
Submitted:
03 May 2023
Posted:
04 May 2023
You are already at the latest version
Abstract
Knee Osteoarthritis (KOA), the most common knee degenerative disease, involve a slow destructive process, leading to disability and ultimately total knee replacement. The progression of KOA is related to the loss of rheological properties of the synovial fluid (SF), due to slow immunological, inflammatory and enzymatic processes that cleave the hyaluronic acid (HA) and decrease the concentration of specific proteins. Since no effective treatments have been found to halt the progression of KOA, injection of HA-based viscoelastic gels combined with physiotherapy (PT) is an alternative to symptomatic therapies. In order to evaluate the effect of viscosupplementation and PT on the SF characteristics, the SF aspirated from the KOA was spectrophotometrically and rheological analyzed, comparing the receiving groups of HA Kombihylan® and groups that received Kombihylan® and complex PT. In patients treated with PT, SF extracted 6 weeks after viscosupplementation had a superior elastic moduli (G') and viscous moduli (G") profile behavior, having a homogeneous distribution of proteins and polysaccharides in the SF, stimulating stronger interactions. In the absence of PT the G' and G" profiles are non-uniform, suggesting an unorganized supplemented SF with some clustering phenomena, proteins aggregation and a low level of entanglement between HA and macromolecular components in the SF.
Keywords:
knee osteoarthritis
; synovial fluid
; hyaluronic acid
; physical therapy
; ATR-FTIR spectroscopy
; rheological properties
; bioadhesion
1. Introduction
Arthritis is a major health problem of the world with prevalence higher than many well-known diseases like cancer, diabetes, and AIDS and raised incidence with the aging of the population [1]. Arthritis is recognized as one of the chronic disabling diseases and seriously affects the quality of life with several clinical symptoms like pain, stiffness, swelling, deformity, and necrosis [2]. More than 100 forms of arthritis have been identified, but mainly include various inflammations in joints such as osteoarthritis (OA) and rheumatoid arthritis (RA), synovitis and gout, bursitis, and traumatic arthritis [3]. This alarming situation recommends more intensive studies for prevention, precise and early diagnostics, and more efficient treatment for patients [4].
OA is an all-articular disease, generally affecting elderly patients, and involves articular cartilage, subchondral bone, ligaments, capsule, synovium, and periarticular muscles, with destroyed structures and lost function, ultimately leading to joint failure. In the case of damaged cartilage, the tendons and the ligaments are stretched, resulting in pain. Eventually, the bones may rub against each other causing severe pain, stiffness, and other symptoms. The joint pain is caused by the absence of suitable synovial fluid (SF) which leads to the failure of boundary lubrication and thereby direct bone-to-bone contact [5,6]. Therefore, the primary property of SF is to serve as a synovial lubricant, absorbing the shocks and, additionally, to be a source of nutrition for the joint cartilage (Figure 1) [7].
One of the main components of SF is the hyaluronic acid (HA), a high molecular weight polysaccharide, which is involved in a wide range of physiological processes in the human body, such as wound healing, tumor progression, and joint lubrication. HA interacts with lipidic membranes in a manner that is related to the interaction of mono- and disaccharides with such biomembranes and contributes to joint lubrication [8,9,10]. The changes in the concentrations of the constituents, rheological properties alteration of degenerated SF, especially the reduced viscosity compared to healthy SF, play a decisive role in the installation of joint diseases such as osteoarthritis and arthrosis [11].
The lack of an effective strategy to understand biochemical and biophysical phenomena from an OA perspective has led to different approaches to this much-discussed pathology, but with modest results. The most effective therapy and medication are sought to ensure the restoration of joint structures or at least preserve the integrity of the joint structures, pain relief, inflammation, and dysfunction reduction, with few side effects and low long-term costs [4].
Common pharmacological treatment options include simple analgesics, nonsteroidal anti-inflammatory drugs (NSAIDs), selective competitive inhibitors of cyclooxygenase (COX-2), intra-articular corticosteroid injections, viscosupplementation, and surgery. However, NSAIDs can cause gastrointestinal problems, stroke, renal failure, and hypertension and have thrombotic potential, especially at high doses [12].
Non-pharmacological strategies are a first-line approach to symptom management, and include exercises, weight loss, and patient education [12,13]. Physical activity of 150 min/week consisting of moderate-intensity aerobic exercises or 2 days/week of moderate to vigorous physical activity in muscle-strengthening exercises is important for maintaining physical function in knee OA (KOA). An effective alternative with limited side effects in the management of KOA is the intra-articular injection with HA-based viscoelastic substances and physical therapy (PT). Although all types of PT that could be effective in reducing the symptoms of KOA are carefully studied, currently, there are no guidelines for standardized PT protocols using effective combinations of physical agents and medications to control the progression of KOA [13].
PT procedures are clinically proven tools and have an anti-inflammatory effect which makes them extremely useful in reducing the symptoms of KOA. Both HA viscosupplementation and PT have anti-inflammatory effects on low-grade inflammation in KOA, and the combination of the two therapies can prolong the effects of HA viscosupplementation over time [14].
The objective of this study was to evaluate in vivo the ability of combined therapy based on intra-articularly HA supplementation (Kombihylan®) and PT to improve the properties of SF collected from knees with moderate KOA. The PT program includes TENS currents, LASER photostimulation, low-dose ultrasound, exercises, and cryotherapy.
TENS (Transcutaneous electrical nerve stimulation) are rectangular single-phase or biphasic pulsed currents that are distributed over the skin to stimulate the underlying nerves to produce intense analgesia [15]. TENS selectively activates the fastest conduction velocity large-diameter non-nociceptive Abeta-fiber, to reduce nociceptor sensitivity and activity at a segmental level [15]. According to Qi and James, Abeta-fiber non-nociceptive primary sensory neurons are involved in the pathogenesis of KOA pain in rat models [16]. TENS reduces pain in KOA by activating native opioid receptors and selectively stimulating large-diameter, non-noxious, dermatome-corresponding afferents [17,18]. TENS also has an anti-inflammatory effect which has been less studied, as it is used in PT mainly for its analgesic effects. TENS may reduce the inflammatory process by lowering pro-inflammatory cytokines levels (especially IL-6) through two possible mechanisms: activates opioid release by the central nervous system and the pain gate mechanism (gate theory) [19,20].
Ultrasound (US) is a high-frequency therapy that uses mechanical vibrations with frequencies between 1 and 3 MHz. The US stimulates cellular and molecular effects within cells that are involved in healing processes [21]. US is a non-invasive and safe form of PT used in KOA. US in KOA controls the symptoms and has a potential cartilage repair effect [22]. US promotes collagen formation, regulates inflammatory responses, and induces cartilage repair at low doses [23,24]. Priscila Daniele de Oliveira Perrucini et al. have shown that US at 0.2 W/cm2 with 10% duty-cycle is much more effective with a higher bio-stimulatory response than US at 0.5 W/cm2 with 20% duty-cycle. Low-dose US decreased IL-6 cytokine production from both- the area directly exposed to treatment and from serum levels [25].
Current KOA treatment protocols do not include Low-Level Laser Therapy (LLLT) for lesser-known reasons. LLLT is a form of low-power LASER photo biostimulation. LLLT has significant analgesic, and anti-inflammatory effects and a bio-modulatory effect on microcirculation which helps to heal tissues and reduce lymphoedema [26,27]. Béla Heged˝us et al. have shown that LLLT in KOA reduced pain and improved knee function in 27 patients who underwent a 4-week therapy program with two sessions per week. The LLLT used was a GaAlAs diode laser with a power of 50 mW and a wavelength of 830 nm [28]. Stausholm MB et al. in a systematic review and meta-analysis of RCTs published in 2019, investigated whether there is an LLLT dose-response relationship in KOA. The study used eligible articles from PubMed, Embase, Physiotherapy Evidence Database, Cumulative Index to Nursing and Allied Health Literature, and Cochrane Central Register of Controlled Trials. According to this study, LLLT significantly reduces pain and inflammation in KOA using two types of LASER: 904 nm wavelength with 1-3 J and 785-860 nm wavelength with 4-8 J power [29].
Cryotherapy is a safe and widely used PT procedure in the control of post-traumatic pain, inflammation, and edema management. Cryotherapy is not usually found in KOA treatment guidelines but Barbosa et al. have shown that this procedure has an anti-inflammatory effect. Cryotherapy reduces leukocyte migration and decreases the concentration of inflammatory cytokines in the synovium on posttraumatic KOA in rat models [30]. Garcia et al. demonstrated in an Evidence-Based Narrative that cryotherapy is used to reduce chronic local pain. Searches were done in PubMed tracking human studies between 2000 and 2020 that included the application of cryotherapy to patients with chronic pain disease. Twenty-five studies were selected that met the criteria, 22 of which were RCTs, that local applications of cryotherapy have analgesic, anti-inflammatory and anti-edematous effects in patients with rheumatic pain including those with degenerative pathology such as KOA [31]. Local cryotherapy positively influences local edema and lower the level of pro-inflammatory cytokines, which are actually key elements in assessing the effectiveness of different treatments on inflammation [32]. Studies have suggested that the anti-inflammatory effect of cryotherapy is due to reduced levels of the pro-inflammatory cytokine TNF-α and increased levels of the anti-inflammatory cytokine IL-10 [33,34,35]. Cryotherapy was used in this study to reduce the joint temperature during the session, especially after exercises, to protect the intraarticular injected HA-biopolymer.
Guidelines from The American Academy of Orthopaedic Surgeons, the American College of Rheumatology, and the European League Against Rheumatism, are consistent in recommending physical exercises (PE) because they can relieve pain, reduce disability and increase the quality of life in KOA [36,37,38]. There is evidence of the benefits of PE in KOA. Individuals who undergo a moderate PE program can expect a reduction in knee pain and disability during and immediately after the program [39]. Strength training PE restores quadriceps muscle strength, relieving knee pain and stiffness and improving shock absorption during walking [40,41,42]. Isokinetic PE is an effective form of training for muscle toning of the quadriceps useful in the management of KOA and has an anti-inflammatory effect by reducing serum levels of C-reactive protein, TNF- and IL-6 [43]. The isometric (static) exercise used in KOA involves isometric contraction of the thigh and calf muscles. Miyaguchi et al. demonstrated that LS increases its viscosity which is associated with increased hyaluronan molecular weight, in groups of subjects who underwent an isometric cavdriceps exercise at a 12-week program. This suggests that isometric PE has a positive effect on the rheological properties of LS, which is degraded in KOA and loses its vasoelastic properties through inflammatory, enzymatic and immunological mechanisms [44].
2. Materials and Methods
2.1. Materials
The viscoelastic material with the commercial name Kombihylan® was purchased from Ropharm® (Romania) and used with approval no. 11306 from 2020. Kombihylan® is a biological matrix with a molecular weight of 3 MDa in the form of a viscoelastic solution containing HA which is obtained by bacterial fermentation of a Streptococcus strain. The study was conducted according to the guidelines of the Declaration of Helsinki and was approved by the Institutional Review Board (or Ethics Committee) of Micromedica Medical Clinic with no. 32 from 28 January 2020. All patients signed informed consent. The product was administered intra-articular by an orthopedic specialist to patients with moderate KOA.
2.2. Study design and Procedure Steps (PS)
The SFs were collected from nine patients divided into 3 groups (Table 1). For patients with no procedure (n=3) 2-3 ml of synovial fluid was aspirated from their knees: Control 1, Control 2, and Control 3. Patients who received Kombihylan® (3 MDa) viscosupplementation and physiotherapy (n=3): P1, P2, and P3; and the patients (n=3) that received injections only: P4, P5, and P6. Patients P1, P2, and P3 underwent 10 consecutive days of PT including TENS currents, LASER biostimulation, low-dose ultrasound, exercise, and cryotherapy. SF samples were taken from all patients immediately after viscosupplementation of the knee joint and after 6 weeks assessed the rheological and spectroscopic behavior.
For inclusion criteria, eligible patients were those diagnosed with symptomatic moderate KOA who showed no signs of local inflammation, and had not infiltrations with other viscoelastic substances or glucocorticoids in the past 12 months. Patients with only one symptomatic knee were also included. Exclusion criteria were: known allergy or hypersensitivity to sodium hyaluronate or any of the Kombihylan® ingredients and patients with signs of local inflammation or hydrarthrosis. Patients with pre-existing infections or skin disease at the injection site, with inflammatory rheumatic disease or systemic disease, or with known systemic bleeding disorders were also excluded.
Few steps (PS1-PS5) were followed in order to perform the experiments.
PS1: Using sterile techniques, an aspiration from the osteoarthritic knee was performed from the suprapatellar region with a needle and syringe to depressurize the joint capsule. About 2-3 mL of SF was aspirated from the knee joint to reduce post-procedural swelling, preventing the increase in intra-articular pressure.
PS2: Intra-articular infiltration was performed with the viscoelastic product Kombihylan® (3 mL) in the suprapatellar region using the same needle.
PS3: After removing the needle, the patient was asked to walk for 5–10 min to “homogenize” the viscoelastic product.
PS4: After 72 h, a group of three patients started the program of PT for 10 consecutive days (2 weeks).
PS5: 6 weeks later, SF was aspirated from the osteoarthritic knee joint and evaluated, rheologically and spectroscopically.
All tested synovial fluids are presented in Table 1.
2.3. Physiotherapy Treatment
PT1: TENS conventional for 30–40 min using two channels at 100 Hz at 100 µs rectangular biphasic pulses.
PT2: LLLT, 904-nm GaAlAs probe, 3 kHz frequency with a 5 Joules/point, and a maximum of 40 Joules/application.
PT3: US: 8 min of 0.2–0.3 W/cm2 at 1 MHz with a 10% duty cycle.
PT4: PE: over 40 min per session with moderate-intensity exercise that included the following: active exercises, isokinetic, isometry and neuro-proprioceptive facilitation (PNF): contract-relax, reversal of antagonists, repeated stretch and hold-relax
PT5: 15 min Cryo-push cryotherapy
2.4. Fluids charactersitics, pH and glucose concentration
Synovial liquid pH measurements were carried out on an multi-parameter (HI2020 - edge® Multiparameter pH Meter, Hanna Instruments, USA). A three point calibration (pH = 4.01, 7.00 and 10.01) was performed, using standard buffer solutions (Hanna Instruments, USA). The concentration of glucose was measured by using a portable glucometer (Accu-chek Performa®, Roche Laboratories, USA).
2.5. Drop Deposition of Synovial Fluid and Attenuated Total Reflectance Fourier Transform Infrared Spectroscopy (ATR-FTIR)
SF specimens were examined for their characteristics and some preparative steps were performed. Small volume (15 μl) drops of synovial fluid were deposited into 24 wells plate for cell culturing, at 37°C, and allowed to dry overnight, semi-covered, then examined the following day using light microscopy (Inverted Phase Contrast Microscope, Leica, Wetzlar, Germany) and stereomicroscopy (Stereomicroscope, Optika, Ponternica, Italy) and Infrared spectroscopy. Attenuated total reflectance Fourier transform infrared spectroscopy – ATR-FTIR (Nicolet Summit Pro FTIR Spectrometer with Everest ATR accessory, Thermo ScientificTM, Waltham, MA, USA) was used to evaluate the compositional changes in the synovial fluid. All samples were acquired using a diamond crystal at room temperature. The measurements were performed in a range of 400–4000 cm−1, with a spectral resolution of 4 cm-1, with 16 repetitious scans averaged for each spectrum. Prior to measurement, the materials were conditioned at 25°C and 65% relative humidity for 24 h.
2.6. Rheological measurements of synovial fluids
The rheometry measurements of the present work were carried out using Kinexus Pro+ rotational rheometer (Malvern Instruments Ltd., Worcestershire, United Kingdom), fitted with parallel plate geometry. All experiments were performed at a controlled temperature of 37 °C, and the experimental data were registered with rSpace for Kinexus Pro 1.7 software. The temperature of the samples was controlled with an accuracy of ± 0.1°C, by the Peltier system of the rheometers, on the testing plate. The amount of sample required for the rheological evaluation was 0.6 ml and the rest was used for the spectroscopic analysis and bioadhesion tests. For the SF viscosity and viscoelastic properties measurements, steady shear test and oscillatory shear test were performed. The strain test was mainly performed to establish the limits of the linear viscoelastic range (LVR). This test offers valuable information regarding the mechanical and structural stability of the SF. For the strain test, the angular frequency was kept constant, 10 rad/s, while the amplitude of deformations was varied between 0.01 and 100%. Frequency sweep tests were carried out at a constant amplitude of 1% (within the LVR), in a frequency domain between 0.01 and 200 rad/s.
2.7. Bioadhesive characteristics
Bioadhesion tests were performed on a TA.XT Plus® Texture Analyzer (Stable Micro Systems, Godalming, United Kingdom) fitted with module for bioadhesion tests [45,46], on two types of surfaces: simulating biological membrane and chicken cartilage. A cellulose membrane from a dialysis tubing 12,000 Da, pre-boiled and cooled at room temperature, has been prepared for in vitro experiments. Fresh cartilage was obtained from condyle of chicken femur and special prepared for experiment. The cartilage pieces were collected from chicken legs at least one week following their slaughter and conserved hydrated in physiological solution, together with the synovial membrane, without freezing.
The cellulose membrane/ cartilage pieces were fixed in the holding device and 200 µL of Phosphate Buffered solution (pH 7.2, 0.01M) was added to simulate the physiological environment; the whole system was introduced in a controlled temperature medium (heated distilled water at 37°C, under stirring, 200 rpm). The dried synovial fluid samples were attached to the bottom of the moving probe (cylindrical graphite probe – 8 mm diameter), which was lowered to the cellulose membrane and maintained for the pre-determined time (30 s) at a contact force of 9.80665 mN. Data collection and analysis were performed using the Texture Exponent software and maximum detachment force and the work of adhesion were calculated based on the force–time plots. Four samples were measured for each synovial fluid-based film.
2.8. Statistical Analysis
The results obtained were expressed as mean ± standard deviation (SD) of the mean values for each experiment, generally made in triplicate. The bioadhesion tests required 6 replicates for the considerable reduction of the method errors. Statistical analysis was performed by applying one-way ANOVA and Tukey posthoc analysis. Differences between groups were considered statistically significant for p <0.05.
3. Results and discussions
3.1. Hyaluronic acid effect on synovial fluid characteristics
SF is a biological gel involved in joint physiology and includes small molecular and macromolecular components, generally secreted by cells. Lubrication in the natural synovial joint is possible due to the particular macromolecular composition of the SF, the interactions between constituents and with the articular surfaces. The principal components of the SF are HA, lubricin, proteins, and surface active phospholipids (especially phosphatidylcholine) [47]. These lubricants are secreted by cells (chondrocytes in articular cartilage and synoviocytes in synovium), and concentrated in the joint cavity and deficiencies in this lubricating composition or structure contribute to the damaging of articulating cartilage surfaces [48]. The main component of the SF is the HA, a linear polysaccharide formed by repeating disaccharide units of D-glucuronic acid and N-acetyl glucosamine linked by β (1, 4) and β (1, 3) glycoside bonds. In physiological conditions, HA appears as a sodium salt (HAs), negatively charged, highly hydrophilic, and surrounded by a sphere of water molecules linked by hydrogen bonds. The architecture of this natural biopolymer exhibits excellent physicochemical and biological properties such as high water-binding capacity and interesting viscoelastic behavior [49], non-immunogenic and non-inflammatory characteristics, and totally biodegradable features [50]. Based on its unique properties, HA is intensively studied for various medical applications, such as wound healing, drug delivery and synovial fluid substitute.
Other components in SF include protein (content is about 2%), proteoglycan 4 (PRG4 - lubricin) and surface active phospholipids (SAPL, especially phosphatidylcoline) [51]. Many proteic components of SF are derived from blood plasma and proteins secreted from the surrounding tissue, and high-abundance proteins include albumin, serotransferrin, apolipoprotein A, and several immunoglobulins [52]. In the synovial joint is secreted lubricin, a glycoprotein which form coatings over the cartilage surface, providing boundary lubrication and preventing protein and cell adhesion [53]. Lubricin-assisted boundary lubrication is produced at very low sliding speeds and is based on formation of a lubricating film with thickness close to the surface roughness or asperities on the opposing cartilage surfaces. In the absence of lubricin, the protein and cell adhesion occurs and the friction increase, favoring a stick-slip phenomenon at the joint [54]. Small molecules, ions and salts are completing the synovial fluid composition.
Laboratory analysis for all tested SFs showed amber-yellow or yellow colour and transparent fluids (Table 1), indicating OA as joint disease. The pH of normal SF is 7.31–7.64 with a mean of 7.43. The pH in the presence of inflammation declines on average to 7.22 and range of 6.85 to 7.41 (mean 7.19) for joint diseases were reported in literature [55]. The pH values in tested SFs are presented in Figure 2.
The SFs in Control group present a wide distribution of pH values with a mean of 7.07, in agreement with other authors’ findings regarding the role of pH in OA development [56]. Values of pH between 7 and 7.2 were also measured for SFs from Group A (supplemented, 5-10 min movement) and Group C (supplemented, 5-10 min movement). The acidifying of the synovial fluid in OA is explained by some authors by initial joint inflammation and activation of cathepsin K, an acidic cysteine endoproteinase that degrades collagen from cartilage, influencing the synovial fluid too. This enzyme overexpressed in OA joints, is produced by phenotypically altered chondrocytes, which may initiate or accelerate cartilage degeneration. The activated cathepsin K stresses the intimate relationship between synovial fluid microenvironment and cartilage, contributing to the progressive degeneration of the cartilage [57]. In Group B - after PT (2 weeks PT + 4 weeks rest), and Group D (supplemented, 5-10 min movement, 6 weeks rest) the pH of the synovial fluid approached the normal values, as a result of the homogenization and lubrication effect induced by Kombihylan®, with a large contribution of the PT.
A high variability of the glucose concentration was observed in tested SFs. The highest values were measured in Control group. High concentrations of glucose have been associated with OA. Under limited amounts of oxygen the glucose is converted to lactate or pyruvate, which then enters the Krebs cycle. Anaerobic glycolysis occurs at an increased rate in OA-affected chondrocytes and glucose is released in synovial fluid[58]. Generally, the supplementation with hyaluronic and PT leaded to reduction of the glucose concentration.
3.2. Fourier-transform infrared (FTIR) data
Various methods have been tested in order to characterize the healthy or pathological SF, from biochemical analysis and structural evaluation of the macro and micro molecular components, to mechanically tests. Fourier-transform infrared (FTIR) spectroscopy was previously shown as being able to distinguish between healthy and serum SF samples with OA and has been considered as screening approach for diagnosis. Chondroitin sulfate (CS) profile in SF from a representative knee injured patient and on aggrecan purified from the same SF sample were compared and modifications in sulfated glycosaminoglycan have been identified [59]. In FTIR spectra differences in the C=O stretching vibrations (amide I region, 1584-1720 cm-1) and in C-O stretching vibrations of carbohydrate moieties (HA, 984-1140 cm-1) have been observed comparing with control, suggesting that FTIR spectroscopy could be an alternative analytical method to detect OA-related changes in HA from the SF, compared to the current immunoassay and chromatographic methods that often require more sophisticated instrumentations and sample processing [60].
In order to evaluate the effect of viscosupplementation and PT on the SF characteristics, the SFs aspirated from the osteoarthritic knee joint were spectrofotometrically analysed and compared with control group, raw Kombihylan® viscoelastic HA, HA and chondroitin sulphate. The ATR-FTIR spectra of pure HA (Figure 3A) presents characteristic peaks: the peak located at 3296.95 cm-1 is associated with intra- and intermolecular stretching vibration of -OH group, and the stretching vibration of the hydrogen bond from -NH- group, respectively; the symmetric stretching vibration from 2855.45 cm-1 corresponds to the -CH2 groups; the bands from 1596.53 cm-1 and 1405.37 cm-1 are correlated with symmetric and asymmetric vibration of COO- ionized group while the peak from 1023.26 cm-1 is related with the C-O-C hemiacetalic system saccharides units [61,62].
In the CS spectra, the region above 3000 cm− 1 is dominated by the OH stretching vibration. The band at 1372.58 cm− 1 was due to the sulfate and that from 1227.81 cm− 1 is attributed to S=O group. The peak at 850 cm− 1 corresponds to the C–O–S vibration [63]. The Kombihylan® product presents both polymers groups with a stronger highlighting of the peaks attributed to HA. It can be observed for all fluids extracted from the control group a decrease in the absorbance bands in 980 - 1140 cm−1 domain, corresponding to the carbohydrate content (sugar bands) and an overexpressed of the amide I region (1584-1720 cm-1), indicating an increased content of total proteins, based on the composition of SF (Figure 3B). ATR-FTIR data for the SF collected from patients with supplemented and PT procedures are presented in Figure 4.
The sugar bands in the domain 980 - 1140 cm−1 are less intense for patients supplemented, 5-10 min movement, with PT treatment (PT, 2 weeks) and finally SF sampling after 4 weeks of resting, comparing to no PT treatment (Figure 4A,B). These results indicate an important role of the PT on the interactions between the supplemented Kombihylan® product and SF: the supplementation gel, rich in HA, interact with synovial fluids and form a homogenous system without any separation and clustering, working as one phase synovial-like fluid [64]. The sugar absorption bands do not change as intensively in the case of keeping the patient at rest after supplementing with Kombihylan® and 5-10 min movement (Figure 4C,D) suggestion that ATR-FTIR spectroscopy could be used as primary screening method for evaluation the treatment evolution in the case of the patients with moderate KOA.
3.3. Rheological properties
The SF rheology influences the joints tribology either in healthy persons, or individuals with pathological background. For instance, there was demonstrating that the rheological behaviour of SF is changed at the appearance of arthritis or OA, exhibiting decreased viscoelasticity. The function of the joints is strongly related to the condition of the SF, especially with the proteins and HA organization and their interactions [65].
It was found that intra-articular injection of HA restores SF viscoelasticity at patients with KOA, and decreases cytokines with pro-inflammatory effect and the number of lining cells, lymphocytes and macrophages; an increased number of fibroblasts and the amount of collagen after the supplementation with HA gels was also observed [66,67].
In the present research the rheological properties were investigated for SF extracted from patients with moderate KOA, after application of different treatments: supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks res); patients supplemented 5-10 min movement and supplemented, 5-10 min movement, 6-week rest (Figure 5, Figure 6 and Figure 7). The research included rheological characterization of solutions of Kombihylan® as well as complete rheological characterization of SF, i.e., viscosity measurements, measurements of the elastic moduli (G)’, viscous moduli (G’’), and δ the ratio of the viscous modulus over the elastic modulus, and indicates the tendency of a fluid to dissipate energy (i.e., more viscous-like) or to store energy (i.e., more elastic-like)). All experiments have been performed in conditions simulating the biological environment (37°C).
The Kombihylan® product, shown in Figure 5A, exhibits the rheological behavior of a polymeric mixture based on low and high molecular weight polymers solution; across the frequency range demonstrate viscoelastic behavior with elastic response at low frequencies (G’>G”, based on CS and HA contribution to the elastic response) and viscous response at high frequencies (G”> G’, based on HA viscous response). The SF from the control group (moderate KOA, no supplementation or treatment) doesn’t present substantially different pattern on their viscoelastic properties. However, the G’ and G” values varied from a patient to another one, indicating that in OA many factors contribute to the variability of the rheological properties of SF, including the modification in inflammatory components, joint geometry, and pathology history. Alterations within the joint determine the properties of the SF to a larger extent. The values ranged from 0.1 Pa to 10 Pa, ten times less than the supplementation fluid based on HA and CS (Kombihylan®).
The G’ and G” of the SF from the patients supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks rest) are presented in Figure 5B,C. For all cases analyzed, G”>G’, as the result of the interactions between polysaccharides from Kombihylan® and components from biological SF, contributing to the viscous response. The values for elastic modulus increased, in some cases doubling up, indicating a uniform distribution of the HA hydrogel among the components of SF, process stimulated in the movement conditions. The lower elastic behavior of the SF, at the physiological shear rates, is evidence for an interaction of hyaluronate with proteins, especial lubricin, where lubricin decreases the degree of entropy of an otherwise stiffer molecule. An increase in the persistence length due to these interactions would stabilize the HA molecule that is likely to form entanglements. PT treatment contributed to a homogenous distributions and new organization of the proteins and polysaccharides into SF, stimulating stronger interactions and G’ and G” slightly decreased (Figure 5C); a higher contribution of the viscous modulus was noticed. The presence of lubricin and other glicoproteins helps synovial fluid to store and dissipate the energy of impact during normal walking gait, and assure the lubrication, together with other HA-binding proteins. In absence of PT(Figure 4D,E) the G’ and G” profiles are non-uniform in frequency sweep tests, suggesting a non-organized supplemented SF, with some clustering phenomena, multi-protein polymeric aggregates, and low level of entanglement between HA and macromolecular component in SF [68].
The PT effect is highlighted in the values of tan δ = G''/G', a measure of how elastic (tan δ < 1) or plastic (tan δ > 1) is the behavior of the tested SF (Figure 6), where tan δ represents the ratio of the viscous to elastic response of a viscoelastic gel or, in another words, the energy dissipation potential of the material.
The values for tan δ are positive for all tested SF, indicating a more elastic fluid then plastic one. Appling a load to the synovial gel, some part of the applied load is dissipated by the energy dissipation mechanisms (such as segmental motions) in the bulk of synovial polymeric network, and other part of the load is stored into polymeric component from SF and will be release upon removal of the load. The tan δ decreasing indicates that the biological gel acts more elastic now and by applying a load, it has more potential to store the load rather than dissipating it; the effect is more pronounced in SF after PT (Figure 6C). The tan δ increasing is associated with more energy dissipation potential in supplemented SF, and it is produced in one case with PT; such behavior is attributed to the presences of intense inflammatory processes that change the synovial proteins interactions with HA.
The application of a constant shear stress on the samples was performed in order to evaluate the time needed for the SF (control and supplemented) to adjust its response to the stress conditions (Figure 7). In general, the viscosity of OA SF is lower compared to healthy SF, attributed to a structural rearrangement of the HA chains, and low molecular weight proteins (e.g., albumin), which significantly contribute to this distribution [69].
The SF presents a time-dependent viscosity effect being considered a thixotropic fluid, and the behavior is emphasized in OA [70]. The supplementation with Kombihylan® determines the increase in viscosity (Figure 7B) but a large variability is present based on patient specificity. Hyaluronan from the supplementation gel could, by its osmotic contributions and formation of flow barriers in the limiting layers, be a regulator of the SF. The time-dependency decreases after PT when, in the share rate test condition, the viscosity reaches constant values (Figure 7C, P1, P3). The supplementation with no mobilization procedure determined a sharp decline of the viscosity in the first’s moments of application of the mechanical loading (Figure 7E). In choosing a combination of treatments that involve lubricants the viscosity should be high enough to provide a continuous fluid film in the contact area, but not too high so as to create friction due to viscous shear. The knee involves low speeds and high loads, and higher viscosity is recommended [71]. Furthermore, the synovial membrane that separates SF from plasma allows small globular proteins (albumin and globulins) to freely interchange between blood and SF and the process is more intense in rheumatoid arthritis. For such patients simultaneously higher albumin concentration was found in their SF and a smaller than normal albumin concentration in their plasma [72].
3.4. Filmogen characteristics and bioadhesive properties
Microscope images of human SF dried drops at low magnification show a heterogeneous deposit (Figure 8).
The supplementation fluid (Kombihylan®) - based film presents a uniform aspect with no cracks and separation. Contrariwise, the SF-based films present two main regions: glassy film with some separation areas at the drop edge and fern-shaped crystalline deposit in the drop center [64]. The crystalline area is more pronounced in SF from patient supplemented, 5-10 min movement (P1 and P5) and is correlated with primary interactions of the supplementation component with proteins and glycoproteins from SF. The application of PT procedure diminished the clustering tendency, a uniform center was resulted and a diffusive border between glassy part and the core area. Such results indicate an integral distribution of the supplementation fluid after PT treatment.
In vitro bioadhesion studies on SF-based films were performed using simulating membrane (cellulose membrane) and a TA.XT Plus texture analyzer. The force required for detachment of the film from the biological membrane was recorded and the high values of the detachment forces indicate strong interactions. Maximum force of detachment and work of adhesion are presented in Figure 9 and Figure 10.
The bioadhesion tests express the composition and interactions in SFs, especial for the polymeric networks and their changes in pathological conditions, composition of the administrated supplementation gels and additional procedures that contribute to the proteins, polysaccharides and glycoproteins interfusion. Proteins and polysaccharides, containing hydrophilic networks with numerous functional polar groups (such as -COOH, -OH, -NH2 and -SO4), which are bioadhesion inducers [73]. It must be taken into account that electrostatic forces, namely, ionic interaction, van der Waal’s forces and hydrogen bonds also contribute to the adhesion process [74,75]. The functional groups, chain length, degree of hydration, concentration, charge, are characteristics that may influence the bioadhesive nature of the protein and polysaccharides [76]. Lubricin is composed of a central mucin domain flanked by globular N- and C-termini, somatomedin B-like domain and hemopexin-like domain. The mucin is an attraction area for the bioadhesive proteins (albumin) or polysaccharide (HA, CS) and their interactions contribute in a joint to the lubrication process [53].
In the performed tests on simulating membranes and cartilage, high values of the maximum force of detachment and work of adhesion were registered for Kombihylan® supplementation product. Component polymers, HA and CS are bioadhesive and have the ability to bind on the cartilage surface and to contribute to the lubrication process. The SF from the control group presents lower values for the registered bioadhesion parameters, suggesting a variety of interactions between polymeric components with less possibilities of distribution onto articular cartilage. The supplementation with Kombihylan® improves the bioadhesion properties of the SF and PT is favorable for the macromolecules distribution and bioadhesion, with potential in increasing the lubrication characteristics. During motion, in OA joint the SF enters and convers the gaps on the cartilage, and the pressure increase as the gap converges; a hydrodynamic lift and forces the surfaces apart like a wedge are created. The thickness of the film formed by the fluid should be slightly greater than the surface roughness in order to minimize asperity contact. Kombihylan® works in synergy with lubricin, while PT contributes to the supplementation fluid distribution and finally improves the SF spreading onto textured cartilage surface.
4. Conclusions
In this study, synovial fluids collected from moderate OA knees were analysed in order to evaluate combined therapy with hyaluronic acid – based supplementation gel (Kombihylan®) and PT. Several changes in SF characteristics (pH normalisation, glucose concentration) were identified and the PT role on the interactions between the supplemented Kombihylan® product and synovial fluid was pointed out. PT treatment contributed to a homogenous distributions and new organization of the proteins and polysaccharides into synovial fluid, translated in higher contribution of the viscous modulus to the viscoelastic rheological behavior. The SF presents a time-dependent viscosity with behavior of thixotropic fluid, and dependency decreases after PT when, in the share rate test condition, the viscosity became constant. HA and CS improve bioadhesive properties of the SF and PT is favorable for the macromolecules distribution and bioadhesion, contributing to the lubrication process. We showed that PT plays a key role in the non-surgical treatment of KOA, effectively controlling the SF composition, biorheology, glycoproteins distribution and the lubrication process with positive effect on the patients.
Author Contributions
Conceptualization, I.O., D.V.M, A.I.G. and L.S.; methodology, I.O., R.G. and L.V.; software, I.O., A.T. and L.V.; validation, I.O., R.G., I.B., D.V.M., L.V., D.C, L.S., A.I.G; formal analysis, I.O., R.G. I.N., F.D.C., L.V., D.V.M.; investigation, I.O., I.B., R.G., I.N., F.D.C., A.T., D.A.I, L.V.; resources, I.O.,D.A.I; data curation, I.O., R.G. I.N., F.D.C., A.T., D.A.I, L.V., D.C., A.I.G, L.S.; writing—original draft preparation, I.O., R.G., L.V., A.I.G, L.S.; writing—review and editing, I.O., R.G. D.V.M, L.V., D.C., A.I.G, L.S.; visualization, I.O., R.G., I.N., F.D.C., A.T., D.V.M., D.A.I, L.V., A.I.G, L.S.; supervision, D.C., A.I.G, L.S.; project administration, I.O., R.G., A.I.G, L.S.; funding acquisition, I.O., D.A.I., A.I.G. All authors have read and agreed to the published version of the manuscript.
Funding
The work of Daniel Andrei Iordan was supported by the project "PRO-INVENT", Contract no. 62487/03.06.2022 - POCU/993/6/13 - Code 153299, financed by The Human Capital Operational Programme 2014–2020 (POCU), Romania.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Micromedica Medical Clinic with no. 32/28 January 2020.
Informed Consent Statement
Informed consent was obtained from all subjects that were involved in the study.
Data Availability Statement
Data are contained within the main text of the article.
Acknowledgments
The work of Daniel Andrei Iordan was supported by the project "PRO-INVENT", Contract no. 62487/03.06.2022 - POCU/993/6/13 - Code 153299, financed by The Human Capital Operational Programme 2014–2020 (POCU), Romania.
Conflicts of Interest
The authors declare no conflict of interest.
Sample Availability
Samples of the synovial fluid are available from the Robert Gherghel and Ilie Onu.
References
- Eakin, G.S., Amodeo, K.L., Kahlon, R.S. Arthritis and its Public Health Burden. Dela J Public Health, 2017, 22(3), 36-44. https://doi.org/10.32481/djph.2017.03.006. [CrossRef]
- Song, P., Cui, Z., Hu, L. Applications and prospects of intra-articular drug delivery system in arthritis therapeutics. Journal of Controlled Release, 2022, 352, 946-960. https://doi.org/10.1016/j.jconrel.2022.11.018. [CrossRef]
- Andreev, D., Kachler, K., Schett, G., Bozec, A. Rheumatoid arthritis and osteoimmunology: The adverse impact of a deregulated immune system on bone metabolism. Bone, 2022, 162, 116468. https://doi.org/10.1016/j.bone.2022.116468. [CrossRef]
- Dinesh, Kumar, L., Karthik, R., Gayathri, N., Sivasudha, T. Advancement in contemporary diagnostic and therapeutic approaches for rheumatoid arthritis. Biomedicine & Pharmacotherapy, 2016, 79, 52-61. https://doi.org/10.1016/j.biopha.2016.02.001. [CrossRef]
- Loeser, R.F., Goldring, S.R., Scanzello, C.R., Goldring, M.B. Osteoarthritis: a disease of the joint as an organ. Arthritis Rheum, 2012 64(6), 1697-707. https://doi.org/10.1002/art.34453. [CrossRef]
- Lei, Y., Wang, X., Liao, J., Shen, J., Li, Y., Cai, Z., et al. Shear-responsive boundary-lubricated hydrogels attenuate osteoarthritis. Bioact, 2022, 16, 472–484. https://doi.org/10.1016/j.bioactmat.2022.02.016. [CrossRef]
- Rothammer, B., Marian, M., Rummel, F., Schroeder, S., Uhler, M., Kretzer, J.P., Tremmel, S., Wartzack, S., Rheological behavior of an artificial synovial fluid – influence of temperature, shear rate and pressure. Journal of the Mechanical Behavior of Biomedical Materials, 2021, 115, 104278. https://doi.org/10.1016/j.jmbbm.2020.104278. [CrossRef]
- Kujath, P., Michelsen, A. Wounds - from physiology to wound dressing. Dtsch Arztebl Int, 2008, 105(13), 239-48. https://doi.org/10.3238/arztebl.2008.0239. [CrossRef]
- Kobayashi, T.; Chanmee, T.; Itano, N. Hyaluronan: Metabolism and Function. Biomolecules 2020, 10, 1525. https://doi.org/10.3390/biom10111525. [CrossRef]
- McNary, S.M., Athanasiou, K.A., Reddi, A.H. Engineering lubrication in articular cartilage. Tissue Eng Part B Rev. 2012, 18(2), 88-100. https://doi.org/10.1089/ten.TEB.2011.0394. [CrossRef]
- Bhuanantanondh, P. Rheological study of viscosupplements and synovial fluid in patients with osteoarthritis, J. Med. Biol. Eng, 2012, 32(1), 12. https://doi.org/10.5405/jmbe.834. [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. https://doi.org/10.1016/j.joca.2019.06.011. [CrossRef]
- Chae, K.J.; Choi, M.J.; Kim, K.Y.; Ajayi, F.F.; Chang, I.S.; Kim, I.S. Osteoarthritis: Careand Management: Clinical Guideline; National Institute for Health and Care, 2014, Available online: https://www.nice.org (accessed on 1 March 2022).
- Onu, I.; Matei, D.; Sardaru, D.-P.; Cascaval, D.; Onu, A.; Gherghel, R.; Serban, I.L.; Mocanu, G.D.; Iordan, D.A.; Murariu, G.; et al. Rehabilitation of Patients with Moderate Knee Osteoarthritis Using Hyaluronic Acid Viscosupplementation and Physiotherapy. Appl. Sci. 2022, 12, 3165. https://doi.org/10.3390/ app12063165. [CrossRef]
- Johnson, M. Transcutaneous Electrical Nerve Stimulation: Mechanisms, Clinical Application and Evidence. Rev Pain. 2007, 1(1),7-11. https://doi.org/10.1177/204946370700100103. [CrossRef]
- Wu, Q.; Henry, JL. Changes in Abeta non-nociceptive primary sensory neurons in a rat model of osteoarthritis pain. Mol Pain. 2010, 6:37. https://doi.org/10.1186/1744-8069-6-37. [CrossRef]
- Iijima, H.; Eguchi, R.; Shimoura, K.; Yamada, K.; Aoyama, T.; Takahashi, M. Transcutaneous Electrical Nerve Stimulation Improves Stair Climbing Capacity in People with Knee Osteoarthritis. Sci. Rep. 2020, 10, 7294. https://doi.org/10.1038/s41598-020-64176-0. [CrossRef]
- Cherian, J.J.; Harrison, P.E.; Benjamin, S.A.; Bhave, A.; Harwin, S.F.; Mont, M.A. Do the Effects of Transcutaneous Electrical Nerve Stimulation on Knee Osteoarthritis Pain and Function Last? J. Knee Surg. 2016, 29, 497–501. https://doi.org/10.1055/s-0035-1566735. [CrossRef]
- Do Carmo Almeida, T.C.; Dos Santos Figueiredo, F.W.; Barbosa Filho, V.C.; de Abreu, L.C.; Fonseca, F.L.A.; Adami, F. Effects of Transcutaneous Electrical Nerve Stimulation on Proinflammatory Cytokines: Systematic Review and Meta-Analysis. Mediat. Inflamm. 2018, 1094352. https://doi.org/10.1155/2018/1094352. [CrossRef]
- Tábata Cristina do Carmo Almeida, et. al "Reduction on Proinflammatory Cytokines after Application of Transcutaneous Electrical Nerve Stimulation (TENS) in Patients with a Breast Cancer: A Nonrandomized, Open, and Single-Arm Study Protocol with Paired Analysis", Mediators of Inflammation, 2022, 8. https://doi.org/10.1155/2022/1350813. [CrossRef]
- Johns LD. Nonthermal effects of therapeutic ultrasound: the frequency resonance hypothesis. J Athl Train. 2002, 37(3), 293-299.
- Paliwal, S.; Mitragotri, S. Therapeutic Opportunities in Biological Responses of Ultrasound. Ultrasonics, 2008, 48, 271–278. https://doi.org/10.1016/j.ultras.2008.02.002. [CrossRef]
- Schumann, D.; Kujat, R.; Zellner, J.; Angele, M.K.; Nerlich, M.; Mayr, E.; Angele, P. Treatment of Human Mesenchymal Stem Cellswith Pulsed Low Intensity Ultrasound Enhances the Chondrogenic Phenotype In Vitro. Biorheology, 2006, 43, 431–443.
- Rothenberg, J.B.; Jayaram, P.; Naqvi, U.; Gober, J.; Malanga, G.A. The Role of Low-Intensity Pulsed Ultrasound on Cartilage Healing in Knee Osteoarthritis: A Review. PM&R, 2017, 9, 1268–1277. https://doi.org/10.1016/j.pmrj.2017.05.008. [CrossRef]
- De Oliveira Perrucini, P.D.; Poli-Frederico, R.C.; de Almeida Pires-Oliveira, D.A.; Dragonetti Bertin, L.; Beltrão Pires, F.; Shimoya- Bittencourt, W.; Martins Santos, V.; Medeiros Coelho, J.; Franco de Oliveira, R. Anti-Inflammatory and Healing Effects of Pulsed Ultrasound Therapy on Fibroblasts. Am. J. Phys. Med. Rehabilit. 2019, 99, 19–25. https://doi.org/10.1097/PHM.0000000000001265. [CrossRef]
- Smoot, B.; Chiavola-Larson, L.; Lee, J.; Manibusan, H.; Allen, D.D. Effect of Low-Level Laser Therapy on Pain and Swelling in Women with Breast Cancer-Related Lymphedema: A Systematic Review and Meta-Analysis. J. Cancer Surviv. 2015, 9, 287–304. https://doi.org/10.1007/s11764-014-0411-1. [CrossRef]
- Hegedus, B.; Viharos, L.; Gervain, M.; Gálfi, M. The Effect of Low-Level Laser in Knee Osteoarthritis: A Double-Blind, Randomized, Placebo-Controlled Trial. Photomed. Laser Surg. 2009, 27, 577–584. https://doi.org/10.1089/pho.2008.2297. [CrossRef]
- Rothenberg, J.B.; Jayaram, P.; Naqvi, U.; Gober, J.; Malanga, G.A. The Role of Low-Intensity Pulsed Ultrasound on Cartilage Healing in Knee Osteoarthritis: A Review. PM&R 2017, 9, 1268–1277. https://doi.org/10.1016/j.pmrj.2017.05.008. [CrossRef]
- Stausholm, MB.; Naterstad, IF.; Joensen, J. et al. Efficacy of low-level laser therapy on pain and disability in knee osteoarthritis: systematic review and meta-analysis of randomised placebo-controlled trials. BMJ Open. 2019, 9,10,031142. https://doi.org/10.1136/bmjopen-2019-031142. [CrossRef]
- Barbosa, G.M.; Cunha, J.E.; Cunha, T.M.; Martinho, L.B.; Castro, P.A.T.S.; Oliveira, F.F.B.; Cunha, F.Q.; Ramalho, F.S.; Salvini, T.F. Clinical-like Cryotherapy Improves Footprint Patterns and Reduces Synovial Inflammation in a Rat Model of Post-Traumatic Knee Osteoarthritis. Sci. Rep. 2019, 9, 14518. doi.org/10.1038/s41598-019-50958-8.
- Garcia, C.; Karri, J.; Zacharias, NA.; Abd-Elsayed, A. Use of Cryotherapy for Managing Chronic Pain: An Evidence-Based Narrative. Pain Ther. 2021 10(1),81-100. https://doi.org/10.1007/s40122-020-00225-w. [CrossRef]
- Dantas, L.O.; Jorge, A.E.; Regina Mendes da Silva Serrão, P.; Aburquerque-Sendín, F.; de Fatima Salvini, T. Cryotherapy Associated with Tailored Land-Based Exercises for Knee Osteoarthritis: A Protocol for a Double-Blind Sham-Controlled Randomised Trial. BMJ. 2020, 10, e035610. https://doi.org/10.1136/bmjopen-2019-035610. [CrossRef]
- Ziemann, E.; Olek, RA.; Kujach, S., et al. Five-day whole-body cryostimulation, blood inflammatory markers, and performance in high-ranking professional tennis players. J Athl Train. 2012, 47, 664–672. https://doi.org/10.4085/1062-6050-47.6.13. [CrossRef]
- Jastrząbek, R.; Straburzyńska-Lupa, A.; Rutkowski, R.; Romanowski, W. Effects of different local cryotherapies on systemic levels of TNF-α, IL-6, and clinical parameters in active rheumatoid arthritis. Rheumatol Int. 2013, 33, 2053–2060. https://doi.org/10.1007/s00296-013-2692-5. [CrossRef]
- Lubkowska, A.; Szyguła, Z.; Chlubek, D.; Banfi, G. The effect of prolonged whole-body cryostimulation treatment with different amounts of sessions on chosen pro-and anti-inflammatory cytokines levels in healthy men. Scand J Clin Lab Invest. 2011, 71, 419–425. https://doi.org/10.3109/00365513.2011.580859. [CrossRef]
- Brophy, Robert H. MD; Fillingham, Yale A. MD. AAOS Clinical Practice Guideline Summary: Management of Osteoarthritis of the Knee (Nonarthroplasty), Third Edition. Journal of the American Academy of Orthopaedic Surgeons, 2022, 30(9), e721-e729. https://doi.org/10.5435/JAAOS-D-21-01233. [CrossRef]
- American College of Rheumatology Subcommittee on Osteoarthritis Guidelines. Recommendations for the medical management of osteoarthritis of the hip and knee: 2000 update. Arthritis Rheum. 2000, 43(9), 1905–15.
- Pendleton, A.; Arden, N.; Dougados, M.; Doherty, M.; Bannwarth, B.; Bijlsma, JW., et al. EULAR recommendations for the management of knee osteoarthritis: report of a task force of the Standing Committee for International Clinical Studies Including Therapeutic Trials (ESCISIT) Ann Rheum Dis. 2000, 59(12), 936–44. https://doi.org/10.1136/ard.59.12.936. [CrossRef]
- Bosomworth, NJ. Exercise and knee osteoarthritis: benefit or hazard? Can Fam Physician. 2009, 55(9),871-8.
- Li, Y.; Su, Y.; Chen, S.; Zhang, Y.; Zhang, Z.; Liu, C.; et al. The effects of resistance exercise in patients with knee osteoarthritis: a systematic review and meta-analysis. Clin. Rehabil. 2016, 30, 947–959. https://doi.org/10.1177/0269215515610039. [CrossRef]
- DeVita, P.; Aaboe, J.; Bartholdy, C.; Leonardis, J. M.; Bliddal, H.; and Henriksen, M. Quadriceps-strengthening exercise and quadriceps and knee biomechanics during walking in knee osteoarthritis: A two-Centre randomized controlled trial. Clin. Biomech. 2018, 59, 199–206. https://doi.org/10.1016/j.clinbiomech.2018.09.016. [CrossRef]
- Chen, H.; Zheng, X.; Huang, H.; Liu, C.; Wan, Q.; and Shang, S. The effects of a home-based exercise intervention on elderly patients with knee osteoarthritis: a quasi-experimental study. BMC Musculoskelet. Disord. 2019, 20,160. https://doi.org/10.1186/s12891-019-2521-4. [CrossRef]
- Samut, G.; Dincer, F.; and Ozdemir, O. The effect of isokinetic and aerobic exercises on serum interleukin-6 and tumor necrosis factor alpha levels, pain, and functional activity in patients with knee osteoarthritis. Mod. Rheumatol. 2015, 25, 919–924. https://doi.org/10.3109/14397595.2015.1038425. [CrossRef]
- Miyaguchi, M.; Kobayashi, A.; Kadoya, Y.; Ohashi, H.; Yamano, Y. and Takaoka, K. Biochemical change in joint fluid after isometric quadriceps exercise for patients with osteoarthritis of the knee. Osteoarthr. Cartil. 2003, 11, 252–259. https://doi.org/10.1016/S1063-4584(02)00372-2. [CrossRef]
- Garg, T., Goyal, A.K. Biomaterial-based scaffolds– current status and future directions. Expert. Opin. Drug. Deliv, 2014, 11, 767-789. https://doi.org/10.1517/17425247.2014.891014. [CrossRef]
- Brako, F., Thorogate, R., Mahalingam, S., Abraham, B.R., Craig, DQM., Edirisinghe, M. Mucoadhesion of Progesterone-Loaded Drug Delivery Nanofiber Constructs. ACS Appl Mater Interfaces, 2018, 10, 13381-13389. https://doi.org/10.1021/acsami.8b03329. [CrossRef]
- Tamer, T.M., Hyaluronan and synovial joint: function, distribution and healing. Interdiscip Toxicol. 2013, 6(3), 111-25. https://doi.org/10.2478/intox-2013-0019. [CrossRef]
- Li, Y.; Yuan, Z.; Yang, H.; Zhong, H.; Peng, W.; Xie, R. Recent Advances in Understanding the Role of Cartilage Lubrication in Osteoarthritis. Molecules 2021, 26, 6122. https://doi.org/10.3390/molecules26206122. [CrossRef]
- Ucm. R., Aem. M., Lhb. Z., Kumar, V., Taherzadeh, M.J., Garlapati, V.K., Chandel A.K. Comprehensive review on biotechnological production of hyaluronic acid: status, innovation, market and applications. Bioengineered, 2022, 13(4), 9645-9661. https://doi.org/10.1080/21655979.2022.2057760. [CrossRef]
- Bayer, I.S. Hyaluronic Acid and Controlled Release: A Review. Molecules 2020, 25, 2649. Doi: 3390/molecules25112649. [CrossRef]
- Prekasan, D., Saju, K.K., Review of the tribological characteristics of synovial fluid. Procedia Technology, 2016, 25, 1170 – 1174. https://doi.org/10.1016/j.protcy.2016.08.235. [CrossRef]
- Bennike, T., Ayturk, U., Haslauer, C.M., Froehlich, J.W., Proffen, B.L., Barnaby, O., Birkelund, S., Murray, M.M., Warman, M.L., Stensballe, A. and Steen, H. A normative study of the synovial fluid proteome from healthy porcine knee joints. J Proteome Res, 2014, 13(10), 4377-87. https://doi.org/10.1021/pr500587x. [CrossRef]
- Jay, G.D., Waller, K.A. The biology of lubricin: near frictionless joint motion. Matrix Biol, 2014, 39, 17-24. https://doi.org/10.1016/j.matbio.2014.08.008. [CrossRef]
- Bayer, I.S. Advances in Tribology of Lubricin and Lubricin-Like Synthetic Polymer Nanostructures. Lubricants 2018, 6, 30. https://doi.org/10.3390/lubricants6020030. [CrossRef]
- Stamm, J., Weißelberg, S., Both, A., Failla, A.V., Nordholt, G., Büttner, H., Linder, S., Aepfelbacher, M., Rohde, H.. Development of an artificial synovial fluid useful for studying Staphylococcus epidermidis joint infections. Front Cell Infect Microbiol. 2022, 29;12:948151. https://doi.org/10.3389/fcimb.2022.948151. [CrossRef]
- Konttinen, Y.T., Mandelin, J., Li, T.F., Salo, J., Lassus, J., Liljestrom, M., Hukkanen, M., Takagi, M., Virtanen, I., Santavirta, S. Acidic cysteine endoproteinase cathepsin K in the degeneration of the superficial articular hyaline cartilage in osteoarthritis. Arthritis Rheum. 2002, 46:953–960. https://doi.org/10.1002/art.10185. [CrossRef]
- Lombardi, A.F., Ma, Y., Jang, H., Jerban, S., Tang, Q., Searleman, A.C., Meyer, R.S., Du, J., Chang, E.Y. AcidoCEST-UTE MRI Reveals an Acidic Microenvironment in Knee Osteoarthritis. Int J Mol Sci., 2022, 18;23(8):4466. https://doi.org/10.3390/ijms23084466. [CrossRef]
- Zhai, G. Alteration of Metabolic Pathways in Osteoarthritis. Metabolites. 2019, 9, 9(1):11. https://doi.org/10.3390/metabo9010011. [CrossRef]
- Malek, S., Marini, F., McClure, J.T. Evaluation of longterm storage on infrared spectral patterns of serum and synovial fluid of dogs with knee, Osteoarthritis. Osteoarthritis and Cartilage, 2022, 30, S81-S438. https://doi.org/10.1016/j.joca.2022.02.135. [CrossRef]
- Das Gupta, S., Shrestha, P., Ali, N., Turkiewicz, A., Hughes, V., Jonsson, E., Tjornstand, J., Neuman, P., €Onnerfjord, P., Rieppo, L., Englund, M., Saarakkala, S. Infrared spectroscopy can detect end-stage steoarthritis from human synovial fluid: a pilot study. Osteoarthritis and Cartilage, 2022, 30, S81-S438. https://doi.org/10.1016/j.joca.2022.02.135. [CrossRef]
- Leone, G., Consumi, M., Lamponi, S., Magnani, A. New hyaluronan derivative with prolonged half-life for ophthalmic formulation. Carbohydrate Polymers, 2012, 88. https://doi.org/10.1016/j.carbpol.2011.12.047. [CrossRef]
- Carole, E. Schante., Zuber, G., Herlin, C., Vandamme, T.F. Chemical modifications of hyaluronic acid for the synthesis of derivatives for a broad range of biomedical application, Carbohydrate Polymers, 2011, 85(3), 469-489. https://doi.org/10.1016/j.carbpol.2011.03.019. [CrossRef]
- Alberto-Silva, C., Malheiros, F.B.M. & Querobino, S.M. Fourier-transformed infrared spectroscopy, physicochemical and biochemical properties of chondroitin sulfate and glucosamine as supporting information on quality control of raw materials. Futur J Pharm Sci, 2020, 6, 98. https://doi.org/10.1186/s43094-020-00120-3. [CrossRef]
- Esmonde-White, K.A., Mandair, G.S., Raaii, F., Jacobson, J.A., Miller, B.S., Urquhart, A.G., Roessler, B.J., Morris, M.D. Raman spectroscopy of synovial fluid as a tool for diagnosing osteoarthritis. J Biomed Opt, 2009, 14(3), 034013. https://doi.org/10.1117/1.3130338. [CrossRef]
- Wang, X., Hunter, D.J., Jin, X., Ding, C. The importance of synovial inflammation in osteoarthritis: current evidence from imaging assessments and clinical trials. Osteoarthritis and Cartilage, 2018, 26(2), 65-174. https://doi.org/10.1016/j.joca.2017.11.015. [CrossRef]
- Vincent, H.K., Percival, S.S., Conrad, B.P., Seay, A.N., Montero, C., Vincent, K.R. Hyaluronic Acid (HA) Viscosupplementation on Synovial Fluid Inflammation in Knee Osteoarthritis: A Pilot Study. Open Orthop J, 2013, 20, 7, 378-84. https://doi.org/10.2174/1874325001307010378. [CrossRef]
- Schumacher, H.R., Paul, C., Hitchon, C.A., El-Gabalawy, H., Zonay, L., Clayburne, G., Sieck, M., Schwab, E. Hyaluronate effects on synovium and synovial fluid. A prospective blinded study in patients with osteoarthritis of the knee. Osteoarthritis Cartilage, 2006, 14(5), 501-3. https://doi.org/10.1016/j.joca.2005.11.013. [CrossRef]
- Neville, A., Morina, A., Liskiewicz, T. and Yan, Y. Synovial joint lubrication – does nature teach more effective engineering lubrication strategies? Proceedings of the Institution of Mechanical Engineers, Part C: Journal of Mechanical Engineering Science, 2007, 221(10), 1223-1230. ISSN 0954-4062, doi: 0.1243/09544062JMES72. [CrossRef]
- Nicholls, M., Manjoo, A., Shaw, P., Niazi, F., Rosen, J. A Comparison Between Rheological Properties of Intra-articular Hyaluronic Acid Preparations and Reported Human Synovial Fluid. Adv Ther, 2018, 35(4), 523-530. https://doi.org/10.1007/s12325-018-0688-y. [CrossRef]
- Hlavácek, M. The thixotropic effect of the synovial fluid in squeeze-film lubrication of the human hip joint. Biorheology, 2001, 38(4), 319-34.
- Logerstedt, D.S., Ebert, J.R., MacLeod, T.D., Heiderscheit, B.C., Gabbett, T.J., Eckenrode, B.J. Effects of and Response to Mechanical Loading on the Knee. Sports Med, 2022, 52(2), 201-235. https://doi.org/10.1007/s40279-021-01579-7. [CrossRef]
- Balakrishnan, L., Bhattacharjee, M., Ahmad, S. et al. Differential proteomic analysis of synovial fluid from rheumatoid arthritis and osteoarthritis patients. Clin Proteom, 2014, 11(1). https://doi.org/10.1186/1559-0275-11-1. [CrossRef]
- Yermak, I.M., Davydova, V.N., Volod’ko, A.V. Mucoadhesive Marine Polysaccharides, Mar. Drugs, 2022, 20(522). https://doi.org/10.3390/md20080522. [CrossRef]
- Suchaoin, W., Bonengel, S., Griessinger, J.A., Pereira de Sousa, I., Hussain, S., Huck, C.W., Bernkop-Schnürch, A. Novel bioadhesive polymers as intra-articular agents: Chondroitin sulfate-cysteine conjugates. Eur J Pharm Biopharm, 2016, 101, 25-32. https://doi.org/10.1016/j.ejpb.2016.01.006. [CrossRef]
- Bernkop-Schnürch, A., Greimel, A. Thiomers. American J. Drug Deliv, 2005, 3, 141-154. doi.org/10.2165/ 00137696-200503030-00001.
- Smart, J.D. The basics and underlying mechanisms of mucoadhesion. Adv. Drug. Deliv. Rev, 2005, 57, 1556–1568. https://doi.org/10.1016/j.addr.2005.07.001. [CrossRef]
Figure 1.
Synovial fluid (SF) macromolecular composition.
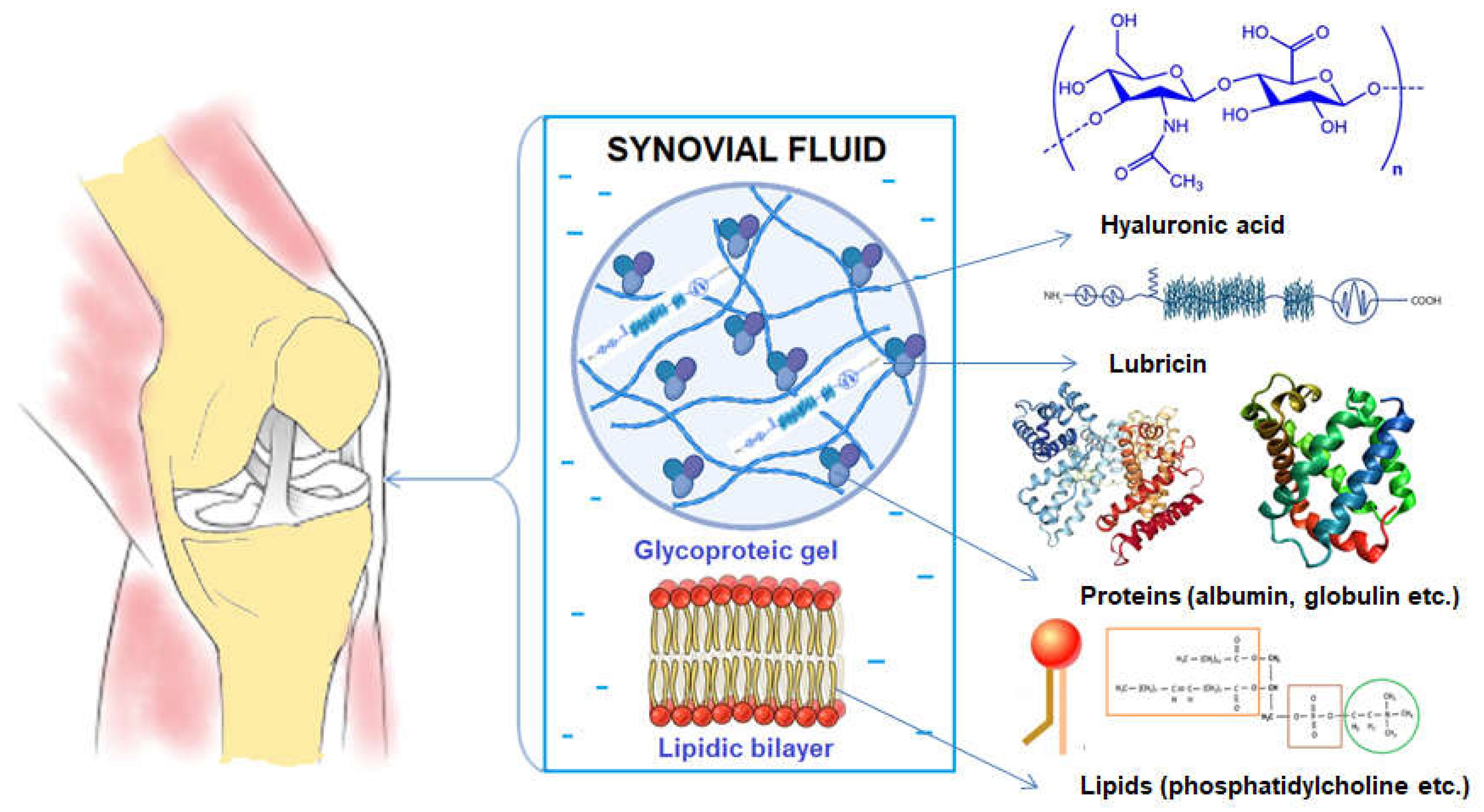
Figure 2.
Value of pH for Kombihylan® and synovial fluids (SF) from Control group, Group A (supplemented, 5-10 min movement), Group B - after PT (2 weeks PT + 4 weeks rest), Group C (supplemented, 5-10 min movement) and Group D (supplemented, 5-10 min movement, 6 weeks rest). Each value represents the mean ± standard error mean (n = 3) (* p < 0.05, ** p < 0.01).
Figure 2.
Value of pH for Kombihylan® and synovial fluids (SF) from Control group, Group A (supplemented, 5-10 min movement), Group B - after PT (2 weeks PT + 4 weeks rest), Group C (supplemented, 5-10 min movement) and Group D (supplemented, 5-10 min movement, 6 weeks rest). Each value represents the mean ± standard error mean (n = 3) (* p < 0.05, ** p < 0.01).
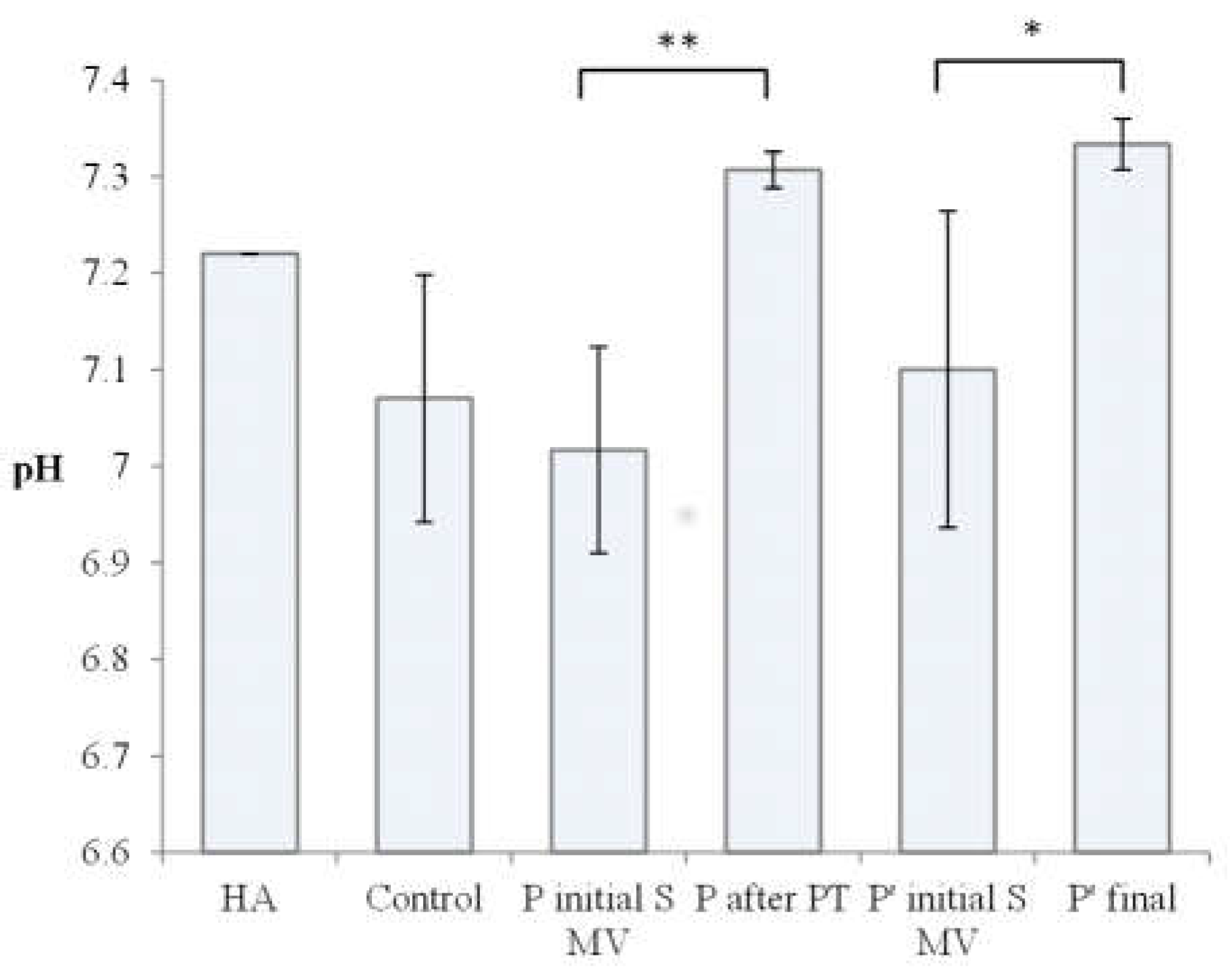
Figure 3.
ATR-FTIR spectra for hyaluronic Acid (HA), Chondroitin sulphate (CS), Kombihylan®, and synovial fluid (SF) collected from the Control Group (CG).
Figure 3.
ATR-FTIR spectra for hyaluronic Acid (HA), Chondroitin sulphate (CS), Kombihylan®, and synovial fluid (SF) collected from the Control Group (CG).
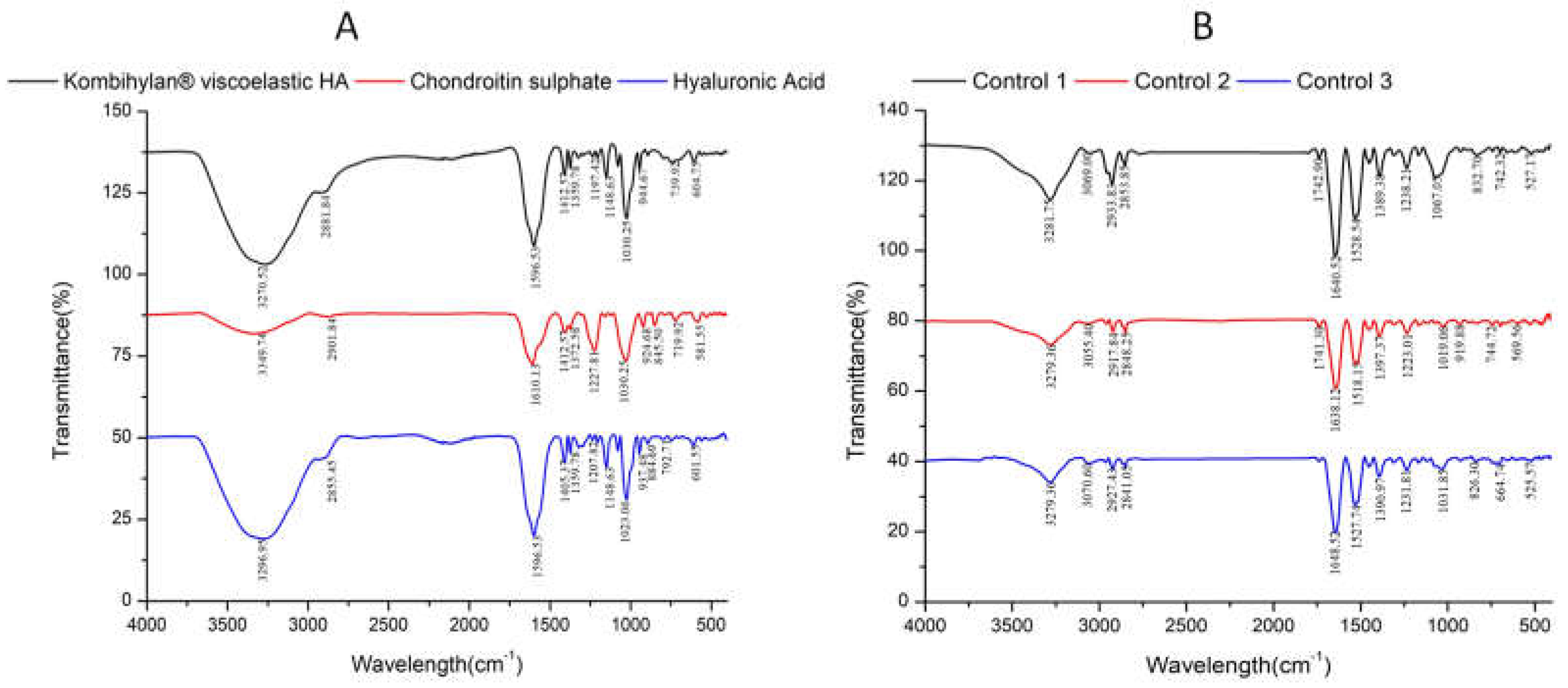
Figure 4.
ATR-FTIR spectra for synovial fluid (SF) collected from patients: Group A (supplemented, 5-10 min movement), Group B - after PT (2 weeks PT + 4 weeks rest), Group C (supplemented, 5-10 min movement) and Group D (supplemented, 5-10 min movement, 6 weeks rest).
Figure 4.
ATR-FTIR spectra for synovial fluid (SF) collected from patients: Group A (supplemented, 5-10 min movement), Group B - after PT (2 weeks PT + 4 weeks rest), Group C (supplemented, 5-10 min movement) and Group D (supplemented, 5-10 min movement, 6 weeks rest).
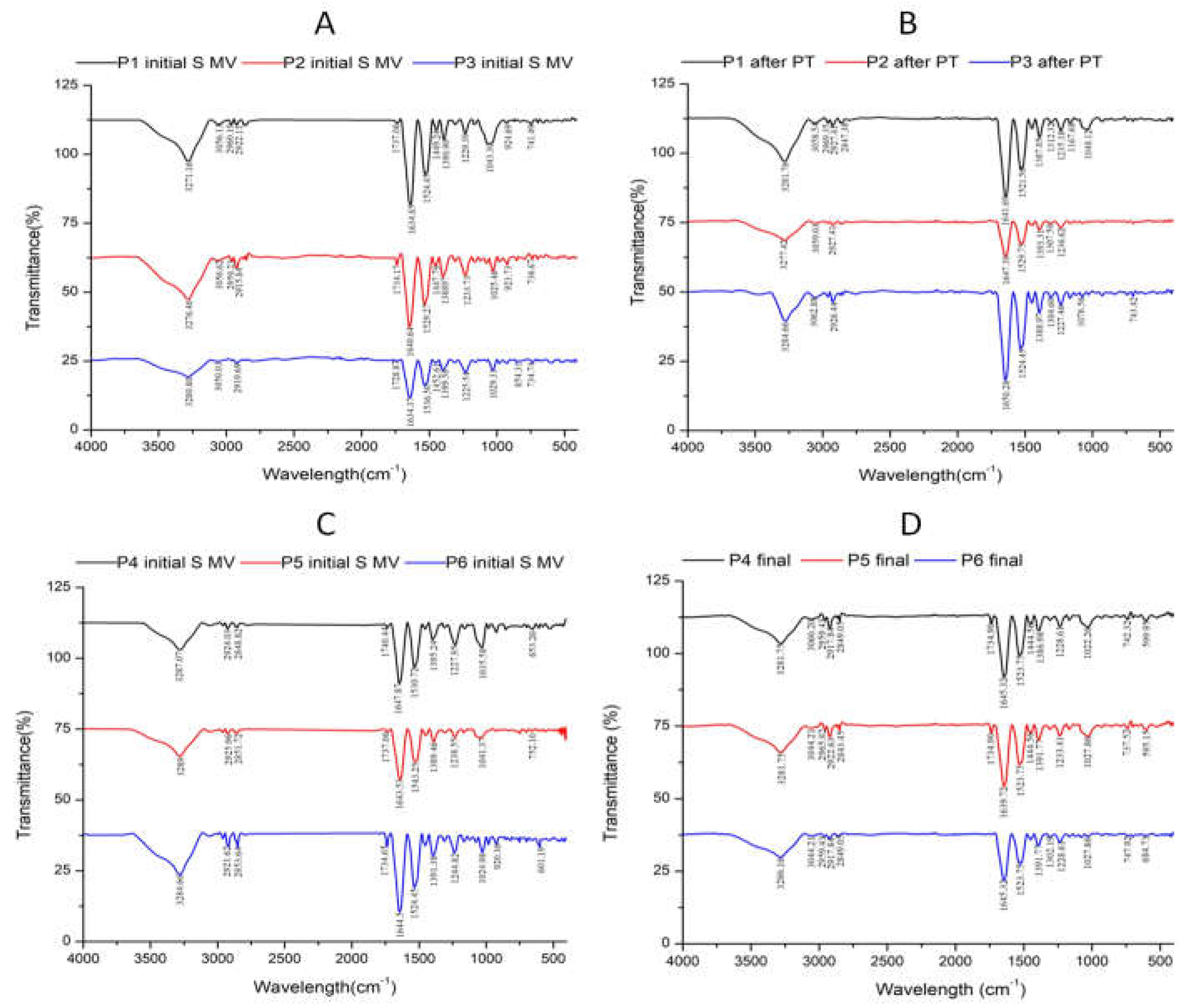
Figure 5.
Elastic (G') and viscous (G") moduli for synovial fluid (SF) collected from: control group (CG) and Kombihylan® product (A); patients supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks rest) (B and C); patients supplemented, 5-10 min movement and supplemented, 5-10 min movement, 6 weeks rest (D and E).
Figure 5.
Elastic (G') and viscous (G") moduli for synovial fluid (SF) collected from: control group (CG) and Kombihylan® product (A); patients supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks rest) (B and C); patients supplemented, 5-10 min movement and supplemented, 5-10 min movement, 6 weeks rest (D and E).
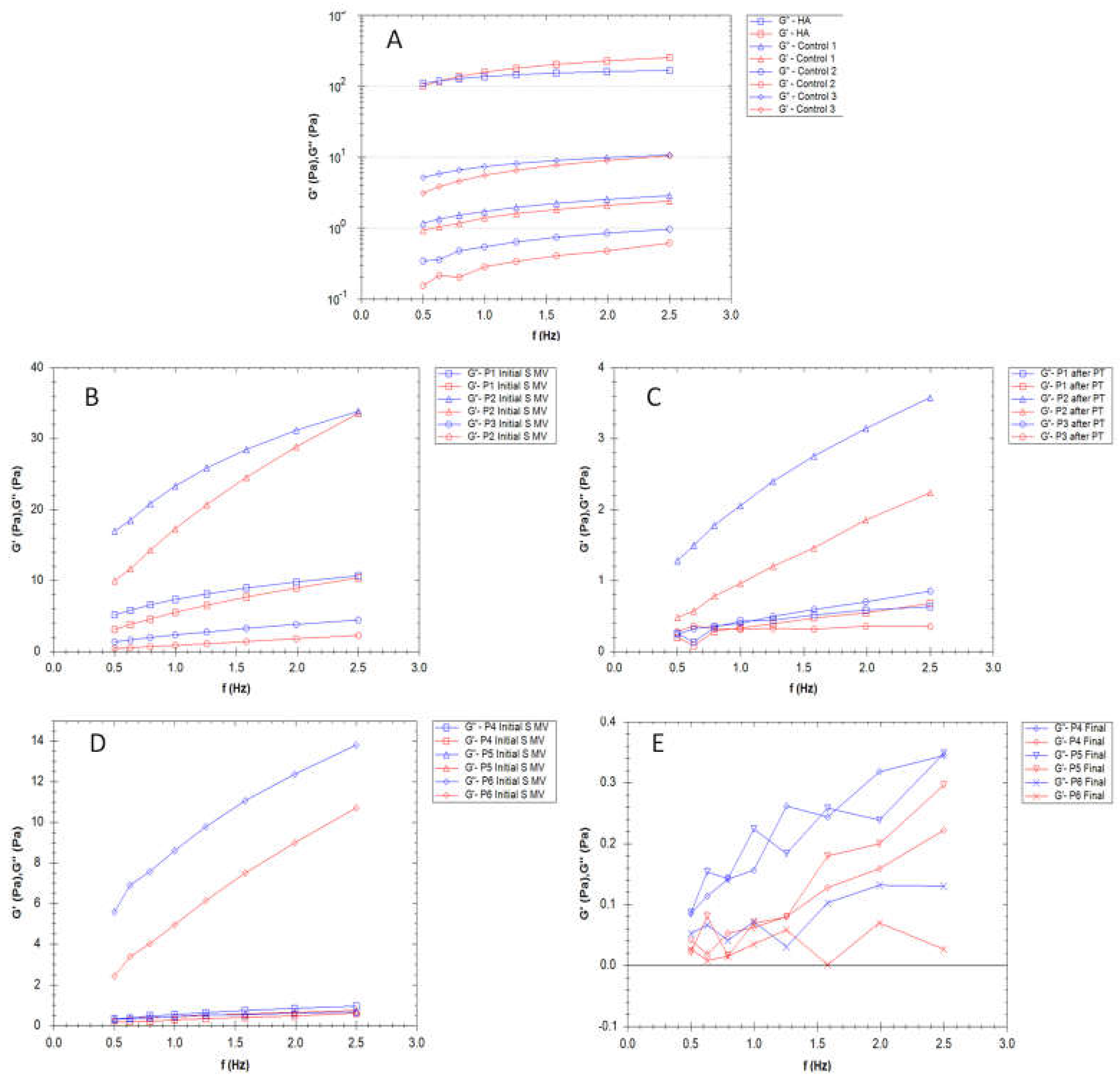
Figure 6.
The variation of tan δ with frequency (Hz) for synovial fluid (SF) collected from: control group (CG) and Kombihylan® product (A); patients supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks rest) (B and C).
Figure 6.
The variation of tan δ with frequency (Hz) for synovial fluid (SF) collected from: control group (CG) and Kombihylan® product (A); patients supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks rest) (B and C).
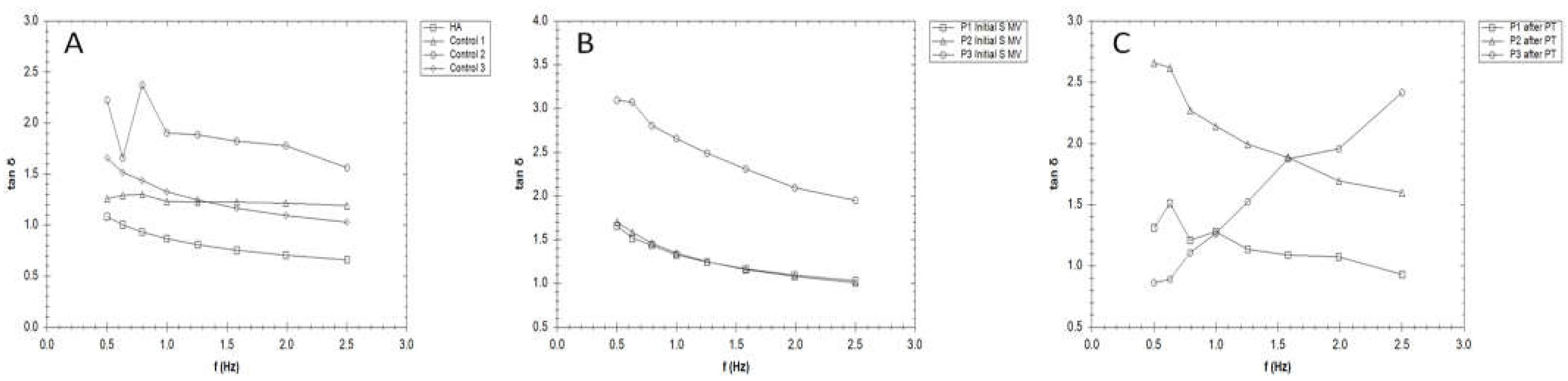
Figure 7.
The variation of viscosity for synovial fluid (SF) collected from: control group (CG) and Kombihylan® product (A); patients supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks rest) (B and C); patients supplemented, 5-10 min movement and supplemented, 5-10 min movement, 6 weeks rest (D and E).
Figure 7.
The variation of viscosity for synovial fluid (SF) collected from: control group (CG) and Kombihylan® product (A); patients supplemented, 5-10 min movement and after PT (2 weeks PT + 4 weeks rest) (B and C); patients supplemented, 5-10 min movement and supplemented, 5-10 min movement, 6 weeks rest (D and E).
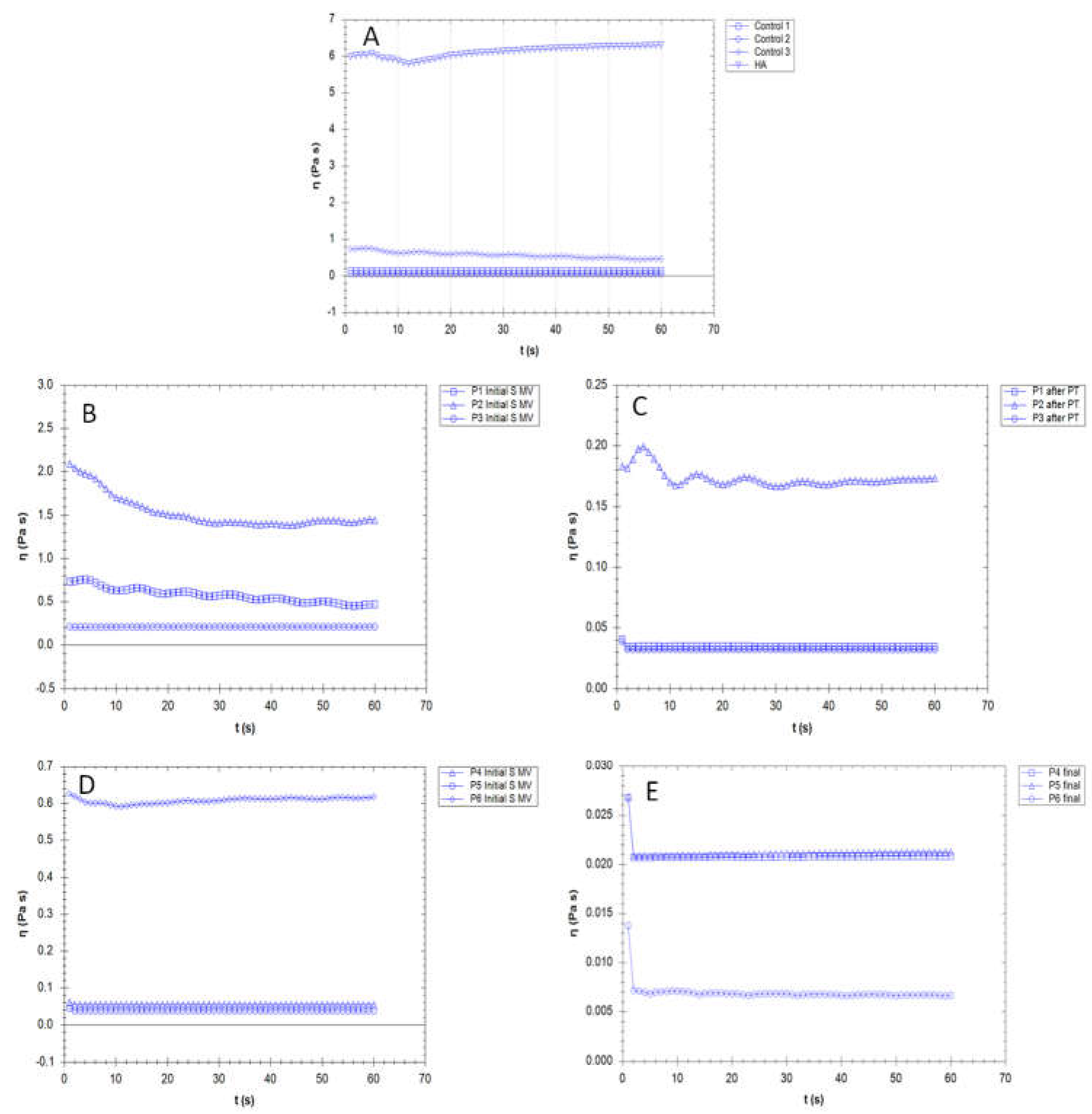
Figure 8.
Microscope images of human synovial fluids (SF) and Kombihylan®.
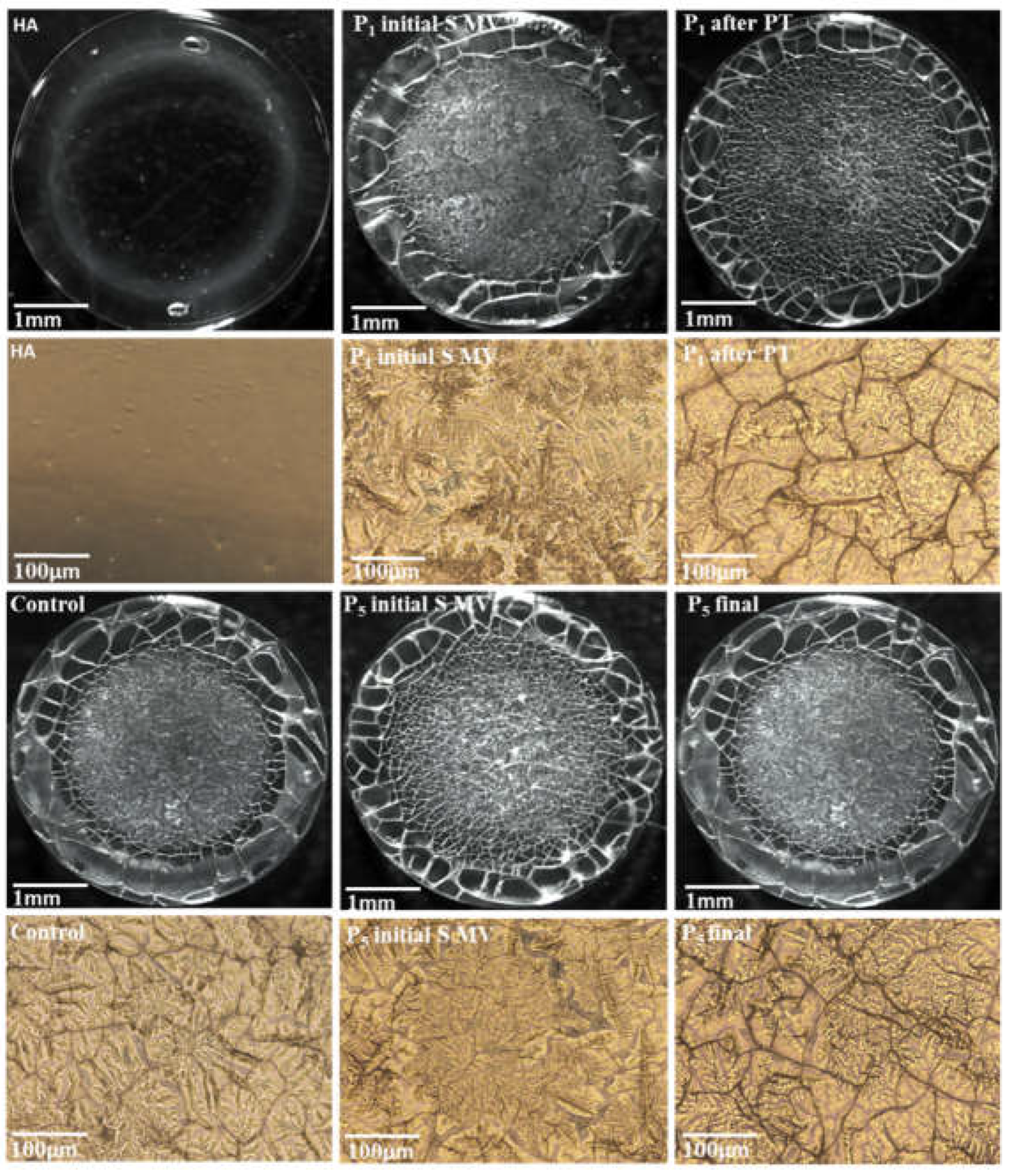
Figure 9.
Bioadhesion properties of synovial fluid-based films, tested on simulating membrane, as detachment force and work of adhesion. Values were expressed as the mean of six independent experiments. Each value represents the mean ± standard error mean (n = 6) (* p < 0.05, ** p < 0.01).
Figure 9.
Bioadhesion properties of synovial fluid-based films, tested on simulating membrane, as detachment force and work of adhesion. Values were expressed as the mean of six independent experiments. Each value represents the mean ± standard error mean (n = 6) (* p < 0.05, ** p < 0.01).
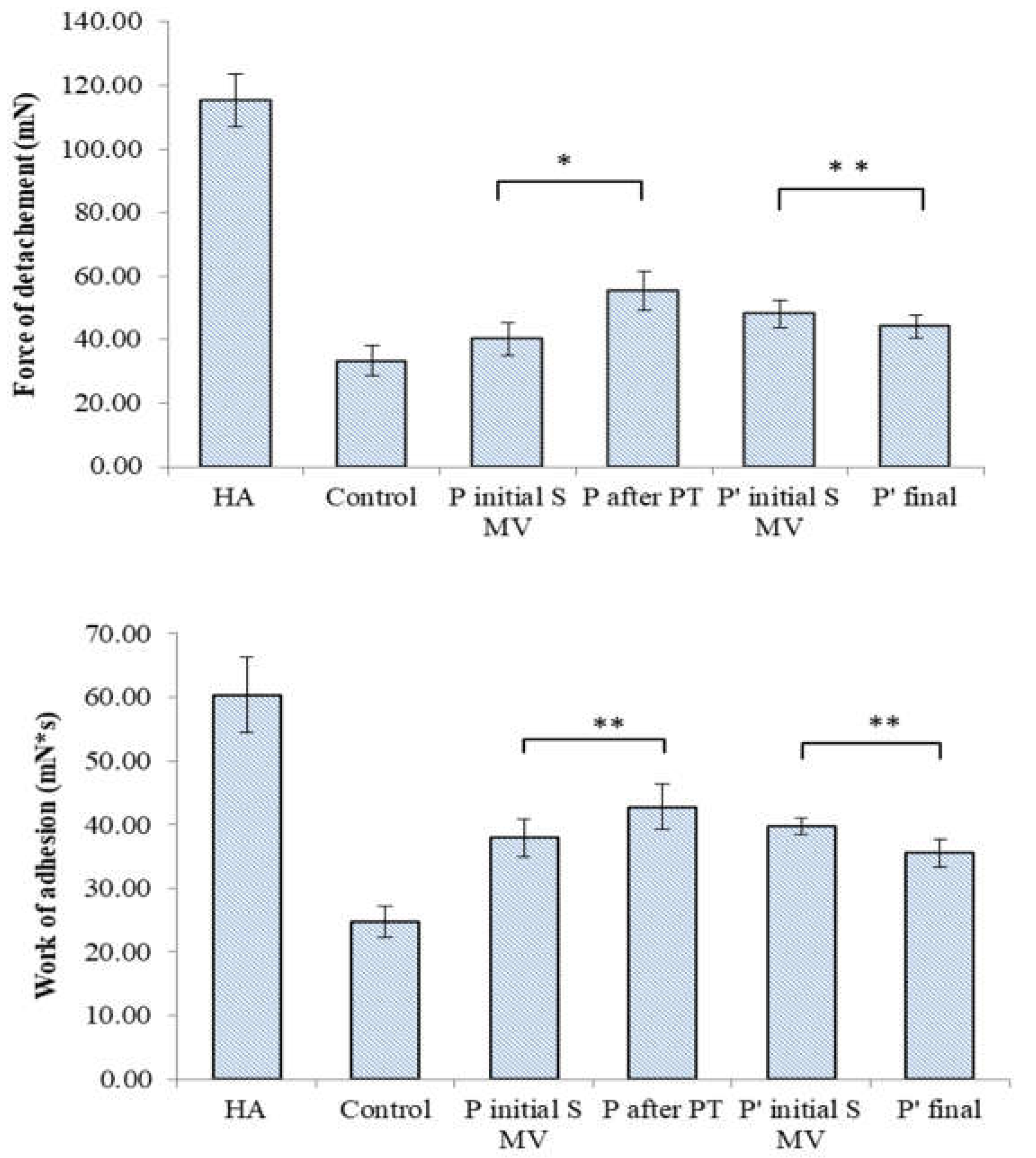
Figure 10.
Bioadhesive properties of synovial fluid-based films tested on chicken cartilage, as detachment force and work of adhesion. Values were expressed as the mean of six independent experiments. Each value represents the mean ± standard error mean (n = 6) (* p < 0.05, ** p < 0.01, *** p < 0.001).
Figure 10.
Bioadhesive properties of synovial fluid-based films tested on chicken cartilage, as detachment force and work of adhesion. Values were expressed as the mean of six independent experiments. Each value represents the mean ± standard error mean (n = 6) (* p < 0.05, ** p < 0.01, *** p < 0.001).
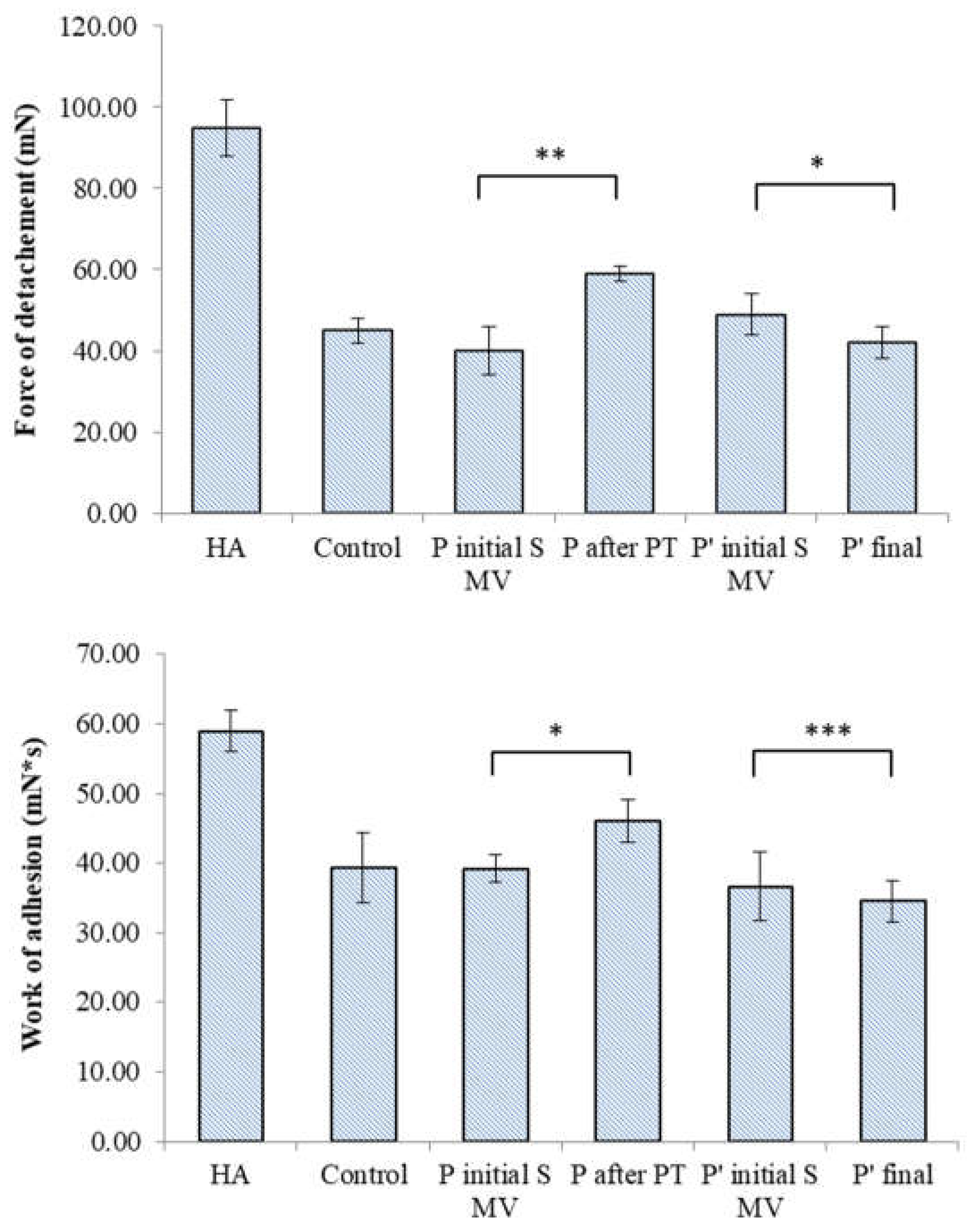

Table 1.
Tested SFs and applied procedure.
| No | Encoded | Characteristics | Solid (mg/ml) |
pH | Colour | Clarity | Glucose* (mg/dL) |
| 1. | HA | Raw Kombihylan® viscoelastic HA | 76 | 7.22 | Clear | Transparent | 0 |
| 2. | Control 1 | Patient with no procedure | 0.88 | 7.14 | Amber-Yellow | Transparent | 144 ± 4 |
| 3. | Control 2 | Patient with no procedure | 0.86 | 7.18 | Amber-Yellow | Transparent | 143 ± 1 |
| 4. | Control 3 | Patient with no procedure | 0.83 | 6.89 | Yellow | Transparent | 101 ± 2 |
| 5. | P1 Initial S MV | Patient 1 initial(supplemented) 5-10 min movement | 0.40 | 7.03 | Yellow | Transparent | 110 ± 3 |
| 6. | P2 Initial S MV | Patient 2 initial(supplemented) 5-10 min movement | 0.68 | 6.88 | Amber-Yellow | Transparent | 61 ± 2 |
| 7. | P3 Initial S MV | Patient 3 initial(supplemented) 5-10 min movement | 0.88 | 7.14 | Amber-Yellow | Transparent | 53 ± 1 |
| 8. | P1 Final | Patient 1 after PT (2 weeks PT + 4 weeks rest) | 0.66 | 7.32 | Amber-Yellow | Transparent | 99 ± 5 |
| 9. | P2 Final | Patient 2 after PT (2 weeks PT + 4 weeks rest) | 0.68 | 7.28 | Amber-Yellow | Transparent | 67 ± 1 |
| 10. | P3 Final | Patient 3 after PT (2 weeks PT + 4 weeks rest) | 0.64 | 7.42 | Amber-Yellow | Transparent | 69 ± 2 |
| 11. | P4 Initial S MV | Patient 4 initial(supplemented) 5-10 min movement | 0.72 | 7.19 | Amber-Yellow | Transparent | 104 ± 2 |
| 12. | P5 Initial S MV | Patient 5 initial(supplemented) 5-10 min movement | 0.76 | 6.87 | Amber-Yellow | Transparent | 120 ± 4 |
| 13. | P6 Initial S MV | Patient 6 initial(supplemented) 5-10 min movement | 0.76 | 7.24 | Amber-Yellow | Transparent | 59 ± 2 |
| 14, | P 4 final | Patient 4 final (6week rest) | 0.74 | 7.32 | Amber-Yellow | Transparent | 113 ± 3 |
| 15. | P 5 final | Patient 5 final (6week rest) | 0.62 | 7.51 | Amber-Yellow | Transparent | 128 ± 3 |
| 16. | P 6 final | Patient 6 final (6week rest) | 0.70 | 7.37 | Amber-Yellow | Transparent | 70 ± 2 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



