
Submitted:
30 April 2023
Posted:
01 May 2023
You are already at the latest version
Abstract
Coinfection of B virus (HBV) and hepatitis Delta virus (HDV) lead to severe forms of progressive liver diseases. However, commercially available antiviral drugs have shown considerable adverse effects and low efficacy in managing these patients. Thus, there is a pressing need to develop new, innovative, and evidence-based therapies for these pathological entities. In line with this, some investigators have attempted to develop anti-viral drugs targeting HBV/HDV coinfection. In another development, investigators have also attempted to establish immune therapy targeting for HBV infection as recovery or effective control of HBV infection also lead to efficient control of HDV infection. This review has discussed an account of the evolving antiviral and immune therapeutic drugs for HBV/HDV infection. Also, based on current scientific knowledge how we have described the pros and cons of these drugs as no suitable drug has been developed during the last forty years for treating HBV infection except the availability of two” repurposed drugs”; interferons and its derivatives and nucleoside analogs, for managing HBV or HBV/HDV coinfection. It seems that an evolving and innovative therapeutic regimen that combines both antiviral drugs and immune modulators may be the best and realistic option for management of HBV/HDV coinfection.
Keywords:
HBV/HDV coinfection
; Evolving antiviral drugs
; innovative immune therapeutic agents
; combination of antiviral and immune therapy
1. Introduction
The hepatitis D virus (HDV) is a small enveloped RNA virus and belongs to the delta virus genus [1,2]. The virus is a single stranded virus with a size of 36 nm in diameter and 1.7 kb RNA genome [3]. On the other hand, hepatitis B virus is a DNA virus and represents an incredible public health problem with about two billion HBV infection in the world [4]. Among them, an estimated 296 million HBV-infected persons are supposed to be chronically infected by the HBV [5]. A chronic HBV infection means that the patient is expressing HBV DNA and hepatitis B surface antigen (HBsAg) in the blood. These patients are permanent and living reservoir of HBV transmission. A considerable proportion of chronic HBV-infected persons also progress to develop progressive liver diseases, such as chronic hepatitis B (CHB) harboring both HBV DNA, HBsAg and variable levels of inflammatory changes in the liver. Some of these patients also develop complications like cirrhosis of liver (LC) and/or hepatocellular carcinoma (HCC) [6,7]. Following the advent of potent vaccines to counter new HBV infection [8], several antiviral drugs have been developed to treat patients with HBV-related CHB, LC and HCC [9,10,11].
In this pretext, HDV infection represents several lines of incredible complexities. HDV requires HBsAg for their replication and establishment of HDV/HBV coinfection [12,13,14,15,16,17]. The prevalence of HDV among HBsAg-positive individuals is highly heterogeneous and varies from country to country or even in different parts of the same country or region. Initially, HDV may appear to present in 5% HBsAg-positive HBV-infected patients [18]. However, with advancement of time, it seems this is highly variable and is dependent on the proportion of HBsAg-positivity. In Taiwan, HDV infection declined from 25% in 1983 to 4% in 1995 [19,20]. However, fall of HDV infection is not a normal consequence of hepatitis viruses for all countries, even not for developed and advanced countries. For example, France has reported an upsurge in HDV due to various regions, including migration of people and immigration policy [21]. Few data about HBV/HDV are available from most developing and resource-constrained countries. However, these countries harbor the majority of patients with CHB. The hot zones of HDV infection include South Eastern Russia, Northern India, Vietnam, and Albania. Mongolia currently harbors the highest percentage of HDV infection, followed by Moldova, Western, and Middle African countries. The World Organization estimated that there might be 12 million HDV cases globally [18], however, some studies reported that the number of infections may be near 50 million [22,23].
Management of HDV infection depends on development of proper and effective therapeutic approaches for chronic HBV infection. If HBsAg production can be regulated in HDV/HBV infected subjects, that will be translated towards management of HDV/HBV infection. However, as of today, there is no satisfactory therapeutic regimen for containment of chronic HBV infection, although several antiviral drugs are recommended and use for treatment of chronic HBV infection [9,10,11]. On the other hand, HDV-infected patients have also been treated by some repurposed antiviral drugs with inspiring but unsatisfactory sustained effects on HDV elimination [24,25,26,27,28,29,30,31,32,33,34], Under these realities, several innovative drugs have been developed and used in CHB patients as a mono-therapeutic approach or as part of a combination therapy.
The limitations of commercially-available and repurposed antiviral drugs for management of HDV infection is now apparent. This necessitates the development of a new batch of treatment modalities for HDV/HBV coinfection. In fact, some innovative drugs have been developed to contain HBD and HBV infection. The present article would provide a bird’s eye view about the scope and limitation of different innovative therapeutic approaches that has been developed to contain HBV replication and control HBsAg production in chronic HBV-infected subjects due to the interdependence of HDV/HBV coinfection. The logical background of development of innovative drugs for HDV/HBV coinfection is shown in Figure 1.
2. Characteristics of HDV/HBV coinfection
Some important features of HDV virology should be properly analyzed to develop insights about HDV-related pathologies, especially liver damage. This will require realizing some realities about HBV/HDV coinfection and also development of therapy for these pathological conditions (Table 1).
In acute hepatitis D, where the infection occurs as a concurrent infection of HBV and HDV, the nature of the illness is indistinguishable from acute hepatitis B. In adults, HDV/HBV concurrent is usually transient and self-limited, as the rate of progression to chronicity is the same as that of HBV mono-infection. An increased risk of acute liver failure has been reported among patients with HBV mono-infection, especially in drug addicts [35]. Superinfection of HDV in patients those are already chronically-infected by HBV may induce severe acute hepatitis that may be self-limited, however, in most cases (up to 80%), the pathogenic processes lead to progression to chronicity [36]. Once chronic HDV infection is established, it usually exacerbates the preexisting CHB [37]. In this article, we would avoid to make a distinction between “Coinfection” and “Superinfection” of HBV/HDV as this usually remain poorly understood in real-life situation.
3. Ongoing therapeutic strategies against HDV
3.1. Fundamental aspects of therapy for HDV/HBV coinfection
Treatment of HDV-related liver diseases is challenging, as HDV infection is always related to HBV infection. Thus, the target of therapy is to contain both HBV and HDV. Alternately, if HBV can properly manage in CHB patients to induce HBsAg negativity by any kind of therapy, that may be of one sort of evidence-based and effective therapeutic approach for HDV/HBV coinfection. However, as of now, different antiviral drugs used for treatment of HBV/HDV infection do not result in satisfactory outcome, both in the context of safety and efficacy. Although, antiviral drugs induce HBV DNA negativity in considerable numbers of CHB patients, HBsAg-negativity is usually remaining unattainable by these drugs [38,39,40,41,42]. Even, HBsAg-positivity with HBV DNA negativity in the sera is not a positive step towards containment of HDV infection.
There are no FDA-approved guidelines for the therapy of HDV infection; however, most of the expert guidelines have targeted to contain HBV infection in patients coinfected with HBV/HDV. The fundamental basis of this concept is related to the idea that if HBV can be eradicated, HDV will be automatically contained and eradicated. Interferon (IFN)-based therapy was initiated to control HDV in the last century. The advent of pegylated IFN (peg-IFN) became the drug of choice to treat delta infection. This trend continues till now as the first choice of therapy for hepatitis delta. In the 1990s, clinical trial was accomplished with low and high doses of IFN [28,29,30]. The initial outcome was somehow encouraging, with 21%-50% being negative for HDV in the sera. However, the sustained antiviral effect of IFN could neither be documented 48 weeks after completion of therapy [28]. When Peg-IFN was approved for chronic hepatitis patients, HDV-infected patients were treated by Peg-IFN. Using various doses of Peg-IFN, it was found that prolonged use of Peg-IFN showed HDV negativity in about 30% of the patients [29,30]. However, proper follow up data are not available in most cases. Also, the role of these drugs on progression to complications like LC and HCC is not clear.
3.2. Treatment of hepatitis delta patients with combination of IFNs with antiviral drugs
Interferon alfa, with and without Peg-IFN, has been used with other antiviral drugs, such as ribavirin, but this combination therapy did not yield any extra benefit regarding containment of HBV. Scheller et al. described nucleoside analog monotherapy’s among HBV/HDV co-infected patients, however, there was no optimisms about this therapy [30]. Also, IFNs have been used with nucleoside analogs (NUCs) to contain HDV infection. However, the therapeutic benefit could not be recorded [31,32,33,34].
4. Fundamental logic of treatment of HBV/HDV coinfection and potentialities of commercially-available antiviral drugs
Treating HBV/HDV coinfection that leads to liver diseases aims at two main targets. The first one is eradicating the virus, if possible, or to induce significant containment. The next is to control the progression of liver disease that may lead to LC and HCC. Another notable factor related to the containment of HDV-mediated liver pathologies on the clearance of HBsAg. From this perspective, the limitation of commercially-available antiviral drugs is understandable, as shown in Table 2 [39,40,41,42].

Table 2.
Factors related to the incapability of commercially-available drugs to contain HBV/HDV co-infection.
Table 2.
Factors related to the incapability of commercially-available drugs to contain HBV/HDV co-infection.
| 1. These drugs are not able to eradicate HBV. |
| 2. The effect of these drugs on cccDNA of HBV is almost negligible even after prolonged use. |
| 3. These drugs’ role in containing HBsAg and inducing seroconversion to antibody to HBsAg (anti-HBs) is insignificant. |
| 4. The immune modulatory capacities of these drugs are not enough to induce protective immunity to contain the pathological processes and control of viral replication and liver damages to satisfactory levels. |
Taken together, the effect of these drugs on HBV infection is insignificant. Thus, it would be an exceptional expectation that these drugs would be effective in HBV/HDV co-infection, when they are unable to contain only HBV efficiently.
5. Evolving therapies targeting the viruses
5.1. Therapies targeting entry of the virus to hepatocytes
When the commercually-avaialable drugs are infective to treat HBV infection effectively and there is option in sight about any antiviral drug that directly eliminate HDV from HBV/HDV-coinfected patients, the target of therapy is switched towards development of new and novel therapies on the basis of nature of viruses and natural course of pathological processes.
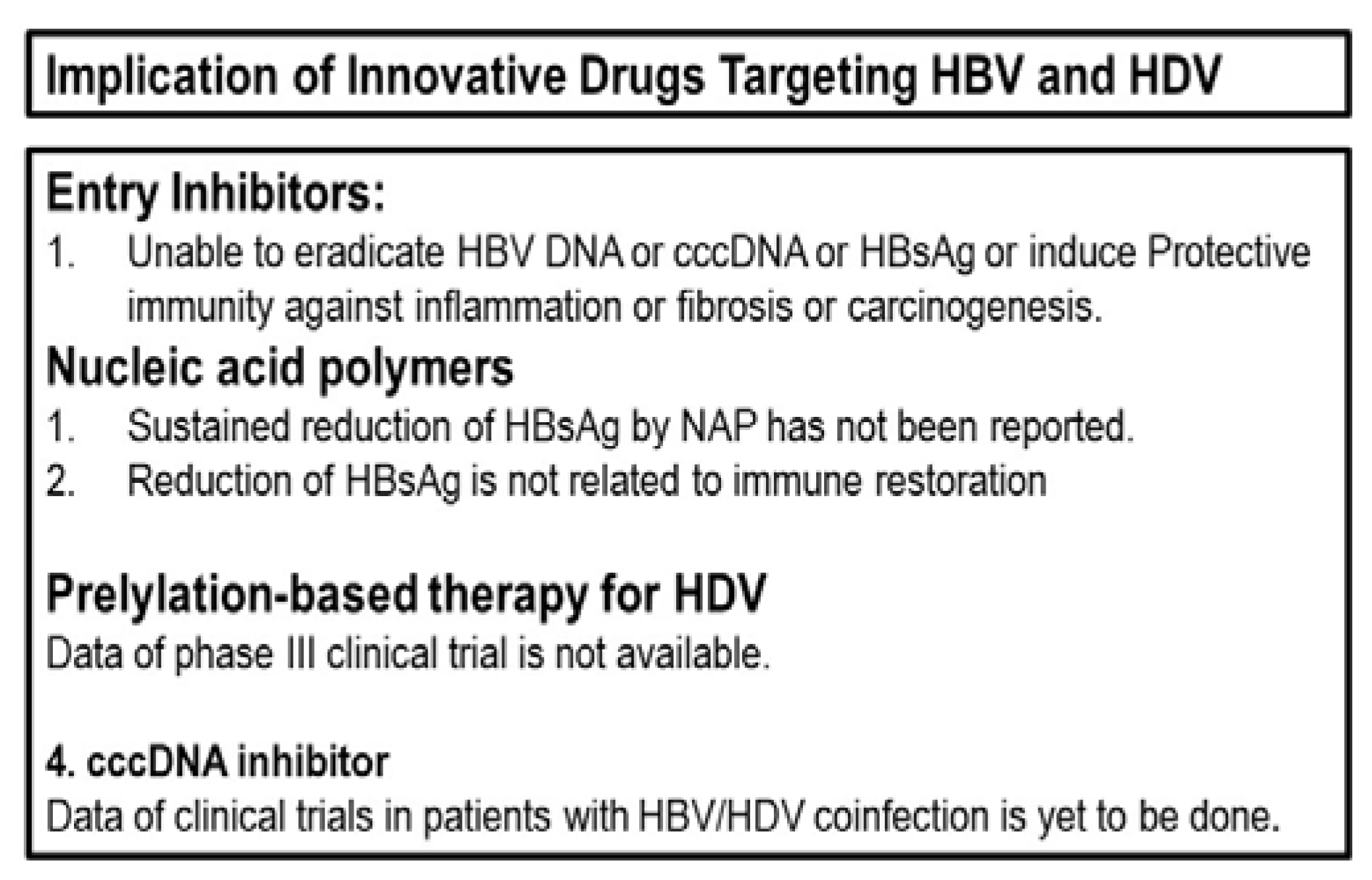
The entry receptor for both HBV and HDV into the hepatocyte has been identified as sodium taurocholate cotrasporting polypeptide (NTCP) [43]. For the entry of HDV, an interaction between NTCP and L-HBsAg is required [44,45]. Thus, it has been assumed that newly developed entry inhibitors may contain the extent of HBV/HDV infections. In line with this, clinical trials have been accomplished in these patients with entry inhibitor, Myrcludex B (buleviritide). The initial outcome was inspiring but not satisfactory. In course of time, entry inhibitor was used with other antiviral agents, such as tenofovir and pegylated IFN. The viral load reduced at the onset of the therapy, but the effect was not sustained [46,47,48,49]. Ferenci et al. showed the impact of entry inhibitors on serum alanine aminotransferase levels by monotherapy and combination treatment with other antivirals [50]. Thus, entry inhibitors have shown promise as an evolving drug, but better outcomes should be provided for their clinical usage. In addition, important data about the role of these drugs on cccDNA is warranted. Most importantly, it should be cleared if they can reduce or eliminate HBsAg in these patients. Finally, the immune regulatory capacity of these drugs should be analyzed.
5.2. HBsAg inhibition by nucleic acid polymers (NAP)
NAPs are endowed with their ability to bind to exposed amphipathic helices on viral fusion glycoproteins and could avert natural protein interactions or conformations [51,52]. Both an entry inhibition and a decrease of HBsAg secretion are possible modes of action of NAPs. Clinical trials have exposed missed outcomes about NAP. REP 2139 have been tested in CHB patients, however, follow-up data are warranted regarding both safety and efficacy of REP 2139 [53], as safety concern in long-term therapy is yet to be documented. The role of NAP on cccDNA should be analyzed and properly demonstrated. The studies about HBsAg inhibitors are in their primary stage. The exact scope of these drugs are yet to be evaluated. It is really difficult to forecast about their clinical usage, but these drugs may be a part of a combination for management of some patient with HBV/HDV coinfection.
5.3. Prelylation-based therapy for HDV
Prenylation plays a vital part in the life cycle of HDV. It is expected that a prenylation inhibitor disrupts the process of prenylation. In that case, the large delta hepatitis antigen (LDHAg) prevents its ability to interact with and form secreted particles with the hepatitis B surface antigen (HBsAg) [54,55]. These drugs are under trial, and although they show some optimism, these should be properly assessed in phase III clinical trials [56,57,58].
5.4. Other evolving drugs for challenging HBV and HDV replication
The innovative antiviral drugs used in clinical trials to address HBV and HDV replications have been comprehensively addrssed above. In addition to this, some prospective medicines may be promising tools for this purpose. Small interfering RNA has been designed to target hepatitis B mRNA and to reduce viral replication [59]. N-(phosphonoacetyl)-L-aspartic acid inhibits carbamoyl-phosphate synthetase 2, aspartate transcarbamylase, and dihydroorotase. It is supposed that they can hinder HDV replication and consequently interfere with the HDV lifecycle [60]. One of the most notable points regarding the containment of HBV and HDV replication is the existence of cccDNA. Recently, ccc_RO8, a cccDNA inhibitor, has been tested in mice. This small molecule specifically reduced cccDNA levels in HBV-infected hepatocytes, and thus considerable optimism has been initiated for a complete cure of HBV replication [61]. Another animal study has shown that it might be impossible to destroy cccDNA, the ultimate target of HBV therapy development. However, these therapies are accomplished on animal models, and their translation research form benches to patients bedsides are yet to be accomplished [62].
6. What is expected from virus-targeting evolving drugs to contain HBV/HDV co-infection
The entry, localization, and replication of HDV are dependent on certain cellular and antigenic components of the HBV. Various evolving drugs are supposed to control HBV replication. However, it is uncertain if they are capable of eradicating the viruses to a level that HBV-related viral antigens would be u nable allow entry of HDV. As of today on the bassi of omgoimg scientific developments, it appears that eradication of HDV in HBV/HDV co-infected subjects is challenging and may not be a practical option. Among the evolving virus-targeting drugs, the scopes and limitations of most drugs are yet to be fully explored, especially since some of these have not been brought to bedsides from benches. Even then, the prospects for HBV-targeting medicines do not seem to be really optimistic. For example, entry inhibitors have been applied in patients with CHB and also in patients with coinfection with HBV/HDV. However, sustained viral control has not been associated with their application in these patients. Even applying entry inhibitors with other antiviral drugs, the outcome was not optimistic. After critically analyzing the mechanisms of pathogenesis of CHB and superinfection of HDV on HBV infection, it seems that temporarily containing HBV is not a suitable mode of therapy. This is because perssitently containment of HBV by NUCs could not resolve the problem of HBV-induced complications of progression to LC and HCC. It is to be mentioned that HBV uses its own polymerase for replications, whereas HDV uses cellular polymerase for existence. Thus, the available entry inhibitors would play insignificant role in the containment of HDV infection. However, there are two options for further development of entry inhibitors. There may be entry inhibitors that can regulate cccDNA either lonely or in conjunction with other drugs of multiple natures. Other evolving antiviral drugs are also endowed with similar limitations. Replicore might be one of the new avenues of drug development, but its role on cccDNA is yet to be ascertained. Similarly, Prelylation-based therapy and other evolving antiviral drugs targetting HBV or HDV are yet to exhibit their sustained antiviral effect and safety profiles before being accepted in clinical setup.
Figure 2.
Limitation of innovative drugs targeting HBV and HDV for management of HBV/HDV coinfection.
Figure 2.
Limitation of innovative drugs targeting HBV and HDV for management of HBV/HDV coinfection.
7. Logics behind the pessimistic view about commerciallly-avaaialble and evolving antiviral drugs for management of HBV/HDV co-infection
The World Health Organization (WHO) has set up a target of “Elimination of Hepatitis by 2030,” as a part of sustainable developmental goal (SGD) in which it is necessary to find out the missing millions of chronically HBV-infected persons because the WHO assumes that less than 10% of the chronic HBV-infected patients are aware of their infection. Additionally, only 5% of chronic HBV-infected subjects are under some medications. The NUCs are now widely used to treat CHB patients, and some of these patients may be co-infected with HDV as well. NUCs are capable of inducing HBV DNA negativity and also seroconversion in some CHB patients. Even then, NUCs could not stand the test of time as an antiviral drug to treat CHB. There are some dominant reasons underlying this. NUCs are incapable of regulating cccDNA [63]. The immune modulatory capacities of NUCs are not purpose-oriented [64]. In addition to these functional limitations, NUCs need to be used for a prolonged duration as it is a mode of infinite therapy. Now, the reality states that most chronic HBV-infected patients live in Asia and Africa’s developing and resource-constrained countries. Any indefinite treatment that needs clinicians’ regular observation is not an appropriate mode of treatment for millions of CHB patients for fullfiling the target of attaining the goal of “Elimination of Hepatitis by 2030.”
8. New modes of innovative therapy targeting the host immunity
The pathogenic processes of patients with chronic HBV infection are highly complex. It is also possible that super-infection with HDV may induce more complexities in this paradigm. In short, CHB is an HBV-induced immune-mediated disease. HBV remains as cccDNA in the liver of CHB patients and may produce virion particles and their antigens as and when necessary. One hepatocyte may have 5–50 cccDNA. The half-life of cccDNA is about ten days to months, depending on the data from in vitro and in vivo studies. Although HBV cccDNA is a culprit and stumbling block for HBV infection, cccDNA is not also cytopathic [65].
Thus, it is natural to ask what types of cellular and molecular mechanisms are responsible for inflammation (hepatitis), progressive fibrosis and cirrhosis, and liver cancer following HBV infection. In fact, complex interactions between the host and the virus and the nature of host immunity appear to have an essential role in this aspect. Many of these cellular and molecular mechanisms could not be fully explored in CHB patients or chronic HBV-infected patients due to ethical and technical limitations; various investigators explored some of the events by studying the events in HBV transgenic mice (HBV TM), a murine model of HBV infection [66,67].
9. A bird’s eye view regarding immune therapy for treating CHB patients
The fundamentals of containing HBV/HDV coinfection is dependent on proper management of HBV replication and containment of liver damages. As it became clear that CHB patients harbor impaired immunity, investigators attempted to upregulate host immunity by different immune modulators like cytokines such as interleukins, growth factors like granulocyte-macrophage colony-stimulating factor, and immune modulators of different natures [68,69,70,71,72,73,74,75,76]. Most of these immune modulators expressed transient antiviral properties in CHB patients. However, in most cases, the effect was not sustained. In addition, there remained safety concerns on the basis of the dose of the immune modulators. In fact, most of these studies were conducted as a pilot study. There were no long-term follow-up observations, and the mechanism of action of these immune modulators has not been explored. The effects of polyclonal immune modulators as evolving drugs were not studied in CHB patients. However, proper designing and phase I/II and III trials may unmask some future beneficial effects of polyclonal immune modulators.
10. Development of antigen-specific immune therapy for CHB patients; Learning of the benches and translated to patients’ bedsides
In the meantime, Maini and her group provided credible evidence that CHB patients are endowed with a very complex impairment of immune responses following host/HBV interactions [77,78,79]. In short, they showed that HBV-specific immunity, especially HBcAg-specific immunity, is protective in nature for CHB patients, whereas polyclonal immunity is usually pathogenic in these patients. HBV antigen-specific immune therapy started in 1994 [80], the works of the Maini group provided a special impetus and credible evidence for accomplishing immune therapy with HBV-related antigens from the start of the 21st century.
Different investigators used different HBV-related antigens for the immune therapy of CHB patients. These include HBsAg-based vaccine, HBsAg-based vaccine with antiviral drugs, DNA-based treatment, and cell-based therapies for treating patients with CHB [80,81,82,83,84,85,86,87,88,89,90,91,92,93]. In these clinical trials, HBsAg was used as immune -inducing agent. In the meantime, it became evident that HBcAg-specific immunity is essential for control of the HBV replication and containment of liver damage. This concept was also supported by a study in HBV transgenic mice, an animal model of chronic HBV carriers state [94]. A new type of therapeutic vaccine was constructed that contains both HBsAg and HBcAg by Center for genetic Engineering and biotechnology (CIGB, Havana, Cuba). This combined antigen vaccine was named NASVAC as this can administered via nasal route. NASVAC was used in treatment-naïve patients with CHB in Bangladesh. First, in the phase I clinical trial, this therapeutic vaccine’s safety, and efficacy were ascertained [95]. Subsequently, phase III clinical trial with NASVAC was done in Bangladesh. The data have shown that NASVAC is able to down regulate HBV DNA and control ALT upregulation in CHB patients. This group provided data on HBV DNA, alanine aminotransferase, and other hepatic functional parameters consecutively (24 weeks after the end of treatment [EOT] [96], two years [97], three years [98] and five years after EOT [99]) after accomplishing a phase III clinical. It appears that the HBsAg/HBcAg-based vaccine is moderately effective in about 60% of patients in inducing HBV DNA negativity and normalization of ALT in CHB patients; all of them had HBV DNA in the sera and elevated ALT during study commencement. Additionally, in another clinical trial in Japan in NUC-experienced patients, the role of this combined therapeutic vaccine, NASVAC, on HBsAg titer in the sera was ascertained [100]. In the course of time, Lok et al. also used multiple HBV-related antigen-based vaccines, and they reported the safety of these vaccines in CHB patients [101].
11. Summation of the evolving therapies and their possible clinical implications to contain HBV/HDV coinfection
HBV represents a global public health problem with billions of infections and about 296 million chronically-infected subjects. Considerable numbers of these populations would develop LC and HCC. Although the WHO provided a target of “Elimination of Hepatitis by 2030”, the target would remain unachievable in the present context. HDV is another hepatitis virus, and HDV may be regarded as a defective virus as its existence is dependent on HBV replication. Currently, it is estimated that there might be about 12 million HBV/HDV co-infected patients worldwide. The clinical course of HBV infection takes a downhill course in many HBV/HDV co-infected subjects. This review is intended to focus on evolving therapies against HBV/HDV co-infection. There is no specific drug for HDV; thus, the discussion target is the elimination or containment of HBV infection.
The evolving drugs for HBV/HDV co-infection can be badly divided into two categories; one that targets the virus (antiviral drugs) and the other that plans for respirations of immunity (immune therapy). Critical analyses have exposed the bitter truth that even the commercially-available antiviral drugs are endowed with potent antiviral capacities, these drugs are not able to stand the test of time due to multiple reasons that have been already discussed. This necessitates developing innovative medicines. As of now, innovative antiviral drugs, such as entry inhibitors or HBsAg-release preventers, or prenylation inhibitors, would be of limited utility. However, opportunities remain if these drugs are used in combination or other types of drugs. A good chance prevails with a cccDNA blocker or destroyer drug, but that is at the initial state, and animal studies are yet to be completed.
The options remain for immune therapy; however, HBsAg-based vaccine therapy is no longer a useful concept for CHB patients; a conclusion drawn after analyzing several trials of that nature during the last 40 year. Multiple HBV-antigen-based vaccines have shown some credible optimism; however, more clinical trials in different populations would be required to optimize their use in HBV/HDV-coinfection.
12. Conclusions
Development of therapies for management of HBV/HDV coinfected patients represent a medical emergency as well a challenge to all branches of medical science. In reality, two major modes of drug development are visualized. One group is dedicated to develop antiviral drugs for this condition and the other group is devoted to come up with immune modulators agents for HBV/HDV coinfection. However, both the HBV and HDV are non-cytopathic virus and immunity of the hosts are distorted by the chronic persistence of the virus. Thus, evolving drugs should check their capacity to destroy the virus as well as restoration of protective host immunity. However there remain two strong cautions for drug developers. The antiviral drugs must contain cccDNA and the HBsAg production. On the other hand, those who are working on restoration of host immunity must emphasize on the restoration of protective immunity and down regulation of pathogenic immunity. Although it may immature to specify now, however, it seems that a combination of evolving drugs with both antiviral and immune modulatory capacities may be the ultimate solution.
Author Contributions
Conceptualization; SMFA; Literature search: SMFA, MAM; Writing of draft; SMFA, MAM, YH; Revision; SMFA, MAM, YH. All authors approved the final version of the manuscript.
Funding
The research received no external findings.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Conflicts of Interest
There is no conflict of interest.
References
- Magnius, L.; Taylor, J.; Mason, W.S.; Sureau, C.; Deny, P.; Norder, H.; Ictv Report, C. ICTV Virus Taxonomy Profile: Deltavirus. J. Gen. Virol. 2018, 99, 1565–1566. [Google Scholar] [CrossRef]
- Alvarado-Mora, M.V.; Locarnini, S.; Rizzetto, M.; Pinho, J.R.R. An update on HDV: Virology, pathogenesis and treatment. Antivir. Ther. 2013, 18, 541–548, Sureau, C.; Negro F. The hepatitis delta virus: replication and pathogenesis. J. Hepatol. 2016, 64 (Suppl. S1), S102–S116. [Google Scholar] [CrossRef] [PubMed]
- Kos, A.; Dijkema, R.; Arnberg, A.C.; van der Meide, P.H.; Schellekens, H. The hepatitis delta (δ) virus possesses a circular RNA. Nature 1986, 323, 558–560. [Google Scholar] [CrossRef] [PubMed]
- Seeger, C.; Mason, W.S. Hepatitis B virus biology. Microbiol. Mol. Biol. Rev. 2000, 64, 51–68. [Google Scholar] [CrossRef] [PubMed]
- Hepatitis, B. World Health Organization. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-b (accessed on 25 April 2023).
- MacLachlan, J.H.; Cowie, B.C. Hepatitis B virus epidemiology. Cold Spring Harb. Perspect. Med. 2015, 5, a021410. [Google Scholar]
- Ganem, D.; Prince, A.M. Hepatitis B virus infection--natural history and clinical consequences. N. Engl. J. Med. 2004, 350, 1118–1129. [Google Scholar] [CrossRef]
- Elbahrawy, A.; Atalla, H.; Alboraie, M.; Alwassief, A.; Madian, A.; El Fayoumie, M.; Tabll, A.A.; Aly, H.H. Recent advances in protective vaccines against hepatitis viruses: A narrative review. Viruses 2023, 15, 214. [Google Scholar] [CrossRef]
- Asselah, T.; Lada, O.; Moucari, R.; Martinot, M.; Boyer, N.; Marcellin, P. Interferon therapy for chronic hepatitis B. Clin. Liver Dis. 2007, 11, 839–849. [Google Scholar] [CrossRef]
- Grossi, G.; Viganò, M.; Loglio, A.; Lampertico, P. Hepatitis B virus long-term impact of antiviral therapy nucleot(s)ide analogues (NUCs). Liver. Int. 2017, 37, 45–51. [Google Scholar] [CrossRef]
- Zoulim, F.; Lebossé, F.; Levrero, M. Current treatments for chronic hepatitis B virus infections. Curr. Opin. Virol. 2016, 18, 109–116. [Google Scholar] [CrossRef]
- Farci, P.; Niro, G.A. Clinical features of hepatitis D. Semin. Liver Dis. 2012, 32, 228–236. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Zhong, G.; Xu, G.; He, W.; Jing, Z.; Gao, Z.; Huang, Y.; Qi, Y.; Peng, B.; Wang, H.; et al. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. Elife 2012, 3, e00049. [Google Scholar] [CrossRef] [PubMed]
- Lai, MM. RNA replication without RNA-dependent RNA polymerase: surprises from hepatitis delta virus. J. Virol. 2005, 79, 7951–7958. [Google Scholar] [CrossRef] [PubMed]
- Chao, M. RNA recombination in hepatitis delta virus: implications regarding the abilities of mammalian RNA polymerases. Virus Res. 2007, 127, 208–215. [Google Scholar] [CrossRef] [PubMed]
- Rizzetto, M.; Hoyer, B.; Canese, M.G.; Shih, J.W.; Purcell, R.H.; Gerin, J.L. Delta agent: association of δ antigen with hepatitis B surface antigen and RNA in serum of δ-infected chimpanzees. Proc. Natl. Acad. Sci. 1980, 77, 6124–6128. [Google Scholar] [CrossRef] [PubMed]
- Lempp, F.A.; Ni, Y.; Urban, S. Hepatitis delta virus: insights into a peculiar pathogen and novel treatment options. Nat. Rev. Gastroenterol. Hepatol. 2016, 13, 580–589. [Google Scholar] [CrossRef] [PubMed]
- Hepatitis Delta. Available online: https://www.who.int/news-room/fact-sheets/detail/hepatitis-d (accessed on 5 April 2023).
- Huo, T.I.; Wu, J.C.; Lin, R.Y.; Sheng, W.Y.; Chang., F.Y.; Lee, S.D. Decreasing hepatitis D virus infection in Taiwan: an analysis of contributory factors. J. Gastroenterol. Hepatol. 1997, 12, 747–751. [Google Scholar] [CrossRef] [PubMed]
- Lee, W, C.; Chen, T.K.; Han, H.F.; Lin, Y.C.; Huang, Y. M.; Kao, J.H.; Chen, P.J.; Liu, C.J. Investigating the prevalence and clinical effects of hepatitis delta viral infection in Taiwan. J Microbiol Immunol Infect 2021, 54, 902–908. [Google Scholar] [CrossRef]
- Servant-Delmas, A. Le Ga, l.F.; Gallian, P.; Gordien, E.; Laperche, S. Increasing prevalence of HDV/HBV infection over 15 years in France. J. Clin. Virol. 2014, 59, 126–128. [Google Scholar] [CrossRef]
- Miao, Z.; Zhang, S.; Ou, X.; Li, S.; Ma, Z.; Wang, W.; Peppelenbosch, M.P.; Liu, J.; Pan, Q. Estimating the global prevalence, disease progression, and clinical outcome of hepatitis delta virus infection. J. Infect. Dis. 2020, 221, 1677–1687. [Google Scholar] [CrossRef]
- Center for Disease Control and Prevention. Hepatitis D Questions and Answers for Health Professionals. Available online: https://www.cdc.gov/hepatitis/hdv/hdvfaq.htm#:~:text=Although%20HDV%20suppresses%20the%20replication,with%20HBV%20alone%20(2) (accessed on 5 April 2023).
- Farci, P.; Mandas, A.; Coiana, A.; Lai, M.E.; Desmet, V.; Van Eyken, P.; Gibo, Y.; Scaccbarozzi, S.; Criscuolo, D. Treatment of chronic hepatitis D with interferon alfa-2a. N Engl J Med 1994, 330, 88–94. [Google Scholar] [CrossRef] [PubMed]
- Heller, T.; Rotman, Y.; Koh, C. , Clark, S.; Haynes-Williams, V.; McBurney, R.; Schmid, P.; Albrecht, D.E.; Ghany, M.G.; Liang, T.J. et al. Long-term therapy of chronic delta hepatitis with peginterferon alfa. Aliment Pharmacol Ther 2014, 40, 93–104. [Google Scholar] [CrossRef] [PubMed]
- Guedj, J.; Rotman, Y.; Cotler, S.J. Koh, C. ; Schmid, P,; Haynes-Williams, V.; Liang, T.J.; Liang, T. J.; Hoofnagle, J.H. et al. Understanding early serum hepatitis D virus and hepatitis B surface antigen kinetics during pegylated interferon-alpha therapy via mathematical modeling. Hepatology 2014, 60, 1902–1910. [Google Scholar]
- Gunsar F, Akarca US, Ersoz G, et al. Two-year interferon therapy with or without ribavirin in chronic delta hepatitis. Antivir Ther 2005, 10, 721–726. [Google Scholar] [CrossRef]
- Niro, G.A.; Ciancio, A.; Gaeta, G.B.; Smedile, A.; Marrone, A.; Olivero, A.; Stanzione, M.; David, E.; Brancaccio, G.; Fontana, R.; et al. Pegylated interferon alpha-2b as monotherapy or in combination with ribavirin in chronic hepatitis delta. Hepatology 2006, 44, 713–720. [Google Scholar] [CrossRef] [PubMed]
- Kaymakoglu, S.; Karaca, C.; Demir, K.; Poruroglu, A.; Badur, S.; Bozaci, M.; Besisik, F.; Bozaci, M.; Besisik, F.; Cakaloglu, Y.; et al. Alpha interferon and ribavirin combination therapy of chronic hepatitis D. Antimicrob Agents Chemother 2005, 49, 1135–1138. [Google Scholar] [CrossRef] [PubMed]
- Scheller, L.; Hilgard, G.; Anstasiou, O.; Dittmer, U.; Kahraman, A.; Wedemeyer, H.; Deterding, K. Poor clinical and virological outcome of nucleos(t)ide analogue monotherapy in HBV/HDV co-infected patients. Medicine 2021, 100, e26571. [Google Scholar] [CrossRef]
- Lampertico, P. Discontinuation of nucleoside analogues in hepatitis B virus infection. Gastroenterol Hepatol 2013, 9, 656–668. [Google Scholar]
- Wolters, L.M.; van Nunen, A.B.; Honkoop, P.; Vossen, A. C.; Niesters, H.G.; Zondervan, P.E.; de Man, R.A. Lamivudine-high dose interferon combination therapy for chronic hepatitis B patients co-infected with the hepatitis D virus. J. Viral. Hepat. 2000, 7, 428–434. [Google Scholar] [CrossRef]
- Wedemeyer H, Yurdaydin C, Ernst S, et al. 96 weeks of pegylated-interferon-alpha-2a plus tenofovir or placebo for the treatment of hepatitis delta: the HIDIT-2 study. Hepatology 2013, 58, 222A–223A.
- Wedemeyer, H.; Yurdaydin, C.; Hardtke, S.; Caruntu, F. A.; Curescu, M. G.; Yalcin, K.; Akarca, U. S.; Gurel, S.; Zeuzem, S.; et al. Peginterferon alfa-2a plus tenofovir disoproxil fumarate for hepatitis D (HIDIT-II): A randomised, placebo controlled, phase 2 trial. Lancet Infect Dis. 2019, 19, 275–286. [Google Scholar] [CrossRef]
- Caredda, F.; d’Arminio Monforte, A.; Rossi, E.; Farci, P.; Smedile, A.; Tappero, G.; Moroni, M. Prospective study of epidemic Delta infection in drug addicts. Prog. Clin. Biol. Res. 1983, 143, 245–250. [Google Scholar]
- Smedile, A.; Farci, P.; Verme, G.; Caredda, F.; Cargnel, A.; Caporaso, N.; Dentico, P.; Trepo, C.; Opolon, P.; Gimson A, et al. Influence of Delta infection on severity of hepatitis B. Lancet 1982, 945–947. [Google Scholar] [CrossRef] [PubMed]
- Smedile, A.; Dentico, P.; Zanetti, A.; Sagnelli, E.; Nordenfelt, E.; Actis, G.C; Rizzetto, M. Infection with the Delta agent in chronic HBsAg carriers. Gastroenterology 1981, 81, 992–997. [Google Scholar] [CrossRef] [PubMed]
- Allen, M.I.; Deslauriers, M.; Andrews, C.W.; Tipples, G.A.; Walters, K.A.; Tyrrell, D.L.; Brown, N.; Condreay, L.D. Identification and characterization of mutations in hepatitis B virus resistant to lamivudine. Lamivudine Clinical Investigation Group. Hepatology 1998, 27, 1670–1677. [Google Scholar] [CrossRef] [PubMed]
- Angus, P.; Vaughan, R.; Xiong, S.; Yang, H.; Delaney, W.; Gibbs, C.; Brosgart, C.; Colledge, D.; Edwards, R.; Ayres, A.; et al. Resistance to adefovir dipivoxil therapy associated with the selection of a novel mutation in the HBV polymerase. Gastroenterology 2003, 125, 292–297. [Google Scholar] [CrossRef] [PubMed]
- Tenney, D.J.; Rose, R.E.; Baldick, C.J.; Pokornowski, K.A.; Eggers, B.J.; Fang, J.; Wichroski, M.J.; Xu, D.; Yang, J.; Wilber, R.B.; et al. Long-term monitoring shows hepatitis B virus resistance to entecavir in nucleoside-naive patients is rare through 5 years of therapy. Hepatology 2009, 49, 1503–1514. [Google Scholar] [CrossRef]
- Lai, C.L.; Wong, D.; Ip, P.; Kopaniszen, M.; Seto, W.K.; Fung, J.; Huang, F.Y.; Lee, B.; Cullaro, G.; Chong, C.K.; et al. Reduction of covalently closed circular DNA with long-term nucleos(t)ide analogue treatment in chronic hepatitis B. J. Hepatol. 2017, 66, 275–281. [Google Scholar]
- Park, E.S.; Lee, A.R.; Kim, D.H.; Lee, J.H.; Yoo, J.J.; Ahn, S.H.; Sim, H.; Park, S.; Kang, H.S.; Won, J.; et al. Identification of a quadruple mutation that confers tenofovir resistance in chronic hepatitis B patients. J. Hepatol. 2019, 70, 1093–1102. [Google Scholar] [CrossRef]
- Yan, H.; Zhong, G.; Xu, G.; He, W.; Jing, Z.; Gao, Z.; Huang, Y.; Qi, Y.; Peng, B.; Wang, H.; et al. Sodium taurocholate cotransporting polypeptide is a functional receptor for human hepatitis B and D virus. eLife 2012, 1, e00049. [Google Scholar] [CrossRef]
- Engelke, M.; Mills, K.; Seitz, S.; Simon, P.; Gripon, P.; Schnolzer, M.; Urban, S. Characterization of a hepatitis B and hepatitis delta virus receptor binding site. Hepatology 2006, 43, 750–760. [Google Scholar] [CrossRef] [PubMed]
- Yan, H.; Wang, C. Key factors for “Fishing” NTCP as functional receptor for HBV and HDV. Viruses 2023, 15, 512. [Google Scholar] [CrossRef] [PubMed]
- Wedemeyer, H.; Bogomolov, P.; Blank, A.; Allweiss, L.; Dandri-Petersen, M.; Bremer, B.; Voronkova, N.; Schöneweis, K.; Pathil, A.; Burhenne, J.; et al. GS-005-Final results of a multicenter, open-label phase 2b clinical trial to assess safety and efficacy of Myrcludex B in combination with Tenofovir in patients with chronic HBV/HDV co-infection. J. Hepatol. 2018, 68, S3. [Google Scholar] [CrossRef]
- Wedemeyer, H.; Aleman, S.; Andreone, P.; Blank, A.; Brunetto, M.; Bogomolov, P.; Chulanov, V.; Geyvandova, N.; Hilgard, G.; Mamonova, N.; et al. Late breaker posters-2730: Bulevirtide monotherapy at low and high dose in patients with chronic hepatitis delta: 24 weeks interim data of the phase 3 MYR301 study. J. Hepatol. 2021, 75, S294. [Google Scholar]
- Asselah, T.; Arama, S.S.; Bogomolov, P.; Bourliere, M.; Fontaine, H.; Gherlan, G.S.; Gorodin, V.; Hilleret, M.N.; Lazar, L.; Mamonova, N.; et al. OS-2717: Safety and efficacy of bulevirtide monotherapy and in combination with Peginterferon alfa-2a in patients with chronic hepatitis delta: 24 weeks interim data of MYR204 Phase 2b study. J. Hepatol. 2021, 75, S291. [Google Scholar]
- Bogomolov, P.; Alexandrov, A.; Voronkova, N.; Macievich, M.; Kokina, K.; Petrachenkova, M.; Lehr, T.; Lempp, F.A.; Wedemeyer, H.; Haag, M.; et al. Treatment of chronic hepatitis D with the entry inhibitor myrcludex B: First results of a phase Ib/IIa study. J. Hepatol. 2016, 65, 490–498. [Google Scholar] [CrossRef] [PubMed]
- Ferenci P, Reiberger T, Jachs M. Treatment of Chronic Hepatitis D with Bulevirtide-A Fight against Two Foes-An Update. Cells. 2022, 11, 3531. [Google Scholar] [CrossRef]
- Vaillant, A. Nucleic acid polymers: Broad spectrum antiviral activity, antiviral mechanisms and optimization for the treatment of hepatitis B and hepatitis D infection. Antivir. Res. 2016, 133, 32–40. [Google Scholar] [CrossRef]
- Vaillant, A.; Juteau, J.-M.; Lu, H.; Liu, S.; Lackman-Smith, C.; Ptak, R.; Jiang, S. Phosphorothioate oligonucleotides inhibit human immunodeficiency virus type 1 fusion by blocking gp41 core formation. Antimicrob. Agents Chemother. 2006, 50, 1393–1401. [Google Scholar] [CrossRef]
- Bazinet, M.; Pantea, V.; Placinta, G.; Moscalu, I.; Cebotarescu, V.; Cojuhari, L.; Jimbei, P.; Iarovoi, L.; Smesnoi, V.; Musteata, T.; et al. Safety and Efficacy of 48Weeks REP 2139 or REP 2165, Tenofovir Disoproxil, and Pegylated Interferon Alfa-2a in Patients with Chronic HBV Infection Naive to Nucleos(t)ide Therapy. Gastroenterology 2020, 8, 2180–2194. [Google Scholar] [CrossRef]
- Einav, S.; Glenn, J.S. Prenylation inhibitors: a novel class of antiviral agents. J Antimicrob Chemother. 2003, 52, 883–886. [Google Scholar] [CrossRef] [PubMed]
- Bordier, B.B.; Marion, P.L.; Ohashi, K.; Kay, M. A.; Greenberg, H. B.; Cassy, J. L.; Glenn, J.S. A prenylation inhibitor prevents production of infectious hepatitis delta virus particles. J Virol. 2002, 76, 10465–10472. [Google Scholar] [CrossRef] [PubMed]
- Yurdaydin, C.; Keskin, O.; Yurdcu, E.; Çali¸skan, A.; Önem, S.; Karakaya, F.; Kalkan, Ç.; Karatayli, E.; Karatayli, S.; Choong, I.; et al. A phase 2 dose-finding study of lonafarnib and ritonavir with or without interferon alpha for chronic delta hepatitis. Hepatology 2022, 75, 1551–1565. [Google Scholar] [CrossRef] [PubMed]
- Yurdaydin, C.; Keskin, O.; Kalkan, Ç.; Karakaya, F.; Çali¸skan, A.; Karatayli, E.; Karatayli, S.; Bozdayi, A.M.; Koh, C.; Heller, T.; et al. Optimizing lonafarnib treatment for the management of chronic delta hepatitis: The LOWR HDV-1 study. Hepatology 2018, 67, 1224–1236. [Google Scholar] [CrossRef] [PubMed]
- Koh, K.; Canini, L.; Dahari, H.; Zhao, X.; Uprichard, S. L.; Hayness-Williams, V.; Winters, M.A.; Subramanya, GCooper, S. L.; Pinto, P; et al. Oral prenylation inhibition with lonafarnib in chronic hepatitis D infection: a proof-of-concept randomised, double-blind, placebo-controlled phase 2A trial. Lancet Infect Dis. 2015, 15, 1167–1174. [Google Scholar] [CrossRef] [PubMed]
- Thi, E.P.; Dhillon, A.P.; Ardzinski, A.; Bidirici-Ertekin, L.; Cobarrubias, K.D.; Cuconati, A.; Kondratowicz, A.S.; Kwak, K.; Li, A.H.L.; Miller, A.; et al. ARB-1740, a RNA Interference Therapeutic for Chronic Hepatitis B Infection. ACS Infect. Dis. 2019, 5, 725–737. [Google Scholar] [CrossRef]
- Verrier, E.R.; Weiss, A.; Bach, C.; Heydmann, L.; Turon-Lagot, V.; Kopp, A.; El Saghire, H.; Crouchet, E.; Pessaux, P.; Garcia, T.; et al. Combined small molecule and loss-of-function screen uncovers estrogen receptor alpha and CAD as host factors for HDV infection and antiviral targets. Gut 2020, 69, 158–167. [Google Scholar] [CrossRef]
- Wang, L.; Zhum, Q.; Zhang, J.D.; Zhang, Y.; Ni, X.; Xiang, K.; Jiang, J.; Li, B.; Yu, Y.; Hu, H.; et al. Discovery of a first-in-class orally available HBV cccDNA inhibitor. J Hepatol. 2023, 78, 742–753. [Google Scholar] [CrossRef]
- Chauhan, R.; Li, Q.; Woodson, M.E.; Gasonoo, M.; Meyers, M.J.; Tavis, J.E. Efficient inhibition of hepatitis B virus (HBV) replication and cccDNA formation by HBV ribonuclease H inhibitors during infection. Antimicrob Agents Chemother. 2021, 65, e014602. [Google Scholar] [CrossRef]
- Allweiss, L.; Dandri, M. The Role of cccDNA in HBV Maintenance. Viruses 2017, 9, 156. [Google Scholar] [CrossRef]
- de Fraga, R.S.; Vaisberg, V.V.; Alfaia Mendes, L.C.; Carrilho, F. J.; Ono, S.K. Adverse events of nucleos(t)ide analogues for chronic hepatitis B: a systematic review. J Gastroenterol. 2020, 55, 496–514. [Google Scholar] [CrossRef] [PubMed]
- Bhat, S.A.; Kazim, S.N. HBV cccDNA-A Culprit and stumbling block for the hepatitis B virus infection: Its presence in hepatocytes perplexed the possible mission for afunctional cure. ACS Omega 2022, 7, 24066–24081. [Google Scholar] [CrossRef] [PubMed]
- Guidotti, L.G.; Chisari, F.V. Immunobiology and pathogenesis of viral hepatitis. Annu. Rev. Pathol. 2006, 1, 23–61. [Google Scholar] [CrossRef] [PubMed]
- Eddleston, A.L.; Mondelli, M. Immunopathological mechanisms of liver cell injury in chronic hepatitis B virus infection. J. Hepatol. 1986, 3 (Suppl. 2), S17–S23. [Google Scholar] [CrossRef] [PubMed]
- Tilg, H.; Vogel, W.; Tratkiewicz, J.; Aulizky, W.E.; Herold, M.; Gruber, M.; Geissler, D.; Umalauft, F.; Judmaier, G.; Schwuelra, U. Pilot study of natural human interleukin-2 in patients with chronic hepatitis B. Immunomodulatory and antiviral effects. J Hepatol. 1993, 19, 259–267. [Google Scholar] [CrossRef] [PubMed]
- Artillo, S.; Pastore, G.; Alberti, A.; Milella, M.; Santantonio, T.; Fattovitch, G.; Guistina, G.; Ryff, J.C.; Chaneac, M.; Bartolome, J.; et al. Double-blind, randomized controlled trial of interleukin-2 treatment of chronic hepatitis B. J. Med. Virol. 1998, 54, 167–172. [Google Scholar] [CrossRef]
- Carreño, V.; Zeuzem, S.; Hopf, U.; Marcellin, P.; Cooksley, W.G.; Fevery, J.; Diuago, M.; Reddy, R.; Peters, M.; Rittweger, K.; et al. A phase I/II study of recombinant human interleukin-12 in patients with chronic hepatitis B. J. Hepatol. 2000, 32, 317–324. [Google Scholar] [CrossRef]
- Martín, J.; Quiroga, J.A.; Bosch, O.; Carreño, V. Changes in cytokine production during therapy with granulocyte-macrophage colony-stimulating factor in patients with chronic hepatitis B. Hepatology 1994, 20, 1156–1161. [Google Scholar] [CrossRef]
- Ruiz-Moreno, M.; García, R.; Rua, M.J.; Serrano, B.; Moraleda, G.; Feijoo, E.; Bartolome, J.; Ortiz, F.; Castillo, I.; Carreno, V. Levamisole and interferon in children with chronic hepatitis B. Hepatology 1993, 18, 264–269. [Google Scholar] [CrossRef]
- Farhat, B.A.; Marinos, G.; Daniels, H.M.; Naoumov, N.V.; Williams, R. Evaluation of efficacy and safety of thymus humoral factor-gamma 2 in the management of chronic hepatitis B. J Hepatol. 1995, 23, 21–27. [Google Scholar] [CrossRef]
- Woltman, A.M.; Ter Borg, M.J.; Binda, R.S.; Sprengers, D.; E von Blomberg, B.M.; Scheper, R.J.; Hayashi, K.; Nishi, N.; Boosnstra, A.; van der Molen, R.; et al. Alpha-galactosylceramide in chronic hepatitis B infection: results from a randomized placebo-controlled Phase I/II trial. Antivir Ther. 2009, 14, 809–818. [Google Scholar] [CrossRef] [PubMed]
- Iino, S.; Toyota, J.; Kumada, H.; Kiyosawa, K.; Kakumu, S.; Suzuki, E.; Martins, E.B. The efficacy and safety of thymosin alpha-1 in Japanese patients with chronic hepatitis B; results from a randomized clinical trial. J. Viral. Hepat. 2005, 12, 300–306. [Google Scholar] [CrossRef] [PubMed]
- You, J.; Zhuang, L.; Cheng, H.-Y.; Yan, S.M.; Yu, L.; Huang, J.H.; Huang, M.L.; Ma, Y.L.; Chongsuvivatwong, V.; Sriplung, H.; et al. Efficacy of thymosin alpha-1 and interferon alpha in treatment of chronic viral hepatitis B: a randomized controlled study. World J Gastroenterol. 2006, 12, 6715–6721. [Google Scholar] [CrossRef] [PubMed]
- Maini, M.K.; Boni, C.; Lee, C.K.; Larrubia, J.R.; Reignat, S.; Ogg, G.S.; King, A.S.; Herberg, J.; Gilson, R.; Alisa, A.; et al. The role of virus-specific CD8(+) cells in liver damage and viral control during persistent hepatitis B virus infection. J. Exp. Med. 2000, 191, 1269–1280. [Google Scholar] [CrossRef] [PubMed]
- Bertoletti, A.; Le Bert, N. Immunotherapy for Chronic Hepatitis B Virus Infection. Gut Liver 2018, 12, 497–507. [Google Scholar] [CrossRef]
- Bertoletti, A.; Maini, M.K.; Ferrari, C. The host-pathogen interaction during HBV infection: immunological controversies. Antivir Ther. 2010, 15 Suppl. 3, 15–24. [Google Scholar] [CrossRef]
- Pol, S.; Driss, F.; Michel, M.L.; Nalpas, B.; Berthelot, P.; Brechot, C. Specific vaccine therapy in chronic hepatitis B infection. Lancet 1994, 344, 342. [Google Scholar] [CrossRef]
- Senturk, H.; Tabak, F.; Akdogan, M.; Erdem, L.; Mert, A.; Ozaras, R.; Sander, E.; Ozbay, G.; Badur, S. Therapeutic vaccination in chronic hepatitis B. J. Gastroenterol. Hepatol. 2002, 17, 72–76. [Google Scholar] [CrossRef]
- Wang, X.Y.; Zhang, X.X.; Yao, X.; Jiang, J.-H.; Xie, Y.-H.; Yuan, Z.-H.; Wen, Y.-M. Serum HbeAg sero-conversion correlated with decrease of HbsAg and HBV DNA in chronic hepatitis B patients treated with a therapeutic vaccine. Vaccine 2010, 28, 8169–8174. [Google Scholar] [CrossRef]
- Yalcin, K.; Acar, M.; Degertekin, H. Specific hepatitis B vaccine therapy in inactive HbsAg carriers: A Randomized Controlled Trial. Infection 2003, 31, 221–225. [Google Scholar] [CrossRef]
- Wen, Y.-M.; Wu, X.-H.; Hu, D.-C.; Zhang, Q.-P.; Guo, S.-Q. Hepatitis B vaccine and anti-HBs complex as approach for vaccine therapy. Lancet 1995, 345, 1575–1576. [Google Scholar] [CrossRef] [PubMed]
- Xu, D.Z.; Zhao, K.; Guo, L.M.; Li, L.J.; Xie, Q.; Ren, H.; Zhang, J.M.; Xu, M.; Wang, H.F.; Huang, W.X.; et al. A randomized con-trolled phase Iib trial of antigen-antibody immunogenic complex therapeutic vaccine in chronic hepatitis B patients. PLoS ONE 2008, 3, e2565. [Google Scholar] [CrossRef]
- Xu, D.Z.; Wang, X.Y.; Shen, X.L.; Gong, G.Z.; Ren, H.; Guo, L.M.; Sun, A.M.; Xu, M.; Li, L.J.; Guo, X.H.; et al. Results of a phase III clinical trial with an HBsAg-HBIG immunogenic complex therapeutic vaccine for chronic hepatitis B patients: Experiences and findings. J. Hepatol. 2013, 59, 450–453. [Google Scholar] [CrossRef] [PubMed]
- Fontaine, H.; Kahi, S.; Chazallon, C.; Bourgine, M.; Varaut, A.; Buffet, C.; Godon, O.; Meritet, J.F.; Saidi, Y.; Michel, M.L.; et al. Anti-HBV DNA vaccination does not prevent relapse after discontinuation of analogues in the treatment of chronic hepatitis B: A randomised trial-ANRS HB02 VAC-ADN. Gut 2015, 64, 139–147. [Google Scholar] [CrossRef] [PubMed]
- Mancini-Bourgine, M.; Fontaine, H.; Bréchot, C.; Pol, S.; Michel, M.L. Immunogenicity of a hepatitis B DNA vaccine administered to chronic HBV carriers. Vaccine 2006, 24, 4482–4489. [Google Scholar] [CrossRef] [PubMed]
- Cova, L. Present and future DNA vaccines for chronic hepatitis B treatment. Expert Opin. Biol. Ther. 2017, 17, 185–195. [Google Scholar] [CrossRef] [PubMed]
- Cavenaugh, J.S.; Awai, D.; Mendy, M.; Hill, A.V.S.; Whittle, H.; McConkey, S. J. Partially randomized, non-blinded trial of DNA and MVA therapeutic vaccines based on hepatitis B virus surface protein for chronic HBV infection. Plos One 2011, 6, e14626. [Google Scholar] [CrossRef]
- Chen, M.; Li, Y.G.; Zhang, D.Z.; Wang, Z.Y.; Zeng, W.Q.; Shi, X.F.; Ren, H. Therapeutic effect of autologous dendritic cell vaccine on patients with chronic hepatitis B: A clinical study. World J. Gastroenterol. 2005, 11, 1806–1808. [Google Scholar] [CrossRef]
- Akbar, S.M.; Furukawa, S.; Horiike, N.; Abe, M.; Hiasa, Y.; Onji, M. Safety and immunogenicity of hepatitis B surface antigen-pulsed dendritic cells in patients with chronic hepatitis B. J. Viral Hepat. 2011, 18, 408–414. [Google Scholar] [CrossRef]
- Luo, J.; Li, J.; Chen, R.L.; Nie, L.; Huang, J.; Liu, Z.W.; Luo, L.; Yan, X.J. Autologus dendritic cell vaccine for chronic hepatitis B carriers: A pilot, open label, clinical trial in human volunteers. Vaccine 2010, 28, 2497–2504. [Google Scholar] [CrossRef]
- Akbar, S.M.; Chen, S.; Al-Mahtab, M.; Abe, M.; Hiasa, Y.; Onji, M. Strong and multi-antigen specific immunity by hepatitis B core antigen (HBcAg)-based vaccines in a murine model of chronic hepatitis B: HBcAg is a candidate for a therapeutic vaccine against hepatitis B virus. Antiviral Res. 2012, 96, 59–64. [Google Scholar] [CrossRef] [PubMed]
- Al-Mahtab, M.; Akbar, S.M.F.; Aguilar, J.C.; Uddin, H.; Khan, S.I.; Rahman, S. Therapeutic potential of a combined hepatitis B virus surface and core antigen vaccine in patients with chronic hepatitis B. Hepatol. Int. 2013, 7, 981–989. [Google Scholar] [CrossRef] [PubMed]
- Al Mahtab, M.; Akbar, S.M.F.; Aguilar, J.C.; Guillen, G.; Penton, E.; Tuero, A.; Yoshida, O.; Hiasa, Y.; Onji, M. Treatment of chronic hepatitis B naïve patients with a therapeutic vaccine containing HBs and HBc antigens (a randomized, open and treat-ment-controlled phase III clinical trial). PLoS ONE 2018, 13, e0201236. [Google Scholar] [CrossRef] [PubMed]
- Akbar, S.M.F.; Al Mahtab, M.; Aguilar, J.C.; Yoshida, O.; Penton, E.; Guillen, G.; Hiasa, Y. Sustained antiviral and liver protection by a nasal therapeutic vaccine (NASVAC), containing both HBsAg and HBcAg) in patients with chronic hepatitis B; 2-year follow-up of phase III clinical trial. Pathogens 2021, 10, 1440. [Google Scholar] [CrossRef] [PubMed]
- Akbar, S.M.F.; Al Mahtab, M.; Aguilar, J.C.; Yoshida, O.; Khan, S.; Penton, E.; Gerardo, G.N.; Hiasa, Y. The Safety and Efficacy of a Therapeutic Vaccine for Chronic Hepatitis B: A Follow-Up Study of Phase III Clinical Trial. Vaccines 2021, 10, 45. [Google Scholar] [CrossRef]
- Al Mahtab, M.; Akbar, S.M.F.; Aguilar, J.C.; Yoshida, O.; Khan, S.; Guillen, G.; Hiasa, Y. Safety profile, antiviral capacity, and liver protection of a nasal therapeutic vaccine in patients with chronic hepatitis B: Five-year-follow-up outcomes after the end of treatment. Front Med (Lausanne), 2023, 10, 1032531. [Google Scholar] [CrossRef]
- Yoshida, O.; Akbar, S.M.F.; Imai, Y.; Sanada, T.; Tsukiyama-Kohara, K.; Miyazaki, T.; Kamishita, T.; Miyake, T.; Tokumoto, Y.; Hikita, H et al. Intranasal therapeutic vaccine containing HBsAg and HBcAg for patients with chronic hepatitis B; 18 months follow-up results of phase IIa clinical study. Hepatol Res 2023, 53, 196–207. [Google Scholar] [CrossRef]
- Lok, A.S.; Pan, C.Q.; Han, S-H.B.; Trinh, H.N.; Fessel, W.J.; Rodell, T.; Massetto, B.; Lin, L.; Gaggar, A.; Subramanian, M.; et al. Randomized phase II study of GS-4774 as a therapeutic vaccine in virally suppressed patients with chronic hepatitis B. J. Hepatol 2016, 65, 509–516. [Google Scholar] [CrossRef]
Figure 1.
Fundamental aspects of drug development for HDV/HBV co-infection.
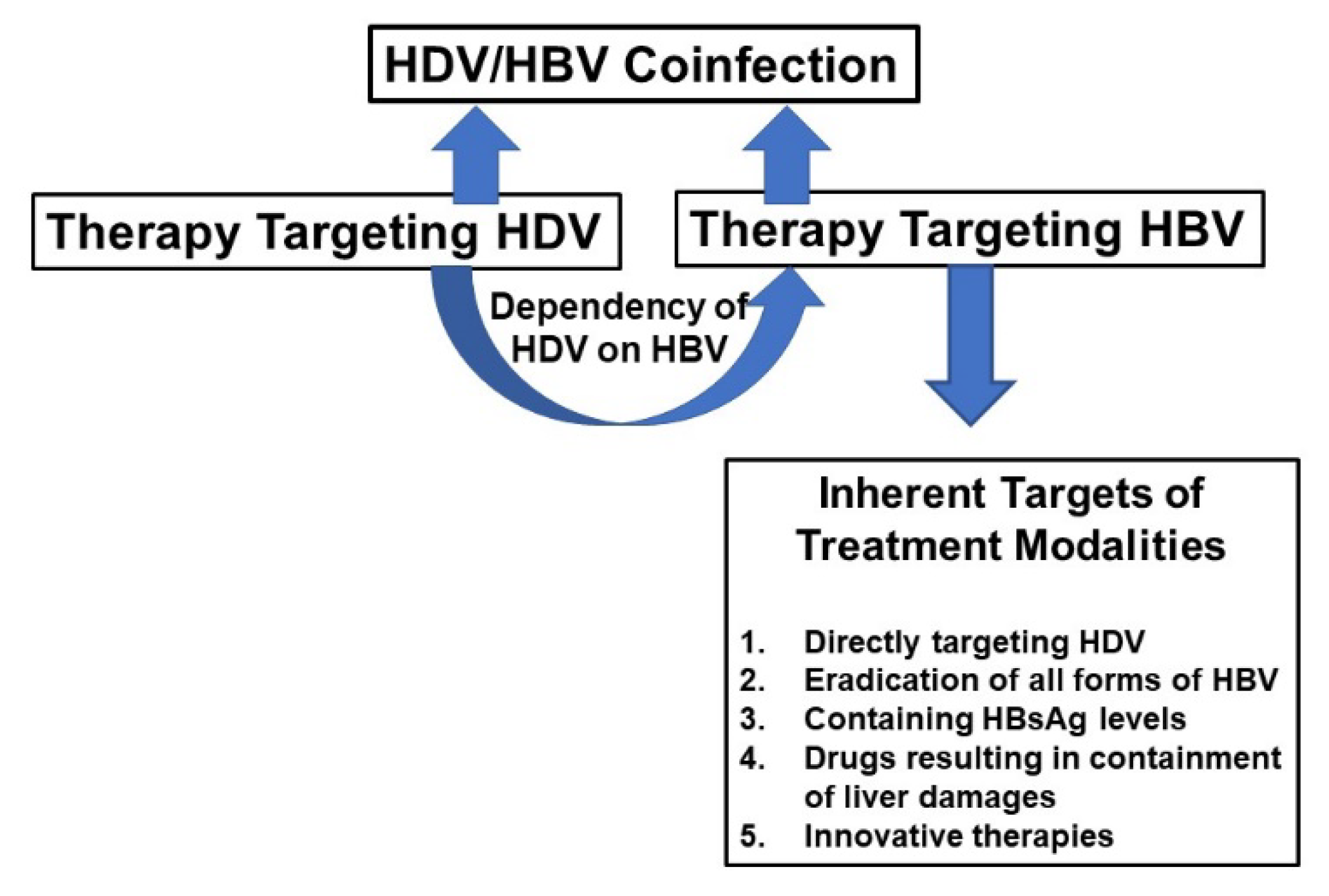
Table 1.
Some specific features of hepatitis B virus and hepatitis delta virus coinfection.
| 1. HBsAg-positivity precedes the detection of HDV DNA |
| 2. HDV may suppress HBV replication following superinfection. |
| 3.The pathogenic mechanisms and liver damage are related to factors like “HBV/HDV” superinfection or “HBV/HDV” coinfection. |
| 4. In the case of “coinfection” replication of both viruses may be contained |
| 5. However, in the case of HDV infection in existing HBV chronic-infected subjects, there may be severe forms of liver damage and their progression to complications |
| 6. HDV does not have its own RNA-dependent RNA polymerase (RDRP); however, HBV is endowed with its own RDRP, and thus therapeutic strategies would be complex to contain these two viruses in the same run. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



