
Submitted:
03 May 2023
Posted:
04 May 2023
You are already at the latest version
Abstract
Background: In regenerative dentistry the graft material influences the success. It should act as an osteoconductive scaffold, providing a mineral substrate during resorption and inducing the activity of osteoinductive cells capable of producing new bone, platelet growth factors, and cell differentiation factors inducing the differentiation of undifferentiated mesenchymal cells into. Given that dentin shares many biochemical characteristics with bone tissue, it has recently attracted considerable interest as a biomaterial for bone repair. The aim of this study is to compare two grinder types in order to determine the optimal method for producing dentinal particles using a mechanical grinder. Materials and methods: A sample of 40 natural human teeth without restorations, prostheses or root canal treatments was used and divided into two groups subjected to two different grinder speeds (high-speed and low-speed). The high-speed showed a greater dispersion (53.5+-9.89% of the tooth) due to the pulverisation (highly thin granules) of part of the tooth. The low-speed grinder does not pulverize the dentin and the percentage of tooth loss is 9.16+/-2.34%. Conclusion: The low-speed gringer allows to save a major part of the tooth and to have a maximum quantity of graft material but requires more time. Further studies must be promoted to optimise the grinding procedures.
Keywords:
autogenous dentin particulate
; bone regeneration
; dental biomaterials
; granules
; grow factors
; high-speed grinder
; low-speed grinder
; osteoclasts
; tooth graft
; tooth transformer
1. Introduction
In recent decades, regenerative medicine has gained a great deal of attention and advancement in the medical profession. Biomaterials research has produced outstanding and reliable outcomes, due in part to biotechnology. Researchers are interested in the study of bone tissue regeneration, which is commonly employed in dentistry [1,2,3,4,5,6]. Researchers have stressed and proved in their studies that for regeneration effectiveness, it is vital to consider the size of the bone defect to be filled. Different forms of bone defects have emerged, posing significant problems to the clinical field, leading to a great need for bone repair materials [7,8].
The graft material must be decontaminatedand must function as an osteoconductive scaffold, providing a mineral substrate during resorption, inducing the activity of osteoinductive cells capable of producing new bone, platelet growth factors, and cell differentiation factors such as morphogenetic proteins (BMPs), which induce the transformation of undifferentiated mesenchymal cells into osteogenic cells (osteoblasts) [9,10,11,12,13].
Dentin has received a lot of interest recently as a biomaterial for bone repair. Its biochemical makeup has been compared to that of bone tissue. Dentin and bone are both composed of 61% inorganic material (HA 3Ca3(PO4)2Ca(OH)2 crystals that are 10 times bigger than those of bone and 300 times smaller than those of enamel) and 39% biological material. The organic component is 90% collagen: 95% collagen type I and 5% collagen types III, V, and XII. Collagen adds strength and suppleness to the structure, making it more resistant to fractures [14].
Non-collagen proteins account for 10% of the total (Osteopontin OPN, Dentin sialoprotein DSP, DGP, DPP-Bone sialoprotein, Osteocalcin, Dentin sialoprotein DSP, Dentin matrix protein-1 DMP-1, Collagen type 1, Cbfa1 RUNx2, Bone morphogenetic protein BMP-2, Transforming growth factor (TGF-) 19). The majority of the proteins found in dentin are likewise found in bone [15,16,17,18,19]
The tooth grafting procedure was introduced by Yeomans and Urist more than 50 years ago, with the discovery of the osteoinduction potential of demineralized dentin matrix [20,21].
Schmidt-Schultz and colleagues conducted one of the earliest studies on the tooth as a biomaterial for grafting, identifying and isolating growth factors such as Insulin Growth Factor-II (IGF-II), Bone Morphogenetic Protein-2 (BMP-2) and TGF- using teeth from the late pre-ceramic Neolithic period (approx. 8,000 years ago), teeth from the early Middle Ages, and recently extracted teeth [22].
More recently, Bessho et al. demonstrated the presence of bone morphogenetic proteins (BMPs) in the human dentin matrix [23]. Thirteen types of BMP proteins have been recognized. They can activate the process of bone neoformation even in heterotopic locations [24]. BMP-2, in particular, stimulates mesenchymal cell development into osteoblasts. BMP-3 promotes bone growth, while BMP-7 promotes osteoblast differentiation [25]. BMPs first drive the replication and migration of mesenchymal cells from surrounding tissues to the regenerated region, and then suppress the WNT signal, which prevents mesenchymal cell differentiation [26,27,28].
In particular, bone formation and the presence of osteoblasts were observed in rat muscles after the insertion of a demineralized human dentin matrix graft [27].
The stimulation mechanisms in demineralized dentin-induced bone regeneration are quite similar to those in autologous bone factors. Both de-mineralized bone matrix (DBM) and demineralized dentin matrix (DDM) include type I collagen, growth factors, and bone morphogenetic proteins after de-mineralization (BMP-2) [29,30].
Fundamental growth factors (GFs) for bone regeneration were found in both the bone and dentin matrices [2,3]. They represent an efficient reserve of BMPs, bioactive GFs, such as transforming growth factor-B (TGF-B), which are involved in the bone-repairing processes [31,32,33]. According to experts, the demineralization process provides for superior bone augmentation than non-demineralized dentin [34,35]. Moreover, the chemical composition of bone and dentin is almost identical, with an inorganic component of hydroxyapatite and an organic component mostly consisting of type 1-collagen and other secondary proteins [36]. For more than 35 years, heterologous or alloplastic grafting materials have been employed for bone augmentation treatments, however they just serve as mechanical scaffolds for host cells and do not provide any osteoinduction stimulus [11,37,38,39,40]. Several authors have recently estabilished the effectiveness and safety of autogenous partially demineralized dentin matrix prepared onsite, for clinical use in implant dentistry bone regeneration treatments such as socket preservation, alveolar ridge augmentation, and maxillary sinus floor augmentation [4,32,41,42].
Various tooth demineralization procedures have been studied, with varying outcomes in bone tissue development. When comparing different tooth crushing systems, the degree of sterilization, the system repeatability,the liquids and their concentrations, the degree of demineralization, the granule size, the residual protein amount after treatment, the wettability and plasticity of the granules, and the ergonomics of the system must all be considered [35,43].
A recent prospective study validated the use of the tooth as a grafting material in socket preservation [44].
Recently, a novel medical tool (Tooth Transformer®) for collecting acceptable tooth transplant materials from the patient's tooth was launched on the market. This technology enables entirely automated cleaning, grinding, and demineralizing procedures with no errors caused by human intervention. TT is a cutting-edge tissue engineering method because it can quickly process and turn a removed tooth into therapeutically viable bone graft material. The graft material, created from the whole tooth, is extremely wettable, allowing for simple handling and placing at the host site. A prior case series revealed the favorable clinical results of bone regeneration following autologous tooth grafting with TT and reported the full filling of bony defects by TT [45].
Previous articles referring to this device have been analyzed:
Human dentin was reduced to particles and demineralized and detoxified. The characterization of native mineral, collagen and BMP-2 were performed by SEM , EDS test and Elisa test . In addition, osteoblastics cells were seeded in tooth derived materials and compared with Xenographic material and the cell response ,with SAOS-2 and MG-63 cells, in terms of adhesion , proliferation and cytotoxicity [46]was measured.
The conclusion was the process, as a combination of chemical and thermal treatments, allowed the preserviation of collagen and increased the BMP-2 bioavailability. The proliferation cells on the surface were analyzed as well as the osteocalcin production, without having any negative indication.
Bianchi et al. found that understanding the biological and morphological reactions of human cells towards different dentinal derivate grafting materials it is fundamental to choose the type of dentin for different specific clinical situations. This study aimed to evaluate human periodontal ligament fibroblasts (hPLF) cells exposed to different dentinal derivate particles. The study design included the in vitro evaluation of mineralized dentine (SG), deproteinized and demineralized dentine (DDP), and demineralized dentine (TT- tooth transformer) as test materials and of deproteinized bovine bone (BIOS) as the positive control material. The CLMS observations showed the expression of the proliferative marker, as well as and the expression of cytoskeletal elements involved in the adhesion process. In particular, the vinculin and integrin signals were stronger at the 72 h follow-up in the sample exposed to TT material; These data confirmed how dentinal derivates present satisfying biocompatibility and high conductivity and inductivity properties fundamental in the regenerative processes [47]. Clinical animal tests were allowed. Four hollow titanium cylinders, termed “Bone Growing Chambers” (BGC), were used to contain the tooth graft. Two BGC cylinders were filled with the tooth graft treated using a Tooth Transformer device while another two were filled with tooth graft without any treatment (control group). All the BGCs were integrated into the mandibular bone after 2 months of healing. At the surgical reentry the BGCs were visible on the crest mandible and easy to distinguish from the surrounding bone. Stable BGCs demonstrated the presence of bone tissue inside the hollow space. A healthy pattern of bone repair process was detected around and inside the chambers. A small amount of bone penetration inside the regenerating space was found in controls BGCs and the granules were not surrounded by new bone. In the BGCs filled with the Tooth Transformer grafting material (test group), the formation of a more compact bone structure was evident and composed of newly formed bone mixed with grafted granules almost completely incorporated in the new trabeculae of the newly formed bone . This study clearly showed that the tooth graft obtained with a specific device has a better integration than the same tooth graft without any treatment [48]. Clinical and histological tests showed the complete absence of inflammation or adverse reactions to the use of the tooth treated with this new device as a grafting material. The clinical tests showed a perfect dentin integration during regeneration. However, it is necessary to better understand what happens in the stage of regeneration. To explore the histomorphometric outcomes of tooth derivative materials, as used as bone substitute material in socket preservation procedure, 101 histomorphometry was performed. The results indicate a mean value of average 38% of new bone produced and only 7% of graft residual after only 5 months [49,50,51,52].
Santos et al in 2021 tested the different results between demineralized dentin and xenograf material in alveolar ridge preservation. 52 patients with 66 implants were recruited and, after healing of the implants, the demineralized dentin showed a significantly higher quantity of newly formed bone and a lower amount of residual graft in histomorphometry results and equal clinical and patient-related outcomes [53].
A prospective, randomized, controlled clinical trial reports clinical, radiographic, histologic and immunohistochemical results of autologous dentin graft (ADG) and its comparison with a mixture of bovine xenograft with autologous bone (BX+AB). A statistically significant difference between the groups was found in the intensity of TNF-_ in the area of newly formed bone (p = 0.0003) and around remaining biomaterial particles (p = 0.0027), and in the intensity of BMP-4 in the area around biomaterial particles (p = 0.0001). Overall, ADG showed biocompatibility and achieved successful bone regeneration similar to BX+AB.[82] The dentin osteoinduction capacities were confirmed in a study by Min et al using two groups of rats comparing macroporous biphasic calcium phosphate and demineralized dentin. The osteoconduction capacity showed in this study suggests that dentin is a useful bone substitute [54].
Grinding is the first step towards using the tooth as a graft material, a protocol must be developed that allows a completely automated device capable of constantly reproducing the same results and maintaining osteoinductive abilities [3].
As regards the surgical use of teeth, extreme care must be taken not to disperse an unrepeatable sample (the extracted tooth) due to grinding techniques, where the disadvantages are the creation of particles not homogeneous in size (for example, too small), resulting often in material loss. Therefore, the size of particles should be as similar as possible to optimal weights. Systems for pulverizing a solid are of two types: high-speed mill and low-speed grinder [55,56].
To our knowledge, this is the first study in literature which analyzes the two grinder types and establishes the procedure to produce a dentinal particulate through a mechanical grinder.
2. Materials and Methods
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the local Ethical Committee for Biomedical Research of Chieti and Pescara (Prot. N. 1869/21.03.2019). This study was executed in accordance with the guidelines of the Declaration of Helsinki.
In the effort of trying to understand which was the system that guaranteed the best performance, two different grinding systems (Figure 1a–c) were evaluated, one at high speed (testing two different grinders), similar to a coffee grinder, and one at low speed, with concentric conical blades. The difference between high speed and low speed is in the RPM which stands for Revolutions Per Minute. Basically, it is how many times in a minute the burrs rotate. The speed is the measurement of one complete revolution of the blades. Most high speed grinders have a hammermill that spins anywhere between 1,100 to 1,200 RPM. These machines are typically assisted with some sort of feeding system. On the other hand, low speed shredders spin at 30 to 40 RPM and are often built without an assisted feeding mechanism.
Low speed: these are at a lower RPM for two reasons. They usually have smaller burrs, and most are conical shaped. The lower RPM grinders usually have less heat buildup. Low speed shredder blades are conical concentrics with sharp edges. They have an accumulation zone of the material to be grinded called the upper chamber and a lower one. The distance between the blades in the lower chamber determines the size of the granulate.
High speed : These usually have flat burr sets, and beefier motors. The flat burrs provide a more consistent grind and the higher RPMs grind the teeth faster. Hi-speed grinders are direct drive, which means less gears to wear or break, and are quieter. The blades of the high-speed shredder are shaped like a specular hammer, rotating on a central pin placed inside a sealed drum. The tooth is placed inside the drum and only after rapid rotation of the hammer the granulate is produced that then must be filtered to the right size of the granules [57,58].
A tooth was triturated, and then analyzed under a microscope to reveal the shape of the produced granules, (Figure 2a,b) filtered through calibrated sieves (Figure 3). A sieve analysis (or gradation test) is a practice or procedure used to assess the particle size distribution (also known as gradation) of a granular material by passing it through a series of sieves with progressively smaller mesh sizes and weighing the amount of material caught by each sieve as a fraction of the total mass [59,60].
The procedure to sieve is: the vertical throwing action is combined with a small circular motion, resulting in sample dispersion throughout the whole sieve surface. The particles are vertically propelled (thrown upwards). When they fall back, they do free rotations in the air and interact with the holes in the sieve mesh. Particles that are smaller than the openings pass past the sieve. They are tossed if they are bigger. The spinning motion while hung increases the likelihood that the particles will have a different orientation to the mesh when they fall back, and so may pass through the mesh. (Wikipedia: https://en.wikipedia.org/wiki/Sieve_analysis).
Finally, granules with a size between 0.5 and 1 mm were weighed.
Tests were carried out to understand the percentage dispersion in terms of the dry weight of a ground tooth and then filtered through a sieve (Figure 3), to keep only the granules with a size between 0.5 and 1 mm. The granules were produced using a grinder (low and high speed) and then filtered by size using metal sieves (Figure 3) (Filtra, SenecoSrl, Milan, Italy) and divided into three groups: i) group A: particles from 200 to 900 μm; ii) group B: particles <200 μm; iii) group C: particles >900 μm. Only granules from group A were used for the tests.
The tooth was weighed using Tanita super precision Mini weighing scale (Arlington Heights IL USA), before grinding and after grinding.
A sample of 40 natural human teeth (Figure 4) was used without restorations, prostheses or root canal treatments. In the case of the low-speed grinder, the teeth were sectioned due to problems of insertion into the space between the blades and this resulted in a weight loss caused by the cuts.
However, it was decided not to weigh the teeth after sectioning because this represents one of the limitations of this system and it must be fully evaluated. The whole teeth were inserted into the high-speed grinder.
The granules filtered through a sieve were then inserted into a device (Mastersizer 3000) allowing the quantification of both dry and wet granules through laser diffraction, to understand if the granules’ dimensions were in line with the requisite.
The laser diffraction test indicated that, the average particle size varied between 406 and 815 μm with peaks up to 1110 μm.
3. Results
Table 1 shows the two types of grinding and the corresponding tooth weight before grinding and after grinding. The weight difference is shown in the percentage of tooth loss.
4. Discussion
In recent years, several researchers have investigated the use of particles derived from autologous teeth as bone grafting material. In the study by Kim et al., once the soft tissues, tartar and foreign materials were removed, the tooth elements were divided and crushed, obtaining particles between 0.5 and 1.0 mm in size. The particles of the crushed teeth were immersed in distilled water and hydrogen oxide solution, dehydrated with ethyl alcohol solution and degreased with ethyl ether solution. Then, after the freeze-drying procedure, they were sterilized with ethylene gas and packaged [61]. Jun et al. also created the material in the form of a powder with particles of 0.5–1.0 [62], while, in another study, sample teeth were pulverized into powder, with each particle having a diameter of 0.4–0.8 mm [63].
Murata et al. described that the teeth were crashed in liquid nitrogen, washed in 1M sodium chloride, and demineralized in HCl solution at pH2.0. The tooth particles were thoroughly rinsed in cold distilled water before being lyophilized into 0.4 and 0.8 mm particles [64]. Nampo et al. obtained the graft material by removing the crown portions of the extracted teeth with scissors and trimming the root portions of the remaining teeth as close to 500 mm as possible. The trimmed tooth was then mixed with a measured amount of β-tricalcium phosphate [65]. Finally in the study by Kim et al. the particle size ranged from 0.2 to 1.2 mm [66].
Various studies have investigated the effect of anorganic bovine bone matrix (ABBM) particle size on bone healing in order to define the perfect dimension of granules for the optimal use in regeneration surgery (Table 2). Histological and radiographic studies were carried out to understand if bone repairing could be influenced by the particle size [61,62,63,64,65,66,67,68,69,70,71,72,73,74].
In the study by Kluppel et al. 18 male New Zealand rabbits were employed, and four cavities were drilled and filled with varying particle sizes of anorganic bovine bone matrix. The first cavity had small particles (under 450 µm), the second cavity included medium particles (450 to 749 µm), and the third cavity contained giant particles (750 to 1000 µm). Particulated autogenous bone was used to fill the fourth cavity (control group). The animals were slaughtered 15, 30, and 60 days following surgery. Before the decalcification process and histological assessment, radiographs of the cranial vault were taken. The authors concluded that anorganic bovine bone matrix particle size effects the bone healing process: smaller particles resorb faster and induce more bone neoformation than bigger particles [74].
Shapoff studied freeze dried bone allograft (FDBA), tiny particles (100–300 µm) combined with bone marrow, and big particles (1000–2000 µm) mixed with bone marrow in six Rhesus monkeys. The findings indicated that the tiny particles produced more bone. The authors indicate the possible superiority of the smaller graft with some reasons: the increase in surface area, the release of a large amount of calcium salts by hydrolytic enzymes, and the increase in the number of pores all encourage bone formation [71].
Different results were reported in the study by Testori et al. [69]. The authors compared vital bone formation after maxillary sinus augmentation using two different particle sizes of anorganic bovine matrix, finding a statistically significant increase in vital bone formation in the larger particle grafts [69].
Kon et al. employed twenty-four rabbit cranial bones to evaluate the augmentation process of two distinct autogenous bone graft particle sizes: large LB (1mm-2mm) and small SB (150–400 µm) particles were used. Autogenous bone is thought to be the gold standard for bone augmentation in the clinical setting. Nevertheless, the capacity to enhance may vary depending on particle size. By 8 weeks, the SB had shrunk to 51.3% and 51% of its initial volume and height, respectively, while the LB had maintained its volume. Finally, they proposed to use big autologous bone particles [75].
In another work demineralized freeze-dried cortical bone allograft (DFDBA) was processed and crushed into two sizes: 250–500 µm) and 850–1000 µm). Ten individuals with intrabony defects were chosen at random and, for each defect, soft and hard tissue measurements were taken. The bone defect fill was computed as a depth reduction from a given position: for the tiny particle group, it was 1.32 mm, while for the big particle group, it was 1.66 mm. This difference did not result as being statistically significant [76].
The osteoconductive capacity of deproteinized bone particles of two distinct diameters (300–500 and 850–1000 mm) in rabbits was compared in the study of Xu et al. The deproteinized bone was made from white rabbit limbs. The cortical bone was cooked in water for 10 hours before being immersed in 1 NHCl. Finally, the bone was sintered in an electric fumace for 5 hours at 600° and 5 hours at 1100°. In a bone mill, the bone was crushed into two particle groups: big particles (850–1000 m) and small particles (300–500 m). Finally, particles were used to create the sinus lift. Small particle groups produced superior outcomes [77].
In sheep femoral condyles, larger particles of silicate-substituted calcium phosphate (diameters of 250–500 or 1000–2000 mm, respectively) tended to preserve the volume of early bone formation better than smaller particles (90–120 mm) [78]. Larger particles tended to be retained in newly produced bone tissue, owing to the longer time required for dissolution or remodeling [72,79]. After successful engraftment, an autogenous bone block graft demonstrated a lower bone resorption rate than the particulates [80].
Koga et al. compared DDM, partial DDM and mineralized dentinal matrix, using three different sizes of graft particles for each group [81]. Defects in the sheep’s cortical bone were realized by inserting scaffolds of different sizes (large, 1–2 mm), (small, <0.5 mm), (medium, 0.5–1 mm); subsequently clean, pulverized human teeth were divided into three groups according to sizes. The best result was obtained from dimensions ranging between 0.5 and 1 mm. Smaller particles are too quickly resorbed to ensure sufficient space retention over time and to allow for bone formation. It is therefore obvious that the best performances are obtained when the dimensions of the granules are homogeneous and they are between 0.5 and 1 mm [81].
Dozza et al. analyzed the demineralized bone matrix (DBM) collagen-based biomaterial. A cortical sheep bone was ground and three different granule graft sizes were inserted and analyzed: Small (<0.5mm) medium (0.5 mm–1 mm) and large (1–2 mm). The authors concluded that medium particles were the best condition for cytocompatibility and recommended the use of an average size of 0.5 to 1 mm [67].
Some authors stated that osteoclast-like multinucleated giant cells appear to prefer small particles (<1 mm) in both autogenous bone and bone substitutes, such as bovine mineralized bone [75,82].
Larger bone replacement particles, on the other hand, can provide a greater quantity of bone augmentation. Larger autogenous bone particles (diameter, 1-2 mm) produced a greater augmented bone volume than smaller particles in a vertical bone augmentation model in rabbit calvaria utilizing polytetrafluoroethylene chambers (diameter, 150–400 mm) [83].
DDM resorbs faster than mineralized dentin, producing the best osteoconduction results, but very small parts may result in rapid graft resorption and failure to preserve volume [52,61].
Dimensions under 400 μm are reabsorbed from osteoclasts in a short time. Conversely, dimensions over 1000 μm are impossible to be reabsorbed. For this reason, granules produced by the two different speed grinders are sieved and the granule dispersion is analyzed using a master sizer 3000, laser diffraction particle size analyzer (Malvern Panalytical Ltd, UK.) This first analysis, despite the limitations due to the number of elements analyzed and the tools used, made it possible to establish that the grinding at low speed, resulted in a more homogeneous grinding andwas more efficient, allowing a greater percentage of the tooth to be available for use.
These findings suggest that bigger particles (1 mm) have stronger mechanical resistance as a mass for space-making than smaller particles (1 mm), and that space-making capability is more critical for early bone formation than the balance of bone resorption and formation. Nevertheless, dentin differs from the other graft materials in several ways. One of the most significant aspects is that no volume is lost during the preparation since it is unable to add (extract) additional material, and this process is based on the use of a removed tooth, thus it makes no sense to remove another tooth for graft usage.This element, which should be a limitation, should instead push to evaluate every single part of the preparation in order to avoid losing any component of the removed and useful teeth for producing grafting material.
As a result, several researchers have investigated the tooth's weight and typical volume. A total of 205 removed teeth were weighed and measured with a millimeter-level syringe using a professional digital micro scale. The average weight varied from 0.68 gr to 1.88 gr, while the average volume was 0.38 cc to 0.96 cc. The volume is sufficient to accomplish the majority of the graft operation, but it is impossible to add more material in the same procedure if production is low. The findings indicated that the material produced from teeth might be adequate to be used as bone grafting material. However, the varying grinding from different machines may alter the volume available for regeneration [84].
The evaluations of the authors are exactly the point and purpose of this study.The only usable engineering solutions for the fragmentation of a solid structure transforming it into granular are: the first is high speed by means of flat blades that rotate inside a capsule container and the structure to be fragmented is placed inside the capsule itself, the second is a concentric conical blades that rotate on the same axis and at low speed where the solid structure must be inserted in the space between the conical blades.
The test anlyzed three different data:
- average tooth weight before the test : each tooth was weighted to be able to compare the weight after the treatement
- average tooth weight after the test: each pulverized tooth was weighed after the treatment to be able to compare with the same tooth weight before the treatment
- lost tooth weight (%): the difference between before and after the treatment was measured in percentage of weight loss
After sieving, the two different speed grinders produced the same particulate. The high speed showed a greater dispersion. The dispersion was due to the pulverization (highly thin granules) of part of the tooth. The shape and the dimension of the granules was very different, so to obtain optima granules for the regeneration surgery a lot of parts of the tooth could be lost (Figure 2a). The percentage of the mean tooth lost with this high-speed grinder is 53.5+-9.89% of the tooth load.
The low-speed grinder does not pulverize the dentin and creates a regular dimension of the tooth granules. The percentage of teeth loss is 9.16+/-2.34%.
5. Conclusions
This study compared a low-speed grinder and a high-speed grinder obtaining different results. Even if the two methods produced the same particles, there was a minor dispersion of tooth material in the low-speed grinder group. From both a clinical and an ethical point of view, is better to save a major part of the tooth to have a maximum quantity of graft material. The tooth is not a commercial graft material and is not possible to buy more graft if the production is not enough. That is the reason why it is necessary to optimize and not lose the volume produced from a single extracted tooth.
The low speed grinder respects this indication but extends the procedure time. In the near future, a new system capable of combining the rapidity of high speed with the maintenance at low speed of the volume should be developed. Further studies must be promoted to achieve this result.
Author Contributions
Conceptualization, E.M., A.P. (Andrea Palermo), A.P. (Assunta Patano), F.I., G.D., G.P. and A.M.I.; methodology, E.M., A.P. (Andrea Palermo), F.P., A.D.I, G.D., A.M.I., and G.M.; writing—original draft preparation, E.M., A.P.(Andrea Palermo), F.I., A.D.I., and G.D; writing—review and editing, A.P.(Assunta Patano), G.M.; F.I., G.D. and A.M.I. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the local Ethical Committee for Biomedical Research of Chieti and Pescara (Prot. N. 1869/21.03.2019). This study was executed in accordance with the guidelines of the Declaration of Helsinki.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| BMPs | Bone morphogenetic proteins |
| GFs | Growth factors |
| DDM | Demineralized Dentin Matrix |
| TGF-B | Transforming growth factor-B |
| TT® | Tooth transformer ®
|
References
- Guided Bone Regeneration in Implant Dentistry. Available online: http://www.quintpub.com/display_detail.php3?psku=B2494#.Y7sD6uzMKdY (accessed on 8 January 2023).
- Romasco, T.; Tumedei, M.; Inchingolo, F.; Pignatelli, P.; Montesani, L.; Iezzi, G.; Petrini, M.; Piattelli, A.; Di Pietro, N. A Narrative Review on the Effectiveness of Bone Regeneration Procedures with OsteoBiol® Collagenated Porcine Grafts: The Translational Research Experience over 20 Years. J Funct Biomater 2022, 13, 121. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Hazballa, D.; Inchingolo, A.D.; Malcangi, G.; Marinelli, G.; Mancini, A.; Maggiore, M.E.; Bordea, I.R.; Scarano, A.; Farronato, M.; et al. Innovative Concepts and Recent Breakthrough for Engineered Graft and Constructs for Bone Regeneration: A Literature Systematic Review. Materials 2022, 15, 1120. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Inchingolo, A.M.; Bordea, I.R.; Xhajanka, E.; Romeo, D.M.; Romeo, M.; Zappone, C.M.F.; Malcangi, G.; Scarano, A.; Lorusso, F.; et al. The Effectiveness of Osseodensification Drilling Protocol for Implant Site Osteotomy: A Systematic Review of the Literature and Meta-Analysis. Materials 2021, 14, 1147. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, F.; Tatullo, M.; Marrelli, M.; Inchingolo, A.M.; Inchingolo, A.D.; Dipalma, G.; Flace, P.; Girolamo, F.; Tarullo, A.; Laino, L.; et al. Regenerative Surgery Performed with Platelet-Rich Plasma Used in Sinus Lift Elevation before Dental Implant Surgery: An Useful Aid in Healing and Regeneration of Bone Tissue. Eur Rev Med Pharmacol Sci 2012, 16, 1222–1226. [Google Scholar] [PubMed]
- Inchingolo, A.D.; Malcangi, G.; Semjonova, A.; Inchingolo, A.M.; Patano, A.; Coloccia, G.; Ceci, S.; Marinelli, G.; Di Pede, C.; Ciocia, A.M.; et al. Oralbiotica/Oralbiotics: The Impact of Oral Microbiota on Dental Health and Demineralization: A Systematic Review of the Literature. Children 2022, 9, 1014. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Liu, Z.; Liu, Y.; Yu, J.; Wang, X.; Tan, Z.; Ye, X. Recent Trends in the Development of Bone Regenerative Biomaterials. Frontiers in Cell and Developmental Biology 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- Mummolo, S.; Mancini, L.; Quinzi, V.; D’Aquino, R.; Marzo, G.; Marchetti, E. Rigenera® Autologous Micrografts in Oral Regeneration: Clinical, Histological, and Radiographical Evaluations. Applied Sciences 2020, 10, 5084. [Google Scholar] [CrossRef]
- Linkhart, T.A.; Mohan, S.; Baylink, D.J. Growth Factors for Bone Growth and Repair: IGF, TGF Beta and BMP. Bone 1996, 19, 1S–12S. [Google Scholar] [CrossRef]
- Canalis, E.; Pash, J.; Varghese, S. Skeletal Growth Factors. Crit Rev Eukaryot Gene Expr 1993, 3, 155–166. [Google Scholar]
- Gargiulo Isacco, C.; Ballini, A.; Paduanelli, G.; Inchingolo, A.D.; Nguyen, K.C.D.; Inchingolo, A.M.; Pham, V.H.; Aityan, S.K.; Schiffman, M.; Tran, T.C.; et al. Bone Decay and beyond: How Can We Approach It Better. J Biol Regul Homeost Agents 2019, 33, 143–154 DENTAL SUPPLEMENT. [Google Scholar]
- Del Corso, M.; Vervelle, A.; Simonpieri, A.; Jimbo, R.; Inchingolo, F.; Sammartino, G.; Dohan Ehrenfest, D.M. Current Knowledge and Perspectives for the Use of Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Oral and Maxillofacial Surgery Part 1: Periodontal and Dentoalveolar Surgery. Curr Pharm Biotechnol 2012, 13, 1207–1230. [Google Scholar] [CrossRef] [PubMed]
- Simonpieri, A.; Del Corso, M.; Vervelle, A.; Jimbo, R.; Inchingolo, F.; Sammartino, G.; Dohan Ehrenfest, D.M. Current Knowledge and Perspectives for the Use of Platelet-Rich Plasma (PRP) and Platelet-Rich Fibrin (PRF) in Oral and Maxillofacial Surgery Part 2: Bone Graft, Implant and Reconstructive Surgery. Curr Pharm Biotechnol 2012, 13, 1231–1256. [Google Scholar] [CrossRef] [PubMed]
- Sieverts, M.; Obata, Y.; Rosenberg, J.L.; Woolley, W.; Parkinson, D.Y.; Barnard, H.S.; Pelt, D.M.; Acevedo, C. Unraveling the Effect of Collagen Damage on Bone Fracture Using in Situ Synchrotron Microtomography with Deep Learning. Commun Mater 2022, 3, 1–13. [Google Scholar] [CrossRef]
- Bhaskar, S.N. Orban’s Oral Histology and Embryology, 9th ed.; Orban, B.J., Ed.; Mosby: St. Louis, 1980; ISBN 978-0-8016-4609-6. [Google Scholar]
- Butler, W.T.; Ritchie, H. The Nature and Functional Significance of Dentin Extracellular Matrix Proteins. Int J Dev Biol 1995, 39, 169–179. [Google Scholar] [PubMed]
- Chen, J.; Shapiro, H.S.; Sodek, J. Development Expression of Bone Sialoprotein MRNA in Rat Mineralized Connective Tissues. J Bone Miner Res 1992, 7, 987–997. [Google Scholar] [CrossRef] [PubMed]
- Ganss, B.; Kim, R.H.; Sodek, J. Bone Sialoprotein. Crit Rev Oral Biol Med 1999, 10, 79–98. [Google Scholar] [CrossRef]
- Zhang, J.; Tu, Q.; Chen, J. Applications of Transgenics in Studies of Bone Sialoprotein. J Cell Physiol 2009, 220, 30–34. [Google Scholar] [CrossRef]
- Yeomans, J.D.; Urist, M.R. Bone Induction by Decalcified Dentine Implanted into Oral, Osseous and Muscle Tissues. Arch Oral Biol 1967, 12, 999–1008. [Google Scholar] [CrossRef]
- Bang, G.; Urist, M.R. Bone Induction in Excavation Chambers in Matrix of Decalcified Dentin. Arch Surg 1967, 94, 781–789. [Google Scholar] [CrossRef]
- Schmidt-Schultz, T.H.; Schultz, M. Intact Growth Factors Are Conserved in the Extracellular Matrix of Ancient Human Bone and Teeth: A Storehouse for the Study of Human Evolution in Health and Disease. Biol Chem 2005, 386, 767–776. [Google Scholar] [CrossRef]
- Bessho, K.; Tanaka, N.; Matsumoto, J.; Tagawa, T.; Murata, M. Human Dentin-Matrix-Derived Bone Morphogenetic Protein. J Dent Res 1991, 70, 171–175. [Google Scholar] [CrossRef] [PubMed]
- ten Dijke, P.; Miyazono, K.; Heldin, C.H. Signaling via Hetero-Oligomeric Complexes of Type I and Type II Serine/Threonine Kinase Receptors. Curr Opin Cell Biol 1996, 8, 139–145. [Google Scholar] [CrossRef] [PubMed]
- Ripamonti, U.; Ramoshebi, L.N.; Matsaba, T.; Tasker, J.; Crooks, J.; Teare, J. Bone Induction by BMPs/OPs and Related Family Members in Primates. J Bone Joint Surg Am 2001, 83-A Suppl 1, S116-127. [Google Scholar] [CrossRef]
- Burchardt, H. The Biology of Bone Graft Repair. Clin Orthop Relat Res 1983, 28–42. [Google Scholar] [CrossRef]
- Lorusso, F.; Inchingolo, F.; Dipalma, G.; Postiglione, F.; Fulle, S.; Scarano, A. Synthetic Scaffold/Dental Pulp Stem Cell (DPSC) Tissue Engineering Constructs for Bone Defect Treatment: An Animal Studies Literature Review. International Journal of Molecular Sciences 2020, 21. [Google Scholar] [CrossRef] [PubMed]
- Vermesan, D.; Prejbeanu, R.; Haragus, H.; Poenaru, D.V.; Mioc, M.L.; Tatullo, M.; Abbinante, A.; Scacco, S.; Tarullo, A.; Inchingolo, F.; et al. Clinical Relevance of Altered Bone Immunopathology Pathways around the Elbow. Eur Rev Med Pharmacol Sci 2014, 18, 2846–2850. [Google Scholar]
- Arafat Kabir, Md.; Murata, M.; Kusano, K.; Mohammad Zakaria, S.; Hena Mohammad Noor, A.; Khuda, F.; Hossain, I.; Sultana, S.; Saito, T. Radiological Evaluation of Human Dentin Autografts in Bangladesh. J. Hard Tissue Biology. 2014, 23, 363–370. [Google Scholar] [CrossRef]
- Isacco, C.G.; Nguyen, K.C.D.; Pham, V.H.; Di Palma, G.; Aityan, S.K.; Tomassone, D.; Distratis, P.; Lazzaro, R.; Balzanelli, M.G.; Inchingolo, F. Searching for a Link between Bone Decay and Diabetes Type 2. Endocr Metab Immune Disord Drug Targets 2022, 22, 904–910. [Google Scholar] [CrossRef]
- Nakashima, M. Bone Morphogenetic Proteins in Dentin Regeneration for Potential Use in Endodontic Therapy. Cytokine Growth Factor Rev 2005, 16, 369–376. [Google Scholar] [CrossRef]
- Ballini, A.; Cantore, S.; Scacco, S.; Perillo, L.; Scarano, A.; Aityan, S.K.; Contaldo, M.; Cd Nguyen, K.; Santacroce, L.; Syed, J.; et al. A Comparative Study on Different Stemness Gene Expression between Dental Pulp Stem Cells vs. Dental Bud Stem Cells. Eur Rev Med Pharmacol Sci 2019, 23, 1626–1633. [Google Scholar] [CrossRef]
- Scarano, A.; Inchingolo, F.; Murmura, G.; Traini, T.; Piattelli, A.; Lorusso, F. Three-Dimensional Architecture and Mechanical Properties of Bovine Bone Mixed with Autologous Platelet Liquid, Blood, or Physiological Water: An In Vitro Study. Int J Mol Sci 2018, 19, 1230. [Google Scholar] [CrossRef] [PubMed]
- Rijal, G.; Shin, H.-I. Human Tooth-Derived Biomaterial as a Graft Substitute for Hard Tissue Regeneration. Regen Med 2017, 12, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Hazballa, D.; Inchingolo, A.D.; Inchingolo, A.M.; Malcangi, G.; Santacroce, L.; Minetti, E.; Di Venere, D.; Limongelli, L.; Bordea, I.R.; Scarano, A.; et al. The Effectiveness of Autologous Demineralized Tooth Graft for the Bone Ridge Preservation: A Systematic Review of the Literature. J Biol Regul Homeost Agents 2021, 35, 283–294. [Google Scholar] [CrossRef] [PubMed]
- Rapone, B.; Inchingolo, A.D.; Trasarti, S.; Ferrara, E.; Qorri, E.; Mancini, A.; Montemurro, N.; Scarano, A.; Inchingolo, A.M.; Dipalma, G.; et al. Long-Term Outcomes of Implants Placed in Maxillary Sinus Floor Augmentation with Porous Fluorohydroxyapatite (Algipore® FRIOS®) in Comparison with Anorganic Bovine Bone (Bio-Oss®) and Platelet Rich Plasma (PRP): A Retrospective Study. Journal of Clinical Medicine 2022, 11, 2491. [Google Scholar] [CrossRef] [PubMed]
- Boyne, P.J. Experimental Evaluation of the Osteogenic Potential of Bone Graft Materials. Annu Meet Am Inst Oral Biol 1969, 13–21. [Google Scholar]
- Mellonig, J.T.; Bowers, G.M.; Cotton, W.R. Comparison of Bone Graft Materials. Part II. New Bone Formation with Autografts and Allografts: A Histological Evaluation. J Periodontol 1981, 52, 297–302. [Google Scholar] [CrossRef]
- Colnot, C.; Romero, D.M.; Huang, S.; Helms, J.A. Mechanisms of Action of Demineralized Bone Matrix in the Repair of Cortical Bone Defects. Clin Orthop Relat Res 2005, 69–78. [Google Scholar] [CrossRef]
- Araújo, M.G.; Sonohara, M.; Hayacibara, R.; Cardaropoli, G.; Lindhe, J. Lateral Ridge Augmentation by the Use of Grafts Comprised of Autologous Bone or a Biomaterial. An Experiment in the Dog. J Clin Periodontol 2002, 29, 1122–1131. [Google Scholar] [CrossRef]
- Minamizato, T.; Koga, T.; I, T.; Nakatani, Y.; Umebayashi, M.; Sumita, Y.; Ikeda, T.; Asahina, I. Clinical Application of Autogenous Partially Demineralized Dentin Matrix Prepared Immediately after Extraction for Alveolar Bone Regeneration in Implant Dentistry: A Pilot Study. Int J Oral Maxillofac Surg 2018, 47, 125–132. [Google Scholar] [CrossRef]
- Kim, S.-Y.; Kim, Y.-K.; Park, Y.-H.; Park, J.-C.; Ku, J.-K.; Um, I.-W.; Kim, J.-Y. Evaluation of the Healing Potential of Demineralized Dentin Matrix Fixed with Recombinant Human Bone Morphogenetic Protein-2 in Bone Grafts. Materials (Basel) 2017, 10, 1049. [Google Scholar] [CrossRef]
- Libonati, A.; Marzo, G.; Klinger, F.G.; Farini, D.; Gallusi, G.; Tecco, S.; Mummolo, S.; De Felici, M.; Campanella, V. Embryotoxicity Assays for Leached Components from Dental Restorative Materials. Reprod Biol Endocrinol 2011, 9, 136. [Google Scholar] [CrossRef] [PubMed]
- Clinical Application of Autogenous Tooth as Bone Graft Material in Extraction Socket- A Prospective Study - Clinical Epidemiology and Global Health. Available online: https://cegh.net/article/S2213-3984(22)00105-1/fulltext (accessed on 3 April 2023)..
- Minetti, E.; Berardini, M.; Trisi, P. A New Tooth Processing Apparatus Allowing to Obtain Dentin Grafts for Bone Augmentation: The Tooth Transformer. TODENTJ 2019, 13, 6–14. [Google Scholar] [CrossRef]
- Bono, N.; Tarsini, P.; Candiani, G. BMP-2 and Type I Collagen Preservation in Human Deciduous Teeth after Demineralization. Journal of Applied Biomaterials & Functional Materials 2019, 17, 228080001878423. [Google Scholar] [CrossRef]
- Bianchi, S.; Mancini, L.; Torge, D.; Cristiano, L.; Mattei, A.; Varvara, G.; Macchiarelli, G.; Marchetti, E.; Bernardi, S. Bio-Morphological Reaction of Human Periodontal Ligament Fibroblasts to Different Types of Dentinal Derivates: In Vitro Study. Int J Mol Sci 2021, 22, 8681. [Google Scholar] [CrossRef] [PubMed]
- Minetti, E.; Palermo, A. Comparison between the Bone Regeneration Using Tooth Graft with or without Tooth Transformer in Sheep. BAOJ Dentistry 5.
- Minetti, E.; Corbella, S.; Taschieri, S.; Canullo, L. Tooth as Graft Material: Histologic Study. Clin Implant Dent Relat Res 2022, 24, 488–496. [Google Scholar] [CrossRef] [PubMed]
- DENTAL SUPPLEMENT; Minetti, E. ; Palermo, A.; Savadori, P.; Barlattani, A.; Franco, R.; Michele, M.; Gianfreda, F.; Bollero, P. Autologous Tooth Graft: A Histological Comparison between Dentin Mixed with Xenograft and Dentin Alone Grafts in Socket Preservation. J Biol Regul Homeost Agents 2019, 33, 189–197. [Google Scholar]
- Minetti, E.; Celko, M.; Contessi, M.; Carini, F.; Gambardella, U.; Giacometti, E.; Santillana, J.; Beca Campoy, T.; Schmitz, J.H.; Libertucci, M.; et al. Implants Survival Rate in Regenerated Sites with Innovative Graft Biomaterials: 1 Year Follow-Up. Materials 2021, 14, 5292. [Google Scholar] [CrossRef]
- Minetti, E.; Giacometti, E.; Gambardella, U.; Contessi, M.; Ballini, A.; Marenzi, G.; Celko, M.; Mastrangelo, F. Alveolar Socket Preservation with Different Autologous Graft Materials: Preliminary Results of a Multicenter Pilot Study in Human. Materials 2020, 13, 1153. [Google Scholar] [CrossRef]
- Santos, A.; Botelho, J.; Machado, V.; Borrecho, G.; Proença, L.; Mendes, J.J.; Mascarenhas, P.; Alcoforado, G. Autogenous Mineralized Dentin versus Xenograft Granules in Ridge Preservation for Delayed Implantation in Post-Extraction Sites: A Randomized Controlled Clinical Trial with an 18 Months Follow-Up. Clin Oral Implants Res 2021, 32, 905–915. [Google Scholar] [CrossRef]
- Oguić, M.; Čandrlić, M.; Tomas, M.; Vidaković, B.; Blašković, M.; Jerbić Radetić, A.T.; Zoričić Cvek, S.; Kuiš, D.; Cvijanović Peloza, O. Osteogenic Potential of Autologous Dentin Graft Compared with Bovine Xenograft Mixed with Autologous Bone in the Esthetic Zone: Radiographic, Histologic and Immunohistochemical Evaluation. Int J Mol Sci 2023, 24, 6440. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.M.; Patano, A.; Di Pede, C.; Inchingolo, A.D.; Palmieri, G.; de Ruvo, E.; Campanelli, M.; Buongiorno, S.; Carpentiere, V.; Piras, F.; et al. Autologous Tooth Graft: Innovative Biomaterial for Bone Regeneration. Tooth Transformer® and the Role of Microbiota in Regenerative Dentistry. A Systematic Review. Journal of Functional Biomaterials 2023, 14, 132. [Google Scholar] [CrossRef] [PubMed]
- Inchingolo, A.D.; Malcangi, G.; Inchingolo, A.M.; Piras, F.; Settanni, V.; Garofoli, G.; Palmieri, G.; Ceci, S.; Patano, A.; De Leonardis, N.; et al. Benefits and Implications of Resveratrol Supplementation on Microbiota Modulations: A Systematic Review of the Literature. International Journal of Molecular Sciences 2022, 23, 4027. [Google Scholar] [CrossRef] [PubMed]
- Schutyser, M. a. I.; Briels, W.J.; Rinzema, A.; Boom, R.M. Numerical Simulation and PEPT Measurements of a 3D Conical Helical-Blade Mixer: A High Potential Solids Mixer for Solid-State Fermentation. Biotechnology and Bioengineering 2003, 84, 29–39. [Google Scholar] [CrossRef] [PubMed]
- Hansen, S.H.; Holmfred, E.; Cornett, C.; Maldonado, C.; Rønsted, N. An Efficient, Robust, and Inexpensive Grinding Device for Herbal Samples like Cinchona Bark. Sci Pharm 2015, 83, 369–376. [Google Scholar] [CrossRef] [PubMed]
- Saarinen, T.; Antikainen, O.; Yliruusi, J. Simultaneous Comparison of Two Roller Compaction Techniques and Two Particle Size Analysis Methods. AAPS PharmSciTech 2017, 18, 3198–3207. [Google Scholar] [CrossRef] [PubMed]
- Ndiaye, M.; Terranova, L.; Mallet, R.; Mabilleau, G.; Chappard, D. Three-Dimensional Arrangement of β-Tricalcium Phosphate Granules Evaluated by Microcomputed Tomography and Fractal Analysis. Acta Biomaterialia 2015, 11, 404–411. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-K.; Kim, S.-G.; Yun, P.-Y.; Yeo, I.-S.; Jin, S.-C.; Oh, J.-S.; Kim, H.-J.; Yu, S.-K.; Lee, S.-Y.; Kim, J.-S.; et al. Autogenous Teeth Used for Bone Grafting: A Comparison with Traditional Grafting Materials. Oral Surg Oral Med Oral Pathol Oral Radiol 2014, 117, e39–45. [Google Scholar] [CrossRef]
- Jun, S.-H.; Ahn, J.-S.; Lee, J.-I.; Ahn, K.-J.; Yun, P.-Y.; Kim, Y.-K. A Prospective Study on the Effectiveness of Newly Developed Autogenous Tooth Bone Graft Material for Sinus Bone Graft Procedure. J Adv Prosthodont 2014, 6, 528–538. [Google Scholar] [CrossRef]
- Kim, Y.-K.; Lee, J.; Um, I.-W.; Kim, K.-W.; Murata, M.; Akazawa, T.; Mitsugi, M. Tooth-Derived Bone Graft Material. J Korean Assoc Oral Maxillofac Surg 2013, 39, 103–111. [Google Scholar] [CrossRef]
- Murata, M. Bone Engineering Using Human Demineralized Dentin Matrix and Recombinant Human BMP-2. J. Hard Tissue Biology. 2005, 14, 80–81. [Google Scholar] [CrossRef]
- Nampo, T.; Watahiki, J.; Enomoto, A.; Taguchi, T.; Ono, M.; Nakano, H.; Yamamoto, G.; Irie, T.; Tachikawa, T.; Maki, K. A New Method for Alveolar Bone Repair Using Extracted Teeth for the Graft Material. J Periodontol 2010, 81, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Kim, Y.-K.; Kim, S.-G.; Byeon, J.-H.; Lee, H.-J.; Um, I.-U.; Lim, S.-C.; Kim, S.-Y. Development of a Novel Bone Grafting Material Using Autogenous Teeth. Oral Surg Oral Med Oral Pathol Oral Radiol Endod 2010, 109, 496–503. [Google Scholar] [CrossRef] [PubMed]
- Dozza, B.; Lesci, I.G.; Duchi, S.; Della Bella, E.; Martini, L.; Salamanna, F.; Falconi, M.; Cinotti, S.; Fini, M.; Lucarelli, E.; et al. When Size Matters: Differences in Demineralized Bone Matrix Particles Affect Collagen Structure, Mesenchymal Stem Cell Behavior, and Osteogenic Potential. J Biomed Mater Res A 2017, 105, 1019–1033. [Google Scholar] [CrossRef] [PubMed]
- Campana, V.; Milano, G.; Pagano, E.; Barba, M.; Cicione, C.; Salonna, G.; Lattanzi, W.; Logroscino, G. Bone Substitutes in Orthopaedic Surgery: From Basic Science to Clinical Practice. J Mater Sci Mater Med 2014, 25, 2445–2461. [Google Scholar] [CrossRef]
- Testori, T.; Wallace, S.S.; Trisi, P.; Capelli, M.; Zuffetti, F.; Del Fabbro, M. Effect of Xenograft (ABBM) Particle Size on Vital Bone Formation Following Maxillary Sinus Augmentation: A Multicenter, Randomized, Controlled, Clinical Histomorphometric Trial. Int J Periodontics Restorative Dent 2013, 33, 467–475. [Google Scholar] [CrossRef]
- Carano, R.A.D.; Filvaroff, E.H. Angiogenesis and Bone Repair. Drug Discov Today 2003, 8, 980–989. [Google Scholar] [CrossRef]
- Shapoff, C.A.; Bowers, G.M.; Levy, B.; Mellonig, J.T.; Yukna, R.A. The Effect of Particle Size on the Osteogenic Activity of Composite Grafts of Allogeneic Freeze-Dried Bone and Autogenous Marrow. J Periodontol 1980, 51, 625–630. [Google Scholar] [CrossRef]
- Pallesen, L.; Schou, S.; Aaboe, M.; Hjørting-Hansen, E.; Nattestad, A.; Melsen, F. Influence of Particle Size of Autogenous Bone Grafts on the Early Stages of Bone Regeneration: A Histologic and Stereologic Study in Rabbit Calvarium. Int J Oral Maxillofac Implants 2002, 17, 498–506. [Google Scholar]
- Gideon Hallel, I.B. A Novel Procedure to Process Extracted Teeth for Immediate Grafting of Autogenous Dentin. J Interdiscipl Med Dent Sci 2014, 02. [Google Scholar] [CrossRef]
- Klüppel, L.E.; Antonini, F.; Olate, S.; Nascimento, F.F.; Albergaria-Barbosa, J.R.; Mazzonetto, R. Bone Repair Is Influenced by Different Particle Sizes of Anorganic Bovine Bone Matrix: A Histologic and Radiographic Study in Vivo. J Craniofac Surg 2013, 24, 1074–1077. [Google Scholar] [CrossRef] [PubMed]
- Kon, K.; Shiota, M.; Ozeki, M.; Yamashita, Y.; Kasugai, S. Bone Augmentation Ability of Autogenous Bone Graft Particles with Different Sizes: A Histological and Micro-Computed Tomography Study. Clin Oral Implants Res 2009, 20, 1240–1246. [Google Scholar] [CrossRef]
- Fucini, S.E.; Quintero, G.; Gher, M.E.; Black, B.S.; Richardson, A.C. Small versus Large Particles of Demineralized Freeze-Dried Bone Allografts in Human Intrabony Periodontal Defects. J Periodontol 1993, 64, 844–847. [Google Scholar] [CrossRef] [PubMed]
- Xu, H.; Shimizu, Y.; Asai, S.; Ooya, K. Experimental Sinus Grafting with the Use of Deproteinized Bone Particles of Different Sizes. Clin Oral Implants Res 2003, 14, 548–555. [Google Scholar] [CrossRef] [PubMed]
- Coathup, M.J.; Cai, Q.; Campion, C.; Buckland, T.; Blunn, G.W. The Effect of Particle Size on the Osteointegration of Injectable Silicate-Substituted Calcium Phosphate Bone Substitute Materials. J Biomed Mater Res B Appl Biomater 2013, 101, 902–910. [Google Scholar] [CrossRef]
- Prieto, E.M.; Talley, A.D.; Gould, N.R.; Zienkiewicz, K.J.; Drapeau, S.J.; Kalpakci, K.N.; Guelcher, S.A. Effects of Particle Size and Porosity on in Vivo Remodeling of Settable Allograft Bone/Polymer Composites. J Biomed Mater Res B Appl Biomater 2015, 103, 1641–1651. [Google Scholar] [CrossRef]
- Gultekin, B.A.; Bedeloglu, E.; Kose, T.E.; Mijiritsky, E. Comparison of Bone Resorption Rates after Intraoral Block Bone and Guided Bone Regeneration Augmentation for the Reconstruction of Horizontally Deficient Maxillary Alveolar Ridges. Biomed Res Int 2016, 2016, 4987437. [Google Scholar] [CrossRef]
- Koga, T.; Minamizato, T.; Kawai, Y.; Miura, K.; I, T.; Nakatani, Y.; Sumita, Y.; Asahina, I. Bone Regeneration Using Dentin Matrix Depends on the Degree of Demineralization and Particle Size. PLoS One 2016, 11, e0147235. [Google Scholar] [CrossRef]
- Chackartchi, T.; Iezzi, G.; Goldstein, M.; Klinger, A.; Soskolne, A.; Piattelli, A.; Shapira, L. Sinus Floor Augmentation Using Large (1-2 Mm) or Small (0.25-1 Mm) Bovine Bone Mineral Particles: A Prospective, Intra-Individual Controlled Clinical, Micro-Computerized Tomography and Histomorphometric Study. Clin Oral Implants Res 2011, 22, 473–480. [Google Scholar] [CrossRef]
- Kon, K.; Shiota, M.; Ozeki, M.; Kasugai, S. The Effect of Graft Bone Particle Size on Bone Augmentation in a Rabbit Cranial Vertical Augmentation Model: A Microcomputed Tomography Study. Int J Oral Maxillofac Implants 2014, 29, 402–406. [Google Scholar] [CrossRef]
- Minetti, E.; Corbella, S.; Taschieri, S. The Weight of Permanent Teeth: An Exploratory Study on a Total of 205 Teeth. Quintessenza Internazionale & Jomi 2019, 34, 85–89. [Google Scholar]
Figure 1.
(a) and (b) Two high speed grinders. (c) the low high speed grinder.
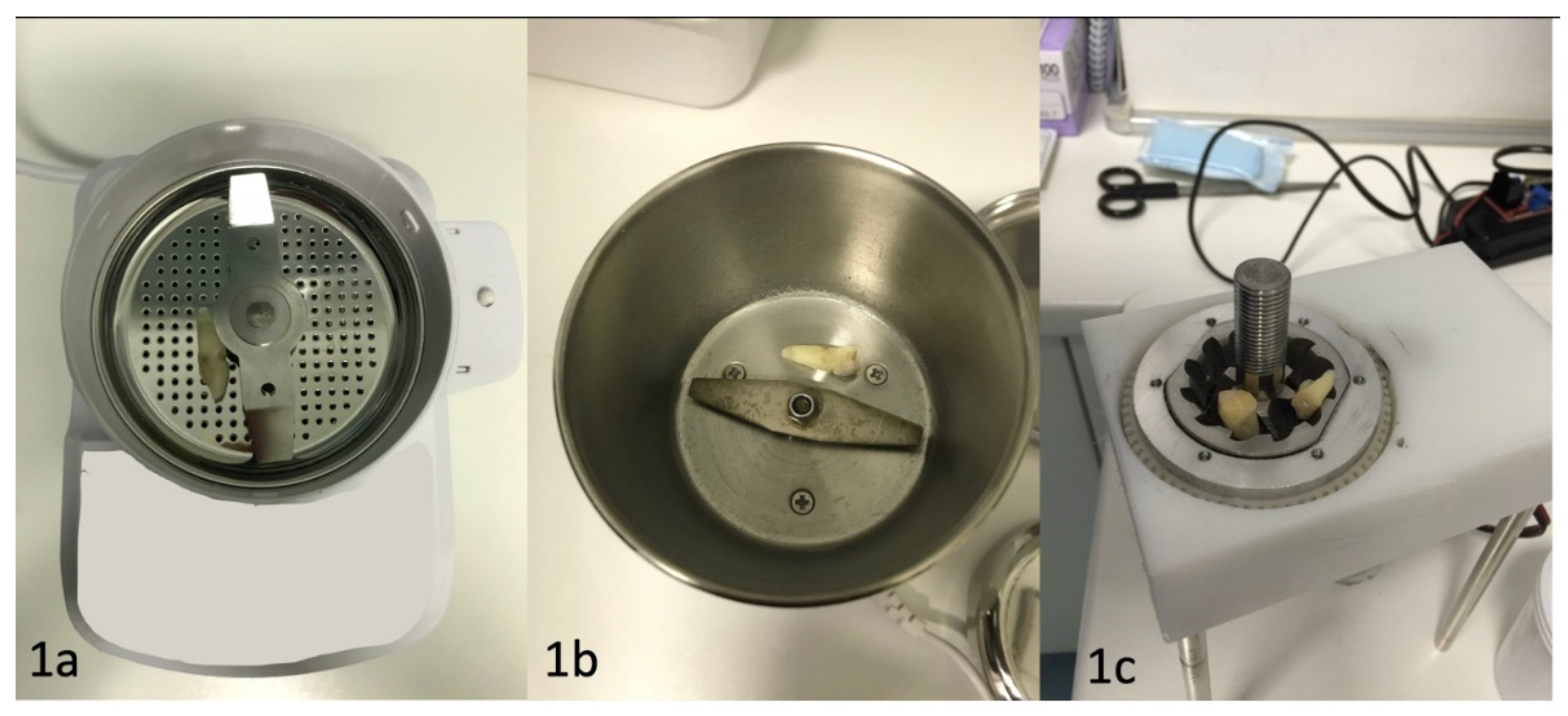
Figure 2.
(a) Granules produced with the high-speed grinder. Different sized granules can be seen, many of which are very small. (b) Granules produced with a lowspeed grinder, similar in size and similar in shape.
Figure 2.
(a) Granules produced with the high-speed grinder. Different sized granules can be seen, many of which are very small. (b) Granules produced with a lowspeed grinder, similar in size and similar in shape.
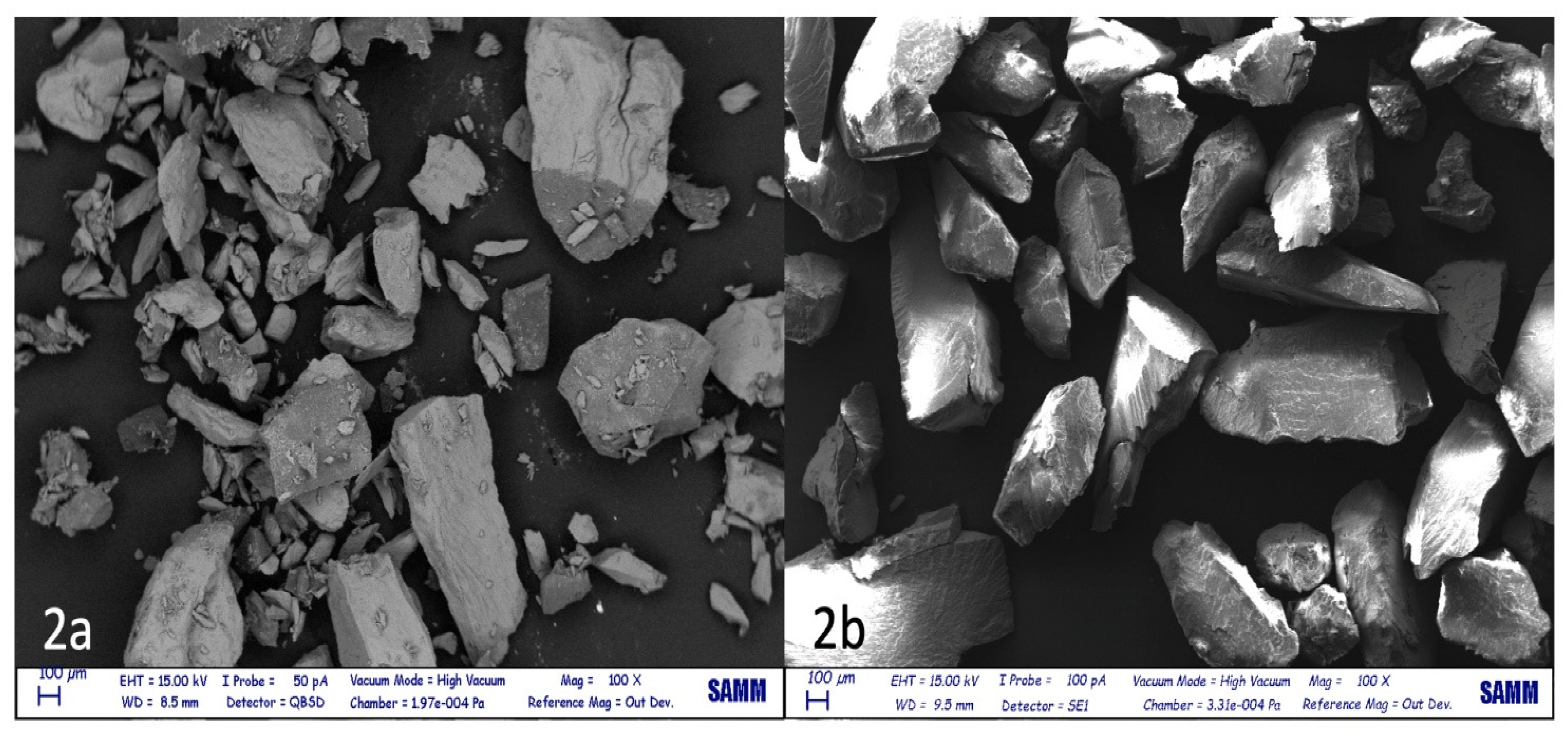
Figure 3.
Calibrated sieve able to differentiate the granules sizes.

Figure 4.
The forty natural human teeth used.


Table 1.
Results of the tests.
| Type of test | Average tooth weight before test | Average tooth weight after test | Lost tooth weight (%) |
|---|---|---|---|
| High speed | 1.2+/-0.53 | 0.56 +/-0.29 | 53.5+/-9.89 |
| Low speed | 1.44 +/-0.62 | 1.32+/-0.58 | 9.16+/-2.34 |
Table 2.
Graft granules’ dimensions reported by different studies. The table indicate what are the size of the granules commonly considered optimal in regeneration and then have a reference.
Table 2.
Graft granules’ dimensions reported by different studies. The table indicate what are the size of the granules commonly considered optimal in regeneration and then have a reference.
| Authors | Granules’ dimensions (mm) |
|---|---|
| Kim, Y., 2013 [61] |
0.5–1.0 |
| Kim, Y., 2013 [63] |
0.4–0.8 |
| Murata M., 2005 [64] |
0.4–0.8 |
| Nampo T., 2010 [65] |
0.5 |
| Kim Y., 2010 [66] |
0.2–1.2 |
| Jun S.H.,2014 [62] |
0.5–1 |
| Binderman I., 2014 [73] |
0.3–1.2 |
| Dozza B., 2017 [67] |
0.5–1.0 |
| Testori T., 2013 [69] |
1–2.0 |
| Kluppel L.E., 2013 [74] |
0.2–0.4 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



