
You are currently viewing a beta version of our website. If you spot anything unusual, kindly let us know.
Preprint
Article
Assessment of Fall-Associated Risk Factors in the Muslim Community-Dwelling Elders of Peshawar, Khyber Pakhtunkhwa, Pakistan
Altmetrics
Downloads
152
Views
64
Comments
0

This version is not peer-reviewed
Applications of Spatial Science and Technology in Health Research
Abstract
Falls are the third-leading cause of disabilities among the elderly population worldwide. In Pakistan, the prevalence is 44%; out of them, 8% develop injuries, placing them at high risk for hospitalization or even premature death. Interestingly, fall is multifactorial, and fall risk depends on individual characteristics (intrinsic factors) and environmental features (extrinsic factors), which can be different from context to context. Therefore, regular assessment of fall risk factors is required to develop a strategy for fall prevention. This study aimed to identify intrinsic risk factors for falls in Pakistani elders living in the communities, and provide evidence for preventive strategies of falls in elderlies. Data were collected from 140 Muslim elders from two residential areas of Peshawar, Khyber Pakhtunkhwa, from July 2022 to August 25, 2022, after taking permission from Zhengzhou University Ethical Review Board (ZUIRB #202254), and District Health Department Office (DHO #14207).Participants were informed and concern was taken before collect data. Data were collected using the Time Up and Go Test (TUGT), the Mini-Mental Status Examination, and interviews regarding the prayer practice. Factors associated with falls were; age, gender, education, cognitive status, TUGT level, incorrect prayer postures, poor vision, and history of falls with a significance of (P.<0.05). Poor cognition, low vision, poor walking speed, and prayers without body movements have good membership with falls risk prediction as (P<0.005) in Omnibus, Lemeshow score (0.77). Hence, our study provides a road map for future risk assessment for falls by adding the four mentioned risk factors as offered in the proposed model to facilitate taking timely action to prevent fall-related ailments in Pakistani elders.
Keywords:
Subject: Public Health and Healthcare - Primary Health Care
1. Introduction
The aging of the population has become a challenging phenomenon for the healthcare system globally. The World Health Organization (WHO) defined the aging population as individuals who are 60 years of age or older[1]. In Pakistan, about 12 million individuals are over 65, and that number is projected to rise to 18 to 25 million by 2050[2]. Although aging is linked to a decline in the physiological and functional capability of the musculoskeletal and neurological systems[3], the prevalence of chronic diseases, and external causes such as falls are major causes of morbidity and mortality in the elder population[4]. Fall is considered the most common geriatric syndrome [5,6,7]. A majority, that is around 40% of elder hospitalization linked to fall-related injuries, fractures, disabilities, and other complications [8].
The prevalence of falls among elders is multifactorial; 1 out of 4 elders age > 65 falls at least once a year. The frequency is more high in older olds that is 75 years [9],females over 70 are more likely to experience of falls[8]. According to the Centers for Disease Control (CDC) report , worldwide 36 million elders report falling each year which accounting for nearly 33% of the falls prevalence in community based older adults [10].The frequency of falls is vary from country to country. For instance, a South-East Asia survey discovered that in China the falls prevalence was 31 to 34%, in 21% falls were in Japan, and 16% were in Latin America [11]. In Pakistan, the fall incident rate is almost nine percent per thousand per year [12].
Falling is the most frequent cause of injuries, disability, and hospitalization for seniors over 65 in Pakistan around 44% of falls were documented in a survey study [2]. which the ratio of female were high than male.
Fall is mostly observed in females [14], mostly reported during daily tasks performance (e.g., walking and initiation of walking or sitting down [14], and in those who have poor musculoskeletal functional ability[9,15,16].
Fall does not occur because of one factor alone but rather when physical, psychological, social, and environmental factors work together to contribute to its prevalence. Several studies have investigated the current state and risk factors for falls [9, 17–19], and divided factors into intrinsic, and extrinsic factors predicted to cause falls in elders[20]. A decrease in habitual walking speed was a measure of physical disability limitation and fall risk in the previous study [21]. The ability to perform rapid walking balance requires various supportive factors involving vision, cognitive ability, physical strength, cardiovascular fitness, and coordination. Some chronic diseases, such as orthostatic hypotension, lumbar spondylosis, high blood pressure, diabetes, cataract, musculoskeletal diseases, and urinary incontinence (UI), are risk the risk factors for falls in the older adults [22]. Muscular atrophy Sarcopenia is another key factor that limits stability control and is more likely to occur in old age people that cause serious injuries, and premature mortality[23]. Commonly identified home hazards that increase the fall risks in elders were home access, i.e., movement around the house, slippery floors, and bathroom-related falls [15, 17, 20]. Fear of falling even without any fall history is another factor of falls in elders. This fear may restrict their activities, and ultimately, they adopt an inactive lifestyle [24]. The use of some drugs, such as psychotropic and antidepressant drugs, can cause drowsiness and impaired coordination and balance; antihypertensive and ant-allergic drugs can lower blood pressure; beta-blockers and diuretics might cause postural hypotension and may cause falls. Anticholinergic medications may impair cognitive function and cause blurred vision, increasing the risk of falls in older adults [17, 22].
Identifying older adults who are at higher risk of falling and require interventions is challenging for clinicians and public health professionals. However, various fall predictors and scales are developed and tested to assess fall risk among elders. Age categories, gender, measures of gait (TUGT), disability index, CDC fall risk assessment 12-point checklist [25], and environmental hazards were some of the highlighted fall risk assessment tools, mentioned in the previous studies(5). Lusardi et al. included the Mini-Mental State Examination in their predictive model for predicting fall risk. Another review created a comprehensive list risk factors assessment [17] in which TUGTS, visual health, and cognitive scores were highly predictive factors. Oshiro et al used psychological and medical characteristics, medication use, and sensory factors to forecast fall risk [26] in which a positive prediction was found between adjusted variables and fall risk of 98%, and a negative predictive value of 8%.
1.1. Predictive models for fall risk assessment
It was difficult to generalize previously constructed model to assess fall risk in Pakistani community dwelling older adults [27]. Fall literature is in debate, whether fall predictions through different models are feasible; such as modifiable factors of falls can be reduced through new interventional strategies. A study conducted by Thurmon and fellows developed a predictive model, namely Random Forest predictive Model, evaluated fall risk in 171 community-dwelling older adults performed 10 meters walk daily, and fall frequency in the six months were followed through a sensor detection of movements. Linear and nonlinear modeling identified that 19% of elders who reported falls in the six months follow-up were had gait problems [27]. A systematic study carried out to examined all prognostic predictive models of fall risk included 30 (out of 86 369 individuals). Only three validated prediction models were reported in the included research, and the frequency of falls ranged from 5.9 percent to 59 percent in approximately 69-designed models. The most common predictors of falls were prior falls, age, gender, assessments of gait quality, walking balance, visual health and level of disability. The range of the area under the curve was 0.62 to 0.69 [17]. Fall prediction models mostly incorporated gait quality scores, cognitive status, and past fall experience. Mishra et al. conducted a study in the USA and developed a model to predict 6-month fall risk using the geriatric TUGT, MMSE, and fall history from 92 older adult residents (age = 86.2 6.4, female = 57). With an AUC of 0.80 (95% CI of 0.76-0.85), and a sensitivity of 0.82 (95% CI of 0.74-0.89) predicting the six-month risk. The activity daily living (ADL) assessment scores, and gait speed were the three most significant contributions to the comparatively increased fall risk in elder’s population. Different approaches were used in the literature to test and evaluate the predictive factors such as decision-tree analysis, fall-prediction algorithm[14], logistic regression, receiver operator characteristics (ROC) analysis, and prognostic model for fall risk screening in the previous studies [28]. However, these six predictors were able to stratify fall incidence, and probabilities that ranging from 30.4% to 71.9%. The decision-tree model in terms of the area under the curve (0.70 vs. 0.64), accuracy (0.65 vs. 0.62) were performed, sensitivity (0.62 vs. 0.50), positive predictive value (0.66 vs. 0.65), and negative predictive value (0.66 vs. 0.65) in the predictive models. There are different predictive models the researchers developed for fall prediction in old age and it is concluded that there is no any model to adopt for fall prediction in all context. Considering this background knowledge and inconsistent literature, information related to falls associated factors and fall risk assessment strategies, there is a need to develop a new fall predictive model for Muslim elders in Pakistan.
1.2. Study Contribution
Fall risk is contextual; more researches are required to identify different risk factors of falls' occurrence among elders living in the community. Older persons in the Pakistani community must therefore undergo routine fall risk assessments in order to create a fall prevention strategy. We, therefore, aim to explore the risk factors related to falls in elders in Khyber Pakhtunkhwa, Pakistan, where 99% of the population belongs to the Muslim community. Our study can help identify new risk factors for falls, so we plan to develop a predictive model to assess fall risk among community-based elders to determine preventive strategies for falls in the elder population.
2. Materials and Methods
2.1. Design and setting
Data was taken from the baseline data of an interventional study at two residential areas of Peshawar district, Khyber-Pakhtunkhwa, Pakistan from July 2022 to August 2022. Different measuring check lists were used such as Mini mental health status examination(MME), Time Up and Go(TUG), and different demographic characteristics, including five questions regarding body movements in five-time prayers from the 140 study subjects were selected for a random control trail study. The sample size were calculated using G-power by assuming 0.05 level of significant that is Alpha (α), power of test (i.e. Beta=0.8, as beta set at 0.20 that is chances of falls negative and 95% confidence level. This sample size was acceptable to develop a model for at least five hypothetical predictors with one dependent variable.
2.2. Inclusion and exclusion criteria
The inclusion and exclusion criteria were followed as the subjects had to be 60 years of age or older with sedentary life style that is <two hours activity in 24 hours, with normal to moderate cognitive functioning, able to follow instructions, and able to walk without taking assistance from another person. The language barrier, unwillingness to participate, and non-registered elders were excluded from this study.
2.3. Ethical considerations
The Helsinki Declaration of 1964 was followed. Permission was taken from the parent institution that is Zhengzhou University, Institute of Ethical Review Board (ZZUIERB #202254) , and the District Health Department Office (DHO #14207).
2.4. Data collection process
Data were collected through validated and reliable checklists approved by the Centers for Disease Control and Prevention (CDC), which is TUGTS scores as walking speed in 3 meters of distance, Mini Mental Examination checklist, five questions regarding prayer technique and procedure, and questionnaires containing information on demographic variables were collected in the interview section. Figure 1 shows the brief process of data collection.
2.5.1. Physical test
The Time Up and Go test was performed in three basic healthcare units (BHUs) in Peshawar. A trained physiotherapist conducted the timed "Up and Go" test (TUGT), in which scores were assigned to go and sit down for which 10 to 19 seconds were considered normal, 20 to 29 on the gray list included in fall risk, and >30 dependent was considered highly risky for falling[29]. The time that a participant needs to rise from a chair, walk 6 meters, turn around, walk back, and sit down on the chair was recorded. During the test, the person is instructed to wear her or his regular, comfortable footwear and use any mobility aids (e.g., a cane or frame) that they would normally require.
2.5.2. Mini Mental Examination
Mini Mental status Examination checklist were used to check cognitive level of participants. The checklist is consisted of 10 scores in which Scores > 4 with no answered considered risk for fall in this study.
2.5.3. Proper posture during five time prayers
Five questions were asked from the participants regarding Muslim five time prayers by considering the seven distinct body postures which are 1) Takbir; 2) standing;3) Rukuk;4) Qiam ; 5) Prostration;6) sitting(Jalsa);7) moving head to right and left. We considered > 5 correct answers for correctly perform prayers in this study.
2.6. Statistical Analyses
Using Statistical package of science (SPSS version 23). Descriptive statistics and the Spearman correlation coefficient test were used to describe and associate factors concerning falls' occurrence in the last year at a significant level of (P.0.05). A binary logistic regression model was used to test the hypotheses of this study, which were: 1) H1. Fall is higher in those with low-speed walking; 2) H2. The falling ratio is high with regard to visual and cognitive problems. The data were checked for normality. The distribution of the feature significance values for each feature was assigned. For instance, lower gait speed values, poor prayer postures; poor cognition scores were hypothetically negatively correlated with fall risk.
The area under the curve was measured to check the sensitivity and specificity of the model under study, and if we kept >75% of the test, it will be considered valid and reliable to check the fall's occurrence with the selected parameters.
2.6.1. Model fit index
In this model, we considered one to indicate a fall risk and zero to indicate no falls risk. Our preferred choice is one because we are interested in seeing the drops in respondents. Zero is given a benchmark as it is significant at 0.03 and shows that when we add an independent variable, it will predict the dependent variable in our model. We applied the Omnibus model of coefficient testing considering the difference between the baseline model and the new model, the Nagelkerke (R2) square >0.50, the pseudo-R square to check the approximate variation in the criterion variable were adjusted for Cox and Snell R, that is, Nagelkerke R2 >0.50 in the criterion variable can be accounted for in the predictive variable. Receiver operating characteristic (ROC) curves and logit rank plots of each variables in the models were plotted to help concluded the list of critical measures from those discovered through binary regression modeling method.
2.6.2. Sensitivity and specificity analysis:
Using ROC the standard errors for the areas under the ROC curve were determined in SPSS, version 23. For each sample participant, the projected probability—calculated as elogit (p)/(1 + elogit(p)), where logit(p) is the indicator derived from the regression model was also analysed. The specificity of the model was assumed that the Receiver Operator Characteristic (ROC) with >75% AUC accurately measures the membership of independent variables on fall risk. We considered that the model correctly predicted not to fall risk, and the model sensitivity ROC > 75% was assuming that the model correctly predicting to fall risk is due to the selected variables. The cut off point for TUGT was =<15 seconds, cognitive function =<5 scores, prayer method=1, and visual function=1. We transformed the numerical data into dichotomous data that is 1 for fall risk, and 0 for no fall risk to check the validity of the tested variables in binary regression model. The equation model in which Odd Ratio that is probability of (A) P (B) in which we interpreted that which independent variable is significantly affect fall or not falls. The beta coefficient values (Exp.b) >1 was considered cutoff point to indicate more probability of the selected outcome occurrence that is no falls or falls in the model in the relationship with the predictive variables.
2.6.3. Validity of the proposed model
The validation research was carried out to assess the discriminating validity of the model by plotting ROC curves for the 30% of subsamples. By analyzing the differences between the areas under the two curves, the calibration validity of a model was established. It is necessary to ascertain whether the predicted probability obtained for subsample, and using the models created agrees with the observed probabilities of model 2.
3. Results
The demographic features, cognitive status, and TUGT level of the participants were assessed. The average age of the study participants was 68.1 + 5 years (ranging from 60 to 82 years old). When education level is taken into account, 42% of the participants were illiterate, and only 14% are recorded as graduates; more than half (54% of the participants in this study were female). Cardiovascular diseases were common (31%), the majority (52% in the extended family system), and most of them were financially dependent on other family members, which is 38%. More than half, or 51%, of the study participants reported at least one fall in the last year. Prayer Body Movements accounted for 32% of those who did not complete all seven steps of body movements due to health issues or personal preference. The cognitive level of the study participants was 47% moderately affected, and only 53% had active memory in this study. Elders in this study had poor vision, as 66% reported having a visual problem.
3.1. Falls reports
The majority of the participants were belong to Pathan tribe that is (40%) in this study. Female participants (44%), as well as those aged 65 to 70 years, reported more falls. In this study, 42% were illiterate, 59% had a spouse who was alive, 59% had another source of income, 56% lived in an extended family system, 93% had a joint problem, 75% had a visual problem, and 71% did not follow body movements in prayer.(see Table 1)
3.2. Factors associated with falls occurrence
There was a significant relationship between income level and education, health, and age as scores ranged from >70 to 0.90. Visual health and age are also correlated with scores > 0.70. In our study, health, status, gender, and living status did not show any significant association (P >0.005) in all mentioned variables. The significant value of moderately low cognitive status and poor vision was associated with a fall history (P.0.001). Visual health and age are also correlated with scores > 0.70%. In our study, health, status, gender, and living status did not show any significant association (P >0.005) in all mentioned variables. The significant value of moderately low cognitive status and poor vision was associated with a fall history (P.0.001). Details of demographic data and risk factors are displayed in Table 1.
In Table 1 the frequency of fall is higher in female as compare to male, age group of 66 to 70 years are more reported falls as presented the data in percentages in descriptive statistics. The figure shows that female participant’s reported falls were (44%), and age group 65 to 70 years (43%) reported history of falls in this study.
3.3. Binary Logistic regression Model
The goodness of the model shows significance (P. 0.001). Age, gender, economic status, education status, health status, and ethnicity were removed from the model as they were non-significant (p > 0.005) in the Omnibus Chi-square test and the Hosmer and Lemeshow test. TUGT level, cognitive status, poor visual equity, and proper body movement in prayers were good fits of the model, as the chi-square test values of each variable in the area model were statistically significant at (P.0.05) and 94% in the Hosmer test. The variation in the criterion variable is significant, as the pseudo-R square of the approximate variation in the criterion variable through the adjusted versions of Cox and Snell R and Nagel-kerke R shows a 77% change in the fall risk can be accounted for by the predictive variables in this study. Our model correctly predicted that fall risk using 81.3% of the selected variables. Results are displayed in Table 2, and the AUC in the ROC shows the high sensitivity and specificity of our hypothetical testing variables in the relationship with fall risk in this study.(See Figure 2).
3.4. Model predictive value
To find the predictive values in our model, we analyzed the equation model in which the beta coefficient Exp (b) value is greater than 1, indicating a higher probability of the selected outcome occurring. Three independent variables, such as cognitive function, TUGT level, and poor vision, were found to predict fall risk in the elderly in this study. The log Odd of TUGT is 2.29 times more likely to fall as the Exp (b) value is (L = 1.11, U = 439.78). Elders' cognitive level is slightly poorer than expected to predict the fall occurrence with Beta value B (2.49) in Exp. b (95%) with Value (0.052), lower (0.65), and upper (4.59) but still needs to be considered in future studies to avoid being neglected. The prayer method predicts the fall's occurrence five times more with (P. 0.004) and Exp (b) = 5.19. In our model of prediction, the vision scores are highly significant for the probability of fall occurrence (P.0.001). Table 3 and Figure 3 present the data of the Odd Ratio with hypothetical variables.

Table 2.
Model of fit analysis under Binary Logistic regression analysis of predictive variables.
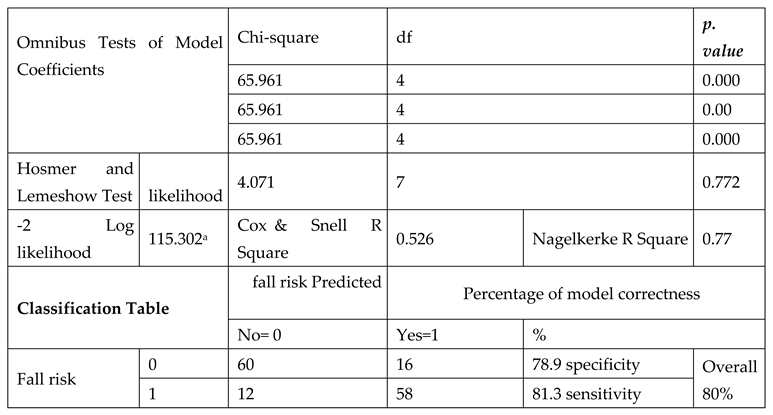
Table 2 In this table the model shows best fit in Omnibus test(P.<0.005),, Hosmer&Lemeshow likelihood value greater than 0.50 that is .0.77 in NagelkerkeR square indicated that our model is good fit with overall 80% validity and reliability scores. This results indicates that poor vision, lack of physical movement, poor gait and walking ability in TUGTs 3 meter walking test for 12 seconds, low cognition in the scale of 10 points are showing the significant of the model appropriateness and can be adopted in future fall risk assessment.
Figure 2.
Probability of fall occurrence with the hypothetical predictors in the Equation Model. N=140.
Figure 2.
Probability of fall occurrence with the hypothetical predictors in the Equation Model. N=140.
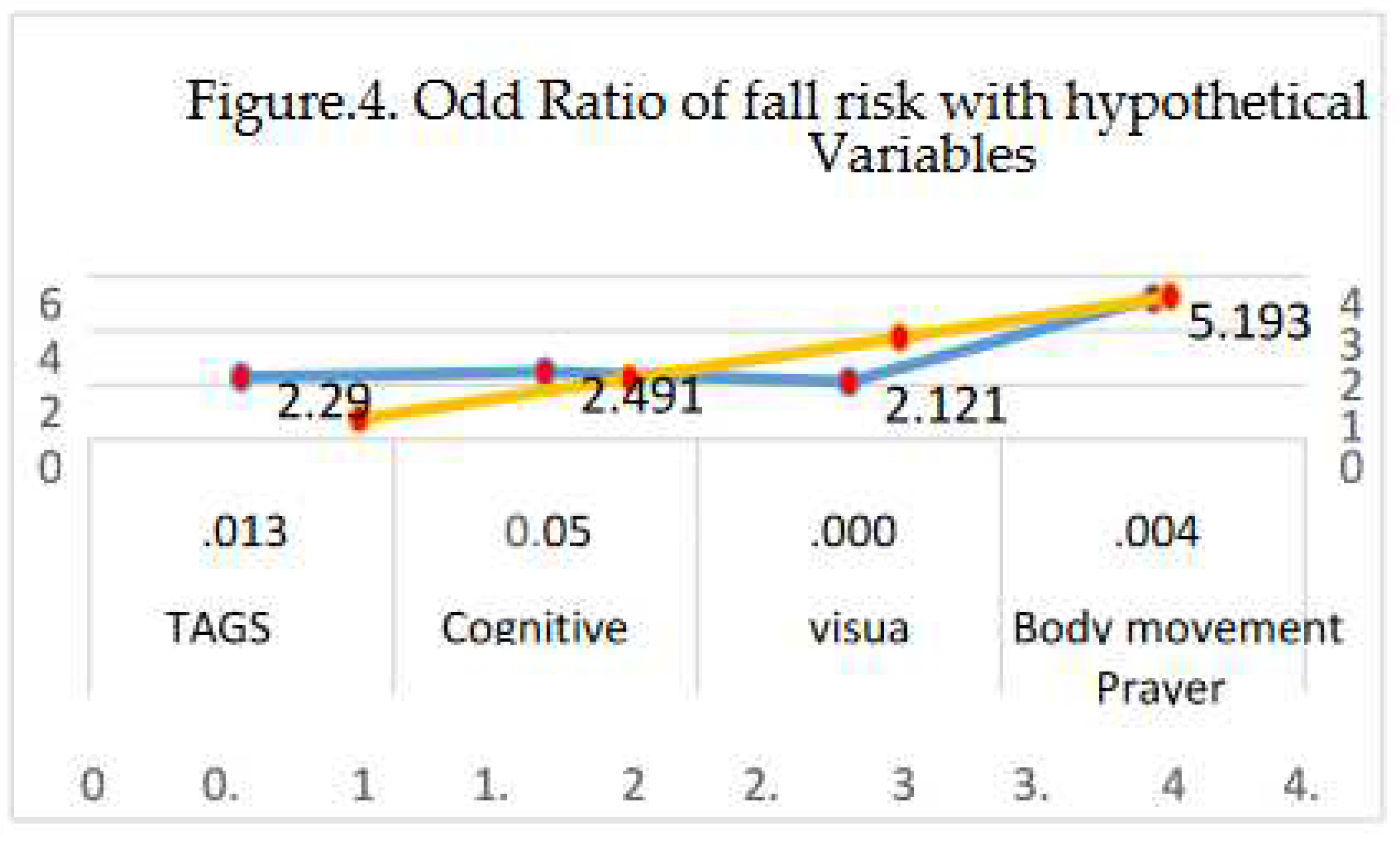
Figure 2. The model is predicting the probability of fall due to the tested variables in this study as the Odd Ratio (Exp(b) of all variables in the Equation model are >1 as TUGT=2.29, Cognitive scores=2.4, Visual=2.1 and not move the body during prayer=5.1. When the score is <1 it means that the model does not show any probability of falls in the future.
Table 3.
Odd Ratio of fall risk with the membership of the predictive variables such as TUGT, cognitive level, Poor vision, and prayer method in the Equation model. N=140.
Table 3.
Odd Ratio of fall risk with the membership of the predictive variables such as TUGT, cognitive level, Poor vision, and prayer method in the Equation model. N=140.
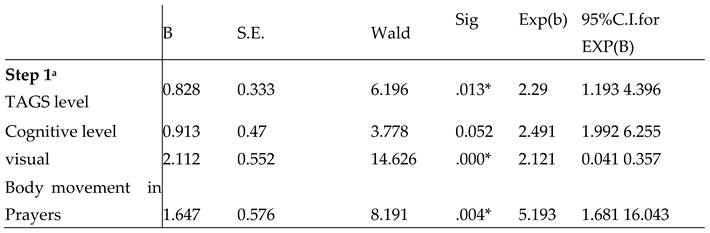
Figure 3.
Receiver operating characteristic curve of the four predictive variables.
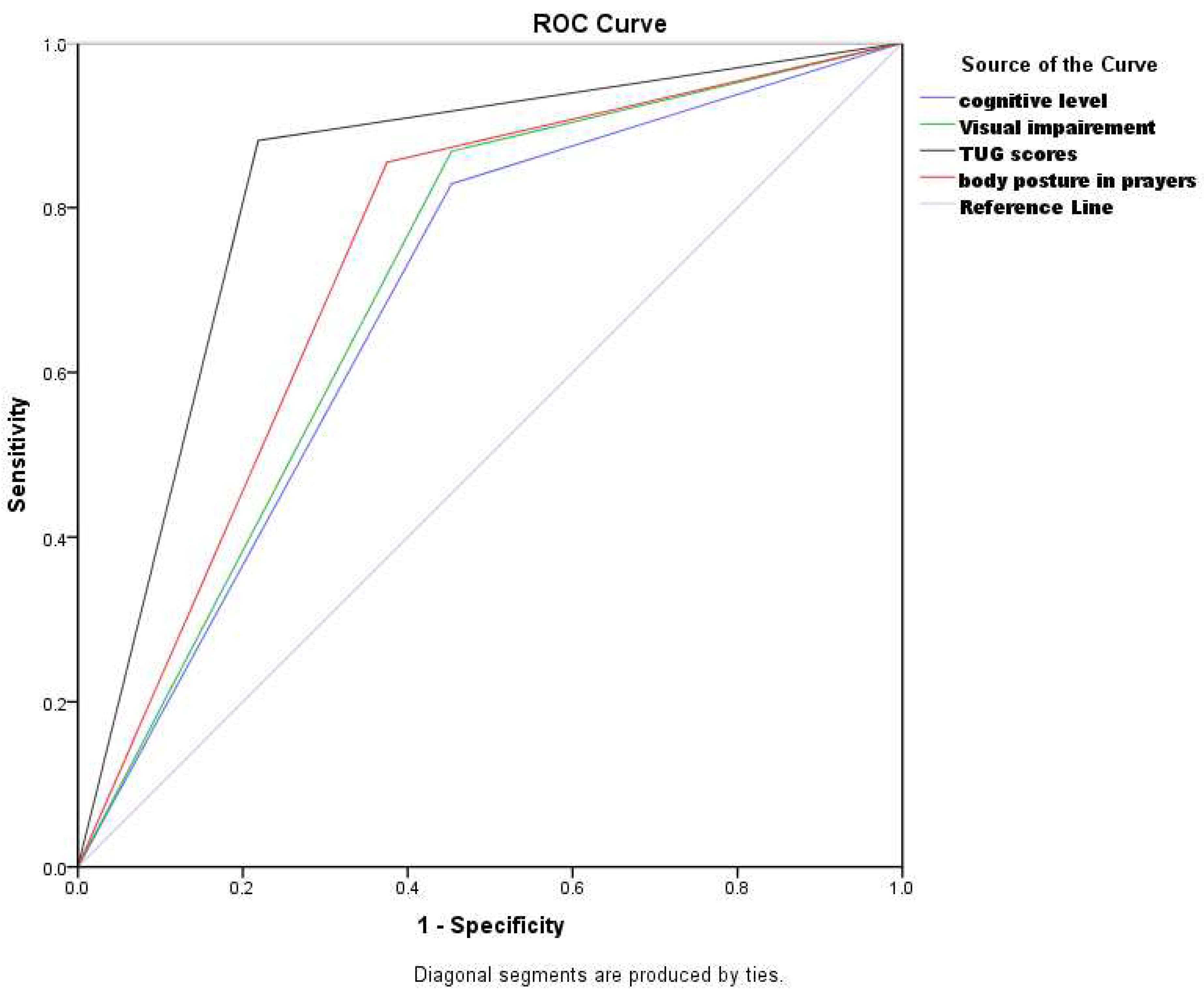
Figure 3. Receiver operating characteristic curve was generated for all the variables to discriminate elders with falls and no falls. The total area under the curve is representing the sensitivity, and specificity of the tested variables. The total area covered for lack of body movement in prayers is (82%), poor cognitive status(80%) area covered with 95% confident interval,(3) poor vision (>85%), and(4)TUGT level >85% correctly specified the accuracy of the testes factors in this model in the membership with fall risk in the study participants. The area under the curve (AUC) of this study model is shown in graphical lines of sensitivity and specificity of the test variables in which all the lines of four variables are moving from left to right with the top point of > 80 % which is near 1. The model is 80% correctly predicting that variables are correctly predicting falls risk in elders.
- External Validity of the Model
The AUC in the ROC in the randomly selected testing sample from the proposed model. Figure 4 of ROC is showing AUC of the testing sample which is supporting that this model is >80% valid and reliable and the chance of occurrence is not over fitted in the model. We are confidents to support our model risk factors can be assessed in elder of Pakistan with the same ethnicity and geographical location. The AUC in ROC is greater than 70% of the area above the straight line and falling from left side to over right side indicated that this model is not over predicting the fall risk in elders due to by chance of factors(see Figure 4 and Figure 5).
Figure 4. Figure of ROC is showing AUC of the testing sample which is supporting that this model is >80% valid and reliable and the chance of occurrence is not over fitted in the model. We are confidents to support our model risk factors can be assessed in elder of Pakistan with the same ethnicity and geographical location. The AUC in ROC is greater than 70% of the area above the straight line and falling from left side to over right side indicated that this model is not over predicting the fall risk in elders due to by chance of factors.
Figure 5.
Validity of the model with Odd Ration with sample of 30% of the total.
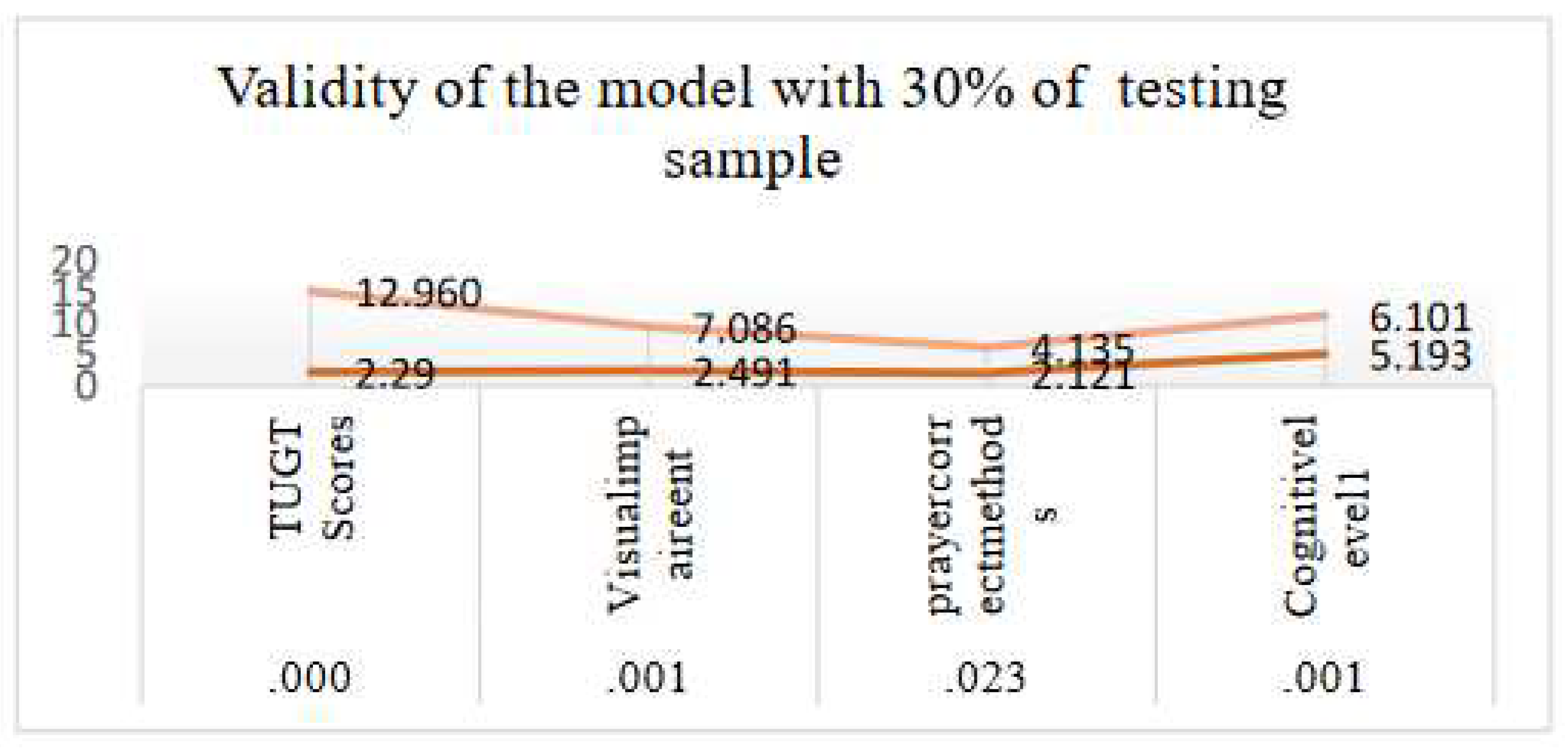
Figure 5. The Odd ratio of the testing sample is greater than 1 in the graph which is showing a high probability of fall occurrence in the study population. The significant value of all four independent variables is significant predictors (P.<0.0051) displayed in the figure. This figure shows the external validity of the model for which we randomly selected 30% of the sample considering it a testing sample and the 70% sample considered a training sample. The binary logistic regression shows Odd Ratio with exponentiated beta (Exp.b) >1 in each of the variables.
4. Discussion
Our purpose in this study was to propose a model to predict fall risk among community dwelling older adults with sedentary lifestyles in Khyber Pakhtunkhwa, Pakistan, using the TUG checklist, MMSE scores, body postures in five time Muslim prayers scores, visual health assessment scores, and fall history. In the demographic data, the average age of the study participants was 68.1 + 5 years (ranging from 60 to 82 years old), and the majority of the participants were 65 to 70 years old in this study, which is similar to the previous study carried out in Faisal Abad, Pakistan[8]. The difference in the age distribution was not a surprise to us because older adults under the age of 60 to 65 typically have a lower risk of falling due to involvement in physical activity lasting longer than two hours daily. Similarly, older adults over the age of 75 mostly become dependent on others for daily living activities due to deteriorating health conditions and disabilities, which limited their ability to participate in this study [9, 22]. When education level is taken into account, 42% of the participants were illiterate, and only 14% are recorded as graduates; more than half, or 54%, of the participants in this study were female. Our results are incompatible with studies carried out in other countries in which education status is high among older adults[14, 30].Education plays a mediating role in preventing falls, ,and education was one of the super variables that negatively affected fall prediction in the previous studies[26]. We believe that education provides opportunities for older adults to live a safe and secure life in old age [31].
Prevalence of fall occurrence: The fall frequency among the study participants in this study was 55% which is quite high compared to previous studies, as the frequency was 44% in a study conducted in Pakistan [8]. The frequency of falling was low, with only 18% of more than one time falling history in the Chinese older adult’s population [14]. But the result was quite similar to a study in Taiwan, in which the frequency of falling was 33% among community-dwelling older adults [32]. In our study, the frequency of falls was much higher among the age group of 65 to 70 years, which is inconsistent with a Brazilian study in which adults >75 years reported more falls[4]. This can be a reason for the lack of risk assessment, the low literacy rate, and the lack of an elder hood awareness program in Pakistan [33].
Associated factors of fall occurrence: We conducted an analysis to forecast older adults' fall risk and risk factors for falls in older adults. Some of the highlighted risk factors in our study were walking speed, poor cognitive level, lack of body movements in five-time prayers, and low vision. 65 to 70 years of age, illiteracy, and being female were some of the risk factors correlated with fall experiences among our study participants. Our findings were contradicted by a study conducted in the United States of America in which medication and fear of falling were more prominent risk factors for falls in older adults [34]. Similar risk factors may not have been observed in other studies because of the multifactorial nature of fall occurrence. However, in our study, the population belonged to only the Muslim community, so the lack of prescriptive body movements in the five times of prayers was one of the prominent factors contributing to the fall risk. In this study, complaints of poor vision, poor walking speed, and low cognitive ability were significantly correlated with history of falls. The same factors were identified in the previous study, in which these factors were associated with a history of falls and 50% of fall risk in elders living in the community of Pakistan [8], but in our study, lack of body movement in prayers was a newly added risk factor significantly correlated (P = 0.04) with fall occurrence. Our result is similar to another study conducted by Makino, et al. in which poor cognition, and visual problems were highlighted as factors responsible for falls in older adults [14]. Some of the risk factors in our study are also similar to those in the Brazilian study, in which sociodemographic traits, vision impairment, and cognitive impairment were associated with fall risk[4],but surprisingly, the age group > 75 years old was a higher risk group for falling in that study, which contradicts our results. Gender, being female, was more associated with a high risk for falls (P = 0.05) in our study, which is consistent with the Brazilian study, where females reported more fall occurrence [20]. Female participants were also more at risk in another study conducted by Khatak et al., in which females constituted 32% of the overall fall prevalence [13]. According to other research, women have a higher tendency to fall than men do, and this difference can be attributed to women's physiological differences in bone and muscle structure, menopausal hormone changes, and multitasking. In Pakistan, there is a male dominant culture; however; females have limited opportunities to participate in physical activities. In this study identified some of the protective factors for fall occurrence, such as gender as manhood, being literate with a graduation level, and proper body movement in five-time prayers with prescribed body motion which were significantly associated with non-fallers group with (P=<0.05). This finding was consistent with the Adriana, et al. study in which education, being a male and social support were protective factors to prevent falls in older adults [4]. Poor gate was significantly correlated with fall risk with P=<0.05) in our study. The same findings were observed in a study carried out in the USA on 92 elders in which poor scores in cognitive status, medication-related drowsiness, poor gait, and balance were highly correlated with falls [34]. Although this study has focused on sociodemographic, contextual, intrinsic, and behavioral factors of falls and gait speed assessment, the way of five-time prayers should also be given priority because of the likelihood that these events will occur as a result of a lack of exercise, especially in women of Pakistan. Hence, this model might be a useful tool to distinguish between elderly people living in Muslim communities in Pakistan who are at high risk of falling and those who are not at risk. Healthcare professionals could incorporate our model to assess and screen the identified risk factors in the general population to take the necessary action to prevent fall risk in elders in Pakistan.
Validity of the model: Our model is good fit by its internal validity. The Nagelkerke R Square is 52% to 77%, which is well supporting to predict that the variables, such as poor cognitive level (scores >7 in the total 10 point scale); poor vision; gait problems (taken >15 seconds in a 3 m distance walk); and lack of seven-style body movement in prayers, are good fits on the fall risk. The coefficient Ex (b) of the independent variables shows a value of >1 in each predictive variable, such as TUGT (2.290), cognitive health (2.491), visual health (2.121), and prayer body movements (5.193). In terms of the components of our model, other studies have demonstrated a connection between older persons' fall histories, poor cognitive scores, TUG, pain, and age group with the falls of older adults. Hence, the items we selected for our binary regression model analysis corroborated this finding with different models, such as the simplified decision-tree algorithm model [14], and the SHapley Additive exPlanations model[34]. The binary regression model is a logistic regression model that can be used to reveal stratified relationships between fall predictors and subsequent fall risk. It includes TUG, cognitive problems, lack of body movement in prayers, and poor vision in an importance-based ordering of predictors. TUG is located at the top of the ROC graph. Poor gait speed is the most influential predictor and is recommended to be assessed to predict falls in the future. Therefore, we believe that the structure of our model is valid. Additionally, our model calculated the optimal cut-off point of TUG as 10 for fall prediction. Regarding the cut-off point of TUG for falls, the >15 previously reported [30] and has been widely used. Our cut-off point was 15 s, which is relatively more power to include all high-risk older adults. The TUG cut-off point should be set faster for older people living independently in the community. The binary regression model outperformed the logistic regression model in terms of AUC, accuracy, sensitivity, probability, and odds ratio, making it suitable for use as a primary screening tool for fall risk. Our model is well supported by Mishra’s study, in which the model supported most of the variables in our model to assess fall risk in older adults [34]. The external validity was checked with randomly selected data from the model. We split our data into two groups: 70% of training data and 30% of testing data from the 140 samples collected through a random sampling method. The testing model >70% accurately tested that the primary model was a valid model as the odd ratio Exp (b) of each variable is >2, with P = 0.01) which supports that our model is valid [35]. The fall risk model can provide guidance to health providers to focus on specific factors of fall risk instead of analyzing individual assessments.
5. Conclusions
Falling is multifactorial; we cannot claim one factor is not responsible for falls in elders. To provide information on prevention and the identification of seniors at risk, multidisciplinary expertise is necessary, which justifies the need for this study. Vision impairment, cognitive impairment, poor gait, and prayers without body motions were the variables linked to the probability of falls in the binary logistic regression model. Therefore, this study could facilitate community health nurses and public health workers including these predictors in their fall risk assessment tools to provide appropriate fall prevention strategies for Muslim elders in Pakistan.
Study limitations
The study does have certain limitations. The data were taken from baseline data of a randomized control trial study; therefore, the data is retrospective. In addition, future analysis with more predictor variables and prospective studies could potentially improve the results, but they could not be applied to other older adult populations. To support the threshold values of the variables in our model, additional longitudinal studies are required. A fall risk assessment checklist, the Berg balance test, certain medications, a sleep quality assessment, and nutritional status can be added in future studies.
Future Implications
This study's model was constructed using a new factor, which can be further examined in randomized control trials. While we think this can be applied successfully to forecast fall risk in Peshawar and in other Muslim populations that are similar, Our study provides valuable information on future predictors; therefore, selecting factors for the prediction model, a literature review, and clinical experience are often used to prevent bias in predictor selection. It is essential to examine the external validity of the developed model in the general population to determine the stability of the model across various populations.
Author Contributions
Conceptualization=Zhang Yan, Rashida Bibi, 2. Methodology: Rashida, Nasar Mian, Data analysis, Rashida, Akhter Zeb, Nasir Anwar, Data collection, and writing literature review; Rashida, Akhter Zeb, Nasar Mian; Wring manuscript: Rashida, Zhang Yan. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
Permission was taken from the parent institution (ZZUIRB #202254) to conduct this study in the community and from the local health department of Peshawar.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All the data is secured and available from the corresponding authors. The corresponding authors may provide the data on the demand of the journal.
Acknowledgments
We are very thankful to Dr. Abdul Razzaq, Department of Ocean Technology and Engineering, Ocean College, Zhejiang University, China, for his untiring guidance and facilitation in developing this paper. We also acknowledge Dr. Yorozoya, a professor at the School of Nursing in Tokyo, Japan, for her time to revise and provide feedback, and we would like to extend our sincere gratitude to Mike, a postgraduate student at Zhengzhou University, China, for his technical expertise. We are grateful to the health department of Khyber Pakhtunkhwa for facilitating this study by permitting the lady health care workers to participate. We are thankful to the research team that carried out the assessment and collected data from the participants.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO, “Active Ageing: A Policy Framework,” Act. Ageing Policy Fram., vol. 5, 2002.
- A. Tu-Allah Khan, R. H. Toor, and Q. Amjad, “Assessment and Management of Geriatric Care in Pakistan,” J. Gerontol. Geriatr. Res., vol. 07, no. 05, 2018. [CrossRef]
- A. M. Briggs et al., “Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health,” The Gerontologist, vol. 56, no. Suppl 2, pp. S243–S255, Apr. 2016. [CrossRef]
- A. de A. Smith, A. O. Silva, R. A. P. Rodrigues, M. A. S. P. Moreira, J. de A. Nogueira, and L. F. R. Tura, “Assessment of risk of falls in elderly living at home,” Rev. Lat. Am. Enfermagem, vol. 25, no. 0, 2017. [CrossRef]
- AKUH, Board on Health Care Services, Health and Medicine Division, and National Academies of Sciences, Engineering, and Medicine, Families Caring for an Aging America. Washington, D.C.: National Academies Press, 2016, p. 23606. [CrossRef]
- P. R. Baker, D. P. Francis, N. N. Hairi, S. Othman, and W. Y. Choo, “Interventions for preventing abuse in the elderly,” Cochrane Database Syst. Rev., Aug. 2016. [CrossRef]
- WHO, “Global Burden of Disease Stud,” 2020. Available: https://www.who.int/health-topics/noncommunicable-diseases.
- M. Mehmood, M. Mushtaq, N. Ansa, and A. Jilani, “Prevalence of Risk of Fall in Community Dwelling Pakistani Male Population over the Age of 65 years,” J. Nov. Physiother., vol. 6, no. 5, 2016. [CrossRef]
- K. Makino et al., “Simplified Decision-Tree Algorithm to Predict Falls for Community-Dwelling Older Adults,” J. Clin. Med., vol. 10, no. 21, p. 5184, Nov. 2021. [CrossRef]
- M. J. Faber.et.al, “Effects of Exercise Programs on Falls and Mobility in Frail and Pre-Frail Older Adults: A Multicenter Randomized Controlled Trial,” vol. 87, no. 7, pp. 885–8896, Jul. 2006. [CrossRef]
- Centers for Disease, Control and Prevention, National Center for Injury, and Prevention and Control, “Stay independent and learn more about fall prevention,” 2017. Available: https://www.cdc.gov/steadi/.
- World Health Organization . WHO, . “global report on falls prevention in older age. Ageing, Life Course Unit, World Health Organization,Geneva,”2008. Available: https://www.who.int/publications/i/item/who-global-report-on-falls-prevention-in-older-age.
- Bachani, A.M., Ghaffar, A. & Hyder, A.A, “Burden of fall injuries in Pakistan - analysis of the National Injury Survey of Pakistan.,” EMHJ - Eastern Mediterranean Health Journal, vol. 17, no. 5, pp. 381–375, 2011.Available: https://apps.who.int/iris/handle/10665/118627.
- H. G. Khattak, H. Arshad, K. Anwar, and Y. Majeed, “Fall Prevalence and Associated Risk Factors in Geriatric Population,” Pak. J. Med. Health Sci., vol. 15, no. 9, pp. 2161–2164, Sep. 2021. [CrossRef]
- M. Yamada and et al, “2010 Oct;58(10): Trail-walking exercise and fall risk factors in community-dwelling older adults: preliminary results of a randomized controlled trial,” Am Geriatr Soc ., vol. 58, no. 10, pp. 1946–51, Sep. 2010. [CrossRef]
- G. Agarwal and M. Brydges, “Effects of a community health promotion program on social factors in a vulnerable older adult population residing in social housing,” BMC Geriatr., vol. 18, no. 1, p. 95, Dec. 2018. [CrossRef]
- Deandrea and et al, “Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis.,” Epidemiology., vol. 21, no. 5, pp. 658–68, 2010. [CrossRef]
- L. Z. Rubenstein, “Falls in older people: epidemiology, risk factors and strategies for prevention,” Age Ageing, vol. 35, no. suppl_2, pp. ii37–ii41, Sep. 2006. [CrossRef]
- Ken Y. T., Christina W. Y., and Hui.Zhan, “The effects of practicing sitting Tai Chi on balance control and eye-hand coordination in the older adults: a randomized controlled trial,” Disability and Rehabilitation, vol. 37, no. 9, pp. 790–794. [CrossRef]
- T. Liu-Ambrose et al., “Action Seniors! - secondary falls prevention in community-dwelling senior fallers: study protocol for a randomized controlled trial,” Trials, vol. 16, no. 1, p. 144, Dec. 2015. [CrossRef]
- Tzuo-Yun Lan 1, David Melzer, Brian D M Tom, Jack M Guralnik and et al, “Performance tests and disability: developing an objective index of mobility-related limitation in older populations,” J Gerontol A Biol Sci Med Sci, vol. 57, no. 5, pp. 294–301, May 2002. [CrossRef]
- Phelan, E. A., Mahoney, J. E., Voit, J. C., & Stevens, J. A., “Assessment and Management of Fall Risk in Primary Care Settings,” The Medical clinics of North America, vol. 99, 2, 2015. [CrossRef]
- Power, Brian H, and Dalton b, “Human neuromuscular structure and function in old age: A brief review Author links open overlay panelGeoffrey,” Journal of Sport and Health Science Volume, vol. 2, no. 4, pp. 215–226, Dec. 2013. [CrossRef]
- G. Bernardelli, C. Roncaglione, S. Damanti, D. Mari, M. Cesari, and M. Marcucci, “Adapted physical activity to promote active and healthy ageing: the PoliFIT pilot randomized waiting list-controlled trial,” Aging Clin. Exp. Res., vol. 31, no. 4, pp. 511–518, Apr. 2019. [CrossRef]
- (Rubenstein et al, “This checklist was developed by the Geriatric Research Education Clinical Center and affilia tes and is a validated fall risk self-assessment tool Res; 2011: 42(6)493-499),” vol. 42, no. 6, pp. 493–499.
- Oshiro and et al, “Fall ascertainment and development of a risk prediction model using electronic medical records.,” J Am Geriatr Soc, vol. 67, no. 7,p. 1417–2, 2019. [CrossRef]
- T. E. Lockhart et al., “Prediction of fall risk among community-dwelling older adults using a wearable system,” Sci. Rep., vol. 11, no. 1, p. 20976, Oct. 2021. [CrossRef]
- S. Buchman and et al, “Physical Activity and Leg Strength Predict Decline in Mobility Performance in Older Persons,” J Am Geriatr Soc, vol. 55:, no. 10, pp. 1618-1623, 2007. [CrossRef]
- T. J. Klotzbier, H. Korbus, B. Johnen, and N. Schott, “Evaluation of the instrumented Timed Up and Go test as a tool to measure exercise intervention effects in nursing home residents: results from a PROCARE substudy,” Ger. J. Exerc. Sport Res., vol. 51, no. 4, pp. 430–442, Dec. 2021. [CrossRef]
- Huang HC, Liu CY, Huang, and YT, Kernohan WG, “Community-based interventions to reduce falls among older adults in Taiwan - long time follow-up randomised controlled study.,” J Clin Nurs., p. 19:959-68, 2010.
- B. M. Chaudhry, D. Dasgupta, and N. V. Chawla, “Successful Aging for Community-Dwelling Older Adults: An Experimental Study with a Tablet App,” Int. J. Environ. Res. Public. Health, vol. 19, no. 20, p. 13148, Oct. 2022. [CrossRef]
- S. Roberts et al., “Ageing in the musculoskeletal system: Cellular function and dysfunction throughout life,” Acta Orthop., vol. 87, no. 363,p. 15–25, Dec. 2016. [CrossRef]
- M. Tousignant, H. Corriveau, P.-M. Roy, J. Desrosiers, N. Dubuc, and R. Hébert, “Efficacy of supervised Tai Chi exercises versus conventional physical therapy exercises in fall prevention for frail older adults: a randomized controlled trial,” Disabil. Rehabil., vol. 35, 17, pp. 1429–1435, Aug. 2013. [CrossRef]
- M. Osama, R. Malik, and S. Fiaz, “Salat (Muslim prayer) as a therapeutic exercise,” J. Pak. Med. Assoc., vol. 69, no. 3, p. 1, 2019. [CrossRef]
- Jon Pynoos, Anna Q D Nguyen and et al, “Fall risk in older adults: roles of self-rated vision, home modifications, and limb function Bernard A Steinman,” J Aging, vol. 21, no. 5, pp. 655–76, Aug. 2009. [CrossRef]
- A. K. Mishra et al., “Explainable Fall Risk Prediction in Older Adults Using Gait and Geriatric Assessments,” Front. Digit. Health, vol. 4, p. 869812, May 2022. [CrossRef]
- Jian Wang, 1 Xiuqin Chen, 2 Xiaoming Sun, 3 Huifen Ma, 2 Yan Yu, 4 Chunxia Yao, 2 Zhipeng Li, 5 Limei, “The Application of ‘Timed up and Go’ Test in Fall Screening of Elderly People in Shanghai: A Cross-Sectional Study Jian,” Iran J Public Health, vol. 50, no. 12, pp. 2567–2575, Dec. 2021. [CrossRef]
- F. Saqib Lodhi, O. Raza, A. Montazeri, S. Nedjat, M. Yaseri, and K. Holakouie-Naieni, “Psychometric properties of the Urdu version of the World Health Organization’s quality of life questionnaire (WHOQOL-BREF),” Med. J. Islam. Repub. Iran, vol. 31, no. 1, pp. 853–859, Dec. 2017. [CrossRef]
Figure 1.
Step by step process for falls risk assessment of study participants=140.
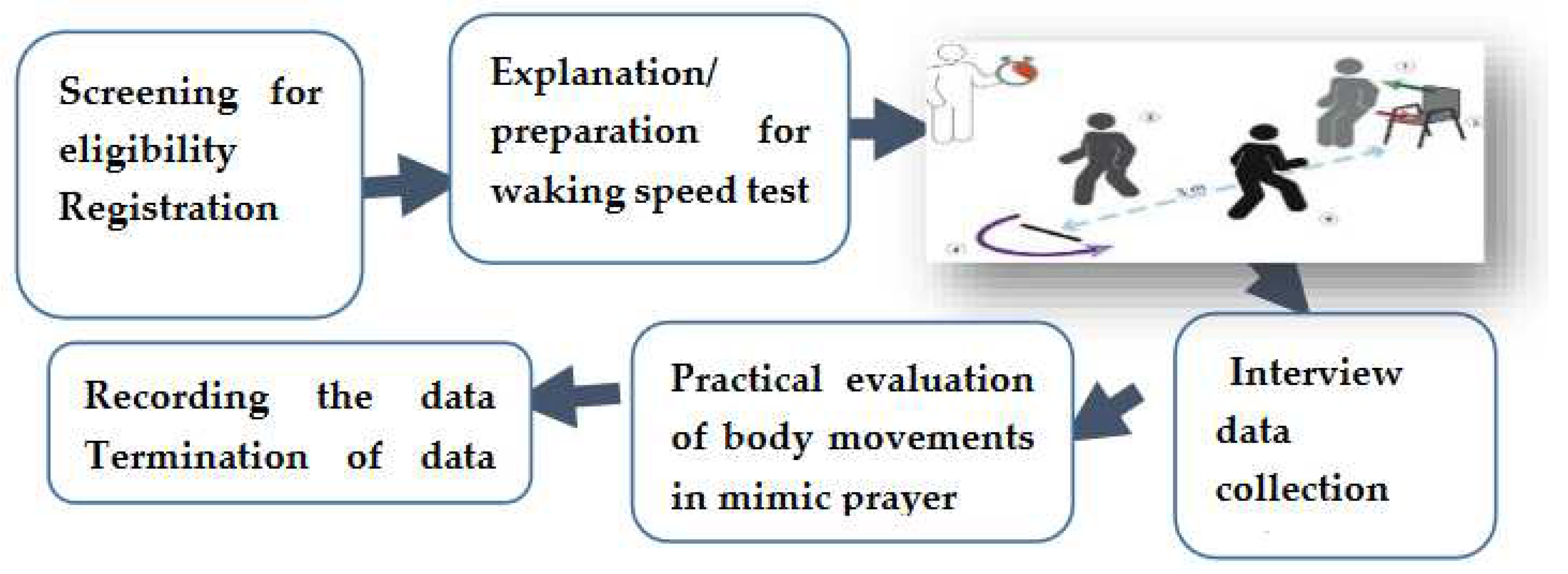
Figure 4.
Validity of the Model AUC in the ROC in the randomly selected testing sample from the proposed model.
Figure 4.
Validity of the Model AUC in the ROC in the randomly selected testing sample from the proposed model.
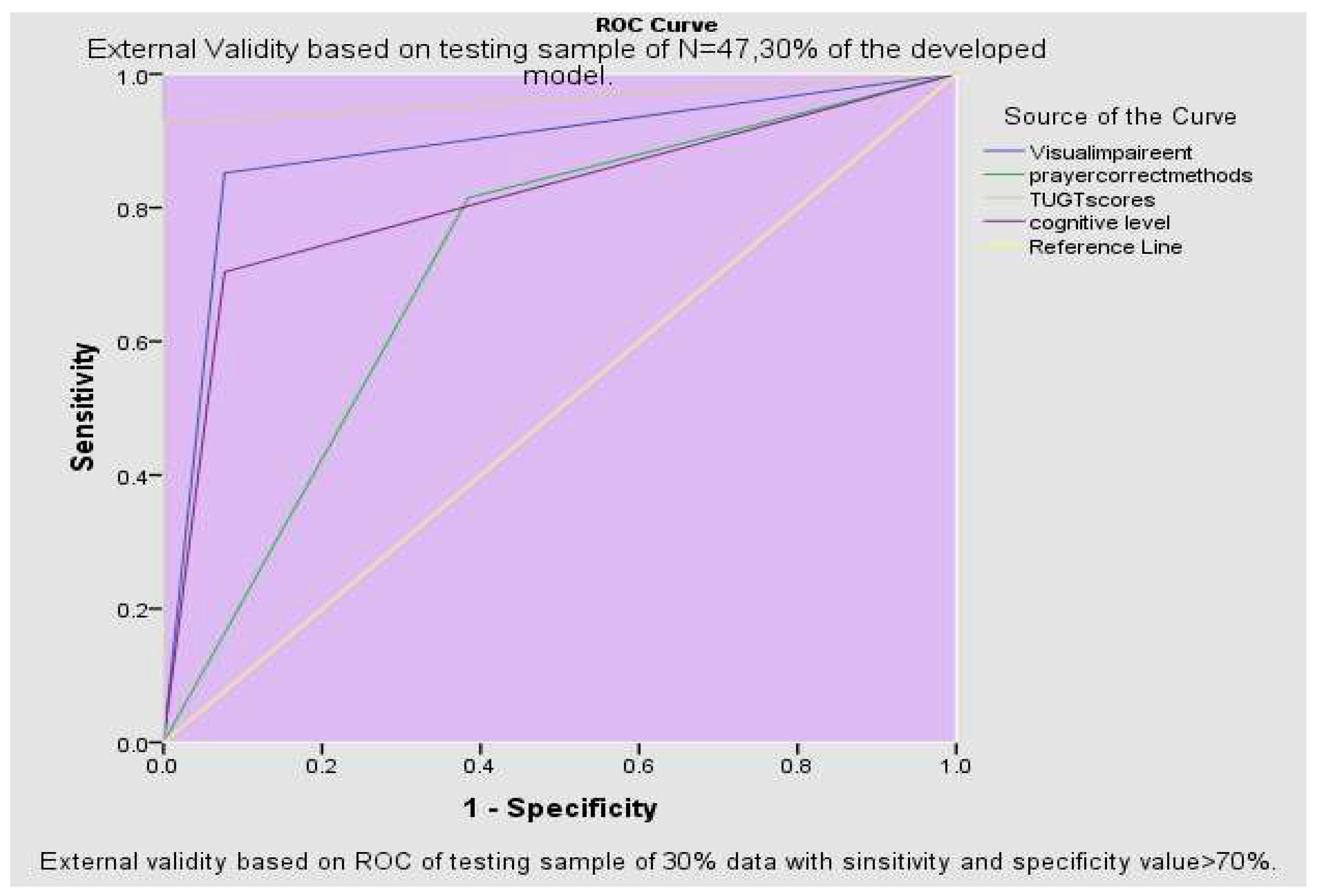
Table 1.
Demographic characteristics, fall frequency, and risk factors of fall occurrence.
| Demographic Variables .N=140 | Total# | Fall history | P.Value | ||||
|---|---|---|---|---|---|---|---|
| % | yes% | No % | |||||
| Gender | Male Female | 46% 54% |
33% 44% |
46% 56% |
0.49 | ||
| Age | 60-65 66-70 71-75 |
46.40% 14.30% 4.30% |
33% 44% 16% |
67% 56% 84% |
0.04 | ||
| >76 | 8.57% | 33% | 67% | ||||
| Education level | Graduate Matric Secondary | 14% 22% 17% |
14% 22% 20% |
86% 78% 80% |
0.021 | ||
| Illiterate | 47% | 42% | 58% | ||||
| Married | Alive Widow |
79% 21% |
59% 41% |
42% 59% |
0.012 | ||
| Source Income | of | Pension Others No, any source |
28% 34% 38% |
57% 59% 48% |
43% 41% 52% |
0.62 | |
| Health status | Cardiovascular Diabetic Joint Pain |
30.70% 22.00% 20% |
51% 21% 93% |
49% 58% 7% |
0.72 | ||
| Other | 4.30% | 33% | 67% | ||||
| No diseases | 9.30% | 46% | 54% | ||||
| Living status | Join family Extended Family |
47% 52% |
54% 56% |
46% 44% |
0.45 | ||
| Visual problem | yes No |
52% 47% |
75% 33% |
25% 67% |
0.002 | ||
| Prayer practice | five-time prescribe | as | 48% | 37% | 63% | 0 | |
| not proper way | 52% | 71% | 29% | ||||
| Ethnicity | Pathan Panjabi Sindhi |
0.4 0.3 0.2 |
58% 47% 28% |
42% 53% 60% |
0.51 |
||
| Chitrali 8% | 0.1 | 21% | 54% | ||||
| Cognitive level | Normal Moderate |
54% 47% |
45 64% | 55% 36% |
0 | ||
| severe | 0% | 7.9 | |||||
| <12 seconds | 48% | 31% | 69% | ||||
| TUGT level | 12-14 seconds | 28% | 64% | 56% | 0.001 | ||
| >14 seconds | 24% | 90% | 10% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.
Submitted:
28 April 2023
Posted:
04 May 2023
You are already at the latest version
Alerts
This version is not peer-reviewed
Applications of Spatial Science and Technology in Health Research
Submitted:
28 April 2023
Posted:
04 May 2023
You are already at the latest version
Alerts
Abstract
Falls are the third-leading cause of disabilities among the elderly population worldwide. In Pakistan, the prevalence is 44%; out of them, 8% develop injuries, placing them at high risk for hospitalization or even premature death. Interestingly, fall is multifactorial, and fall risk depends on individual characteristics (intrinsic factors) and environmental features (extrinsic factors), which can be different from context to context. Therefore, regular assessment of fall risk factors is required to develop a strategy for fall prevention. This study aimed to identify intrinsic risk factors for falls in Pakistani elders living in the communities, and provide evidence for preventive strategies of falls in elderlies. Data were collected from 140 Muslim elders from two residential areas of Peshawar, Khyber Pakhtunkhwa, from July 2022 to August 25, 2022, after taking permission from Zhengzhou University Ethical Review Board (ZUIRB #202254), and District Health Department Office (DHO #14207).Participants were informed and concern was taken before collect data. Data were collected using the Time Up and Go Test (TUGT), the Mini-Mental Status Examination, and interviews regarding the prayer practice. Factors associated with falls were; age, gender, education, cognitive status, TUGT level, incorrect prayer postures, poor vision, and history of falls with a significance of (P.<0.05). Poor cognition, low vision, poor walking speed, and prayers without body movements have good membership with falls risk prediction as (P<0.005) in Omnibus, Lemeshow score (0.77). Hence, our study provides a road map for future risk assessment for falls by adding the four mentioned risk factors as offered in the proposed model to facilitate taking timely action to prevent fall-related ailments in Pakistani elders.
Keywords:
Subject: Public Health and Healthcare - Primary Health Care
1. Introduction
The aging of the population has become a challenging phenomenon for the healthcare system globally. The World Health Organization (WHO) defined the aging population as individuals who are 60 years of age or older[1]. In Pakistan, about 12 million individuals are over 65, and that number is projected to rise to 18 to 25 million by 2050[2]. Although aging is linked to a decline in the physiological and functional capability of the musculoskeletal and neurological systems[3], the prevalence of chronic diseases, and external causes such as falls are major causes of morbidity and mortality in the elder population[4]. Fall is considered the most common geriatric syndrome [5,6,7]. A majority, that is around 40% of elder hospitalization linked to fall-related injuries, fractures, disabilities, and other complications [8].
The prevalence of falls among elders is multifactorial; 1 out of 4 elders age > 65 falls at least once a year. The frequency is more high in older olds that is 75 years [9],females over 70 are more likely to experience of falls[8]. According to the Centers for Disease Control (CDC) report , worldwide 36 million elders report falling each year which accounting for nearly 33% of the falls prevalence in community based older adults [10].The frequency of falls is vary from country to country. For instance, a South-East Asia survey discovered that in China the falls prevalence was 31 to 34%, in 21% falls were in Japan, and 16% were in Latin America [11]. In Pakistan, the fall incident rate is almost nine percent per thousand per year [12].
Falling is the most frequent cause of injuries, disability, and hospitalization for seniors over 65 in Pakistan around 44% of falls were documented in a survey study [2]. which the ratio of female were high than male.
Fall is mostly observed in females [14], mostly reported during daily tasks performance (e.g., walking and initiation of walking or sitting down [14], and in those who have poor musculoskeletal functional ability[9,15,16].
Fall does not occur because of one factor alone but rather when physical, psychological, social, and environmental factors work together to contribute to its prevalence. Several studies have investigated the current state and risk factors for falls [9, 17–19], and divided factors into intrinsic, and extrinsic factors predicted to cause falls in elders[20]. A decrease in habitual walking speed was a measure of physical disability limitation and fall risk in the previous study [21]. The ability to perform rapid walking balance requires various supportive factors involving vision, cognitive ability, physical strength, cardiovascular fitness, and coordination. Some chronic diseases, such as orthostatic hypotension, lumbar spondylosis, high blood pressure, diabetes, cataract, musculoskeletal diseases, and urinary incontinence (UI), are risk the risk factors for falls in the older adults [22]. Muscular atrophy Sarcopenia is another key factor that limits stability control and is more likely to occur in old age people that cause serious injuries, and premature mortality[23]. Commonly identified home hazards that increase the fall risks in elders were home access, i.e., movement around the house, slippery floors, and bathroom-related falls [15, 17, 20]. Fear of falling even without any fall history is another factor of falls in elders. This fear may restrict their activities, and ultimately, they adopt an inactive lifestyle [24]. The use of some drugs, such as psychotropic and antidepressant drugs, can cause drowsiness and impaired coordination and balance; antihypertensive and ant-allergic drugs can lower blood pressure; beta-blockers and diuretics might cause postural hypotension and may cause falls. Anticholinergic medications may impair cognitive function and cause blurred vision, increasing the risk of falls in older adults [17, 22].
Identifying older adults who are at higher risk of falling and require interventions is challenging for clinicians and public health professionals. However, various fall predictors and scales are developed and tested to assess fall risk among elders. Age categories, gender, measures of gait (TUGT), disability index, CDC fall risk assessment 12-point checklist [25], and environmental hazards were some of the highlighted fall risk assessment tools, mentioned in the previous studies(5). Lusardi et al. included the Mini-Mental State Examination in their predictive model for predicting fall risk. Another review created a comprehensive list risk factors assessment [17] in which TUGTS, visual health, and cognitive scores were highly predictive factors. Oshiro et al used psychological and medical characteristics, medication use, and sensory factors to forecast fall risk [26] in which a positive prediction was found between adjusted variables and fall risk of 98%, and a negative predictive value of 8%.
1.1. Predictive models for fall risk assessment
It was difficult to generalize previously constructed model to assess fall risk in Pakistani community dwelling older adults [27]. Fall literature is in debate, whether fall predictions through different models are feasible; such as modifiable factors of falls can be reduced through new interventional strategies. A study conducted by Thurmon and fellows developed a predictive model, namely Random Forest predictive Model, evaluated fall risk in 171 community-dwelling older adults performed 10 meters walk daily, and fall frequency in the six months were followed through a sensor detection of movements. Linear and nonlinear modeling identified that 19% of elders who reported falls in the six months follow-up were had gait problems [27]. A systematic study carried out to examined all prognostic predictive models of fall risk included 30 (out of 86 369 individuals). Only three validated prediction models were reported in the included research, and the frequency of falls ranged from 5.9 percent to 59 percent in approximately 69-designed models. The most common predictors of falls were prior falls, age, gender, assessments of gait quality, walking balance, visual health and level of disability. The range of the area under the curve was 0.62 to 0.69 [17]. Fall prediction models mostly incorporated gait quality scores, cognitive status, and past fall experience. Mishra et al. conducted a study in the USA and developed a model to predict 6-month fall risk using the geriatric TUGT, MMSE, and fall history from 92 older adult residents (age = 86.2 6.4, female = 57). With an AUC of 0.80 (95% CI of 0.76-0.85), and a sensitivity of 0.82 (95% CI of 0.74-0.89) predicting the six-month risk. The activity daily living (ADL) assessment scores, and gait speed were the three most significant contributions to the comparatively increased fall risk in elder’s population. Different approaches were used in the literature to test and evaluate the predictive factors such as decision-tree analysis, fall-prediction algorithm[14], logistic regression, receiver operator characteristics (ROC) analysis, and prognostic model for fall risk screening in the previous studies [28]. However, these six predictors were able to stratify fall incidence, and probabilities that ranging from 30.4% to 71.9%. The decision-tree model in terms of the area under the curve (0.70 vs. 0.64), accuracy (0.65 vs. 0.62) were performed, sensitivity (0.62 vs. 0.50), positive predictive value (0.66 vs. 0.65), and negative predictive value (0.66 vs. 0.65) in the predictive models. There are different predictive models the researchers developed for fall prediction in old age and it is concluded that there is no any model to adopt for fall prediction in all context. Considering this background knowledge and inconsistent literature, information related to falls associated factors and fall risk assessment strategies, there is a need to develop a new fall predictive model for Muslim elders in Pakistan.
1.2. Study Contribution
Fall risk is contextual; more researches are required to identify different risk factors of falls' occurrence among elders living in the community. Older persons in the Pakistani community must therefore undergo routine fall risk assessments in order to create a fall prevention strategy. We, therefore, aim to explore the risk factors related to falls in elders in Khyber Pakhtunkhwa, Pakistan, where 99% of the population belongs to the Muslim community. Our study can help identify new risk factors for falls, so we plan to develop a predictive model to assess fall risk among community-based elders to determine preventive strategies for falls in the elder population.
2. Materials and Methods
2.1. Design and setting
Data was taken from the baseline data of an interventional study at two residential areas of Peshawar district, Khyber-Pakhtunkhwa, Pakistan from July 2022 to August 2022. Different measuring check lists were used such as Mini mental health status examination(MME), Time Up and Go(TUG), and different demographic characteristics, including five questions regarding body movements in five-time prayers from the 140 study subjects were selected for a random control trail study. The sample size were calculated using G-power by assuming 0.05 level of significant that is Alpha (α), power of test (i.e. Beta=0.8, as beta set at 0.20 that is chances of falls negative and 95% confidence level. This sample size was acceptable to develop a model for at least five hypothetical predictors with one dependent variable.
2.2. Inclusion and exclusion criteria
The inclusion and exclusion criteria were followed as the subjects had to be 60 years of age or older with sedentary life style that is <two hours activity in 24 hours, with normal to moderate cognitive functioning, able to follow instructions, and able to walk without taking assistance from another person. The language barrier, unwillingness to participate, and non-registered elders were excluded from this study.
2.3. Ethical considerations
The Helsinki Declaration of 1964 was followed. Permission was taken from the parent institution that is Zhengzhou University, Institute of Ethical Review Board (ZZUIERB #202254) , and the District Health Department Office (DHO #14207).
2.4. Data collection process
Data were collected through validated and reliable checklists approved by the Centers for Disease Control and Prevention (CDC), which is TUGTS scores as walking speed in 3 meters of distance, Mini Mental Examination checklist, five questions regarding prayer technique and procedure, and questionnaires containing information on demographic variables were collected in the interview section. Figure 1 shows the brief process of data collection.
2.5.1. Physical test
The Time Up and Go test was performed in three basic healthcare units (BHUs) in Peshawar. A trained physiotherapist conducted the timed "Up and Go" test (TUGT), in which scores were assigned to go and sit down for which 10 to 19 seconds were considered normal, 20 to 29 on the gray list included in fall risk, and >30 dependent was considered highly risky for falling[29]. The time that a participant needs to rise from a chair, walk 6 meters, turn around, walk back, and sit down on the chair was recorded. During the test, the person is instructed to wear her or his regular, comfortable footwear and use any mobility aids (e.g., a cane or frame) that they would normally require.
2.5.2. Mini Mental Examination
Mini Mental status Examination checklist were used to check cognitive level of participants. The checklist is consisted of 10 scores in which Scores > 4 with no answered considered risk for fall in this study.
2.5.3. Proper posture during five time prayers
Five questions were asked from the participants regarding Muslim five time prayers by considering the seven distinct body postures which are 1) Takbir; 2) standing;3) Rukuk;4) Qiam ; 5) Prostration;6) sitting(Jalsa);7) moving head to right and left. We considered > 5 correct answers for correctly perform prayers in this study.
2.6. Statistical Analyses
Using Statistical package of science (SPSS version 23). Descriptive statistics and the Spearman correlation coefficient test were used to describe and associate factors concerning falls' occurrence in the last year at a significant level of (P.0.05). A binary logistic regression model was used to test the hypotheses of this study, which were: 1) H1. Fall is higher in those with low-speed walking; 2) H2. The falling ratio is high with regard to visual and cognitive problems. The data were checked for normality. The distribution of the feature significance values for each feature was assigned. For instance, lower gait speed values, poor prayer postures; poor cognition scores were hypothetically negatively correlated with fall risk.
The area under the curve was measured to check the sensitivity and specificity of the model under study, and if we kept >75% of the test, it will be considered valid and reliable to check the fall's occurrence with the selected parameters.
2.6.1. Model fit index
In this model, we considered one to indicate a fall risk and zero to indicate no falls risk. Our preferred choice is one because we are interested in seeing the drops in respondents. Zero is given a benchmark as it is significant at 0.03 and shows that when we add an independent variable, it will predict the dependent variable in our model. We applied the Omnibus model of coefficient testing considering the difference between the baseline model and the new model, the Nagelkerke (R2) square >0.50, the pseudo-R square to check the approximate variation in the criterion variable were adjusted for Cox and Snell R, that is, Nagelkerke R2 >0.50 in the criterion variable can be accounted for in the predictive variable. Receiver operating characteristic (ROC) curves and logit rank plots of each variables in the models were plotted to help concluded the list of critical measures from those discovered through binary regression modeling method.
2.6.2. Sensitivity and specificity analysis:
Using ROC the standard errors for the areas under the ROC curve were determined in SPSS, version 23. For each sample participant, the projected probability—calculated as elogit (p)/(1 + elogit(p)), where logit(p) is the indicator derived from the regression model was also analysed. The specificity of the model was assumed that the Receiver Operator Characteristic (ROC) with >75% AUC accurately measures the membership of independent variables on fall risk. We considered that the model correctly predicted not to fall risk, and the model sensitivity ROC > 75% was assuming that the model correctly predicting to fall risk is due to the selected variables. The cut off point for TUGT was =<15 seconds, cognitive function =<5 scores, prayer method=1, and visual function=1. We transformed the numerical data into dichotomous data that is 1 for fall risk, and 0 for no fall risk to check the validity of the tested variables in binary regression model. The equation model in which Odd Ratio that is probability of (A) P (B) in which we interpreted that which independent variable is significantly affect fall or not falls. The beta coefficient values (Exp.b) >1 was considered cutoff point to indicate more probability of the selected outcome occurrence that is no falls or falls in the model in the relationship with the predictive variables.
2.6.3. Validity of the proposed model
The validation research was carried out to assess the discriminating validity of the model by plotting ROC curves for the 30% of subsamples. By analyzing the differences between the areas under the two curves, the calibration validity of a model was established. It is necessary to ascertain whether the predicted probability obtained for subsample, and using the models created agrees with the observed probabilities of model 2.
3. Results
The demographic features, cognitive status, and TUGT level of the participants were assessed. The average age of the study participants was 68.1 + 5 years (ranging from 60 to 82 years old). When education level is taken into account, 42% of the participants were illiterate, and only 14% are recorded as graduates; more than half (54% of the participants in this study were female). Cardiovascular diseases were common (31%), the majority (52% in the extended family system), and most of them were financially dependent on other family members, which is 38%. More than half, or 51%, of the study participants reported at least one fall in the last year. Prayer Body Movements accounted for 32% of those who did not complete all seven steps of body movements due to health issues or personal preference. The cognitive level of the study participants was 47% moderately affected, and only 53% had active memory in this study. Elders in this study had poor vision, as 66% reported having a visual problem.
3.1. Falls reports
The majority of the participants were belong to Pathan tribe that is (40%) in this study. Female participants (44%), as well as those aged 65 to 70 years, reported more falls. In this study, 42% were illiterate, 59% had a spouse who was alive, 59% had another source of income, 56% lived in an extended family system, 93% had a joint problem, 75% had a visual problem, and 71% did not follow body movements in prayer.(see Table 1)
3.2. Factors associated with falls occurrence
There was a significant relationship between income level and education, health, and age as scores ranged from >70 to 0.90. Visual health and age are also correlated with scores > 0.70. In our study, health, status, gender, and living status did not show any significant association (P >0.005) in all mentioned variables. The significant value of moderately low cognitive status and poor vision was associated with a fall history (P.0.001). Visual health and age are also correlated with scores > 0.70%. In our study, health, status, gender, and living status did not show any significant association (P >0.005) in all mentioned variables. The significant value of moderately low cognitive status and poor vision was associated with a fall history (P.0.001). Details of demographic data and risk factors are displayed in Table 1.
In Table 1 the frequency of fall is higher in female as compare to male, age group of 66 to 70 years are more reported falls as presented the data in percentages in descriptive statistics. The figure shows that female participant’s reported falls were (44%), and age group 65 to 70 years (43%) reported history of falls in this study.
3.3. Binary Logistic regression Model
The goodness of the model shows significance (P. 0.001). Age, gender, economic status, education status, health status, and ethnicity were removed from the model as they were non-significant (p > 0.005) in the Omnibus Chi-square test and the Hosmer and Lemeshow test. TUGT level, cognitive status, poor visual equity, and proper body movement in prayers were good fits of the model, as the chi-square test values of each variable in the area model were statistically significant at (P.0.05) and 94% in the Hosmer test. The variation in the criterion variable is significant, as the pseudo-R square of the approximate variation in the criterion variable through the adjusted versions of Cox and Snell R and Nagel-kerke R shows a 77% change in the fall risk can be accounted for by the predictive variables in this study. Our model correctly predicted that fall risk using 81.3% of the selected variables. Results are displayed in Table 2, and the AUC in the ROC shows the high sensitivity and specificity of our hypothetical testing variables in the relationship with fall risk in this study.(See Figure 2).
3.4. Model predictive value
To find the predictive values in our model, we analyzed the equation model in which the beta coefficient Exp (b) value is greater than 1, indicating a higher probability of the selected outcome occurring. Three independent variables, such as cognitive function, TUGT level, and poor vision, were found to predict fall risk in the elderly in this study. The log Odd of TUGT is 2.29 times more likely to fall as the Exp (b) value is (L = 1.11, U = 439.78). Elders' cognitive level is slightly poorer than expected to predict the fall occurrence with Beta value B (2.49) in Exp. b (95%) with Value (0.052), lower (0.65), and upper (4.59) but still needs to be considered in future studies to avoid being neglected. The prayer method predicts the fall's occurrence five times more with (P. 0.004) and Exp (b) = 5.19. In our model of prediction, the vision scores are highly significant for the probability of fall occurrence (P.0.001). Table 3 and Figure 3 present the data of the Odd Ratio with hypothetical variables.
Table 2.
Model of fit analysis under Binary Logistic regression analysis of predictive variables.
Table 2 In this table the model shows best fit in Omnibus test(P.<0.005),, Hosmer&Lemeshow likelihood value greater than 0.50 that is .0.77 in NagelkerkeR square indicated that our model is good fit with overall 80% validity and reliability scores. This results indicates that poor vision, lack of physical movement, poor gait and walking ability in TUGTs 3 meter walking test for 12 seconds, low cognition in the scale of 10 points are showing the significant of the model appropriateness and can be adopted in future fall risk assessment.
Figure 2.
Probability of fall occurrence with the hypothetical predictors in the Equation Model. N=140.
Figure 2.
Probability of fall occurrence with the hypothetical predictors in the Equation Model. N=140.
Figure 2. The model is predicting the probability of fall due to the tested variables in this study as the Odd Ratio (Exp(b) of all variables in the Equation model are >1 as TUGT=2.29, Cognitive scores=2.4, Visual=2.1 and not move the body during prayer=5.1. When the score is <1 it means that the model does not show any probability of falls in the future.
Table 3.
Odd Ratio of fall risk with the membership of the predictive variables such as TUGT, cognitive level, Poor vision, and prayer method in the Equation model. N=140.
Table 3.
Odd Ratio of fall risk with the membership of the predictive variables such as TUGT, cognitive level, Poor vision, and prayer method in the Equation model. N=140.
Figure 3.
Receiver operating characteristic curve of the four predictive variables.
Figure 3. Receiver operating characteristic curve was generated for all the variables to discriminate elders with falls and no falls. The total area under the curve is representing the sensitivity, and specificity of the tested variables. The total area covered for lack of body movement in prayers is (82%), poor cognitive status(80%) area covered with 95% confident interval,(3) poor vision (>85%), and(4)TUGT level >85% correctly specified the accuracy of the testes factors in this model in the membership with fall risk in the study participants. The area under the curve (AUC) of this study model is shown in graphical lines of sensitivity and specificity of the test variables in which all the lines of four variables are moving from left to right with the top point of > 80 % which is near 1. The model is 80% correctly predicting that variables are correctly predicting falls risk in elders.
- External Validity of the Model
The AUC in the ROC in the randomly selected testing sample from the proposed model. Figure 4 of ROC is showing AUC of the testing sample which is supporting that this model is >80% valid and reliable and the chance of occurrence is not over fitted in the model. We are confidents to support our model risk factors can be assessed in elder of Pakistan with the same ethnicity and geographical location. The AUC in ROC is greater than 70% of the area above the straight line and falling from left side to over right side indicated that this model is not over predicting the fall risk in elders due to by chance of factors(see Figure 4 and Figure 5).
Figure 4. Figure of ROC is showing AUC of the testing sample which is supporting that this model is >80% valid and reliable and the chance of occurrence is not over fitted in the model. We are confidents to support our model risk factors can be assessed in elder of Pakistan with the same ethnicity and geographical location. The AUC in ROC is greater than 70% of the area above the straight line and falling from left side to over right side indicated that this model is not over predicting the fall risk in elders due to by chance of factors.
Figure 5.
Validity of the model with Odd Ration with sample of 30% of the total.
Figure 5. The Odd ratio of the testing sample is greater than 1 in the graph which is showing a high probability of fall occurrence in the study population. The significant value of all four independent variables is significant predictors (P.<0.0051) displayed in the figure. This figure shows the external validity of the model for which we randomly selected 30% of the sample considering it a testing sample and the 70% sample considered a training sample. The binary logistic regression shows Odd Ratio with exponentiated beta (Exp.b) >1 in each of the variables.
4. Discussion
Our purpose in this study was to propose a model to predict fall risk among community dwelling older adults with sedentary lifestyles in Khyber Pakhtunkhwa, Pakistan, using the TUG checklist, MMSE scores, body postures in five time Muslim prayers scores, visual health assessment scores, and fall history. In the demographic data, the average age of the study participants was 68.1 + 5 years (ranging from 60 to 82 years old), and the majority of the participants were 65 to 70 years old in this study, which is similar to the previous study carried out in Faisal Abad, Pakistan[8]. The difference in the age distribution was not a surprise to us because older adults under the age of 60 to 65 typically have a lower risk of falling due to involvement in physical activity lasting longer than two hours daily. Similarly, older adults over the age of 75 mostly become dependent on others for daily living activities due to deteriorating health conditions and disabilities, which limited their ability to participate in this study [9, 22]. When education level is taken into account, 42% of the participants were illiterate, and only 14% are recorded as graduates; more than half, or 54%, of the participants in this study were female. Our results are incompatible with studies carried out in other countries in which education status is high among older adults[14, 30].Education plays a mediating role in preventing falls, ,and education was one of the super variables that negatively affected fall prediction in the previous studies[26]. We believe that education provides opportunities for older adults to live a safe and secure life in old age [31].
Prevalence of fall occurrence: The fall frequency among the study participants in this study was 55% which is quite high compared to previous studies, as the frequency was 44% in a study conducted in Pakistan [8]. The frequency of falling was low, with only 18% of more than one time falling history in the Chinese older adult’s population [14]. But the result was quite similar to a study in Taiwan, in which the frequency of falling was 33% among community-dwelling older adults [32]. In our study, the frequency of falls was much higher among the age group of 65 to 70 years, which is inconsistent with a Brazilian study in which adults >75 years reported more falls[4]. This can be a reason for the lack of risk assessment, the low literacy rate, and the lack of an elder hood awareness program in Pakistan [33].
Associated factors of fall occurrence: We conducted an analysis to forecast older adults' fall risk and risk factors for falls in older adults. Some of the highlighted risk factors in our study were walking speed, poor cognitive level, lack of body movements in five-time prayers, and low vision. 65 to 70 years of age, illiteracy, and being female were some of the risk factors correlated with fall experiences among our study participants. Our findings were contradicted by a study conducted in the United States of America in which medication and fear of falling were more prominent risk factors for falls in older adults [34]. Similar risk factors may not have been observed in other studies because of the multifactorial nature of fall occurrence. However, in our study, the population belonged to only the Muslim community, so the lack of prescriptive body movements in the five times of prayers was one of the prominent factors contributing to the fall risk. In this study, complaints of poor vision, poor walking speed, and low cognitive ability were significantly correlated with history of falls. The same factors were identified in the previous study, in which these factors were associated with a history of falls and 50% of fall risk in elders living in the community of Pakistan [8], but in our study, lack of body movement in prayers was a newly added risk factor significantly correlated (P = 0.04) with fall occurrence. Our result is similar to another study conducted by Makino, et al. in which poor cognition, and visual problems were highlighted as factors responsible for falls in older adults [14]. Some of the risk factors in our study are also similar to those in the Brazilian study, in which sociodemographic traits, vision impairment, and cognitive impairment were associated with fall risk[4],but surprisingly, the age group > 75 years old was a higher risk group for falling in that study, which contradicts our results. Gender, being female, was more associated with a high risk for falls (P = 0.05) in our study, which is consistent with the Brazilian study, where females reported more fall occurrence [20]. Female participants were also more at risk in another study conducted by Khatak et al., in which females constituted 32% of the overall fall prevalence [13]. According to other research, women have a higher tendency to fall than men do, and this difference can be attributed to women's physiological differences in bone and muscle structure, menopausal hormone changes, and multitasking. In Pakistan, there is a male dominant culture; however; females have limited opportunities to participate in physical activities. In this study identified some of the protective factors for fall occurrence, such as gender as manhood, being literate with a graduation level, and proper body movement in five-time prayers with prescribed body motion which were significantly associated with non-fallers group with (P=<0.05). This finding was consistent with the Adriana, et al. study in which education, being a male and social support were protective factors to prevent falls in older adults [4]. Poor gate was significantly correlated with fall risk with P=<0.05) in our study. The same findings were observed in a study carried out in the USA on 92 elders in which poor scores in cognitive status, medication-related drowsiness, poor gait, and balance were highly correlated with falls [34]. Although this study has focused on sociodemographic, contextual, intrinsic, and behavioral factors of falls and gait speed assessment, the way of five-time prayers should also be given priority because of the likelihood that these events will occur as a result of a lack of exercise, especially in women of Pakistan. Hence, this model might be a useful tool to distinguish between elderly people living in Muslim communities in Pakistan who are at high risk of falling and those who are not at risk. Healthcare professionals could incorporate our model to assess and screen the identified risk factors in the general population to take the necessary action to prevent fall risk in elders in Pakistan.
Validity of the model: Our model is good fit by its internal validity. The Nagelkerke R Square is 52% to 77%, which is well supporting to predict that the variables, such as poor cognitive level (scores >7 in the total 10 point scale); poor vision; gait problems (taken >15 seconds in a 3 m distance walk); and lack of seven-style body movement in prayers, are good fits on the fall risk. The coefficient Ex (b) of the independent variables shows a value of >1 in each predictive variable, such as TUGT (2.290), cognitive health (2.491), visual health (2.121), and prayer body movements (5.193). In terms of the components of our model, other studies have demonstrated a connection between older persons' fall histories, poor cognitive scores, TUG, pain, and age group with the falls of older adults. Hence, the items we selected for our binary regression model analysis corroborated this finding with different models, such as the simplified decision-tree algorithm model [14], and the SHapley Additive exPlanations model[34]. The binary regression model is a logistic regression model that can be used to reveal stratified relationships between fall predictors and subsequent fall risk. It includes TUG, cognitive problems, lack of body movement in prayers, and poor vision in an importance-based ordering of predictors. TUG is located at the top of the ROC graph. Poor gait speed is the most influential predictor and is recommended to be assessed to predict falls in the future. Therefore, we believe that the structure of our model is valid. Additionally, our model calculated the optimal cut-off point of TUG as 10 for fall prediction. Regarding the cut-off point of TUG for falls, the >15 previously reported [30] and has been widely used. Our cut-off point was 15 s, which is relatively more power to include all high-risk older adults. The TUG cut-off point should be set faster for older people living independently in the community. The binary regression model outperformed the logistic regression model in terms of AUC, accuracy, sensitivity, probability, and odds ratio, making it suitable for use as a primary screening tool for fall risk. Our model is well supported by Mishra’s study, in which the model supported most of the variables in our model to assess fall risk in older adults [34]. The external validity was checked with randomly selected data from the model. We split our data into two groups: 70% of training data and 30% of testing data from the 140 samples collected through a random sampling method. The testing model >70% accurately tested that the primary model was a valid model as the odd ratio Exp (b) of each variable is >2, with P = 0.01) which supports that our model is valid [35]. The fall risk model can provide guidance to health providers to focus on specific factors of fall risk instead of analyzing individual assessments.
5. Conclusions
Falling is multifactorial; we cannot claim one factor is not responsible for falls in elders. To provide information on prevention and the identification of seniors at risk, multidisciplinary expertise is necessary, which justifies the need for this study. Vision impairment, cognitive impairment, poor gait, and prayers without body motions were the variables linked to the probability of falls in the binary logistic regression model. Therefore, this study could facilitate community health nurses and public health workers including these predictors in their fall risk assessment tools to provide appropriate fall prevention strategies for Muslim elders in Pakistan.
Study limitations
The study does have certain limitations. The data were taken from baseline data of a randomized control trial study; therefore, the data is retrospective. In addition, future analysis with more predictor variables and prospective studies could potentially improve the results, but they could not be applied to other older adult populations. To support the threshold values of the variables in our model, additional longitudinal studies are required. A fall risk assessment checklist, the Berg balance test, certain medications, a sleep quality assessment, and nutritional status can be added in future studies.
Future Implications
This study's model was constructed using a new factor, which can be further examined in randomized control trials. While we think this can be applied successfully to forecast fall risk in Peshawar and in other Muslim populations that are similar, Our study provides valuable information on future predictors; therefore, selecting factors for the prediction model, a literature review, and clinical experience are often used to prevent bias in predictor selection. It is essential to examine the external validity of the developed model in the general population to determine the stability of the model across various populations.
Author Contributions
Conceptualization=Zhang Yan, Rashida Bibi, 2. Methodology: Rashida, Nasar Mian, Data analysis, Rashida, Akhter Zeb, Nasir Anwar, Data collection, and writing literature review; Rashida, Akhter Zeb, Nasar Mian; Wring manuscript: Rashida, Zhang Yan. All authors have read and agreed to the published version of the manuscript
Funding
This research received no external funding.
Institutional Review Board Statement
Permission was taken from the parent institution (ZZUIRB #202254) to conduct this study in the community and from the local health department of Peshawar.
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
All the data is secured and available from the corresponding authors. The corresponding authors may provide the data on the demand of the journal.
Acknowledgments
We are very thankful to Dr. Abdul Razzaq, Department of Ocean Technology and Engineering, Ocean College, Zhejiang University, China, for his untiring guidance and facilitation in developing this paper. We also acknowledge Dr. Yorozoya, a professor at the School of Nursing in Tokyo, Japan, for her time to revise and provide feedback, and we would like to extend our sincere gratitude to Mike, a postgraduate student at Zhengzhou University, China, for his technical expertise. We are grateful to the health department of Khyber Pakhtunkhwa for facilitating this study by permitting the lady health care workers to participate. We are thankful to the research team that carried out the assessment and collected data from the participants.
Conflicts of Interest
The authors declare no conflict of interest.
References
- WHO, “Active Ageing: A Policy Framework,” Act. Ageing Policy Fram., vol. 5, 2002.
- A. Tu-Allah Khan, R. H. Toor, and Q. Amjad, “Assessment and Management of Geriatric Care in Pakistan,” J. Gerontol. Geriatr. Res., vol. 07, no. 05, 2018. [CrossRef]
- A. M. Briggs et al., “Musculoskeletal Health Conditions Represent a Global Threat to Healthy Aging: A Report for the 2015 World Health Organization World Report on Ageing and Health,” The Gerontologist, vol. 56, no. Suppl 2, pp. S243–S255, Apr. 2016. [CrossRef]
- A. de A. Smith, A. O. Silva, R. A. P. Rodrigues, M. A. S. P. Moreira, J. de A. Nogueira, and L. F. R. Tura, “Assessment of risk of falls in elderly living at home,” Rev. Lat. Am. Enfermagem, vol. 25, no. 0, 2017. [CrossRef]
- AKUH, Board on Health Care Services, Health and Medicine Division, and National Academies of Sciences, Engineering, and Medicine, Families Caring for an Aging America. Washington, D.C.: National Academies Press, 2016, p. 23606. [CrossRef]
- P. R. Baker, D. P. Francis, N. N. Hairi, S. Othman, and W. Y. Choo, “Interventions for preventing abuse in the elderly,” Cochrane Database Syst. Rev., Aug. 2016. [CrossRef]
- WHO, “Global Burden of Disease Stud,” 2020. Available: https://www.who.int/health-topics/noncommunicable-diseases.
- M. Mehmood, M. Mushtaq, N. Ansa, and A. Jilani, “Prevalence of Risk of Fall in Community Dwelling Pakistani Male Population over the Age of 65 years,” J. Nov. Physiother., vol. 6, no. 5, 2016. [CrossRef]
- K. Makino et al., “Simplified Decision-Tree Algorithm to Predict Falls for Community-Dwelling Older Adults,” J. Clin. Med., vol. 10, no. 21, p. 5184, Nov. 2021. [CrossRef]
- M. J. Faber.et.al, “Effects of Exercise Programs on Falls and Mobility in Frail and Pre-Frail Older Adults: A Multicenter Randomized Controlled Trial,” vol. 87, no. 7, pp. 885–8896, Jul. 2006. [CrossRef]
- Centers for Disease, Control and Prevention, National Center for Injury, and Prevention and Control, “Stay independent and learn more about fall prevention,” 2017. Available: https://www.cdc.gov/steadi/.
- World Health Organization . WHO, . “global report on falls prevention in older age. Ageing, Life Course Unit, World Health Organization,Geneva,”2008. Available: https://www.who.int/publications/i/item/who-global-report-on-falls-prevention-in-older-age.
- Bachani, A.M., Ghaffar, A. & Hyder, A.A, “Burden of fall injuries in Pakistan - analysis of the National Injury Survey of Pakistan.,” EMHJ - Eastern Mediterranean Health Journal, vol. 17, no. 5, pp. 381–375, 2011.Available: https://apps.who.int/iris/handle/10665/118627.
- H. G. Khattak, H. Arshad, K. Anwar, and Y. Majeed, “Fall Prevalence and Associated Risk Factors in Geriatric Population,” Pak. J. Med. Health Sci., vol. 15, no. 9, pp. 2161–2164, Sep. 2021. [CrossRef]
- M. Yamada and et al, “2010 Oct;58(10): Trail-walking exercise and fall risk factors in community-dwelling older adults: preliminary results of a randomized controlled trial,” Am Geriatr Soc ., vol. 58, no. 10, pp. 1946–51, Sep. 2010. [CrossRef]
- G. Agarwal and M. Brydges, “Effects of a community health promotion program on social factors in a vulnerable older adult population residing in social housing,” BMC Geriatr., vol. 18, no. 1, p. 95, Dec. 2018. [CrossRef]
- Deandrea and et al, “Risk factors for falls in community-dwelling older people: a systematic review and meta-analysis.,” Epidemiology., vol. 21, no. 5, pp. 658–68, 2010. [CrossRef]
- L. Z. Rubenstein, “Falls in older people: epidemiology, risk factors and strategies for prevention,” Age Ageing, vol. 35, no. suppl_2, pp. ii37–ii41, Sep. 2006. [CrossRef]
- Ken Y. T., Christina W. Y., and Hui.Zhan, “The effects of practicing sitting Tai Chi on balance control and eye-hand coordination in the older adults: a randomized controlled trial,” Disability and Rehabilitation, vol. 37, no. 9, pp. 790–794. [CrossRef]
- T. Liu-Ambrose et al., “Action Seniors! - secondary falls prevention in community-dwelling senior fallers: study protocol for a randomized controlled trial,” Trials, vol. 16, no. 1, p. 144, Dec. 2015. [CrossRef]
- Tzuo-Yun Lan 1, David Melzer, Brian D M Tom, Jack M Guralnik and et al, “Performance tests and disability: developing an objective index of mobility-related limitation in older populations,” J Gerontol A Biol Sci Med Sci, vol. 57, no. 5, pp. 294–301, May 2002. [CrossRef]
- Phelan, E. A., Mahoney, J. E., Voit, J. C., & Stevens, J. A., “Assessment and Management of Fall Risk in Primary Care Settings,” The Medical clinics of North America, vol. 99, 2, 2015. [CrossRef]
- Power, Brian H, and Dalton b, “Human neuromuscular structure and function in old age: A brief review Author links open overlay panelGeoffrey,” Journal of Sport and Health Science Volume, vol. 2, no. 4, pp. 215–226, Dec. 2013. [CrossRef]
- G. Bernardelli, C. Roncaglione, S. Damanti, D. Mari, M. Cesari, and M. Marcucci, “Adapted physical activity to promote active and healthy ageing: the PoliFIT pilot randomized waiting list-controlled trial,” Aging Clin. Exp. Res., vol. 31, no. 4, pp. 511–518, Apr. 2019. [CrossRef]
- (Rubenstein et al, “This checklist was developed by the Geriatric Research Education Clinical Center and affilia tes and is a validated fall risk self-assessment tool Res; 2011: 42(6)493-499),” vol. 42, no. 6, pp. 493–499.
- Oshiro and et al, “Fall ascertainment and development of a risk prediction model using electronic medical records.,” J Am Geriatr Soc, vol. 67, no. 7,p. 1417–2, 2019. [CrossRef]
- T. E. Lockhart et al., “Prediction of fall risk among community-dwelling older adults using a wearable system,” Sci. Rep., vol. 11, no. 1, p. 20976, Oct. 2021. [CrossRef]
- S. Buchman and et al, “Physical Activity and Leg Strength Predict Decline in Mobility Performance in Older Persons,” J Am Geriatr Soc, vol. 55:, no. 10, pp. 1618-1623, 2007. [CrossRef]
- T. J. Klotzbier, H. Korbus, B. Johnen, and N. Schott, “Evaluation of the instrumented Timed Up and Go test as a tool to measure exercise intervention effects in nursing home residents: results from a PROCARE substudy,” Ger. J. Exerc. Sport Res., vol. 51, no. 4, pp. 430–442, Dec. 2021. [CrossRef]
- Huang HC, Liu CY, Huang, and YT, Kernohan WG, “Community-based interventions to reduce falls among older adults in Taiwan - long time follow-up randomised controlled study.,” J Clin Nurs., p. 19:959-68, 2010.
- B. M. Chaudhry, D. Dasgupta, and N. V. Chawla, “Successful Aging for Community-Dwelling Older Adults: An Experimental Study with a Tablet App,” Int. J. Environ. Res. Public. Health, vol. 19, no. 20, p. 13148, Oct. 2022. [CrossRef]
- S. Roberts et al., “Ageing in the musculoskeletal system: Cellular function and dysfunction throughout life,” Acta Orthop., vol. 87, no. 363,p. 15–25, Dec. 2016. [CrossRef]
- M. Tousignant, H. Corriveau, P.-M. Roy, J. Desrosiers, N. Dubuc, and R. Hébert, “Efficacy of supervised Tai Chi exercises versus conventional physical therapy exercises in fall prevention for frail older adults: a randomized controlled trial,” Disabil. Rehabil., vol. 35, 17, pp. 1429–1435, Aug. 2013. [CrossRef]
- M. Osama, R. Malik, and S. Fiaz, “Salat (Muslim prayer) as a therapeutic exercise,” J. Pak. Med. Assoc., vol. 69, no. 3, p. 1, 2019. [CrossRef]
- Jon Pynoos, Anna Q D Nguyen and et al, “Fall risk in older adults: roles of self-rated vision, home modifications, and limb function Bernard A Steinman,” J Aging, vol. 21, no. 5, pp. 655–76, Aug. 2009. [CrossRef]
- A. K. Mishra et al., “Explainable Fall Risk Prediction in Older Adults Using Gait and Geriatric Assessments,” Front. Digit. Health, vol. 4, p. 869812, May 2022. [CrossRef]
- Jian Wang, 1 Xiuqin Chen, 2 Xiaoming Sun, 3 Huifen Ma, 2 Yan Yu, 4 Chunxia Yao, 2 Zhipeng Li, 5 Limei, “The Application of ‘Timed up and Go’ Test in Fall Screening of Elderly People in Shanghai: A Cross-Sectional Study Jian,” Iran J Public Health, vol. 50, no. 12, pp. 2567–2575, Dec. 2021. [CrossRef]
- F. Saqib Lodhi, O. Raza, A. Montazeri, S. Nedjat, M. Yaseri, and K. Holakouie-Naieni, “Psychometric properties of the Urdu version of the World Health Organization’s quality of life questionnaire (WHOQOL-BREF),” Med. J. Islam. Repub. Iran, vol. 31, no. 1, pp. 853–859, Dec. 2017. [CrossRef]
Figure 1.
Step by step process for falls risk assessment of study participants=140.
Figure 4.
Validity of the Model AUC in the ROC in the randomly selected testing sample from the proposed model.
Figure 4.
Validity of the Model AUC in the ROC in the randomly selected testing sample from the proposed model.
Table 1.
Demographic characteristics, fall frequency, and risk factors of fall occurrence.
| Demographic Variables .N=140 | Total# | Fall history | P.Value | ||||
|---|---|---|---|---|---|---|---|
| % | yes% | No % | |||||
| Gender | Male Female | 46% 54% |
33% 44% |
46% 56% |
0.49 | ||
| Age | 60-65 66-70 71-75 |
46.40% 14.30% 4.30% |
33% 44% 16% |
67% 56% 84% |
0.04 | ||
| >76 | 8.57% | 33% | 67% | ||||
| Education level | Graduate Matric Secondary | 14% 22% 17% |
14% 22% 20% |
86% 78% 80% |
0.021 | ||
| Illiterate | 47% | 42% | 58% | ||||
| Married | Alive Widow |
79% 21% |
59% 41% |
42% 59% |
0.012 | ||
| Source Income | of | Pension Others No, any source |
28% 34% 38% |
57% 59% 48% |
43% 41% 52% |
0.62 | |
| Health status | Cardiovascular Diabetic Joint Pain |
30.70% 22.00% 20% |
51% 21% 93% |
49% 58% 7% |
0.72 | ||
| Other | 4.30% | 33% | 67% | ||||
| No diseases | 9.30% | 46% | 54% | ||||
| Living status | Join family Extended Family |
47% 52% |
54% 56% |
46% 44% |
0.45 | ||
| Visual problem | yes No |
52% 47% |
75% 33% |
25% 67% |
0.002 | ||
| Prayer practice | five-time prescribe | as | 48% | 37% | 63% | 0 | |
| not proper way | 52% | 71% | 29% | ||||
| Ethnicity | Pathan Panjabi Sindhi |
0.4 0.3 0.2 |
58% 47% 28% |
42% 53% 60% |
0.51 |
||
| Chitrali 8% | 0.1 | 21% | 54% | ||||
| Cognitive level | Normal Moderate |
54% 47% |
45 64% | 55% 36% |
0 | ||
| severe | 0% | 7.9 | |||||
| <12 seconds | 48% | 31% | 69% | ||||
| TUGT level | 12-14 seconds | 28% | 64% | 56% | 0.001 | ||
| >14 seconds | 24% | 90% | 10% | ||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.
Prevalence and Associated Factors of Falls among Older Adults between Urban and Rural Areas of Shantou City, China
Xiaodong Chen
et al.
IJERPH,
2021



MDPI Initiatives
Important Links
© 2024 MDPI (Basel, Switzerland) unless otherwise stated