
Submitted:
27 April 2023
Posted:
03 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Coronavirus disease (COVID-19) has had devastating impacts on the global economy and public health. This study aimed to assess the level of COVID-19 vaccine acceptance, hesitancy, and associated factors among staff and students of the Federal University of Health Sciences Otukpo, Benue State, Nigeria. A web-based cross-sectional survey was conducted between November 2021 and April 2022, and data were collected and analyzed using descriptive and inferential statistics. Of the 150 completed and analyzed questionnaires, the majority of respondents (80.0%) were between 16 and 45 years old. The study found that 58.4% of participants indicated vaccine hesitancy, with skepticism about the vaccine's fast production/rollout and fear of vaccine side effects being the most common reasons for hesitation. Respondents' age, religion, and category were significant factors influencing vaccine acceptance and hesitancy (P < 0.05). The university community has a high level of awareness of COVID-19 but low vaccine acceptance, resulting in high levels of vaccine hesitancy. The study recommends that policymakers and public health officials should prioritize testing and vaccination for job categories with higher risk of exposure to COVID-19. They should provide accurate information about COVID-19 testing and vaccination and implement workplace-based testing and vaccination programs. These interventions can help to increase COVID-19 testing and vaccination uptake among the university community and mitigate the spread of COVID-19.
Keywords:
Acceptance
; COVID-19
; Cross-sectional study
; Federal University of Health Sciences Otukpo
; Vaccine hesitancy
; Nigeria
1. Introduction
The first case of Corona virus (COVID-19) was discovered in Wuhan City, Hubei Province, China, during a respiratory sickness outbreak [1]. Globally, there is growing concern about new viral infections such as Ebola, COVID-19, and Zika, which have no cure at the present but are being researched [2]. The twenty-first century has seen an increase in severe infectious disease outbreaks, the most recent of which was the COVID-19 pandemic, which has had a devastating impact on lives and livelihoods all across the world [3]. Most people infected with the virus experience mild to moderate respiratory symptoms and recover without medical intervention [4]. However, elderly individuals and those with underlying medical conditions like cardiovascular disease, diabetes, chronic respiratory disease, or cancer are more susceptible to severe illness [5]. WHO was notified of the virus on December 31, 2019, and declared it a global health emergency on January 30, 2020. On March 11, 2020, the WHO declared COVID-19 a global pandemic, which was the first since the H1N1 influenza pandemic in 2009 [6].
The global outbreak of COVID-19 was a shocking event that caused most countries’ health systems to be completely overwhelmed. As of June 7, 2020, there are more over seven million instances worldwide, with the United States over 2 million cases, Brazil over 700,000 cases, Russia over 500,000 cases, and South Africa over 54,000 cases, and Egypt over 38,000 cases bearing the brunt [7,8]. Following the WHO declaration, the Corona Virus Preparedness Group was established in Nigeria on January 31. WHO has identified Nigeria as one of the 13 high-risk African countries where COVID-19 transmission is a major concern [8,9]. Additionally, Nigeria’s healthcare system is considered vulnerable due to a shortage of healthcare workers and the lack of healthcare facilities in some parts of the country [8,10,12]. If effective measures are not taken to combat the pandemic, Africa may end up bearing the ultimate burden of the COVID-19 outbreak, according to projections [13]. The pandemic has caused global social disruption by limiting social interactions, which are fundamental to human society. The practice of “social distancing” goes against regular social interaction, which is the foundation of human society [14]. The highly contagious nature of the disease also disrupts the usual norms of close physical contact, as it spreads through contact with infected individuals. COVID-19 has caused a de-globalization of the world in terms of human migration, with airports and social events being affected. On February 27 [15,16], Nigeria acquired its COVID-19 index case from Italy. This raised concerns about the effectiveness of safety at airports, and as a result, the overall preparedness of the country. Despite testing positive for COVID-19, the index case had been to a few additional federated nations. The pre-COVID-19 preparation was woefully insufficient. From a single imported index case, numerous cases and fatalities occurred in many countries, including Nigeria. Since Nigeria’s first index case, COVID -19 incidence has increased quickly, but thanks to the government’s proactive response and public health intervention, the pandemic is now drastically declining in Nigeria [8].
The use of vaccines can stop and contain outbreaks of contagious diseases. They contribute to the protection of global health and will be a vital tool in the battle against antibiotic resistance [17]. Despite the enormous progress, many individuals lack adequate access to immunisations worldwide [18,19]. Progress has stagnated or even reversed in some nations, and there is a serious danger that complacency will undo prior successes [20]. The percentage of children around the world who receive the required immunisations has remained stable over the past few years, according to data on global vaccination coverage [21,22].Many lives are saved each year through the use of vaccines in the prevention of infectious diseases, which has proven to be a success story for global health and development. Creating safe and effective COVID-19 vaccination is critical for resuming normal human social interactions. Hence, getting vaccinated help prevent the risks of contracting COVID-19 disease since the vaccines works with the body immune system to build protection against the disease. Currently, a lot of vaccines such as Astrazeneca, modema, Pfizer, sinovac, and sinophen are available for different age group which are used to prevent life threatening diseases including COVID-19. They are the foundation of global health security and will be a critical tool in the fight against the scourge of global pandemics that endanger human life. WHO mandated that Immunization becomes a key component of primary health care and as well as one of fundamental human right.
The pandemic have had detrimental effects on academic activities leading to school closures, authorities must create a long-term strategy for sustaining educational activities amidst any eventuality because the educational system is crucial to the development of a nation [23]. Although the economies of nations were also damaged, there has been a slow rebound from the pandemic’s devastation. A health-related behaviour called vaccine hesitancy poses obstacles to the successful uptake and distribution of vaccines [24,25,26]. There is unequal distribution of vaccines globally which has to be eliminated and countries must adopt multi-sectorial approach that engages key stakeholders to determine which specific factors are view as compelling arguments for and against vaccination and develop new strategies to influence those who are unsure [27,28]. According to WHO and others, creative methods must be searched out in order to engage groups are at risk, address insensitivity, and advance tactics based on respectful discourse and cultural sensitivity [26].
Country-specific remedies are required because the causes of the low rates of COVID-19 vaccination and resistance to the vaccine vary across Sub-Saharan Africa [29,30]. There has been a plea for compassionate, culturally appropriate public health intervention that acknowledges the role of historical, structural, and other system dynamics. To achieve these goals, nations should base their national corrective action plans on the measures that WHO has recommended for fostering healthy behaviour. Innovation and task shifting away from traditionally relied-upon types of health informatics as well as engagement to increase health literacy and achieve health equity via action are examples of measures of demonstrated value that are pertinent to COVID-19 vaccination uptake [30].
According to studies, there is a low percentage of COVID-19 immunization and resistance in Africa for a variety of regionally specific reasons [31,32]. It is really heartening to see so many vaccinations demonstrating and entering development as stopping the COVID-19 pandemic depends on balanced availability of effective and secure vaccines [19]. While scientists worldwide are working tirelessly to develop, produce, and use safe and effective vaccines. The vaccination distribution success in any country is dependent on vaccine availability and acceptance. When there is a lot of fear and uncertainty as per what might be the outcome of taking the vaccine due to reasons best known to members of the public. This poses threat to combating the deadly disease and may lead to failure of the vaccination program. In order to manage the global COVID-19 pandemic, the COVID-19 vaccination has a higher impact in countries with the highest adoption rates. The main obstacle, nonetheless, is vaccination resistance. In especially in low- and middle-income countries, the WHO had recognised COVID-19 vaccination hesitancy as an international concern [33]. In order to prevent the emergence and spread of new variants that can override immunity provided by vaccines and prior disease, this study aimed to understand the associated factors of COVID-19 vaccine acceptance and hesitancy in the university community in Nigeria.
2. Materials and Methods
2.1. Study setting
The federal university of health sciences in Otukpo, Benue state, Nigeria, which has 450 staff members, 800 students. It is a tertiary entity in charge of undergraduate and graduate education. It is Nigeria’s first government university for the health sciences. It is located at the heart of Otukpo local government area of Benue State with a population density of close to 2 million people, served as the site of this study.
2.2. Study design and period
Between November 2021 and April 2022, community members at Federal University of Health Sciences, Otukpo, Benue State, Nigeria, were polled via a web-based cross-sectional survey to determine the factors that influence COVID-19 vaccination acceptability and hesitancy.
2.3. Inclusion and exclusion criteria
The responses included people who had valid forms of identification and were both employed and students. Exclusion criteria included not employed by the university or not admitted as a student throughout the data collecting period.
2.4. Sample size determination and sampling techniques
Using the sample size formula of [34], a university study’s acceptance rate for the COVID-19 vaccination was found to be 27.7%, with 10% attrition. Using a single population proportion calculation, the sample size (n = 150) was calculated by adding the 62.7% acceptance rate, 50% vaccine hesitancy, 5% margin of error, and at 95% confidence range [35]. The link to the online survey was supplied with data collectors with the intention of the study and a consent form after five faculties/colleges in the university were purposefully chosen. If there were visits while data collection was taking place, only those who fit the inclusion requirements were chosen to avoid information saturation.
2.5. Data collection tool and procedures
Data were gathered using a structured survey that was created using Google Forms platforms after a thorough literature review [29] with the assistance of the designated investigators, respondents were surveyed online. There are a total of 27 items in the questionnaire, which were divided into 4 sections: sociodemographic, general COVID-19 and personal health questions, COVID-19 vaccination-related questions, and attitude and perspective questions about COVID-19 and its vaccine. Using a vaccine conspiracy belief Likert scale [32,36,37], attitude and beliefs were evaluated. With the assistance of the designated data collectors, residents were surveyed online.
2.6. Data quality assurance
The survey’s questionnaire was written in English, which is Nigeria’s official language, to improve public engagement and comprehension. About 15% of the sample size underwent a pre-test. Before the start of data collection, the pre-test called for any necessary adjustments. Data collectors received instructions on using Google Forms platform questionnaires, making questions understandable, and interacting with study participants. To maintain the integrity of the data, regular monitoring, supervision, and reviews of the completed questionnaire were conducted.
2.7. Statistical analysis
The data entry and analysis were performed using IBM SPSS software version 2.0. The descriptive statistics and inferential statistics were used to determine frequencies and percentages of levels of knowledge and awareness of COVI-19 vaccine among subjects with socio-demographic variables. Similarly, chi-square test for independence was used to compare participant’s socio-demographics for potential associated factors with acceptance and hesitation to COVID-19 Vaccination.
3. Results
3.1. Respondents’ Socio-demographic characteristics
Respondents’ thoughts were gathered after the link to the questionnaires was distributed. A response rate of 33.3% (150) was noted. Most (64%, 96/150) respondents were postgraduates, of the respondents Christian faith has majority (80%, 132/150). The proportion of responders for each study population in the institution (academics, non-academics, healthcare professionals, and tertiary students). Of the 150 respondents in all, 96 of whom were men (64%) took part in the study. Students made up 32% (n=48) of the respondents, followed by academics (23.3%) (n=35), then non-academics (23.7%) (n=41) and lastly health professionals with (17.3%) (n=26), in terms of occupations/job descriptions. The majority 120(80.0%) of the respondents were aged 16–45 years (Table 1). The table also shows the association between various socio-demographic factors and test for COVID-19 among the respondents. The study found significant associations (p < 0.05) between testing for COVID-19 infection and some socio-demographic factors. Respondent’s category showed a significant difference in testing for COVID-19, while the other factors showed no significant statistical association (p > 0.05). Similarly, the study found there were significant positive associations between COVID-19 vaccination and job category, and religion with gender and education having moderate effect (as shown in Table 1). Overall, socio-demographic variables were not significant, except for job category and religion (p < 0.05), which showed a significant difference in COVID-19 testing and vaccination. This suggests that job category may play a role in determining COVID-19 testing and vaccination behavior among the university community.
3.2. Knowledge, attitude and practices towards COVID-19 and vaccination
Majority of the respondents 116 (77.3%) have been tested for the virus to know their status. Among the 34 that have not been tested few are willing (45%) to be tested showing high level of hesitancy towards test and vaccination. Only 1.3% of the respondents had tested positive for COVID-19 with most 98.7% confirmed not to have had based on negative test results. Most people (74.7%) have not recently been exposed to a positive case. Figure 1 provides further information as well as information on the respondents’ contact with those who were confirmed to have COVID-19 or to have passed away from the illness, are shown in Figure 1.
2.3. COIVD-19 Vaccine Availability, Accessibility, Acceptance, and Hesitancy
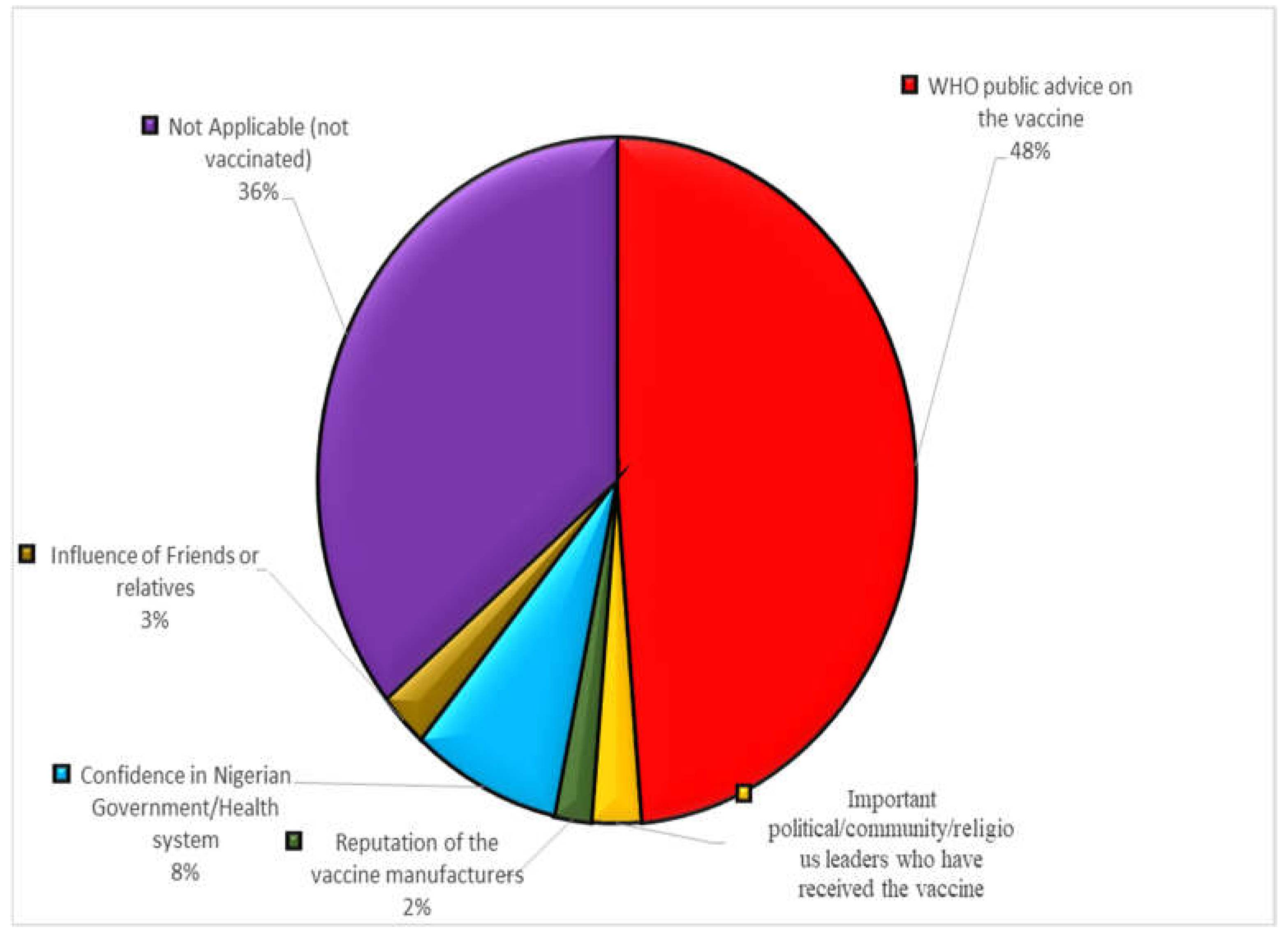
Only (41.6%) of the respondents accepted to take the vaccine mainly because of world health organization public advice on the importance of the vaccine. In total, 58.4% (87.6) of trial participants indicated hesitancy to get the COVID-19 vaccine. On the high side also are the unvaccinated members of the university community (42.7%) followed by others who took because of influence of family members and friends and confidence in Nigerian healthcare system, in contrast few (4.5%) based theirs on reputation of vaccine manufacturers.
Most (72.7%) respondents reported that WHO-approved COVID-19 vaccines were available for use in their locality but only 48.7% of those surveyed were vaccinated (Figure 2). The unvaccinated population is on the high side with 53.1%. Respondents agreed that vaccine is available and they are willing to take.
It was also observed that AstraZeneca/ Oxford vaccine was the most used based on date collect on the type of vaccine respondents who got vaccinated received (Figure 3). Details on vaccine brands received and the proportion of each vaccine are presented in Figure 3.
Majority of the respondents, 37 (41.6%) accepted to take the vaccine mainly because of world health organization public advice on the importance of the vaccine. A few others took because of influence of family members and friends 9%, important political, community and religious leaders 6.7%, similarly 4.5% based theirs on reputation of vaccine manufacturers. The study found that the percentage of unvaccinated people was higher than those who have been vaccinated. Figure 3 below shows 52.5% of the university community members are not vaccinated however 47.5% indicated affirmative to have taken the vaccine. The WHO’s public health recommendation for the vaccine (48%) was the main factor in informing them of COVID-19 vaccine recipients about the efficacy and safety of the vaccine (Figure 2). Further probing reveals that majority 26% and 24% as shown below were not vaccinated because they were having bad feelings towards the vaccine due to conspiracy theories surrounding vaccine as heard from social media and internet sources, also suspicious of the safety concern in hatsful manufacturing of the vaccines.
Figure 5.
Reasons that informed the confidence of COVID-19 vaccinated respondents on the safety and efficacy of the vaccine.
Figure 5.
Reasons that informed the confidence of COVID-19 vaccinated respondents on the safety and efficacy of the vaccine.
3.4. Associated factors of COVID-19 vaccine hesitancy
There was a significant difference (p < 0.05) in testing and vaccination among the different staff category of members of the university community (Academics, Non-academics, Students and Health workers). When given the COVID-19 vaccination, the responders claimed a number of reasons why they did not want to take it. These comprised: Skepticism about the vaccine due to hasty production/roll out 48(32.0%), Bad feelings towards the vaccines due to negative social media reports/rumors 35(23.3%), Influence from anti-COVID-19-vaccine movements 22(14.7%) were found to significant percentage influence on reasons for vaccine hesitancy among respondents.
4. Discussion
In a university community in Otukpo, Benue State, Nigeria, and this study evaluated the COVID-19 vaccine and the socio-demographic factors that influence vaccine acceptance and reluctance. Since it was declared a global pandemic, the COVID-19 pandemic has posed a significant challenge, and numerous preventive measures have been tried to stop it. One of the most effective ways to stop the spread of the COVID-19 epidemic was vaccination. Recent research suggested that 60–70% of society need receive vaccinations in order to limit the COVID-19 pandemic’s spread and build herd immunity [33]. A total of 150 questionnaires were distributed using a web-based cross-sectional survey to academics, non-academics, students, and health professionals who served as the research’s data sources. To encourage COVID-19 immunization, it is important to understand whether people are willing to receive the vaccine, why they are or are not, and which sources of information they trust the most. Our study used a standard set of survey questions to analyse the acceptance of the COVID-19 vaccine and its determinants in higher education setting. According to our findings, survey respondents gave the vaccine acceptance a low to moderate rating. Among the 150 respondents, 132(88%) agreed that the disease is real as such a global public health threat. Only 47.5% of those who said they knew where to get the COVID-19 vaccine have actually received it showing high hesitancy towards the vaccine uptake. Our study’s acceptance rate was comparable to Njoga’s stated figure [35,38]. Misconceptions about the vaccine are a predictor of low levels of testing and immunisation among the responders, as does fear engendered by societal conspiracy theories concerning COVID-19 infection. Being immunised or having a favourable attitude towards the vaccine can help forecast who will accept the vaccine the most. We found that participants were hesitant or unwilling to get a COVID-19 vaccine when available, suggesting that increasing public awareness through the use of individuals with prior disease experience may enhance vaccination uptake.
According to COVID-19 information hosted on the website of the World Health Organisation, Nigeria had just nine and three completely vaccinated individuals per 100 inhabitants, respectively [39]. In comparison to the 52 people who make up the global average, this number of fully immunised individuals per 100 people is incredibly low [39]. Since the respondents are predominantly highly educated individuals and in university community, one would have expected high level of awareness translates into high level of vaccine acceptance and vaccine uptake but different pattern was observed as the level of awareness about COVID-19 was high but does not translate into high testing rate and vaccination rate. However, we found out that a lot of determinants such as fear from the unknown, social media conspiracy contribute to low vaccination. Few responders have had their COVID-19 status tested, therefore they are probably hesitant to get the vaccine. People who find a disease terrifying are more likely to request a vaccine against it, according to earlier research [40].
Nigerians were receiving COVID-19 vaccines in response to the continuing pandemic [41]. On March 5, 2021, vaccinations started. 17,914,944 individuals had gotten their first dose of the COVID-19 vaccination as of February 28, 2022 [1]. By the end of April, 14.9 million people had received all three vaccine doses, totaling 38.4 million [16].The most common vaccine taken was AstraZeneca/ oxford 42.2%, followed by moderna 6%, with minute number of respondents taken Johnson and Johnson, Pfizer/ biotech, sinovac, sinopharm and 41% of unvaccinated people. The study reveals that, of the 150 respondents, 88% agreed that the disease is a genuine global public health concern. Only 47.5% of those who said they knew where to get the COVID-19 vaccine have actually received it. The respondent category, religion, age and level of education were strongly associated with COVID-19 vaccine acceptance and hesitancy. Furthermore, this study’s hesitation rate is consistent with [42,43] findings of moderately high hesitancy amongst nations, making it difficult to get the necessary vaccinations (60–70%) to halt the COVID-19 pandemic’s spread. The perception spread by social media that the COVID-19 virus was created by humans may be to blame for the poor level of vaccination uptake. This conspiracy theory has permeated people’s perspectives on the COVID-19 outbreak all around the world. People hold false beliefs about the history of vaccines as well as their potential safety and effectiveness. This study can be used by the government and those in the education industry to provide targeted training and interventions to increase vaccine uptake and, as a result, compliance with national guidelines. Vaccine hesitancy is a complex global public health issue that differs across cultures, time, location, and vaccine type [44]. Nonetheless, it is influenced by factors such as complacency, convenience, and over confidence [43]. Skepticism about the vaccine due to fear of unknown conspiracy theories, negative feelings toward vaccines due to negative social media reports/rumors, and the influence of anti-COVID-19 vaccine movements all had a significant impact on vaccine acceptance in this study.
5. Conclusion
Based on the study’s findings, it can be concluded that socio-demographic factors such as job category, religion, gender, and education may influence COVID-19 testing and vaccination behavior among the university community. Respondent’s category also showed a significant difference in COVID-19 testing behavior. To increase COVID-19 testing and vaccination uptake among the university community, the study recommends the implementation of targeted interventions that take into account socio-demographic factors. This could involve increasing awareness through targeted messaging and communication strategies, providing incentives for testing and vaccination, and addressing concerns and misconceptions about COVID-19 testing and vaccination. Additionally, the study recommends that policymakers and public health officials work closely with employers to ensure that job categories with higher risk of exposure to COVID-19 are prioritized for testing and vaccination. This could involve providing workplace-based testing and vaccination programs, as well as ensuring that employees have access to accurate information about COVID-19 testing and vaccination. Overall, these interventions could help to increase COVID-19 testing and vaccination uptake among the university community, and ultimately help to mitigate the spread of COVID-19.
Author Contributions
Conceptualization, SZ; methodology, SZ, HZ, and COO; software, JEI, ADN and AOE; validation, SBI, AOI, and EAO; formal analysis, JEI, and ESA ; investigation, BCA, and AOE; resources, ESC, and SBI; data curation, BCA; writing—original draft preparation, SZ; writing—review and editing, SZ, ADN, JAO; visualization, COO, and HZ; supervision, JAO; project administration, JAO and AOI. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The Oviedo Convention and the Helsinki Declaration were followed during the study’s execution, and the institutional Health Research Ethics Committee (HREC) waived the requirement for ethical approval because it posed little risk (Waiver No. UHS/A021/43). Before taking part in the trial, each subject gave verbal informed consent. The questionnaire was made voluntary, and it was written in a way that respects participants’ identity and confidentiality. The study participants were notified that the information they gave would be handled with absolute confidentiality.
Informed Consent Statement
Informed consent was obtained from all participants involved in the study.
Acknowledgments
We would like to convey our gratitude for the diligent efforts of all the Federal University of Health Sciences Otukpo staff members, who took the time to complete the survey questionnaire and helped with its distribution during the course of this study. We appreciate Associate Professor Clarence Yah’s technical assistance in the development of the study report from Wits University in South Africa.
Conflicts of Interest
Authors declare that no conflict of interest exist.
References
- CDC. Basics of COVID-19. Center for disease control and prevention. 2021 [cited 2021 Jan 12]. Available from: https://www.cdc.gov/coronavirus/2019-ncov/your-health/about-covid-19/basics-covid-19.html.
- Gbore DJ, Zakari S, Yusuf L. In silico studies of bioactive compounds from Alpinia officinarum as inhibitors of Zika virus protease. Informatics in Medicine Unlocked. 2023;38:101214. [CrossRef]
- Baker RE, Mahmud AS, Miller IF, Rajeev M, Rasambainarivo F, Rice BL, et al. Infectious disease in an era of global change. Nat Rev Microbiol. 2022;20(4):193–205. [CrossRef]
- Hanna P, Issa A, Noujeim Z, Hleyhel M, Saleh N. Assessment of COVID-19 vaccines acceptance in the Lebanese population: a national cross-sectional study. J of Pharm Policy and Pract. 2022;15(1):5. [CrossRef]
- WHO. Coronavirus disease (COVID-19) [Internet]. Coronavirus disease (COVID-19) pandemic. 2021 [cited 2021 Jan 12]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019?adgroupsurvey={adgroupsurvey}&gclid=CjwKCAjw6IiiBhAOEiwALNqncQzxt9lOFSQ_yUNnYCf4XFPxqiTsXkz3Bej34UV0IVUbEKUKmvMrzxoCznoQAvD_BwE.
- WHO. Coronavirus disease (COVID-19) [Internet]. World Health Orgaanization. 2023 [cited 2023 Apr 21]. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/coronavirus-disease-covid-19.
- Fehintola JO. Challenges and Coping Strategies for Covid-19 among the Civil Populace in Southwest, Nigeria. 2021;20(1):1–13.
- Amzat J, Aminu K, Kolo VI, Akinyele AA, Ogundairo JA, Danjibo MC. Coronavirus outbreak in Nigeria: Burden and socio-medical response during the first 100 days. International Journal of Infectious Diseases. 2020 Sep;98:218–24.
- Dan-Nwafor C, Ochu CL, Elimian K, Oladejo J, Ilori E, Umeokonkwo C, et al. Nigeria’s public health response to the COVID-19 pandemic: January to 20. Journal of Global Health. 2020;10(2):020399. [CrossRef]
- WHO. Chronic staff shortfalls stifle Africa’s health systems: WHO study [Internet]. WHO Africa. 2022 [cited 2023 Apr 21]. Available from: https://www.afro.who.int/news/chronic-staff-shortfalls-stifle-africas-health-systems-who-study.
- Azevedo MJ. The State of Health System(s) in Africa: Challenges and Opportunities. In: Historical Perspectives on the State of Health and Health Systems in Africa, Volume II [Internet]. Cham: Springer International Publishing; 2017 [cited 2023 Apr 21]. p. 1–73. Available from: http://link.springer.com/10.1007/978-3-319-32564-4_1.
- Ong SWX, Young BE, Lye DC. Lack of detail in population-level data impedes analysis of SARS-CoV-2 variants of concern and clinical outcomes. The Lancet Infectious Diseases. 2021;21(9):1195–7.
- Priya Joi. Why Africa’s critically ill COVID-19 patients have the world’s highest death rates [Internet]. VaccinesWork. 2021 [cited 2023 Apr 21]. Available from: https://www.gavi.org/vaccineswork/why-africas-critically-ill-covid-19-patients-have-worlds-highest-death-rates?gclid=CjwKCAjw6IiiBhAOEiwALNqncZ5X-8YAR9gB5U_TH9rk8UOkEGkC1zkPfY7U-JqQnDu0-OXHKKJXShoC2TUQAvD_BwE.
- Adinde K, Emmanuel N, Onyebuchi AA, Ogbonna F. Developing the Rural Poor: A Trajectory to Curbing the Spread of COVID-19 Pandemic in Nigeria. 2021;6(3):507.
- Akor O. COVID-19: Two Years After Nigeria’s Index Case [Internet]. dailytrust. 2022 [cited 2023 Apr 21]. Available from: https://dailytrust.com/covid-19-two-years-after-nigerias-index-case/.
- Olu-Abiodun O, Abiodun O, Okafor N. COVID-19 vaccination in Nigeria: A rapid review of vaccine acceptance rate and the associated factors. Elelu N, editor. PLoS ONE. 2022;17(5):e0267691.
- Alghamdi S. The role of vaccines in combating antimicrobial resistance (AMR) bacteria. Saudi Journal of Biological Sciences. 2021;28(12):7505–10. [CrossRef]
- Yarlagadda H, Patel MA, Gupta V, Bansal T, Upadhyay S, Shaheen N, et al. COVID-19 Vaccine Challenges in Developing and Developed Countries. Cureus [Internet]. 2022 Apr 8 [cited 2023 Apr 21]; Available from: https://www.cureus.com/articles/92762-covid-19-vaccine-challenges-in-developing-and-developed-countries.
- Forman R, Shah S, Jeurissen P, Jit M, Mossialos E. COVID-19 vaccine challenges: What have we learned so far and what remains to be done? Health Policy. 2021;125(5):553–67.
- Teng YM, Wu KS, Wang WC, Xu D. Assessing the Knowledge, Attitudes and Practices of COVID-19 among Quarantine Hotel Workers in China. Healthcare. 2021;9(6):772. [CrossRef]
- Rachlin A, Holliday CD, Murphy P, Sodha S, Wallace A. Routine Vaccination Coverage — Worldwide, 2021 [Internet]. Center for disease control and prevention. 2022 [cited 2023 Apr 21]. Available from: https://www.cdc.gov/mmwr/volumes/71/wr/mm7144a2.htm.
- Guglielmi G. Pandemic drives largest drop in childhood vaccinations in 30 years. Nature. 2022;608(7922):253–253. [CrossRef]
- Choube D, Dr. Mamta Bansal, Narang M. Covid 19 Pandemic Impact on Social Relations. 2022 Feb 15 [cited 2023 Apr 21]; Available from: https://zenodo.org/record/6085976.
- Babatope T, Ilyenkova V, Marais D. COVID-19 vaccine hesitancy: a systematic review of barriers to the uptake of COVID-19 vaccine among adults in Nigeria. Bull Natl Res Cent. 2023;47(1):45. [CrossRef]
- Saied SM, Saied EM, Kabbash IA, Abdo SAE. Vaccine hesitancy: Beliefs and barriers associated with COVID-19 vaccination among Egyptian medical students. Journal of Medical Virology. 2021;93(7):4280–91. [CrossRef]
- Heneka MT, Golenbock D, Latz E, Morgan D, Brown R. Immediate and long-term consequences of COVID-19 infections for the development of neurological disease. Alz Res Therapy. 2020;12(1):69. [CrossRef]
- Chukwuocha UM, Emerole CO, Iwuoha GN, Dozie UW, Njoku PU, Akanazu CO, et al. Stakeholders’ hopes and concerns about the COVID-19 vaccines in Southeastern Nigeria: a qualitative study. BMC Public Health. 2022(1):330. [CrossRef]
- Wouters OJ, Shadlen KC, Salcher-Konrad M, Pollard AJ, Larson HJ, Teerawattananon Y, et al. Challenges in ensuring global access to COVID-19 vaccines: production, affordability, allocation, and deployment. The Lancet. 2021;397(10278):1023–34. [CrossRef]
- Gudayu TW, Mengistie HT. COVID-19 vaccine acceptance in sub-Saharan African countries: A systematic review and meta-analysis. Heliyon. 2023;9(2):e13037. [CrossRef]
- Ajeigbe O, Arage G, Besong M, Chacha W, Desai R, Doegah P, et al. Culturally relevant COVID-19 vaccine acceptance strategies in sub-Saharan Africa. The Lancet Global Health. 2022;10(8):e1090–1. [CrossRef]
- Miner CA, Timothy CG, Percy K, Mashige, Osuagwu UL, Envuladu EA, et al. Acceptance of COVID-19 vaccine among sub-Saharan Africans (SSA): a comparative study of residents and diasporan dwellers. BMC Public Health. 2023;23(1):191. [CrossRef]
- Ekowo OE, Manafa C, Isielu RC, Okoli CM, Chikodi I, Onwuasoanya AF, et al. A cross sectional regional study looking at the factors responsible for the low COVID-19 vaccination rate in Nigeria. Pan Afr Med J [Internet]. 2022 [cited 2023 Apr 21];41. Available from: https://www.panafrican-med-journal.com/content/article/41/114/full. [CrossRef]
- Tadesse TA, Antheneh A, Teklu A, Teshome A, Alemayehu B, Belayneh A, et al. COVID-19 Vaccine Hesitancy and its Reasons in Addis Ababa, Ethiopia: A Cross-Sectional Study. Ethiop J Health Sci. 2022;32(6):1061–70. [CrossRef]
- Uzochukwu IC, Eleje GU, Nwankwo CH, Chukwuma GO, Uzuke CA, Uzochukwu CE, et al. COVID-19 vaccine hesitancy among staff and students in a Nigerian tertiary educational institution. Therapeutic Advances in Infection. 2021:204993612110549. [CrossRef]
- Okai GA, Abekah-Nkrumah G. The level and determinants of COVID-19 vaccine acceptance in Ghana. Mossong J, editor. PLoS ONE. 2022;17(7):e0270768. [CrossRef]
- Katoto PDMC, Parker S, Coulson N, Pillay N, Cooper S, Jaca A, et al. Predictors of COVID-19 Vaccine Hesitancy in South African Local Communities: The VaxScenes Study. Vaccines. 2022;10(3):353. [CrossRef]
- Engelbrecht M, Heunis C, Kigozi G. COVID-19 Vaccine Hesitancy in South Africa: Lessons for Future Pandemics. IJERPH. 2022;19(11):6694. [CrossRef]
- Njoga EO, Mshelbwala PP, Abah KO, Awoyomi OJ, Wangdi K, Pewan SB, et al. COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria. Vaccines. 2022;10(4):626. [CrossRef]
- WHO. Statement of the Independent Allocation of Vaccines Group (IAVG) of COVAX [Internet]. https://www.who.int/news/item/23-12-2021-achieving-70-covid-19-immunization-coverage-by-mid-2022. 2022 [cited 2023 Apr 21]. Available from: https://www.who.int/news/item/23-12-2021-achieving-70-covid-19-immunization-coverage-by-mid-2022.
- Karlsson LC, Soveri A, Lewandowsky S, Karlsson L, Karlsson H, Nolvi S, et al. Fearing the disease or the vaccine: The case of COVID-19. Personality and Individual Differences. 2021;172:110590. [CrossRef]
- Njoga EO, Mshelbwala PP, Abah KO, Awoyomi OJ, Wangdi K, Pewan SB, et al. COVID-19 Vaccine Hesitancy and Determinants of Acceptance among Healthcare Workers, Academics and Tertiary Students in Nigeria. Vaccines. 2022;10(4):626. [CrossRef]
- Sallam M, Dababseh D, Eid H, Al-Mahzoum K, Al-Haidar A, Taim D, et al. High Rates of COVID-19 Vaccine Hesitancy and Its Association with Conspiracy Beliefs: A Study in Jordan and Kuwait among Other Arab Countries. Vaccines. 2021;9(1):42. [CrossRef]
- Sallam M. COVID-19 Vaccine Hesitancy Worldwide: A Concise Systematic Review of Vaccine Acceptance Rates. Vaccines. 2021;9(2):160. [CrossRef]
- MacDonald NE. Vaccine hesitancy: Definition, scope and determinants. Vaccine. 2015;33(34):4161–4.
Figure 1.
COVID-19 testing and infection status of respondents (n = 150).
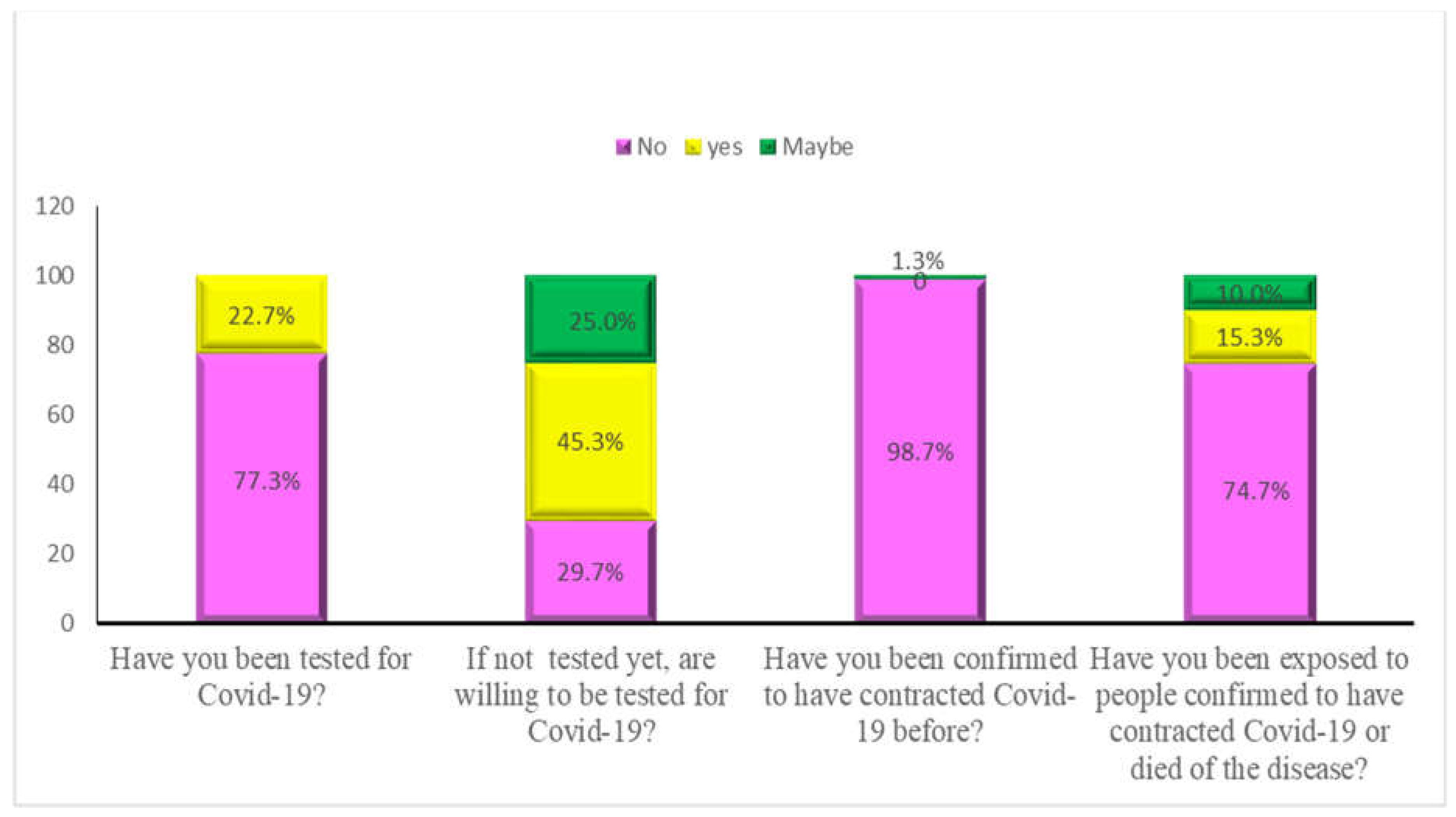
Figure 2.
Reasons for accepting to receive COVID-19 vaccine.
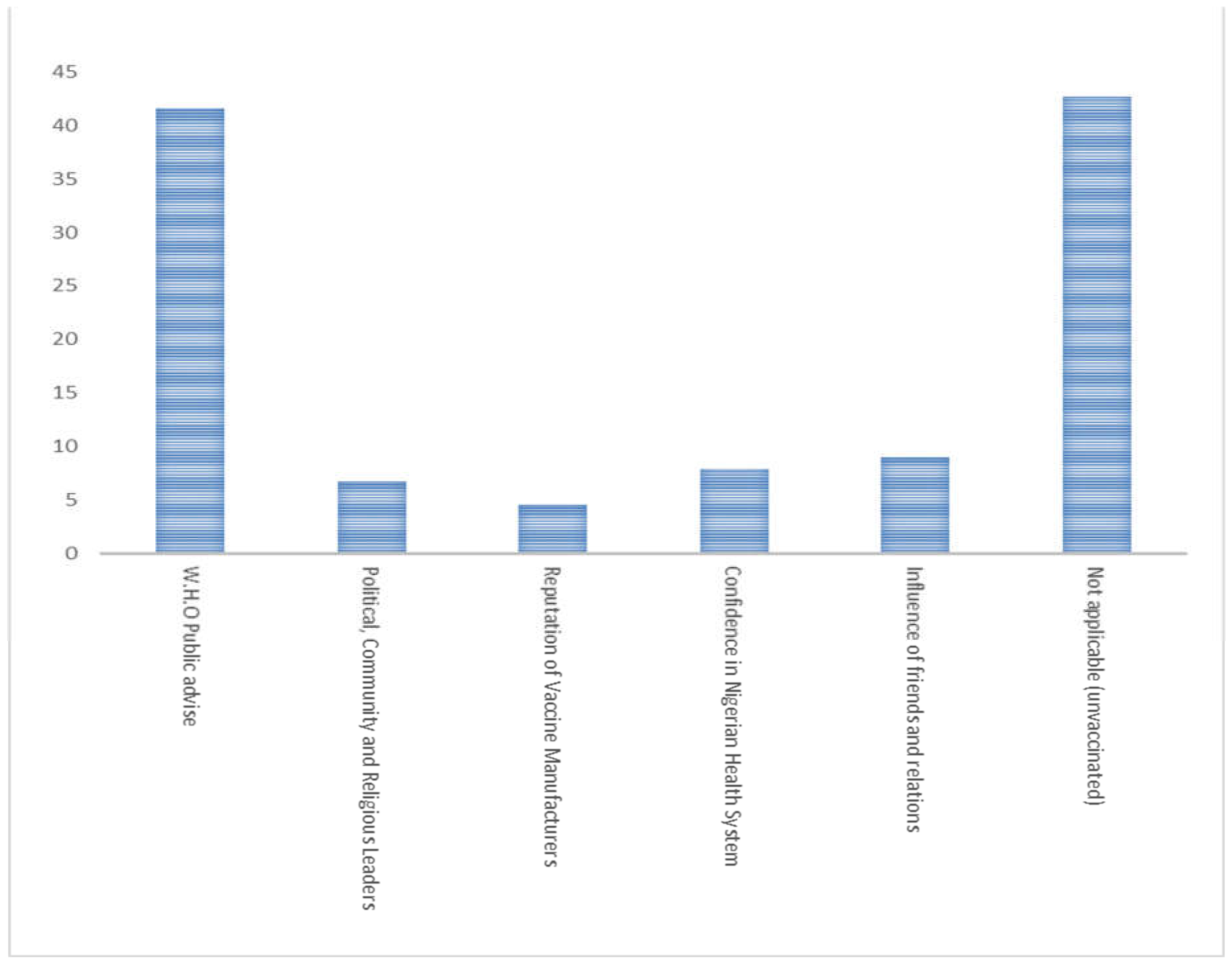
Figure 3.
COVID-19 vaccine availability, accessibility, and acceptance.
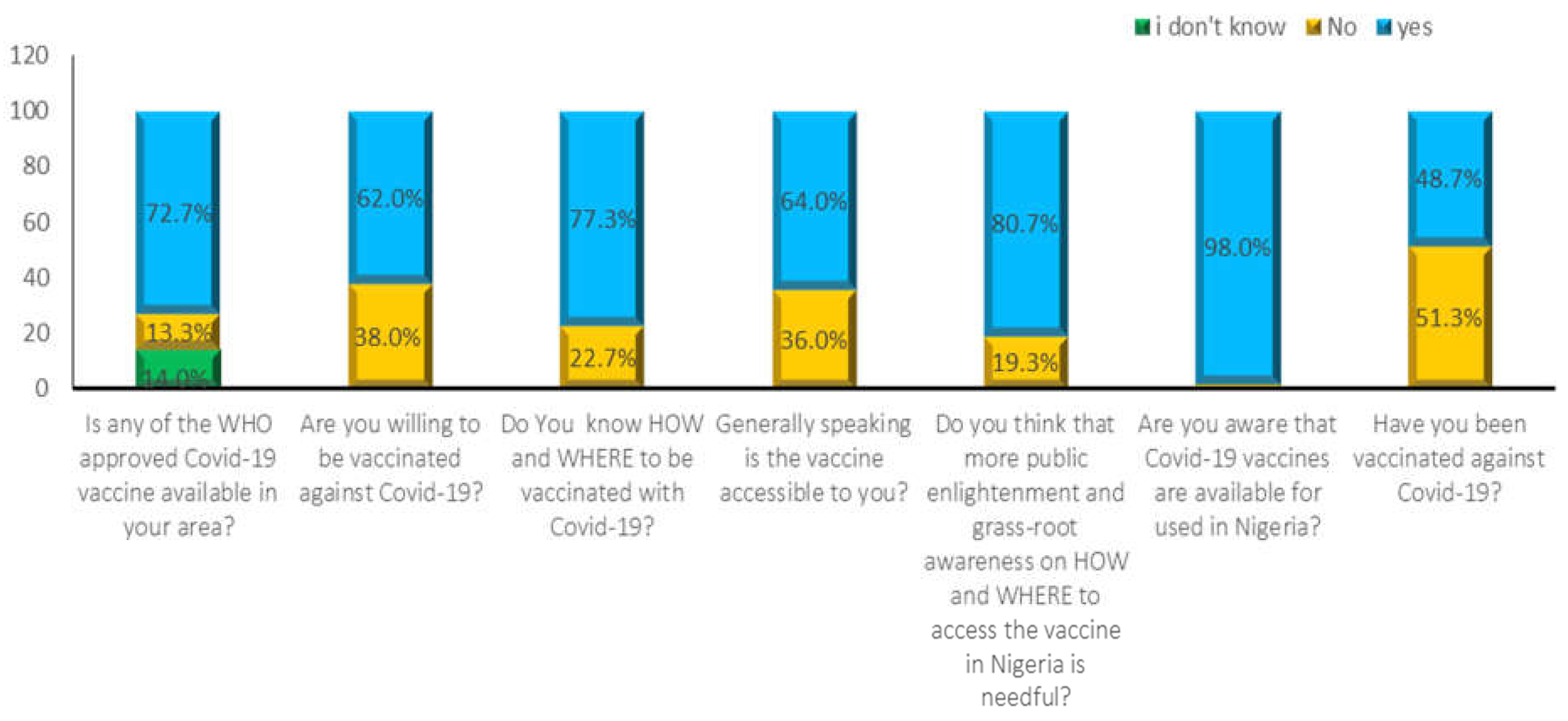
Figure 4.
Distribution of COVID-19 vaccine brands received by vaccinated respondents.
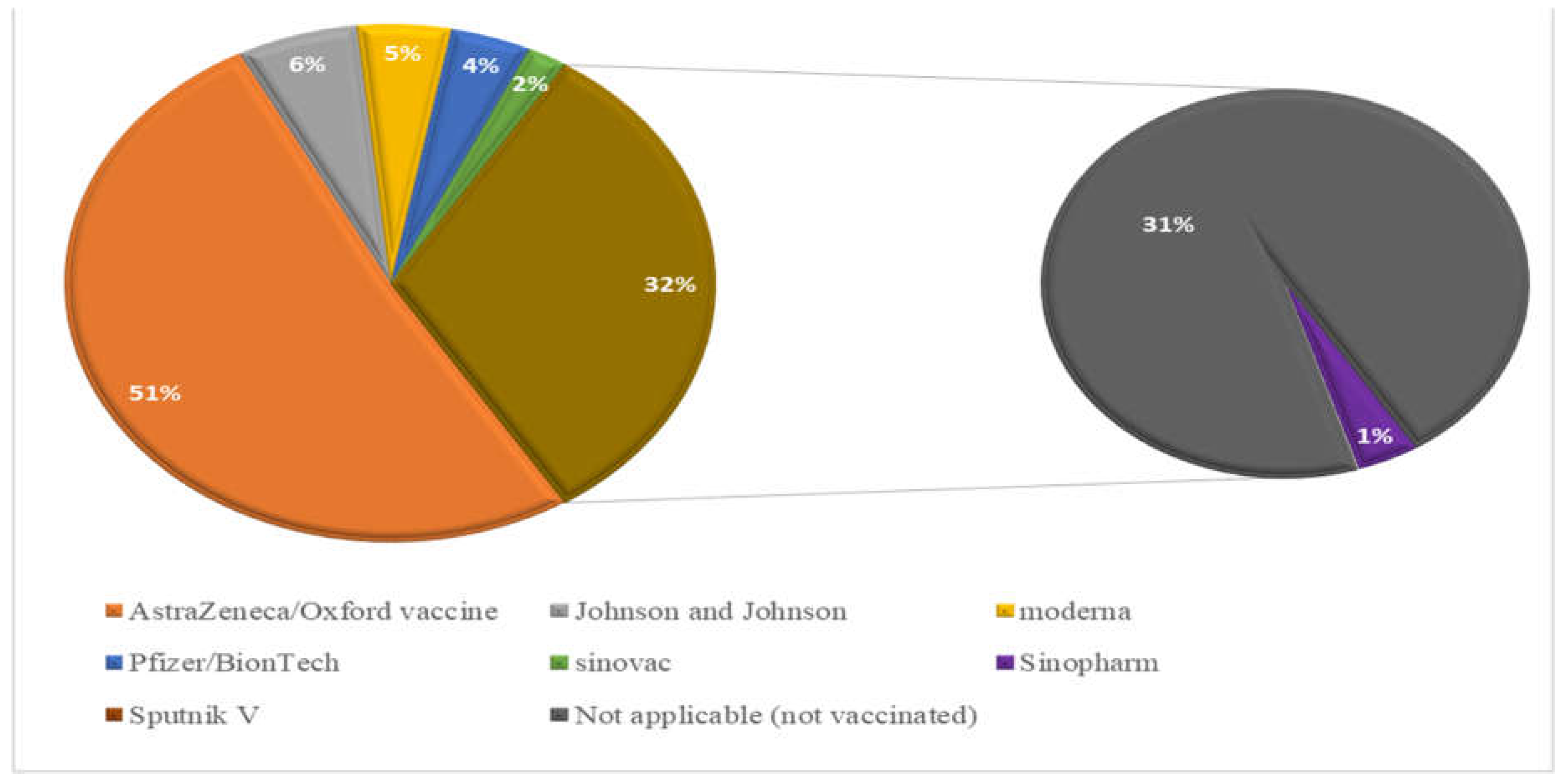

Table 1.
Association between socio-demographic characteristics of the respondents.
| Test Variable | Percentage (% | X2-Value | P-Value |
|---|---|---|---|
| Test and Vaccination against COVID-19 | |||
|
Gender Male Female |
64 36 |
2.968 0.602 |
0.085 0.438 |
|
Marital Status Married Single Divorced |
42.7 56.7 0 |
0.060 2.189 |
0.741 0.335 |
|
Age 16-30 31-45 46-60 |
|||
| 30.7 60.0 |
1.766 0.579 |
0.414 0.748 |
|
| 9.3 | |||
|
Respondent’s category Academic Non-academic Student Health workers |
32.2 17.3 27.3 |
8.365 2.860 |
0.039 0.000 |
| 23.3 | |||
|
Education Secondary ND/NCE Graduate Postgraduate |
|||
| 5.3 | 1.635 | 0.651 | |
| 8.0 22.7 |
7.048 |
0.070 |
|
| 64.0 | |||
|
Religion Christians Muslims Others |
88.0 |
0.777 |
0.678 |
| 10.7 1.3 |
9.241 |
0.010 |
Table 2.
Reasons for COVID-19 vaccine hesitancy and measures to improve the vaccine availability and acceptance.
Table 2.
Reasons for COVID-19 vaccine hesitancy and measures to improve the vaccine availability and acceptance.
| S/No Questions Asked or Information Required Number of Respondents (%) |
|---|
| Reasons for non-vaccination among unvaccinated respondents (n = 150) |
| COVID-19 vaccine registration protocol is difficult 6(4.0) |
| Suspicion/doubts on safety of novel vaccines 19(12.7) |
| Herbal medicines/home remedies are effective for 2(1.3) |
| cure/ management of COVID-19 |
| COVID-19 is a hoax 5(3.3) |
| The vaccines are not available/accessible in my locality 6(4.0) |
| Influence from anti-COVID-19-vaccine movements 22(14.7) |
| Vaccination is against my religious beliefs or personal ideology 0(0) |
| Concerns about long term health/side effects 4(2.7) |
| Skepticism about the vaccine due to hasty production/roll out 48(32.0) |
| Preventive measures are enough to protect against COVID-19 3(2.0) |
| Bad feeling due to negative social media reports/rumors 35(23.3) |
| 2. Some health concerns that prevented respondents from getting vaccinated |
| Allergic reaction 37(24.7) |
| Blood clot issues among women 2(1.3) |
| New or worsening muscle/joint pains 0(0) |
| Innate immunity problems/misconceptions 16(10.7) |
| *Not applicable 95(63.3) |
*Those without health challenges
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



