
Submitted:
01 May 2023
Posted:
02 May 2023
You are already at the latest version
Abstract
Mothers’ own milk (MOM) for premature babies is considered a life-saving drug for its proven protective action against the complications of prematurity and for the effects on the outcome in the short and long term, especially the neurological one. We studied the use of the MOM for WLBWs over a 5-year period. Statistical comparisons concerned data on feeding with the MOM during stay in NICU and at discharge with respect to maternal and neonatal variables (gestational age, birth weight, type of pregnancy if single or twin, maternal age) and to feeding data (timing of the start of the Minimal Enteral Feeding and the availability of the MOM, the achievement of the Full Enteral Feeding, the type of nutrition at discharge). We observed an increase, between 2017 and 2021, of MOM use (p=0.003). The availability of the MOM occurred on average on the fourth day of life and improved over the years. Start of MEF with human milk averaged 1.78 days and 54.3% of VLBWs received MEF with donor milk on the first day of life (50% within the first 6 hours). The average MOM at discharge was 47.6% with 36.1% exclusive MOM (EMOM) and an increase from 45.8% in 2017 (EMOM 33.3%) to 58.82% (EMOM 41.18%) in 2021. The mean average daily growth of the weight improved (p<0.001) during this period. There is no statistical difference between infants fed with MOM and those fed with bank milk. The maternal age, the start day of the MOM feeding and gestational age have a significant impact on the type of feeding at discharge.
Keywords:
Mothers' Own Milk
; Preterm feeding
; VLBW
1. Introduction
Preterm birth is the leading cause of death under five years of age, responsible for about one million deaths in 20151-3. There was a wide variation in preterm birth trends in European countries4. Preterm and low birth weight infants are among the most vulnerable in our society5 and deserve special attention as well as a greater commitment to care in all aspects, especially nutritional ones which impact mortality and morbidity. MOM for premature babies is considered an important opportunity of life and health because it reduces the risk of major complications of prematurity, but also an investment for life for of its long-term outcomes including neurological and cognitive ones6-8. Much has changed over the years on the awareness that a correct nutritional practice in the early periods of life can affect the present and future well-being7,8. Scientific evidence regarding the benefits of human milk is recognized by the world’s leading health authorities and international bodies9-11.
In fact, even politics both nationally and internationally has given and is giving important contribution to the promotion of breast feeding with official statements, specific dedicated documents, guidelines, reports. So small signs of a greater diffusion of breast milk use in NICUs are recorded, of which, moreover, it is also a recognized index of quality. The exception is Sweden12, one of the most historically virtuous countries on breastfeeding, where the percentage of ELBW babies fed at discharge with MOM went from 55% in 2004 to 16% in 2016.
If the data of the type of feeding at discharge is more present in the literature, what concerns the first weeks of life in NICU, crucial for the development of VLBWs, is sparse. We refer to the nutrition with the MOM obtained by expressing the breast and then directly to the breast.
In this study we evaluated the three key moments of nutritional care in NICU: the start of enteral feeding, the achievement of FEF and the type of feeding at discharge.
2. Description of the study
2.1. Objectives: Evaluate
n° VLBWs fed with MOM in the first weeks of life, n° VLBW discharged with MOM, a correlation between maternal and neonatal factors with MOM feeding; Analyze: the start times of the MEF with DM and with MOM, the timing of reaching the FEF; the trend over years of the feeding with MOM during hospitalization and discharge.
The last aim is to identify the margins for improvement in nutrition performance with MOM with actions aimed at the categories most at risk of not receiving their mother’s milk.
2.2. Design, setting and methods
The sample includes VLBWs admitted to the NICU from 2017 to 2021. 97 VLBWs were recruited.
We obtained informed consent from mothers with a dedicated and signed form.
Transferred infants, babies with malformations with intrinsic interference with nutrition and those born to mothers with pathologies incompatible with milk production and extraction were excluded.
Nutrition with MOM during hospitalization means a minimum of 2 continuous weeks with exclusive or prevalent MOM (MOM>50%).
The data have been extrapolated from medical records, care cards and HMB’s databases, and relate to the variables: neonatal and maternal data: GA, BW, type of pregnancy if single or twin, MA; feeding data: timing of: the start of the MEF, the availability of the MOM, the achievement of the FEF; the type of nutrition at discharge and data relating to the length of stay and weight increase. Statistical comparisons concerned data on feeding with MOM in the NICU and at discharge with respect to variables.
Demographical and clinical characteristics were reported as mean and standard deviation for continuous variables and as frequency and percentage for categorical variables.
Group comparisons were performed using ANOVA or t-test for continuous variables and Pearson chi-squared test or Fisher exact test for categorical variables.
A p-value <0.05 was considered as statistically significant. All analyses were performed using the software R-project.
2.3. Results
The characteristics of the sample of the 97 VLBWs recruited are summarized in Table n° 1 while the trend over the years is represented in Table No. 2.
The average maternal age was 32.62 years, but it grew over the years from 31.86 years in 2017 to 35.65 years in 2021.
69.5% of mothers of premature babies provided their own milk.
We observed an increase, between the year 2017 and 2021, of MOM users (p=0.003) although the low percentage in 2020 is probably due to the small number of observations in this year.
In particular, the percentage of feeding VLBWs with MOM has grown over the years in a statistically significant way, with a positive peak of over 91% in 2019, and a negative trend of 14.9% in 2020, the year of the Covid pandemic.
The availability of the mother’s milk occurred on average on the fourth day of life; over the years it improved, occurring on the third day in 2021.
Initiation of MEF with human milk averaged 1.78 days. 54.3% of VLBWs received MEF with DM on the first day of life (50% within the first 6 hours) and 36.9% on the second day while MEF with MOM started on day 2 for 10%, on day 3 for 21.6% and between the 4th and 5th day for 51.6%.
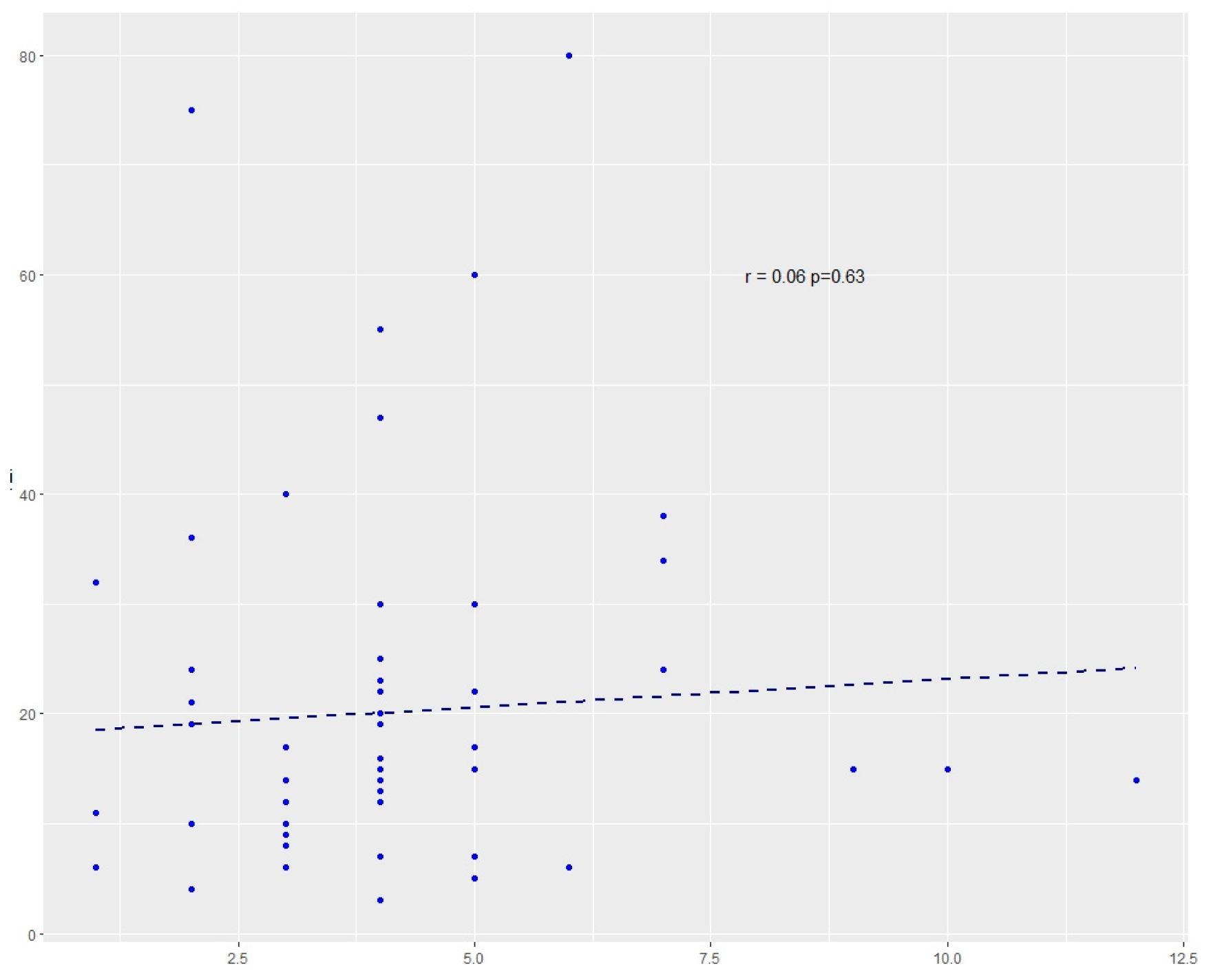
On an average stay of 62 days, the achievement of the FEF occurred in 18 days, and a median of 14. 26 (26.8%) out of 97 reached the FEF within the tenth day of life. The trend of the FEF compared to the start of the MOM availability is shown in Figure 1.
The average MOM feeding at discharge was 47.6% with 36.1% exclusive with an increase from 45.8% in 2017 (EMOM 33.3%) to 58.82% (EMOM 41.18%) in 2021.
The average daily weight gain was 24 grams, with an increase over the years from 21.08 grams in 2017 to 31.36 grams in 2021. Moreover, we also observed a growth of the mean weight increase (p<0.001) during this period. There is no statistically significant difference between infants fed with their mother’s milk and those fed with bank milk.
There was no statistical significance of gestational age, weight, type of delivery and pregnancy if single or twin and maternal age on the availability of MOM during hospitalization (Table n° 3).
The maternal age and the onset of breast milk have a statistically significant impact on the type of feeding at discharge (Table n° 4) if the three categories (EMOM, MMOM, FM) are distinguished and, if two HM groups (EMOM + MMOM) and FM are compared, gestational age at birth is also significant.
All patients discharged with BM alone or BM with FM, started with MOM feeding earlier than those discharged with preterm formula (p=0.032).

| Overall (N=97) | |
|---|---|
| GA | |
| Mean (SD) | 28.56 (2.73) |
| Median (Q1, Q3) | 29.00 (27.00, 30.00) |
| Min - Max | 23.00 - 35.00 |
| Non missing N | 97 |
| Birth Weight | |
| Mean (SD) | 1091.48 (287.93) |
| Median (Q1, Q3) | 1110.00 (870.00, 1320.00) |
| Min - Max | 520.00 - 1495.00 |
| Non missing N | 97 |
| Year | |
| 2017 | 24 (24.7%) |
| 2018 | 24 (24.7%) |
| 2019 | 24 (24.7%) |
| 2020 | 8 (8.2%) |
| 2021 | 17 (17.5%) |
| Non missing N | 97 |
| Single/Twin | |
| T | 36 (37.5%) |
| S | 60 (62.5%) |
| Non missing N | 96 |
| Missing N | 1 |
| Delivery | |
| V | 14 (14.6%) |
| CS | 82 (85.4%) |
| Non missing N | 96 |
| Missing N | 1 |
| MA | |
| Mean (SD) | 32.62 (6.11) |
| Median (Q1, Q3) | 33.00 (28.50, 37.50) |
| Min - Max | 19.00 - 46.00 |
| Non missing N | 95 |
| Missing N | 2 |
| DM ml | |
| Mean (SD) | 4015.88 (3840.05) |
| Median (Q1, Q3) | 2900.00 (500.00, 7100.00) |
| Min - Max | 12.00 - 12200.00 |
| Non missing N | 68 |
| Missing N | 29 |
| Start MEF | |
| Mean (SD) | 1.78 (1.03) |
| Median (Q1, Q3) | 2.00 (1.00, 2.00) |
| Min - Max | 1.00 - 7.00 |
| Non missing N | 96 |
| Missing N | 1 |
| MOM | |
| NO | 29 (30.5%) |
| YES | 66 (69.5%) |
| Non missing N | 95 |
| Missing N | 2 |
| Start MOM | |
| Mean (SD) | 4.11 (1.93) |
| Median (Q1, Q3) | 4.00 (3.00, 5.00) |
| Min - Max | 1.00 - 12.00 |
| Non missing N | 65 |
| Missing N | 32 |
| FEF | |
| Mean (SD) | 18.53 (14.30) |
| Median (Q1, Q3) | 15.00 (9.00, 22.00) |
| Min - Max | 3.00 - 80.00 |
| Non missing N | 86 |
| Missing N | 11 |
| Days of hospitalization | |
| Mean (SD) | 62.14 (25.76) |
| Median (Q1, Q3) | 58.00 (45.25, 76.00) |
| Min - Max | 22.00 - 161.00 |
| Non missing N | 94 |
| Missing N | 3 |
| Weight at discharge | |
| Mean (SD) | 2538.55 (529.59) |
| Median (Q1, Q3) | 2390.00 (2157.50, 2802.50) |
| Min - Max | 1781.00 - 4960.00 |
| Non missing N | 96 |
| Missing N | 1 |
| Feeding at discharge | |
| FM | 51 (52.6%) |
| MOM | 35 (36.1%) |
| MOM+FM | 11 (11.3%) |
| Non missing N | 97 |
| Average daily weight increment | |
| Mean (SD) | 24.02 (7.22) |
| Median (Q1, Q3) | 23.00 (19.67, 26.85) |
| Min - Max | 12.20 - 71.30 |
| Non missing N | 92 |
| Missing N | 5 |
Table 2.
Trend over the years.
| Year | 2017 | 2018 | 2019 | 2020 | 2021 | p |
|---|---|---|---|---|---|---|
| n° | 24 | 24 | 24 | 8 | 17 | |
| GA (mean (SD)) | 27.29 (2.37) | 28.58 (2.89) | 29.00 (2.59) | 29.25 (3.28) | 29.35 (2.57) | 0.097 |
| Weight (mean (SD)) | 1030.00 (316.32) | 1085.46 (281.31) | 1139.29 (298.99) | 1052.50 (243.35) | 1137.65 (270.64) | 0.680 |
| Sing_Twins = S (%) | 17 (70.83) | 16 (66.67) | 15 (65.22) | 5 ( 62.50) | 7 ( 41.18) | 0.372 |
| CS (%) | 18 (78.26) | 21 (87.50) | 18 (75.00) | 8 (100.00) | 17 (100.00) | 0.117 |
| Maternal age (mean (SD)) | 31.86 (6.15) | 32.38 (6.98) | 31.04 (5.71) | 33.75 (4.13) | 35.65 (5.48) | 0.168 |
| MOM =YES (%) | 16 (66.67) | 15 (62.50) | 21 (91.30) | 1 ( 14.29) | 13 ( 76.47) | 0.003 |
| Start MOM (mean (SD)) | 4.44 (2.16) | 4.47 (2.53) | 4.00 (1.63) | 4.00 (0.00) | 3.30 (1.16) | 0.602 |
| DM ml (mean (SD)) | 3211.25 (3324.12) | 4599.29 (4045.35) | 3200.57 (3510.58) | 9883.33 (2116.99) | 2125.00 (1935.94) | <0.001 |
| Start MEF (mean (SD)) | 1.52 (0.73) | 2.04 (1.40) | 1.67 (0.48) | 2.38 (1.92) | 1.65 (0.61) | 0.180 |
| FEF (mean (SD)) | 22.77 (21.76) | 15.58 (7.37) | 16.22 (10.72) | 20.88 (14.95) | 19.89 (12.75) | 0.433 |
| Length of stay(mean (SD)) | 65.71 (30.32) | 68.54 (28.76) | 60.58 (22.10) | 59.50 (19.34) | 52.12 (21.49) | 0.331 |
| Average daily weight increment (mean (SD)) | 21.08 (3.44) | 22.27 (4.46) | 23.83 (5.72) | 21.55 (3.95) | 31.36 (11.25) | <0.001 |
GA Gestational Age, MOM: Mother’s Own Milk, CS: Cesarean Section, MEF: Minimal Enteral Feeding, FEF: Full Enteral Feeding, DM: Donor Milk.
Table 3.
MOM feeding during hospitalization.
| NO | YES | p | |
|---|---|---|---|
| n° | 29 | 66 | |
| GA (mean (SD)) | 29.28 (2.95) | 28.23 (2.57) | 0.084 |
| Weight (mean (SD)) | 1169.24 (291.62) | 1059.64 (281.78) | 0.087 |
| Sing_Twins = S (%) | 14 (50.00) | 44 (66.67) | 0.198 |
| CS (%) | 24 (82.76) | 56 (86.15) | 0.910 |
| Maternal Age (mean (SD)) | 32.00 (7.19) | 32.83 (5.68) | 0.553 |
| Start MOM (mean (SD)) | 3.00 (2.83) | 4.07 (1.84) | 0.429 |
| Length of stay (mean (SD)) | 57.34 (27.31) | 64.59 (25.00) | 0.213 |
| Average daily weight increment (mean (SD)) | 23.38 (4.44) | 24.43 (8.26) | 0.527 |
| Start MEF (mean (SD)) | 1.90 (1.18) | 1.72 (0.98) | 0.457 |
| FEF (mean (SD)) | 14.88 (7.30) | 19.53 (15.73) | 0.162 |
GA: Gestational Age, MOM: Mother’s Own Milk, CS: Cesarean Section, MEF: Minimal Enteral Feeding, FEF: Full Enteral Feeding.
Table 4.
Feeding at discharge.
| FM vs MOM vs MOM+FM | FM vs MOM | |
|---|---|---|
| p | p | |
| GA (mean (SD)) | 0.101 | 0.032 |
| Weight (mean (SD)) | 0.182 | 0.065 |
| Sing_Twins = S (%) | 0.584 | 0.460 |
| CS (%) | 0.323 | 0.538 |
| Maternal Age (mean (SD)) | 0.048 | 0.059 |
| Start MOM (mean (SD)) | 0.032 | 0.009 |
| Length of stay(mean (SD)) | 0.622 | 0.733 |
| Average daily weight increment(mean (SD)) | 0.845 | 0.562 |
| Start MEF (mean (SD)) | 0.719 | 0.670 |
| FEF (mean (SD)) | 0.225 | 0.620 |
GA: Gestational Age, MOM: Mother’s Own Milk, CS: Cesarean Section, MEF: Minimal Enteral Feeding, FEF: Full Enteral Feeding, FM: Formulated Milk.
3. Discussion
Preterm infants are a high-risk population and prematurity is a leading cause of neonatal morbidity and mortality. Feeding with breast milk during first days and months, is one of the factors that most impact the health of these vulnerable infants, as it reduces the incidence and severity of complications associated with prematurity and their related costs13-15. In addition, exposure to MOM, particularly in the first weeks of life, also improves long-term outcomes, especially the neurodevelopment16-18, and reduces disease and rehospitalization rates in the first year of life15. These effects are attributable to immunological, antimicrobial, anti-inflammatory, antioxidant, epigenetic, growth-promoting, and intestinal colonizing functions exerted by multiple bioactive factors, many of which are present in higher concentrations in the breast milk of mothers of preterm infants6. The protective action is a dose-response relationship, with higher and prolonged doses of MOM providing maximum protection19. Breast milk exposure rates vary widely between studies.
The first discussion item is just the fragmentation and inhomogeneity of the data on this topic, which instead is fundamental in the care of infants in NICU because it conditions their survival, their outcome and therefore their future. In the literature, there are monocentric reports like this and rare and unsystematic multicenter reports or data from national or international registers. Institutions dealing with child health should plan a program of constant monitoring of this aspect of life in NICU, which starts from the individual realities and extends to nations and continents.
Besides, the analysis of each center and the sharing of data also has its value for improving quality, whose tools cannot disregard from the collection, analysis, understanding and communication of data.
The percentages of feeding with MOM of 69.5% recorded in our NICU are not satisfactory but better than the European20-24 (France 49%, Germany 47-60%, 44% in Portugal, 53.6%-78% in Greece, 49% in Sweden) and the Chinese25 data (58%) and in line with those of the United States26-28 (70%-75%); above all, they are values that have been growing over the years except for 2020, the year of the Covid 19 pandemic. This trend is common to other countries that recorded a 10-20% increase over the years20. In contrast is the resounding data of Sweden12, which has gone from 55% of exclusive feeding with MOM of very preterm babies in 2004 to 16% in 2013, from 41% to 34% in preterm newborns between 28 and 31 weeks and from 64% to 49% in moderately preterm infants (GA 32-36 weeks).
The most virtuous model remains Brazil, which has national standardized the integrated system of assistance in NICU and promotion of breastfeeding and donation, which it also exports to other states. In Brazil29 the prevalence of exclusive breastfeeding was 65.2% at discharge, 51% at 3 months, and 20.6% at 6 months.
Our data confirm the devastating effect of the pandemic on feeding babies with MOM (Table n°2), as well as the dramatic reduction in milk donation. In 2020 the phenomenon was so important that all associations and scientific societies drew up documents to try to remove fears, reassuring about breastfeeding and revive the spirit of generosity of women who have a surplus of milk. In contrast with the general trend, in our HMB30 milk donations grew in those critical months. Most probably this result was due to the spirit of solidarity which was very strong in the first period together with the sharing of our HMB with women donors which has never stopped and actually strengthened during those difficult days.
Initiation of MEF with DM averaged 1.78 days and with MOM 4.11 days. In our study, the start MEF with MOM has been improving over the years, from an average of 4.44 days to 3.3 days. The start of feeding with MOM was a factor that significantly influenced the type of milk at discharge (p=0.009), in line with other authors28 who found that the main predictor of breastfeeding at discharge was the reception of MOM by the third day of age. It is known that the first hours and days after birth are a decisive moment for the start of breastfeeding.
Although there is no clear consensus in the guidelines regarding EF, more reports recommend the early and progressive EF31-39. In particular, it is advisable to start in the first 6 hours40, if the clinical conditions allow it, and in any case within the first 24-72 hours of life. Initiation of enteral feeding within 72 hours of birth41,42 appears to reduce mortality, risk of sepsis, of bronchodysplasia, and length of hospital stay. To have maternal colostrum readily available, it is important to avoid a delay in secretory activation, also because the transition from differentiation to secretory activation within 72 hours of birth has an impact on long-term milk production43. Early, frequent, and effective expression is crucial for both the effect on health and on the duration of breastfeeding.
It is believed that for premature babies the early expression of breast milk has a value comparable to the early onset of breastfeeding for full-term infants on the success of prolonged exclusive breastfeeding. Parker et al44. reported that first milk expression within 8 hours was superior to 9-24 hours with respect to maximal duration of provision of mother’s milk for hospitalized VLBW infants, but emphasizes that to establish the causal relationship between timing of first milk expression and long-term lactation success, randomized control trials are needed.
This suggests intensifying compliance with the breast stimulation protocol that recommends starting within 6 hours of delivery43. In this study, the data of the time of the first breast stimulation is missing. However, data in the literature show unsatisfactory percentages for mothers who start expressing milk within 6 hours of delivery (36% in Finland45, 17% in Japan46, 3.3% in India47).
The most effective intervention to achieve the objective of an early and frequent expression of milk is the preventive information. When mothers receive adequate information, with scientific and practical content, about the importance of their breast milk, the results are more satisfactory48.
In our maternity unit, all women after premature birth are equipped with a breast pump, along with indications and recommendations on the practice of systematic breast stimulation; nevertheless, we would like to emphasize that the care of mothers on this aspect, ranging from information to systematic dialogue, monitoring of milk production and support for extraction and direct breastfeeding, must become central in the day-to-day economy of assistance for premature babies.
In our study, one of the most important elements for the aim of ensuring a longer duration of exposure of VLBWs to breast milk, which is that of the transition to the breast, was not analyzed. NICU infants face a unique set of challenges, and infants’ progression to breastfeeding is often complicated by clinical criticalities, gastro-immaturity, and underlying medical comorbidities. Supportive practices such as oral therapy, skin-to-skin care and non-nourishing sucking are of great importance for the earlier initiation of breastfeeding, but also for the development and relationship of the dyad. Research49-51 has shown that these practices support breast milk volumes and the baby’s transition from enteral feed to breastfeeding, thus leading to higher breastfeeding rates. These are carried out systematically in our NICU and this could explain the improvement of data over the years, but they must be better accompanied by a total cultural change of pace in the monitoring and in the continuous improvement of care.
Maximum protection induced by breast milk is achieved when vulnerable infants receive high doses and long exposure to MOM31. Daily volumes of at least 500 ml before day 14 are indicated to be associated with significantly higher breastfeeding rates at discharge52. Breast milk volumes should be monitored to adapt clinical practice interventions. There are sporadic reports on this focus. One of the few examples is mPINC survey, a biennial census of all maternity care hospitals in the United States and territories to monitor practices and policies related to infant feeding.
The achievement of FEF occurred within 14 days for 65% of VLBWs with an a median of 15 days. This is also important data to monitor, because the achievement of FEF translates into the suspension of parenteral nutrition and central venous access, with all what this entails in terms of complications related to both factors. We have not found comparable data on the average time to reach the FEF in the literature, and this element could also be a starting point for dedicated monitoring53,54. Two recent systematic reviews and meta-analyses55 and other studies56 show that the use of HM (MOM or DM) vs the formula leads to a better food tolerance, allows starting enteral feeding earlier, to increase milk volumes more rapidly with the faster achievement of FEF and allows reducing the use of parenteral nutrition and the related risks. Our NICU with attached HMB can be a confirmation57. In this regard, it should not be surprising that in our study no association was found between the use of MOM and the achievement of FEF or the length of hospitalization, which also reduced over the years, because no FM is used but only human milk since 2010.
In other NICUs, central catheters are removed when patients achieve an EF of 100 mL/kg/day58.
Even without a precise rule, but with an individualized approach, our cutoff varies between 80 and 100 ml/kg/day and we have a dedicated protocol on the progression of enteral feeding. There are some studies that have compared the effects between a slow increase in intake and a more aggressive progression of volumes.
The evidence-oriented literature is more likely to consider that enteral feeding, specifically early onset and faster enteral advancement, impacts on preterm infants’ health during the first month of life, acting on the intestine promoting its maturation e a more beneficial microbiome composition, but also reducing inflammation and improving brain growth and neurodevelopment. Instead, delaying MEF and FEF may decrease the functional adaptation of the gastrointestinal tract and disrupt microbial colonization patterns59,60, promote inflammation17 that increases the risk of comorbidities61,62 and therapies to manage them, like steroid use, can impair linear growth63. Small and large randomized31-38 trials seem to show that rapid enteral advancement and, even, early aggressive feeding regimens are feasible also in very small infants (750-1250 g), because they are not associated with increased risk of feed intolerance or NEC; maybe they do not reduce significantly mortality or morbidity during hospitalization but decreases the days to reach FEF and reduce the mean NICU stay duration. Also, in a review of 201955 a more sustained advancement appears to be safe and feasible in stable VLBW infants with birth weight >1000-1200 g, although it is believed that a large, randomized trial is needed to confirm the benefits.
In addition, the management of the advancement of enteral inputs also changes with respect to the country since, in many high-income countries, the conservative approach with a slower increase in volumes prevails, fearing that early FEF could increase the risk of hypoglycemia, food intolerance, gastro-esophageal reflux, ab ingestis and NEC in very preterm infants or VLBW38,39,64-66. However, in low- and middle-income countries with fewer resources for neonatal care, the practice tends to favor the early introduction and advancement of enteral feeds for stable infants67.
Others68 indicate that slow advancement of enteral feed volumes compared to faster rates probably does not reduce the risk of NEC, death, or food intolerance in very preterm or VLBW infants, and instead may slightly increase the risk of invasive infection.
We also consider once again that the increase in the duration of parenteral nutrition is associated with infectious and metabolic complications that increase mortality and morbidity, prolong hospital stay and negatively affect growth and development69. For these reasons, some authors20 believe that an early transition to full-volume enteral feeding should be seen as an ideal therapy to promote appropriate growth, body composition and development in preterm infants.
Discharge is a more studied topic. The data of breastfeeding at discharge are very unsatisfactory, with an average percentage of BF of 47.4%, if we consider the objectives indicated by national and transnational institutions. The numbers have grown over the years, except for 2020, the year of the pandemic. Data in line with those reported by VON70, where National data from more than 800 NICUs showed that provision of human milk at discharge among VLBW infants has increased from 44% in 2008 to 52% in 2017.
In Germany, 60.1% of patients were discharged with exclusive MOM feeds out of a sample of 368 premature babies21. This rate was higher than in the EPIPAGE-2 cohort study20, which reported 25% exclusive feeding and 47% of some MOM feeds at discharge in children under 32 weeks. In Greece, 48% of breastfeeding at discharge is reported24.
In the cohort from 11 countries in 19 European regions, 58.5% of preterm infants < 32 weeks received human milk at discharge20 with important regional differences in breastfeeding rates and significant variations reaching from 36% to 80%. Rates ranging from 49% to 87% among NICUs have been reported in the United States28.
In a multicentric study71 45% of infants <1500 g birth weight and 23% of infants >2500 g did not receive MOM at discharge in Italy. In a more recent report72 of a single NICU, the 66% of preterm infants received any breastfeeding at discharge of which 27% were exclusively breastfed. A more up-to-date Italian survey would be desirable.
Very few reports have evaluated breastfeeding in the months following discharge.
Few Portuguese studies73 have reported a low and variable (1.0% to 27.0%) prevalence of exclusive breastfeeding at 6 months and any breast milk at 12 months (8.0% to 12.0%). In another Greek study74, 58.1% were exclusively breastfed during the first month, with a gradual decrease to 36.9% to the third month of life and 19.4% to the sixth. The prevalence of breastfed infants reached 14.7% and 7.5% at the ages of twelve and eighteen months, respectively.
Young maternal age is indicated in some studies as a risk factor for NMOM feeding at discharge. Every year of MA was associated with a 1.24-fold increase in direct breastfeeding at hospital discharge, or infants with mothers younger than 25 years were 30% less likely to be breastfed than infants with older mothers75. Mothers aged <25 years ceased breastfeeding more often before discharge and before six months of age than mothers over the age of 2576.
In our study, feeding with HM at discharge was 54.5% for mothers aged 36 to 40 years and 21.4% for those aged 21 to 30 years with the only statistically significant difference (p value<0.005), and maternal age was a factor that significantly influenced breastfeeding at discharge. Thus, younger mothers represent a category to be supported more.
Of the 13 GA≤25 weeks infants, 77% received MOM in the first few weeks and 61.5% received at discharge. For the 30 infants born of GA ≥30 weeks, 58% received MOM in NICU and 35% at discharge. Statistically significant association was found between gestational age and MOM feeding at discharge. In our previous report77, mothers of preterm babies of GA ≤29-week were more likely to produce breast milk.
Probably, the care dedicated to the mothers of VLBW is more effective both for the predisposition of mothers who recognize, in the extraction of milk, the only act they can make available for the survival and health of their children, and for the health personnel, who welcome a newborn who will undergo a long hospitalization. The data is interesting, considering that the milk produced by the mothers of VLBWs has a specific composition tailored to this fragile category of premature babies77,78. But it is objectively paradoxical that babies born at a higher gestational age and who are therefore more able, have been fed less with MOM.
37.5% of VLBW premature babies are twins.
Of the 37 twins, 50% received MOM in NICU compared to 66.7% of those born from single pregnancies with unexpectedly higher rates of MOM in discharge for twins (48.3% vs 43.1%). This confirm a trend of our NICU79, and comparing it with the few other reports available, we can state that multiples were not at higher risk of NMOM feed than singletons in some cases. But the data on multiple births are controversial, since some studies show an association with exclusive breastfeeding80, while others75,81,,82 show an association with NMOM feeds or discontinuation of breastfeeding before six months of age. Further studies to clarify this point would be needed.
The type of delivery, although with clearly prevalent CS, did not affect the type of feeding either during hospitalization or at discharge. Weight growth is one of the most important factors in the management of VLBWs for their implications on the outcome. Average daily weight gain has improved significantly and this is an encouraging achieved goal.
There is a debate about the comparison between breast milk and donated milk, and their impact on VLBW growth. In our report there is no statistical significance in monitoring weight gain with respect to the type of diet (in our NICU, only human milk is used for VLBW), namely there was no significant difference in the daily weight trend between those fed with DM and those fed with their mother’s milk, both fortified at the right time. Santiago83 et al. conducted a review with heterogeneous results regarding weight gain and linear growth in infants’ fed with human milk, fortified human milk or preterm formula76. The data in the literature are controversial but it is shown that the presence of HMBs and/or the use of DM in NICU are associated with an increased incidence of breastfeeding both during hospitalization and at discharge84. And this is also our experience.
An international survey85 on differences in feeding practices found that most NICUs with access to DM started enteral feeding earlier and progressed more rapidly. Units without access to DM often delayed the introduction of enteral feeds until MOM was available86.
We believe that providing DM to vulnerable infants who do not have MOM can save lives and raise awareness of the value of breastfeeding and human milk in NICU and in the community.
Few modifiable factors were included in our study. However, it should be remembered that in the NICU, the most significant results are obtained when the staff is trained to promote breastfeeding and donation87. The role of health professionals in a multidisciplinary framework is fundamental in supporting mothers in breastfeeding in neonatal intensive care, in accompanying early and frequent expression of milk, in promoting skin to skin and direct breast attack when conditions allow it. They should be prepared to identify and counteract psychological, physical, social and cultural barriers to successful milk extraction and to breastfeeding. It is a question of priorities that should be established and integrated into the cultural background and in daily actions.
4. Conclusions and relevance
VLBWs pose a significant nutritional challenge. Feeding rates with MOM during hospitalization and at discharge have improved increasing by 13% circa in recent years, a common trend to other countries, but these levels are still very far from those indicated by the WHO and the national and international bodies and agency. The year of the pandemic was devastating also for our NICU, with a marked reduction in the use of MOM and in breastfeeding. The timing of the start of EF resulted the most important predictive element of MOM feeding, which, over the years, is back to 72 hours of life. ELBW infants’ mothers extract more milk, and young mothers feed less their preterm babies with MOM. No significant differences have been registered in the trend of the VLBW babies’ weight between those fed with MOM and those fed with DM. The literature lacks systematic and coherent data, which are useful for a necessary monitoring of feeding in NICU and in the months after discharge, if you consider the quantitative and qualitative impact of the use of mother’s milk on development and outcome, therefore on the future of this vulnerable category of children.
Abbreviations
| MOM | Mother’s Own Milk |
| EMOM | Exclusive Mother’s Own Milk |
| MMOM | Mixed Mother’s Own Milk |
| NMOM | No Mother’s Own Milk |
| HM | Human Milk |
| DM | Donor Milk |
| FM | Formula Milk |
| HMB | Human Milk Bank |
| BF | Breastfeeding |
| EBF | Exclusive Breastfeeding |
| EF | Enteral Feeding |
| MEF | Minimal Enteral Feeding |
| FEF | Full Enteral Feeding |
| VLBW | Very Low Birth Weight |
| ELBW | Estremely Low Birth Weight |
| NEC | Necrotizing Enterocolitis |
References
- Cao, G.; Liu, J.; Liu, M. Global, Regional, and National Incidence and Mortality of Neonatal Preterm Birth, 1990-2019. JAMA Pediatr. 2022, 176, 787–796. [Google Scholar] [CrossRef] [PubMed]
- Walani, S.R. Global burden of preterm birth. Int. J. Gynecol. Obstet. 2020, 150, 31–33. [Google Scholar] [CrossRef] [PubMed]
- Liu, L.; Oza, S.; Hogan, D.; Chu, Y.; Perin, J.; Zhu, J.; Lawn, J.E.; Cousens, S.; Mathers, C.; Black, R.E. Global, regional, and national causes of under-5 mortality in 2000–15: an updated systematic analysis with implications for the Sustainable Development Goals. Lancet 2016, 388, 3027–3035. [Google Scholar] [CrossRef] [PubMed]
- Zeitlin, J.; Szamotulska, K.; Drewniak, N.; Mohangoo, A.; Chalmers, J.; Sakkeus, L.; Irgens, L.; Gatt, M.; Gissler, M.; Blondel, B.; et al. Preterm birth time trends in Europe: a study of 19 countries. BJOG: Int. J. Obstet. Gynaecol. 2013, 120, 1356–1365. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization. Causes of newborn mortality and morbidity in the European Region. Ac-cessed June 26, 2020. https://www.euro.who.int/en/health-topics/Life-stages/maternal-and-newborn-health/causes-of-newborn-mortality-and-morbidity-inthe-european-region.
- Boquien, C.-Y. Human Milk: An Ideal Food for Nutrition of Preterm Newborn. Front. Pediatr. 2018, 6, 295. [Google Scholar] [CrossRef] [PubMed]
- Bertino, E., Di Nicola, P., Giuliani, F., Peila, C., Cester, E., Vassia, C., Pirra, A., Tonetto, P., & Coscia, A. 2012. Benefits of human milk in preterm infant feeding. Journal of Pediatric and Neonatal Individualized Medicine, 1(1), 19-24. [CrossRef]
- Sankar, M.J.; Sinha, B.; Chowdhury, R.; Bhandari, N.; Taneja, S.; Martines, J.; Bahl, R. Optimal breastfeeding practices and infant and child mortality: a systematic review and meta-analysis. Acta Paediatr. 2015, 104, 3–13. [Google Scholar] [CrossRef] [PubMed]
- Victora, C.G.; Bahl, R.; Barros, A.J.D.; Franca, G.V.A.; Horton, S.; Krasevec, J.; Murch, S.; Sankar, M.J.; Walker, N.; Rollins, N.C.; et al. Breastfeeding in the 21st century: epidemiology, mechanisms, and lifelong effect. Lancet 2016, 387, 475–490. [Google Scholar] [CrossRef]
- Moro, G.E.; Arslanoglu, S.; Bertino, E.; Corvaglia, L.; Montirosso, R.; Picaud, J.-C.; Polberger, S.; Schanler, R.J.; Steel, C.; van Goudoever, J.; et al. XII. Human Milk in Feeding Premature Infants. J. Pediatr. Gastroenterol. Nutr. 2015, 61, S16–S19. [Google Scholar] [CrossRef]
- WHO Guidelines on optimal feeding of low birth-weight infants in low- and middle-income countries. https://www.who.int/maternal_child_adolescent/documents/infant_feeding_low_bw/en/.
- Ericson, J.; Flacking, R.; Hellström-Westas, L.; Eriksson, M. Changes in the prevalence of breast feeding in preterm infants discharged from neonatal units: a register study over 10 years. BMJ Open 2016, 6, e012900. [Google Scholar] [CrossRef]
- Johnson, T.J.; Patel, A.L.; Schoeny, M.E.; Meier, P.P. Cost Savings of Mother’s Own Milk for Very Low Birth Weight Infants in the Neonatal Intensive Care Unit. PharmacoEconomics - Open 2022, 6, 451–460. [Google Scholar] [CrossRef]
- Patel, A.L.; Johnson, T.J.; Robin, B.; Bigger, H.R.; Buchanan, A.; Christian, E.; Nandhan, V.; Shroff, A.; Schoeny, M.; Engstrom, J.L.; et al. Influence of own mother's milk on bronchopulmonary dysplasia and costs. Arch. Dis. Child. - Fetal Neonatal Ed. 2016, 102, F256–F261. [Google Scholar] [CrossRef] [PubMed]
- Meier, P.P. More evidence: Mothers’ own milk is personalized medicine for very low birthweight infants. Cell Rep. Med. 2022, 3, 100710. [Google Scholar] [CrossRef] [PubMed]
- Lechner, B.E.; Vohr, B.R. Neurodevelopmental Outcomes of Preterm Infants Fed Human Milk: A Systematic Review. Clin. Perinatol. 2017, 44, 69–83. [Google Scholar] [CrossRef] [PubMed]
- Thoene, M.; Anderson-Berry, A. Early Enteral Feeding in Preterm Infants: A Narrative Review of the Nutritional, Metabolic, and Developmental Benefits. Nutrients 2021, 13, 2289. [Google Scholar] [CrossRef] [PubMed]
- Twilhaar, E.S.; Wade, R.M.; de Kieviet, J.F.; van Goudoever, J.B.; van Elburg, R.M.; Oosterlaan, J. Cognitive Outcomes of Children Born Extremely or Very Preterm Since the 1990s and Associated Risk Factors: A Meta-analysis and Meta-regression. JAMA Pediatr. 2018, 172, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Xu, Y.; Yu, Z.; Li, Q.; Zhou, J.; Yin, X.; Ma, Y.; Yin, Y.; Jiang, S.; Zhu, R.; Wu, Y.; et al. Dose-dependent effect of human milk on Bronchopulmonary dysplasia in very low birth weight infants. BMC Pediatr. 2020, 20, 1–8. [Google Scholar] [CrossRef] [PubMed]
- Mitha, A.; Piedvache, A.; Khoshnood, B.; Fresson, J.; Glorieux, I.; Roué, J.; Blondel, B.; Durox, M.; Burguet, A.; Ancel, P.; et al. The impact of neonatal unit policies on breast milk feeding at discharge of moderate preterm infants: The EPIPAGE-2 cohort study. Matern. Child Nutr. 2019, 15, e12875. [Google Scholar] [CrossRef] [PubMed]
- Heller, N.; Rüdiger, M.; Hoffmeister, V.; Mense, L. Mother’s Own Milk Feeding in Preterm Newborns Admitted to the Neonatal Intensive Care Unit or Special-Care Nursery: Obstacles, Interventions, Risk Calculation. Int. J. Environ. Res. Public Heal. 2021, 18, 4140. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Severo, M.; Zeitlin, J.; Barros, H.; (, O.B.O.T.P.E. The Type of Feeding at Discharge of Very Preterm Infants: Neonatal Intensive Care Units Policies and Practices Make a Difference. Breastfeed. Med. 2018, 13, 50–59. [Google Scholar] [CrossRef]
- Daglas, Maria; Sidiropoulou, Charikleia; Galanis, Petros; Bilali, Angeliki; Antoniou, Evangelia; Iatrakis, Georgios Maternal and Neonatal Factors Associated with Successful Breastfeeding in Preterm Infants. International Journal of Caring Sciences January– April 2020 Volume 13 | Issue 1| Page 152 www.internationaljournalofcaringsciences.org.
- Iliodromiti, Z., Papamichail, D., Ekizoglou, Ch., Nteka, E., Mavrika, P., Zografaki, E., Koutentakis, K., Zidropoulos, S., Stavrou, D., Panagiotopoulos, T., Antoniadou-Koumatou, I. (2018). National Study to estimate the frequency and determinants of Breastfeeding in Greece. Athens: Institute of Child Health.
- Dong, D.; Ru, X.; Huang, X.; Sang, T.; Li, S.; Wang, Y.; Feng, Q. A prospective cohort study on lactation status and breastfeeding challenges in mothers giving birth to preterm infants. Int. Breastfeed. J. 2022, 17, 1–13. [Google Scholar] [CrossRef]
- USA Boundy EO, Perrine CG, Nelson JM, Hamner HC. Disparities in hospital reported breast Milk use in neonatal intensive care units - United States, 2015. MMWR Morb Mortal Wkly Rep. 2017;66(48):1313–7. [CrossRef]
- Kalluri, N.S.; Burnham, L.A.; Lopera, A.M.; Stickney, D.M.; Combs, G.L.; Levesque, B.M.; Philipp, B.L.; Parker, M.G. A Quality Improvement Project to Increase Mother’s Milk Use in an Inner-City NICU. Pediatr. Qual. Saf. 2019, 4, e204. [Google Scholar] [CrossRef] [PubMed]
- Dinesh Dharel, MD1,2, Nalini Singhal, MD1, Christel Wood, LC1, Zenon Cieslak, MD3, Fabiana Bacchi-ni, MSc4, Prakesh S. Shah, MD5, Xiang Y. Ye, MSc5, and Belal Alshaikh, MD, MSc, MSCE1, on behalf of the Canadian Neonatal Network (CNN) and Canadian Preterm Birth Network (CPTBN) Investigators. Rates and Determinants of Mother’s Own Milk Feeding in Infants Born Very Preterm Pediatr 2021;236:21-7).
- Silva, M.D.B.; Oliveira, R.d.V.C.d.; Alves, D.d.S.B.; Melo, E.C.P. Predicting risk of early discontinuation of exclusive breastfeeding at a Brazilian referral hospital for high-risk neonates and infants: a decision-tree analysis. Int. Breastfeed. J. 2021, 16, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Quitadamo, P. A. (2020). Correspondence: the donation of human milk during the COVID-19 pandemic. Journal of Pediatric and Neonatal Individualized Medicine (JPNIM), 10(1), e100131. [CrossRef]
- Meier, P.P. Prioritizing High-Dose Long Exposure to Mothers' Own Milk During the Neonatal Intensive Care Unit Hospitalization. Breastfeed. Med. 2019, 14, S20–20. [Google Scholar] [CrossRef]
- Modi, M.; Ramji, S.; Jain, A.; Kumar, P.; Gupta, N. Early Aggressive Enteral Feeding in Neonates Weighing 750–1250 Grams: A Randomized Controlled Trial. Indian Pediatr. 2019, 56, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Montealegre-Pomar, A.d.P.; Bertolotto-Cepeda, A.M.; Romero-Marquez, Y.; -Ramírez, K.J.M. Effectiveness and Safety of Fast Enteral Advancement in Preterm Infants Between 1000 and 2000 g of Birth Weight. J. Parenter. Enter. Nutr. 2020, 45, 578–586. [Google Scholar] [CrossRef] [PubMed]
- Raban, S.; Santhakumaran, S.; Keraan, Q.; Joolay, Y.; Uthaya, S.; Horn, A.; Modi, N.; Harrison, M. A randomised controlled trial of high vs low volume initiation and rapid vs slow advancement of milk feeds in infants with birthweights ≤ 1000 g in a resource-limited setting. Ann. Trop. Paediatr. 2016, 36, 288–295. [Google Scholar] [CrossRef]
- Abbott, J.; Berrington, J.; Bowler, U.; Boyle, E.; Dorling, J.; Embleton, N.; Juszczak, E.; Leaf, A.; Linsell, L.; et al.; The Sift Investigators Group The Speed of Increasing milk Feeds: a randomised controlled trial. BMC Pediatr. 2017, 17, 1–6. [Google Scholar] [CrossRef]
- Ahmed, F.; Dey, S.K.; Shahidullah, M.; A Mannan, M.; Raj, A.Y.; Sharmin, S. Early Versus Delayed Enteral Feeding for Achieving Full Feeding in Preterm Growth-Restricted Infants: A Randomized Clinical Trial. 2020, 29, 638–645. [Google Scholar]
- Nangia, S.; Vadivel, V.; Thukral, A.; Saili, A. Early Total Enteral Feeding versus Conventional Enteral Feeding in Stable Very-Low-Birth-Weight Infants: A Randomised Controlled Trial. Neonatology 2019, 115, 256–262. [Google Scholar] [CrossRef]
- de Waard, M.; Li, Y.; Zhu, Y.; Ayede, A.I.; Berrington, J.; Bloomfield, F.H.; Busari, O.O.; Cormack, B.E.; Embleton, N.D.; van Goudoever, J.B.; et al. Time to Full Enteral Feeding for Very Low-Birth-Weight Infants Varies Markedly Among Hospitals Worldwide But May Not Be Associated With Incidence of Necrotizing Enterocolitis: The NEOMUNE-NeoNutriNet Cohort Study. J. Parenter. Enter. Nutr. 2018, 43, 658–667. [Google Scholar] [CrossRef]
- Maas, C.; Franz, A.R.; von Krogh, S.; Arand, J.; Poets, C.F. Growth and morbidity of extremely preterm infants after early full enteral nutrition. Arch. Dis. Child. - Fetal Neonatal Ed. 2017, 103, F79–F81. [Google Scholar] [CrossRef] [PubMed]
- Leaf, A. Introducing enteral feeds in the high-risk preterm infant. Semin. Fetal Neonatal Med. 2013, 18, 150–154. [Google Scholar] [CrossRef] [PubMed]
- Chitale, R.; Ferguson, K.; Talej, M.; Yang, W.-C.; He, S.; Edmond, K.M.; Smith, E.R. Early Enteral Feeding for Preterm or Low Birth Weight Infants: a Systematic Review and Meta-analysis. PEDIATRICS 2022, 150. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.; Chen, X.; Zhu, J.; Jiang, C.; Yu, Z.; Su, A. Effect of First Mother's Own Milk Feeding Time on the Risk of Moderate and Severe Bronchopulmonary Dysplasia in Infants With Very Low Birth Weight. Front. Pediatr. 2022, 10, 887028. [Google Scholar] [CrossRef] [PubMed]
- Parker, L.A.; Sullivan, S.; Krueger, C.; Mueller, M. Association of Timing of Initiation of Breastmilk Expression on Milk Volume and Timing of Lactogenesis Stage II Among Mothers of Very Low-Birth-Weight Infants. Breastfeed. Med. 2015, 10, 84–91. [Google Scholar] [CrossRef] [PubMed]
- Parker, M.G.; Melvin, P.; Graham, D.A.; Gupta, M.; Burnham, L.A.; Lopera, A.M.; Zera, C.A.; Belfort, M.B. Timing of First Milk Expression to Maximize Breastfeeding Continuation Among Mothers of Very Low-Birth-Weight Infants. Obstetrics & Gynecology 2019, 133, 1208–1215. [Google Scholar] [CrossRef]
- Ikonen, R.; Paavilainen, E.; Helminen, M.; Kaunonen, M. Preterm infants’ mothers’ initiation and frequency of breast milk expression and exclusive use of mother's breast milk in neonatal intensive care units. J. Clin. Nurs. 2017, 27, e551–e558. [Google Scholar] [CrossRef]
- Murase, M.; Nommsen-Rivers, L.; Morrow, A.L.; Hatsuno, M.; Mizuno, K.; Taki, M.; Miyazawa, T.; Nakano, Y.; Aizawa, M.; Itabashi, K. Predictors of Low Milk Volume among Mothers Who Delivered Preterm. J. Hum. Lact. 2014, 30, 425–435. [Google Scholar] [CrossRef]
- Daljeet KAK, Geetanjli K, Praveen K. Current practices related to feeding preterm neonates with ex-pressed breast milk: a pilot project. COJ Nurse Health Care. 2018;3(3).
- Alves, E.; Magano, R.; Amorim, M.; Nogueira, C.; Silva, S. Factors Influencing Parent Reports of Facilitators and Barriers to Human Milk Supply in Neonatal Intensive Care Units. J. Hum. Lact. 2016, 32, 695–703. [Google Scholar] [CrossRef]
- Parker, M.G.; Patel, A.L. Using quality improvement to increase human milk use for preterm infants. Semin. Perinatol. 2017, 41, 175–186. [Google Scholar] [CrossRef]
- Spatz, D.L.; Froh, E.B.; Schwarz, J.; Houng, K.; Brewster, I.; Myers, C.; Prince, J.; Olkkola, M. Pump Early, Pump Often: A Continuous Quality Improvement Project. J. Périnat. Educ. 2015, 24, 160–170. [Google Scholar] [CrossRef] [PubMed]
- Takako, H.; Mizue, M.; Izumi, H.; Chie, O.; Harue, T.; Uchida, M.; Spatz, D.L. Improving Human Milk and Breastfeeding Rates in a Perinatal Hospital in Japan: A Quality Improvement Project. Breastfeed. Med. 2020, 15, 538–545. [Google Scholar] [CrossRef] [PubMed]
- Hoban, R.; Bigger, H.; Schoeny, M.; Engstrom, J.; Meier, P.; Patel, A.L. Milk Volume at 2 Weeks Predicts Mother's Own Milk Feeding at Neonatal Intensive Care Unit Discharge for Very Low Birthweight Infants. Breastfeed. Med. 2018, 13, 135–141. [Google Scholar] [CrossRef] [PubMed]
- Bigger, H.R.; Fogg, L.J.; Patel, A.; Johnson, T.; Engstrom, J.L.; Meier, P.P. Quality indicators for human milk use in very low-birthweight infants: are we measuring what we should be measuring? J. Perinatol. 2014, 34, 287–291. [Google Scholar] [CrossRef] [PubMed]
- WHO. Indicators for assessing breastfeeding practices; 2021.
- Alshaikh, B.; Dharel, D.; Yusuf, K.; Singhal, N. Early total enteral feeding in stable preterm infants: a systematic review and meta-analysis. J. Matern. Neonatal Med. 2019, 34, 1479–1486. [Google Scholar] [CrossRef] [PubMed]
- Oddie, S.J.; Young, L.; McGuire, W. Slow advancement of enteral feed volumes to prevent necrotising enterocolitis in very low birth weight infants. Cochrane Database Syst. Rev. 2021, 2021, CD001241. [Google Scholar] [CrossRef] [PubMed]
- Quitadamo, P.A.; Palumbo, G.; Cianti, L.; Lurdo, P.; Gentile, M.A.; Villani, A. The Revolution of Breast Milk: The Multiple Role of Human Milk Banking between Evidence and Experience—A Narrative Review. Int. J. Pediatr. 2021, 2021, 1–11. [Google Scholar] [CrossRef]
- Hair AB. Approach to enteral nutrition in the premature infant. Available at: https://www.uptodate.com/contents/approach-to-enteral-nutrition-in-the-premature-infant.
- Walsh, V.; Brown, J.V.E.; Copperthwaite, B.R.; Oddie, S.J.; McGuire, W. Early full enteral feeding for preterm or low birth weight infants. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef]
- Embleton, N.D.; Berrington, J.E.; Dorling, J.; Ewer, A.K.; Juszczak, E.; Kirby, J.A.; Lamb, C.A.; Lanyon, C.V.; McGuire, W.; Probert, C.S.; et al. Mechanisms Affecting the Gut of Preterm Infants in Enteral Feeding Trials. Front. Nutr. 2017, 4, 14. [Google Scholar] [CrossRef]
- Walsh, V.; Brown, J.V.E.; Copperthwaite, B.R.; Oddie, S.J.; McGuire, W. Early full enteral feeding for preterm or low birth weight infants. Cochrane Database Syst. Rev. 2020, 2020. [Google Scholar] [CrossRef]
- Thoene, M.; Anderson-Berry, A. Early Enteral Feeding in Preterm Infants: A Narrative Review of the Nutritional, Metabolic, and Developmental Benefits. Nutrients 2021, 13, 2289. [Google Scholar] [CrossRef] [PubMed]
- Cuestas, E.; Aguilera, B.; Cerutti, M.; Rizzotti, A. Sustained Neonatal Inflammation Is Associated with Poor Growth in Infants Born Very Preterm during the First Year of Life. J. Pediatr. 2019, 205, 91–97. [Google Scholar] [CrossRef] [PubMed]
- Twilhaar, E.S.; Wade, R.M.; de Kieviet, J.F.; van Goudoever, J.B.; van Elburg, R.M.; Oosterlaan, J. Cognitive Outcomes of Children Born Extremely or Very Preterm Since the 1990s and Associated Risk Factors: A Meta-analysis and Meta-regression. JAMA Pediatr. 2018, 172, 361–367. [Google Scholar] [CrossRef] [PubMed]
- Linafelter, A.; Cuna, A.; Liu, C.; Quigley, A.; Truog, W.E.; Sampath, V.; Oschman, A. Extended course of prednisolone in infants with severe bronchopulmonary dysplasia. Early Hum. Dev. 2019, 136, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Leaf, A. Introducing enteral feeds in the high-risk preterm infant. Semin. Fetal Neonatal Med. 2013, 18, 150–154. [Google Scholar] [CrossRef]
- Conde-Agudelo, A.; Díaz-Rossello, J.L. Kangaroo mother care to reduce morbidity and mortality in low birthweight infants. Cochrane Database Syst. Rev. 2016, 2017, CD002771. [Google Scholar] [CrossRef] [PubMed]
- Alshaikh, B.; Dharel, D.; Yusuf, K.; Singhal, N. Early total enteral feeding in stable preterm infants: a systematic review and meta-analysis. J. Matern. Neonatal Med. 2019, 34, 1479–1486. [Google Scholar] [CrossRef]
- Embleton, N.D. Early nutrition and later outcomes in preterm infants. World Rev. Nutr. Diet 2013, 106, 26–32. [Google Scholar] [CrossRef]
- Parker, M.G.; Greenberg, L.T.; Edwards, E.M.; Ehret, D.; Belfort, M.B.; Horbar, J.D. National Trends in the Provision of Human Milk at Hospital Discharge Among Very Low-Birth-Weight Infants. JAMA Pediatr. 2019, 173, 961–968. [Google Scholar] [CrossRef]
- Davanzo, R.; Monasta, L.; Ronfani, L.; Brovedani, P.; Demarini, S.; Breastfeeding in Neonatal Intensive Care Unit Study Group. Breastfeeding at NICU discharge: A multicenter Italian study. J. Hum. Lact. 2012, 29, 374–380. [Google Scholar] [CrossRef]
- Gianni, M.L.; Bezze, E.N.; Sannino, P.; Baro, M.; Roggero, P.; Muscolo, S.; Plevani, L.; Mosca, F. Maternal views on facilitators of and barriers to breastfeeding preterm infants. BMC Pediatr. 2018, 18, 283. [Google Scholar] [CrossRef] [PubMed]
- Rodrigues, C.; Teixeira, R.; Fonseca, M.J.; Zeitlin, J.; Barros, H.; Portuguese EPICE (Effective Perinatal Intensive Care in Europe) Network. Prevalence and duration of breast milk feeding in very preterm infants: A 3-year follow-up study and a systematic literature review. Paediatr. Périnat. Epidemiology 2018, 32, 237–246. [Google Scholar] [CrossRef] [PubMed]
- Sokou, R.; Parastatidou, S.; Ioakeimidis, G.; Tavoulari, E.-F.; Makrogianni, A.; Isaakidou, E.; Iacovidou, N.; Konstantinidi, A. Breastfeeding in Neonates Admitted to an NICU: 18-Month Follow-Up. Nutrients 2022, 14, 3841. [Google Scholar] [CrossRef] [PubMed]
- Bonnet, C.; Blondel, B.; Piedvache, A.; Wilson, E.; Bonamy, A.E.; Gortner, L.; Rodrigues, C.; Van Heijst, A.; Draper, E.S.; Cuttini, M.; et al. Low breastfeeding continuation to 6 months for very preterm infants: A E uropean multiregional cohort study. Matern. Child Nutr. 2019, 15, e12657. [Google Scholar] [CrossRef]
- Casey, L.; Fucile, S.; Dow, K.E. Determinants of Successful Direct Breastfeeding at Hospital Discharge in High-Risk Premature Infants. Breastfeed. Med. 2018, 13, 346–351. [Google Scholar] [CrossRef]
- Quitadamo, P. A., Palumbo, G., Gatta, A., Cianti, L., Copetti, M., Gentile, M. A., & Cristalli, P. (2018). How do characteristics of donors and their children influence volume and composition of banked milk?. Journal of Pediatric and Neonatal Individualized Medicine (JPNIM), 7(1), e070121. [CrossRef]
- Gates, A.; Marin, T.; De Leo, G.; Waller, J.L.; Stansfield, B.K. Nutrient composition of preterm mother’s milk and factors that influence nutrient content. Am. J. Clin. Nutr. 2021, 114, 1719–1728. [Google Scholar] [CrossRef]
- Quitadamo, P.A.; Comegna, L.; Palumbo, G.; Copetti, M.; Lurdo, P.; Zambianco, F.; Gentile, M.A.; Villani, A. Feeding Twins with Human Milk and Factors Associated with Its Duration: A Qualitative and Quantitative Study in Southern Italy. Nutrients 2021, 13, 3099. [Google Scholar] [CrossRef]
- Pineda, R.G. Predictors of Breastfeeding and Breastmilk Feeding Among Very Low Birth Weight Infants. Breastfeed. Med. 2011, 6, 15–19. [Google Scholar] [CrossRef]
- Hilditch, C.; Howes, A.; Dempster, N.; Keir, A. What evidence-based strategies have been shown to improve breastfeeding rates in preterm infants? J. Paediatr. Child Heal. 2019, 55, 907–914. [Google Scholar] [CrossRef]
- Zachariassen, G.; Faerk, J.; Grytter, C.; Esberg, B.; Juvonen, P.; Halken, S. Factors associated with successful establishment of breastfeeding in very preterm infants. Acta Paediatr. 2010, 99, 1000–1004. [Google Scholar] [CrossRef]
- Santiago, A.C.T.; da Cunha, L.P.M.; Vieira, N.S.A.; Moreira, L.M.O.; de Oliveira, P.R.; Lyra, P.P.R.; Alves, C.d.A.D. Breastfeeding in children born small for gestational age and future nutritional and metabolic outcomes: a systematic review. J. de Pediatr. 2018, 95, 264–274. [Google Scholar] [CrossRef] [PubMed]
- Arslanoglu, S.; Moro, G.E.; Bellù, R.; Turoli, D.; De Nisi, G.; Tonetto, P.; Bertino, E. Presence of human milk bank is associated with elevated rate of exclusive breastfeeding in VLBW infants. jpme 2012, 41, 129–131. [Google Scholar] [CrossRef] [PubMed]
- Klingenberg, C.; Embleton, N.D.; E Jacobs, S.; O'Connell, L.A.F.; A Kuschel, C. Enteral feeding practices in very preterm infants: an international survey. Arch. Dis. Child. - Fetal Neonatal Ed. 2011, 97, F56–F61. [Google Scholar] [CrossRef] [PubMed]
- Shlomai, N.O.; Patt, Y.S.; Wazana, Y.; Ziv-Baran, T.; Strauss, T.; Morag, I. Early Enteral Feeding of the Preterm Infant—Delay until Own Mother’s Breastmilk Becomes Available? (Israel, 2012–2017). Nutrients 2022, 14, 5035. [Google Scholar] [CrossRef]
- Maastrup, R.; Rom, A.L.; Walloee, S.; Sandfeld, H.B.; Kronborg, H. Improved exclusive breastfeeding rates in preterm infants after a neonatal nurse training program focusing on six breastfeeding-supportive clinical practices. PLOS ONE 2021, 16, e0245273. [Google Scholar] [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



