
Submitted:
02 May 2023
Posted:
03 May 2023
You are already at the latest version
Abstract
Background: Knowledge of vascular anatomy and its possible variations is essential for performing embolization or revascularization procedures and complex surgery in the pelvis. The obturator artery (OA) is a branch of the anterior division of the internal iliac artery (IIA), and it has the highest frequency of variation between branches of the internal iliac artery. Possible anomalies of the origin of the obturator artery (OA) should be known when performing pelvic and groin surgery, where its control or ligation may be required. The purpose of this systematic review and meta-analysis, based on Sanudo’s classification, is to analyse the origin of the obturator artery (OA) and its variants.
Methods: Thirteen articles, published between 1952 and 2020, were included in this systematic review and meta-analysis.
Results: The obturator artery (OA) was present in almost all cases (99.8%): the pooled prevalence estimate for internal iliac artery (IIA) was 77.7% (95% CI 71.8% – 83.1%) vs 22.3% (95% CI 16.9% – 28.2%) for the external iliac artery (EIA). In most cases, the obturator artery (OA) originated from the anterior division trunk of the internal iliac artery (IIA) (61.6%).
Conclusion: Performing preoperative radiological studies to know the pelvic vascular pattern and having awareness to evaluate possible changes in the obturator artery can reduce the risk of iatrogenic injury and complications
Keywords:
obturator artery (OA)
; Internal Iliac Artery (IIA)
; External Iliac Artery (EIA)
1. Introduction
The Obturator Artery (OA) is an extrapelvic parietal branch of the Internal Iliac Artery (IIA) that supplies the medial thigh muscles. The OA runs forward and down on the lateral wall of the small pelvis, subsequently exiting through the obturator canal and to enter the medial compartment of the thigh. Near the obturator foramen, the OA divides into its anterior and posterior branches.
In common clinical practice the following OA variations may be commented on when:
- The OA is aberrant when it does not originate from the anterior division of the IIA, but it originates from the External Iliac Artery (EIA) or from a branch of it.
- The OA is accessory when there is a double OA.
In 2011, Sanudo et al. [1] standardized the classification of OA variations, in which six different types were reported. In Type A the OA origins from the anterior division of the IIA; in Type B the artery origins instead from the deep Inferior Epigastric Artery (IEA). These two types of variations are also the most common. In Type C, the origin is at the level of the posterior division of the IIA, while in Type D the artery derives from the IIA, above its final branching. Finally, the rarest cases are distinguished as Type E when the artery derives from the EIA and Type F where is arises from the femoral artery. Furthermore, in some cases, an accessory OA may perform an anastomosis with the external iliac artery ("corona mortis”).
It is essential for physicians to be familiar with the anatomical variations of OA when performing invasive procedures involving the pelvis. Surgeons should be aware of the course of the arteries and their potential different path to prevent undesirable and potentially life-threatening complications.
Although the anatomical variations of the OA are well documented according to Sanudo's classification[1], there is still a lack of a global estimation regarding their prevalence in the scientific literature. Considering these elements, the aim of this systematic review and meta-analysis was to determine the prevalence of the OA and its anatomical variants according to Sanudo’s [1] classification.
2. Materials and methods
A systematic review and meta-analysis were performed according to the guidelines set out in "the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines" (Moher 2009).
Research strategies
This systematic search, updated to January 1, 2023, was performed using PubMed, SCOPUS and Web of Science (WOS). PubMed terms used for the search were the following: "Obturator Artery" and "variants". No language restrictions were made.
The research has been expanded with “Google Scholar” and the Pubmed’s function “related articles”.
Selection criteria: inclusion and exclusion criteria
In order to include a study in the meta-analysis, it needed to meet the following criterion: a prevalence of reported data on the origin of the OA. All case reports, editorials, letters, reviews and studies with irrelevant or incomplete data were excluded from the study.
Data extraction
Two authors (M.M. and R.C.) extracted data from the included studies, including: the surname of the first author of the study, the year of publication, the country of origin of the hospital where the study was carried out, the type of study and the number of patients included.
Statistical Methods
In addition to calculating raw prevalence, we used MetaXL (Version 5.3) to estimate multinomial pooled prevalence estimates (PPEs) and their 95% CIs using a DerSimonian and Laird random effects model with double arcsine transformations. Multinomial pooled prevalence estimates were normalized such that the summated prevalences equaled 1.0. Heterogeneity was examined statistically through the I2 statistic and LFKindex. Barendregt and Doi’s (2016) LFKindex is an effect-size like statistic for measuring the degree of asymmetry in a funnel-type display of study effects. We used the standard criteria reported in Higgins et al. (2021) for judging heterogeneity via the I2 statistic. In the lesser known LFKindex, a value of 0.00 indicates symmetry, values between 0.00 and ± 2.00 indicate minor asymmetry, and values greater ±2.00 indicate major asymmetry (Barendregt & Doi, 2016). Heterogeneity was examined visually with forest plots, Doi plots, and funnel plots, which can be found in the supplemental file. To examine the sensitivity of models to individual study outliers, we conducted a leave-one-out analysis.
Risk of bias assessment of the studies included
Quality assessment and bias risk analysis of all selected full-text articles were performed using the International Evidence-Based Anatomy (iEBA) Group's Anatomical Quality Assurance (AQUA) tool [Henry et al., 2016]. Two of the authors (R.C. and M.M) screened the articles and assessed the risk of bias according to the five domains used in the AQUA tool. In case of a discordant evaluation, a third author (S.A) was involved to reach a consensus.
3. Results of systematic research
Identification of studies
An initial search yielded 1900 potentially relevant articles and 147 articles from additional documents identified through other sources (grey literature). After removing duplicates and analysing remaining titles and abstracts, further articles were excluded, leaving 30 studies for full-text analysis. Of these, 17 were excluded due to the absence of data reported in the article or to a different nomenclature of arterial vessels. Therefore, 13 articles were included in this systematic review and meta-analysis (Figure 1).
Features of the included studies
Thirteen articles (N = 561 patients), published between 1952 and 2020, were included (Table 1).
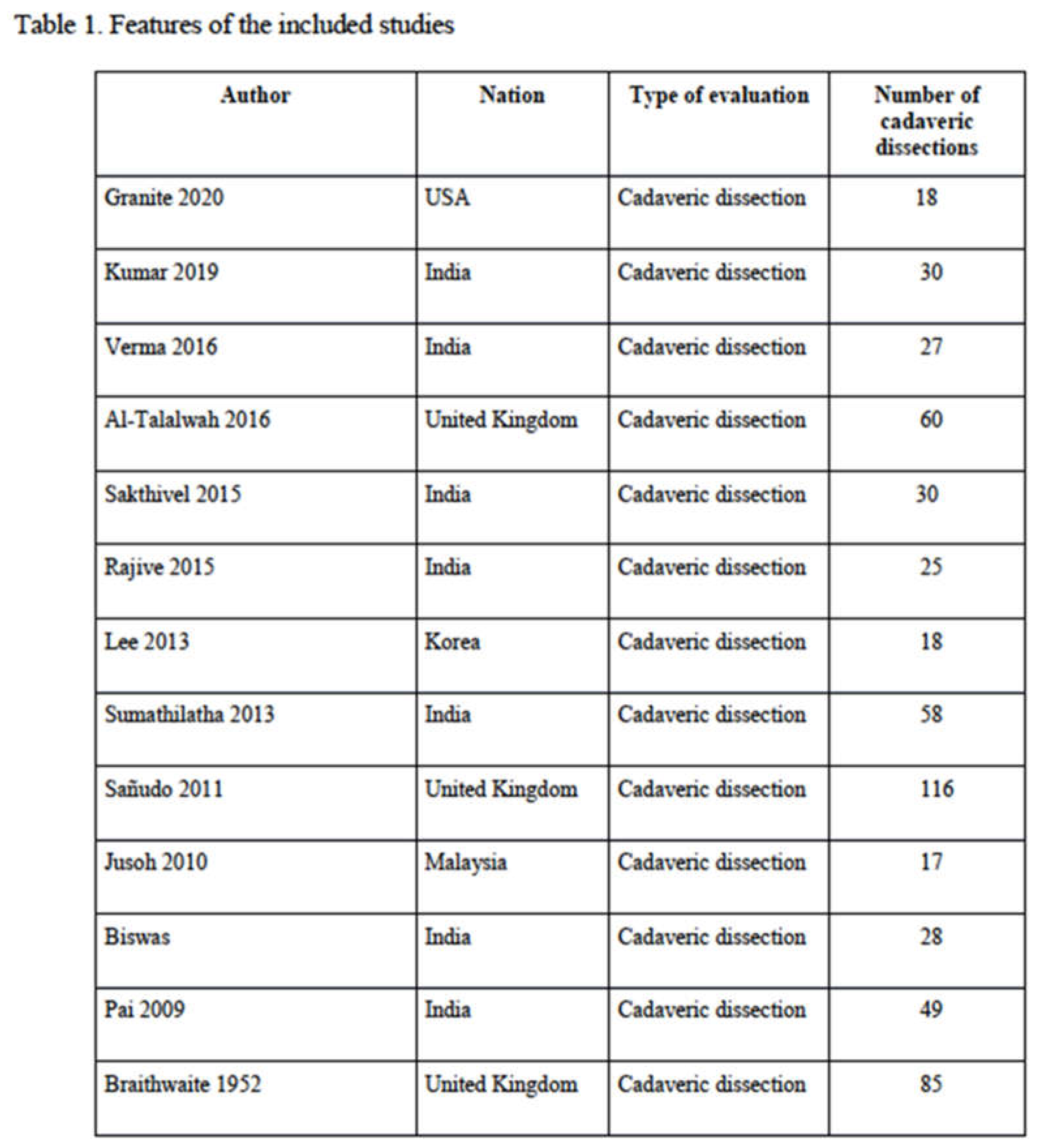
In our review, we highlighted only studies carried out on cadaveric dissections, otherwise studies based on radiological investigations or intraoperative findings were excluded as they were often case reports. In addition, some studies based on cadaveric dissections were also excluded as only case reports were presented and it was not possible to establish the prevalence of the origin of the OA. Geographically, most studies were conducted in Asia (9 studies: 282 patients, 50.3%) (Kumar 2019, Verma 2016, Sakthivel 2015, Rajive 2015, Lee 2013, Sumathilatha 2013, Jusoh 2010, Biswas 2010, Pai 2009); only a few studies were performed in Europe (3 studies: 261 patients, 46.5%) (Al-Talalwah 2016, Sañudo 2011, Braithwaite 1952) and in North America (1 study: 18 patients, 3.2%) (Granite 2020). No studies were carried out in Africa or Australasia. In Asia, the majority of studies were conducted in India (247 patients, 44%) (Kumar 2019, Verma 2016, Sakthivel 2015, Rajive 2015, Sumathilatha 2013, Biswas 2010, Pai 2009), only 1 study in Korea (18 patients, 3.2%) (Lee 2013) and 1 study in Malaysia (17 patients, 3.0%) (Jusoh 2010) In Europe, the studies were carried out in the United Kingdom only and in North America in the USA.
The AQUA tool probes for potential risk of bias in 13 studies domains (objectives and subject characteristics, study design, methodology characterization, descriptive anatomy and reporting of results). The risk of bias within each domain is normally categorized as “Low”, “High” or “Unclear”. Three of the included studies showed high risk in domain one (Objective and Study Characteristics), mainly because the methods applied in them were not described enough detail to be reproduced. Similarly, one study had high risk of bias in domain two (objective and subjective characteristics), three (methodology) and five (reporting of results). A summary of the assessment of quality and risk of bias by the AQUA tool is displayed below (Figure 2).
Analysis of the results of the systematic review
Main outcomes:
Origin of OA. In all studies, the presence of the OA was revealed in 99.8% (560 patients) and it was absent in only 1 case (0.2%) (Braithwaite 1952). In all cases the OA originated from the IIA or EIA, the origin from the Femoral Artery was never recorded as evidenced in the previous revision of Sañudo (1.7%) (Sañudo 2011). Rarely, the OA was double in 15 patients (2.7%) [1,7,10,12,13,14] and 1 patient had triple arteries (0.2%)[1], consisting of an upper, middle and a lower branch.
In the cadaveric dissections, the most common origin of the OA was from the IIA (813 hemipelvis, 74.4%), in the remaining cadaveric dissections (279 hemipelvis, 25.6%) the origin of the OA was from the EIA (Table 2).
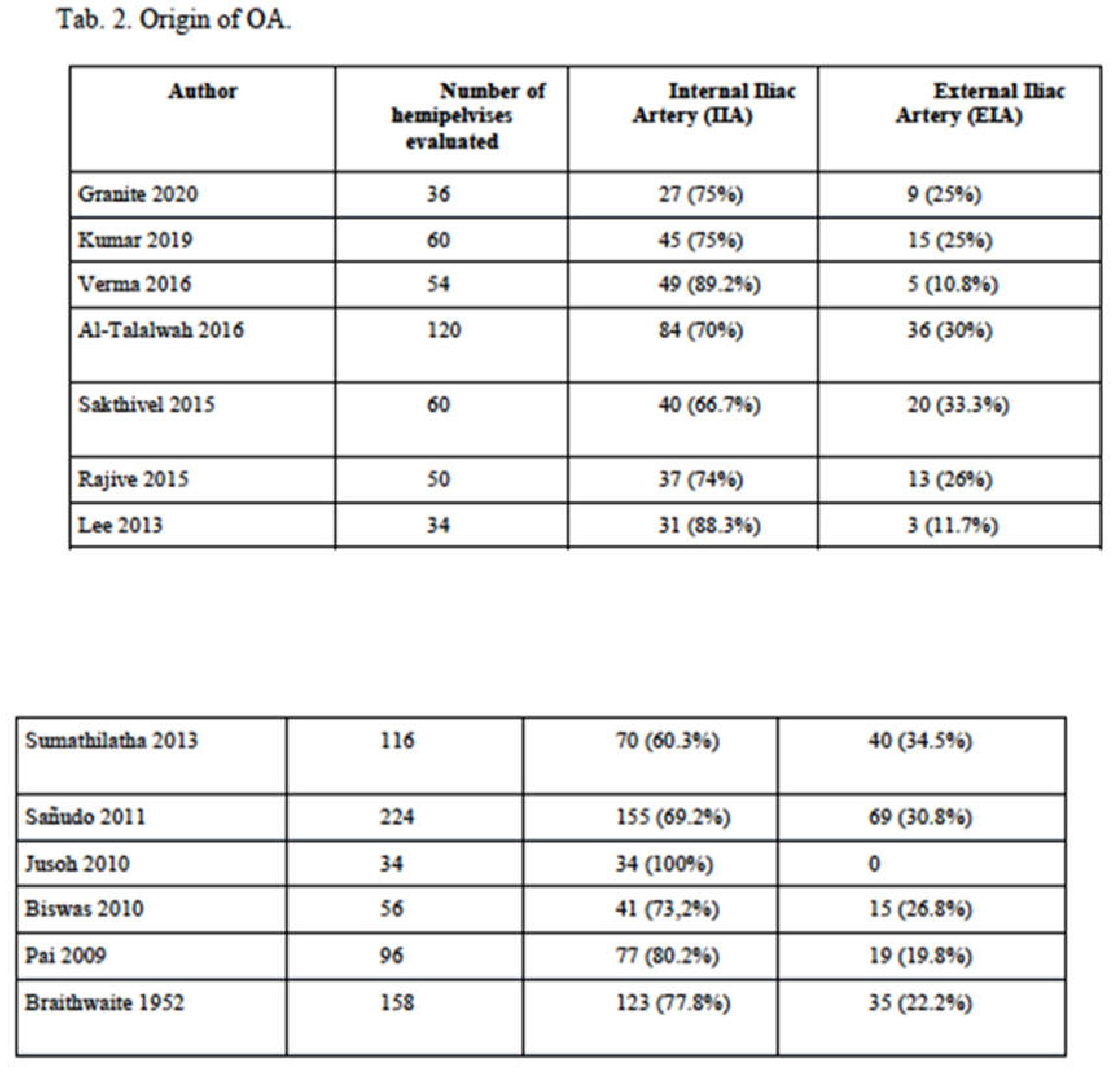
Pooled Prevalence Estimates of origin of OA from IIA versus EIA. Across the 13 studies that reported on the prevalence of internal iliac artery (IIA) versus the external iliac artery (EIA) origin, the pooled prevalence estimate (PPE) for IIA was 77.7% (95% CI 71.8% – 83.1%) compared to 22.3% (95% CI 16.9%% – 28.2%) for the EIA. There was substantial heterogeneity for this finding; I2 = 79.3% (95% CI 65.2% – 87.6%) (see the forest plots in Figure 1a and Figure 2a), Q(1) = 57.86, p < .001; and there was evidence of minor asymmetry with an LFKindex of ±1.85. Leave-one-out PPEs ranged from 75.0% to 78.9% for the IIA (Figure 3b,c) and the 21.1% to 25.0% for the EIA (Figure 4b,c). The Jusoh 2010 study appeared to be an outlier with a reported prevalence of 100.0% (95% CI 95.0% – 100.0%) for the EIA.
Secondary outcomes
Origin of the OA from IIA. The origin of the OA from the IIA has been divided into three subgroups, already identified in the review of Sañudo:
- Sañudo A (Figure 5a): origin from the anterior division trunk of the IIA (482 hemipelvis, 61.6%). In the literature this variant represents this condition is considered as the “normal anatomy”.
- Sañudo C (Figure 5b): origin from the posterior division trunk of the IIA (251 hemipelvis, 32.1%) (Table 3). The limitation of the latter classification proposed by Sañudo is related to the fact that many vessels were included in the posterior trunk (Sañudo C), even if they had a separate origin. For this reason, we have carried out a new analysis of the true prevalence of these individual vessels considering the common trunk as a vascular structure usually constituted by the common origin of the Inferior Gluteal Artery and the Internal Pudendal Artery.
- Sañudo D (Figure 5c): origin from the main trunk of the IIA (22 hemipelvis, 2.8%).
The new analysis of the origin of the OA shows us the following prevalence:
- origin from the main trunk of the IIA (22 hemipelvis, 2.8%)
- origin from the anterior division trunk of the IIA (482 hemipelvis, 61.6%)
- origin from the posterior common trunk consisting of the origin of the inferior gluteal artery and the internal pudendal artery (174 hemipelvis, 22.3%)
- origin from the superior gluteal artery (65 hemipelvis, 8.3%)
- origin from the inferior gluteal artery (23 hemipelvis, 2.9%)
- origin from the iliolumbar artery (8 hemipelvis, 1%)
- origin from the internal pudendal artery (7 hemipelvis, 0.9%)
- origin from the inferior bladder artery (1 hemipelvis, 0.1%)
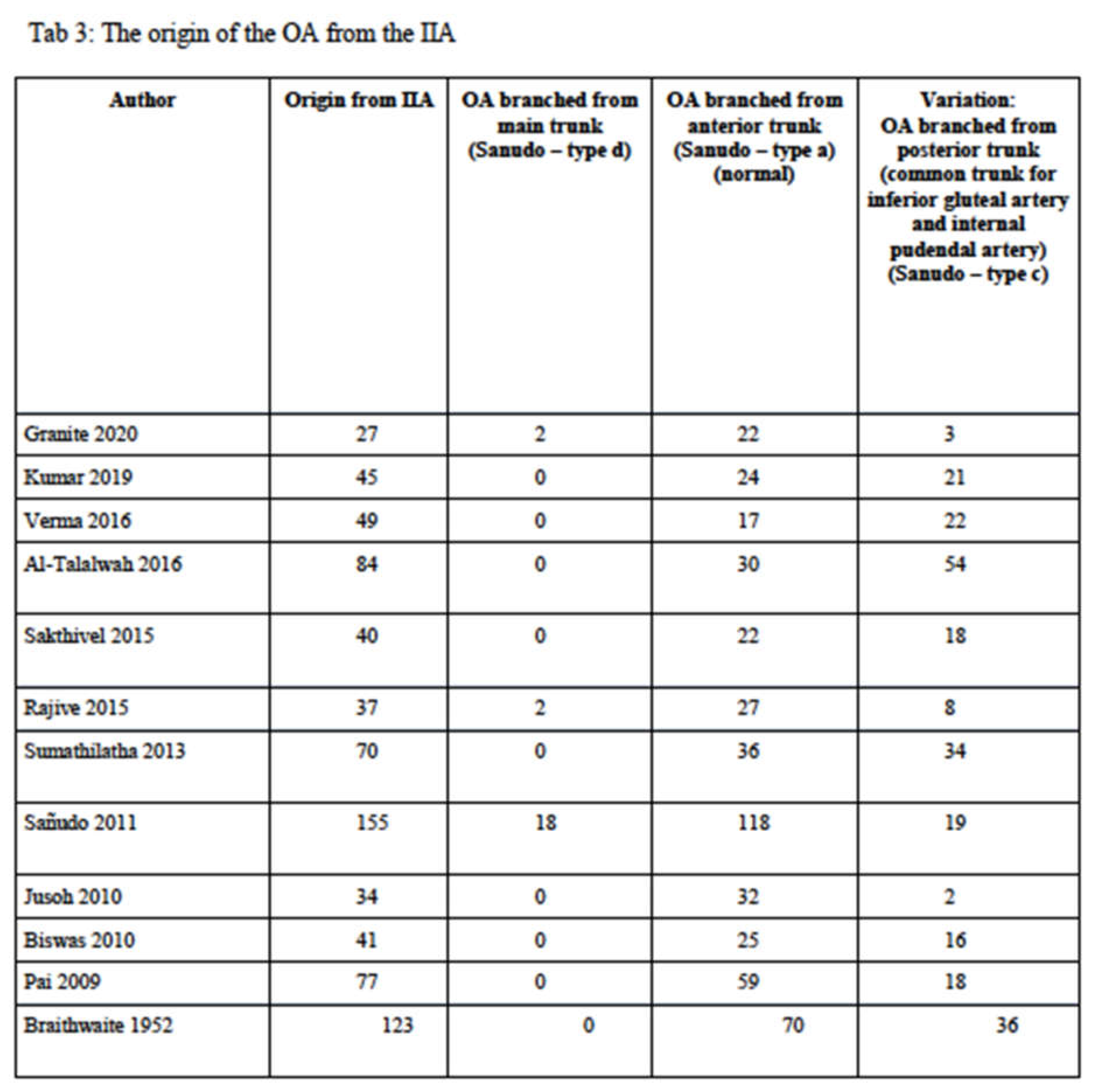
Pooled Prevalence Estimates of the origin of the IIA: Type A, Type C, and Type D. Of the PPEs for Type A, Type C, and Type D origins of the IIA, 66.3% (95% CI 50.1% – 94.7%) were of Type A origin, 31.8% (95% CI 18.8% – 44.0%) were of Type C origin, and 1.8% (95% CI 0.0% – 6.3%) were of Type D origin (see Figure 6b through Figure 8b). There was a considerable degree of heterogeneity across the 11 studies included in this comparison; I2 = 91.8% (95% CI 0.0% – 6.3%), Q(2) = 121.21, p < .001; and minor asymmetry, with LFKindices ranging between -1.38 and 1.20. The leave-one-out range of PPEs was 62.9% – 69.3%, 28.7% – 35.1%, and 2.1% – 1.4% for IIA Type A (see Figure 6c and Figure 6d), Type C (see Figure 7c and Figure 7d), and Type D (see Figure 8c and Figure 8d), respectively.
Origin of the OA from EIA. The origin of the OA from the EIA has been divided into only two subgroups, both already identified in the review of Sañudo 2011 (Table 4):
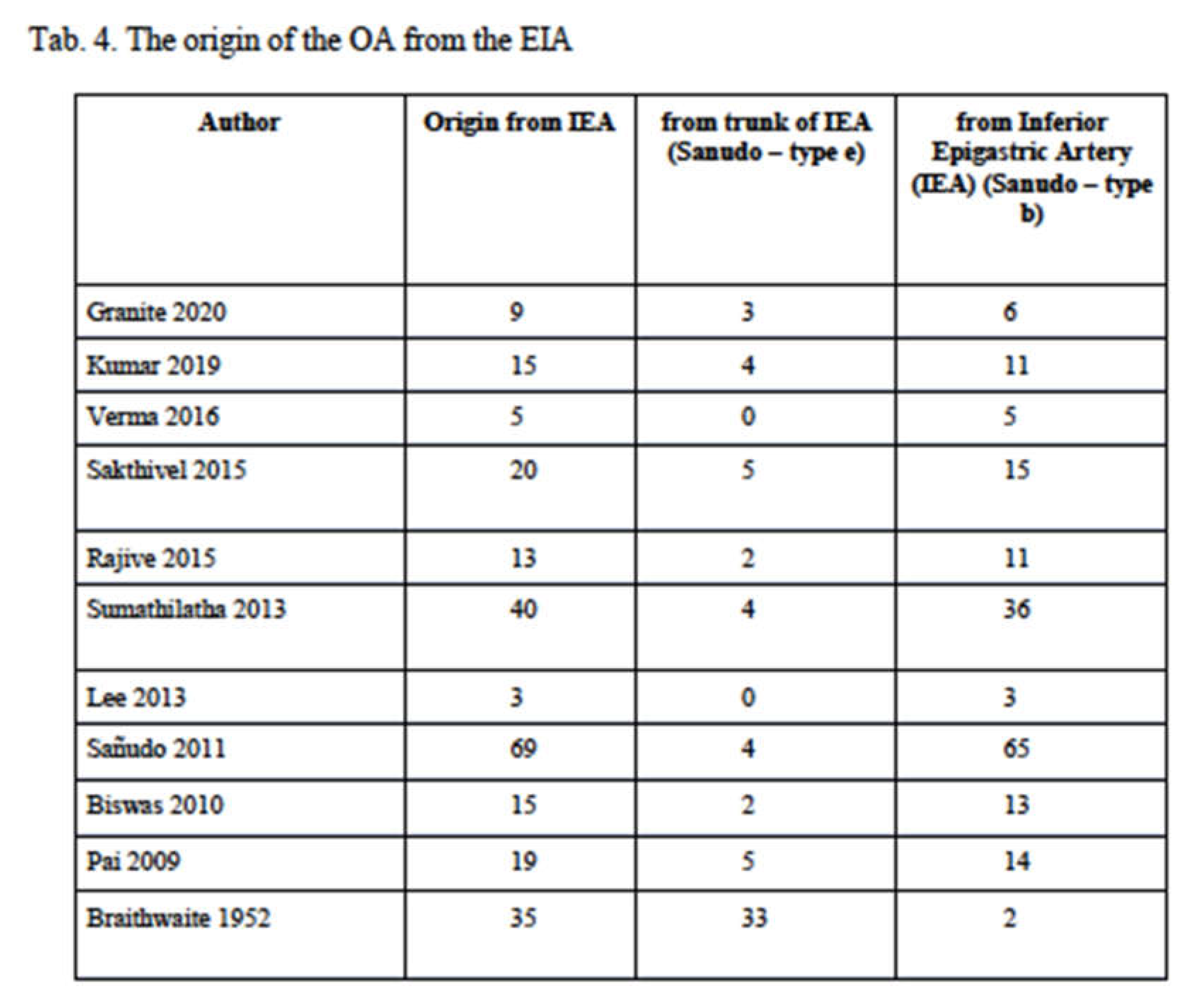
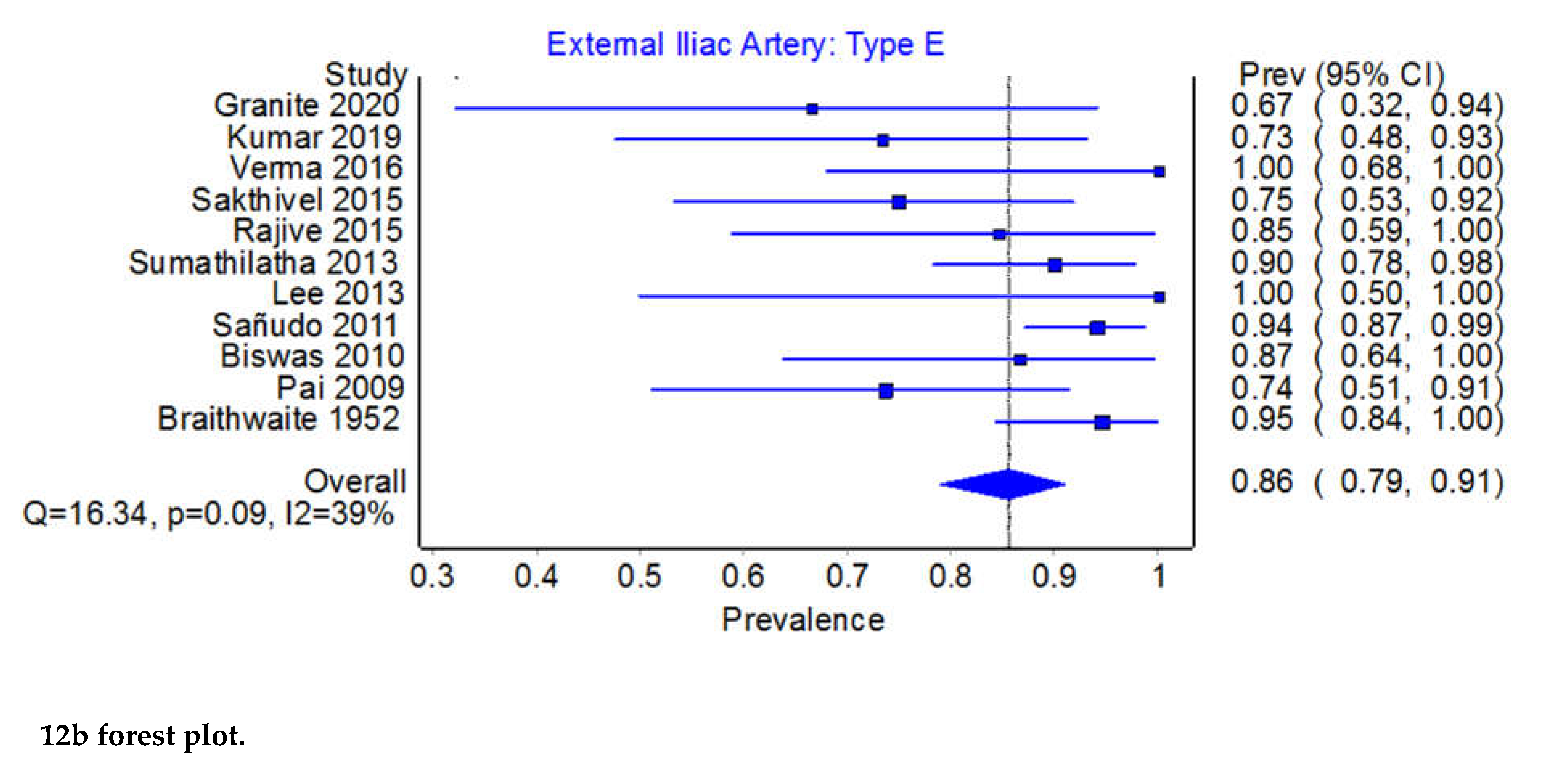
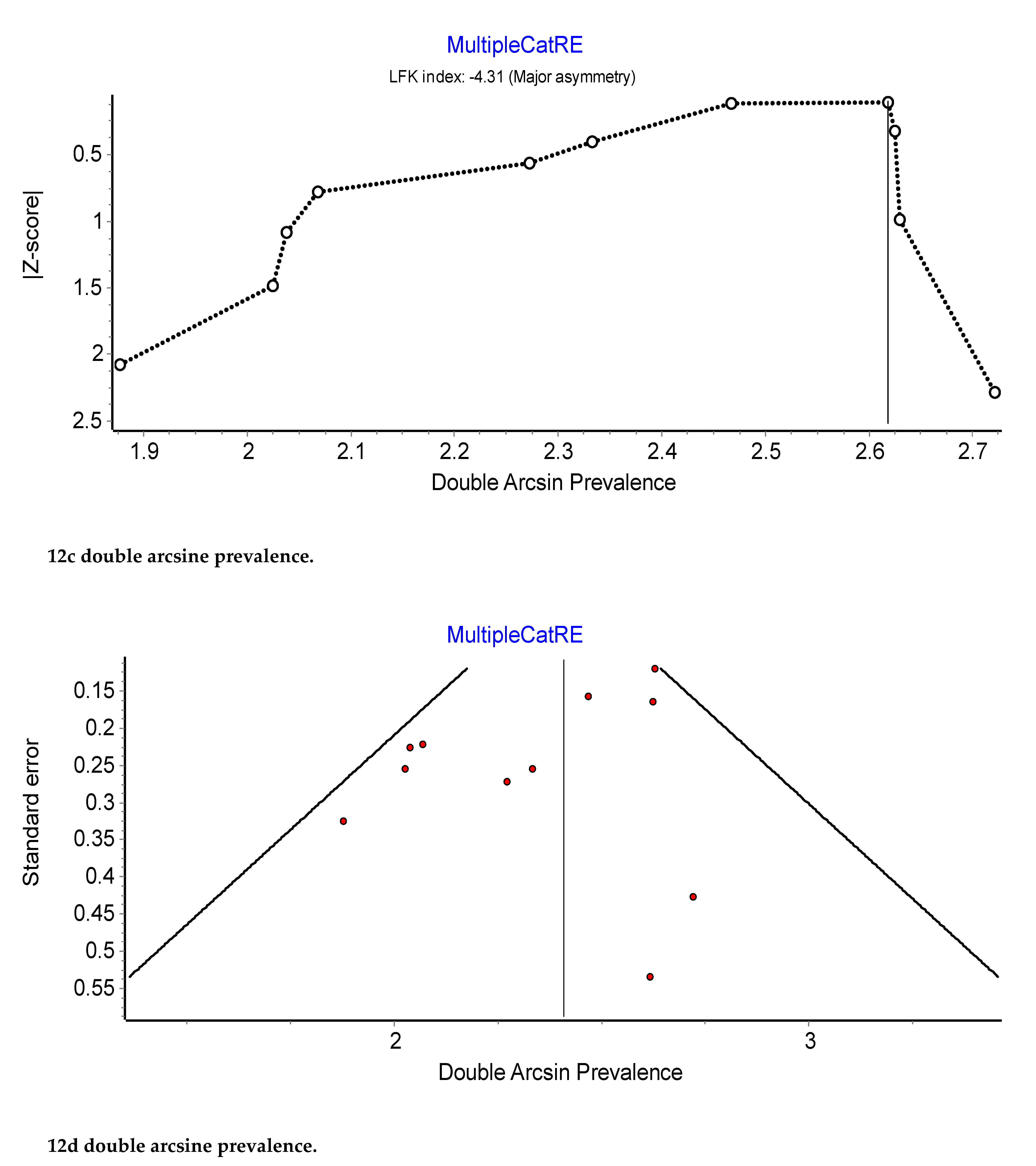
Prevalence of the origin of the EIA: type B or type E. Across 11 studies that examined the origin of the EIA, the PPE for Type B was 85.6% (95% CI 79.0% – 81.1%) compared to 14.4% (95% CI 8.9% – 21.1%) for Type E (see Figure 11b and Figure 12b). The I2 heterogeneity was moderate at 38.8% (95% CI 0.0% – 69.9%), Q(1) = 16.33, p = 0.09, but exhibited major asymmetry as evidenced in the relatively empty areas of Doi plot and its LFKindex of ±4.31(see Figure 11c,d). The leave-one-out PPEs range from 13.0% to 16.3% for Type E and 83.7% and 87.0% for Type B (see Figure 12c,d).
4. Discussion
In this systematic review and meta-analysis, the OA was reported in almost all cases (99.8%): the PPE for IIA was 77.7% (95% CI 71.8% – 83.1%) vs 22.3% (95% CI 71.8% – 83.1%) for the EIA. In most cases, the OA originated from the anterior division trunk of the IIA (61.6%).
Variation of the OA origin is an important anatomical issue which has implications for a wide range of surgical procedures in different fields like gynecology, orthopedics, urology, vascular as well as for oncological surgery. For instance, in the case of inguinal dissection (alone or in combination with an iliac/obturator lymph node dissection) for melanoma, identification and control of the origin of the OA represents a critical step. Again, in cases of pelvic trauma, this considerable variation in origin may be a significant source of persistent bleeding that might be difficult to manage. The frequency with which vascular surgeons are called to treat groin complications is rapidly increasing also because of the widespread use of percutaneous procedures. Therefore, infected groin problems that often involve foreign prosthetic material or remnants of percutaneous femoral closure devices might be challenging and require control of bleeding, removal of foreign material, wide debridement, and sometimes arterial resection. Management of the consequential limb ischemia in such cases is controversial and an obturator foramen bypass is a classic approach for the treatment of contemporary groin infection, thus requiring a perfect knowledge of the OA course[15].
Another very important variant of the aberrant OA, which can be encountered during pelvic procedures, it is called the corona mortis (CMOR), or crown of death. The corona mortis is a vascular abnormality affecting the presence of abnormal communication between the OA and the external iliac artery or deep inferior epigastric artery. The name of this anatomical variation comes from the high risk of death connected to its possible injury, which can lead to hemorrhage and difficulty in control. These retropubic vessels are very important for surgeons who treat pelvic and acetabular trauma, pelvic malignancy, totally extraperitoneal inguinal hernioplasty (TEP), in particular when fixing the mesh on Cooper's ligament, herniorrhaphy, catheter embolization, surgery of muscle grafts, lymphadenectomies, catheterizations and during aneurysm repairs of the internal iliac artery.
Surgery in the pelvic region must be conducted with extreme caution and with in-depth knowledge of possible vascular variations of the OA in particular.
The presence of an aberrant OA should be contemplated as a resource in case of IIA and its collateral branches are ligated or obstructed. An aberrant OA can therefore provide collateral circulation, especially in the region of the femoral head.
The presence of an aberrant OA should be contemplated as a resource in case of IIA and its collateral branches are ligated or obstructed. An aberrant OA can therefore provide collateral circulation, especially in the region of the femoral head.
On the contrary, it may be considered as a risk factor for surgical complications. In this context, the presence of an aberrant AO also becomes relevant in the context of medico-legal opinions on the surgeon's activity. The presence of an aberrant AO can make surgical acts, that are usually easily performed considerably difficult. This issue will impose meditated evaluations in the medico-legal sphere because, even if the surgeon's awareness of the possible presence of an aberrant AO should induce to always act with the utmost prudence and expertise, the presence of an anatomical variant of the AO is not always easy to identify. It follows that the occurrence of lesion of an aberrant AO in the course of a surgical act should not always be characterized as a consequence of the surgeon's incorrect behavior.
A thorough knowledge of the vascular pattern and awareness of potential arterial variations may decrease the risk of iatrogenic complications and may allow modification of the surgical/procedural approach to minimize this risk.
5. Conclusion
The variations in the origin of the obturator artery have been reviewed systematically and subjected to meta-analysis for the first time A thorough understanding of pelvic vascular anatomy is fundamental in performing procedures like embolization, revascularization, treatment of pelvic fractures, surgery for advanced pelvic malignancy and groin hernia surgery (both laparoscopic and open). A preoperative radiological/angiographic evaluation to know the pelvic vascular pattern and knowledge of obturator artery variants could help reduce the risk of iatrogenic injuries. It may also modify surgical strategy in order to minimize post-operative complications that can generate medical-legal disputes that are not easy to resolve.
Author Contributions
Conceptualization and methodology, G.B., B.C.; formal analysis and data curation M.M, P.S.; writing—original draft preparation, R.C., A.F., S.A.; writing—review and editing, I.C, G.T., P.F. and J.D.; supervision, J.R., G.B., B.C. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| OA | obturator artery |
| IIA | internal iliac artery |
| OA | obturator artery |
| EIA | external iliac artery |
References
- Sañudo, J.R.; Mirapeix, R.; Rodriguez-Niedenführ, M.; Maranillo, E.; Parkin, I.G.; Vázquez, T. Obturator artery revisited. Int. Urogynecology J. 2011, 22, 1313–1318. [Google Scholar] [CrossRef] [PubMed]
- Kumar, S.; Minz, S. A study of variations in the origin of obturator artery in the human cadavers and its clinical significance. Natl J Clin Anat 2017, 6, 42–50. [Google Scholar] [CrossRef]
- ShashiKant, V.; Natwar, L.A. Variation in the origin of obturator artery in population of Mahakaushal region and its clinical importance. International Journal of Scientific Research 2016, 5. [Google Scholar]
- Sakthivel; Priyadarshini, S. Variability of origin of obturator artery and its clinical significance. International Journal of Anatomy and Research 2015, 3, 1704–1709. [Google Scholar] [CrossRef]
- Pillay, M. A Study of Variations in the Origin of Obturator Artery and its Clinical Significance. J. Clin. Diagn. Res. 2015, 9, AC12–AC15. [Google Scholar] [CrossRef] [PubMed]
- Lee, E.Y.; Kim, J.Y.; Kim, H.N.; Sohn, H.-J.; Seo, J.H. Variant Origin of Obturator Artery: A Branch of Inferior Epigastric Artery from External Iliac Artery. Korean J. Phys. Anthr. 2013, 26, 125–130. [Google Scholar] [CrossRef]
- Sumathilatha, S.; Sharmila, A.; Sakthivelavan D., S.; Christilda F., J. Variability of the obturator artery and its surgical implications in a South Indian population. European journal of anatomy 2013, 17, 159–165. [Google Scholar]
- Jusoh, A.R.; Rahman, N.A.; Latiff, A.A.; Othman, F.; Das, S.; Ghafar, N.A.; Suhaimi, F.H.; Hussan, F.; Sulaiman, I.M. The anomalous origin and branches of the obturator artery with its clinical implications. Rom J Morphol Embryol. 2010, 51, 163–6. [Google Scholar] [PubMed]
- Biswas, S.; Bandopadhyay, M.; Adhikari, A.; Kundu, P.; Roy, R. Variation of Origin of Obturator Artery in Eastern Indian Population - A Study. J. Anat. Soc. India 2010, 59, 168–172. [Google Scholar] [CrossRef]
- Pai, M.M.; Krishnamurthy, A.; Prabhu, L.V.; Pai, M.V.; Kumar, S.A.; Hadimani, G.A. Variability in the Origin of the Obturator Artery. Clinics 2009, 64, 897–901. [Google Scholar] [CrossRef]
- Waseem, A.T.; Zainab, A. H.; Shorok, A. D.; Halimah, A.H.; Adel, Y.; Hasan, A.M. The clinical significance of the obturator artery in origin variability. Indian J. Sci. Res. 2016. [Google Scholar]
- Braitwaite, J.L. Variations in origin of the parietal branches of the internal iliac artery. J Anat. 1952, 86, 423–30. [Google Scholar]
- Kumar, S.; Minz, S. A study of variations in the origin of obturator artery in the human cadavers and its clinical significance. Natl J Clin Anat 2017, 6, 42–50. [Google Scholar] [CrossRef]
- Granite, G.; Meshida, K.; Wind, G. Frequency and Clinical Review of the Aberrant Obturator Artery: A Cadaveric Study. Diagnostics 2020, 10, 546. [Google Scholar] [CrossRef] [PubMed]
- Dunphy, K.M.; Hassey, J.; Vallabhaneni, R.; Alfawaz, A.A.; Kiguchi, M.M.; Fatima, J.; Woo, E.Y.; Abramowitz, S.D. Results of Obturator Foramen Bypass in Patients with Groin Infection and Arterial Involvement. Ann. Vasc. Surg. 2021, 75, 144–149. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Prisma flow chart of literature search.
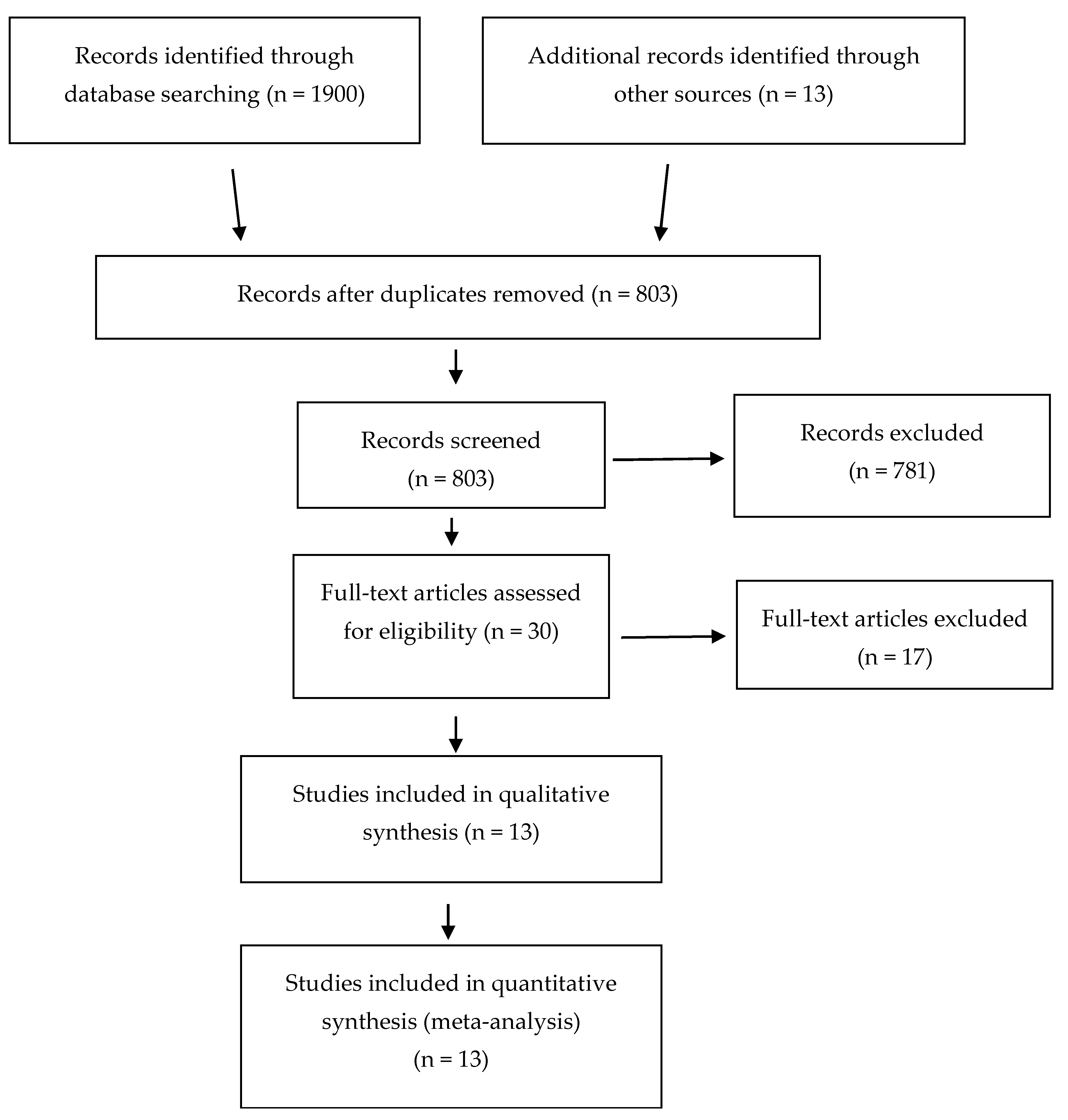
Figure 2.
Summary Chart Quality and risk of bias assessment as determined by the AQUA tool. The risk of bias of each domain is normally cztegorized as “low”, “high” or “unclear”. Five different domains are taken into consideration: objectives and study characteristics, study design, methodology characterization, descriptive anatomy and reporting of results.
Figure 2.
Summary Chart Quality and risk of bias assessment as determined by the AQUA tool. The risk of bias of each domain is normally cztegorized as “low”, “high” or “unclear”. Five different domains are taken into consideration: objectives and study characteristics, study design, methodology characterization, descriptive anatomy and reporting of results.
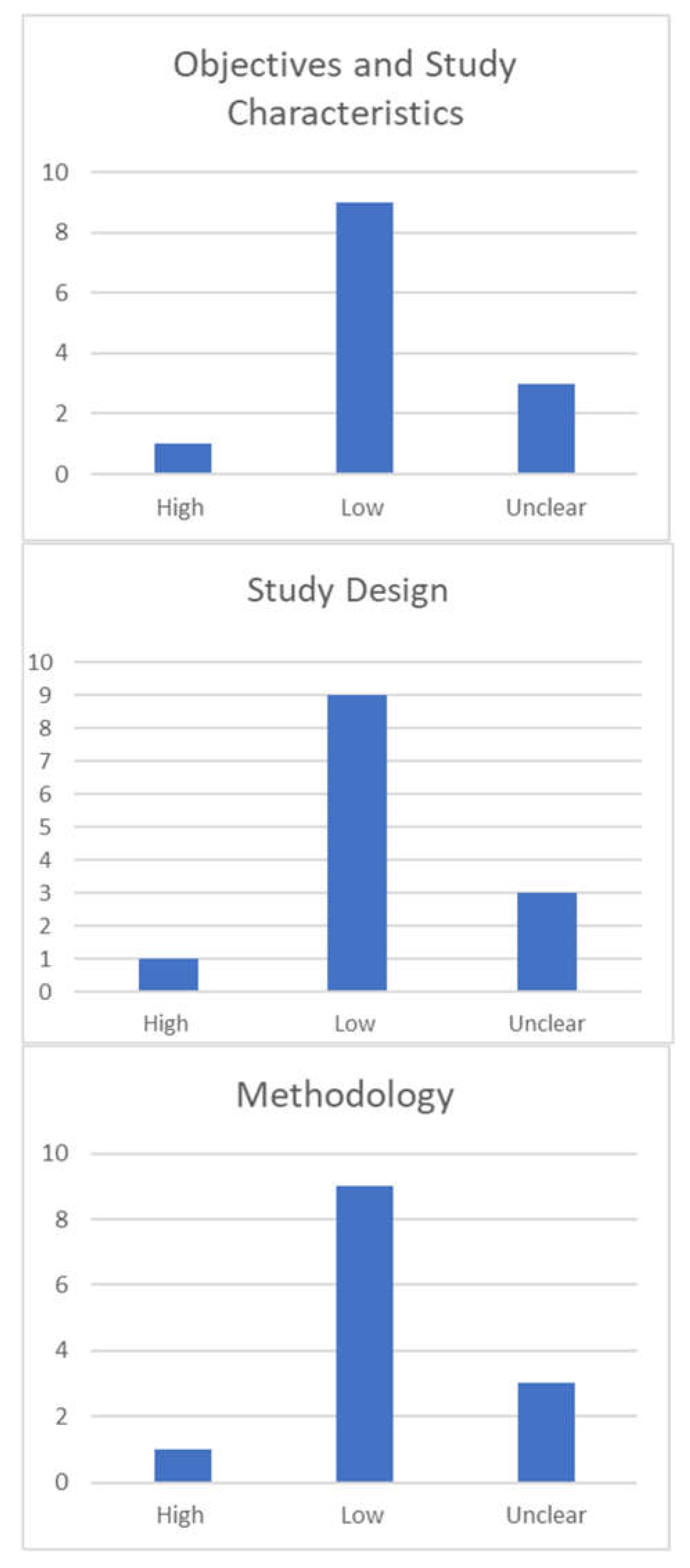
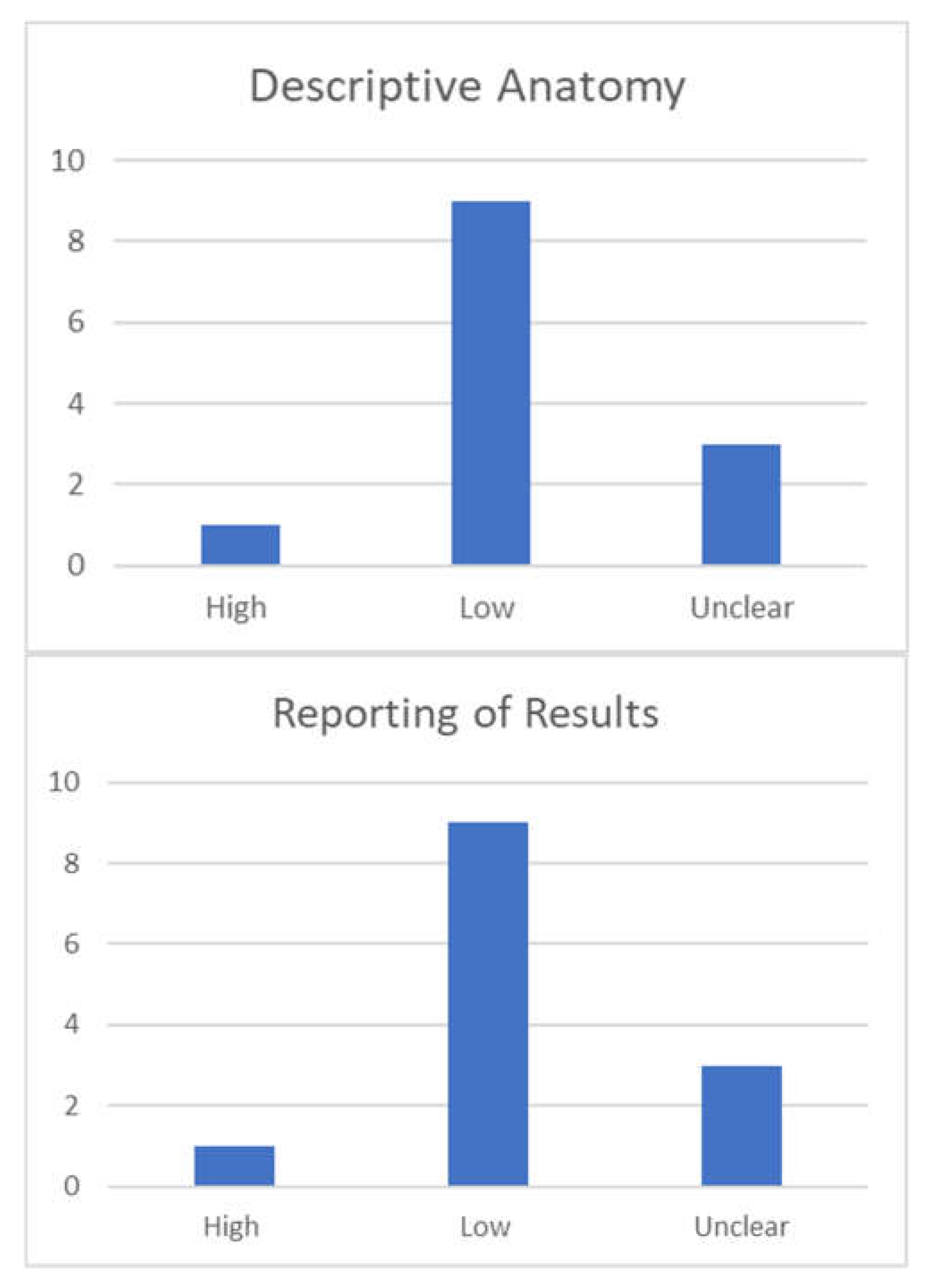
Figure 3.
Prevalence from the Internal Iliac Artery.
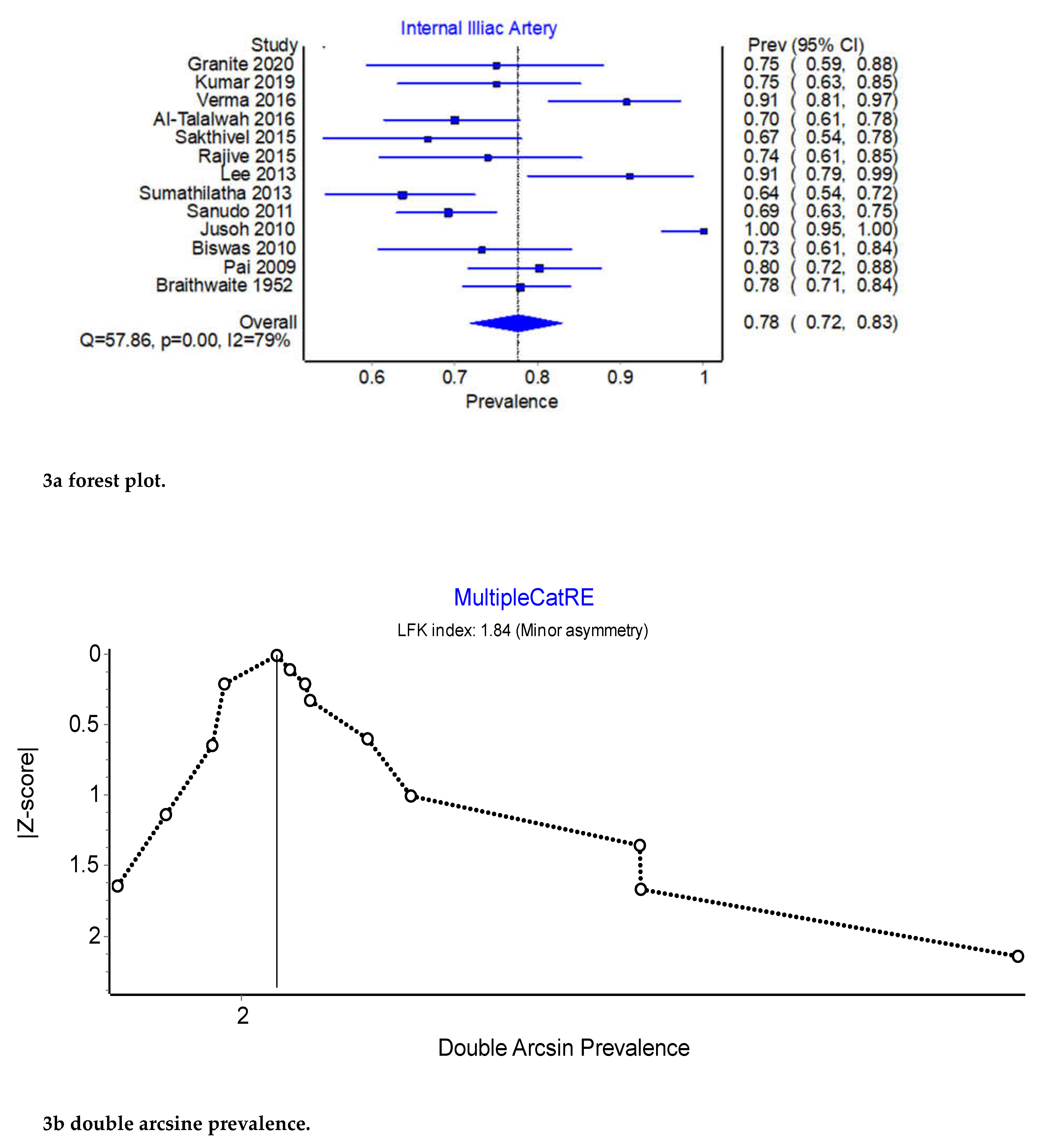
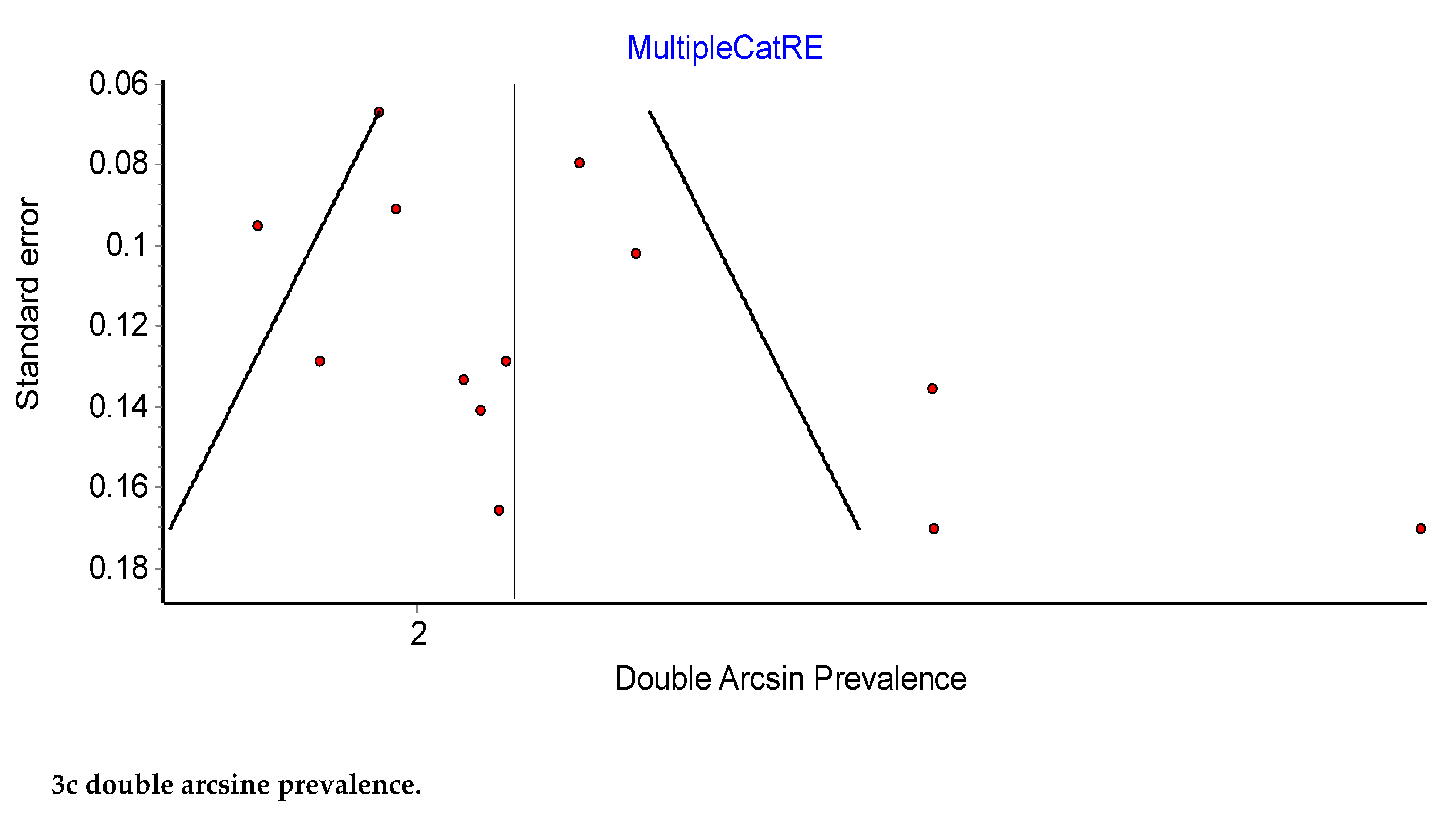
Figure 4.
Prevalence of the External Iliac Artery.
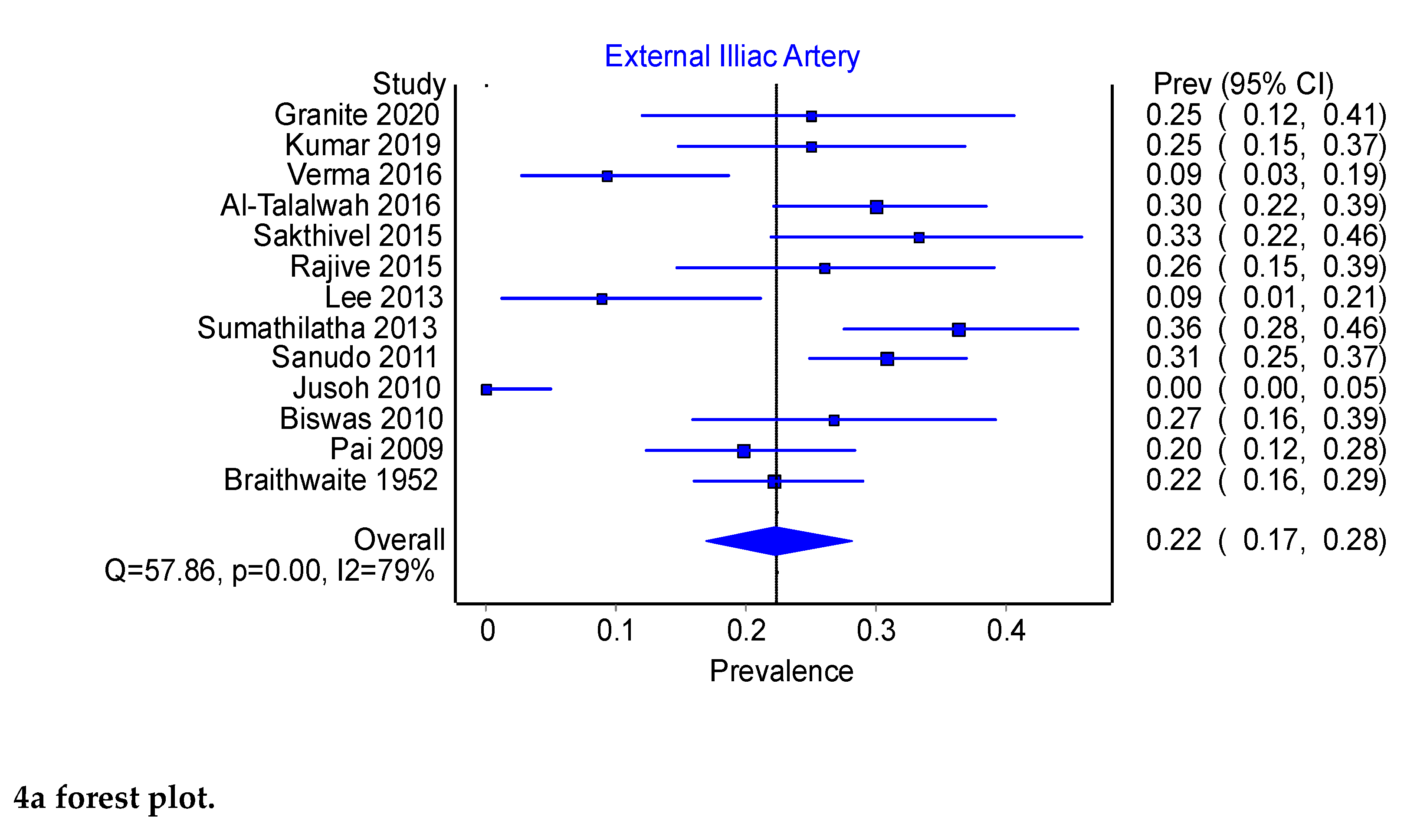
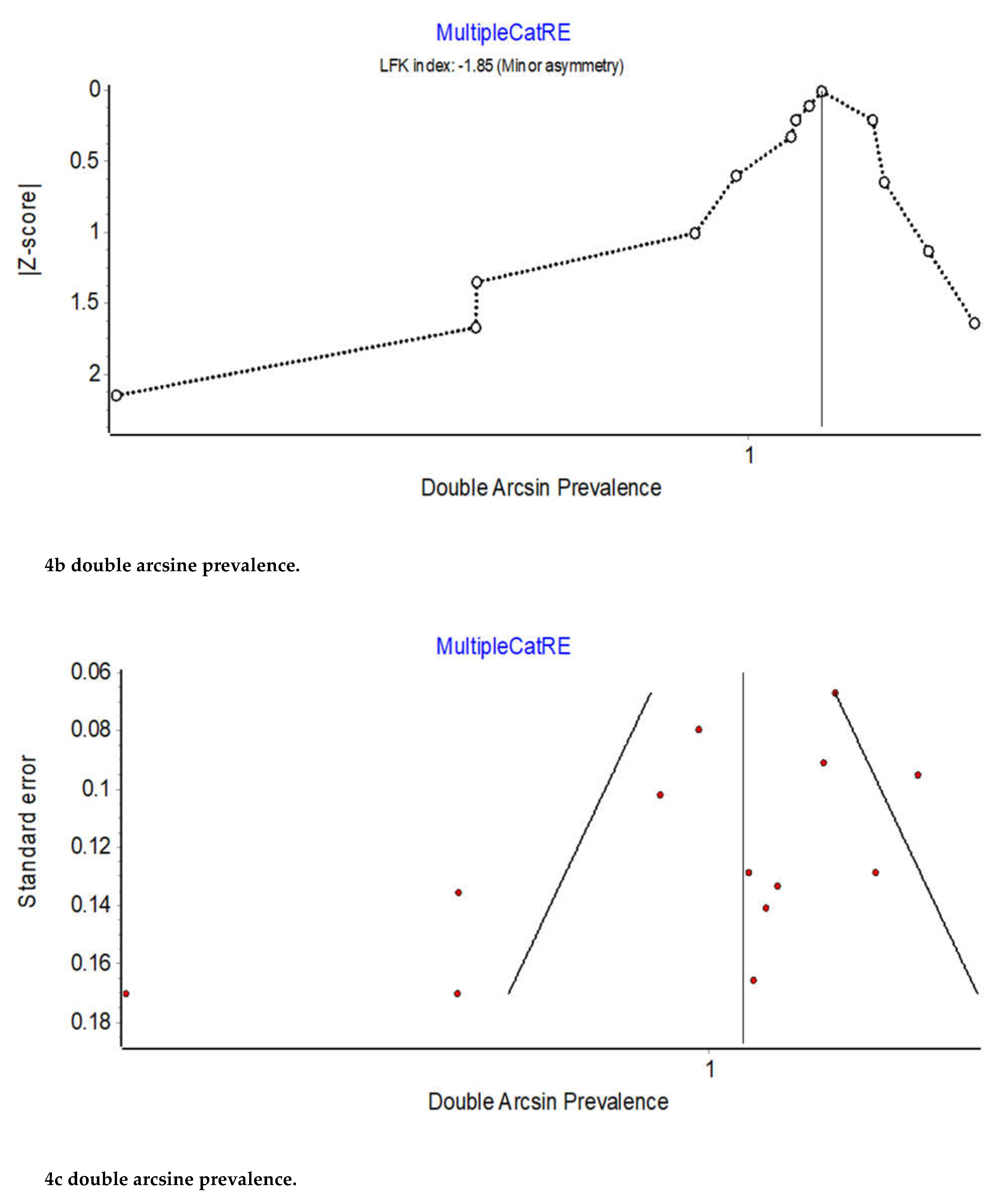
Figure 5.
(a) Type A. Obturator artery arising from the anterior trunk of the internal iliac artery. CI: circumflex iliac artery; EIA: external iliac artery; EIV: external iliac vein; IIA: internal iliac artery; IEA: inferior epigastric artery; IM: iliac muscle; OA: obturator artery; ON: obturator nerve; OV: obturator vein. (b) Type C. Obturator artery arising from the posterior trunk of the internal iliac artery.EIA: external iliac artery; IIA: internal iliac artery; OA: obturator artery; ON: obturator nerve; P: psoas muscle; PT: posterior trunk of the internal iliac artery; RI: right iliac artery; UA: umbilical artery. (c) Type D. Obturator artery arising from the internal iliac artery, main trunk. EIV: external iliac vein; IIA: internal iliac artery; OA: obturator artery; ON: obturator nerve; P: psoas muscle; RI: right iliac artery.
Figure 5.
(a) Type A. Obturator artery arising from the anterior trunk of the internal iliac artery. CI: circumflex iliac artery; EIA: external iliac artery; EIV: external iliac vein; IIA: internal iliac artery; IEA: inferior epigastric artery; IM: iliac muscle; OA: obturator artery; ON: obturator nerve; OV: obturator vein. (b) Type C. Obturator artery arising from the posterior trunk of the internal iliac artery.EIA: external iliac artery; IIA: internal iliac artery; OA: obturator artery; ON: obturator nerve; P: psoas muscle; PT: posterior trunk of the internal iliac artery; RI: right iliac artery; UA: umbilical artery. (c) Type D. Obturator artery arising from the internal iliac artery, main trunk. EIV: external iliac vein; IIA: internal iliac artery; OA: obturator artery; ON: obturator nerve; P: psoas muscle; RI: right iliac artery.
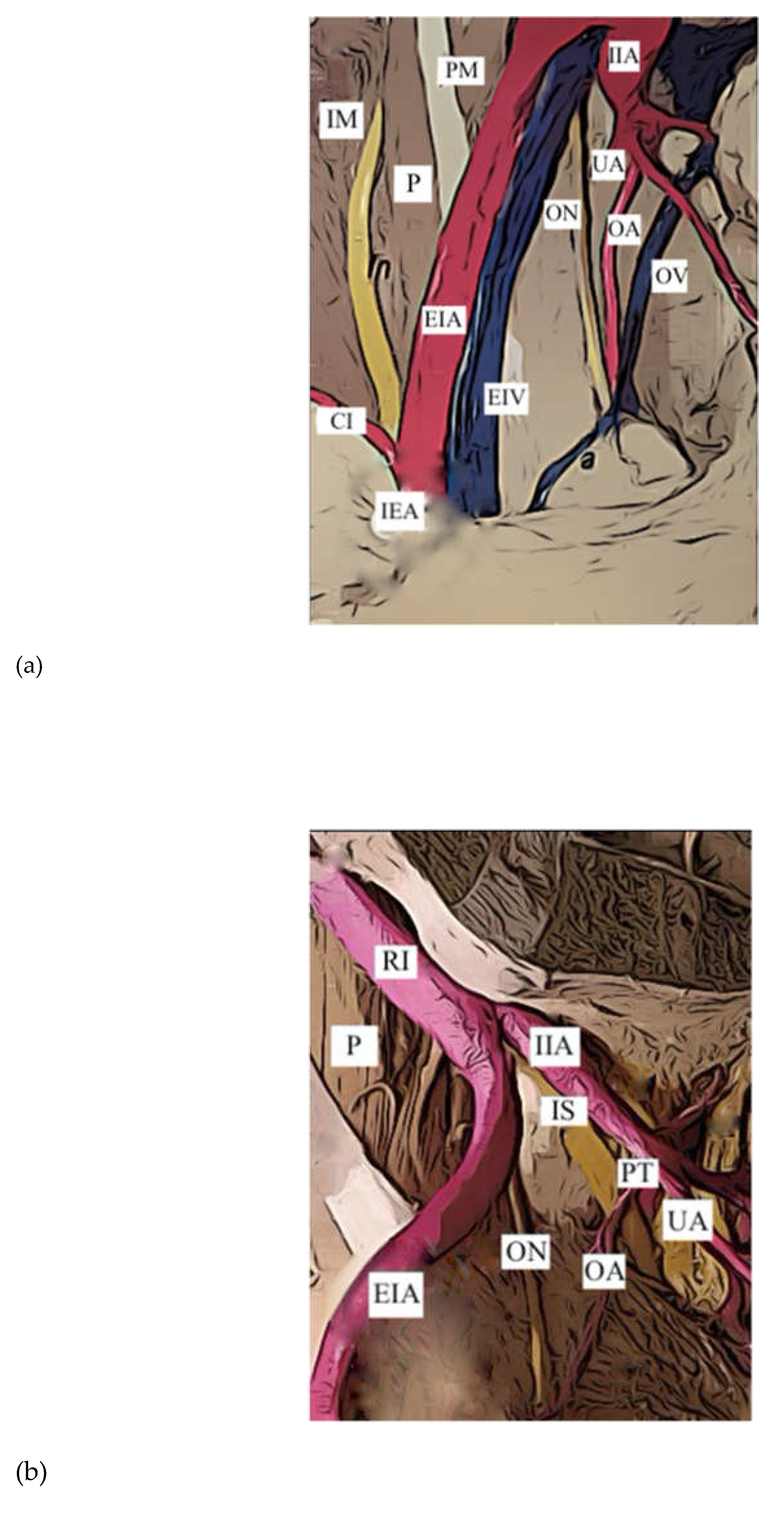
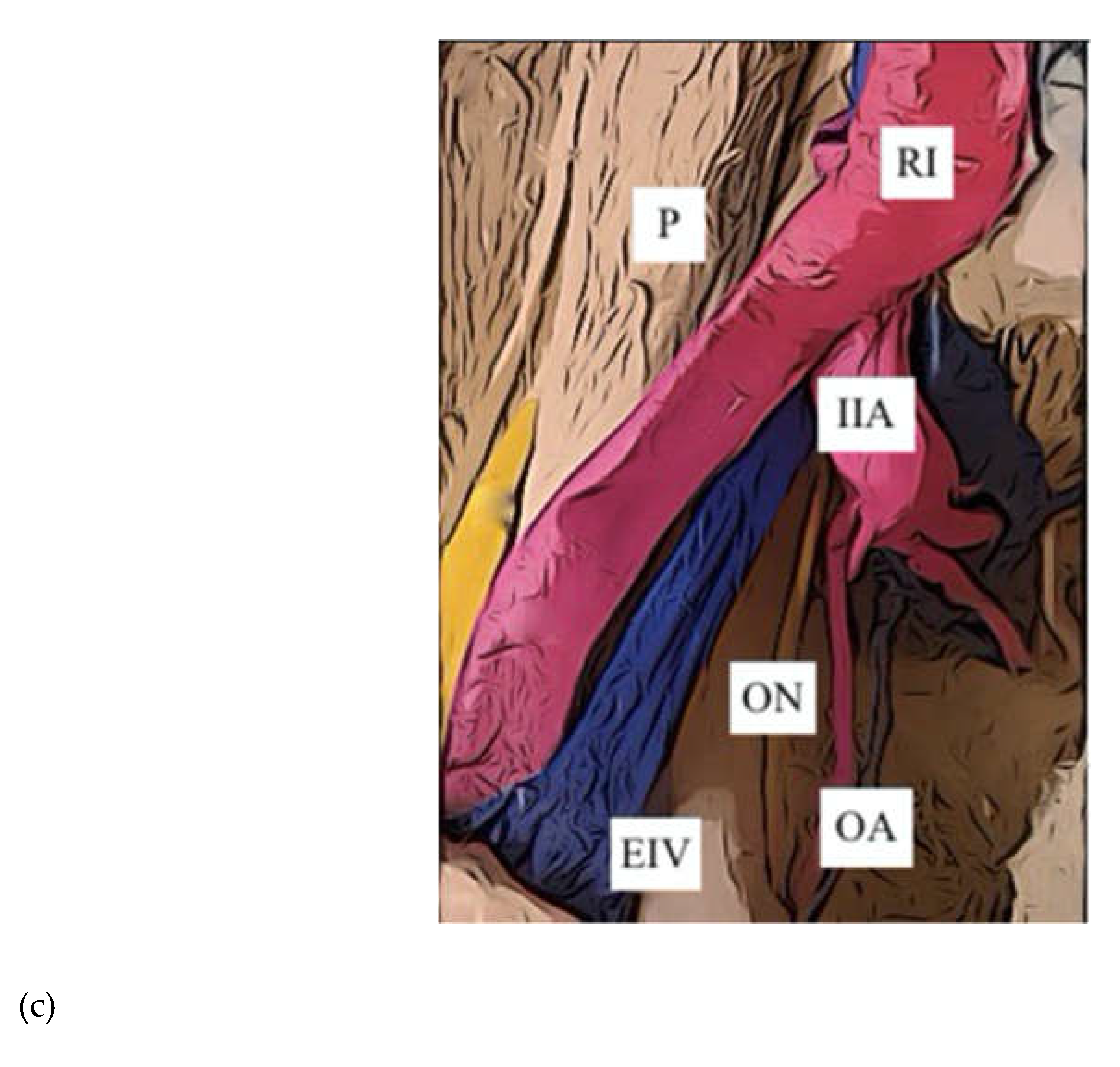
Figure 6.
Prevalence of the Internal Iliac Artery: Type A.
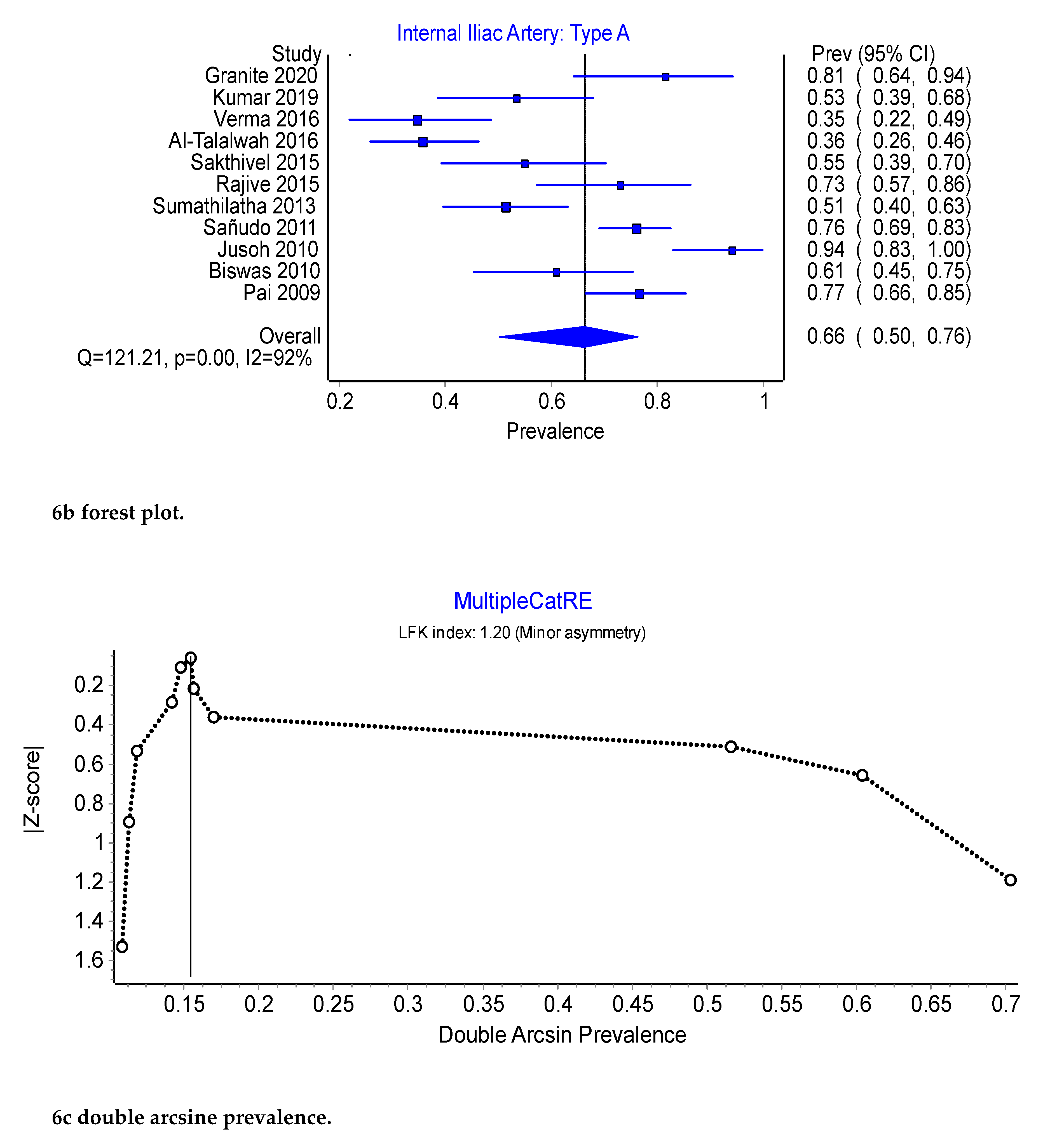
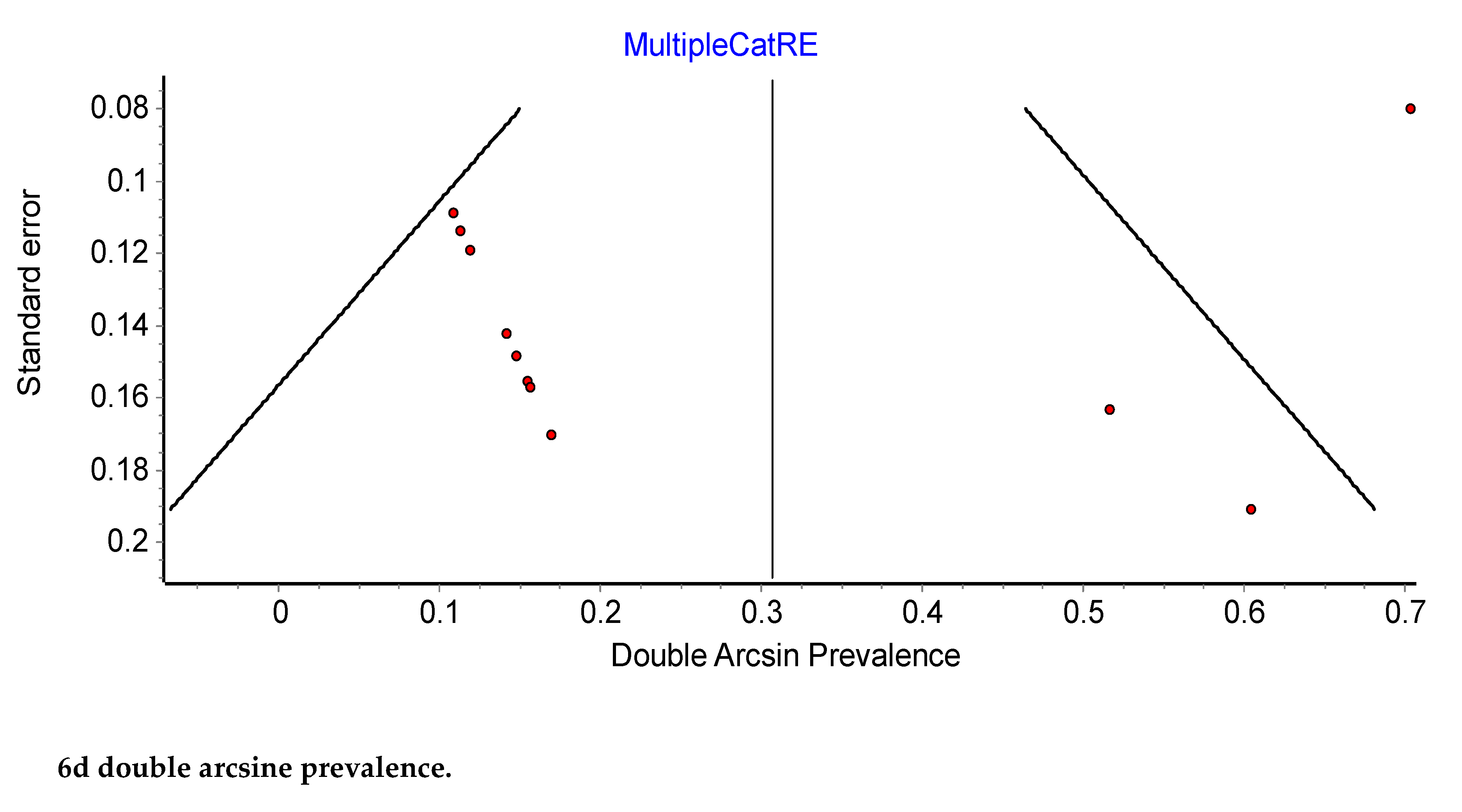
Figure 7.
Prevalence of the Internal Iliac Artery: Type C.
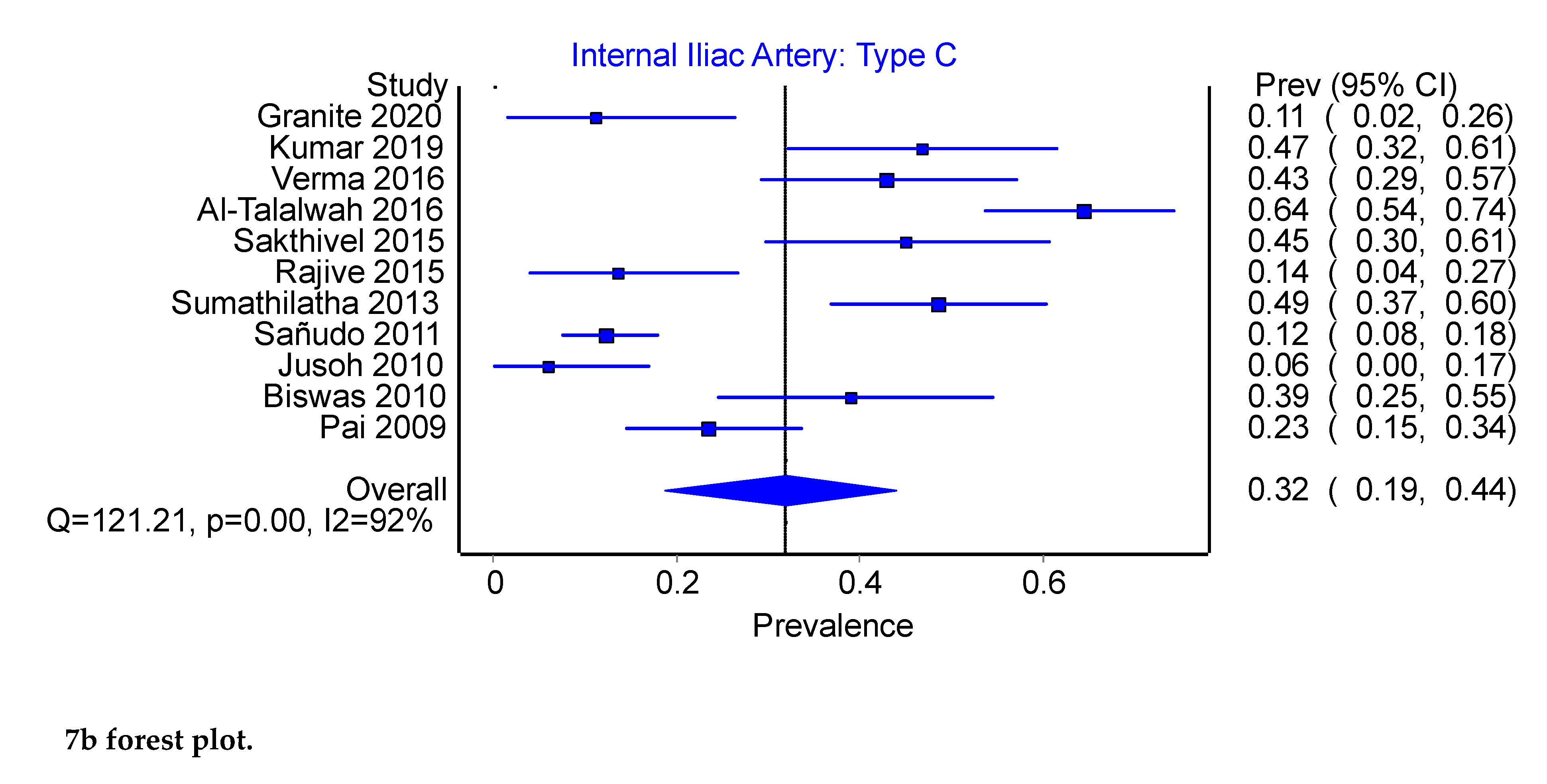
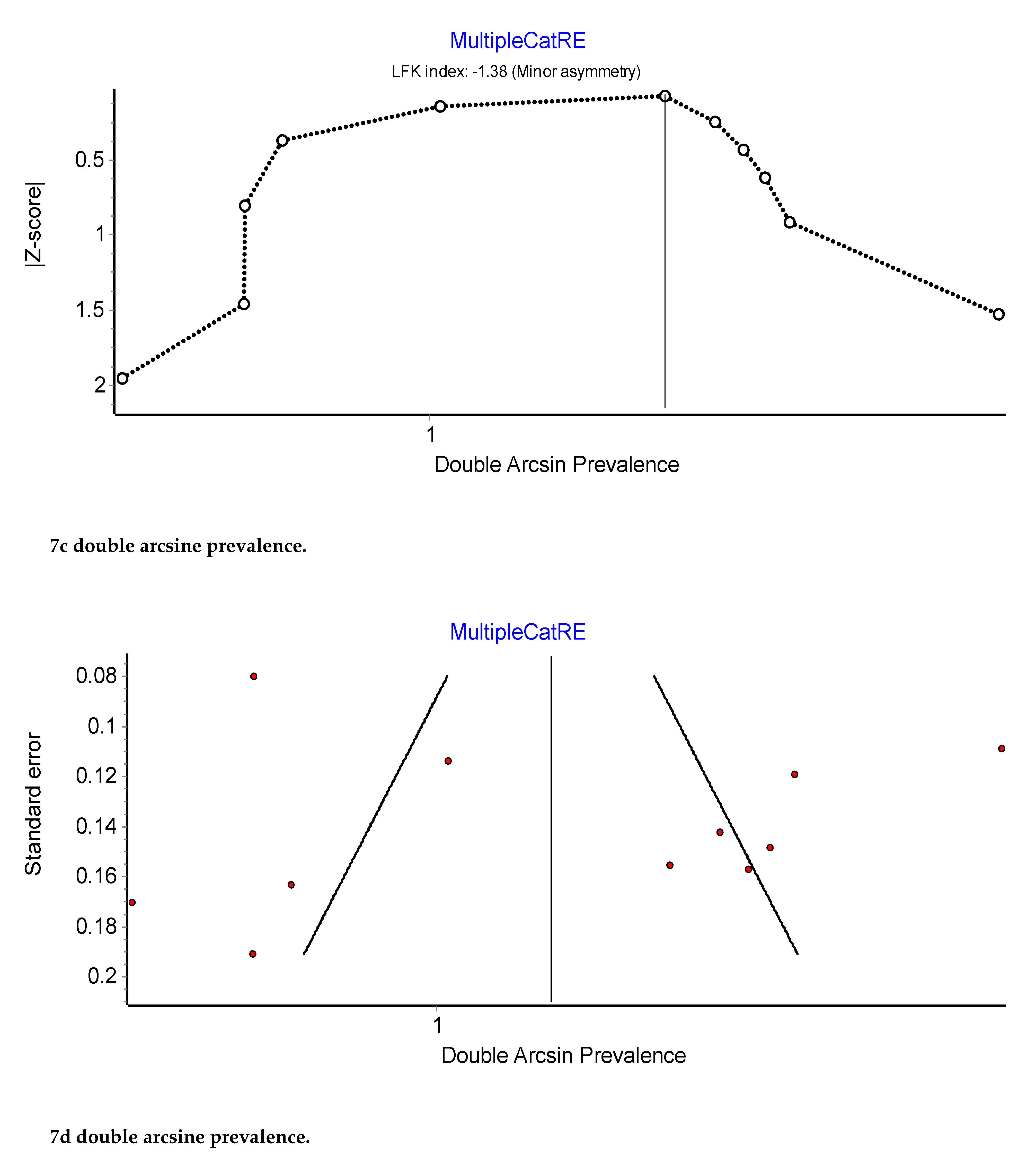
Figure 8.
Prevalence of the Internal Iliac Artery: Type D.
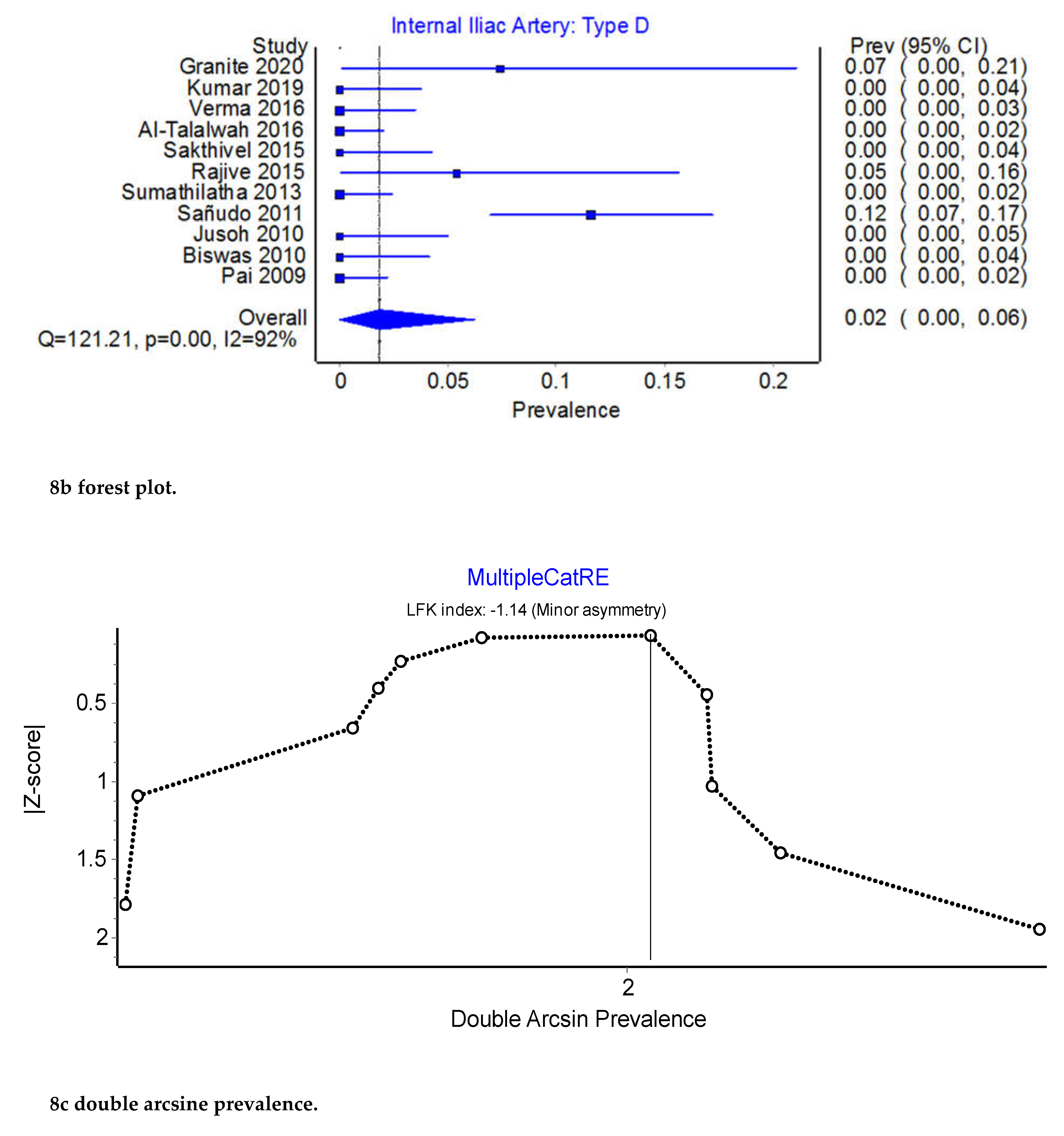
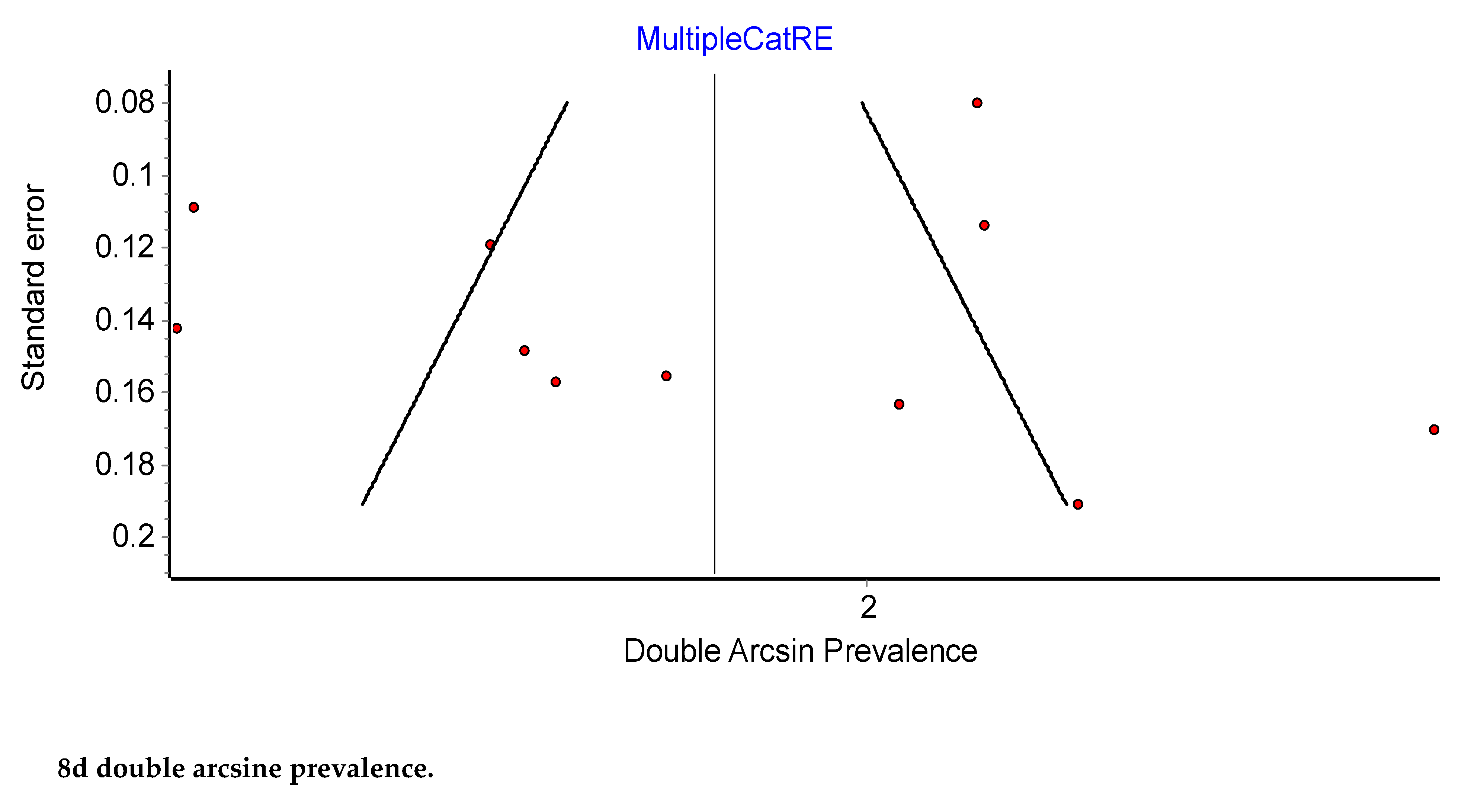
Figure 9.
Type B. Obturator artery arising from the inferior epigastric artery. EIA: external iliac artery; EIV: external iliac vein; IIA: internal iliac artery; IEA: inferior epigastric artery; OA: obturator artery; OM: obturator muscle; OV: obturator vein; P: psoas muscle; U: umbilical artery.
Figure 9.
Type B. Obturator artery arising from the inferior epigastric artery. EIA: external iliac artery; EIV: external iliac vein; IIA: internal iliac artery; IEA: inferior epigastric artery; OA: obturator artery; OM: obturator muscle; OV: obturator vein; P: psoas muscle; U: umbilical artery.
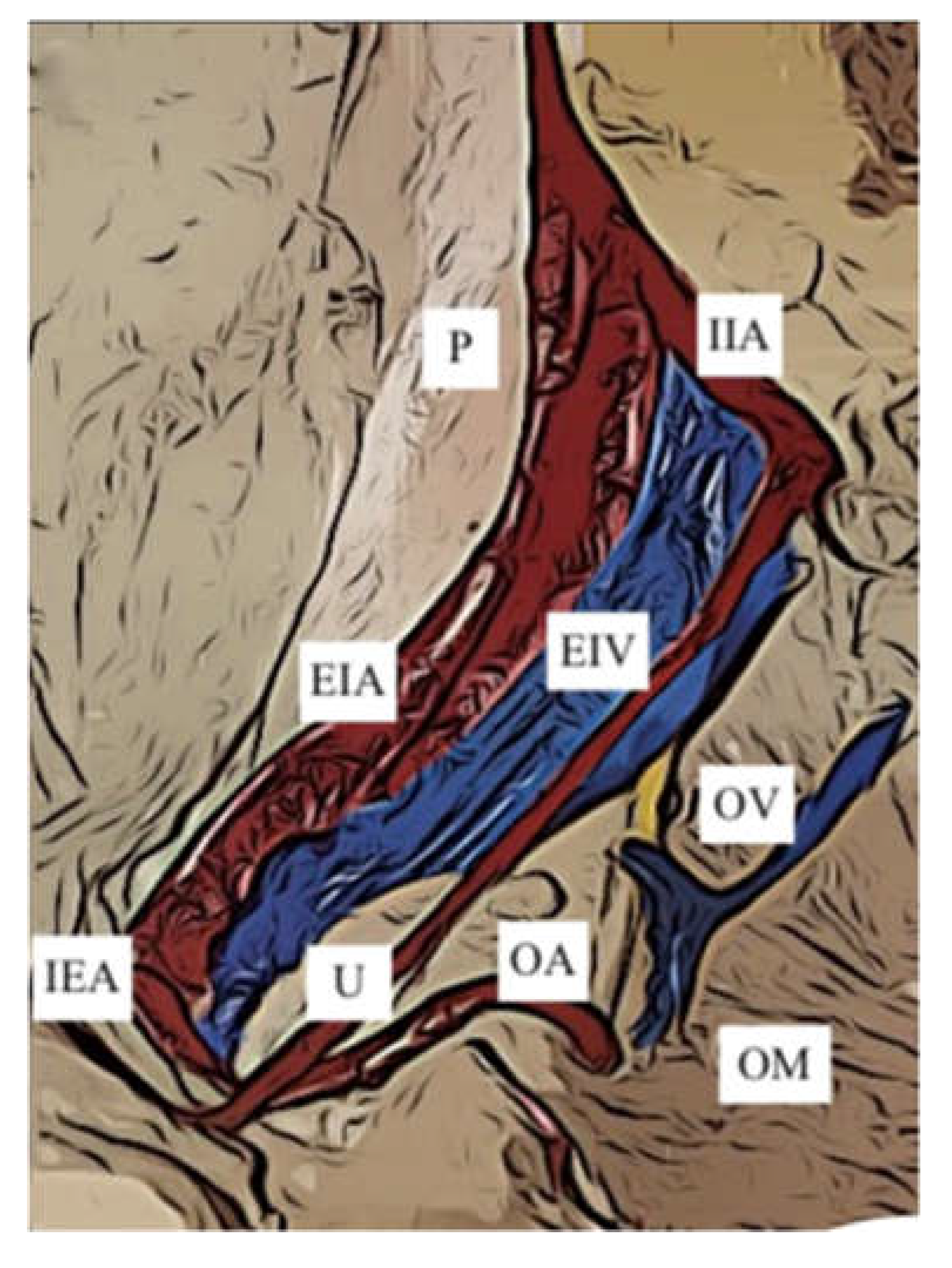
Figure 10.
Type E. Obturator artery arising from the external iliac artery. EIA: external iliac artery; EIV: external iliac vein; IEA: inferior epigastric artery; IIA: internal iliac artery; OA: obturator artery; ON: obturator nerve; OV: obturator vein; P: psoas muscle; PT: posterior trunk of the internal iliac artery; RI: right iliac artery.
Figure 10.
Type E. Obturator artery arising from the external iliac artery. EIA: external iliac artery; EIV: external iliac vein; IEA: inferior epigastric artery; IIA: internal iliac artery; OA: obturator artery; ON: obturator nerve; OV: obturator vein; P: psoas muscle; PT: posterior trunk of the internal iliac artery; RI: right iliac artery.
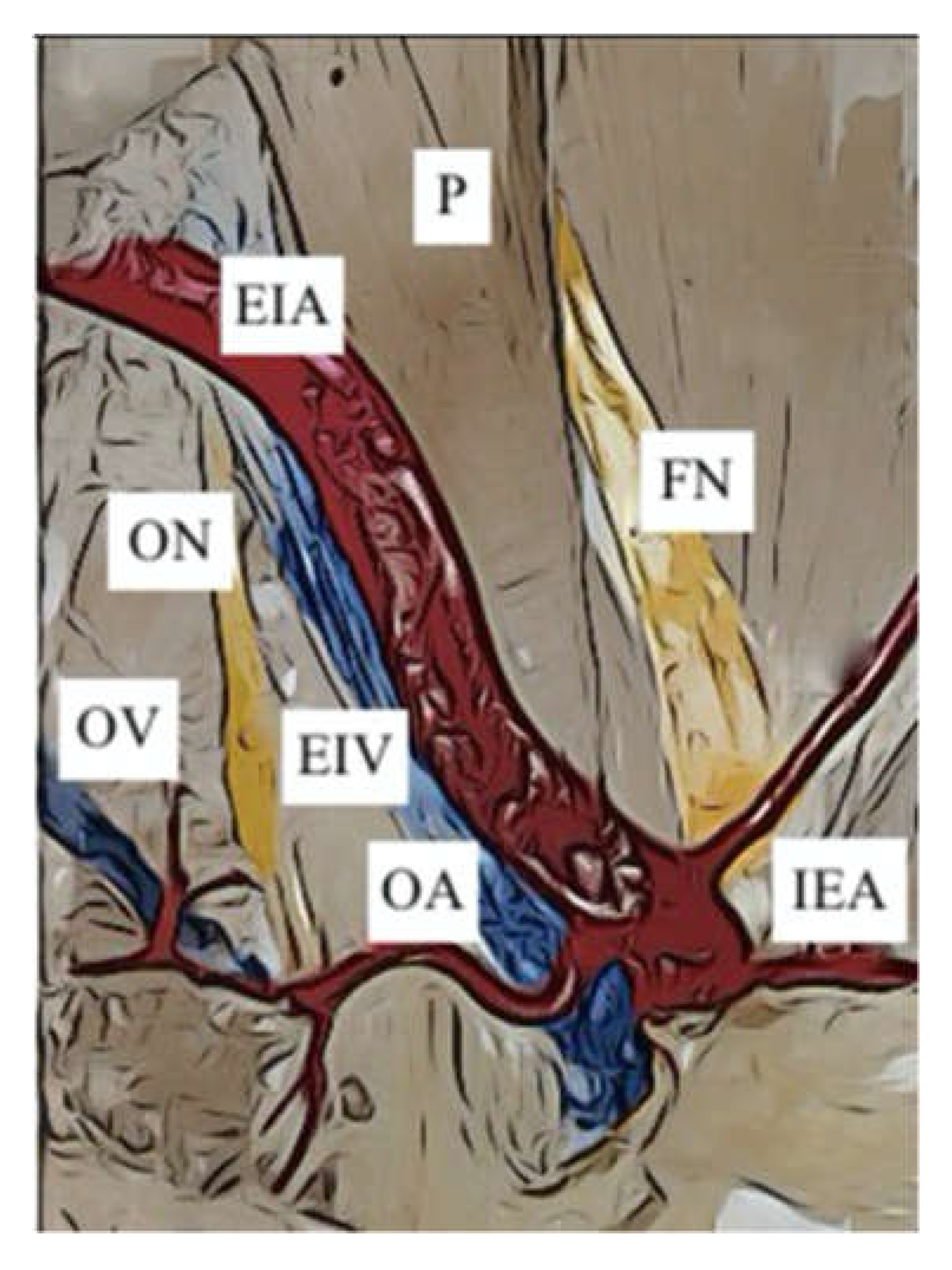
Figure 11.
Prevalence of the External Iliac Artery: Type B.
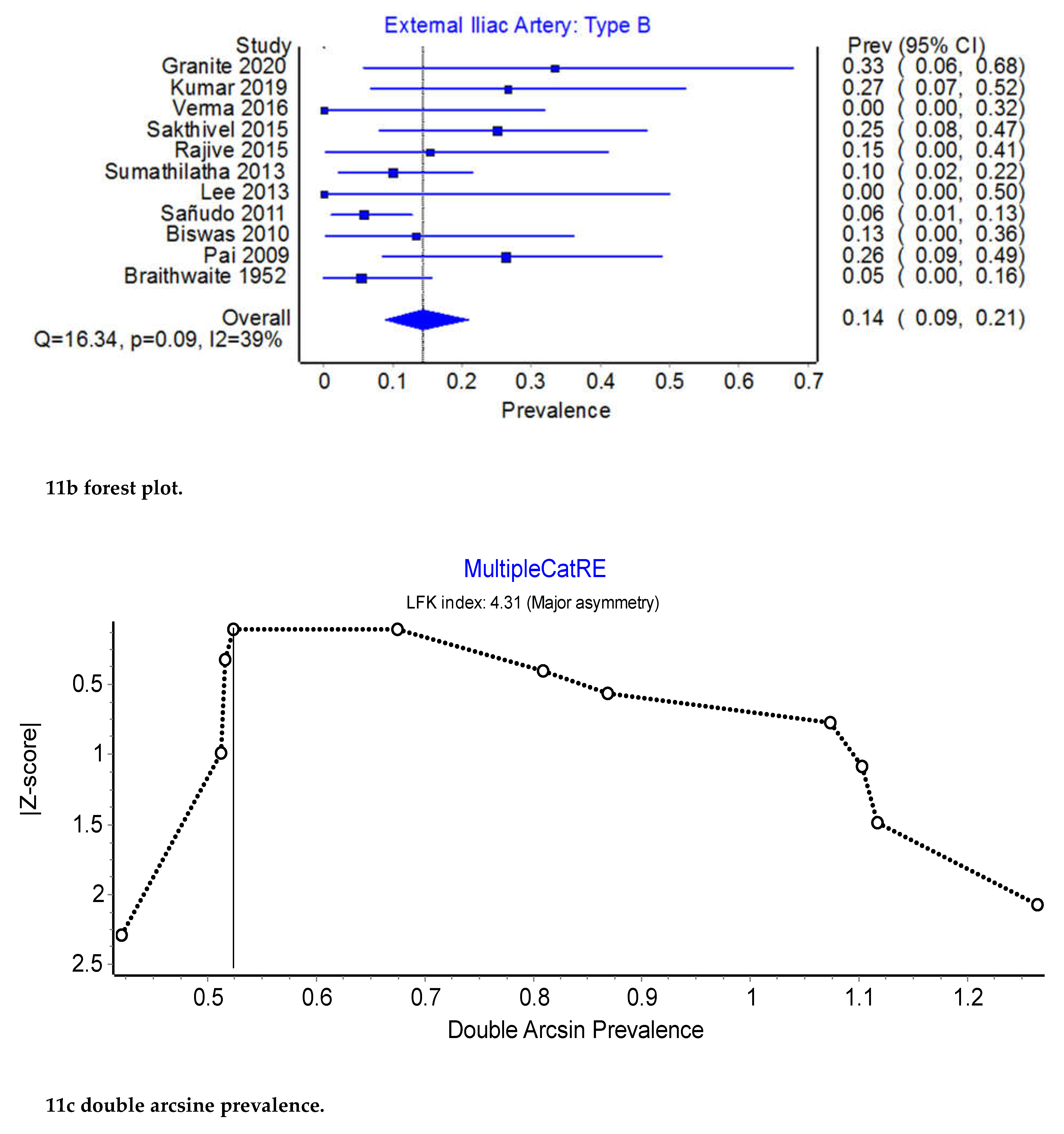
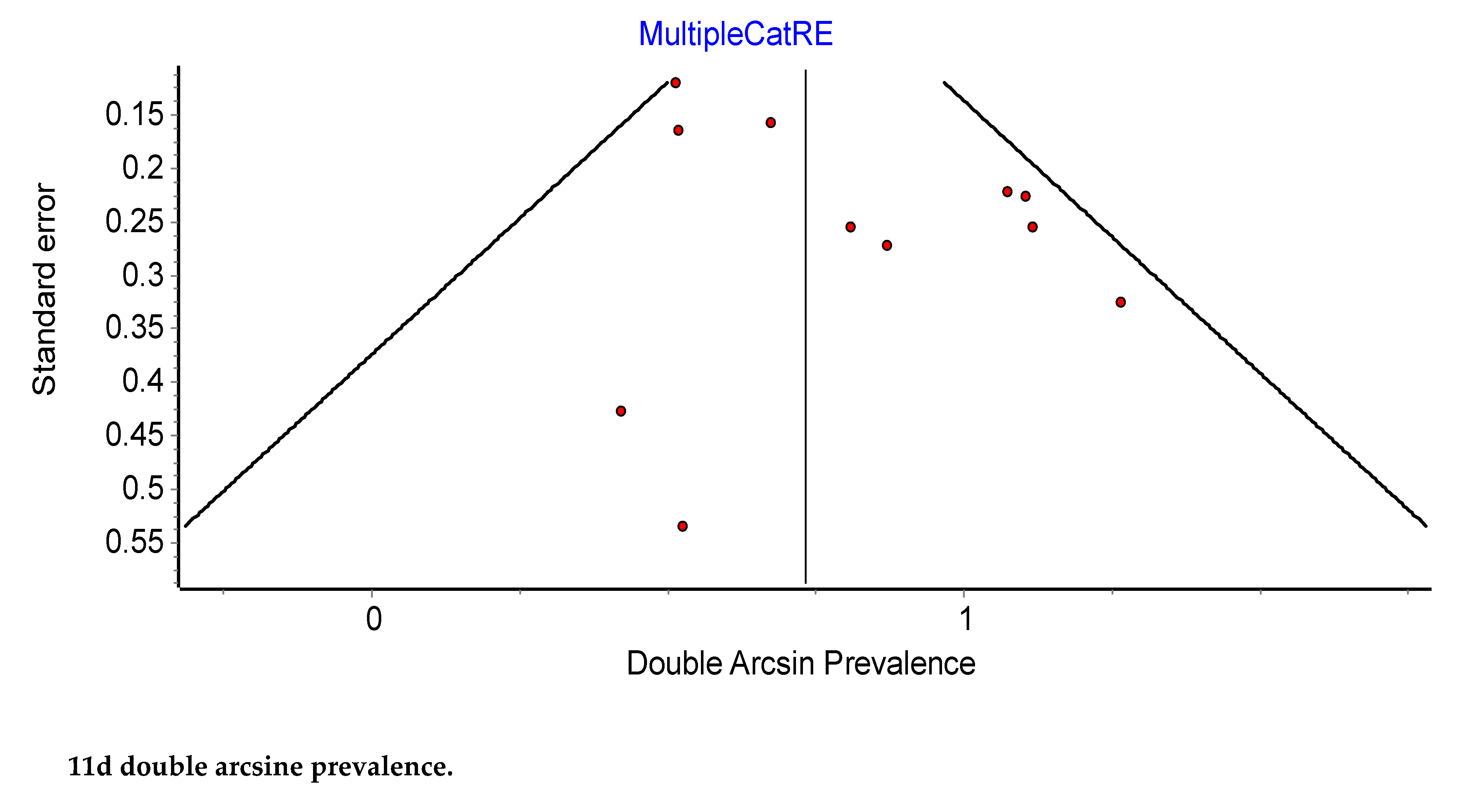
Figure 12.
Prevalence of the External Iliac Artery: Type E.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



