
Submitted:
25 April 2023
Posted:
26 April 2023
You are already at the latest version
Abstract
Preliminary clinical data suggest pain reduction through fasting in different diagnoses. This uncontrolled observational clinical study examined the effects of prolonged modified fasting on pain and functional parameters in hip and knee osteoarthritis. Patients admitted to the inpatient department of Internal Medicine and Nature-based Therapies of the Immanuel Hospital Berlin between February 2018 and March 2020, answered questionnaires at the beginning and end of inpatient treatment, as well as 3, 6 and 12 months after discharge. Additionally, selected blood and anthropometric parameters were routinely assessed during the inpatient stay. Fasting was performed as part of a multimodal integrative treatment program, with daily caloric intake of <600 kcal for 7.7 ± 1.7 days. N=125 consecutive patients were included.
Results revealed an amelioration of overall symptomatology (WOMAC Index score: -14.8±13.31; p<0.001; d=0.78), and pain alleviation (NRS Pain: -2.7±1.98, p<0.001, d=1.48). Pain medication was reduced, stopped, or replaced by herbal remedies in 36% of patients. Improvements were also observed in secondary outcome parameters, including increased quality of life (WHO-5: +4.5±4.94, p<0.001, d=0.94), reduced anxiety (HADS-A: -2.1±2.91, p<0001, d=0.55) and depression (HADS-D: -2.3±3.01, p<0.001, d=0.65), decreases in body weight (-3.6 kg ± 1.65, p< 0.001, d=0.21), and blood pressure (systolic: -6.2±15.93, p<0.001, d= 0.43; diastolic: -3.7±10.55, p<0.001, d=0.43). Results suggest that patients with osteoarthritis of the lower extremities may profit from a prolonged fast embedded in a multimodal integrative treatment regarding quality of life, pain, and disease-specific functional parameters. Confirmatory RCTs are warranted to further investigate these hypotheses.
Keywords:
fasting
; caloric restriction
; osteoarthritis
; dietary intervention
; fasting-mimicking diet
; integrative medicine
; complementary medicine
; Traditional European Medicine
; nutrition
; multimodal in-tegrative treatment
1. Introduction
Osteoarthritis (OA) is the most common joint disorder worldwide [1] and involves inflammation and destruction of cartilaginous and adjacent bone structures, leading to pain, stiffness and disability [2]. Morbidity has been estimated at about 17.9% in German adults, its prevalence increasing with age and feminine gender [1]. Impairments in overall mobility are most pronounced in lower limb OA, while approximately half of OA patients have at least one knee joint, and a quarter of them at least one hip joint affected [1].
OA is also a prominent cause of disability worldwide [3]. Its symptoms, ranging from pain during physical activity to ankylosis, can include pain during rest or sleep, stiffness, and gait unsteadiness. OA also seems to be associated with higher incidence of mental health disorders, such as depression and suicidality, as well as higher cardiovascular risk [3]. Hence, it is obvious that OA consumes a substantial amount of healthcare resources, primarily due to joint replacement surgery costs [3].
Nutritional factors have been found to influence the prevention and management of knee and hip OA. The mechanisms discussed include weight loss, reduction of inflammation and promotion of antioxidation [4]. This has led to plant-based diets and the Mediterranean diet being suggested for patients suffering from OA of the lower limbs [4].
Fasting has been shown to activate, enhance and accelerate analogous mechanisms, inducing weight loss, anti-inflammation, cell-repair, stem cell production and antioxidation [5]. It also seems to improve mood and reduce pain perception due to serotonin enhancement [6]. Additionally, it can positively influence cardiometabolic risk factors, by increasing insulin sensitivity, reducing mammalian target of rapamycin (mTOR) activity and reducing unfavorable blood lipids [7,8]. The gut microbiome also changes during fasting, and it has been recently suggested by human and animal data that the microbiome is associated with OA disease progression [9]. Moreover, fasting has been reported to support long-term dietary and lifestyle changes by enhancing self-efficacy, opening a window of opportunity for creating new habits [10] and sensitizing taste, especially to salt and sugar.
It seems reasonable to infer that fasting could possibly support conventional OA care, as experimental data hold for influencing short and long-term pathomechanisms fueling OA progression. In one small uncontrolled study n=8 hip and n=12 knee OA patients fasted for one week with a daily intake of 300 kcal. The results showed pain reduction, improved articular function and improvement in weight, BMI and waist circumference [11]. Furthermore, there is evidence from clinical studies and a systematic review, supporting the efficacy of fasting in treating symptoms of rheumatoid arthritis [12,13,14,15].
In Germany, inpatient fasting in hospitals is usually offered as the main part of a multimodal individualized treatment plan, based on traditional European, nature-based medical concepts in some specialized departments [7,16]. For patients with OA this can include physiotherapy, moderate exercise, dietary counselling, cold or warm local applications, herbal medicines, and other methods. This renders it impossible to observe the effect of fasting only, as patients do not follow only one therapy at a time, as would be necessary for an efficacy RCT. Instead, it gives an excellent opportunity to examine the real-world implications of therapeutic fasting, as patients usually combine therapeutic options in clinical settings.
The aim of this observational study was to observe effects of a therapeutic prolonged fast offered to patients suffering from knee and/or hip OA during a multimodal hospital treatment with a focus on nature-based Traditional European Medicine (TEM) and complementary and integrative medicine (CIM).
2. Materials and Methods
2.1. Study design
This trial was designed as an explorative, single-arm, prospective, single-center, open-label, observational study. The study protocol was approved by the institutional review board of Charité Universitätsmedizin Berlin (Charitéplatz 1, 10117 Berlin) in October 2015 (ID: EA4/005/17), was registered with ClinicalTrials.gov (ClinicalTrials ID: NCT03785197) and conducted according to the standards of the Declaration of Helsinki. Written informed consent was obtained from all participants prior to study entry.
2.2. Setting
Participants were recruited between February 2018 and December 2020 at the Immanuel Hospital Berlin. This is a hospital of 195 beds with approximately 5000 inpatient admissions per year including orthopedic, surgical, rheumatological and osteological wards as well as ward for Internal Medicine and Nature-based Therapies (IMNT) ward of 60 beds and a day care clinic using nature-based (NB) and mind-body medicine approaches. Most patients are admitted by German statutory health insurance coverage, and few come as privately insured patients or self-payers.
The Department of IMNT at the Immanuel Hospital Berlin is one of the leading institutions regarding the application of NB and traditional medicinal approaches [17,18,19,20,21,22] including TEM [23,24,25,26,27,28,29]. It is especially experienced in applying prolonged fasting as a therapeutic intervention in diverse disease entities [6,16,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52].
It was decided to focus on the four most prevalent diagnoses for inpatient treatment in 2017, which included osteoarthritis (knee and hip- ICD-codes M17.9 and M16.9 respectively). The other diagnoses were rheumatoid arthritis (M06.9), fibromyalgia syndrome (M79.7) and type 2 diabetes mellitus (E11.61), the results for which will be reported elsewhere.
After admission to the inpatient department of IMNT and the first medical consultation, the main diagnosis, and an individual, multimodal treatment plan, including a dietary regimen, were determined. Based on these, study personnel screened patients for eligibility. If eligible, patients were informed in detail about the option to participate in the observational study. For details on eligibility criteria please refer to section “2.4 Participants”.
Study visits at the beginning and end of the inpatient treatment included validated questionnaires on patient-reported outcomes. The questionnaires were handed to the patients on a tablet in electronic form on the first or second as well as on one of the two last days of the inpatient treatment. Laboratory tests included in the standard procedures of the inpatient ward at admission and discharge were also assessed for study purposes. Data on the use of pain medication, blood pressure, body weight, side effects of fasting and their management were extracted from the documentation of nurses and doctors in the patient record after patients were discharged.
During their hospital stay, patients usually receive visits from the ward’s physicians four to five times a week while the nursing staff has daily contact with each patient. On the first day of the inpatient stay, a blood test is routinely performed. These blood tests usually include a complete blood count without differential, blood glucose, blood lipids, electrolytes, and standard parameters of kidney and liver function; if there are findings that need to be controlled, another blood test is prescribed by the responsible physician and performed towards the end of the inpatient stay. This routine was established before the commencement of this study and remained unchanged throughout the whole study period.
Follow-ups after three, six and twelve months were conducted through questionnaires only, either electronically (if e-mail addresses were provided by participants) or by mail.
2.3. Interventions
When fasting is prescribed by the physician as part of routine inpatient care, the first complete day of the hospital stay is a preparatory day with a light plant-based diet. The procedure is based on the consensus guidelines for fasting therapy [16]. On this day, the patient eats a calorie-reduced light diet of approximately 1200 kcal. This is accompanied by a TEM bowel cleansing procedure, which is induced by taking laxatives, such as Glauber's salt, or an enema. On the second day, fasting starts. It is usually scheduled for at least five days and a maximum of twelve days, the length depending on the individual constitution of the patient and the regulation of the inpatient stay according to diagnosis, disease severity and ICD-10 code. During fasting, only natural juices, unsweetened teas and water are consumed. The daily caloric intake is between 200 and 300 calories. During the SARS-CoV-2-pandemic, starting from April 2020 to the end of the study in December 2020, the prescribed fasting regimen was modified to a fasting mimicking diet (FMD), due to uncertainties about the role of fasting in the immunological response to SARS-CoV-2. Daily caloric intake was raised to a maximum of 600 kcal, including solid foods, like porridge, potatoes, steamed vegetables, and vegetable soups. Foods did not contain sugar or sweeteners and the salt content was reduced.
The inpatient fasting treatment is embedded in a set of other therapeutic interventions, which are prescribed by the doctor for each patient individually. The multimodal CIM/TEM treatment program is a defined and established concept, commonly reimbursed by German statutory health insurance companies. It consists of at least 120 minutes of non-pharmacological treatment modalities and lifestyle counselling per day and is tailored according to the individual patient's diagnosis and needs. These interventions comprise nutritional counselling, exercise, physiotherapy, thermal treatments, mind-body medicine elements and other aspects from traditional medicine. These treatments are a recommended part of traditional fasting as published earlier [16]. After the fasting days, the fast is broken on the last day by eating an apple. The following one to three days, depending on the length of the fast, solid foods are gradually reintroduced, following a light plant-based diet. During these days, medication that was paused or adapted during fasting to ensure a safe fast, is gradually reintroduced where necessary. After the fasting cure, usually a normocaloric plant-based diet is recommended as a follow-up diet.
2.4. Participants
All patients who received an inpatient treatment that included therapeutic fasting at the Department for IMNT at the Immanuel Hospital Berlin between February 2018 and December 2020 were screened for eligibility.
Inclusion criteria were an age between 18 and 85 years and written informed consent given during the first 24 hours of the inpatient treatment.
Patients with symptomatic gallstones, history of gout or eating disorders, cachexia or sarcopenia, acute psychosis, severe psychiatric pathologies and severe metabolic conditions like liver or kidney dysfunction insufficiency were excluded, as these conditions present contraindications for fasting [16].
Further exclusion criteria were language barriers, dementia or other major cognitive impairments, pregnancy or lactation and participation in any other study.
2.5. Variables
The main outcome was the Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC, Version 3.1), a validated questionnaire specific for osteoarthritis of the knee and the hip. We used the WOMAC Index in the 5-point Likert-scale version that gives a global score on a range between 0 and 96 points. Clinically relevant changes / minimal clinically important differences (MCID) for the WOMAC Index are 10 points for the newer 0-240 VAS/NRS scale [53] and thus 4 points for the 0-96 scale used here. Secondary outcomes included the Hospital Anxiety and Depression Scale (HADS), the Mindful Attention Awareness Scale (MAAS) and the WHO Quality of Life questionnaire (WHO-5). We also collected data for acute pain on a numerical rating scale (NRS), as documented in the patient record. A clinically relevant change for pain on the NRS has been defined as a reduction of one point, while a NRS change score of -2.0 have been associated with the concept of "much better" improvement [54]. Furthermore, body weight, blood pressure and medication were extracted from the patient record as well as triglycerides, total cholesterol, LDL and HDL.
2.6. Data collection/measurement
Questionnaires were filled in digitally with tablets during inpatient stay, and in digital or analogue form at follow ups, depending on patient preference. Blood samples that were collected under routine care conditions on the first day and, if deemed necessary by the responsible physician, also, on one of the last two days of the inpatient stay, have been used for study purposes. The fasting blood samples were taken by hospital physicians between 7.30 and 08.15 AM each day, before breakfast.
2.7. Bias
All limitations of observational studies apply here, among those a missing control group and randomization as well as the inevitable impossibility of blinding patients in nutritional interventions. Especially fasting can per se not be blinded, neither for the patient nor for the hospital personnel.
The study personnel were only involved in the recruitment of the participants and in ensuring that they filled out the questionnaires; however, they were not involved in any other aspect of the inpatient hospital stay. As such the study personnel had no influence on the length of fasting, any adjustments to therapeutic modalities, or any other direct or indirect influence on the patients’ therapy.
To detect any reporting bias during follow-ups connected to subjective improvement or deterioration of symptoms, we controlled for strong positive or negative responses to fasting.
2.8. Study size
Based on the data of previous years, it was estimated that during the 3 years of the study, n = 150 patients with OA, of which n = 125 would agree to participate in this study, would be admitted to the ward and would be prescribed therapeutic fasting as part of their inpatient treatment. In this setting of an exploratory pre-post-comparison using the t-test and standard parameters of alpha = 0.05 and beta = 0.20 (corresponding to a power of 80%), the number of n = 125 patients is sufficient to detect all large, medium and small effects with a minimal effect size of Cohen’s d >= 0.23. No interim analyses were planned or performed.
2.9. Statistical methods
In this explorative, observational, single-arm study, t-tests were used to compare participant’s scores and vital parameters between baseline (V0) and subsequent visits (V1= at discharge, V2= 3 months after baseline, V3= 6 months after baseline and V4= 12 months after baseline) by means of unadjusted t-tests. To estimate the effect size of the interaction, data for the primary endpoint (WOMAC and its subscales) were additionally analyzed for the subgroups of knee and hip OA by ANOVAs using the group affiliation (knee/hip) as a second factor next to the visits. As usual in exploratory studies, no correction for multiple testing (alpha adjustment) was applied.All analyses were based on the set of complete cases available for the individual questionnaire or parameter.
To determine whether there was a reporting bias connected to subjective improvement or deterioration of symptoms in the follow-ups, patients were subdivided according to their gains in the WOMAC score (primary endpoint) at V1 into high, medium, and low gainers. For subsequent follow-ups we cross-checked whether any subgroup was under- or over-represented.
3. Results
In this longitudinal, uncontrolled observational study, n = 125 hospitalized patients (n = 107 females and n = 18 males) with knee or hip OA undergoing inpatient prolonged medical fasting between 02/2018 and 12/2020 were recruited. For baseline characteristics please refer to Table 1. In n = 97 (78%) participants, OA mainly affected the knee joint(s), in n = 28 (22%) the hip joints. Patients were mostly between n = 50 and n = 65 years of age with an average of 61.3 (±10.2) years. The majority (n=108, 86.4%) reported a moderate to strong subjective sense of physical ill health during the two weeks preceding inpatient treatment, n=55 (44%) stated a moderate to strong affection of their psychological health in the same time frame. While most patients (n=86; 68%) were familiar with the concept of Integrative Medicine, for n = 83 (66.4%) it was the first hospital admission of this kind and n = 56 (44.8%) did not have previous experiences with therapeutic fasting. However, expectations of efficacy were moderately high (6.4 ±2.0) on a NRS (0-10) scale (Table 1).
During the stay, n=18 (14%) of the initial n = 125 patients discontinued participation in the study, leaving n = 107 patients for the V1 visit (86%). Between V1 and V2 the number of responding patients fell by n = 31 (25%) to n = 76 (61%), and n = 60 (48%) patients participated in the follow-up visits V3 and V4 (Figure 1).
Study participants fasted between 3 and 12 days during their hospital stay, with a peak between 7 and 9 days (7.73±1.70 days), cf. Figure 2a. There was a marked reduction of self-reported pain from 6.2 (±1.72) to 3.5 (±1.87) on a NRS ranging from 0 to 10 (corresponding to a drop of -2.7 points or –45%, T = 10.8, p < 0.001; cf. Figure 3a and Table 2). This reduction corresponds to a clinically significant improvement, exceeding the threshold for an improvement that feels “much better” for the patient. Fasting also resulted in a weight loss of 3.6 (±1.65) kg between the first day after hospital admission (day 1) and V1 (T = 23.3, p < = 0.001; cf. Figure 3b and Table 2). We decided against using the weight measure at V0 (admission day), as patients do not arrive at admission fasted, and thus participants had to be weighed on the morning of the day after admission (d01) to get a valid measurement by the wards personnel; cf. Table 2). The hospital stay was also associated with a discrete drop in systolic (-6.2 ± 15.9 mmHg, T = 4.2, p < 0.001) and a somewhat smaller reduction in diastolic blood pressure (-3.7 ± 10.6 mmHg, T = 3.7, p < 0.001) between V0 and V1 (Figure 3c and Table 2). Serum cholesterol levels sank noticeably from 239.2 ± 44.86 mg/dL to 201.1 ± 48.85 mg/dL (T=10.2, p < 0.001), as did levels for LDL (155.9 ± 38.27 mg/dL to 129.8 ± 46.91 mg/dL, T = 6.29, p <0.001), HDL 58.2 ± 13.80 mg/dL to 49.2 ± 12.61 mg/dL, T = 8.12, p < 0.001) and triglycerides (133.7 ± 66.42 mg/dL to 113.1 ± 47.25 mg/dL, T = 2.92, p = 0.005).
Pain medication was categorized into non-steroidal anti-inflammatory drugs (NSAID) on the one hand, including ibuprofen, diclofenac, coxibs, paracetamol, metamizole among others, and opioids/opiates on the other. Medications targeting neuropathic pain components such as carbamazepin or gabapentin, biologicals and corticosteroids were listed separately, as were herbal remedies. For the first two categories (NSAIDs and opioids) we applied a self-developed scale to approximate whether the dosage had been raised or reduced. On a scale from -2 (medication was stopped) and -1 (dosage was reduced significantly, including i.e., stopping of rescue medication or reduction from daily intake to rescue medication only), to 0 (no noteworthy change in dosage), +1 (new medication or 1,5 to 2,5-fold rise in dosage) and +2 (at least 3-fold increase of medication) we rated both categories separately (cf. Figure 2 b-d). Regarding medication used for neuropathic pain components, in n=3 patients medication remained stable, while n=1 patient reduced dosage during hospital stay. Biologicals or immunosuppressants were taken by n=2 patients, and the dosage remained stable during the inpatient stay. N=5 patients were taking corticosteroids at the beginning of fasting, and two reduced their medication notably during the stay, while one patient received corticosteroids as a new treatment during hospital stay. Herbal remedies were only taken by a minority of the patients at the time of admission and were prescribed to a larger number of patients during their hospital stay (Table 2).
Self-reported adverse effects of fasting were reported mainly during the first days and included mild headaches in approximately 50% of cases, feelings of hunger and reduced mood in approximately 20%, and gastrointestinal complaints and stronger headache/migraine in a further 10% of the patients. However, counterchecking these complaints in the medical records revealed that, except for mild headaches and nausea, most of these complaints were not reported to medical staff or nurses (see Figure 3d).
The pain reduction measured by the NRS shown above is mirrored by the results of the WOMAC Index. The overview in Figure 4a-d show that pain, joint stiffness, and constraints of physical function were, in each WOMAC subscale and globally, significantly reduced by approximately 40% across the stay. In detail, the global WOMAC global score was reduced by 14.9 points (on the 0-96 scale), thus exceeding the Minimum Clinically Important Difference (MCID) of 4. The finer depiction in Figure 3e-h indicates that this was true for all OA patients taken together as a group (black bars), as well as for those with knee OA (dark green bars) vs hip OA (light green bars) separately. Differences between the two subgroups were not significant.
Figures 4a-d additionally show long-term effects. As expected, the strong effect faded towards the follow-up visits after 3, 6 and 12 months (V2, V3, and V4, respectively). However, even after 12 months (V4), values for stiffness were still reduced by 15% in comparison to baseline values, while the effects were even better on the WOMAC Global Index score, as well as on the subscales for pain and physical function, with a remaining significant reduction of 25% compared to baseline values (for details see Table 3). The reductions between baseline and V2 for pain, and between baseline and all visits for the other three subscales represent moderate-sized effects (Cohen’s d >= 0.50).
Similar effects were observed for the quality of life measured by the WHO-5 questionnaire (Figure 4e). The score increases from 11.1 (±4.74) at baseline to 15.4 (±4.75; T = 9.3, p < 0.001) and stays at an elevated level (14.3 ± 4.61) until V4, again with moderate effect sizes of d >= 0.5.
The increase of the MAAS questionnaire score, measuring mindfulness, (3.9±0.87 to 4.1±0.77, T = 4.1, p <=0.001) has a smaller effect size (d= 0.29) and lasts until V4 (Figure 4f).
Notable reductions were also registered for anxiety (10.3 ± 3.73 to 8.2 ± 3.69, T = 7.28, p < 0.001; cf. Figure 4g) and depression (10.89 ±3.74 to 8.5 ± 3.32, T = 7.9, p < 0.001, cf. Figure 4h) measured by the HADS depression and anxiety questionnaire. Both effect sizes were moderate between V0-V1. The effects remained on a similar level (d>0.5) until after the first follow-up visit (V2).
In a final test, we checked whether the positive long-term results could be due to a selective loss to follow-up of those who did not gain strongly from the interventions. However, identifying and tracking those who gained most, moderately, and least revealed that losses to follow up happened to a larger extent in patients that had gained either most or least during the stay and to a smaller extent in the central group. In conclusion, the long-term results seem not to stem from a selective loss of those who had gained less from the intervention.
4. Discussion
In this explorative, single-arm, prospective, single-center, open-label, observational study prolonged modified fasting with a max. intake of 600 kcal daily, an average duration of 8 days and embedded in a complex therapeutic inpatient CIM/TEM intervention, resulted in improvements in several parameters relevant to osteoarthritis of the knee and hip. Relevant improvements were observed for patient-reported outcomes on pain, functionality, and quality of life as well as for clinical, anthropometric and laboratory parameters.
In osteoarthritis, pain often is one of the leading symptoms that makes up for much of the disease burden and need for medication. Our data show a decrease in subjective and objective measures of pain with clinical significance. In the WOMAC Index subscale for pain we observed a drop in experienced pain from hospital admission to discharge, and the effect seemed to last until one year post intervention. At the same time, data derived from the patient files show a pronounced reduction of reported pain on a numerical rating scale, exceeding a clinical rating of feeling “much better”. Dosage of pain medication remained stable or was reduced, in favor of the prescription of milder herbal remedies.
Functionality is another aspect important to OA patients. Impaired functionality not only in itself potentially lowers quality of life, but it also often contributes to less mobility and exercise and thus may increase cardiovascular and metabolic disease risk. Our results show a marked decrease of joint stiffness and physical impairment in the WOMAC Index subscales stiffness and physical function for the whole year post intervention, with effects reducing slightly over the course of time.
We suggest three main pathomechanisms for symptom reduction in OA through fasting. One is the anti-inflammatory effect of fasting that has been shown in animal and human studies [5,13,34,55]. This is probably mediated by cellular stress-response mechanisms such as autophagy, mitophagy and sirtuine-activation, as well as systemic hormonal and metabolic responses to nutrient deprivation [5,56]. Pathogenesis and symptomatology of OA seem to be partly mediated by low-grade inflammatory processes [57]. Additionally, during fasting, patients are educated on healthy nutrition, so that some may shift to a more plant-based diet following the fasting period. Healthy plant-based diets have been shown to possess anti-inflammatory properties [4]. Following a Mediterranean diet, also known to reduce systemic inflammation, has likewise shown symptom relief in OA patients [58]. Secondly, fasting contributes to weight loss [5], as we also saw in our sample. This may lessen mechanical load on the joints of the lower extremities, possibly contributing to pain reduction [59]. Furthermore, lipid metabolism is improved by fasting [60]. Even in patients with normal BMI, metabolic factors have shown to be associated with disease severity [61]. It seems that, apart from the above-mentioned systemic low-grade inflammation associated with higher visceral fat, cholesterol metabolism [62,63] and adipokines [59,61] play a pivotal role in disease progression as they activate diverse cartilage-degrading mechanisms. Thirdly, fasting has been shown to possess antioxidative capacities [5], that can also make up for part of the effect, as has been described for other nutritional therapeutic approaches to OA [4]. Oxidative processes have, in vitro and in vivo, been found to impact pathogenesis and disease severity in OA [63,64]. To which extent enhancement of serotonin pathways in the central nervous system [6] and the switch in the microbiota [35] that have been described in prolonged fasting play a role in this context cannot be determined yet.
Taking together the positive findings on pain and functionality, we expected to see quality of life increase in our data set. Quality of life measured by WHO-5, as well as depression and anxiety measured by the HADS questionnaire, showed marked improvements from V0 to V1 that were sustained for up to one year. This finding is in line with those from other studies that have shown that fasting affects mood and quality of life positively [30,65,66].
Metabolic parameters measured included anthropometric and laboratory parameters, such as weight and blood lipids. All decreased notably in the eight average days of fasting. This change is not only positive because of its swiftness and its above-mentioned effects on OA symptomatology. It may also merit attention because OA patients tend to carry a higher cardiovascular risk [3].
There are several limitations to this study. Firstly, there is no control group, a fact that significantly restricts the interpretability of the results. It was not possible to randomize inpatients to different groups, as hospitalized patients need and expect the optimal individual therapy possible; therefore, we chose an observational study design. All inpatients who were not prescribed a fasting intervention were assigned so due to contraindications, such as being underweight or having eating disorders and would not have served as a sensible control group. As dietary interventions per se do not lend themselves to blinding - neither for patients nor for medical personnel - this is one more methodological limitation which we were not able to avoid. Since the hospital program allows for individualized complex CIM/TEM therapies, it is difficult, if not impossible, to differentiate between the effects of fasting and those of the other interventions. However, in its traditional form, prolonged therapeutic fasting is regularly accompanied by some exercise and mind-body interventions. This is practiced to overcome hunger or other adverse effects, to support fasting adherence and to frame the exceptional experience of renouncing solid food for several days or even weeks [16]. Also, dietary changes of patients during the follow-ups were not recorded, which makes it impossible to differentiate effects of fasting per se from any dietary changes that shaped eating habits after the hospital stay. Furthermore, we did not differentiate OA with the commonly used Kellgren-Lawrence scale or other classifications. Finally, limitations of questionnaire follow-ups always include less responses over the course of time. However, in this study the response rates were relatively good, and the answers did not only come from patients who profited most from the hospital stay.
Considering all these limitations, our results can only serve as preliminary data showing feasibility, safety, and potential effects of a traditional therapeutic fasting approach in knee and hip OA patients. Safety and feasibility of fasting therapies have been shown for other indications, such as rheumatoid arthritis [30], fibromyalgia syndrome [43], diverse cardiometabolic conditions [7] and type 2 diabetes mellitus [38]. Effects on disease symptomatology have also been shown before in a small cohort of 30 OA patients [11], which included 20 patients with OA of the lower limbs.
In summary, fasting could hold promising therapeutic potential for both the immediate and the secondary disease burden of knee and hip OA. Future studies should on the one hand provide control groups and more rigorously controlled conditions. On the other hand, the pragmatic exploration of therapeutic fasting or fasting-mimicking diets in outpatient settings under their real-life conditions seems equally warranted. From a perspective of health economy, it would be interesting to investigate cost-effectiveness, considering savings related to medication and its side-effects, necessity for other therapies, as well as sick days leave. If a short-term dietary intervention like a 5-10 day fast could influence joint health in a clinically meaningful and sustainable way, it seems worthwhile to be explored further.
5. Conclusions
Prolonged modified fasting could potentially support patients with OA of the knee or hip as part of an integrative multimodal approach for this common chronic condition.
Funding
This research received no external funding. All costs were covered by the Immanuel Hospital Berlin, where the research was conducted.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the institutional review board of Charité Universitätsmedizin Berlin (Charitéplatz 1, 10117 Berlin) in October 2015 (ID: EA4/137/15).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Data can be obtained from the corresponding author on justified request.
Acknowledgments
Special thanks goes to our study nurses Miriam Rösner and Nadine Sylvester, who have contributed to this study with their diligent work, as well as to all the personnel on the ward that enabled this study through their precious everyday work. Our gratitude also goes to Dimitra Varvarezou, who has diligently edited the present manuscript.
Conflicts of Interest
AMi and DK have co-founded the Academy of Integrative Fasting (AIF). AMi is also Co-founder of the SALUFAST company and DK serves as a consultant for a mobile application on intermittent fasting (FASTIC) as well as a company producing plant-based supplements (EVERYYIN). All other authors declare no conflict of interest related to this manuscript.
References
- RKI. 12-Monats-Prävalenz von Arthrose in Deutschland: RKI; 2017 [Available from: https://www.rki.de/DE/Content/Gesundheitsmonitoring/Gesundheitsberichterstattung/GBEDownloadsJ/FactSheets/JoHM_03_2017_Praevalenz_Arthrose.pdf.
- Knapik JJ, Pope R, Orr R, Schram B. Osteoarthritis: Pathophysiology, Prevalence, Risk Factors, and Exercise for Reducing Pain and Disability. J Spec Oper Med. 2018;18(3):94-102. [CrossRef]
- Vina ER, Kwoh CK. Epidemiology of osteoarthritis: literature update. Curr Opin Rheumatol. 2018;30(2):160-7. [CrossRef]
- Wei N, Dai Z. The Role of Nutrition in Osteoarthritis: A Literature Review. Clin Geriatr Med. 2022;38(2):303-22. [CrossRef]
- Di Francesco A, Di Germanio C, Bernier M, de Cabo R. A time to fast. Science. 2018;362(6416):770-5. [CrossRef]
- Michalsen, A. Prolonged fasting as a method of mood enhancement in chronic pain syndromes: a review of clinical evidence and mechanisms. Curr Pain Headache Rep. 2010;14(2):80-7. [CrossRef]
- Wilhelmi de Toledo F, Grundler F, Bergouignan A, Drinda S, Michalsen A. Safety, health improvement and well-being during a 4 to 21-day fasting period in an observational study including 1422 subjects. PLoS One. 2019;14(1):e0209353. [CrossRef]
- Drinda S, Grundler F, Neumann T, Lehmann T, Steckhan N, Michalsen A, et al. Effects of Periodic Fasting on Fatty Liver Index-A Prospective Observational Study. Nutrients. 2019;11(11). [CrossRef]
- Hasanpour-Dehkordi A, Kabiri F, Dris F. Comparing the Effects of Massage Therapy and Aromatherapy on Knee Pain, Morning Stiffness, Daily Life Function, and Quality of Life in Patients with Knee Osteoarthritis. Complement Med Res. 2021;28(4):292-9. [CrossRef]
- Ring RM, Eisenmann C, Kandil FI, Steckhan N, Demmrich S, Klatte C, et al. Mental and Behavioural Responses to Baha'i Fasting: Looking behind the Scenes of a Religiously Motivated Intermittent Fast Using a Mixed Methods Approach. Nutrients. 2022;14(5). [CrossRef]
- Schmidt S, Stange R, Lischka E, Kiehntopf M, Deufel T, Loth D, et al. [Uncontrolled clinical study of the efficacy of ambulant fasting in patients with osteoarthritis]. Forsch Komplementmed. 2010;17(2):87-94. [CrossRef]
- Kjeldsen-Kragh J, Sumar N, Bodman-Smith K, Brostoff J. Changes in glycosylation of IgG during fasting in patients with rheumatoid arthritis. Br J Rheumatol. 1996;35(2):117-9. [CrossRef]
- Kjeldsen-Kragh J, Mellbye OJ, Haugen M, Mollnes TE, Hammer HB, Sioud M, et al. Changes in laboratory variables in rheumatoid arthritis patients during a trial of fasting and one-year vegetarian diet. Scand J Rheumatol. 1995;24(2):85-93. [CrossRef]
- Kjeldsen-Kragh J, Haugen M, Borchgrevink CF, Laerum E, Eek M, Mowinkel P, et al. Controlled trial of fasting and one-year vegetarian diet in rheumatoid arthritis. Lancet. 1991;338(8772):899-902. [CrossRef]
- Muller H, de Toledo FW, Resch KL. Fasting followed by vegetarian diet in patients with rheumatoid arthritis: a systematic review. Scand J Rheumatol. 2001;30(1):1-10. [CrossRef]
- Wilhelmi de Toledo F, Buchinger A, Burggrabe H, Holz G, Kuhn C, Lischka E, et al. Fasting therapy - an expert panel update of the 2002 consensus guidelines. Forsch Komplementmed. 2013;20(6):434-43.
- Fischer JM, Kandil FI, Kessler CS, Nayeri L, Zager LS, Rocabado Hennhofer T, et al. Stress Reduction by Yoga versus Mindfulness Training in Adults Suffering from Distress: A Three-Armed Randomized Controlled Trial including Qualitative Interviews (RELAX Study). J Clin Med. 2022;11(19). [CrossRef]
- Kessler CS, Jeitler M, Dhiman KS, Kumar A, Ostermann T, Gupta S, et al. Ayurveda in Knee Osteoarthritis-Secondary Analyses of a Randomized Controlled Trial. J Clin Med. 2022;11(11). [CrossRef]
- Bringmann HC, Michalsen A, Jeitler M, Kessler CS, Brinkhaus B, Brunnhuber S, et al. Meditation-based lifestyle modification in mild to moderate depression-A randomized controlled trial. Depress Anxiety. 2022;39(5):363-75. [CrossRef]
- Jeitler M, Michalsen A, Schwiertz A, Kessler CS, Koppold-Liebscher D, Grasme J, et al. Effects of a Supplement Containing a Cranberry Extract on Recurrent Urinary Tract Infections and Intestinal Microbiota: A Prospective, Uncontrolled Exploratory Study. J Integr Complement Med. 2022;28(5):399-406. [CrossRef]
- Jeitler M, Wottke T, Schumann D, Puerto Valencia LM, Michalsen A, Steckhan N, et al. Ayurvedic vs. Conventional Nutritional Therapy Including Low-FODMAP Diet for Patients With Irritable Bowel Syndrome-A Randomized Controlled Trial. Front Med (Lausanne). 2021;8:622029. [CrossRef]
- Jeitler M, Michalsen A, Frings D, Hubner M, Fischer M, Koppold-Liebscher DA, et al. Significance of Medicinal Mushrooms in Integrative Oncology: A Narrative Review. Front Pharmacol. 2020;11:580656. [CrossRef]
- Jeitler M, Roth S, Steckhan N, Meier L, Koppold-Liebscher DA, Kandil FI, et al. Therapeutic Phlebotomy in Patients with Grade 1 Hypertension: A Randomized-Controlled Trial. J Integr Complement Med. 2022;28(6):530-9. [CrossRef]
- Hohmann CD, Stange R, Steckhan N, Robens S, Ostermann T, Paetow A, et al. The Effectiveness of Leech Therapy in Chronic Low Back Pain. Dtsch Arztebl Int. 2018;115(47):785-92. [CrossRef]
- Michalsen A, Ludtke R, Cesur O, Afra D, Musial F, Baecker M, et al. Effectiveness of leech therapy in women with symptomatic arthrosis of the first carpometacarpal joint: a randomized controlled trial. Pain. 2008;137(2):452-9. [CrossRef]
- Michalsen A, Klotz S, Ludtke R, Moebus S, Spahn G, Dobos GJ. Effectiveness of leech therapy in osteoarthritis of the knee: a randomized, controlled trial. Ann Intern Med. 2003;139(9):724-30. [CrossRef]
- Michalsen A, Moebus S, Spahn G, Esch T, Langhorst J, Dobos GJ. Leech therapy for symptomatic treatment of knee osteoarthritis: results and implications of a pilot study. Altern Ther Health Med. 2002;8(5):84-8.
- Michalsen A, Ludtke R, Buhring M, Spahn G, Langhorst J, Dobos GJ. Thermal hydrotherapy improves quality of life and hemodynamic function in patients with chronic heart failure. Am Heart J. 2003;146(4):728-33. [CrossRef]
- Jeitler M, Jaspers J, von Scheidt C, Koch B, Michalsen A, Steckhan N, et al. Mind-body medicine and lifestyle modification in supportive cancer care: A cohort study on a day care clinic program for cancer patients. Psychooncology. 2017;26(12):2127-34. [CrossRef]
- Hartmann AM DOM, Spoo M, Fischer JM, Steckhan N, Jeitler M, Häupl T, Kandil FI, Michalsen A, Koppold-Liebscher DA and Kessler C. To eat or not to eat—an exploratory randomized controlled.
- trial on fasting and plant-based diet in rheumatoid arthritis (NutriFast-study).. Front Nutr 2022;9:1030380.
- Jeitler M, Lauche R, Hohmann C, Choi KA, Schneider N, Steckhan N, et al. A Randomized Controlled Trial of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: Effects on Patient-Reported Outcomes. Nutrients. 2022;14(17). [CrossRef]
- Cramer H, Hohmann C, Lauche R, Choi KA, Schneider N, Steckhan N, et al. Effects of Fasting and Lifestyle Modification in Patients with Metabolic Syndrome: A Randomized Controlled Trial. J Clin Med. 2022;11(16). [CrossRef]
- Koppold-Liebscher DA, Klatte C, Demmrich S, Schwarz J, Kandil FI, Steckhan N, et al. Effects of Daytime Dry Fasting on Hydration, Glucose Metabolism and Circadian Phase: A Prospective Exploratory Cohort Study in Baha'i Volunteers. Front Nutr. 2021;8:662310.
- Hartmann AM, Dell'Oro M, Kessler CS, Schumann D, Steckhan N, Jeitler M, et al. Efficacy of therapeutic fasting and plant-based diet in patients with rheumatoid arthritis (NutriFast): study protocol for a randomised controlled clinical trial. BMJ open. 2021;11(8):e047758. [CrossRef]
- Maifeld A, Bartolomaeus H, Löber U, Avery EG, Steckhan N, Markó L, et al. Fasting alters the gut microbiome reducing blood pressure and body weight in metabolic syndrome patients. Nat Commun. 2021;12(1):1970. [CrossRef]
- Koppold-Liebscher D, Kessler CS, Steckhan N, Bahr V, Kempter C, Wischnewsky M, et al. Short-term fasting accompanying chemotherapy as a supportive therapy in gynecological cancer: protocol for a multicenter randomized controlled clinical trial. Trials. 2020;21(1):854. [CrossRef]
- Bahr LS, Bock M, Liebscher D, Bellmann-Strobl J, Franz L, Pruss A, et al. Ketogenic diet and fasting diet as Nutritional Approaches in Multiple Sclerosis (NAMS): protocol of a randomized controlled study. Trials. 2020;21(1):3. [CrossRef]
- Li C, Sadraie B, Steckhan N, Kessler C, Stange R, Jeitler M, et al. Effects of A One-week Fasting Therapy in Patients with Type-2 Diabetes Mellitus and Metabolic Syndrome - A Randomized Controlled Explorative Study. Exp Clin Endocrinol Diabetes. 2017;125(9):618-24. [CrossRef]
- Choi IY, Piccio L, Childress P, Bollman B, Ghosh A, Brandhorst S, et al. A Diet Mimicking Fasting Promotes Regeneration and Reduces Autoimmunity and Multiple Sclerosis Symptoms. Cell Rep. 2016;15(10):2136-46. [CrossRef]
- Michalsen A, Li C. Fasting therapy for treating and preventing disease - current state of evidence. Forsch Komplementmed. 2013;20(6):444-53. [CrossRef]
- Stange R, Pflugbeil C, Michalsen A, Uehleke B. Therapeutic fasting in patients with metabolic syndrome and impaired insulin resistance. Forsch Komplementmed. 2013;20(6):421-6. [CrossRef]
- Li C, Ostermann T, Hardt M, Ludtke R, Broecker-Preuss M, Dobos G, et al. Metabolic and psychological response to 7-day fasting in obese patients with and without metabolic syndrome. Forsch Komplementmed. 2013;20(6):413-20. [CrossRef]
- Michalsen A, Li C, Kaiser K, Ludtke R, Meier L, Stange R, et al. In-Patient Treatment of Fibromyalgia: A Controlled Nonrandomized Comparison of Conventional Medicine versus Integrative Medicine including Fasting Therapy. Evid Based Complement Alternat Med. 2013;2013:908610. [CrossRef]
- Michalsen A, Li C, Kaiser K, Lüdtke R, Meier L, Stange R, et al. In-Patient Treatment of Fibromyalgia: A Controlled Nonrandomized Comparison of Conventional Medicine versus Integrative Medicine including Fasting Therapy. Evid Based Complement Alternat Med. 2013;2013:908610. [CrossRef]
- Abendroth A, Michalsen A, Ludtke R, Ruffer A, Musial F, Dobos GJ, et al. Changes of Intestinal Microflora in Patients with Rheumatoid Arthritis during Fasting or a Mediterranean Diet. Forsch Komplementmed. 2010;17(6):307-13. [CrossRef]
- Michalsen A, Frey UH, Merse S, Siffert W, Dobos GJ. Hunger and mood during extended fasting are dependent on the GNB3 C825T polymorphism. Ann Nutr Metab. 2009;54(3):184-8. [CrossRef]
- Michalsen A, Kuhlmann MK, Ludtke R, Backer M, Langhorst J, Dobos GJ. Prolonged fasting in patients with chronic pain syndromes leads to late mood-enhancement not related to weight loss and fasting-induced leptin depletion. Nutr Neurosci. 2006;9(5-6):195-200. [CrossRef]
- Michalsen A, Hoffmann B, Moebus S, Backer M, Langhorst J, Dobos GJ. Incorporation of fasting therapy in an integrative medicine ward: evaluation of outcome, safety, and effects on lifestyle adherence in a large prospective cohort study. J Altern Complement Med. 2005;11(4):601-7. [CrossRef]
- Michalsen A, Riegert M, Lüdtke R, Bäcker M, Langhorst J, Schwickert M, et al. Mediterranean diet or extended fasting's influence on changing the intestinal microflora, immunoglobulin A secretion and clinical outcome in patients with rheumatoid arthritis and fibromyalgia: an observational study. BMC Complement Altern Med. 2005;5:22. [CrossRef]
- Michalsen A, Schlegel F, Rodenbeck A, Ludtke R, Huether G, Teschler H, et al. Effects of short-term modified fasting on sleep patterns and daytime vigilance in non-obese subjects: results of a pilot study. Ann Nutr Metab. 2003;47(5):194-200. [CrossRef]
- Michalsen A, Schneider S, Rodenbeck A, Ludtke R, Huether G, Dobos GJ. The short-term effects of fasting on the neuroendocrine system in patients with chronic pain syndromes. Nutr Neurosci. 2003;6(1):11-8. [CrossRef]
- Michalsen A, Weidenhammer W, Melchart D, Langhorst J, Saha J, Dobos G. [Short-term therapeutic fasting in the treatment of chronic pain and fatigue syndromes--well-being and side effects with and without mineral supplements]. Forsch Komplementarmed Klass Naturheilkd. 2002;9(4):221-7.
- Clement ND, Bardgett M, Weir D, Holland J, Gerrand C, Deehan DJ. What is the Minimum Clinically Important Difference for the WOMAC Index After TKA? Clin Orthop Relat Res. 2018;476(10):2005-14.
- Ariani A, Bazzichi L, Sarzi-Puttini P, Salaffi F, Manara M, Prevete I, et al. The Italian Society for Rheumatology clinical practice guidelines for the diagnosis and management of fibromyalgia Best practices based on current scientific evidence. Reumatismo. 2021;73(2):89-105. [CrossRef]
- Oudmaijer CAJ, Minnee RC, Pol RA, van den Boogaard WMC, Komninos DSJ, van de Wetering J, et al. Fasting before living-kidney donation: effect on donor well-being and postoperative recovery: study protocol of a multicenter randomized controlled trial. Trials. 2022;23(1):18. [CrossRef]
- Hofer SJ, Carmona-Gutierrez D, Mueller MI, Madeo F. The ups and downs of caloric restriction and fasting: from molecular effects to clinical application. EMBO Mol Med. 2022;14(1):e14418. [CrossRef]
- Thijssen E, van Caam A, van der Kraan PM. Obesity and osteoarthritis, more than just wear and tear: pivotal roles for inflamed adipose tissue and dyslipidaemia in obesity-induced osteoarthritis. Rheumatology (Oxford). 2015;54(4):588-600.
- Morales-Ivorra I, Romera-Baures M, Roman-Vinas B, Serra-Majem L. Osteoarthritis and the Mediterranean Diet: A Systematic Review. Nutrients. 2018;10(8). [CrossRef]
- Tu C, He J, Wu B, Wang W, Li Z. An extensive review regarding the adipokines in the pathogenesis and progression of osteoarthritis. Cytokine. 2019;113:1-12. [CrossRef]
- Gabriel S, Ncube M, Zeiler E, Thompson N, Karlsen MC, Goldman DM, et al. A Six-Week Follow-Up Study on the Sustained Effects of Prolonged Water-Only Fasting and Refeeding on Markers of Cardiometabolic Risk. Nutrients. 2022;14(20). [CrossRef]
- Andersson M, Haglund E, Aili K, Bremander A, Bergman S. Associations between metabolic factors and radiographic knee osteoarthritis in early disease - a cross-sectional study of individuals with knee pain. BMC Musculoskelet Disord. 2022;23(1):938. [CrossRef]
- Papathanasiou I, Anastasopoulou L, Tsezou A. Cholesterol metabolism related genes in osteoarthritis. Bone. 2021;152:116076. [CrossRef]
- Song Y, Liu J, Zhao K, Gao L, Zhao J. Cholesterol-induced toxicity: An integrated view of the role of cholesterol in multiple diseases. Cell Metab. 2021;33(10):1911-25. [CrossRef]
- Ertürk C, Altay MA, Bilge A, Çelik H. Is there a relationship between serum ox-LDL, oxidative stress, and PON1 in knee osteoarthritis? Clin Rheumatol. 2017;36(12):2775-80.
- Fond G, Macgregor A, Leboyer M, Michalsen A. Fasting in mood disorders: neurobiology and effectiveness. A review of the literature. Psychiatry Res. 2013;209(3):253-8. [CrossRef]
- Watkins E, Serpell L. The Psychological Effects of Short-Term Fasting in Healthy Women. Front Nutr. 2016;3:27. [CrossRef]
Figure 1.
Flowchart of participants. Legend: FU = follow up, m = months, V = visit.
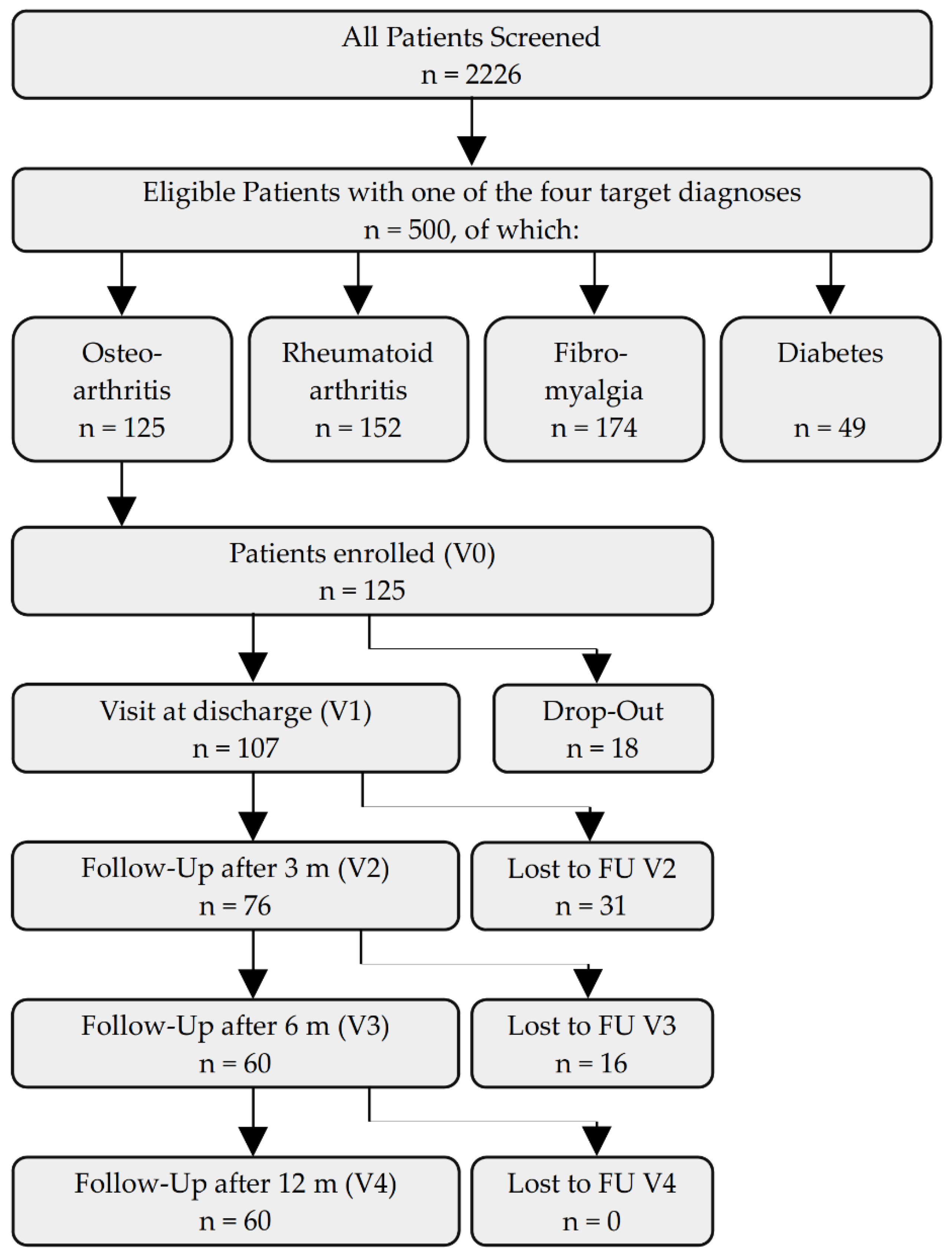
Figure 2.
(A) Histograms of the fasting duration (in days) and changes of the intake of pain medications during the inpatient hospital stay regarding (B) opioids, (C) other pain medication and (D) herbal remedies. In B-D: (-2) = medication was stopped, (-1) = dosage was substantially reduced, -0,5 change from daily intake of herbal remedies to rescue medication, (0) = no noteworthy change in dosage, (+0,5) = slight increase in dosage or new herbal remedies as rescue medication, (+1) = new medication or 1,5 to 2,5-fold rise in dosage, (+1,5) = new daily herbal remedy plus a herbal remedy as rescue medication, and (+2) = at least 3-fold increase of medication, or two new daily herbal remedies.
Figure 2.
(A) Histograms of the fasting duration (in days) and changes of the intake of pain medications during the inpatient hospital stay regarding (B) opioids, (C) other pain medication and (D) herbal remedies. In B-D: (-2) = medication was stopped, (-1) = dosage was substantially reduced, -0,5 change from daily intake of herbal remedies to rescue medication, (0) = no noteworthy change in dosage, (+0,5) = slight increase in dosage or new herbal remedies as rescue medication, (+1) = new medication or 1,5 to 2,5-fold rise in dosage, (+1,5) = new daily herbal remedy plus a herbal remedy as rescue medication, and (+2) = at least 3-fold increase of medication, or two new daily herbal remedies.

Figure 3.
Results for physiological data (a-c), side effects (d) and the WOMAC Index (on the traditional 0-96 point scale) (e-h). Overall, black bars indicate means and SDs for the whole group, while green and light green bars show results for the patients suffering mainly from knee and hip OA, respectively. In (d) black bars show percentages of side effects mentioned in the questionnaires, while gray bars indicate percentages of complaints expressed towards the ward team or physicians as documented in patient files. V0, V1, V2, V3, V4 = visit at the beginning and the end of the fasting stay and after 3, 6 and 12 months. d00 indicates the day of admission (noon), d01 the day after admission, in which the measurements were done in a standardized mode in the morning.
Figure 3.
Results for physiological data (a-c), side effects (d) and the WOMAC Index (on the traditional 0-96 point scale) (e-h). Overall, black bars indicate means and SDs for the whole group, while green and light green bars show results for the patients suffering mainly from knee and hip OA, respectively. In (d) black bars show percentages of side effects mentioned in the questionnaires, while gray bars indicate percentages of complaints expressed towards the ward team or physicians as documented in patient files. V0, V1, V2, V3, V4 = visit at the beginning and the end of the fasting stay and after 3, 6 and 12 months. d00 indicates the day of admission (noon), d01 the day after admission, in which the measurements were done in a standardized mode in the morning.
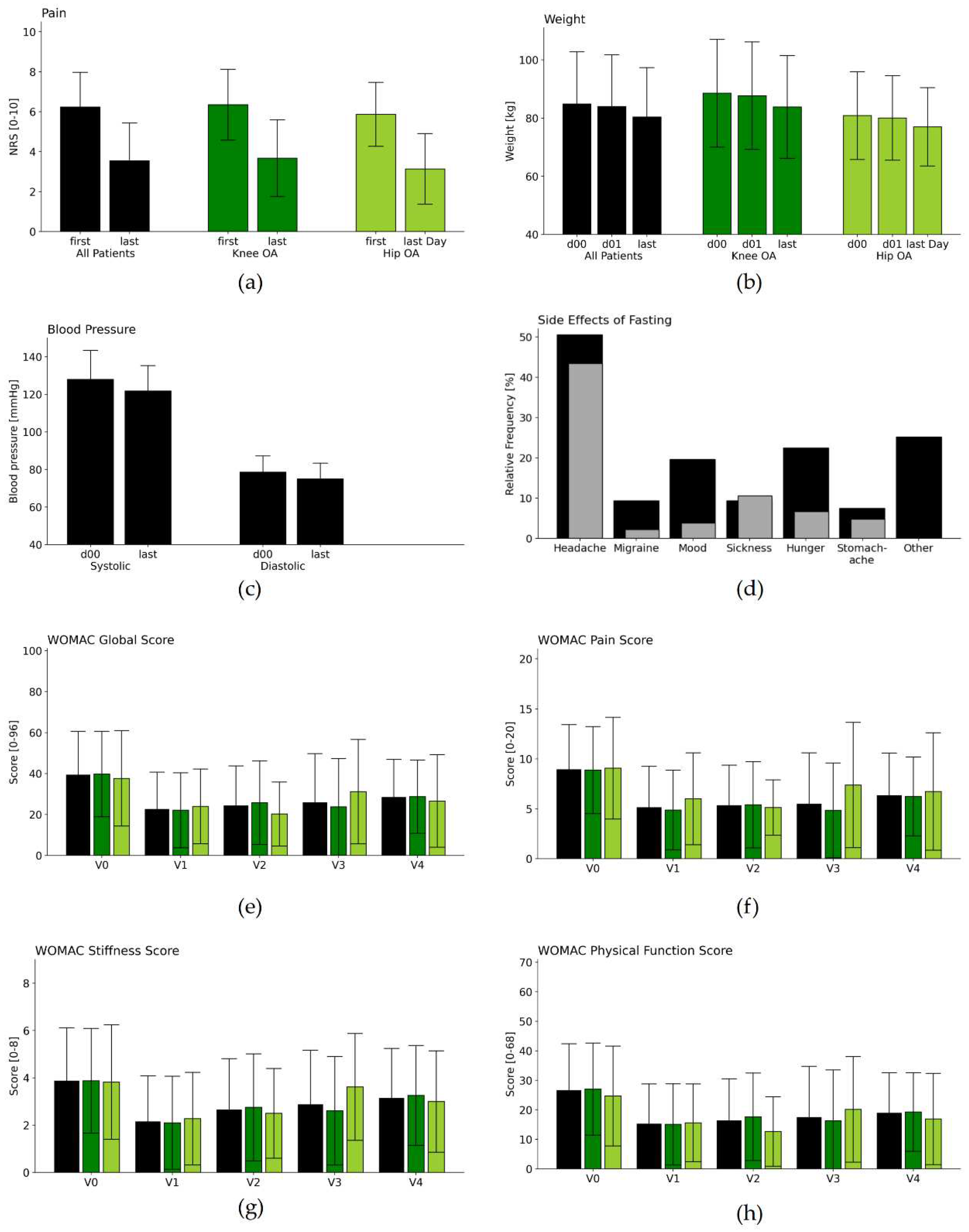
Figure 4.
Questionnaire results. Results from the validated WOMAC Index (on the traditional 0-96 point scale) (a-d), WHO-5 (e), MAAS (f), and HADS (g and h) across the five visits V0, V1, V2, V3, V4, i.e., at the beginning and the end of the fasting stay and after 3, 6 and 12 months. Higher values in WHO-5 (e) and MAAS (f), and lower values in all other scores indicate better results in terms of the patients’ health.
Figure 4.
Questionnaire results. Results from the validated WOMAC Index (on the traditional 0-96 point scale) (a-d), WHO-5 (e), MAAS (f), and HADS (g and h) across the five visits V0, V1, V2, V3, V4, i.e., at the beginning and the end of the fasting stay and after 3, 6 and 12 months. Higher values in WHO-5 (e) and MAAS (f), and lower values in all other scores indicate better results in terms of the patients’ health.
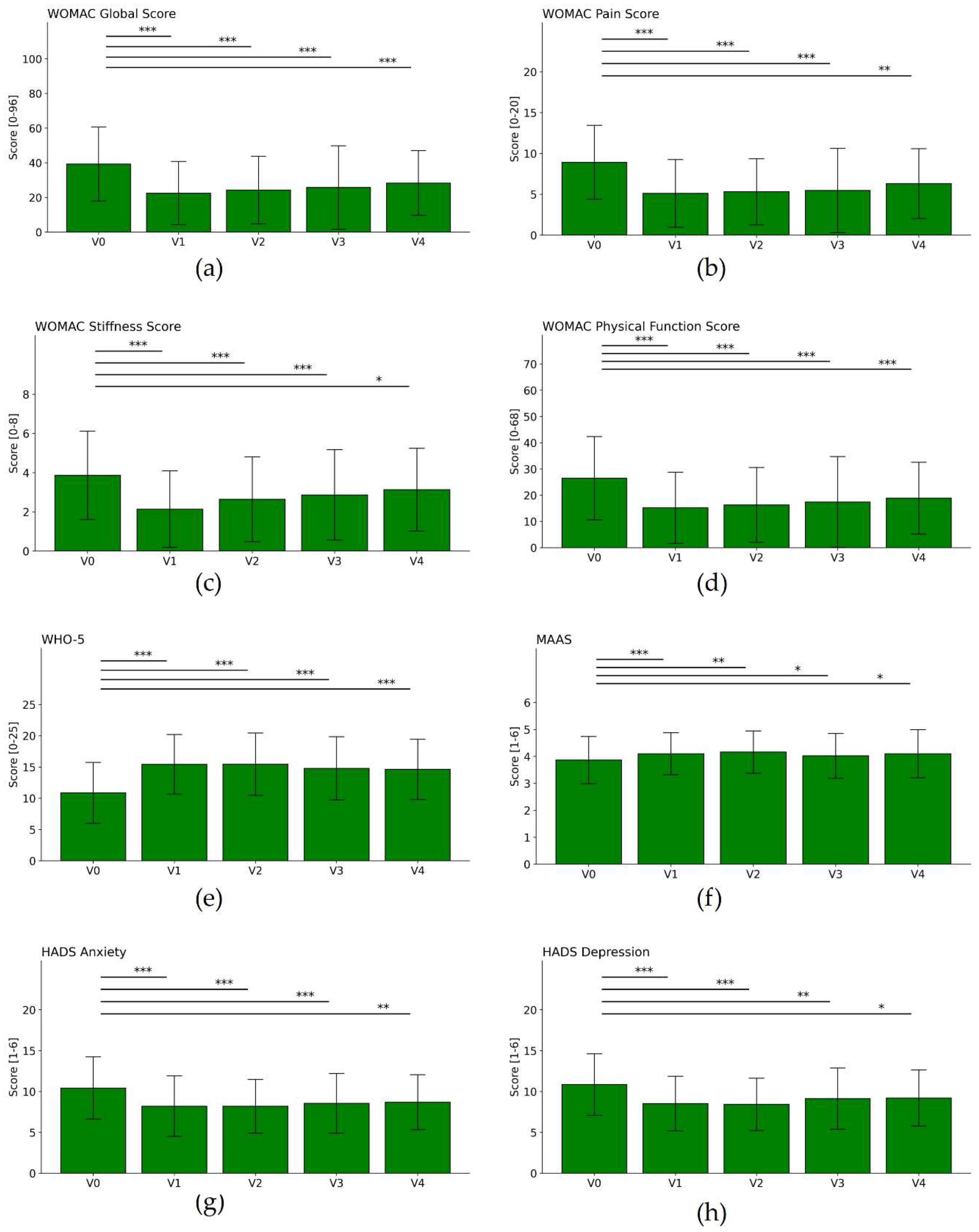

Table 1.
Baseline Characteristics.
| Parameter | Value | All Patients | Knee OA | Hip OA |
|---|---|---|---|---|
| Total | 125 (100.0%) | 97 (100.0%) | 28 (100.0%) | |
| Sex | Female | 107 (85.6%) | 81 (83.5%) | 26 (92.9%) |
| Male | 18 (14.4%) | 16 (16.5%) | 2 (7.1%) | |
| Age Group (years) | 18-35 | 2 (1.6%) | 2 (2.1%) | 0 (0.0%) |
| 36-50 | 8 (6.4%) | 5 (5.2%) | 3 (10.7%) | |
| 51-65 | 77 (61.6%) | 64 (66.0%) | 13 (46.4%) | |
| 66-80 | 38 (30.4%) | 26 (26.8%) | 12 (42.9%) | |
| Marital Status | single | 16 (12.8%) | 14 (14.4%) | 2 (7.1%) |
| married | 69 (55.2%) | 51 (52.6%) | 18 (64.3%) | |
| separated or divorced | 29 (23.2%) | 23 (23.7%) | 6 (21.5%) | |
| widowed | 9 (7.2%) | 7 (7.2%) | 2 (7.1%) | |
| other | 2 (1.6%) | 2 (2.1%) | 0 (0.0%) | |
| Household | single | 43 (34.4%) | 36 (37.1%) | 7 (25.0%) |
| with partner | 61 (48.8%) | 43 (44.3%) | 18 (64.3%) | |
| single with children | 4 (3.2%) | 4 (4.1%) | 0 (0.0%) | |
| with partner and children | 15 (12.0%) | 12 (12.4%) | 3 (10.7%) | |
| other | 2 (1.6%) | 2 (1.2%) | 0 (0.0%) | |
| Highest Educational Level | primary schooling | 8 (6.4%) | 6 (6.2%) | 2 (7.1%) |
| secondary schooling | 34 (27.2%) | 26 (26.8%) | 8 (28.6%) | |
| high school | 21 (16.8%) | 17 (17.5%) | 4 (14.3%) | |
| university degree | 56 (44.8%) | 43 (44.3%) | 13 (46.4%) | |
| other | 6 (4.8%) | 5 (5.2%) | 1 (3.6%) | |
| Occupation | self-employed | 12 (9.6%) | 10 (10.3%) | 2 (7.1%) |
| civil servant | 5 (4.0%) | 4 (4.1%) | 1 (3.6%) | |
| employed | 39 (31.2%) | 31 (32.0%) | 8 (28.6%) | |
| worker | 2 (1.6%) | 1 (1.0%) | 1 (3.6%) | |
| homemaker | 3 (2.4%) | 3 (3.1%) | 0 (0.0%) | |
| unemployed | 5 (4.0%) | 5 (5.2%) | 0 (0.0%) | |
| retired | 43 (34.4%) | 30 (30.9%) | 13 (46.4%) | |
| permanently disabled | 12 (9.6%) | 10 (10.3%) | 2 (7.1%) | |
| other | 4 (3.2%) | 3 (3.1%) | 1 (3.6%) | |
| Annual Gross Salary |
< 20.000 Euros | 49 (39.2%) | 40 (41.2%) | 9 (32.1%) |
| 20-40.000 Euro | 42 (33.6%) | 33 (34.0%) | 9 (32.1%) | |
| 40-60.000 Euro | 21 (16.8%) | 14 (14.4%) | 7 (25.0%) | |
| 60-80.000 Euro | 11 (8.8%) | 8 (8.2%) | 3 (10.7%) | |
| > 80.000 Euro | 2 (1.6%) | 2 (2.1%) | 0 (0.0%) | |
| Subjective Physical Health Status | not impaired | 1 (0.8%) | 1 (1.0%) | 0 (0.0%) |
| mildly impaired | 16 (12.8%) | 11 (11.3%) | 5 (17.9%) | |
| impaired | 76 (60.8%) | 59 (60.8%) | 17 (60.7%) | |
| strongly impaired | 32 (25.6%) | 26 (26.8%) | 6 (21.4%) | |
| Subjective Psychological Health Status | not impaired | 21 (16.8%) | 15 (15.5%) | 6 (21.4%) |
| mildly impaired | 49 (39.2%) | 36 (37.1%) | 13 (46.4%) | |
| impaired | 38 (30.4%) | 32 (33.0%) | 6 (21.4%) | |
| strongly impaired | 17 (13.6%) | 14 (14.4%) | 3 (10.7%) | |
| Psychotherapy | none so far | 49 (39.2%) | 37 (38.1%) | 12 (42.9%) |
| ealier | 57 (45.6%) | 45 (46.4%) | 12 (42.9%) | |
| currently | 19 (15.2%) | 15 (15.5%) | 4 (14.3%) | |
| Integrative Medicine | familiar with concept | 86 (68.8%) | 65 (67.0%) | 21 (75.0%) |
| Stay at this clinic | first | 83 (66.4%) | 67 (69.1%) | 16 (57.1%) |
| second | 23 (18.4%) | 16 (16.5%) | 7 (25.0%) | |
| third | 12 (9.6%) | 8 (8.2%) | 4 (14.3%) | |
| fourth | 7 (5.6%) | 6 (6.2%) | 1 (3.6%) | |
| Fasting Experience | never | 56 (44.8%) | 44 (45.4%) | 12 (42.9%) |
| once | 17 (13.6%) | 12 (12.4%) | 5 (17.9%) | |
| twice | 18 (14.4%) | 14 (14.4%) | 4 (14.3%) | |
| 3 times | 9 (7.2%) | 7 (7.2%) | 2 (7.1%) | |
| 4 times | 5 (4.0%) | 5 (5.2%) | 0 (0.0%) | |
| 5 times and more | 20 (16.0%) | 15 (15.5%) | 5 (17.9%) | |
| Medication atadmission | Opioids | 11 (8.8%) | 8 (8.2%) | 3 (10.7%) |
| Pain Medication | 115 (92.0%) | 88 (90.7%) | 27 (96.4%) | |
| Herbal Remedies | 52 (41.6%) | 40 (41.2%) | 12 (42.9%) | |
| Subjective Impairment by OA | NRS [0-10]: M±SD | 6.1 (± 1.6) | 6.2 (± 1.6) | 5.9 (± 1.5) |
| Anticipation of Efficacy | NRS [0-10]: M±SD | 6.4 (± 2.0) | 6.4 (± 1.9) | 6.4 (± 2.5) |
Legend: M = Mean, SD = Standard Deviation, NRS = Numerical Rating Scale, OA = Osteoarthritis.
Table 2.
Results of metabolic and physiological parameters.
| Difference between V1 and V0 * | |||||||||
| Parameter | Visit | M | SD | n | M | SD | T | p | d |
| Cholesterol [mg/dL] | V0 | 239.2 | 44.86 | 84 | |||||
| V1 | 201.1 | 48.85 | 70 | -38.4 | 31.20 | 10.23 | <0.001 | 0.80 | |
| LDL [mg/dL] |
V0 | 155.9 | 38.27 | 81 | |||||
| V1 | 129.8 | 46.91 | 63 | -24.5 | 30.72 | 6.29 | <0.001 | 0.56 | |
| HDL [mg/dL] |
V0 | 58.2 | 13.80 | 81 | |||||
| V1 | 49.2 | 12.61 | 62 | -8.0 | 7.74 | 8.12 | <0.001 | 0.59 | |
| Triglycerides [mg/dL] |
V0 | 133.7 | 66.42 | 84 | |||||
| V1 | 113.1 | 47.25 | 66 | -24.5 | 67.43 | 2.92 | 0.005 | 0.42 | |
| NRSPain [scale 0-10] | V0 | 6.2 | 1.72 | 90 | |||||
| V1 | 3.5 | 1.87 | 64 | -2.7 | 1.98 | 10.8 | <0.001 | 1.48 | |
| Weight [kg] | V0 | 84.8 | 17.9 | 115 | |||||
| D 01 | 83.9 | 17.74 | 115 | ||||||
| V1 | 80.3 | 16.88 | 115 | -3.6 | 1.65 | 23.29 | <0.001 | 0.21 | |
| Systolic BP [mmHg] | V0 | 128.0 | 15.34 | 115 | |||||
| V1 | 121.8 | 13.42 | 115 | -6.2 | 15.93 | 4.15 | <0.001 | 0.43 | |
| Diastolic BP [mmHg] | V0 | 78.6 | 8.61 | 115 | |||||
| V1 | 74.9 | 8.4 | 115 | -3.7 | 10.55 | 3.70 | <0.001 | 0.43 | |
* between V1 and the day after hospital admission (day 01) in the case of weight. Legend: Differences and statistics were calculated only for complete cases regarding each individual parameter. Since patients are admitted at noon, weight was assessed on the morning after admission (day 1) and V1. M = Mean, SD = Standard Deviation, n = number of participants, T = Test statistic and p = p-value of the paired t-test, d = Effect size (Cohen’s d), NRS = Numerical Rating Scale, LDL = Low-density lipoprotein, HDL = High-density lipoprotein, BP = Blood Pressure. Units: mg = milligram, dL = deciliter (0.1 liter), kg = kilogram, mmHG = millimeter / mercury.
Table 3.
Questionnaire results.
| Difference to V0 | |||||||||
|---|---|---|---|---|---|---|---|---|---|
| Parameter | Visit | M | SD | n | M | SD | T | p | d |
| WHO 5 | V0 | 11 | 4.74 | 107 | |||||
| V1 | 15.4 | 4.75 | 107 | 4.5 | 4.94 | 9.29 | <0.001 | 0.94 | |
| V2 | 15.3 | 4.96 | 68 | 3.6 | 4.27 | 7 | <0.001 | 0.74 | |
| V3 | 14.9 | 5.04 | 56 | 3.4 | 4.54 | 5.57 | <0.001 | 0.67 | |
| V4 | 14.3 | 4.61 | 53 | 2.7 | 5.05 | 3.8 | <0.001 | 0.56 | |
| MAAS | V0 | 3.9 | 0.87 | 107 | |||||
| V1 | 4.1 | 0.77 | 107 | 0.2 | 0.61 | 4.07 | 0.001 | 0.29 | |
| V2 | 4.2 | 0.79 | 68 | 0.2 | 0.6 | 3.28 | 0.002 | 0.28 | |
| V3 | 4 | 0.81 | 56 | 0.1 | 0.57 | 1.87 | 0.067 | 0.18 | |
| V4 | 4 | 0.91 | 53 | 0.2 | 0.71 | 1.98 | 0.053 | 0.21 | |
| HADS Depression | V0 | 10.9 | 3.74 | 107 | |||||
| V1 | 8.5 | 3.32 | 107 | -2.3 | 3.01 | 7.94 | <0.001 | 0.65 | |
| V2 | 8.5 | 3.17 | 68 | -2 | 3.13 | 5.35 | <0.001 | 0.59 | |
| V3 | 9.1 | 3.64 | 56 | -1.5 | 3.3 | 3.29 | 0.002 | 0.37 | |
| V4 | 9.5 | 3.37 | 53 | -0.9 | 2.76 | 2.32 | 0.024 | 0.24 | |
| HADS Anxiety | V0 | 10.3 | 3.73 | 107 | |||||
| V1 | 8.2 | 3.69 | 107 | -2.1 | 2.91 | 7.28 | <0.001 | 0.55 | |
| V2 | 8.3 | 3.18 | 68 | -1.7 | 2.4 | 5.91 | <0.001 | 0.52 | |
| V3 | 8.6 | 3.6 | 56 | -1.7 | 2.84 | 4.38 | <0.001 | 0.45 | |
| V4 | 9 | 3.36 | 53 | -1.1 | 2.96 | 2.76 | 0.008 | 0.32 | |
| WOMAC Global Score [0-96] |
V0 | 37.7 | 19.33 | 107 | |||||
| V1 | 22.5 | 18.16 | 101 | -14.9 | 13.37 | 11.18 | <0.001 | 0.79 | |
| V2 | 23.3 | 17.25 | 68 | -12.9 | 13.84 | 7.65 | <0.001 | 0.71 | |
| V3 | 24.6 | 22.98 | 56 | -11.4 | 20.17 | 4.19 | <0.001 | 0.53 | |
| V4 | 28 | 17.98 | 53 | -10 | 18.5 | 3.89 | <0.001 | 0.55 | |
| WOMAC Pain Score [0-20] |
V0 | 8.5 | 3.98 | 107 | |||||
| V1 | 5.1 | 4.12 | 101 | -3.4 | 3.61 | 9.29 | <0.001 | 0.82 | |
| V2 | 5.1 | 3.64 | 68 | -3.1 | 3.67 | 6.98 | <0.001 | 0.81 | |
| V3 | 5.2 | 5.02 | 56 | -2.7 | 4.42 | 4.58 | <0.001 | 0.59 | |
| V4 | 6.3 | 4.24 | 53 | -2 | 4.57 | 3.1 | 0.003 | 0.47 | |
| WOMAC Subscale Stiffness Score [0-8] |
V0 | 3.8 | 2.18 | 107 | |||||
| V1 | 2.1 | 1.94 | 101 | -1.6 | 1.81 | 8.79 | <0.001 | 0.76 | |
| V2 | 2.6 | 2.03 | 68 | -1.2 | 1.83 | 5.26 | <0.001 | 0.56 | |
| V3 | 2.7 | 2.14 | 56 | -1 | 1.92 | 3.73 | <0.001 | 0.46 | |
| V4 | 3.2 | 2.11 | 53 | -0.6 | 2.42 | 1.91 | 0.062 | 0.31 | |
| WOMAC Physical Function Score [0-68] |
V0 | 25.4 | 14.5 | 107 | |||||
| V1 | 15.2 | 13.5 | 101 | -10 | 9.8 | 10.22 | <0.001 | 0.71 | |
| V2 | 15.6 | 12.73 | 68 | -8.6 | 9.93 | 7.09 | <0.001 | 0.64 | |
| V3 | 16.6 | 16.54 | 56 | -7.7 | 14.96 | 3.81 | <0.001 | 0.49 | |
| V4 | 53 | -7.3 | 13.08 | 4.05 | <0.002 | 0.55 | |||
Legend: On the left side, descriptive statistics are given for each visit separately, while on the right side the differences between the respective visit and the baseline visit (V0) are presented. Differences and statistics were calculated only for the complete cases for the individual parameter and visit. M = Mean, SD = Standard Deviation, n = number of participants, T = Test statistic and p = p-value of the paired t-test, d = Effect size (Cohen’s d).
Table 4.
Changes in medication during inpatient stay.
| Change | -2 | -1 | -0.5 | 0 | +0.5 | +1 | +1.5 | +2 |
|---|---|---|---|---|---|---|---|---|
| Opioids | 5 | 3 | 0 | 3 | 0 | 0 | 0 | 0 |
| Pain Medication | 5 | 25 | 0 | 73 | 0 | 12 | 0 | 0 |
| Herbal Remedies | 1 | 0 | 0 | 2 | 25 | 16 | 3 | 5 |
Legend: (-2) = medication was stopped, (-1) = dosage was significantly reduced, -0,5 change from daily intake of herbal remedies to rescue medication, (0) = no noteworthy change in dosage, (+0,5) = slight increase in dosage or new herbal remedies as rescue medication, (+1) = new medication or 1,5 to 2,5-fold rise in dosage, (+1,5) = new daily herbal remedy plus a herbal remedy as rescue medication, and (+2) = at least 3-fold increase of medication, or two new daily herbal remedies.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



