
Submitted:
03 May 2023
Posted:
04 May 2023
You are already at the latest version
Abstract
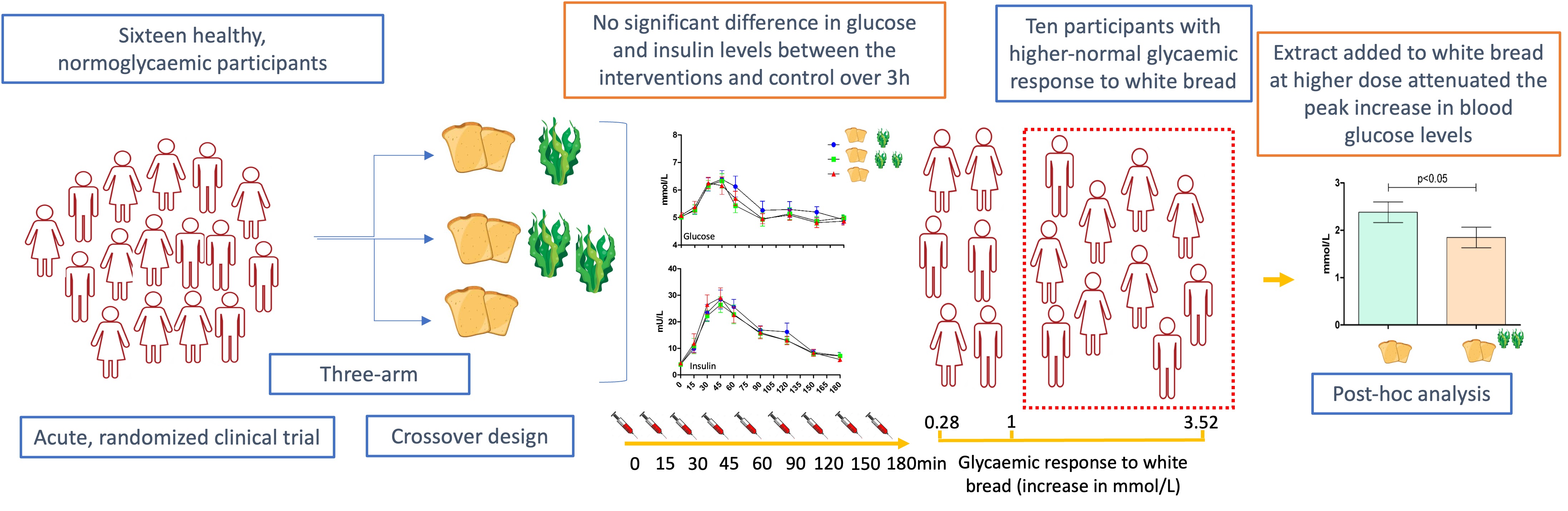
The effects of the consumption of an extract of the brown seaweed Ascophyllum nodosum (BSW) on postprandial glucose and insulin response to white bread were investigated in an acute, randomized, double-blind, three-arm, crossover, controlled trial in healthy, normoglyacemic subjects. Sixteen subjects were administrated either control white bread (50 g total digestible carbohydrates), or white bread with either 500 mg or 1000 mg of BSW extract. Biochemical parameters were measured in venous blood over 3h. Significant inter-individual variation in the glycaemic response to white bread was observed. Analysis of the response of all subjects to either 500 mg or 1000 mg of BSW extract versus control revealed no significant effects of treatments. The variation in response to the control was used to classify individuals into glyacemic responders and non-responders. In the sub-cohort of 10 subjects with peak glucose levels after white bread above 1mmol/L we observed a significant decrease in maximum levels of plasma glucose after the intervention meal with 1000 mg of extract, compared with control. No adverse effects were reported. Further work defining all factors that determine “responders” to the effects of brown seaweed extracts and identify the cohort that would benefit the most from their consumption, is warranted.
Keywords:
brown seaweed
; Ascophyllum nodosum
; refined carbohydrates
; postprandial glycaemia
; insulin
; diabetes
; RCT
; fucoidan
; algal polyphenols
; phlorotaninins
1. Introduction
Numerous global challenges faced by humanity today are directly or indirectly related to food. Countries around the globe are facing major public health challenges due to the increasing prevalence of diet related diseases, including obesity and diabetes, as major risk factors for cardiovascular diseases [1,2] and contributors to mortality [3]. It is estimated that 463 million adults around the globe live with diabetes and about 347 million with impaired glucose tolerance. Incidence of these conditions are projected to increase by up to 50% by 2045 [1]. At the same time, the eating patterns and food system in general are considered environmentally unsustainable [4], with food insecurity on the rise [5].
Starch-rich foods are a staple part of diets across the globe representing an important source of macro and micronutrients and contributing up to 80% of the total energy intake in some countries [6]. In terms of the greenhouse gas emissions, energy, land and water use, waste production and effects on soil, they are considered as more environment-friendly compared to animal foods [7]. However, their effects on human health are not straightforward. Whole grains are recognized as a crucial component of a healthy sustainable diet [7] with their intake positively associated with lower rates of type 2 diabetes [8], CVD and other chronic diseases [9]. However the intake of refined grains and starchy vegetables is found to be associated with a higher risk of diabetes [9], major cardiovascular disease, stroke and early death [10]. Furthermore, while the intake of whole grains is still far below the recommended levels [11], white bread, pastries and other refined grain products remain a staple part of the diet in Western countries, raising the need for an alternative approach to mitigate the adverse effects of high glycaemic index diets on health [12,13].
Food fortification and supplementation of the habitual diet with functional ingredients that have the potential to inhibit or slow down the digestion of carbohydrates and the uptake of simple sugars from the gut, is a promising strategy in lowering the health risks of a starch rich diet [14].
Algae are considered as “blue foods” with the lowest stress on the environment compared to other aquatic organisms [15]. Brown algae are rich sources of nutrients and bioactive compounds shown previously to interact with carbohydrate metabolism [16]. The main brown seaweed bioactives are specific polyphenols, phlorotannins, and bioactive sulfated polysaccharides [17]. In vitro inhibition of enzymes of carbohydrate digestion, salivary and pancreatic α-amylases and α-glucosidases [16,18,19,20], and inhibition of trans-epithelial glucose transport [21], are the main mechanisms of action of brown seaweed bioactives that rationalize further studies in humans.
Despite the potential of brown seaweed extracts to modulate carbohydrate metabolism, demonstrated in vitro, their effects on biomarkers of postprandial glycaemic control in humans are limited and often inconsistent [22,23]. Factors potentially responsible for this inconsistency may include incomplete characterization of the extract [24] and observed variation in the composition of the extract across studies [22], along with the lack of information of the interaction of the main bioactives in vivo.
At the same time glycaemic response to carbohydrates is shown to vary significantly between individuals [25], and depends on subject characteristics, such as health status, age and sex [26], diet [27], physical activity [28], ethnicity [24] etc. Another phenotype feature shown to influence the glycaemic response to white bread and starchy foods is the level of the initial enzyme in starch digestion - salivary amylase [29]. As far as the authors are aware, the impact of salivary amylase levels on the potential of bioactive compounds to inhibit digestion of starch has not been investigated before.
We have reported previously the comparative analysis of the chemical composition of several brown seaweed extracts from different algal species and the correlation with their potential to inhibit several enzymes of carbohydrate digestion [18]. The chemical composition of the Ascophyllum nodosum extract was characterized by the unique composition of the fucoidan fraction, in terms of the size distribution, and the specific ratio of polyphenols and fucoidans, which was found to be relevant for the observed inhibition of alpha-glucosidases (maltase and sucrase) in vitro [18].
The present study aims to assess the effects of this brown seaweed Ascophyllum nodosum extract on postprandial glucose and insulin levels in response to white bread in normoglycaemic, healthy subjects. The role of the variation in the glycaemic response to white bread was also addressed.
2. Results
2.1. Participant Characteristics
Baseline characteristics of participants are presented in Table 1. Sixteen volunteers, 9 women and 7 men completed the study. Values for all biochemical parameters were in the normal range, including biochemical parameters of cardiometabolic risk. Systolic blood pressure (SDB) and diastolic blood pressure (DBP) were also within the normal values. Based on calculated body mass index (BMI) values, 4/16 participants were overweight (24.9-30kg/m2) and one was obese (>30kg/m2).
The distribution of fasting glucose levels at each of the 3 intervention days is shown in Figure S1 in the supplementary material. No differences in fasting glucose or insulin were found between the intervention days.
The distribution of fasting glucose values (Co) and maximal postprandial glucose values (Cmax) in response to control and intervention meals is shown in Figure 1, where a large distribution of response is seen across the population group after each intervention.
2.2. Effects on Postprandial Glucose Levels
No time x treatment interaction was found in the repeated measures of glucose levels (Figure 2). Peak plasma glucose concentrations (Cmax) were reached 30 min after the control meal, and 45 min after low dose brown seaweed meal (LDM) and high dose brown seaweed meal (HDM) (Figure 2). Incremental Cmax values after the control, LDM and HDM intervention were 1.7 (±1.06) mmol/L; 1.81 (±1.12) mmol/L and 1.56 (±0.71) mmol/L, respectively, as mean (±SD), with no significant difference observed between them.
No significant difference was observed either at any time point on glucose concentrations or incremental areas under the curve (iAUC). IAUC values for glucose over 180 min after the control, LDM and HDM intervention were 79.52 (±67.15) mmol x min/L; 116.4 (±19.8) mmol x min/ L and 81.25 (±63.44) mmol x min/L, respectively, as mean (±SD).
The peak glucose concentration (Cmax) for the control meal (white bread) for all 16 subjects was 6.78 (±1.11) mmol/L and the incremental peak glucose concentration (iCmax) was 1.7 (±1.06) mmol/L, as mean (±SD), with the range of 0.28-3.52 mmol/L. Six out of sixteen subjects had incremental glucose response to the control meal lower than 1 mmol/L.
Based on the response to the carbohydrate load of the control meal, and using 1 mmol/L as a reproducibly measurable increase for iCmax, we defined the “lower-normal” and “higher-normal” responder sub-cohorts, with the range in iCmax values between 0.28-0.97 mmol/L, and 1.33-3.52 mmol/L respectively. The values for parameters of postprandial glycaemia after the consumption of control meal in two sub-cohorts were given in the Table 2, with the significant difference between sub-cohorts observed for all of the parameters. Importantly, there was no observed difference in the fasting glucose levels between two sub-cohorts.
In the “higher-normal“ sub-cohort we observed the time × treatment interaction in the repeated measures of glucose levels and a significant difference between both Cmax and iCmax values after HDM compared to the control meal (p<0.05) (Figure 4). Incremental Cmax values after the control and HDM intervention were 2.38 (±0.69) mmol/L, and 1.85 (±0.69) mmol/L, respectively, indicating that the brown seaweed extract decreased the peak glucose concentration after the consumption of white bread by 22.3%. There was no effect of the intervention on iCmax in the lower-normal subcohort (Figure S2).
2.3. Effects on Postprandial Insulin Levels
No time × treatment interaction was found in the repeated measures of insulin level. No significant difference was observed at any time point on insulin concentrations or incremental areas under the insulin curve over 180 min after the control, LDM and HDM intervention. Peak plasma insulin concentrations (Cmax) were reached at 45 min with all 3 intervention meals (Figure 4). Incremental peak insulin levels (iCmax) after the control, LDM and HDM intervention as mean (±SD), were 29.48 (±14.14) mU/L; 26.8 (±13.45) mU/L and 29.93 (±15.64) mU/L and iAUC values over 3h were 2201.61 (±986.54) mU x min/L, 1915.66 (±899.18) mU x min/L and 2086.05 (±953.97) mU x min/L, respectively.
Insulin level, incremental insulin level or iAUC for insulin after the consumption of control meal between the two sub-cohorts were not significantly different. No time × treatment interactions were found in the repeated measures for any of the analyzed parameters either.
No adverse or unexpected effects immediately following consumption, during 24 h after the consumption or anytime between two study visits were reported.
3. Discussion
In this acute, randomized, crossover study we investigated if the extract obtained from the brown seaweed Ascophyllum nodosum can modulate the rise in blood glucose and insulin levels observed in healthy subjects following consumption of a refined carbohydrate-rich meal.
A significant variation in the glycaemic response to the starch-rich meal (white bread) between subjects was observed in the trial. Significant effects on either glucose or insulin levels were not observed in the total group of 16 subjects included in the trial. However, a shift in the time of the detected peak glucose values (tmax), from 30 min after the control meal to 45 min was observed after both intervention meals (with either low or high dose of the extract). Clustering the subjects into two sub-cohorts based on their peak glucose response to the control meal allowed comparison of responders with significantly different responses from baseline to the carbohydrate load, in terms of iCmax, Cmax or iAUC for glucose. In the sub-cohort of “higher-normal” responders, the brown seaweed extract significantly decreased the maximum incremental concentration of glucose after the starch-rich meal by 22% (p<0.05). This supports the hypothesis that the apparent efficacy of the brown seaweed extract could depend on the individual`s glycaemic response to the carbohydrate load, with the extract primarily affecting subjects with higher spikes in glucose levels.
Postprandial hyperglycaemia is a well-established, independent cardiovascular risk factor in patients with diabetes [30]. Moreover, epidemiological data indicates that it can be considered as an independent predictor of cardiovascular events even in non-diabetic subjects [31]. The adverse effects of increased glucose levels following a meal are mediated by oxidative stress, directly proportional to glucose levels, that subsequently triggers an inflammatory response and impaired endothelial function, activates platelets and other atherotrombotic factors [31]. A significant decrease in flow mediated vasodilatation, as a parameter of endothelial function, was observed in healthy subjects an hour after the consumption of a meal containing 40 g of carbohydrates [32]. The impairment of endothelial function induced by 75 g of glucose persisted even longer [32]. There is a hypothesis that atherosclerosis, the underlying cause of the vast majority of cardiovascular events, is a postprandial phenomenon [33]. It is evident that the risk caused by postprandial hyperglycaemia correlates with the level of hyperglycaemia itself, rather than fasting glucose values, and its modulation in normoglycaemic individuals is considered a rational approach in lowering the risk [34]. Our results have shown that subjects at higher risk in terms of postprandial hyperglycaemia responded to the intervention with the brown seaweed Ascophyllum nodosum extract.
In a recent study, Hall et al. used continuous glucose monitoring to evaluate the frequency of elevations in postprandial glucose over 2-4 weeks. They identified three “glucotypes”i.e. glucose fluctuation patterns: low-variability, moderate variability and severe variability pattern [35]. The evaluation of the glycemic responses to standardized meals highlighted the personal nature of glucose regulation with further confirmation of the unfavorable effects of meals with refined carbohydrates. These types of meals were shown to cause significant increase in glycaemia and a longer time in the pre-diabetic and diabetic range even in subjects with normal outcomes from standardized tests: fasting glucose, HbA1c and postprandial response to glucose [35]. Our results rationalize further investigation of the effects of brown seaweed bioactives, targeted specifically to the most vulnerable “glucotypes”.
The number of previous studies that tested the impact of brown seaweed extract on glycaemic control after a meal is limited. Paradis et al. [23] investigated the effect of a polyphenol-rich extract from Ascophyllum nodosum and Fucus vesiculosus on postprandial glycaemia/insulinemia induced by white bread. They reported the reduction in incremental area under the insulin curve and insulin sensitivity, without the observed effects on glycaemia. The authors did not address the role of the response to the control meal, but the reported data show that mean peak glucose values for the total cohort were higher than in our cohort. In our study there was no significant effect observed on insulin at any time point. However, acknowledging the importance and health benefits of the improved insulin sensitivity, we prioritized the attenuation of postprandial glycaemia (defined as a primary outcome) as it directly correlates with acute change in biomarkers of CVD risk, while there was no correlation with insulin [36]. Additionally, reducing postprandial glycaemia without increasing insulin level is considered as a beneficial postprandial effect as defined by the EFSA NDA Panel ( [37].
In another set of studies, the role of postprandial glycaemic response was examined by testing the effects of Fucus vesiculosus extract on glycaemia and insulinemia in response to white bread in the mornings and evenings. The studies reported lower responses to the challenge meal in the mornings than the evenings [24,38]. However, there was no effect of the treatments in both settings on either postprandial glucose or insulin levels. The chemical analysis of several algal extracts on the market, including the one used in this trail, have shown that this Ascophyllum nodosum extract has a unique composition, regarding both polyphenols and poly/oligosaccharides [18]. Importantly, the mechanisms of enzyme inhibition were shown to be different, which could explain the difference in the observed in vivo effects to previous studies [18].
Whilst no effect was seen on the total population, the current study identified a cohort who were responsive to the treatments. In nutrition research, individuals’ responses to dietary interventions are known to be highly variable [25,39,40]. It is important to identify and understand these variances, not only can they affect the interpretation of the results, but they can also support the development of tailored nutrition advice and delivery of personalised nutrition [41]. Tailoring nutrition or dietary advice to an individual based on their needs and requirements is known as precision nutrition and this approach can improve overall health as well as reducing the risk of diet-related diseases [42,43]. Similar to our study, Wascher et al. [36] examined the effects of acarbose on flow mediated vasodilatation (FMD) decrease in response to sucrose load in subjects with impaired glucose tolerance. The authors also performed sub-analysis with respect to glycaemic responders to the challenge meal. In the study cohort, the subjects above the median of the glycaemic response to sucrose, administering acarbose resulted in both reduction of postprandial glycaemia and improvement in FMD. However, in the group bellow the median the response to sucrose was significantly lower, the FMD did not change and there was no effect of acarbose on either postprandial glycaemia or FMD [36].
Synthetic alpha-glucosidase inhibitors (acarbose, voglibose and miglitol) are therapeutics used for the treatment or prevention of type 2 diabetes and its complications [44]. They have been shown to be effective in modulating postprandial hyperglycaemia and lowering glycated haemoglobin [45]. At the same time, they have a significant side effects profile, with abdominal symptoms (i.e. flatulence, abdominal fullness) reported in approximately 50% of patients [46]. Natural inhibitors of carbohydrate digestion enzymes with less side effects are widely promoted as a rational alternative [47], especially in healthy subjects and subjects at risk of developing diabetes, taking into account the risk level and an acceptable ratio between the safety and efficacy [48].
There are some limitations in this study. Our primary outcome was iCmax, however, the participants were not recruited based on iCmax or any other parameter of glycaemic control. Secondly, the number of participants was calculated based on the results from a pilot study that reported a 50% higher iCmax value in response to a control meal. In addition, the study wasn`t controlled for various factors reported to affect postprandial glycaemic response that might have contributed to the observed inter-individual variability. We did however try to minimise the intra-individual variability by controlling some of those factors (diet, physical activity, stress) at the individual level.
In conclusion, our results demonstrate that 1000 mg of an Ascophyllum nodosum extract has the potential to modulate postprandial glycaemic response to a 50g carbohydrate load from white bread. This effect was specifically shown in the sub-cohort of subjects with a sizeable glycaemic response (>1 mmol/l) to the challenge meal. This finding suggests that the 1000 mg treatment would be beneficial in subjects who may be at higher risk for postprandial hyperglycaemia. Further study of the phenotype and/or genotype profiles that may define the consistent response to Ascophyllum nodosum bioactives, and their effects on carbohydrate digestion and postprandial glycaemic control, is needed. Ascophyllum nodosum is an abundant source of nutrients and non-nutritive compounds, which as part of blue food, has an important role in the shift towards healthy and sustainable food systems. However, strong evidence of its effect on health, and a clear understanding of who may benefit the most from its consumption, is essential for its use as a food or nutraceutical.
4. Materials and Methods
4.1. Study Design
This study was designed as an acute, randomized, double-blind, three-arm, crossover, controlled trial. The study was approved by UCD Ethics Committee, and it was performed in accordance with the Declaration of Helsinki, at the UCD Institute of Food and Health, Ireland. Participants provided the informed consent before participating in any trial related procedures, and were assigned with an anonymized study ID. This trial was registered at clinicaltrials.gov (NCT05460884).
4.2. Participants
Participants were recruited through public adverts (posters and leaflets) displayed around and in the proximity of the campus. Inclusion criteria were as follows: healthy, i.e. with no known health problems, and age between 18-60 years. Exclusion criteria included smoking, pregnancy or lactation, previous diagnosis of any chronic illness (including diabetes, hypertension, gastrointestinal diseases etc.), long-term prescribed medical therapy (except contraceptives), allergy to fruits, vegetables, pollen, seafood or seaweed. A special diet or dietary regimen (for weight management or regularly consuming fruit and herbal extract supplements), blood donation within 4 weeks before study commenced or an intention to donate blood during the study or less than 4 weeks after the last study visit, and participation in another trial that involves dietary intervention or sampling of blood, were also considered as exclusion criteria. Participants were assessed for eligibility and recruited on ongoing basis to complete the study with16 subjects.
4.3. Study Protocol
Participants recruited for the study were scheduled for 3 study visits, at least 7 days apart. The allocation sequence of three interventions was generated by block randomization (block size of 6) using a computer random number generator (https://www.randomizer.org/).
Before the first study visit, participants were instructed to follow and record their usual diet and physical activity (PA) over the 3 days preceding the study. Participants were asked to follow the same dietary and PA regiment for 3 days before the next study visits and record their diet and PA again. On each study visit all participants were instructed to fast for 12 h before their arrival, but to freely consume water and to have at least 7 h of sleep. After arriving at the site (Human Intervention Suite at the UCD Institute for Food and Health) between 7.30 and 9 and after an initial 10 min rest, blood pressure, heart rate measurements, anthropometric and body composition assessments were completed. Participants rested for 20 minutes before providing the first saliva, following which, a nurse placed a cannula in an antecubital vein without taking any blood. A second sample of saliva was collected, followed by the baseline blood collection. Participants were then served the test meal (described below) and the time needed to complete consumption was recorded. All participants completed all test meals (100% compliance) and there were no dropouts during the study. Blood samples were collected again at 15, 30, 45, 60, 90, 120, 150 and 180min after the first bite was reported to be swallowed. Participants rested in a reclined position and remained sedentary for the duration of the study day. Each visit lasted ~4 hours and following completion participants were provided with lunch.
During each study visit, participants were given a list of common adverse and unexpected effects observed in clinical trials and asked to report if they experienced any of them immediately following consumption, during 24 h after the consumption or anytime between two study visits.
4.4. Anthropometric, Body Composition, Blood Pressure and Heart Rate Measurements
Body height (cm) was measured using a stadiometer, and weight (kg), BMI, and body composition parameters (%fat, total fat, total visceral mass) were measured using a dual frequency bioimpendance scale (Tanita, model DC430MA). Blood pressure and heart rate were measured using a digital blood pressure monitor (OMRON M6 Comfort, Omron Healthcare Co, LTD, Kyoto, Japan). Blood pressure and heart rate were measured 3 times consecutively, and if the variation was less than 10%, the average value was calculated.
4.5. Blood Collection and Biochemical Analyses
The first 2 mL of each blood sample drawn were discarded, followed by collection in 3 different tubes (Vacuette®, Greiner bio-one): NaF /K-Oxalate tube for isolation of plasma (for glucose levels), K2EDTA for plasma (for insulin levels) and clot activator tubes for serum. Tubes for plasma separation were kept on ice and centrifuged immediately, at 1100 g for 10 minutes, aliquoted and stored at -80°C until further analysis. After at least 30 min at RT to allow clotting, serum was isolated by centrifugation (1100 g, 10 min, RT), samples were aliquoted and stored at -80°C until further analysis.
Glucose in plasma, and total triglycerides (TG), low-density lipoprotein cholesterol (LDLc), high-density lipoprotein cholesterol (HDLc), and total cholesterol (TC) in serum were measured using an enzymatic and colorimetric assay on a Pentra C400 Clinical Chemistry analyzer (HORIBA Medical, France). Insulin was determined by ELISA (Mercodia AB, Uppsala, Sweden).
4.6. Saliva Collection and Analysis
Unstimulated total saliva was collected by direct expectoration (spitting) method, as previously described [49]. Briefly, at each time point, subjects were seated comfortably and asked to allow spontaneous saliva flow during 1 min and expectorate the whole saliva content into previously weighed, sterile plastic tubes. This was repeated 3 times over 3 minutes, and samples were combined. Tubes were weighed, and stored immediately at -80 °C for at least 4h to allow mucin to precipitate, thawed on ice, centrifuged for 15 min at 1500 x g, at 4 °C, separated from the sediment and aliquoted. Salivary flow rate was calculated by dividing the sample volume (mL) with the time (min) taken to produce it. For the estimation of salivary flow rate, it was assumed that saliva density was 1.00 g/mL. Amylase activity was determined using commercial enzymatic assay (Salimetrics, PA, USA). Salivary amylase secretion rate (U/min) was calculated as amylase activity in the volume of saliva secreted per minute.
4.7. Intervention and Control Meal
The tested product was a commercial, proprietary extract of the brown seaweed Ascophyllum nodosum, kindly provided by the company (Marigot Ltd). The source and the chemical caracterization of the extract used in the intervention, and its effect on the enzymes of carbohydrate digestion were reported previously [18]. Briefly, the content of polyphenols, as mean (±SD), was 6.57 (±0.33) w/w% and the fucoidan content, calculated as the sum of fucose, sulphate and other monosaccharides, was 19.34 (±0.14) w/w% [18]. The concentrations of the extract that induced 50% inhibition of maltase (10 mm) and sucrase (25mM) activity (IC50 values) were 0.26 (±0.01) mg/mL and 0.83 (±0.21) mg/mL, respectively [18]. The extract was tested by Southern Scientific Services Ltd, a third-party laboratory, for its chemical and microbiological safety, and the intake of micronutrients present (i.e. iodine) with the intervention was confirmed to be in line with the recommendations [50]. Two different doses of the extract, 500 mg and 1000 mg per meal, were tested. Extracts were pre-measured in the test tubes labelled with the random intervention codes. Empty tubes labeled with the codes according to the allocation sequence indicated the control intervention. For the duration of the study all tubes were stored at -20 °C in a humidity protected environment.
The control meal consisted of 108g or appx. 2 white bread buns (Bundy`s originals, Johnston Mooney & O’Brien Bakery, Dublin, Ireland) that provided 50 g of available carbohydrates as measured by the commercial kit (Megazyme International Ireland Ltd., Bray, Ireland), and was always served fresh.
The intervention meal consisted of the same amount of white bread (108g or appx. 2 buns) and either 500 mg or 1000 mg of the brown seaweed extract distributed evenly between the two bun halves. Intervention and control meals were prepared daily according to the allocation sequence by technical staff not included in the trial and served in a double blinded fashion (participant and researchers). However, due to the taste of the extract subjects were ultimately not considered as blinded as they reported post hoc the taste revealed the higher dose intervention.
4.8. Statistical Analysis
The change in the maximal incremental plasma glucose level (iCmax) between baseline and endpoint within intervention groups vs. control was predefined as the primary outcome measure of the study. Changes in the insulin levels and the incremental area under the curve (iAUC) were secondary outcome measures. Area under curve (AUC) for glucose and insulin were calculated using the trapezoidal rule and net AUC was calculated by subtracting the AUC below baseline values. Normality of the obtained data was analyzed by the Shapiro–Wilk test. The repeated measures ANOVA with subjects as fixed effects and treatment and time as repeated measures was employed to analyze glucose and insulin levels over time, with Bonferroni adjustment for multiple comparisons. Correlation was evaluated with Pearson or Spearman correlation as appropriate. Differences were considered significant at P< 0.05. Data in the text and tables are shown as mean (±standard deviation; SD). In the figures, data are presented as mean ((±standard error; SE). Statistical analyses were performed with SPSS software (version 27, IBM SPSS Statistics). GraphPad Prism (version 7.02; Graphpad Software, CA, USA) was used for graphical representation. The sample size was determined based on Cmax for glucose reduction as the primary outcome, obtained in a pilot study with a statistical power of 80%.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org. Figure S1: Scatter-plot of fasting blood glucose levels at each study visit; Figure S2: Incremental peak glucose concentration in a sub-cohort of 6 “lower-normal” responders; Figure S3: Graphical representation of the study design; Figure S4: Consort-2010-flow-diagram; Table S1: Consort-2010-checklist.
Author Contributions
Conceptualization, A.K.R., E.R.G, S.R. and S.O’C.; methodology, A.K.R., E.R.G and S.O’C.; validation, A.K.R. and E.R.G; formal analysis, A.K.R. and E.R.G.; investigation, A.K.R. and E.R.G.; resources, A.K.R. and E.R.G.; data curation, A.K.R. and E.R.G.; writing—original draft preparation, A.K.R. and E.R.G.; writing—review and editing, A.K.R., E.R.G., S.R., M.A. and S.O’C; visualization, A.K.R.; funding acquisition, A.K.R., E.R.G, S.R. and S.O’C. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the Marie Sklodowska Curie Career-FIT Fellowship grant received by AKR. Carrer-FIT has received funding from the European Union’s Horizon2020 research and innovation programme under the Marie Sklodowska-Curie grant agreement No.13654.
Institutional Review Board Statement
The study protocol (LS-19-84-Ristic-Gibney) was assessed and approved by the UCD Human Research Ethics Committee on 20th of December 2019 (REC Ref. No. HREC-LS-19-295522). The study was conducted from autumn 2020 to autumn 2022 at the UCD Institute of Food and Health, Ireland, and in accordance with the Declaration of Helsinki of 1975, revised in 2013. All subjects provided their informed consent for inclusion before they participated in any trial related procedures, and were assigned with an anonymized study ID.
Informed Consent
The informed consent was also obtained from all subjects for the use of their anonymized data in the publication of scientific papers. This trial was registered at clinicaltrials.gov (NCT05460884).
Data Availability Statement
The access to study data is controlled. The data may be shared for further collaborative research projects in anonymized form, after reviewing data access requests and by following the “Good Practice Principles for Sharing Individual Participant Data from Publicly Funded Clinical Trials”. (Tudur Smith C, Hopkins C, Sydes M, Woolfall K, Clarke M, Murray G, Williamson P., 2015; https://www.ukri.org/wp-content/uploads/2021/08/MRC-12082021-Datasharingguidance2015.pdf, assessed December 2019). Consent to share the data for such purposes is requested in the study consent form.
Acknowledgments
The brown seaweed extract was provided by Marigot Ltd.
Conflicts of Interest
The study was funded by the European Union’s Horizon 2020. The company Marigot Ltd. supplied the investigated product and provided support in the form of salary for S.R., M. A. and S.O’C. They had no control of the title, scientific content, methodology, results and conclusions. Their participation in the research did not affect the outcome or the dissemination of the outcome or when and where findings should be presented and published. The research was performed independently of the funding agency and the industrial partner and was not influenced by them. AKR and ERG declare no conflict of interest.
References
- Saeedi, P.; Petersohn, I.; Salpea, P.; Malanda, B.; Karuranga, S.; Unwin, N.; Colagiuri, S.; Guariguata, L.; Motala, A.A.; Ogurtsova, K.; Shaw, J.E.; Bright, D.; Williams, R.; Committee, I.D.F.D.A. Global and regional diabetes prevalence estimates for 2019 and projections for 2030 and 2045: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract 2019, 157, 107843. [Google Scholar] [CrossRef] [PubMed]
- Townsend, N.; Kazakiewicz, D.; Lucy Wright, F.; Timmis, A.; Huculeci, R.; Torbica, A.; Gale, C.P.; Achenbach, S.; Weidinger, F.; Vardas, P. Epidemiology of cardiovascular disease in Europe. Nat Rev Cardiol 2022, 19, 133–143. [Google Scholar] [CrossRef] [PubMed]
- Saeedi, P.; Salpea, P.; Karuranga, S.; Petersohn, I.; Malanda, B.; Gregg, E.W.; Unwin, N.; Wild, S.H.; Williams, R. Mortality attributable to diabetes in 20-79 years old adults, 2019 estimates: Results from the International Diabetes Federation Diabetes Atlas, 9(th) edition. Diabetes Res Clin Pract 2020, 162, 108086. [Google Scholar] [CrossRef] [PubMed]
- Tufford, A.R.; Calder, P.C.; Van’t Veer, P.; Feskens, E.F.; Ockhuizen, T.; Kraneveld, A.D.; Sikkema, J.; de Vries, J. Is nutrition science ready for the twenty-first century? Moving towards transdisciplinary impacts in a changing world. Eur J Nutr 2020, (Suppl 1) (Suppl 1), 1–10. [Google Scholar] [CrossRef]
- FAO; IFAD; UNICEF; WFP; WHO. The State of Food Security and Nutrition in the World 2021. Transforming food systems for food security, improved nutrition and affordable healthy diets for all; FAO: Rome, Italy, 2021. [Google Scholar] [CrossRef]
- FAO. Food Balance Sheets – A Handbook. Food and Agricultural Organization of the United Nations: Rome, 2001. Organization of the United Nations.
- Willett, W.; Rockstrom, J.; Loken, B.; Springmann, M.; Lang, T.; Vermeulen, S.; Garnett, T.; Tilman, D.; DeClerck, F.; Wood, A.; Jonell, M.; Clark, M.; Gordon, L.J.; Fanzo, J.; Hawkes, C.; Zurayk, R.; Rivera, J.A.; De Vries, W.; Majele Sibanda, L.; Afshin, A.; Chaudhary, A.; Herrero, M.; Agustina, R.; Branca, F.; Lartey, A.; Fan, S.; Crona, B.; Fox, E.; Bignet, V.; Troell, M.; Lindahl, T.; Singh, S.; Cornell, S.E.; Srinath Reddy, K.; Narain, S.; Nishtar, S.; Murray, C.J.L. Food in the Anthropocene: the EAT-Lancet Commission on healthy diets from sustainable food systems. Lancet 2019, 393, 447–492. [Google Scholar] [CrossRef] [PubMed]
- Hu, Y.; Ding, M.; Sampson, L.; Willett, W.C.; Manson, J.E.; Wang, M.; Rosner, B.; Hu, F.B.; Sun, Q. Intake of whole grain foods and risk of type 2 diabetes: results from three prospective cohort studies. BMJ 2020, 370, m2206. [Google Scholar] [CrossRef] [PubMed]
- Aune, D.; Keum, N.; Giovannucci, E.; Fadnes, L.T.; Boffetta, P.; Greenwood, D.C.; Tonstad, S.; Vatten, L.J.; Riboli, E.; Norat, T. Whole grain consumption and risk of cardiovascular disease, cancer, and all cause and cause specific mortality: systematic review and dose-response meta-analysis of prospective studies. BMJ 2016, 353, i2716. [Google Scholar] [CrossRef]
- Swaminathan, S.; Dehghan, M.; Raj, J.M.; Thomas, T.; Rangarajan, S.; Jenkins, D.; Mony, P.; Mohan, V.; Lear, S.A.; Avezum, A.; Lopez-Jaramillo, P.; Rosengren, A.; Lanas, F.; AlHabib, K.F.; Dans, A.; Keskinler, M.V.; Puoane, T.; Soman, B.; Wei, L.; Zatonska, K.; Diaz, R.; Ismail, N.; Chifamba, J.; Kelishadi, R.; Yusufali, A.; Khatib, R.; Xiaoyun, L.; Bo, H.; Iqbal, R.; Yusuf, R.; Yeates, K.; Teo, K.; Yusuf, S. Associations of cereal grains intake with cardiovascular disease and mortality across 21 countries in Prospective Urban and Rural Epidemiology study: prospective cohort study. BMJ 2021, 372, m4948. [Google Scholar] [CrossRef]
- Toups, K.E. Global approaches to promoting whole grain consumption. Nutr Rev 2020, (Suppl 1) (Suppl 1), 54–60. [Google Scholar] [CrossRef]
- Jenkins, D.J.A.; Dehghan, M.; Mente, A.; Bangdiwala, S.I.; Rangarajan, S.; Srichaikul, K.; Mohan, V.; Avezum, A.; Diaz, R.; Rosengren, A.; Lanas, F.; Lopez-Jaramillo, P.; Li, W.; Oguz, A.; Khatib, R.; Poirier, P.; Mohammadifard, N.; Pepe, A.; Alhabib, K.F.; Chifamba, J.; Yusufali, A.H.; Iqbal, R.; Yeates, K.; Yusoff, K.; Ismail, N.; Teo, K.; Swaminathan, S.; Liu, X.; Zatonska, K.; Yusuf, R.; Yusuf, S.; Investigators, P.S. Glycemic Index, Glycemic Load, and Cardiovascular Disease and Mortality. N Engl J Med 2021, 384, 1312–1322. [Google Scholar] [CrossRef]
- Livesey, G.; Taylor, R.; Livesey, H.F.; Buyken, A.E.; Jenkins, D.J.A.; Augustin, L.S.A.; Sievenpiper, J.L.; Barclay, A.W.; Liu, S.; Wolever, T.M.S.; Willett, W.C.; Brighenti, F.; Salas-Salvado, J.; Bjorck, I.; Rizkalla, S.W.; Riccardi, G.; Vecchia, C.L.; Ceriello, A.; Trichopoulou, A.; Poli, A.; Astrup, A.; Kendall, C.W.C.; Ha, M.A.; Baer-Sinnott, S.; Brand-Miller, J.C. Dietary Glycemic Index and Load and the Risk of Type 2 Diabetes: A Systematic Review and Updated Meta-Analyses of Prospective Cohort Studies. Nutrients 2019, 11, 1280. [Google Scholar] [CrossRef] [PubMed]
- Wee, M.S.M.; Henry, C.J. Reducing the glycemic impact of carbohydrates on foods and meals: Strategies for the food industry and consumers with special focus on Asia. Compr Rev Food Sci Food Saf 2020, 19, 670–702. [Google Scholar] [CrossRef] [PubMed]
- Gephart, J.A.; Henriksson, P.J.G.; Parker, R.W.R.; Shepon, A.; Gorospe, K.D.; Bergman, K.; Eshel, G.; Golden, C.D.; Halpern, B.S.; Hornborg, S.; Jonell, M.; Metian, M.; Mifflin, K.; Newton, R.; Tyedmers, P.; Zhang, W.; Ziegler, F.; Troell, M. Environmental performance of blue foods. Nature 2021, 597, 360–365. [Google Scholar] [CrossRef] [PubMed]
- Murugan, A.C.; Karim, M.R.; Yusoff, M.B.; Tan, S.H.; Asras, M.F.; Rashid, S.S. New insights into seaweed polyphenols on glucose homeostasis. Pharm Biol 2015, 53, 1087–1097. [Google Scholar] [CrossRef] [PubMed]
- Sharifuddin, Y.; Chin, Y.X.; Lim, P.E.; Phang, S.M. Potential Bioactive Compounds from Seaweed for Diabetes Management. Mar Drugs 2015, 13, 5447–5491. [Google Scholar] [CrossRef] [PubMed]
- Attjioui, M.; Ryan, S.; Ristic, A.K.; Higgins, T.; Goni, O.; Gibney, E.R.; Tierney, J.; O’Connell, S. Comparison of edible brown algae extracts for the inhibition of intestinal carbohydrate digestive enzymes involved in glucose release from the diet. J Nutr Sci 2021, 10, e5. [Google Scholar] [CrossRef]
- Gunathilaka, T.L.; Samarakoon, K.; Ranasinghe, P.; Peiris, L.D.C. Antidiabetic Potential of Marine Brown Algae-a Mini Review. J Diabetes Res 2020, 2020, 1230218. [Google Scholar] [CrossRef]
- Lee, S.H.; Jeon, Y.J. Anti-diabetic effects of brown algae derived phlorotannins, marine polyphenols through diverse mechanisms. Fitoterapia 2013, 86, 129–136. [Google Scholar] [CrossRef]
- Kim, H.K. Ecklonia cava Inhibits Glucose Absorption and Stimulates Insulin Secretion in Streptozotocin-Induced Diabetic Mice. Evid Based Complement Alternat Med 2012, 2012, 439294. [Google Scholar] [CrossRef]
- Murray, M.; Dordevic, A.L.; Bonham, M.P.; Ryan, L. Do marine algal polyphenols have antidiabetic, antihyperlipidemic or anti-inflammatory effects in humans? A systematic review. Crit Rev Food Sci Nutr 2018, 58, 2039–2054. [Google Scholar] [CrossRef]
- Paradis, M.E.; Couture, P.; Lamarche, B. A randomised crossover placebo-controlled trial investigating the effect of brown seaweed (Ascophyllum nodosum and Fucus vesiculosus) on postchallenge plasma glucose and insulin levels in men and women. Appl Physiol Nutr Metab 2011, 36, 913–919. [Google Scholar] [CrossRef] [PubMed]
- Murray, M.; Dordevic, A.L.; Ryan, L.; Bonham, M.P. The Impact of a Single Dose of a Polyphenol-Rich Seaweed Extract on Postprandial Glycaemic Control in Healthy Adults: A Randomised Cross-Over Trial. Nutrients 2018, 10, 270. [Google Scholar] [CrossRef]
- Zeevi, D.; Korem, T.; Zmora, N.; Israeli, D.; Rothschild, D.; Weinberger, A.; Ben-Yacov, O.; Lador, D.; Avnit-Sagi, T.; Lotan-Pompan, M.; Suez, J.; Mahdi, J.A.; Matot, E.; Malka, G.; Kosower, N.; Rein, M.; Zilberman-Schapira, G.; Dohnalova, L.; Pevsner-Fischer, M.; Bikovsky, R.; Halpern, Z.; Elinav, E.; Segal, E. Personalized Nutrition by Prediction of Glycemic Responses. Cell 2015, 163, 1079–1094. [Google Scholar] [CrossRef] [PubMed]
- Basu, R.; Dalla Man, C.; Campioni, M.; Basu, A.; Klee, G.; Toffolo, G.; Cobelli, C.; Rizza, R.A. Effects of age and sex on postprandial glucose metabolism: differences in glucose turnover, insulin secretion, insulin action, and hepatic insulin extraction. Diabetes 2006, 55, 2001–2014. [Google Scholar] [CrossRef] [PubMed]
- Numao, S.; Kawano, H.; Endo, N.; Yamada, Y.; Konishi, M.; Takahashi, M.; Sakamoto, S. Short-term low carbohydrate/high-fat diet intake increases postprandial plasma glucose and glucagon-like peptide-1 levels during an oral glucose tolerance test in healthy men. Eur J Clin Nutr 2012, 66, 926–931. [Google Scholar] [CrossRef] [PubMed]
- Simper, T.N.; Morris, C.; Lynn, A.; O’Hagan, C.; Kilner, K. Responses to oral glucose challenge differ by physical activity volume and intensity: A pilot study. J Sport Health Sci 2020, 9, 645–650. [Google Scholar] [CrossRef] [PubMed]
- Atkinson, F.S.; Hancock, D.; Petocz, P.; Brand-Miller, J.C. The physiologic and phenotypic significance of variation in human amylase gene copy number. Am J Clin Nutr 2018, 108, 737–748. [Google Scholar] [CrossRef] [PubMed]
- Ceriello, A. Postprandial hyperglycemia and diabetes complications: is it time to treat? Diabetes 2005, 54, 1–7. [Google Scholar] [CrossRef] [PubMed]
- O’Keefe, J.H.; Bell, D.S. Postprandial hyperglycemia/hyperlipidemia (postprandial dysmetabolism) is a cardiovascular risk factor. Am J Cardiol 2007, 100, 899–904. [Google Scholar] [CrossRef]
- Suzuki, K.; Watanabe, K.; Futami-Suda, S.; Yano, H.; Motoyama, M.; Matsumura, N.; Igari, Y.; Suzuki, T.; Nakano, H.; Oba, K. The effects of postprandial glucose and insulin levels on postprandial endothelial function in subjects with normal glucose tolerance. Cardiovasc Diabetol 2012, 11, 98. [Google Scholar] [CrossRef]
- Mamo, J.C.; Yu, K.C.; Elsegood, C.L.; Smith, D.; Vine, D.; Gennat, H.C.; Voevodin, M.; Proctor, S.D. Is atherosclerosis exclusively a postprandial phenomenon? Clin Exp Pharmacol Physiol 1997, 24, 288–293. [Google Scholar] [CrossRef] [PubMed]
- Blaak, E.E.; Antoine, J.M.; Benton, D.; Bjorck, I.; Bozzetto, L.; Brouns, F.; Diamant, M.; Dye, L.; Hulshof, T.; Holst, J.J.; Lamport, D.J.; Laville, M.; Lawton, C.L.; Meheust, A.; Nilson, A.; Normand, S.; Rivellese, A.A.; Theis, S.; Torekov, S.S.; Vinoy, S. Impact of postprandial glycaemia on health and prevention of disease. Obes Rev 2012, 13, 923–984. [Google Scholar] [CrossRef] [PubMed]
- Hall, H.; Perelman, D.; Breschi, A.; Limcaoco, P.; Kellogg, R.; McLaughlin, T.; Snyder, M. Glucotypes reveal new patterns of glucose dysregulation. PLoS Biol 2018, 16, e2005143. [Google Scholar] [CrossRef] [PubMed]
- Wascher, T.C.; Schmoelzer, I.; Wiegratz, A.; Stuehlinger, M.; Mueller-Wieland, D.; Kotzka, J.; Enderle, M. Reduction of postchallenge hyperglycaemia prevents acute endothelial dysfunction in subjects with impaired glucose tolerance. Eur J Clin Invest 2005, 35, 551–557. [Google Scholar] [CrossRef] [PubMed]
- EFSA Panel on Dietetic Products, N. Allergies, Guidance on the scientific requirements for health claims related to appetite ratings, weight management, and blood glucose concentrations. EFSA Journal 2012, 10, 2604. [Google Scholar] [CrossRef]
- Murray, M.; Dordevic, A.L.; Ryan, L.; Bonham, M.P. A Single-Dose of a Polyphenol-Rich Fucus Vesiculosus Extract is Insufficient to Blunt the Elevated Postprandial Blood Glucose Responses Exhibited by Healthy Adults in the Evening: A Randomised Crossover Trial. Antioxidants (Basel) 2019, 8, 49. [Google Scholar] [CrossRef]
- Konstantinidou, V.; Daimiel, L.; Ordovas, J.M. Personalized nutrition and cardiovascular disease prevention: From Framingham to PREDIMED. Adv Nutr 2014, 5, 368S–371S. [Google Scholar] [CrossRef]
- van Ommen, B.; Keijer, J.; Kleemann, R.; Elliott, R.; Drevon, C.A.; McArdle, H.; Gibney, M.; Muller, M. The challenges for molecular nutrition research 2: quantification of the nutritional phenotype. Genes Nutr 2008, 3, 51–59. [Google Scholar] [CrossRef]
- Gibney, E.R. Personalised nutrition - phenotypic and genetic variation in response to dietary intervention. Proc Nutr Soc 2020, 79, 236–245. [Google Scholar] [CrossRef]
- Celis-Morales, C.; Lara, J.; Mathers, J.C. Personalising nutritional guidance for more effective behaviour change. Proc Nutr Soc 2015, 74, 130–138. [Google Scholar] [CrossRef]
- Curtis, P.J.; Adamson, A.J.; Mathers, J.C. Effects on nutrient intake of a family-based intervention to promote increased consumption of low-fat starchy foods through education, cooking skills and personalised goal setting: the Family Food and Health Project. Br J Nutr 2012, 107, 1833–1844. [Google Scholar] [CrossRef] [PubMed]
- DiNicolantonio, J.J.; Bhutani, J.; O’Keefe, J.H. Acarbose: safe and effective for lowering postprandial hyperglycaemia and improving cardiovascular outcomes. Open Heart 2015, 2, e000327. [Google Scholar] [CrossRef]
- Hedrington, M.S.; Davis, S.N. Considerations when using alpha-glucosidase inhibitors in the treatment of type 2 diabetes. Expert Opin Pharmacother 2019, 20, 2229–2235. [Google Scholar] [CrossRef] [PubMed]
- Kageyama, S.; Nakamichi, N.; Sekino, H.; Nakano, S. Comparison of the effects of acarbose and voglibose in healthy subjects. Clin Ther 1997, 19, 720–729. [Google Scholar] [CrossRef] [PubMed]
- Dirir, A.M.; Daou, M.; Yousef, A.F.; Yousef, L.F. A review of alpha-glucosidase inhibitors from plants as potential candidates for the treatment of type-2 diabetes. Phytochem Rev 2022, 21, 1049–1079. [Google Scholar] [CrossRef] [PubMed]
- Dominguez Diaz, L.; Fernandez-Ruiz, V.; Camara, M. The frontier between nutrition and pharma: The international regulatory framework of functional foods, food supplements and nutraceuticals. Crit Rev Food Sci Nutr 2020, 60, 1738–1746. [Google Scholar] [CrossRef]
- Miletic, I.D.; Schiffman, S.S.; Miletic, V.D.; Sattely-Miller, E.A. Salivary IgA secretion rate in young and elderly persons. Physiol Behav 1996, 60, 243–248. [Google Scholar] [CrossRef]
- EFSA NDA Panel (EFSA Panel on Panel on Dietetic Products Nutrition and Allergies), Scientific Opinion on Dietary Reference Values for iodine. EFSA Journal 2014, 12, 3660. [CrossRef]
Figure 1.
Scatter plot of fasting (Co) and maximum glucose levels (Cmax) after the control meal (CM), intervention meal with lower dose of brown seaweed extract (LDM) and intervention meal with higher dose of brown seaweed extract (HDM) in sixteen subjects. Values are means with standard errors.
Figure 1.
Scatter plot of fasting (Co) and maximum glucose levels (Cmax) after the control meal (CM), intervention meal with lower dose of brown seaweed extract (LDM) and intervention meal with higher dose of brown seaweed extract (HDM) in sixteen subjects. Values are means with standard errors.
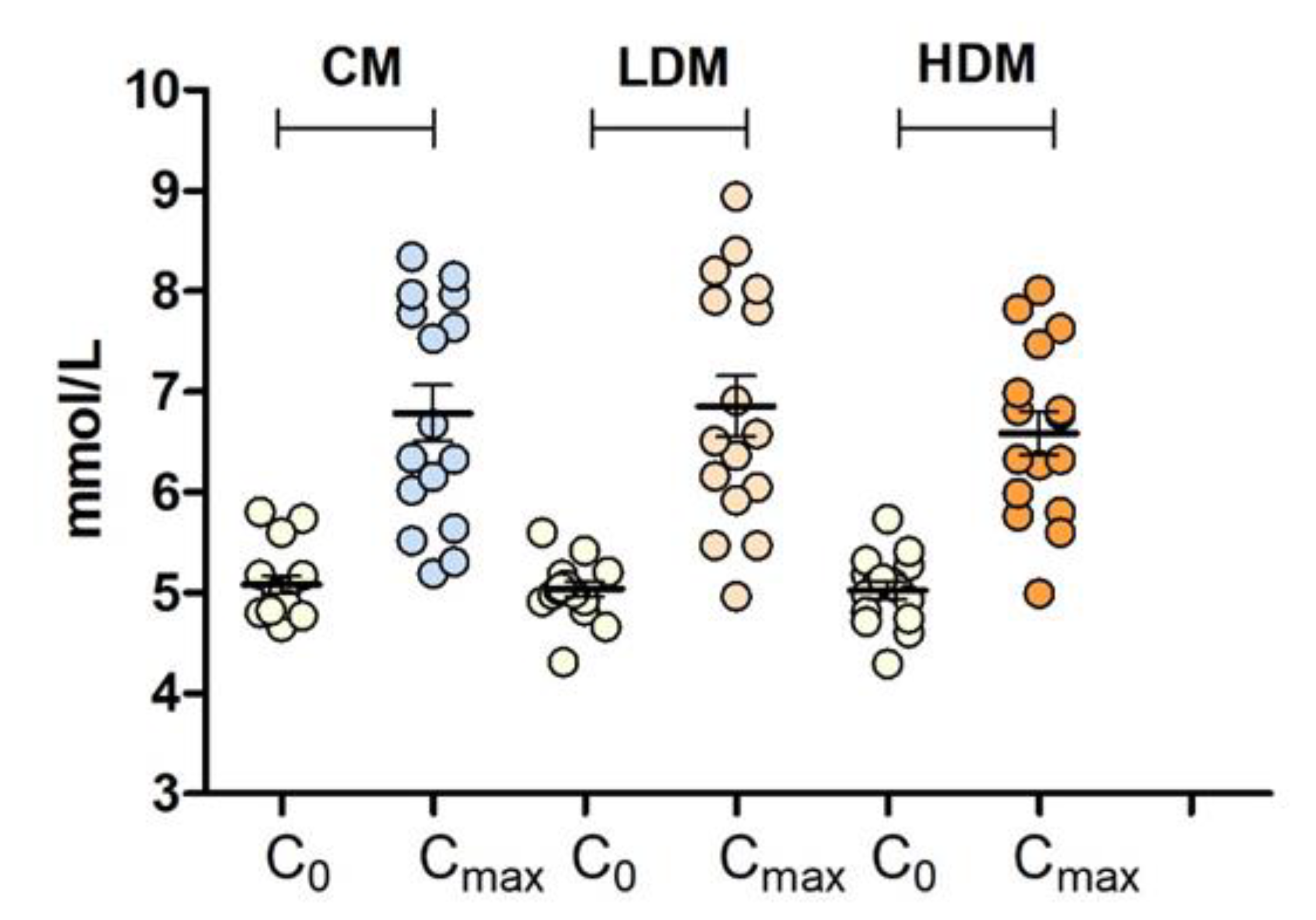
Figure 2.
Concentrations of plasma glucose in sixteen healthy subjects over 3h after the consumption of control meal (CM), intervention meal with lower dose of brown seaweed extract (LDM) and intervention meal with higher dose of brown seaweed extract (HDM). Values are means with standard errors.
Figure 2.
Concentrations of plasma glucose in sixteen healthy subjects over 3h after the consumption of control meal (CM), intervention meal with lower dose of brown seaweed extract (LDM) and intervention meal with higher dose of brown seaweed extract (HDM). Values are means with standard errors.
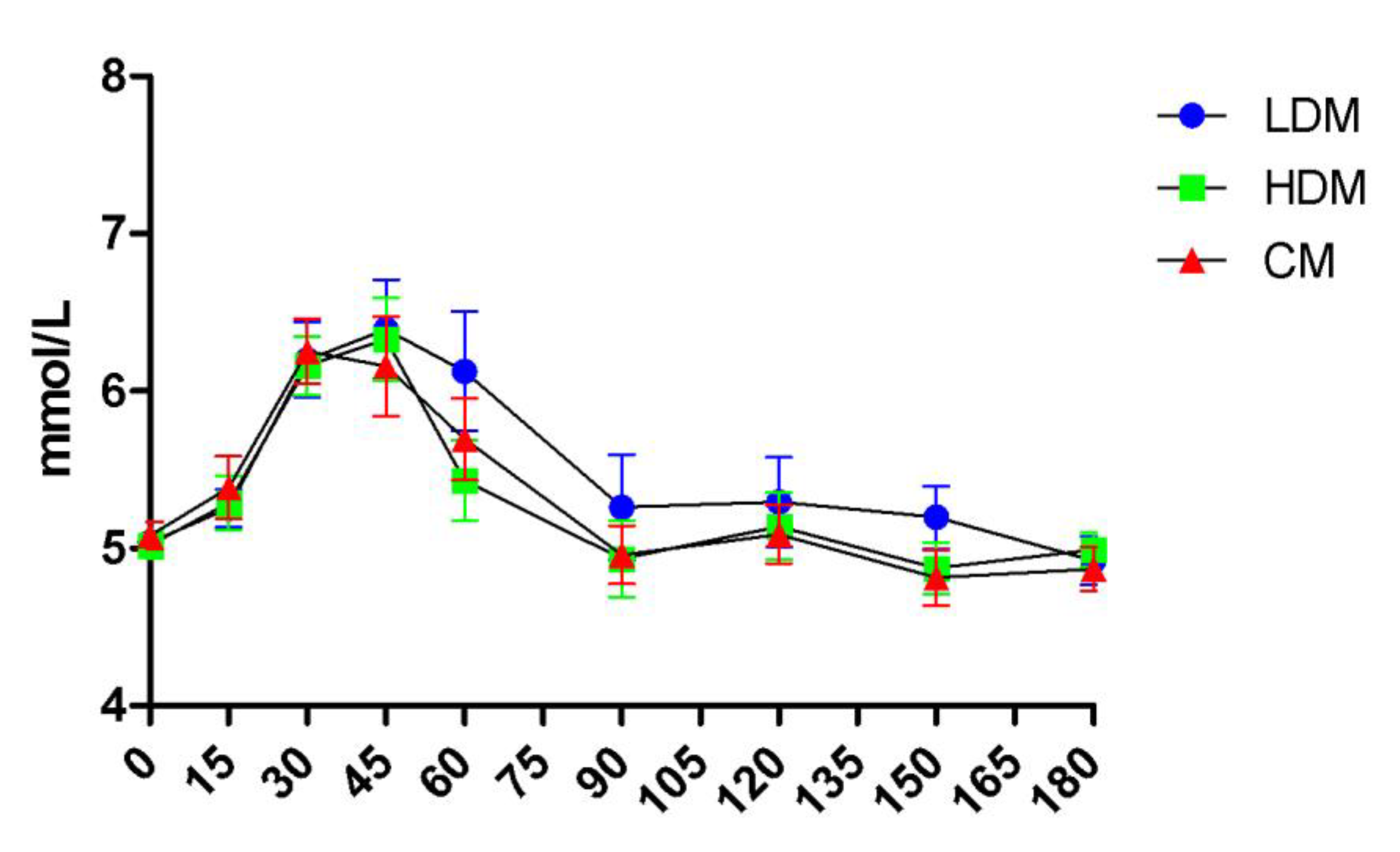
Figure 3.
Incremental peak glucose concentration in a subcohort of 10 healthy subjects (“higher-normal” responders to refined starch load) after the consumption of control meal (CM) and intervention meal with higher dose of brown seaweed extract (HDM). Values are means with standard errors.
Figure 3.
Incremental peak glucose concentration in a subcohort of 10 healthy subjects (“higher-normal” responders to refined starch load) after the consumption of control meal (CM) and intervention meal with higher dose of brown seaweed extract (HDM). Values are means with standard errors.
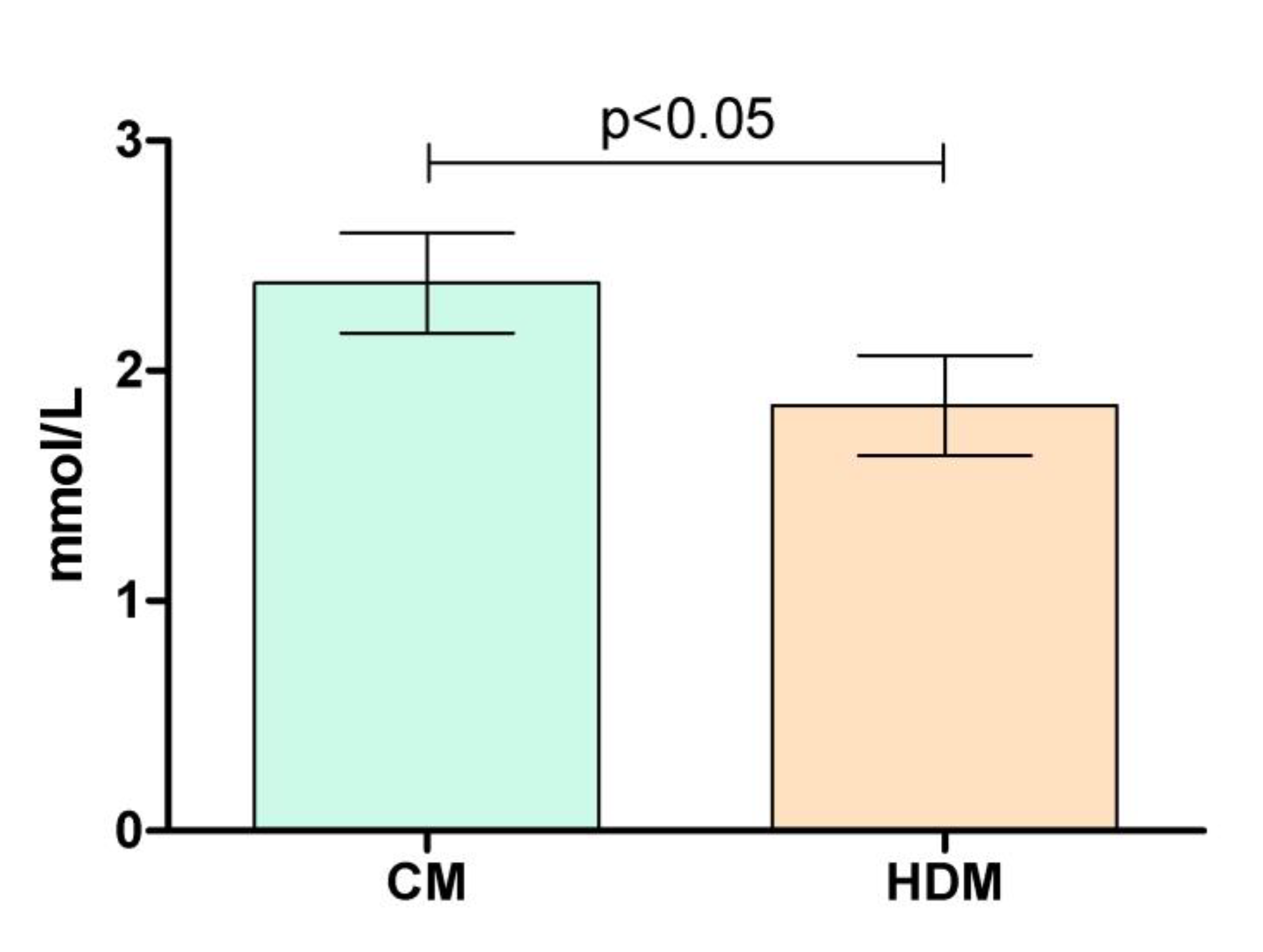
Figure 4.
Concentrations of insulin in sixteen healthy subjects over 3h after the consumption of control meal (CM), intervention meal with higher dose of brown seaweed extract (HDM) and intervention meal with low dose of brown seaweed extract (LD) Values are means with standard errors.
Figure 4.
Concentrations of insulin in sixteen healthy subjects over 3h after the consumption of control meal (CM), intervention meal with higher dose of brown seaweed extract (HDM) and intervention meal with low dose of brown seaweed extract (LD) Values are means with standard errors.
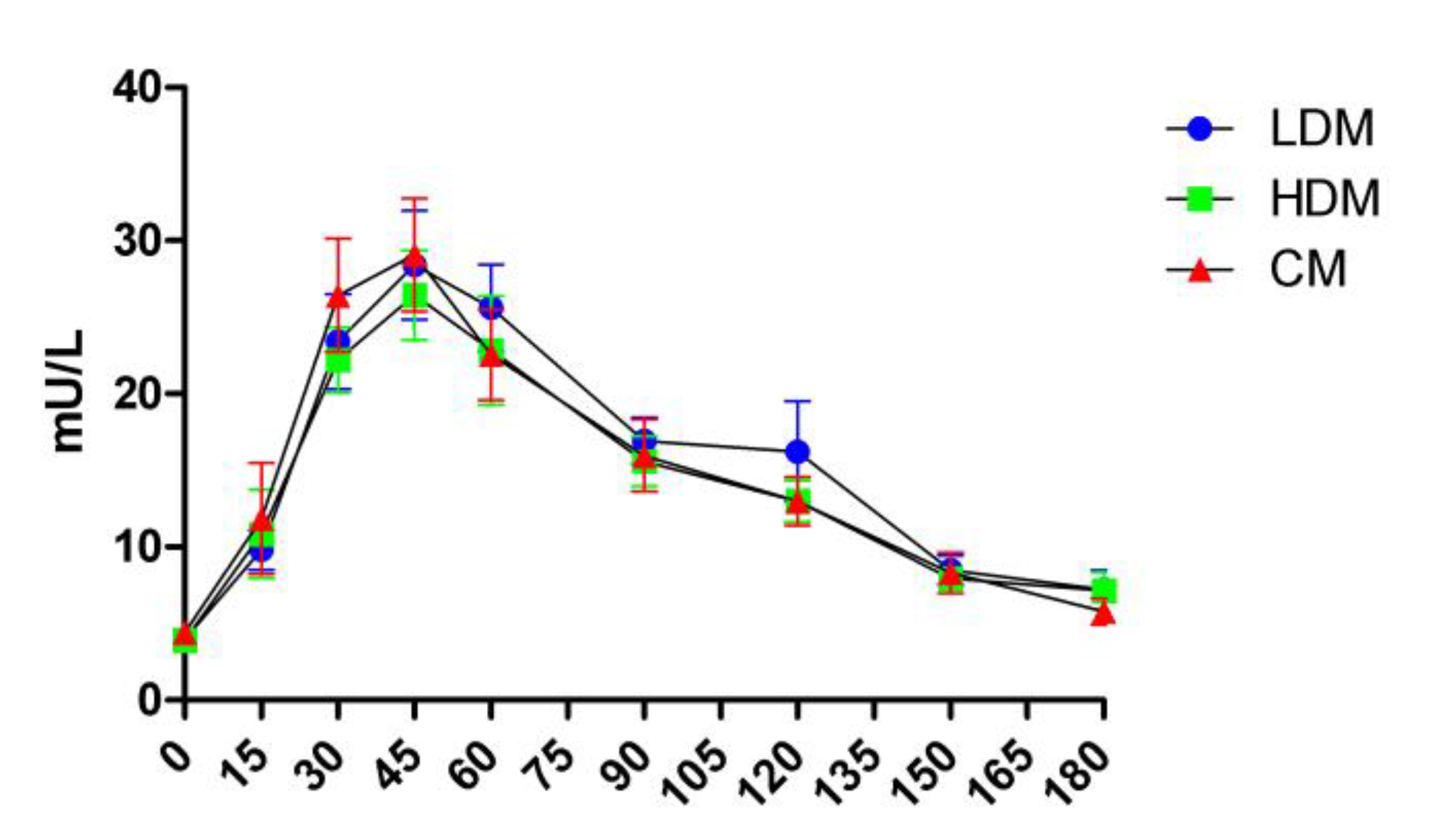

Table 1.
Baseline clinical characteristics of the study participants.
| Characteristics | Mean (SD) | Range |
|---|---|---|
| N | 16 | na |
| Male/Female | 7/9 | na |
| Age (y) | 29.6 (±10.4) | 18-57 |
| Body weight (kg) | 73.85 (±11.4) | 60.5-93.4 |
| BMI (kg/m2) | 24.5 (±3.9) | 18.1-32.1 |
| DBP (mmHg) | 110.4 (±9.2) | 90-125 |
| SDP (mmHg) | 69.2 (±8.2) | 52-82 |
| Heart rate | 68.6 (±11.5) | 49-95 |
| TG (mmol/L) | 0.88 (±0.53) | 0.39-2.26 |
| TCHOL(mmol/L) | 4.67 (±0.91) | 3.47-6.31 |
| HDL(mmol/L) | 1.21 (±0.22) | 0.79-1.49 |
| LDL (mmol/L) | 2.44 (±0.69) | 1.29-3.49 |
| Fasting plasma glucose (mmol/L) | 5.11 (±0.32) | 4.31-5.6 |
| Salivary flow (ml/min) | 0.393 (±0.22) | 0.154-0.867 |
| Salivary amylase (U/ml) | 66.5 (±46.94) | 16.63-181.53 |
| Salivary amylase secretion rate (U/min) | 37.73 (±30.03) | 2.63-136.66 |
* Data are presented as mean (±SD); BMI, body mass index; SDB, systolic blood pressure; DBP, diastolic blood pressure; TG, triglycerides; TCHOL, total cholesterol; HDL, high-density lipoprotein cholesterol; LDL, low-density lipoprotein cholesterol.
Table 2.
Parameters of postprandial glucose response to control in two sub-cohorts.
| Parameters | “Lower-normal” | “Higher-normal” | Difference |
|---|---|---|---|
| Cmax | 5.64 (±0.38) | 7.47 (±0.75) | p<0.0001 |
| iCmax | 0.57 (±0.29) | 2.38 (±0.69) | p<0.0001 |
| iAUC180 | 19.83 (±25.72) | 115.3 (±57.85) | P=0.002 |
* Data are presented as mean (±SD); Cmax, peak glucose concentration; iCmax, incremental peak glucose concentration; iAUC, incremental area under the glucose curve over 3h.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



