Submitted:
25 April 2023
Posted:
26 April 2023
You are already at the latest version
Abstract
The oral health of older individuals can be negatively impacted by various systemic health factors, leading to rapid oral health deterioration. Older people are at risk of experiencing adverse reactions to medications due to multimorbidity, polypharmacy, and changes in pharmacokinetics and pharmacodynamics. Hyposalivation, a significant side effect of some medications, can be induced by both the type and number of medications used. Frailty, disability, sarcopenia, care dependency, and limited access to professional oral healthcare can also compromise the oral health of older people. To prevent rapid oral health deterioration, a comprehensive approach is required that involves effective communication between oral healthcare providers, other healthcare providers, and informal carers. Regardless of their health status, it is crucial to prioritize the well-being of older people. Oral healthcare providers have a responsibility to advocate for the importance of maintaining adequate oral health and to raise awareness of the serious consequences of weakened oral health. By doing so, we can prevent weakened oral health from becoming a geriatric syndrome.
Keywords:
oral health care
; older people
; multimorbidity
; polypharmacy
; frailty
; sarcopenia
; disability
; care dependency
Introduction
The physical and psychological functions of many older adults are being negatively impacted by poor oral health. Difficulties with chewing, biting, swallowing, tasting, speaking, communicating, smiling, appearance, aesthetics, and self-esteem are common [1]. Among the frailest and most care-dependent older adults, dental caries, periodontal disease, tooth loss, and xerostomia are particularly prevalent [1,2,3,4]. Despite the fact that most chronic oral diseases are preventable and treatable, a variety of factors make it difficult to maintain good oral health as people age. This paper aims to review the published evidence on systemic health factors that contribute to rapid oral health deterioration in older individuals and to explore the implications of these factors for both general healthcare and oral healthcare provision.
Ageing
Ageing is typically viewed as a gradual decline in the functioning of various bodily systems, stemming from the accumulation of damaged tissue and substances caused by intrinsic or extrinsic mechanisms [5]. The process of biological ageing is a multifaceted and intricate phenomenon, and although the exact molecular mechanisms behind its onset and progression remain unclear, ample evidence suggests that oxidative stress may play a significant role [6. Kinases, phosphatases, and transcription factors are particularly sensitive to changes in cellular redox status, and chronic or severe disruptions in this homeostasis can result in cell death or proliferation. Immune senescence, or the quantitative and qualitative changes in the immune system that accompany ageing, is another hallmark of the process. While immune senescence doesn't necessarily entail a progressive decline in immune function, it often leads to cytokine dysregulation, which can cause a chronic, low-grade inflammatory state. This inflammation may serve as a biological foundation for ageing and contribute to the onset of age-related diseases, increasing the risk of multimorbidity and mortality [6,7,8,9].
Ageing and Telomere Length
Telomere length is considered a useful biomarker of cellular ageing, as it reflects the repeated sequences of nucleotides that protect the ends of chromosomes [10]. With each replication of cells, telomeres shorten due to incomplete lagging strand replication, leading to cellular senescence once they reach a critically short length [11]. Studies have suggested that telomere length is sensitive to inflammation, as higher rates of telomere loss have been observed in a pro-inflammatory environment with increased blood cell replication [12]. This has prompted some researchers to explore the relationship between periodontal disease and telomere length [13,14,15,16]. In a NHANES study involving 21,000 participants aged 35-75 years, a significant correlation was found between periodontal disease and telomere length, particularly among women, overweight or obese individuals, and those with cardiometabolic comorbidities [17].
Diseases and Oral Health
Several studies have suggested a strong link between noncommunicable diseases and oral health, with demonstrated associations with oral diseases for various conditions including cancer, diabetes, cardiovascular diseases, depression, neurodegenerative conditions, rheumatic diseases, inflammatory bowel disease, gastric helicobacter pylori, obesity, and asthma [18]. The connection between oral health and these diseases is largely attributed to inflammation, although there are two other pathways that may explain the association [19,20,21]. Firstly, some systemic diseases have direct links to negative impacts on oral health and oral health-related quality of life (OHRQoL), such as Crohn’s disease, Beçhet’s disease, oral cancer, Sjögren’s syndrome, and scleroderma [22,23,24,25,26,27,28,29,30,31,32]. Secondly, some chronic diseases may indirectly affect oral health because they can lead to reduced motivation regarding oral hygiene and care. For example, psychiatric and neurological diseases, as well as Alzheimer’s disease, and rheumatic, oncological and cardiovascular diseases can all have an impact [33,34,35,36,37,38,39,40,41,42,43,44,45].
Early diagnosis and treatment of oral conditions among older people with chronic diseases could prevent weak oral health and decline in OHRQoL. However, individuals with cognitive disorders and those receiving palliative care may lose their ability to communicate their oral health needs, leading to under-reporting and underestimation of oral conditions [46]. This could result in healthcare providers failing to fully appreciate the extent of the problem, leading to untreated oral conditions and prolonged discomfort among these patients.
Multimorbidity and Polypharmacy
In 2013, a group of European researchers established a definition for multimorbidity, which refers to any combination of chronic disease with at least one other disease (acute or chronic) or bio-psychosocial factor (associated or not) or somatic risk factor. This definition recognizes that any bio-psychosocial factor, somatic risk factor, social network, burden of diseases, healthcare consumption, and patient coping strategies may modify the effects of multimorbidity. Multimorbidity can lead to increased disability, decreased quality of life, or frailty. While the concept of multimorbidity has been recognized and enhanced by European general practitioners, [47] studies on its prevalence have not yet been conducted.
In populations of older adults with multimorbidity, the use of multiple medications is common, a phenomenon referred to as polypharmacy. Polypharmacy is associated with adverse outcomes, including medication-medication interactions, medication-disease interactions, decreased renal and hepatic function, reduced lean body mass, hearing, vision, cognition, and mobility [50]. A meta-analysis showed that 38% of community-dwelling adults aged 60 years and older use five or more medications daily [48]. Additionally, almost half of care home residents are exposed to potentially inappropriate medications [49]. A systematic review identified 138 definitions of polypharmacy, but a numerical definition alone is insufficient in assessing the safety and appropriateness of medication use. Therefore, a shift towards the term "appropriate polypharmacy" using a holistic approach that considers comorbidities present is needed [50].
Frailty and Oral Health
The concept of frailty has become increasingly important in recent decades, but a consensus on its definition has not yet been reached. There are two main approaches to defining frailty: one that focuses solely on physical functioning, and another that takes into account other domains, such as memory and mood. For example, the Fried frailty phenotype considers unintentional weight loss, self-reported exhaustion, physical activity, hand grip strength, and walking speed, while the multidimensional frailty index by Rockwood et al. also considers cognitive and psychological factors (Figure 1) [51,52]. The prevalence of frailty varies depending on the approach used, with higher rates found for multidimensional assessments [53].
A systematic review investigated the link between oral health and frailty, focusing on five longitudinal studies that used Fried's frailty phenotype. These studies found that the number of teeth, oral functions, accumulation of oral health problems, and dry mouth symptoms were significantly associated with the incidence of frailty [54]. In community-dwelling older adults, oral pain was associated with weight loss and low handgrip, while chewing problems were associated with low physical activity and low gait speed. Those who required dental prostheses were more likely to be prefrail or frail than others [55]. Further research is needed to determine whether oral health indicators can be used to assess frailty.
Sarcopenia and Oral Health
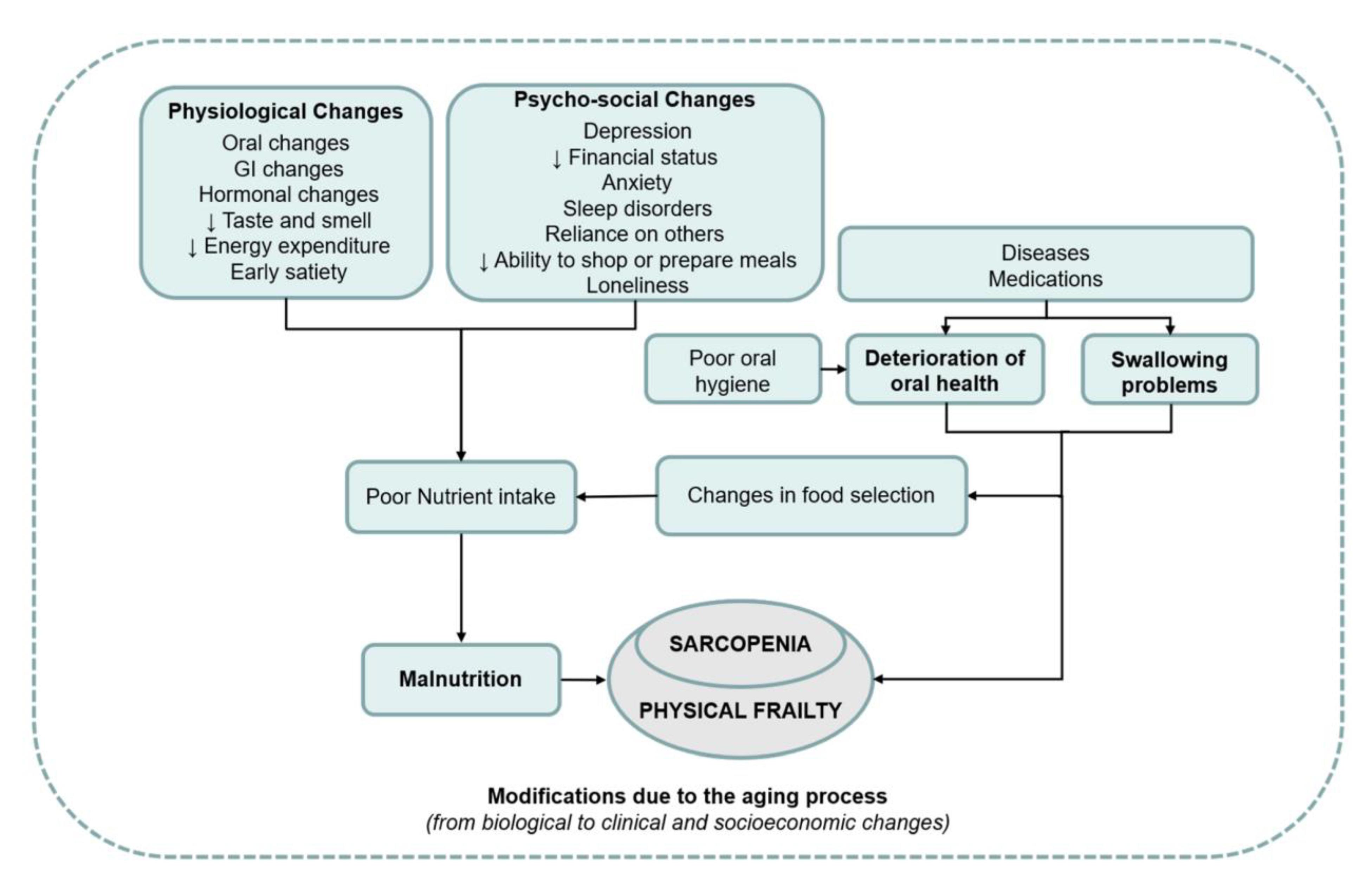
Sarcopenia is a condition that affects older individuals and causes a decline in muscle mass and strength. The prevalence of sarcopenia varies widely between 3.2% to 40%, with the highest incidence in older people above the age of 80 and those living in institutions [58,59,60]. Several risk factors have been identified, including age, chronic diseases, and physical activity levels. Chronic obstructive pulmonary disease, diabetes mellitus, and hypertension are some of the chronic diseases that have been linked to sarcopenia [59]. Although it is a common issue in older adults, sarcopenia can be managed and even prevented with appropriate exercise and nutrition [56,57,58]. Interestingly, sarcopenia can also affect oral health in ways that are not well-known. As muscle mass declines, individuals may experience weaker temporomandibular and orofacial muscles, resulting in difficulty with chewing and swallowing [59]. This can negatively affect a person's ability to maintain a healthy diet and may increase the risk of choking. Moreover, the loss of oral muscle mass can cause hyposalivation, which can lead to tooth decay.
Figure 2.
Overview of the associations between weak oral health, malnutrition, and sarcopenia [60].
Figure 2.
Overview of the associations between weak oral health, malnutrition, and sarcopenia [60].
Disability and Oral Health
Among older adults, there are bidirectional associations between oral health and disability, where both health outcomes can impact each other. Tooth loss, for instance, may lead to disability such as limitations in activities of daily living, instrumental activities of daily living, and mobility [61,62,63,64,65]. Conversely, disability may be associated with chronic illnesses, weak oral health, and reduced quality of life among older people [66]. The World Health Organization defines disability as an impairment that may be physical, cognitive, mental, sensory, emotional, developmental, or a combination of these, and which may occur during a person’s lifetime or from birth. Disabilities can cause physical and cognitive impairments, activity limitations, and participation restrictions [67]. To prevent disability among older adults, self-efficacy must be improved, and physical activity must be promoted [68]. Physical and cognitive functioning of older individuals can be assessed through several assessment instruments [69]. It is possible to analyze the order in which age-related declines occur by examining individuals and groups that are ageing physically and cognitively at different rates [70,71].
Impact of Ageing and Age-Related Diseases on General Healthcare Provision
There is a new trend in healthcare provision for older people, which focuses on preventing premature admission to care homes. This trend offers various healthcare options, including the use of mobility aids, assistive technology devices, domiciliary healthcare, respite care, and telecare. By using assistive technology, the rate of functional decline in frail older people can be slowed down, while domiciliary healthcare aims to maximize independence, self-esteem, self-image, and quality of life [72,73]. Evidence suggests that domiciliary healthcare has positive outcomes, including improved quality of life and functional status, and reduced costs [74]. Informal care provision through visiting nurses, hospice carers, and physical therapists can also help older people live at home for a longer period. Respite care, which offers temporary relief to informal carers, has shown some positive effects, but more research is needed to support this claim [75,76,77].
Telecare, which involves the use of personal and environmental sensors in older people's homes, has been available for several decades. New options include sensors for falls, epilepsy, enuresis, and security monitoring for temperature, carbon monoxide, and smoke detection. Although the benefits of telecare are not yet fully understood due to limited research data, it presents an opportunity to identify what works best for each individual and in which circumstances [78]. Despite the new healthcare options, informal carers, such as spouses, children, relatives, and friends, will still have to provide much of the domiciliary care to frail older people.
Impact of Multimorbidity and Polypharmacy on Oral Healthcare Provision
Multimorbidity can lead to a range of physical and psychosocial issues in older adults. The complexity of this condition means that symptoms may be difficult to diagnose, and diseases may be masked or exacerbated by other health problems. In addition, treatment of one disease may be affected by the presence of other diseases. This can result in a gradual decline in overall health. Oral healthcare providers who work with older adults should have a thorough understanding of geriatrics and pharmacology, and collaborate closely with physicians and pharmacists to provide individualized care [79]. Older adults are particularly susceptible to adverse reactions to medication due to age-related changes in pharmacokinetics and pharmacodynamics, as well as the prevalence of polypharmacy [80,81,82]. Many medications can cause a decrease in saliva secretion rate, leading to dry mouth and a range of oral health problems [81]. Oral healthcare providers should consider the impact of medication on oral health and be cautious in prescribing medication to patients with polypharmacy. The modified Summated Xerostomia Inventory (Table 1) can be used to assess xerostomia. Practical treatments are available to alleviate the symptoms of dry mouth and improve overall physical and psychosocial well-being [83,84].
Impact of Frailty, Disability, and Care Dependency on Oral Healthcare Provision
It is crucial for both formal and informal caregivers of older adults to understand that those who are frail or disabled are at significant risk of developing oral health problems. Caregivers should therefore take the responsibility of organizing a consultation with an oral healthcare provider. On the other hand, sudden deterioration of oral health in older individuals can be an early indicator of frailty and should prompt oral healthcare providers to arrange a consultation with a physician or geriatrician. Multiple epidemiological studies suggest that professional oral healthcare is urgently needed to address the unmet needs of older adults. To improve oral healthcare provision, there should be integration of oral healthcare into general healthcare, community programs that promote healthy behaviors, and access to preventive oral healthcare [85]. A crucial strategy is the development and implementation of an oral healthcare guideline to cater to older adults living in the community. As older adults prefer to age in place, new options of oral healthcare provision such as domiciliary oral healthcare, customised oral hygiene care aids, visiting dental hygienists and nurses, and oral hygiene telecare should be developed. Unfortunately, not all oral healthcare offices are easily accessible for older adults who are frail, disabled, or care-dependent. Therefore, it is the responsibility of oral healthcare providers to make their premises easily and safely accessible for this group of individuals. Only when oral healthcare providers accept and face this responsibility can dentistry be transformed into medical oral healthcare and dentists be upgraded to oral physicians.
Epilogue
The risk of rapid deterioration in oral health is heightened by ageing, age-related diseases, multimorbidity, polypharmacy, frailty, disability, sarcopenia, and inappropriate oral hygiene care. To prevent such deterioration, it is important to take an integrated approach to oral health and hygiene care, involving communication and collaboration between oral healthcare providers, other healthcare providers, and informal caregivers. The ultimate goal is to promote the well-being of older people, regardless of their health status. It is crucial for care providers to raise awareness about the importance of maintaining good oral health and the consequences of neglecting it, in order to prevent weakened oral health from becoming a geriatric syndrome [4].
References
- van der Putten GJ, De Visschere L, Maarel-Wiering van der C, Vanobbergen J, Schols J: The importance of oral health in (frail) elderly people - a review. Eur. Geriatr. Med. 2013, 4, 339–344. [CrossRef]
- Kossioni AE, Maggi S, Muller F, Petrovic M: Oral health in older people: Time for action. Eur. Geriatr. Med. 2018, 9, 3–4. [CrossRef] [PubMed]
- Marengoni A, von Strauss E, Rizzuto D, Winblad B, Fratiglioni L: The impact of chronic multimorbidity and disability on functional decline and survival in elderly persons. A community-based, longitudinal study. J. Intern. Med. 2009, 265, 288–295.
- van der Putten GJ, de Baat C, De Visschere L, Schols J: Poor oral health, a potential new geriatric syndrome. Gerodontology 2014, 31 Suppl 1, 17–24. [CrossRef]
- Strehler BL: Understanding aging. Methods Mol. Med. 2000, 38, 1–19.
- Michaud M, Balardy L, Moulis G, Gaudin C, Peyrot C, Vellas B, Cesari M, Nourhashemi F: Proinflammatory cytokines, aging, and age-related diseases. J. Am. Med. Dir. Assoc. 2013, 14, 877–882. [CrossRef] [PubMed]
- Miller RA: The aging immune system: Primer and prospectus. Science 1996, 273, 70–74. [CrossRef] [PubMed]
- Sansoni P, Vescovini R, Fagnoni F, Biasini C, Zanni F, Zanlari L, Telera A, Lucchini G, Passeri G, Monti D et al: The immune system in extreme longevity. Exp. Gerontol. 2008, 43, 61–65. [CrossRef]
- Sadighi Akha AA: Aging and the immune system: An overview. J. Immunol. Methods 2018, 463, 21–26. [CrossRef]
- Sanders JL, Newman AB: Telomere length in epidemiology: A biomarker of aging, age-related disease, both, or neither? Epidemiol. Rev. 2013, 35, 112–131. [CrossRef]
- Lu W, Zhang Y, Liu D, Songyang Z, Wan M: Telomeres-structure, function, and regulation. Exp. Cell Res. 2013, 319, 133–141. [CrossRef]
- Zhang J, Rane G, Dai X, Shanmugam MK, Arfuso F, Samy RP, Lai MK, Kappei D, Kumar AP, Sethi G: Ageing and the telomere connection: An intimate relationship with inflammation. Ageing Res. Rev. 2016, 25, 55–69. [CrossRef] [PubMed]
- Masi S, Gkranias N, Li K, Salpea KD, Parkar M, Orlandi M, Suvan JE, Eng HL, Taddei S, Patel K et al: Association between short leukocyte telomere length, endotoxemia, and severe periodontitis in people with diabetes: A cross-sectional survey. Diabetes Care 2014, 37, 1140–1147. [CrossRef] [PubMed]
- Masi S, Salpea KD, Li K, Parkar M, Nibali L, Donos N, Patel K, Taddei S, Deanfield JE, D'Aiuto F et al: Oxidative stress, chronic inflammation, and telomere length in patients with periodontitis. Free Radic. Biol. Med. 2011, 50, 730–735. [CrossRef]
- Sanders AE, Divaris K, Naorungroj S, Heiss G, Risques RA: Telomere length attrition and chronic periodontitis: An ARIC Study nested case-control study. J. Clin. Periodontol. 2015, 42, 12–20. [CrossRef] [PubMed]
- Takahashi K, Nishida H, Takeda H, Shin K: Telomere length in leukocytes and cultured gingival fibroblasts from patients with aggressive periodontitis. J. Periodontol. 2004, 75, 84–90. [CrossRef]
- Song W, Yang J, Niu Z: Association of periodontitis with leukocyte telomere length in US adults: A cross-sectional analysis of NHANES 1999 to 2002. J Periodontol 2021, 92, 833–843. [CrossRef]
- Botelho J, Mascarenhas P, Viana J, Proenca L, Orlandi M, Leira Y, Chambrone L, Mendes JJ, Machado V: An umbrella review of the evidence linking oral health and systemic noncommunicable diseases. Nat. Commun. 2022, 13, 7614. [CrossRef]
- Gurenlian JR: Inflammation: The relationship between oral health and systemic disease. Dent. Assist. 2009, 78, 8–10, 12-14, 38-40; quiz 41-13.
- Peric M, Marhl U, Gennai S, Marruganti C, Graziani F: Treatment of gingivitis is associated with reduction of systemic inflammation and improvement of oral health-related quality of life: A randomized clinical trial. J. Clin. Periodontol. 2022, 49, 899–910. [CrossRef]
- Bui FQ, Almeida-da-Silva CLC, Huynh B, Trinh A, Liu J, Woodward J, Asadi H, Ojcius DM: Association between periodontal pathogens and systemic disease. Biomed. J. 2019, 42, 27–35. [CrossRef]
- de Vries SAG, Tan CXW, Bouma G, Forouzanfar T, Brand HS, de Boer NK: Salivary Function and Oral Health Problems in Crohn's Disease Patients. Inflamm. Bowel Dis. 2018, 24, 1361–1367. [CrossRef]
- Rikardsson S, Jonsson J, Hultin M, Gustafsson A, Johannsen A: Perceived oral health in patients with Crohn's disease. Oral. Health Prev. Dent. 2009, 7, 277–282.
- Ali S, Nagieb CS, Fayed HL: Effect of Behcet's disease-associated oral ulcers on oral health related quality of life. Spec. Care Dentist 2022.
- Mumcu G, Ergun T, Inanc N, Fresko I, Atalay T, Hayran O, Direskeneli H: Oral health is impaired in Behcet's disease and is associated with disease severity. Rheumatology 2004, 43, 1028–1033. [CrossRef] [PubMed]
- Senusi A, Higgins S, Fortune F: The influence of oral health and psycho-social well-being on clinical outcomes in Behcet's disease. Rheumatol. Int. 2018, 38, 1873–1883. [CrossRef]
- Albilia JB, Lam DK, Blanas N, Clokie CM, Sandor GK: Small mouths. .. Big problems? A review of scleroderma and its oral health implications. J. Can. Dent. Assoc. 2007, 73, 831–836.
- Beaty KL, Gurenlian JR, Rogo EJ: Oral Health Experiences of the Limited Scleroderma Patient. J. Dent. Hyg. 2021, 95, 59–69.
- Chung M, York BR, Michaud DS: Oral Health and Cancer. Curr. Oral. Health Rep. 2019, 6, 130–137. [CrossRef]
- Jobbins J, Bagg J, Finlay IG, Addy M, Newcombe RG: Oral and dental disease in terminally ill cancer patients. BMJ 1992, 304, 1612. [CrossRef]
- Vermaire JA, Partoredjo ASK, de Groot RJ, Brand HS, Speksnijder CM: Mastication in health-related quality of life in patients treated for oral cancer: A systematic review. Eur J Cancer Care (Engl) 2022, 31, e13744.
- Zhang J, Bellocco R, Sandborgh-Englund G, Yu J, Sallberg Chen M, Ye W: Poor Oral Health and Esophageal Cancer Risk: A Nationwide Cohort Study. Cancer Epidemiol. Biomarkers Prev. 2022, 31, 1418–1425. [CrossRef]
- Auffret M, Meuric V, Boyer E, Bonnaure-Mallet M, Verin M: Oral Health Disorders in Parkinson's Disease: More than Meets the Eye. J. Parkinsons Dis. 2021, 11, 1507–1535. [CrossRef] [PubMed]
- de Baat C, van Stiphout MAE, Lobbezoo F: [The objective oral health of Parkinson's disease patients]. Ned. Tijdschr. Tandheelkd. 2020, 127, 318–322. [CrossRef] [PubMed]
- Nakayama Y, Washio M, Mori M: Oral health conditions in patients with Parkinson's disease. J. Epidemiol. 2004, 14, 143–150. [CrossRef]
- Persson M, Osterberg T, Granerus AK, Karlsson S: Influence of Parkinson's disease on oral health. Acta Odontol. Scand. 1992, 50, 37–42. [CrossRef]
- Ribeiro GR, Campos CH, Garcia RC: Oral Health in Elders with Parkinson's Disease. Braz. Dent. J. 2016, 27, 340–344. [CrossRef] [PubMed]
- Saft C, Andrich JE, Muller T, Becker J, Jackowski J: Oral and dental health in Huntington's disease - an observational study. BMC Neurol. 2013, 13, 114.
- Manchery N, Henry JD, Nangle MR: A systematic review of oral health in people with multiple sclerosis. Community Dent. Oral. Epidemiol. 2020, 48, 89–100. [CrossRef]
- Hamza SA, Asif S, Bokhari SAH: Oral health of individuals with dementia and Alzheimer's disease: A review. J. Indian. Soc. Periodontol. 2021, 25, 96–101. [CrossRef]
- Ahola K, Saarinen A, Kuuliala A, Leirisalo-Repo M, Murtomaa H, Meurman JH: Impact of rheumatic diseases on oral health and quality of life. Oral. Dis. 2015, 21, 342–348. [CrossRef]
- Carvalho CG, Medeiros-Filho JB, Ferreira MC: Guide for health professionals addressing oral care for individuals in oncological treatment based on scientific evidence. Support. Care Cancer 2018, 26, 2651–2661. [CrossRef]
- Aleksandric S: Poor oral health: Cause or risk factor for future cardiovascular diseases. Int. J. Cardiol. 2022, 352, 150–151. [CrossRef]
- Gianos E, Jackson EA, Tejpal A, Aspry K, O'Keefe J, Aggarwal M, Jain A, Itchhaporia D, Williams K, Batts T et al: Oral health and atherosclerotic cardiovascular disease: A review. Am. J. Prev. Cardiol. 2021, 7, 100179. [CrossRef] [PubMed]
- Meurman JH, Bascones-Martinez A: Oral Infections and Systemic Health - More than Just Links to Cardiovascular Diseases. Oral. Health Prev. Dent. 2021, 19, 441–448.
- Venkatasalu MR, Murang ZR, Ramasamy DTR, Dhaliwal JS: Oral health problems among palliative and terminally ill patients: An integrated systematic review. BMC Oral. Health 2020, 20, 79.
- Le Reste JY, Nabbe P, Manceau B, Lygidakis C, Doerr C, Lingner H, Czachowski S, Munoz M, Argyriadou S, Claveria A et al: The European General Practice Research Network presents a comprehensive definition of multimorbidity in family medicine and long term care, following a systematic review of relevant literature. J. Am. Med. Dir. Assoc. 2013, 14, 319–325.
- Loya AM, Gonzalez-Stuart A, Rivera JO: Prevalence of polypharmacy, polyherbacy, nutritional supplement use and potential product interactions among older adults living on the United States-Mexico border: A descriptive, questionnaire-based study. Drugs Aging 2009, 26, 423–436. [CrossRef]
- Le Reste JY, Nabbe P, Lazic D, Assenova R, Lingner H, Czachowski S, Argyriadou S, Sowinska A, Lygidakis C, Doerr C et al: How do general practitioners recognize the definition of multimorbidity? A European qualitative study. Eur. J. Gen. Pract. 2016, 22, 159–168.
- Masnoon N, Shakib S, Kalisch-Ellett L, Caughey GE: What is polypharmacy? A systematic review of definitions. BMC Geriatr. 2017, 17, 230.
- Rockwood K, Mitnitski A: Frailty in relation to the accumulation of deficits. J. Gerontol. A Biol. Sci. Med. Sci. 2007, 62, 722–727. [CrossRef]
- Rockwood K, Song X, MacKnight C, Bergman H, Hogan DB, McDowell I, Mitnitski A: A global clinical measure of fitness and frailty in elderly people. CMAJ 2005, 173, 489–495. [CrossRef]
- Collard RM, Boter H, Schoevers RA, Oude Voshaar RC: Prevalence of frailty in community-dwelling older persons: A systematic review. J. Am. Geriatr. Soc. 2012, 60, 1487–1492. [CrossRef] [PubMed]
- Kamdem B, Seematter-Bagnoud L, Botrugno F, Santos-Eggimann B: Relationship between oral health and Fried's frailty criteria in community-dwelling older persons. BMC Geriatr. 2017, 17, 174.
- de Andrade FB, Lebrao ML, Santos JL, Duarte YA: Relationship between oral health and frailty in community-dwelling elderly individuals in Brazil. J. Am. Geriatr. Soc. 2013, 61, 809–814. [CrossRef]
- Ferreira LF, Scariot EL, da Rosa LHT: The effect of different exercise programs on sarcopenia criteria in older people: A systematic review of systematic reviews with meta-analysis. Arch. Gerontol. Geriatr. 2023, 105, 104868. [CrossRef] [PubMed]
- Zhao H, Cheng R, Song G, Teng J, Shen S, Fu X, Yan Y, Liu C: The Effect of Resistance Training on the Rehabilitation of Elderly Patients with Sarcopenia: A Meta-Analysis. Int. J. Environ. Res. Public. Health 2022, 19(23).
- Yoo JI, Ha YC, Cha Y: Nutrition and Exercise Treatment of Sarcopenia in Hip Fracture Patients: Systematic Review. J. Bone Metab. 2022, 29, 63–73. [CrossRef] [PubMed]
- Hatta K, Ikebe K: Association between oral health and sarcopenia: A literature review. J. Prosthodont. Res. 2021, 65, 131–136. [CrossRef] [PubMed]
- Azzolino D, Passarelli PC, De Angelis P, Piccirillo GB, D'Addona A, Cesari M: Poor Oral Health as a Determinant of Malnutrition and Sarcopenia. Nutrients 2019, 11(12).
- Holm-Pedersen P, Schultz-Larsen K, Christiansen N, Avlund K: Tooth loss and subsequent disability and mortality in old age. J. Am. Geriatr. Soc. 2008, 56, 429–435. [CrossRef]
- Komiyama T, Ohi T, Miyoshi Y, Murakami T, Tsuboi A, Tomata Y, Tsuji I, Watanabe M, Hattori Y: Association Between Tooth Loss, Receipt of Dental Care, and Functional Disability in an Elderly Japanese Population: The Tsurugaya Project. J. Am. Geriatr. Soc. 2016, 64, 2495–2502. [CrossRef]
- Komiyama T, Ohi T, Tomata Y, Tanji F, Tsuji I, Watanabe M, Hattori Y: Dental Status is Associated With Incident Functional Disability in Community-Dwelling Older Japanese: A Prospective Cohort Study Using Propensity Score Matching. J. Epidemiol. 2020, 30, 84–90. [CrossRef] [PubMed]
- Matsuyama Y, Listl S, Jurges H, Watt RG, Aida J, Tsakos G: Causal Effect of Tooth Loss on Functional Capacity in Older Adults in England: A Natural Experiment. J. Am. Geriatr. Soc. 2021, 69, 1319–1327. [CrossRef]
- Yin Z, Yang J, Huang C, Sun H, Wu Y: Eating and communication difficulties as mediators of the relationship between tooth loss and functional disability in middle-aged and older adults. J. Dent. 2020, 96, 103331. [CrossRef] [PubMed]
- Kotronia E, Brown H, Papacosta O, Lennon LT, Weyant RJ, Whincup PH, Wannamethee SG, Ramsay SE: Oral health problems and risk of incident disability in two studies of older adults in the United Kingdom and the United States. J. Am. Geriatr. Soc. 2022, 70, 2080–2092. [CrossRef] [PubMed]
- Organization WH: World report on Disability.. In.; 2011.
- Motl RW, McAuley E: Physical activity, disability, and quality of life in older adults. Phys. Med. Rehabil. Clin. N. Am. 2010, 21, 299–308. [CrossRef]
- Clouston SA, Brewster P, Kuh D, Richards M, Cooper R, Hardy R, Rubin MS, Hofer SM: The dynamic relationship between physical function and cognition in longitudinal aging cohorts. Epidemiol. Rev. 2013, 35, 33–50. [CrossRef]
- Bossers WJ, van der Woude LH, Boersma F, Scherder EJ, van Heuvelen MJ: Recommended measures for the assessment of cognitive and physical performance in older patients with dementia: A systematic review. Dement. Geriatr. Cogn. Dis. Extra 2012, 2, 589–609. [CrossRef]
- Gill TM: Assessment of function and disability in longitudinal studies. J. Am. Geriatr. Soc. 2010, 58 Suppl 2(Suppl 2):S308-312.
- Mann WC, Ottenbacher KJ, Fraas L, Tomita M, Granger CV: Effectiveness of assistive technology and environmental interventions in maintaining independence and reducing home care costs for the frail elderly. A randomized controlled trial. Arch. Fam. Med. 1999, 8, 210–217.
- Parsons J, Rouse P, Robinson EM, Sheridan N, Connolly MJ: Goal setting as a feature of homecare services for older people: Does it make a difference? Age Ageing 2012, 41, 24–29. [CrossRef]
- Ryburn B, Wells Y, Foreman P: Enabling independence: Restorative approaches to home care provision for frail older adults. Health Soc. Care Community 2009, 17, 225–234. [CrossRef]
- Evans D: Exploring the concept of respite. J. Adv. Nurs. 2013, 69, 1905–1915. [CrossRef]
- Shaw C, McNamara R, Abrams K, Cannings-John R, Hood K, Longo M, Myles S, O'Mahony S, Roe B, Williams K: Systematic review of respite care in the frail elderly. Health Technol. Assess. 2009, 13, 1–224, iii.
- Hogan L, Boron JB, Masters J, MacArthur K, Manley N: Characteristics of dementia family caregivers who use paid professional in-home respite care. Home Health Care Serv. Q. 2022, 41, 310–329. [CrossRef] [PubMed]
- Parker SG, Hawley MS: Telecare for an ageing population? Age Ageing 2013, 42, 424–425. [CrossRef] [PubMed]
- Dolan TA: Professional education to meet the oral health needs of older adults and persons with disabilities. Spec. Care Dentist 2013, 33, 190–197. [CrossRef] [PubMed]
- Corsonello A, Pedone C, Incalzi RA: Age-related pharmacokinetic and pharmacodynamic changes and related risk of adverse drug reactions. Curr. Med. Chem. 2010, 17, 571–584. [CrossRef] [PubMed]
- Liu B, Dion MR, Jurasic MM, Gibson G, Jones JA: Xerostomia and salivary hypofunction in vulnerable elders: Prevalence and etiology. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. 2012, 114, 52–60. [CrossRef]
- Ship JA, Pillemer SR, Baum BJ: Xerostomia and the geriatric patient. J. Am. Geriatr. Soc. 2002, 50, 535–543. [CrossRef]
- van der Putten GJ, Brand HS, Schols JM, de Baat C: The diagnostic suitability of a xerostomia questionnaire and the association between xerostomia, hyposalivation and medication use in a group of nursing home residents. Clin. Oral. Investig. 2011, 15, 185–192. [CrossRef]
- Thomson WM, van der Putten GJ, de Baat C, Ikebe K, Matsuda K, Enoki K, Hopcraft MS, Ling GY: Shortening the xerostomia inventory. Oral. Surg. Oral. Med. Oral. Pathol. Oral. Radiol. Endod. 2011, 112, 322–327. [CrossRef]
- Griffin SO, Jones JA, Brunson D, Griffin PM, Bailey WD: Burden of oral disease among older adults and implications for public health priorities. Am. J. Public. Health 2012, 102, 411–418. [CrossRef]
Figure 1.
Clincal Frailty Scale.
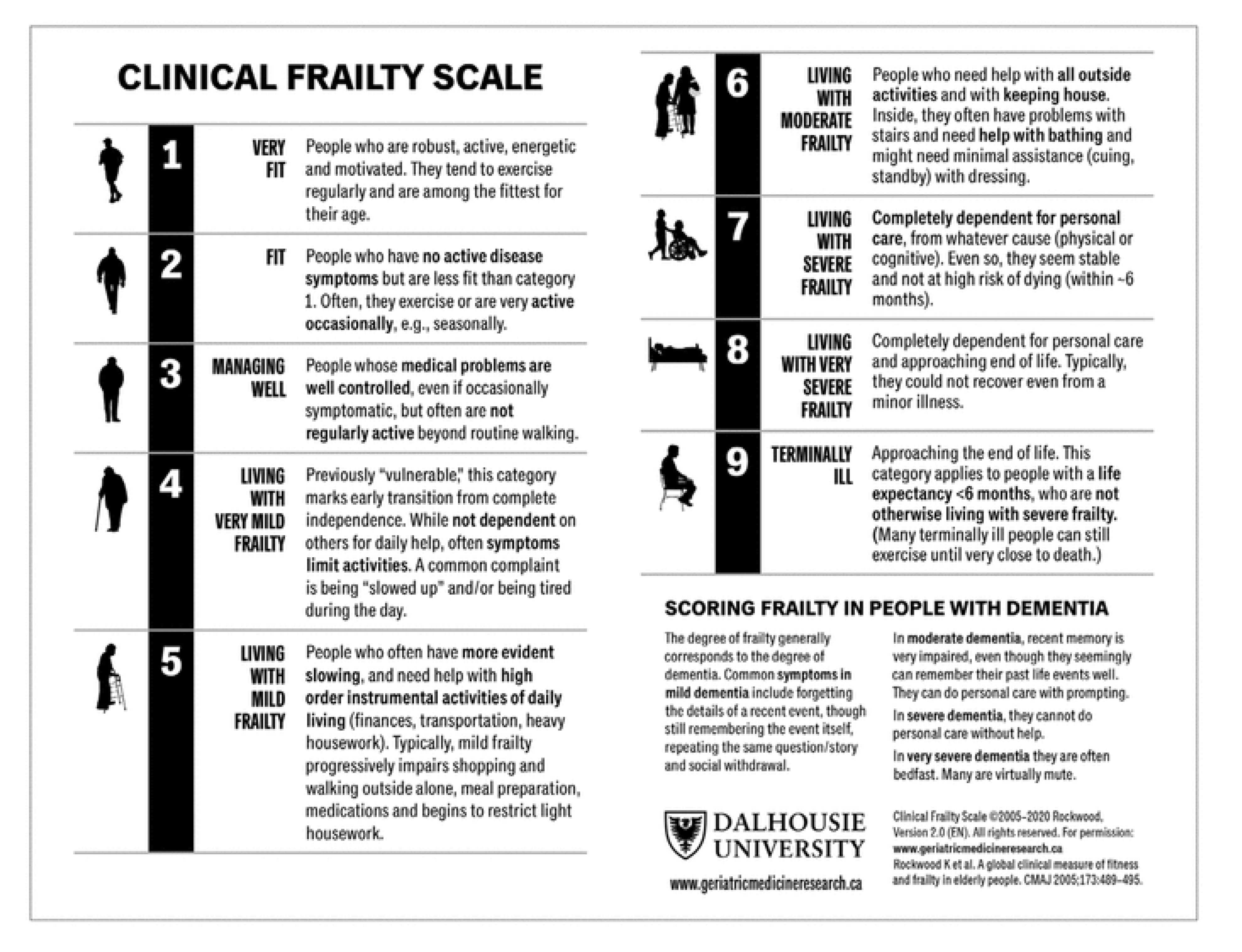

Table 1.
Modified Summated Xerostomia Inventory.
| Never | Ocasionally | Often | ||
|---|---|---|---|---|
| 1 | My mouth feels dry when eating a meal | 1 | 2 | 3 |
| 2 | My mouth feels dry | 1 | 2 | 3 |
| 3 | I have difficulty in eating dry foods | 1 | 2 | 3 |
| 4 | I Have difficulties swallowing certain foods | 1 | 2 | 3 |
| 5 | My lips feel dry | 1 | 2 | 3 |
Summatedscore < 8 no xerostomia. Summated score≥8 xerostomia.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



