
Submitted:
05 May 2023
Posted:
06 May 2023
You are already at the latest version
Abstract
Nutraceuticals are bioactive compounds present in foods, utilized to ameliorate health, prevent diseases, and support the proper functioning of the human body. They have gained attention due to their ability to hit multi-targets and act as antioxidants, anti-inflammatory agents, and modulators of immune response and cell death. Therefore, nutraceuticals are being studied to prevent and treat liver ischemia–reperfusion injury (IRI). This study evaluated the effect of a nutraceutical solution formed by resveratrol, quercetin, omega-3 fatty acid, selenium, ginger, avocado, leucine, and niacin on liver IRI. IRI was performed with 60 min of ischemia and 4 hours of reperfusion in male Wistar rats. Afterward, the animals were euthanized to study hepatocellular injury, cyto-kines, oxidative stress, gene expression of apoptosis-related genes, TNF-alpha and Caspase 3 proteins, and histology. Our results show that the nutraceutical solution was able to decrease apoptosis and histologic injury. The suggested mechanisms of action are a reduction in gene expression and the Caspase 3 protein and a reduction in the TNF-alpha protein in liver tissue. The nutraceutical solution was unable to decrease transaminases and cytokines. These findings suggest that the nutraceuticals used favored the protection of hepatocytes and their combination represent a promising therapeutic proposal against liver IRI.
Keywords:
nutraceuticals
; liver
; ischemia-reperfusion injury
; apoptosis
1. Introduction
Nutraceuticals are natural bioactive or chemical compounds which, in addition to playing a nutritional role, enhance health, cure illnesses, or have preventive properties [1,2]. They are dietary supplements, and from the nutritional point of view, nutraceuticals are a source of nutrients (lipids, carbohydrates, vitamins, proteins, minerals) and non-nutrients (prebiotics, probiotics, phytochemicals, enzymatic regulators) [1,3]. Nutraceuticals can be extracted from both vegetal and animal food, concentrated and administered in a suitable pharmaceutical form with the aim of improving health in dosages that exceed those obtainable from normal foods [4,5].
In vitro and in vivo studies have provided evidence that nutraceuticals have antioxidant, anti-inflammatory, antibacterial, antiviral, and antifungal activities, as well as to the fact that they act as modulators of immune response, angiogenesis, and cell death [4,6,7,8]. These effects are possible due to the multi-targets of nutraceuticals: endogenous glutathione, interleukins, cytokines, tumor necrosis factor, transcription factor nuclear factor-κB, growth factors, caspases, etc. [9,10].
By reaching all these targets, nutraceuticals are able to prevent several diseases, such as Diabetes mellitus, obesity, cardiovascular diseases, cancer, eye disorders, neurologic diseases, and liver IRI [11,12]. The latter is caused by a limited blood supply and subsequent blood supply recovery during surgical procedures including management of liver trauma, hepatic resection, and liver transplantation [13,14,15]. It represents the main underlying cause of primary graft dysfunction or non-function, liver failure post-transplantation, as well as it being an important risk factor for acute and chronic rejection [14,16].
Hepatic IRI remains a major unresolved problem in clinical practice [14]. Nutraceuticals are a rising therapy due to their nutritional and therapeutic benefits, as well as safety profile [11]. Some of them have already been studied and exhibited promising results, such as resveratrol, quercetin, omega-3 fatty acid, selenium, ginger, and avocado [17,18,19,20,21,22,23].
Currently, attention has been focused on the synergistic effects of nutraceutical combinations [24,25]. The “synergism concept” was introduced by Liu et al. [26,27]. In this regard, the combination of polyphenols and vitamins is extremely effective in preventing osteoporosis, cardiovascular diseases, cancer, diabetes mellitus, and neurodegenerative diseases [28].
This study aimed to formulate a nutraceutical solution comprising resveratrol, quercetin, omega-3 fatty acid, selenium, ginger, avocado, leucine, and niacin to target the various signaling pathways of liver IRI and decrease its effects. We studied hepatocellular injury, inflammatory mediators, apoptosis by TUNEL, gene expression of apoptosis-related genes, TNF-α and Caspase 3 proteins in liver tissue, and histology. We compared the results between five groups: CONTROL—no intervention; IR—rats submitted to liver IRI; NUTRACEUTICALS + IR (NUT + IR)—rats that received the nutraceutical solution by gavage for 7 days and underwent liver IRI; NUTRACEUTICALS (NUT)—rats that received the nutraceutical solution for 7 days; and SHAM—rats submitted only to hepatic manipulation.
2. Results
2.1. Hepatocellular Injury
The rats of the IR group exhibited a significant increase in serum levels of aspartate transaminase (AST) and alanine transaminase (ALT) compared to the CONTROL and NUT groups. The NUT + IR group presented a significant increase in serum levels of AST and ALT compared to the CONTROL group (Figure 1).
2.2. Inflammatory Mediators
There was no difference in terms of IL-1β, IL-6, and IL-10 among the groups. The serum TNF-α level was significantly increased in the IR group compared with the SHAM group (Figure 2).
2.3. Lipid Peroxidation
The CONTROL group exhibited a significantly higher level of MDA in liver tissue when compared to the IR, NUT + IR, and SHAM groups. The same was also observed in the NUT group compared to the NUT + IR group.
2.4. Gene Expression of Apoptosis: BAX, BCL-2, CASPASE 8, and CASPASE 3
The gene expression of BAX and BCL-2 was significantly higher in the NUT + IR group compared to the CONTROL and SHAM groups and similar to the NUT and IR groups. The latter group exhibited a significant increase in the gene expression of BAX compared to the CONTROL, NUT, and SHAM groups. Among the gene expression of CASPASES, there was only one difference with CASPASE 3. The gene expression of CASPASE 3 was significantly lower in the NUT + IR group than in the IR group, which in turn had a significantly higher gene expression compared to the CONTROL and SHAM groups (Figure 4).
2.5. Immunohistochemistry: Apoptosis, Cleaved Caspase 3, and TNF-α Proteins in the Liver
Apoptosis—TUNEL Assay
The TUNEL assay was used to determinate the apoptosis of the liver cells. The NUT + IR group exhibited a significant decrease in percentage of apoptosis compared to the IR group. Moreover, the IR group had a significantly higher percentage of apoptosis than the CONTROL, NUT, and SHAM groups (Figure 5).
Cleaved Caspase 3 Protein
The immunohistochemistry analysis showed that cleaved Caspase 3 protein in liver tissue was significantly lower in the NUT + IR group than in the IR group. This means that the nutraceutical solution was able to decrease both gene expression and Caspase 3 protein in IR injury. The IR group had a significantly higher Cleaved Caspase 3 protein level compared to the CONTROL and SHAM groups (Figure 6).
TNF-α Protein
In relation to TNF-α protein in liver tissue, the NUT group presented the highest significant percentage compared to all other groups. The IR group had a significantly higher TNF-α compared to the NUT + IR and SHAM groups (Figure 7).
2.5. Liver Histology Injury
According to the liver histological score used, the IR group (score 37) had a significantly higher liver injury when compared to the NUT+IR group (score 25). It was also observed that the immunohistochemical analysis of Caspase 3 showed a marked presence in the related field to IR injury by hematoxylin–eosin (HE), demonstrating a correlation between histological and immunohistochemical findings (Figure 8).
3. Discussion
Preexisting nutritional status affects post-operative metabolism, liver function, inflammation, and liver regenerative capacity [29,30]. Therefore, the patient condition plays an important role in predicting postoperative complications [12]. Particularly in hepatic IRI, the preexisting nutritional status is a major determinant of hepatocyte injury [31].
Several dietary components significantly benefit health, presenting antioxidant or anti-inflammatory properties [30,32]. Hence, the re-establishment and maintenance of correct nutritional status by these nutraceuticals before, during, and/or after surgery could lead to improvements in complications related to IRI. Thus, they represent a potential approach alone or in combination with other therapies to improve patient outcomes [12].
Our nutraceutical solution was unable to decrease the transaminases and cytokines released by liver IRI. One of the probable reasons for that is the fact that this study was conducted only in the early phase of IRI, not in the late phase when the peak of transaminases and necrosis occur [33,34]. Moreover, the inflammatory mediators reach their peaks at different moments: TNF-α peaks between 30min and 2 hours after reperfusion; IL-1β after 8h; IL-6 after 12h; and IL-10 between 30min and 3h after reperfusion [35,36,37,38,39]. Therefore, it is necessary to conduct further work to study the effect of nutraceutical solutions on the inflammatory process of hepatic IRI on a timeline.
During liver IRI, Kupffer cells produce reactive oxygen species (ROS) [40]. ROS play a dual role in IRI: they promote apoptosis and stimulate inflammatory mediators, as well as facilitating cell survival under hypoxic conditions and inducing antioxidant defenses [41]. In a healthy liver, in response to IRI, levels of PGC-1α, which is a transcriptional co-activator that controls the expression of metabolic pathways, which allow for cellular adaptation to limited nutrient availability, are stimulated, and this results in increased antioxidant defenses of the cell [42,43]. Supporting this fact, Fukai et al. demonstrated increased total glutathione and reduced glutathione after IRI [44]. This increased antioxidant capacity in non-lethal oxidative stress is one of the mechanisms of the protective effect of ischemic preconditioning [45], and may be the reason for which rats in the IR and NUT + IR groups exhibited lower levels of MDA than those in the CONTROL and NUT groups, respectively.
Following the line of not altering the inflammatory process, the nutraceutical solution was able to decrease apoptosis, which is a non-inflammatory subtype of cell death during hepatic IRI [46]. Apoptosis is a form of cell death which is critical in regulating tissue homeostasis, and it is considered the key mechanism of injury during the early phase of hepatic IRI in both experimental and human grafts [47,48,49]. During liver transplantation, apoptosis is involved in cellular injury in acute rejection, as well as in ductopenia seen in chronic rejection [50]. In addition, apoptosis of the donor’s liver is an important predictive factor for early graft dysfunction and its high rate is associated with shorter graft survival [51].
Furthermore, the histological evaluation adapted from Quireze et al.’s score [52] showed that the nutraceutical solution was also able to significantly reduce tissue injury caused by hepatic IRI. This finding is in accordance with the literature, which has demonstrated that inhibition of apoptosis can decrease IRI in liver grafts [49,53].
After seeing the effect of the nutraceutical solution on apoptosis, we investigated its possible mechanism of action and found that it causes a decrease in gene expression and the CASPASE 3 protein in liver tissue. These facts may characterize the nutraceutical solution as a Caspase inhibitor, that is a novel target to protect the liver from IRI [54]. In this regard, there are some compounds being studied such as IDN-6556 and F573. The pan-caspase inhibitor IDN-6556 inhibits caspase 3 activation and reduces sinusoidal endothelium cell apoptosis when used as an additive in the University of Wisconsin storage solution during the preservation period of rat livers [55]. Moreover, when it is administered in cold storage and flush solutions during human liver transplantation, it provides local therapeutic protection against IR injury and apoptosis [47]. IDN-6556 also protects both murine and human islets in culture and after transplantation, slows down the aminotransferase activity in HCV patients, and lowers portal pressure in patients with compensated cirrhosis and severe portal hypertension [56,57,58].
The other pan-caspase inhibitor F573, in turn, also mitigates liver IRI by reductions in the cytokine TNF-α, apoptosis, and the ALT level [59]. Another application of this caspase inhibitor was shown with the reduction in apoptosis of human and mouse pancreatic islets in vitro, and an improvement in their function when they are transplanted into the portal vein [60].
Besides our nutraceutical solution working as a caspase inhibitor, it was also able to decrease the TNF-α protein level in the liver tissue, which is another mechanism of action that may have contributed to decreasing apoptosis. In this regard, Ben-Ari et al. showed that treatment with the anti-TNF-α monoclonal antibody before ischemia is able to mitigate apoptosis by inhibiting the activity of caspases 9 e 3 [61].
There are many other diseases such as inflammatory disorders (psoriasis, arthritis, sepsis), neurologic diseases (Alzheimer’s, epilepsy), metabolic diseases (obesity, diabetes, nonalcoholic liver fatty disease), and cancer that are strongly associated with abnormal activity of caspases and apoptosis [62,63,64,65]. All these pathologies have already been studied and submitted to caspase inhibitor therapy, which opens up new perspectives for the clinical use of this nutraceutical combination.
All these studies broaden our horizons and make us think about other possibilities for the clinical use of the nutraceutical combination, in addition to liver IRI. However, before that, there is a need for further studies to establish all the mechanisms of action and the effects of this nutraceutical combination.
4. Materials and Methods
4.1. Animals
Thirty-seven male Wistar rats (245-345g) were obtained from the Institute of Medical Sciences of University of Sao Paulo and housed in LIM37 from University of São Paulo Medical School. They were placed at room temperature between 20° and 22°C, in a 12-hour light/dark cycle. The rats were fed with commercial Nuvilab CR-1 Irradiated feed (Nuvital®, Quimtia S.A) and hydrated with filtered water ad libitum. The experimental protocol was approved by the Ethics Committee in the use of animals of our institution (909).
4.2. Preparation of the Nutraceutical Solution
For the nutraceutical formulation, carboxymethyl cellulose (CMC) syrup 0.5% (Bio Idêntica Manipulation Pharmacy) was used as a vehicle [66,67].
In the preparation of the nutraceutical solution, omega-3 powder (Natural Products & Technologies) was weighed and transferred to a porcelain mortar, in which 0.5 ml of sunflower oil was added for its solubilization. Then, each remaining component was weighed separately, in the following order: resveratrol, quercetin, chelated selenium, dry ginger extract, avocado powder, leucine, and nicotinamide (Via Farma and Infinity Pharma). They were mixed with the solubilized omega-3 (Table 1).
The concentration of each nutraceutical ingredient was calculated for a rat with an average weight of 250 g and in a 100 ml solution, without exceeding the toxic limits of each one (Table 1).
4.3. Anesthesia and Surgical Procedures
The rats were anesthetized with 5% ketamine hydrochloride (Ketalar® Cristália) 100mg/kg and 2% xylazine hydrochloride (Rompum® Bayer), at a dose of 10mg/kg, intraperitoneally. The animals were submitted to orotracheal intubation with a Jelco 16 catheter (Jelco®) and ventilated with a tidal volume of 0.08 ml/g of weight, a respiratory rate of 60 cycles/min, and a FiO2 of 0.21 (Small Animal Ventilator model 683, Harvard Apparatus, Holliston, MA, USA).
A midline laparotomy was performed and the pedicles of the left lateral and median hepatic lobes were occluded with a 2.5 mm microvascular clamp, inducing the ischemia of approximately 70% of the total liver volume for 60 minutes [72,73]. The abdominal incision was closed with a continuous 4.0 nylon suture during this period of ischemia to prevent dehydration and hypothermia in animals.
After 60 minutes of ischemia, the abdomen of the rats was opened again and the clamp was removed to allow for 4 hours of liver reperfusion [72,73]. The incision was closed again, and the animals returned to individual cages.
Following the reperfusion time, rats were anesthetized again, and a new midline laparotomy with median thoracotomy was performed. A blood sample was collected through cardiac puncture. Then, the left ventricle was punctured with a Jelco 16 catheter and connected to a 250ml 0.9% saline solution; the rats were euthanized, and their organs were carefully washed with saline solution [74].
After the liver had been washed homogeneously, a partial hepatectomy of previously ischemic lobes was performed.
4.4. Experimental Design
The rats were allocated into five groups. In the CONTROL group (n=8), the rats did not undergo any surgical procedure. In the IR Group (n=8), the animals were submitted to hepatic IR. In the NUT + IR group (n=8), the rats received a nutraceutical solution for seven consecutive days before hepatic IR was performed. In the NUT group (n=8), the animals received a nutraceutical solution for seven consecutive days. Additionally, in the SHAM group (n=5), the rats underwent midline laparotomy and the liver was manipulated without pedicled clamping.
4.5. Serum Biochemical Analysis
Serum aspartate aminotransferase (AST) and alanine aminotransferase (ALT) were used as indicators of liver injury. AST and ALT activities were assayed 4 hours after reperfusion by ultraviolet kinetic method (COBAS C111, Roche, Indianapolis, USA) according to the International Federation of Clinical Chemistry. The results are expressed in units per liter (U/L).
The following inflammatory mediators were also evaluated: interleukin 1 beta (IL1-ß), interleukin 6 (IL-6), interleukin 10 (IL-10), and TNF-α. Plasma specimens were prepared for analysis in a 96-well plate utilizing a kit of 13-cytokine Milliplex MAP Human Cytokine/Chemokine Magnetic Bead Panel (Millipore Corp., Billerica, MA) following the manufacturer’s recommendations.
Concentrations of cytokines were determined from a standard curve of the mean fluorescence intensity versus pg/ml.
4.6. Oxidative Stress
The MDA concentration was determined by reverse-phase High-Performance Liquid Chromatography (HPLC) according to Hong et al. [75]. Liver tissue homogenate (1/40 PBS v/v) (0.05 mL) was submitted to alkaline hydrolysis with 12.5 µL of 0.2% butylated hydroxytoluene in ethanol and 6.25 µL of a 10 M sodium hydroxide aqueous solution. This mixture was incubated at 60°C for 30 min and 750 µL of 7.2% TCA aqueous solution containing 1% KI were added. The samples were kept on ice for 10 min and centrifuged at 10,000 x g for 10 min. The supernatant (500 µL) was mixed with 250 µL of 0.6% TBA and heated at 95°C for 30 min. After cooling, the MDA was extracted from the solution with 750µL of n-butanol and analyzed by HPLC (Agilent Technologies 1200 series; Santa Clara, CA, USA). The TBA-MDA conjugate derivative (50 µL) was injected into a Phenomenex reverse-phase C18 analytical column (250 x 4.6 mm; 5 µm, Phenomenex, Torrance, CA, USA) with a LC8-D8 pre-column (Phenomenex AJ0-1287) and was quantified using fluorometric detection at excitation and emission wavelengths of 515 and of 553 nm, respectively [75].
The analysis was run under isocratic conditions, using a mobile phase of 60% phosphate-buffered saline (PBS) (50 mmol, pH 7.1) + 40% methanol at a flow rate of 1.0 mL/min. A standard curve (15 – 80 µmol MDA, r= 0.9981) was prepared using 1,1,3,3-tetraethoxypropane. The protein concentration was measured by the BCA method using the Pierce BCA kit (Thermo Fisher Scientific, Massachusetts, USA) as per the manufacturer’s instructions and a solution of bovine serum albumin as standard for the calibration curve (0.025 – 2.00 mg ptn/mL, r= 0.9969) [75]. Samples were analyzed using a Synergy HT Spectrophotometer (BioTek, Vermont, USA) with Gen5 software (BioTek). The results are expressed as μg MDA/mg protein.
4.7. Gene Expression of Apoptosis
Liver tissue from animals in each group was collected, immediately frozen in liquid nitrogen, and stored at -80ºC until RNA extraction was performed. For the extraction of total RNA, TRIZOL™ reagent (Life Technologies Carlsbad, USA) was used according to the protocol proposed by the manufacturer.
The RNA concentration was determined by NanoDrop ND-1000 spectrophotometer. The degree of RNA purity was evaluated by 260/280nm ratio, using only those whose ratio was ≥ 1.8. The integrity profile of extracted RNA was evaluated by electrophoresis to verify the presence of bands corresponding to 18S and 28S ribosomal RNAs. The quantified RNA was stored at -80ºC until use.
The design of oligonucleotides was conducted with the Primer 3 program (http://primer3.ut.ee). Analysis of the expression of mRNA levels of BAX, Bcl-2, Caspase 3, and Caspase 8 genes was performed on Rotor-Gene RG-3000 thermocycler (Corbett Research, Sydney, Australia). The commercial kit SuperScript™ III Platinum® SYBR Green One-Step qRT-PCR (Life Technologies Corporation) was used. Beta-actin gene was used as a normalizer of qRT-PCR reactions. The 2-Delta Delta CT method was used for relative quantification of gene expression (Livak & Schmittgen, 2001).
4.8. Immunohistochemistry
Apoptosis
For the in situ detection of apoptosis in a single cell, the final identification deoxynucleotidyl transferase (TdT) test was used (TUNEL; Boehringer Mannhein, Germany) [76,77]. According to the standard established in the Laboratory of Histomorphometry and Lung Genomics at the University of São Paulo Medical School, 3-4µm thick sections of liver tissue were made and placed on silanized slides (Sigma Chemical Co.; St. Louis, Missouri, USA) on a suitable support, as previously described by Souza et al. [78].
Cleaved Caspase 3 and TNF-α Proteins
Subserial sections from the paraffin blocks were used for immunohistochemistry. The antibodies used were Caspase 3 and TNF-α (Table 2). Immunohistochemistry was performed according to the manufacturer’s instructions.
Briefly, after the deparanifinization process and the hydration of the liver tissue sections, the recovery of antigenic sites was performed by high temperature in citrate pH 6 for Caspase 3 and TRIS-EDTA pH 9 for TNF-α. Endogenous peroxidase blocking was performed with 10v (3%) oxygenated water four times for 5 minutes for caspase 3 and for TNF-α with methanol and oxygenated water, volume by volume, two times for 10 minutes. In the latter two antibodies, protein blots were made, and then the slides were washed in tap water, followed by distilled water, and left in TBS buffer at pH 7.4.
The antibodies were diluted at concentrations shown in the table below (Table 2). The slides were incubated overnight at 4°C in a humid chamber. Subsequently, incubation was performed with the secondary antibody (ABC Elite, Vector Laboratories Inc) specific for each species and the antibody was produced for 30 minutes in an incubator at 37ºC. Diaminobenzidine (DAB) (Sigma-Aldrich Chemie, Steinheim, Germany) was used as the chromogen. Then, counterstaining was performed with Harris’ Hematoxylin (Merck, Darmstadt, Germany).
4.9. Histology
Samples from the median and left anterolateral liver lobes were collected 4 hours after reperfusion and fixed in 10% formalin for standard hematoxylin and eosin (HE) staining. A single-blinded pathologist performed the histologic evaluation.
The histologic injury was evaluated according to the scoring system proposed by Quireze et al. [52], which was adapted based on the presence and intensity of the following alterations: ballooning, steatosis, apoptosis, loss of hepatic trabeculae, and necrosis. Those lesions were graded according to the absence (grade 0) or presence of minimal (grade 1), moderate (grade 2), or severe (grade 3) alterations, as determined by the pathologist.
5.0. Data Processing
Data were statistically analyzed using GraphPad Prism software (version 9.5.1). One-way analysis of variance (ANOVA) was used to assess differences between tested groups, followed by Tukey’s multiple comparison tests. The non-parametric results of transaminases and gene expression were analyzed by the Kruskal–Wallis test, followed by Dunn’s test. Categorical data of liver histological injury were analyzed using the Chi-square statistic. The results are presented as means ± standard errors of means (SEM). A p-value less than 0.05 was considered statistically significant.
5. Conclusions
In summary, we proposed a nutraceutical solution that was able to decrease apoptosis and histologic injury caused by liver IRI. Its suggested mechanisms of action are a reduction in gene expression and Caspase 3 protein, as well as a reduction in TNF-α protein in liver tissue. These findings suggest that the nutraceutical combination used in the present study favors the protection of hepatocytes and represents a promising therapeutic proposal against liver IRI.
Author Contributions
Conceptualization, F.H.G. and V.R.S.; methodology, F.H.G and I.A.C.; investigation, C.A.P. and M.S.K.; writing—original draft preparation, C.A.P.; writing—review and editing, M.S.K. and V.R.S.; visualization, M.S.K.; supervision, L.A.C.D.; project administration, F.H.G.; funding acquisition, L.A.C.D.
Funding
This research and the APC were funded by Coordenação de Aperfeiçoamento de Pessoal de Nível Superior (CAPES – 00690623909), an institutional quota.
Institutional Review Board Statement
The animal study protocol was approved by the Comitê de Ética no Uso de Animais (CEUA) of University of São Paulo Medical School (registration number 909/2017 and date of approval 13 September 2017).
Data Availability Statement
The data presented in this study are available upon request from the corresponding author.
Acknowledgments
This work was developed in the Medical Research Laboratories (LIM 37 and 03) at the University of São Paulo Medical School. Special thanks to our colleagues Sandra Nassa Sampietri, Cinthia Lanchotte, Regina Célia Teixeira Gomes, Ângela Batista Gomes dos Santos, Esmeralda Miristeni Eher, and Sandra de Morais Fernezlian.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Sachdeva, V.; Roy, A.; Bharadvaja, N. Current Prospects of Nutraceuticals: A Review. Curr Pharm Biotechnol 2020, 21, 884–896. [Google Scholar] [CrossRef] [PubMed]
- Brower, V. Nutraceuticals: Poised for a Healthy Slice of the Healthcare Market? Nat Biotechnol 1998, 16, 728–731. [Google Scholar] [CrossRef] [PubMed]
- Bergamin, A.; Mantzioris, E.; Cross, G.; Deo, P.; Garg, S.; Hill, A.M. Nutraceuticals: Reviewing Their Role in Chronic Disease Prevention and Management. Pharmaceut Med 2019, 33, 291–309. [Google Scholar] [CrossRef] [PubMed]
- D’Angelo, S.; Scafuro, M.; Meccariello, R. BPA and Nutraceuticals, Simultaneous Effects on Endocrine Functions. Endocr Metab Immune Disord Drug Targets 2019, 19, 594–604. [Google Scholar] [CrossRef] [PubMed]
- Espín, J.C.; García-Conesa, M.T.; Tomás-Barberán, F.A. Nutraceuticals: Facts and Fiction. Phytochemistry 2007, 68, 2986–3008. [Google Scholar] [CrossRef] [PubMed]
- Prasad, S.; Gupta, S.C.; Tyagi, A.K. Reactive Oxygen Species (ROS) and Cancer: Role of Antioxidative Nutraceuticals. Cancer Lett 2017, 387, 95–105. [Google Scholar] [CrossRef] [PubMed]
- Song, J.-M.; Lee, K.-H.; Seong, B.-L. Antiviral Effect of Catechins in Green Tea on Influenza Virus. Antiviral Res 2005, 68, 66–74. [Google Scholar] [CrossRef]
- de Mejia, E.G.; Dia, V.P. The Role of Nutraceutical Proteins and Peptides in Apoptosis, Angiogenesis, and Metastasis of Cancer Cells. Cancer and Metastasis Reviews 2010, 29, 511–528. [Google Scholar] [CrossRef]
- Aggarwal, B.B.; Van Kuiken, M.E.; Iyer, L.H.; Harikumar, K.B.; Sung, B. Molecular Targets of Nutraceuticals Derived from Dietary Spices: Potential Role in Suppression of Inflammation and Tumorigenesis. Exp Biol Med 2009, 234, 825–849. [Google Scholar] [CrossRef]
- Liu, B.; Cheng, Y.; Zhang, B.; Bian, H.; Bao, J. Polygonatum Cyrtonema Lectin Induces Apoptosis and Autophagy in Human Melanoma A375 Cells through a Mitochondria-Mediated ROS–P38–P53 Pathway. Cancer Lett 2009, 275, 54–60. [Google Scholar] [CrossRef]
- Puri, V.; Nagpal, M.; Singh, I.; Singh, M.; Dhingra, G.A.; Huanbutta, K.; Dheer, D.; Sharma, A.; Sangnim, T. A Comprehensive Review on Nutraceuticals: Therapy Support and Formulation Challenges. Nutrients 2022, 14, 4637. [Google Scholar] [CrossRef] [PubMed]
- Cornide-Petronio, M.E.; Álvarez-Mercado, A.I.; Jiménez-Castro, M.B.; Peralta, C. Current Knowledge about the Effect of Nutritional Status, Supplemented Nutrition Diet, and Gut Microbiota on Hepatic Ischemia-Reperfusion and Regeneration in Liver Surgery. Nutrients 2020, 12, 284. [Google Scholar] [CrossRef] [PubMed]
- Eltzschig, H.K.; Eckle, T. Ischemia and Reperfusion—from Mechanism to Translation. Nat Med 2011, 17, 1391–1401. [Google Scholar] [CrossRef] [PubMed]
- Jiménez-Castro, M.B.; Cornide-Petronio, M.E.; Gracia-Sancho, J.; Peralta, C. Inflammasome-Mediated Inflammation in Liver Ischemia-Reperfusion Injury. Cells 2019, 8, 1131. [Google Scholar] [CrossRef] [PubMed]
- Oliveira, T.H.C. de; Marques, P.E.; Proost, P.; Teixeira, M.M.M. Neutrophils: A Cornerstone of Liver Ischemia and Reperfusion Injury. Laboratory Investigation 2018, 98, 51–62. [Google Scholar] [CrossRef] [PubMed]
- Zhai, Y.; Petrowsky, H.; Hong, J.C.; Busuttil, R.W.; Kupiec-Weglinski, J.W. Ischaemia–Reperfusion Injury in Liver Transplantation—from Bench to Bedside. Nat Rev Gastroenterol Hepatol 2013, 10, 79–89. [Google Scholar] [CrossRef] [PubMed]
- He, D.; Guo, Z.; Pu, J.-L.; Zheng, D.-F.; Wei, X.-F.; Liu, R.; Tang, C.-Y.; Wu, Z.-J. Resveratrol Preconditioning Protects Hepatocytes against Hepatic Ischemia Reperfusion Injury via Toll-like Receptor 4/Nuclear Factor-ΚB Signaling Pathway in Vitro and in Vivo. Int Immunopharmacol 2016, 35, 201–209. [Google Scholar] [CrossRef] [PubMed]
- Su, J.-F.; Guo, C.-J.; Wei, J.-Y.; Yang, J.-J.; Jiang, Y.-G.; Li, Y.-F. Protection against Hepatic Ischemia-Reperfusion Injury in Rats by Oral Pretreatment with Quercetin. Biomed Environ Sci 2003, 16, 1–8. [Google Scholar]
- Calder, P.C. Mechanisms of Action of (n-3) Fatty Acids, J Nutr 2012, 142, 592S–599S. [Google Scholar] [CrossRef]
- Zapletal, C.; Heyne, S.; Breitkreutz, R.; Gebhard, M.M.; Golling, M. The Influence of Selenium Substitution on Microcirculation and Glutathione Metabolism after Warm Liver Ischemia/Reperfusion in a Rat Model. Microvasc Res 2008, 76, 104–109. [Google Scholar] [CrossRef]
- Abdel-Azeem, A.S.; Hegazy, A.M.; Ibrahim, K.S.; Farrag, A.-R.H.; El-Sayed, E.M. Hepatoprotective, Antioxidant, and Ameliorative Effects of Ginger ( Zingiber Officinale Roscoe ) and Vitamin E in Acetaminophen Treated Rats. J Diet Suppl 2013, 10, 195–209. [Google Scholar] [CrossRef]
- Maghsoudi, S.; Gol, A.; Dabiri, S.; Javadi, A. Preventive Effect of Ginger (Zingiber Officinale) Pretreatment on Renal Ischemia-Reperfusion in Rats. European Surgical Research 2011, 46, 45–51. [Google Scholar] [CrossRef]
- Eser, O.; Songur, A.; Yaman, M.; Cosar, M.; Fidan, H.; Sahin, O.; Mollaoglu, H.; Buyukbas, S. The Protective Effect of Avocado Soybean Unsaponifilables on Brain Ischemia/Reperfusion Injury in Rat Prefrontal Cortex. Br J Neurosurg 2011, 25, 701–706. [Google Scholar] [CrossRef]
- Araujo, Q.R. De; Gattward, J.N.; Almoosawi, S.; Parada Costa Silva, M. das G.C.; Dantas, P.A.D.S.; Araujo Júnior, Q.R. De Cocoa and Human Health: From Head to Foot—A Review. Crit Rev Food Sci Nutr 2016, 56, 1–12. [Google Scholar] [CrossRef]
- Singh, C.K.; Siddiqui, I.A.; El-Abd, S.; Mukhtar, H.; Ahmad, N. Combination Chemoprevention with Grape Antioxidants. Mol Nutr Food Res 2016, 60, 1406–1415. [Google Scholar] [CrossRef]
- Liu, R.H. Health Benefits of Fruit and Vegetables Are from Additive and Synergistic Combinations of Phytochemicals. Am J Clin Nutr 2003, 78, 517S–520S. [Google Scholar] [CrossRef]
- Liu, R.H. Potential Synergy of Phytochemicals in Cancer Prevention: Mechanism of Action. J Nutr 2004, 134, 3479S–3485S. [Google Scholar] [CrossRef]
- Hegazy, A.M.; El-Sayed, E.M.; Ibrahim, K.S.; Abdel-Azeem, A.S. Dietary Antioxidant for Disease Prevention Corroborated by the Nrf2 Pathway. J Complement Integr Med 2019, 16. [Google Scholar] [CrossRef]
- Saïdi, S.; Abdelkafi, S.; Jbahi, S.; van Pelt, J.; El-Feki, A. Temporal Changes in Hepatic Antioxidant Enzyme Activities after Ischemia and Reperfusion in a Rat Liver Ischemia Model. Hum Exp Toxicol 2015, 34, 249–259. [Google Scholar] [CrossRef]
- Silva, R.M. da; Malafaia, O.; Torres, O.J.M.; Czeczko, N.G.; Marinho Junior, C.H.; Kozlowski, R.K. Evaluation of Liver Regeneration Diet Supplemented with Omega-3 Fatty Acids: Experimental Study in Rats. Rev Col Bras Cir 2015, 42, 393–397. [Google Scholar] [CrossRef]
- Domenicali, M.; Vendemiale, G.; Serviddio, G.; Grattagliano, I.; Pertosa, A.M.; Nardo, B.; Principe, A.; Viola, A.; Trevisani, F.; Altomare, E.; et al. Oxidative Injury in Rat Fatty Liver Exposed to Ischemia-Reperfusion Is Modulated by Nutritional Status. Digestive and Liver Disease 2005, 37, 689–697. [Google Scholar] [CrossRef]
- Chandrasekara, A.; Josheph Kumar, T. Roots and Tuber Crops as Functional Foods: A Review on Phytochemical Constituents and Their Potential Health Benefits. Int J Food Sci 2016, 2016, 1–15. [Google Scholar] [CrossRef]
- Hasegawa, T.; Ito, Y.; Wijeweera, J.; Liu, J.; Malle, E.; Farhood, A.; McCuskey, R.S.; Jaeschke, H. Reduced Inflammatory Response and Increased Microcirculatory Disturbances during Hepatic Ischemia-Reperfusion Injury in Steatotic Livers of Ob/Ob Mice. American Journal of Physiology-Gastrointestinal and Liver Physiology 2007, 292, G1385–G1395. [Google Scholar] [CrossRef]
- Fang, H.; Liu, A.; Dahmen, U.; Dirsch, O. Dual Role of Chloroquine in Liver Ischemia Reperfusion Injury: Reduction of Liver Damage in Early Phase, but Aggravation in Late Phase. Cell Death Dis 2013, 4, e694–e694. [Google Scholar] [CrossRef]
- Perry, B.C.; Soltys, D.; Toledo, A.H.; Toledo-Pereyra, L.H. Tumor Necrosis Factor-α in Liver Ischemia/Reperfusion Injury. Journal of Investigative Surgery 2011, 24, 178–188. [Google Scholar] [CrossRef]
- Kato, A.; Gabay, C.; Okaya, T.; Lentsch, A.B. Specific Role of Interleukin-1 in Hepatic Neutrophil Recruitment after Ischemia/Reperfusion. Am J Pathol 2002, 161, 1797–1803. [Google Scholar] [CrossRef]
- Cui, L.-Z.; Wang, B.; Chen, L.-Y.; Zhou, J. The Effect of Ischemic Precondition to IL-6 on Rat Liver Ischemia-Reperfusion Injury in Transplantation. Asian Pac J Trop Med 2013, 6, 395–399. [Google Scholar] [CrossRef]
- Oreopoulos, G.D.; Wu, H.; Szaszi, K.; Fan, J.; Marshall, J.C.; Khadaroo, R.G.; He, R.; Kapus, A.; Rotstein, O.D. Hypertonic Preconditioning Prevents Hepatocellular Injury Following Ischemia/Reperfusion in Mice: A Role for Interleukin 10. Hepatology 2004, 40, 211–220. [Google Scholar] [CrossRef]
- Guimarães Filho, M.A.C.; Cortez, E.; Garcia-Souza, É.P.; Soares, V. de M.; Moura, A.S.; Carvalho, L.; Maya, M.C. de A.; Pitombo, M.B. Effect of Remote Ischemic Preconditioning in the Expression of IL-6 and IL-10 in a Rat Model of Liver Ischemia-Reperfusion Injury. Acta Cir Bras 2015, 30, 452–460. [Google Scholar] [CrossRef]
- Kaltenmeier, C.; Wang, R.; Popp, B.; Geller, D.; Tohme, S.; Yazdani, H.O. Role of Immuno-Inflammatory Signals in Liver Ischemia-Reperfusion Injury. Cells 2022, 11, 2222. [Google Scholar] [CrossRef]
- Prieto, I.; Monsalve, M. ROS Homeostasis, a Key Determinant in Liver Ischemic-Preconditioning. Redox Biol 2017, 12, 1020–1025. [Google Scholar] [CrossRef]
- Sánchez-Ramos, C.; Prieto, I.; Tierrez, A.; Laso, J.; Valdecantos, M.P.; Bartrons, R.; Roselló-Catafau, J.; Monsalve, M. PGC-1α Downregulation in Steatotic Liver Enhances Ischemia-Reperfusion Injury and Impairs Ischemic Preconditioning. Antioxid Redox Signal 2017, 27, 1332–1346. [Google Scholar] [CrossRef]
- Summermatter, S.; Handschin, C. PGC-1α and Exercise in the Control of Body Weight. Int J Obes 2012, 36, 1428–1435. [Google Scholar] [CrossRef]
- Fukai, M.; Hayashi, T.; Yokota, R.; Shimamura, T.; Suzuki, T.; Taniguchi, M.; Matsushita, M.; Furukawa, H.; Todo, S. Lipid Peroxidation during Ischemia Depends on Ischemia Time in Warm Ischemia and Reperfusion of Rat Liver. Free Radic Biol Med 2005, 38, 1372–1381. [Google Scholar] [CrossRef]
- Rüdiger, H.A.; Graf, R.; Clavien, P.-A. Sub-Lethal Oxidative Stress Triggers the Protective Effects of Ischemic Preconditioning in the Mouse Liver. J Hepatol 2003, 39, 972–977. [Google Scholar] [CrossRef]
- Hirao, H.; Nakamura, K.; Kupiec-Weglinski, J.W. Liver Ischaemia–Reperfusion Injury: A New Understanding of the Role of Innate Immunity. Nat Rev Gastroenterol Hepatol 2022, 19, 239–256. [Google Scholar] [CrossRef]
- Baskin-Bey, E.S.; Washburn, K.; Feng, S.; Oltersdorf, T.; Shapiro, D.; Huyghe, M.R.; Burgart, L.; Garrity-Park, M.; Van Vilsteren, F.G.I.; Oliver, L.K.; et al. Clinical Trial of the Pan-Caspase Inhibitor, IDN-6556, in Human Liver Preservation Injury. American Journal of Transplantation 2007, 7, 218–225. [Google Scholar] [CrossRef]
- Sindram, D.; Porte, R.J.; Hoffman, M.R.; Bentley, R.C.; Clavien, P. Platelets Induce Sinusoidal Endothelial Cell Apoptosis upon Reperfusion of the Cold Ischemic Rat Liver. Gastroenterology 2000, 118, 183–191. [Google Scholar] [CrossRef]
- Kuo, P.C.; Drachenberg, C.I.; de la Torre, A.; Bartlett, S.T.; Lim, J.W.; Plotkin, J.S.; Johnson, L.B. Apoptosis and Hepatic Allograft Reperfusion Injury. Clin Transplant 1998, 12, 219–223. [Google Scholar]
- PAROLIN, M.B.; REASON, I.J.M. Apoptose Como Mecanismo de Lesão Nas Doenças Hepatobiliares. Arq Gastroenterol 2001, 38, 138–144. [Google Scholar] [CrossRef]
- Zhu, Z.; Tang, Y.; Huang, S.; Zhao, Q.; Schroder, P.M.; Zhang, Z.; Zhang, Y.; Sun, C.; Wang, L.; Ju, W.; et al. Donor Liver Apoptosis Is Associated with Early Allograft Dysfunction and Decreased Short-Term Graft Survival after Liver Transplantation. Clin Transplant 2018, e13438. [Google Scholar] [CrossRef]
- Quireze, C.; de Souza Montero, E.F.; Leitão, R.M.C.; Juliano, Y.; Fagundes, D.J.; Poli-de-Figueiredo, L.F. Ischemic Preconditioning Prevents Apoptotic Cell Death and Necrosis in Early and Intermediate Phases of Liver Ischemia-Reperfusion Injury in Rats. Journal of Investigative Surgery 2006, 19, 229–236. [Google Scholar] [CrossRef]
- Zhang, Y.; Ye, Q.-F.; Lu, L.; Xu, X.-L.; Ming, Y.-Z.; Xiao, J.-S. Panax Notoginseng Saponins Preconditioning Protects Rat Liver Grafts from Ischemia/Reperfusion Injury via an Antiapoptotic Pathway. Hepatobiliary Pancreat Dis Int 2005, 4, 207–212. [Google Scholar]
- Mao, X.; Cai, Y.; Chen, Y.; Wang, Y.; Jiang, X.; Ye, L.; Li, S. Novel Targets and Therapeutic Strategies to Protect Against Hepatic Ischemia Reperfusion Injury. Front Med (Lausanne) 2022, 8. [Google Scholar] [CrossRef]
- Natori, S. The Caspase Inhibitor IDN-6556 Prevents Caspase Activation and Apoptosis in Sinusoidal Endothelial Cells during Liver Preservation Injury. Liver Transplantation 2003, 9, 278–284. [Google Scholar] [CrossRef]
- McCall, M.; Toso, C.; Emamaullee, J.; Pawlick, R.; Edgar, R.; Davis, J.; Maciver, A.; Kin, T.; Arch, R.; Shapiro, A.M.J. The Caspase Inhibitor IDN-6556 (PF3491390) Improves Marginal Mass Engraftment after Islet Transplantation in Mice. Surgery 2011, 150, 48–55. [Google Scholar] [CrossRef]
- Pockros, P.J.; Schiff, E.R.; Shiffman, M.L.; McHutchison, J.G.; Gish, R.G.; Afdhal, N.H.; Makhviladze, M.; Huyghe, M.; Hecht, D.; Oltersdorf, T.; et al. Oral IDN-6556, an Antiapoptotic Caspase Inhibitor, May Lower Aminotransferase Activity in Patients with Chronic Hepatitis C. Hepatology 2007, 46, 324–329. [Google Scholar] [CrossRef]
- Garcia-Tsao, G.; Fuchs, M.; Shiffman, M.; Borg, B.B.; Pyrsopoulos, N.; Shetty, K.; Gallegos-Orozco, J.F.; Reddy, K.R.; Feyssa, E.; Chan, J.L.; et al. Emricasan (IDN-6556) Lowers Portal Pressure in Patients With Compensated Cirrhosis and Severe Portal Hypertension. Hepatology 2019, 69, 717–728. [Google Scholar] [CrossRef]
- Bral, M.; Pawlick, R.; Marfil-Garza, B.; Dadheech, N.; Hefler, J.; Thiesen, A.; James Shapiro, A.M. Pan-Caspase Inhibitor F573 Mitigates Liver Ischemia Reperfusion Injury in a Murine Model. PLoS One 2019, 14. [Google Scholar] [CrossRef]
- Pepper, A.R.; Bruni, A.; Pawlick, R.; Wink, J.; Rafiei, Y.; Gala-Lopez, B.; Bral, M.; Abualhassan, N.; Kin, T.; Shapiro, A.M.J. Engraftment Site and Effectiveness of the Pan-Caspase Inhibitor F573 to Improve Engraftment in Mouse and Human Islet Transplantation in Mice. Transplantation 2017, 101, 2321–2329. [Google Scholar] [CrossRef]
- Ben-Ari, Z.; Hochhauser, E.; Burstein, I.; Papo, O.; Kaganovsky, E.; Krasnov, T.; Vamichkim, A.; Vidne, B.A. Role of Anti-Tumor Necrosis Factor-Alpha in Ischemia/Reperfusion Injury in Isolated Rat Liver in a Blood-Free Environment. Transplantation 2002, 73, 1875–1880. [Google Scholar] [CrossRef]
- Dhani, S.; Zhao, Y.; Zhivotovsky, B. A Long Way to Go: Caspase Inhibitors in Clinical Use. Cell Death Dis 2021, 12, 949. [Google Scholar] [CrossRef]
- Ghavami, S.; Shojaei, S.; Yeganeh, B.; Ande, S.R.; Jangamreddy, J.R.; Mehrpour, M.; Christoffersson, J.; Chaabane, W.; Moghadam, A.R.; Kashani, H.H.; et al. Autophagy and Apoptosis Dysfunction in Neurodegenerative Disorders. Prog Neurobiol 2014, 112, 24–49. [Google Scholar] [CrossRef]
- Sassmann-Schweda, A.; Singh, P.; Tang, C.; Wietelmann, A.; Wettschureck, N.; Offermanns, S. Increased Apoptosis and Browning of TAK1-Deficient Adipocytes Protects against Obesity. JCI Insight 2016, 1. [Google Scholar] [CrossRef]
- Pfeffer, C.; Singh, A. Apoptosis: A Target for Anticancer Therapy. Int J Mol Sci 2018, 19, 448. [Google Scholar] [CrossRef]
- Rani, M.; Rudhziah, S.; Ahmad, A.; Mohamed, N. Biopolymer Electrolyte Based on Derivatives of Cellulose from Kenaf Bast Fiber. Polymers (Basel) 2014, 6, 2371–2385. [Google Scholar] [CrossRef]
- Javanbakht, S.; Shaabani, A. Carboxymethyl Cellulose-Based Oral Delivery Systems. Int J Biol Macromol 2019, 133, 21–29. [Google Scholar] [CrossRef]
- Brai, B.; Adisa, R.; Odetola, A. Hepatoprotective Properties Of Aqueous Leaf Extract Of Persea Americana, Mill (Lauraceae) ‘Avocado’ Against Ccl4-Induced Damage In Rats. African Journal of Traditional, Complementary and Alternative Medicines 2014, 11, 237. [Google Scholar] [CrossRef]
- Iwasaki, W.; Kume, M.; Kudo, K.; Uchinami, H.; Kikuchi, I.; Nakagawa, Y.; Yoshioka, M.; Yamamoto, Y. Changes in the Fatty Acid Composition of the Liver with the Administration of N-3 Polyunsaturated Fatty Acids and the Effects on Warm Ischemia/Reperfusion Injury in the Rat Liver. Shock 2010, 33, 306–314. [Google Scholar] [CrossRef]
- Zúñiga, J.; Venegas, F.; Villarreal, M.; Núñez, D.; Chandía, M.; Valenzuela, R.; Tapia, G.; Varela, P.; Videla, L.A.; Fernández, V. Protection against in Vivo Liver Ischemia-Reperfusion Injury by n-3 Long-Chain Polyunsaturated Fatty Acids in the Rat. Free Radic Res 2010, 44, 854–863. [Google Scholar] [CrossRef]
- Miyauchi, T.; Uchida, Y.; Kadono, K.; Hirao, H.; Kawasoe, J.; Watanabe, T.; Ueda, S.; Jobara, K.; Kaido, T.; Okajima, H.; et al. Preventive Effect of Antioxidative Nutrient-Rich Enteral Diet Against Liver Ischemia and Reperfusion Injury. Journal of Parenteral and Enteral Nutrition 2019, 43, 133–144. [Google Scholar] [CrossRef] [PubMed]
- Rocha-Santos, V.; Figueira, E.R.; Rocha-Filho, J.A.; Coelho, A.M.; Pinheiro, R.S.; Bacchella, T.; Machado, M.C.; D’Albuquerque, L.A. Pentoxifylline Enhances the Protective Effects of Hypertonic Saline Solution on Liver Ischemia Reperfusion Injury through Inhibition of Oxidative Stress. Hepatobiliary & Pancreatic Diseases International 2015, 14, 194–200. [Google Scholar] [CrossRef]
- Figueira, E.R.R.; Bacchella, T.; Coelho, A.M.M.; Sampietre, S.N.; Molan, N.A.T.; Leitão, R.M.C.; Machado, M.C.C. Timing-Dependent Protection of Hypertonic Saline Solution Administration in Experimental Liver Ischemia/Reperfusion Injury. Surgery 2010, 147, 415–423. [Google Scholar] [CrossRef] [PubMed]
- Fernandes, D.C.; Gonçalves, R.C.; Laurindo, F.R.M. Measurement of Superoxide Production and NADPH Oxidase Activity by HPLC Analysis of Dihydroethidium Oxidation. In; 2017; pp. 233–249.
- Hong, Y.-L.; Yeh, S.-L.; Chang, C.-Y.; Hu, M.-L. Total Plasma Malondialdehyde Levels in 16 Taiwanese College Students Determined by Various Thiobarbituric Acid Tests and an Improved High-Performance Liquid Chromatography-Based Method. Clin Biochem 2000, 33, 619–625. [Google Scholar] [CrossRef] [PubMed]
- Gavrieli, Y.; Sherman, Y.; Ben-Sasson, S.A. Identification of Programmed Cell Death in Situ via Specific Labeling of Nuclear DNA Fragmentation. Journal of Cell Biology 1992, 119, 493–501. [Google Scholar] [CrossRef]
- Wijsman, J.H.; Jonker, R.R.; Keijzer, R.; van de Velde, C.J.; Cornelisse, C.J.; van Dierendonck, J.H. A New Method to Detect Apoptosis in Paraffin Sections: In Situ End-Labeling of Fragmented DNA. Journal of Histochemistry & Cytochemistry 1993, 41, 7–12. [Google Scholar] [CrossRef]
- Souza, P.; Rizzardi, F.; Noleto, G.; Atanazio, M.; Bianchi, O.; Parra, E.R.; Teodoro, W.R.; Carrasco, S.; Velosa, A.P.P.; Fernezlian, S.; et al. Refractory Remodeling of the Microenvironment by Abnormal Type V Collagen, Apoptosis, and Immune Response in Non-Small Cell Lung Cancer. Hum Pathol 2010, 41, 239–248. [Google Scholar] [CrossRef]
Figure 1.
Serum levels of transaminases of each group: (a) AST—aspartate aminotransferase; (b) ALT—alanine aminotransferase. The data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; Δ p < 0.05 vs. NUT group.
Figure 1.
Serum levels of transaminases of each group: (a) AST—aspartate aminotransferase; (b) ALT—alanine aminotransferase. The data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; Δ p < 0.05 vs. NUT group.
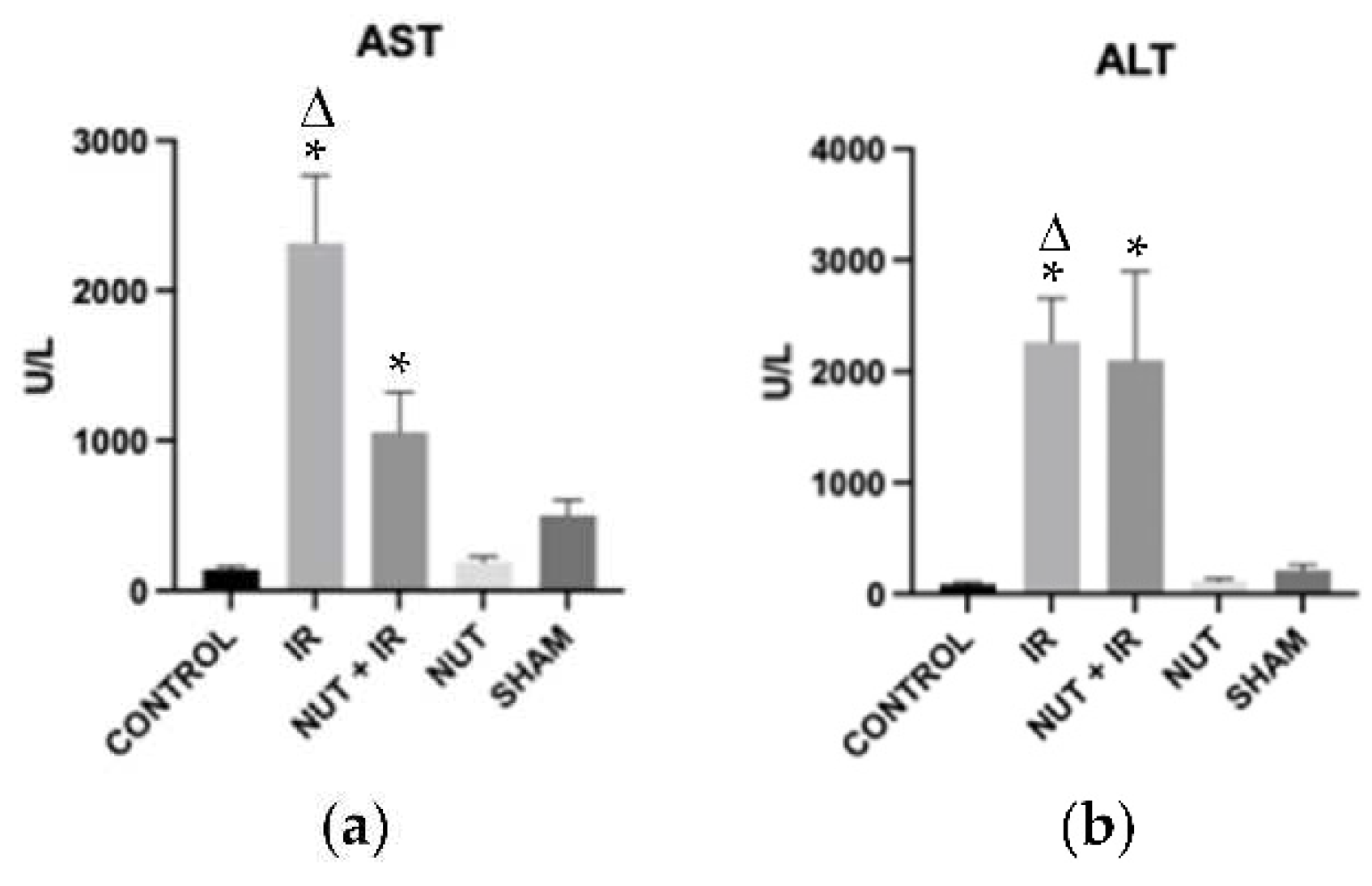
Figure 2.
Inflammatory mediators: (a) IL-1β, (b) IL-6, (c) IL-10, and (d) TNF-α. The data shown are mean ± SEM; * p < 0.05 vs. SHAM group.
Figure 2.
Inflammatory mediators: (a) IL-1β, (b) IL-6, (c) IL-10, and (d) TNF-α. The data shown are mean ± SEM; * p < 0.05 vs. SHAM group.

Figure 3.
MDA in liver tissue of each group. The data shown are mean ± SEM; * p < 0.05 vs. IR group; ● p < 0.05 vs. NUT+IR group; Δ p < 0.05 vs. SHAM group.
Figure 3.
MDA in liver tissue of each group. The data shown are mean ± SEM; * p < 0.05 vs. IR group; ● p < 0.05 vs. NUT+IR group; Δ p < 0.05 vs. SHAM group.

Figure 4.
Gene expression of apoptosis—related genes in all groups: (a) BAX, (b) BCL-2, (c) CASPASE 8, and (d) CASPASE 3 genes. The data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; p < 0.05 vs. NUT + IR group; ● p < 0.05 vs. NUT group; Δ p < 0.05 vs. SHAM group.
Figure 4.
Gene expression of apoptosis—related genes in all groups: (a) BAX, (b) BCL-2, (c) CASPASE 8, and (d) CASPASE 3 genes. The data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; p < 0.05 vs. NUT + IR group; ● p < 0.05 vs. NUT group; Δ p < 0.05 vs. SHAM group.
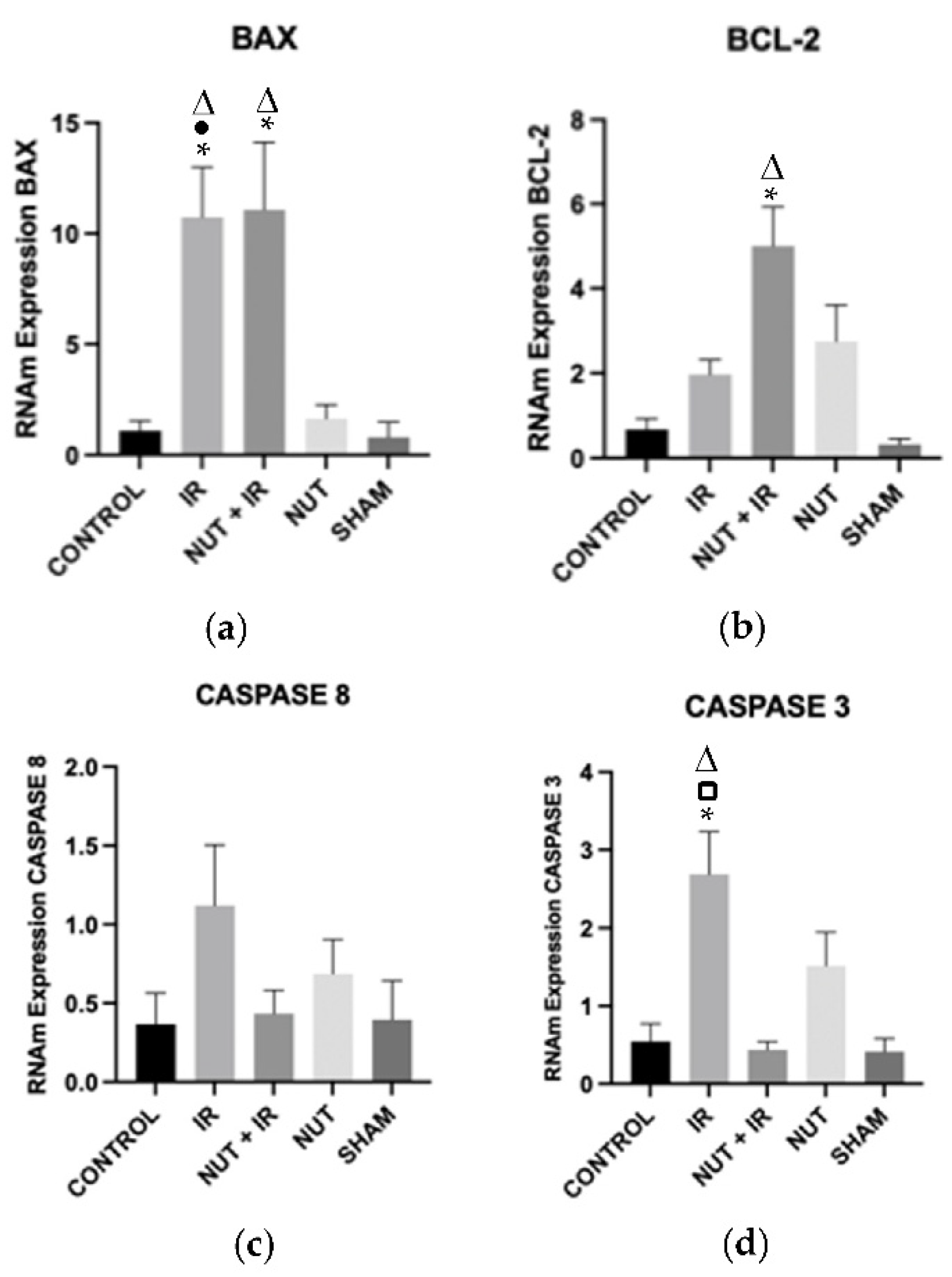
Figure 5.
TUNEL assay of hepatic tissues from the different groups: (a) data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; Δ p < 0.05 vs. NUT + IR group; p < 0.05 vs. NUT group; ● p < 0.05 vs. SHAM group. Arrows and highlighted boxes indicate TUNEL positive cells in each group: (b) CONTROL; (c) IR; (d) NUT + IR; (e) NUT and (f) SHAM. All images were obtained with 50x magnification and highlighted boxes with 400x magnification, with scale bars of 500μm and 50μm, respectively.
Figure 5.
TUNEL assay of hepatic tissues from the different groups: (a) data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; Δ p < 0.05 vs. NUT + IR group; p < 0.05 vs. NUT group; ● p < 0.05 vs. SHAM group. Arrows and highlighted boxes indicate TUNEL positive cells in each group: (b) CONTROL; (c) IR; (d) NUT + IR; (e) NUT and (f) SHAM. All images were obtained with 50x magnification and highlighted boxes with 400x magnification, with scale bars of 500μm and 50μm, respectively.
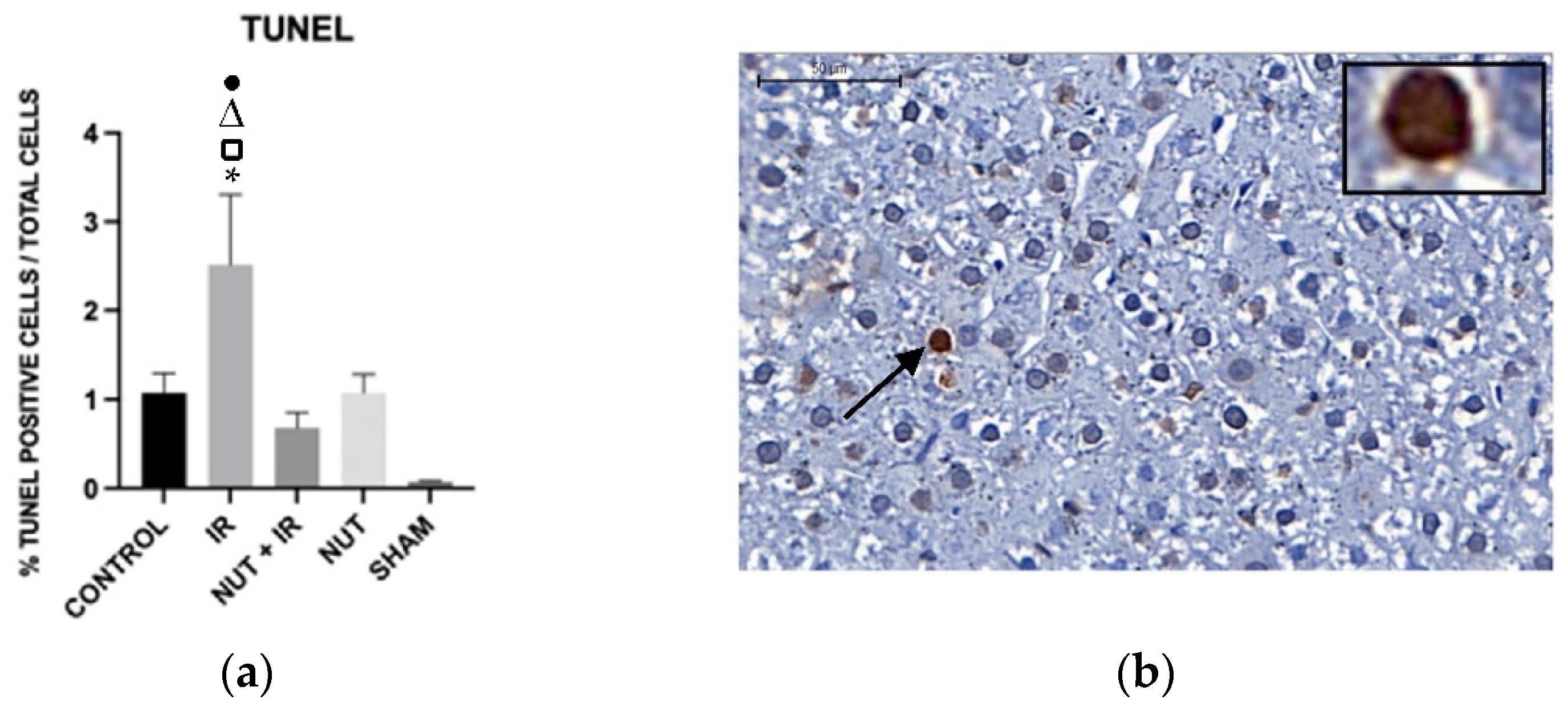

Figure 6.
Immunohistochemistry. Cleaved caspase 3 protein in liver tissue from the different groups: (a) data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; p < 0.05 vs. NUT + IR group; Δ p < 0.05 vs. SHAM group. Arrows and highlighted boxes indicate CLEAVED CASPASE 3 positive cells in each group: (b) CONTROL; (c) IR; (d) NUT + IR; (e) NUT and (f) SHAM. All images were obtained with 50x magnification and highlighted boxes with 400x magnification, with scale bars of 500μm and 50μm, respectively.
Figure 6.
Immunohistochemistry. Cleaved caspase 3 protein in liver tissue from the different groups: (a) data shown are mean ± SEM; * p < 0.05 vs. CONTROL group; p < 0.05 vs. NUT + IR group; Δ p < 0.05 vs. SHAM group. Arrows and highlighted boxes indicate CLEAVED CASPASE 3 positive cells in each group: (b) CONTROL; (c) IR; (d) NUT + IR; (e) NUT and (f) SHAM. All images were obtained with 50x magnification and highlighted boxes with 400x magnification, with scale bars of 500μm and 50μm, respectively.
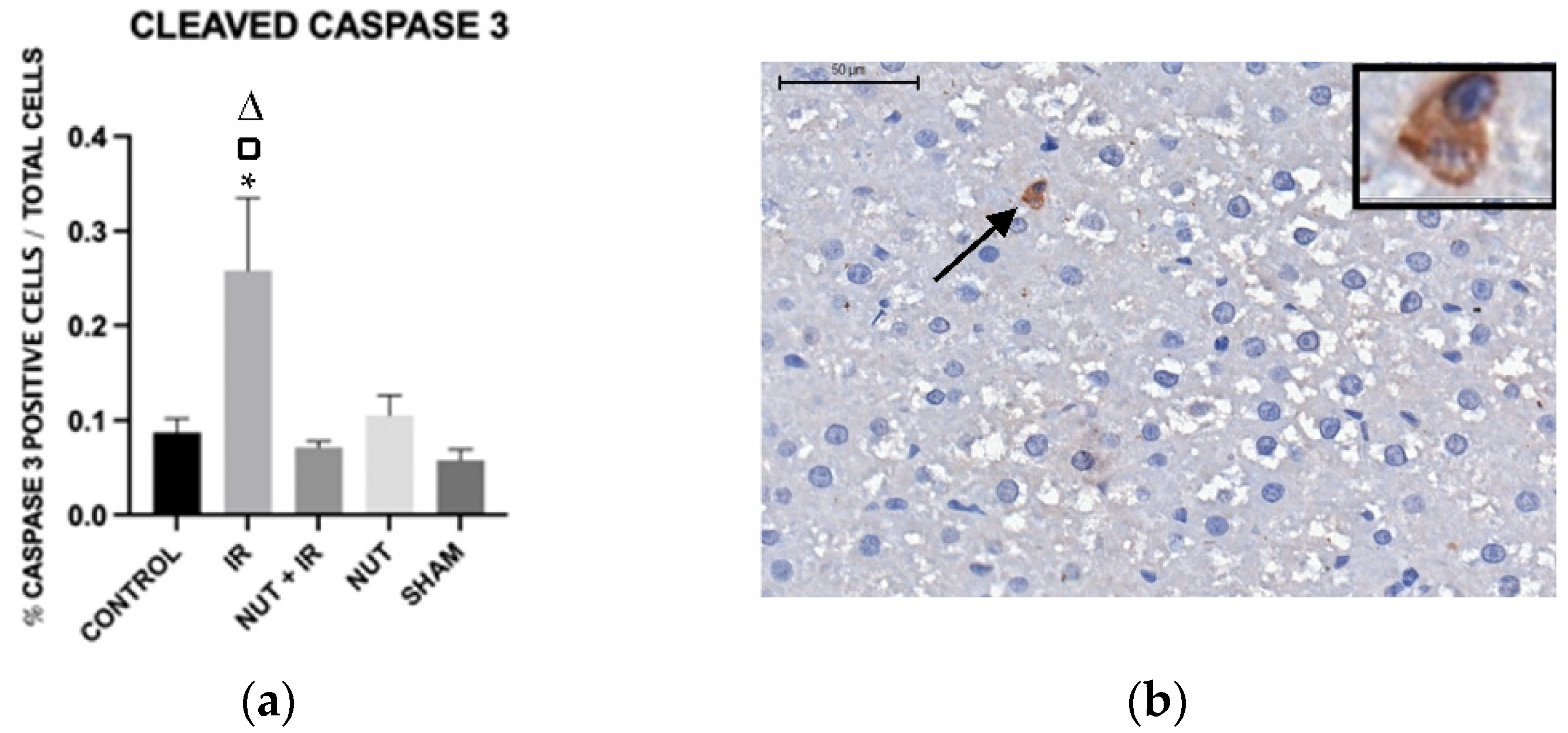
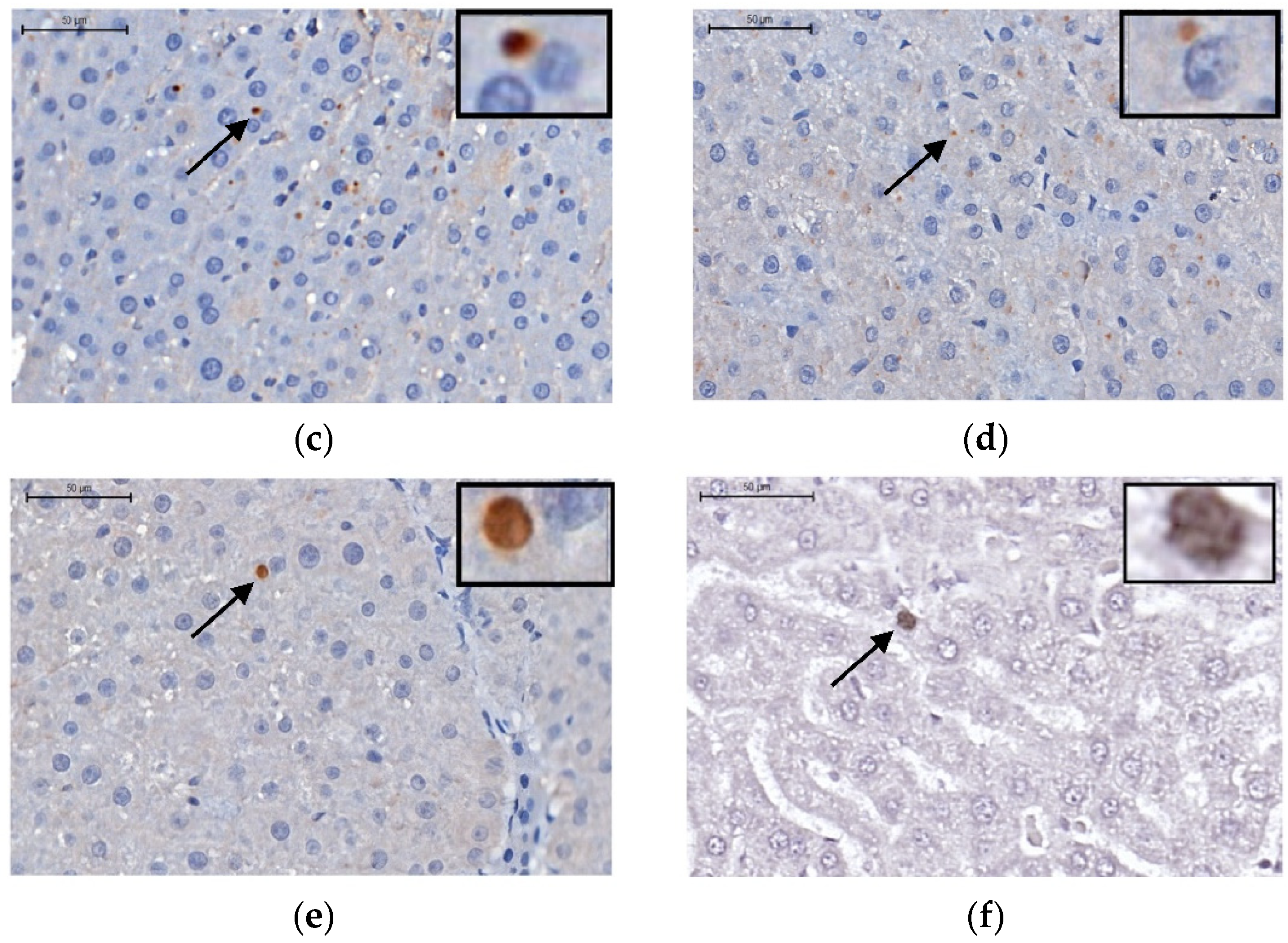
Figure 7.
Immunohistochemistry. TNF-α protein in liver tissue from different groups: (a) data shown are mean ± SEM; * p < 0.05 vs. IR group; Δ p < 0.05 vs. NUT group; ● p < 0.05 vs. CONTROL group. □ p <0.05 vs. SHAM group. Arrows and highlighted boxes indicate TNF-α positive cells in each group: (b) CONTROL; (c) IR; (d) NUT + IR; (e) NUT; and (f) SHAM. All images were obtained with 50x magnification and highlighted boxes with 400x magnification, with scale bars of 500μm and 50μm, respectively.
Figure 7.
Immunohistochemistry. TNF-α protein in liver tissue from different groups: (a) data shown are mean ± SEM; * p < 0.05 vs. IR group; Δ p < 0.05 vs. NUT group; ● p < 0.05 vs. CONTROL group. □ p <0.05 vs. SHAM group. Arrows and highlighted boxes indicate TNF-α positive cells in each group: (b) CONTROL; (c) IR; (d) NUT + IR; (e) NUT; and (f) SHAM. All images were obtained with 50x magnification and highlighted boxes with 400x magnification, with scale bars of 500μm and 50μm, respectively.
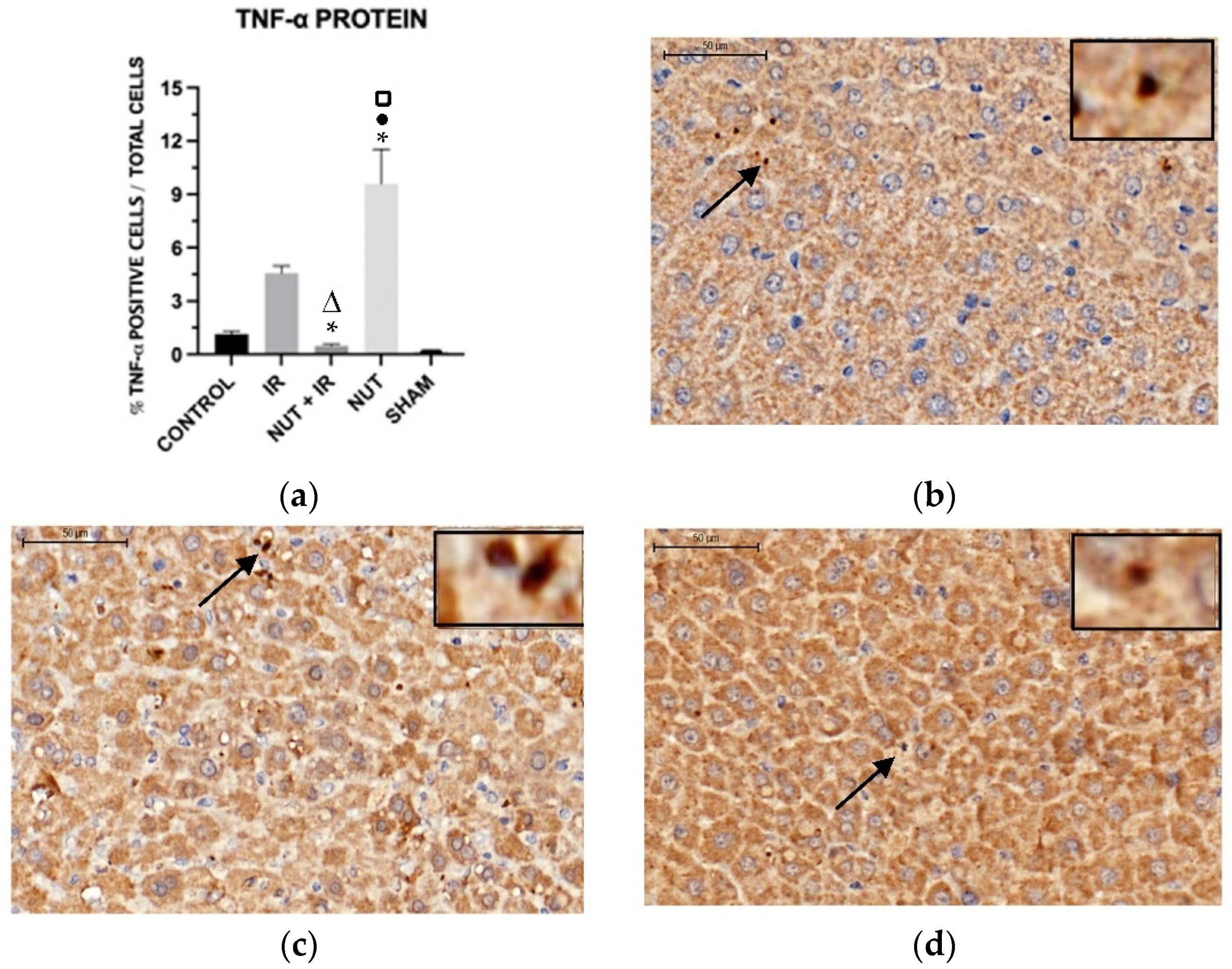
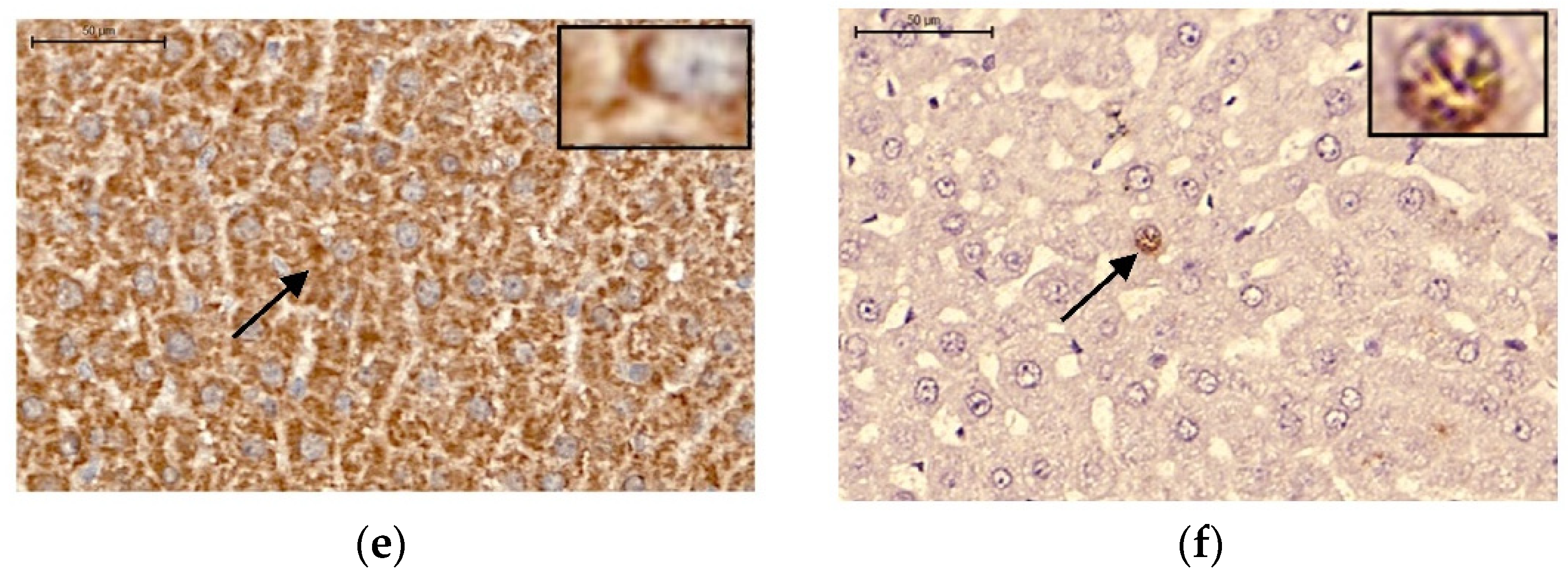
Figure 8.
Histological and immunohistochemistry analysis: (a) total liver histology score from different groups; * p < 0.05 vs. IR group. (b) HE (Hematoxylin–eosin—600X): photomicrograph of hepatic parenchyma showing ischemic changes (ballooning, apoptosis, destrabeculation, and sinusoid congestion). (c) Caspase 3 (Immunohistochemistry—600X): photomicrograph of hepatic parenchyma showing positivity in cytoplasm (intracytoplasmic brown granular pattern).
Figure 8.
Histological and immunohistochemistry analysis: (a) total liver histology score from different groups; * p < 0.05 vs. IR group. (b) HE (Hematoxylin–eosin—600X): photomicrograph of hepatic parenchyma showing ischemic changes (ballooning, apoptosis, destrabeculation, and sinusoid congestion). (c) Caspase 3 (Immunohistochemistry—600X): photomicrograph of hepatic parenchyma showing positivity in cytoplasm (intracytoplasmic brown granular pattern).
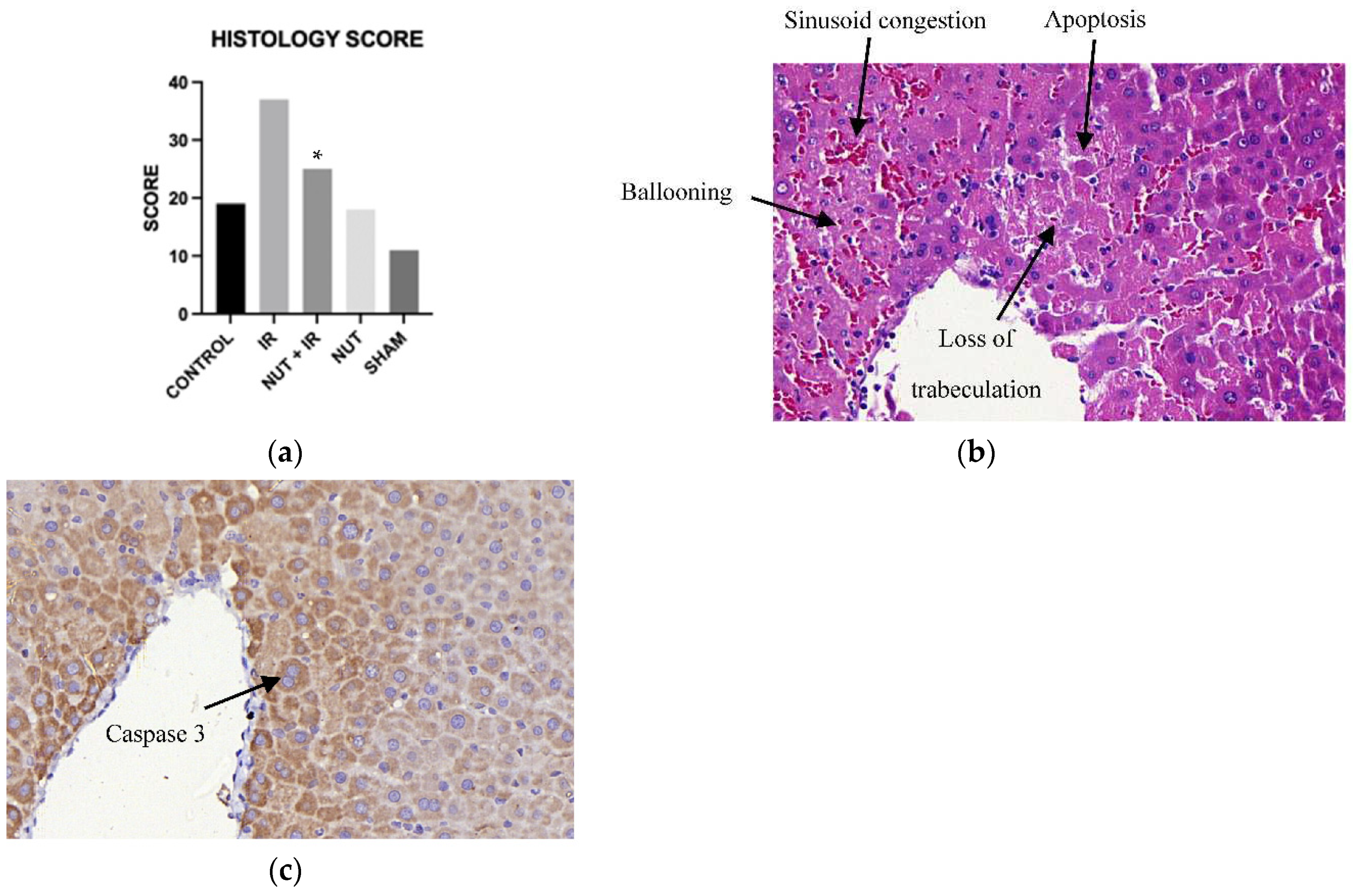

Table 1.
Amount of each nutraceutical.
| Nutraceuticals | mg/kg | mg/ml | Amount (g) in 100 ml |
|---|---|---|---|
| Resveratrol | 2,96 | 0,74 | 0,074 |
| Quercetin | 3,56 | 0,89 | 0,0908 |
| Chelated selenium | 1,76 | 0,44 | 2,6831 |
| Omega-3 | 2,0 | 0,50 | 0,05 |
| Ginger extract | 3,24 | 0,81 | 0,081 |
| Avocado powder | 5,08 | 1,27 | 0,127 |
| Leucine | 4,44 | 1,11 | 0,111 |
| Nicotinamide | 20,0 | 5,0 | 0,5 |
Table 2.
Immunohistochemical markers.
| Antibody | Concentration | Brand | Code | Clone |
|---|---|---|---|---|
| Caspase 3 | 1:200 | Novocastra | NCL-CPP32 | - |
| TNF-α | 1:200 | Santa Cruz | sc-1348 | - |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



