M.G.; Snijders, P.J.F.; et al. Presence of human papillomavirus in semen of healthy men is firmly associated with HPV infections of the penile epithelium. Fertil Steril. 2015, 104, 838–844e8. [Google Scholar] [CrossRef] [PubMed]
- Tuan, L.A.; Prem, K.; Pham, Q.D.; Toh, Z.Q.; Tran, H.P.; Nguyen, P.D.; et al. Anal human papillomavirus prevalence and risk factors among men who have sex with men in Vietnam. Int J Infect Dis. 2021, 112, 136–143. [Google Scholar] [CrossRef]
- Shapiro, G.K. HPV Vaccination: An Underused Strategy for the Prevention of Cancer. Curr Oncol. 2022, 29, 3780–3792. [Google Scholar] [CrossRef] [PubMed]
- Kisling, L.A.; M Das, J. Prevention Strategies. 2022 May 8. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2022.
- Swedish, K.A.; Factor, S.H.; Goldstone, S.E. Prevention of recurrent high-grade anal neoplasia with quadrivalent human papillomavirus vaccination of men who have sex with men: a nonconcurrent cohort study. Clin Infect Dis. 2012, 54, 891–8. [Google Scholar] [CrossRef]
- Deshmukh, A.A.; Cantor, S.B.; Fenwick, E.; Chiao, E.Y.; Nyitray, A.G.; Stier, E.A.; Goldstone, S.E.; Wilkin, T.; Chhatwal, J. Adjuvant HPV vaccination for anal cancer prevention in HIV-positive men who have sex with men: The time is now. Vaccine. 2017, 35, 5102–5109. [Google Scholar] [CrossRef]
- Ghelardi, A.; Parazzini, F.; Martella, F.; Pieralli, A.; Bay, P.; Tonetti, A.; Svelato, A.; Bertacca, G.; Lombardi, S.; Joura, E.A. SPERANZA project: HPV vaccination after treatment for CIN2. Gynecol Oncol. 2018, 151, 229–234. [Google Scholar] [CrossRef]
- Michalczyk, K.; Misiek, M.; Chudecka-Głaz, A. Can Adjuvant HPV Vaccination Be Helpful in the Prevention of Persistent/Recurrent Cervical Dysplasia after Surgical Treatment? -A Literature Review. Cancers (Basel). 2022, 14, 4352. [Google Scholar] [CrossRef]
- Di Donato, V.; Caruso, G.; Bogani, G.; Cavallari, E.N.; Palaia, G.; Perniola, G.; Ralli, M.; et al. HPV Vaccination after Primary Treatment of HPV-Related Disease across Different Organ Sites: A Multidisciplinary Comprehensive Review and Meta-Analysis. Vaccines (Basel). 2022, 10, 239. [Google Scholar] [CrossRef]
- Kin Cho Goon, P.; Scholtz, L.U.; Sudhoff, H. Recurrent respiratory papillomatosis (RRP)-time for a reckoning? Laryngoscope Investig Otolaryngol. 2017, 2, 184–186. [Google Scholar] [CrossRef] [PubMed]
- Swedish, K.A.; Goldstone, S.E. Prevention of anal condyloma with quadrivalent human papillomavirus vaccination of older men who have sex with men. PLoS One. 2014, 9, e93393. [Google Scholar] [CrossRef] [PubMed]
- Goon, P.; Sauzet, O.; Schuermann, M.; Oppel, F.; Shao, S.; Scholtz, L.U.; Sudhoff, H.; Goerner, M. Recurrent Respiratory Papillomatosis (RRP)-Meta-analyses on the use of the HPV vaccine as adjuvant therapy. NPJ Vaccines. 2023, 8, 49. [Google Scholar] [CrossRef] [PubMed]
- Husein-ElAhmed, H. Could the human papillomavirus vaccine prevent recurrence of ano-genital warts?: a systematic review and meta-analysis. Int J STD AIDS. 2020, 31, 606–612. [Google Scholar] [CrossRef] [PubMed]
- Mirghani, H.; Jung, A.C.; Fakhry, C. Primary, secondary and tertiary prevention of human papillomavirus-driven head and neck cancers. Eur J Cancer. 2017, 78, 105–115. [Google Scholar] [CrossRef] [PubMed]
- Rettig, E.M.; Wentz, A.; Posner, M.R.; Gross, N.D.; Haddad, R.I.; Gillison, M.L.; et al. Prognostic implication of persistent human papillomavirus type 16 DNA detection in oral rinses for human papillomavirus-related oropharyngeal carcinoma. JAMA Oncol 2015, 1, 907e15. [Google Scholar] [CrossRef] [PubMed]
- Fakhry, C.; Qualliotine, J.R.; Zhang, Z.; Agrawal, N.; Gaykalova, D.A.; Bishop, J.A.; et al. Serum antibodies to HPV16 early proteins warrant investigation as potential biomarkers for risk stratifica- tion and recurrence of HPV-associated oropharyngeal cancer. Cancer Prev Res (Phila) 2016, 9, 135e41. [Google Scholar] [CrossRef] [PubMed]
- Dahlstrom, K.R.; Li, G.; Hussey, C.S.; Vo, J.T.; Wei, Q.; Zhao, C.; et al. Circulating human papillomavirus DNA as a marker for disease extent and recurrence among patients with oropharyngeal cancer. Cancer 2015, 121, 3455e64. [Google Scholar] [CrossRef]
- Lin, J.C.; Wang, W.Y.; Chen, K.Y.; Wei, Y.H.; Liang, W.M.; Jan, J.S.; et al. Quantification of plasma Epstein-Barr virus DNA in patients with advanced nasopharyngeal carcinoma. N Engl J Med 2004, 350, 2461e70. [Google Scholar] [CrossRef]
- Twu, C.W.; Wang, W.Y.; Liang, W.M.; Jan, J.S.; Jiang, R.S.; Chao, J.; et al. Comparison of the prognostic impact of serum anti-EBV anti- body and plasma EBV DNA assays in nasopharyngeal carcinoma. Int J Radiat Oncol Biol Phys 2007, 67, 130e7. [Google Scholar] [CrossRef]
- Chrysostomou, A.C.; Stylianou, D.C.; Constantinidou, A.; Kostrikis, LG. Cervical Cancer Screening Programs in Europe: The Transition Towards HPV Vaccination and Population-Based HPV Testing. Viruses. 2018, 10, 729. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Age-standardized incidence rates of cervical cancer in the world (2020) (Source: International Agency Research on Cancer, WHO 2020).
Figure 1.
Age-standardized incidence rates of cervical cancer in the world (2020) (Source: International Agency Research on Cancer, WHO 2020).
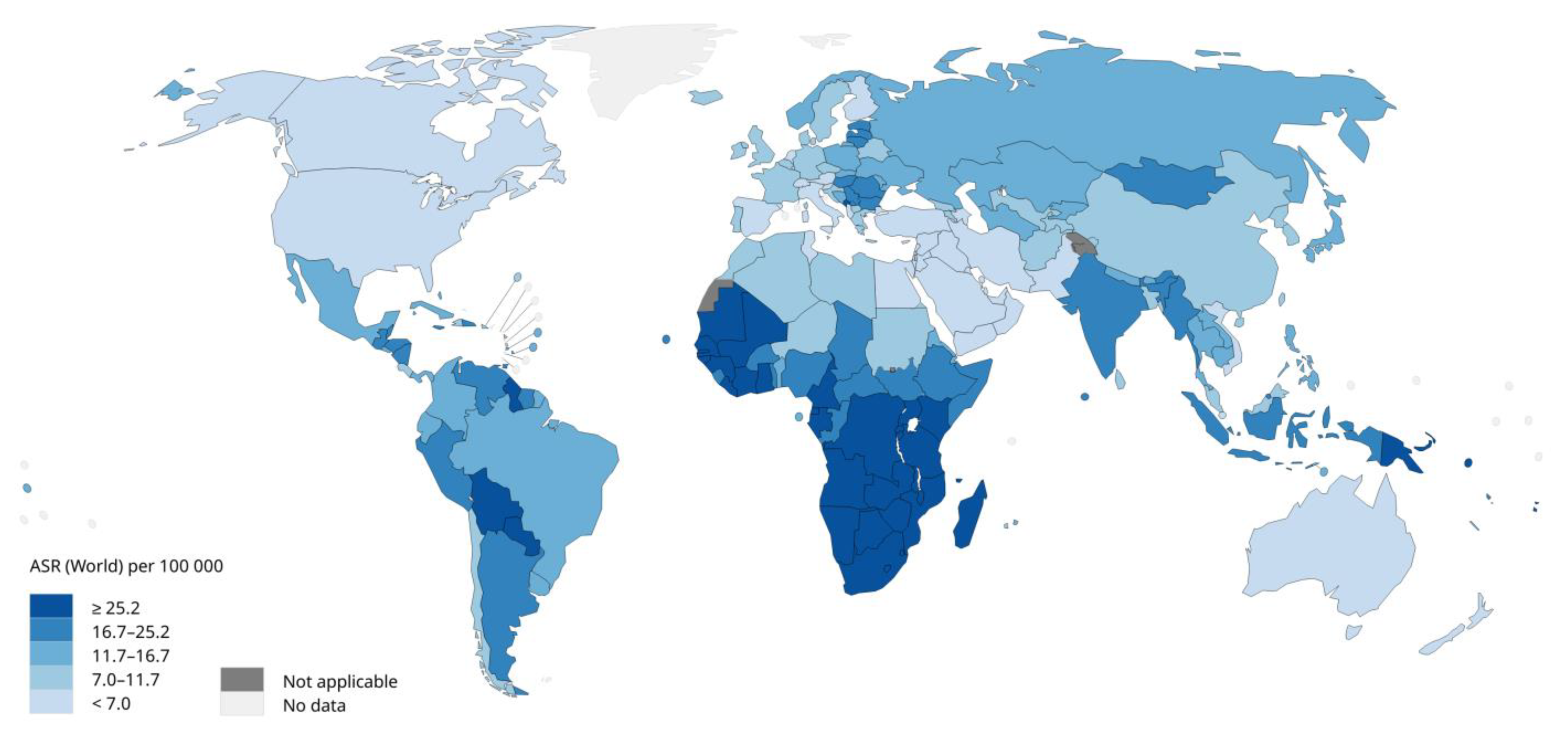
Figure 2.
Countries which provide and recommend HPV vaccines through routine services (2021). Source: OurWorldInData.org/vaccination • CC BY).
Figure 2.
Countries which provide and recommend HPV vaccines through routine services (2021). Source: OurWorldInData.org/vaccination • CC BY).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



