
Submitted:
02 May 2023
Posted:
03 May 2023
You are already at the latest version
Abstract
The majority of EGFR mutations (85–90%) are exon 19 deletions and L858R point mutation of exon 21, characterized by high sensitivity to EGFR-tyrosine kinase inhibitors (TKIs). Less is known about uncommon mutations (10-15% of EGFR mutations). Predominant mutation types in this category include exon 18 point mutations, exon 21 L861X, exon 20 insertions and exon 20 S768I. This group presents a heterogeneous prevalence, partly due to the different testing methods and to the presence of compound mutation, which in some cases leads to shorter overall survival and different sensitivity to different TKIs than simple mutations. EGFR-TKI sensitivity may also vary depending on the specific mutation and the tertiary structure of the protein. The best strategy remains uncertain and the data of TKIs efficacy are founded of few prospective and some retrospective series. Newer investigational agents are still under study and there are no other approved specific treatment targeting uncommon EGFR mutations. Defining the best treatment option for this patient population remain un unmet medical need. The objective of this review is to evaluate existing data on outcomes, epidemiology and clinical characteristics of lung cancer patients with rare EGFR mutations, with a focus on intracranial activity and response to immunotherapy.
Keywords:
Non-small cell lung cancer (NSCLC)
; EGFR
; Tyrosine kinase inhibitors (TKIs)
; Uncommon mutation
; Compound mutation
; Intracranial activity
; Immunotherapy
1. Introduction
Despite emerging treatment strategies in the recent years, lung cancer remained the leading cause of cancer death worldwide, with an estimated 1.8 million deaths every year.[1] Most treatment advances in lung cancer occurred in the field of targeted therapies and EGFR mutant NSCLC.
EGFR is a transmembrane receptor and has a crucial function in cancer cell proliferation, neoangiogenesis and inhibition of the apoptosis.[2] EGFR overexpression correlates with aggressive disease and poor prognosis,[3], therefore, it represents an optimal target for cancer therapy. The major achievements in the field of EGFR tyrosine kinase inhibitors (TKIs) have been obtained in patients with NSCLC.
Prevalence of EGFR mutations ranges from 14% in European patients to 38% in Chinese patients;[4] EGFR mutation occurs mainly in adenocarcinoma histology, female gender and non-smoker patients.[4] The majority of EGFR mutations (85%–90% of all EGFR-mutant patients) are deletion of exon 19 (Ex19del) in the Leu Arg Glu Ala (LREA) residues (amino acid residues 747 to 750; 45% of EGFR mutations) and L858R point mutation of exon 21 (40%); these are known as activating EGFR mutations and are characterized by high sensitivity to EGFR-tyrosine kinase inhibitors (TKIs).[5] Exon 20 T790M is an uncommon at NSCLC diagnosis, mostly associated to about half cases of resistance after first or second generation EGFR TKIs.[6,7]
Less is known about other mutations, defined as uncommon mutations, accounting for approximatively 10-15% of all EGFR mutations (ranging between 1% and 18,2% across different series) and usually showing a lower sensitivity to EGFR TKIs with some exceptions with the use of afatinib.[8,9,10,11,12]
Unfortunately, uncommon mutations are no or underrepresented in most phase III clinical trials comparing EGFR TKIs with chemotherapy or different EGFR TKI generations. Available evidence on the drug sensitivity and treatment outcome of EGFR TKIs in patients harboring uncommon mutations is mostly retrospective on Asian patients and focused on the most frequent mutations among uncommon (G719X exon 18; L861X exon 21; S768I exon 20).[10,13,14,15,16,17]
Although most clinicians agree and expert consensus recommend a front-line treatment with EGFR TKIs instead of chemotherapy, defining and tailoring the optimal treatment strategy for this patient population is still un unmet medical need.
The aim of this review is to describe epidemiology and clinical features of lung cancer patients affected by uncommon EGFR mutations and discuss available data on patients’ outcome receiving different treatment options.
2. Epidemiology of uncommon EFGR mutation
As mentioned above the most frequent types of EGFR mutations are Ex19del in the LREA motif and mutation L858R, characterized by high sensitivity to EGFR-tyrosine kinase inhibitors (TKIs),[5] and mutation T790M associated to 40-55% of cases of resistance to first or second generation EGFR TKIs. [6,7] Significantly less evidence is available on mutations other than ex19del, L858R and exon 20 T790M, defined as uncommon mutations and accounting for about 10-15% of all EGFR mutations. John et al. analyzed the prevalence of uncommon EGFR mutation across ten studies, of which the majority conducted in China, showing an occurrence rate of uncommon mutations ranging from 1.0% to 18.2%.[9]
The clinical features of this patient population are similar to patients with common EGFR mutations, although some studies have shown an association with smoking history and older age.[8,18]
In a series of 5363 Chinese patients, the frequency of EGFR mutation was found to be 34%. Among these patients, the frequency of uncommon mutations was 11.9%. It was observed that there were more male patients (54.1% vs. 44.4%) and smoker patients (30.7% vs. 24.3%), in the group with uncommon mutations compared to the group with common mutations. This difference was found to be statistically significant with a p respectively of 0.007 and 0.039.[17] Some mutation types predominate within this group, such as point mutations in exon 18 at position G719X (0.9–4.8%), the exon 21 L861X mutation (0.5–3.5%), the insertions in exon 20 (Ex20ins; 0.8–4.2%), and S768I in exon 20 (0.5–2.5%).[9] Other uncommon alterations comprise: exon 18 indel (i.e. pE709_T710delinsD) involving codon 709 of exon 18 such as pE709K/A/G/V, as single or complex mutations, EGFR amplification, exon 21 missense, exon 19 insertions, EGFR Variant III. [19,20] Although less frequent than activating mutations, the prevalence of some uncommon mutations is comparable to the one of other druggable alterations, such as RET or ROS1 fusions.[18]
Furthermore, the prevalence of EGFR mutations in exons 18–21 varies geographically. Graham et al conducted a survey about the EGFR test performed in selected laboratory worldwide during a year. The survey included 170 clinical laboratories from 20 different countries, accounting for a total of 136,533 tests. The survey found that mutation prevalence was 30-46% in Asia, 16% in Africa and the Middle East, 13% in Europe, and 8-9% in North and South America.[21] The L861Q mutation and exon 20 mutations, were less frequently detected, as expected. Exon 20 mutations were more prevalent in Africa and the Middle East, while L861Q in northern Asia. The low number of samples for these uncommon mutations precluded statistical analysis. [21] The prevalence of rare EGFR mutation is made even more heterogeneous by the different testing methods and type of reports, referring to uncommon mutations as single drivers or within compound mutations.[22]
Whereas some reports shows that G719X, L861Q and S768I confer sensitivity to EGFR-TKIs, albeit with a lower treatment response than common mutations, the Ex20ins are known as resistant to first and third generation EGFR-TKIs.[5,9,19,23]
There are no approved TKI or established guidelines for the treatment of this subgroup of patients where the standard of care is chemotherapy [23].
3. EGFR mutation testing methods
The incidence of EGFR uncommon mutations is increasing during the last years, and this is likely due to the improvement of detection methods with particular reference to the use of next-generation sequencing (NGS)[18].
Over the years more and more methods have become available to determine the EGFR gene mutations; some of them can identify the most common genetic alterations and miss other mutations, emphasizing the importance of sequencing-based techniques to detect uncommon mutations.[24,25] Available evidence showed that Sanger sequencing and real time PCR (RT-PCR) have lower detection rate of single, uncommon or compound EGFR mutations compared with NGS.[25,26]
Sanger sequencing is used for the detection of single nucleotide variants, insertions, deletions in clinical practice, it steel represents the gold standard for such uses[22], but has some limitations due to the low sensitivity (15-20%).[22,27,28] It has been showed by Mao et al. that the detection rate of Sanger Sequencing were significantly lower when compared to NGS and RT-PCR.[29] RT-PCR technique is based on the use of fluorescent probes in order to amplify specifically the known mutation; also this method have some limitations, because it may not detect uncommon or compound mutations[22,24] Other technique used are Pyrosequencing system[19,22] and Digital PCR.[22] The Pirosequencing system is a quantitative methodology, based on the clonal amplification of emulsion PCR and the subsequent detection of light signals of the DNA growing chain.[30] Digital PCR is a technique able to detect and quantify in a precise and accurate manner a target molecule[31]; in particular digital droplet PCR (ddPCR) showed a high sensitivity in a previous analysis of Gu et al., the sensitivity was 96% for ddPCR in comparison to RT-PCR and NGS[32].
Finally NGS is able to detect an ever-increasing number of EGFR mutations and concomitant alterations; a several number of NGS panel are available to date allowing a concurrent evaluation of several target hotspots.[22] The use of NGS technique on cell-free DNA (cfDNA) could solve the need of biopsies, which are difficult to obtain in certain cases; a previous study exploring NGS analysis on ctDNA showed sensitivity of 75 % and a specificity of 100 %.[33]
NGS showed benefit in comparison to Sanger sequencing and RT-PCR by providing the highest number of EGFR mutations and by identifying other non-EGFR mutations with potential targeted drugs.[29]
NGS allowed us to detect not only classical EGFR mutations, but also a broad number of concomitant mutations, rare mutations and mechanisms of resistance, impacting treatment outcome and the therapeutic chance to the patient.[22] However no prospective large trials have evaluated the clinical impact in detection of rare and compound mutations and further evidences are needed.[19,20]
As per ESMO guidelines it is currently recommended to use NGS technique for patients with advanced non-squamous NSCLC (plasma or tumor sample), in order to detect ESCAT (ESMO Scale for Clinical Actionability of molecular) level I alterations for which is available a drug validated in clinical trials, driving treatment decision.[34]
This may not be always feasible in a real world scenario. In particular, focusing on ex20ins, and its heterogeneity, the occurrence of the mutation may not be accurately detected due to the limitations of the testing methods used in clinical practice. Baumi et al. studied a sample of 175 patients with ex20ins detected by NGS, and noticed that only 89 (50.9%) would have been identified by a PCR test. A second dataset comprising 627 patients provided confirmation of this concern, as per the results, PCR testing was expected to overlook 51.4% of exon20ins cases that were detected by NGS.[35]
4. From exon-based to structure-based classification of EGFR mutation
The EGFR gene could harbor different mutations and despite several of them may appear similar to classical ones, the response to EGFR-TKIs as well as any resistance to treatments may be heterogeneous and not easy to predict.[22]
In this context a predictive system for classifying EGFR mutations on the basis of their sensitivity would be of crucial interest in order to guide treatment decisions.[22,23]. Robichaux et al. studied a large database of EGFR mutant NSCLC developing a new preclinical model of 76 different EGFR mutations, treated with 18 different EGFR inhibitors (first, second and third generation, as well as ex20ins TKIs).[23,36] Based on the response to EGFR-TKI a new structured-based classification has been outlined, stratifying the non-classical EGFR mutations into four main subgroups: classical-like mutations (distant to the ATP binding pocket), T790M-like mutations (within the hydrophobic core), insertion in the C-terminal end of αC-helix in exon 20; and finally, mutations within the ATP binding pocket or C-terminal end of the αC-helix, which compress the P-loop and the αC-helix itself (PACC mutations). A simplification of the tertiary structure of EGFR is shown in Figure 1.[23]
This structure-function-based classification seems to better identify drugs sensitivity compared with a simple exon-based classification; thus, it is possible that mutations in different gene sites may induce similar changes in the tertiary structure of the receptor such as in case of PACC mutations.[23,36]
It was seen that classical-like, atypical EGFR mutations have small effect on the EGFR global structure compared with wild-type EGFR and are sensitive to all EGFR TKIs.[23]
Robichaux et al. found that not all exon 20 mutations have the same response to EGFR-TKIs: exon 20 point mutations were sensitive to second-generation EGFR-TKI and belong to the subgroup of PACC mutations, differently from the majority of ex20ins in the αC-helix, that behave similarly to “classical-like” mutations; differently, ex20ins in the C-terminal loop of the αC-helix seemed to be more sensitive to second generation EGFR-TKI.[36] In particular the mutations nearer to the C-terminal loop were found to be more sensitive to EGFR-TKIs than the farther ones.[36] In addition it was found that in case of a classical EGFR mutation co-occurring with a PACC mutation the model seemed to predict a response to the second generation EGFR-TKI.[23,36] Such evidence needs to be further confirmed, hopefully in prospective clinical trials, as could bring important clinical-therapeutic implications in EGFR mutant NSCLC.[36]
5. Compound mutations
Heterogeneous outcome in patients harboring uncommon mutations is also coming from the co-occurrence of uncommon mutations within compound mutations both associated with common and uncommon alterations.[37,38] Thus we can assume that the presence of co-occurring alterations contributes to increase spatial and temporal heterogeneity of EGFR-mutant NSCLC,[39,40] in which some subclones gain proliferative advantage under treatment pressure, leading to acquired resistance which may arise sooner or later. In a recent work it was seen that EGFR compound mutations were virtually homogeneous inter-and intratumor in a little series of patients and the optimal treatment should be chosen based on the EGFR mutation detected, including the type of compound mutations.[38] Attili et al. proposed four main categories of compound EGFR mutations: combined common EGFR mutations (exon 21 p.L858R + exon 19 deletions), combined common (exon 21 p.L858R + exon 19 deletions) plus uncommon EGFR mutations (any but exon 21 p.L858R, exon 19 deletions or de novo exon 20 p.T790M), combined uncommon EGFR mutations and combined EGFR mutation (any) plus de novo exon 20 p.T790M (Table 1).[41]
Compound EGFR mutations are represented as double or multiple nonsynonymous mutations of the EGFR tyrosine kinase domain, in which a typical EGFR mutation (i.e., ex19del, L858R) in the majority of the cases is identified together with an atypical mutation, or a combination of 2 uncommon mutations.[5,37] The clinical significance of compound mutation is still unclear, and they’re frequently detected with advances in sequencing technology, such as NGS.[37]
The incidence of compound mutations is highly heterogenous and varies across the studies from 3% to 26% of total EGFR mutant cases; this heterogeneity is probably dependent on the different testing methods used, the patient population and the specific mutations considered.[42,43]
The study conducted by Kim et al. found compound EGFR mutations in 24.6% of the cases of EGFR-mutant lung adenocarcinoma and the majority of them were represented by a combination of the atypical mutation and typical mutation. Examples of partner alterations were mutations in exon 18 (V689L, I706T, and E709K), in exon 20 (H773Y and R776H), or in exon 21 (L833V, H870R, and A871G). One patient harbors a compound mutation of L858R and E19del.[37] Kim et al. also found that patients with compound mutations were most likely to have a higher burden of missense mutations.[37] It was seen that the patients with compound mutation had shorter overall survival than those with simple mutations (83.7 vs. 72.8 m), thus the need to closely monitor these patients during follow-up.[37]
The subtypes associated with poor clinical outcomes, such as papillary/micropapillary types and solid with mucin production type, were more frequently detected in cases with compound mutations. OS was significantly poorer in the cases with compound mutations, but there was no difference in the duration of disease control between groups with compound or simple mutations treated with EGFR TKIs at the recurrence.[37] Kobayashi et al. found compound EGFR mutations in 14% of the patients included in their study: most patients had an EGFR sensitizing mutation (i.e. G719X, ex19del, L858R and L861Q) and an atypical mutation.[5] Reporting the genotype-response pattern of NSCLCs with EGFR compound and uncommon mutations will be helpful to guide the appropriate decision-making for the treatment of patients with EGFR-mutant NSCLC.[5]
Preclinical data suggested that patients with NSCLC harboring EGFR compound mutations are associated with different sensitivity response to different TKIs.[38] A few papers have reported the presence of different responses to the EGFR-TKIs among patients harboring compound EGFR mutations.[37]
In a series of 106 patients receiving first generation EGFR-TKIs, the mPFS of patients with compound mutations was significantly poorer compared to patients with a single common mutation (9.1 vs. 13.0 months, p < 0.001).[42] Furthermore the RR to the treatment of patients harboring compound mutations was lower than that of patients with single common mutations, even though without statistically significant difference (50.9 % vs 67.8%, p=0.088).[42] Within the group harboring compound mutations, the patients with double rare mutations (i.e., co-occurring mutation in exon 20) had worse mPFS than patients with other compound mutations or a common mutation (6.5 vs. 9.1 vs. 13.0 months, p = 0.002).[42] Other evidence suggests that patients with 2 common EGFR mutations treated with first generation EGFR TKI had a similar RR and PFS to patients with a single common mutation.[43,44]
The ORR and PFS to TKIs in patients with common plus rare mutations is largely heterogeneous.[42]
Patients with single exon 20 mutations are considered resistant to TKIs[42] but whether patients with an EGFR exon 20 mutation accompanied by another mutation are candidates for TKIs therapy remains unanswered; previous reports showed that patients with ex20 compound mutations obtained response to EGFR-TKI while other patients with single ex20 mutation had PD at the first evaluation.[45,46]
Besides compound mutations within the EGFR gene, different commutations are mostly present with very rare EGFR mutations, and the more frequent TP53 seems to have a detrimental effect on TKIs treatment outcome. This is certainly another reason to make the knowledge of tumor heterogeneity relevant in defining the treatment sequence.[47] Another mutation in a different gene is PIK3CA driving resistance to EGFR-TKI by activating bypass AKT signaling; it is found in 4% of patients with lung cancers[40] and in 3.5% of EGFR mutant NSCLC.[48]
5. Treatment activity data of different TKIs
5.1. The more common among uncommon: L861Q, G719X and S768I
Three generations of EGFR TKIs have been introduced in the clinical practice as standard of care for common EGFR mutations.[49,50] These molecules have different pharmacological characteristics and modes of action: the first generation erlotinib and gefitinib are reversible EGFR TKIs,[51,52,53,54,55,56] and prevent auto-phosphorylation of the EGFR, which in turn stop downstream signaling by competitively engaging with the ATP-binding region. The second generation afatinib and dacomitinib bind to the EGFR kinase domain via covalent, irreversible bonds and might be more active against other receptors of the ErbB receptors family.[54,55,57,58] The third generation irreversible TKI osimertinib has been designed to specifically target the gatekeeper T790M mutation, which confer resistance to first and second generation TKIs by interfering with the bond to the ATP binding site.[59] The optimal treatment of patients with tumors harboring uncommon EGFR activating mutations remains uncertain.
Data about the efficacy of EGFR TKIs in patients with NSCLC harboring uncommon EGFR mutations are limited to few prospective studies with afatinib (LUX-lung 2, 3 and 6)[13], one prospective study with osimertinib (KCSG-LU15–09)[60] and several retrospective series and case reports.[14,15,16,17]
The available data show clinical activity and efficacy for the treatment of the mutations G719X, L861Q, and S768I,[13] for which has been shown that first line treatment with EGFR-TKIs (afatinib in particular) significantly improve the PFS compared with first line chemotherapy.[61,62]
The exon 20 point mutation pS768I showed a good response to afatinib (median PFS of 14.7 months) in trial LUX-lung 2, 3 and 6 [13] and a PFS of 12.3 months in patients treated with osimertinib in a recent trial.[60] One real-world study with afatinib, focusing on Chinese patients, shows a prevalence of 12% of uncommon mutation; the whole patient population harboring uncommon mutation had a PFS of 9.06 months.[63] A recent large study on a database of 693 EGFR mutant patients harboring 98 different uncommon mutations, explored the efficacy of afatinib; the data has been collected from randomized clinical trials and phase IIIb trials, compassionate-use/expanded-access programs, noninterventional trials, case series or case studies.[64,65] For the 272 untreated patients harboring the mutations G719X, L861Q, and S768I, median time to treatment failure (TTF) was almost 1 year, while for patients with ex20ins and other uncommon mutations was 4.2 and 4.5 months respectively; afatinib showed efficacy even in patients with compound mutation with a median TTF of 14.7 months, and even higher if one of the mutation was common (16.6 months).[64] Another study confirmed the clinical activity of afatinib for patients with compound EGFR mutation and a better PFS comparing to gefitinib and erlotinib. The FDA on 2018 approved afatinib for the treatment of patient harboring the following uncommon EGFR mutations: L861Q, G719X, and S768I, on the basis of a combined analysis of the above mentioned LUX-lung 2, 3 and 6 trials,[13,66]
Preclinical data from NSCLC models harboring these three uncommon mutations tempt to suggest a clinical activity of osimertinib in this setting.[67] Results from the prospective phase II study KCSG-LU15-09 with first line osimertinib in patients with NSCLC with uncommon EGFR mutations, showed an ORR of 50%, median PFS of 8.2 months and median OS not reached.[60] Few data are available regarding the outcomes of osimertinib in patients with uncommon EGFR mutations in the real world.[65] A retrospective study showed activity of osimertinib in patients with NSCLC harboring uncommon mutation, although with a lower clinical benefit compared to common mutation; L861Q and ex19delins have a better outcome.[68]
5.2. Focus on exon 18
Ex18 mutations account for 3-4% of EGFR mutations and comprise mutations in codon 719 (G719A/S/C) and 709 (E709X), less frequently del-ins.[18]
Mutation G719X, after ex20 ins, is the most frequent uncommon mutation and, although heterogeneously, shows sensitivity to TKIs, in particular an high ORRs (75–78%) with afatinib[13] and neratinib[69], in respect to first generation TKIs, comparable to response with common mutations.[18] Mutations involving codon 709 such as pE709K/A/G/V, as single or complex mutations, are known to be resistant to first generation TKIs but some of them are sensitive to afatinib (pE709K/A)[19,70,71], and generally occurs as part of compound mutation.[14]
The most common ex18 deletion is delE790_T710insD, and in preclinical model it has been shown to be the less sensitive to EGFR TKIs among ex18 mutations;[72] very few clinical data are available showing some activity of afatinib.[14] Patients may harbor del-ins with other uncommon mutations (ex20 T790M).[18,73]
5.3. Focus on exon 19
Mutations in ex19 are the most common EGFR mutations, but their sensitivity to EGFR TKIs varies largely; the deletions in LRE fragment (L747 to E749) are known to be sensitive to EGFR TKIs while non-LRE deletions have a lower response to EGFR TKIs.[74] Uncommon ex19 deletions-insertions variants (ex19delins) accounts for 5% of EGFR mutant NSCLC and have different sensitivity to EGFR TKIs.[75] Some variants have similar structure to ex19del, reported sensitivity to first/second-generation EGFR TKIs in vitro and in vivo[76] and have significant better PFS when treated with first generation TKIs compared to common ex19del; the most common variant is L747_A750delinsP known to be sensitive to afatinib,[75] and likewise for some ex19del between aminoacid residues 745-753, showing sensitivity to TKIs.[19] Other exon 19 insertions such as p.L747S, p.D761Y and p.T854A confer resistance to EGFR TKIs.[77] Interestingly, patients with uncommon ex19delins showed a better PFS than patients with common ex19del, nevertheless when treated with first line EGFR TKIs the two groups have a similar risk of developing resistance by acquiring the T790M mutation. Subsequently when treated with osimertinib second line the patients with ex19delins showed a significant poorer outcome (except variant L747_A750P).[75]
5.4. Focus on exon 20
Ex20ins are the largest group among uncommon EGFR mutations, consisting in insertions or duplications within 15 amino acids residues 761-775, with heterogeneous response to EGFR TKIs, the vast majority being resistant.[19,78] The residues 761-766 code fort the C-helix of the protein while residues 767-775 code for the loop following the C-helix.[77] The differences in the structure are supposed to be the cause of heterogeneous response to EGFR TKIs.[18] Indeed some data showed promising response to afatinib.[64] Preclinical evidence showed that insertions in codons 769 to 775 could lead to drug resistance whereas the one on more proximal codons might have a similar structure to classical mutations.[19] One of the most frequent mutations (5-6% of ex20ins) is p.A763_Y764insFQEA, which confer to the protein a structure similar to the one of L858R mutation and showed response to erlotinib (partial response or stable disease)[46,79]. Another ex20 mutation, p.A767_V769dupASV, which is identical to p.V769_D770insASV, showed some preclinical activity, in terms of tumor growth inhibition, in response to afatinib combined with cetuximab but clinical evidence is lacking.[80] Different types of ex20ins were found to be sensitive to afatinib: p.773_774HVinsGHPH, p.A767delinsASVD39 and p.A767_S768insSVA.[61,64] On the contrary the mutation p.D770_N771insSVD confers low sensitivity to all TKIS.[19] thus confirming the heterogeneity of patients harboring ex20ins.[5] The acquired point mutation in exon 20 p.C797S, together with T790M are the most common mechanism of resistance to third generation TKIs; when the mutation is detected in trans a combination of first and third generation TKIs could result in clinical efficacy, when is detected in cis confers resistance to TKIs in combination or alone,[19] thus suggesting a significant impact on the tertiary structure of the protein. Before the introduction of novel drugs targeting ex20ins, the gold standard of treatment for this subgroup of patients was platinum-based chemotherapy[18] but in recent years are becoming available novel treatment strategies for patients with ex20ins.
Poziotinib is a novel EGFR-TKI studied in a phase II trial, that showed clinical activity in patients with EGFR ex20ins and HER2 ex20ins.[81,82] The small size of the drug and the flexibility are the key to its effectiveness against these mutations which limit the TKI bonding site.[82] Despite the effectiveness, results from the expanded access program showed a high rate of toxicity (66% of the patients report G3 AEs) and dose interruption, thus limiting at the moment its clinical development.[83] Another TKI specifically targeting ex20ins is mobocertinib, a selective EGFR/HER2 TKI, oral and irreversible, that demonstrated a significant benefit in pretreated NSCLC patients with EGFR ex20ins.[84] Mobocertinb received in September 2021 the accelerated approval by the FDA.[85] Finally, amivantamab is a bispecific monoclonal antibody targeting MET and EGFR, which has been approved by the FDA, in May 2021, and more recently the European Medicines Agency (EMA) in December 2021 [86,87] for the treatment of patients with NSCLC harboring ex20ins, based on the results of CHRYSALIS trial demonstrating durable efficacy and a manageable safety profile.[88] The objective response rate achieved by the study population was 40%, with a mPFS of 8.3 months. The majority of adverse events observed in the study were rash (86%), followed by infusion-related reactions (66%) and paronychia (45%). 5% of the patients developed a hypokalemia G3-4, 13% of patients needed a dose reduction and 4% discontinued the treatment.[88] Focusing on infusion related reactions (IRR), Park et al. noticed that it was a frequent AE but mostly G1-2, limited to the first administration and treated with antihistamine, steroid, antipyretic and infusion holding.[89]. Subsequent infusions were not affected by the initial IRR, and only 1% of the patients discontinued their treatment due to this AE.[89] Newer investigational agents still under study in clinical trials demonstrated promising results in the treatment of patients with ex20ins. Sunvozertinib (DZD9008) is a novel, irreversible EGFR and HER2 TKI, under investigation in phase1/2 studies (NCT03974022, CTR201920) which showed antitumor activity in different types of EGFR ex20ins with a ORR of 39.3%.[90] Other novel drugs in study which revealed clinical activity in patients harboring EGFR ex20ins are CLN-081 (TAS6417),[91] and tarloxotinib.[92]
The toxicity and response rates of the inhibitors listed above are detailed in Table 2.
5.5. Focus on exon 21
6. Intracranial activity of different EGFR TKIs in uncommon mutations
Brain represents one of the most common site of metastasis for patients with NSCLC, occurring in about 40% of EGFR mutant cases during the disease course, thus representing a clinical challenge in those patients. Most EGFR TKIs showed lack of evidence about intracranial activity.[96] The FLAURA trial showed us that osimertinib has a potent activity against BMs in patients with EGFR-mutant NSCLC compared to erlotinib or gefitinib;[97] it also was associated with promising efficacy in patients with de novo T790M mutation.[96]
The clinical outcome of patients harboring uncommon EGFR mutations and BMs, treated in first line with TKIs is still unknown.[96] Clinical evidences suggest that patients harboring uncommon EGFR mutations have a significant higher prevalence of brain metastasis[98] and first-line EGFR-TKIs seemed to be less effective in controlling and preventing brain metastasis in this patient population.[96]
A previous study showed a benefit from the treatment with afatinib, but with limitations due to the small number of the patients treated; seven patients with uncommon EGFR mutations and BM were treated: 4 patients respond to treatment, 3 patients received afatinib a 1 icotinib.[99]
A retrospective study examining EGFR-mutant NSCLC patients receiving first-line EGFR-TKIs (86% gefitinib and erlotinib, 4.8% afatinib and 9.2% osimertinib), showed that among the group of patients with baseline brain metastasis, those harboring uncommon mutations has a significantly shorter intracranial time to progression compared to patients with L858R mutation (23.6 months vs 68.0 months, p=0.003) and ex19del (23.6 months vs NR, p<0.001).[96] Furthermore, patients with uncommon EGFR mutations had a higher risk of intracranial PD, thus suggesting that it will be important to implement treatment strategies, in order to prevent and control BMs.[96]
Furthermore, emerging data suggest a significant intracranial activity with second generation TKIs, in particular dacomitinib; among 32 patients included in the study conducted by Zhang et al, 30 were evaluable with measurable or non-measurable CNS lesions: the iORR was 66.7% (95% CI 47.2-82.7%) and the iDCR was 100% (95% CI 48.7-95.7%), median iDOR and median iPFS were not reached.[100] The study showed a significant CNS efficacy of dacomitinib in patients with EGFR-mutated NSCLC first line in the real-world setting.[100]
Another recent study exploring the activity of dacomitinib in patient with EGFR mutant NSCLC with BMs, included one patient with G719A and I706T co-mutations: the patient had a CNS response and an overall PR to the treatment.[101] Finally regarding the new drugs under study, it was noticed that the above mentioned CLN-081 may have an intracranial activity. Three patients treated with brain metastases have been reported: one patient achieved a SD and one patient obtained a partial response.[102] Considering the drugs approved for ex20ins, Mobocertinib despite being a small molecule, appears to have a low brain penetrance, as shown by the worse confirmed objective response rate and high number of brain PD (25%) presented by the patients with brain metastasis comparing to the group without SNC disease, in the phase 1/2 trial.[103]
Due to its large molecular size, amivantamab is unlikely to cross the blood-brain barrier and expected to have poor activity to treat brain metastases, therfore its clinical use as a monotherapy may be limited in patients with brain metastases.[104] To address this challenge studies with combination therapies are ongoing, such as CHRYSALIS-2, assessing amivantamab and lazertinib versus lazertinib monotherapy in patients with EGFR-mutant non–small cell lung cancer, and will include patients with treated brain metastases.[105]
7. Response to immunotherapy and chemoimmunotherapy
With some exceptions within the group of exon 20 insertions, EGFR TKIs seem to be the best treatment option for uncommon EGFR mutation and recent data confirm a modest activity of immune checkpoint inhibitors.[18,106] This is probably due to tumor immune microenvironment of EGFR mutant NSCLC, associated with uninflamed characteristics, low PD-L1 expression/CD8+ TILs and low tumor mutational burden (TMB).[107,108] Interestingly some patients with smoking history and high PD-L1 expression,[109] even though harboring EGFR mutation, may benefit from treatment with ICIs, especially patients harboring uncommon mutations.[65,73,109]. Recently, an association between high PD-L1 expression and uncommon EGFR mutation has been shown (Figure 2) [73].
Moreover, a recent study demonstrated that treatment with EGFR-TKI may change tumor microenvironment, by increasing PD-L1 expression (Figure 3) and TMB, modifying CD8+/FOXP3 TILs and CD73 expression: the patients with high PD-L1 expression after TKI treatment achieved longer PFS in subsequent treatment with ICI (pembrolizumab or nivolumab), respectively 7.1 months vs. 1.7 months, with a p statistically significant of 0.0033.[110]
Focusing on ex20 mutations, a recent study showed that in this subgroup of patients is evident a tumor immune infiltration suggesting a role for ICI.[111] A retrospective study conducted on patients with EGFR mutant NSCLC who were treated with ICIs found that those with ex20ins had a better response rate, disease control rate, and progression-free survival than those with common EGFR mutations.[112] This could potentially be attributed to the fact that patients with uncommon mutations tend to have a higher tumor mutational burden (TMB).[106] On the contrary, patients who have acquired the T790M mutation have a poorer prognosis when treated with ICIs, as well as with a combination of ICIs and chemotherapy, compared to those with other acquired resistance mechanisms.[113] This is likely because patients with acquired resistance to TKIs (other than T790M) may exhibit higher levels of PD-L1.[113]
The majority of clinical trials with ICIs including oncogene addicted NSCLC did not report details about the type of EGFR mutations or uncommon mutations.[18] The immunotarget registry, where a considerable % of uncommon or compound mutations received ICIs, showed a response rate of 12%, median PFS and OS of 2.1 and 10 months respectively.[114] Higher PD-L1 expression and a better survival have been shown in some series in patients with uncommon compared to common mutations.[114] The hypothesis that patients with uncommon mutation and without T790M mutation could have a better response to ICIs was also supported by a retrospective analysis of Yamada et al: the mutation G719X and ex20ins significantly correlated with outcome.[115]
The combination of chemotherapy and immunotherapy seems to be more promising compared with the single agent immune checkpoint inhibitor in patients with EGFR mutant NSCLC even though previous series included only a small proportion of uncommon mutation.[113,116] The Impower 150 trial, with atezolizumab combined with carboplatin/paclitaxel/bevacizumab was associated with a better OS, compared with the same regimen without ICIs, for patients with EGFR mutations, including uncommon.[117,118] These data suggested that the combination could represent a therapeutic option in EGFR-mutated NSCLC. However recent results from the final analysis showed a loss of statistically significant OS.[119] One retrospective observational study exploring the efficacy of ICIs or ICIs in combination with chemotherapy in EGFR mutant NSCLC, included 13% of patients with uncommon EGFR mutation, in particular ex20ins, G719X, one L861Q.[113] The group of patients treated with ICIs, compared to chemotherapy plus ICIs, had a longer PFS although there was no significant difference in OS (Figure 4).[113] Recently a role for pembrolizumab was hypothesized in patients harboring G719X mutation and high PD-L1 expression (≥50%) although the small number of patients does not allow for conclusions to be drawn.[73]
8. How to define a treatment sequence
The treatment sequence should be defined considering first of all the resistance mechanisms and the available treatments for the subpopulation of EGFR mutant lung cancer. Acquired resistance mechanisms to first/second and third generation TKIs are different, mainly subclassified in the following three categories: mutations in target genes (on-target mutations), alternative pathway activation (off-target mutations) and histological transformation.[120] The resistance mechanism after PD to first and second generation TKIs are more commonly EGFR-dependent (i.e. T790M mutation, accounting for 50% of cases with acquired resistance to gefitinib or erlotinib, second-point mutations, such as D761Y, T854A, or L747S) while are more heterogeneous and EGFR-independent after Osimertinib (MET/HER2 amplification, activation of the MAPK or PI3K pathways).[59] Moreover, uncommon mutations may emerge within compound mutations as resistance mechanisms, driving treatment decision, switching to a different generation of TKIs. Finally, osimertinib seems to have the best safety profile compared to other TKIs, showing a lower incidence of grade 3 or 4 AEs compared to first or second generation TKIs.[121] With regard to afatinib, a systematic review and meta-analysis, showed that the second generation TKIs had a comparable rate grade 3 or 4 AEs respect to erlotinib, but greater than gefitinib.[122] This is confirmed by LUX-lung7 trial showing a greater rate of AEs of grade 3-4 but the overall incidence was comparable.[123]
In order to define the best treatment sequence in this setting we have to take in consideration the available survival data derived from the literature. Unfortunately we do not have randomized trials comparing second and third generations TKIs, however data from the GioTag study demonstrated that a sequence of second and third generation TKIs can achieve a clinically significant survival, although no uncommon mutation was included.[124]
A recent multicenter cohort study including a small subgroup of patients with uncommon EGFR mutations showed no survival difference in the overall population receiving afatinib compared with Osimertinib. At the subgroup analysis, a better outcome with Osimertinib was observed in particular in patients with brain metastases.[98] However emerging data, as already mentioned, suggest intracranial activity with second generation TKIs, in particular dacomitinib.[100,101]
9. Ongoing clinical trials
Probably the answer about the best treatment sequencing in patients harboring uncommon EGFR mutations may come from the ongoing phase II study CAPLAND (NCT04811001), exploring the best treatment sequencing of dacomitinib followed by or subsequent to osimertinib in patients NSCLC harboring classical or uncommon EGFR mutations; furthermore, the efficacy of dacomitinib will be defined in patients with brain metastases.
Among other EGFR TKIs lazertinib, a new third generation EGFR-TKI, is currently under investigation in combination with amivantamab a bispecific antibody targeting MET and EGFR, in the phase 1/1b CHRYSALIS-2 study, in patients with EGFR mutant NSCLC in progression on osimertinib. The cohort C of the study includes patients with uncommon mutations other than exon 20 insertion.[105]
The updated results presented at ASCO 2022 showed that the combination has a durable activity after progression on both chemotherapy and osimertinib[125]: the combination demonstrated an ORR of 33% with a median DOR of 9.6 months. The phase 3 trial MARIPOSA and MARIPOSA-2 are currently ongoing, evaluating amivantamab in combination with lazertinib as first line treatment and in combination with carboplatin and pemetrexed after PD to osimertinib.
10. Conclusions
The optimal treatment strategy for NSCLC patients harboring uncommon EGFR mutations remain an unmet medical need. In the next future, ongoing clinical trials will try to define the best therapeutic sequence in different subgroups of mutation. Currently, the best treatment pathway for affected patients should consider higher activity and efficacy data according to the specific type of uncommon mutations, the safety of the available drugs and finally the acquired resistance mechanisms.
Author Contributions
GPa: Conceptualization; Supervision; Validation, Writing - original draft; Writing - review and editing. GPr: Conceptualization; Writing - original draft preparation. MS, CCS and GC: Writing - review and editing. All authors contributed to the article and approved the submitted version.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Figure created in BioRender.com.
Conflicts of Interest
Not applicable.
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F.; Bsc, M.F.B.; Me, J.F.; Soerjomataram, M.I.; et al. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA: A Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Ciardiello, F.; Tortora, G. EGFR Antagonists in Cancer Treatment. N. Engl. J. Med. 2008, 358, 1160–1174. [Google Scholar] [CrossRef] [PubMed]
- Linardou, H.; Dahabreh, I.J.; Bafaloukos, D.; Kosmidis, P.; Murray, S. Somatic EGFR mutations and efficacy of tyrosine kinase inhibitors in NSCLC. Nat. Rev. Clin. Oncol. 2009, 6, 352–366. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.-L.; Yuan, J.-Q.; Wang, K.-F.; Fu, X.-H.; Han, X.-R.; Threapleton, D.; Yang, Z.-Y.; Mao, C.; Tang, J.-L. The prevalence of EGFR mutation in patients with non-small cell lung cancer: a systematic review and meta-analysis. Oncotarget 2016, 7, 78985–78993. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S.; Canepa, H.M.; Bailey, A.S.; Nakayama, S.; Yamaguchi, N.; Goldstein, M.A.; Huberman, M.S.; Costa, D.B. Compound EGFR Mutations and Response to EGFR Tyrosine Kinase Inhibitors. J. Thorac. Oncol. 2013, 8, 118–122. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, S. , et al., EGFR mutation and resistance of non-small-cell lung cancer to gefitinib. N Engl J Med 2005, 352, 786–792. [Google Scholar] [CrossRef]
- Westover, D.; Zugazagoitia, J.; Cho, B.C.; Lovly, C.M.; Paz-Ares, L. Mechanisms of acquired resistance to first- and second-generation EGFR tyrosine kinase inhibitors. Ann. Oncol. 2018, 29, i10–i19. [Google Scholar] [CrossRef]
- Evans, M.; O’sullivan, B.; Smith, M.; Hughes, F.; Mullis, T.; Trim, N.; Taniere, P. Large-Scale EGFR Mutation Testing in Clinical Practice: Analysis of a Series of 18,920 Non-Small Cell Lung Cancer Cases. Pathol. Oncol. Res. 2019, 25, 1401–1409. [Google Scholar] [CrossRef]
- John, T.; Taylor, A.; Wang, H.; Eichinger, C.; Freeman, C.; Ahn, M.-J. Uncommon EGFR mutations in non-small-cell lung cancer: A systematic literature review of prevalence and clinical outcomes. Cancer Epidemiology 2022, 76, 102080. [Google Scholar] [CrossRef]
- Wu, Y.-L.; Xu, C.-R.; Hu, C.-P.; Feng, J.; Lu, S.; Huang, Y.; Li, W.; Hou, M.; Shi, J.H.; Märten, A.; et al. Afatinib versus gemcitabine/cisplatin for first-line treatment of Chinese patients with advanced non-small-cell lung cancer harboring EGFR mutations: subgroup analysis of the LUX-Lung 6 trial. OncoTargets Ther. 2018, 11, 8575–8587. [Google Scholar] [CrossRef]
- Ho, G.-F.; Chai, C.-S.; Alip, A.; Wahid, M.I.A.; Abdullah, M.M.; Foo, Y.-C.; How, S.-H.; Zaatar, A.; Lam, K.-S.; Leong, K.-W.; et al. Real-world experience of first-line afatinib in patients with EGFR-mutant advanced NSCLC: a multicenter observational study. BMC Cancer 2019, 19, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Chang, G.-C.; Lam, D.C.-L.; Tsai, C.-M.; Chen, Y.-M.; Shih, J.-Y.; Aggarwal, S.; Wang, S.; Kim, S.-W.; Kim, Y.-C.; Wahid, I.; et al. Experience from Asian centers in a named-patient-use program for afatinib in patients with advanced non-small-cell lung cancer who had progressed following prior therapies, including patients with uncommon EGFR mutations. Int. J. Clin. Oncol. 2021, 26, 841–850. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.-H.; Sequist, L.V.; Geater, S.L.; Tsai, C.-M.; Mok, T.S.K.; Schuler, M.; Yamamoto, N.; Yu, C.-J.; I Ou, S.-H.; Zhou, C.; et al. Clinical activity of afatinib in patients with advanced non-small-cell lung cancer harbouring uncommon EGFR mutations: a combined post-hoc analysis of LUX-Lung 2, LUX-Lung 3, and LUX-Lung 6. Lancet Oncol. 2015, 16, 830–838. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; Mok, T.; Peters, S.; Popat, S.; Ahn, M.-J.; de Marinis, F. Recent Advances on the Role of EGFR Tyrosine Kinase Inhibitors in the Management of NSCLC With Uncommon, Non Exon 20 Insertions, EGFR Mutations. J. Thorac. Oncol. 2021, 16, 764–773. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; de Marinis, F.; Tu, H.-Y.; Laktionov, K.K.; Feng, J.; Poltoratskiy, A.; Zhao, J.; Tan, E.H.; Gottfried, M.; Lee, V.; et al. Afatinib in EGFR TKI-Naïve Patients with Locally Advanced or Metastatic EGFR Mutation-Positive Non-Small Cell Lung Cancer: A Pooled Analysis of Three Phase IIIb Studies. Front. Oncol. 2021, 11. [Google Scholar] [CrossRef] [PubMed]
- Popat, S.; Hsia, T.-C.; Hung, J.-Y.; Jung, H.A.; Shih, J.-Y.; Park, C.K.; Lee, S.H.; Okamoto, T.; Ahn, H.K.; Lee, Y.C.; et al. Tyrosine Kinase Inhibitor Activity in Patients with NSCLC Harboring Uncommon EGFR Mutations: A Retrospective International Cohort Study (UpSwinG). Oncol. 2022, 27, 255–265. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.-Y.; Ke, E.-E.; Yang, J.-J.; Sun, Y.-L.; Yan, H.-H.; Zheng, M.-Y.; Bai, X.-Y.; Wang, Z.; Su, J.; Chen, Z.-H.; et al. A comprehensive review of uncommon EGFR mutations in patients with non-small cell lung cancer. Lung Cancer 2017, 114, 96–102. [Google Scholar] [CrossRef]
- Russo, A.; Franchina, T.; Ricciardi, G.; Battaglia, A.; Picciotto, M.; Adamo, V. Heterogeneous Responses to Epidermal Growth Factor Receptor (EGFR) Tyrosine Kinase Inhibitors (TKIs) in Patients with Uncommon EGFR Mutations: New Insights and Future Perspectives in this Complex Clinical Scenario. Int. J. Mol. Sci. 2019, 20, 1431. [Google Scholar] [CrossRef]
- Gristina, V.; Malapelle, U.; Galvano, A.; Pisapia, P.; Pepe, F.; Rolfo, C.; Tortorici, S.; Bazan, V.; Troncone, G.; Russo, A. The significance of epidermal growth factor receptor uncommon mutations in non-small cell lung cancer: A systematic review and critical appraisal. Cancer Treat. Rev. 2020, 85, 101994. [Google Scholar] [CrossRef]
- Mehta, A.; Vasudevan, S. Rare epidermal growth factor receptor gene alterations in non-small cell lung cancer patients, tyrosine kinase inhibitor response and outcome analysis. Cancer Treat. Res. Commun. 2021, 28, 100398. [Google Scholar] [CrossRef]
- Graham, R.P.; Treece, A.L.; Lindeman, N.I.; Vasalos, P.; Shan, M.; Jennings, L.J.; Rimm, D.L. Worldwide Frequency of Commonly Detected EGFR Mutations. Arch. Pathol. Lab. Med. 2018, 142, 163–167. [Google Scholar] [CrossRef] [PubMed]
- Malapelle, U.; Pilotto, S.; Passiglia, F.; Pepe, F.; Pisapia, P.; Righi, L.; Listì, A.; Bironzo, P.; Belluomini, L.; Tabbò, F.; et al. Dealing with NSCLC EGFR mutation testing and treatment: A comprehensive review with an Italian real-world perspective. Crit. Rev. Oncol. 2021, 160, 103300. [Google Scholar] [CrossRef] [PubMed]
- Robichaux, J.P.; Le, X.; Vijayan, R.S.K.; Hicks, J.K.; Heeke, S.; Elamin, Y.Y.; Lin, H.Y.; Udagawa, H.; Skoulidis, F.; Tran, H.; et al. Structure-based classification predicts drug response in EGFR-mutant NSCLC. Nature 2021, 597, 732–737. [Google Scholar] [CrossRef] [PubMed]
- Sousa, A.; Silveira, C.; Janeiro, A.; Malveiro, S.; Oliveira, A.; Felizardo, M.; Nogueira, F.; Teixeira, E.; Martins, J.; Carmo-Fonseca, M. Detection of rare and novel EGFR mutations in NSCLC patients: Implications for treatment-decision. Lung Cancer 2020, 139, 35–40. [Google Scholar] [CrossRef] [PubMed]
- Ma, W.; Brodie, S.; Agersborg, S.; Funari, V.A.; Albitar, M. Significant Improvement in Detecting BRAF, KRAS, and EGFR Mutations Using Next-Generation Sequencing as Compared with FDA-Cleared Kits. Mol. Diagn. Ther. 2017, 21, 571–579. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Li, J.; Hua, P.; Liu, N.; Li, Q.; Zhu, X.; Jiang, L.; Zheng, K.; Su, X. Targeted next-generation sequencing in cytology specimens for molecular profiling of lung adenocarcinoma. 2018, 11, 3647–3655. [Google Scholar]
- Warth, A.; Penzel, R.; Brandt, R.; Sers, C.; Fischer, J.R.; Thomas, M.; Herth, F.J.F.; Dietel, M.; Schirmacher, P.; Bläker, H. Optimized algorithm for Sanger sequencing-based EGFR mutation analyses in NSCLC biopsies. Virchows Arch. 2012, 460, 407–414. [Google Scholar] [CrossRef]
- Liang, C.; Wu, Z.; Gan, X.; Liu, Y.; You, Y.; Liu, C.; Zhou, C.; Liang, Y.; Mo, H.; Chen, A.M.; et al. Detection of Rare Mutations inEGFR-ARMS-PCR-Negative Lung Adenocarcinoma by Sanger Sequencing. Yonsei Med J. 2018, 59, 13–19. [Google Scholar] [CrossRef]
- Mao, L.; Zhao, W.; Li, X.; Zhang, S.; Zhou, C.; Zhou, D.; Ou, X.; Xu, Y.; Tang, Y.; Ou, X.; et al. Mutation Spectrum of EGFR From 21,324 Chinese Patients With Non-Small Cell Lung Cancer (NSCLC) Successfully Tested by Multiple Methods in a CAP-Accredited Laboratory. Pathol. Oncol. Res. 2021, 27, 602726. [Google Scholar] [CrossRef]
- Siqueira, J.F.; Fouad, A.F.; Rôças, I.N. Pyrosequencing as a tool for better understanding of human microbiomes. J. Oral Microbiol. 2012, 4. [Google Scholar] [CrossRef]
- Kanagal-Shamanna, R. Digital PCR: Principles and Applications. Methods Mol Biol 2016, 1392, 43–50. [Google Scholar] [PubMed]
- Gu, J.; Zang, W.; Liu, B.; Li, L.; Huang, L.; Li, S.; Rao, G.; Yu, Y.; Zhou, Y. Evaluation of digital PCR for detecting low-level EGFR mutations in advanced lung adenocarcinoma patients: a cross-platform comparison study. Oncotarget 2017, 8, 67810–67820. [Google Scholar] [CrossRef] [PubMed]
- Li, B.; Janku, F.; Jung, B.; Hou, C.; Madwani, K.; Alden, R.; Razavi, P.; Reis-Filho, J.; Shen, R.; Isbell, J.; et al. Ultra-deep next-generation sequencing of plasma cell-free DNA in patients with advanced lung cancers: results from the Actionable Genome Consortium. Ann. Oncol. 2019, 30, 597–603. [Google Scholar] [CrossRef] [PubMed]
- Mosele, F.; Remon, J.; Mateo, J.; Westphalen, C.; Barlesi, F.; Lolkema, M.; Normanno, N.; Scarpa, A.; Robson, M.; Meric-Bernstam, F.; et al. Recommendations for the use of next-generation sequencing (NGS) for patients with metastatic cancers: a report from the ESMO Precision Medicine Working Group. Ann. Oncol. 2020, 31, 1491–1505. [Google Scholar] [CrossRef] [PubMed]
- Bauml, J.; Viteri, S.; Minchom, A.; Bazhenova, L.; Ou, S.; Schaffer, M.; Le Croy, N.; Riley, R.; Mahadevia, P.; Girard, N. FP07.12 Underdiagnosis of EGFR Exon 20 Insertion Mutation Variants: Estimates from NGS-based Real-World Datasets. J. Thorac. Oncol. 2021, 16, S208–S209. [Google Scholar] [CrossRef]
- Yenerall, P.; Kittler, R.; Minna, J. Structure-based classification of EGFR mutations informs inhibitor selection for lung cancer therapy. Cancer Cell 2021, 39, 1455–1457. [Google Scholar] [CrossRef]
- Kim, E.Y. , et al., Compound EGFR mutation is frequently detected with co-mutations of actionable genes and associated with poor clinical outcome in lung adenocarcinoma. Cancer Biol Ther 2016, 17, 237–245. [Google Scholar] [CrossRef]
- Suda, K.; Sakai, K.; Obata, K.; Ohara, S.; Fujino, T.; Koga, T.; Hamada, A.; Soh, J.; Nishio, K.; Mitsudomi, T. Inter- and Intratumor Heterogeneity of EGFR Compound Mutations in Non–Small Cell Lung Cancers: Analysis of Five Cases. Clin. Lung Cancer 2021, 22, e141–e145. [Google Scholar] [CrossRef]
- Roper, N.; Brown, A.-L.; Wei, J.S.; Pack, S.; Trindade, C.; Kim, C.; Restifo, O.; Gao, S.; Sindiri, S.; Mehrabadi, F.; et al. Clonal Evolution and Heterogeneity of Osimertinib Acquired Resistance Mechanisms in EGFR Mutant Lung Cancer. Cell Rep. Med. 2020, 1, 100007. [Google Scholar] [CrossRef]
- Chen, H.; Cheng, X. Tumor heterogeneity and resistance to EGFR-targeted therapy in advanced nonsmall cell lung cancer: challenges and perspectives. OncoTargets Ther. 2014, 7, 1689–1704. [Google Scholar] [CrossRef]
- Attili, I.; Passaro, A.; Pisapia, P.; Malapelle, U.; de Marinis, F. Uncommon EGFR Compound Mutations in Non-Small Cell Lung Cancer (NSCLC): A Systematic Review of Available Evidence. Curr. Oncol. 2022, 29, 255–266. [Google Scholar] [CrossRef] [PubMed]
- Yu, X. , et al., First-generation EGFR tyrosine kinase inhibitor therapy in 106 patients with compound EGFR-mutated lung cancer: a single institution's clinical practice experience. Cancer Commun (Lond) 2018, 38, 51. [Google Scholar] [PubMed]
- Hata, A.; Yoshioka, H.; Fujita, S.; Kunimasa, K.; Kaji, R.; Imai, Y.; Tomii, K.; Iwasaku, M.; Nishiyama, A.; Ishida, T.; et al. Complex Mutations in the Epidermal Growth Factor Receptor Gene in Non-small Cell Lung Cancer. J. Thorac. Oncol. 2010, 5, 1524–1528. [Google Scholar] [CrossRef] [PubMed]
- Xu, J.; Jin, B.; Chu, T.; Dong, X.; Yang, H.; Zhang, Y.; Wu, D.; Lou, Y.; Zhang, X.; Wang, H.; et al. EGFR tyrosine kinase inhibitor (TKI) in patients with advanced non-small cell lung cancer (NSCLC) harboring uncommon EGFR mutations: A real-world study in China. Lung Cancer 2016, 96, 87–92. [Google Scholar] [CrossRef] [PubMed]
- Lund-Iversen, M.; Kleinberg, L.; Fjellbirkeland, L.; Helland. ; Brustugun, O.T. Clinicopathological Characteristics of 11 NSCLC Patients with EGFR-Exon 20 Mutations. J. Thorac. Oncol. 2012, 7, 1471–1473. [Google Scholar] [CrossRef] [PubMed]
- Klughammer, B.; Brugger, W.; Cappuzzo, F.; Ciuleanu, T.; Mok, T.; Reck, M.; Tan, E.H.; Delmar, P.; Klingelschmitt, G.; Yin, A.-Y.; et al. Examining Treatment Outcomes with Erlotinib in Patients with Advanced Non–Small Cell Lung Cancer Whose Tumors Harbor Uncommon EGFR Mutations. J. Thorac. Oncol. 2016, 11, 545–555. [Google Scholar] [CrossRef] [PubMed]
- Zhang, R.; Tian, P.; Chen, B.; Wang, T.; Li, W. The prognostic impact of TP53 comutation in EGFR mutant lung cancer patients: a systematic review and meta-analysis. Postgrad. Med. 2019, 131, 199–206. [Google Scholar] [CrossRef] [PubMed]
- Guo, Y.; Song, J.; Wang, Y.; Huang, L.; Sun, L.; Zhao, J.; Zhang, S.; Jing, W.; Ma, J.; Han, C. Concurrent Genetic Alterations and Other Biomarkers Predict Treatment Efficacy of EGFR-TKIs in EGFR-Mutant Non-Small Cell Lung Cancer: A Review. Front. Oncol. 2020, 10, 610923. [Google Scholar] [CrossRef]
- Shah, R.; Lester, J.F. Tyrosine Kinase Inhibitors for the Treatment of EGFR Mutation-Positive Non–Small-Cell Lung Cancer: A Clash of the Generations. Clin. Lung Cancer 2020, 21, e216–e228. [Google Scholar] [CrossRef]
- Alanazi, A.; Yunusa, I.; Elenizi, K.; I Alzarea, A. Efficacy and safety of tyrosine kinase inhibitors in advanced non-small-cell lung cancer harboring epidermal growth factor receptor mutation: a network meta-analysis. Lung Cancer Manag. 2021, 10, LMT43. [Google Scholar] [CrossRef]
- Reck, M.; van Zandwijk, N.; Gridelli, C.; Baliko, Z.; Rischin, D.; Allan, S.; Krzakowski, M.; Heigener, D. Erlotinib in Advanced Non-small Cell Lung Cancer: Efficacy and Safety Findings of the Global Phase IV Tarceva Lung Cancer Survival Treatment Study. J. Thorac. Oncol. 2010, 5, 1616–1622. [Google Scholar] [CrossRef] [PubMed]
- Shepherd, F.A.; Rodrigues Pereira, J.; Ciuleanu, T.E.; Tan, E.H.; Hirsh, V.; Thongprasert, S.; Campos, D.; Maoleekoonpiroj, S.; Smylie, M.; Martins, R.; et al. Erlotinib in Previously Treated Non–Small-Cell Lung Cancer. N. Engl. J. Med. 2005, 353, 123–132. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C.; Wu, Y.-L.; Chen, G.; Feng, J.; Liu, X.-Q.; Wang, C.; Zhang, S.; Wang, J.; Zhou, S.; Ren, S.; et al. Erlotinib versus chemotherapy as first-line treatment for patients with advanced EGFR mutation-positive non-small-cell lung cancer (OPTIMAL, CTONG-0802): a multicentre, open-label, randomised, phase 3 study. Lancet Oncol. 2011, 12, 735–742. [Google Scholar] [CrossRef] [PubMed]
- Douillard, J.-Y.; Ostoros, G.; Cobo, M.; Ciuleanu, T.; McCormack, R.; Webster, A.; Milenkova, T. First-line gefitinib in Caucasian EGFR mutation-positive NSCLC patients: a phase-IV, open-label, single-arm study. Br. J. Cancer 2014, 110, 55–62. [Google Scholar] [CrossRef] [PubMed]
- Inoue, A.; Kobayashi, K.; Usui, K.; Maemondo, M.; Okinaga, S.; Mikami, I.; Ando, M.; Yamazaki, K.; Saijo, Y.; Gemma, A.; et al. First-Line Gefitinib for Patients With Advanced Non–Small-Cell Lung Cancer Harboring Epidermal Growth Factor Receptor Mutations Without Indication for Chemotherapy. J. Clin. Oncol. 2009, 27, 1394–1400. [Google Scholar] [CrossRef] [PubMed]
- Mok, T.S.; Wu, Y.-L.; Thongprasert, S.; Yang, C.-H.; Chu, D.-T.; Saijo, N.; Sunpaweravong, P.; Han, B.; Margono, B.; Ichinose, Y.; et al. Gefitinib or Carboplatin–Paclitaxel in Pulmonary Adenocarcinoma. N. Engl. J. Med. 2009, 361, 947–957. [Google Scholar] [CrossRef] [PubMed]
- Wu, Y.-L.; Cheng, Y.; Zhou, X.; Lee, K.H.; Nakagawa, K.; Niho, S.; Tsuji, F.; Linke, R.; Rosell, R.; Corral, J.; et al. Dacomitinib versus gefitinib as first-line treatment for patients with EGFR-mutation-positive non-small-cell lung cancer (ARCHER 1050): a randomised, open-label, phase 3 trial. Lancet Oncol. 2017, 18, 1454–1466. [Google Scholar] [CrossRef] [PubMed]
- Paz-Ares, L.; Tan, E.-H.; O’byrne, K.; Zhang, L.; Hirsh, V.; Boyer, M.; Yang, J.-H.; Mok, T.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib in patients with EGFR mutation-positive advanced non-small-cell lung cancer: overall survival data from the phase IIb LUX-Lung 7 trial. Ann. Oncol. 2017, 28, 270–277. [Google Scholar] [CrossRef]
- Leonetti, A.; Sharma, S.; Minari, R.; Perego, P.; Giovannetti, E.; Tiseo, M. Resistance mechanisms to osimertinib in EGFR-mutated non-small cell lung cancer. Br. J. Cancer 2019, 121, 725–737. [Google Scholar] [CrossRef]
- Cho, J.H. , et al., Osimertinib for Patients With Non-Small-Cell Lung Cancer Harboring Uncommon EGFR Mutations: A Multicenter, Open-Label, Phase II Trial (KCSG-LU15-09). J Clin Oncol 2020, 38, 488–495. [Google Scholar] [CrossRef]
- Janning, M.; Süptitz, J.; Albers-Leischner, C.; Delpy, P.; Tufman, A.; Velthaus-Rusik, J.-L.; Reck, M.; Jung, A.; Kauffmann-Guerrero, D.; Bonzheim, I.; et al. Treatment outcome of atypical EGFR mutations in the German National Network Genomic Medicine Lung Cancer (nNGM). Ann. Oncol. 2022, 33, 602–615. [Google Scholar] [CrossRef] [PubMed]
- Li, H.; Wang, C.; Wang, Z.; Hu, Y.; Zhang, G.; Zhang, M.; Zheng, X.; Zhang, X.; Yang, J.; Ma, Z.; et al. Efficacy and long-term survival of advanced lung adenocarcinoma patients with uncommon EGFR mutations treated with 1st generation EGFR-TKIs compared with chemotherapy as first-line therapy. Lung Cancer 2019, 130, 42–49. [Google Scholar] [CrossRef] [PubMed]
- Tu, H.Y. , et al., A Phase IIIb Open-Label, Single-Arm Study of Afatinib in EGFR TKI-Naive Patients with EGFRm+ NSCLC: Final Analysis, with a Focus on Patients Enrolled at Sites in China. Target Oncol 2022, 17, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Yang, J.C.-H.; Schuler, M.; Popat, S.; Miura, S.; Heeke, S.; Park, K.; Märten, A.; Kim, E.S. Afatinib for the Treatment of NSCLC Harboring Uncommon EGFR Mutations: A Database of 693 Cases. J. Thorac. Oncol. 2020, 15, 803–815. [Google Scholar] [CrossRef] [PubMed]
- Yamada, Y. , et al., Treatment of Patients With Non-small-cell Lung Cancer With Uncommon EGFR Mutations in Clinical Practice. Anticancer Res 2020, 40, 5757–5764. [Google Scholar] [CrossRef] [PubMed]
- UPDATES, F. , New Indication Approved for Afatinib in NSCLC. Oncology Times 2018, 40, 18. [Google Scholar]
- Floc'H, N.; Lim, S.; Bickerton, S.; Ahmed, A.; Orme, J.; Urosevic, J.; Martin, M.J.; Cross, D.A.; Cho, B.C.; Smith, P.D. Osimertinib, an Irreversible Next-Generation EGFR Tyrosine Kinase Inhibitor, Exerts Antitumor Activity in Various Preclinical NSCLC Models Harboring the Uncommon EGFR Mutations G719X or L861Q or S768I. Mol. Cancer Ther. 2020, 19, 2298–2307. [Google Scholar] [CrossRef] [PubMed]
- Ji, J.; Aredo, J.V.; Piper-Vallillo, A.; Huppert, L.; Rotow, J.K.; Husain, H.; Stewart, S.; Cobb, R.; Wakelee, H.A.; Blakely, C.M.; et al. Osimertinib in NSCLC With Atypical EGFR-Activating Mutations: A Retrospective Multicenter Study. JTO Clin. Res. Rep. 2023, 4, 100459. [Google Scholar] [CrossRef]
- Sequist, L.V. , et al., Neratinib, an irreversible pan-ErbB receptor tyrosine kinase inhibitor: results of a phase II trial in patients with advanced non-small-cell lung cancer. J Clin Oncol 2010, 28, 3076–83. [Google Scholar] [CrossRef]
- Heigener, D.F.; Schumann, C.; Sebastian, M.; Sadjadian, P.; Stehle, I.; Märten, A.; Lüers, A.; Griesinger, F.; Scheffler, M. ; for the Afatinib Compassionate Use Consortium (ACUC) Afatinib in Non-Small Cell Lung Cancer Harboring Uncommon EGFR Mutations Pretreated With Reversible EGFR Inhibitors. Oncol. 2015, 20, 1167–1174. [Google Scholar] [CrossRef]
- Costa, D.B.; B. , D. Kinase inhibitor-responsive genotypes in EGFR mutated lung adenocarcinomas: moving past common point mutations or indels into uncommon kinase domain duplications and rearrangements. Transl. Lung Cancer Res. 2016, 5, 331–337. [Google Scholar] [CrossRef] [PubMed]
- Kobayashi, Y. , et al., EGFR Exon 18 Mutations in Lung Cancer: Molecular Predictors of Augmented Sensitivity to Afatinib or Neratinib as Compared with First- or Third-Generation TKIs. Clin Cancer Res 2015, 21, 5305–5313. [Google Scholar] [CrossRef] [PubMed]
- Taniguchi, Y.; Takeda, M.; Tamiya, A.; Kasai, T.; Atagi, S. Programmed death-ligand 1 expression in uncommon epidermal growth factor receptor mutation-positive non-small-cell lung cancer. Ann. Oncol. 2018, 29, 2262–2263. [Google Scholar] [CrossRef] [PubMed]
- Chung, K.P. , et al., Clinical outcomes in non-small cell lung cancers harboring different exon 19 deletions in EGFR. Clin Cancer Res 2012, 18, 3470–3477. [Google Scholar] [CrossRef]
- Peng, X.; Long, X.; Liu, L.; Zeng, L.; Yang, H.; Jiang, W.; Liao, D.; Li, K.; Wang, J.; Lizaso, A.; et al. Clinical impact of uncommon epidermal growth factor receptor exon 19 insertion-deletion variants on epidermal growth factor receptor-tyrosine kinase inhibitor efficacy in non-small-cell lung cancer. Eur. J. Cancer 2020, 141, 199–208. [Google Scholar] [CrossRef] [PubMed]
- He, M. , et al., EGFR exon 19 insertions: a new family of sensitizing EGFR mutations in lung adenocarcinoma. Clin Cancer Res 2012, 18, 1790–1797. [Google Scholar] [CrossRef] [PubMed]
- Passaro, A.; Leighl, N.; Blackhall, F.; Popat, S.; Kerr, K.; Ahn, M.; Arcila, M.; Arrieta, O.; Planchard, D.; de Marinis, F.; et al. ESMO expert consensus statements on the management of EGFR mutant non-small-cell lung cancer. Ann. Oncol. 2022, 33, 466–487. [Google Scholar] [CrossRef]
- Vyse, S.; Huang, P.H. Targeting EGFR exon 20 insertion mutations in non-small cell lung cancer. Signal Transduct. Target. Ther. 2019, 4, 51. [Google Scholar] [CrossRef]
- Vasconcelos, P.E.; Gergis, C.; Viray, H.; Varkaris, A.; Fujii, M.; Rangachari, D.; VanderLaan, P.A.; Kobayashi, I.S.; Kobayashi, S.S.; Costa, D.B. EGFR-A763_Y764insFQEA Is a Unique Exon 20 Insertion Mutation That Displays Sensitivity to Approved and In-Development Lung Cancer EGFR Tyrosine Kinase Inhibitors. JTO Clin. Res. Rep. 2020, 1. [Google Scholar] [CrossRef]
- Hasegawa, H.; Yasuda, H.; Hamamoto, J.; Masuzawa, K.; Tani, T.; Nukaga, S.; Hirano, T.; Kobayashi, K.; Manabe, T.; Terai, H.; et al. Efficacy of afatinib or osimertinib plus cetuximab combination therapy for non-small-cell lung cancer with EGFR exon 20 insertion mutations. Lung Cancer 2018, 127, 146–152. [Google Scholar] [CrossRef]
- Elamin, Y.Y.; Robichaux, J.P.; Carter, B.W.; Altan, M.; Gibbons, D.L.; Fossella, F.V.; Lam, V.K.; Patel, A.B.; Negrao, M.V.; Le, X.; et al. Poziotinib for Patients With HER2 Exon 20 Mutant Non–Small-Cell Lung Cancer: Results From a Phase II Trial. J. Clin. Oncol. 2022, 40, 702–709. [Google Scholar] [CrossRef] [PubMed]
- Elamin, Y.Y.; Robichaux, J.P.; Carter, B.W.; Altan, M.; Tran, H.; Gibbons, D.L.; Heeke, S.; Fossella, F.V.; Lam, V.K.; Le, X.; et al. Poziotinib for EGFR exon 20-mutant NSCLC: Clinical efficacy, resistance mechanisms, and impact of insertion location on drug sensitivity. Cancer Cell 2022, 40, 754–767. [Google Scholar] [CrossRef] [PubMed]
- Prelaj, A.; Bottiglieri, A.; Proto, C.; Russo, G.L.; Signorelli, D.; Ferrara, R.; Galli, G.; De Toma, A.; Viscardi, G.; Brambilla, M.; et al. Poziotinib for EGFR and HER2 exon 20 insertion mutation in advanced NSCLC: Results from the expanded access program. Eur. J. Cancer 2021, 149, 235–248. [Google Scholar] [CrossRef] [PubMed]
- Zhou, C. , et al., Treatment Outcomes and Safety of Mobocertinib in Platinum-Pretreated Patients With EGFR Exon 20 Insertion-Positive Metastatic Non-Small Cell Lung Cancer: A Phase 1/2 Open-label Nonrandomized Clinical Trial. JAMA Oncol 2021, 7, e214761. [Google Scholar] [CrossRef] [PubMed]
- FDA. EDA grants accelerated approval to mobocertinib for metastatic non-small cell lung cancer with EGFR exon 20 insertion mutations. 2022 , 2022]; Available from: https://www.fda.gov/drugs/resources-information-approved-drugs/fda-grants-accelerated-approval-mobocertinib-metastatic-non-small-cell-lung-cancer-egfr-exon-20. 10 April.
- FDA. FDA Approves First Targeted Therapy for Subset of Non-Small Cell Lung Cancer. 2022 Accessed , 2022]; Available from: https://www.fda.gov/news-events/press-announcements/fda-approves-first-targeted-therapy-subset-non-small-cell-lung-cancer. 10 April.
- Agency, E.M. Rybrevant. 2022 , 2022]; Available from: https://www.ema.europa.eu/en/medicines/human/EPAR/rybrevant. 10 April.
- Park, K.; Haura, E.B.; Leighl, N.B.; Mitchell, P.; Shu, C.A.; Girard, N.; Viteri, S.; Han, J.-Y.; Kim, S.-W.; Lee, C.K.; et al. Amivantamab in EGFR Exon 20 Insertion–Mutated Non–Small-Cell Lung Cancer Progressing on Platinum Chemotherapy: Initial Results From the CHRYSALIS Phase I Study. J. Clin. Oncol. 2021, 39, 3391–3402. [Google Scholar] [CrossRef] [PubMed]
- Park, K.; Sabari, J.K.; Haura, E.B.; Shu, C.A.; Spira, A.; Salgia, R.; Reckamp, K.L.; Sanborn, R.E.; Govindan, R.; Bauml, J.M.; et al. Management of infusion-related reactions (IRRs) in patients receiving amivantamab in the CHRYSALIS study. Lung Cancer 2023, 178, 166–171. [Google Scholar] [CrossRef] [PubMed]
- Janne, P.; Wang, M.; Mitchell, P.; Fang, J.; Nian, W.; Chiu, C.; Zhou, J.; Zhao, Y.; Su, W.; Camidge, D.; et al. OA15.02 Phase 1 Studies of DZD9008, an Oral Selective EGFR/HER2 Inhibitor in Advanced NSCLC with EGFR Exon20 Insertion Mutations. J. Thorac. Oncol. 2021, 18, S874. [Google Scholar] [CrossRef]
- Piotrowska, Z.; Nguyen, D.; Koczywas, M.; Tchekmedyian, N.; Clancy, M.; Witter, D.; Page, A.; Zawel, L.; Yu, H. 1345P Preliminary safety and activity of CLN-081 in NSCLC with EGFR exon 20 insertion mutations (Ins20). Annals of Oncology 2020, 31 (Suppl. S4), S754–S840. [Google Scholar] [CrossRef]
- S. V. Liu, L.C.V., V.H.F. Lee, V.W. Zhu, C.S. Baik, A. Sacher, C.E. McCoach, D. Nguyen, J.Y. Li, J.M. Pacheco, C. Kim, T.F. Burns, E.L. Schenk, N. Leighl, L. Tozzi, D.R. Camidge, LBA61 - First analysis of RAIN-701: Study of tarloxotinib in patients with non-small cell lung cancer (NSCLC) EGFR Exon 20 insertion, HER2-activating mutations & other solid tumours with NRG1/ERBB gene fusions. Annals of Oncology 2020, 31 (suppl_4), S1142–S1215. [Google Scholar]
- De Pas, T.; Toffalorio, F.; Manzotti, M.; Fumagalli, C.; Spitaleri, G.; Catania, C.; Delmonte, A.; Giovannini, M.; Spaggiari, L.; de Braud, F.; et al. Activity of Epidermal Growth Factor Receptor-Tyrosine Kinase Inhibitors in Patients with Non-small Cell Lung Cancer Harboring Rare Epidermal Growth Factor Receptor Mutations. J. Thorac. Oncol. 2011, 6, 1895–1901. [Google Scholar] [CrossRef]
- Galli, G.; Corrao, G.; Imbimbo, M.; Proto, C.; Signorelli, D.; Ganzinelli, M.; Zilembo, N.; Vitali, M.; de Braud, F.; Garassino, M.C.; et al. Uncommon mutations in epidermal growth factor receptor and response to first and second generation tyrosine kinase inhibitors: A case series and literature review. Lung Cancer 2018, 115, 135–142. [Google Scholar] [CrossRef] [PubMed]
- Massarelli, E.; Johnson, F.M.; Erickson, H.S.; Wistuba, I.I.; Papadimitrakopoulou, V. Uncommon Epidermal Growth Factor Receptor mutations in non-small cell lung cancer and their mechanisms of EGFR tyrosine kinase inhibitors sensitivity and resistance. Lung Cancer 2013, 80, 235–241. [Google Scholar] [CrossRef] [PubMed]
- Zeng, Y.; Guo, T.; Zhou, Y.; Zhao, Y.; Chu, L.; Chu, X.; Yang, X.; Ni, J.; Zhu, Z. Clinical outcomes of advanced non-small cell lung cancer patients harboring distinct subtypes of EGFR mutations and receiving first-line tyrosine kinase inhibitors: brain metastasis and de novo T790M matters. BMC Cancer 2022, 22, 1–11. [Google Scholar] [CrossRef] [PubMed]
- Soria, J.C. , et al. Osimertinib in Untreated EGFR-Mutated Advanced Non-Small-Cell Lung Cancer. N Engl J Med. 2018, 378, 113–125. [Google Scholar] [CrossRef] [PubMed]
- Ito, K.; Morise, M.; Wakuda, K.; Hataji, O.; Shimokawaji, T.; Takahashi, K.; Furuya, N.; Takeyama, Y.; Goto, Y.; Abe, T.; et al. A multicenter cohort study of osimertinib compared with afatinib as first-line treatment for EGFR-mutated non-small-cell lung cancer from practical dataset: CJLSG1903. ESMO Open 2021, 6, 100115. [Google Scholar] [CrossRef] [PubMed]
- Ma, C.; Zhang, J.; Tang, D.; Ye, X.; Li, J.; Mu, N.; Li, Z.; Liu, R.; Xiang, L.; Huang, C.; et al. Tyrosine Kinase Inhibitors Could Be Effective Against Non-small Cell Lung Cancer Brain Metastases Harboring Uncommon EGFR Mutations. Front. Oncol. 2020, 10, 224. [Google Scholar] [CrossRef] [PubMed]
- Zhang, J.; Wang, Y.; Liu, Z.; Wang, L.; Yao, Y.; Liu, Y.; Hao, X.Z.; Wang, J.; Xing, P.; Li, J. Efficacy of dacomitinib in patients with EGFR-mutated NSCLC and brain metastases. Thorac. Cancer 2021, 12, 3407–3415. [Google Scholar] [CrossRef] [PubMed]
- Peng, W.; Pu, X.; Jiang, M.; Wang, J.; Li, J.; Li, K.; Xu, Y.; Xu, F.; Chen, B.; Wang, Q.; et al. Dacomitinib induces objective responses in metastatic brain lesions of patients with EGFR-mutant non-small-cell lung cancer: A brief report. Lung Cancer 2021, 152, 66–70. [Google Scholar] [CrossRef]
- CLN-081 Produces Antitumor Activity With Acceptable Safety in Heavily Pretreated EGFR Exon 20 Insertion+ NSCLC. 2022; Available from: https://www.onclive.com/view/cln-081-produces-antitumor-activity-with-acceptable-safety-in-heavily-pretreated-egfr-exon-20-insertion-nsclc.
- Janne, P.A.; Ramalingam, S.S.; Yang, J.C.-H.; Riely, G.J.; Bunn, V.; Jin, S.; Zhou, C.; Camidge, D.R. Mobocertinib (TAK-788) in EGFR exon 20 insertion (ex20ins)+ metastatic non–small cell lung cancer (mNSCLC): Treatment (tx) beyond progressive disease (PD) in platinum-pretreated patients (pts) with and without intracranial PD. J. Clin. Oncol. 2022, 40, 9099–9099. [Google Scholar] [CrossRef]
- Vyse, S. and P.H. Huang, Amivantamab for the treatment of EGFR exon 20 insertion mutant non-small cell lung cancer. Expert Rev Anticancer Ther 2022, 22, 3–16. [Google Scholar] [CrossRef]
- Catherine, A. Shu, K.G., Byoung Chul Cho, Frank Griesinger, James Chih-Hsin Yang, Enriqueta Felip, John Xie, Jun Chen, Janine Mahoney, Meena Thayu, Roland Elmar Knoblauch, Leonardo Trani, Joshua Bauml, CHRYSALIS-2: A phase 1/1b study of lazertinib as monotherapy and in combination with amivantamab in patients with EGFR-mutant NSCLC. J Clin Oncol 2021, 39. [Google Scholar]
- Hastings, K.; Yu, H.; Wei, W.; Sanchez-Vega, F.; DeVeaux, M.; Choi, J.; Rizvi, H.; Lisberg, A.; Truini, A.; Lydon, C.; et al. EGFR mutation subtypes and response to immune checkpoint blockade treatment in non-small-cell lung cancer. Ann. Oncol. 2019, 30, 1311–1320. [Google Scholar] [CrossRef] [PubMed]
- Dong, Z.-Y.; Zhang, J.-T.; Liu, S.-Y.; Su, J.; Zhang, C.; Xie, Z.; Zhou, Q.; Tu, H.-Y.; Xu, C.-R.; Yan, L.-X.; et al. EGFR mutation correlates with uninflamed phenotype and weak immunogenicity, causing impaired response to PD-1 blockade in non-small cell lung cancer. OncoImmunology 2017, 6, e1356145. [Google Scholar] [CrossRef] [PubMed]
- Kapoor, S.S.; Zaiss, D.M.W. Emerging Role of EGFR Mutations in Creating an Immune Suppressive Tumour Microenvironment. Biomedicines 2021, 10, 52. [Google Scholar] [CrossRef] [PubMed]
- Garassino, M.C.; Cho, B.-C.; Kim, J.-H.; Mazières, J.; Vansteenkiste, J.; Lena, H.; Jaime, J.C.; Gray, J.E.; Powderly, J.; Chouaid, C.; et al. Durvalumab as third-line or later treatment for advanced non-small-cell lung cancer (ATLANTIC): an open-label, single-arm, phase 2 study. Lancet Oncol. 2018, 19, 521–536. [Google Scholar] [CrossRef]
- Isomoto, K.; Haratani, K.; Hayashi, H.; Shimizu, S.; Tomida, S.; Niwa, T.; Yokoyama, T.; Fukuda, Y.; Chiba, Y.; Kato, R.; et al. Impact of EGFR-TKI Treatment on the Tumor Immune Microenvironment in EGFR Mutation–Positive Non–Small Cell Lung Cancer. Clin. Cancer Res. 2020, 26, 2037–2046. [Google Scholar] [CrossRef]
- Kirchner, M.; Kluck, K.; Brandt, R.; Volckmar, A.-L.; Penzel, R.; Kazdal, D.; Endris, V.; Neumann, O.; Seker-Cin, H.; Goldschmid, H.; et al. The immune microenvironment in EGFR- and ERBB2-mutated lung adenocarcinoma. ESMO Open 2021, 6, 100253. [Google Scholar] [CrossRef]
- Lau, S.C.; Fares, A.F.; Le, L.W.; Mackay, K.M.; Soberano, S.; Chan, S.W.; Smith, E.; Ryan, M.; Tsao, M.S.; Bradbury, P.A.; et al. Subtypes of EGFR- and HER2-Mutant Metastatic NSCLC Influence Response to Immune Checkpoint Inhibitors. Clin. Lung Cancer 2021, 22, 253–259. [Google Scholar] [CrossRef]
- Shen, C.-I.; Chao, H.-S.; Shiao, T.-H.; Chiang, C.-L.; Huang, H.-C.; Luo, Y.-H.; Chiu, C.-H.; Chen, Y.-M. Comparison of the outcome between immunotherapy alone or in combination with chemotherapy in EGFR-mutant non-small cell lung cancer. Sci. Rep. 2021, 11, 1–9. [Google Scholar] [CrossRef]
- Mazieres, J.; Drilon, A.; Lusque, A.B.; Mhanna, L.; Cortot, A.; Mezquita, L.; Thai, A.A.; Mascaux, C.; Couraud, S.; Veillon, R.; et al. Immune checkpoint inhibitors for patients with advanced lung cancer and oncogenic driver alterations: results from the IMMUNOTARGET registry. Ann. Oncol. 2019, 30, 1321–1328. [Google Scholar] [CrossRef]
- Yamada, T.; Hirai, S.; Katayama, Y.; Yoshimura, A.; Shiotsu, S.; Watanabe, S.; Kikuchi, T.; Hirose, K.; Kubota, Y.; Chihara, Y.; et al. Retrospective efficacy analysis of immune checkpoint inhibitors in patients with EGFR-mutated non-small cell lung cancer. Cancer Med. 2019, 8, 1521–1529. [Google Scholar] [CrossRef] [PubMed]
- Kuo, C.-H.S.; Wang, C.-C.; Huang, Y.-C.; Pavlidis, S.; Liu, C.-Y.; Ko, H.-W.; Chung, F.-T.; Lin, T.-Y.; Wang, C.-L.; Guo, Y.-K.; et al. Comparison of a combination of chemotherapy and immune checkpoint inhibitors and immune checkpoint inhibitors alone for the treatment of advanced and metastatic non-small cell lung cancer. Thorac. Cancer 2019, 10, 1158–1166. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Mok, T.S.K.; Nishio, M.; Jotte, R.M.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodríguez-Abreu, D.; Moro-Sibilot, D.; et al. Atezolizumab plus bevacizumab and chemotherapy in non-small-cell lung cancer (IMpower150): key subgroup analyses of patients with EGFR mutations or baseline liver metastases in a randomised, open-label phase 3 trial. Lancet Respir. Med. 2019, 7, 387–401. [Google Scholar] [CrossRef] [PubMed]
- Reck, M.; Mok, T.; Socinski, M.; Jotte, R.; Lim, D.-T.; Cappuzzo, F.; Orlandi, F.; Stroyakovskiy, D.; Nogami, N.; Rodriguez-Abreu, D.; et al. 1293P IMpower150: Updated efficacy analysis in patients with EGFR mutations. Annals of Oncology 2020, 31 (Suppl. S4), S754–S840. [Google Scholar] [CrossRef]
- Nogami, N.; Barlesi, F.; Socinski, M.A.; Reck, M.; Thomas, C.A.; Cappuzzo, F.; Mok, T.S.; Finley, G.; Aerts, J.G.; Orlandi, F.; et al. IMpower150 Final Exploratory Analyses for Atezolizumab Plus Bevacizumab and Chemotherapy in Key NSCLC Patient Subgroups With EGFR Mutations or Metastases in the Liver or Brain. J. Thorac. Oncol. 2021, 17, 309–323. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.-G.; Shih, J.-Y. Management of acquired resistance to EGFR TKI–targeted therapy in advanced non-small cell lung cancer. Mol. Cancer 2018, 17, 1–14. [Google Scholar] [CrossRef] [PubMed]
- Zhou, J.-Y.; Liu, S.-Y.; Wu, Y.-L. Safety of EGFR-TKIs for EGFR mutation-positive non-small cell lung cancer. Expert Opin. Drug Saf. 2020, 19, 589–599. [Google Scholar] [CrossRef] [PubMed]
- Yang, Z. , et al., Comparison of gefitinib, erlotinib and afatinib in non-small cell lung cancer: A meta-analysis. Int J Cancer 2017, 140, 2805–2819. [Google Scholar] [CrossRef]
- Park, K.; Tan, E.-H.; O'Byrne, K.; Zhang, L.; Boyer, M.; Mok, T.; Hirsh, V.; Yang, J.C.-H.; Lee, K.H.; Lu, S.; et al. Afatinib versus gefitinib as first-line treatment of patients with EGFR mutation-positive non-small-cell lung cancer (LUX-Lung 7): a phase 2B, open-label, randomised controlled trial. Lancet Oncol. 2016, 17, 577–589. [Google Scholar] [CrossRef]
- Hochmair, M.J.; Morabito, A.; Hao, D.; Yang, C.-T.; A Soo, R.; Yang, J.C.-H.; Gucalp, R.; Halmos, B.; Wang, L.; Märten, A.; et al. Sequential afatinib and osimertinib in patients with EGFR mutation-positive non-small-cell lung cancer: updated analysis of the observational GioTag study. Futur. Oncol. 2019, 15, 2905–2914. [Google Scholar] [CrossRef]
- Options, C.C. CHRYSALIS-2: Update of Amivantamab + Lazertinib in EGFR-Mutant NSCLC After Progression on Osimertinib and Chemotherapy. 2022; Available from: https://clinicaloptions.com/CE-CME/chrysalis-2-update/100003234.
Figure 1.
Simplification of the tertiary structure of EGFR; C-terminal and N-terminal, αC-helix, p-loop. EGF: epidermal growth factor.
Figure 1.
Simplification of the tertiary structure of EGFR; C-terminal and N-terminal, αC-helix, p-loop. EGF: epidermal growth factor.
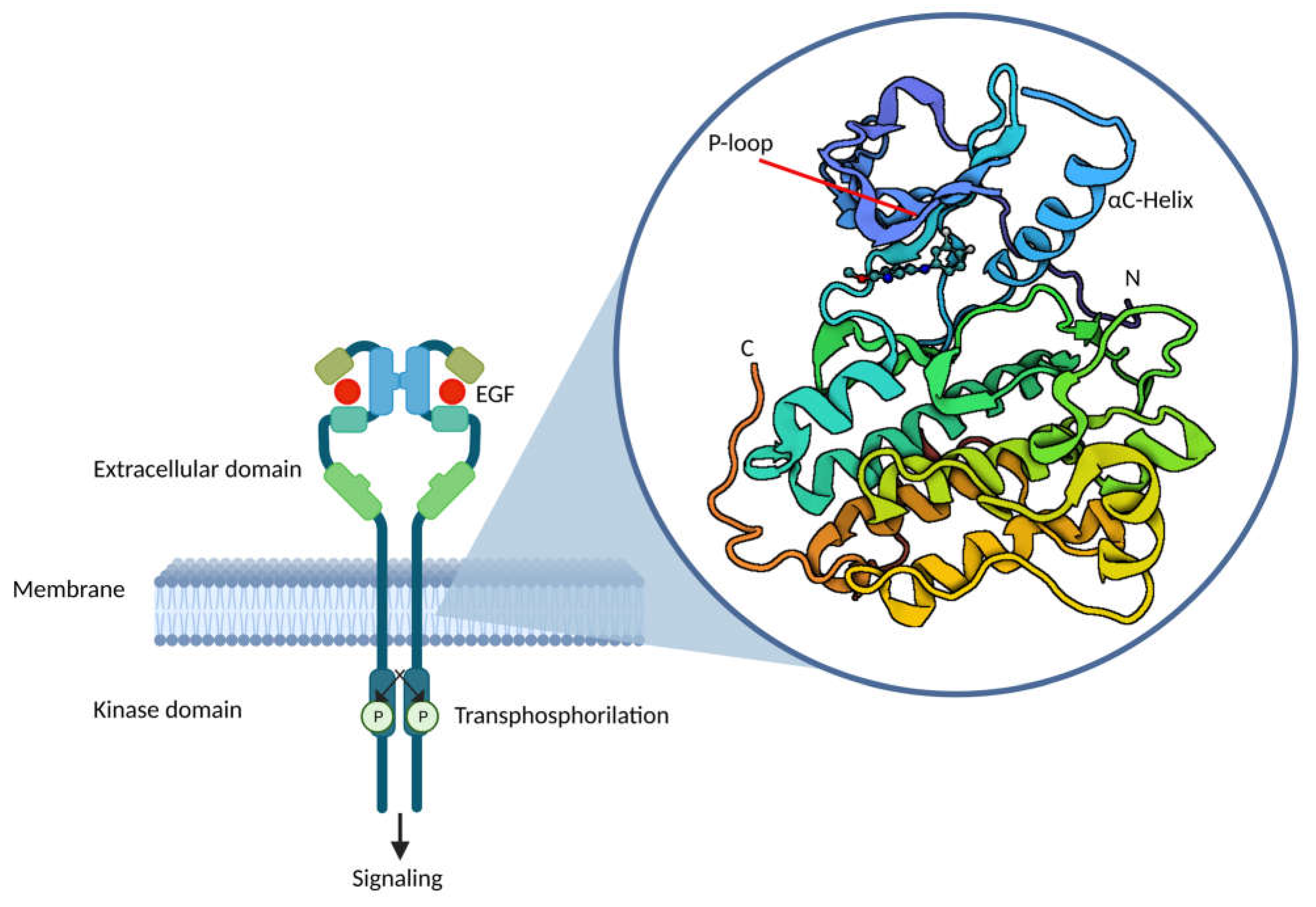
Figure 2.
Tumor microenvironment of EGFR common and uncommon mutations: Association between high PD-L1 expression and uncommon EGFR mutation: larger PD-L1 overexpression is in patients with uncommon compared to common EGFR-mutation. PD-L1: Programmed death-ligand-1.
Figure 2.
Tumor microenvironment of EGFR common and uncommon mutations: Association between high PD-L1 expression and uncommon EGFR mutation: larger PD-L1 overexpression is in patients with uncommon compared to common EGFR-mutation. PD-L1: Programmed death-ligand-1.
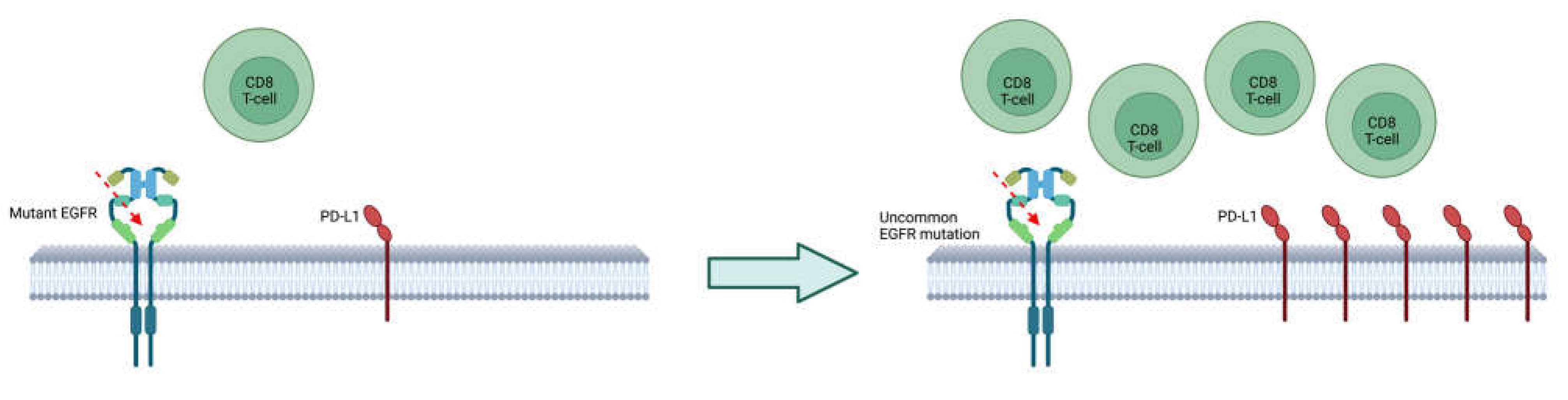
Figure 3.
Tumor microenvironment after treatment with TKI: Treatment with EGFR-TKI change the tumor microenvironment, by increasing PD-L1 expression. PD-L1: Programmed death-ligand-1.
Figure 3.
Tumor microenvironment after treatment with TKI: Treatment with EGFR-TKI change the tumor microenvironment, by increasing PD-L1 expression. PD-L1: Programmed death-ligand-1.
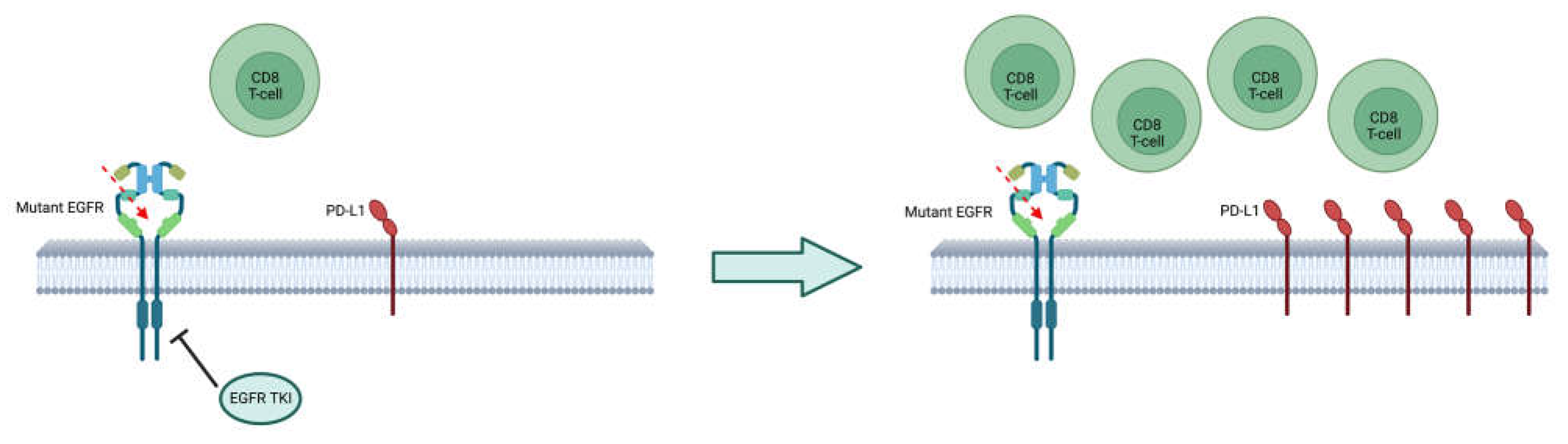
Figure 4.
Immunotherapy VS. chemoimmunotherapy: The patients treated with ICIs, compared to chemotherapy plus ICIs, had a longer PFS although not significant OS. PD-L1: Programmed death-ligand 1. PD-1: Programmed death-1.
Figure 4.
Immunotherapy VS. chemoimmunotherapy: The patients treated with ICIs, compared to chemotherapy plus ICIs, had a longer PFS although not significant OS. PD-L1: Programmed death-ligand 1. PD-1: Programmed death-1.
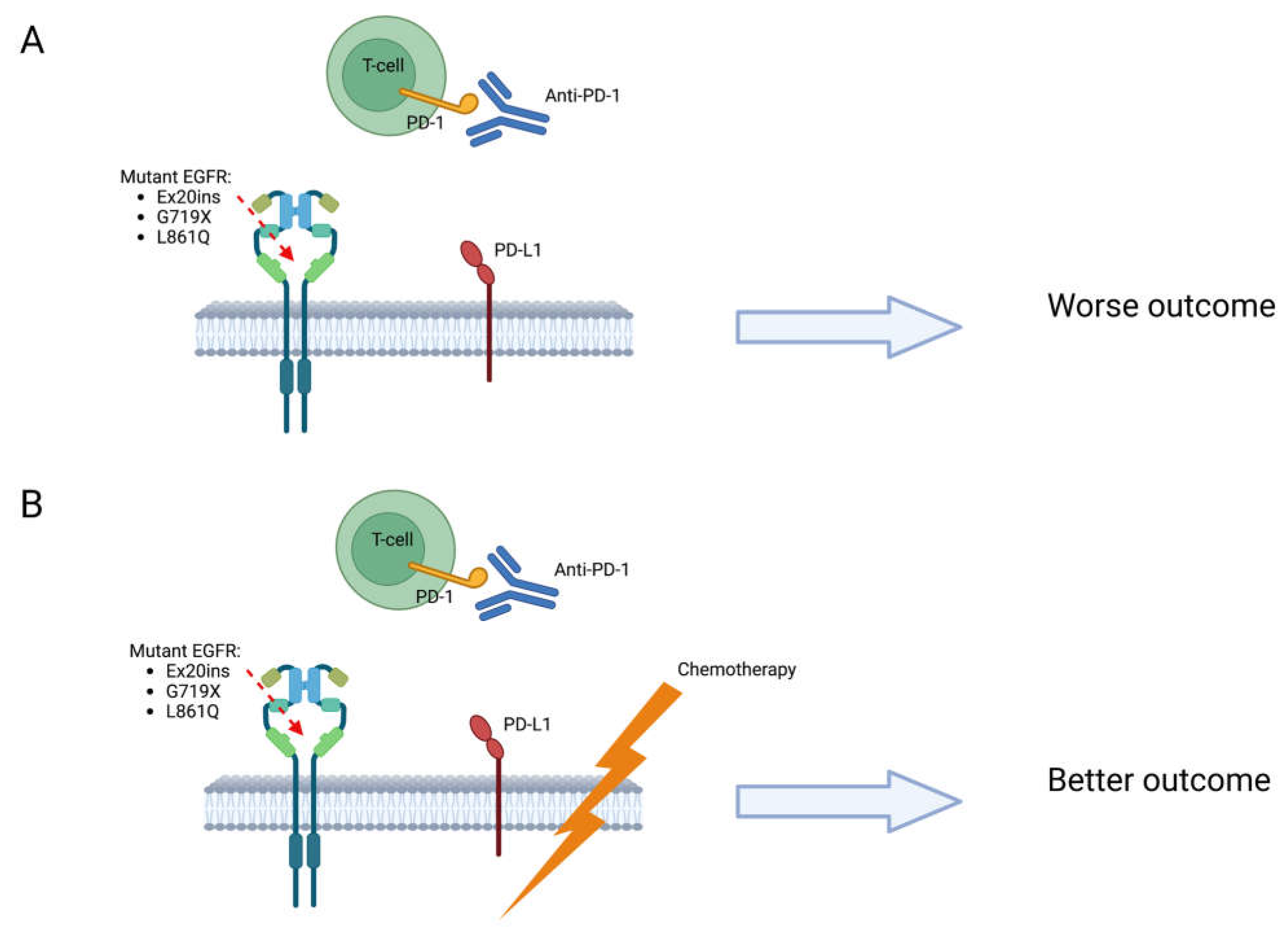

Table 1.
Compound EGFR mutations and treatment [41].
Table 1.
Compound EGFR mutations and treatment [41].
| Compound mutation | Response to treatment | Proposed treatment |
|---|---|---|
| Combined common EGFR mutations (ex21 p.L858R + ex19del) |
Response rate (RR) ≥ 75% with either 1st or 2nd generation TKIs | 1st or 2nd gen TKIs |
| Combined common (ex21 p.L858R + ex19del) plus uncommon EGFR mutations (any but ex21 p.L858R, ex19del or de novo ex20 p.T790M) |
RR 40–80% and 100% with 1st generation TKIs and afatinib | Afatinib |
| Combined uncommon EGFR mutations | RR 20–70%, ~80% and ~75% with 1st generation TKIs, afatinib and osimertinib, respectively | Afatinib |
| Combined EGFR mutation (any) plus de novo ex20 p.T790M | Primary resistance to first- and second-generation EGFR TKIs; osimertinib (RR 33.3%, DCR 100%) | Osimertinib |
Ex: exon; Del: deletion.
Table 2.
Ex20 ins inhibitors.
| Ex20 inhibitor | Trial | Toxicity | Response to treatment |
|---|---|---|---|
| Poziotinib | NCT03066206 | Diarrhea 92%, skin rash 90%, oral mucositis 68%, paronychia 68%, dry skin 60% (66% of G3 AEs on EAP) | ORR 32%, mPFS 5.5 m, mOS 19.2 m ORR of 46% and 0% in near (aa A767 to P772) vs far loop ins |
| Mobocertinib | NCT02716116 |
PPP cohort 69% G≥3 AEs 46% SAE EXCLAIM cohort 66% G≥3 AEs 44% SAE |
PPP cohort ORR 28% by IRC and 35% by investigator assessment, mPFS 7.3 m by IRC, mOS 24.0 m EXCLAIM cohort ORR 25% by IRC and 32% by investigator assessment |
| Amivantamab | NCT02609776 | At RP2D 39% G≥3 AEs, 31% SAE | ORR 40%, mPFS 8.3 m |
| Sunvozertinib (DZD9008) | NCT03974022 and CTR20192097 | Most common TEAEs: diarrhea (G3 5.2%) and skin rash (G3 1%) |
ORR 39.3% across all dose levels; dose level of 300 mg once daily, ORR 48.4% and DCR 90.3% |
| CLN-081 (TAS6417) | NCT04036682 | Constipation 8%, diarrhea 8%, dizziness 8%, fatigue 8%, and chest pain 8% | 5 evaluable pts: 2 pts PR, 3 pts SD |
| Tarloxotinib | NCT03805841 | G3 TEAEs: prolonged QTc 34.8%, rash 4.3%, diarrhea 4.3%, increased ALT 4.3% | DCR 60% |
AEs: adverse events; EAP: expanded access program; ORR: objective response rate; mPFS: median progression free survival; mOS: median overall survival; aa: amino acids; PPP: platinum-pretreated patients; SAE: severe adverse event; IRC: independent review committee; RP2D: recommended phase 2 dose; PR: partial response; SD: stable disease; TEAEs: treatment emergent adverse events; DCR: disease control rate.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



