
Submitted:
19 April 2023
Posted:
20 April 2023
You are already at the latest version
Abstract
Introduction: The concept of hypersexuality belongs to modern parlance, according to a predominantly clinical meaning, understood as a psychological and behavioural alteration as a result of which sexually motivated stimuli are sought in inappropriate ways, often experienced in a way that is not completely satisfactory. Methods: Literature up to February 2023 was reviewed. Results: Forty-two articles were included in the review. Conclusion: Hypersexuality is a potentially clinically relevant condition, consisting of one or more dysfunctional and pathological behaviours of one's sexual sphere and graded according to the severity of impairment of subjective acting out; for this reason, the Perrotta Hypersexuality Global Scale (PH-GS) is suggested, which distinguishes high-functioning forms (pro-active and dynamic hypersexuality) from those of attenuated and corrupted functioning (dysfunctional and pathological hypersexuality of grade I and II). Future research is hoped to address the practical needs of this condition, such as the exact etiopathology, the role of oxytocin in dopaminergic hypotheses (and its ability to attenuate the symptomatology suffered by the patient in terms of manic drive), the best structural and functional personality framing of the subject, and the appropriate therapy to pursue.
Keywords:
Hypersexuality
; Nymphomania
; Satyriasis
; Personality disorders
; Bipolarism
; Sexual arousal
1. Introduction
1.1. General and historical profiles
The concept of “hypersexuality” belongs to modern parlance, according to a predominantly clinical meaning, understood as a psychological and behavioural alteration as a result of which sexually motivated stimuli are sought in inappropriate ways, often experienced in a way that is not completely satisfactory; it is a psychopathological label strongly desired by the scientific community to replace terms previously used in other areas of study as well, such as nymphomania and satyriasis, the former referring to the female sexual gender and the latter to the male sexual gender. [1] Such terminologies draw on Greek mythological culture, referring to the nymphs who were young and beautiful maidens whose beauty attracted the desire of many men. It was they, in fact, according to mythological tradition, who first used the art of seduction to continually procure new sexual partners, and thus the satisfaction of their pleasures. However, the nymphs, like the sirens, hid a dark side: their company was as deadly as it was pleasurable. They often fell prey to the satyrs, bearded beings who were half-man, half-animal (goat or horse), and also devoted to lustful wildlife. The dances of the satyrs and nymphs are depicted in very famous works, which capture precisely the peculiarity and complementarity of their sexual behaviour. Nymphomania and satyriasis are, therefore, the female and male equivalent of today's hypersexuality, which, in the past, was considered a morbid accentuation of sexual impulses. In later centuries then, popular tradition extolled these aspects in many artistic representations, thus giving rise to myths and stories, widely using the terms now replaced with hypersexuality beginning in 1771 A.D. in the edited work "Nymphomania. Treatise on Uterine Fury" by French physician Giambatist De Bienville. [2]
1.2. Clinical profiles
Today, hypersexuality is proposed differently and with a predominantly clinical connotation; in fact, it is present in the two main diagnostic manuals of psychiatric problems: the International Classification of Diseases (ICD) [3] and the Diagnostic and Statistical Manual of Mental Disorders (DSM) [4]. The ICD is the international classification proposed by the World Health Organization; it is not specific to mental disorders alone, to which, however, a section is dedicated anyway, and it encapsulates the diagnostic criteria for all possible organic disorders. The DSM, on the other hand, is the proposal from the American Psychiatric Association group and, currently, the most widely used classification in the international scientific community, being then devoted entirely to psychopathologies. But if usually, the two classification systems are equivalent, in terms of formulation and representation, this is not true for several clinical hypotheses, including hypersexuality itself; this is an expression of a difficulty on the part of the expert editors to frame this particular clinical case in a structural and sharable way. Hypersexuality falls under "Sexual Compulsive Behavior Disorder" (code 6C72) for ICD-11, while for DSM-5 it is considered a behavioural addiction that can characterize the subject's pathological conduct and even be a dysfunctional trait in other disorders. The diagnostic criteria advanced by the World Health Organization on the subject of hypersexuality are: A) For at least six months, recurrent and intense sexual fantasies, sexual urges or sexual behaviour in association with 3 or more of the following: Time spent in repetitive sexual fantasies, impulses, or behaviours that interfere with other important (non-sexual) goals, activities, or obligations; Repetitive engagement in sexual fantasies, impulses, or behaviours in response to dysphoric mood states (e.g., anxiety, depression, boredom, or irritability); Repetitive engagement in sexual fantasies, impulses, or behaviours in response to stressful life events; Repetitive but unsuccessful efforts to control or significantly reduce such fantasies, impulses, or behaviours; Repetitive engagement in sexual behaviours, disregarding the risk of physical or emotional harm to self or others. B) There is clinically significant personal distress or impairment in the social, work, or other important areas associated with the frequency and intensity of these sexual fantasies, impulses, or behaviours. C) These sexual fantasies, impulses, or behaviours are not a direct result of medical conditions (e.g., brain tumours or dementia) or substance intake (e.g., a substance of abuse or medication). [3,5]
1.3. Aim
A review was conducted to determine as precisely as possible the exact aetiology of pathological hypersexuality, in its various meanings. The object of this discussion is to try to determine whether, in the current state of scientific knowledge, the following research questions can be answered:
- Is it possible to distinguish one or more forms of hypersexuality? And if so, is there a pathological form and how does it differ from the other hypotheses?
- Is it possible to say that pathological hypersexuality is a clinical condition, medically relevant, or is it a subjective maladaptive behaviour? And if it is a condition, is it primary or secondary?
- Is it possible to identify the aetiology of pathological hypersexuality with scientific certainty, thus in a reproducible and agreeable manner?
2. Materials and methods
2.1. Study Design
Literature up to February 2023 was reviewed.
2.2. Review Questions
To identify the important aspects of the examination, the writer focused on the elements that could determine whether or not pathological hypersexuality could be considered a nosographic category in its own right, or whether it could fall under obsessive-compulsive disorders or impulsive conduct disorders or among behavioural addictions, up to the hypothesis that interprets hypersexuality as one of the typical features of certain psychiatric disorders (e.g., bipolar, borderline personality disorder, and pathological narcissism).
2.3. Materials and methods
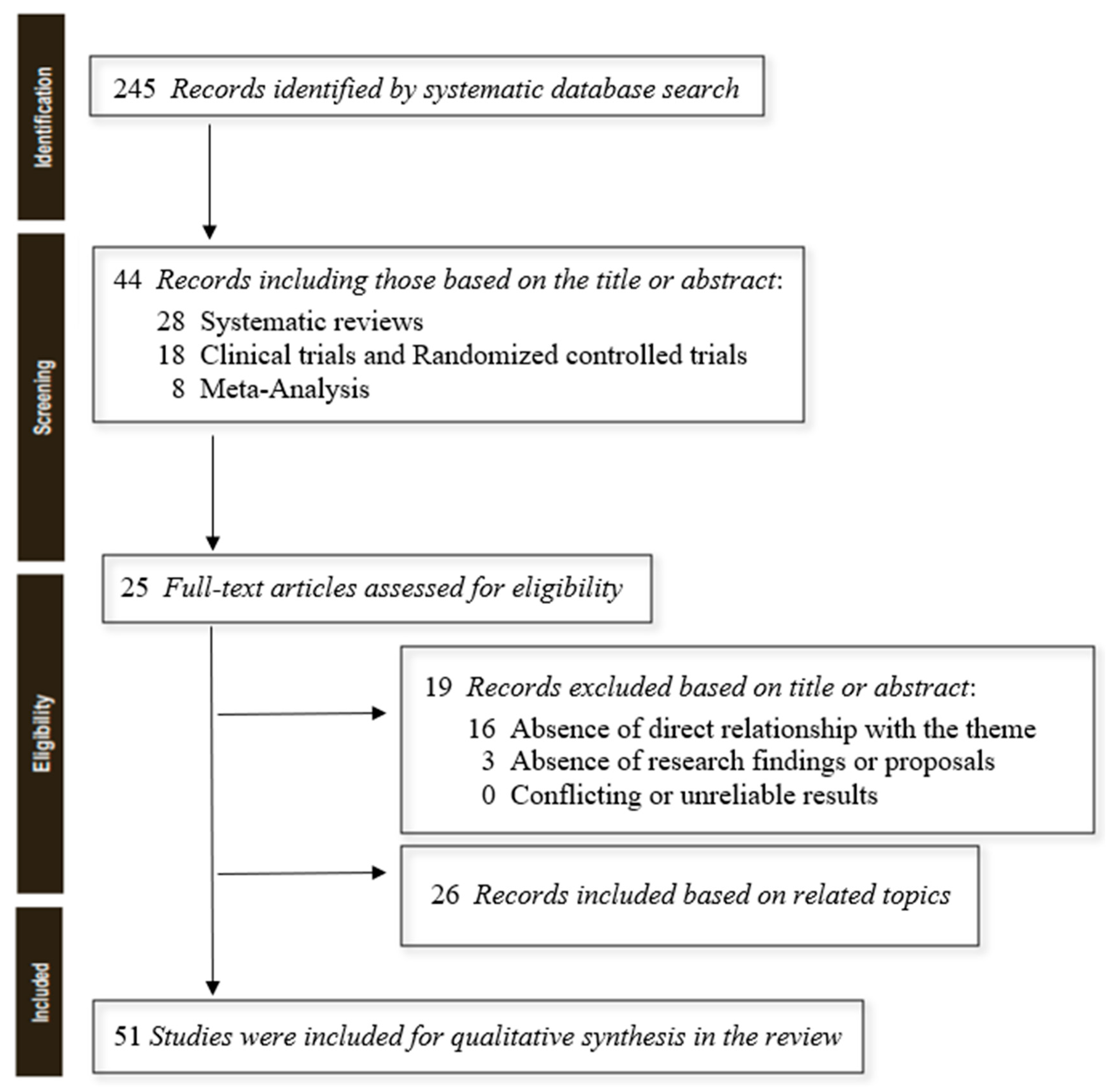
The author searched PubMed, until February 2023, systematic reviews, clinical trials and randomized controlled trials using the keyword "hypersexuality", selecting 245 useful results. To have a greater and complete overview of the topic, ultimately selecting a total of 25 studies, still adding 21 more reviews to be able to argue the elaborated content (to more easily contextualize definitions and clinical-diagnostic profiles), for an overall total of 46 results. Simple reviews, opinion contributions, or publications in popular volumes were excluded because they were not relevant or redundant for this work. The search was limited to English-language papers.
Figure 1.
PRISMA flow diagram template for systematic reviews. Matthew J Page et al. BMJ 2021;372:bmj.n71.
Figure 1.
PRISMA flow diagram template for systematic reviews. Matthew J Page et al. BMJ 2021;372:bmj.n71.
3. Results
3.1. The different forms of hypersexuality
No work appears in the literature that clearly and precisely differentiates the different forms of hypersexuality. Although the shared use of this terminology has replaced the previous terms "nymphomania" and "satyriasis" concretely no one has ever put in place a real classification capable of differentiating and grading hypersexuality. This first limitation thus confuses both the structure and function of the term concerning the clinical profiles investigated here. Trying to fill this gap, it could be argued that the concept of hypersexuality in itself is too general and does not apply exclusively to pathological hypotheses; it is, therefore, necessary to expand the knowledge derived from the current definitions and try to derive from them what is necessary to arrive at a possible separation of terms. We know that hypersexuality becomes pathological: a) when the subject experiences clinically significant discomfort concerning his or her sexual conduct, which, however, does not always coincide with an inner discomfort in realizing one's urges but depends on the social judgment of the community in which he or she lives (be it the couple, friendship, family, work or social nucleus); b) when the subject manifests the presence of a significant and disproportionate increase in the sexual drive for at least 6 months, which, however, does not always correspond to the satisfaction of one's sexual desire, and consisting of recurrent and intrusive fantasies and thoughts, excessive sexual behaviour, and an inability to control one's sexuality, despite the negative consequences resulting from it; c) when the subject, in the realization of one's sexual drives, engages in paraphiliac dysfunctional conduct, thus in comorbidity with them or with sexual dysfunction [6,7,8].
3.2. Hypersexuality as a clinical condition or maladaptive behaviour?
There is still debate in the scientific community about the age-old question of whether hypersexuality is a maladaptive subjective behaviour, due to a traumatic psychophysical event, or is rather a clinical condition. There is no definitive answer, and this gap prevents further exploration of the issue; however, by reviewing what is in the literature, it is possible to define hypersexuality as a psychological and behavioural alteration as a result of which people seek sexually motivated stimuli in inappropriate ways, often experienced in a manner that is not completely satisfactory [1]. This definition indirectly allows hypersexuality to be labelled as a potentially clinically relevant condition, the result of one or more subjective behaviours maladaptive to the expected statistical mean. And by this assumption, there is always debate in the literature as to whether hypersexuality is a primary or secondary condition, that is, whether or not it depends on other causes. Today, the majority position seems to reasonably lean toward the secondary hypothesis, as it appears to be a dysfunctional adaptation to a primary fact that secondarily induces the onset of the hypersexual condition. In fact, all etiological hypotheses underlying hypersexuality confirm this reasoning: a) neurological syndromes [9,10,11,12,13,14,15,16,17,18,19,20], such as Klüver-Bucy syndrome (consisting of a bilateral lesion of the amygdala), typical and atypical dementias with temporo-frontal involvement, Pick's dementia, Kleine-Levin syndrome (or recurrent hypersomnia), autism, and attention-deficit/hyperactivity disorder (ADHD); b) psychiatric forms [21,22,23,24,25,26,27,28,29,30,31,32], such as bipolarism and borderline disorder (in their euphoric/sub-euphoric components typical of manic and/or hypomanic), sub-obsessive forms, sexually oriented behavioral addictions, and high-functioning personality disorders, such as covert-type narcissism; c) traumas of the encephalon [33], in the regions used for rationality and impulse control (temporofrontal and limbic system in general); d) implications arising from the use of excitatory drugs (such as methamphetamine, cocaine, synthetic drugs, and hallucinatory drugs) and from the therapeutic use of certain drugs, such as the use of L-dopa and prolactin inhibitors in Parkinson's dementia (indeed, dopaminergic drugs have been shown to influence conscious processing of rewarding stimuli and are associated with impulsive-compulsive behaviors, such as hypersexuality, by going on to activate the nucleus accumbens and dorsal anterior cingulate when shown subliminal sexual stimuli), anabolic drugs, and testosterone and other sex hormone products. [34]. And it is precisely in the presence, therefore, of the fulfilment of generally accepted diagnostic criteria, out of any other physiological condition (albeit deviating from the statistical mean of the reference population) that the diagnosis of sexual conduct dysfunction due to hypersexuality is reached, resulting in the evaluation of a multidisciplinary therapeutic approach considering individual and/or group psychotherapy, mainly of cognitive-behavioural or constructivist-strategic approach (to correct reinforcers and coping strategies, work on one's emotions, motivational recovery and metacognitive functions), and psychopharmacological treatment based on symptomatology, with anxiolytics, antidepressants, mood stabilizers and antipsychotics. [35,36,37,38]
3.3. The etiopathological theories of hypersexuality
Several etiopathological theories in the literature try to explain hypersexuality, but all of them do not seem to be fully satisfactory enough to answer the question in a supportable and reproducible way. However, if the compulsive, impulsive, and psycho-traumatic models can partially explain the hypersexual condition, the neurobiological model manages to be more precise. Below is the table is a schematization of the main etiopathological theories:

Table 2.
Table of major etiopathological theories of hypersexuality.
| Theoretical models | Content |
|---|---|
| Compulsive | Hypersexuality is a modality of obsessive-compulsive disorder (OCD), in that they would manifest as recurrent and intense sexual fantasies that interfere with the performance of normal daily activities, while compulsions could be configured as sexual behaviours that are very difficult to counteract and take up a lot of the person's available time. In addition, the sexual act (whether masturbatory or through intercourse with a partner) is seen as a libidinal drive release mechanism that increases concerning times of high stress. However, unlike OCD, thoughts and behaviours related to sexuality are egosyntonic, i.e., consistent with one's self; they do not create discomfort for the person and are seen as natural and devoid of any problematic aspects, on par with personality disorders. Those suffering from obsessive-compulsive disorder, on the other hand, perceive obsessions as highly intrusive. Hypersexuality cannot, therefore, be part of the category of obsessive-compulsive and related disorders, strictly speaking. |
| Impulsive | The impulsive dysfunctional model is the one deemed correct by the World Health Organization, in which hypersexuality is seen as an impulse control disorder. Underlying it is the idea that the hypersexual person is unable to adequately manage his or her sexual impulses: he or she would act on them, without modulating them, the moment he or she feels them. This presupposes a sexual tension that cannot be procrastinated before the act and its release during the act, which would be followed by guilt. The lack of inhibition is due to frontal lobe malfunction. This position, however, clashes with the behavioural representation of the hypersexual subject who is anything but impulsive in organizational acting out: although the impulse may be correctly labelled as irrepressible, in most cases the subject then comes to plan his or her activities in a lucid, rational and methodical manner. |
| Additional (neurobiology) | The addiction model attempts to explain hypersexuality as a behavioral addiction because of the peculiar characteristics common to addictions precisely: the tendency to tolerate sexual activity (sexual intercourse is less and less satisfying); the occurrence of withdrawal symptoms in the absence of sexual activity, such as rumination, anxiety and guilt; the difficulty in reducing, or otherwise controlling, sexual behaviors (such as compulsive masturbation, heavy use of pornography, seeking sexual stimulation through the Internet and social networks, cybersex practices, promiscuous, multiple and/or casual sexuality, disinterest in the risk of contracting diseases through unprotected sexual conduct, prostitution, need for infidelity); the use of more and more considerable time aimed at seeking partners; the reduction of time devoted to other activities (sociality disappears in favor of sexual activity); the act is perpetrated despite the fact that it entails negative consequences more or less impacting the subject's personal and social life. Moreover, this model finds particular reinforcement from scientific evidence, which has been derived from studies of the neurophysiological correlates of hypersexuality. Neuroimaging techniques have revealed dysfunction in the dopaminergic and serotonergic systems, frameworks typical of addictions, precisely underlying the compulsive and uncontrolled pursuit of sexual satisfaction. The dopamine neurotransmitter emitted by neurons located in the limbic system (nucleus accumbens) would be released in a dysregulated manner in individuals with hypersexuality, due to an exaggerated and disproportionate overactivity of the Mesolimbic-dopaminergic and nigrostriatal pathways. In individuals with impulse dysregulation disorders and obsessive-compulsive disorder, it is precisely this function that would be affected. Although not yet definitively validated by significant scientific research, scholars have also theorized the involvement in the aetiology of hypersexuality of the neurotransmitter serotonergic, a neuronal hormone that makes people experience the feeling of happiness, satiety and fulfilment. The same reasoning must also be applied to oxytocin [41], which is directly involved in social and affective relationships. |
| Psychodramatic | It distinguishes the disorder of hypersexuality from normal intense sexual activity, citing traumatic reasons behind the establishment of dysfunctional behaviour. Psychometric instruments are used to shareable label the clinical response. [1,39,40,42] |
Table 3.
Research Questions/Answers.
| Questions | Answers |
|---|---|
| Is it possible to distinguish one or more forms of hypersexuality? And if so, is there a pathological form and how does it differ from the other hypotheses? | Currently, it is not possible in the literature to distinguish between the different forms of hypersexuality, except by trying to identify the form deemed pathological because it meets the diagnostic criteria proposed by ICD-11. For this reason, the Perrotta Hypersexuality Scale (PHS-1) was suggested. |
| Is it possible to say that pathological hypersexuality is a clinical condition, medically relevant, or is it a subjective maladaptive behaviour? And if it is a condition, is it primary or secondary? | Hypersexuality is a potentially clinically relevant condition, secondary to another medical condition (encephalic trauma, neurological, drugs, substance abuse, and psychiatric) and consisting of one or more dysfunctional and pathological behaviours of one's sexual sphere. |
| Is it possible to identify the aetiology of pathological hypersexuality with scientific certainty, thus in a reproducible and agreeable manner? | Several etiopathological theories in the literature try to explain hypersexuality, but all of them do not seem to be fully satisfactory enough to answer the question in a supportable and reproducible way. However, if the compulsive, impulsive, and psycho-traumatic models can partially explain the hypersexual condition, the neurobiological model manages to be more precise. |
Table 4.
Selected manuscripts on the theme of hypersexuality. RES (Clinical trial or Randomized controlled trial); M (Meta-Analysis); R (Review and Systematic review); E (Editorial).
Table 4.
Selected manuscripts on the theme of hypersexuality. RES (Clinical trial or Randomized controlled trial); M (Meta-Analysis); R (Review and Systematic review); E (Editorial).
| Author (Year) | Objectives | Type | Key Results and Conclusions |
|---|---|---|---|
| Montgomery-Graham, S. (2017) | Conceptualization and Assessment of Hypersexual Disorder | R | The Hypersexual Disorder Screening Inventory, the measures proposed for the clinical screening of HD by the DSM-5 workgroup, currently has the strongest psychometric support. |
| Parra-Dìaz, P. et al. (2020) | Impulse control disorders (ICDs) and Parkinson's disease (PD) | R | The tendency towards a different ICD profile in different geographical areas may be attributable to socio-economical, cultural or political influences in the phenomenology of these disorders. |
| Soldati, L. et al. (2020) | Sexual Function/Dysfunctions and ADHD | M | ADHD is a mental disorder affecting sexual health. Further studies are warranted to learn more about sexuality in subjects with ADHD. |
| Korchia, T. et al. (2022) | ADHD prevalence in patients with hypersexuality and paraphilic disorders | M | ADHD is much more frequent in populations with hypersexuality or paraphilic disorders compared to the general population. |
| Latella, D. et al. (2021) | Hypersexuality in neurological diseases | M | Hypersexuality is a frequent sexual disorder in patients with neurological disorders, especially neurodegenerative ones. |
| Codling, D. et al. (2015) | Hypersexuality in Parkinson's Disease | R | A brief survey of the neurobiology of sexuality, suggests possible avenues for further research and treatment of HS. |
| Nakum, S., Cavanna, A.E. (2016) | Hypersexuality in Parkinson's Disease | R | Hypersexuality is not rare in patients with PD treated with DRT, particularly in those on dopamine agonists. |
| de Oliveira, M. et al. (2013) | Pharmacological treatment for Kleine-Levin syndrome | R | Therapeutic trials of pharmacological treatment for Kleine-Levin syndrome with a double-blind, placebo-controlled design are needed. |
| Burley, C.V. et al. (2022) | Pharmacological and nonpharmacological approaches and dementia | R | Pharmacological and nonpharmacological approaches to reduce disinhibited behaviours in dementia |
| de Alarcòn, R. et al. (2019) | Online Porn Addiction | R | Hypersexual disorder fits this model and may be composed of several sexual behaviours, like problematic use of online pornography (POPU). |
| Karila, L. et al. (2014) | Sexual addiction or hypersexual disorder | R | Addictive, somatic and psychiatric disorders coexist with sexual addiction. |
| Castellini, G. et al. (2016) | Sexuality in eating disorders patients | R | The analysis of the literature showed an association between sexual orientation and gender dysphoria with EDs psychopathology and pathological eating behaviours, confirming the validity of research developing new models of maintaining factors of EDs related to the topic of self-identity. |
| Kowatch, R.A. et al. (2005) | Phenomenology and clinical characteristics of mania in children and adolescents | M | The clinical picture that emerges is that of children or adolescents with periods of increased energy (mania or hypomania), accompanied by distractibility, pressured speech, irritability, grandiosity, racing thoughts, decreased need for sleep and euphoria/elation. |
| de Oliveira, L. et al. (2020) | The Link Between Boredom and Hypersexuality | R | Although current literature identifies a link between boredom and hypersexuality, further substantive research is still much needed to clarify the associations between the 2 constructs. |
| Schultz, K. et al. (2014) | Nonparaphilic Hypersexual Behavior and Depressive Symptoms | M | There was a moderate, positive relation between non-paraphilic hypersexual behaviour and depressive symptoms. This relation was similar across gender, sexual orientation, and age. |
| Jennings, T.L. (2021) | Compulsive sexual behaviour, religiosity, and spirituality | R | Although research examining CSB and religiosity has flourished, such growth is hampered by cross-sectional samples lacking in diversity. Moral incongruence assists in explaining the relationship between religiosity and PPU, but future research should consider other manifestations of CSB beyond PPU. |
| Landgren, V. (2022) | Effects of testosterone suppression on desire, hypersexuality, and sexual interest in children in men with pedophilic disorder | RES | The effects of testosterone withdrawal on significant correlates of paedophilic disorder (PeD) are largely unknown. The purpose of this study was to explore in detail the effects of testosterone suppression from degarelix as compared to placebo on desire, hypersexuality, and subjectively experienced sexual interest in participants with PeD. We compared the sexual effects of degarelix, a GnRH antagonist, on men with PeD assigned to degarelix or placebo. Sexual Desire Inventory scores decreased significantly at two weeks and ten weeks in participants assigned degarelix, whereas HBI ratings did not differ significantly at two weeks, but did so at ten weeks. 15 out of 26 individuals (58%) in the group given degarelix and 3 out of 26 (12%) in the group given the placebo reported no further sexual interest in children, at ten weeks. |
| Walton, M.T. (2017) | Hypersexuality | R | Our discussion of hypersexuality covers a diversity of research and clinical perspectives. |
| Hallberg, J. (2017) | A Cognitive-Behavioral Therapy Group Intervention for Hypersexual Disorder | RES | Although participants reported decreased HD symptoms after attending the CBT program, future studies should evaluate the treatment program with a larger sample and a randomized controlled procedure to ensure treatment effectiveness. |
| Hallberg, J. (2017) | A Randomized Controlled Study of Group-Administered Cognitive Behavioral Therapy for Hypersexual Disorder in Men | RES | A significantly greater decrease in HD symptoms and sexual compulsivity, as well as significantly greater improvements in psychiatric well-being, were found for the treatment condition compared with the waitlist. These effects remained stable at 3 and 6 months after treatment. |
| Schecklmann, M. (2020) | Repetitive Transcranial Magnetic Stimulation as a Potential Tool to Reduce Sexual Arousal | RES | The results indicate that 1 session of high-frequency rTMS (10 Hz) of the right DLPFC could significantly reduce subjective sexual arousal induced by visual stimuli in healthy subjects. |
| Chatzittofis, A. (2016) | HPA axis dysregulation in men with hypersexual disorder | RES | Hypersexual disorder integrating pathophysiological aspects such as sexual desire deregulation, sexual addiction, impulsivity and compulsivity was suggested as a diagnosis for the DSM-5. The patients reported significantly more childhood trauma and depression symptoms compared to healthy volunteers. The diagnosis of hypersexual disorder was significantly associated with DST non-suppression and higher plasma DST-ACTH even when adjusted for childhood trauma. The results suggest HPA axis dysregulation in male patients with hypersexual disorder |
| Oei, N.Y.L. et al. (2012) | Dopamine modulates reward system activity during the subconscious processing of sexual stimuli | RES | Brain activation was assessed during a backwards-masking task with subliminally presented sexual stimuli. Results showed that levodopa significantly enhanced the activation in the nucleus accumbens and dorsal anterior cingulate when subliminal sexual stimuli were shown, whereas haloperidol decreased activations in those areas. Dopamine thus enhances activations in regions thought to regulate 'wanting' in response to potentially rewarding sexual stimuli that are not consciously perceived. This running start of the reward system might explain the pull of rewards in individuals with compulsive reward-seeking behaviours such as hypersexuality and patients who receive dopaminergic medication |
4. Discussion and limitations
The pathological concept of "hypersexuality" and its clinical reference is well established in the literature; however, it is not possible to clarify whether only that person who manifests such behaviours because of his promiscuity or even if he enacts them exclusively with one person should be considered "hypersexual" likewise, at present, it is not possible to clarify whether pathological hypersexuality depends on the number of relationships (understood in the quantitative sense) or the intensity of them (understood in the qualitative sense), due to the time spent and resources used.
Although there are no established criteria for hypersexuality, traits that are commonly seen in a hypersexual person or sexual addict include: [43]
1. You’re obsessed with sex. You spend a lot of time fantasizing about your sexual urges and engaging in sexual behaviour.
2. You masturbate often (once to several times daily).
3. You frequently view pornography. Sources include videos, adult magazines, and the internet (websites, webcams). You often masturbate while viewing pornography.
4. You spend an excessive amount of time planning sexual activity. You spend a lot of time figuring out where and how you’ll get your next sexual “high.”
5. You frequently use sexual services. This is a step up, in that your activities now involve human interaction. Behaviours could include phone sex, connections made through internet chat rooms, paying for sexual encounters, visits to strip clubs, having multiple partners or frequent one-night stands.
6. Your behaviour escalates to reckless sexual activity. You may add substance abuse to your sexual activity or add sexual aggression or dangerous sexual activity (such as autoerotic asphyxiation) to your behaviours.
7. You engage in sexual behaviours that go against your values, religious beliefs or what society deems appropriate.
8. You frequently engage in paraphilia. These are sexual behaviours that involve another person’s psychological distress, injury or death. Examples include exhibitionism (exposing genitals to strangers), voyeurism (watching or engaging in sexual activities with others), sadomasochism (sexual pleasure from inflicting pain or humiliation on others) and paedophilia (sexual feelings toward children).
9. You can’t stop your sexual behaviour despite negative consequences to your finances, relationships, health or emotions.
The physiological and pathological boundary seems to be marked exclusively by adherence or non-adherence to the shared and widely used diagnostic criteria in psychiatric practice, but such a view seems overly stringent labelling, and impractical concerning the subjective emotional universe of the person. "Hypersexual" should therefore be considered those who, in compliance with the above diagnostic criteria, present an accentuation of the individual sexual dynamic plot, of a presumed neuropsychiatric matrix of dimensional type (and not purely categorical) [44,45], such as to condition one's own and others' lives according to sexual activity; the more it presents itself as conditioning and limiting concerning other spheres of life (family, work, social relations, affective and sentimental relationships), in reason of its qualitative and quantitative manifestation, the more hypersexuality presents dysfunctional pathological connotations, deserving of clinical intervention.
Another issue that is not unanimously answered in the literature concerns the relationship between hypersexuality and paraphilia. It is unclear whether hypersexuality can be considered paraphilia or is simply the summation of behaviours aimed at the intensification of sexual activity beyond the limits predetermined by the reference context. In this regard, the inference that seems most consistent with the topic analyzed is to consider hypersexuality as a behavioural status, with a strong emotional impact, that can manifest itself with or without the presence of one or more paraphilias: in essence, paraphilias become the means used by the hypersexual to fuel his dysfunctional state, but they may not be present or may be limited to a precise context or still be attenuated or nuanced concerning the main conduct of seeking sexual activity. A hypersexual who has one or more paraphilias structured into a paraphiliac disorder is markedly pathological, compared to a hypersexual who does not have such a disorder in his or her personological profile.
Yet another issue concerns the relationship between hypersexuality and mental disorders nosographically framed in psychiatry. The literature here is rich on this topic, and hypersexuality is always associated with pathological and dysfunctional personality frameworks as is the case with borderline, histrionic, narcissistic, and antisocial disorder, but also with markedly manic bipolar profiles, in obsessive-compulsive disorder, sadistic and masochistic personalities, and in psychosis with erotically motivated features; however, it is not clear whether hypersexuality is the factor that fuels dysfunctionality in these morbidities or is rather a constitutive element of them. [46]
No research, in the literature, has focused on the possible role of oxytocin in hypersexuality, and thus the neurobiological relationship with dopaminergic accesses, instead widely studied in sexual conduct-related disorders.
Various psychometric instruments are used to assess the degree of functional impairment of hypersexual individuals, such as in the case of the Sex-relation Evaluation Schedule Assessment Monitoring (SESAMO), which explores sexual and relational aspects, the Sexual Addiction Screening Test (SAST) and the Sexual Compulsivity Scale (SCS), which investigate the compulsive component of dependent sexuality, of the Hypersexual Behavior Inventory (HBI), which investigates hypersexual behaviours, and the Childhood trauma questionnaire (CTQ), which investigates psycho-traumatic profiles of the infant; [5] however, none of these instruments clearly and comprehensively define a graded scale of hypersexuality capable of distinguishing between highly functional and dysfunctional forms.
Because of these limitations, it was decided to propose a scale to comprehensively assess the severity of the symptoms of hypersexuality, capable of collecting the range of the main hypotheses, thus grading the behaviour according to the different factors involved; this classification (Perrotta Hypersexuality Global Scale, PH-GS) therefore intends to fill the content gap found here in the literature, to propose a comprehensive measure, pending validation using a representative sample. Following is the table:
Table 5.
Perrotta Hypersexuality Scale, PHS-1.
| High-functioning pathological | |||
|---|---|---|---|
| Level | Colour | Definition | Behaviour |
| 1 | Pink | Pro-active hypersexuality | The subject presents an accentuation of the sexual storyline, in terms of drive needs that are higher than the statistical average of the reference population but still fall within the physiological framework or subjective normality because they do not respond to any existing nosographic pathological profile. He or she can moderate his or her behaviour and adapt to the social context, despite feeling a reasonably more significant drive present than expected, due to age and individual and collective relational context. The fulfilment of these needs is embodied in a greater drive to seek and achieve them, but no dysfunctional conduct, relevant paraphiliac comorbidities, or excessively impulsive acts are present. |
| 2 | Yellow | Dynamic hypersexuality | The subject presents a marked accentuation of the sexual plot, in terms of drive needs higher than the statistical average of the reference population but still falling within the physiological framework or subjective normality, because they do not respond to any existing nosographic pathological profile. He is still able to moderate his behaviour and adapt to the social context, despite feeling an unreasonably more significant drive present than expected, due to age and individual and collective relational context. The fulfilment of these needs is embodied in a greater propulsive drive in the pursuit and realization in practice, but dysfunctional behaviours and paraphiliac comorbidities of mild significance are already present, in the absence, however, of excessively impulsive or egregious acts. |
| Pathological attenuated functioning | |||
| Level | Colour | Definition | Behaviour |
| 3 | Orange | Dysfunctional hypersexuality | The subject presents a significantly marked accentuation of the sexual plot, in terms of drive needs that are higher than the statistical average of the reference population and no longer within the physiological or subjective normal framework. He moderates his behaviour with difficulty, and his functional adaptation to the social context appears coarse and irreverent, precisely because of the markedly more significant sexual drive than expected, due to age and individual and collective relational context. The fulfilment of these needs is substantiated by an excessive propulsive drive in the concrete pursuit and realization, dysfunctional conduct, paraphiliac comorbidities of moderate significance, and impulsive acts out of context are present. |
| 4 | Red | Pathological hypersexuality (grade I) | The subject presents a disproportionate accentuation of the sexual plot, in terms of drive needs that are higher than the statistical average of the reference population and no longer within the physiological framework or subjective normality. He is hardly able to moderate his behaviour and his functional adaptation to the social context appears out of context and often excessive, precisely because of the significantly more pronounced sexual drive than expected, due to age and individual and collective relational context. The fulfilment of these needs is substantiated by an extreme drive in the concrete pursuit and realization, and dysfunctional behaviours, paraphiliac comorbidities of serious relevance, and impulsive out-of-context acts are present; however, he is aware of his acts and is concerned about the possible negative implications in the social context (ego-dystonia) but is not fully attuned to his emotional plan |
| Pathological to corrupt functioning | |||
| Level | Colour | Definition | Behaviour |
| 5 | Purple | Pathological hypersexuality (grade II) | The subject presents a disproportionate and unreasonable accentuation of the sexual plot, in terms of drive needs well above the statistical average of the reference population and no longer within the physiological or subjective normalcy framework. He is unable to moderate his behaviour, and his functional adaptation to the social context appears severely compromised, precisely because of the significantly more pronounced sexual drive than expected, due to age and individual and collective relational context. He exposes himself to danger to himself and others, gives no weight to the negative consequences of his behaviour, and adopts insane, promiscuous, impulsive and instinctive conduct. The fulfilment of such needs is substantiated by an uncontrollable propulsive drive in concrete pursuit and fulfilment, and severe dysfunctional conduct, paraphiliac comorbidities of extreme pathological relevance, and impulsive and irrational acts out of context are present. He is not aware of his acting out (ego-syntony) and his emotional plane, although he may display emotions and feelings that seemingly may prove otherwise. |
5. Conclusions
Hypersexuality is the term that describes a series of heterogeneous conditions, substantiated by behaviours of a sexual nature that must be graded, according to their severity of impairment of subjective agency. If the terms nymphomania and satyriasis now appear judgmental, it is only correct to speak of hypersexuality if a grading scale is put in place to help the practitioner distinguish between the different hypotheses; for this reason, the Perrotta Hypersexuality Global Scale (PH-GS) is suggested, which distinguishes high-functioning forms (pro-active and dynamic hypersexuality) from those of attenuated and corrupt functioning (dysfunctional and pathological grade I and II hypersexuality). Hypersexuality, therefore, is a potentially clinically relevant condition, secondary to another medical condition and consisting of one or more dysfunctional and pathological behaviours of one's sexual sphere, which can be explained in a more shareable and reproducible way according to the neurobiological theoretical model. Future research is hoped to address the practical needs of this condition, such as the exact etiopathology, the role of oxytocin in the dopaminergic hypotheses (and its ability to attenuate the symptomatology suffered by the patient in terms of manic drive), the best structural and functional personality framing of the subject, and the appropriate therapy to be pursued.
6. Implications for Clinical Practice
Systematically defining the gradation of hypersexuality means being able to frame the subject more structurally and functionally, by the most appropriate treatment, avoiding letting the therapist decide based on his or her subjective assumption or interpretation of the patient's symptomatic experience. It is therefore extremely important to be able to complete such an operation, to give clinical dignity to a condition that to date is not fully explained, and which is often interpreted only as a personality trait or accentuation of the sexual pattern because of the primary medical condition.
Funding
This work received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The author declares no conflict of interest.
References
- Bernorio, R.; Mori, G.; Casnici, F.; Polloni, G. L’approccio diagnostico in sessuologia. 2020, Franco Angeli Ed.
- Simonelli, C. L’approccio integrato in sessuologia clinica. 2006, Franco Angeli Ed.
- World Health Organization (WHO) ICD-11: International classification of diseases (11th revision). 2022: https://icd.who.int/.
- American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders (5th ed.). <b>2013</b>: Washington, DC. American Psychiatric Association (APA). Diagnostic and statistical manual of mental disorders (5th ed.). 2013: Washington, DC.
- Montgomery-Graham, S. Conceptualization and Assessment of Hypersexual Disorder: A Systematic Review of the Literature. Sex Med Rev 2017, 5, 146–162. [Google Scholar] [CrossRef] [PubMed]
- Parra-Dìaz, P.; Chico-Garcìa, J.L.; Beltràn-Corbellini, A.; Rodrìguez-Jorge, F.; Fernàndez-Escandòn, C.L.; Alonso-Cànovas, A.; Martìnez-Castrillo, J.C. Does the Country Make a Difference in Impulse Control Disorders? A Systematic Review. Mov Disord Clin Pract 2020, 8, 25–32. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, G. Paraphilic disorder: definition, contexts and clinical strategies. Neuro Research 2019, 1, 4. [Google Scholar] [CrossRef]
- Perrotta, G. Dysfunctional sexual behaviours: definition, clinical contexts, neurobiological profiles and treatments. Int J Sex Reprod Health Care 2020, 3, 61–69. [Google Scholar]
- Soldati, L.; Bianchi-Demicheli, F.; Schockaert, P.; Kohl, J.; Bolmont, M.; Hasler, R.; Perroud, N. Association of ADHD and hypersexuality and paraphilias. Psychiatry Res 2021, 295, 113638. [Google Scholar] [CrossRef] [PubMed]
- Korchia, T.; Boyer, L.; Deneuville, M.; Etchecopar-Etchart, D.; Lancon, C.; Fond, G. ADHD prevalence in patients with hypersexuality and paraphilic disorders: a systematic review and meta-analysis. Eur Arch Psychiatry Clin Neurosci 2022, 272, 1413–1420. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, G. Attention Deficit Hyperactivity Disorder: definition, contexts, neural correlates and clinical strategies. J Addi Adol Beh 2019, 2, 1. [Google Scholar] [CrossRef]
- Latella, D.; Maggio, M.G.; Andaloro, A.; Marchese, D.; Manuli, A.; Calabrò, R.S. Hypersexuality in neurological diseases: do we see only the tip of the iceberg? J Integr Neurosci 2021, 20, 477–487. [Google Scholar] [CrossRef]
- Codling, D.; Shaw, P.; David, A.S. Hypersexuality in Parkinson's Disease: Systematic Review and Report of 7 New Cases. Mov Disord Clin Pract 2015, 2, 116–126. [Google Scholar] [CrossRef]
- Nakum, S.; Cavanna, A.E. The prevalence and clinical characteristics of hypersexuality in patients with Parkinson's disease following dopaminergic therapy: A systematic literature review. Parkinsonism Relat Disord 2016, 25, 10–6. [Google Scholar] [CrossRef]
- de Oliveira, M.M.; Conti, C.; Prado, G.F. Pharmacological treatment for Kleine-Levin syndrome. Cochrane Database Syst Rev 2016, 5, CD006685. [Google Scholar] [CrossRef] [PubMed]
- Burley, C.V.; Burns, K.; Brodaty, H. Pharmacological and nonpharmacological approaches to reduce disinhibited behaviors in dementia: a systematic review. Int Psychogeriatr 2022, 1–17. [Google Scholar] [CrossRef] [PubMed]
- Perrotta; G. General overview of “human dementia diseases”: definitions, classifications, neurobiological profiles and clinical treatments. Gerontol & Geriatric stud. 2020, 6, 1. [Google Scholar]
- Perrotta, G. Autism Spectrum Disorder: Definition, contexts, neural correlates and clinical strategies. J Neurol Neurother 2019, 4, 2–136. [Google Scholar]
- Perrotta; G. Sleep-wake disorders: Definition, contexts and neural correlations. J Neurol Psychol. 2019, 7, 09. [Google Scholar] [CrossRef]
- de Alarcon, R.; de la Iglesia, J.; Casado, N.M.; Montejo, A.L. Online Porn Addiction: What We Know and What We Don't-A Systematic Review. J Clin Med 2019, 8, 91. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, G. Obsessive-Compulsive Disorder: definition, contexts, neural correlates and clinical strategies. Journal of Neurology 2019, 1, 8–16. [Google Scholar]
- Perrotta, G. Behavioral addiction disorder: definition, classifications, clinical contexts, neural correlates and clinical strategies. J Addi Adol Beh 2019, 2, 1. [Google Scholar] [CrossRef]
- Perrotta, G. Bipolar disorder: definition, differential diagnosis, clinical contexts and therapeutic approaches. J. Neuroscience and Neurological Surgery 2019, 5, 1. [Google Scholar] [CrossRef]
- Perrotta, G. Borderline Personality Disorder: definition, differential diagnosis, clinical contexts and therapeutic approaches. Ann Psychiatry Treatm 2020, 4, 43–56. [Google Scholar]
- Perrotta, G. Narcissism and psychopathological profiles: definitions, clinical contexts, neurobiological aspects and clinical treatments. J Clin Cases Rep 2020, 4, 12–25. [Google Scholar]
- Karila, L.; Wery, A.; Weinstein, A.; Cottencin, O.; Petit, A.; Reynaud, M.; Billieux, J. Sexual addiction or hypersexual disorder: different terms for the same problem? A review of the literature. Curr Pharm Des 2014, 20, 4012–20. [Google Scholar] [CrossRef] [PubMed]
- Castellini, G.; Lelli, L.; Ricca, V.; Maggi, M. Sexuality in eating disorders patients: etiological factors, sexual dysfunction and identity issues. A systematic review. Horm Mol Biol Clin Investig 2016, 25, 71–90. [Google Scholar] [CrossRef] [PubMed]
- Kowatch, R.A.; Youngstrom, E.A.; Danielyan, A.; Findling, R.L. Review and meta-analysis of the phenomenology and clinical characteristics of mania in children and adolescents. Bipolar Disord 2005, 7, 483–96. [Google Scholar] [CrossRef] [PubMed]
- de Oliveira, L.; Carvalho, J. The Link Between Boredom and Hypersexuality: A Systematic Review. J Sex Med 2020, 17, 994–1004. [Google Scholar] [CrossRef] [PubMed]
- Schultz, K.; Hook, J.N.; Davis, D.E.; Penberthy, J.K.; Reid, R.C. Nonparaphilic hypersexual behavior and depressive symptoms: a meta-analytic review of the literature. J Sex Marital Ther 2014, 40, 477–87. [Google Scholar] [CrossRef]
- Jennings, T.L.; Lyng, T.; Gleason, N.; Finotelli, I.; Coleman, E. Compulsive sexual behavior, religiosity, and spirituality: A systematic review. J Behav Addict 2021, 10, 854–878. [Google Scholar]
- Landgren, V.; Olsson, P.; Briken, P.; Rahm, C. Effects of testosterone suppression on desire, hypersexuality, and sexual interest in children in men with pedophilic disorder. World J Biol Psychiatry 2022, 23, 560–571. [Google Scholar] [CrossRef]
- Schwartz, M.F. Sexually Compulsive Behavior: Hypersexuality (Psychiatric Clinics of North America), Vol. 31, No. 4. 2008, Sauders Pub.
- Walton, M.T. Hypersexuality: A Critical Review and Introduction to the "Sexhavior Cycle". Arch Sex Behav 2017, 46, 2231–2251. [Google Scholar] [CrossRef]
- Perrotta, G. The strategic clinical model in psychotherapy: theoretical and practical profiles. J Addi Adol Beh 2020, 3, 1. [Google Scholar] [CrossRef]
- Hallberg, J.; Kaldo, V.; Arver, S.; Dhejne, C.; Oberg, K.G. A Cognitive-Behavioral Therapy Group Intervention for Hypersexual Disorder: A Feasibility Study. J Sex Med 2017, 14, 950–958. [Google Scholar] [CrossRef] [PubMed]
- Hallberg, J.; Kaldo, V.; Arver, S.; Dhejne, C.; Jokinen, J.; Oberg, K.G. A Randomized Controlled Study of Group-Administered Cognitive Behavioral Therapy for Hypersexual Disorder in Men. J Sex Med 2019, 16, 733–745. [Google Scholar] [CrossRef] [PubMed]
- Schecklmann, M.; Sakreida, K.; Oblinger, B.; Langguth, B.; Poeppl, T.B. Repetitive Transcranial Magnetic Stimulation as a Potential Tool to Reduce Sexual Arousal: A Proof of Concept Study. J Sex Med 2020, 17, 1553–1559. [Google Scholar] [CrossRef] [PubMed]
- Chatzittofis, A.; Arver, S.; Oberg, K.; Hallberg, J.; Nordstrom, P.; Jokinen, J. HPA axis dysregulation in men with hypersexual disorder. Psychoneuroendocrinology 2016, 63, 247–53. [Google Scholar] [CrossRef] [PubMed]
- Oei, N.Y.L.; Rombouts, S.A.; Soeter, R.P.; van Gerven, J.M.; Both, S. Dopamine modulates reward system activity during subconscious processing of sexual stimuli. Neuropsychopharmacology 2012, 37, 1729–37. [Google Scholar] [CrossRef] [PubMed]
- Perrotta, G. Oxytocin and the role of “regulator of emotions”: definition, neurobiochemical and clinical contexts, practical applications and contraindications. Arch Depress Anxiety 2020, 6, 001–005. [Google Scholar]
- Cantelmi, T.; Lambiase, E. Schiavi del sesso. 2016, Alpes Ed.
- Cleveland Clinic. Source: https://my.clevelandclinic.org/health/treatments/22690-sex-addiction-hypersexuality-and-compulsive-sexual-behavior.
- Asiff, M.; Sidi, H.; Masiran, R.; Kumar, J.; Das, S.; Hatta, N.H.; Alfonso, C. Hypersexuality As a Neuropsychiatric Disorder: The Neurobiology and Treatment Options. Curr Drug Targets. 2018, 19, 1391–1401. [Google Scholar] [CrossRef]
- Graham, F.J.; Walters, G.D.; Harris, D.A.; Knight, R.A. Is Hypersexuality Dimensional or Categorical? Evidence From Male and Female College Samples. J Sex Res. 2016, 53, 224–38. [Google Scholar] [CrossRef]
- Walton, M.T.; Cantor, J.M.; Bhullar, N.; Lykins, A.D. Hypersexuality: A Critical Review and Introduction to the "Sexhavior Cycle". Arch Sex Behav. 2017, 46, 2231–2251. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



