Submitted:
23 May 2023
Posted:
25 May 2023
Read the latest preprint version here
Abstract
Aims: Multidisciplinary diabetic foot clinics have been shown to be an effective therapeutic model for reducing major amputations and mortality rates. The aim of this article is to assess the economic impact of the implementation of a multidisciplinary diabetic foot clinic in a hospital in Barcelona, Spain. Methods: Observational cost-benefit study of all subjects with diabetes admitted with the diagnosis of a major amputation due to diabetic foot from 2010 to 2020. Direct and indirect costs were compared before and after the introduction of the multidisciplinary diabetic foot clinic. Results: The individual cost per patient with diabetic foot was €14,768 before the implementation of the unit. After the implementation of the clinic, the expected cost was reduced to €5,985 due to a 40% reduction in the probability of hospitalization. Overall, the implementation of the clinic resulted in cost savings per patient valued at €8,783, of which, €7,165 are related to hospital benefits. Conclusion: The results of this analysis contributes to the evidence suggesting that multidisciplinary diabetic foot clinics are cost-effective, by demonstrating that they have a positive impact on patient health while also reducing the utilization of healthcare resources.
Keywords:
Multidisciplinary pain clinic
; Diabetic foot
; Amputation
; Foot ulcer
; Diabetes Mellitus
; Economic evaluation
; Cost Benefit Analysis
1. INTRODUCTION
The incidence of diabetes mellitus (DM) has increased dramatically over the last 30 years [1] with an estimated global adult prevalence of 9.3% in 2019 [2]. With this rising incidence, complications associated with it are also growing, being diabetic foot (DF) the leading cause of hospitalization among these patients [3].
DF is defined by the International Working Group on the Diabetic Foot (IWGDF) as “an infection, ulceration, or destruction of tissues of the foot of a person with currently or previously diagnosed DM, often accompanied by neuropathy and/or peripheral artery disease in the lower extremity” [4]. A 2019 meta-analysis found that the global prevalence of DF was 6.3%, with higher rates reported in males and people suffering from type 2 diabetes (T2D) [5]. It is estimated that 15% of DM patients will develop a lower extremity ulcer during the course of their illness and a majority of them will require amputation [3].
Diabetes and DF represent a major global burden for patients and the healthcare system. Diverse studies have assessed the economic impact of DF across different countries and populations. In Canada, a DF ulcer admission can cost up to $22,754 [6], while in the United States, the estimated cost of DF is up to $28,000 per patient per year [3]. In Spain, the cost rises up to €15,235-€16,765 if amputation is needed, without considering indirect costs [7].
In recent years, evidence has shown that reductions in major amputations [8] and mortality [9] in patients with DF can be achieved with multidisciplinary diabetic foot clinics (MDFC). This approach is now the recommended model to treat these patients by the IWGDF [4]. Moreover, MDFCs have been shown to reduce the costs of treatment and improve patient outcomes [10].
Despite the positive impact of introducing MDFCs, it has not been thoroughly assessed in the context of Spain. In this context, the present analysis aims to assess the economic impact of establishing an MDFC in a tertiary hospital in Barcelona, Spain.
2. MATERIAL AND METHODS
2.1. Study design
This is a retrospective observational cost-benefit study of all subjects with the diagnosis of a major amputation due to diabetic foot from 2010 to 2020 admitted to the Germans Trias i Pujol University Hospital, a publicly-owned tertiary care center in Barcelona, Spain. The study compares the direct and indirect costs of DF before and after the introduction of the multidisciplinary diabetic foot clinic. The study considers the probability of patients with DF visiting the emergency room, requiring hospitalization, or attending outpatient clinics. The follow up period under study was one year.
2.2. Health care setting
The Catalan health system provides publicly financed universal health coverage that is free at the point of access, ensuring that everyone who lives in Catalonia has the right to receive healthcare. The system operates under a mixed health model funded through taxes, with equal access to a wide range of benefits offered by a single publicly available network of health resources, not all of which are publicly owned. The healthcare network includes a range of organizations, such as public corporations, foundations, non-for-profit organizations and health consortiums, which have historically provided healthcare [11]. Approximately, one in three individuals in Catalonia has additional private health insurance, which does not affect their right to access public healthcare services.
2.3. Circuit of a patient with diabetic foot before and after the multidisciplinary diabetic foot clinic implementation
Before the implementation of the multidisciplinary diabetic foot clinic at Germans Trias i Pujol Hospital, patients with DF were evaluated at their Primary Care center by a General Practitioner (GP). According to the severity of their ulcer(s), they were referred to the vascular or plastic surgeon outpatient clinic or to the emergency room. If hospital admission was required, the vascular surgeon team was usually in charge and in some cases the plastic surgery team. If the patient presented a poor metabolic control, a consultation with the endocrinology service was made. After discharge, the vascular surgeon would oversee the patient’s follow-up care (Figure 1).
The MDFC began its activity in January 2015 and comprises a team of medical professionals, including an endocrinologist, podiatrist, vascular surgeon, plastic surgeon, infectious disease specialist, trauma surgeon, radiologist, dietician, rehabilitation physician, and a specialist in hospital at home unit. As part of this unit, a diabetic foot clinic (DFC) was created as an outpatient clinic where the vascular surgeon and podiatrist assess the patients together. The remaining members of the team work together with an integrated treatment clinical protocol during the whole care process. In this new healthcare model, patients are also evaluated at their primary care center, but they are usually referred to the DFC for further evaluation and treatment of their lesions. Depending on the severity of the condition, the patient may require hospital admission or follow-up care at the outpatient DFC. In cases where hospital admission is necessary, patients are assigned a room in the endocrinology ward and are evaluated by various members of the medical team. The endocrinologist evaluates the patient’s diabetic control, diabetic systemic complications and prescribes medical treatment accordingly. They are also in charge of coordinating the activity among the rest of the specialties involved in evaluating the patient. The podiatrist and vascular surgeon work as a team assessing the lesion and deciding its treatment, which may include revascularization, surgical debridement, and minor or major amputation. In some cases, a consultation with a trauma surgeon may be necessary. The podiatrist is also responsible for optimizing the use of orthotic equipment. Specific antibiotic treatment and the evaluation of other infectious diseases that the patient may present are assessed by the infectious disease specialist. The plastic surgery service is involved in cases where reconstruction surgery is necessary. According to the wound evolution and the necessity of long-term antibiotic treatment, patients are evaluated by the hospital at home unit (HaHU). A weekly clinical session is held where all specialists participate to decide patients’ management and treatments of particularly challenging cases. In these meetings, a radiologist specialist is present for reviewing all the imaging procedures. After discharge, the patient’s follow-up is made in the DFC, in the endocrinology outpatient clinic and by the HaHU if needed (Figure 1).
2.4. Cost analysis
To assess the impact of the multidisciplinary diabetic foot clinic on costs, both direct and indirect costs before and after its introduction have been estimated, measured in monetary units (euros 2019) and without including a discount rate. The average costs per patient have been obtained by considering the costs associated with emergency room visits, outpatient clinic visits and diabetic foot clinic visits, as well as hospitalization in the ward or intensive care unit (ICU) [12]. The cost of amputation has been approximated by taking the mean value of the cost of below-knee amputation (€2,856) and above-knee amputation (€3,044) performed in the generic surgical block. The value for society associated with the loss of work productivity of a hospitalized patient has been calculated by determining the gross daily salary for patients below retirement age and adjusting it for their age group and corresponding unemployment rate [13-14]. The cost of antibiotics is calculated based on the mean cost of the medication that a DF patient requires during the hospitalization, according to a reference study [15]. Finally, to quantify the monetary value associated with the increase in morbidity caused by amputation, the decrease in 0.29 quality-adjusted life years (QALY) [16] and the social value associated with each QALY in Spain (€25,000) [17-18] have been considered (Table 1).
2.5. Statistical methods
To compare the characteristics of the patients before and after the introduction of the unit, a chi-square test was used for categorical variables and a t-student test for continuous ones. In both cases, statistically significant differences were considered if their p-value was less than 0.01 (two-sided). The analysis followed the Consolidated Health Economic Evaluation Reporting Standards [19].
The study was conducted according to the guidelines of the Declaration of Helsinki. The Ethics Committee of the Germans Trias i Pujol Hospital (protocol code PI-23-064) waived the Ethical review approval for this study as this is a retrospective study on the quality of care which does not require informed consent from the patients. Data was retrieved from the endocrinology service database.
3. RESULTS
3.1. Characteristics of patients with amputations
We analyzed a total of 232 subjects with diabetes who had undergone major amputation. Of these, 150 were admitted before the implementation of the multidisciplinary diabetic foot clinic (2010-2014), while 82 after its implementation (2015-2020) (Table 2). The median age was 71.4 ± 10.7 years and 68% were male, with a mean BMI of 28 ± 6 Kg/m2. Almost all of the patients (96%) had type 2 diabetes, with a mean disease evolution time of 13 years and an HbA1C level of 6.85%. Most were treated with insulin (78%) and oral antidiabetic agents (66%). The majority of patients had other comorbidities such as hypertension, dyslipidemia and Charcot's foot. Most of the patients showed microvascular (65.1% retinopathy, 67.2% nephropathy and 71.3% DF) as well as macrovascular (21.9% stroke, 37% ischemic heart disease and 95.4% peripheral arterial disease) complications (Table 2). There are no significant differences in any of the variables between the two periods.
3.2. In-hospital care characteristics
In the pre-MDFC compared to the MDFC group, 60% vs. 40% of the patients were referred from their GP to the ER department and 40% vs. 20% to vascular or plastic surgery outpatient clinics. In the MDFC group, the remaining 40% were referred to the Diabetic Foot Clinic. The median hospital length of stay was shorter in the MDFC group, with a duration of 10.08 days compared to 14.33 days in the pre-MDFC group. In more than half of the patients (60.40% vs. 52.43%, p=0.302) an above-knee amputation was performed. The main reason for amputation in both groups was an irreversible grade IV obliterative arterial disease (92% vs. 100%, p=0.041). During admission, medical and postsurgical complications were observed in 8.57% and 12.82% of patients in the pre-MDFC and MDFC groups, respectively (p=0.445), mostly due to bleeding and/or dehiscence of the wound or sepsis. Admission to the ICU was required only in two patients (2.59%), in both cases due to septic shock. Antibiotic treatment was administered in over 90% of the episodes. The most used antibiotics in the pre-MDFC group were piperacillin/tazobactam (28.06%), ciprofloxacin (14.04%) and amoxicillin-clavulanic acid (14.04%); and for the MDFC group were piperacillin/tazobactam (25.58%), meropenem (13.95%) and amoxicillin-clavulanic acid (13.95%), with no statistically significant differences between the groups. Re-admission in less than 30 days after discharge was required in 27.33% vs 18.29% of the patients, mainly due to complications related to the surgical wound.
3.3. Estimation of direct and indirect costs
To estimate the direct costs, the expected cost per patient associated with antibiotic use was calculated by multiplying the cost of antibiotics by the probability of a patient being hospitalized (73% pre-MDFC and 34% after). The cost of using the emergency room, outpatient clinic and Diabetic Foot Clinic services was calculated by multiplying the cost of each service by the probability of a patient being referred to each service from primary care (60%, 40% and 0%, respectively, pre-MDFC; and 40%, 20% and 40%, respectively, after). In the same way, the expected cost of ICU admission was calculated by multiplying its cost by the probability of requiring admission (0% pre-MDFC and 2.59% after). Likewise, the cost of hospitalization has been weighted according to the average length of stay for patients with diabetic foot (14.33 pre-MDFC and 10.08 after) and to the probability of urgent readmission within 30 days (27% pre-MDFC and 18% after). Similarly, the expected cost per patient for the surgical amputation was calculated by multiplying the cost of the procedure by the probability of a patient requiring it (39% pre-MDFC and 24% after).
In terms of indirect costs, the loss of productivity was calculated by multiplying the opportunity cost by the average number of days a patient with diabetic foot is hospitalized. Finally, to quantify the morbidity associated with amputation, the decrease in QALYs was multiplied by its associated social value, which was then multiplied by the probability of amputation occurring.
3.4. Total costs per patient
The results suggest that each patient with diabetic foot incurred a cost of €14,768 before the introduction of the unit, mainly due to direct costs (76% of the total cost). More than half corresponds to the cost of hospitalization, while the cost associated with morbidity due to amputation also had a significant impact (20% of the total cost). After launching the unit, the expected cost was reduced to €5,985. In this case, the proportion of direct and indirect costs is more balanced than before (67% direct vs. 33% indirect). This is because the introduction of the unit has significantly reduced the probability of hospitalization by almost 40%, which was the main driver of direct costs. As a result, the weight of hospitalization cost has dropped to 46%, although it still remains one of the main factors contributing to the total cost.
Additionally, the weight of the cost associated with the morbidity caused by amputation is higher after the introduction of the unit (29%). In this case, the cost attributed to the loss of labor productivity during admission is only 4%. Overall, the introduction of the unit has resulted in a cost-saving per patient of €8,783, of which €7,165 corresponds to savings in hospital-related costs (Table 3).
3.5. Sensitivity Analysis
The savings obtained from the MDFC activity are mainly due to the reduction in the probability of hospitalization (73% vs. 34%). To comparatively evaluate the final result, a sensitivity analysis was performed by varying the hospitalization probability assumption by +/-20%. In the first case, the expected cost of hospitalization with the MDFC launch increased by €1,607 and, therefore, the total saving per patient remained positive €6,793. In the second case, the expected cost decreased by the same value and the saving increased to €10,773. The results show that although the probability of hospitalization varies by 20%, the benefits of introducing a MDFC still outweigh the costs.
4. DISCUSSION
The results of this study show that the implementation of a Multidisciplinary Diabetic Foot Clinic in a tertiary hospital reduces the costs associated with the treatment of patients with Diabetic Foot. The cost savings are attributed to an improved health care model with a holistic treatment and, more specifically, to a reduction in the number of hospitalizations and major limb amputations.
In this regard, it is universally accepted and recommended that DF care should be carried out by a multidisciplinary team in order to achieve better results. Accordingly, the Germans Trias i Pujol Hospital established a Multidisciplinary Diabetic Foot Clinic in 2015, in response to the objectives of the Catalan health plan 2016-2020. This plan recommends a 10% reduction in the number of major limb amputations due to DF in individuals with DM [20]. With a prevalence of DM in Spain of almost 15% [21], these reductions in amputations are aligned to reduce costs and improve the quality of health and life of individuals with DM.
On the other hand, the baseline characteristics of our patients are similar to those described in previous literature [6,10,22]. Specifically, those studies that have analyzed the impact of a multidisciplinary diabetic foot clinic on patient outcomes and cost have found that most of the patients had a high degree of systemic diabetes-related disease, particularly of vascular origin. Common pre-existing conditions included peripheral artery disease, ischemic heart disease, chronic kidney disease and hypercholesterolemia [6,10]. Most of our patients had microvascular and macrovascular complications, with peripheral arterial disease being the most common, as expected. Also, the duration of diabetes among our patients (13.4 years) and the type of diabetes were consistent with previous studies [22].
Regarding the costs associated with patients with DF, a Canadian multicenter study found that DF ulcer admission cost was twice higher when compared with the top five most expensive general internal medicine conditions ($22,754 vs. $10,169). Furthermore, when compared to admissions for other diabetes-related complications, the cost of admission for diabetic foot complications was nearly three times higher ($22,754 vs. $8,350) [6]. In the United States, DF is estimated to cost up to $28,000 per patient per year if amputation is required [3]. In Europe, a healed DF ulcer costs €7,147, while the cost rises to €18,790 if healing is not achieved, and up to €24,540 in case of amputation [14]. In Spain, the estimated cost of DF without amputation ranges from €1,465 to €2,301 per year, which increases to €15,235 to €16,765 if amputation is necessary, without including indirect costs [7]. The CODE-2 study (Cost of Diabetes in Europe – Type 2) showed that the average annual healthcare cost per patient with diabetes in Spain had a 1.6-fold increase in patients with microvascular complications, and a 2.3-fold increase in patients with macrovascular complications [23]. In this context, approaches to prevent the health burden of DF-related pathologies seem justified and necessary.
The results obtained in the present study are in line with those obtained in previous research which suggests that the implementation of a MDFC is associated with a reduction in the number of major amputations in individuals with diabetic foot complications [10,24]. A retrospective single-center study conducted in New Zealand found that a MDFC resulted in a 25% median reduction in the cost per wound episode compared to costs prior to implementation (p<0.001 for total and outpatient costs), as well as fewer major amputations (3.8% vs. 27.5%) and lower mortality rates (7.5% vs. 19.2%) [10]. Moreover, the present study not only demonstrates the positive impact of MDFCs on patient health outcomes but also confirms their cost-effectiveness for healthcare provider organizations.
Our study has several limitations. Firstly, the two periods being compared (5 vs. 6 years) and the number of patients included (150 vs. 82) are not identical. Additionally, the COVID-19 pandemic occurred during the latter period, which may have affected the outcomes. Secondly, the coefficients used to estimate the shift in the use of healthcare resources before and after the introduction of the MDFC were based on the experience of the unit's professionals. Thirdly, we assumed that the cost of the DFC is similar to that of other outpatient clinic services in the hospital, although it could be possible that, due to its nature, it could be slightly higher than other services.
Regarding the comparison with similar studies, it should be noted that each MDFC has different characteristics. For example, the team defined by Joret et al. identifies other professional profiles not included in our center, such as a vascular and a diabetic foot nurse specialist [10]. However, our center includes other professionals, such as a radiologist, a plastic surgeon, an infectious disease specialist, and a hospital-at-home specialist. Rinkel, W.D., et al. with a smaller sample size (n=59), does not compare the impact of the MDFC with the previous scenario, but gives detail on the costs associated with each specialist [22]. Both studies consider whether the amputations are minor or major, but they did not consider the impact of productivity loss during admission or the loss of mobility after amputation.
4.1. Conclusions
The present study provides further evidence, in line with previous research conducted in other countries, that MDFCs are a cost-effective intervention with a positive impact on patient health. Furthermore, the findings demonstrate that the implementation of MDFCs in a tertiary hospital located in Catalonia has led to a reduction in the use of healthcare resources.
Author Contributions
All authors had full access to all of the data in this study and took complete responsibility for the integrity of the data and accuracy of the data analysis. All named authors meet the International Committee of Medical Journal Editors (ICMJE) criteria for authorship for this manuscript, take responsibility for the integrity of the work as a whole, and have given final approval for the version to be published.
Funding
No funding or sponsorship was received for this study or publication of this article.
Conflicts of Interest
The authors declare that the research was conducted in the absence of any commercial or financial relationships that could be construed as a potential conflict of interest.
References
- World Health Organization. (16 September 2022). Diabetes. https://www.who.int/news-room/fact-sheets/detail/diabetes.
- Saeedi, P., Petersohn, I., Salpea, P., Malanda, B., Karuranga, S., Unwin, N., ... & IDF Diabetes Atlas Committee. (2019). Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas. Diabetes research and clinical practice, 157, 107843. [CrossRef]
- Nieto-Gil, P., Ortega-Avila, A. B., Pardo-Rios, M., Cobo-Najar, M., Blasco-Garcia, C., & Gijon-Nogueron, G. (2018). Hospitalisation cost of patients with diabetic foot ulcers in valencia (Spain) in the period 2009–2013: a retrospective descriptive analysis. International journal of environmental research and public health, 15(9), 1831. [CrossRef]
- Schaper, N. C., van Netten, J. J., Apelqvist, J., Bus, S. A., Hinchliffe, R. J., Lipsky, B. A., & IWGDF Editorial Board. (2020). Practical guidelines on the prevention and management of diabetic foot disease (IWGDF 2019 update). Diabetes/Metabolism Research and Reviews, 36, e3266. [CrossRef]
- Zhang, P., Lu, J., Jing, Y., Tang, S., Zhu, D., & Bi, Y. (2017). Global epidemiology of diabetic foot ulceration: a systematic review and meta-analysis. Annals of medicine, 49(2), 106-116. [CrossRef]
- Syed, M. H., Salata, K., Hussain, M. A., Zamzam, A., de Mestral, C., Wheatcroft, M., ... & Al-Omran, M. (2020). The economic burden of inpatient diabetic foot ulcers in Toronto, Canada. Vascular, 28(5), 520-529. [CrossRef]
- González, P., Faure, E., & Del Castillo, A. (2006). Coste de la diabetes mellitus en España. Medicina clínica, 127(20), 776-784.
- Wang, C., Mai, L., Yang, C., Liu, D., Sun, K., Song, W., ... & Yan, L. (2016). Reducing major lower extremity amputations after the introduction of a multidisciplinary team in patient with diabetes foot ulcer. BMC endocrine disorders, 16(1), 1-8. [CrossRef]
- Cahn, A., Elishuv, O., & Olshtain-Pops, K. (2014). Establishing a multidisciplinary diabetic foot team in a large tertiary hospital: a workshop. Diabetes/Metabolism Research and Reviews, 30(5), 350-353. [CrossRef]
- Joret, M. O., Osman, K., Dean, A., Cao, C., van der Werf, B., & Bhamidipaty, V. (2019). Multidisciplinary clinics reduce treatment costs and improve patient outcomes in diabetic foot disease. Journal of vascular surgery, 70(3), 806-814. [CrossRef]
- López Seguí, F., Vidal-Alaball, J., Sagarra Castro, M., García-Altés, A., & García Cuyàs, F. (2020). General practitioners’ perceptions of whether teleconsultations reduce the number of face-to-face visits in the Catalan public primary care system: retrospective cross-sectional study. Journal of medical Internet research, 22(3), e14478. [CrossRef]
- Generalitat de Catalunya. Ordre SLT/71/2020, de 2 de juny, per la qual es regulen els supòsits i conceptes facturables i s'aproven els preus públics corresponents als serveis que presta l'Institut Català de la Salut. 2020. Available at: https://cido.diba.cat/legislacio/10263520/ordre-slt712020-de-2-de-juny-per-la-qual-es-regulen-els-suposits-i-conceptes-facturables-i-saproven-els-preus-publics-corresponents-als-serveis-que-presta-linstitut-catala-de-la-salut-departament-de-salut . Accessed 13 Dec 2022.
- Idescat. Annual indicators. Annual gross salary. By sex and age groups. 2019. (2021, July 5). https://www.idescat.cat/indicadors/?id=anuals&n=10400&t=201900.
- Idescat. Indicators of the economic situation. Activity, employment and unemployment rates. By sex and age groups. Q4/2019. (2020, January 28). https://www.idescat.cat/indicadors/?id=conj&n=10218&t=201904.
- Prompers, L., Huijberts, M., Schaper, N., Apelqvist, J., Bakker, K., Edmonds, M., ... & Tennvall, G. R. (2008). Resource utilisation and costs associated with the treatment of diabetic foot ulcers. Prospective data from the Eurodiale Study. Diabetologia, 51, 1826-1834. [CrossRef]
- Jafary, M. R., Amini, M. R., Sanjari, M., Aalaa, M., Goudarzi, Z., Najafpour, Z., & Mohajeri Tehrani, M. R. (2020). Comparison home care service versus hospital-based care in patients with diabetic foot ulcer: an economic evaluation study. Journal of Diabetes & Metabolic Disorders, 19, 445-452. [CrossRef]
- Vallejo-Torres, L., García-Lorenzo, B., & Serrano-Aguilar, P. (2018). Estimating a cost-effectiveness threshold for the Spanish NHS. Health economics, 27(4), 746-761. [CrossRef]
- Vallejo-Torres, L., García-Lorenzo, B., Rivero-Arias, O., & Pinto-Prades, J. L. (2020). The societal monetary value of a QALY associated with EQ-5D-3L health gains. The European Journal of Health Economics, 21(3), 363-379. [CrossRef]
- Husereau, D., Drummond, M., Petrou, S., Carswell, C., Moher, D., Greenberg, D., ... & Loder, E. (2013). Consolidated health economic evaluation reporting standards (CHEERS) statement. International journal of technology assessment in health care, 29(2), 117-122. [CrossRef]
- Generalitat de Catalunya. Departament de Salut. (2016). Pla de Salut de Catalunya 2016-2020: Un sistema centrat en la persona: públic, universal i just. https://www.salutweb.gencat.cat/url/pladesalut.
- Magliano, D., & Boyko, E. J. (2021). IDF Diabetes Atlas (10.a ed.). International Diabetes Federation.
- Rinkel, W. D., Luiten, J., van Dongen, J., Kuppens, B., Van Neck, J. W., Polinder, S., ... & Coert, J. H. (2017). In-hospital costs of diabetic foot disease treated by a multidisciplinary foot team. Diabetes research and clinical practice, 132, 68-78. [CrossRef]
- Mata, M., Antoñanzas, F., Tafalla, M., & Sanz, P. (2002). El coste de la diabetes tipo 2 en España: El estudio CODE-2. Gaceta Sanitaria, 16, 511-520. [CrossRef]
- Nason, G. J., Strapp, H., Kiernan, C., Moore, K., Gibney, J., Feeley, T. M., ... & Tierney, S. (2013). The cost utility of a multi-disciplinary foot protection clinic (MDFPC) in an Irish hospital setting. Irish journal of medical science, 182, 41-45. [CrossRef]
Figure 1.
Circuit of a DF patient before and after the MDFC implementation.
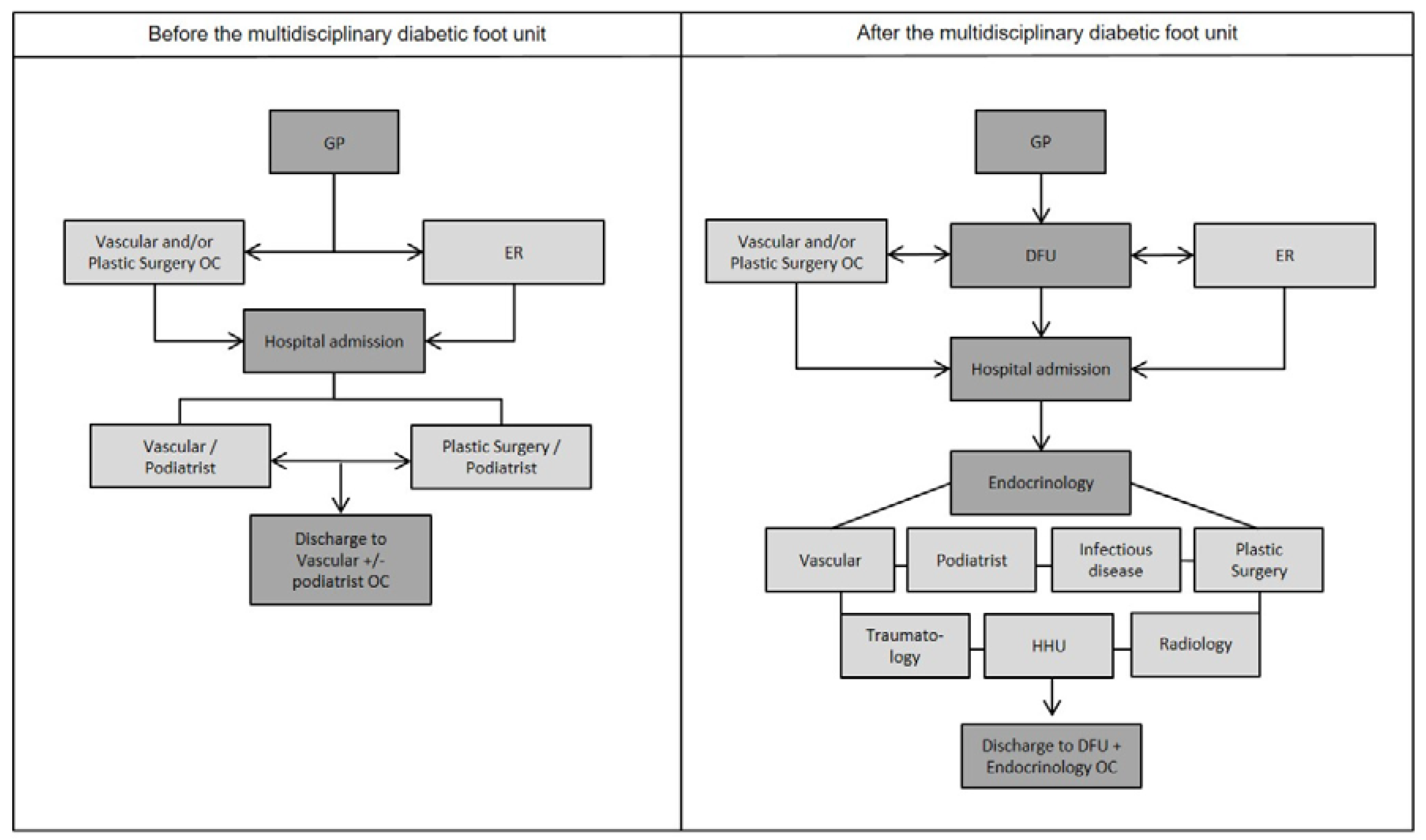

Table 1.
Resource type and associated cost.
| Resource | Cost | Unit |
| Emergency room | €194 | Per visit |
| Outpatient clinic | €77 | Per visit |
| DFC | €77 | Per visit |
| Hospitalization | €674 | Per staying day |
| ICU | €1,037 | Per visit |
| Amputation | €2,950 | Per intervention |
| Median gross patient salary | €71 | Per staying day |
| Antibiotic | €1,197 | Per hospital stay |
| QALY | 0.29 units | Per amputation |
Table 2.
Characteristics of the patients with amputations attended before and after the constitution of the MDFC.
Table 2.
Characteristics of the patients with amputations attended before and after the constitution of the MDFC.
| General | pre-MDFU (n=150) | MDFU (n=82) | p | |
|---|---|---|---|---|
| Age (ye ars, SD) | 71.4 (10.7) | 70.6 (11.12) | 70 (9.98) | 0.673 |
| Men (%) | 68.1 | 62.7 | 78 | 0.024 |
| BMI (kg/m2) (N, SD) | 28.14 (6.01) | 28.81 (6.39) | 27.22 (5.38) | 0.206 |
| T2D (%) | 95.9 | 96.7 | 94.3 | 0.649 |
| Time of evolution of T2D (years, SD) | 13.4 | 12 (8.21) | 15.7 (9.80) | 0.043 |
| HbA1c (%, SD) | 6.85 (1.27) | 6.55 (1.02) | 6.95 (1.34) | 0.259 |
| Nephropathy (%) | 67.2 | 63.5 | 73.9 | 0.186 |
| Retinopathy (%) | 65.1 | 65.5 | 64.3 | 0.982 |
| Diabetic Foot (%) | 71.3 | 72.6 | 70 | 0.843 |
| Ischemic heart disease (%) | 37 | 38.1 | 35.1 | 0.764 |
| Stroke (%) | 21.9 | 22.5 | 20.8 | 0.897 |
| Peripheral arterial disease (%) | 95.4 | 94.4 | 97.4 | 0.491 |
| Charcot foot (%) | 0.9 | 0.7 | 1.3 | 0.759 |
| Oral antidiabetic agents (%) | 65.9 | 71.2 | 56 | 0.037 |
| Insulin (%) | 77.8 | 73.8 | 85.3 | 0.076 |
| Oral antidiabetic agents + insulin (%) | 44.7 | 45.7 | 42.7 | 0.776 |
| Hypertension (%) | 93.1 | 91.4 | 96.1 | 0.297 |
| Dyslypidemia (%) | 73.2 | 71.9 | 75.3 | 0.706 |
Table 3.
Multidisciplinary Diabetic Foot Clinic impact on costs per patient.
| Expected value before MDFC | % of total | Expected value after MDFC | % of total | |||
|---|---|---|---|---|---|---|
| Direct costs | Antibiotic | €874 | 5.92% | €407 | 6.80% | |
| Emergency room | €116 | 0.79% | €78 | 1.30% | ||
| Outpatient clinic | €31 | 0.21% | €15 | 0.25% | ||
| Hospitalization | €8,979 | 60.80% | €2,733 | 45.66% | ||
| ICU | €0 | 0.00% | €27 | 0.45% | ||
| DFC | €0 | 0.00% | €31 | 0.51% | ||
| Amputation | €1,164 | 7.88% | €709 | 11.85% | ||
| Total direct costs per patient | €11,164 | 75.60% | €3,999 | 66.82% | ||
| Indirect costs | Loss of productivity during admission | €744 | 5.04% | €244 | 4.07% | |
| Loss of mobility due to amputation | €2,860 | 19.37% | €1,742 | 29.10% | ||
| Total indirect costs per patient | €3,604 | 24.41% | €1,986 | 33.17% | ||
| Total costs per patient | €14,768 | 100% | €5,985 | 100% | ||
| Total savings per patient with MDFC | €8,783 | |||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



