
Submitted:
04 May 2023
Posted:
05 May 2023
You are already at the latest version
Abstract
The medical use of Cannabis has a very long history. Although many principles are present in cannabis, called cannabinoids, Δ9tetrahydrocannabinol (Δ9-THC), cannabidiol (CBD) and can-nabinol (CBN) are the three main cannabinoids most present and described. CBD itself is not re-sponsible for psychotropic effects of cannabis since does not produce the typical behavioral effects associated to the consumption of this drug. Cannabidiol (CBD) has recently gained growing at-tention in modern society and seems to be more and more explored in dentistry. Several subjective findings suggest some therapeutic effects of CBD, which are strongly supported by research evi-dence. However, there is a plethora of data regarding CBD’s mechanism of action and therapeutic potential, which are in many cases contradictory. We will first provide an overview of scientific evidence on the molecular mechanism of CBD’s action. Furthermore, we will map the recent de-velopments regarding possible oral benefits of CBD. In summary, we will highlight CBD’s prom-ising biological features for dentistry application, despite exiting patents suggest current the compositions for oral care as the main interest for industry.
Keywords:
plants
; cannabinoids
; CBD
; pharmacology
; dental medicine
; patents
1. Introduction
The use of Cannabis sativa L. for medical purposes dates back to an Egyptian medical papyrus (circa 1550 BC) [1]. Among the multitude of cannabinoids present in this plant, Δ9tetrahydrocannabinol (Δ9-THC), cannabidiol (CBD) and cannabinol (CBN) are the three main cannabinoids most present and best described components due also to their massive presence [2,3].Cannabis is used in three different forms with different THC concentrations: marijuana, hashish and hash oil [4].
Cannabinoids recognize and bind to specific receptors, the main ones being recognized in CB1 and CB2 receptors. They are G-protein-coupled. Their polypeptide chain crosses the cell membrane 7 times. The amine end remains on the extracellular side, while the carboxyl end remains on the intracellular side. They are characterized by three extracellular loops and three intracellular loops (Figure 1).
The CB1 receptor consists of a longer polypeptide chain than CB2 (472 amino acids in CB1, 360 amino acids in CB2). The amino-terminal (extracellular) domain of CB2 is shorter. The complete amino acid sequence of the two receptors is homologous in 44%, in the transmembrane domains the sequence is equal in 68% [5,6] (Figure 2).
Another receptor belonging to the GPCR family that binds to ECs is the G-protein coupled receptor 55 (GPR55), also known as CB3. It is supposed to modulate memory, motor activity and cognitive function because of its high expression in the brain, particularly in the cerebellum [7,8]. At the peripheral level, GPR55s, being present in osteoblasts and osteoclasts, would modulate bone metabolism [9].
Widely present in humans is GPR119, which has been shown to represent another cannabinoid receptor, encoded by the GPR119 gene [8]. It is present predominantly in pancreatic (beta cells) and gastrointestinal cells. Recent studies attributed to GPR119 therapeutic ability on diabetes and obesity by directly acting on insulin release by pancreatic cells and indirectly at the level of intestinal enteroendocrine cells on the production of glucagon-like peptide 1 (GLP-1) [10,11].
Δ9-THC is the main psychoactive principle of cannabis and is known as the canonical agonist of both cannabinoid receptors, namely CB1 and CB2, but with a relatively higher intrinsic affinity for CB1 than for CB2. THC is a hydrophobic and lipophilic compound [12,13]. Thus, many studies have been performed focusing on pharmacology, therapeutic potential and toxicity of Δ9-THC as classical cannabinoid molecule in the last 70 years. These studies promoted the discovery and characterization of the endocannabinoid system (ECS) [14]. ECS is made by G-protein coupled (GPCR) cannabinoid receptors (CB1 and CB2) and their endogenous ligands, anandamide (AEA) and 2-arachidonoylglycerol (2AG), which go under the name of endocannabinoids (ECs) [14]. In addition to CB1 and CB2 receptors, the ECS also includes peroxisome proliferator-activated receptor alpha (PPARα), GPR119, GPR55, transient receptor potential vanilloid 1 (TRPV1) receptors [15]. ECs are metabolized by multiple specific and non-specific enzymes. Amongst the first there are fatty acid amide hydrolase (FAAH, for metabolism of AEA) and monoacylglycerol lipase (MAGL, for metabolism of 2-AG) [16]. Interestingly, since ECs share many structural similarities with prostaglandins several interactions have between shown between metabolic pathways for endocannabinoids and inflammatory lipids, to date lipoxygenases and cyclooxygenases [16].
CB1 and CB2 receptors, encoded by the CNR1 and CNR2 genes, respectively, are the main receptors of ECs. They have different functionalities despite sharing more than 44% of amino acid sequences [17]. CB1 are present in the central nervous system (cerebellum, cerebral cortex, hippocampus, etc.), acting on cognitive functions, memory, locomotion, pain. At the peripheral level CB1s are present in multiple locations, cardiac cells, lung cells, immune cells, reproductive tissues, gastrointestinal system tissues, in the ganglia of the sympathetic nervous system, in the urinary bladder, and in adrenal gland cells, where their functions have been recognized but not well defined [18,19]. Peripherally, CB2 is localized in monocytes/macrophages and poly-morphonuclear neutrophils, lymphocytes and natural killer cells, testis, skeleton, liver and spleen. In the central nervous system (CNS), CB2 is localized in the hippocampus and substantia nigra, neuronal, glial and endothelial cells of the cortex. At the CNS level, the functions of CB2 are not yet clear but it is assumed that it may affect the neuro-immunological system [19] (Figure 3).
CBD has been isolated and described earlier [20] than Δ9-THC however, it has remained a less studied molecule of cannabis forgetting its participation in the psychotropic effects of this plant, since CBD use is not associated to typical behavioral cannabinoid effects [21]. CBD is a unisomer of THC, and is known to produces better effects on anxiety, cognition, pain, with little psychoactivity. Compared with THC, CBD has better affinity for CB1 and CB2 with predominance for the latter and could also interfere with the 'activity of THC [22,23,24].
Cannabinoids are mainly synthetized as acidic forms (A) thus Δ9-THC(A) and CBD(A), are the end-products of the enzymatic biosynthesis of cannabinoids. When exposed to heat (pyrolysis during smoking or baking), radiation, or spontaneously during storage, the compounds undergo decarboxylation and 'spontaneous rearrangement' reactions [25]. C. sativa accumulates THC and CBD in glandular trichomes in the aerial parts of the plant but not on the root surface. Upon trichome thermal or mechanical ruptures, its contents form a sticky coating on the plant surface due the viscous, non-crystallizing properties of cannabinoids, which will protect the plant from dessication and/or potential herbivores [26]. The amount of cannabinoids formed in the thrichomes correlates positively with increased temperatures and imposed heat stress, as well as with low soil moisture and poor mineral nutrient content [27]. Cannabinoid production may also provide an evolutionary advantage by functioning as sun-screens that absorb biologically destructive UV-B radiation (280–315 nm) as significantly increased cannabinoid production was measured in Cannabis flowers after UV-B-induced stress [28]. Furthermore, cannabinoids in general [29], and CBD in particular [30] possesses high antimicrobial action, which confers to cannabis high climate resistance and soil adaptability. Thus phytocannabinoids convey various biologically beneficial properties for the plant.
The use of CBD has always represented a complicated legal issue around the world, which often restricted the scientific studies and professional awareness about its therapeutic application. Apart from this, numerous individual findings suggest some therapeutic effects of CBD, which has been reported to be antipsychotic, anticonvulsant, neuroprotective, anxiolytic and sleep-promoting [31]. Furthermore, pre-clinical and clinical studies attributed to CBD a desirable safety profile [31], associated to its anti-inflammatory effects [32]. However, elucidating the pharmacodynamics of CBD has always proven to be difficult for several scientists, starting from initial reports in which CBD was shown to weakly bind to cannabinoid receptor orthosteric sites, when compared to canonical agonists [33], indicating that CBD effects might be independent of cannabinoid receptors. This conclusion proved to be partially true by other studies, in which researches found direct CBD interaction with several receptors, enzymes and ion channels. Recently however, some reports found both direct and indirect modulation of ECS activity by CBD [33]. Taken together, these findings points out CBD as a novel promising phytocannabinoid-based medicine. Indeed therapeutic uses of CBD are mostly linked to its anti-inflammatory, antioxidant, and analgesic properties [34]. Thus CBD is endowed with many potential application such as in bone tissue processes [35,36], neuroprotection, epilepsy, anxiety and cancer [37]. CBD has also some other effects that are not yet fully studied, including relaxation, sleep improvement and stress relief, given edible, tincture, and vape formulations of the drug (Figure 4).
In the last years, thanks to various public and private institutions, many research and development of CBD have been performed, especially regarding its therapeutic uses. Indeed, approximately USD 30 are expected to be reached by CBD market in 2025 [38]. Amongst the various potential uses of cannabinoids [39] and CBD in particular [40], dentistry and oral medicine have been recently caught growing attention [15]. In particular, studies have been exploring the possible medical applications of CBD use in the oral cavity [41] together with functional and anatomical characterization of the ECS in this body part [15,41,42,43] and its modulation by pathological status [15,44]. The aim of this narrative review is to provide an historical overview on cannabis use and the endocannabinoid system, as well as to explore the mechanism of action of CBD and to summarize the recent scientific and technological discoveries of current CBD use and possible future applications in oral health (Figure 5).
1.1. Cannabis and the Endocannabinoid System in the Human Hystory
Consumed in the form of Marijuana, hashish, or bhang, cannabis sativa extracts are the most widely used recreational drugs, with more than 200 million cannabis users worldwide (World Drug Report 2020, United Nations Publication). Its recreational and therapeutical use are due to its psychoactive effects amongst others, such as changes in sensory perception, relaxation, and euphoria [45]. However, the plant Cannabis Sativa is one of the first plants used by man for fiber, food, medicine, religious or recreational contexts. The first reference to the use of cannabis as medicine comes from a Chinese pharmacological treatise attributed to Emperor Shen Nung (3000 BCE), which makes cannabis one of the recreational drugs with the longest recorded history of human use [45].
The medicinal use of cannabis was present in most ancient civilizations such as Assyrians, Egyptians, Greeks, and Romans. The Aryan, Indo-European populations who lived in ancient Iran and India (source Treccani.it, Britannica.com), employed cannabis in their societies, and given their migrations in prehistoric times, they might have passed on their knowledge [46]. Cannabis had several applications: as a bandage for swelling and bruiser; in fumes for arthritis; either as a drink or in the food for depression of spirits, for kidney stones, for impotence, and for annulling witchcraft. In ancient India, it was prepared in a mild drink, called bhang, and it was described as an anti-anxiety drug thanks to its power «to free from distress» (circa 1500 BCE).
Ancient civilizations were aware of the dual nature of cannabis and its psychoactive proprieties, and some texts defined it as «the drug which takes away the mind». Likewise, accounts of nefarious effects are reported: «hashish eases the muscles of the limbs, but it produces senseless talks», and «if taken in excess it produces hallucinations and a staggering gate. If taken over a long term it causes people to communicate with spirits» [47]. Nonetheless, in some traditions such as Indian medicine, the use of cannabis persisted over centuries. Around 1840, William O’Shaughnessy, an Irish doctor working in India with the British Army, observed the proprieties of cannabis-derived drugs as treatment for cramps, headaches, convulsions, neuralgia, sciatica, and tetanus [46]. The medical use of cannabis was then re-introduced in Europe, and experimental work suggested that the Indian claims about cannabis-based treatment were indeed likely founded [23].
The beginning of the 20th century saw medicinal cannabis curtailed, due to its chemical and physical properties which made impossible the creation of standardized and reliable preparations. In the same period, the development of synthetic fibers, such as nylon, led to a sharp decline in cannabis cultivation for textile purposes [48]. Although cannabis used by textile industries represents a variety without psychoactive properties, called hemp, its application was deeply associated with the drug-like cannabis, marijuana. Indeed, in 1937 a US federal law, the Marijuana Tax Act, restricted the usage and cultivation of all cannabis, without distinction between hemp and marijuana. After that, since its popularization for recreational use all around the world, cannabis was classified as a substance of abuse, and any application of the plant was prohibited [48,49,50].
The prohibition of cannabis had a negative impact also on scientific research. However, investigations on the chemistry and pharmacology of the plant did not completely stop and the analysis of resin extracts allowed the identification of several compounds. Among these, tetrahydrocannabinol (THC) was suspected to be the main psychoactive constituent of cannabis, but its structure was not fully characterized [51]. Only 20 years after, the development of Nuclear Magnetic Resonance (NMR) spectroscopy allowed the designation of Δ9-tetrahydrocannabinol [52]. This event opened new frontiers in understanding cannabis proprieties and its related neuronal substrates. Indeed cannabis is the source of at least 66 compounds now known as cannabinoids [53]. Cannabinol (CBN;, which is probably formed from THC during the conservation of harvested cannabis, was the first plant cannabinoids (phytocannabinoids) to be discovered at the end of the 19th century, from a red oil extract of cannabis. CBN structures was determined in the early 1930s by R.S. Cahn, with its chemical synthesis first achieved in 1940 in the laboratories of R. Adams in the U.S.A. and Lord Todd in the U.K. A second phytocannabinoid, (−)-cannabidiol (CBD), was first obtained from cannabis in the same year by Adams and colleagues, probably associated to cannabidiolic acid, while THCs were first extracted from cannabis in 1942 by Wollner, Matchett, Levine and Loewe, most likely as a mixture of (−)-Δ8- and (−)-Δ9-THC. Both THC and CBD are present in cannabis mainly as decarboxylated acids upon cannabis heating and combustion. The structures and stereochemistry of CBD and Δ9-THC, naturally occurring as (−)-enantiomer, were discovered by Raphael Mechoulam and colleagues, in particular in 1963 for CBD and in 1964 for Δ9-THC, respectively. It was also in Mechoulam's laboratory, in 1965, that (±)-Δ9-THC and (±)-CBD were first synthesized, developments that were soon followed by the synthesis of the (+)- and (−)-enantiomers, both of these two cannabinoids and of Δ8-THC [54].
Since the last decade, in several countries all around the world cannabis legislation changed. A large number of countries around the world approved the legalization of medicinal cannabis and hemp (finally discerned by marijuana). Additionally, Uruguay, Canada, Georgia, Mexico, South Africa, and 18 US states, legalized recreational cannabis consumption, and in many other countries mostly in Asia, the use of cannabis is decriminalized [55]. Globally, the public acceptance of legalizing cannabis and its medical application increase, and therefore a better understanding of its plethora of effects on the human brain and body is of central interest.
After the THC discovery extensive studies on pharmacology and biochemistry of cannabis were carried on, with particular interest regarding the mode of action of THC, and other cannabinoids of the plant. Two mechanisms were postulated: the first hypothesis was based on the lipophilic nature of cannabinoids, suggesting that they might act via chemical interaction with biological membranes, modifying their proprieties; the second one suggested that cannabinoids might act through still undiscovered receptors, thereby modulating cellular signaling. This second hypothesis was based on the observation that THC acts reducing the activity of adenylyl cyclase (AC), but only in particular cell types, indicating the specific and not ubiquitous action of THC, as expected for cannabinoid-induced membrane fluidity changes [56].
The development of synthetic cannabinoids helped to address this issue. Indeed, compounds such as CP-55,940, 10-100 times more potent in vivo than THC, allowed the autoradiography of cannabinoid-specific binding sites in brain sections from several mammalian species, including human. The study revealed a specific and conserved labeling profile, suggesting the presence of a specific receptor [56,57].
In 1990, at a conference of the National Academy of Science’s Institute of Medicine, Dr. Lisa Matsuda announced a fundamental discovery, the identification of the precise DNA sequence coding for THC-sensitive receptors. These were highly expressed in the brain, in accordance with the psychoactive effects of cannabinoids. The receptor was successfully cloned and called Cannabinoid-type1 receptors (CB1; [58]). Even though its physiological role was still a mystery, the high-level of expression and distribution of CB1 receptors suggested the existence of endogenous ligands. Few years after, in 1992, an endogenous brain molecule binding to the same receptor that is sensitive to THC has been identified. This substance, arachidonoylethanolamide (AEA), was called Anandamide after the sanskrit word ananda (bliss). Composed by ethanolamide and arachidonic acid, it represents the first discovered endogenous cannabinoid, or endocannabinoid (eCB; [59]). From now, the interest of research in the field of cannabinoids notably increased, leading to fundamental discoveries. Munro and colleagues, in 1993, identified a second receptor, CB2 that differently from CB1, is mainly expressed in peripheral cells and in the immune system [60]. Furthermore, a second endocannabinoid has been discovered, 2-arachidonoylglycerol (2-AG), which similarly to AEA, is a derivative of arachidonic acid [61]. Altogether, this evidence promoted the concept of the endocannabinoid system (ECS), which participates in the regulation of physiological processes [62]. The ECS was then identified in several animal species, including cnidaria, the first animal organism to have develop a neural network [63]. The high degree of evolutionary conservation of the ECS across the species, suggest its importance in physiology, animal adaptation and survival [64].
1.2. Biological Targets of CBD Action
GPCRs. As previously introduced, binding of CBD to cannabinoid receptors is relatively weak [33,65] although, one exception of a partial CBD agonism of human CB2 receptors in heterologous system has been reported [65]. However, low concentrations of CBD, are able to antagonize the effects CB1 and CB2 receptors agonists [66], a phenomenon explained by a negative allosteric receptor-modulation of by recent pharmacological studies [33,65,67]. On the other hand, CBD’s main mechanisms action have been proposed to be independent from the ECS. Several evidence proposed that some of these effects seem be mediated by the serotoninergic 5HT1a receptor (5HT1a), is coupled to the Gi protein (like CB1 and CB2). Indeed, although a relatively weak binding to 5HT1a, CBD showed a positive allosteric modulation of this receptor [68,69]. Various orphan GPCRs have also been proposed as targets for CBD. This drug antagonizes GPR55 [70], involved in actin cytoskeletal processes during movement and migration [71] (thanks to G13 alpha coupling). CBD is also an inverse agonist for GPR3, GPR6 and GPR12 [72], which can explain CBD actions both on cell survival, proliferation and neurite outgrowth as well as neuropathic pain [72]. Other Gi-coupled receptors have been proposed by many studies as binding sites for CBD, like μ- and δ-opioid, high-affinity D2- and D3-dopamine receptors [73].
Ionotropic Receptors. The physiological effects of CBD might significantly be explained by its high affinity for inotropic receptors. CBD potently activates cationic channels belonging to the family of transient receptor potential (TRP) channels on different cell types (in particular TRPA1, TRPV1, TRPV2 and TRPV4 [74,75,76,77]]). Further ionotropic receptors negatively modulated by CBD are TRPM8, which is directly antagonized [78], and α7 nicotinic acetylcholine receptor and serotonin receptor 5HT3a [79,80] on which CBD acts as a negative allosteric modulator. Positive allosteric modulator by CBD has been observed for anionic ion channels, such as glycine (GlyRs) and GABAA receptors [81,82]. CBD also acts on voltage-gated calcium Cav3.1/Cav3.2 and sodium channels Cav3.3, inhibiting cationic currents, as well as decreasing the conductance of voltage-dependent anion channel 1 (VDAC1) [83,84,85].
Transporters. Several reports highlighted CBD interaction with intracellular transporters of endocannabinoids, with a direct inhibition of anandamide uptake, in particular fatty acid binding proteins (FABP) 1, 3, 5 and 7, resulting in potentiation of ECs actions [86]. Indeed, CBD boosts AEA levels in rat brains in and in human serum via an N-acyl phosphatidylethanolamine phospholipase D dependent mechanism [87,88]. Another target for the anti-inflammatory and sedating effects of CBD is the blockade of adenosine uptake acting through the equilibrative nucleoside transporter (ENT) [89,90]. ATP-binding cassette super-family G member 2 (ABCG2) or P-glycoprotein), multidrug resistance proteins (multidrug resistance-associated protein 1 (ABCC1) and Mg2+-ATPase also have been showed to be modulated by CBD [91,92] (Figure 3).
Enzymes. CBD also modulates the activity of several enzymes. First, the members of cytochrome P450 superfamily (CYPs) as their interaction with CBD may influence clearance of various drugs, including non-steroidal anti-inflammatory ones. CBD inhibits various CYPs superfamily members (CYP1B1, CYP2C19, CYP2C9, CYP3A4 and CYPC3A70) [93]. According to its structural properties, CBD it also might interact with various lipid metabolism enzymes, and in particular AEA. Indeed FAAH activity is inhibited by with discrepant results between rat and human isoforms [74,75]. Interestingly Lipooxygenases (LOXs), are targets of CBD [94]. Always in regarding inflammatory processes CBD stimulates COX1 and COX2 while inhibiting phospholipase A2 (PLA2) [95,96]. At mitochondrial level, CBD is able to inhibit, although with low potency, mitochondrial complex I, II and IV [97]. CBD also interferes with serotonin to melatonin metabolism, as well as with in tryptophan catabolism, by acting on indoleamine-pyrrole 2,3-dioxygenase (IDO) [98,99]. CBD’s interaction with enzymes involved in steroid metabolism such as acyl-CoA cholesterin acyltransferase (ACAT) or testosterone hydroxylase were examined in few studies although not consistent results were provided [100,101].
Nuclear factors. In the context of inflammation, nuclear receptor peroxisome proliferator-activated receptor gamma (PPARγ) appears to be one of the most relevant targets of CBD. Indeed CBD is a weak full agonist] of this receptor [102]. Moreover, nuclear factor erythroid-derived 2-like 2 (Nrf2) in activated microglia, is also described as a putative culprit for alterations of inflammatory gene expression patterns by CBD [103].
Inflammatory mediators. Mechanistically, CBD administration is currently known to suppress the immune responses by impairing cytokine production and inflammation [104]. As previously mentioned CBD affinity for CB1 and CB2 receptors is not very high, thus its pharmacological activity might not mediated by cannabinoid receptors. Instead, CBD exerts anti-inflammatory action by modulating TRPV1 receptor, as shown by blockage of CBD-effects by TRPV1 antagonists [105,106]. A regulation of immune responses by the Janus kinase/signal transducers and activators of transcription (JAK/STAT) signaling pathway, is also negatively modulated by CBD. Indeed, triggering of JAK/STAT via release of TNF-α, Interferon-γ (IFN- γ), Interleukin-1 (IL-1), IL-2, and IL-6, inflammatory cytokine, is attenuated by CBD in vitro and in vivo [107]. CBD is also capable to prevent nucleotide-binding oligomerization domain-like receptors (NLR) inflammasome complex activation, involving NF-κB, MAPK, and IFN pro-inflammatory pathways, thereby reducing pro-inflammatory cytokines, such as IL-1β and IL-18 [108]. Furthermore, inhibition of rapid cellular uptake of adenosine by ENT [89], CBD has also been studied to modulate adenosine, inducing protective anti-inflammatory effects via A2A receptor [109]. Thus, during inflammation, inhibition of intracellular adenosine uptake by CBD might promotes a protective signaling mechanism [109]. In summary, understanding the mechanism behind the pharmacological reduction of inflammation by CBD will further provide a strong rationale for the medical use of CBD as a novel therapeutical option for inflammatory diseases (Figure 4).
1.3. CBD in Dentistry
1.3.1. Oral mucosa
In the use of cannabinoids, the oral mucosa is the tissue that primarily comes into contact and interacts with them. Studying their physiological, therapeutic and non-therapeutic role in more detail, and evaluating their effects is of 'significant importance.
CB1 and CB2 receptors have been detected on oral mucosal epithelial cells. They modulate their functions: CB2s stimulate the proliferation and differentiation of human epithelial keratinocytes while CB1s have the opposite effect [18].
Cannabinoid receptors, CB1 and CB2, have also been identified at the level of the connective tissue of the lamina propria. However current scientific data regarding cannabinoids on receptors in oral mucosal tissues are still scarce [110]. Interestingly, CB1 and CB2 receptors are also present in the epithelial cells and taste buds of the tongue where their function would appear to be regulated by the physiological-pathological conditions of the tongue [110]. One example is the presence of burning mouth syndrome, which is associated to a decrease of CB1 expression while CB2 expression increases. Also oncological conditions such as mobile tongue squamous cell carcinoma, seems to involve activation of ECS, since expression of both CB1 and CB2 receptors has been shown to be increased [111,112]. There are few data on CB1 and CB2 receptors presence in the dental pulp, where CB1 receptors have been detected in the sympathetic nerve fibers of the and on the surface of the pulp bordering dentin [113]. This would suggest a possible therapeutic target against dental pain, although this role of cannabinoids needs further study. CB1s are also present on human odontoblasts where it is proposed to respond to immune challenges [114,115]. Indeed its activation and subsequent cyclic adenosine mono-phosphate (cAMP) signaling enables tran-sient receptor potential vanilloid 1 (TRPV1)-mediated extracellular Ca(2+)ion passage (TRPV1) via extrusion Na(+)-Ca(2+) exchangers (NCXs), promoting the production of a secondary dentin bridge in re-sponse to odontoblast stimuli [116]. In the salivary glands, CB1 and CB2 receptors have specific localizations. In the major salivary glands, CB1 expression is found at the striatal duct cells, while CB2 is found in the acinar cells, especially in the myoepithelial cells, deputed to the secretion of saliva [117,118]. Interestingly, the presence and distribution of CB1s in salivary glands would appear to be regulated by the type and amount of food [119] and, furthermore, salivary secretion is modulated by both CB1 and CB2 receptors [120,121,122].
1.3.2. Periodontal tissue
CB1 and CB2 receptors are expressed in the periodontium, and their distribution changes based on periodontal tissue conditions [42]. In healthy periodontium CB1s are more highly expressed in the periodontal ligament(PDL), and are more active in the 'epithelium than in the PDL [123,124]. Interestingly, the presence of bacteria increases the expression of CB2 receptors, whereas in a situation of sterile inflammation, both receptors are more highly expressed in DPL, but not in cementum and alveolar bone [125]. Thus different expression patterns of the two receptors would appear to be related to different cellular at-activity (differentiation and proliferation), control of inflammation, and healing of the affected site [126]. Several reports seem to suggest a role for CB2 in periodontal tissue healing, especially by modulating migration and adhesion of periodontal cells upon input from the focal adhesion kinase (FAK) and mitogen-activated protein kinase (MAPK) system [124,126,127,128].
Consistent beneficial effects of CBD have been described in vitro and in vivo in addition to conventional periodontal therapy. Using the CBD analog HU-308, authors found a role for CB2 receptor in modulating the extent of periodontal damage and its impact on the gingival tissue, alveolar bone, and salivary function [129]. In the same study, CBD possessed anti-inflammatory and anti-bone resorption properties, by inhibiting the RANK/RANKL system and reducing levels of pro-inflammatory cytokines [129]. An alternative approach to periodontal therapy might be the CBD-mediated activation of gingival fibroblasts with repairing growth factors and/or the inhibition of metalloproteinases [130,131]. CBD has also been observed to attenuate bacterial inflammatory periodontal diseases thanks to its have antimicrobial properties [132,133]. This drug might also be a suitable medicinal alternative in oral mucositis, given its anti-inflammatory properties, which can reduce lesions’ severity and extent [36,134] since, CBD also promotes the curative process of common ulcers. Similarly to synthetic oral medicines CBD is as effective in reducing the bacterial charge in dental plaque [133]. Furthermore, CBD is endowed with biocompatibility and osteoinductivity [126,135] as shown to promote fracture healing possibly activating p42/44 pathway in mesenchymal cells which then differentiate into osteoblasts [73] at the lesion site. Thus, analgesic, anti-inflammatory, biological, antimicrobial, and osteoinductive properties of CBD might underlie its positive effects in dentistry as suggested by most of the recent literature suggests. This paved the way to the development of some patents for the implement of CBD formulations in dentistry.
2. Discussion
The subjects described in the studies on possible CBD use in dentistry, as well as the patents reviewed which will be discussed in the following sections are endodontic therapy, periodontology, oral medicine, and oral surgery, together with the oral heath potentials of CBD, and the future research questions.
Endodontic therapy (direct hooding). The exposure and subsequent bacterial contamination of exposed vital dental pulp as a result of trauma, deep caries is a treatment that if not well performed could lead to pulp inflammation, pain and necrosis, in immature teeth to an arrest of the root maturation process, with risk of loss of dental elements [136]. Thus, induction of odontogenesis, using bioactive materials, would lead to the preservation of pulpal viability [137].
Given the expression of cannabinoid receptors in dental pulp it is not surprising that that cannabinoids (including CBD) induced odonto/osteogenic differentiation, stimulating proliferation ,migration and differentiation of dental pulp stem cells , producing increased collagen synthesis and mineralization, with protective effects on pulpal vitality in some studies [114,136,138]. Furthermore, CBD is also capable to inhibit the action of TNF-α which blocks stem cell differentiation, reduces the action of pro-inflammatory cytokines TNF-α, interleukin (IL)-1β and IL-6 [139] and, by activating CB1 receptors, to stimulate extracellular Ca 2+ entry inducing reparative dentin formation in odontoblasts [140,141].
By activating CB2 receptors, and stimulating Mitogen-Activated Protein Kinase (MAPK) pathway, CBD enhances the expression of angiogenic and odontogenic genes, such as Osteopontin (OPN), RUNX family transcription factor 2 (Runx2), Vascular Endothelial Growth Factor- Based angiostatics (VEGFR1), intercellular adhesion molecule 1(ICAM-1), dentinal sialophosphoprotein (DSPP), dentinal matrix acid phosphoprotein 1(DMP-1), alkaline phosphatase (ALP) [136,142,143].
Periodontal Therapy. In a pre-clinical model of periodontitis, CBD is able to prevent alveolar bone loss [131] thanks to its anti-inflammatory action. Indeed the specific activation of CB2 receptors by CBD is endowed by analgesic and anti-inflammatory benefits, preventing any secondary effects due to CB1 receptors activation [34,104], since CB2 receptors activation physiologically protects periodontal tissues against excess inflammatory processes [131]. Furthermore, the antagonistic effect of CBD on NT-kB, prevents the production of interleukins and other inflammatory mediators such as cytokines, chemokines, and pro-inflammatory growth factors [104]. This effect is often accompanied to reduced macrophage and neutrophil migration with less oxidative stress [104]. As for the ECs, the anti-inflammatory potential of CBD, directly or indirectly act trough cannabinoid receptors [34,104], and is often associated to increased gingival fibrosis, with CBD increasing the production of gingival fibroblasts [130], via induction of transforming growth factor beta (TGFβ) levels [130]. Last but not least, CBD-induced increase in the levels of AEA, may also promote fibrosis via cannabinoid and other receptors [135].
Oral Medicine. Anti-inflammatory and analgesic readouts of CBD administration are dose-dependent, without ideal doses having possible antioxidant and anti-inflammatory action [36,73,144]. This synergy between different CBD effects may render this drug more potent than classical antioxidants, against pathological states such as oral mucositis [41,145]. Thus CBD is a novel potential therapy for the treatment of symptoms characterizing this condition, improving epithelial changes in ulcer lesions extent in vivo [41,145]. An important feature of CBD for generating this type of tissue response is the action on keratinocytes with no undesirable effects. However, despite reducing the global inflammatory status, CBD did not accelerate wound healing [134] making keratinocytes action of this drug controversial with the need of understanding its mechanisms of action. In vivo administration of the synthetic analog HU-308 [129], prevented inflammation and alveolar bone loss in gingival tissues in a model of LPS periodontitis. This effect, mediated by CB2 receptors, was mainly localized and due to reduced osteoclastogenesis, indicating CB2 receptor-mediated prevention of bone loss by targeting bone cells together with inhibition of pro-reabsorption factors [129]. CBD is also effective as antimicrobial agent. Indeed high doses of CBD suppresses the growth of key bacterial components of subgingival microbiota in dental plaque [133]. Dental plaque is mainly composed by Gram-positive bacteria, susceptible targets for the well-known antimicrobial action of CBD mentioned above [30,139]. When compared with other oral hygiene products, CBD strikingly reduced the density in bacterial colonies like other well-established oral hygiene formulations with variations in efficacy due to the heterogeneity of oral biofilms [133].
Traumatology/Surgery. As previously mentioned, CBD possess promising biological and osteoinductive properties. Alone or in combination with other drugs, CBD effectively and consistently improved cell migration and bone differentiation migration of microglial cells via the ECS [131]. ECS is present in both skeletal sympathetic nerves and bone cells, and cannabinoids play a key role in homeostasis of bone mass [15]. In this scenario, CBD has been shown to stimulate the expression of PLOD1 gene [73,146], showing an increased collagen maturation which triggers bone protein expression and mineralization. These actions may results in neobone formation and improvement of bone tissue biomechanical properties, making CBD a suitable therapeutical adjuvant for bone loss due to surgery or trauma.
Other comorbidities
CBD can be useful in patients with malignancies. Indeed, a frequent side effect of cancer-related chemotherapy and radiation, which kills both cancerous and healthy tissues, is oral mucositis. Despite the paucity of research, CBD antioxidant properties imply that it might be used to reduce the oxidative stress linked to oral mucositis [145]. Furthermore, the most upsetting side effects experienced by oncology patients receiving anticancer treatments are nausea and vomiting. This can bear severe consequences in the mouth as the acidity of gastric juice favors alteration of the oral microbiota with inflammation of the mucosa as well as erosion of dental enamel. Vomiting and nausea in particular continue to be difficult to cure with the present therapies, stressing the need for substitute therapies. In this scenario CBD proved to be effective in reducing nausea and vomiting [147], and might attenuate all oral cavity related-damages [148]. Another application of CBD representing a possible advantage in dentistry is in the treatment of arthritis that often involves the temporomandibular joint. Indeed CBD has shown potential beneficial effects in preclinical studies for reducing inflammation and pain associated with arthritis [149]. For example, CBD inhibits T-cell proliferation, thus preventing the production of IFN- and TNF- and the development of Th1-mediated autoimmune rheumatoid arthritis [150]. Due primarily to its anti-inflammatory and antioxidant qualities, CBD has a variety of advantageous effects in the context of hyperglycemia. Interestingly, type 2 diabetes and obesity have both been linked to chronic overactivation of the endocannabinoid system [151] which raises the possibility that CBD could also be used therapeutically to treat type 2 diabetes [152]. Indeed this pathological state has an important impact on oral health and in particular oral infections brought on by diabetes can also get worse [153]. Last but not least, CBD is also effective in treating epilepsy, according to randomised, placebo-controlled research that showed a significant reduction in seizure frequency [154,155]. This CBD effect might also possess beneficial aspects on oral health as it reduces the risk of trauma and injuries to the lip and oral tissues that often occur during epileptic seizures [156].
Current scientific and technological knowledge. According to the recent studies on the actions of CBD in the mouth, there is a growing attention in technological exploitation and appropriation relative the implementation of CBD preparations in dentistry. However, only one patent [157] published in 2018 was accompanied by in a scientific study [130] in 2020, despite the increasing progress for this kind of developments. The patents registered for applying CBD in dentistry are mostly related to oral care formulations rather than its use for oral diseases. Thus, given also the modern tendency in the use of natural products [158] there is plenty of space for CBD exploration for potential dentistry-related applications. Furthermore, thanks to the low cost of these plant derived compounds [159] nowadays CBD and synthetic analogs are promising drugs for several diseases. However, also some limitation can be highlighted. First, there is no clear governmental regulation for the quality of CBD [160], which could result in different sources of its manufacture, leading to variable efficiency of CBD preparations. Second, the components of plant-derived natural products vary greatly, because of the heterogeneity in environmental conditions, making the quality and the levels of natural products depend on several conditions, such as vegetation, geographic location, extraction conditions [161]. Therefore, natural preparation may contain different chemicals that influence their therapeutic activities. Second, there is no standardized practice of analytical techniques characterizing the products. Thus changes in control of these materials’s origin, storage conditions, production and possible contaminations, are all factors to be kept into account for the value of products and their therapeutic effects [162].
3. Conclusions
Despite the growing interest of CBD use for medical purposes, little scientific literature and few patents are nowadays present its applications in oral health. Studies on the effects of cannabis use on oral tissues and oral health are irrelevant. Research evidence so far promotes CBD as analgesic, antimicrobial, anti-inflammatory, and osteoinductive drug with potential application in periodontal and dentistry applications, although patents available relies on compositions for oral care products such as toothpaste, mouthwash, and dental floss.
Author Contributions
Conceptualization, L.B., A.P., A.D.I., A.M.I. and G.M.; methodology, F.I., G.D., B.R., E.D.R., and A.M.I., software, C.G.I., F.L. A.S. and G.D.; validation, L.B., A.P., F.I., G.M., A.S. and A.M.I.; formal analysis, L.B., A.P., A.D.I. and G.M.; resources, A.D.I., A.M.I., A.M., G.M., F.L. and B.R.; data curation, L.B., C.G.I., E.D.R. and G.D.; writing—original draft preparation, A.D.I., A.P., A.M., E.D.R., F.I. and G.D.; writing—review and editing, A.P., F.L., A.S., A.M., and A.M.I. visualization, C.G.I., B.R., A.D.I. and F.I..; supervision, L.B., A.S., G.M. and F.I.; project administration, L.B., F.I. and A.M.I.. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| Δ9-THC | Δ9tetrahydrocannabinol |
| CBD | cannabidiol |
| ECS | endocannabinoid system |
| GPCR | cannabinoid receptors |
| AEA | anandamide |
| 2AG | 2-arachidonoylglycerol |
| FAAH | fatty acid amide hydrolase |
| MAGL | monoacylglycerol lipase |
| 5HT1a | 5HT1a receptor |
| TRP | transient receptor potential |
| GlyRs | glycine |
| FABP | fatty acid binding proteins |
| ENT | equilibrative nucleoside transporter |
| ABCG2 | ATP-binding cassette super-family G member 2 |
| LOXs | Lipooxygenases |
| PLA2 | phospholipase A2 |
| IDO | indoleamine-pyrrole 2,3-dioxygenase |
| ACAT | acyl-CoA cholesterin acyltransferase |
| PPARγ, | peroxisome proliferator-activated receptor gamma |
| Nrf2 | nuclear factor erythroid-derived 2-like 2 |
| IFN- γ | Interferon-γ |
| IL-1 | Interleukin-1 |
| NLR, | nucleotide-binding oligomerization domain-like receptors |
| TGFβ | transforming growth factor beta |
References
- Russo, E.B. History of Cannabis and Its Preparations in Saga, Science, and Sobriquet. Chem. Biodivers. 2007, 4, 1614–1648. [Google Scholar] [CrossRef]
- Ladha, K.S.; Ajrawat, P.; Yang, Y.; Clarke, H. Understanding the Medical Chemistry of the Cannabis Plant Is Critical to Guiding Real World Clinical Evidence. Molecules 2020, 25, 4042. [Google Scholar] [CrossRef]
- Lowe, H.; Steele, B.; Bryant, J.; Toyang, N.; Ngwa, W. Non-Cannabinoid Metabolites of Cannabis Sativa L. with Therapeutic Potential. Plants 2021, 10, 400. [Google Scholar] [CrossRef]
- Joshi, S.; Ashley, M. Cannabis: A Joint Problem for Patients and the Dental Profession. Br. Dent. J. 2016, 220, 597–601. [Google Scholar] [CrossRef]
- Hua, T.; Vemuri, K.; Pu, M.; Qu, L.; Han, G.W.; Wu, Y.; Zhao, S.; Shui, W.; Li, S.; Korde, A.; et al. Crystal Structure of the Human Cannabinoid Receptor CB1. Cell 2016, 167, 750–762.e14. [Google Scholar] [CrossRef]
- Li, X.; Hua, T.; Vemuri, K.; Ho, J.-H.; Wu, Y.; Wu, L.; Popov, P.; Benchama, O.; Zvonok, N.; Locke, K.; et al. Crystal Structure of the Human Cannabinoid Receptor CB2. Cell 2019, 176, 459–467.e13. [Google Scholar] [CrossRef]
- Moriconi, A.; Cerbara, I.; Maccarrone, M.; Topai, A. GPR55: Current Knowledge and Future Perspectives of a Purported “Type-3” Cannabinoid Receptor. Curr. Med. Chem. 2010, 17, 1411–1429. [Google Scholar] [CrossRef]
- Godlewski, G.; Offertáler, L.; Wagner, J.A.; Kunos, G. Receptors for Acylethanolamides—GPR55 and GPR119. Prostaglandins Other Lipid Mediat. 2009, 89, 105–111. [Google Scholar] [CrossRef]
- Whyte, L.S.; Ryberg, E.; Sims, N.A.; Ridge, S.A.; Mackie, K.; Greasley, P.J.; Ross, R.A.; Rogers, M.J. The Putative Cannabinoid Receptor GPR55 Affects Osteoclast Function in Vitro and Bone Mass in Vivo. Proc. Natl. Acad. Sci. 2009, 106, 16511–16516. [Google Scholar] [CrossRef]
- Overton, H.A.; Fyfe, M.C.T.; Reynet, C. GPR119, a Novel G Protein-Coupled Receptor Target for the Treatment of Type 2 Diabetes and Obesity. Br. J. Pharmacol. 2008, 153, S76–S81. [Google Scholar] [CrossRef]
- Chu, Z.-L.; Jones, R.M.; He, H.; Carroll, C.; Gutierrez, V.; Lucman, A.; Moloney, M.; Gao, H.; Mondala, H.; Bagnol, D.; et al. A Role for β-Cell-Expressed G Protein-Coupled Receptor 119 in Glycemic Control by Enhancing Glucose-Dependent Insulin Release. Endocrinology 2007, 148, 2601–2609. [Google Scholar] [CrossRef] [PubMed]
- Howlett, A.C. International Union of Pharmacology. XXVII. Classification of Cannabinoid Receptors. Pharmacol. Rev. 2002, 54, 161–202. [Google Scholar] [CrossRef] [PubMed]
- Garrett, E.R.; Hunt, C.A. Physicochemical Properties, Solubility, and Protein Binding of Δ9 -Tetrahydrocannabinol. J. Pharm. Sci. 1974, 63, 1056–1064. [Google Scholar] [CrossRef]
- Piomelli, D. The Molecular Logic of Endocannabinoid Signalling. Nat. Rev. Neurosci. 2003, 4, 873–884. [Google Scholar] [CrossRef] [PubMed]
- Bellocchio, L.; Inchingolo, A.D.; Inchingolo, A.M.; Lorusso, F.; Malcangi, G.; Santacroce, L.; Scarano, A.; Bordea, I.R.; Hazballa, D.; D’Oria, M.T.; et al. Cannabinoids Drugs and Oral Health—From Recreational Side-Effects to Medicinal Purposes: A Systematic Review. Int. J. Mol. Sci. 2021, 22, 8329. [Google Scholar] [CrossRef] [PubMed]
- Toczek, M.; Malinowska, B. Enhanced Endocannabinoid Tone as a Potential Target of Pharmacotherapy. Life Sci. 2018, 204, 20–45. [Google Scholar] [CrossRef] [PubMed]
- Felder, C.C.; Joyce, K.E.; Briley, E.M.; Mansouri, J.; Mackie, K.; Blond, O.; Lai, Y.; Ma, A.L.; Mitchell, R.L. Comparison of the Pharmacology and Signal Transduction of the Human Cannabinoid CB1 and CB2 Receptors. Mol. Pharmacol. 1995, 48, 443–450. [Google Scholar] [PubMed]
- Maccarrone, M.; Di Rienzo, M.; Battista, N.; Gasperi, V.; Guerrieri, P.; Rossi, A.; Finazzi-Agrò, A. The Endocannabinoid System in Human Keratinocytes. J. Biol. Chem. 2003, 278, 33896–33903. [Google Scholar] [CrossRef]
- Howlett, A.C.; Abood, M.E. CB 1 and CB 2 Receptor Pharmacology. In; 2017; pp. 169–206.
- Adams, R.; Hunt, M.; Clark, J.H. Structure of Cannabidiol, a Product Isolated from the Marihuana Extract of Minnesota Wild Hemp. I. J. Am. Chem. Soc. 1940, 62, 196–200. [Google Scholar] [CrossRef]
- Mechoulam, R.; Shani, A.; Edery, H.; Grunfeld, Y. Chemical Basis of Hashish Activity. Science (80-. ). 1970, 169, 611–612. [Google Scholar] [CrossRef]
- Hall, W.; Degenhardt, L. Adverse Health Effects of Non-Medical Cannabis Use. Lancet 2009, 374, 1383–1391. [Google Scholar] [CrossRef] [PubMed]
- Mechoulam, R.; Hanuš, L.O.; Pertwee, R.; Howlett, A.C. Early Phytocannabinoid Chemistry to Endocannabinoids and Beyond. Nat. Rev. Neurosci. 2014, 15, 757–764. [Google Scholar] [CrossRef]
- Pisanti, S.; Malfitano, A.M.; Ciaglia, E.; Lamberti, A.; Ranieri, R.; Cuomo, G.; Abate, M.; Faggiana, G.; Proto, M.C.; Fiore, D.; et al. Cannabidiol: State of the Art and New Challenges for Therapeutic Applications. Pharmacol. Ther. 2017, 175, 133–150. [Google Scholar] [CrossRef] [PubMed]
- Tahir, M.N.; Shahbazi, F.; Rondeau-Gagné, S.; Trant, J.F. The Biosynthesis of the Cannabinoids. J. Cannabis Res. 2021, 3, 7. [Google Scholar] [CrossRef]
- Gülck, T.; Møller, B.L. Phytocannabinoids: Origins and Biosynthesis. Trends Plant Sci. 2020, 25, 985–1004. [Google Scholar] [CrossRef] [PubMed]
- Bazzaz, F.A.; Dusek, D.; Seigler, D.S.; Haney, A.W. Photosynthesis and Cannabinoid Content of Temperate and Tropical Populations of Cannabis Sativa. Biochem. Syst. Ecol. 1975, 3, 15–18. [Google Scholar] [CrossRef]
- Eichhorn Bilodeau, S.; Wu, B.-S.; Rufyikiri, A.-S.; MacPherson, S.; Lefsrud, M. An Update on Plant Photobiology and Implications for Cannabis Production. Front. Plant Sci. 2019, 10. [Google Scholar] [CrossRef] [PubMed]
- van Klingeren, B.; ten Ham, M. Antibacterial Activity of Δ9-Tetrahydrocannabinol and Cannabidiol. Antonie Van Leeuwenhoek 1976, 42, 9–12. [Google Scholar] [CrossRef]
- Schofs, L.; Sparo, M.D.; Sánchez Bruni, S.F. The Antimicrobial Effect behind Cannabis Sativa. Pharmacol. Res. Perspect. 2021, 9. [Google Scholar] [CrossRef]
- Iffland, K.; Grotenhermen, F. An Update on Safety and Side Effects of Cannabidiol: A Review of Clinical Data and Relevant Animal Studies. Cannabis Cannabinoid Res. 2017, 2, 139–154. [Google Scholar] [CrossRef]
- Atalay, S.; Jarocka-Karpowicz, I.; Skrzydlewska, E. Antioxidative and Anti-Inflammatory Properties of Cannabidiol. Antioxidants 2019, 9, 21. [Google Scholar] [CrossRef]
- Tham, M.; Yilmaz, O.; Alaverdashvili, M.; Kelly, M.E.M.; Denovan-Wright, E.M.; Laprairie, R.B. Allosteric and Orthosteric Pharmacology of Cannabidiol and Cannabidiol-Dimethylheptyl at the Type 1 and Type 2 Cannabinoid Receptors. Br. J. Pharmacol. 2019, 176, 1455–1469. [Google Scholar] [CrossRef]
- Burstein, S. Cannabidiol (CBD) and Its Analogs: A Review of Their Effects on Inflammation. Bioorg. Med. Chem. 2015, 23, 1377–1385. [Google Scholar] [CrossRef]
- Apostu, D.; Lucaciu, O.; Mester, A.; Benea, H.; Oltean-Dan, D.; Onisor, F.; Baciut, M.; Bran, S. Cannabinoids and Bone Regeneration. Drug Metab. Rev. 2019, 51, 65–75. [Google Scholar] [CrossRef]
- Whyte, L.; Ford, L.; Ridge, S.; Cameron, G.; Rogers, M.; Ross, R. Cannabinoids and Bone: Endocannabinoids Modulate Human Osteoclast Function in Vitro. Br. J. Pharmacol. 2012, 165, 2584–2597. [Google Scholar] [CrossRef]
- Sholler, D.J.; Schoene, L.; Spindle, T.R. Therapeutic Efficacy of Cannabidiol (CBD): A Review of the Evidence From Clinical Trials and Human Laboratory Studies. Curr. Addict. Reports 2020, 7, 405–412. [Google Scholar] [CrossRef]
- Technavio CBD Oil Market by Product and Geography - Forecast and Analysis 2022-2026.
- Abidi, A.H.; Alghamdi, S.S.; Derefinko, K. A Critical Review of Cannabis in Medicine and Dentistry: A Look Back and the Path Forward. Clin. Exp. Dent. Res. 2022, 8, 613–631. [Google Scholar] [CrossRef]
- David, C.; Elizalde-Hernández, A.; Barboza, A.; Cardoso, G.; Santos, M.; Moraes, R. Cannabidiol in Dentistry: A Scoping Review. Dent. J. 2022, 10, 193. [Google Scholar] [CrossRef]
- Cuba, L. de F.; Salum, F.G.; Guimarães, F.S.; Cherubini, K.; Borghetti, R.L.; Figueiredo, M.A.Z. Cannabidiol on 5-FU-induced Oral Mucositis in Mice. Oral Dis. 2020, 26, 1483–1493. [Google Scholar] [CrossRef]
- Konermann, A.; Jäger, A.; Held, S.A.E.; Brossart, P.; Schmöle, A. In Vivo and In Vitro Identification of Endocannabinoid Signaling in Periodontal Tissues and Their Potential Role in Local Pathophysiology. Cell. Mol. Neurobiol. 2017, 37, 1511–1520. [Google Scholar] [CrossRef]
- Miyashita, K.; Oyama, T.; Sakuta, T.; Tokuda, M.; Torii, M. Anandamide Induces Matrix Metalloproteinase-2 Production through Cannabinoid-1 Receptor and Transient Receptor Potential Vanilloid-1 in Human Dental Pulp Cells in Culture. J. Endod. 2012, 38, 786–790. [Google Scholar] [CrossRef]
- Ataei, A.; Rahim Rezaee, S.A.; Moeintaghavi, A.; Ghanbari, H.; Azizi, M. Evaluation of Cannabinoid Receptors Type 1–2 in Periodontitis Patients. Clin. Exp. Dent. Res. 2022, 8, 1040–1044. [Google Scholar] [CrossRef]
- Pacher, P.; Bátkai, S.; Kunos, G. The Endocannabinoid System as an Emerging Target of Pharmacotherapy. Pharmacol. Rev. 2006, 58, 389–462. [Google Scholar] [CrossRef]
- Crocq, M.-A. History of Cannabis and the Endocannabinoid System. Dialogues Clin. Neurosci. 2020, 22, 223–228. [Google Scholar] [CrossRef]
- Miller, L.L.; Branconnier, R.J. Cannabis: Effects on Memory and the Cholinergic Limbic System. Psychol. Bull. 1983, 93, 441–456. [Google Scholar] [CrossRef]
- Cherney, J.; Small, E. Industrial Hemp in North America: Production, Politics and Potential. Agronomy 2016, 6, 58. [Google Scholar] [CrossRef]
- Monthony, A.S.; Page, S.R.; Hesami, M.; Jones, A.M.P. The Past, Present and Future of Cannabis Sativa Tissue Culture. Plants 2021, 10, 185. [Google Scholar] [CrossRef] [PubMed]
- Pisanti, S.; Bifulco, M. Modern History of Medical Cannabis: From Widespread Use to Prohibitionism and Back. Trends Pharmacol. Sci. 2017, 38, 195–198. [Google Scholar] [CrossRef]
- Adams, R. Marihuana: Harvey Lecture, February 19, 1942. Bull. N. Y. Acad. Med. 1942, 18, 705–730. [Google Scholar] [PubMed]
- Gaoni, Y.; Mechoulam, R. Isolation, Structure, and Partial Synthesis of an Active Constituent of Hashish. J. Am. Chem. Soc. 1964, 86, 1646–1647. [Google Scholar] [CrossRef]
- ElSohly, M.A.; Gul, W. Constituents of Cannabis Sativa. In Handbook of Cannabis; Oxford University Press, 2014; pp. 3–22.
- Mechoulam, R.; Hanuš, L. A Historical Overview of Chemical Research on Cannabinoids. Chem. Phys. Lipids 2000, 108, 1–13. [Google Scholar] [CrossRef]
- Alharbi, Y.N. Current Legal Status of Medical Marijuana and Cannabidiol in the United States. Epilepsy Behav. 2020, 112, 107452. [Google Scholar] [CrossRef]
- Howlett, A.C.; Fleming, R.M. Cannabinoid Inhibition of Adenylate Cyclase. Pharmacology of the Response in Neuroblastoma Cell Membranes. Mol. Pharmacol. 1984, 26, 532–538. [Google Scholar]
- Devane, W.A.; Dysarz, F.A.; Johnson, M.R.; Melvin, L.S.; Howlett, A.C. Determination and Characterization of a Cannabinoid Receptor in Rat Brain. Mol. Pharmacol. 1988, 34, 605–613. [Google Scholar]
- Matsuda, L.A.; Lolait, S.J.; Brownstein, M.J.; Young, A.C.; Bonner, T.I. Structure of a Cannabinoid Receptor and Functional Expression of the Cloned CDNA. Nature 1990, 346, 561–564. [Google Scholar] [CrossRef]
- Devane, W.A.; Hanuš, L.; Breuer, A.; Pertwee, R.G.; Stevenson, L.A.; Griffin, G.; Gibson, D.; Mandelbaum, A.; Etinger, A.; Mechoulam, R. Isolation and Structure of a Brain Constituent That Binds to the Cannabinoid Receptor. Science (80-. ). 1992, 258, 1946–1949. [Google Scholar] [CrossRef]
- Munro, S.; Thomas, K.L.; Abu-Shaar, M. Molecular Characterization of a Peripheral Receptor for Cannabinoids. Nature 1993, 365, 61–65. [Google Scholar] [CrossRef]
- Mechoulam, R.; Ben-Shabat, S.; Hanus, L.; Ligumsky, M.; Kaminski, N.E.; Schatz, A.R.; Gopher, A.; Almog, S.; Martin, B.R.; Compton, D.R.; et al. Identification of an Endogenous 2-Monoglyceride, Present in Canine Gut, That Binds to Cannabinoid Receptors. Biochem. Pharmacol. 1995, 50, 83–90. [Google Scholar] [CrossRef]
- Di Marzo, V.; Stella, N.; Zimmer, A. Endocannabinoid Signalling and the Deteriorating Brain. Nat. Rev. Neurosci. 2015, 16, 30–42. [Google Scholar] [CrossRef]
- Di Marzo, V.; Melck, D.; Bisogno, T.; De Petrocellis, L. Endocannabinoids: Endogenous Cannabinoid Receptor Ligands with Neuromodulatory Action. Trends Neurosci. 1998, 21, 521–528. [Google Scholar] [CrossRef]
- Elphick, M.R. The Evolution and Comparative Neurobiology of Endocannabinoid Signalling. Philos. Trans. R. Soc. B Biol. Sci. 2012, 367, 3201–3215. [Google Scholar] [CrossRef] [PubMed]
- Martínez-Pinilla, E.; Varani, K.; Reyes-Resina, I.; Angelats, E.; Vincenzi, F.; Ferreiro-Vera, C.; Oyarzabal, J.; Canela, E.I.; Lanciego, J.L.; Nadal, X.; et al. Binding and Signaling Studies Disclose a Potential Allosteric Site for Cannabidiol in Cannabinoid CB2 Receptors. Front. Pharmacol. 2017, 8. [Google Scholar] [CrossRef]
- Thomas, A.; Baillie, G.L.; Phillips, A.M.; Razdan, R.K.; Ross, R.A.; Pertwee, R.G. Cannabidiol Displays Unexpectedly High Potency as an Antagonist of CB 1 and CB 2 Receptor Agonists in Vitro. Br. J. Pharmacol. 2007, 150, 613–623. [Google Scholar] [CrossRef]
- Navarro, G.; Reyes-Resina, I.; Rivas-Santisteban, R.; Sánchez de Medina, V.; Morales, P.; Casano, S.; Ferreiro-Vera, C.; Lillo, A.; Aguinaga, D.; Jagerovic, N.; et al. Cannabidiol Skews Biased Agonism at Cannabinoid CB1 and CB2 Receptors with Smaller Effect in CB1-CB2 Heteroreceptor Complexes. Biochem. Pharmacol. 2018, 157, 148–158. [Google Scholar] [CrossRef] [PubMed]
- Rock, E.; Bolognini, D.; Limebeer, C.; Cascio, M.; Anavi-Goffer, S.; Fletcher, P.; Mechoulam, R.; Pertwee, R.; Parker, L. Cannabidiol, a Non-Psychotropic Component of Cannabis, Attenuates Vomiting and Nausea-like Behaviour via Indirect Agonism of 5-HT1A Somatodendritic Autoreceptors in the Dorsal Raphe Nucleus. Br. J. Pharmacol. 2012, 165, 2620–2634. [Google Scholar] [CrossRef]
- Russo, E.B.; Burnett, A.; Hall, B.; Parker, K.K. Agonistic Properties of Cannabidiol at 5-HT1a Receptors. Neurochem. Res. 2005, 30, 1037–1043. [Google Scholar] [CrossRef]
- Ryberg, E.; Larsson, N.; Sjögren, S.; Hjorth, S.; Hermansson, N.-O.; Leonova, J.; Elebring, T.; Nilsson, K.; Drmota, T.; Greasley, P.J. The Orphan Receptor GPR55 Is a Novel Cannabinoid Receptor. Br. J. Pharmacol. 2007, 152, 1092–1101. [Google Scholar] [CrossRef]
- Lauckner, J.E.; Jensen, J.B.; Chen, H.-Y.; Lu, H.-C.; Hille, B.; Mackie, K. GPR55 Is a Cannabinoid Receptor That Increases Intracellular Calcium and Inhibits M Current. Proc. Natl. Acad. Sci. 2008, 105, 2699–2704. [Google Scholar] [CrossRef]
- Laun, A.S.; Shrader, S.H.; Brown, K.J.; Song, Z.-H. GPR3, GPR6, and GPR12 as Novel Molecular Targets: Their Biological Functions and Interaction with Cannabidiol. Acta Pharmacol. Sin. 2019, 40, 300–308. [Google Scholar] [CrossRef]
- Petrescu, N.B.; Jurj, A.; Sorițău, O.; Lucaciu, O.P.; Dirzu, N.; Raduly, L.; Berindan-Neagoe, I.; Cenariu, M.; Boșca, B.A.; Campian, R.S.; et al. Cannabidiol and Vitamin D3 Impact on Osteogenic Differentiation of Human Dental Mesenchymal Stem Cells. Medicina (B. Aires). 2020, 56, 607. [Google Scholar] [CrossRef] [PubMed]
- De Petrocellis, L.; Ligresti, A.; Moriello, A.S.; Allarà, M.; Bisogno, T.; Petrosino, S.; Stott, C.G.; Di Marzo, V. Effects of Cannabinoids and Cannabinoid-Enriched Cannabis Extracts on TRP Channels and Endocannabinoid Metabolic Enzymes. Br. J. Pharmacol. 2011, 163, 1479–1494. [Google Scholar] [CrossRef] [PubMed]
- Bisogno, T.; Hanuš, L.; De Petrocellis, L.; Tchilibon, S.; Ponde, D.E.; Brandi, I.; Moriello, A.S.; Davis, J.B.; Mechoulam, R.; Di Marzo, V. Molecular Targets for Cannabidiol and Its Synthetic Analogues: Effect on Vanilloid VR1 Receptors and on the Cellular Uptake and Enzymatic Hydrolysis of Anandamide. Br. J. Pharmacol. 2001, 134, 845–852. [Google Scholar] [CrossRef] [PubMed]
- Qin, N.; Neeper, M.P.; Liu, Y.; Hutchinson, T.L.; Lubin, M.L.; Flores, C.M. TRPV2 Is Activated by Cannabidiol and Mediates CGRP Release in Cultured Rat Dorsal Root Ganglion Neurons. J. Neurosci. 2008, 28, 6231–6238. [Google Scholar] [CrossRef] [PubMed]
- Nabissi, M.; Morelli, M.B.; Santoni, M.; Santoni, G. Triggering of the TRPV2 Channel by Cannabidiol Sensitizes Glioblastoma Cells to Cytotoxic Chemotherapeutic Agents. Carcinogenesis 2013, 34, 48–57. [Google Scholar] [CrossRef] [PubMed]
- De Petrocellis, L.; Vellani, V.; Schiano-Moriello, A.; Marini, P.; Magherini, P.C.; Orlando, P.; Di Marzo, V. Plant-Derived Cannabinoids Modulate the Activity of Transient Receptor Potential Channels of Ankyrin Type-1 and Melastatin Type-8. J. Pharmacol. Exp. Ther. 2008, 325, 1007–1015. [Google Scholar] [CrossRef] [PubMed]
- Mahgoub, M.; Keun-Hang, S.Y.; Sydorenko, V.; Ashoor, A.; Kabbani, N.; Al Kury, L.; Sadek, B.; Howarth, C.F.; Isaev, D.; Galadari, S.; et al. Effects of Cannabidiol on the Function of A7-Nicotinic Acetylcholine Receptors. Eur. J. Pharmacol. 2013, 720, 310–319. [Google Scholar] [CrossRef] [PubMed]
- Yang, K.-H.; Galadari, S.; Isaev, D.; Petroianu, G.; Shippenberg, T.S.; Oz, M. The Nonpsychoactive Cannabinoid Cannabidiol Inhibits 5-Hydroxytryptamine 3A Receptor-Mediated Currents in Xenopus Laevis Oocytes. J. Pharmacol. Exp. Ther. 2010, 333, 547–554. [Google Scholar] [CrossRef]
- Ahrens, J.; Demir, R.; Leuwer, M.; de la Roche, J.; Krampfl, K.; Foadi, N.; Karst, M.; Haeseler, G. The Nonpsychotropic Cannabinoid Cannabidiol Modulates and Directly Activates Alpha-1 and Alpha-1-Beta Glycine Receptor Function. Pharmacology 2009, 83, 217–222. [Google Scholar] [CrossRef]
- Bakas, T.; van Nieuwenhuijzen, P.S.; Devenish, S.O.; McGregor, I.S.; Arnold, J.C.; Chebib, M. The Direct Actions of Cannabidiol and 2-Arachidonoyl Glycerol at GABA A Receptors. Pharmacol. Res. 2017, 119, 358–370. [Google Scholar] [CrossRef]
- Ross, H.R.; Napier, I.; Connor, M. Inhibition of Recombinant Human T-Type Calcium Channels by Δ9-Tetrahydrocannabinol and Cannabidiol. J. Biol. Chem. 2008, 283, 16124–16134. [Google Scholar] [CrossRef]
- Ghovanloo, M.-R.; Shuart, N.G.; Mezeyova, J.; Dean, R.A.; Ruben, P.C.; Goodchild, S.J. Inhibitory Effects of Cannabidiol on Voltage-Dependent Sodium Currents. J. Biol. Chem. 2018, 293, 16546–16558. [Google Scholar] [CrossRef] [PubMed]
- Rimmerman, N.; Ben-Hail, D.; Porat, Z.; Juknat, A.; Kozela, E.; Daniels, M.P.; Connelly, P.S.; Leishman, E.; Bradshaw, H.B.; Shoshan-Barmatz, V.; et al. Direct Modulation of the Outer Mitochondrial Membrane Channel, Voltage-Dependent Anion Channel 1 (VDAC1) by Cannabidiol: A Novel Mechanism for Cannabinoid-Induced Cell Death. Cell Death Dis. 2013, 4, e949–e949. [Google Scholar] [CrossRef] [PubMed]
- Elmes, M.W.; Kaczocha, M.; Berger, W.T.; Leung, K.; Ralph, B.P.; Wang, L.; Sweeney, J.M.; Miyauchi, J.T.; Tsirka, S.E.; Ojima, I.; et al. Fatty Acid-Binding Proteins (FABPs) Are Intracellular Carriers for Δ9-Tetrahydrocannabinol (THC) and Cannabidiol (CBD). J. Biol. Chem. 2015, 290, 8711–8721. [Google Scholar] [CrossRef] [PubMed]
- Leweke, F.M.; Piomelli, D.; Pahlisch, F.; Muhl, D.; Gerth, C.W.; Hoyer, C.; Klosterkötter, J.; Hellmich, M.; Koethe, D. Cannabidiol Enhances Anandamide Signaling and Alleviates Psychotic Symptoms of Schizophrenia. Transl. Psychiatry 2012, 2, e94–e94. [Google Scholar] [CrossRef] [PubMed]
- Leishman, E.; Manchanda, M.; Thelen, R.; Miller, S.; Mackie, K.; Bradshaw, H.B. Cannabidiol’s Upregulation of N -Acyl Ethanolamines in the Central Nervous System Requires N -Acyl Phosphatidyl Ethanolamine-Specific Phospholipase D. Cannabis Cannabinoid Res. 2018, 3, 228–241. [Google Scholar] [CrossRef]
- Carrier, E.J.; Auchampach, J.A.; Hillard, C.J. Inhibition of an Equilibrative Nucleoside Transporter by Cannabidiol: A Mechanism of Cannabinoid Immunosuppression. Proc. Natl. Acad. Sci. 2006, 103, 7895–7900. [Google Scholar] [CrossRef] [PubMed]
- Mijangos-Moreno, S.; Poot-Aké, A.; Arankowsky-Sandoval, G.; Murillo-Rodríguez, E. Intrahypothalamic Injection of Cannabidiol Increases the Extracellular Levels of Adenosine in Nucleus Accumbens in Rats. Neurosci. Res. 2014, 84, 60–63. [Google Scholar] [CrossRef] [PubMed]
- Holland, M.L.; Allen, J.D.; Arnold, J.C. Interaction of Plant Cannabinoids with the Multidrug Transporter ABCC1 (MRP1). Eur. J. Pharmacol. 2008, 591, 128–131. [Google Scholar] [CrossRef]
- GILBERT, J.C.; PERTWEE, R.G.; WYLLIE, M.G. EFFECTS OF Δ9-TETRAHYDROCANNABINOL AND CANNABIDIOL ON A Mg2+-ATPase OF SYNAPTIC VESICLES PREPARED FROM RAT CEREBRAL CORTEX. Br. J. Pharmacol. 1977, 59, 599–601. [Google Scholar] [CrossRef]
- Doohan, P.T.; Oldfield, L.D.; Arnold, J.C.; Anderson, L.L. Cannabinoid Interactions with Cytochrome P450 Drug Metabolism: A Full-Spectrum Characterization. AAPS J. 2021, 23, 91. [Google Scholar] [CrossRef]
- Takeda, S.; Usami, N.; Yamamoto, I.; Watanabe, K. Cannabidiol-2′,6′-Dimethyl Ether, a Cannabidiol Derivative, Is a Highly Potent and Selective 15-Lipoxygenase Inhibitor. Drug Metab. Dispos. 2009, 37, 1733–1737. [Google Scholar] [CrossRef] [PubMed]
- Wheal, A.J.; Cipriano, M.; Fowler, C.J.; Randall, M.D.; O’Sullivan, S.E. Cannabidiol Improves Vasorelaxation in Zucker Diabetic Fatty Rats through Cyclooxygenase Activation. J. Pharmacol. Exp. Ther. 2014, 351, 457–466. [Google Scholar] [CrossRef] [PubMed]
- Evans, A.T.; Formukong, E.; Evans, F.J. Activation of Phospholipase A 2 by Cannabinoids. FEBS Lett. 1987, 211, 119–122. [Google Scholar] [CrossRef] [PubMed]
- Fišar, Z.; Singh, N.; Hroudová, J. Cannabinoid-Induced Changes in Respiration of Brain Mitochondria. Toxicol. Lett. 2014, 231, 62–71. [Google Scholar] [CrossRef]
- Koch, M.; Dehghani, F.; Habazettl, I.; Schomerus, C.; Korf, H.-W. Cannabinoids Attenuate Norepinephrine-Induced Melatonin Biosynthesis in the Rat Pineal Gland by Reducing Arylalkylamine N-Acetyltransferase Activity without Involvement of Cannabinoid Receptors. J. Neurochem. 2006, 98, 267–278. [Google Scholar] [CrossRef]
- Jenny, M.; Santer, E.; Pirich, E.; Schennach, H.; Fuchs, D. Δ9-Tetrahydrocannabinol and Cannabidiol Modulate Mitogen-Induced Tryptophan Degradation and Neopterin Formation in Peripheral Blood Mononuclear Cells in Vitro. J. Neuroimmunol. 2009, 207, 75–82. [Google Scholar] [CrossRef]
- Cornicelli, J.A.; Gilman, S.R.; Krom, B.A.; Kottke, B.A. Cannabinoids Impair the Formation of Cholesteryl Ester in Cultured Human Cells. Arterioscler. An Off. J. Am. Hear. Assoc. Inc. 1981, 1, 449–454. [Google Scholar] [CrossRef]
- Watanabe, K.; Motoya, E.; Matsuzawa, N.; Funahashi, T.; Kimura, T.; Matsunaga, T.; Arizono, K.; Yamamoto, I. Marijuana Extracts Possess the Effects like the Endocrine Disrupting Chemicals. Toxicology 2005, 206, 471–478. [Google Scholar] [CrossRef]
- Hegde, V.L.; Singh, U.P.; Nagarkatti, P.S.; Nagarkatti, M. Critical Role of Mast Cells and Peroxisome Proliferator–Activated Receptor γ in the Induction of Myeloid-Derived Suppressor Cells by Marijuana Cannabidiol In Vivo. J. Immunol. 2015, 194, 5211–5222. [Google Scholar] [CrossRef]
- Juknat, A.; Pietr, M.; Kozela, E.; Rimmerman, N.; Levy, R.; Gao, F.; Coppola, G.; Geschwind, D.; Vogel, Z. Microarray and Pathway Analysis Reveal Distinct Mechanisms Underlying Cannabinoid-Mediated Modulation of LPS-Induced Activation of BV-2 Microglial Cells. PLoS ONE 2013, 8, e61462. [Google Scholar] [CrossRef]
- Peyravian, N.; Deo, S.; Daunert, S.; Jimenez, J.J. Cannabidiol as a Novel Therapeutic for Immune Modulation. ImmunoTargets Ther. 2020, Volume 9, 131–140. [Google Scholar] [CrossRef]
- Costa, B.; Giagnoni, G.; Franke, C.; Trovato, A.E.; Colleoni, M. Vanilloid TRPV1 Receptor Mediates the Antihyperalgesic Effect of the Nonpsychoactive Cannabinoid, Cannabidiol, in a Rat Model of Acute Inflammation. Br. J. Pharmacol. 2004, 143, 247–250. [Google Scholar] [CrossRef] [PubMed]
- Fonseca, B.M.; Correia-da-Silva, G.; Teixeira, N.A. Cannabinoid-Induced Cell Death in Endometrial Cancer Cells: Involvement of TRPV1 Receptors in Apoptosis. J. Physiol. Biochem. 2018, 74, 261–272. [Google Scholar] [CrossRef]
- Kozela, E.; Pietr, M.; Juknat, A.; Rimmerman, N.; Levy, R.; Vogel, Z. Cannabinoids Δ9-Tetrahydrocannabinol and Cannabidiol Differentially Inhibit the Lipopolysaccharide-Activated NF-ΚB and Interferon-β/STAT Proinflammatory Pathways in BV-2 Microglial Cells. J. Biol. Chem. 2010, 285, 1616–1626. [Google Scholar] [CrossRef]
- Liu, C.; Ma, H.; Slitt, A.L.; Seeram, N.P. Inhibitory Effect of Cannabidiol on the Activation of NLRP3 Inflammasome Is Associated with Its Modulation of the P2X7 Receptor in Human Monocytes. J. Nat. Prod. 2020, 83, 2025–2029. [Google Scholar] [CrossRef]
- Mecha, M.; Feliú, A.; Iñigo, P.M.; Mestre, L.; Carrillo-Salinas, F.J.; Guaza, C. Cannabidiol Provides Long-Lasting Protection against the Deleterious Effects of Inflammation in a Viral Model of Multiple Sclerosis: A Role for A2A Receptors. Neurobiol. Dis. 2013, 59, 141–150. [Google Scholar] [CrossRef]
- Borsani, E.; Majorana, A.; Cocchi, M.A.; Conti, G.; Bonadeo, S.; Padovani, A.; Lauria, G.; Bardellini, E.; Rezzani, R.; Rodella, L.F. Epithelial Expression of Vanilloid and Cannabinoid Receptors: A Potential Role in Burning Mouth Syndrome Pathogenesis. Histol. Histopathol. 2014, 29, 523–533. [Google Scholar] [CrossRef] [PubMed]
- Theocharis, S.; Giaginis, C.; Alexandrou, P.; Rodriguez, J.; Tasoulas, J.; Danas, E.; Patsouris, E.; Klijanienko, J. Evaluation of Cannabinoid CB1 and CB2 Receptors Expression in Mobile Tongue Squamous Cell Carcinoma: Associations with Clinicopathological Parameters and Patients’ Survival. Tumor Biol. 2016, 37, 3647–3656. [Google Scholar] [CrossRef]
- Rosenblatt, K.A.; Daling, J.R.; Chen, C.; Sherman, K.J.; Schwartz, S.M. Marijuana Use and Risk of Oral Squamous Cell Carcinoma. Cancer Res. 2004, 64, 4049–4054. [Google Scholar] [CrossRef]
- Beneng, K.; Renton, T.; Yilmaz, Z.; Yiangou, Y.; Anand, P. Cannabinoid Receptor CB1-Immunoreactive Nerve Fibres in Painful and Non-Painful Human Tooth Pulp. J. Clin. Neurosci. 2010, 17, 1476–1479. [Google Scholar] [CrossRef]
- Que, K.; He, D.; Jin, Y.; Wu, L.; Wang, F.; Zhao, Z.; Yang, J.; Deng, J. Expression of Cannabinoid Type 1 Receptors in Human Odontoblast Cells. J. Endod. 2017, 43, 283–288. [Google Scholar] [CrossRef] [PubMed]
- Navarro-Saiz, L.; Bernal-Cepeda, L.; Castellanos, J. Immune Challenges Upregulate the Expression of Cannabinoid Receptors in Cultured Human Odontoblasts and Gingival Fibroblasts. Acta Odontológica Latinoam. 2022, 35, 80–89. [Google Scholar] [CrossRef] [PubMed]
- Tsumura, M.; Sobhan, U.; Muramatsu, T.; Sato, M.; Ichikawa, H.; Sahara, Y.; Tazaki, M.; Shibukawa, Y. TRPV1-Mediated Calcium Signal Couples with Cannabinoid Receptors and Sodium–Calcium Exchangers in Rat Odontoblasts. Cell Calcium 2012, 52, 124–136. [Google Scholar] [CrossRef] [PubMed]
- Thoungseabyoun, W.; Tachow, A.; Pakkarato, S.; Rawangwong, A.; Krongyut, S.; Sakaew, W.; Kondo, H.; Hipkaeo, W. Immunohistochemical Localization of Cannabinoid Receptor 1 (CB1) in the Submandibular Gland of Mice under Normal Conditions and When Stimulated by Isoproterenol or Carbachol. Arch. Oral Biol. 2017, 81, 160–166. [Google Scholar] [CrossRef] [PubMed]
- Pirino, C.; Cappai, M.G.; Maranesi, M.; Tomassoni, D.; Giontella, A.; Pinna, W.; Boiti, C.; Kamphues, J.; Dall’Aglio, C. The Presence and Distribution of Cannabinoid Type 1 and 2 Receptors in the Mandibular Gland: The Influence of Different Physical Forms of Diets on Their Expression in Piglets. J. Anim. Physiol. Anim. Nutr. (Berl). 2018, 102, e870–e876. [Google Scholar] [CrossRef]
- Yoshida, R.; Ohkuri, T.; Jyotaki, M.; Yasuo, T.; Horio, N.; Yasumatsu, K.; Sanematsu, K.; Shigemura, N.; Yamamoto, T.; Margolskee, R.F.; et al. Endocannabinoids Selectively Enhance Sweet Taste. Proc. Natl. Acad. Sci. 2010, 107, 935–939. [Google Scholar] [CrossRef]
- Prestifilippo, J.P.; Fernandez-Solari, J.; Medina, V.; Rettori, V.; Elverdin, J.C. Role of the Endocannabinoid System in Ethanol-Induced Inhibition of Salivary Secretion. Alcohol Alcohol. 2009, 44, 443–448. [Google Scholar] [CrossRef]
- Prestifilippo, J.P.; Fernández-Solari, J.; Cal, C. de la; Iribarne, M.; Suburo, A.M.; Rettori, V.; McCann, S.M.; Elverdin, J.C. Inhibition of Salivary Secretion by Activation of Cannabinoid Receptors. Exp. Biol. Med. 2006, 231, 1421–1429. [Google Scholar] [CrossRef]
- Andreis, K.; Billingsley, J.; Naimi Shirazi, K.; Wager-Miller, J.; Johnson, C.; Bradshaw, H.; Straiker, A. Cannabinoid CB1 Receptors Regulate Salivation. Sci. Rep. 2022, 12, 14182. [Google Scholar] [CrossRef]
- Jirasek, P.; Jusku, A.; Simanek, V.; Frankova, J.; Storch, J.; Vacek, J. Cannabidiol and Periodontal Inflammatory Disease: A Critical Assessment. Biomed. Pap. 2022, 166, 155–160. [Google Scholar] [CrossRef]
- Liu, C.; Qi, X.; Alhabeil, J.; Lu, H.; Zhou, Z. Activation of Cannabinoid Receptors Promote Periodontal Cell Adhesion and Migration. J. Clin. Periodontol. 2019, 46, 1264–1272. [Google Scholar] [CrossRef] [PubMed]
- Raphael-Mizrahi, B.; Gabet, Y. The Cannabinoids Effect on Bone Formation and Bone Healing. Curr. Osteoporos. Rep. 2020, 18, 433–438. [Google Scholar] [CrossRef] [PubMed]
- Kozono, S.; Matsuyama, T.; Biwasa, K.K.; Kawahara, K.; Nakajima, Y.; Yoshimoto, T.; Yonamine, Y.; Kadomatsu, H.; Tancharoen, S.; Hashiguchi, T.; et al. Involvement of the Endocannabinoid System in Periodontal Healing. Biochem. Biophys. Res. Commun. 2010, 394, 928–933. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.G.; Miyazu, M.; Xiang, P.; Li, S.N.; Sokabe, M.; Naruse, K. Stretch-Induced Cell Proliferation Is Mediated by FAK-MAPK Pathway. Life Sci. 2005, 76, 2817–2825. [Google Scholar] [CrossRef] [PubMed]
- Lanza Cariccio, V.; Scionti, D.; Raffa, A.; Iori, R.; Pollastro, F.; Diomede, F.; Bramanti, P.; Trubiani, O.; Mazzon, E. Treatment of Periodontal Ligament Stem Cells with MOR and CBD Promotes Cell Survival and Neuronal Differentiation via the PI3K/Akt/MTOR Pathway. Int. J. Mol. Sci. 2018, 19, 2341. [Google Scholar] [CrossRef] [PubMed]
- Ossola, C.A.; Surkin, P.N.; Mohn, C.E.; Elverdin, J.C.; Fernández-Solari, J. Anti-Inflammatory and Osteoprotective Effects of Cannabinoid-2 Receptor Agonist HU-308 in a Rat Model of Lipopolysaccharide-Induced Periodontitis. J. Periodontol. 2016, 87, 725–734. [Google Scholar] [CrossRef] [PubMed]
- Rawal, S.Y.; Dabbous, M.K.; Tipton, D.A. Effect of Cannabidiol on Human Gingival Fibroblast Extracellular Matrix Metabolism: MMP Production and Activity, and Production of Fibronectin and Transforming Growth Factor β. J. Periodontal Res. 2012, 47, 320–329. [Google Scholar] [CrossRef] [PubMed]
- Napimoga, M.H.; Benatti, B.B.; Lima, F.O.; Alves, P.M.; Campos, A.C.; Pena-dos-Santos, D.R.; Severino, F.P.; Cunha, F.Q.; Guimarães, F.S. Cannabidiol Decreases Bone Resorption by Inhibiting RANK/RANKL Expression and pro-Inflammatory Cytokines during Experimental Periodontitis in Rats. Int. Immunopharmacol. 2009, 9, 216–222. [Google Scholar] [CrossRef]
- Gu, Z.; Singh, S.; Niyogi, R.G.; Lamont, G.J.; Wang, H.; Lamont, R.J.; Scott, D.A. Marijuana-Derived Cannabinoids Trigger a CB2/PI3K Axis of Suppression of the Innate Response to Oral Pathogens. Front. Immunol. 2019, 10. [Google Scholar] [CrossRef]
- Stahl, V.; Vasudevan, K. Comparison of Efficacy of Cannabinoids versus Commercial Oral Care Products in Reducing Bacterial Content from Dental Plaque: A Preliminary Observation. Cureus 2020. [Google Scholar] [CrossRef]
- Klein, M.; de Quadros De Bortolli, J.; Guimarães, F.S.; Salum, F.G.; Cherubini, K.; de Figueiredo, M.A.Z. Effects of Cannabidiol, a Cannabis Sativa Constituent, on Oral Wound Healing Process in Rats: Clinical and Histological Evaluation. Phyther. Res. 2018, 32, 2275–2281. [Google Scholar] [CrossRef] [PubMed]
- Nakajima, Y.; Furuichi, Y.; Biswas, K.K.; Hashiguchi, T.; Kawahara, K.; Yamaji, K.; Uchimura, T.; Izumi, Y.; Maruyama, I. Endocannabinoid, Anandamide in Gingival Tissue Regulates the Periodontal Inflammation through NF-ΚB Pathway Inhibition. FEBS Lett. 2006, 580, 613–619. [Google Scholar] [CrossRef]
- Qi, X.; Liu, C.; Li, G.; Luan, H.; Li, S.; Yang, D.; Zhou, Z. Investigation of in Vitro Odonto/Osteogenic Capacity of Cannabidiol on Human Dental Pulp Cell. J. Dent. 2021, 109, 103673. [Google Scholar] [CrossRef] [PubMed]
- Luiz de Oliveira da Rosa, W.; Machado da Silva, T.; Fernando Demarco, F.; Piva, E.; Fernandes da Silva, A. Could the Application of Bioactive Molecules Improve Vital Pulp Therapy Success? A Systematic Review. J. Biomed. Mater. Res. Part A 2017, 105, 941–956. [Google Scholar] [CrossRef]
- Qi, X.; Liu, C.; Li, G.; Al-Alfe, D.; Paurazas, S.; Askar, M.; Yang, D.; Zhou, Z. Evaluation of Cannabinoids on the Odonto/Osteogenesis in Human Dental Pulp Cells In Vitro. J. Endod. 2021, 47, 444–450. [Google Scholar] [CrossRef]
- Yu, L.; Zeng, L.; Zhang, Z.; Zhu, G.; Xu, Z.; Xia, J.; Weng, J.; Li, J.; Pathak, J.L. Cannabidiol Rescues TNF-α-Inhibited Proliferation, Migration, and Osteogenic/Odontogenic Differentiation of Dental Pulp Stem Cells. Biomolecules 2023, 13, 118. [Google Scholar] [CrossRef]
- Duncan, H.F.; Galler, K.M.; Tomson, P.L.; Simon, S.; El-Karim, I.; Kundzina, R.; Krastl, G.; Dammaschke, T.; Fransson, H.; Markvart, M.; et al. European Society of Endodontology Position Statement: Management of Deep Caries and the Exposed Pulp. Int. Endod. J. 2019, 52, 923–934. [Google Scholar] [CrossRef]
- Sáez, M.D.M.; López, G.L.; Atlas, D.; de la Casa, M.L. Evaluation of PH and Calcium Ion Diffusion from Calcium Hydroxide Pastes and MTA. Acta Odontol. Latinoam. 2017, 30, 26–32. [Google Scholar]
- Schmuhl, E.; Ramer, R.; Salamon, A.; Peters, K.; Hinz, B. Increase of Mesenchymal Stem Cell Migration by Cannabidiol via Activation of P42/44 MAPK. Biochem. Pharmacol. 2014, 87, 489–501. [Google Scholar] [CrossRef]
- Smith, A.J.; Smith, J.G.; Shelton, R.M.; Cooper, P.R. Harnessing the Natural Regenerative Potential of the Dental Pulp. Dent. Clin. North Am. 2012, 56, 589–601. [Google Scholar] [CrossRef]
- Libro, R.; Scionti, D.; Diomede, F.; Marchisio, M.; Grassi, G.; Pollastro, F.; Piattelli, A.; Bramanti, P.; Mazzon, E.; Trubiani, O. Cannabidiol Modulates the Immunophenotype and Inhibits the Activation of the Inflammasome in Human Gingival Mesenchymal Stem Cells. Front. Physiol. 2016, 7. [Google Scholar] [CrossRef]
- Cuba, L.F.; Salum, F.G.; Cherubini, K.; Figueiredo, M.A.Z. Cannabidiol: An Alternative Therapeutic Agent for Oral Mucositis? J. Clin. Pharm. Ther. 2017, 42, 245–250. [Google Scholar] [CrossRef]
- Kamali, A.; Oryan, A.; Hosseini, S.; Ghanian, M.H.; Alizadeh, M.; Baghaban Eslaminejad, M.; Baharvand, H. Cannabidiol-Loaded Microspheres Incorporated into Osteoconductive Scaffold Enhance Mesenchymal Stem Cell Recruitment and Regeneration of Critical-Sized Bone Defects. Mater. Sci. Eng. C 2019, 101, 64–75. [Google Scholar] [CrossRef] [PubMed]
- Rock, E.M.; Limebeer, C.L.; Pertwee, R.G.; Mechoulam, R.; Parker, L.A. Therapeutic Potential of Cannabidiol, Cannabidiolic Acid, and Cannabidiolic Acid Methyl Ester as Treatments for Nausea and Vomiting. Cannabis Cannabinoid Res. 2021, 6, 266–274. [Google Scholar] [CrossRef]
- Good, P.; Haywood, A.; Gogna, G.; Martin, J.; Yates, P.; Greer, R.; Hardy, J. Oral Medicinal Cannabinoids to Relieve Symptom Burden in the Palliative Care of Patients with Advanced Cancer: A Double-Blind, Placebo Controlled, Randomised Clinical Trial of Efficacy and Safety of Cannabidiol (CBD). BMC Palliat. Care 2019, 18, 110. [Google Scholar] [CrossRef]
- Frane, N.; Stapleton, E.; Iturriaga, C.; Ganz, M.; Rasquinha, V.; Duarte, R. Cannabidiol as a Treatment for Arthritis and Joint Pain: An Exploratory Cross-Sectional Study. J. Cannabis Res. 2022, 4, 47. [Google Scholar] [CrossRef]
- Malfait, A.M.; Gallily, R.; Sumariwalla, P.F.; Malik, A.S.; Andreakos, E.; Mechoulam, R.; Feldmann, M. The Nonpsychoactive Cannabis Constituent Cannabidiol Is an Oral Anti-Arthritic Therapeutic in Murine Collagen-Induced Arthritis. Proc. Natl. Acad. Sci. 2000, 97, 9561–9566. [Google Scholar] [CrossRef] [PubMed]
- Di Marzo, V. The Endocannabinoid System in Obesity and Type 2 Diabetes. Diabetologia 2008, 51, 1356–1367. [Google Scholar] [CrossRef] [PubMed]
- Weiss, L.; Zeira, M.; Reich, S.; Har-Noy, M.; Mechoulam, R.; Slavin, S.; Gallily, R. Cannabidiol Lowers Incidence of Diabetes in Non-Obese Diabetic Mice. Autoimmunity 2006, 39, 143–151. [Google Scholar] [CrossRef]
- Kudiyirickal, M.G.; Pappachan, J.M. Diabetes Mellitus and Oral Health. Endocrine 2015, 49, 27–34. [Google Scholar] [CrossRef]
- Lattanzi, S.; Trinka, E.; Striano, P.; Rocchi, C.; Salvemini, S.; Silvestrini, M.; Brigo, F. Highly Purified Cannabidiol for Epilepsy Treatment: A Systematic Review of Epileptic Conditions Beyond Dravet Syndrome and Lennox–Gastaut Syndrome. CNS Drugs 2021, 35, 265–281. [Google Scholar] [CrossRef] [PubMed]
- Samanta, D. Cannabidiol: A Review of Clinical Efficacy and Safety in Epilepsy. Pediatr. Neurol. 2019, 96, 24–29. [Google Scholar] [CrossRef] [PubMed]
- Nonato, E.R.; Borges, M.A. Oral and Maxillofacial Trauma in Patients with Epilepsy: Prospective Study Based on an Outpatient Population. Arq. Neuropsiquiatr. 2011, 69, 491–495. [Google Scholar] [CrossRef]
- Stahl, V. Cannabis and Derivatives Thereof for the Treatment of Pain and Inflammation Related with Dental Pulp and Bone Regeneration Related to Dental Jaw Bone Defects.
- Dick, T.N.A.; Marques, L.C.; Lopes, A. de A.L.; Candreva, M.S.; Santos, L.R.; Picciani, B.L.S. Phytotherapy in Dentistry: A Literature Review Based on Clinical Data. European J. Med. Plants 2020, 1–13. [Google Scholar] [CrossRef]
- Nelson, K.M.; Bisson, J.; Singh, G.; Graham, J.G.; Chen, S.-N.; Friesen, J.B.; Dahlin, J.L.; Niemitz, M.; Walters, M.A.; Pauli, G.F. The Essential Medicinal Chemistry of Cannabidiol (CBD). J. Med. Chem. 2020, 63, 12137–12155. [Google Scholar] [CrossRef]
- Koturbash, I.; MacKay, D. Cannabidiol and Other Cannabinoids: From Toxicology and Pharmacology to the Development of a Regulatory Pathway. J. Diet. Suppl. 2020, 17, 487–492. [Google Scholar] [CrossRef]
- Bernardini, S.; Tiezzi, A.; Laghezza Masci, V.; Ovidi, E. Natural Products for Human Health: An Historical Overview of the Drug Discovery Approaches. Nat. Prod. Res. 2018, 32, 1926–1950. [Google Scholar] [CrossRef]
- Abubakar, A.; Haque, M. Preparation of Medicinal Plants: Basic Extraction and Fractionation Procedures for Experimental Purposes. J. Pharm. Bioallied Sci. 2020, 12, 1. [Google Scholar] [CrossRef]
Figure 1.
Structural architecture of CB.
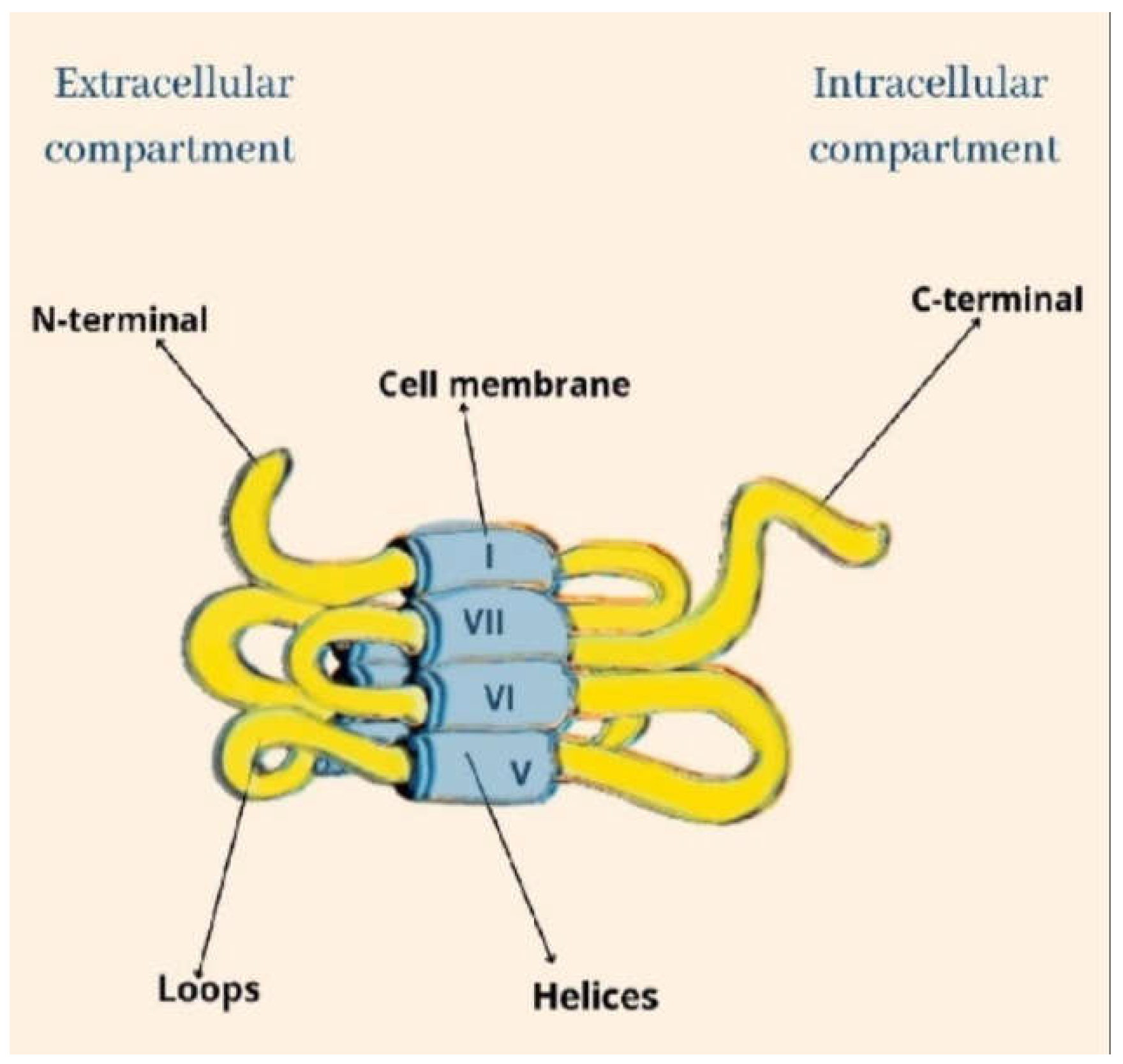
Figure 2.
Amino acid sequence of CB1 and CB2.
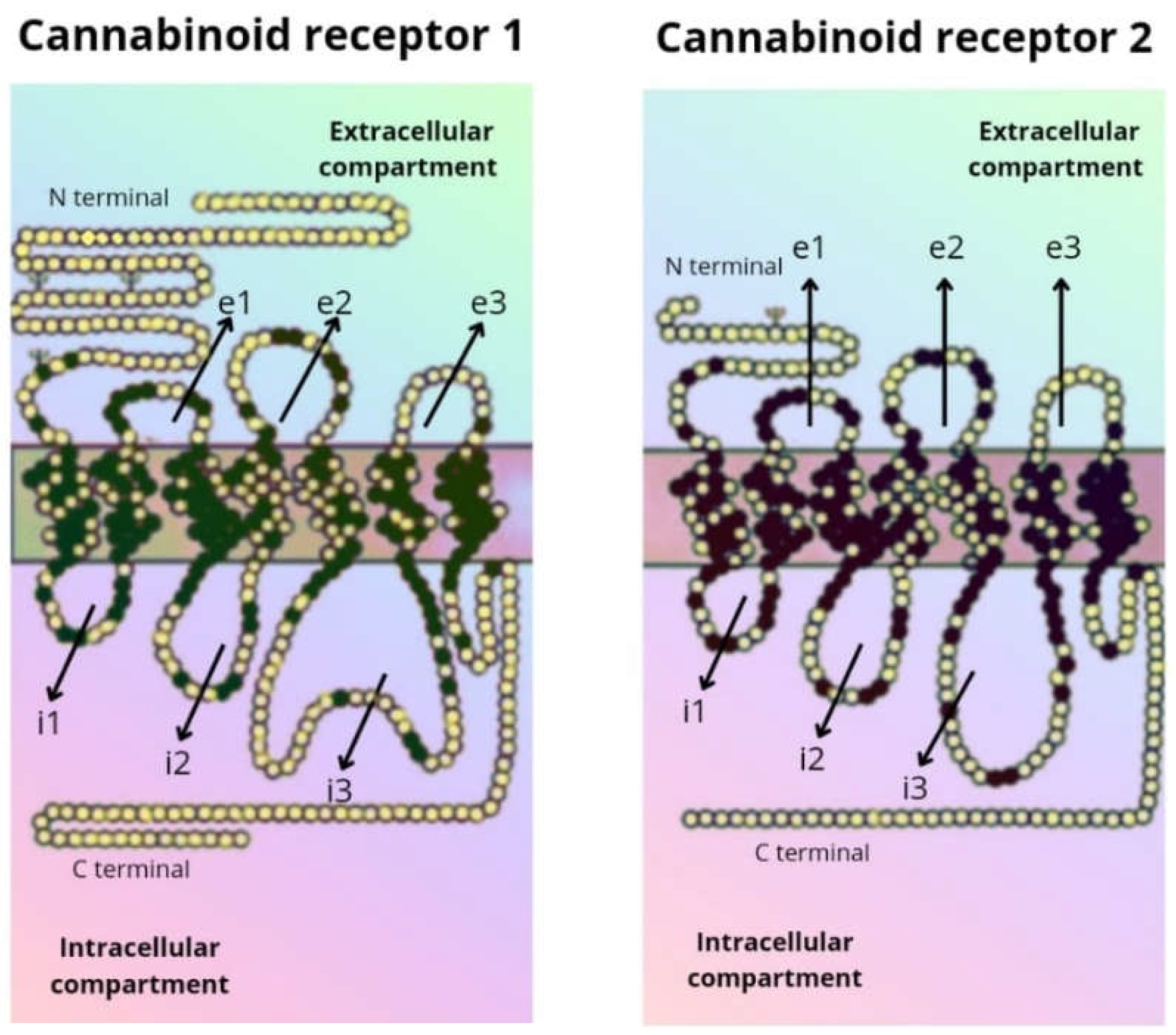
Figure 3.
Location of the cannabinoid receptors (CB1 and CB2) in the human body.
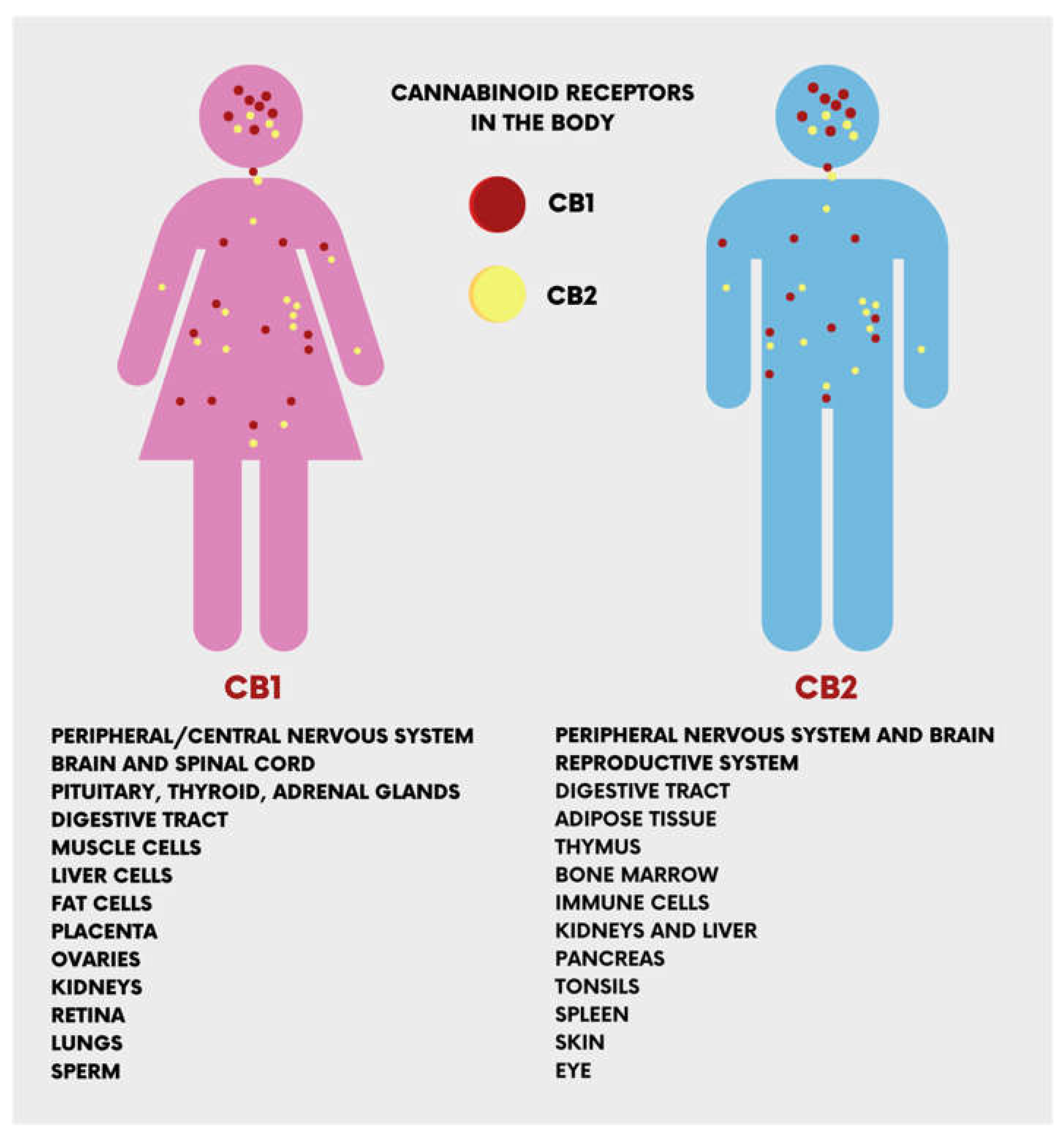
Figure 4.
Classification of the different cannabinoids compounds derived from cannabis and their therapeutical properties.
Figure 4.
Classification of the different cannabinoids compounds derived from cannabis and their therapeutical properties.
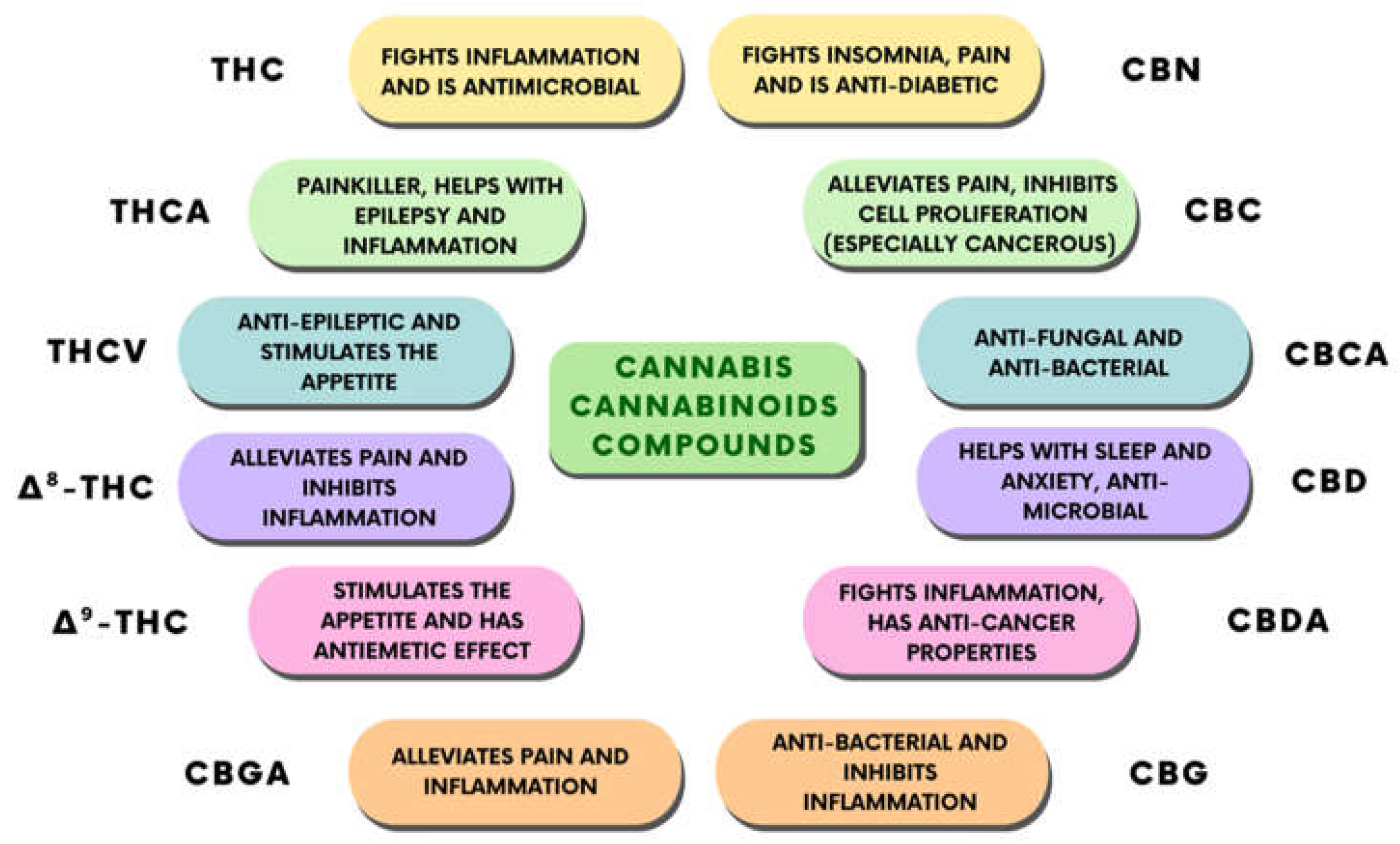
Figure 5.
Benefits of cannabinoids compounds and their effects on the human body.
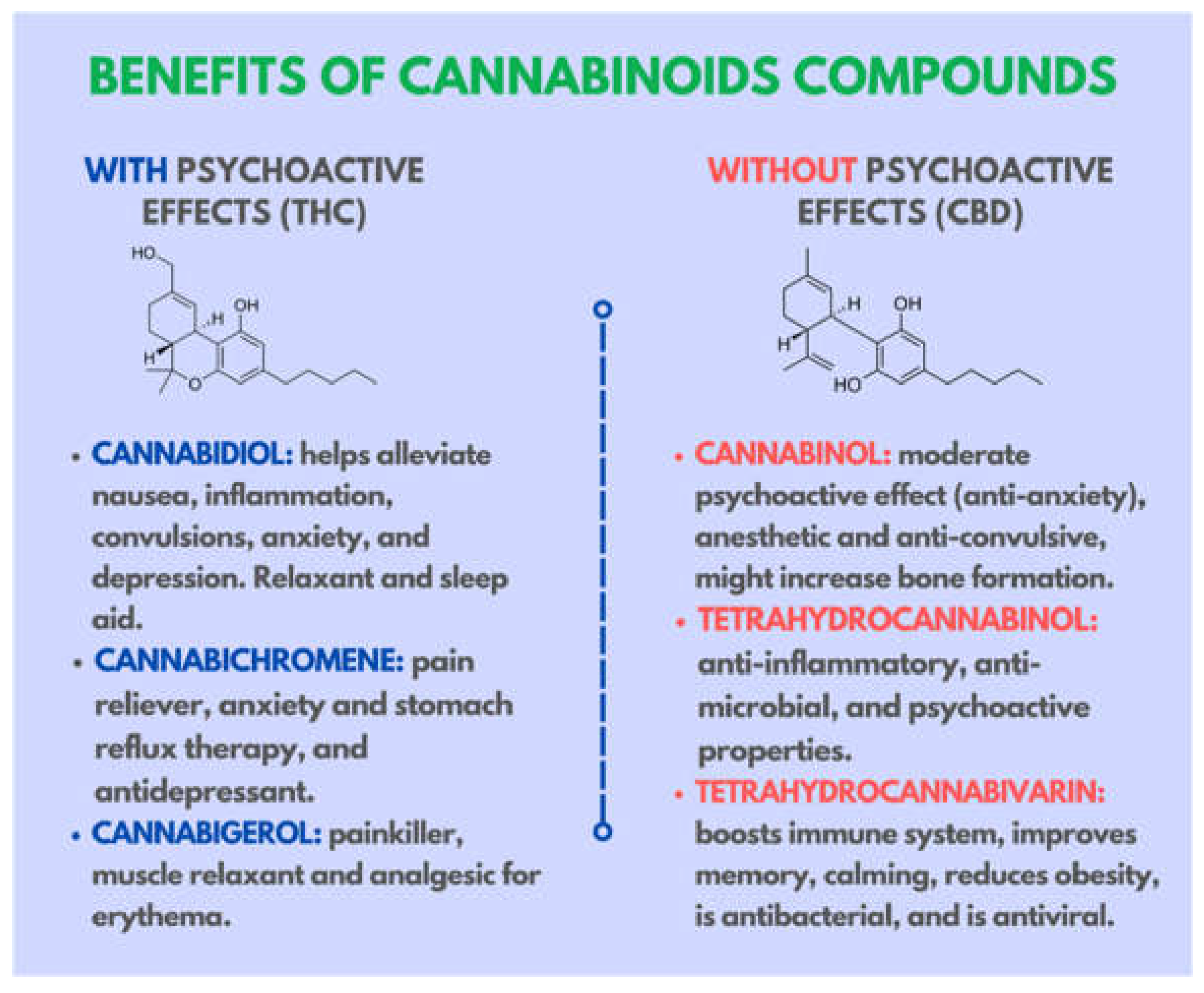
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



