
Submitted:
02 May 2023
Posted:
03 May 2023
You are already at the latest version
Abstract
Background: The prevalence of physical inactivity has been rising in many countries in recent years, adding to the burden of non-communicable diseases and affecting overall health worldwide. The aim of this study is to determine the impact of physical activity on mortality from ischemic heart disease (IHD) separately for those respondents who were diagnosed with IHD and for those who were not diagnosed with IHD in their baseline health survey. Methods: In the baseline survey (2006–2008), 7100 men and women ages 45–72 were examined within the framework of the international study Health, Alcohol, and Psychosocial Factors in Eastern Europe (HAPIEE). 6770 participants were available for statistical analysis (after excluding 330 respondents due to missing information on study variables). Physical activity was determined by leisure-time physical activities (hours/week). All participants in the baseline survey were followed up for IHD mortality events until December 31, 2018. Results: Using multivariate Cox regression analysis, it was found that moderate and higher levels of physical activity significantly reduced the risk of IHD mortality (HR=0.54 and HR=0.60 respectively) in men who were not diagnosed with IHD at baseline compared with physically inactive subjects. It was found that among men and women who were diagnosed with IHD at baseline, physical activity reduced the risk of mortality from IHD compared with those who were physically inactive (HR=0.54 and HR=0.41 respectively). Using mediation analysis, was found that physical activity directly predicted statistically lower IHD mortality (P<0.05) in men and women. Conclusion: Physical activity was a significant factor that directly predicted statistically lower IHD mortality, regardless of whether subjects had IHD at baseline or not.
Keywords:
physical activity
; mortality risk
; ischaemic heart disease
; longitudinal cohort study
1. Introduction
Despite earlier diagnosis and treatment of cardiovascular diseases (CVD), Lithuania has for many years had the highest mortality rate from CVDs among all causes of death. According to the data of the Center for Health Information of the Institute of Hygiene (Lithuania), in 2020, more than half of all deaths, i.e., 52.7%, were due to diseases of the circulatory system [1]. Thus, CVDs are a prevalent problem not only in Lithuania, where they rank first among all deaths, but also in Europe and worldwide. In the member countries of the European Society of Cardiology, an estimated 12.7 million new cases of CVD were diagnosed in 2019, and 113 million people have been diagnosed with CVD [2]. CVDs are also the most common cause of death in the 57 member countries of the European Society of Cardiology, with ischaemic heart disease (IHD) accounting for 45.0% of deaths in women and 39.0% of deaths in men [2].
Insufficient physical activity is one of the main risk factors for mortality worldwide. The prevalence of physical inactivity has been rising in many countries in recent years, adding to the burden of non-communicable diseases and affecting overall health worldwide [3,4]. Globally, 1 in 4 adults does not meet the recommended level of physical activity, and up to 5 million deaths per year could be prevented if the world's population were more active [3]. People who are insufficiently active have about 30.0% increased risk of death in comparison with people who are sufficiently active [3]. World Health Organization (WHO) guidelines demonstrate that compared to less active adult men and women, individuals who are more active have lower rates of all-cause mortality, coronary heart disease, stroke morbidity, high blood pressure, and metabolic syndrome [5].
The aim of this study is to determine the impact of physical activity on mortality from IHD separately for those respondents who were diagnosed with IHD and for those who were not diagnosed with IHD in their baseline health survey in the context of other risk factors.
2. Materials and Methods
2.1. Study Design and Population
Health, Alcohol, and Psychosocial Factors in Eastern Europe (HAPIEE) study, a population-based urban cohort study conducted in Kaunas (Lithuania) [6]. Baseline data collection was carried out between 2006 and 2008. A sample of 7100 Kaunas men and women aged 45–72 years, stratified by sex and 5-year age groups, was randomly selected from the Kaunas population register. The response rate was 64.8%. The data from 6,770 respondents (3065 men and 3705 women) were used for the statistical analysis. The study protocol was approved by the Kaunas Regional Biomedical Research Ethics Committee (11 January 2005, Protocol No. 05/09). All participants signed an informed consent form.
2.2. Sociodemographic, Lifestyle Factors, and Psychological Well-Being
Sociodemographic factors were determined at the baseline survey using a standard questionnaire (age and education) [6]. Age was used as a continuous variable. Education was categorized into groups: 1. secondary education and lower; 2. college and higher education.
Lifestyle factors such as physical activity, nutrition, and smoking habits were evaluated using a standard questionnaire [6]. In order to assess the physical activity of the participants in their leisure time, 5 questions were asked. Physical activity was determined by the mean length of time spent per week during leisure time in autumn-winter and spring-summer seasons for walking, moderate and hard work, such as gardening, maintenance of the house, and other physical activities, such as engaging in sports, games, or hiking. Responses were based on the subjective opinions of the subjects. The calculation of physical activity hours per week showed statistically significant differences in means between men and women, so further analysis was calculated separately for men and women. Physical activity (hours/week) was ranked from minimum to maximum, dividing the respondents into three levels: inactive (tertile 1), moderately physically active (tertile 2), and higher physically active (tertile 3). Physical activity levels in the population aged 45–72 years are presented in Table 1.
Food frequency questionnaires (FFQs) were used to assess dietary habits. Subjects were asked about the frequency of consumption of 20 food groups (fresh or cooked vegetables, fruit, potatoes, cereals, meat, fish, dairy products, eggs, sweets, etc.). Subjects could choose one of six possible answer options: "rarely and never", "2–3 times a month", "once a week", "2–3 times a week", "4–6 times a week" or "daily". Factor analysis was used to reduce the number of foods reported by the responders. Data on explanatory factor analysis were presented in our previous publication [7]. Factor analysis of the main dietary patterns revealed five-factor nutrition habits: consumption of fresh vegetables and fruit, consumption of sweets, consumption of porridge and cereals, consumption of meat, potatoes, and eggs, and consumption of chicken and fish. A dichotomous-dependent variable was constructed by dividing factor scores into two groups (1: more frequent than average consumption of a particular food group, 0: less frequent than average consumption).
Smoking status was classified as never smoking, former smoking, and current smoking. Current smokers were individuals who regularly smoked at least 1 cigarette per day.
Psychological well-being was assessed by a Control, Autonomy Self-realization, and Pleasure (CASP12) questionnaire [8]. For this measurement, participants were presented with a list of 12 statements that described their lives or how they felt. Their answers on a 4-point scale ranged from "never" to "often", resulting in scores ranging from 12 to 48. The internal consistency of the CASP-12 scale was good (Cronbach’s alpha = 0.74). The psychological well-being scores of participants were classified into the category of a higher psychological well-being group if the scores were equal to or higher than the median (baseline survey: >40 in men and >38 in women). Participants with psychological well-being scores lower than the median were classified into the group with lower psychological well-being.
2.3. Objective Measurements
At the baseline survey, objective measurements (blood pressure, waist circumference), and biochemical analyses (high-density lipoprotein (HDL) cholesterol, fasting glucose, and triglycerides) were determined. Blood pressure (BP) was measured three times with an oscillometric device (Omron M5-1) after at least 5 minutes of rest in a seated position, and the mean values of systolic blood pressure (BP) and diastolic BP were taken. Fasting blood serum samples were analysed at the WHO Regional Lipid Reference Center, Institute of Clinical and Experimental Medicine, Prague (Czech Republic). Lipid concentrations (triglycerides and high-density lipoprotein (HDL) cholesterol) in serum were measured on a Roche COBAS MIRA auto-analyser, using a conventional enzymatic method with reagents from Boehringer-Mannheim Diagnostics and Hoffmann-La Roche. The WHO Regional Lipid Reference Center was responsible for the quality control of biochemistry measures. The concentration of glucose in capillary blood was determined by an individual glucometer, “Glucotrend” [9].
Metabolic syndrome was diagnosed according to the National Cholesterol Education Program Adult Treatment Panel III (NCEP–ATP III) criteria [10]. Individuals with three or more of the five components were diagnosed with metabolic syndrome: 1) elevated arterial blood pressure (≥130/85 mmHg); 2) central obesity (waist circumference ≥102 cm for men, ≥88 cm for women); 3) impaired glucose regulation (fasting blood glucose ≥6.1 mmol/l); 4) elevated triglyceride levels (≥1.7 mmol/L); 5) low high-density lipoprotein (HDL) cholesterol concentration (<1.04 mmol/L in men, <1.3 mmol/L in women).
The epidemiological criteria for the identification of IHD at the baseline survey were, by priority: 1) exposure to myocardial infarction and/or ischaemic changes on the electrocardiogram (ECG), as assessed by Minnesota codes 1–1, 1–2, verified by information in medical documents (medical records, outpatient charts, etc.) [11]; 2) exertional angina pectoris identified using the G. Rose questionnaire [12]; 3) ischaemic ECG changes assessed using the following Minnesota codes: 1–3, 4–1, 4–2, 4–3, 5–1, 5–2, 5–3, 6–1, 6–2, 7–1, 8–3. Causes of death from IHD were coded according to the International Classification of Diseases (ICD)-10 codes (I20-I25).
The mortality from IHD among the study participants was monitored from the start of the primary health survey (2006) until December 31, 2018. The mean duration of follow-up and standard deviation were 10.55±2.59 years.
2.4. Statistical Analysis
All data were analysed using IBM SPSS (IBM Corp. Released 2020. IBM SPSS Statistics for Windows, Version 27.0. Armonk, NY: IBM Corp) software package. All analyses were performed separately for men and women. Descriptive statistics were used for data analysis: means, standard deviations, min., max. meanings. The distributions of variables were compared in sex groups at the baseline survey using chi-square and z-tests. Mean differences were tested using a t-test. P<0.05 values were considered statistically significant. The association between physical activity levels and mortality from IHD was investigated using multivariate Cox regression analysis and mediation analysis. Using Cox regression analysis hazard ratios (HR) were calculated with a 95% confidence interval (CI), and the model was adjusted for age, education, metabolic syndrome, smoking, assessment of psychological well-being, and dietary habits. A mediation analysis was performed using the PROCESS macro for the SPSS (SPSS, Chicago, IL, USA) statistical package (mediation analysis was performed using model 4) [13]. Process plugin allows you to assess several mediators (metabolic syndrome, smoking, and psychological well-being) in parallel at the same time and calculate the cumulative (sum) effect of mediators.
3. Results
The characteristics of men and women at the baseline survey of the Kaunas HAPIEE study (2006-2008) are presented in Table 2. Women were higher educated, and they were more likely to have higher PWB compared with men. However, the rate of metabolic syndrome and its components, such as increased waist circumference and low HDL cholesterol levels, were more prevalent in women compared with men. The rate of arterial hypertension and increased triglyceride levels were more prevalent in men compared with women; also, men were more often regular smokers, and they were more likely to have unhealthy nutrition habits compared with women. The prevalence of IHD at baseline was 21.0% among men and 22.3% among women.
During the follow-up period, there were 338 (225 men and 113 women) deaths from IHD, 848 (512 men and 336 women) deaths from other causes, and 5584 responders (2328 men and 3256 women) survived.
Table 3 presents an association of physical activity with the risk of mortality from IHD in the Kaunas city population aged 45–72 years according to sex and IHD status at baseline. It was found that moderate and higher levels of physical activity (tertiles 2 and 3) reduced the risk of IHD mortality (HR=0.54; p=0.016 and HR=0.60; p=0.031 respectively) in men who were not diagnosed with IHD at baseline study compared with physically inactive subjects (tertile 1). Also, it was found that among men who were diagnosed with IHD at baseline, higher physical activity (tertile 3) significantly reduced the risk of mortality from IHD in men compared with those who were physically inactive (HR=0.54; p=0.021), and in the women group, moderate physical activity (tertile 2) significantly reduced the risk of mortality from IHD compared with those who were physically inactive (HR=0.41; p=0.025).
A mediation analysis was performed to analyse the associations between physical activity and other risk factors (metabolic syndrome, smoking, and psychological well-being assessment) and mortality from IHD, controlling for age as a confounder. Figure 1 shows the effect of physical activity on mortality from IHD mediated by other risk factors in men (A) and women (B) groups aged 45–72 years. The estimation of direct associations between physical activity and the risk of mortality from IHD showed, that physical activity directly predicted a statistically lower IHD mortality risk (P<0.05) in men (Fig.1 A; path c) and women (Fig.1 B; path c) groups. The estimation of indirect (risk factor-mediated) associations between physical activity and the risk of mortality from IHD showed that all three analysed risk factors (metabolic syndrome, smoking, and psychological well-being) concurrently mediate the association between physical activity and mortality risk from IHD only in the men group. The more physically active men were, the less likely they were to have metabolic syndrome (Fig.1 A; path a1) (P<0.001), the less they smoked (Fig.1 A; path a2) (P<0.05), and the better they assessed their own psychological well-being (Fig.1 A; path a3) (P<0.001). As the results of those analyses showed, metabolic syndrome (Fig.1 A; path b1) and smoking (Fig.1 A; path b2) are associated with an increased risk of mortality of IHD, while a better assessment of psychological well-being (Fig.1 A; path b3) is associated with a decreased risk of mortality from IHD in the men's group (P<0.05). Despite the fact, that physical activity directly reduces the risk of mortality from IHD in the women group (Fig.1 B; path c), the other mediators are not so important, except for psychological well-being. Physical activity increases the psychological well-being of women (Fig.1 B; path a3) (P<0.001), which significantly reduces the risk of mortality from IHD (Fig.1 B; path b3) (P<0.05). Also, the more physically active women were, the less they smoked (Fig.1 B; path a2) (P<0.05); however, smoking was not associated with an increased risk of mortality from IHD (Fig.1 B; path b2) (P>0.05), and this was probably due to the low number of women who were smokers.
4. Discussion
Physical inactivity is indeed a major global public health concern. One of the reasons for the global decline in physical activity is the increasing prevalence of sedentary behaviour [5,14]. This includes prolonged sitting at work, during leisure time, and while commuting. Increased use of electronic devices such as smartphones, tablets, and computers has also contributed to sedentary behaviour.
Our longitudinal cohort study results show that physical activity in leisure time was a significant factor that directly predicted statistically lower IHD mortality in men and women groups aged 45–72 years, regardless of whether subjects had IHD at baseline or not. The estimation of indirect (risk factor-mediated) associations between physical activity and the risk of mortality from IHD showed that all three analysed risk factors (metabolic syndrome, smoking, and psychological well-being) acting in combination, are a significant mediator of the examined association in the men's group. In the women's group, physical activity in leisure time increases the psychological well-being of women, which significantly reduces the risk of mortality from IHD. There is strong evidence that physical activity during leisure time is associated with a reduced risk of IHD mortality.
Previous examination of physical activity in the Framingham cohort revealed that mortality due to IHD was inversely related to the level of physical activity for men [15]. The effect of being sedentary on mortality is rather modest compared to the effects of other risk factors, but in mortality due to IHD, it persists when these factors are considered; however, for women, the effect is negligible [15]. Several large-scale studies have consistently shown that individuals who engage in regular physical activity during their leisure time have a lower risk of developing and dying from IHD [16,17]. For example, a meta-analysis of 21 prospective cohort studies found that high levels of leisure-time physical activity have a beneficial effect on cardiovascular health by reducing the overall risk of incident coronary heart disease among men and women by 20 to 30% [16]. The protective effect of physical activity on IHD mortality is thought to be due to its beneficial effects on cardiovascular health, including improvements in blood lipid levels, blood pressure, glucose metabolism, and endothelial function [16,17]. Moreover, physical activity can also reduce the risk of other risk factors for IHD mortality, such as metabolic syndrome, which is a cluster of metabolic abnormalities that include central obesity, high blood pressure, high blood sugar, and abnormal blood lipid levels, all of which increase the risk of developing cardiovascular disease [18]. Physical activity can help to prevent or manage metabolic syndrome by improving insulin sensitivity, reducing central obesity, and lowering blood pressure and blood lipid levels [4,18]. Similar results are also found in the studies of other scientists conducted in Europe and around the world. Moderate and intense physical activity reduced the possibility of metabolic syndrome by 3-10% for residents of the Canary Islands [19]. The Spanish population, which was less physically active during leisure time, had metabolic syndrome, was more obese, and had a larger waist circumference [20]. The results from other studies from Spain looked at an elderly population with CVD risk factors. It was found that residents with average or higher leisure time physical activity had a lower chance of acquiring metabolic syndrome [21] and participants who were physically inactive during leisure time had a higher incidence of metabolic syndrome than those who were moderately or more physically active [22]. In a cohort of American men, higher leisure-time physical activity was associated with lower odds of metabolic syndrome [23], and in a cohort of Japanese men and women with higher daily physical activity who exercised more during leisure time, the prevalence of metabolic syndrome was lower compared to those who were physically inactive [24]. It can be assumed that any physical activity in the population of any age, even for those at risk of CVD, is an important factor in avoiding metabolic syndrome.
The results of our mediation analysis indicated indirect (risk factor-mediated) associations between physical activity and the risk of mortality from IHD acting in combination with smoking habits, which is a significant mediator of the examined association in the men's group. Similar results were obtained in a Norwegian study: smokers tend to be less physically active in their leisure time than non-smokers [25]. When comparing physically active Finnish residents with inactive and less active peers, it was found that the frequency of smoking was lower among increasingly active women and men and constantly active men [26]. In another population study, it was found that regularly physically active Finns are mostly non-smokers, while physically inactive and little active Finns are mostly smokers [27]. The results of this and the reviewed studies confirm that individuals who are physically active are less likely to smoke.
In addition, physical activity can improve psychological well-being by reducing symptoms of anxiety and depression, improving mood, and promoting stress management, which can indirectly reduce the risk of developing IHD [14]. The results of some studies have shown that physical activity during leisure time can have positive effects on psychological well-being, including reduced symptoms of anxiety and depression, improved mood, and increased self-esteem [28]. It is important to note that the relationship between physical activity, psychological well-being, and IHD mortality is complex and may be bidirectional. For example, individuals who have better psychological well-being may be more likely to engage in physical activity, and physical activity may, in turn, improve psychological well-being and reduce the risk of IHD mortality. In summary, physical activity during leisure time has been associated with both improved psychological well-being and a reduced risk of IHD mortality. The exact mechanisms underlying these associations are complex and likely involve multiple factors.
There are some strengths and limitations in this study. Strengths of the present study are that it’s the prospective design, a large sample size, and a wide age interval of study participants including middle-aged and elderly individuals (45-72 years at baseline). Other strengths are that data collection using standardized and validated study methods [6], long follow-up period (from 2006-2008 to 2018), and many potential confounders included in statistical analyses (metabolic syndrome, smoking, assessment of psychological well-being, eating habits, age, and education). The limitation is that confounding by other lifestyle factors such as alcohol consumption may be a plausible part of the explanation for an inverse association between physical activity and mortality risk. However, in our study, we did not adjust data by alcohol consumption.
5. Conclusions
Our longitudinal cohort study suggests that engaging in regular physical activity during leisure time has been associated with a lower risk of IHD mortality, likely due to its beneficial effects on cardiovascular health and reduction of other risk factors. Preventive actions are necessary to increase physical activity and improve cardiovascular health. Reinforced efforts shall be prioritized and scaled up for broadening and ameliorating the application of physical activity guidelines, especially in specific populations with IHD or with some risk factors such as metabolic syndrome or low psychological well-being status.
Author Contributions
D.L. conceptualization, and writing-review and editing. D.L., A.T., R.R., V. J. methodology, investigation, data curation, writing-original draft preparation, review. R.R., M.B., conceptualization, data curation, and supervision. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by Wellcome Trust, 081081/Z/06/Z. US National Institute on Aging, 1R0I AG23522, and Research Council of Lithuania (grant number SEN-02/2015).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Research data are available by request to the corresponding author.
Acknowledgments
Many thanks go to all the workers and the whole team who have collected data and especially D. Virvičiūtė for helping with the data analysis.
Conflicts of Interest
The authors declare that there is no conflict of interest regarding the publication of this paper.
References
- Official statistics portal. The population of Lithuania (edition 2021) Causes of death. Available online: https://osp.stat.gov.lt/lietuvos-gyventojai-2021/mirtingumas/gyventoju-mirties-priezastys (accessed on 10 March, 2023).
- Timmis, A.; Vardas, P.; Townsend, N.; Torbica, A.; Katus, H.; De Smedt, D.; Gale, C.P.; Maggioni, A.P.; Petersen, S.E.; Huculeci, R.; et al. European Society of Cardiology: cardiovascular disease statistics 2021. Eur. Heart J. 2022, 43, 716–799. [Google Scholar] [CrossRef] [PubMed]
- World Health Organization (WHO). Physical activity. 2021. Available online: https://www.who.int/news-room/fact-sheets/detail/physical-activity (accessed on 16 March, 2023).
- Saint-Maurice, P.F.; Coughlan, D.; Kelly, S.P.; Keadle, S.K.; Cook, M.B.; Carlson, S.A.; Fulton, J.E.; Matthews, C.E. Association of Leisure-Time Physical Activity Across the Adult Life Course with All-Cause and Cause-Specific Mortality. JAMA Netw. Open. 2019, 2, e190355. [Google Scholar] [CrossRef]
- WHO guidelines on physical activity and sedentary behaviour. 2020. Available online: https://www.who.int/publications/i/item/9789240015128 (accessed on 20 February, 2023).
- Peasey, A.; Bobak, M.; Kubinova, R.; Malyutina, S.; Pajak, A.; Tamosiunas, A.; Pikhart, H.; Nicholson, A.; Marmot, M. Determinants of cardiovascular disease and other non-communicable diseases in Central and Eastern Europe: rationale and design of the HAPIEE study. BMC Public Health 2006, 6, 255. [Google Scholar] [CrossRef]
- Sapranaviciute-Zabazlajeva, L.; Luksiene, D.; Virviciute, D.; Bobak, M.; Tamosiunas, A. Link between healthy lifestyle and psychological well-being in Lithuanian adults aged 45-72: a cross-sectional study. BMJ Open. 2017, 7, e014240. [Google Scholar] [CrossRef] [PubMed]
- Hyde, M.; Wiggins, R.D.; Higgs, P.; Blane, D. A measure of quality of life in early old age: the theory, development and properties of a need’s satisfaction model (CASP-19). Aging Ment Health 2003, 7, 186–194. [Google Scholar] [CrossRef] [PubMed]
- Norkus, A.; Ostrauskas, R.; Sulcaite, R.; Baranauskiene, E.; Baliutaviciene, D. Classification and diagnosis of diabetes mellitus (methodology recommendations). Lith. Endocrinol. 2000, 3, 234–241. [Google Scholar]
- Third Report of the National Cholesterol Education Program (NCEP) expert panel on detection, evaluation and treatment of high blood cholesterol in adults (Adult Treatment Panel III) final report. Circulation. 2002, 106, 3143–3421. [CrossRef]
- Prineas, R.J.; Crow, R.S.; Blackburn, H.W. The Minnesota code manual of electrocardiographic findings: standards and procedures for measurement and classification. Boston Mass: J. Wright, 1982; p 229.
- Rose, G.A.; Blackburn, H.; Gillum, R.F. Cardiovascular survey methods. World Heal Organ - Monogr Ser. 1982; p 56.
- Hayes, A.F. Introduction to mediation, moderation, and conditional process analysis: A regression-based approach. Little TD (ed) Guilford Press. 2013; p 507.
- World Health Organization (WHO). Global action plan on physical activity 2018-2030. Available online: https://apps.who.int/iris/bitstream/handle/10665/272722/9789241514187-eng.pdf (accessed on 20 February, 2023).
- Kannel, W.B; Sorlie, P. Some Health Benefits of Physical Activity: The Framingham Study. Arch. Intern. Med. 1979, 139, 857–861. [Google Scholar] [CrossRef]
- Li, J.; Siegrist, J. Physical activity and risk of cardiovascular disease--a meta-analysis of prospective cohort studies. Int. J. Environ. Res. Public Health 2012, 9, 391–407. [Google Scholar] [CrossRef]
- Kodama, S.; Saito, K.; Tanaka, S.; Maki, M.; Yachi, Y.; Asumi, M.; Sugawara, A.; Totsuka, K.; Shimano, H.; Ohashi, Y.; et al. Cardiorespiratory Fitness as a Quantitative Predictor of All-Cause Mortality and Cardiovascular Events in Healthy Men and Women: A Meta-analysis. JAMA 2009, 301, 2024–2035. [Google Scholar] [CrossRef]
- Saklayen, M.G. The Global Epidemic of the Metabolic Syndrome. Curr. Hypertens. Rep. 2018, 20, 12. [Google Scholar] [CrossRef]
- Serrano-Sánchez, J.A.; Fernández-Rodríguez, M.J.; Sanchis-Moysi, J.; del Cristo Rodríguez-Pérez, M.; Marcelino-Rodríguez, I.; de León, A.C. Domain and intensity of physical activity are associated with metabolic syndrome: A population-based study. PLoS One 2019, 14, e0219798. [Google Scholar] [CrossRef]
- Gallardo-Alfaro, L.; Bibiloni, M.D.M.; Mateos, D.; Ugarriza, L.; Tur, J.A. Leisure-Time Physical Activity and Metabolic Syndrome in Older Adults. Int. J. Environ. Res. Public Health 2019, 16, 3358. [Google Scholar] [CrossRef] [PubMed]
- Gallardo-Alfaro, L.; Bibiloni, M.; Bouzas, C.; Mascaró, C.M.; Martínez-González, M.Á.; Salas-Salvadó, J.; Corella, D.; Schröder, H.; Alfredo Martínez, J.A.; Alonso-Gómez, A.M.; et al. Physical activity and metabolic syndrome severity among older adults at cardiovascular risk: 1-Year trends. Nutr. Metab. Cardiovasc. Dis. 2021, 31, 2870–2886. [Google Scholar] [CrossRef]
- Gallardo-Alfaro, L.; Bibiloni, M.D.M.; Mascaró, C.M.; Montemayor, S.; Ruiz-Canela, M.; Salas-Salvadó, J.; Corella, D.; Fitó, M.; Romaguera, D.; Vioque, J.; et al. Leisure-Time Physical Activity, Sedentary Behaviour and Diet Quality are Associated with Metabolic Syndrome Severity: The PREDIMED-Plus Study. Nutrients 2020, 12, 1013. [Google Scholar] [CrossRef]
- Sagawa, N.; Rockette-Wagner, B.; Azuma, K.; Ueshima, H.; Hisamatsu, T.; Takamiya, T.; El-Saed, A.; Miura, K.; Kriska, A.; Sekikawa, A. Physical activity levels in American and Japanese men from the ERA-JUMP Study and associations with metabolic syndrome. J. Sport Heal. Sci. 2020, 9, 170–178. [Google Scholar] [CrossRef] [PubMed]
- Uemura, H.; Katsuura-Kamano, S.; Iwasaki, Y.; Arisawa, K.; Hishida, A.; Okada, R.; Tamura, T.; Kubo, Y.; Ito, H.; Oze, I.; et al. Independent relationships of daily life activity and leisure-time exercise with metabolic syndrome and its traits in the general Japanese population. Endocrine 2019, 64, 552–563. [Google Scholar] [CrossRef] [PubMed]
- Morseth, B.; Jacobsen, B.K.; Emaus, N.; Wilsgaard, T.; Jørgensen, L. Secular trends and correlates of physical activity: The Tromsø Study 1979-2008. BMC Public Health 2016, 16, 1215. [Google Scholar] [CrossRef] [PubMed]
- Lounassalo, I.; Hirvensalo, M.; Palomäki, S.; Salin, K.; Tolvanen, A.; Pahkala, K.; Rovio, S.; Fogelholm, M.; Yang, X.; Hutri-Kähönen, N.; et al. Life-course leisure-time physical activity trajectories in relation to health-related behaviors in adulthood: the Cardiovascular Risk in Young Finns study. BMC Public Health 2021, 21, 533. [Google Scholar] [CrossRef]
- Salin, K.; Kankaanpää, A.; Hirvensalo, M,; Lounassalo, I. ; Yang, X.; Magnussen, C.G.; Hutri-Kähönen, N.; Rovio, S.; Viikari, J.; Raitakari, O.T.; et al. Smoking and physical activity trajectories from childhood to midlife. Int. J. Environ. Res. Public Health 2019, 16, 974. [Google Scholar] [CrossRef]
- Min, S.; Masanovic, B.; Bu, T.; Matic, R.M.; Vasiljevic, I.; Vukotic, M.; Li, J.; Vukovic, J.; Fu, T.; Jabucanin, B.; et al. The Association Between Regular Physical Exercise, Sleep Patterns, Fasting, and Autophagy for Healthy Longevity and Well-Being: A Narrative Review. Front. Psychol. Sec. Health Psychology 2021, 12, 803421. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The effect of physical activity on the risk of mortality from IHD, mediated by other risk factors, in men (A) and women (B) groups aged 45-72 years. a – relationship between the input variable and the mediating variable. b – relationship between the mediating variable and the output variable. c – direct effect of an input variable on an output variable. c’ – indirect effect of an input variable on an output variable. MS – metabolic syndrome. PWB – psychological well-being assessment. *P<0.05; **P<0.001. # Nagelkerke R2=0.1317 for the men's group; ¥ Nagelkerke R2=0.1952 for the women's group.
Figure 1.
The effect of physical activity on the risk of mortality from IHD, mediated by other risk factors, in men (A) and women (B) groups aged 45-72 years. a – relationship between the input variable and the mediating variable. b – relationship between the mediating variable and the output variable. c – direct effect of an input variable on an output variable. c’ – indirect effect of an input variable on an output variable. MS – metabolic syndrome. PWB – psychological well-being assessment. *P<0.05; **P<0.001. # Nagelkerke R2=0.1317 for the men's group; ¥ Nagelkerke R2=0.1952 for the women's group.
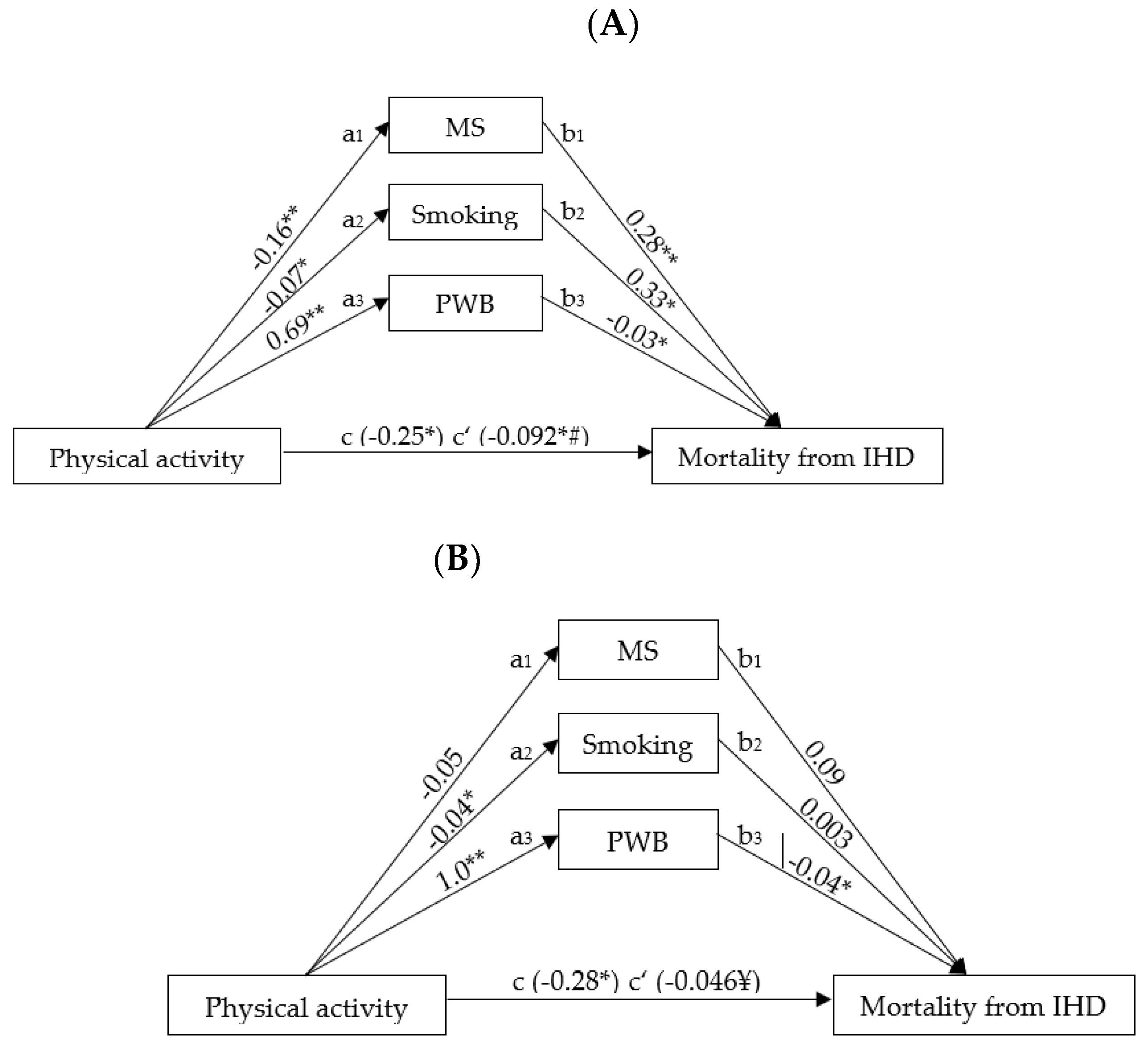

Table 1.
Physical activity levels in population aged 45–72 years (hours/week).
| Physical Activity Levels / Tertiles | Men | Women | ||
|---|---|---|---|---|
| Min–max* | Mean (SD) | Min–max* | Mean (SD) | |
| Physically inactive (1st tertile) | 0.0–10.0 | 5.8 (3.1) | 0.0–13.5 | 8.6 (3.4) |
| Moderately physically active (2nd tertile) | 10.5–19.5 | 14.7 (2.6) | 14.0–22.0 | 17.5 (2.6) |
| Higher physically active (3rd tertile) | 20.0–42.0 | 26.8 (5.9) | 22.5–42.0 | 29.2 (5.1) |
SD – Standard deviation. *Minimum (Min) is the lowest evaluation, and maximum (max) is the highest evaluation.
Table 2.
Baseline characteristics of men and women at the baseline survey of the Kaunas HAPIEE study (2006-2008).
Table 2.
Baseline characteristics of men and women at the baseline survey of the Kaunas HAPIEE study (2006-2008).
| Variables | MEN n=3065 |
WOMEN n=3705 |
P |
|---|---|---|---|
| Age, years, mean ± SD | 57.3±7.87 | 57.1±7.84 | 0.217 |
| Education, % | <0.001 | ||
| Secondary and lower | 46.8 | 37.5 | |
| College and higher | 53.2 | 62.5 | |
| Metabolic syndrome, % | 27.5 | 33.8 | <0.001 |
| Arterial hypertension (≥130/85 mm/Hg), % | 83.4 | 69.7 | <0.001 |
| Increased waist circumference, % | |||
| Men ≥102 cm, women ≥88 cm | 27.3 | 48.6 | <0.001 |
| HDL cholesterol, | |||
| Men <1.0 mmol/L, women <1.3 mmol/L, % | 12.1 | 23.2 | <0.001 |
| Triglycerides ≥1.7 mmol/L, % | 28.3 | 25.0 | 0.001 |
| Fasting glucose ≥6.1 mmol/L, %, | 30.8 | 30.9 | 0.475 |
| Psychological well-being groups | 0.004 | ||
| Higher | 52.8 | 56.3 | |
| Lower | 47.2 | 43.7 | |
| Regular smoking, % | 37.7 | 13.6 | <0.001 |
| Nutrition habits, % | |||
| More frequent consumption of fresh fruit and vegetables | 51.1 | 59.4 | <0.001 |
| More frequent consumption of sweets | 51.4 | 48.9 | 0.020 |
| More frequent consumption of cereals, and infrequent consumption of meat | 32.7 | 58.0 | <0.001 |
| More frequent consumption of meat, potatoes, and eggs | 61.4 | 42.6 | <0.001 |
| More frequent consumption of chicken and fish | 55.4 | 49.3 | <0.001 |
| Prevalence of IHD at baseline survey, % | 21.0 | 22.3 | 0.197 |
Data weighted by age (WEIGHT10). The chi-square test for distributions and the T-test for means and z-test for two percentages were used to compare differences in variables between sexes. SD- standard deviation; HDL – high-density lipoprotein; IHD – ischaemic heart disease.
Table 3.
An association of physical activity with the risk of mortality from IHD in Kaunas city population aged 45–72 years according to sex and IHD status at baseline study.
Table 3.
An association of physical activity with the risk of mortality from IHD in Kaunas city population aged 45–72 years according to sex and IHD status at baseline study.
| IHD status | ||||
|---|---|---|---|---|
| Without IHD HR (95 % CI) |
P | With IHD HR (95 % CI) |
P | |
| MEN | N=2422 | N=643 | ||
| Physically inactive | 1 | 1 | ||
| Moderately physically active | 0.54 (0.33–0.89) | 0.016 | 0.69 (0.43–1.10) | 0.121 |
| Higher physically active | 0.60 (0.37–0.95) | 0.031 | 0.54 (0.32–0.91) | 0.021 |
| WOMEN | N=2877 | N=828 | ||
| Physically inactive | 1 | 1 | ||
| Moderately physically active | 0.75 (0.40–1.39) | 0.354 | 0.41 (0.19–0.89) | 0.025 |
| Higher physically active | 0.73 (0.38–1.38) | 0.331 | 0.54 (0.25–1.18) | 0.123 |
IHD – ischaemic heart disease. HR – hazard ratio. CI – confidence interval. Multivariate Cox regression. Variables included in the model: metabolic syndrome, smoking, assessment of psychological well-being, eating habits, age, and education. Reference group: physically inactive – tertile 1. Moderately physically active – tertile 2. Higher physically active – tertile 3.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



