
Submitted:
21 April 2023
Posted:
23 April 2023
You are already at the latest version
Abstract
Migratory movements are a political, social and public health issue on a global scale. Access to sexual and reproductive health services for irregular migrant women (IMW) is a public health issue. The aim of this study is to identify qualitative evidence on IMW's experiences of sexual and reproductive health care in emergency and primary care settings. Methods: meta-synthesis of qualitative studies. Synthesis includes assembling and categorising findings based on the simili-arty in meaning. The search was conducted between January 2010 and June 2022 using PubMed, WOS and CINAHL databases. Results: of 131 articles found in the initial search, only 9 articles met the criteria and were included in the review. Four main themes were established: (1) The need to focus emergency care on sexual and reproductive health, (2) Unsatisfactory clinical experiences, (3) Forced reproduction, (4) Alternating between formal and informal healthcare services. Con-clusions: IMW’s attitudes towards sexual and reproductive health are influenced by culture, ed-ucational level, fear, barriers and the attitude of healthcare providers. Healthcare institutions need to be aware of the IMW’s experiences to understand the specific difficulties they face. IMW call for socially and culturally sensitive health care, cultural mediators, improved communication and safe environments that ensure confidentiality.
Keywords:
irregular migrant women
; metasynthesis
; qualitative data
; public health
1. Introduction
Migratory movements are a major political, social and public health issue on a global scale [1]. The United Nations (UN) defines ‘international migrant’ as a person who has changed their country of habitual residence, distinguishing between short-term migrants (3 months - 1 year) and long-term migrants (≥ 1 year). According to the International Organization for Migration (IOM) the number of international migrants in 2019 reached 271.6 million people (3.5% of the world's population), of which 47.9% were women [2]. Europe has traditionally been a destination for international migrants; in 2019 it received 82.3 million, 51.4% of whom were women [2]. Almost 87 million international migrants were living in Europe in 2020, 16% more than in 2015 [3]. Spain ranked tenth in destinations of international migrants in 2020 with 5.5 million people [4], of which 2.2 million were men and 2.3 million were women [5].
The term irregular migration refers to the movement of people outside the laws, regulations or international agreements governing the entry into or exit from the country of origin, transit or destination [6]. Irregular migrants (IMs) enter a country without legal recourse, documentation or refugee status, and are not authorised to remain [7]. North Africa is a major transit hub and departure point for IMs from the Maghreb and sub-Saharan Africa heading to Europe. Tens of thousands of migrants attempt to reach Europe from North Africa via the Mediterranean routes every yerar [3], fleeing political persecution, armed conflict, climate change or seeking better life opportunities.
European countries must address the health needs of IMs. In Spain, the approval of Royal Decree-Law 16/2012 introduced restrictions on IMs' access to health services [8]. However, the subsequent approval of Royal Decree-Law 7/2018 [9] guaranteed all people in Spanish territory the right to health care regardless of their administrative status. The number of women of foreign origin in Spain has tripled since the beginning of the century, especially women of childbearing age [5]. In 2017, two out of ten children born in Spain were born to foreign mothers (mainly African and especially Moroccan). Foreign women accounted for 31% of hospitalisations for childbirth in 2018, as well as for hospitalisations of children. Providing care to IMs is a challenge for receiving countries, where women and children in particular may have limited access to healthcare services [10]. The high birth rate among these communities leads them to use sexual health, pregnancy and childbirth services more frequently [5].
Irregular migrant women (IMW) experience high-risk sexual encounters and exploitation at various stages of the migration process. IMW are more exposed to sexually transmitted diseases, sexual violence, rape, unwanted pregnancies and unsafe abortions [11]. Providing IMW with access to sexual and reproductive health (SRH) services has become a major public health objective. Several studies have examined this problem on an epidemiological, socio-economic or clinical level [1,12,13]. Understanding the experiences of physicians [14], nurses [15] and healthcare providers in caring for IMW could be important for removing barriers, introducing improvements and developing specific protocols. Likewise, gaining insight into the experiences of accompanied and unaccompanied minors [16], as well as those of IMW in accessing emergency and primary care services is key to improving their care. Although several studies focus on the experiences of IMW [17,18], a synthesis of aggregated data is needed to gain a deeper understanding of the phenomenon [19] in order to guide clinical practice and provide quality care to these women. The research question guiding this review is: What are the experiences of IMW with regard to SRH care in emergency and primary care? The aim of the study is to identify qualitative evidence on IMW's experiences of SRH care in emergency and primary care settings.
2. Materials and Methods
2.1. Design
This is a systematic review and metasynthesis of qualitative studies. The metasynthesis involves assembling and categorising findings based on similarity of meaning, resulting in a set of statements that consolidate and reflect on knowledge in the field. This review follows the ENTREQ (Enhancing Transparency in Reporting the Synthesis of Qualitative Research) guidelines [20].
2.2. Search methods.
PubMed, WOS and CINAHL databases were searched for qualitative studies in English and Spanish, published between 2010 and January 2023. The SPIDER method was used for qualitative research (sample, phenomenon of interest, design, evaluation and type of research) [21]. The terms used to carry out the search were divided into three blocks. The terms "illegal", "irregular", "undocumented" were joined with the Boolean operator "OR". This process was carried out with "migrant", "immigrant", "foreigners", "noncitizen", as well as with "pregnancy", "sexual health", "maternal health", "health care", "reproductive health" and "qualitative research" and "women". After performing these searches separately, they were joined together using the Boolean operator "AND". (((((((migrant) OR immigrant) OR foreigner)) AND (((((undocumented) OR illegal) OR irregular)) OR noncitizen)) AND ((((((pregnancy) OR sexual health) OR Maternal health) OR health care) OR reproductive health) OR health services)) AND ((women) OR human female)) AND ((qualitative research) OR qualitative design). In addition to electronic searches, a manual search of grey literature was carried out.
2.3. Inclusion and exclusion criteria.
Inclusion criteria: IMW who have experienced SRH care in emergency and primary care; qualitative research or mixed methodology articles (phenomenology, ethnography, grounded theory, etc.); complete original research published in English or Spanish between 2010 and 2023. Exclusion criteria: non-primary articles, editorials, opinion pieces or abstracts.
2.4. Results of the search.
A 5-stage selection process was performed: duplicate elimination, title selection, abstract review, full paper review and reference tracking. A total of 131 studies were found; 9 articles fulfilled the inclusion criteria and were included in this review (Figure 1).
2.5. Quality assessment.
Each primary study was assessed using the Joanna Briggs Institute's Qualitative Assessment Rating Instrument (QARI) [22]. The included articles were considered to be of high quality based on their objectives, design, analysis, results, and useful insights into the topic (Table 1). No studies were excluded as a result of the quality assessment. All studies demonstrated clear objectives and appropriate research.
| Keygnaert et al., 2014 |
2.6. Data extraction
All duplicate records were removed. The researchers analysed the selected studies by extracting data on author, year, country, design, sample, age and research topic. It was not necessary to contact authors of primary studies to obtain recommendations. The references of included papers were reviewed.
Data synthesis and analysis
The included studies were analysed thematically. The synthesis was undertaken by (AGV) and verified by (JGM). Two independent reviewers with expertise in IMW and qualitative research verified the results. The thematic synthesis of qualitative data (Table 2) included line-by-line coding, developing descriptive themes and generating themes and sub-themes in three stages [23]:
| STAGE 2 |
2.7. Rigor
To assess the validity of the review we kept structured summaries of each original study. We checked whether emerging findings were transferable to different study contexts, and we tried to distinguish between primary care or emergency care participants. In addition, we looked to see if our synthesis findings could be attributed to a particular group of IMW. Following the thematic synthesis, we examined the studies' contributions to the final analytical themes and recommendations for intervention.
3. Results
The nine qualitative studies comprised a total sample of 179 IMW from Cambodia, Nigeria, Bolivia, Ecuador, Portugal, Brazil, Bangladesh, Dominican Republic, Nigeria, Morocco, Spain, Macedonia, Romania, Bosnia, Albania, Somalia, Afghanistan, Ethiopia and Mexico, aged between 18 and 40 (Table 3). Thematic synthesis is an inductive process in which 4 themes and 9 sub-themes emerged (Table 4).
3.1. The need to focus emergency care on SRH.
Migratory travel under adverse conditions increases the vulnerability of IMW, who can often be victims of physical, psychological and sexual violence. It is necessary to implement emergency care protocols focused on these women’s SRH and on the physical and psychological traumas they suffer. Healthcare professionals need to know how to intervene and therefore require specific training on SRH.
3.1.1. IMW: victims of trafficking and sexual exploitation.
During the migration process, IMW are handed over to human trafficking networks that use them as bargaining chips for border crossings, bribes and exchanges. When IMW arrive in the country of destination with physical, psychological or social problems, the emergency care they are provided should specifically cover SRH and safety. This care not only includes physical, obstetric and gynaecological assessment, but also the recognition of scars, bruises or tattoos indicative of violence and trafficking. As one participant says, specific screening is needed to address their physical health, and to ascertain whether they are victims of human trafficking or covert prostitution.
“They come and rape you for days and when it suits them, they leave you there, bleeding... and you have to get on with the journey as best you can" [10]
3.1.2. The need to develop suitable safety protocols.
The migration journey has consequences for IMW that need to be understood by healthcare providers. IMW are often distrustful and depressed with fragile and unpredictable states of mind. Alongisde the health care they are provided, IMW also need reassurance, respect and time, which means developing culturally adapted care protocols. IMW arrive with concerns for their health and that of their children, as well as for the families they have left behind in Africa. The mafia often prostitute IMW on their arrival in Europe by coercing them with threats to their families. IMW need healthcare protocols to be implemented that focus on both SRH and their safety.
“Who is protecting my baby? Who is protecting my family?” [10]
IMW are particularly exposed during all phases of the migration process and reach emergency care feeling exhausted, fearful and unsafe. They may have suffered rape, genital mutilation, backstreet abortions, or received informal care for SRH problems, thus increasing their risk of having health issues. The prevention and follow-up of STIs should also be emphasised as a key issue to be taken into account in primary healthcare settings.
3.2. Unsatisfactory clinical experiences.
The clinical studies on healthcare providers reveal a lack of awareness and training when dealing or interacting with IMW. These women often have little information and are unaware of their rights to legal residence permits, building links with local communities and the provision of healthcare services etc. These needs are not always addressed by healthcare providers, and when they are, they are not adapted to their culture.
3.2.1. The need for interpreters.
Most IMW do not speak the language of the host country, which hinders communication and the clinical assessment of SRH. This communication barrier, along with a lack of information, heightens IMW’s perception of being vulnerable and unable to access care. They sometimes referred to a lack of control, a fear of not being understood and an inability to understand healthcare professionals’ recommendations. IMW’s perception of being misled and ignored leads them to feel distrustful and unsafe. They believe that the healthcare professionals treat them differently to others, which worsens the therapeutic relationship.
"I rang the bell several times asking for help, I was worried that something was wrong with the baby who was screaming and screaming. After a long time, the staff came in and said something incomprehensible in Swedish, then they left and did not come back.” [24]
The inadequate explanation of medical procedures that IMW undergo, such as first trimester risk assessment for trisomy, leads to feelings of confusion, fear, misunderstanding, anxiety and even denial. This is how one IMW explains it:
“She (the physician) didn't explain what the test would be like properly; I thought it was the one with the needle, so I said no.” [18]
3.2.2. Healthcare providers’ lack of cultural competence.
IMW can feel rejected when attending emergency or primary care services. Healthcare providers are often cagey and unempathetic, which leads IMW to feel insecure. Some healthcare professionals expressed concerns about the undocumented status of IMW, reflecting their lack of cultural competence in providing care. This leads to feelings of fear, rejection and discrimination. IMW feel that healthcare professionals normalise significant health conditions they present, do not listen to them and doubt what they are telling them, which makes them more concerned about their situation. An IMW who went to the emergency room due to a premature rupture of membranes stated:
"They claimed it was not amniotic fluid, but rather I had urinated on myself. I said I had already given birth to four children. I know the difference between urine and amniotic fluid. They never looked at the amniotic fluid and never performed a cardiotocography. The fluid and blood continued to leak out over the next week.” [18]
3.3. Forced reproduction.
Many IMW undertake the migratory journey while pregnant; they get pregnant either by their partner or through rape and sexual abuse. This problem is compounded by not using contraception, abortions in precarious circumstances or the use of informal health resources. IMW lack knowledge about sexually transmitted diseases and have little control over their pregnancies, which increases complications in pregnancy, childbirth or abortions.
3.3.1. Practices that put the IMW’s personal health at risk.
IMW's knowledge of sexually transmitted diseases is conditioned by the level of education they received in their country of origin. They have heard of potential risks but do not gauge how serious they are. They sometimes have unprotected sex, even with their partners, and often consent to risky sexual practices out of obligation, sometimes in exchange for protection and food. IMW sex workers are often unable to access resources to prevent sexually transmitted infections.
“HIV and cancer are diseases… in my eyes, HIV is the worst” [25]
IMW often do not have access to contraception and complain that it is not provided by healthcare personnel. However, there is also a cultural factor as they may refuse to use contraception out of tradition. On the contrary, they may use it and hide it from their partners or family, who would not accept such a practice. IMW can also be uninformed on the topic so they may use any method they are aware of despite its unreliability. This is what one woman related:
"For example, I used the calendar method as contraception. For a year and a half, I only used the calendar method for contraception " [1]
3.3.2. Pregnancies characterised by IMW’s irregular status.
Pregnant IMW live in fear of having their irregular status discovered; they seek perinatal care later than others, have fewer home visits, spend fewer days in hospital and make fewer visits to healthcare centres. This leads to increased risks during pregnancy and complications in childbirth, such as foetal distress, excessive bleeding or premature births. In addition, if IMW have not experienced complications in previous births, they do not believe they will have problems with the rest, and therefore deal with them in the same way.
"With my two children I always started going to the gynaecologist after 6 months of pregnancy. With the other one I went at eight months and I had no problems with my son. I said to myself ‘I can have my daughter without anyone needing to care for me'." [17]
The language barrier is present in the health care they are provided throughout the postpartum and childbirth period, which reduces the quality of care. Due to their culture and origin, IMW are afraid and are not aware of all of the pregnancy monitoring methods available. Consequently, they tend to seek fewer obstetric and gynaecological check-ups during their pregnancies. This is how one IMW put it:
“The doctor might check the baby and put the instruments inside the baby, which could accidentally damage it and cause a miscarriage.” [18]
Moreover, IMW fear losing their jobs if they become pregnant. They often choose to hide their pregnancies during the first few months and go to healthcare services much later, this increasing the potential risks.
"I got pregnant and was working at the time. I said: ... 'The lady will fire me because she doesn't want me to work.’ So I didn't say anything to the lady.” [18]
3.3.3. Unsafe sex life.
In the face of financial hardship, IMW find themselves forced to have sex with unknown men. They do this as a sign of gratitude or payment for taking care of them, but it is actually prostitution in disguise. These sexual relations are usually unprotected and nonconsensual. Depending on the culture of origin, men may be having sex with several women at the same time and usually do not want to use contraception. This situation increases the risk for IMW:
“I asked my partner to use condoms, but he said that masculinity should be felt and left free, not tied to a condom. And he told me that he would leave with his other girlfriends and I should find another partner.” [11]
In the case of sex workers, this is a very common situation. They may get used to treating themselves at the first sign of symptoms, an issue that also concerns their partners.
“No, I don't use protection with my boyfriend' (sex worker). If it itches you can use antibiotics or preventative gels..." [24]
3.4. Alternating between formal and informal healthcare services.
The IMW's Irregular status limits their ability to access public health services. IMW are more afraid of deportation than suffering from a serious illness. Moreover, their beliefs about SRH are influenced by their cultural backgrounds.
3.4.1. Access to information and care.
To access information about SRH, IMW often seek advice from family, friends and neighbours. They claim that doctors do not understand them and will not understand their conditions. When faced with SRH problems, going to primary care is not their first option. They lack knowledge and have misconceptions about their health and different conditions. Furthermore, their illegal status is a source of stress for them as they fear being deported. Barkensjö's (2018) article shows how access to public health care for IMW is not always easy.
“They said they couldn't do anything because I don’t have papers,'you're undocumented', after sitting there for 10 hours.... We felt ignored and drove home.” [24]
IMW perceive a severe lack of information, do not feel that their wishes are listened to or respected, and they even argue that they may be forced into childbirth at the instruction of healthcare professionals. They generally believe that their opinion is not taken into account by healthcare providers when it comes to making decisions or undergoing risky interventions.
"No one listened to my wishes. I was forced to have a vaginal delivery, regardless of my pre-existing risks." [26]
IMW also feel that they are not taken seriously, and that they are not treated or given the same amount of time as other women.
"It was really challenging, I was in labour for two days. The doctors came, the interns came, the nurses came, they kept coming, but they didn't treat me." [26].
3.4.2. Unsafe abortions.
Unsafe abortions lead to gynaecological complications and severe dangers for IMW. However, the women themselves underestimate the risks of this practice, that is exacerbated by the beliefs, culture and tradition of their countries of origin. Some IMW claim that contraception causes infertility, so despite the risk, they turn to untrained midwives or take advice from other IMW in similar situations.
“If I ever notice I miss my period in the first month, I will start clenching and banging my stomach very hard. I will work hard physically, I will jump and massage myself. I will drink a lot of herbal water. If I start early, I will be able to get the baby out easily.” [26]
4. Discussion
The aim of this study is to identify qualitative evidence on IMW's experiences of sexual and reproductive health care in emergency and primary care settings. IMW experience high-risk situations, high rates of physical trauma, extortion, mental illness and lack of medical care during the migration process [27,28]. In addition, violence, robbery, sexual harassment and/or rape make them a very vulnerable group [29]. IMW arriving in Europe in small boats have a history of violence, rape, forced pregnancy, prostitution and/or trafficking [27]. Regularising their status in the destination country improves their perceived rights, freedoms and access to healthcare services.
Emergency care for IMW should include gynaecological examinations and screening for sexual violence and trafficking [10,16]. In primary care, IMW seek consultation on unwanted pregnancies, abortion, family planning, difficulty in obtaining contraception and menstrual irregularity. However, there is low demand for gynaecological examinations [31,32]. The barriers IMW face in accessing emergency and primary care need to be addressed [28]. Furthermore, healthcare providers do not possess sufficient cultural awareness to adapt their practice [7,15]. For IMW to feel respected, it is fundamental that they know their rights [32]. Positive clinical encounters improve their well-being, peace of mind, empowerment and trust in healthcare providers; conversely, negative clinical encounters inflict emotional distress and fear [24]. Screening for sexually transmitted diseases and unintended pregnancies is key; healthcare providers can gain the trust of IMW by accompanying them to hospitals in migrant communities and promoting secondary prevention [33]. Physical assessment protocols are needed in emergency care, along with improved coordination between healthcare providers and law enforcement [1,10].
IMW's concerns about pregnancy, loss of virginity or sexually transmitted infections need to be addressed. IMW turn to unsafe abortion [11] as they may consider it their only option due to financial constraints or cultural bias. IMW have a higher rate of complications during pregnancy, delivery and puerperium [18,26], and seek prenatal care later. This is associated with reduced prenatal home visits and obstetric follow-up [34], use of informal resources due to fear of deportation, job loss and difficulty accessing public health care [24,26,35]. The division of gender roles consigns women to childcare, while men are in charge of decisions about sex, contraception and SRH. This would partly explain the frequency of unwanted pregnancies and the use of unsafe contraception [17], thus reflecting the need to involve male partners in caring for IMW [36].
Migrants with infectious or potentially transmissible diseases have a higher perception of stigma [37]. Safe spaces are needed for IMW care in the resettlement phase [38,39]. Many IMW have undergone genital mutilation and need gynaecological check-ups [40] but are discouraged by their perception of healthcare providers' lack of understanding, as well as their unempathetic and threatening attitudes [41]. Service provision models should include prenatal and gynaecological screening, language support, well-defined care pathways, community participation and involvement of healthcare providers [42]. Screening and follow-ups for sexually transmitted diseases is critical [43]. Young IMW and sex workers face barriers to accessing SRH services [44]. Studies show associations between irregular migration, sexually transmitted diseases [11] and insufficient contraception [17]. Sex workers are aware of STD risks with clients, but not with their partners [45]. They also refuse to use contraception to avoid infertility, resulting in unwanted pregnancies and unsafe abortions [11,24].
IMW have social expectations, cultural norms and limited understanding of SRH [11]; their socioeconomic level in their country of origin is related to making responsible choices [1,45]. These women tend to look for information from their peers or from religious institutions, whereas men prefer to look on the internet. Institutions often do not have information and they are not familiar with the system [1,18,35]. The situation also differs depending on the country; it is easier for IMW to access SRH services in Spain than it is n Switzerland or Lebanon [18,26].
Healthcare providers see an abundance of mental health conditions, a lack of social support, fear and psychological trauma among IMW. Postraumatic stress, depression and anxiety increase the risk of postpartum depression, hence the need to include mental health screening in SRH care [1,10,18,24]. Fear of deportation is also an obstacle for IMW seeking medical care; in countries like Sweden, clearer guidelines for healthcare professionals and IMW are needed [46]. Strategies for improving IMW’s access to care include training professionals, giving IMW access to community volunteers and cultural mediators, and creating an open-door culture for accessing health care [47]. There is also a need to break down language barriers so that IMW can make medical appointments and avoid misunderstandings [10,18,24,35]. Some studies argue that the use of interpreters leads to a lack of confidentiality [18]. Nonethless, this issue needs to be addressed as the language barrier causes stress and misunderstandings, resulting in IMW feeling distrustful, discriminated against and discouraged to return to formal healthcare services [2,35].
5. Conclusions
The harsh migration journey increases the vulnerability of IMW, who are victims of physical, psychological and sexual violence. Safety protocols and emergency/primary care focused on SRH need to be established for IMW. Care includes physical, obstetric and gynaecological assessments, as well as detection of sexual violence and human trafficking. IMW's lack of information increases their perception of risk as they feel deceived and ignored. IMW find themselves forced to have children due to gender issues; men are in control of decisions surrounding reproduction and IMW are often victims of rape and human trafficking. IMW's irregular status can have a negative impact on pregnancy and the associated health checks. When IMW go to healthcare centres regarding STDs or pregnancy, they feel afraid, insecure, neglected, stigmatised and uninformed. Cultural aspects and fear of deportation can be linked to IMW not seeking care and undergoing unsafe abortions. Healthcare providers lack awareness and training surrounding care for IMW. In order to provide competent care, they require specific training in SRH.
Author Contributions
Conceptualization, J.G.M. and A.S.G.V.; methodology, M.M.J.L. and M.D.R.F.; software, G.G.H.; formal analysis, A.F.F. and I.M.F.M.; writing—original draft preparation, A.S.G.V., G.G.H and A.F.F.; writing—review and editing, J.G.M., I.M.F.M. and M.M.J.L.; project administration, M.M.J.L.; funding acquisition, J.G.M.. All authors have read and agreed to the published version of the manuscript.”
Funding
This study has been funded by the General Nursing Council of Spain (PNI_CGE88) and UAL-FEDER (UAL 2020- CTS- D2031). It has had the support of the Health Sciences Research Group [CTS-451] of the University of Almería.
Institutional Review Board Statement
This study not require ethical approval.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Keygnaert, I.; Vettenburg, N.; Roelens, K.; Temmerman, M. Sexual health is dead in my body: Participatory assessment of sexual health determinants by refugees, asylum seekers and undocumented migrants in Belgium and the Netherlands. BMC Public Health 2014, 14, 1–13. [Google Scholar] [CrossRef] [PubMed]
- International Organization of Migration. World Migration Report 2020. Available online: https://publications.iom.int/system/files/pdf/wmr_2020.pdf (accessed on 27 March 2023).
- International Organization of Migration. World Migration Report 2022. Available online: https://publications.iom.int/system/files/pdf/WMR-2022.pdf (accessed on 27 March 2023).
- Instituto Nacional de Estadística (INE) [National Institue of Statistics]. Available online: https://www.ine.es/jaxi/Datos.htm?path=/t20/e245/p08/l0/&file=02005.px (accessed on 27 March 2023).
- Consejo Económico y Social (CES) [Economic and Social Council] (2019). La inmigración en España: Efectos y oportunidades. [Immigration in Spain: Effects and opportunities] Available online:. Available online: https://www.ces.es/documents/10180/5209150/Inf0219.pdf (accessed on 27 March 2023).
- International Organization for Migration. Glossary on Migration. Available online: https://publications.iom.int/system/files/pdf/iml_34_glossary.pdf (accessed on 27th March 2023).
- Granero-Molina, J.; Jiménez-Lasserrrotte, M. D. M.; Fernández-Sola, C.; Hernández-Padilla, J. M.; Sánchez Hernández, F.; López Domene, E. Cultural Issues in the Provision of Emergency Care to Irregular Migrants Who Arrive in Spain by Small Boats. J Transcult Nurs. 2019, 30, 371–379. [Google Scholar] [CrossRef] [PubMed]
- Real Decreto-ley 16/2012, de 20 de abril, de medidas urgentes para garantizar la sostenibilidad del Sistema Nacional de Salud y mejorar la calidad y seguridad de sus prestaciones. [Royal Decree-Law 16/2012, of 20th April, on urgent measures to guarantee the sustainability of the National Health System and improve the quality and safety of its services.] Available online:. Available online: https://www.boe.es/buscar/pdf/2012/BOE-A-2012-5403-consolidado.pdf (accessed on 27 March 2023).
- Real Decreto-ley 7/2018, de 27 de julio, sobre el acceso universal al Sistema Nacional de Salud. [Royal Decree-Law 7/2018, of 27th July, on universal access to the National Health System.] Available online:. Available online: https://www.boe.es/boe/dias/2018/07/30/pdfs/BOE-A-2018-10752.pdf (accessed on 27 March 2023).
- López-Domene, E.; Granero-Molina, J.; Fernández-Sola, C.; Hernández-Padilla, J. M.; López-Rodríguez, M.M.; Fernández-Medina, I. M. , Guerra-Martín, M. D., Jiménez-Lasserrrotte, M. M. Emergency care for women irregular migrants who arrive in spain by small boat: A qualitative study. Int J Environ Res Public Health, 2019, 16(18). [CrossRef]
- Hegde, S.; Hoban, E.; Nevill, A. Unsafe abortion as a birth control method: Maternal mortality risks among unmarried Cambodian migrant women on the Thai-Cambodia border. Asia Pac J Public Health, 2012, 24, 989–1001. [CrossRef]
- Chiarenza, A.; Dauvrin, M.; Chiesa, V.; Baatout, S.; Verrept, H. Supporting access to healthcare for refugees and migrants in European countries under particular migratory pressure. BMC Health Serv Res, 2019, 19, 1–14. [CrossRef]
- Gustafsson, C. (2018). “For a better life …“A study on migration and health in Nicaragua.’ Glob Health Action, 2018, 11, 1428467. [CrossRef]
- Granero-Molina, J.; Jiménez-Lasserrotte, M.D.M.; Ruiz-Fernández, M.D.; Hernández-Padilla, J.M.; Fernández-Medina, I.M.; López-Rodríguez, M.M. , Fernández-Sola, C. Physicians' experiences of providing emergency care to undocumented migrants arriving in Spain by small boats. Int Emerg Nurs, 2021, 56, 101006. [CrossRef]
- Granero-Molina, J.; Jiménez-Lasserrotte, M.D.M.; Fernández-Medina, I.M.; Ruiz-Fernández, M.D.; Hernández-Padilla, J.M.; Fernández-Sola, C. Nurses' experiences of emergency care for undocumented migrants who travel by boats. Int Nurs Rev. 2022, 69, 69–79. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Lasserrotte, M.D.M.; López-Domene, E. ; Fernández-Sol,a C.; Hernández-Padilla, J.M.; Fernández-Medina, I.M.; Granero-Molina J. Accompanied child irregular migrants who arrive to Spain in small boats: Experiences and health needs. Glob Public Health, 2020a, 15, 345-357. [CrossRef]
- Barona-Vilar, C.; Más-Pons, R.; Fullana-Montoro, A.; Giner-Monfort, J.; Grau-Muñoz, A.; Bisbal-Sanz, J. Perceptions and experiences of parenthood and maternal health care among Latin American women living in Spain: A qualitative study. Midwifery, 2013, 29, 332–337. [CrossRef]
- Sami, J.; Lötscher, K. C. Q.; Eperon, I.; Gonik, L.; De Tejada, B. M.; Epiney, M.; Schmidt, N. C. Giving birth in Switzerland: A qualitative study exploring migrant women’s experiences during pregnancy and childbirth in Geneva and Zurich usingfocus groups. Reprod Health, 2019, 16, 1–9. [CrossRef]
- Florczak, K. L. In the Zeal to Synthesize: A Call for Congruency. Nurs Sci Q, 2013, 26, 220–225. [CrossRef]
- Tong, A.; Sainsbury, P.; Craig, J. Consolidated criteria for reporting qualitative research (COREQ): A 32-item checklist for interviews and focus groups. Int J Qual Health Care, 2007, 19, 349–357. [CrossRef]
- Cooke, A.; Smith, D.; Booth, A. Beyond PICO: The SPIDER tool for qualitative evidence synthesis. Qual Health Res, 2012, 22, 1435–1443. [CrossRef]
- Joanna Briggs Institute. (2020). Checklist for qualitative research. Available online: https://jbi.global/critical-appraisal-tools (accessed on 28 March 2023).
- Thomas, J.; Harden, A. Methods for the thematic synthesis of qualitative research in systematic reviews. BMC Med Res Methodol, 2008, 8, 45. [CrossRef]
- Barkensjö, M.; Greenbrook, J. T. V; Rosenlundh, J.; Ascher, H.; Elden, H. The need for trust and safety inducing encounters: a qualitative exploration of women's experiences of seeking perinatal care when living as undocumented migrants in Sweden. BMC Pregnancy Childbirth, 2018, 18, 217. [CrossRef]
- Coma, N.; Mejía-Lancheros, C.; Berenguera, A. Pujol-Ribera, E. Risk perception of sexually transmitted infections and HIV in Nigerian commercial sex workers in Barcelona: a qualitative study. BMJ Open, 2015, 5:e006928. [CrossRef]
- Fernandez, B. Health inequities faced by Ethiopian migrant domestic workers in Lebanon. Health Place, 2018, 50, 154–161. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Lasserrotte, M. D. M. , López-Domene, E., Hernández-Padilla, J. M., Fernández-Sola, C., Fernández-Medina, I. M., Faqyr, K. E. M. E., Dobarrio-Sanz, I., & Granero-Molina, J. Understanding Violence against Women Irregular Migrants Who Arrive in Spain in Small Boats. Healthcare (Basel, Switzerland), 2020, 8, 299. [CrossRef]
- Pottie, K.; Martin, J. P.; Cornish, S.; Biorklund, L.M.; Gayton, I.; Doerner, F. Schneider, F. Access to healthcare for the most vulnerable migrants: a humanitarian crisis. Conflict health, 2015; Volume 9, p. 16. [CrossRef]
- Matose, T.; Maviza, G.; Nunu, W. N. Pervasive irregular migration and the vulnerabilities of irregular female migrants at Plumtree border post in Zimbabwe. J Migr Health, 2022; 5, 100091. [Google Scholar] [CrossRef]
- Agadjanian, V.; Oh, B.; Menjívar, C. ). (Il) legality and psychosocial well-being: Central Asian migrant women in Russia. J Eth Migr Stud, 2022, 48, 53–73. [CrossRef]
- Mamuk, R.; Şahin, N. H. Reproductive health issues of undocumented migrant women living in Istanbul. Eur J Contracep Reprod Health Care, 2021, 26, 202–208. [CrossRef]
- Bahamondes, L.; Laporte, M.; Margatho, D.; de Amorim, H. S. F.; Brasil, C.; Charles, C. M.; Becerra, A.; Hidalgo, M. M. Maternal health among Venezuelan women migrants at the border of Brazil. BMC Public Health, 2020, 20, 1771. [CrossRef]
- Marti Castaner, M.; Slagstad, C.; Damm Nielsen, S.; Skovdal, M. Tactics employed by healthcare providers in the humanitarian sector to meet the sexual and reproductive healthcare needs of undocumented migrant women in Denmark: A qualitative study. Sex Reprod Healthc, 2022. 34. [CrossRef]
- Funge, J. K.; Boye, M. C.; Parellada, C. B.; Norredam, M. Demographic characteristics, medical needs and utilisation of antenatal Care among pregnant undocumented migrants living in Denmark between 2011 and 2017. Scand J Public Health, 2022, 50, 575–583. [CrossRef]
- Deeb-Sossa, N.; Olavarrieta, C. D.; Juárez-Ramírez, C.; García, S. G.; Villalobos, A. Experiences of undocumented Mexican migrant women when accessing sexual and reproductive health services in California, USA: a case study. Cad Saude Publica, 2013, 29, 981–991. [CrossRef]
- Mengesha, Z. B.; Perz, J.; Dune, T.; Ussher, J. Refugee and migrant women's engagement with sexual and reproductive health care in Australia: A socio-ecological analysis of health care professional perspectives. PloS one, 2017, 12, e0181421. [Google Scholar] [CrossRef] [PubMed]
- Ndumbi, P.; Del Romero, J.; Pulido, F.; Velasco, M.; Dronda, F.; Blanco, J. R.; García, P.; Ocaña, I.; Belda-Ibañez, J. , Del Amo, J.; … Barriers to health care services for migrants living with HIV in Spain. Eur J Public Health, 2018, 28, 451–457. [CrossRef]
- Zimmerman, C.; Hossain, M.; Watts, C. Human trafficking and health: a conceptual model to inform policy, intervention and research. Soc Sci Med, 2011, 73, 327–335. [CrossRef]
- Metusela, C.; Ussher, J.; Perz, J.; Hawkey, A.; Morrow, M.; Narchal, R.; Estoesta, J.; Monteiro, M. "In My Culture, We Don't Know Anything About That": Sexual and Reproductive Health of Migrant and Refugee Women. Int J Behav Med, 2017, 24, 836–845. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Linares, J. M.; López-Entrambasaguas, O. M.; Fernández-Medina, I. M.; Berthe-Kone, O.; Fernández-Sola, C.; Jiménez-Lasserrotte, M.D.M.; Hernández-Padilla, J.M.; Canet-Vélez, O. Lived experiences and opinions of women of sub-Saharan origin on female genital mutilation: A phenomenological study. J Clin Nurs, 2022, 10.1111/jocn.16294. [CrossRef]
- González-Timoneda, A.; González-Timoneda, M.; Cano, A.; Ruiz, V. Female Genital Mutilation Consequences and Healthcare Received among Migrant Women: A Phenomenological Qualitative Study. Int J Environ Res Public Health, 2021, 18(13), 7195. [CrossRef]
- Evans, C.; Tweheyo, R.; McGarry, J.; Eldridge, J.; Albert, J.; Nkoyo, V.; Higginbottom, G. Improving care for women and girls who have undergone female genital mutilation/cutting: qualitative systematic reviews. NIHR Journals Library, 2019. [CrossRef]
- Visalli, G.; Facciolà, A.; Carnuccio, S. M.; Cristiano, P.; D'Andrea, G.; Picerno, I.; Di Pietro, A. Health conditions of migrants landed in north-eastern Sicily and perception of health risks of the resident population. Public health, 2020. 185, 394–399. [CrossRef]
- Garbett, A.; de Oliveira, N. C.; Riggirozzi, P.; Neal, S. The paradox of choice in the sexual and reproductive health and rights challenges of south-south migrant girls and women in Central America and Mexico: A scoping review of the literature. J Migr Health, 2022, 7, 100143. [CrossRef]
- Auli, N. C.; Mejía-Lancheros, C.; Berenguera, A.; Pujol-Ribera, E. Risk perception of sexually transmitted infections and HIV in Nigerian commercial sex workers in Barcelona: A qualitative study. BMJ Open, 2015, 5. [CrossRef]
- Mona, H.; Andersson, L. M. C.; Hjern, A.; Ascher, H. Barriers to accessing health care among undocumented migrants in Sweden - a principal component analysis. BMC Health Serv Res, 2021, 21, 830. [CrossRef]
- Serre-Delcor, N.; Oliveira, I.; Moreno, R.; Treviño, B.; Hajdók, E.; Esteban, E.; Muri-as-Closas, A.; Denial, A.; Evangelidou, S. A Cross-Sectional Survey on Profes-sionals to Assess Health Needs of Newly Arrived Migrants in Spain. Front Public Health, 2021. 9, 667251. [CrossRef]
Figure 1.
Flowchart.
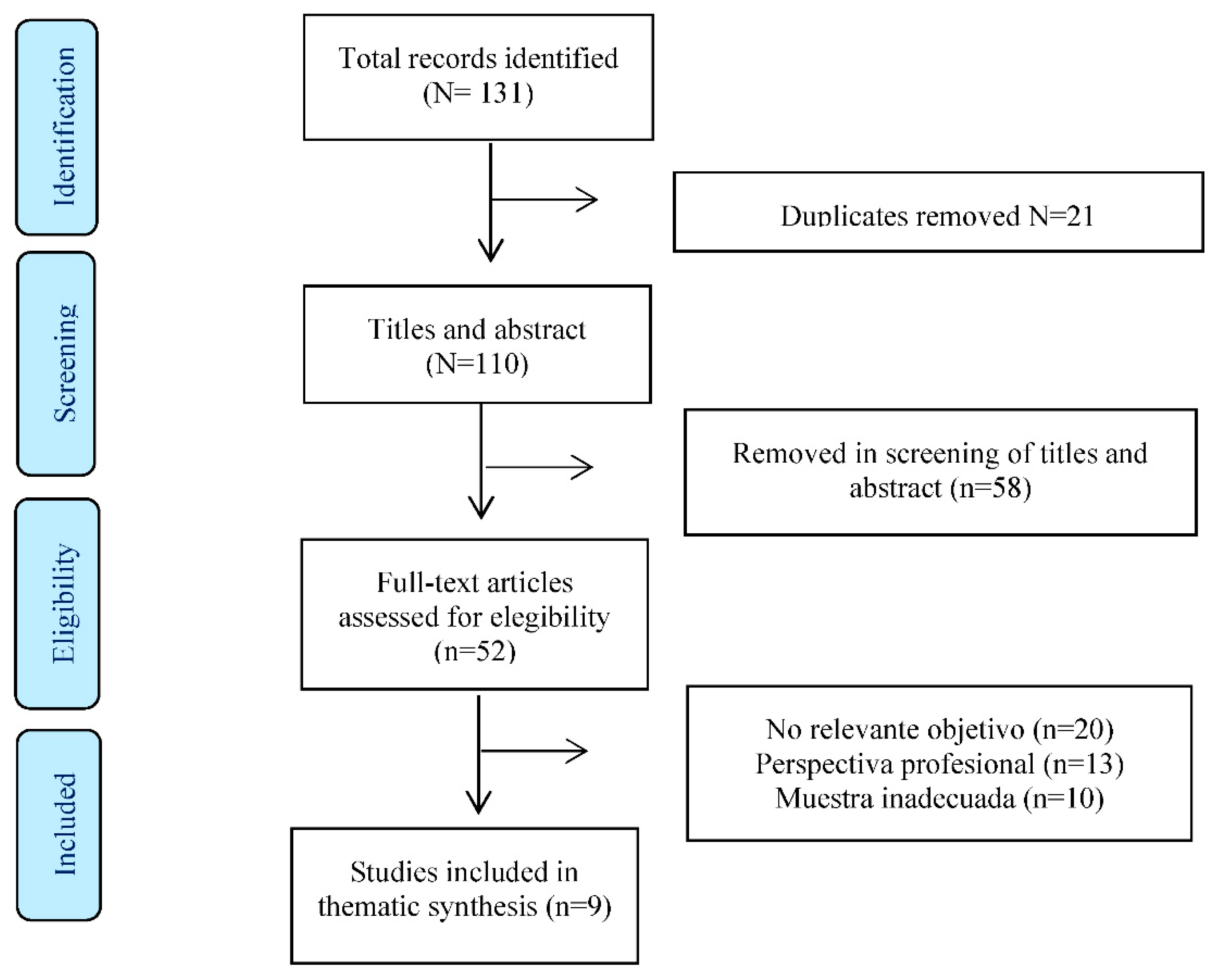

Table 1.
Evaluation of the quaality of the studies [22].
Table 1.
Evaluation of the quaality of the studies [22].
| Article | 1 | 2 | 3 | 4 | 5 | 6 | 7 | 8 | 9 | 10 |
|---|---|---|---|---|---|---|---|---|---|---|
| Hedge et al, 2012 | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ | ✔ |
| Keygnaert et al., 2014 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| Auli et al., 2015 | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ | ✔ |
| Barona-Vilar et al., 2013 | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ↔ | ✔ |
| Sami et al., 2019 | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ | ✔ |
| López-Domene et al., 2019 | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ | ✔ |
| Barkensjö et al., 2018 | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ↔ | ✔ | ✔ | ✔ |
| Fernández, 2018 | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ | ✔ |
| Deeb-Sossa et al., 2013 | ✔ | ✔ | ✔ | ✔ | ✔ | ↔ | ✔ | ✔ | ✔ | ✔ |
* ✔ Yes, ↔ Unclear, ✘ No. 1. Congruence of philosophical perspective/methodology 2. Congruence of methodology/objectives 3. Congruence of methodology/data collection 4. Congruence of methodology/data analysis 5. Congruence of methodology/interpretation of results 6. Cultural and theoretical context of the researcher. 7. Influence of the researcher on the research 8. Participants represented. Research Ethics Committee Approval 10. Conclusions from data analysis/interpretation.
Table 2.
Stages in the thematic synthesis process [23].
Table 2.
Stages in the thematic synthesis process [23].
| Stage | Description | Steps |
|---|---|---|
| STAGE 1 | Text coding | Recall review question Read/re-read findings of the studies Line-by-line inductive coding Review of codes in relation to the text |
| STAGE 2 | Development of descriptive themes | Search for similarities/differences between codes Inductive generation of new codes Write preliminary and final report |
| STAGE 3 | Development of analytica themes | Inductive analysis of sub-themes Individual/independent analysis Pooling and group review |
Table 3.
Characteristics of the chosen studies.
| Author and year | Country | Sample (IMW) | Age (years) | Interview duration | Data collection |
Data analisys |
Main Theme |
|---|---|---|---|---|---|---|---|
| Hegde et al.,2012 | Cambodia | 15 | 18-28 | Not interviewed | IDI | Manual analysis of codede data | Attitudes /practice of unsafe abortions |
| Auli et al., 2015 | Spain | 8 | 23-40 | 30 min. | IDI | Content analysis | Risk of STIs and HIV in sex workers |
| Barona-Vilar et al., 2013) | Spain | 26 | 20-35 | 3 h. | FGs | Thematic analyss | IMW’s experiences of maternity care |
| Sami et al., 2019 | Switzerland | 33 | 21-40 | Not interviewed | FGs | Analysis of themes and subthemes | Experiences of maternal health services |
| López-Domene et a., 2019 | Spain | 13 | 18-35 | 18 min. | IDI | Valerie Fleming stages | IMW’s health needs |
| Barkensjö et al., 2018 | Sweden | 13 | 18-36 | 45 min | IDI | Qualitative analysis of content | Clincial experiences of birth/pregnancy |
| Fernández, 2018 | Lebanon | 35 | Not provided | 1 h. | IDI | Ethnographic analysis of themes | Unequal access to care for IMW |
| Deeb-Sossa et al., 2013 | United States | 8 | 20-45 | Not interviewed | Life story | Analysis of statements | Cultural needs and access restrictions |
| Keygnaert et al., 2014 | Belgium Netherlands |
14 | 15-49 | Not interviewed | IDI | Inductive analysis | Sexual health determinants |
IMW= irregular migrant women. IDI:= in-depth interview. FGs=focus groups.
Table 4.
Themes, subthemes and codes.
| Themes | Subthemes |
|---|---|
| 3.1 The need to focus emergency care on SRH | 3.1.1 IMW: victims of trafficking and sexual exploitation. |
| 3.1.2 The need to develop suitable safety protocols. | |
| 3.2. Unsatisfactory clinical experiences | 3.2.1 The need for interpreters. |
| 3.2.2 Healthcare providers’ lack of cultural competence. | |
| 3.3 Forced reproduction | 3.3.1 Practices that put the IMW’s personal health at risk. |
| 3.3.2 Pregnancies characterised by the IMW’s irregular status. | |
| 3.3.3 Unsafe sex life. | |
| 3.4 Alternating between formal and informal healthcare services. | 3.4.1 Access to information and care. |
| 3.4.2 Unsafe abortions. |
SRH= Sexual and reproductive Health. IMW= Irregular Migrant Women
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



