
Submitted:
03 May 2023
Posted:
05 May 2023
You are already at the latest version
Abstract
Inflammatory bowel disease (IBD), comprising Crohn's disease (CD) and ulcerative colitis (UC), defines as an idiopathic, chronic, relapsing, inflammatory disease affecting the gastrointestinal tract and leading to chronic damage. Endoscopy with biopsies is considered the gold standard for IBD diagnosis, whereas magnetic resonance (MRI) for CD extension and complication assess-ment. However, the latter are invasive procedures; thus, the need for a reliable, accessible and noninvasive way to perform IBD diagnosis and monitoring in the tight control era, like intestinal ultrasound (IUS) is. Compared to endoscopy and MRI, IUS has shown reliable diagnostic accuracy in assessing CD and UC severity and extension. Performing IUS in a point-of-care setting (POCIUS) can guide the clinician in driving the diagnostic and therapeutic pathway, thus accel-erating clinical decisions. POCIUS performed with pocket devices can represent the future of physical examination in outpatient or inpatient examination. Accordingly, we performed a liter-ature review about the application of IUS in CD and UC diagnosis. Furthermore, we explored the technical aspects of this imaging technique and its application in a point-of-care setting.
Keywords:
Intestinal ultrasound
; Point-of-care ultrasound
; Crohn's disease
; Ulcerative colitis
1. Introduction
Inflammatory bowel disease (IBD), comprising Crohn's disease (CD) and ulcerative colitis (UC), defines as an idiopathic, chronic, relapsing, inflammatory disease possibly affecting any part of the gastrointestinal tract in CD and colonic wall continuously from the rectum in UC. Over the last few years, their incidence and prevalence have arisen across the globe, resulting in areas with "compounding prevalence" or "acceleration in incidence"[1]. Thus, the need for a reliable and accessible way to perform IBD diagnosis and monitoring has become a priority to direct the diagnostic path efficiently and avoid time-consuming and expensive procedures.
The use of laboratory biomarkers, such as C-reactive protein (CRP) and faecal calprotectin (FC), together with clinical symptoms, does not accurately provide comprehensive information about disease extent and severity[2]. Indeed, due to the transmural involvement of the bowel wall in CD and the submucosal in UC, cross-sectional imaging techniques comprising magnetic resonance (MRI), computed tomography (CT) and intestinal ultrasound (IUS) are considered a precious resource for suggesting or completing an IBD diagnosis and evaluating the disease course with possible extramural complications, even though endoscopy with biopsies remains mandatory[3,4,5]. In this context, IUS has been gaining attention, being a noninvasive, cost-effective, reliable tool for IBD evaluation without needing bowel preparation or contrast media. Nonetheless, performing IUS in a point-of-care setting (POCIUS), such as completing a routine physical examination, can ameliorate IBD-related outcomes, thus ensuring an earlier diagnosis and prompt therapy beginning[6,7,8]. Due to the increasing interest in POCIUS, some training programs, such as the International Bowel Ultrasound Group (IBUS Group), were born to standardise imaging reports and facilitate communication between physicians.
The aim of this review is to explore the technical aspects of POCIUS and its role in IBD diagnosis with its advantages and disadvantages. Moreover, we will explore the topic of the standardisation and optimisation of reporting IUS in IBD.
2. Materials and Methods
We performed a narrative review with the findings obtained from research on the previously exposed topic on the PubMed database. Our search terms were included as follows: "Inflammatory bowel disease" OR "IBD" OR "Crohn's disease" OR "Post-operative recurrence" OR "ulcerative colitis" AND "intestinal ultrasound" OR "Point of care ultrasound" OR "POCUS" OR "bowel ultrasound". We selected articles, abstracts, systematic reviews, meta-analyses in English, and references from the most relevant articles and ClinicalTrials.gov.
3. Results
3.1. Technical aspects of IUS performing and reporting
Performing IUS does not need fasting conditions. It can be generally conducted with two probes, a low-frequency (1-5 MHz) convex and a high-frequency (6-13 MHz) linear probe. The first provides a panoramic overview of the abdomen; the second ensures a specific visualisation of bowel wall layers. The bowel wall consists of 5 layers: superficial mucosal layer (hyperechoic), deep mucosal layer (hypoechoic), submucosal layer (hyperechoic), muscular layer (hypoechoic), serosa layer (hyperechoic). The practical aspects of the IUS examination are not yet well established; thus, it generally depends upon each centre. The most common approach is searching for left iliac vessels and psoas muscle as a reference point for the sigmoid colon, then tracking each colonic segment till caecum and terminal ileum recognition. Aftermath, an entire abdomen scan through multiple linear movements should be performed to ensure a global evaluation of possible complications. During the examination, the probe should be fanned with different grades of compression to identify air and all bowel layers; at least two 90-degree rotations at the splenic and hepatic flexure are needed to follow the colonic structure[9,10].
The intramural findings that should be reported in an IUS examination are the following[11]:
- -
- Bowel wall thickness (BWT), measured in two planes from the superficial mucosal layer to the serosal layer, has a pathological finding of > 3mm for both the ileal and colonic walls;
- -
- Colour Doppler signal (CDS), measured at the most thickened bowel segment and reported at least with the intramural and/or extramural signal presence;
- -
- Bowel wall stratification (BWS), considered normal, focally or extensively lost.
- -
- Presence or absence of haustrations, ulcers, peristaltic movements and significant/persistent stenoses.
About the extramural findings, they should generally be reported as the presence or absence of enlarged inflammatory lymph nodes, mesenteric fat inflammation, free fluid, fistula (< 2 cm diameter hypoechoic tract generally starting from bowel wall and extending through mesentery towards other bowel loops, bladder, or urogenital tract) and abscesses (irregular anechoic lesions with posterior wall enhancement without vascularisation signals).
Using oral or intravenous contrast media agents has extensively been proposed and studied. Although it can add some information to basal IUS, it can make the examination more invasive and time-consuming, thus reducing its cost-effectiveness.
Some technical aspects can limit the reliability of the IUS examination. First, the patient's body status, especially when obesity is present, can reduce the correct visualisation of abdominal organs. Secondly, given that rectum is the most affected colonic part in UC, its "deep" and pelvic anatomic position represents a further limitation for the complete reliability of disease evaluation due to difficulty reaching it during the exam[11].
3.2. IUS in the diagnosis of CD
The role of IUS in CD diagnosis in patients with symptoms suggesting IBD has been well-analysed through literature. The diagnostic accuracy of IUS for patients without an established diagnosis of CD is summarised in Table 1. Sensitivity and specificity were assessed in 11 studies[12,13,14,15,16,17,18,19,20]: results ranged from 50 to 100% for the first and 91.9% to 100% for the second. The comparison between IUS and MRI [18]showed no difference in terms of sensitivity (94% for IUS vs 96% for MRI) and specificity(97% for IUS vs 94% for MRI) with overlapping confidence intervals, although MRI performed better than IUS for disease extension. The latter results are confirmed and comprised in a systematic review conducted by Calabrese E. et al.[21], where the sensitivity and specificity for the US were respectively 79.7%% (71.9–87.5%%, CI 95%) and 96.7%% (95.1–98.4%%, CI 95%). However, as shown in the METRIC study conducted in 2018 by Taylor et al.[22], MRE performed better than IUS for ileal CD presence detection (97% vs 92%; p=0,025), while IUS performed better than MRE for colonic disease detection (73% vs 64%; p=0,202) in terms of sensitivity. In the same study specificity of MRE and IUS were not statistically different(96% vs 84%; p=0.054 for ileal CD and 96% vs 96%; p=1,000 for colonic CD). The latter is the only randomised control trial (therefore, the most methodologically correct study) regarding the use of ultrasound for CD diagnosis. Accordingly, IUS can be considered a reliable tool for the first-level examination of patients with clinical and laboratory findings suggestive of IBD. Performing ultrasound in a point-of-care setting can drive the diagnostic and therapeutic pathway in different clinical conditions, such as IBD, bowel infections, IBS, acute diverticulitis or bowel cancer (Figure 1).
This tool's high specificity can help physicians exclude IBD in patients with non-specific gastrointestinal symptoms and negative laboratory findings.
3.3. IUS in defining CD localisation and extension
The role of IUS in defining disease localisation is reported in the studies summarised in Table 2.
Those findings confirm ultrasound's reliability with a ranging sensitivity and specificity of 73-96% and 67-98%[12,14,15,18,23,24,25,26,27,28,29]. In a systematic review conducted by Panes et al.[30]in 2011, the overall sensitivity and specificity were found to be 84% and 94%. The diagnostic accuracy of IUS did not significantly differ from MRE in a study conducted by our group [18], where sensitivity and specificity for CD location for ultrasound were 73% and 92%. Subsequently, Calabrese E. et al.[21]analysed the sensitivity and specificity of IUS in detecting anatomical lesions for each bowel wall segment: they were 55.6% and 98.5% for jejunal lesions, 92,7% and 88.2% for ileal lesions, 81.8% and 95.3% for colonic lesions.
On the other hand, the evaluation of disease extension differs from the disease location. In a study conducted by our group in 2013[18], the concordance between IUS and MRI regarding disease extension was moderate (r=0.69); this result was more evident when the disease involved longer (> 30 cm) ileal segments. The concordance between the two procedures seems to become higher when IUS was performed with oral contrast administration (SICUS), as stated in the studies conducted by Pallotta et al. [16]and Calabrese E. et al. [31]. According to the results from the METRIC study[22], IUS has a sensitivity of 29% and a specificity of 61% in evaluating disease extension in both ileal and colonic involvement. At the same time, MRE had a sensitivity of 44% (p=0.002) and a specificity of 80% (p=0.337). Those results are even worse if only colonic extension evaluation (17% sensitivity) is considered.
3.4. IUS in defining complicated CD
3.4.1. Strictures
CD disease patients can develop small bowel and, less commonly, colonic strictures. It usually causes obstructive symptoms, and the detection of this complication requires either an intensive medical treatment escalation or surgery. However, up to 20% of small bowel strictures in CD does not cause any symptom[32]. Thus, early detection of this kind of complication is crucial in CD diagnosis and monitoring. The accepted definition for luminal stenoses at cross-sectional imaging and ultrasound comprises the presence of a fixed luminal narrowing associated with an upstream loop dilation≥ 3 cm [11]. IUS has a sensitivity and specificity in detecting stenosis compared to surgery of 75-100% and 0-91%, respectively[33–37]. A complete overview of this evaluation is available in Table 3.
Three out of five studies applied SICUS(35–37), which seems to perform better than IUS in detecting strictures. According to Panes et al.[30], IUS's pooled sensitivity and specificity are 79% and 92%, even though not all the studies considered surgery as a reference standard. The concordance of IUS and other radiologic techniques, such as MRE, was evaluated by our group in 2013[18]: the results showed fair concordance(k=0.082; p=0.01) between those two techniques in detecting small bowel stenoses. Therefore, IUS can be considered a reliable tool for detecting stenotic complications of CD. However, as for the other imaging techniques, it has never been demonstrated a role in stenosis characterisation. Indeed, knowing its nature (either inflammatory or fibrotic) could be a turning point for CD management decision-making. An attempt in this direction has been made by describing BWS: in a study conducted by Maconi et al. [38], the loss of stratification in the bowel wall was related to inflammatory stenosis, while a stratified pattern suggested a stenotic disease behaviour. The latter results, although promising, have not been studied in deeper, probably due to the subjectivity of the choice of the different stratification patterns. The use of elastography and contrast-enhanced ultrasound (CEUS) seems promising in this field, despite the small sample size of studies and different methodologies in measurement [39].
3.4.2. Abscesses
After stenoses, the formation of abscesses is one of the most common extramural complications in CD. On ultrasound, these are described as an ill-defined inflammatory mass without concrete walls and with peripheral and internal CDS [11]. The role of IUS in abscess detection has been extensively analysed in the literature. The sensitivity and specificity of IUS ranged from 80% to 100% and 80% to 96%, using surgery as the comparator in three out of four studies[12,29,33,36,38]. Results are summarised in Table 4. In the study conducted by Maconi et al. in 2003[38], CT performed better than IUS in detecting abscesses (92% CT vs 87% IUS for diagnostic accuracy): both techniques failed to detect "deep" abscesses, such as interloop, appendicular and mesenteric ones, according to the systematic review conducted by Calabrese E. et al.[21], IUS's overall sensitivity and specificity was 86.5% (95% CI; 83.3%–88%), while the specificity was 94.5% (95% CI, 87.9%–100%).
Regarding the concordance between MRI and IUS, in the study conducted by our group in 2013[18], it was excellent (k=0.88; p=0.01). Hence, IUS can be considered a reliable tool for detecting abscess formation in CD.
3.4.3. Intrabdominal fistula
The evaluation of intrabdominal fistulas is a crucial point for IUS. These are defined as a hypoechoic duct with < 2 cm diameter (differentiating them from perienteric abscesses) with or without gas filling; additionally, the fistula site and organ involvement (entero-enteric,entero-cutaneous and enterovesical) should be reported[11]. According to the results summarised in Table 5, the sensitivity of ultrasound without oral contrast administration ranges from 60% to 87%[12,29,33,35,36]; those results improve when SICUS is performed. In more recent works, the global sensitivity of IUS (either with or without oral contrast) was 70.1% (95% CI, 59.7%–80.6%), while the specificity was 95.6% (95% CI, 92.5%–98.8%)[21]. Moreover, IUS showed no good concordance with MRI regarding fistula detection (k=0.67; p=0.01) [18]. However, in a more recent prospective study including 60 CD patients, IUS showed a sensitivity of 100% and a specificity of 98% in detecting fistulas with 98% diagnostic accuracy compared to MRI [29].
3.5. IUS in post-operative recurrence detection
CD patients require surgery in up to 70% of cases in ten years, and disease recurrence after bowel resection can occur in up to 90% without therapy within five years [40]. Although it is not possible to talk about a proper "diagnosis", early detection of CD post-operative recurrence (POR) is crucial for IBD management. Colonoscopy with biopsies within 6-12 months after surgery [41]remains the gold standard for POR detection, but IUS shows good accuracy in its recognition [42]. Moreover, IUS can help the physician accelerate its early identification and introduce or escalate therapy faster. In 1998, Andreoli et al.[43]first described IUS as a reliable first-line tool to detect CD POR, despite the machine performance of that time: in their study conducted on 41 patients, they found a sensitivity of 81%, a specificity of 86%, and a diagnostic accuracy of 83% for BWT > 5 mm in detecting recurrence compared to endoscopy.
Rispo et al.[44] compared the diagnostic accuracy of IUS with endoscopy one year after surgery: they found sensitivity, specificity, positive predictive value and negative predictive value, respectively of 79%,95%, 95%, and 80%. Furthermore, a cut-off of BWT > 5 mm differentiated mild from severe endoscopic recurrence with excellent agreement with endoscopy (k=0.90). In 2008, Castiglione et al.[45] conducted a prospective study on 40 patients who had undergone surgery. After one year of follow-up, IUS, SICUS and IC were executed: the sensitivity and specificity of IUS and SICUS were comparable (77% and 94% for IUS, 82% and 94% for SICUS) with a cut-off of BWT> 3 mm without statistically significant different results. On the other side, a cut-off of 5 mm for IUS and 4 mm for SICUS showed an excellent AUROC in the detection of severe POR, both with a diagnostic accuracy of 97%. The threshold values differ between the two techniques because the oral contrast agent flattens the bowel wall, thus making it thinner.
On the other side, Calabrese E. et al.[46] found a significant correlation (r= 0.67; p < 0.0001) between BWT evaluated with SICUS and Rutgeerts score, defining CD recurrence in the presence of BWT> 3 mm for at least 4 cm length at the perianastomotic area, bowel dilation > 2.5 cm and bowel stricture defined as < 1 cm bowel lumen diameter In 2016, Onali et al.[47] reported in a five years experience sensitivity and specificity for SICUS of 98% and 75% for SICUS performed one year after surgery. However, BWT was not correlated with clinical outcomes at the end of the follow-up. Furthermore, in a 2021 retrospective study on 201 patients by Dal Piaz et al.[48], IUS recurrence and BWT ≥4 mm predicted surgical recurrence with an OR = 6.04 and 2.58, respectively.
The latter results support the routine use of IUS and SICUS in clinical practice for POR detection within one year after surgery, especially in the first months, in order to detect early recurrence.
3.6. IUS in UC diagnosis
The utility of IUS in UC has been gaining attention over the last few years. Whilst its utility in defining disease extension and activity is well known, IUS has not been proven reliable for diagnosing UC. The findings from the literature show an overlap regarding sonographic findings among the most common conditions affecting the colon, such as UC, colonic CD, radiation, infectious and ischaemic colitis [25,49,50,51]. Even though some studies report a marked BWT associated with colonic CD, this finding can not reliably distinguish it from a severe UC. Hence, IUS can represent a valuable tool for recognising colonic disease, thus guiding an indication by the physician to an early endoscopic examination, which remains the gold standard for UC diagnosis together with biopsy sampling[4].
3.7. IUS in UC extension
Since IUS cannot provide specific features for UC diagnosis, it is a reliable tool for defining disease extent and severity. Already in 1992, Schwerk et al. [52], in a prospective study including 30 patients diagnosed with UC, found a 100% sensitivity for IUS in detecting extensive colitis, 95% for left colitis and 50% for rectal disease. Other studies subsequently confirmed the latter results in terms of diagnostic accuracy [15,25]. In 2018, Allocca et al. [53] found a good correlation between UC extension measured with IUS and endoscopy (0.660, 95% CI: 0.474-0.790, p < 0.0001). Subsequently, Kinoshita et al. [54] demonstrated a moderate concordance between IUS evaluation and endoscopy for all colonic segments except for the rectum (k=0.33). As well as rectal and perianal involvement for CD is poorly assessed with transabdominal ultrasound, rectal visualisation in UC is limited by its distance from the abdominal wall. Thus, Sagami et al. proposed [55] the adoption of trans-perineal ultrasound (TPUS) approach for rectal involvement evaluation in UC. According to the results coming from the latter study, BWT < 4mm measured with TPUS was an independent predictor for endoscopic and histologic healing in the rectum (p < 0.05).
3.8. IUS in UC disease activity
During the last few years, the growing evidence for the reliability of IUS in UC activity evaluation has made spreading its use and literature interest. Several studies assessed endoscopic disease severity and activity according to heterogenic criteria[15,56,57,58,59]: findings are summarised in Table 6. Bozkurt et al.[56] in 1996 first evaluated UC activity through ultrasound: among the 36 patients diagnosed with UC, BWT > 4 mm and BWS were considered features correlated with endoscopic and histological severe activity (p<0.01). Subsequently, an increasing number of studies have been conducted. To date, the need for standardisation in the definition of UC activity has led to the proposal of unified scores. In 2018, Allocca et al.[53] developed a score and externally validated it in 2020 as Milano Ultrasound Criteria (MUC)[58]: a MUC score > 6.2 was the cut-off best correlated with a Mayo endoscopic score (MES) ≥ 2 [sensitivity 0.85, specificity 0.94; AUC 0.902 (95% CI 0.772–0.971)]. In 2021, Bots et al.[59] defined and internally validated the UC-IUS index as a score showing a strong correlation with endoscopic disease activity (MES r=0.830; p < 0.001, Ulcerative Colitis Endoscopic Index of Severity UCEIS r=0.759; p < 0.001). Therefore, UC activity can be assessed through IUS with a good correlation with endoscopic activity.
3.9. Reproducibility and scoring
The reproducibility of the technique remains one of the most crucial key-point for defining the role of IUS in IBD management. In 2008, Fraquelli et al. [60] demonstrated good-to-excellent reproducibility among expert sonographers (k values for BWT ranged between 0.7 and 1). Subsequently, other studies confirmed those results and added new data: De Voogd et al. [61] found a strong intraclass correlation coefficient (ICC=0.96) for BWT in UC, with substantial results also for CDS (k=0.63). However, the need for standardisation in non-expert centres was noticeable. Thus, a need for standardisation of exam execution has given rise to the development of training courses, like the one from the International Bowel Ultrasound Group (IBUS), to educate physicians in the oriented performance of IUS. Furthermore, the need for a unique way to communicate the findings and correlate them with disease activity made it necessary to develop eco-graphic activity scores. Two scores have been developed for CD: Novak et al. [62] in 2021 presented a Delphi consensus which defined the International Bowel Ultrasound Segment Activity Score (IBUS-SAS), calculated through BWT, i-fat, CDS and BWS, and showing an ICC of 0.97 (0.95–0.99, p < 0.001). Moreover, Allocca et al. [63] elaborated bowel-US-score (BUSS), calculated using the following formula BUSS=0.75*BWT+1.65*CDS. BUSS significantly correlated with endoscopic activity (r=0.55; p < 0.01), and the cut-off of 3.52 discriminated between endoscopically active and non-active disease. Nonetheless, the same cut-off predicted disease course at 12 months, determining patients' group at higher risk of treatment escalation (p<0.001) and need for surgery (p<0.001).
Regarding UC, we already discussed the MUC score in the above paragraph. Also of note is the predictive value of this score: in a prospective study on 98 UC patients followed-up for a median time of 1.6 years, MUC score and MES well correlated at baseline (r = 0.653; p < 0.001) and lower cumulative probability of treatment escalation, the need of corticosteroids, hospitalisation and colectomy were found among patients who had MUC ≤ 6.2 at baseline as compared to patients with MUC > 6.2 (p < 0.05)[64].
Hence, IUS scores are a well-established way to express disease activity and severity, nonetheless, to drive therapeutic decisions based on the predictor value of ultrasound findings.
3.10. Point-of-care Intestinal Ultrasound (POCIUS)
Performing IUS in a POC setting is an increasing way to complete physical examinations in outpatient visits. With the spreading use of pocket probes, POC ultrasound can increase the sensitivity and specificity of daily clinical activity, as already done in cardiologic and emergency scenarios [65,66,67,68]. Thus, a new discipline called "echoscopy" has been named by the European Federation of Societies for Ultrasound in Medicine and Biology (EFSUMB) as a targeted ultrasound examination directed to the specifically interested suspected disease site. In the attempt to apply those concepts to the IBD study, in a pilot cohort study, our group recently assessed the diagnostic accuracy of handheld IUS (HHIUS) in detecting CD, compared with MRI, finding fair agreement and no significant differences in diagnostic accuracy between the two techniques (89.41% for HHBS vs 92.94% for MRE; p = n.s.)[20]. We further demonstrated a substantial agreement between HHIUS and MRI in the assessment of CD location (k = 0.81; p<0.01) and evaluation of stenoses (k = 0.75; P < .01), abscesses (k = 0.68; P < .01) and fistulas (k = 0.65; P < .01). On the other hand, a significant underestimation of HHIUS in CD extension assessment (r = 0.67; P < .01) has been found. As done for CD, we also applied HHIUS to UC management, comparing it to traditional IUS in the MUC score evaluation for UC. No statistically significant results between the two techniques were found between the assessment of BWT, CDS, BWS and MUC score evaluation [69].
Hence, POCIUS can be considered a valuable tool in IBD diagnosis, speeding up the definitive diagnosis, driving a therapeutic decision and optimising resources.
4. Conclusions
Current literature suggests IUS as an accurate, safe, cost-effective tool for IBD diagnosis, localisation, and behaviour evaluation. During the last decades, its role has evolved from a first-line tool for suspicious IBD and the definition of active vs non-active disease to a finished imaging technique that the physician can count on in IBD management. Indeed, IUS is emerging with a double role: a point-of-care test to speed up clinical and therapeutic decision-making in everyday practice with the spreading use of pocket devices, moreover an ideal tool for evaluating IBD in the entirety of the bowel wall.
Certainly, gastroenterologists need to train extensively to acquire the essential IUS expertise and to unify how the technique is performed and reported.
In conclusion, it is reasonable to state that IUS is a compulsory tool in Gastroenterology Units for evaluating patients with suspected IBD. In addition, its use can benefit disease management for standard physical examination integration and in settings where endoscopy is not firmly necessary.
Author Contributions
GC and AT conceived, wrote and reviewed the manuscript. OMN, ADG and GF provided contribution to manuscript draft. AR critically reviewed the manuscript. FC conceived, critically reviewed, and supervised the manuscript.
Funding
This research received no external funding
Conflicts of Interest
The authors declare no conflict of interest.
References
- Kaplan GG, Windsor JW. The four epidemiological stages in the global evolution of inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021, 18, 56–66. [Google Scholar] [CrossRef]
- Turner D, Ricciuto A, Lewis A, D’Amico F, Dhaliwal J, Griffiths AM, et al. STRIDE-II: An Update on the Selecting Therapeutic Targets in Inflammatory Bowel Disease (STRIDE) Initiative of the International Organization for the Study of IBD (IOIBD): Determining Therapeutic Goals for Treat-to-Target strategies in IBD. Gastroenterology. 2021, 160, 1570–1583. [Google Scholar] [CrossRef]
- Maaser C, Sturm A, Vavricka SR, Kucharzik T, Fiorino G, Annese V, et al. ECCO-ESGAR Guideline for Diagnostic Assessment in IBD Part 1: Initial diagnosis, monitoring of known IBD, detection of complications. Journal of Crohn's and Colitis. 2019, 13, 144–164K. [Google Scholar] [CrossRef]
- Magro F, Gionchetti P, Eliakim R, Ardizzone S, Armuzzi A, Barreiro-de Acosta M, et al. Third European Evidence-based Consensus on Diagnosis and Management of Ulcerative Colitis. Part 1: Definitions, Diagnosis, Extra-intestinal Manifestations, Pregnancy, Cancer Surveillance, Surgery, and Ileo-anal Pouch Disorders. Journal of Crohn's and Colitis. 2017, 11, 649–670. [Google Scholar] [CrossRef]
- Rimola J, Torres J, Kumar S, Taylor SA, Kucharzik T. Recent advances in clinical practice: advances in cross-sectional imaging in inflammatory bowel disease. Gut. 2022, gutjnl-2021-326562.
- Bots S, De Voogd F, De Jong M, Ligtvoet V, Löwenberg M, Duijvestein M, et al. Point-of-care Intestinal Ultrasound in IBD Patients: Disease Management and Diagnostic Yield in a Real-world Cohort and Proposal of a Point-of-care Algorithm. Journal of Crohn's and Colitis. 2022, 16, 606–615. [Google Scholar] [CrossRef]
- de Voogd FAE, Verstockt B, Maaser C, Gecse KB. Point-of-care intestinal ultrasonography in inflammatory bowel disease. Nat Rev Gastroenterol Hepatol. 2021, 18, 209–210. [Google Scholar] [CrossRef]
- Nardone OM, Calabrese G, Testa A, Caiazzo A, Fierro G, Rispo A, et al. The Impact of Intestinal Ultrasound on the Management of Inflammatory Bowel Disease: From Established Facts Toward New Horizons. Front Med. 2022, 9, 898092. [Google Scholar] [CrossRef]
- Allocca M, Furfaro F, Fiorino G, Peyrin-Biroulet L, Danese S. Point-of-Care Ultrasound in Inflammatory Bowel Disease. Journal of Crohn's and Colitis. 2021, 15, 143–151. [Google Scholar] [CrossRef]
- Allocca M, Kucharzik T, Rubin DT. Intestinal Ultrasound in the Assessment and Management of Inflammatory Bowel Disease: Is It Ready for Standard Practice? Gastroenterology. 2023, 164, 851–855. [Google Scholar] [CrossRef]
- Kucharzik T, Tielbeek J, Carter D, Taylor SA, Tolan D, Wilkens R, et al. ECCO-ESGAR Topical Review on Optimizing Reporting for Cross-Sectional Imaging in Inflammatory Bowel Disease. Journal of Crohn’s and Colitis. 2022, 16, 523–543. [Google Scholar] [CrossRef]
- Maconi G, Parente F, Bollani S, Cesana B, Bianchi Porro G. Abdominal ultrasound in the assessment of extent and activity of Crohn's disease: clinical significance and implication of bowel wall thickening. Am J Gastroenterol. 1996, 91, 1604–1609. [Google Scholar]
- Astegiano M, Bresso F, Cammarota T, Sarno A, Robotti D, Demarchi B, et al. Abdominal pain and bowel dysfunction: diagnostic role of intestinal ultrasound. European Journal of Gastroenterology & Hepatology. 2001, 13, 927–931. [Google Scholar]
- Parente, F. Bowel ultrasound in assessment of Crohn's disease and detection of related small bowel strictures: a prospective comparative study versus x ray and intraoperative findings. Gut. 2002, 50, 490–495. [Google Scholar] [CrossRef]
- Pascu M, Roznowski AB, Müller HP, Adler A, Wiedenmann B, Dignass AU. Clinical Relevance of Transabdominal Ultrasonography and Magnetic Resonance Imaging in Patients With Inflammatory Bowel Disease of the Terminal Ileum and Large Bowel. Inflammatory Bowel Diseases. 2004, 10, 373–382. [Google Scholar] [CrossRef]
- Pallotta N, Tomei E, Viscido A, Calabrese E, Marcheggiano A, Caprilli R, et al. Small Intestine Contrast Ultrasonography: An Alternative to Radiology in the Assessment of Small Bowel Disease. Inflammatory Bowel Diseases. 2005, 11, 146–153. [Google Scholar] [CrossRef]
- Rispo A, Imbriaco M, Celentano L, Cozzolino A, Camera L, Mainenti PP, et al. Noninvasive Diagnosis of Small Bowel Crohnʼs Disease: Combined Use of Bowel Sonography and Tc-99M-Hmpao Leukocyte Scintigraphy. Inflammatory Bowel Diseases. 2005, 11, 376–382. [Google Scholar] [CrossRef]
- Castiglione F, Mainenti PP, De Palma GD, Testa A, Bucci L, Pesce G, et al. Noninvasive Diagnosis of Small Bowel Crohn’s Disease: Direct Comparison of Bowel Sonography and Magnetic Resonance Enterography. Inflammatory Bowel Diseases. 2013, 19, 991–998. [Google Scholar] [CrossRef]
- Pallotta N, Civitelli F, Di Nardo G, Vincoli G, Aloi M, Viola F, et al. Small Intestine Contrast Ultrasonography in Pediatric Crohn's Disease. The Journal of Pediatrics. 2013, 163, 778–784. [Google Scholar] [CrossRef]
- Rispo A, de Sire R, Mainenti PP, Imperatore N, Testa A, Maurea S, et al. David Against Goliath: Direct Comparison of Handheld Bowel Sonography and Magnetic Resonance Enterography for Diagnosis of Crohn’s Disease. Inflammatory Bowel Diseases. 2022, izac116.
- Calabrese E, Maaser C, Zorzi F, Kannengiesser K, Hanauer SB, Bruining DH, et al. Bowel Ultrasonography in the Management of Crohnʼs Disease. A Review with Recommendations of an International Panel of Experts. Inflammatory Bowel Diseases. 2016, 22, 1168–1183. [Google Scholar] [CrossRef]
- Taylor SA, Mallett S, Bhatnagar G, Baldwin-Cleland R, Bloom S, Gupta A, et al. Diagnostic accuracy of magnetic resonance enterography and small bowel ultrasound for the extent and activity of newly diagnosed and relapsed Crohn's disease (METRIC): a multicentre trial. The Lancet Gastroenterology & Hepatology. 2018, 3, 548–558. [Google Scholar]
- Reimund JM, Jung-Chaigneau E, Chamouard P, Wittersheim C, Duclos B, Baumann R. [Diagnostic value of high resolution sonography in Crohn's disease and ulcerative colitis]. Gastroenterol Clin Biol. 1999, 23, 740–746. [Google Scholar]
- Bru C, Sans M, Defelitto MM, Gilabert R, Fuster D, Llach J, et al. Hydrocolonic Sonography for Evaluating Inflammatory Bowel Disease. American Journal of Roentgenology. 2001, 177, 99–105. [Google Scholar] [CrossRef]
- Parente F, Greco S, Molteni M, Cucino C, Maconi G, Sampietro GM, et al. Role of early ultrasound in detecting inflammatory intestinal disorders and identifying their anatomical location within the bowel: BOWEL ULTRASOUND FOR DETECTION OF INFLAMMATORY DISEASE. Alimentary Pharmacology & Therapeutics. 2003, 18, 1009–1016. [Google Scholar]
- Parente, F. Oral contrast enhanced bowel ultrasonography in the assessment of small intestine Crohn's disease. A prospective comparison with conventional ultrasound, x ray studies, and ileocolonoscopy. Gut. 2004, 53, 1652–1657. [Google Scholar] [CrossRef]
- Martínez MJ, Ripollés T, Paredes JM, Blanc E, Martí-Bonmatí L. Assessment of the extension and the inflammatory activity in Crohn's disease: comparison of ultrasound and MRI. Abdom Imaging. 2009, 34, 141–148. [Google Scholar] [CrossRef]
- Rispo A, Imperatore N, Testa A, Mainenti P, De Palma GD, Luglio G, et al. Bowel Damage in Crohnʼs Disease: Direct Comparison of Ultrasonography-based and Magnetic Resonance-based Lemann Index. Inflammatory Bowel Diseases. 2017, 23, 143–151. [Google Scholar] [CrossRef]
- Allocca M, Fiorino G, Bonifacio C, Furfaro F, Gilardi D, Argollo M, et al. Comparative Accuracy of Bowel Ultrasound Versus Magnetic Resonance Enterography in Combination With Colonoscopy in Assessing Crohn’s Disease and Guiding Clinical Decision-making. Journal of Crohn’s and Colitis. 2018, 12, 1280–1287. [Google Scholar] [CrossRef]
- Panés J, Bouzas R, Chaparro M, García-Sánchez V, Gisbert JP, Martínez de Guereñu B, et al. Systematic review: the use of ultrasonography, computed tomography and magnetic resonance imaging for the diagnosis, assessment of activity and abdominal complications of Crohn's disease: Systematic review: cross-sectional imaging in Crohn's disease. Alimentary Pharmacology & Therapeutics. 2011, 34, 125–145. [Google Scholar]
- Calabrese E, La Seta F, Buccellato A, Virdone R, Pallotta N, Corazziari E, et al. Crohnʼs Disease: A Comparative Prospective Study of Transabdominal Ultrasonography, Small Intestine Contrast Ultrasonography, and Small Bowel Enema. Inflammatory Bowel Diseases. 2005, 11, 139–145. [Google Scholar] [CrossRef]
- Ismail MS, Charabaty A. Management of Crohn's stricture: medical, endoscopic and surgical therapies. Frontline Gastroenterol. 2022, 13, 524–530. [Google Scholar] [CrossRef]
- Gasche C, Moser G, Turetschek K, Schober E, Moeschl P, Oberhuber G. Transabdominal bowel sonography for the detection of intestinal complications in Crohn's disease. Gut. 1999, 44, 112–117. [Google Scholar] [CrossRef]
- Kohn A, Cerro P, Milite G, De Angelis E, Prantera C. Prospective Evaluation of Transabdominal Bowel Sonography in the Diagnosis of Intestinal Obstruction in Crohnʼs Disease: Comparison with Plain Abdominal Film and Small Bowel Enteroclysis. Inflammatory Bowel Diseases. 1999, 5, 153–157. [Google Scholar] [CrossRef]
- Pallotta N, Vincoli G, Montesani C, Chirletti P, Pronio A, Caronna R, et al. Small intestine contrast ultrasonography (SICUS) for the detection of small bowel complications in crohnʼs disease: A prospective comparative study versus intraoperative findings. Inflammatory Bowel Diseases. 2012, 18, 74–84. [Google Scholar] [CrossRef]
- Onali, S. Small intestine contrast ultrasonography vs computed tomography enteroclysis for assessing ileal Crohn's disease. WJG. 2012, 18, 6088. [Google Scholar] [CrossRef]
- Kumar S, Hakim A, Alexakis C, Chhaya V, Tzias D, Pilcher J, et al. Small intestinal contrast ultrasonography for the detection of small bowel complications in Crohn's disease: Correlation with intraoperative findings and magnetic resonance enterography: Small intestinal contrast ultrasonography in Crohn's disease. J Gastroenterol Hepatol. 2015, 30, 86–91. [Google Scholar] [CrossRef]
- Maconi G, Sampietro GM, Parente F, Pompili G, Russo A, Cristaldi M, et al. Contrast Radiology, Computed Tomography and Ultrasonography in Detecting Internal Fistulas and Intra-Abdominal Abscesses in Crohn's Disease: A Prospective Comparative Study. American Journal of Gastroenterology. 2003, 98, 1545–1555. [Google Scholar] [CrossRef]
- Grażyńska A, Kufel J, Dudek A, Cebula M. Shear Wave and Strain Elastography in Crohn's Disease—A Systematic Review. Diagnostics. 2021, 11, 1609. [Google Scholar] [CrossRef]
- Torres J, Mehandru S, Colombel JF, Peyrin-Biroulet L. Crohn's disease. The Lancet. 2017, 389, 1741–1755. [Google Scholar] [CrossRef]
- Adamina M, Bonovas S, Raine T, Spinelli A, Warusavitarne J, Armuzzi A, et al. ECCO Guidelines on Therapeutics in Crohn’s Disease: Surgical Treatment. Journal of Crohn’s and Colitis. 2020, 14, 155–168. [Google Scholar] [CrossRef]
- Rispo A, Imperatore N, Testa A, Nardone OM, Luglio G, Caporaso N, et al. Diagnostic Accuracy of Ultrasonography in the Detection of Postsurgical Recurrence in Crohn's Disease: A Systematic Review with Meta-analysis. Inflammatory Bowel Diseases. 2018, 24, 977–988. [Google Scholar] [CrossRef]
- Andreoli A, Prantera C. Role of Ultrasonography in the Diagnosis of Postsurgical Recurrence of Crohn's Disease. 1998, 93.
- Rispo A, Bucci L, Pesce G, Sabbatini F, de Palma GD, Grassia R, et al. Bowel sonography for the diagnosis and grading of postsurgical recurrence of Crohnʼs disease. Inflammatory Bowel Diseases. 2006, 12, 486–490. [Google Scholar] [CrossRef]
- Castiglione F, Bucci L, Pesce G, De Palma GD, Camera L, Cipolletta F, et al. Oral contrast-enhanced sonography for the diagnosis and grading of postsurgical recurrence of Crohnʼs disease. Inflammatory Bowel Diseases. 2008, 14, 1240–1245. [Google Scholar] [CrossRef]
- Calabrese E, Petruzziello C, Onali S, Condino G, Zorzi F, Pallone F, et al. Severity of postoperative recurrence in crohnʼs disease: Correlation between endoscopic and sonographic findings. Inflammatory Bowel Diseases. 2009, 15, 1635–1642. [Google Scholar] [CrossRef]
- Onali S, Calabrese E, Petruzziello C, Lolli E, Ascolani M, Ruffa A, et al. Post-operative recurrence of Crohn's disease: A prospective study at 5 years. Digestive and Liver Disease. 2016, 48, 489–494. [Google Scholar] [CrossRef]
- Dal Piaz G, Mendolaro M, Mineccia M, Randazzo C, Massucco P, Cosimato M, et al. Predictivity of early and late assessment for post-surgical recurrence of Crohn's disease: Data from a single-center retrospective series. Digestive and Liver Disease. 2021, 53, 987–995. [Google Scholar] [CrossRef]
- S. Hollerbach, A. Geissler, H. Schi. The Accuracy of Abdominal Ultrasound in the Assessment of Bowel Disorders. Scandinavian Journal of Gastroenterology. 1998, 33, 1201–1208. [Google Scholar] [CrossRef]
- Truong M, Atri M, Bret PM, Reinhold C, Kintzen G, Thibodeau M, et al. Sonographic appearance of benign and malignant conditions of the colon. American Journal of Roentgenology. 1998, 170, 1451–1455. [Google Scholar] [CrossRef]
- Lim JH, Ko YT, Lee DH, Lim JW, Kim TH. Sonography of inflammatory bowel disease: findings and value in differential diagnosis. American Journal of Roentgenology. 1994, 163, 343–347. [Google Scholar] [CrossRef] [PubMed]
- Schwerck W, Beckh K, Raith M. A prospective evaluation of high resolution sonography in the diagnosis of inflammatory bowel disease.
- Allocca M, Fiorino G, Bonovas S, Furfaro F, Gilardi D, Argollo M, et al. Accuracy of Humanitas Ultrasound Criteria in Assessing Disease Activity and Severity in Ulcerative Colitis: A Prospective Study. Journal of Crohn’s and Colitis. 2018, 12, 1385–1391. [Google Scholar] [CrossRef]
- Kinoshita K, Katsurada T, Nishida M, Omotehara S, Onishi R, Mabe K, et al. Usefulness of transabdominal ultrasonography for assessing ulcerative colitis: a prospective, multicenter study. J Gastroenterol. 2019, 54, 521–529. [Google Scholar] [CrossRef]
- Sagami S, Kobayashi T, Miyatani Y, Okabayashi S, Yamazaki H, Takada T, et al. Accuracy of Ultrasound for Evaluation of Colorectal Segments in Patients With Inflammatory Bowel Diseases: A Systematic Review and Meta-analysis. Clinical Gastroenterology and Hepatology. 2021, 19, 908–921. [Google Scholar] [CrossRef]
- Bozkurt T, Rommel T, Stabenow-Lohbauer U, Langer M, Schmiegelow P, Lux G. Sonographic bowel wall morphology correlates with clinical and endoscopic activity in crohn's disease and ulcerative colitis. European Journal of Ultrasound. 1996, 4, 27–33. [Google Scholar] [CrossRef]
- Antonelli E, Giuliano V, Casella G, Villanacci V, Baldini V, Baldoni M, et al. Ultrasonographic assessment of colonic wall in moderate–severe ulcerative colitis: Comparison with endoscopic findings. Digestive and Liver Disease. 2011, 43, 703–706. [Google Scholar] [CrossRef]
- Allocca M, Filippi E, Costantino A, Bonovas S, Fiorino G, Furfaro F, et al. Milan ultrasound criteria are accurate in assessing disease activity in ulcerative colitis: external validation. United European Gastroenterol j. 2021, 9, 438–442. [Google Scholar] [CrossRef]
- Bots S, Nylund K, Löwenberg M, Gecse K, D'Haens G. Intestinal Ultrasound to Assess Disease Activity in Ulcerative Colitis: Development of a novel UC-Ultrasound Index. Journal of Crohn's and Colitis. 2021, 15, 1264–1271. [Google Scholar] [CrossRef]
- Fraquelli M, Sarno A, Girelli C, Laudi C, Buscarini E, Villa C, et al. Reproducibility of bowel ultrasonography in the evaluation of Crohn's disease. Digestive and Liver Disease. 2008, 40, 860–866. [Google Scholar] [CrossRef]
- De Voogd F, Wilkens R, Gecse K, Allocca M, Novak K, Lu C, et al. A Reliability Study: Strong Inter-Observer Agreement of an Expert Panel for Intestinal Ultrasound in Ulcerative Colitis. Journal of Crohn's and Colitis. 2021, 15, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Novak KL, Nylund K, Maaser C, Petersen F, Kucharzik T, Lu C, et al. Expert Consensus on Optimal Acquisition and Development of the International Bowel Ultrasound Segmental Activity Score [IBUS-SAS]: A Reliability and Inter-rater Variability Study on Intestinal Ultrasonography in Crohn's Disease. Journal of Crohn's and Colitis. 2021, 15, 609–616. [Google Scholar] [CrossRef] [PubMed]
- Allocca M, Craviotto V, Dell’Avalle C, Furfaro F, Zilli A, D’Amico F, et al. Bowel ultrasound score is accurate in assessing response to therapy in patients with Crohn's disease. Aliment Pharmacol Ther. 2022, 55, 446–454. [Google Scholar] [CrossRef]
- Allocca M, Dell’Avalle C, Craviotto V, Furfaro F, Zilli A, D’Amico F, et al. Predictive value of Milan ultrasound criteria in ulcerative colitis: A prospective observational cohort study. UEG Journal. 2022, 10, 190–197. [Google Scholar] [CrossRef]
- Mjolstad OC, Dalen H, Graven T, Kleinau JO, Salvesen O, Haugen BO. Routinely adding ultrasound examinations by pocket-sized ultrasound devices improves inpatient diagnostics in a medical department. European Journal of Internal Medicine. 2012, 23, 185–191. [Google Scholar] [CrossRef]
- Wastl D, Löwe A, Dietrich CF. Echoscopy in scanning abdominal diseases in a critical care setting. Med Klin Intensivmed Notfmed [Internet]. 2022 Jun 2. Available online: https://link.springer.com/10.1007/s00063-022-00926-4 (accessed on 31 October 2022).
- Barreiros A, Cui X, Ignee A, De Molo C, Pirri C, Dietrich C. EchoScopy in Scanning Abdominal Diseases: Initial Clinical Experience. Z Gastroenterol. 2014, 52, 269–275. [Google Scholar] [CrossRef]
- Testuz A, Muller H, Keller PF, Meyer P, Stampfli T, Sekoranja L, et al. Diagnostic accuracy of pocket-size handheld echocardiographs used by cardiologists in the acute care setting. European Heart Journal - Cardiovascular Imaging. 2013, 14, 38–42. [Google Scholar] [CrossRef]
- Rispo A, Calabrese G, Testa A, Imperatore N, Patturelli M, Allocca M, et al. Hocus Pocus: the Role of Handheld Ultrasonography in Predicting Disease Extension and Endoscopic Activity in Ulcerative Colitis. Journal of Crohn's and Colitis. 2023, jjad024.
Figure 1.
Point-of-care Intestinal Ultrasound (POCIUS) positioning in IBD suspicion.
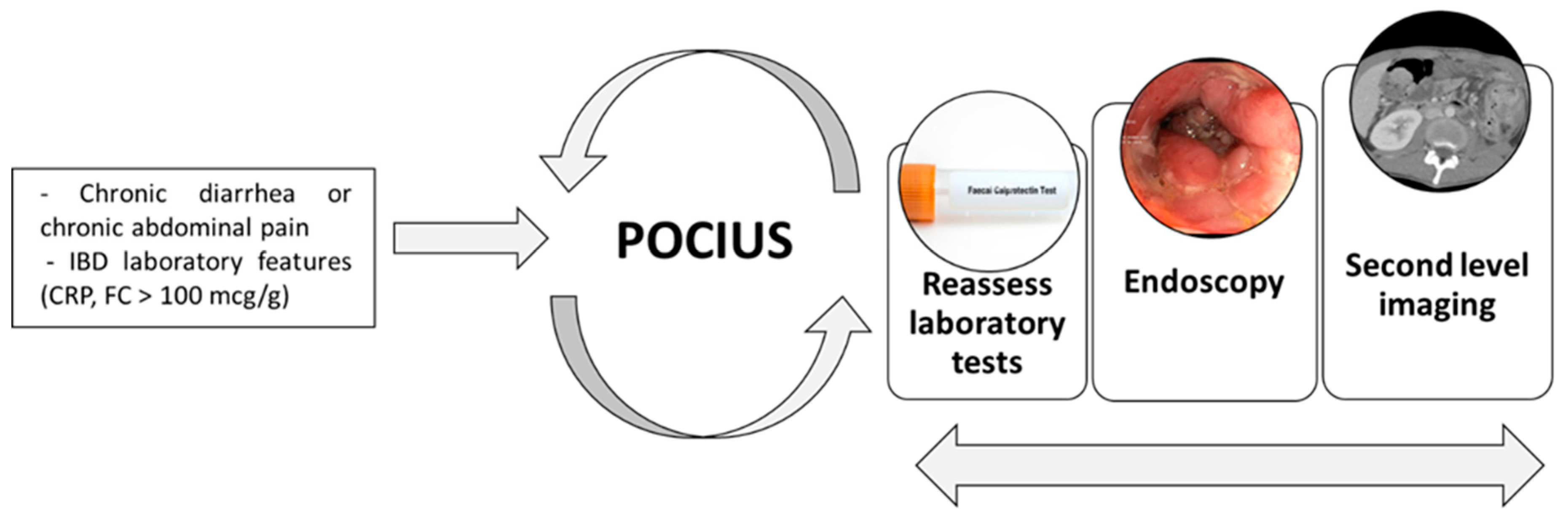

Table 1.
Sensitivity and specificity of IUS in suspected CD compared to endoscopic evaluation.
| STUDY | YEAR | COMPARISON | SEGMENT | SENSITIVITY (%) | SPECIFICITY (%) |
|---|---|---|---|---|---|
| MACONI[12] ET AL. | 1996 | IC, radiology, histology | Ileum, colon | 89.1 | 94 |
| ASTEGIANO[13] ET AL. | 2001 | IC, radiology, clinical evaluation | Ileum, colon | 74 | 98 |
| PARENTE[14] ET AL. | 2002 | IC, radiology, surgery | Ileum, colon | 93.4 | 97.3 |
| PASCU[15] ET AL. | 2004 | IC | Ileum, colon | 82 | 97 |
| PALLOTTA[16] ET AL. | 2005 | IC, radiology, surgery, clinical evaluation | Jejunum, ileum | 57; 94.3 | 100; 98 |
| RISPO[17] ET AL. | 2005 | IC, radiology | Ileum | 92 | 97 |
| CASTIGLIONE[18] ET AL. | 2013 | IC | Ileum, colon | 94 | 97 |
| PALLOTTA[19] ET AL.^ | 2013 | IC, radiology, clinical evaluation | Jejunum, ileum | 75 | 100 |
| RISPO[20] ET AL.* | 2022 | IC, radiology | Ileum, colon | 87.5 | 91.9 |
| IUS: INTESTINAL ULTRASOUND; CD: CROHN’S DISEASE; IC: ILEOCOLONOSCOPY . ^STUDY CONDUCTED ON CHILDREN*IUS HAS BEEN PERFORMED WITH HANDHELD DEVICE | |||||
Table 2.
Sensitivity and specificity of IUS in assessing CD localisation.
| STUDY | YEAR | COMPARISON | SEGMENT | SENSITIVITY (%) | SPECIFICITY (%) |
|---|---|---|---|---|---|
| MACONI[12] ET AL. | 1996 | IC, enteroclysis | Ileum and colon | 89 | 94 |
| REIMUND[23] ET AL. | 1999 | IC, enteroclysis | Ileum and colon | 83 | 67 |
| BRU[24] ET AL. | 2001 | IC | Ileum and colon | 83 | 87 |
| PARENTE[14] ET AL. | 2002 | IC, enteroclysis | Ileum and colon | 93 | 97 |
| PARENTE[25] ET AL. | 2003 | IC, enteroclysis, CT, surgery | Ileum and colon | 77 | 95 |
| PASCU[15] ET AL. | 2004 | IC | Ileum and colon | 74 | 97 |
| PARENTE[26] ET AL. | 2004 | IC, enteroclysis | Small bowel | 96 | 98 |
| MARTINEZ[27] ET AL. | 2009 | IC, enteroclysis, CT | Small bowel and colon | 91 | 98 |
| CASTIGLIONE[18] ET AL. | 2013 | IC, MRE, surgery | Small bowel and colon | 73 | 92 |
| RISPO[28] ET AL. | 2017 | IC, MRE | Small bowel and colon | 78 | 94 |
| ALLOCCA[29] ET AL. | 2018 | IC, MRE | Ileum and colon | 88 | 96 |
| IUS: INTESTINAL ULTRASOUND; CD: CROHN’S DISEASE; IC: ILEOCOLONOSCOPY; MRE: MAGNETIC RESONANCE ENTEROGRAPHY | |||||
Table 3.
Sensitivity and specificity of IUS in assessing CD strictures.
| STUDY | YEAR | COMPARISON | US TECHNIQUES | SENSITIVITY (%) | SPECIFICITY (%) | |
|---|---|---|---|---|---|---|
| GASCHE[33] ET AL. | 1999 | Surgery | US | 100 | 91 | |
| KOHN[34] ET AL. | 1999 | Surgery | US | 75 | 89 | |
| PALLOTTA[35] ET AL. | 2012 | Surgery | US/SICUS | 80 | 75 | |
| ONALI[36] ET AL. | 2012 | Surgery | SICUS | 92 | 0 | |
| KUMAR[37] ET AL. | 2015 | Surgery | SICUS | 88 | 88 | |
| IUS: INTESTINAL ULTRASOUND; CD: CROHN’S DISEASE; SICUS: SMALL INTESTINE CONTRAST ULTRASONOGRAPHY | ||||||
Table 4.
Sensitivity and specificity of IUS in assessing CD abscesses.
| STUDY | YEAR | COMPARISON | US TECHNIQUES | SENSITIVITY (%) | SPECIFICITY (%) |
|---|---|---|---|---|---|
| MACONI[12] ET AL. | 1996 | Endoscopy, CT, enteroclysis | US | 83 | 94 |
| GASCHE[33] ET AL. | 1999 | Surgery | US | 100 | 92 |
| MACONI[38] ET AL. | 2003 | Surgery | US | 80 | 93 |
| ONALI[36] ET AL. | 2012 | Surgery | SICUS | 100 | 80 |
| ALLOCCA[29] ET AL. | 2018 | IC, MRI | IUS | 100 | 96 |
| IUS: INTESTINAL ULTRASOUND; CD: CROHN’S DISEASE; CT: COMPUTED TOMOGRAPHY; MRI: MAGNETIC RESONANTE IMAGING | |||||
Table 5.
Sensitivity and specificity of IUS in assessing CD fistula.
| STUDY | YEAR | COMPARISON | US TECHNIQUES | SENSITIVITY (%) | SPECIFICITY (%) |
|---|---|---|---|---|---|
| MACONI[12] ET AL. | 1996 | Endoscopy, CT, enteroclysis | US | 66 | 96 |
| GASCHE[33] ET AL. | 1999 | Surgery | US | 87 | 90 |
| PALLOTTA[35] ET AL. | 2012 | Surgery | SICUS | 96 | 90.5 |
| ONALI[36] ET AL. | 2012 | Surgery | SICUS | 60 | 88 |
| ALLOCCA[29] ET AL. | 2018 | IC, MRI | IUS | 100 | 98 |
| IUS: INTESTINAL ULTRASOUND; CD: CROHN’S DISEASE; CT: COMPUTED TOMOGRAPHY; IC: ILEOCOLONOSCOPY; MRI: MAGNETIC RESONANCE IMAGING | |||||
Table 6.
Studies assessing UC activity compared to endoscopy.
| STUDY | YEAR | COMPARISON | RESULTS |
|---|---|---|---|
| BOZKURT[56] ET AL. | 1996 | IC, CRP | Three grades based upon BWT > 4 mm, BWS and haustration |
| PASCU[15] ET AL. | 2004 | IC, CRP | Four levels based upon BWT > 3 mm, CD and BWS |
| ANTONELLI[57] ET AL. | 2011 | IC, CRP | BWT > 4 mm |
| ALLOCCA[29] ET AL. | 2018 | IC | BWT > 3 mm, CD, BWS, lymph nodes mesentery inflammation |
| KINOSHITA[54] ET AL. | 2019 | IC, barium studies, clinics | Four grades based upon BWT and BWS |
| ALLOCCA[58] ET AL. | 2021 | IC | MUC ( MUC = 1.4 x BWT +2.0 x CD) > 6.2 |
| BOTS[59] ET AL. | 2021 | IC | UC-IUS (0-7) = BWT >2 mm + CD + haustration + fat wrapping |
| UC: ULCERATIVE COLITIS; IC: ILEO-COLONOSCOPY; CRP: C-REACTIVE PROTEIN; BWT: BOWEL WALL THICKNESS; BWS:BOWEL WALL STRATIFICATION; MUC: MILAN ULTRASOUND CRITERIA; UC-IUS: ULCERATIVE COLITIS INTESTINAL ULTRASOUND | |||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



