
Submitted:
25 April 2023
Posted:
26 April 2023
You are already at the latest version
Abstract
Background: Primary infection has been questioned as the pathogenetic cause of acute appendicitis. We attempted to identify the bacteria involved, and to investigate if their species, types, or combinations affected the severity of acute appendicitis in children. Methods: Samples from both the appendiceal lumen and the peritoneal cavity of 72 children who underwent appendectomy were collected to perform bacterial culture analysis. The outcomes were studied to see if and how they were associated with the severity of the disease. Regression analysis was performed to identify any risk factors associated with complicated appendicitis. Results: Escherichia coli, Pseudomonas aeruginosa and Streptococcus species were the most common pathogens found in the study population. The same microorganisms, either combined or separate, were the most common in the appendiceal lumen and the peritoneal cavity of patients with complicated appendicitis. Gram-negative bacteria, polymicrobial cultures in the peritoneal fluid and in the appendiceal lumen, were associated with complicated appendicitis. Polymicrobial cultures in the peritoneal cavity presented four times higher risk of complicated appendicitis. Conclusion: Polymicrobial presentation and gram-negative bacteria are associated with complicated appendicitis. Antibiotic regimens should target the combinations of the most frequently identified pathogens, speculating the value of early antipseudomonal intervention.
Keywords:
acute appendicitis
; bacterial culture
; children
; appendiceal lumen
; peritoneal cavity
; complicated appendicitis
1. Introduction
The most common cause of acute abdominal pain requiring surgery is acute appendicitis. In the developed world, a total of 5.7–50 per 100,000 inhabitants is affected by acute appendicitis every year [1]. More than 30% of the patients are children, with a peak incidence at 11-12 years of age [2]. Children younger than five years often present atypical symptoms, with a complication rate of up to 50% [3,4,5]. The fact that there are still children with peritonitis, in the era of highly accurate diagnostic modalities, constitutes a challenge for the present generation of clinicians and researchers [6]. The incidence of complicated appendicitis may reach 100% in children under the age of three years [7,8,9]. Early detection and administration of antibiotics is essential, as timely treatment affects prognosis [10].
Though acute appendicitis has been studied extensively, its pathogenesis is still a matter of debate. Obstruction of the appendiceal lumen has been traditionally considered as the trigger of inflammation [11,12]. However, the theory that acute appendicitis is caused by primary bacterial infection with secondary luminal obstruction, has been gaining ground. This is supported by evidence that acute appendicitis occurs in clusters, presents seasonal variation, and is less common in rural areas of the developing world [13,14].
During the last two decades, there is a trend to consider acute appendicitis as a double entity; a disease characterized as uncomplicated, which may regress under certain circumstances, with or without the help of antibiotics, and a disease which is characterized as complicated, and should be treated timely with open or laparoscopic appendectomy [15,16]. It is known that not only uncomplicated but occasionally complicated appendicitis, such as abscess or phlegmon, can be initially treated safely and effectively with antibiotics as well [15,16]. In both types, the intervention of any antibiotic involved should be focused on the appropriate bacteria. Therefore, it is considered essential to study the microbiome of the appendix and the peritoneal cavity of patients with acute appendicitis, especially children.
In the present study, we aimed to describe the bacterial profile of the appendiceal lumen and the peritoneal cavity in a cohort of children with acute appendicitis, using a culture-based approach. Furthermore, we aimed to investigate any possible association between the culture outcomes and the severity of appendicitis, dividing the cohort into patients with uncomplicated and complicated appendicitis, targeting the accomplishment of a most effective anti-microbial regimen.
2. Materials and Methods
Study population
This is a prospective study on a cohort of children with acute appendicitis, who underwent appendectomy with laparoscopy or open surgery, during a period of one year. Medical history, clinical examination, and routine laboratory tests were recorded on admission. Patients with chronic disorders (respiratory, cardiovascular, renal, metabolic, etc.), hematological diseases or malignancies, and those who had received antibiotics prior to admission, were not included in the study. Children younger than four years, and those without postoperative histopathological evidence of acute appendicitis were excluded as well. Cefuroxime and metronidazole were administrated, according to the department’s protocol, for a maximum period of 18 hours prior to surgery. Amikacin was added if the anticipated diagnosis was complicated appendicitis, according to the clinical presentation and the preoperative ultrasound findings. The antibiotic regimen was adjusted postoperatively, according to the intraoperative findings. The initial macroscopic assessment of the stage of appendicitis during surgery was confirmed by histopathology.
Sample collection
After inspecting the abdominal cavity and prior to any manipulation, a sample of peritoneal fluid was obtained with aspiration through a sterilized feeding tube. The excised appendix was washed under sterile conditions with normal saline 0.9%. The material from the appendiceal lumen was extracted by light milking into a sterilized plastic sample cup. Finally, the appendix was placed into formalin for histopathological analysis.
Histopathology
The laparoscopic grading system was adopted to define the appendicitis stage [15]. The score includes normal appendix (grade 0), hyperemia and oedema (grade 1), fibrinous exudate (grade 2), segmental necrosis (grade 3a), necrosis at the base of the appendix (grade 3b), abscess (grade 4a), regional peritonitis (grade 4b), and diffuse peritonitis (grade 5) [17,18]. Grades 1-2 are characterized as non-complicated appendicitis, while grades 3-5 are characterized as complicated [17,19]. Patients with grade 0 were not included in the study.
Microbiological assessment
The fluid from the peritoneal cavity was injected into blood culture bottles (BACT/ALERT FA Plus, BACT/ALERT FN Plus - bioMérieux, France) immediately after sampling, and together with the material from the lumen, were transferred to the microbiology department. Once arrived, the sample from the sample cup was diluted with normal saline 0.9% and inoculated in MacConkey agar plates and Schaedler agar plates with 5% horse blood (Oxoid Ltd., Ireland). The plates were incubated in aerobic and anaerobic atmospheres in 37 oC, and bacterial growth was examined after 24 and 48 hours of incubation. All bacteria isolated in aerobic and anaerobic conditions were identified with the VITEK 2 system (bioMérieux, France), and the API 20A system (bioMérieux, France). Antimicrobial susceptibility testing was performed with the automated VITEK-2 system (bioMérieux, France) and the ETEST method (bioMérieux, France), according to the principles of the European committee on antimicrobial susceptibility testing (EUCAST).
According to the culture outcomes, the bacteria were described as single units or as groups, and were clustered as aerobic, facultative, and obligatory anaerobic, Gram-positive, and Gram-negative. The cultures were categorized as monomicrobial and polymicrobial, according to the growth of one and at least two bacteria respectively. Patients with negative cultures of the lumen of the appendix were excluded from the study.
Statistical analysis
For the data analysis, the potential effect of the independent (outcomes from the cultures of the lumen of the appendix and the peritoneal cavity) on the dependent variables (uncomplicated and complicated acute appendicitis) was examined, using descriptive statistics of the correlation coefficient. In some parts of the statistical analysis, the correlation between a qualitative and a quantitative variable was tested. For this reason, the t-Kendall was used as optimal correlation coefficient, which converges faster to the normal distribution than Spearman's correlation coefficient because of the rank orders. For the rest of the analysis, the correlation between qualitative independent and dependent variables, chi-square test was employed with the respective measures of correlation (phi coefficient, Cramer's V, contingency coefficient). For the analysis of the possible correlation between the culture outcomes and the severity of appendicitis, a logistic regression model was used (Logit regression). All statistical analyses were performed using the SPSS Statistical Software Package version 25 (IBM Corp., Armonk NY, USA). The threshold for statistical significance was defined as p < 0.05.
Ethical considerations
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Patras Children’s Hospital (2619/04.03.2019). Informed consent was obtained from the parents of the patients prior to their enrolment in the study.
3. Results
A cohort of 72 children (43 boys and 29 girls), who were submitted to appendectomy from January 1st to December 31st, 2020, were enlisted in the study. The mean age of the study population was 10.6 years (range: 6-16 years). The demographic characteristics, clinical presentation, and laboratory findings are presented in Table 1. There were 42 children (58.3%) with uncomplicated, and 30 (41.7%) with complicated appendicitis (Table 1).
A total of 8.30% of specimens presented histopathologic findings of hyperemia and oedema (grade I), and 50% presented fibrinous exudate (grade II), both considered as uncomplicated appendicitis. Complicated appendicitis represented 9.7% of specimens with base necrosis (grade 3a), 16.6% with abscess (grade 4a), 12.5% with local peritonitis (grade 4b), and 2.8% with general peritonitis (grade 5) (Figure 1).
Appendiceal lumen outcomes
The cultures of the lumen of the appendix showed that 73.6% of the isolated bacteria of the study population were Gram-negative and 23.4% a mixed population of Gram-positive and Gram-negative microorganisms. No culture included exclusively Gram-positive bacteria.
Aerobic and facultative anaerobic bacteria were developed in the lumen in 82% of cultures, obligatory aerobic in 2.7%, and combined in 15.3%. Polymicrobial cultures were 55.5% and monomicrobial 45.5%.
Escherichia coli was the most commonly identified microorganism in the appendiceal lumen (83.4%, in 34.7% as single entity), followed by Pseudomonas aeruginosa (19.5%), Streptococcus species (spp) (12.5%), Enterococcus faecalis (11.1%), which was found always in association with other bacteria, and Klebsiella pneumoniae (8.3%) (Table 2).
E. coli was found in 76.2% of the cultures of the appendiceal lumen in patients with uncomplicated appendicitis (35.7% as the only pathogen), followed by P. aeruginosa (21.5%) and K. pneumoniae (14.3%) (Table 3).
E. coli was also the predominant microorganism in complicated appendicitis, (96.4%, 63.1% of them in combination with other bacteria). The next most common pathogens were Streptococcus spp (20%), and P. aeruginosa (16.6%) (Table 3).
Peritoneal cavity outcomes
A total of 45% of the cultures from the peritoneal cavity were positive for bacteria. The percentages that follow refer exclusively to the positive culture outcomes.
Gram-negative bacteria were developed in 62.5% of the cultures, Gram-positive in 31.2%, and a combination of Gram-positive and Gram-negative in 6.3%.
In all these cultures, except for one, all microorganisms were aerobic and facultative anaerobic. 59.4% of the cultures of the peritoneal fluid were monomicrobial and 41.5% polymicrobial.
E. coli was the most common pathogen (77.4%, 45.2% as monomicrobial culture), followed by Streptococcus spp (19.3%) and P. aeruginosa (9.2%, always combined with other bacteria) (Table 4).
In the uncomplicated cases, E. coli was the most commonly identified bacterium (54,6%, 45.5% as the only pathogen of the culture), while K. pneumoniae and E. faecalis shared the equal percentage of 18.2% (Table 5).
In patients with complicated appendicitis, E. coli (90%, 45% as monomicrobial culture) and Streptococcus spp, (30%, 5% as monomicrobial) were the most frequent bacteria encountered (Table 5). P. aeruginosa was found in 10% combined with E. coli, while Pseudomonas vesicularis in 5%, combined with Streptococcus spp (Table 5).
Interpretation of the culture outcomes
When a possible association between the culture outcomes and the severity of appendicitis was questioned in regard to the bacterial species, none was found statistically significant, both in the appendiceal lumen and the peritoneal cavity.
Nevertheless, when the bacteria were categorized in groups, Gram-negative bacteria (p = 0.003) and polymicrobial cultures (p < 0.01) in the peritoneal fluid, and polymicrobial cultures in the lumen of the appendix (p = 0.04), were found associated with complicated appendicitis.
With the logistic regression analysis, we tried to find out if the correlations that were displayed herein with conventional statistical methods were valid towards a certain direction, i.e., if the different groupings of the culture outcomes affected the presence of uncomplicated or complicated appendicitis. With this method, we created multiple models from the combinations of the formed groups, and we evaluated their possible association with the dependent variables through Wald testing. The coefficient of each model corresponded to a particular p-value, resulting in the significance or not of the way an independent variable affected the dependent one.
Among all combinations, the model with the value (2) according to Wald test was the only one that presented statistical significance with a p-value lower than 0.05 (Table 6). For the needs of analysis, the value (1) was given to the model of non-complicated cases of acute appendicitis, and the value (2) to model of the complicated ones (as the dependent variable). Accordingly, the value (1) was given to the cultures with a single microorganism, and to those with two or more microorganisms the value (2) (independent variables). The outcome that resulted was that when there was more than one species of bacteria in the culture of the peritoneal fluid (polymicrobial culture), there was significant risk of presentation of complicated appendicitis (Table 6).
Thus, it was shown that polymicrobial cultures in the peritoneal fluid were correlated with a four times higher risk of complicated appendicitis (Odds ratio: 3.88, 95% confidence interval: 1.82 – 8.25) (Table 6).
4. Discussion
In this study we attempted to identify the bacteria of the appendiceal lumen and the peritoneal cavity in a cohort of children with acute appendicitis, and to find any association with the severity of inflammation and the risk of complications. Similar studies have been performed, intending to clarify the pathophysiology of the disease, and to create protocols of therapy [9,11,12].
We live in the era of a shifting trend from immediate appendectomy in all cases with acute appendicitis, to watchful observation regarding non-complicated appendicitis, and delayed treatment, either with surgery if the clinical presentation worsens, or with conservative management with antibiotics [20,21,22]. The vermiform appendix is not considered anymore as a redundant useless apparatus of the gastrointestinal tube [23,24]. In opposite, it is considered as a reservoir of a biofilm of bacteria which colonize the caecum and the large intestine, providing protection against pathogenic microorganisms [25,26]. A gene sequencing study proved the development of fungi in a healthy population with appendectomy, in contrary to controls who kept their appendix [27].
According to international guidelines, delayed appendectomy, until the first 24 hours after the presentation of symptoms, is safe in most cases, and does not increase the risks of complications [24,28]. According to the recent international guidelines on appendicitis, complicated cases of diffuse peritonitis should be treated with surgery no more than 8 hours after diagnosis, while the surgical management of special forms such as phlegmons may be anticipated [16,29].
The recent restriction measures during the COVID-19 pandemic and their impact on the incidence and the treatment strategies of acute appendicitis, especially on the use of antibiotics during this period, played a critical role in the conservative management. This resulted in a stricter selection for operative treatment, and a longer waiting time between the onset of symptoms and intervention. This policy continued as a clinical practice after the end of the pandemic [30,31,32].
The current management of acute appendicitis renders the selection of the antibiotic regimen extremely important for an optimal effect on the pathogenic factors, and achievement of the better possible outcome [33]. Therefore, the knowledge of the most common bacteria which are implicated in this process is of great value. The bacterial flora of the appendix and/or the peritoneal cavity in children with acute appendicitis has been described in numerous studies [18,34,35,36,37,38,39,40,41,42,43,44,45,46]. The association between certain bacteria and the stage of appendicitis has been investigated as well [18,34,35,39,42,43,45,46].
Traditional culture techniques [18,34,35,36,37,38,39,40], culture-independent methods like rRNA or rDNA gene sequencing [41,42,43,44,45], or both [46], have been used to investigate the microbial content and its role in the different grades of appendicitis. Supporters of the gene sequencing studies reported that traditional cultures failed to identify the majority of the microorganisms [39], as children with acute appendicitis presented an abundance of the genera Fusobacteria and a decrease of the genera Bacteroides, compared to controls [42,44]. These studies reported association with severity of inflammation, but they did not reach statistical significance and did not assign causality [42,44].
Based on the theory that gene sequencing techniques cannot distinguish between viable and non-viable bacteria, other studies preferred traditional cultures, after collecting fluid from the peritoneal cavity [18,34,35,36,37,38,39,40]. Schülin, et al. collected samples from the lumen of the appendix [46]. This study was the only one to our knowledge, in which both traditional cultures and genetic material sequencing were simultaneously used [46].
E. coli is reported as the most common microorganism, followed by P. aeruginosa, Bacteroides spp and Streptococcus spp [28,34,35,36,37,38,39,40,46]. No statistically significant association has ever been reported between specific bacterial strains and the different stages of appendicitis, although in some studies P. aeruginosa was often identified in gangrenous and most severe forms of appendicitis [18,46]. Increase of Streptococcus milleri group has been reported in complicated cases as well [39,47].
Our results agreed with those of most of the studies, with E. Coli, P. aeruginosa and Streptococcus spp being the most frequent pathogens [18,34,35,36,37,38,39,40,48]. In perforated appendicitis, Streptococcus spp and P. aeruginosa were also common in the lumen, while Streptococcus spp and P. aeruginosa in the peritoneal cavity. However, in our study population, it was not certain species, but the categories and combinations of bacteria which presented statistically significant association with severe inflammation.
Given the high prevalence of P. aeruginosa, isolated in the cases of complicated appendicitis, antibiotic regimens with antipseudomonal activity in early clinical stages could potentially be considered more intensively in the future [49,50]. Furthermore, as conservative approach is currently under discussion for uncomplicated appendicitis, well designed studies may perhaps address this issue and clarify any possible effect of regimens, including anti-pseudomonas coverage in the outcome of such cases, versus standard antimicrobial care.
This study has certain limitations. We must also take into consideration that the age selection criteria resulted in outcomes representative of the study age group, as younger children, who represent an age group with higher prevalence of complicated appendicitis, have been excluded. The study population is limited, and the nature of the study is prospective cohort, instead of a randomized controlled one. Thus, further research is required to confirm the sample outcomes in a larger population, ideally through a multicenter approach.
5. Conclusions
E. coli, P. aeruginosa and Streptococcus spp are the most common microorganisms in children with acute appendicitis. However, the presence of more than one bacterium, both in the lumen of the appendix, and in the peritoneal cavity, seems to be the most important factor, associated with the severity of inflammation and the presence of complications. As non-invasive treatment of acute appendicitis gains more ground lately, antibiotic treatment should be targeted to combinations of the most often identified pathogens. In particular, application of regimens including antipseudomonal agents in a more routine way may become a game changer and might be considered for the early phases of the management.
Author Contributions
Conceptualization, K.Z. and X.S.; methodology, K.Z., F.K., D.G., S.F., X.S.; software, K.Z., S.F., and X.S.; validation, K.Z., F.K., and X.S.; formal analysis, K.Z., F.K., D.G., S.R., V.A., and X.S.; investigation, K.Z., A.P, V.A., S.R., G.G., and X.S.; resources, F.K., A.P., S.F., E.K., A.V., T.D., and G.G.; data curation, K.Z., F.K., A.P., D.G., E.K., S.R., A.V., T.D., and X.S.; writing—original draft preparation, K.Z., F.K., and X.S.; writing—review and editing, K.Z., F.K., A.P., D.G., S.F., V.A., E.K., S.R., A.V., T.D., G.G., and X.S.; visualization K.Z., F.K., A.P., D.G., S.F., V.A., E.K., S.R., A.V., T.D., G.G., and X.S.; supervision, X.S.; project administration, K.Z., F.K., G.G., and X.S.; All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Ethics Committee of the Patras Children’s Hospital (2619/04.03.2019).
Informed Consent Statement
Informed consent was obtained from the parents of the patients involved in the study.
Data Availability Statement
Data is unavailable due to privacy.
Acknowledgments
We thank Prof. Athanasios Tsagkanos and Dr. Spyridon Skiadopoulos, for their valuable contribution to the statistical analysis of the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Viniol, A.; Keunecke, C.; Biroga, T.; Stadje, R.; Dornieden, K.; Bosner, S.; Donner-Banzhoff, N.; Haasenritter, J.; Becker, A. Studies of the symptom abdominal pain—A systematic review and metaanalysis. Family Practice 2014, 31, 517–529. [Google Scholar] [CrossRef] [PubMed]
- Glass, C.C.; Rangel, S.J. Overview, and diagnosis of acute appendicitis in children. Semin. Pediatr. Surg. 2016, 25, 198–203. [Google Scholar] [CrossRef] [PubMed]
- Mc Cabe, K.; Babl, F.E.; Dalton, S. ; Paediatric Research in Emergency Departments International Collaborative (PREDICT). Management of children with possible appendicitis: a survey of emergency physicians in Australia and New Zealand. Emerg. Med. Australas. 2014, 26, 481–486. [Google Scholar] [CrossRef] [PubMed]
- Colvin, J.M.; Bachur, R.; Kharbanda, A.T. Presentation of appendicitis in preadolescent children. Pediatr. Emerg. Care. 2007, 23, 849–855. [Google Scholar] [CrossRef] [PubMed]
- Kharbanda, A.B.; Taylor, G.A.; Fishman, S.J.; Bachur, R.G. A clinical decision rule to identify children at low risk for appendicitis. Pediatrics 2005, 116, 709–716. [Google Scholar] [CrossRef] [PubMed]
- Sakellaris, G.; Sinopidis, X.; Zachos, K.; Spyridakis, I. Acute appendicitis in children: Causes and treatment. In: Appendicitis-Causes and treatments, Intechopen, Eds., London, United Kingdom, 2023; eBook. [CrossRef]
- Lee, S.L.; Stark, R.; Yaghoubian, A.; Shekherdimian, S.; Kaji, A. Does age affect the outcomes and management of pediatric appendicitis? J. Pediatr. Surg. 2011, 46, 2342–2345. [Google Scholar] [CrossRef] [PubMed]
- Alloo, J.; Gerstle, T.; Shilyansky, J.; Ein, S.H. Appendicitis in children less than 3 years of age: a 28-year review. Pediatr. Surg. Int. 2004, 19, 777–779. [Google Scholar] [CrossRef] [PubMed]
- Panagidis, A.; Sinopidis, X.; Zachos, K.; Alexopoulos, V.; Vareli, A.; Varvarigou, A.; Georgiou, G. Neonatal perforated Amyand’s hernia presenting as an enterocutaneous scrotal fistula. Asian J. Surg. 2015, 38, 177–179. [Google Scholar] [CrossRef]
- Zachos, K.; Fouzas, S.; Kolonitsiou, F.; Skiadopoulos, S.; Gkentzi, D.; Karatza, A.; Marangos, M.; Dimitriou, G.; Georgiou, G.; Sinopidis, X. Prediction of complicated appendicitis risk in children. Eur. Rev. Med. Pharmacol. Sci. 2021, 25, 7346–7353. [Google Scholar] [CrossRef]
- Jones, B.; Demetriades, D.; Segal, I.; Burkitt, D.P. The prevalence of appendiceal fecaliths in patients with and without appendicitis. A comparative study from Canada and South Africa. Ann. Surgery 1985, 202, 80–82. [Google Scholar] [CrossRef]
- Nitecki, S.; Karmeli, R.; Sarr, M. Appendiceal calculi and fecaliths as indications for appendectomy. Surg. Gynecol. Obstet. 1990, 171, 185–188. [Google Scholar] [PubMed]
- Deng, Y.; Chang, D.C.; Zhang, Y.; Webb, J.; Gabre-Kidan, A.; Abdullah, F. Seasonal and day of the week variations of perforated appendicitis in US children. Pediatr. Surg. Int. 2010, 26, 691–696. [Google Scholar] [CrossRef]
- Andersson, R.; Hugander, A.; Thulin, A.; Nyström, P.O.; Olaison, G. Clusters of acute appendicitis further evidence for an infectious aetiology. Int. J. Epidemiol. 1995, 24, 829–833. [Google Scholar] [CrossRef] [PubMed]
- Kastritsi, O.; Sinopidis, X.; Barbagadakis, S.; Sakellaris, S.; Matzakanis, G.; Kastritsi, E.D.; Sakellaris, G. Non-operative management of acute appendicitis in children: single center, cohort study. Chirurgia 2022, 35, 138–142. [Google Scholar] [CrossRef]
- Di Saverio, S.; Podda, M.; De Simone, B.; Ceresoli, M.; Augustin, G.; Gori, A.; Boermeester, M.; Sartelli, M.; Coccolini, F.; Tarasconi, A.; De' Angelis, N.; Weber, D.G.; Tolonen, M.; Birindelli, A.; Biffl, W.; Moore, E.E.; Kelly, M.; Soreide, K.; Kashuk, J.; Ten Broek, R.; Gomes, C.A.; Sugrue, M.; Davies, R.J. Damaskos, D; Leppäniemi, A.; Kirkpatrick, A.; Peitzman, A.B.; Fraga, G.P.; Maier, R.V.; Coimbra, R.; Chiarugi, M.; Sganga, G.; Pisanu A.; De' Angelis, G.L.; Tan, E.; Van Goor, H.; Pata, F.; Di Carlo, I.; Chiara, O.; Litvin, A.; Campanile, F.C.; Sakakushev, B.; Tomadze, G.; Demetrashvili, Z.; Latifi, R.; Abu-Zidan, F.; Romeo, O.; Segovia-Lohse, H.; Baiocchi, G.; Costa, D.; Rizoli, S.; Balogh, Z.J.; Bendinelli, C.; Scalea, T.; Ivatury, R.; Velmahos, G.; Andersson, R.; Kluger, Y.; Ansaloni, L.; Catena, F. Diagnosis and treatment of acute appendicitis: 2020 update of the WSES Jerusalem guidelines. World J. Emerg. Surg. 2020, 15, 27. [Google Scholar] [CrossRef]
- Gomes, C.A.; Nunes, T.A.; Chebli, J.M.F.; Junior, C.S.; Gomes, C.C. Laparoscopic grading system of acute appendicitis: new insight for future trials. Surg. Laparosc. Endosc. Percutan. Tech. 2012, 22, 463–466. [Google Scholar] [CrossRef] [PubMed]
- Kroiča, J.; Reinis, A.; Mohit, K.; Delorme, M.; Broks, R.; Asare, L.; Berezovska, M.; Jansins, V.; Zviedre, A.; Engelis, A.; Saxena, A.; Petersons, A. Culture based evaluation of microbiota in children with acute appendicitis. Proceed. Latv. Acad. Sci. 2020, 74, 100–105. [Google Scholar] [CrossRef]
- Mariage, M.; Sabbagh, C.; Grelpois, G.; Prevot, F.; Darmon, I.; Regimbeau, J.M. Surgeon’s definition of complicated appendicitis: a prospective video survey study, Euroasian J. Hepatogastroenterol. 2019, 9, 1–4. [Google Scholar] [CrossRef]
- Vaos, G.; Dimopoulou, A.; Gkioka, E.; Zavras, N. Immediate surgery or conservative treatment for complicated acute appendicitis in children? A meta-analysis. J. Pediatr. Surg. 2019, 54, 1365–1371. [Google Scholar] [CrossRef]
- Coccolini, F.; Fugazzola, P.; Sartelli, M.; Cicuttin, E.; Sibilla, M.G.; Leandro, G.; De’ Angelis, G.L.; Gaiani, F.; Di Mario, F.; Tomasoni, M.; Catena, F.; Ansaloni, L. Conservative treatment of acute appendicitis. Acta Biomed. 2018, 89, 119–134. [Google Scholar] [CrossRef]
- Park, H.C.; Kim, M.J.; Lee, B.H. Randomized clinical trial of antibiotic therapy for uncomplicated appendicitis. Br. J. Surg. 2017, 104, 1785–1790. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L. The vermiform cecal appendix, expendable or essential? A narrative review. Curr. Opin. Gastroenterol. 2022, 38, 570–576. [Google Scholar] [CrossRef] [PubMed]
- Andersson, R.E. The natural history and traditional management of appendicitis revisited: spontaneous resolution and predominance of prehospital perforations imply that a correct diagnosis is more important than an early diagnosis. World J. Surg. 2007, 31, 86–92. [Google Scholar] [CrossRef] [PubMed]
- Vitetta, L.; Chen, J.; Clarke, S. The vermiform appendix: an immunological organ sustaining a microbiome inoculum. Clin. Sci. (Lond.) 2019, 133, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Randal Bollinger, R.; Barbas, A.S.; Bush, E.L.; Lin, S.S.; Parker, W. Biofilms in the large bowel suggest an apparent function of the human vermiform appendix. J. Theor. Biol. 2007, 21, 249, 826–831. [Google Scholar] [CrossRef]
- Cai, S.; Fan, Y.; Zhang, B.; Lin, J.; Yang, X.; Liu, Y.; Liu, J.; Ren, J.; Xu, H. Appendectomy is associated with alteration of human gut bacterial and fungal communities. Front. Microbiol. 2021, 12, 724980. [Google Scholar] [CrossRef]
- Maita, S.; Andersson, B.; Svensson, J.F.; Wester, T. Nonoperative treatment for nonperforated appendicitis in children: a systematic review and meta-analysis. Pediatr. Surg. Int. 2020, 36, 261–269. [Google Scholar] [CrossRef]
- Fugazzola, P.; Coccolini, F.; Tomasoni, M.; Stella, M.; Ansaloni, L. Early appendectomy vs. conservative management in complicated acute appendicitis in children: A meta-analysis. J. Pediatr. Surg. 2019, 54, 2234–2241. [Google Scholar] [CrossRef]
- Köhler, F.; Müller, S.; Hendricks, A.; Kastner, C.; Reese, L.; Boerner, K.; Flemming, S.; Lock, J.F. ; Germer, G-T.; Wiegering, A. Changes in appendicitis treatment during the COVID-19 pandemic – A systematic review and meta-analysis. Int. J. Surg. 2021, 95, 106148. [Google Scholar] [CrossRef]
- Köhler, F.; Acar, L.; van den Berg, A.; Flemming, S.; Kastner, C.; Müller, S.; Diers, J. ; Germer, C-T.; Lock, J.F.; L'hoest, H.; Marschall, U.; Wiegering, A. Impact of the COVID-19 pandemic on appendicitis treatment in Germany - a population - based analysis. Langenbecks Arch. Surg. 2021, 406, 377–383. [Google Scholar] [CrossRef]
- Willms, A.G.; Oldhafer, K.J.; Conze, S.; Thasler, W.E.; von Schassen, C.; Hauer, T.; Huber, T.; Germer, C.T.; Günster, S.; Bulian, D.R.; Hirche, Z.; Filser, J.; Stavrou, G.A.; Reichert, M.; Malkomes, P.; Seyfried, S.; Ludwig, T.; Hillebrecht, H.C.; Pantelis, D.; Brunner, S.; Rost, W.; Lock, J.F. ; CAMIN Study Group. Langenbecks Arch. Surg. 2021, 406, 367–375. [Google Scholar] [CrossRef] [PubMed]
- Podda, M.; Gerardi, C.; Cillara, N.; Fearnhead, N.; Gomes, C.A.; Birindelli, A.; Mulliri, A.; Davies, R.J.; Di Saverio, S. Antibiotic treatment and appendectomy for uncomplicated acute appendicitis in adults and children: a systematic review and meta-analysis. Ann. Surg. 2019, 270, 1028–1040. [Google Scholar] [CrossRef] [PubMed]
- Guillet-Caruba, C.; Cheikhelard, A.; Guillet, M.; Bille, E.; Descamps, P.; Yin, L.; Khen-Dunlop, N.; Berche, P.; Ferroni, A. Bacteriologic epidemiology and empirical treatment of pediatric complicated appendicitis. Diagn. Microbiol. Infect. Dis. 2011, 69, 376–381. [Google Scholar] [CrossRef] [PubMed]
- Schmitt, F.; Clermidi, P.; Dorsi, M.; Cocquerelle, V.; Gomes, C.F.; Becmeur, F. Bacterial studies of complicated appendicitis over a 20-year period and their impact on empirical antibiotic treatment. J. Pediatr. Surg. 2012, 47, 2055–2062. [Google Scholar] [CrossRef] [PubMed]
- Kadhim, M.M. Appendectomy in pediatrics: the value of peritoneal fluid smear and its bacteriological profile. Open J. Med. Microbiol. 2012, 2, 147–152. [Google Scholar] [CrossRef]
- Fallon, S.C.; Hassan, S. F, Larimer, E.L. Modification of an evidence-based protocol for advanced appendicitis in children. J. Surg. Res. 2013, 185, 273–277. [Google Scholar] [CrossRef] [PubMed]
- Obinwa, O.; Casidy, M.; Flynn, J. The microbiology of bacterial peritonitis due to appendicitis in children. Ir. J. Med. Sci. 2014, 183, 585–591. [Google Scholar] [CrossRef] [PubMed]
- Dabaja-Younis, H.; Farah, H.; Miron, R.; Geffen, Y.; Slijper, N.; Steinberg, R.; Kassis, I. The intraperitoneal bacteriology and antimicrobial resistance in acute appendicitis among children: a retrospective cohort study between the years 2007-2017. Eur. J. Pediatr. 2021, 180, 2091–2098. [Google Scholar] [CrossRef]
- Plattner, A.S.; Newland, J.G.; Wallendorf, M.J.; Shakhsheer, B.A. Management and microbiology of perforated appendicitis in pediatric patients: A 5-year retrospective study. Infect. Dis. Ther. 2021, 10, 2247–2257. [Google Scholar] [CrossRef]
- Zhong, D.; Brower-Sinning, R.; Firek, B.; Morowitz, M.J. Acute appendicitis in children is associated with an abundance of bacteria from the phylum Fusobacteria. J. Pediatr. Surg. 2014, 49, 441–446. [Google Scholar] [CrossRef]
- Jackson, H.T.; Mongodin, E.F.; Davenport, K.P.; Fraser, C.M.; Sandler, A.D.; Zeichner, S.L. Culture-independent evaluation of the appendix and rectum microbiomes in children with and without appendicitis. PLoS One 2014, 9, e95414. [Google Scholar] [CrossRef] [PubMed]
- Rogers, M.B.; Brower-Sinning, R.; Firek, B.; Zhong, D.; Morowitz, M.J. Acute appendicitis in children is associated with a local expansion of fusobacteria. Clin. Infect. Dis. 2016, 63, 71–78. [Google Scholar] [CrossRef] [PubMed]
- Salö, M.; Marungruang, N.; Roth, B.; Sundberg, T.; Stenstrom, P.; Arnbjörnsson, E.; Fak, F.; Ohlsson, B. Evaluation of the microbiome in children's appendicitis. Int. J. Colorectal Dis. 2017, 32, 19–28. [Google Scholar] [CrossRef] [PubMed]
- The, S.M.L.; Bakx, R.; Budding, A.E.; de Meij, T.G.J.; van der Lee, J.H.; Bunders, M.J.; Poort, L.; Heij, H.A.; van Heurn, L.W.E.; Gorter, R.R. Microbiota of children with complex appendicitis: different composition and diversity of the microbiota in children with complex compared with simple appendicitis. Pediatr. Infect. Dis. J. 2019, 38, 1054–1060. [Google Scholar] [CrossRef]
- Schülin, S.; Schlichting, N.; Blod, C.; Opitz, S.; Suttkus, A.; Stingu, C.S.; Barry, K.; Lacher, M.; Buhligen, U.; Mayer, S. The intra- and extraluminal appendiceal microbiome in pediatric patients: A comparative study. Medicine (Baltimore) 2017, 96, e9518. [Google Scholar] [CrossRef]
- Hardwick, R.H; Taylor, A.; Thompson, M.H.; Jones, E.; Roe, A.M. Association between Streptococcus milleri and abscess formation after appendicitis. Ann. R. Coll. Surg. Engl. 2000, 82, 24–26. [Google Scholar]
- Martin, B.; Subramanian, T.; Arul, S.; Patel, M.; Jester, I. Using microbiology culture in pediatric appendicitis to risk stratify patients: a cohort study. Surg. Infect. (Larchmt). 2023, 24, 183–189. [Google Scholar] [CrossRef]
- Theodorou, C.M.; Stokes, S.C.; Hegazi, M.S.; Brown, E.G. , Saadai, P. Is Pseudomonas infection associated with worse outcomes in pediatric perforated appendicitis? J. Pediatr. Surg. 2021, 56, 1826–1830. [Google Scholar] [CrossRef]
- Dreznik, Y.; Feigin, E.; Samuk, I.; Kravarusic, D.; Baazov, A.; Levy, I.; Livni, G.; Freud, E. Dual versus triple antibiotics regimen in children with perforated acute appendicitis. Eur. J. Pediatr. Surg. 2018, 28, 491–494. [Google Scholar] [CrossRef]
Figure 1.
Operative histopathologic findings of the study population.
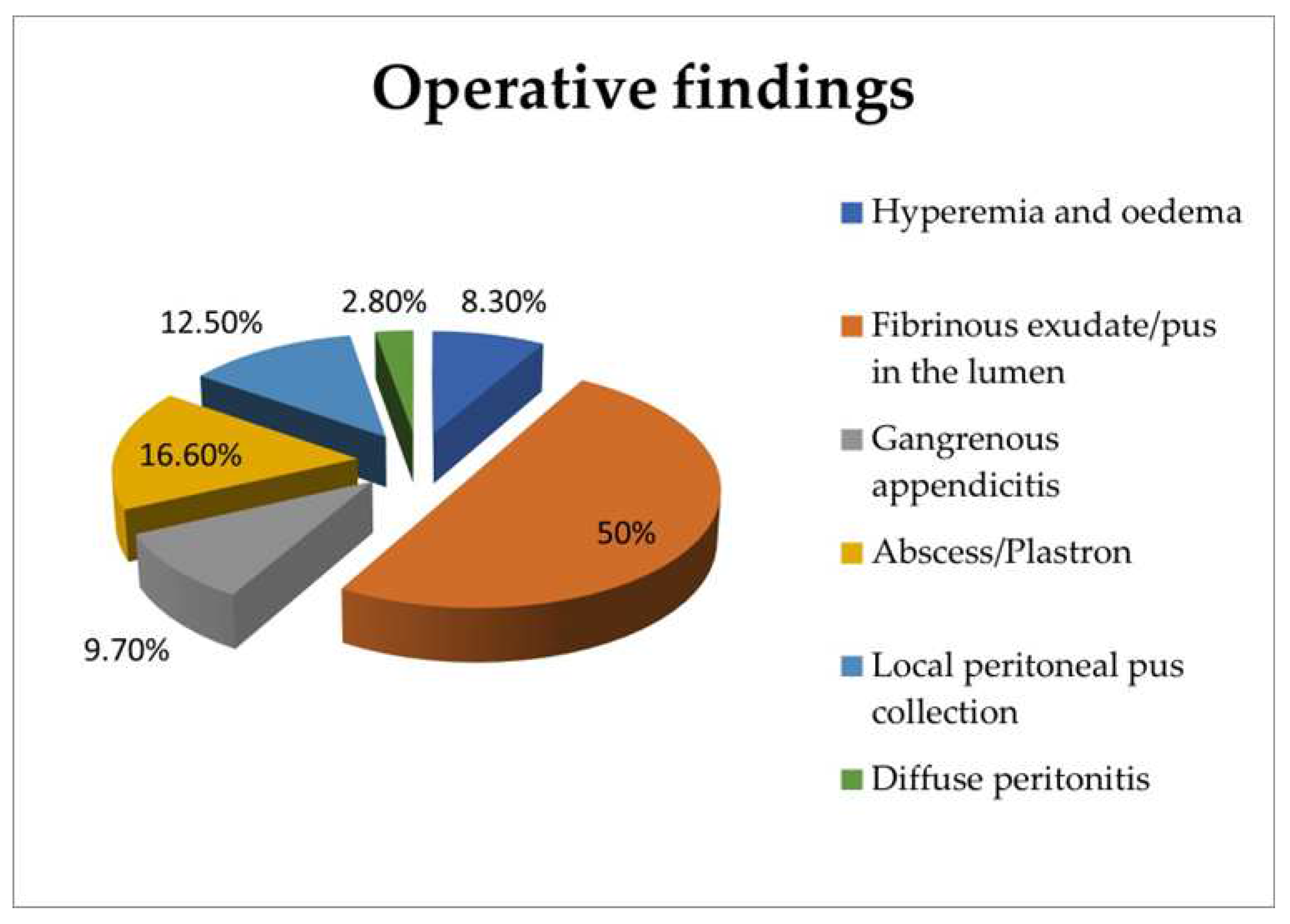

Table 1.
Demographic, clinical, and laboratory outcomes of the study population.
| Variables | Uncomplicated appendicitis | Complicated appendicitis | p-value |
|---|---|---|---|
| n | 42 | 30 | |
| Female | 16 | 13 | 0.444 |
| Male | 26 | 17 | 0.069 |
| Age (years) | 10.8 ± 2.4 | 10.4±3.0 | 0.449 |
| Weight (kg) | 41.5 ± 13.4 | 41.2±15.7 | 0.932 |
| Height (cm) | 151.5 ± 13.7 | 148.7±19 | 0.467 |
| BMI (kg/m2) | 17.6 ± 3.6 | 17.9±3.2 | 0.515 |
| RLQ tenderness | 41 (97.6%) | 30 (100%) | 0.583 |
| Excessive RLQ tenderness | 21 (50%) | 19 (63.3%) | 0.262 |
| Pain migration | 18 (42.9%) | 14 (46.7%) | 0.748 |
| Anorexia | 31 (73.8%) | 25 (83.3%) | 0.338 |
| Nausea/emesis | 28 (66.7%) | 27 (90%) | 0.022 |
| Temperature max (oC) | 37.3±0.8 | 38.0 ± 0.7 | <0.001 |
| WBC (10³/μL) | 14.0±3.5 | 16.0 ± 4.2 | 0.017 |
| Neutrophil count (10³/μL) | 11±3.6 | 13.5 ± 3.9 | 0.007 |
| Neutrophils % | 77.6 ± 8.8 | 83.6 ± 4,6 | <0.001 |
| Hb (g/dL) | 12.96 ± 1.02 | 12.93 ± .18 | 0.685 |
| CRP (mg/dL) | 3.4 ± 4.6 | 6.9 ± 5.9 | 0.015 |
Abbreviations: BMI: Body mass index, RLQ: Right lower quadrant, WBC: White blood cells, CRP: C-reactive protein.
Table 2.
Bacteria and their combinations as they were identified in the lumen of the appendix of the study population.
Table 2.
Bacteria and their combinations as they were identified in the lumen of the appendix of the study population.
| Bacteria | % |
|---|---|
| Escherichiacoli | 34.7 |
| Escherichia coli + Pseudomonas aeruginosa | 12.5 |
| Escherichia coli + Streptococcus spp | 9.7 |
| Escherichia coli + Enterococcus faecalis | 8.3 |
| Klebsiella pneumoniae | 6.9 |
| Escherichia coli + Bacteroides spp (non-fragilis) | 5.6 |
| Pseudomonas aeruginosa | 2.8 |
| Escherichia coli + Bacteroides fragilis | 2.8 |
| Bacteroides fragilis | 1.4 |
| Escherichia coli + Klebsiella pneumonia | 1.4 |
| Escherichia coli + Enterococcus avium | 1.4 |
| Escherichia coli + Enterococcus gallinarum | 1.4 |
| Escherichia coli + Proteus mirabilis | 1.4 |
| Streptococcus spp + Bacteroides spp | 1.4 |
| Escherichia coli + Propionebacterium spp | 1.4 |
| Escherichia coli + Pseudomonas aeruginosa + Enterococcus faecalis | 1.4 |
| Escherichia coli + Providencia rettgeri + Clostridium spp | 1.4 |
| Pseudomonas aeruginosa + Providencia rettgeri + Bacteroides ovatus | 1.4 |
| Pseudomonas aeruginosa + Klebsiella pneumoniae + Enterococcus faecalis | 1.4 |
| Escherichia coli + Streptococcus spp + Βacteroides spp + Enterobacter aerogenes | 1.4 |
Table 3.
Bacteria identified in the lumen of the appendix in uncomplicated and complicated appendicitis.
Table 3.
Bacteria identified in the lumen of the appendix in uncomplicated and complicated appendicitis.
| Bacteria | % |
|---|---|
| Uncomplicated appendicitis | |
| Escherichiacoli | 35.7 |
| Klebsiella pneumoniae | 11.9 |
| Escherichia coli + Pseudomonas aeruginosa | 11.9 |
| Escherichia coli + Enterococcus faecalis | 9.5 |
| Escherichia coli + Bacteroides spp (non-fragilis) | 7.1 |
| Pseudomonas aeruginosa | 4.8 |
| Escherichia coli + Streptococcus spp | 4.8 |
| Bacteroides fragilis | 2.4 |
| Escherichia coli + Enterococcus gallinarum | 2.4 |
| Escherichia coli + Bacteroides fragilis | 2.4 |
| Pseudomonas aeruginosa + Pseudomonas rettgeri + Bacteroides ovatus | 2.4 |
| Pseudomonas aeruginosa + Klebsiella pneumoniae + Enterococcus faecalis | 2.4 |
| Escherichia coli + Streptococcus spp + Bacteroides spp (non-fragilis) + Enterobacter aerogenes | 2.4 |
| Complicated appendicitis | |
| Escherichiacoli | 33.3 |
| Escherichia coli + Streptococcus spp | 16.7 |
| Escherichia coli + Pseudomonas aeruginosa | 13.3 |
| Escherichia coli + Enterococcus faecalis | 6.7 |
| Escherichia coli + Klebsiella pneumoniae | 3.3 |
| Escherichia coli + Bacteroides spp (non-fragilis) | 3.3 |
| Escherichia coli + Enterococcus avium | 3.3 |
| Escherichia coli + Enterococcus gallinarum | 3.3 |
| Escherichia coli + Bacteroides fragilis | 3.3 |
| Streptococcus spp + Bacteroides spp | 3.3 |
| Escherichia coli + Propionebacterium spp | 3.3 |
| Escherichia coli + Pseudomonas aeruginosa + Enterococcus faecalis | 3.3 |
| Escherichia coli + Providencia rettgeri + Clostridium spp | 3.3 |
Table 4.
Bacteria and their combinations as they were identified in the peritoneal cavity of the study population.
Table 4.
Bacteria and their combinations as they were identified in the peritoneal cavity of the study population.
| Bacteria | % |
|---|---|
| Escherichiacoli | 45.2 |
| Escherichia coli + Streptococcus spp | 12.9 |
| Escherichia coli + Pseudomonas aeruginosa | 9.7 |
| Enterococcus faecalis | 3.2 |
| Bacteroides fragilis | 3.2 |
| Klebsiella pneumoniae | 3.2 |
| Providencia rettgeri | 3.2 |
| Streptococcus spp | 3.2 |
| Escherichia coli + Enterococcus faecalis | 3.2 |
| Escherichia coli + Enterococcus avium | 3.2 |
| Escherichia coli + Enterococcus gallinarum | 3.2 |
| Streptococcus spp + Pseudomonas vesicularis | 3.2 |
| Klebsiella pneumoniae + Enterococcus faecalis | 3.2 |
Table 5.
Bacteria identified in the peritoneal cavity in uncomplicated and complicated appendicitis.
Table 5.
Bacteria identified in the peritoneal cavity in uncomplicated and complicated appendicitis.
| Bacteria | % |
|---|---|
| Uncomplicated appendicitis | |
| Escherichiacoli | 45.5 |
| Enterococcus faecalis | 9.1 |
| Bacteroides fragilis | 9.1 |
| Klebsiella pneumoniae | 9.1 |
| Providencia rettgeri | 9.1 |
| Escherichia coli + Pseudomonas aeruginosa | 9.1 |
| Enterococcus faecalis + Klebsiella pneumoniae | 9.1 |
| Complicated appendicitis | |
| Escherichiacoli | 45 |
| Escherichiacoli + Streptococcus spp | 20 |
| Escherichia coli + Pseudomonas aeruginosa | 10 |
| Streptococcus spp | 5 |
| Escherichia coli + Enterococcus faecalis | 5 |
| Escherichia coli + Enterococcus avium | 5 |
| Escherichia coli + Enterococcus gallinarum | 5 |
| Streptococcus spp + Pseudomonas vesicularis | 5 |
Table 6.
Logistic regression analysis tested the correlation of peritoneal fluid and appendiceal lumen cultures of patients with complicated appendicitis with monomicrobial and polymicrobial cultures. Statistically significant outcomes are shown in bold characters.
Table 6.
Logistic regression analysis tested the correlation of peritoneal fluid and appendiceal lumen cultures of patients with complicated appendicitis with monomicrobial and polymicrobial cultures. Statistically significant outcomes are shown in bold characters.
| Variable | Model value | Number of patients | |||
| Operative findings | Complicated appendicitis (2) | 30 | |||
| Uncomplicated appendicitis (1) | 42 | ||||
| Total | 72 | ||||
| Prediction coefficient | Coef. | SE Coef. | Z | p-value | Odds Ratio |
| Variable | -1.39208 | 1.57541 | -0.88 | 0.377 | |
| Peritoneal fluid culture (2) | 1.35473 | 0.385695 | 3.51 | 0.001 | 3.88 |
| Appendiceal lumen culture (2) | 0.658258 | 0.544083 | 1.21 | 0.226 | 1.93 |
| 95% CI | |||||
| Prediction coefficient | Lower | Upper | |||
| Variable | |||||
| Peritoneal fluid culture (2) | 1.82 | 8.25 | |||
| Appendiceal lumen culture (2) | 0.66 | 5.61 | |||
| Log-Likelihood = -41.802 | |||||
| Test that all slopes are zero: G = 22.504, DF = 4, p-value = 0.000 | |||||
| Goodness-of-fit tests | |||||
| Method | Chi square | DF | p-value | ||
| Pearson | 64.9860 | 56 | 0.192 | ||
| Deviance | 71.4668 | 56 | 0.080 | ||
| Hosmer-Lemeshow | 6.9920 | 8 | 0.537 | ||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



