
Submitted:
18 April 2023
Posted:
19 April 2023
You are already at the latest version
Abstract
Mood and anxiety disorders affect pregnant people and their families at increased rates throughout the perinatal period. Geographic, financial, and social barriers persist in identification and access to care that preclude adequate diagnosis and treatment of anxiety and mood disorders. These challenges have been exacerbated by the COVID-19 pandemic, particularly for Black and Indigenous People and People of Color (BIPOC) who already experience increased risk for adverse mental health outcomes and faced structural barriers to accessing perinatal mental health care at baseline. The literature shows that integrated care can improve mental health outcomes and save billions of dollars in annual healthcare costs. This study evaluated a novel statewide integrated care effort designed to facilitate access to perinatal mental health care for OB/GYN patients. In addition to enrollment data, variables studied were maternal program satisfaction, retention rates, and preliminary maternal mental health outcomes. 285 patients were ever referred for care. Of this, we contacted 259 patients (91%) and enrolled 209 (72%). Of the 209, 48 were lost to follow up, while 107 remained enrolled at the time of data analysis. 54 patients met their treatment goals. 97% of individuals asserted they were satisfied with the services they received. Black race and public insurance predicted faster attrition from treatment; risk for interpersonal violence exposure and substance use were not related to attrition. Preliminary mental health outcomes showed significant decreases in anxiety and depression, with the most dramatic decreases in the first month of treatment. The MC3 Perinatal care program is a viable, patient-endorsed collaborative care model that increases access to perinatal mental health and facilitate access to outside resources.
Keywords:
perinatal mental health
; integrated care
; psychiatry consultation
; collaborative care
; implementation science
1. Introduction
Mood and anxiety disorders affect pregnant people and their families at increased rates throughout the perinatal period. Perinatal depression affects between 11-15% of obstetric populations [1-4]. According to a 2013 study by Wisner et al., individuals experienced onset of depressive episodes at the highest rate during postpartum (40.1%), pregnancy (33.4%), and before pregnancy (26.5%) [5]. Further, 19.3% of individuals across the peripartum period experience suicidal ideations [5], and suicidality in pregnancy and postpartum is on the rise in the US [6]. Of those who screen positive for unipolar depression, approximately 20% of individuals meet criteria for bipolar depression [1]. Anxiety affects up to 20% of individuals during pregnancy, and as many as 50% of individuals immediately postpartum [7]. Substance use occurs among at least 10% of perinatal individuals, and estimates hold that it accounts for 8-22% of maternal mortality [1]. Yet despite these prevalence rates, adequate detection and treatment are sparse; prior work suggests that up to 70% of patients go undetected, approximately 85% go untreated, up to 93% are inadequately treated, and as many as 97% of patients continue to suffer from symptoms without remission [8,9].
Undertreated and underdiagnosed mental health concerns can impact families in a myriad of ways. A 2021 study found that people with perinatal mental health disorders experienced 50% higher rates of severe maternal morbidity, and 87% higher rates among those with trauma- or stress-related mental health disorders, as compared with people without perinatal mental health disorders [4]. This study also estimated an increased annual delivery cost of $102 million in the US among people with perinatal mental health conditions, versus those without [4]. Mild and moderate symptoms may interfere with functioning and one’s ability to maintain jobs and households; severe symptoms may result in self-harm and even suicide or infanticide [8.9]. Moreover, even if not with fatal consequences to the child, mental illness can confer negative impact on parenting and in turn, infant emotional development, and self-regulation, posing risk to the mental health of the developing child [10-12].
In the midst of the COVID-19 pandemic, mental health challenges became exacerbated. Data from a recent Canadian study suggest increased rates of perinatal depression and anxiety during the COVID-19 pandemic, with more than a third of pregnant individuals reporting depression symptoms and more than half reporting anxiety symptoms [13,14]. Many health care institutions also saw increased rates of substance use and interpersonal violence (IPV), both of which confer additional risk for mental health concerns [15-17]. Prior to COVID-19, Black and Indigenous People and People of Color (BIPOC) already experienced increased risk for adverse mental health outcomes and faced structural barriers to accessing perinatal mental health care at baseline. The pandemic only compounded these existing inequities [18].
The vast majority of pregnant people in America interact with medical professionals over the course of their pregnancies. In 2016, 77.1% of gestational patients received obstetric care beginning in their first trimester of pregnancy [19]. Only 1.6% of pregnant individuals received no prenatal care prior to delivery [19]. Obstetrician-gynecologists (OB/GYNs) are, in many cases, the only healthcare provider that women of childbearing age see on a regular basis [20,21]. OB/GYN visits represent one-third of all office visits for women between the ages of 18-45, and most non-illness related office visits for women under 65 years of age [20,21]. As established, providers see increased rates of mental health challenges during perinatal periods (preconception, pregnancy and postpartum); however, these mental health symptoms are often undertreated due to lack of training, staffing shortages, and time constraints within OB/GYN office settings, as well as the sociocultural stigma surrounding mental health conditions which makes patients reticent to admit to symptoms [20]. Given the near ubiquity of OB/GYN care, combined with the barriers to accessing dedicated mental healthcare, OB/GYN offices are an optimal site for addressing perinatal mental health conditions through integrated care.
Research shows that integrating mental health into primary and obstetrical care can greatly improve mental health outcomes and save healthcare costs [20,21]. US obstetric trials have shown improved depression outcomes in pregnancy and postpartum when integrative collaborative care includes an engagement session, assessment by a member of the care team, a patient-led choice between an antidepressant medication or psychotherapy, and patient outreach following any missed appointments [3]. Integrating mental health screening within obstetric care aligns with current recommendations from the American College of Obstetrics and Gynecologists (ACOG), which recommends screening for depression, bipolar disorder, anxiety, trauma, IPV, adverse childhood experiences (ACEs), substance use disorders, and social determinants of health (SDOH) [1,22]. Other professional organizations, including both the American Psychiatric Association (APA) and the US Preventive Services Task Force (USPSTF), advocate for mental health screening as well [1]. Programs like the Massachusetts Child Psychiatry Access Program (MCPAP) for Moms seek to expand screening for pregnant individuals among obstetric providers, building capacity both at the provider and practice levels to promote appropriate treatment and diagnosis [18,23].
One of the models of integrated behavioral healthcare is the Collaborative Care (CoCM or IMPACT) model. CoCM emphasizes patient-centered care and integration of the patients’ goals into the treatment plan while also prioritizing population-based care or a shared registry of patients. As part of CoCM, a behavioral health consultant (BHC) and a psychiatrist regularly meet to ensure all individuals receive appropriate services. The BHC then communicates back to the clinic about the recommendations from the psychiatrist. This model emphasizes the importance of communication between the health care provider, the clinic, and the BHC.
The CoCM has been successfully employed in primary care and obstetric care. Work conducted by Nancy Grote and others at the University of Washington has demonstrated benefits of the model within obstetrics in improving depression symptoms [24], and that providing behavioral activation and problem-solving therapy to women with depression demonstrates improved engagement in the program [25]. The focus for the CoCM is the female patient and her wellness. To date, only one program recommends attention to the parent-child relationship and highlights the importance of mothers’ mental health in supporting their children’s development; however, this program (The Maternal Infant Dyad Implementation Initiative (MIND-I) from the University of Washington) appears to be in early implementation with no published research at the time of this writing [26].
1.1. The Michigan Clinical Consultation and Care in Perinatal (MC3 Perinatal) Model
MC3 Perinatal, funded by the state of Michigan health department and housed at Michigan Medicine in the Department of Psychiatry, combines the CoCM framework (“care” arm) with a Perinatal Psychiatry Consultation program (“consultation” arm). The consultation arm offers free-of-charge, same-day consultation services to obstetrical providers across the entire state of Michigan (50 counties) and was originally established in 2014. Providers can access same-day consultation to discuss any topics of concern related to mental health as they are treating perinatal patients in their offices (e.g., which medications to select, therapy options available in the region, diagnostic clarifications based on presenting symptoms, etc.). Enrollment is simple, and access to the consultation service is available during weekdays either by phone call or an online consult form; upon review of the request by a care coordinator, the consultation request can either be answered by the coordinator (e.g., regional resources), or the consulting psychiatrist-of-the day, who responds via a direct phone conversation to the provider’s medical questions. Each consultation ends with a written summary of recommendations that are shared with the provider via a secure email.
More recently, in response to the critical need for perinatal psychotherapy across Michigan, a direct “care” arm pilot was added in 2021, presently serving 6 counties (with the intent to fully expand across Michigan over time). The care arm enables instant access to virtual one-on-one psychotherapy services for perinatal patients and is grounded in a CoCM. The full MC3 Perinatal model is depicted in Figure 1.
The consultation arm of MC3 Perinatal resembles other established Perinatal Psychiatry Consultation programs across the US, for example, the MCPAP for Moms program in Massachusetts [23]. Overall, there are currently 26 states `with perinatal consultation access programs, and all of them are part of a National Network of Perinatal Psychiatry Access Programs under an umbrella called Lifeline for Moms. We have reported on the consultation program elsewhere [27]. However, the coupling of this consultation service for providers with a direct patient-facing care model is a novel, unique, critical enhancement of our Michigan program. We have not yet reported on this care model nor presented data. Thus, in this paper, we will elaborate on the clinical workings of the “care” arm, the MC3 Perinatal Care model, and present our pilot implementation data since the model’s inception in 2021.
1.2. Clinical Workflow of the MC3 Perinatal Care Arm
The goal of the MC3 Care arm is to connect patients presenting to obstetrical care to licensed behavioral health consultants (BHCs) and initiate instant connection, allow for a mental health evaluation, and start (if indicated) promptly a brief one-on-one therapy process. Patients either self-refer in response to flyers in their obstetrician’s waiting room, or are encouraged by their providers to enroll; in both cases, enrollment is user-friendly using a QR code that directly links the patient to a secure intake webpage. Once enrolled, patients automatically connect to the BHC, who initiates a same-day telephone or text connection and schedules an initial intake interview at the patient’s convenience. The BHCs are highly trained therapists, either PhD level clinical psychologists or Licensed Masters-level Social Workers (LMSW).
In accordance with the CoCM, all patients are entered into a patient registry after the initial evaluation and are discussed in the weekly panel review with the perinatal psychiatrist. Each patient is discussed at least once at intake and again if the clinical presentation is not improving, as measured objectively by asking patients to fill out monthly metrics for depression and anxiety. During panel review, a 90-minute group meeting with one perinatal psychiatrist staffing 3 BHCs, the team collaboratively determines medication, therapy, and resource needs. If medications are recommended, the BHCs coordinate with the obstetrical provider to initiate the prescription of the psychotropic medicine. If obstetrical providers have concerns or questions, they can consult via telephone with the perinatal psychiatrist using the MC3 Perinatal Consult arm same day.
All patients in MC3 Care are standardly offered up to 8 sessions therapy with the BHCs. Patients who have longer-term therapy needs are connected through a “warm hand-off” to community therapy resources, for example, home visiting programs. Patients who are hard to refer to community resources are bridged until they can be connected, even if they require more than 8 sessions. The BHCs are trained in many evidence-based interventions, including Cognitive Behavioral Therapy (CBT), Dialectical Behavioral Therapy (DBT), Acceptance and Commitment Therapy (ACT), Interpersonal Therapy (IPT), Motivational Interviewing, and Infant Mental Health (IMH) [28-33]. In addition to therapy, BHCs are also trained to provide case management and resourcing to meet tangible needs (e.g., housing, food, diapers, etc.).
All patients provide monthly self-ratings on depression and anxiety measures (PHQ-9 and GAD-7) until 12 months postpartum, even after they complete their brief therapy course and are referred to the community. These self-rating metrics on depression and anxiety determine ongoing wellbeing and response to initial treatment. With patient consent, the results of the monthly metrics are also shared with the patient providers (either the obstetric provider or primary care provider). If a patient is not showing a decrease in symptom scores on the metrics, the case is re-presented at panel review and additional care recommendations are implemented and shared with the patient providers.
The MC3 Perinatal Care arm is similar to the consultation arm in that it is free of charge and is delivered to patients fully remote via phone, text messaging, video chat, or email, based on patient preference and ability, at a pace that aligns with patient needs and wishes. Some patients choose weekly therapy/counseling sessions, and some want to space sessions more or less frequently. Session length is individually adjusted based on patient need and preference. Patients are empowered to co-create the care they receive, and as such, the program is culturally responsive, combats stigma, and provides equitable care to vulnerable perinatal populations. Cultural responsiveness is achieved by maintaining a diverse staff from many racial and ethnic backgrounds that is highly experienced in providing perinatal care to urban and rural populations alike. Currently, the MC3 Perinatal Care staff is comprised of three part-time perinatal psychiatrists covering panel reviews and consults, six full or part-time BHCs, and an administrative team for evaluation, outreach, and training activities.
The primary aim of this manuscript is to present initial pilot data on care arm of the MC3 Perinatal program in Michigan. We will share initial program implementation outcomes since program inception in 2021, including number of patients served, patient demographics, number and type of treatments delivered, patient satisfaction, retention rates in program, and preliminary findings on maternal mental health benefits. We hope to encourage other perinatal health care systems to adopt a similar integrated approach that will ultimately benefit their perinatal patients with mental health concerns.
2. Materials and Methods
2.1. Participants and Procedures
Individuals enrolled in the MC3 Perinatal care arm connect to the BHCs either self-referred in response to flyers in the obstetrician’s waiting room or are referred by their obstetrical provider to enroll; in both cases, patients access a user-friendly QR code that directly links them to a secure intake webpage to provide their name and contact information for the remote BHC to contact the patient at patient’s convenience. Patients who are eligible to receive BHC care through the MC3 Perinatal care arm are 18-years and older, currently pregnant or postpartum within 12 months of birthing, and are not actively suicidal or homicidal requiring emergency care. If an eligible patient connects successfully with the BHC, they electronically complete an informed consent for care and a baseline intake and are at that time counted as enrolled in the program.
Once enrolled, patients engage in brief therapy, care coordination, or case management, and can select the goals of the sessions in collaboration with the therapist. Therapy includes an array of evidence-based practices (e.g. Cognitive Behavioral Therapy (CBT), Mindfulness, Dialectical Behavior Therapy (DBT), Infant Mental Health (IMH)) and is tailored to meet the patient’s needs. This manuscript reports aggregate data collected between 7/2021 to 12/2022 (18 months) for enrolled patients who consented to receive clinical care and provided baseline intake metrics. The project is approved as a Quality Improvement, Quality Assurance project within the University of Michigan by our Institutional Review Board (IRB).
2.2. Measures
Patient Descriptors: A) Patient Demographics: At intake patients self-reported age, race, and type of insurance (which was used as a proxy for socio-economic status, SES). B) Patient presenting concerns: At referral, patients indicated the concerns they hoped to address through services.
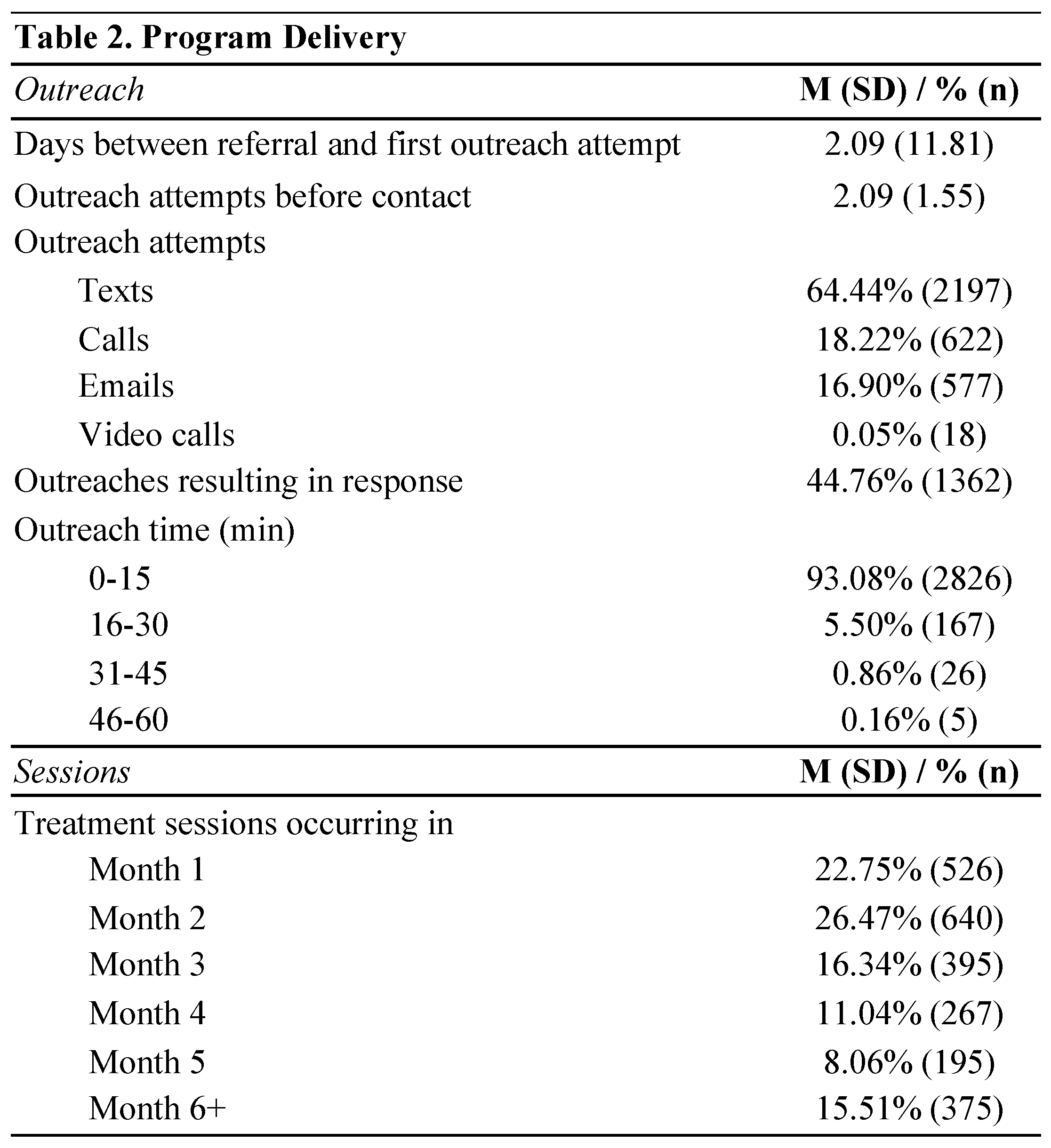
Program Descriptors: A) Number of Outreach sessions: BHCs reach out to patients to schedule sessions, check in, and offer resources. All BHC outreach sessions/attempts to patients are documented, including categorical time spent on outreach (0-15 minutes, 16-30 minutes, 31-45 minutes, 46-60 minutes, and 61-75 minutes), method of outreach (phone, text, email, virtual), whether a response was received from the patient, and any miscellaneous additional comments. We computed the total number of outreach attempts, total number of times a clinician outreach resulted in a response from the patient, and the total time spent on outreach in two ways: 1) as the numeric average of the categorical ranges, summed across all outreaches and individuals, and 2) as the percent of outreaches conducted in each category of time.
B) Number of therapy sessions: BHC therapy sessions are documented in two ways: 1) in surveys where BHCs document for each patient and session time spent in session (0-15 minutes, 16-30 minutes, 31-45 minutes, 46-60 minutes, and 61-75 minutes), which metrics used in particular session, and interventions utilized during session, and 2) in a patient tracking tool where BHCs indicated the date on which a session was scheduled, missed, or successfully completed. Total number of sessions are computed as the total number of successfully completed sessions. Total time spent in sessions is computed as the numeric average of the categorical ranges of time, summed across all sessions and individuals.
C) Patient Satisfaction: Patient satisfaction is completed at baseline, and once a month for each month the patient is enrolled in services. This measure includes six items from the Client Satisfaction Questionnaire (CSQ-8) which determined patient levels of satisfaction on a 4-point scale, from “Strongly Disagree” to “Strongly Agree” [34]. For this paper, the “Strongly Agree” and “Agree” rating categories were combined and the “Disagree” and “Strongly Disagree” rating categories were combined. This measure also includes three open-ended questions assessing what the patient felt was most and least useful about the program, and what they would change to make the program better. Response themes from open-ended satisfaction questions were coded and verified by the study team. The Satisfaction surveys were not implemented until July 2022; therefore, this paper reflects data collected from July 2022 to February 2023.
Mental Health Variables: A) The 5Ps Prenatal Substance Abuse Screen: We assessed for risk of substance abuse at baseline with the 5Ps Prenatal Substance Abuse Screen [35]. This measure includes questions about whether the patient’s parents, friends, or partners have had problems with alcohol or drug use, and whether the participant has had problems with alcohol or drug use prior to pregnancy. An endorsement of any of the 5Ps items was used to indicate risk of substance use.
B) Interpersonal Violence Risk Screen: We assessed for risk of interpersonal violence (IPV) at baseline with 4 items created by the study team. This measure asks, in the last year, whether you have been: “afraid of someone close (or less close) to you?”, “hit, slapped, kicked, pushed, shoved, or otherwise physically hurt by someone close (or less close) to you?”, “frequently made upset, ashamed, or embarrassed by someone close (or less close) to you?”, and “forced to have sex by someone close (or less close) to you?”. Endorsement of one or more items was flagged as risk of IPV.
C) Generalized Anxiety Disorder-7: The Generalized Anxiety Disorder-7 (GAD-7), a 7-item questionnaire, was used to assess symptoms of generalized anxiety disorder (GAD) [36,37]. Participants answered questions on a 4-point Likert scale (0 = “Not at all” to 3 = “Nearly every day”) indicating how often they have been bothered by problems, for example: “Not being able to stop or control worrying,” and “Becoming easily annoyed or irritable.” Scores were totaled to suggest current severity of symptoms: <4 = minimal anxiety, 5-9 mild anxiety, 10-14 moderate anxiety, and 15-21 = severe anxiety. This measure was completed at baseline, as well as once per month for each month the patient was enrolled in services.
D) Patient Health Questionnaire: is a 9-item self-report measure used to assess symptoms of major depressive disorder [38,39]. Participants answer questions on a 4-point likert type scale (0 = “Not at all” to 3 = “Nearly every day”) indicating how often they have been bothered by problems, for example: “Feeling down, depressed, or hopeless,” and “Trouble concentrating on things.” Scores were then totaled to suggest current severity of symptoms. The clinical cutoff of 10 was used to differentiate probable depression diagnosis. This measure was completed at baseline, and once a month for each month the patient was enrolled in services.
2.3. Statistical Methods
Data analyses were performed using SAS 9.4 and Mplus v. 8.8. We provide descriptive statistics of the population presenting for services, including their presenting concerns, and levels of mental health symptoms from time of recruitment into services. Survival analysis, using Cox regression (SAS PROC PHREG), was used to examine retention in services. SAS PROC LIFETEST was used to plot the survival trajectories. Trajectories of mental health symptoms were modeled using latent growth modeling in Mplus, using full information maximum likelihood to handle missing data.
3. Results
3.1. Patient and Program Descriptors
As illustrated in Figure 2, since program inception in 7/2021, 285 patients have been referred for MC3 Perinatal direct care. Of this, the BHC contacted 259 patients (91%) and enrolled 209 (72%). Of the 209, 48 were lost to follow up, while 107 remained currently enrolled at the time of data analysis. 54 patients met their treatment goals.
3.1.1. Demographics and Presenting Concerns
Of 285 patients who were referred to the program since inception (7/2021), 247 indicated their race, 271 indicated their age, 235 indicated their insurance status, and 175 indicated their concerns which they hoped to have addressed in services. Of these patients, 66% endorsed white race, 30% endorsed Black race, and 2% endorsed Asian race (Table 1). 47% were enrolled in public insurance (2% were uninsured), and the mean age was 29.9 years (SD=5.5 years).
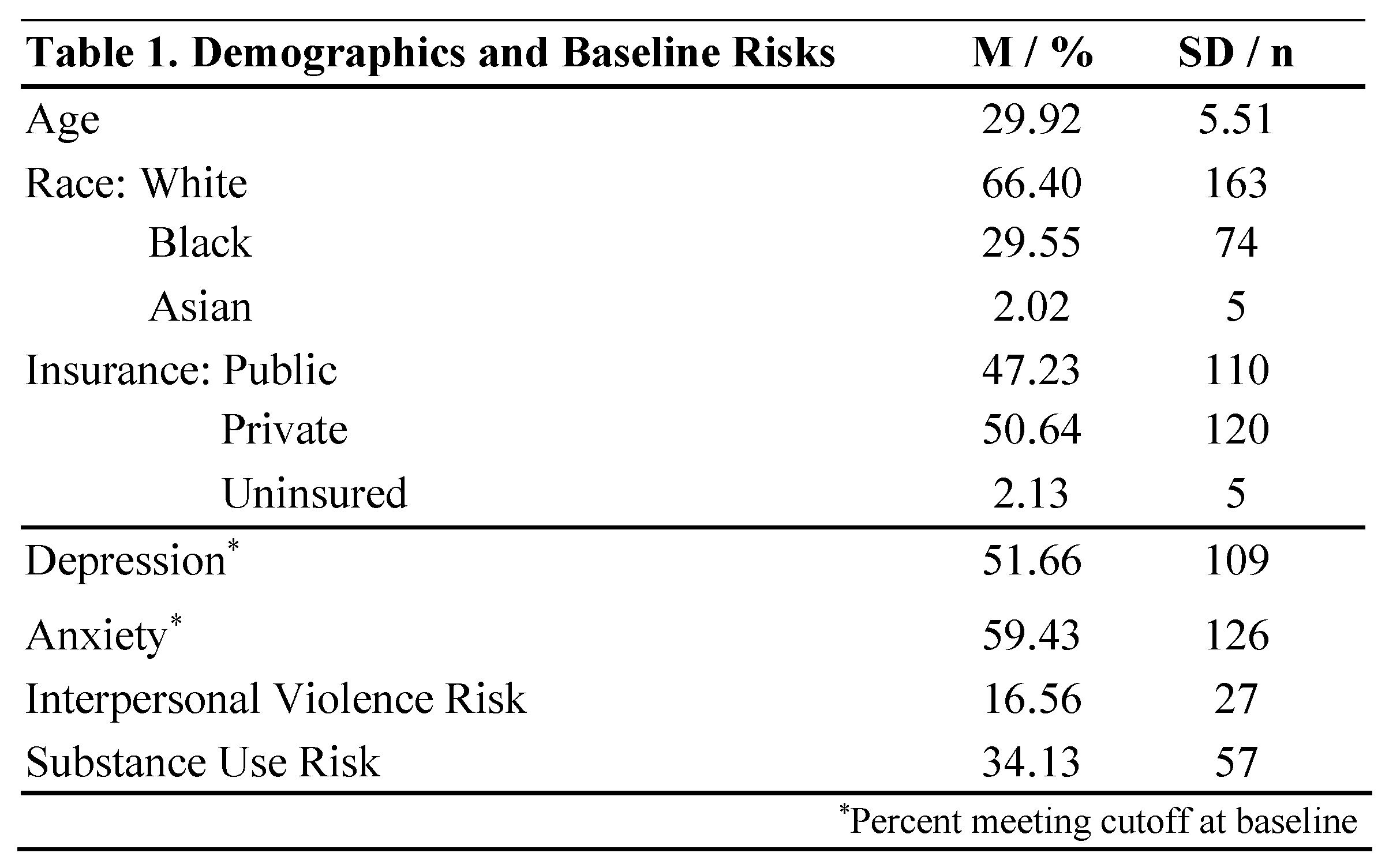
At referral, 175 patients expressed the priority issues they wanted to address in services. A majority were seeking clinical support for anxiety (65%) and depression (51%), followed closely by general and parenting stress (43%). Other concerns included breastfeeding, high risk pregnancy or miscarriage, Post-traumatic Stress Disorder (PTSD), trauma, panic attacks, parenting and general life support and resources, medication management, and mood challenges.
3.1.2. Outreach and Treatment Sessions
Of 285 referred patients, we have BHC outreach data on 284. Table 2 describes the outreach by clinicians to enroll patients. Of the 285 referred, a total of 209 patients enrolled in the treatment sessions (72%). Enrolled patients received 1 to 25 sessions, with an average of 6.6 (SD=4.5) sessions. Clinicians conducted 1,386 sessions for a total of 845 hours in session with an average of 4.9 (SD=3.9) hours in session per patient.
3.1.3. Patient Satisfaction
Overall, satisfaction with the MC3 Perinatal Care service was high, with 97% of individuals asserting they were satisfied with the services they received (See Table 3). The aggregate results from open-ended questions (not shown in table) suggested the most useful parts of the program were the support or therapy they received (endorsed by 71% of patients), along with the resources provided - including medication management (46%). Also noted as useful parts of the program were care coordination (13%) and flexibility of the BHCs and zero program costs (21%). When asked what their least favorite parts of the program were, most patients (86%) indicated they found it all useful, while some indicated difficulty finding referrals to outside services (9%) and that there were not enough visits with BHCs (5%). When asked what they would change to make the program better, most patients indicated they were satisfied with the program as it is (73%), with some indicating they would like the program to be more well known by the public (7%) and the ability to include spouses in the services (7%).

3.1.4. Retention in Treatment
For the 209 enrolled patients, we examined predictors of remaining in treatment, including race, type of insurance (as a proxy for socioeconomic status), IPV risk, and substance use risk. We tested these predictors using Cox regression, and report hazard ratios (HR). Black race (HR = 2.42, p=.007) and public insurance (HR = 2.54, p = .007) predicted faster attrition from treatment; IPV risk (HR=0.58, p = .46) and substance use risk (HR= 1.40, p = .44) were not related to attrition rate. Figure 3 shows plots of survival to termination of treatment separated by a) race and b) type of insurance. Those who endorsed white as race were more likely to remain in treatment longer (Fig. 3a). From the beginning of treatment, there was less attrition in the white group, and the differences increased over time. At six months following baseline, 77% of those who endorsed white were still engaged in treatment, whereas only 56% of those who did not endorse white were still engaged. Similarly, those who reported having public insurance or no insurance were likely to leave treatment before those who reported having private insurance (Fig. 3b). These differences are substantial early in treatment. By one month post-baseline, 94% of those with private insurance remained in treatment whereas only 79% of those with public insurance remained.
3.2. Mental Health Outcomes
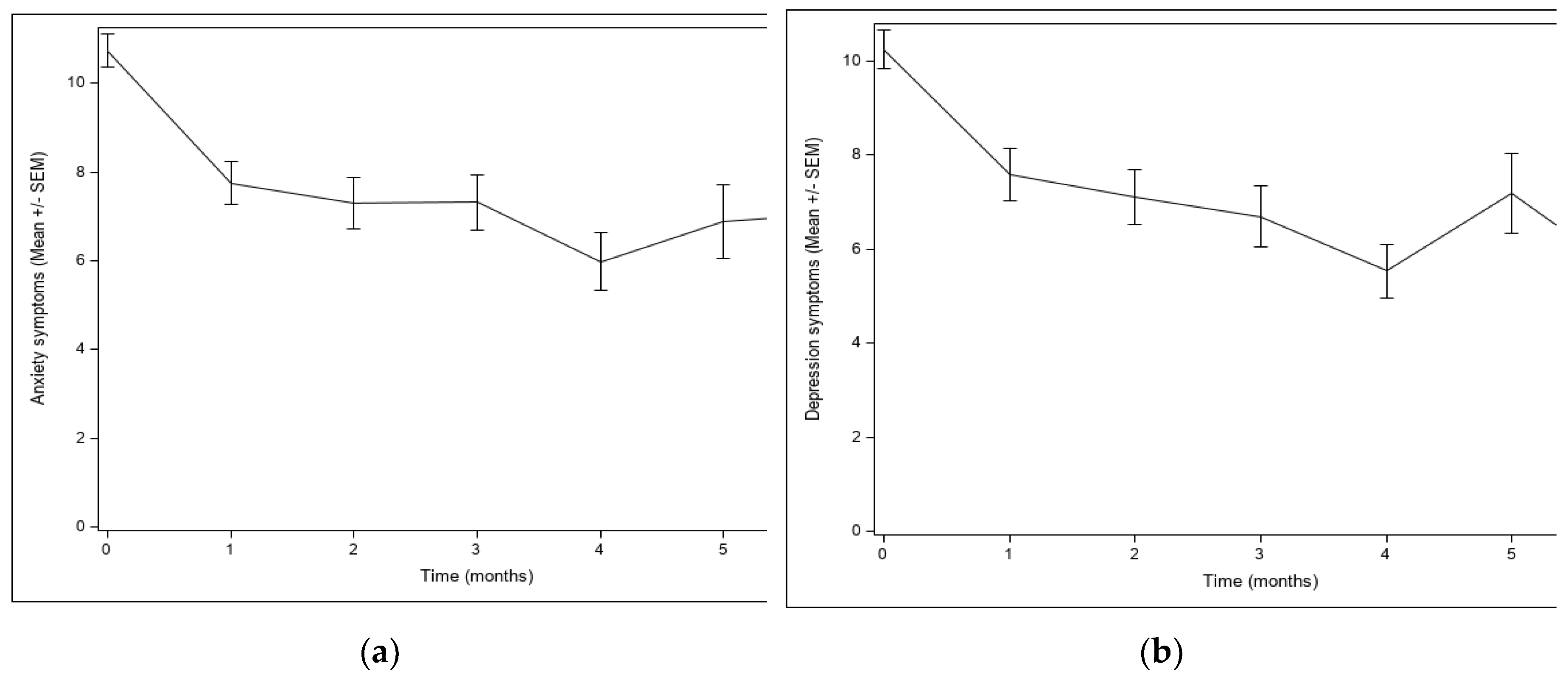
Trajectories of anxiety and depression symptoms were modeled for the 209 enrolled participants using latent growth modeling . For anxiety and depression symptoms separately, we fit models forthe baseline and each of the first six months of follow-up assessments, for which there was sufficient data to avoid convergence problems in estimation. For both anxiety and depression symptoms, cubic models had better fit than linear or quadratic models. As seen in Figure 4, means levels of symptoms for both anxiety (Fig. 4a) and depression symptoms (Fig. 4b) decreased over time The most dramatic decreases were in the first month, when most of the treatment occurred. Modeling showed significant decreases in anxiety from baseline to month 1 (delta=2.36, Wald test=46.96, p <.0001), as well as from month 1 to month 6 (delta= 1.96, Wald test = 7.94, p = .0048) and in depression from baseline to month 1 (delta = 2.30, Wald test = 53.42, p < .0001) and from month 1 to month 6 (delta = 1.94, Wald test = 14.46, p = .0001).
4. Discussion
Mental health disorders affect pregnant people at increased rates during the perinatal period. Geographic, financial, and social barriers persist in identification and access to care that preclude adequate diagnosis and treatment of anxiety and mood disorders. The COVID-19 pandemic has precipitated a synergistic effect in worsening these challenges, particularly for Black and Indigenous People and People of Color (BIPOC) who already experienced increased risk for adverse mental health outcomes and faced structural barriers to accessing perinatal mental health care. The literature shows that integrated care models within obstetric care can improve mental health outcomes for the parent-child dyad and can reduce annual healthcare costs. In this manuscript, we presented a novel perinatal mental health integrated care model, MC3 Perinatal, which combines instant access to remote psychotherapy for perinatal patients (“care” arm) with same-day provider consultation on medication questions (“consultation” arm). We present implementation data for the care arm, including patient demographics, program features, patient satisfaction, retention, and mental health outcomes.
The preliminary results presented in this manuscript demonstrate that MC3’s perinatal patient-facing “care” arm services are needed. Of 285 referred patients in the past 18 months since the pilot began, we connected with 259 patients (91% of those referred) and enrolled into services 209 (72% of those referred). This rate of engagement is higher than some similar studies, such as one 2014 study that reported a 56% enrollment rate in a CBT program for perinatal depression [40]. However, a 2014 Australian study of the implementation of a dedicated perinatal and infant mental health service found 71% engagement in at-risk perinatal patients [41]. This, combined with our finding of 72% engagement, suggests the special utility of perinatal mental health care in this particular population.
97% of enrolled individuals asserted they were satisfied with the services they received. CoCM generally garners high patient satisfaction across specialties, including both patient-reported and provider-perceived satisfaction [42]. A meta-analysis of 167 studies of integrated care found strong evidence for the relationship between integrated care and high patient satisfaction, and a 2022 study of CoCM for low-income racial-ethnic minority groups found similarly high (74%) patient-reported satisfaction [43,44]. MOMCare, a CoCM intervention for at-risk perinatal populations, found rates of self-reported patient satisfaction ranged from 62% at 18-months to 71% at 3 months [45]. Integrated care, specifically CoCM, is a model of care that is generally well-liked by both patients and providers – a sentiment corroborated by our findings as well.
Our outreach data indicates we successfully reached individuals across the spectrum of race, socioeconomic status, and mental health conditions - including a relatively even split of depression and anxiety, as well as representation of other risk factors, such as IPV (16% of patients) and substance use (34%), and public insurance or uninsured status (~50%). However, we also found that despite our ability to initially engage vulnerable groups including BIPOC, we were less successful in retention of these populations. Black race and public insurance predicted faster attrition from treatment. Non-white patients in general were less engaged with care at six months than white patients, at 56% of non-white patients versus 77% of white patients. This finding is commensurate with national data and speaks to the challenges that Black patients may face in staying in mental health care [46,47]. The existing literature cites potential barriers for Black patients in access to mental health care on multiple levels of society. Such barriers include broader systemic factors (wait times, lack of access to childcare or transportation, geographical challenges, financial barriers, etc.), practitioner-specific factors (racism and discrimination from staff, paucity of non-white or Black providers, inability to offer culturally competent care, etc.), and personal or community-related factors (internalized stigma, cumulative trauma, sociocultural expectations, etc.) [48-50]. One 2020 study noted support from family and friends and a good relationship with providers as facilitators to follow-through with care [51]. A 2021 study identified a significant increase in utilization of urgent telemedicine mental health care among Black patients, suggesting that Black patients may be more comfortable accessing this type of mental health care [52]. Because the patient facing MC3 Perinatal care arm is centered around telehealth counseling, it is likely that this fact positively influenced initial engagement with the service. It is important to note, that, for BIPOC communities, pregnancy, birth, and the postpartum period are journeys of life with deep spiritual, mental, and emotional connotations [53]. Care that focuses solely on the individual and excludes their families and communities may not be the most optimal way to sustainably engage BIPOC patients [53]. This sentiment is possibly supported by our finding that 7% of MC3 patients commented on their desire to include spouses in services. Our program did not achieve sustained engagement, and future work will need to focus on better understanding how to keep engagement over time and prevent premature attrition.
Historically, SUD and IPV are predictors of poor retention in mental health programming, particularly when combined with underlying severe psychopathology – such as severe perinatal anxiety [54-60]. In our study, because IPV and substance use risk did not predict attrition from the program, this highlights the importance of accessible, patient-facing mental healthcare for these particularly vulnerable patient populations. This type of integrated care is doubly important for these patients, as studies have established a significant link between experiencing domestic violence and high-level symptoms of perinatal depression, anxiety, and PTSD [57-59,61]. In addition, IPV is a risk factor for catastrophic consequences - including suicide of perinatal mothers, as discovered by the US National Violent Death Reporting System, which found IPV in nearly half of mothers who died by suicide [62]. Substance use is also a factor in perinatal death, as noted in a 2020 study that established a link between perinatal death, substance use, and poor mental health care [62]. Critically, a 2021 article commented on the importance of initial identification of these risk factors, as providers cannot assist patients if they are not aware of their histories [63]. This emphasizes the importance of open communication between OB/GYN providers and perinatal mental health care clinicians, both in order to identify overall risk and to offer tailored resources and interventions to mitigate catastrophic negative outcomes.
Finally, our mental health data show significant decreases in anxiety and depression over time, with the most dramatic decreases in the first month of treatment, supporting the benefit of the care component to patient wellbeing across the perinatal period. Patient satisfaction was also high, with 97% of individuals reporting that they were satisfied with the services they received. Patients felt that the most useful parts of the program were the support or therapy they received (endorsed by 71% of patients), in addition to the resources provided - including medication management (46%). Also noted as useful parts of the program were care coordination and flexibility of the clinicians and program costs. Most patients (86%) indicated they found all services useful, an encouraging finding. Improvement suggestions seemed to be relatively easy to incorporate, including ideas such as improved referrals to outside services, increased visit numbers with clinicians, increased public knowledge of the program, and the ability to include spouses in the services. When asked what they would change to make the program better, most patients indicated they were satisfied with the program as it is (73%).
The encouraging outcomes described in this paper highlight the benefit of MC3 Perinatal in vulnerable populations - in this case, persons with a history of IPV and substance abuse - and the progress MC3 Perinatal makes toward the ultimate goal of equitable, accessible care. We are attempting to address attrition from the program by continuing to follow up with patients. We have recently implemented an extended outreach protocol that stipulates contact for up to one year - or if the patient indicates they are no longer interested in services.
This study is not without limitations. We lack a comparison group of perinatal women against whom to objectively evaluate the efficacy of the program. This was not done because of the challenges presented in obtaining comparison data on a matched group of perinatal patients in counties not yet included in this program. We only presented data on a small pilot sample, especially in regard to follow up data on depression and anxiety across the postpartum period, as the program is relatively new and has been in existence since 2021. However, enrollment is rising, and data collection is ongoing, which will strengthen confidence in our promising findings.
5. Conclusions
The MC3 Perinatal care program is a viable, patient-endorsed collaborative model of care that increases equitable access to perinatal mental health and facilitates access to outside resources. MC3 Perinatal steps beyond traditional case management and connection to resources as more typical for the CoCM, but also offers short-term evidence-based psychotherapy and yearlong monitoring of symptoms beyond the active therapy episode. In such MC3 Perinatal care provides holistic and ongoing care that is specifically tailored to perinatal patients’ needs. The BHCs receive ongoing training and consultation to provide evidence-based services specific to the population. Finally, the model is delivered remotely and based on the modality and frequency that is desired and accepted by the patient, which increases access and acceptance for the service. This integrated, technology-assisted program addresses the complexity of treatment access and acceptance for vulnerable patients and allows needs identification within the context of a behavioral health and medical team, while also providing immediate, direct source of supports.
Author Contributions
Conceptualization, Maria Muzik; methodology, Maria Muzik, Rena A. Menke, Meriam Issa; formal analysis, Meriam Issa, Jordan Charles, Jennifer Jester; investigation, Maria Muzik, Rena A. Menke, Meriam Issa, and Jordan Charles; resources, Maria Muzik; data curation, Meriam Issa, Jordan Charles and Jennifer Jester; writing—original draft preparation, Maria Muzik, Rena A. Menke, Meriam Issa, Chelsea Fisk, Jordan Charles, Jennifer Jester; writing—review and editing, Maria Muzik and Chelsea Fisk; validation, Meriam Issa, Jordan Charles and Jennifer Jester; visualization, Meriam Issa; supervision, Maria Muzik; project administration, Meriam Issa and Rena Menke; funding acquisition, Maria Muzik. All authors have read and agreed to the published version of the manuscript.” Please turn to the CRediT taxonomy for the term explanation. Authorship must be limited to those who have contributed substantially to the work reported.
Funding
This research was funded by the Center of Medicare and Medicaid Services through the Michigan Department of Health and Human Services., grant number MDHHS E20234275-00 and E20234297-00 (PI Muzik).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of University of Michigan as non-regulated/exempt study ((HUM00194265 on 2/4/2021).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data available on request due to restrictions (privacy & ethical). Deidentified data presented in this study are available on request from the corresponding author. The data are not publicly available due to clinical privacy restrictions.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Byatt, N.; Masters, G.A.; Bergman, A.L.; Simas, T.A.M. Screening for Mental Health and Substance Use Disorders in Obstetric Settings. Curr. Psychiatry Rep. 2020, 22, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Postpartum Support International. Depression During Pregnancy & Postpartum. Available online: https://www.postpartum.net/learn-more/depression/ (accessed on 20 August 2021).
- Howard, L.M.; Khalifeh, H. Perinatal mental health: A review of progress and challenges. World Psychiatry 2020, 19, 313–327. [Google Scholar] [CrossRef] [PubMed]
- Brown, C.C.; Adams, C.E.; George, K.E.; Moore, J.E. Mental Health Conditions Increase Severe Maternal Morbidity By 50 Percent And Cost $102 Million Yearly In The United States: Study estimates hospitalization cost, length of stay, and severe maternal morbidity associated with perinatal mental health disorders. Health Aff. 2021, 40, 1575–1584. [Google Scholar]
- Wisner, K.L.; Sit, D.K.Y.; McShea, M.C.; Rizzo, D.M.; Zoretich, R.A.; Hughes, C.L.; Eng, H.F.; Luther, J.F.; Wisniewski, S.R.; Costantino, M.L.; et al. Onset Timing, Thoughts of Self-harm, and Diagnoses in Postpartum Women With Screen-Positive Depression Findings. JAMA Psychiatry 2013, 70, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Admon, L.K.; Dalton, V.K.; Kolenic, G.E.; Ettner, S.L.; Tilea, A.; Haffajee, R.L.; Brownlee, R.M.; Zochowski, M.K.; Tabb, K.M.; Muzik, M.; et al. Trends in Suicidality 1 Year Before and After Birth Among Commercially Insured Childbearing Individuals in the United States, 2006-2017. JAMA Psychiatry 2021, 78, 171–176. [Google Scholar] [CrossRef] [PubMed]
- Wallace, K.; Araji, S.; Griffin, A.; Dixon, L.; Spencer, S.-K.; Peavie, C. An Overview of Maternal Anxiety During Pregnancy and the Post-Partum Period. J. Ment. Health Clin. Psychol. 2020, 4, 47–56. [Google Scholar] [CrossRef]
- Kimmel, M. Maternal Mental Health MATTERS. North Carol. Med, J. 2020, 81, 45–50. [Google Scholar] [CrossRef]
- Cox, E.Q.; Sowa, N.A.; Meltzer-Brody, S.E.; Gaynes, B.N. The Perinatal Depression Treatment Cascade. J. Clin. Psychiatry 2016, 77, 1189–1200. [Google Scholar] [CrossRef]
- Martinez-Torteya, C.; Katsonga-Phiri, T.; Rosenblum, K.L.; Hamilton, L.; Muzik, M. Postpartum depression and resilience predict parenting sense of competence in women with childhood maltreatment history. Arch. Women's Ment. Health 2018, 21, 777–784. [Google Scholar] [CrossRef]
- McGinnis, R.S.; McGinnis, E.W.; Hruschak, J.; Lopez-Duran, N.L.; Fitzgerald, K.; Rosenblum, K.L.; Muzik, M. Rapid detection of internalizing diagnosis in young children enabled by wearable sensors and machine learning. PLoS ONE 2019, 14, e0210267. [Google Scholar] [CrossRef]
- McGinnis, E.W.; Anderau, S.P.; Hruschak, J.; Gurchiek, R.D.; Lopez-Duran, N.L.; Fitzgerald, K.; Rosenblum, K.L.; Muzik, M.; McGinnis, R.S. Giving Voice to Vulnerable Children: Machine Learning Analysis of Speech Detects Anxiety and Depression in Early Childhood. IEEE J. Biomed. Health Inform. 2019, 23, 2294–2301. [Google Scholar] [CrossRef] [PubMed]
- Lebel, C.; MacKinnon, A.; Bagshawe, M.; Tomfohr-Madsen, L.; Giesbrecht, G. Elevated depression and anxiety symptoms among pregnant individuals during the COVID-19 pandemic. J. Affect. Disord. 2020, 277, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Motrico, E.; Bina, R.; Domínguez-Salas, S.; Mateus, V.; Contreras-García, Y.; Carrasco-Portiño, M.; Ajaz, E.; Apter, G.; Christoforou, A.; Dikmen-Yildiz, P.; et al. Impact of the Covid-19 pandemic on perinatal mental health (Riseup-PPD-COVID-19): Protocol for an international prospective cohort study. BMC Public Health 2021, 21, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Avena, N.M.; Simkus, J.; Lewandowski, A.; Gold, M.S.; Potenza, M.N. Substance Use Disorders and Behavioral Addictions During the COVID-19 Pandemic and COVID-19-Related Restrictions. Front. Psychiatry 2021, 12, 653674. [Google Scholar] [CrossRef] [PubMed]
- Su, Z.; McDonnell, D.; Roth, S.; Li, Q.; Šegalo, S.; Shi, F.; Wagers, S. Mental health solutions for domestic violence victims amid COVID-19: A review of the literature. Glob. Health 2021, 17, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Howard, L.M.; Wilson, C.A.; Chandra, P.S. Intimate partner violence and mental health: Lessons from the COVID -19 pandemic. World Psychiatry 2022, 21, 311–313. [Google Scholar] [CrossRef] [PubMed]
- Byatt, N.; , Yonkers, KA. Addressing Maternal Mental Health: Progress, Challenges, and Potential Solutions. Psychiatric News. (2021). Available online: https://psychnews.psychiatryonline.org/doi/full/10.1176/appi.pn.2021.4.7 (accessed on 15 July 2021).
- Osterman, M.J.K.; A. Martin, J. Timing and Adequacy of Prenatal Care in the United States 2016. Natl Vital Stat Rep 2018, 67, 1–14. Available online: https://www.cdc.gov/nchs/data/nvsr/nvsr67/nvsr67_03.pdf (accessed on 15 July 2021). [PubMed]
- Mehralizade, A.; Schor, S.; Coleman, C.M.; E. Oppenheim, C.; A Denckla, C.; Borba, C.P.; Henderson, D.C.; Wolff, J.; Crane, S.; Nettles-Gomez, P.; et al. Mobile Health Apps in OB-GYN-Embedded Psychiatric Care: Commentary. JMIR mHealth uHealth 2017, 5, e152–e152. [Google Scholar] [CrossRef]
- Melville, J.L.; Reed, S.D.; Russo, J.; Croicu, C.A.; Ludman, E.; LaRocco-Cockburn, A.; Katon, W. Improving Care for Depression in Obstetrics and Gynecology. Obstet. Gynecol. 2014, 123, 1237–1246. [Google Scholar] [CrossRef]
- National Alliance on Mental Health. The Doctor is Out. Available online: https://www.nami.org/Support-Education/Publications-Reports/Public-Policy-Reports/The-Doctor-is-Out (accessed on 15 July 2021).
- Byatt, N.D.; Straus, J.; Stopa, A.B.; Biebel, K.; Mittal, L.; Simas, T.A.M. Massachusetts Child Psychiatry Access Program for Moms. Obstet. Gynecol. 2018, 132, 345–353. [Google Scholar] [CrossRef]
- University of Washington. MOMCare. Available online: http://depts.washington.edu/momcare/ (accessed on 25 September 2021).
- AIMS Center Advancing Integrated Mental Health Solutions. Collaborative Care for High Risk Mothers. Available online: https://aims.uw.edu/collaborative-care-high-risk-mothers (accessed on 25 September 2021).
- The Maternal-Infant Dyad Implementation (MIND-I) Initiative. Available online: https://aims.uw.edu/maternal-infant-dyad-implementation-mind-i-initiative (accessed on 20 March 2023).
- Marcus, S.; Malas, N.; Dopp, R.; Quigley, J.; Kramer, A.C.; Tengelitsch, E.; Patel, P.D. The Michigan Child Collaborative Care Program: Building a Telepsychiatry Consultation Service. Psychiatr. Serv. 2019, 70, 849–852. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, P.; Panday, R. Psychoeducation an Effective Tool as Treatment Modality in Mental Health. Int. J. Indian Psychol. 2016, 4. [Google Scholar] [CrossRef]
- Sarkhel, S.; Singh, O.; Arora, M. Clinical Practice Guidelines for Psychoeducation in Psychiatric Disorders General Principles of Psychoeducation. Indian J. Psychiatry 2020, 62, 319–8323. [Google Scholar] [CrossRef] [PubMed]
- O'Neill, L.; Latchford, G.; McCracken, L.; Graham, C. (2019). The Acceptance and Commitment Therapy Fidelity Measure (ACT-FM). Form 2019. [Google Scholar] [CrossRef]
- Alexander, R.A.; Goldstein, E. Mindfulness, Trauma, and Trance: A Mindfulness-Based Psychotherapeutic Approach. The Wiley Blackwell Handbook of Mindfulness.
- Pollak, S.M.; Pollak, S.; Pedulla, T.; Siegel, R.D. Sitting together: Essential skills for mindfulness-based psychotherapy. Guilford Publications. 2014.
- Pinheiro, R.T.; Trettim, J.P.; de Matos, M.B.; Pinheiro, K.A.T.; da Silva, R.A.; Martins, C.R.; da Cunha, G.K.; Coelho, F.T.; Motta, J.V.d.S.; Coelho, F.M.d.C.; et al. Brief cognitive behavioral therapy in pregnant women at risk of postpartum depression: Pre-post therapy study in a city in southern Brazil. J. Affect. Disord. 2021, 290, 15–22. [Google Scholar] [CrossRef]
- Attkisson, C.; Zwick, R. The client satisfaction questionnaire: Psychometric properties and correlations with service utilization and psychotherapy outcome. Evaluation Program Plan. 1982, 5, 233–237. [Google Scholar] [CrossRef]
- Watson, E. The evolution and application of the 5 P’S behavioral risk screening tool. Source 2010, 20, 27–29. [Google Scholar]
- Spitzer, R.L.; Kroenke, K.; Williams, J.B.; Löwe, B. A brief measure for assessing generalized anxiety disorder: The GAD-7. Arch. Intern. Med. 2006, 166, 1092–1097. [Google Scholar] [CrossRef]
- Zhong, Q.-Y.; Gelaye, B.; Zaslavsky, A.M.; Fann, J.R.; Rondon, M.B.; Sánchez, S.E.; Williams, M.A. Diagnostic Validity of the Generalized Anxiety Disorder - 7 (GAD-7) among Pregnant Women. PLoS ONE 2015, 10, e0125096. [Google Scholar] [CrossRef]
- Kroenke, K.; Spitzer, R.L.; Williams, J.B. The PHQ-9: Validity of a brief depression severity measure. J. Gen. Intern. Med. 2001, 16, 606–613. [Google Scholar] [CrossRef] [PubMed]
- O’Connor, E.; Rossom, R.C.; Henninger, M.; Groom, H.C.; Burda, B.U. (Primary care screening for and treatment of depression in pregnant and postpartum women: Evidence report and systematic review for the US Preventive Services Task Force. JAMA 2016, 315, 388–406. [Google Scholar] [CrossRef] [PubMed]
- Dimidjian, S.; Goodman, S.H.; Felder, J.N.; Gallop, R.; Brown, A.P.; Beck, A. An open trial of mindfulness-based cognitive therapy for the prevention of perinatal depressive relapse/recurrence. Arch. Women's Ment. Health 2014, 18, 85–94. [Google Scholar] [CrossRef]
- Myors, K.A.; Johnson, M.; Cleary, M.; Schmied, V. Engaging women at risk for poor perinatal mental health outcomes: A mixed-methods study. Int. J. Ment. Health Nurs. 2014, 24, 241–252. [Google Scholar] [CrossRef] [PubMed]
- Cheng, A.L.; Snider, E.M.; Prather, H.; Dougherty, N.L.; Wilcher-Roberts, M.; Hunt, D.M. Provider-Perceived Value of Interprofessional Team Meetings as a Core Element of a Lifestyle Medicine Program: A Mixed-Methods Analysis of One Center’s Experience. Am. J. Lifestyle Med. 2022. [Google Scholar] [CrossRef]
- Baxter, S.; Johnson, M.; Chambers, D.; Sutton, A.; Goyder, E.; Booth, A. The effects of integrated care: A systematic review of UK and international evidence. BMC Health Serv. Res. 2018, 18, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Blackmore, M.A.; Patel, U.B.; Stein, D.; Carleton, K.E.; Ricketts, S.M.; Ansari, A.M.; Chung, H. Collaborative Care for Low-Income Patients From Racial-Ethnic Minority Groups in Primary Care: Engagement and Clinical Outcomes. Psychiatr. Serv. 2022, 73, 842–848. [Google Scholar] [CrossRef] [PubMed]
- Grote, N.K.; Katon, W.J.; Russo, J.E.; Lohr, M.J.; Curran, M.; Galvin, E.; Carson, K. COLLABORATIVE CARE FOR PERINATAL DEPRESSION IN SOCIOECONOMICALLY DISADVANTAGED WOMEN: A RANDOMIZED TRIAL. Depression Anxiety 2015, 32, 821–834. [Google Scholar] [CrossRef]
- Black, D.S.; Amaro, H. Moment-by-Moment in Women's Recovery (MMWR): Mindfulness-based intervention effects on residential substance use disorder treatment retention in a randomized controlled trial. Behav. Res. Ther. 2019, 120, 103437. [Google Scholar] [CrossRef]
- McClendon, J.; Dean, K.E.; Galovski, T. Addressing Diversity in PTSD Treatment: Disparities in Treatment Engagement and Outcome Among Patients of Color. Curr. Treat. Options Psychiatry 2020, 7, 275–290. [Google Scholar] [CrossRef]
- Alang, S.M. Mental health care among blacks in America: Confronting racism and constructing solutions. Health Serv. Res. 2019, 54, 346–355. [Google Scholar] [CrossRef] [PubMed]
- Nazroo, J.Y.; Bhui, K.S.; Rhodes, J. Where next for understanding race/ethnic inequalities in severe mental illness? Structural, interpersonal and institutional racism. Sociol. Health Illn. 2019, 42, 262–276. [Google Scholar] [CrossRef] [PubMed]
- Taylor, R.E.; Kuo, B.C.H. Black American psychological help-seeking intention: An integrated literature review with recommendations for clinical practice. J. Psychother. Integr. 2019, 29, 325–337. [Google Scholar] [CrossRef]
- Fante-Coleman, T.; Jackson-Best, F. Barriers and Facilitators to Accessing Mental Healthcare in Canada for Black Youth: A Scoping Review. Adolesc. Res. Rev. 2020, 5, 115–136. [Google Scholar] [CrossRef]
- Chunara, R.; Zhao, Y.; Chen, J.; Lawrence, K.; A Testa, P.; Nov, O.; Mann, D.M. Telemedicine and healthcare disparities: A cohort study in a large healthcare system in New York City during COVID-19. J. Am. Med Informatics Assoc. 2020, 28, 33–41. [Google Scholar] [CrossRef] [PubMed]
- Foster, V.A.; Harrison, J.M.; Williams, C.R.; Asiodu, I.V.; Ayala, S.; Getrouw-Moore, J.; Mask Jackson, F. Reimagining Perinatal Mental Health: An Expansive Vision For Structural Change: Commentary describes changes needed to improve perinatal mental health care. Health Aff. 2021, 40, 1592–1596. [Google Scholar] [CrossRef]
- Amaro, H.; Chernoff, M.; Brown, V.; Arévalo, S.; Gatz, M. Does integrated trauma-informed substance abuse treatment increase treatment retention? J. Community Psychol. 2007, 35, 845–862. [Google Scholar] [CrossRef]
- Ganetsky, V.S.P.; Heil, J.M.; Yates, B.; Jones, I.L.; Hunter, K.M.; Rivera, B.M.; Wilson, L.L.; Salzman, M.; Baston, K.E.M. A Low-threshold Comprehensive Shared Medical Appointment Program for Perinatal Substance Use in an Underserved Population. J. Addict. Med. 2021, 16, e203–e209. [Google Scholar] [CrossRef]
- Galvin, S.L.; Ramage, M.; Mazure, E.; Coulson, C.C. The association of cannabis use late in pregnancy with engagement and retention in perinatal substance use disorder care for opioid use disorder: A cohort comparison. J. Subst. Abus. Treat. 2020, 117, 108098. [Google Scholar] [CrossRef]
- Dichter, M.E.; Sorrentino, A.E.; Haywood, T.N.; Tuepker, A.; Newell, S.; Cusack, M.; True, G. Women's participation in research on intimate partner violence: Findings on recruitment, retention, and Participants' experiences. Women's Health Issues 2019, 29, 440–446. [Google Scholar] [CrossRef]
- Gilroy, H.; McFarlane, J.; Maddoux, J.; Sullivan, C. Homelessness, housing instability, intimate partner violence, mental health, and functioning: A multi-year cohort study of IPV survivors and their children. J. Soc. Distress Homeless 2016, 25, 86–94. [Google Scholar] [CrossRef]
- Hodges, M.; Chambers, J.E.; Denne, S.; Wiehe, S.E.; Tang, Q.; Park, S.; Litzelman, D. Associations of Mental Health Measures and Retention in a Community-Based Perinatal Care Recovery Support Program for Women of Childbearing Age With Substance Use Disorder. J. Dual Diagn. 2022, 18, 211–219. [Google Scholar] [CrossRef] [PubMed]
- Staudt, M. Best practices for enhancing substance abuse treatment retention by pregnant women. Best Pract. Ment. Health 2018, 14, 48–63. [Google Scholar]
- Howard, L.M.; Oram, S.; Galley, H.; Trevillion, K.; Feder, G. Domestic Violence and Perinatal Mental Disorders: A Systematic Review and Meta-Analysis. PLOS Med. 2013, 10, e1001452. [Google Scholar] [CrossRef]
- Howard, L.M.; Khalifeh, H. Perinatal mental health: A review of progress and challenges. World Psychiatry 2020, 19, 313–327. [Google Scholar] [CrossRef]
- Jasthi, D.L.; Nagle-Yang, S.; Frank, S.; Masotya, M.; Huth-Bocks, A. Associations Between Adverse Childhood Experiences and Prenatal Mental Health and Substance Use Among Urban, Low-Income Women. Community Ment. Health J. 2021, 58, 595–605. [Google Scholar] [CrossRef]
Figure 1.
Graphic depiction of the Michigan Clinical Consultation and Care in Perinatal (MC3 Perinatal) Model.
Figure 1.
Graphic depiction of the Michigan Clinical Consultation and Care in Perinatal (MC3 Perinatal) Model.
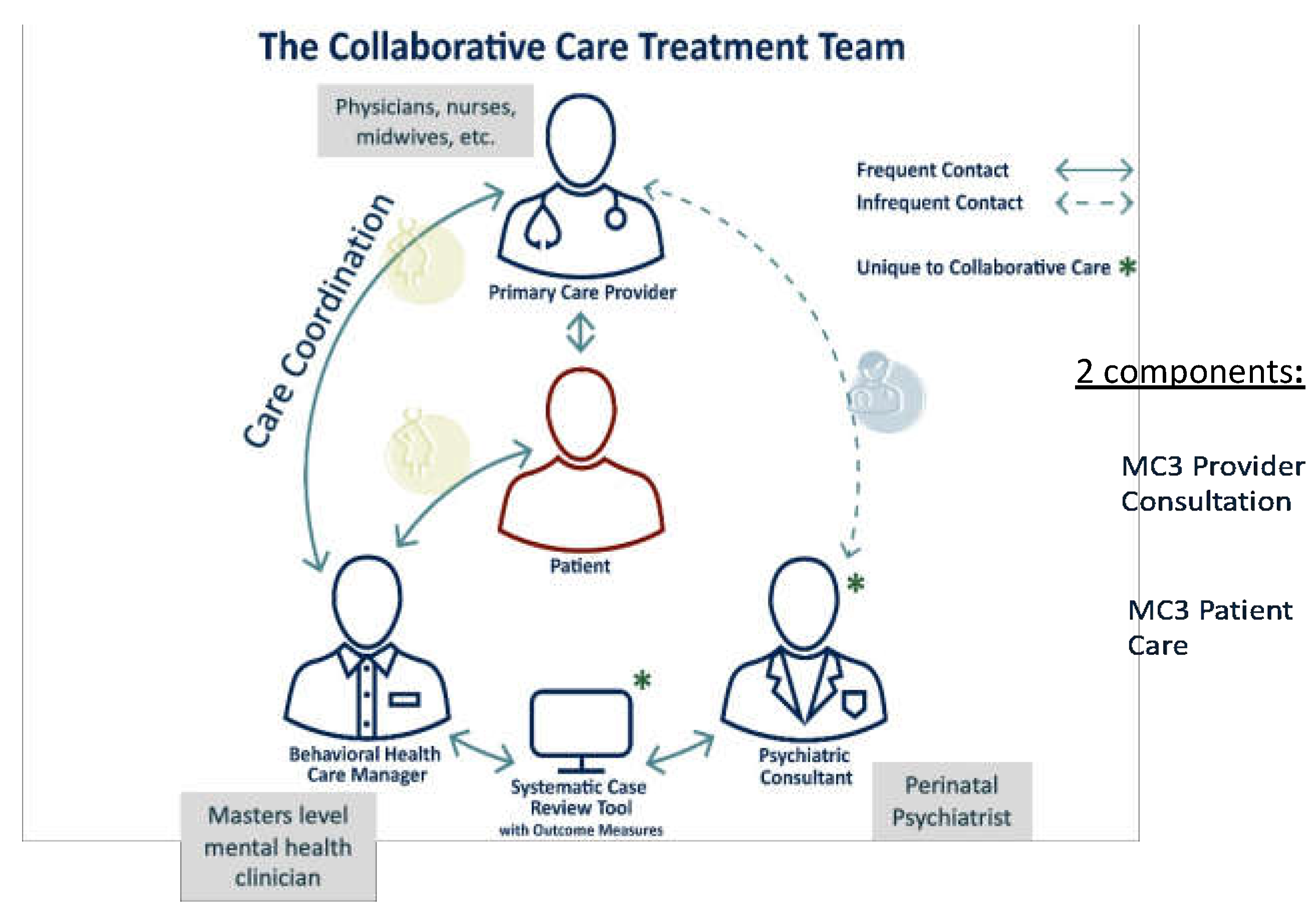
Figure 2.
Consort Diagram.

Figure 3.
Plots of survival to termination of treatment separated by (a) race; (b) type of insurance.
Figure 3.
Plots of survival to termination of treatment separated by (a) race; (b) type of insurance.

Figure 4.
Mental health symptoms over time: (a) Anxiety symptoms over time (mean and standard deviation); (b) Depression symptoms over time (mean and standard deviation).
Figure 4.
Mental health symptoms over time: (a) Anxiety symptoms over time (mean and standard deviation); (b) Depression symptoms over time (mean and standard deviation).
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



