Submitted:
19 April 2023
Posted:
20 April 2023
You are already at the latest version
Abstract
The 22q11.2 deletion syndrome is a multisystemic disorder characterized by a marked variability of phenotypic features making the diagnosis challenging for clinicians. The wide spectrum of clinical manifestations includes congenital heart defects, most frequently conotruncal cardiac anomalies, thymic hypoplasia and predominating cellular immune deficiency, laryngeal developmental defects, midline anomalies with cleft palate and velar insufficiency, structural airway defects, facial dysmorphism, parathyroid and thyroid gland hormonal dysfunctions, speech delay, developmental delay, neurocognitive and psychiatric disorders. Significant progress has been made in understanding the complex molecular genetic etiology of the 22q11.2 deletion syndrome underpinning the heterogeneity of clinical manifestations. The deletion is caused by chromosomal rearrangements in meiosis and is mediated by non-allelic homologous recombination events between low copy repeats or segmental duplications in the 22q11.2 region. A range of genetic modifiers, environmental factors as well as the impact of hemizygosity on the remaining allele contribute to the intricate genotype-phenotype relationships. This comprehensive review has been aimed at highlighting the molecular genetic background of 22q11.2 deletion syndrome in correlation with a clinical multidisciplinary approach.
Keywords:
22q11.2 deletion
; microdeletion
; DiGeorge syndrome
; velocardiofacial syndrome
; dysmorphism
; inborn errors of immunity
; thymus
; congenital heart defect
; hypocalcemia
Introduction
The chromosome 22q11.2 deletion syndrome (22q11.2DS), also known as DiGeorge syndrome (DGS) or velocardiofacial syndrome (VCFS) is a genetic condition resulting from the impaired development of structures originating from the third and fourth pharyngeal pouches in the germinal stage. The clinical features of the syndrome include hypoparathyroidism and hypocalcemia, thymic hypoplasia, conotruncal heart defects, facial dysmorphism, and palatoschisis. The complex phenotype of children affected with 22q11.2DS may show considerable intersubject variability and the expanded clinical manifestations comprise craniofacial, neurological, cognitive, behavioral, ocular, speech and hearing, musculoskeletal, and internal organs, such as airway, gastrointestinal or renal abnormalities as well [1]. The phenotypes may considerably vary among patients with immunodeficiency and immune dysregulation including autoimmunity, allergy, and lymphoproliferative sequelae.
The incidence of 22q11.2DS has been estimated to range from 1:3000 [2] to 1:4000 live births [1] placing it among frequent syndromic diseases. However, the rate of its clinical suspicion is still challenging and the process of establishing the definitive diagnosis is an odyssey [3] due to the remarkable heterogeneity of clinical phenotypic expressions and overlapping manifestations with other categories of syndromic disorders [4,5,6]. The disease entities, such as, but not limited to coloboma-heart defects-choanal atresia-retardation of growth and development-ear anomalies (CHARGE) syndrome [7,8], cardio-facio-cutaneous (CFC) syndrome [9,10], and Takenouchi-Kosaki syndrome (TKS) [11,12] require special pediatrician’s awareness and multidisciplinary care as their distinctive phenotypes are associated with immunodeficiencies. Furthermore, a common denominator of 22q11.2DS and other syndromic disorders is an increased susceptibility to recurrent infections, which may not only result from inborn errors of immunity but also a multiplicity of developmental anatomical malformations and organ dysfunctions are important contributing factors. These extra-immune phenotypes in 22q11.2 DS, with neurological, psychomotor, hormonal, circulatory, and respiratory pathophysiological mechanisms are substantially underpinning the definitive clinical manifestations.
However, there is a paucity of reports on the clinical course of 22q11.2DS in pediatric patients and the data are scattered thereby making them difficult to apply in the all-embracing pediatric practice. In this review, we aimed to establish a comprehensive molecular genetic and clinical approach to 22q11.2DS addressed to pediatricians and specialists in other fields of medicine who encounter children affected with this syndrome and provide in-depth clinical care. We also sought to determine what is known and what is new in the multidisciplinary genetic and clinical diagnostic process, prophylactic measures as well as therapeutic modalities in 22q11.2DS.
Pathophysiology
The 22q11.2 DS comprises several clinical disorders, such as velocardiofacial (VCF, pharyngeal dysfunction, cardiac anomaly, facial dysmorphism) and DiGeorge (DGS, cardiac anomaly, hypoparathyroidism, thymic hypoplasia) syndromes, also known as a group of disorders described by an acronym CATCH22 (cardiac defect, abnormal facial features, thymic hypoplasia, cleft palate, hypocalcemia). The nomenclature may be confusing due to the remarkable heterogeneity of clinical phenotype and marked intersubject variability of presenting symptomatology in 22q11.2 DS [13]. A variety of anatomical and functional developmental abnormalities occur in the fetus and multiple conditions appear later in childhood. The syndrome is characterized by haploinsufficiency resulting from a hemizygous deletion in the region 11.2 on the long arm of chromosome 22, meaning that the gene allele have no homologic counterparts. Interestingly, a deletion on 22q11.2 in combination with a single gene variant on the other allele can reveal autosomal recessive conditions, such as Bernard-Soulier syndrome with thrombocytopenia and increased megakaryocytes (platelet glycoprotein 1B beta-polypeptide, GP1BB variant) and cerebral dysgenesis (polymicrogyria), neuropathy, ichthyosis, palmoplantar keratoderma (CEDNIK) syndrome (synaptosomal-associated protein 29 kDa, SNAP29 variant) [14].
The deletion types and sizes in 22q11.2 DS show a high degree of variability due to several low copy number repeat sequences (LCR22A, LCR22B, LCR22C, LCR22D, LCR22E, and LCR22F), flanking the deleted region. Most patients (about 90%) show a 2.54 Mb heterozygous deletion comprising four repeats extending from LCR22A to LCR22D and involving approximately 40 genes [15]. The disease-causing genes mapping to the region spanned by LCR22A-LCR22D are, among others, TBX1, proline dehydrogenase PRODH, catechol-O-methyltransferase COMT, cell division cycle 45 CDC45, GP1BB, SNAP29, DiGeorge critical regions DGCR2, DGCR6, DGCR6L, DGCR8. A proximal 1.25 Mb deletion, comprising LCR22A-LCR22B affects about 5% of individuals with 22q11.2 DS., whereas 2% of them show a deletion spanning the LCR22A-LCR22C region, and the next 5% have a smaller, atypical nested deletion extending from LCR22B or LCR22C to LCR22D. Distal deletions, flanked by LCR22D-E and LCR22D-F have been reported less frequently [15,16]. The complexity of 22q11.2 genetics is even more prominent due to the regulatory effect of deleted DGCR6, DGCR6L, and DGCR8 gene allele and mi-RNAs, such as miR-185, miR-4716, miR-3618, miR-1286, miR-1306, and miR-6816. Several miRs, miR-96-5, miR-451a, and miR-17-92 target TBX1 thereby influencing its expression and consequently, the clinical phenotype [17,18,19]. The 22q11.2 region encompassing protein-coding genes, long non-coding RNAs, microRNAs and genes expressed in functional haploinsufficiency in 22q11.2 DS are displayed in Figure 1. Additionally, genome-wide DNA methylation analysis in a group of patients with 22q11.2 DS has demonstrated differentially methylated regions located apart from the chromosome 22, which may involve clinically relevant genes or regulatory elements thereby determining the variability of phenotypic features. This phenomenon may also shed light on the impact of 22q11.2 haploinsufficiency in altering the genomic methylation level [20].
The de novo occurrence of the syndrome is observable in about 90-95% of affected individuals in all populations yet autosomal dominant inheritance has also been ascertained in 6-28% of subjects [17]. With it’s prevalence ranging broadly from 1:2000 to 1:6000 live births [14], 22q11.2 DS is put among frequent syndromic disorders. Furthermore, the current estimation of 22q11.2 DS frequency needs to take into consideration the reproductive fitness and increase in survival of children who can pass on the deletion to their offspring thereby increasing the frequency of its occurrence [21,22,23]. Although 22q11.2 DS is the most common microdeletion in humans, it may be underdiagnosed in diverse populations due to the heterogeneity of clinical phenotypic features, including less recognizable facial dysmorphism largely depending on the patient’s ethnicity [24]. Thus, the recognition rate of 22q11.2 in affected children of non-European, in particular, African or Asian descent may be insufficient and the actual prevalence underestimated.
The Burden of 22q11.2 in Pediatrics
With its average frequency estimated to be 1:4000 live births and 1:1000 in unselected fetuses [14], the 22q.11.2 DS has a global burden and remarkable impact on affected patients, their families, society, and health providers as well. Whereas the number of patients reported in the medical literature is disproportionately lower than anticipated due to the estimated frequency, important concerns are raised regarding all the newborns awaiting the genetic molecular diagnosis or children who escaped from the timely recognition of this syndrome [25]. The latter group of undiagnosed individuals may embrace all those children who experience a protracted period of the diagnostic odyssey [2] consequently burdened by unfavorable outcomes. Of note, 22q11.2 DS is an important cause of morbidity and mortality across the lifespan, and both major birth defects and complications that develop later in childhood or even adulthood make an early definitive diagnosis of paramount importance. 22q11.2 DS is the most common cause of syndromic palatal anomalies and velopharyngeal dysfunction [26,27], the most common cause of schizophrenia [28,29] the second most common cause of developmental delay and congenital heart disease after Down syndrome, as well as a more common cause of conotruncal heart disease [30,31]. 22q11.2 deletion is found in about 2% of all subjects with congenital heart disease [32,33] and thus, the syndrome should be always considered in prenatal settings in fetuses affected with congenital heart developmental abnormalities [34]. Notably, after the surgery for congenital heart disease, the rate of postoperative non-cardiac complications such as infections or the need for dialysis [35], length of stay in the intensive care unit, and hypocalcemia [36] is higher in children with 22q11.2 DS than in those with no chromosomal defects. Furthermore, severe forms of congenital heart disease are a primary factor contributing to a lower life expectancy in adults with 22q11.2 DS as the probability to survive by the age of 45 years is approximately 72% in those individuals [22].
Clinical Symptomatology
Craniofacial dysmorphism in 22q11.2 DS is characterized by a multiplicity of facial phenotypic features and some of these facial characteristics are not easily recognized clinically in children as are mild in nature and the age is an important determinant of facial morphology. The elongated face, hypertelorism, wide nasal bridge, hooded eyelids, upslanted palpebral fissures, epicanthus, long nose with a bulbous tip, narrow alar base, short philtrum, small mouth, micrognathia, and low-set, posteriorly rotated small ears. The retrognathic posture of the mandible, inward displacement of the lower part of the face and the ocular region, and an enlarged cranial base angle have been identified as the uppermost dysmorphology features in the cephalometric and spatially dense 3-dimensional analysis [37]. High prevalence of dental features, including tooth abnormalities of their eruption, shape, and number, such as agenesis of permanent dentition or supernumerary teeth as well as enamel hypomineralization and hypoplasia are attributable to 22q11 DS [37,38,39].
Among oropharyngeal developmental disorders, palatoschisis is a frequently observable phenotypic feature, occurring in the form of open cleft, submucosal cleft, palatopharyngeal disproportion, and cleft lingula [40,41]. Velopharyngeal insufficiency and hypotonia accompanied by hypernasal speech have been estimated to occur in as many as 30-80% of children with 22q11.2 DS, rendering the surgical intervention, particularly challenging due to the complexity of coexisting serious medical conditions [41,42].
Developmental disorders of the upper airways in 22q11.2 DS include congenital laryngeal anomalies. Laryngeal atresia due to a glottic web or partial laryngeal stenosis, laryngomalacia, laryngeal cleft, and vocal fold abnormalities are characteristic parts of the syndromic features [43,44]. The laryngeal web has been estimated to be the most frequent upper airway anomaly and 40% sensitive for suggesting a diagnosis of 22q11.2 DS [45]. Velopharyngeal and laryngeal anomalies may be accompanied by lower respiratory tract disorders, such as tracheal stenosis, tracheo- and bronchomalacia, short trachea with reduced numbers of tracheal rings, tracheoesophageal fistula as well as aberrant tracheal bronchus [46,47]. These structural airway abnormalities may be related to obstruction due to anatomically and functionally reduced patency, recurrent and persistent respiratory tract infections, atelectasis of the lung, and pulmonary edema resulting from congenital heart disease. All these overlapping clinical encumbrances may be a significant cause of morbidity and mortality in children with 22q11.2 DS and result in respiratory distress and the need for ventilation support and tracheostomy. Impaired coordination of swallowing and breathing, the risk of aspiration, nasopharyngeal reflux as well as the need to provide caloric and nutritional support necessitate the placement of an enteral percutaneous feeding tube [48].
Congenital heart disease has been recognized in approximately 60-80% of children affected with 22q11.2 DS. The most commonly occurring subset of cardiac anomaly is a conotruncal defect, such as tetralogy of Fallot, pulmonary atresia with ventricular septal defect, truncus arteriosus, interrupted aortic arch type B, conoventricular and/or atrial septal defects, and aortic arch anomalies [32]. The anatomical complexity of congenital heart disease in 22q11.2DS requires special perioperative care, particularly in children with pulmonary atresia-ventricular septal defect (PA-VSD) and major portopulmonary collateral arteries (MAPCAs) posing the risk of increased mortality due to vasomotor instability, airway hyperresponsiveness, coexisting airway abnormalities, increased frequency of airway bleeding, and infectious, mainly fungal complications [49]. The syndrome is therefore associated with unfavorable early perioperative results which, in turn, may be associated with worse cognitive and neuropsychiatric outcomes [50]. Cardiovascular complications are the most common cause of premature death in adults with 22q11.2 DS. Major associated conditions, such as hypocalcemia, thyroid disorders, autoimmune diseases, behavioral problems, and neurodevelopmental disability contribute to the worse fallout [51]. Interestingly, It has been suggested that variance in congenital heart disease, conotruncal type penetration in the population of individuals with 22q11.2 DS may be associated with variants in GH22J020947 affecting the expression of CRKL encoding for a cytoplasmic adaptor protein (CRK-like proto-oncogene) involved in growth factor signaling [52]. Moreover, it has been hypothesized that rare copy number variants outside the deleted 22q11.2 region may act as modifiers of the risk of congenital heart disease in 22q11.2 microdeletion-affected children [53].
The complex and variable phenotypes related to 22q11.2 DS also include mild to moderate intellectual disability, which occurs in approximately one-third of affected pediatric patients [54]. In these patients, global reduction in brain volume, with widespread decay in frontal, temporal, parietal, and occipital lobes, atrophy of the cerebellum and hippocampus, as well as polymicrogyria and altered cortical thickness observable in neuroradiological imaging [55,56]. The syndrome is associated with neurological disorders, such as epilepsy and increased incidence of seizures which may be provoked by other concomitant conditions and complications, among others hypoxia due to congenital heart disease and cardiac surgery, hypocalcemia, thyroid hormonal dysfunction, infections, and fever [57]. Movement disorders in 22q11.2 DS include catatonia and the increased risk of Parkinson’s disease [58].
Noteworthy, 22q11.2 DS is one of the rare examples of a cytogenetic abnormality occurring in conjunction with a psychiatric disease, schizophrenia, autism spectrum disorders (ASD) with some level of social-communication impairement, and attention deficit/hyperreactivity disorder (ADHD) which occur in as many as 20% of affected children and adolescents [54,59]. The spectrum of psychopathology in 22q11.2 DS is complex and comprises anxiety disorders, disruptive and mood disorders. Importantly, symptoms of psychotic conditions may be misinterpreted and wrongly attributed to cognitive impairment, with low social and communicative skills. Moreover, both low intellectual ability early in life and its subsequent decline, impaired verbal and perceptual reasoning abilities as well as altered auditory and visual processing from preschool to adolescence are associated with increased risk of schizophrenia [60,61,62,63]. Ocular abnormalities are frequently encountered in children with 22q11.2 DS in the form of refractive errors, strabismus, amblyopia, and other structural ophthalmological disorders such as posterior embryotoxon aka Axenfeld-Rieger anomaly which may contribute to learning difficulties and cognitive impairment [64,65].
Endocrine manifestations are hallmarks of 22q11.2 DS and primarily comprise hypoparathyroidism, thyroid dysfunction, and growth retardation [66,67]. Hypocalcemia is considered a classical feature of the syndrome, resulting from low parathormone serum levels, accompanied by 25(OH)D3 deficiency. In addition to the major effect of parathyroid gland endocrinopathy, hypothyroidism, and hypomagnesemia may play a role in hypocalcemia by suppressing parathyroid hormone, and thereby are further contributing factors to hypocalcemia [68]. The presentation of hypocalcemia may considerably vary ranging from transient neonatal silent hypocalcemia to hypocalcemic tetany and overt hypoparathyroidism throughout the lifespan. Affected patients may also experience fatigue, paresthesia, as well as more severe manifestations including low seizure threshold and prolongation of the QT interval, significantly affecting both early life neurodevelopment [69] and clinical outcome in cardiac and non-cardiac surgical procedures [70,71,72]. Thyroid dysfunction is commonly due to autoimmune thyroiditis and thyroid autoantibodies, particularly anti-thyroperoxidase antibodies have been found in up to 5% of children and in approximately 30% of adults affected with 22q11.2 DS [73]. Two clinical disease entities of autoimmune thyroiditis have been reported in children with the syndrome: Hashimoto thyroiditis occurs in 20% of them and is characterized by inhomogeneous thyroid echostructure and progression from normal function to hypothyroidism and, less frequently, Grave’s disease which presents with overt hyperthyroidism and is observable in 1,4% of affected pediatric patients [67,73,74,75,76,77]. Congenital thyroid gland abnormalities have also been recognized in children with 22q11.2 DS and included an absent thyroid isthmus, retrocarotid and retroesophageal extension, and absence/hypoplasia of the left thyroid lobe. Noteworthy, developmental thyroid disorders coexisted in as many as 71% of children with congenital heart disease, compared to 31% of those with normal thyroid volume, highlighting the role of the TBX1 gene in the formation of cardiac outflow structure and positioning of the thyroid gland [78]. Growth restriction due to growth hormone deficiency consistent from infancy to final height has been reported and the association between patients’ height and congenital heart disease has been shown in pediatric and young adult patients with 22q11.2 DS [66]. Whereas immune dysregulation is associated with 22q11.2 DS, autoimmune endocrinopathies, such as diabetes mellitus with serum insulin antibodies [79] or adrenal antibodies yet with normal adrenal function [80] are concomitant clinical features. Metabolic disorders, such as type 2 diabetes [81], hypertriglyceridemia [82], and obesity [83] have been noted in the syndrome, with the high frequency of the latter condition, reaching approximately 43% of adult individuals affected with 22q11.2 DS [83].
Immune Deficiency and Immune Dysregulation
Immunodeficiency is a key feature of 22q11.2 DS and is secondary to thymic aplasia or hypoplasia with subsequent impaired thymocyte development. The third and fourth pharyngeal pouches are a common embryonic precursor for the thymus, parathyroid glands, and conotruncal regions of the heart. In 22q11.2 DS, maldevelopment of these organs is due to impaired migration of the neural crest cell into pouch ectoderm [85]. In the setting of abnormal thymic migration but the preservation of residual microscopic nests of thymic epithelial cells, mild to moderate reductions in T cell numbers accompanied by only mild deficit in T cell function occur in most affected children. However, even in these patients, the T-cell thymic output of recent thymic emigrants assessed by T-cell receptor excision circles (TRECs) analysis, is very low and decreases with age [86,87]. Full thymic aplasia appears occasionally, in approximately 1% of cases with 22q11.2 DS [86,88]. Interestingly, beyond the TBX1 hemizygosity, also other genes, such as CRKL in the affected 22q11.2 region may have a gene dosing, modifying effect on the phenotypic expression of the syndrome. CRKL is expressed in neural crest-derived tissues and involves thymic development. The effect of compound heterozygosity for TBX1 and CRKL deletion on clinical features and thymus development is additive [89].
Consequently, a wide spectrum of T-cell alterations is seen in 22q11.2 DS, ranging from near normal to near completely immunodeficient. Mild T cell immunodeficiency may be found in children with apparently hypoplastic thymus as ectopic retropharyngeal thymic tissue may be preserved [90,91]. Furthermore, dynamic changes in the immunodeficiency are observable over time and the direct effect of thymic hypoplasia on T cell counts is most apparent in the early infancy [86,87] and they tend to normalize by adulthood in most patients due to the increased secretion of interleukin (IL)-7 that stimulates the thymic output and peripheral proliferation of T cells [92]. The most common deficits include low total CD3+ T cell percentage and absolute count as well as low numbers of naive CD4+ T helper and CD8+ T cytotoxic/ suppressor cells. The naive T cell compartment shows a progressive decline with patients’ age leading to a predominantly memory phenotype of T cells at the periphery [93].
Referring to anatomical maldevelopment and dysfunction in generating T cells, the humoral immunodeficiency and B cell abnormalities in children with 22q11.2 DS, are secondary to T cell deficits [94]. Low immunoglobulin production, most frequently affecting IgM and occasionally IgG, rendering the need for immunoglobulin replacement therapy, as well as the defective immune response to polysaccharide antigens have been reported in children with the syndrome [95]. Among the B cell subsets, low switched memory B cells expanding by adulthood accompanied by decreased somatic hypermutation despite increased follicular T helper cells, have been shown, reflecting a dysregulated B cell compartment and compromised T cell help [96,97,98]. Recurrent respiratory infections, such as adenotonsillitis, otitis media, bronchitis, pneumonia as well as sepsis [99,100].
Immune dysregulation in 22q11.2 DS has been foremostly ascribed to T-cell lymphopenia and deficiency in CD3+CD4+CD25++, FOXP3+ regulatory T cells, playing a crucial role in maintaining immune homeostasis and self-tolerance. Reduced thymic output related to an increased naive T cell subset and subsequent T regulatory cell activation control the expansion of the T cell compartment. A reduced number of regulatory T cells with their activated phenotype and loss of suppressive capacity in children with 22q11.2 DS are key features of deregulated T cell homeostasis [101]. Beyond the T cell compartment, immunophenotype anomalies also encompass peculiar B cell developmental disorders with increased naive B cells and deficit in switched memory B cells [102] which are biomarkers of immune dysregulation in 22q11.2 DS. It has been postulated, that the individual patient’s immunophenotype may be influenced by genetic modifiers outside the microdeletion locus which regulate the expression of TBX1. Rare DNA variants in transcriptional regulators involved in retinoic acid signaling, NCOR2 and EP300 were found to be associated with parameters of the immune functions, such as immunoglobulin levels, lymphocyte response to antigens and mitogens, and flow cytometric lymphocyte compartment. Retinoic acid plays an important role in maintaing immune homeostasis by enhancing the differentiation of regulatory T cells, modulates epithelial and mucosal immune responses, and regulates proinflammatory cytokine activity. Hence, genetic modifiers contributing to the individual’s genetic background and modulating variable penetrance, may influence the immune response in 22q11.2 DS [103,104].
Autoimmune disorders have been described in as many as 23% of pediatric patients with the syndrome [105], manifesting as autoimmune thyroid disease, juvenile idiopathic arthritis, autoimmune cytopenia (thrombocytopenia, hemolytic anemia, neutropenia), celiac disease, psoriasis, vitiligo, autoimmune hepatitis, and inflammatory bowel disease [100,105,106,107]. It has also been hypothesized that psychotic disorders, developmental regression, and cognitive impairment in children with 22q11.2 DS may have a causal relationship with autoimmune encephalitis [108].
The peripheral homeostatic expansion of T cells driven by low thymic output and T cell lymphopenia may contribute to Th2-skewed lymphocyte phenotype and atopic manifestations, such as eczema and asthma [109]. In these children with 22q.11.2 DS, the overall frequency of atopic diseases has been estimated to reach 70%, and the frequency of asthma to as many as 50% [110], and coexisting gastroesophageal reflux and sinopulmonary infections may have an impact on its clinical course [111].
The thymus dysfunction and immunophenotypic abnormalities within the T cell compartments in 22q11.2 DS make affected children susceptible to cancerogenic viruses, such as Epstein-Barr virus (EBV) and human papilloma virus (HPV) that might be linked to an increased risk of malignant transformation. It has also been postulated that chronic immune activation of peripherally expanded T cell population in dysfunctional cellular immunity may underpin the predisposition to developing lymphoproliferative disorders and lymphomagenesis [112] as T cell and B cell lymphomas [113,114,115] as well as acute lymphoblastic leukemia [116] have been reported in children with 22q11.2 DS. The spectrum of malignancies in affected pediatric patients also includes solid tumors, namely Wilms tumor, hepatoblastoma, neuroblastoma, thyroid carcinoma [116], pineoblastoma [112], and xanthoastrocytoma [117].
Diagnosis
The chromosomal 22q11.2 DS is a clinically highly variable microdeletion syndrome with differently expressed phenotypes, with wide interfamilial and intrafamilial variability in patients sharing the same genetic underpinnings [118]. This is due to both the remarkable complexity of the 22q11.2 region with LCR blocks and the high susceptibility of this region to meiotic errors as well as the epigenomic and environmental factors influencing the phenotypic variability [119]. Based on functional genomic assessments, it has also been hypothesized that theories on single-gene haploinsufficiency in 22q11.2 DS can not be supported. In the setting of diminished 22q11.2 gene dosage, shared molecular functions, convergence on cellular processes, and related consequences on the genetic level point to the matrix or multigenic interactions which translate into the multiplicity of phenotypes [120]. All these genetic factors, together with age-related developing symptomatology, contribute to diagnostic challenges in 22q11.2 DS pediatric patients on the diverse individual, family, social, and population levels. The summary of modifying variants influencing the TBX1 penetrance and related phenotypic expression is shown in Table 2 (17-19,52,53,103,104,118,120-124).
The diagnosis of 22q11.2 DS has been traditionally based on the recognition of clinical features and cytogenetic testing using the fluorescence in situ hybridization (FISH) technique. FISH is perceived as the golden standard genetic testing method to confirm the diagnosis of microdeletion syndromes. However, poor clinical accuracy, the low confirmatory rate in the screening of suspected microdeletion syndromes, and failure to detect other than the targeted microdeletion are the major drawbacks of this method. FISH is admittedly inexpensive, yet still a highly labor-intensive and time-consuming procedure [125] Importantly, due to a marked clinical variability from minimal to full manifestation in patients with 22q11.2 DS, precision in defining clinical criteria is important for referring patients to perform FISH analysis. Genotype first approach has been therefore proposed and whole genome sequencing as the first line method, with FISH to be used as a confirmation of patient and family screening results [125]. Since FISH alone can not provide a reliable diagnosis of 22q11.2 DS, other diagnostic methods have been developed, such as comparative genomic hybridization (CGH), multiplex ligation-dependent probe amplification (MLPA), multiplex quantitative real-time polymerase chain reaction (qPCR), and high-resolution single-nucleotide polymorphism (SNP) microarray analysis [126]. Although the FISH method is still routinely used in laboratories, MLPA assay has been perceived as an alternative but superior to the FISH technique as it is less costly, less time-consuming, and laborious, and does not require cell cultures. It has been proposed, that a locus-specific approach, using FISH or MLPA assays could be offered to children strongly meeting clinical and dysmorphology criteria for 22q11.2 DS [126,127].
Newborn screening (NBS) for severe combined immunodeficiency (SCID) is identifying a subset of infants with 22q11.2 DS due to T cell lymphopenia and low TREC numbers, and hence, it is not a universally reliable detecting method. Therefore, direct NBS for 22q11.2 DS to recognize affected neonates using the genomic approach with multiplex qPCR assay, targeted to the TBX1 gene within the LCR22A-B region and CRKL within the LCR22C-D region has been elaborated [128].
Whereas postnatal phenotypes have been widely characterized and categorized, prenatal diagnosis of 22q11.2 DS remains challenging due to a low rate of inheritance (10% of cases) and mild unrecognized parental features. Fetal ultrasound imaging may provide information on findings characteristic for 22q11.2 DS, such as polyhydramnios, hypoplasia or aplasia of the fetal thymus, central nervous system anomalies, such as asymmetric ventriculomegaly and dilated cavum septum pellucidum, and rarely, skeletal anomalies, among others bilateral talipes and anomalous vertebrae [129].
The golden standard method for detecting 22q11.2 microdeletions remains first trimester combined screening by chromosomal microarray (CMA), which is performed in invasively obtained prenatal samples, such as chorionic villi and amniotic fluid. An important technical advance in prenatal noninvasive screening for 22q11.2 is cell-free DNA testing [130]. Cell-free DNA fragments present in maternal plasma which derive both from the mother and the embryo as a result of apoptosis of the cytotrophoblast, an external layer of the placenta are used for qualitative and quantitative assays. The fetal fraction is screened for common trisomy and 22q11.2 deletion as well as for other rare trisomies and microdeletions. Targeted technologies, such as single-nucleotide polymorphism (SNP)-based, digital analysis of selected regions (DANSR), and targeted capture enrichment assay (TCEA) technologies as well as genome-wide methodology, massively parallel shotgun sequencing (MPSS) are advanced techniques used in cell-free DNA analysis [130,131,132,133].
Therapeutic Approach
Marked phenotypic variability of 22q11.2 DS is accompanied by a wide scope of immune deficits ranging from mild to moderate T cell lymphopenia in the partial form of DiGeorge syndrome (pDGS) to profound combined T and B cell immunodeficiency in the complete form (cDGS). In the first case, hypoplastic ectopic thymus or microscopic thymic rests are found and successful spontaneous immunocorrection has been reported, whereas the latter case is characterized by complete athymia [134]. In those most severely immunocompromised children, immune reconstitution may be achieved by thymus transplantation providing the ability to produce naive T cells showing a broad T cell receptor repertoire. Another approach to cDGS is T cell-replete hematopoietic stem cell transplantation, yet due to the absence of the thymus, engraftment of post-thymic T cells may result in poor quality of immune reconstitution [135,136]. Although 22q11.2 DS has been perceived as a T cell deficiency, disorders of B cell maturation and reduced numbers and functions in naive, unswitched, and switched memory B cells have also been reported. Humoral immunodeficiency in children with 22q11.2 DS may considerably vary from hypogammaglobulinemia with low all immunoglobulin isotypes and the need to receive immunoglobulin replacement therapy ( approximately 6% and 3% of them, respectively) [95] to low serum IgA or IgM and impaired antigen-specific vaccine response in sporadic cases [137,138]. Despite the vast majority of children with 22q11.2 DS having normal serum immunoglobulin levels, due to the variable degree of cellular immunity impairment, they are susceptible to acute and recurrent infections, among others such as sinusitis, otitis media, mastoiditis, pneumonia, urinary tract infections, and viral infections [139,140]. Important questions are then raised on indications for preventive measures against infections in those children who do not qualify for immunoglobulin replacement therapy but present with T-cell lymphopenia. Antibiotic prophylaxis is indicated for children with 22q11.2 DS, first of all in those with low IgA serum levels and panhypogammaglobulinemia presenting with recurrent respiratory tract infections during epidemic season. The prophylactic regimens include daily or alternate-daily use of amoxicillin or azithromycin and co-trimoxazole in children with advanced T-cell lymphopenia posing the risk of Pneumocystis jiroveci infection [134,140,142].
Active immunization in children with 22q11.2 DS requires optimizing to provide vaccination coverage against vaccine-preventable infections. Live vaccine practices with Bacille Calmette-Guerin (BCG), vaccines against measles-mumps-rubella (MMR), varicella (VAR), and an intranasal live attenuated influenza vaccine (LAIV) are contraindicated in children with this syndrome as T cell lymphopenia makes them susceptible to adverse effects following live immunization (AEFLI). Furthermore, in those children, who due to hypogammaglobulinemia receive immunoglobulin replacement therapy, either intravenously or subcutaneously, live vaccines are inactivated by administered antibodies and thereby are contraindicated. Inactivated vaccines can be safely administered to immunodeficient patients as they do not pose the risk of an uncontrolled spreading of vaccine microorganisms in the patient’s body and they are not inactivated by supplemented immunoglobulins. However, the immune response to vaccines with antigen-specific antibodies and memory B cell generation may be significantly reduced [143].
However, many individuals with 22q11.2 DS with mild to moderate immunosuppression, receive live viral MMR and varicella vaccines despite the known diagnosis and tolerate them well without serious adverse effects [144,145]. Given the risk of natural infection, the benefits of protection following immunizations with live vaccines outweigh the risks of potential AEFLI. To assess the safety of live attenuated vaccines and evaluate the ability to generate an effective immune response in children with 22q11.2 DS, immunological investigations prior to the administration of live vaccines have been proposed [146]. The recommended immunology workup practices include lymphocyte immunophenotyping with the evaluation of total CD3+ T cells, CD4+ T helper cells, CD8+ T cytotoxic cells, and CD3+CD4+CD45RA+CD31+ recent thymic emigrants as well as response to mitogen phytohemagglutinin (PHA). Live vaccines can be safely administered in children showing a total T cell count above 0.5x109/L, cytotoxic T cell count above 0.2x109/L, and a normal response to mitogen [146].
Conclusions
Reports on nationwide studies capturing patients with 22q11.2 DS [89,140,147] stand in contrast to the frequency of the syndrome which has been estimated to occur in approximately from 1:3000 to 1:4000 births and show a remarkable discrepancy between the estimated frequency and the diagnostic rate in 22q11.2 DS. Whereas clinical symptomatology of the syndrome may be heterogeneous and finding the genetic etiology may be arduous due to complex molecular genetics, the role of genetic modifiers, epigenetic, and environmental factors, as well as the influence of mutations on the remaining genes uncovering rare recessive conditions as shown in Table 3 [14,148,149], the clinical diagnosis may be challenging for clinicians. Increased awareness of pediatricians and specialists in different fields of medicine about the broad spectrum of phenotypic features of 22q11.2 DS they may encounter, is therefore, indispensable. Comprehensive multidisciplinary care should be provided to patients with 22q11.2 DS by cardiologists, cardiosurgeons, endocrinologists, laryngologists, neurologists, surgeons, and geneticists, under the clinical immunologist’s supervision [150,151,152].
Author Contributions
ASzP: Conceptualization, methodology, data curation, writing—original draft preparation, review and editing, supervision; ES: data curation, writing– original draft preparation, ZC, AG, TK, MM, MO, PO: writing- original draft preparation (These six authors equally contributed to this work); JB: writing– revision.
Funding
No fundings have been secured for this study.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
All authors declare no existing conflict of interest regarding this manuscript
References
- Cortes-Martin J, Lopez Penuela N, Sanchez-Garcia JC, Montiel-Troya M, Diaz-Rodriguez L, Rodriguez-Blanque R. Deletion syndrome 22q11.2: a systematic review. Children. 2022, 9, 1168. [Google Scholar] [CrossRef] [PubMed]
- Fomin ABF, Pastorino AC, Kim CA, Pereira AC, Carneiro-Sampaio M, Abe Jacob CM. DiGeorge syndrome: a not so rare disease. Clinics. 2010, 65, 865–869. [Google Scholar] [CrossRef] [PubMed]
- Palmer LD, Butcher NJ, Boot E, Hodgkinson KA, Heung T, Chow EWC, et al. Elucidating the diagnostic odyssey of 22q11.2 deletion syndrome. Am J Med Genet. 2018, 176, 936–944. [Google Scholar] [CrossRef] [PubMed]
- Kersseboom R, Brooks A, Weemaes C. Educational paper: Syndromic forms of primary immunodeficiency. Eur J Pediatr. 2011, 170, 295–308. [Google Scholar] [CrossRef] [PubMed]
- Demaret Bardou ML, Teixeira Henriques M, Sevciovic Grumach A. Inborn errors of immunity associated with characteristic phenotypes. J Pediatr. 2021, 97, 75–83. [Google Scholar] [CrossRef] [PubMed]
- Szczawińska-Popłonyk A, Begier K, Dorota A, Dąbrowska M, Gałecka D, Wawrzeniak K, Wróblewski K. Syndromic immunodeficiencies: a pediatrician’s perspective on selected diseases. Allergol Immunopathol. 2020, 49, 117–136. [Google Scholar]
- Hsu P, Ma A, Wilson G, Williams M, Curotta J, Munns CF, et al. CHARGE syndrome: a Review. J Paediatr Child Health. 2014, 50, 504–511.
- Trider CL, Arra-Robar A, van Ravensvaaij-Arts C, Blake K. Developing a CHARGE syndrome checklist: Health supervision across the lifespan (from head to toe). Am J Med. Genet. 2017, 173A, 684–691. [Google Scholar]
- Szczawińska-Popłonyk A, Popłonyk N, Niedziela M, Sowińska-Seidler A, Sztromwasser P, Jamsheer A, Obara-Moszyńska M. Case report: The cardio-facio-cutaneous syndrome due to a novel germline mutation in MAP2K1: a multifaceted disease with immunodeficiency and short stature. Front Pediatr. 2022, 10, 990111. [Google Scholar] [CrossRef]
- Pierpont ME, Magoulas PL, Adi S, Kavamura MI, Neri G, Noonan J, et al. Cardio-facio-cutaneous syndrome: clinical features, diagnosis and management guidelines. Pediatrics. 2014, 134, 1149–1162. [Google Scholar] [CrossRef]
- Bucciol G, Pillay B, Casas-Martin J, Delafontaine S, Proesmans M, Lorent N, et al. Systemic inflammation and myelofibrosis in a patient with Takenouchi-Kosaki syndrome due to CDC42 Tyr64Cys mutation. J Clin Immunol. 2020, 40, 567–570. [Google Scholar] [CrossRef]
- Martinelli S, Crumbach OHF, Pantaleoni F, Coppola S, Amin E, Pannone L, et al. Functional dysregulation of CDC42 causes diverse developmental phenotypes. Am J Hum Genet. 2018, 102, 309–320. [Google Scholar] [CrossRef]
- Kobrynski LJ, Sullivan KE. Velocardiofacial syndrome, DiGeorge syndrome: the chromosome 22q11.2 deletion syndrome. Lancet. 2007, 370, 1443–1452. [Google Scholar] [CrossRef]
- McDonald-McGinn DM, Sullivan KE, Marino B, Philip N, Swillen A, Vorstman JAS, et al. 22q11.2 deletion syndrome. Nat Rev Dis Primers. 2016, 1, 15071. [Google Scholar]
- Gavril EC, Popescu R, Nuca I, Ciobanu CG, Butnariu LI, Rusu C, et al. Different types of deletions created by low-copy repeats sequences location in 22q11.2 deletion syndrome: Genotype-phenotype correlation. Genes. 2022, 13, 2083. [Google Scholar] [CrossRef] [PubMed]
- Burnside, RD. 22q11.21 deletion syndromes: A Review of proximal, central, and distal deletions and their associated features. Cytogenet Genet Res 2015;146:89-99. [CrossRef]
- Funato, N. Craniofacial phenotypes and genetics of DiGeorge syndrome. J Dev Biol. 2022, 10, 18. [Google Scholar] [CrossRef] [PubMed]
- Gao S, Moreno M, Eliason S, Cao H, Li X, Yu W, et al. TBX1 protein interactions and microRNA-96-5 regulation controls cell proliferation during craniofacial and dental development: Implications for 22q11.2 deletion syndrome. Hum Mol Genet. 2015, 24, 2330–2348. [Google Scholar] [CrossRef] [PubMed]
- Du Q, de la Morena MT, Van Oers NSC. The genetics and epigenetics of 22q11.2 deletion syndrome. Front Genet. 2020, 10, 1365. [Google Scholar] [CrossRef]
- Rooney K, Levy MA, Haghshenas S, Kerkhof J, Rogaia D, Tedesco MG, et al. Identification of a DNA methylation episignature in the 22q11.2 deletion syndrome. Int J Mol Sci. 2021, 22, 8611. [Google Scholar] [CrossRef] [PubMed]
- Costain G, Chow EW, Silversides CK, Basset AS. Sex differences in reproductive fitness contribute to preferential maternal transmission of 22q11.2 deletions. J Med Genet. 2011, 48, 819–824. [Google Scholar] [CrossRef]
- Van L, Heung T, Graffi J, Ng E, Malecki S, Van Mil S, et al. All-cause mortality and survival in adults with 22q11.2 deletion syndrome. Genet Med. 2019, 21, 2328–2335. [Google Scholar] [CrossRef] [PubMed]
- Palmer LD, McManus Z, Heung T, McAlpine G, Blagojevic C, Corral M, et al. Reproductive outcomes in adults with 22q11.2 deletion syndrome. Genes. 2022, 23, 2126. [Google Scholar]
- Kruszka P, Addissie YA, McGinn DE, Porras AR, Biggs E, Share M, et al. 22q11.2 deletion syndrome in diverse populations. Am J Med Genet. 2017, 173, 879–888. [Google Scholar] [CrossRef] [PubMed]
- Mc Donald-McGinn, D. 22q11.2 deletion syndrome: a tiny piece leading to a big picture. Nat Rev Dis Primers. 2020, 6, 33. [Google Scholar] [CrossRef] [PubMed]
- Jackson O, Crowley TB, Sharkus R, Smith R, Jeong S, Solot C, et al. Palatal evaluation and treatment in 22q11.2 deletion syndrome. Am J Med Genet A. 2019, 179, 1184–1195. [Google Scholar] [CrossRef]
- Seselgyte R, Swan MC, Birch MJ, Kangesu L. Velopharyngeal incompetence in children with 22q11.2 deletion syndrome: velar and pharyngeal dimensions. J Craniofac Surg. 2021, 32, 578–580. [Google Scholar] [CrossRef]
- Claynen I, Engchuan W, Hestand MS, Heung T, Holleman AM, Johnston HR, et al. Genetic contributors to risk of schizophrenia in the presence of a 22q.11.2 deletion syndrome. Mol Psychiatry. 2021, 26, 4496–4510. [Google Scholar] [CrossRef]
- Van L, Boot E, Basset AS. Update on the 22q11.2 deletion syndrome and its relevance to schizophrenia. Curr Opin Psychiatry. 2017, 30, 191–196. [Google Scholar] [CrossRef]
- Putotto C, Pugnaloni F, Unolt M, Maiolo S, Trezzi M, Digilio MC, et al. 22q11.2 deletion syndrome: impact of genetics on the treatment of conotruncal heart defects. Children. 2022, 9, 722.
- Calcagni G, Pugnaloni F, Digilio MC, Unolt M, Putotto C, Niceta M, et al. Cardiac defects and genetic syndromes: old incertainities and new insights. Genes. 2021, 12, 1047. [Google Scholar] [CrossRef]
- Goldmuntz, E. 22q11.2 deletion syndrome and congenital heart disease. Am J Med Genet. 2020, 184, 64–72. [Google Scholar] [CrossRef] [PubMed]
- Tan M, Wang X, Liu H, Peng X, Yang Y, Yu H, et al. Genetic diagnostic yield and novel causal genes of congenital heart disease. Front Genet. 2022, 13, 941364. [Google Scholar] [CrossRef] [PubMed]
- Schindewolf E, Khalek N, Johnson MP, Gebb J, Coleman B, Crowley TB, et al. Expanding the fetal phenotype: prenatal sonographic findings and perinatal outcomes in a cohort of patients with a confirmed 22q11.2 deletion syndrome. Am J Med Genet. 2018, 176, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- McDonald R, Dodgen A, Goyal S, Gossett JM, Shinkawa T, Uppu S. C., et al. Impact of 22q11.2 deletion on the postoperative course of children after cardiac surgery. Pediatr Cardiol. 2013, 34, 341–347. [Google Scholar] [CrossRef]
- Cuturilo G, Drakulic D, Jovanovic I, Ilic S, Kalanj J, Vulicevic I, et al. The impact of 22q11.2 microdeletion on cardiac surgery postoperative outcome. Pediatr Cardiol. 2017, 38, 1680–1685. [Google Scholar] [CrossRef] [PubMed]
- Lewyllie A, Roosenboom J, Indecleeft K, Claes P, Swillen A, Devriendt K, et al. A comprehensive craniofacial study of 22q11.2 deletion syndrome. J Dent Res. 2017, 96, 1386–1391. [Google Scholar] [CrossRef] [PubMed]
- AlQarbi MA, Alharbi A, Merdad L. Dental management of a patient with 22q11.2 deletion syndrome (22q11.2DS). BMJ Case Rep. 2018, 2018, bcr2018225765. [Google Scholar]
- Wong DH, Rajan S, Hallett KB, Manton DJ. Medical and dental characteristics of children with 22q11.2 deletion syndrome at the Royal Children’s Hospital, Melbourne. Int J Paediatr Dent. 2021, 31, 682–690. [Google Scholar] [CrossRef]
- Cardenas-Nieto D, Forero-Castro M, Esteban-Perez C, Martinez-Lozano J, Briceno-Balcazar I. The 22q11.2 microdeletion in pediatric patients with cleft lip, palate, or both and congenital heart disease: a systematic review. J Pediatr Genet. 2020, 9, 1–8.
- Kirschner RE, Baylis AL. Surgical considerations in 22q11.2 deletion syndrome. Clin Plast Surg. 2014, 41, 271–272. [Google Scholar] [CrossRef]
- Failla S, You P, Rajakumar C, Dworschak-Stokan A, Doyle PC, Husein M. Characteristics of velopharyngeal dysfunction in 22q11.2 deletion syndrome: a retrospective case-control study. J Otolaryngol Head Neck Surg. 2020, 49, 54. [Google Scholar] [CrossRef]
- Abe Y, Hirade T, Koike D, Matama C, Kato F. Laryngeal web with 22q11.2 deletion syndrome. Int J Pediatr Adolesc Med. 2022, 9, 182–184. [Google Scholar] [CrossRef]
- Komasińska P, Szczawińska-Popłonyk A, Jończyk-Potoczna K, Bręborowicz A. Congenital atresia of the larynx and esophagus in a girl with 22q11.2 deletion—a case report. Polish J Pediatr. 2017, 92, 335–341. [Google Scholar]
- Hankey PB, Ghulmiyyah J, Yeh HW, Tracey N, Arganbright J. Airway anomalies in patients with 22q11.2 deletion syndrome: a scoping review. Int J Pediatr Otorhinolaryngol. 2022, 163, 11373.
- Verheij E, Speleman L, Mink van der Molen AB, Thomeer HGXM. Congenital respiratory tract disorders in 22q11.2 deletion syndrome. Int J Pediatr Otorhinolaryngol. 2018, 104, 1–4. [Google Scholar] [CrossRef] [PubMed]
- Huang RY, Shapiro NL. Structural airway anomalies in patients with DiGeorge syndrome: a current review. Am J Otolaryngol. 2000, 21, 326–330. [Google Scholar] [CrossRef] [PubMed]
- Ebert B, Morrell N, Zavala H, Chinnadurai S, Tibesar R, Barnett Roby B. Percutaneous enteral feeding in patients with 22q11.2 deletion syndrome. Cleft Palate Craniofac. 2022, 59, 121–125. [Google Scholar] [CrossRef] [PubMed]
- Unolt M, Versacci P, Anaclerio S, Lambiase C, Calgagni G, Trezzi M, et al. Congenital heart diseases and cardiovascular abnormalities in 22q11.2 deletion syndrome: From well-established knowledge to new frontiers. Am J Med Genet. 2018, 176, 2087–2098.
- Yi JJ, Tang SX, McDonald-McGinn DM, Calkins ME, Whinna DA, Souders MC, et al. Contribution of congenital heart disease to neuropsychiatric outcome in school-age children with 22q11.2 deletion syndrome. Am J Med Genet B Neuropsychiatr Genet 2014, 165B, 137–147.
- Rayannavat A, Levitt Katz LE, Crowley TB, Lessig M, Grand K, Goldmuntz E, et al. Association of hypocalcemia with congenital heart disease in 22q11.2 deletion syndrome. Am J Med. Genet A. 2018, 176, 2099–2103. [Google Scholar] [CrossRef]
- Zhao Y, Diacou A, Johnston HR, Mousfee FI, McDonald-McGinn DM, McGinn D, et al. Complete sequence of the 22q11.2 allele in 1,053 subjects with 22q11.2 deletion syndrome reveals modifiers of conotruncal heart defects. Am J Hum Genet. 2020, 106, 26–40. [Google Scholar] [CrossRef] [PubMed]
- Mlynarski EE, Xie M, Taylor D, Sheridan MB, Guo T, Racedo SE, et al. Rare copy number variants and congenital heart defects in the 22q11.2 deletion syndrome. Hum Genet. 2016, 135, 273–285. [Google Scholar] [CrossRef]
- Quach TT, Stratton HS, Khanna R, Kolattukudy PE, Honorrat J, Meyer K, et al. Intellectual disability: dendritic anomalies and emerging genetic perspectives. Acta Neuropathol. 2021, 141, 139–158. [Google Scholar] [CrossRef] [PubMed]
- Hopkins SE, Cadehumbe M, Blaine Crowley T, Zackai EH, Bilaniuk LT, McDonald-McGinnDM, et al. Neurologic challenges in 22q11.2 deletion syndrome. Am J Med Genet A. 2018, 176, 2140–2145. [Google Scholar] [CrossRef] [PubMed]
- Bagautdinova J, Zoller D, Schaer M, Padula MC, Mancini V, Schneider M, et al. Altered cortical thickness development in 22q11.2 deletion syndrome and association with psychotic symptoms. Mol Psychiatry. 2021, 26, 7671–7678. [Google Scholar] [CrossRef] [PubMed]
- Mudigoudar B, Nune S, Fulton S, Dayyat E, Wheeless JW. Epilepsy in 22q11.2 deletion syndrome: a case series and literature review. Pediatr Neurol. 2017, 76, 86–90. [Google Scholar] [CrossRef] [PubMed]
- Bayat M, Bayat A. Neurologic manifestations of 22q11.2 deletion syndrome. Neurol Sci. 2022, 43, 1695–1700. [Google Scholar] [CrossRef] [PubMed]
- Osley O, Evans NA, Fernandes-Carriba S, Smearman EL, Rockers K, Morrier MJ, et al. Examining the overlap between autism spectrum disorders and 22q11.2 deletion syndrome. Int J Mol Sci. 2017, 18, 1071. [Google Scholar] [CrossRef]
- Fiksinski AM, Schneider M, Zinstok J, Baribeau D, Chawner SJRA, Vorstman JAS. Neurodevelomental trajectories and psychiatric morbidity: lessons learned from the 22q11.2 deletion syndrome. Curr Psychiatry Rep. 2021, 23, 13. [Google Scholar] [CrossRef]
- Swillen, A. The importance of understanding cognitive trajectories: the case of 22q11.2 deletion syndrome. Curr Opin Psychiatry. 2016, 29, 133–137. [Google Scholar] [CrossRef]
- Biria M, Tomescu MI, Custo A, Cantonas LM, Song KW, Schneider M, et al. Visual processing deficits in 22q11.2 deletion syndrome. Neuroimage Clin. 2017, 17, 976–986. [Google Scholar]
- Francisco AA, Foxe JJ, Horsthuis DJ, DeMaio D, Molholm S. Assessing auditory processing endophenotypes associated with schizophrenia in individuals with 22q11.2 deletion syndrome. Transl Psychiatry. 2020, 10, 85. [Google Scholar] [CrossRef]
- Casteels I, Casaer P, Gewillig M, Swillen A, Devriendt K. Ocular findings in children with a microdeletion in chromosome 22q11.2. Eur J Pediatr. 2008, 167, 751–755. [Google Scholar] [CrossRef]
- Gokturk G, Topcu-Yilmaz P, Bozkurt B, Yildrim MS, Guner SN, Sayar EH, et al. Ocular findings in children with 22q11.2 deletion syndrome. J Pediatr Ophthalmol Strabismus. 2016, 53, 218–222. [Google Scholar] [CrossRef] [PubMed]
- Levy-Shraga Y, Gothelf D, Goichberg Z, Katz U, Somech R, Pinhas-Hamiel O, et al. Growth characteristics and endocrine abnormalities in 22q11.2 deletion syndrome. Am J Med Genet. 2017, 9999, 1–7. [Google Scholar]
- Choi JH, Shin YL, Kim GH, Seo EJ, Kim Y, Park IS, et al. Endocrine manifestations of chromosome 22q11.2 microdeletion syndrome. Horm Res. 2005, 63, 294–299. [Google Scholar]
- Cheung ENM, George SR, Costain GA, Andrade DM, Chow EWC, Silversides CK, et al. Prevalence of hypocalcemia and its associated features in 22q11.2 deletion syndrome. Clin Endocrinol. 2014, 81, 190–196. [Google Scholar] [CrossRef] [PubMed]
- Cheung EN, George SR, Andrade DM, Chow EW, Silversides CK, Bassett AS. Neonatal hypocalcemia, neonatal seizures and intellectual disability in 22q11.2 deletion syndrome. Genet Med. 2014, 16, 40–44. [Google Scholar] [CrossRef] [PubMed]
- Arganbright JM, Tracy M, Feldt M, Narayanan S, Mahadev A, Noel-McDonnell J. Postoperative hypocalcemia following non-cardiac surgical procedures in children with 22q11.2 deletion syndrome. Genes. 2022, 13, 1905. [Google Scholar] [CrossRef]
- Jang C, Ge J, Zhang R, Chen C, Yi L, Shen L, et al. The correlation between severity of postoperative hypocalcemia and perioperative mortality in chromosome 22q11.2 microdeletion (22q11.2DS) patient after cardiac-correction surgery: a retrospective analysis. Heart Surg Forum. 2022, 23, 549–555. [Google Scholar]
- Fujii S, Nakanishi T. Clinical manifestations and frequency of hypocalcemia in 22q11.2 deletion syndrome. Pediatr Int. 2015, 57, 1086–1089. [Google Scholar] [CrossRef] [PubMed]
- Kyritsi EM, Kanaka-Gantenbaum C. Autoimmune thyroide disease in specific genetic syndromes in childhood and adolescence. Front Endocrinol. 2020, 11, 543. [Google Scholar] [CrossRef] [PubMed]
- Ricci S, Sarli WA, Lodi L, Canessa C, Lippi F, Azzari C, et al. Characterization of autoimmune thyroid disease in cohort of 73 pediatric patients affected by 22q11.2 deletion syndrome: longitudinal single-centre study. Genes. 2022, 13, 1552. [Google Scholar] [CrossRef] [PubMed]
- Shugar AI, Shapiro JM, Cytrynbaum C, Hedges S, Weksberg R, Fishman L. An increased prevalence of thyroid disease in children with 22q11.2 deletion syndrome. Am J Med Genet A. 2015, 167, 1560–1564. [Google Scholar] [CrossRef] [PubMed]
- Ueda Y, Uraki S, Inaba H, Nakashima S, Ariyasu H, Iwakura H, et al. Grave’s disease in pediatric and elederly patients with 22q11.2 deletion syndrome. Intern Med. 2017, 56, 1169–1173. [Google Scholar] [CrossRef] [PubMed]
- Brown JJ, Datta V, Browning MJ, Swift PGF. Graves’ disease in DiGeorge syndrome: patient report with a review of endocrine autoimmunity associated with 22q.11.2 deletion. J Pediatr Endocrinol Metab. 2004, 17, 1575–1579. [Google Scholar]
- Stagi S, Lapi E, Gambineri E, Salti R, Genuardi M, Colarusso G, et al. Thyroid function and morphology in subjects with microdeletion of chromosome 22q11 (del(22)q11). Clin Endocrinol. 2010, 72, 839–844. [Google Scholar] [CrossRef]
- Elder DA, Kaiser-Rogers K, Aylsworth AS, Calikoglu AS. Type I diabetes mellitus in a patient with 22q11.2 deletion syndrome. Am J Med. Genet. 2001, 101, 17–19. [Google Scholar] [CrossRef]
- Lima K, Abrahamsen TG, Wolff AB, Husebye E, Alimohammadi M, Kampe O, et al. Hypoparathyroidism and autoimmunity in the 22q11.2 deletion syndrome. Eur J Endocrinol. 2011, 165, 345–352. [Google Scholar] [CrossRef]
- Van L, Heung T, Malecki SL, Fenn C, Tyrer A, Sanches R, et al. 22q11.2 microdeletion and risk for type 2 diabetes. EClinicalMedicine. 2020, 26, 100528. [Google Scholar] [CrossRef]
- Blagojevic C, Heung T, Malecki S, Ying C, Cancelliere S, Hegele RA, et al. Hypertriglyceridemia in young adults with a 22q11.2 microdeletion. Eur J Endocrinol. 2022, 187, 91–99. [Google Scholar] [CrossRef]
- Voll SL, Boot E, Butcher NJ, Cooper S, Heung T, Chow EWC, et al. Obesity in adults with 22q11.2 deletion syndrome. Genet Med. 2017, 19, 204–208. [Google Scholar] [CrossRef]
- Sullivan, KE. Chromosome 22q11.2 deletion syndrome and DiGeorge syndrome. Immunol Rev. 2019, 287, 186–201. [Google Scholar] [CrossRef]
- Gennery, AR. Immunological aspects of 22q11.2 deletion syndrome. Cell Mol Life Sci. 2012, 69, 17–27. [Google Scholar] [CrossRef]
- Dar N, Gothlef D, Korn D, Frisch A, Weizman A, Michaelovsky E, et al. Thymic and bone marrow output in individuals with 22q11.2 deletion syndrome. Pediatr Res. 2015, 77, 579–585. [Google Scholar] [CrossRef]
- Gul KA, Overland T, Osnes L, Baumbusch LO, Pettersen RD, Lima K, et al. Neonatal levels of T-cell receptor excision circles (TREC) in patients with 22q11.2 deletion syndrome and later disease features. J Clin Immunol. 2015, 35, 408–415. [Google Scholar] [CrossRef]
- Collins C, Sharpe E, Silber A, Kulke S, Hsieh EWY. Congenital athymia: genetic etiologies, clinical manifestations, diagnosis, and treatment. J Clin Immunol. 2021, 41, 881–895. [Google Scholar] [CrossRef]
- Guris DI, Duester G, Papaioannou VE, Imamoto A. Dose-dependent interaction of Tbx1 and Crkl and locally aberrant RA signaling in a model of del22q11 syndrome. Dev Cell. 2006, 10, 81–92. [Google Scholar] [CrossRef]
- Shah SS, Lai SY, Ruchelli E, Kazahaya K, Mahboubi S. Retropharyngeal aberrant thymus. Pediatrics. 2001, 108, 94. [Google Scholar] [CrossRef]
- Grudzień K, Kuzaj J, Dębicka M, Kwiatkowski S, Milczarek O. Retropharyngeal ectopic thymus in a pediatric patient with 22q11.2 deletion syndrome. Cureus. 2023, 15, e33350. [Google Scholar]
- Crowley B, Ruffner M, McDonald-Mc Ginn DM, Sullivan KE. Variable immune deficiency related to deletion size in chromosome 22q11.2 deletion syndrome. Am J Med Genet. 2018, 176, 2082–2086. [Google Scholar] [CrossRef]
- Giardino G, Borzacchiello C, De Luca M, Romano R, Prencipe R, Cirillo E, et al. T-cell immunodeficiencies with congenital alterations of thymic development: genes implicated and differential immunological and clinical features. Front Immunol. 2020, 11, 1837. [Google Scholar] [CrossRef]
- Davies, EG. Immunodeficiency in DiGeorge syndrome and options for treating cases with complete athymia. Front Immunol. 2013, 4, 322. [Google Scholar] [CrossRef]
- Patel K, Akhter J, Kobrynski L, Gathmann MA, Davis O, Sullivan KE. Immunoglobulin deficiencies: the B lymphocyte side of DiGeorge syndrome. J Pediatr. 2012, 161, 950–953. [Google Scholar] [CrossRef]
- Zemble R, Luning Prak E, McDonald K, McDonald-McGinn D, Zackai E, Sullivan K. Secondary immunologic consequences in chromosome 22q11.2 deletion syndrome (DiGeorge syndrome/Velocardiofacial syndrome). Clin Immunol. 2010, 136, 409–418. [Google Scholar] [CrossRef]
- Derfalvi B, Maurer K, McDonald-McGinn DM, Zackai E, Meng W, Luning Prak ET, et al. B cell development in chromosome 22q11.2 deletion syndrome. Clin Immunol. 2016, 163, 1–9. [Google Scholar] [CrossRef]
- Montin D, Marolda A, Licciardi F, Robasto F, Di Cesare S, Ricotti E, et al. Immunophenotype anomalies predict the development of autoimmune cytopenia in 22q11.2 deletion syndrome. J Allergy Clin Immunol Pract. 2019, 7, 2369–2376. [Google Scholar] [CrossRef]
- Wahrmann S, Kainulainen L, Kyto V, Lempainen J. Childhood manifestations of 22q11.2 deletion syndrome: a Finnish nationwide register-based cohort study. Acta Paediatr. 2023. epub ahead of print. [CrossRef]
- Di Cesare S, Puliafito P, Ariganello P, Marcovecchio GE, Mandolesi M, Capolino S, et al. Autoimmunity and regulatory T cells in 22q11.2 deletion syndrome patients. Pediatr Allergy Immunol. 2015, 26, 578–594. [Google Scholar]
- Fernando-Martinez S, Lorente R, Gurbindo D, De Jose MA, Leal M, Munoz-Fernandez MA, et al. Low thymic output, peripheral homeostatsis deregulation, and hastened regulatory T cells differentiation in children with 22q11.2 deletion syndrome. J Pediatr. 2014, 164, 882–889. [Google Scholar] [CrossRef]
- Montin D, Marolda A, Licciardi F, Robasto F, Di Cesare S, Ricotti E. Immunophenotype anomalies predict the development of autoimmune cytopenia in 22q11.2 deletion syndrome. J Allergy Clin Immunol Pract. 2019, 7, 2369–2376. [Google Scholar] [CrossRef]
- Pinnaro CT, Henry T, Major HJ, Parida M, DesJardin LE, Manak JR, et al. Candidate modifier genes for immune function in 22q11.2 deletion syndrome. Mol Genet Genomic Med. 2020, 8, e1057. [Google Scholar] [CrossRef]
- Oliveira LM, Teixeira FME, Sato MN. Impact of retinoic acid on immune cells and inflammatory diseases. Mediators Inflamm. 2018, 2018, 3067126. [Google Scholar]
- Cancrini C, Puliafito P, Digilio MC, Soresina A, Martino S, Rondelli R, Consolini R, et al. Clinical features and follow-up in patients with 22q11.2 deletion syndrome. J Pediatr. 2014, 164, 1475–1480. [Google Scholar] [CrossRef]
- Deshpande DR, Demirdag YY, Marsh RA, Sullivan KE, Orange JS. Relationship between severity of T cell lymphopenia and immune dysregulation in patients with DiGeorge syndrome (22q11.2 deletion and/or related TBX1 mutations: a USIDNET study. J Clin Immunol. 2021, 41, 29–37. [Google Scholar] [CrossRef]
- Mahe P, Nagot N, Portales P, Lozano C, Vincent T, Sarda P, et al. Risk factors of clinical dysimmune manifestations in a cohort of 86 children with 22q11.2 deletion syndrome: a retrospective study in France. Am J Med Genet. 2019, 179A, 2207–2213. [Google Scholar]
- Ciano-Petersen NL, Hamad-Cueto O, Drissi-Reyes H, Dona-Diaz A, Garcia-Martin G. Case report: Autoimmune psychosis in 22q11.2 deletion syndrome. Front Immunol. 2021, 12, 708625. [Google Scholar] [CrossRef]
- Jesenak M, Zelieskova M, Repko M, Banovcin P. Successful treatment of severe allergic asthma with omalizumab in a girl with DiGeorge syndrome. Centr Eur J Immunol. 2020, 45, 361–363. [Google Scholar] [CrossRef]
- Morsheimer M, Brown Whitehorn TF, Heimall J, Sullivan KE. The immune deficiency of chromosome 22q11.2 deletion syndrome. Am J Med Genet. 2017, 9999, 1–7. [Google Scholar]
- Maggadottir SM, Sullivan KE. The diverse clinical features of chromosome 22q11.2 deletion syndrome (DiGeorge syndrome). J Allergy Clin Immunol Pract. 2013, 1, 589–594. [Google Scholar] [CrossRef]
- Stevens T, van der Werff Ten Bosch J, De Rademaeker M, Van Den Bogaert A, van den Akker M. Risk of malignancy in 22q11.2 deletion syndrome. Clin Case Rep. 2017, 5, 486–490. [Google Scholar] [CrossRef]
- Itoh S, Ohno T, Kakizaki S, Ichinohasama R. Epstein-Barr virus-positive T-cell lymphoma cells having chromosome 22q11.2 deletion: an autopsy report of DiGeorge syndrome. Hum Patol. 2011, 42, 2037–2041. [Google Scholar] [CrossRef] [PubMed]
- Hong R, Shen V, Rooney C, Hughes DP, Smith C, Comoli P, et al. Correction od DiGeorge anomaly with EBV-induced lymphoma by transplantation of organ-cultured thymus and Epstein Barr-specific cytotixic T lymphocytes. Clin Immunol. 2001, 91, 54–61. [Google Scholar]
- Pongpruttipan T, Cook JR, Reyes-Mugica M, Spahr E, Swerdlow SH. Pulmonary extranodal marginal zone lymphoma of mucosa-associated lymphoid tissue associated with granulomatous inflammation in a child with chromosome 22q11.2 deletion syndrome (DiGeorge syndrome). J Pediatr. 2012, 161, 954–958. [Google Scholar] [CrossRef] [PubMed]
- McDonald-McGinn DM, Reilly A, Wallgren-Pettersson C, Hoyme HE, Yang SP, Adam MP, et al. Malignancy in chromosome 22q11.2 deletion syndrome (DiGeorge syndrome/velocardiofacial syndrome). Am J Med Genet A. 2006, 140, 906–909. [Google Scholar]
- Murray JC, Donahue DJ, Malik SI, Dzurik YB, Braly EZ, Dougherty MJ, et al. Temporal lobe pleomorphic xanthoastrocytoma and acquired BRAF mutation in an adolescent with the constitutional 22q11.2 deletion syndrome. J Neurooncol. 2011, 102, 509–514. [Google Scholar] [CrossRef] [PubMed]
- Digilio MC, Angioni A, De Santis M, Lombardo A, Giannotti A, Dallapicola B, et al. Spectrum of clinical variability in familial deletion 22q11.2: from full manifestation to extremely mild clinical anomalies. Clin Genet. 2003, 63, 308–313. [Google Scholar] [CrossRef] [PubMed]
- Karbarz, M. Consequences of 22q11.2 microdeletion on the genome, individual and population level. Genes. 2020, 11, 977. [Google Scholar] [CrossRef]
- Motahari Z, Moody SA, Maynard TM, LaMantia AS. In the line-up: deleted genes associated with DiGeorge/22q11.2 deletion syndrome: are they all suspects? J Neurodev Disord. 2019, 11, 7. [Google Scholar] [CrossRef]
- Giacomelli M, Kumar R, Soresina A, Tamassia N, Lorenzini T, Moratto D, et al. Reduction of CRKL expression in patients with partial DiGeorege syndrome is associated with impairment of T cell functions. J Allergy Clin Immunol. 2016, 138, 229–240. [Google Scholar] [CrossRef]
- Guo T, Chung JH, Wang T, McDonald-McGinn DM, Kates WR, Hawuła W, et al. Histone modifier genes alter conotruncal heart phenotypes in 22q11.2 deletion syndrome. Am J Hum Genet. 2015, 97, 869–877. [Google Scholar] [CrossRef]
- Leon LE, Benavides F, Espinoza K, Vial C, Alvarez P, Palomares M, et al. Partial microduplication in the histone acetyltransferase complex member KANSL1 is associated with congenital heart defects in 22q11.2 microdeletion syndrome patients. Nature. 2017, 7, 1795. [Google Scholar]
- Mlynarski EE, Sheridan MB, Xie M, Guo T, Racedo SE, McDonald-McGinn DM, et al. Copy-number variation of the glucose transporter gene SLC2A3 and congenital heart defects in the 22q11.2 deletion syndrome. Am J Hum Genet. 2015, 96, 753–764. [Google Scholar] [CrossRef] [PubMed]
- Halder A, Jain M, Chaudhary I, Gupta N, Kabra M. Fluorescence in situ hybridization (FISH) using non-commercial probes in the diagnosis of clically suspected microdeletion syndromes. Indian J Med Res. 2013, 138, 135–142. [Google Scholar]
- Maran S, Faten SA, Lim SHE, Lai KS, Ibrahim WPW, Ankathil R, et al. Screening of 22q11.2 DS using multiplex ligation as alternative diagnostic method. Biomed Res Int. 2020, 6945730. [Google Scholar]
- Monteiro FP, Vieira TP, Sgardioli IC, Molck MC, Damiano AP, Souza J, et al. Defining new guidelines for screening the 22q11.2 deletion based on a clinical and dysmorphologic evaluation of 194 individuals and review of the literature. Eur J Pediatr. 2013, 172, 927–945. [Google Scholar] [CrossRef] [PubMed]
- Barry JC, Blaine Crowley T, Jyonouchi S, Heimall J, Zackai EH, Sullivan KE, et al. Identification of 22q11.2 deletion syndrome via newborn screening for severe combined immunodeficiency. J Clin Immunol. 2017, 37, 476–485. [Google Scholar] [CrossRef] [PubMed]
- Schindewolf E, Khalek N, Johnson MP, Gebb J, Coleman B, Crowlet TB, et al. Expanding the fetal phenotype: prenatal sonographic findings and perinatal outcomes in a cohort of patients with a confirmed 22q11.2 deletion syndrome. Am J Med. Genet A. 2018, 176, 1735–1741. [Google Scholar] [CrossRef] [PubMed]
- Grati FR, Gross SJ. Noninvasive screening by cell-free DNA for 22q11.2 deletion: benefits, limitations, and challenges. Prenat Diagn. 2019, 39, 70–80. [Google Scholar] [CrossRef]
- Bevilacqua E, Jani CC, Chaoui R, Suk EKA, Palma-Dias R, Ko TM, et al. Performance of targeted cell-free DNA prenatal test for 22q11.2 deletion in a large clinical cohort. Ultrasound Obstet Gynecol. 2021, 58, 597–602. [Google Scholar] [CrossRef]
- Dar P, Jacobsson B, Clifton R, Egbert M, Malone F, Wapner RJ, et al. Cell-free DNA screening for prenatal detection of 22q11.2 deletion syndrome. Am J Obstet Gynecol. 2022, 227, 79. [Google Scholar]
- Kagan KO, Hoopmann M, Pfaff T, Prodan N, Wagner P, Schmid M, et al. First trimester screening for common trisomies and microdeletion 22q11.2 syndrome using cell-free DNA: a prospective clinical study. Fetal Diagn Ther. 2020, 47, 841–851. [Google Scholar] [CrossRef] [PubMed]
- Biggs SE, Gilchrist B, May KR. Chromosome 22q11.2 deletion (DiGeorge syndrome): immunologic features, diagnosis, and management. Curr Allergy Asthma Rep. 2023, 23, 213–222. [Google Scholar] [CrossRef] [PubMed]
- Davies, EG. Immunodeficiency in DiGeorge syndrome and options for treating cases with complete athymia. Front Immunol. 2013, 4, 322. [Google Scholar] [CrossRef] [PubMed]
- Davies EG, Cheung M, Gilmour K, Maimaris J, Curry J, Furmanski A, et al. Thymus transplantation for complete DiGeorge syndrome: European experience. J Allergy Clin Immunol. 2017, 140, 1660–1670. [Google Scholar] [CrossRef] [PubMed]
- Caka C, Cimen O, Kahyaoglu, Tezcan I, Cagdas D. Selective IgM deficiency: follow-up and outcome. Pediatr Allergy Immunol. 2021, 32, 1327–1334. [Google Scholar] [CrossRef] [PubMed]
- Kung SJ, Gripp KW, Stephan MJ, Fairchok MP, McGeady SJ. Selective IgM deficiency and 22q11.2 deletion syndrome. Ann Allergy Asthma Immunol. 2007, 99, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Ozen S, Akcal O, Taskirdi I, Haci AI, Karaca NE, et al. 22q11.2 deletion syndrome: 20 years of experience from two pediatric immunology units and review of clues for diagnosis and disease management. Allergol Immunopathol. 2021, 49, 95–100. [Google Scholar] [CrossRef]
- Nissan E, Katz U, Levy-Shraga Y, Frizinsky S, Carmel E, Gothelf D, et al. Clinical features in a large cohort of patients with 22q11.2 deletion syndrome. J Pediatr. 2021, 238, 215–220. [Google Scholar] [CrossRef]
- Habel A, Herriot R, Kumararatne D, Allgrove J, Baker K, Baxendale H, et al. Toward a safety net for management of 22q11.2 deletion syndrome: guidelines for our times. Eur J Pediatr. 2014, 173, 757–765.
- Kuruvilla M, de la Morena MT. Antibiotic prophylaxis in primary immune deficiency disorders. J Allergy Clin Immunol Pract. 2013, 1, 573–582. [Google Scholar] [CrossRef]
- Szczawińska-Popłonyk A, Bręborowicz A, Samara H, Ossowska L, Dworacki G. Impaired antigen-specific immune response to vaccines in children with antibody production defects. Clin Vaccine Immunol. 2015, 22, 875–882. [Google Scholar] [CrossRef] [PubMed]
- Hofstetter AM, Jakob K, Klein NP. , Dekker CL, Edwards KM, Halsey NA, et al. Live vaccine use and safety in DiGeorge syndrome. Pediatrics. 2014, 13, 946–954. [Google Scholar]
- Lim SM, Shin JH, Baek JY, Lee JY, Kang JM, Ahn JG. Safety of live immunization in DiGeorge syndrome: a retrospective single-center study in Korea, 2005-2021. Vaccines. 2022, 10, 2163. [Google Scholar]
- Berkhout A, Preece K, Varghese V, Prasad V, Heussler H, Clark J, et al. Optimising immunisation in children with 22q11 microdeletion. Ther Adv Vaccines Immunother. 2020, 8, 2515135520957139. [Google Scholar]
- Morrow B, McDonald-McGinn DM, Emanuel BS, Vermeesch JR, Scambler PJ. Molecular Genetics of 22.q11.2 deletion syndrome. Am J Med Genet. 2018, 176, 2070–2081. [Google Scholar] [CrossRef] [PubMed]
- Mustillo PJ, Sullivan KE, Chinn IK, Notarangelo LD, Haddad E, Davies EG, et al. Clinical practice guidelines for the immunological management of chromosome 22q11.2 deletion syndrome and other defects in thymic development. J Clin Immunol. 2023, 43, 247–270. [Google Scholar] [CrossRef] [PubMed]
- Cohen JL, Crowley TB, McGinn D, McDougall C, Unolt M, Lambert MC, et al. 22q and two: 22q11.2 deletion syndrome and coexisting conditions. Am J Med Genet. 2018, 176, 2203–2214. [Google Scholar] [CrossRef] [PubMed]
- McGovern PE, Crowley TB, Zackai EH, Burrows E, McDonald-McGinn DM, Nance ML. Surgical insights and management in patients with 22q11.2 deletion syndrome. Pediatr Surg Int. 2022, 38, 899–905. [Google Scholar] [CrossRef]
- Abu-Ghname A, Perdanasari AT, Raj S, Seema J, Wilson KT, Maricevich RS. Access to multidisciplinary care for patients with 22q11.2 deletion syndrome: Identifying breakdowns in the screening process. J Craniofac Surg. 2020, 31, 428–431. [Google Scholar] [CrossRef]
- Boot E, Oskarsdottir S, Loo JCY, Crowley TB, Orchanian-Cheff A, Andrade DM, et al. Updated clinical practice recommendations for managing adults with 22q11.2 deletion syndrome. Genet Med. 2023, 25, 100344. [Google Scholar] [CrossRef]
Figure 1.
The schematic representation of the 22q11.2 region encompassing protein-coding genes, long non-coding RNAs, microRNAs and genes expressed in functional haploinsufficiency in 22q11.2 DS.
Figure 1.
The schematic representation of the 22q11.2 region encompassing protein-coding genes, long non-coding RNAs, microRNAs and genes expressed in functional haploinsufficiency in 22q11.2 DS.
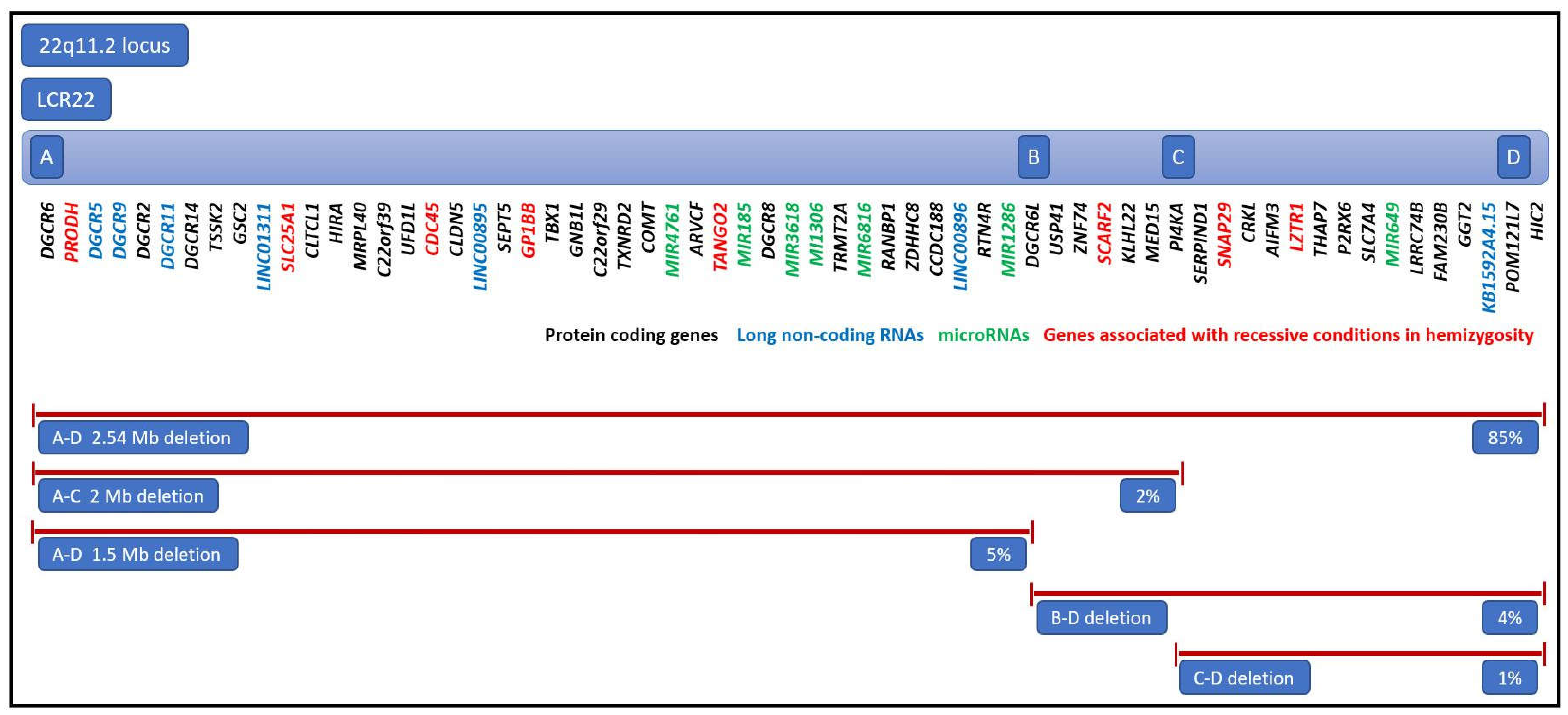

Table 1.
Multisystemic anatomical anomalies and dysfunctions in patients with 22q11.2 deletion syndrome.
Table 1.
Multisystemic anatomical anomalies and dysfunctions in patients with 22q11.2 deletion syndrome.
| Systemic involvement | Phenotypic features | Frequency in 22q11.2 DS |
|---|---|---|
| Facial dysmorphism | Elongated face Hooded eyelids Upslanted palpebral fissures Epicanthus Wide nasal bridge Long nose with a bulbous tip Narrow alar base Short philtrum Small mouth Micrognathia and retrognathia Low-set small ears |
80-99% |
| Ocular findings | Posterior embryotoxon Tortous retinal vessels Refractive errors Strabismus Amblyopia |
7-70% |
| Dentition | Delayed teeth eruption Agenesis of permanent dentition Supernumerary teeth Enamel hypoplasia Impaired enamel calcification |
2.5% |
| Palatal anomalies | Velopharyngeal insufficiency and hypotonia Cleft palate Submucous cleft palate Bifid uvula |
69-100% |
| Laryngeal anomalies | Glottic web Laryngeal stenosis Laryngeal cleft Laryngomalacia Vocal fold anomalies |
25-43% |
| Lower airway anomalies | Tracheo and bronchomalacia Tracheal stenosis Short trachea with reduced tracheal rings Aberrant tracheal bronchus Tracheoesophageal fistula |
21% |
| Cardiovascular anomalies | Interrupted aortic arch type B Truncus arteriosus Tetrealogy of Fallot Conoventricular septal defect Isolated aortic arch anomaly Double outlet right ventricle Transposision of the great arteries Hypoplastic left heart syndrome Valvar pulmonary stenosis |
49-83% |
| Genitourinary anomalies | Renal agenesis Multicystic dysplastic kidney Hydronephrosis Duplicated collecting system Absent uterus Hypospadias, cryptorchidism |
33% |
| Gastrointestinal anomalies | Gastroesophageal reflux Esophageal atresia Impaired swallowing Hirschprung disease Imperforate anus |
30% |
| Central nervous system anomalies | Cerebral atrophy Polymicrogyria Atrophy of the hippocampus Cerebellar atrophy |
8% |
| Endocrine anomalies | Thyroid gland aplasia/hypoplasia Retrocarotid and retroesphageal thyroid extension Inhomogeneous thyroid structure Parathyroid gland dysfunction Growth hormone deficiency |
65% |
| Skeletal and muscular anomalies | Cervical spine anomalies Thoracic vertebral anomalies Arachnodactyly, Camptodactyly, Syndactyly Hammer toes Skull malformations Diaphragmatic hernia |
17-19% |
| Immune disorders | Athymia Thymic hypoplasia Ectopic thymus |
75% |
Table 2.
Genetic modifiers influencing the TBX1 penetrance and affecting the phenotypic expression in 22q11.2 DS.
Table 2.
Genetic modifiers influencing the TBX1 penetrance and affecting the phenotypic expression in 22q11.2 DS.
| Genetic modifier | Role | Phenotypic expression |
|---|---|---|
|
CRKL (CRK like proto-oncogene adaptor protein) |
Activates the RAS and JUN kinase signaling pathways, mediates transduction of intracellular signals | Development of organs originating from the neural crest, thymus, parathyroid glands, craniofacial structures, T lymphocytes, cardiac outflow region |
|
SLC2A3 aka GLUT3 (Solute carrier family 2 member 3) |
Facilitated glucose transporter | Conotruncal heart region, aortic arch |
|
KANSL1 (KAT8 regulatory NSL complex subunit 1) |
Histone acetyltransferase complex member | Developmment of aortic arch, semilunar valve, cardiac septa, pulmonary artery |
|
JMJD1C (jumonji domain containing 1C) |
Chromatin expression modification, histone demethylation | Pharyngeal apparatus, cardiac outflow region |
|
RREB1 (Ras responsive element binding protein 1) |
Chromatin expression modification, histone demethylation | Conotruncal heart region |
|
SEC24C (SEC24 family member C) |
Role in transporting proteins from the endoplasmic reticulum to the Golgi apparatus | Embryonic development, cardiac outflow region |
|
MINA (MYC induced nuclear antigen) |
Chromatin expression modification, histone demethylation | Cardiac development |
|
KDM7A (Lysine-specific demethylase 7A) |
Chromatin expression modification, histone demethylation | Cardiac development |
|
DGCR 8 (DiGeorge syndrome critical region 8) |
miRNAs and lnRNAs regulation | Embryo development, Immune, naurological, and cardiac functions |
|
NCOR2 (Nuclear receptor corepressor 2) |
Transcriptional regulator of the retinoic acid signaling | B and T lymphocytes, regulation of the immune response |
|
EP300 (E1A binding protein P300) |
Transcriptional regulator of the retinoic acid signaling | B and T lymphocytes, regulation of the immune response |
Table 3.
Autosomal recessive conditions resulting from mutations associated with 22q11.2 hemizygosity.
Table 3.
Autosomal recessive conditions resulting from mutations associated with 22q11.2 hemizygosity.
| Gene | Disease | OMIM# | Phenotype |
|---|---|---|---|
| PRODH | Hyperprolinemia type 1 | 239500 | General: neurological deficits Specific: psychomotor delay, hypotonia, and seizures |
| SLC25A1 | D2A2AD syndrome | 615182 | General: severe muscular weakness, respiratory distress, failed psychomotor development, early death Specific: encephalopathy, seizures |
| GP1BB | Bernard-Soulier syndrome | 231200 | Specific: hematologic disease, thrombocytopenia, increased megakaryocytes |
| SCARF2 | Van den Ende-Gupta syndrome | 600920 | General: joint dislocations Specific: contractual arachnodactyly, hooked clavicles, and blepharophimosis |
| SNAP29 | CEDNIK syndrome | 609528 | General: neuropathy Specific: cerebral dysgenesis, ichtyosis, and keratoderma |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



