
Submitted:
03 May 2023
Posted:
08 May 2023
You are already at the latest version
Abstract
The detection of subtle changes in the pituitary dimensions has relevant implications since this gland is crucial for the endocrine system. In cats, few studies established the cut-offs values of the pituitary gland’s dimensions, but using small and inhomogeneous samples. The aims of this study were: to determine by computed tomography (CT) the pituitary linear dimensions and the pituitary-to-brain (P:B) ratio in a sample of domestic short-haired (DSH) cats; to assess the effects of sex, age and weight on pituitary dimensions; to evaluate the inter- and intra-observer agreement for such measurements. Exclusion criteria were: clinical, laboratory or CT alterations of pituitary gland or brain diseases, fractures of the neurocranium, or diabetes mellitus. Pituitary dimensions and brain area were assessed by two different observers using multiplanar reconstructions and automated segmentation tools. Fifty-one cats were included in the final sample. The intraclass correlation coefficient for intra- and inter-observer reliability showed good/excellent and moderate/good reliability, respectively. No differences between sexes were detected, and negligible correlations were found with age and weight. Findings from the current study provided normal reference values for pituitary height (1.88 – 4.01 mm) and P:B ratio (0.25 – 0.49), useful for assessing abnormally enlarged pituitary gland in DSH cats.
Keywords:
acromegaly
; adenoma
; diabetes
; feline
; hypophysis
; microadenoma
1. Introduction
The pituitary gland plays a pivotal role in regulating the endocrine system through the production, storage, and release of various hormones [1]. Pituitary tumors can originate from different cell lineages and can be either functional or non-functional [2,3,4,5,6]. The clinical signs associated with the neoplasm depend on the secretory proprieties but also on the tumor’s size [2,4,6,7,8,9]. Indeed, also non-functional tumors can become clinically relevant when they enlarge enough to cause neurologic signs by direct compression of other intracranial structures [3,4,5,6,10]. Furthermore, pituitary tumors can be incidental findings when skull imaging is performed for unrelated reasons (so-called incidentalomas) [8]. In humans, according to 2017 WHO “classification of tumors of the pituitary gland”, pituitary neoplasms can be classified as adenomas or carcinomas. The latter are defined only by demonstrating metastatic spread [5]. This classification mainly focuses on immunohistochemical classification according to the hormone that the tumor expresses and so can be further subdivided into melanotroph, corticotroph, thyrotroph, lactotroph, somatotroph or gonadotroph. In dogs, corticotroph (ACTH-secreting) adenomas and adenocarcinomas responsible for pituitary-dependent hyperadrenocorticism prevail, while in cats, somatotroph (growth hormone – GH – secreting) tumors are the most reported [6]. In the latter case, the excessive secretion of GH can result in chronic hypersomatotropism that can cause acromegaly and insulin resistance, due to the concomitant increase of insulin-like growth factor-1 (IGF-1). Of note, cats affected by somatotroph pituitary tumors are often brought to consultation for clinical signs related to poorly controlled diabetes, such as polyuria, polydipsia and polyphagia, rather than somatic changes due to acromegaly [10,11,12]. Somatotroph adenoma is the most reported pituitary tumor in middle-aged to older male cats. Domestic short-haired (DSH) cats and Maine Coons seem predisposed [10,11,12].
The detection of anatomical alterations of the pituitary gland is usually performed using Magnetic Resonance Imaging (MRI) or Computed Tomography (CT) [7]. These imaging techniques are paramount for diagnosis and for surgical planning or radiotherapy [8]. In many cases, the diagnosis of pituitary macroadenoma is straightforward since the pituitary mass dorsally protrudes from the sella turcica and compresses the adjacent brain parenchyma, sometimes with associated neurological signs [7,8,9]. Differently, in the case of microadenomas, there are often only subtle changes in pituitary size and contours that may not be visible [9,12]. In order to increase diagnostic accuracy in the detection of pituitary microadenomas, the pituitary gland was also evaluated using CT dynamic scans, since pituitary tumors can alter the normal network of pituitary vessels and, consequently, the enhancement pattern [13].
Few studies tried to establish the linear dimensions of the pituitary gland (height, width, and length) in cats using either MRI [14] or CT [13,15,16]. In order to address variation in pituitary gland size between dogs and cats of different sizes and breeds, the pituitary height-to-brain ratio (P:B ratio) was introduced [15,16,17]. However, those studies performed in cats used third-generation CT devices [15] or thick MRI slices [14] and included small and inhomogeneous samples. More recently, a study aimed to evaluate possible differences in pituitary size between mesaticephalic and brachycephalic cats found a significant difference between the two skull morphotypes [16]. These results highlight the need to obtain reference measures of the pituitary gland according to morphotype or, even better, according to the breed. To date, a single study, including only DSH cats, described the pituitary dimensions and P:B ratio [15]. However, in our clinical experience, cats without hematological, clinical and CT findings of pituitary disease had pituitary dimensions outside the previously proposed cut-off values. Consequently, we hypothesized that the reference intervals for pituitary linear dimensions (height, length, and width) and the P:B ratio in DSH cats would be different than previously reported.
Therefore, the primary aim of the present study was to verify if the previously reported cut-off values for pituitary linear dimension and P:B ratio were respected in a larger sample of DSH cats and eventually, establish new reference values. Secondary objectives were to evaluate the influence of age, body weight and sex on pituitary dimensions and P:B ratio. Finally, we evaluated the intra- and inter-observer agreement among two observers with different levels of expertise.
2. Materials and Methods
2.1. Selection and description of subjects
This single-center, retrospective, reference interval, intra- and inter-observer agreement study was approved by the Ethical Animal Care and Use Committee of the University of Napoli “Federico II” (Prot. N. PG/2023/0050567). The electronic clinical records and CT studies of cats referred to the Interdepartmental Centre of Veterinary Radiology of the University of Napoli Federico II in the set study period between September 2018 and October 2022 were retrieved from the picture archiving and communication system (dcm4chee-arc-light version 5.11.1, http://www.dcm4che.org) [18]. The inclusion criteria were: DSH breed, same CT unit and scanning protocol. Patients were excluded from the study if they had clinical, laboratory, or CT final report referring any alteration related to a) pituitary gland disease, b) neurologic signs different from vestibular symptoms, c) intracranial lesion detected on CT, d) fractures or conformational alterations of the neurocranium, e) polyuria or polydipsia, f) signs of acromegaly, d) definitive diagnosis of diabetes mellitus.
2.2. CT scan protocol
All patients were positioned in sternal recumbency within a radiolucent polyurethane vacuum immobilization mattress (Vacuumat, Génia, St. Hilaire de Chaléons, France) and with the forelimbs pulled caudally along the thorax, under general anesthesia (the anesthetic protocol adopted varied depending on the decision of the anesthesiologist in charge). Computed tomography studies were obtained using a 16-slices multi-detector computed tomography (MDCT) unit (BrightSpeed, General Electric Healthcare, Milwaukee, WI, USA). The acquisition protocol was: helical mode; slice thickness 1.25 mm; pitch 0.9375:1; 120 kVp, 160-200 mA, 1-second tube rotation speed; soft tissue and bone reconstruction algorithms (General Electric proprietary “standard” and “bone” filters). All the patients received a standardized intravenous dose (740 mgI/kg, i.e., 2 ml/kg) of contrast media (Iopamidol, Iopamiro 370 mgI/ml, Bracco Imaging s.p.a., Milano, Italy) using an infusion rate of 1 ml/s followed by a 5 ml saline flush through a double-barrel power injector (EmpowerCTA+, Bracco Imaging s.p.a., Milano, Italy); post-contrast images were acquired after a fixed delay of 60 seconds.
2.3. Data recording and image analysis
A preliminary evaluation was performed by a Veterinary radiologist (L.M., full professor of Veterinary Radiology with a Ph.D. and >25 years of experience) to include or exclude each cat from the definitive sample group. The CT studies were excluded if: a) the postcontrast series of the skull acquired with soft tissue reconstruction algorithm was not available, b) the images quality was inadequate for a correct interpretation, c) the presence of beam hardening artifacts was detected, preventing a correct evaluation of the pituitary gland. The same author anonymized all the CT studies before submitting them to two observers who reviewed the images using a commercial DICOM viewer software (Philips Extended Brilliance Workspace v. 4.5.5, Philips Medical System Nederland B.V., Best, The Netherlands). Observer 1 (D.C., a third-year Ph.D. student in Veterinary Diagnostic Imaging) and observer 2 (P.C, a veterinarian with two years of expertise in CT imaging) were blinded regarding the clinical data and reasons for CT examination. All the measurements were performed once by each observer, independently and blinded to the results reported by the other observer. A pituitary gland measurement method was established prior to the analysis by two authors (D.C. and L.M) and recorded on a portable document file. Pituitary linear dimensions (height, length, width) expressed in millimeters (mm) were measured using electronic calipers on post-contrast images displayed using a standardized window [window width (WW): 450, window level (WL): 200], although WW and WL could be manually adjusted by the observers if deemed necessary. Measurements were made on multiplanar reconstructions (MPR) images in order to obtain the best visualization of the pituitary gland and avoid interpreting the dorsum sellae as a pituitary mass [9]. The pituitary height (PH) was measured at the level of the pituitary fossa, perpendicular to the basisphenoid bone, where the maximal pituitary height was visible, both on the transverse plane (PHT) (Figure 1A) and on the sagittal plane (PHS) (Figure 1B). The pituitary length (PL) was measured on the sagittal plane where the maximal length was visible, parallel to the basisphenoid bone (Figure 1B). The pituitary width (PW) was determined on the transverse plane at the point of maximal width of the gland (Figure 1C). The brain area (BA) expressed in mm2 was measured on the same slice of the PHT using an automated segmentation tool (Figure 1D). When deemed necessary, the observer used the bone reconstruction algorithms with associated high contrast window (WW = 2000, WL = 800) to better delineate the brain edges. All the data were reported in an electronic spreadsheet (Microsoft Excel version 16.52 2021, Microsoft Corp. Redmond, WA, USA) and the P:B ratio was automatically computed for each cat as follow: P:B ratio = [PHT(mm)×100/BA(mm2)] [17]. To assess the intra-observer agreement, the measurements were repeated independently by the two observers two months after the first evaluation on a smaller sample of thirty re-anonymized and re-randomly selected CT exams. The sex, neutering status, weight (in kilograms), and age (in months) were recorded for each cat included in the final sample group.
2.4. Statistical analysis
Statistical analyses were performed by one of the authors (L.A., former researcher with a Ph.D. and >10 years of experience and training in statistics) using commercial software (JMP Pro, v. 16.0, SAS Institute, Cary, NC, USA; MedCalc version 19.2.6, MedCalc Software Ltd, Ostend, Belgium; IBM SPSS, v. 26.0, IBM, Armonk, NY, USA). The normality of data was assessed with the Shapiro-Wilk’s W test. Continuous data were reported as mean ± standard deviation (SD) or median (range) depending on the distribution.
The reference range for each measurement was calculated according to the American Society for Veterinary Clinical Pathology (ASCVP) guidelines for reference intervals [19]. Briefly, outliers were automatically identified according to Reed et al. [20]. Then, data distribution was tested automatically with the Shapiro-Wilk’s W test. Reference lower and upper limits, and the corresponding 90% confidence intervals (CIs) were then calculated employing the robust method following Clinical Laboratory and Standards Institute (CLSI) recommendations (CLSI C28-A3), with bootstrapping (1000 iterations) [21]. A Bland-Altman plot was used to explore the differences between PHS and PHT. The bias and 95% limits of agreement were calculated. Correlations between the measurements and body weight were tested with Pearson’s correlation coefficient (r), whereas those between the measurements and age using Spearman’s rank correlation coefficient (rs). Finally, differences between males and females were tested with a pooled Student’s t-test, with Welch’s correction since variances resulted significantly different at the F test (PL, PW, BA, and P:B ratio), or a Mann-Whitney’s U test (PHT and PHS), according to within sex distribution and non-considering the neutering status. No partitioning into subclasses based on age, body weight or sex was applied in the reference range calculations due to the lack of correlation with the measurements.
For inter-observer reliability, measurements belonging to all the patients were included in the analysis, while for the intra-observer reliability, only the measurements of the smaller sample were considered. For both inter- and intra-observer agreement, a two-way mixed effects intraclass correlation coefficient (ICC) for single measurement or single observer accordingly, and absolute agreement was calculated; the relative 95% CI were calculated, as well. The ICC was categorized according to Koo and Li. [22]. Based on the reliability analysis results, all intra- and inter-observer measurements with an ICC > 0.80 were averaged and subsequently analyzed. For measurements that did not reach this value, the first measurements of observer 1, considered the most experienced, were used. In all analyses, p < .05 was considered statistically significant.
3. Results
A total of 59 CT studies performed in the set period met the inclusion criteria. After the preliminary review, eight cases were excluded for the following reasons: brain neoplasia (n = 4), deformed cranium (n = 2), and lack of post-contrast images (n = 2). Fifty-one DSH cats were included in the final sample; they were 4 intact females (8%), 26 (51%) spayed females, 7 (14%) intact males, and 14 (27%) castrated males. The median age was 72 months (range 2 – 180), and the weight 4.6 ± 1.5 kg.
In all the cats included in the final sample, the pituitary gland was distinguishable from the adjacent structures with a good contrast enhancement and all the predetermined measurements were obtained. In three cases it was challenging to identify the pituitary edges with absolute precision due to the pituitary gland's small size. The automated segmentation tool allowed for a rapid delimitation of the BA in all cases.
All the measurements described resulted normally distributed, and no outliers were detected in any of them. The reference intervals, mean ± SD and range (minimum to maximum) for linear measurements and P:B ratio are reported in Table 1.
Regarding the pituitary height, the mean (±SD) PHT was 2.94 ± 0.52 mm and the PHS 2.95 ± 0.55 mm, and the Bland-Altman evaluation resulted in a bias of -0.01 and limits of agreement of -0.79 – 0.76 (Figure 2).
All measurements showed negligible to low correlation with body weight, whereas only PHS and PL showed a low correlation with age. Correlation coefficients and relative p-values are summarized in Table 2. No differences between sexes were detected for any measurement (PHT, p = 0.40; PHS, p = 0.68; PL, p = 0.31; PW, p = 0.21; BA, p = 0.30; P:B ratio, p = 0.94).
Abbreviations: CI, confidence interval; BA, brain area; P:B ratio, pituitary gland height to brain area ratio; PHS, maximal pituitary height on the sagittal plane; PHT, maximal pituitary height on the transverse plane; PL: pituitary length; PW: pituitary width; r: Pearson’s correlation coefficient; rs: Spearman’s rank correlation coefficient.
Results for inter-observer agreement are summarized in Table 3. All measurements were within the moderate reliability class, but the BA for which good reliability was detected.
Results for the intra-observer agreement are summarized in Table 4. Reliability was good for all measurements from observer 1, but for PL that resulted moderate; on the other hand, reliability resulted moderate for all measurements from observer 2, but for BA that resulted excellent.
4. Discussion
The primary aim of the present study was to verify if the previously reported cut-off values for pituitary linear dimension and P:B ratio were respected in a larger sample of DSH cats and eventually, establish new reference values. The obtained values partly differ from those already reported in the literature [13,14,15,16]. This discrepancy might be related to differences in sample sizes. Effectively, to obtain reliable reference values, a sample size of 120 healthy patients should be collected [19,20,23]; nonetheless, robust statistical methods have been developed for sample sizes less than 120 and more than 40, such as that used in our work, which allow the calculation of the reference limits and 90% CI [19]. In this study the reference values for the pituitary linear dimensions and P:B ratio were found according to the guidelines of the ASCVP [19]. Calculation of the reference limits and 90% CI for sample sizes less than 40 have been discouraged [19,23].
Another possible cause of discrepancy between reported values and those from the current study, may be the use of different imaging techniques (CT vs. MRI), different CT devices or scan protocols. It is well known that MRI has a higher soft tissues contrast compared to CT, that might give more accurate and reproducible results [7,24]. On the other hand, older MRI devices might not have enough field strength, or precise electronic calipers in the range of millemeters [11]. Differences between CT devices, scan protocols [25,26], or even contrast dosage and infusion rate [27], can all affect images quality and, consequently, correctness, reproducibility and accuracy of the measurements. In the current study, all the CT studies were performed using a MDCT unit providing high spatial resolution and real isotropic reconstructions [26]. These technical aspects gave true MPRs and allowed precise assessment of the pituitary gland [28].
Moreover, we selected only DSH cats, reducing an eventual inter-breeds variability. A significant difference in pituitary gland linear measures between brachycephalic and mesaticephalic cats has already been demonstrated [16], therefore, it is reasonable hypothesize that other factors, e.g. the breed, might have some influence on those measures. Larger samples of cats stratified by breed might confirm this hypothesis.
In other studies [11,14], both PHT and PHS have been reported, whereas Nadimi et al., reported only the PHT [15]. In the current study, the Bland-Altman plot showed minimal bias (- 0.01) between PHT and PHS. This finding represents an indirect validation of the accuracy of the measurements reported, further confirmed by the differences in all the reported statistics (mean, SD, range, reference interval and 90% CI) that deviate from each other in the order of 0.1 mm. Therefore, according to us, both the transversal and the sagittal scans can be used interchangeably to determine the pituitary height.
Partitioning, i.e. the stratification into sub-groups, is an important step during reference range evaluation [19], as well as in other cohort studies [29]. Sub-groups might be planned in advance based on expected physiological differences, e.g. due to sex and age, or might be identified during data analysis. In the latter case, a strong statistical result should justify the stratification [29].
One of the secondary objectives of this work was to evaluate the influence of age, body weight and sex on the pituitary measurements, also to evaluate if any sub-group had to be generated. All the linear measurements had negligible/low correlation with body weight, and only PHS and PL had a low correlation with age. In a previous study, performed on fifteen cats [15], ten of which were DSH, the authors found a significant correlation between pituitary dimensions and body weight; however, the degree of this correlation was not reported. Additionally, considering only the DSH cats, the authors reported a significant difference between those weighing < 3 kg and those above that body weight [15]. In our study, although body weight was positively correlated with all pituitary dimensions, the degree of correlation was negligible/low, in partial agreement with other studies [14,16]. Therefore, we did not consider it worth of creating subgroups based on body weight. Further studies, with larger sample sizes should explore this association. Nonetheless, in the authors’ opinion, the body weight per se might not be the best variable to be explored. Perharps, other body metrics, e.g. the body surface, body condition score, etc., could act as a better predictor of differences in pituitary gland dimensions. However, the P:B ratio might eliminate any influence of body weight and dimensions.
In humans it is well-known the progressive growth of the pituitary gland during puberty [30,31] and the small size of the pituitary gland in elderly people [32]. In cats, Häußler et al. [16] found a positive correlation between age and pituitary height, width and length in the sub-group of brachycephalic cats, but 25% of them was less than 15 months, whereas this correlation was not explored in the mesaticephalic group. In our sample, 11 cats (21%) were less than 15 months old, but we detected only a low correlation of PHS and PL with age. Consequently, no conclusions can be drawn about the different results reported. Further studies should be designed to explore whether in the feline species a pattern of pituitary growth and late reduction in size, similar to that of human beings, exists.
Finally, no correlation was found between gender and pituitary dimensions. This finding agrees with a previous study [15], but partially disagrees with the study from Häußler et al. [16] where male cats had significantly larger pituitary width compared to female. However, the authors did not show the correlation coefficient, and significance was reached only in the mesaticephalic sub-group. In our study, the high number of neutered females and castrated males, which compose more than two third of the whole sample (78%), might have introduced a bias, even if the neutering status has been reported to have no influence on the pituitary dimensions [13]. Again, further studies with homogeneous gender larger groups are needed to clarify the influence of gender and neutering on the pituitary gland dimensions.
The other secondary objective was the evaluation of the intra- and inter-observer agreement. Results of the ICC for the intra-observer agreement suggest that it was influenced mainly by the experience of the operator. Indeed, the observer 1, considered the most experienced, showed good reliability and, except for PL and BA, displayed higher ICC values compared to observer 2. The ICC for inter-observer agreement revealed a moderate/good agreement between observers. In a previous study, assessing the intra- and interobserver agreement accuracy and reproducibility of CT measurements of the pituitary gland in dogs on a phantom model, the authors found an excellent level of agreement for PH and P:B ratio between the observers [33]. However, a systematic and significant difference was present between them. The authors concluded that due to this systematic variation, intra- and inter-patient comparisons have to be performed preferably by the same observer [33]. In another study, Van Hoe et al. suggested a fundamental role of image windowing in the manual measurement of small parts [34]. Accordingly, in the current study, notwithstanding the suggested pre-defined windowing, the moderate agreement between observers may rely on the operator's experience and ability in setting the window level and width, when it was considered necessary to better measure the pituitary gland. The ICC results for BA indirectly supports this hypothesis. Indeed, the BA was the measurement with the higher level of agreement between observers and this is probably related to the automated segmentation tool used, thus eliminating the operator dependence.
The main limitation of this study is the absence of IGF-1 assay in cats included in the final sample. Consequently, it is impossible to exclude categorically acromegaly. However, none of the subjects had clinical, CT or laboratory findings consistent with acromegaly or diabetes mellitus. Given the small number of laboratories that perform this analysis and the relatively high cost, the assay for IGF-1 is not performed as part of the routine serum analysis panel at our institution, as it is reserved for cats with clinical suspicion of acromegaly. Another limitation is the absence of necropsy and, therefore, the possibility of ruling out pituitary lesions and also to verify the agreement between the actual ex vivo dimensions of the pituitary gland and those obtained on CT images.
5. Conclusions
This study provides reference values for pituitary dimensions and P:B ratio in DSH cats. The reference values are wider than the mean values previously reported. Pituitary linear dimensions and P:B ratio exhibit a good intra-operator agreement, but a moderate inter-operator agreement, likely due to the different expertise. Software that automatically defines the structures of interest may help to reduce this operator-dependent variability. In the sample analyzed, significant but negligible to low correlations were found between body weight and pituitary size and between age and pituitary height and length. Hence, the actual effect of these variables on the pituitary gland remains questionable. In addition, no differences between genders were found.
According to this study, a pituitary gland height > 4 mm or a P:B ratio > 0.49 mm should be considered enlarged. The reference ranges obtained from this study may help assess pituitary gland size in DSH cats with suspected neoplastic lesions affecting the pituitary gland, in surgical or radiation therapy planning, and in monitoring response to treatment.
Author Contributions
Conceptualization, D.C. and L.M.; methodology, D.C., P.C., L.A. and L.M.; validation, D.C., L.M., L.A., L.M. and A.G.; formal analysis, D.C., P.C., L.M., L.A. and A.G; investigation, D.C., P.C., L.N. and E.C.; resources, D.C., P.C., L.M., E.C. and L.N.; data curation, D.C., L.A., P.C and L.M.; writing—original draft preparation, D.C., L.A. and L.M.; writing—review and editing, D.C., L.A., L.M., P.C., E.C and A.G.; visualization, D.C., P.C., E.C., L.N. and L.M.; supervision, D.C., L.M., E.C., L.N. and A.G.; project administration, D.C., A.G. and L.M.All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The animal study protocol was approved by Clinical Ethical Review Board of the University of Napoli “Federico II” (Prot. N. PG/2023/0050567).
Informed Consent Statement
Written informed consent has been obtained from the patients’ owner.
Data Availability Statement
The data supporting the findings of this study are available from the corresponding author, upon reasonable request.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Davis, S.W.; Ellsworth, B.S.; Peréz Millan, M.I.; Gergics, P.; Schade, V.; Foyouzi, N.; Brinkmeier, M.L.; Mortensen, A.H.; Camper, S.A. Pituitary gland development and disease: from stem cell to hormone production. Curr Top Dev Biol 2013, 106, 1–47. [Google Scholar] [CrossRef] [PubMed]
- Rosol, T.J.; Meuten, D.J. Tumors of the Endocrine Glands. In Tumors in Domestic Animals; 2016; pp. 766-833. [CrossRef]
- Polledo, L.; Grinwis, G.C.M.; Graham, P.; Dunning, M.; Baiker, K. Pathological Findings in the Pituitary Glands of Dogs and Cats. Vet Pathol 2018, 55, 880–888. [Google Scholar] [CrossRef] [PubMed]
- Lunn, K.F.; Boston, S.E. 26 - Tumors of the Endocrine System. In Withrow and MacEwen's Small Animal Clinical Oncology (Sixth Edition), Vail, D.M., Thamm, D.H., Liptak, J.M., Eds.; W.B. Saunders: St. Louis (MO), 2020; pp. 565–596. [Google Scholar]
- Lopes, M.B.S. The 2017 World Health Organization classification of tumors of the pituitary gland: a summary. Acta Neuropathologica 2017, 134, 521–535. [Google Scholar] [CrossRef] [PubMed]
- Sanders, K.; Galac, S.; Meij, B.P. Pituitary tumour types in dogs and cats. Vet J 2021, 270, 105623. [Google Scholar] [CrossRef] [PubMed]
- Holmes, S.P. Imaging the Feline Neurologic System. In Feline Diagnostic Imaging; 2020; pp. 77-111.
- Owen, T.J.; Martin, L.G.; Chen, A.V. Transsphenoidal Surgery for Pituitary Tumors and Other Sellar Masses. Veterinary Clinics of North America: Small Animal Practice 2018, 48, 129–151. [Google Scholar] [CrossRef]
- Hecht, S.; Schwarz, T. Pituitary Gland. In Veterinary Computed Tomography; 2011; pp. 197-203. [CrossRef]
- Gunn-Moore, D. Feline endocrinopathies. Veterinary Clinics of North America: Small Animal Practice 2005, 35, 171–210. [Google Scholar] [CrossRef]
- Reusch, C.E. Chapter 2 - Disorders of Growth Hormone. In Canine and Feline Endocrinology (Fourth Edition), Feldman, E.C., Nelson, R.W., Reusch, C.E., Scott-Moncrieff, J.C.R., Eds.; W.B. Saunders: St. Louis, 2015; pp. 37–76. [Google Scholar]
- Niessen, S.J.M.; Forcada, Y.; Mantis, P.; Lamb, C.R.; Harrington, N.; Fowkes, R.; Korbonits, M.; Smith, K.; Church, D.B. Studying Cat (Felis catus) Diabetes: Beware of the Acromegalic Imposter. PLOS ONE 2015, 10, e0127794. [Google Scholar] [CrossRef]
- Tyson, R.; Graham, J.P.; Bermingham, E.; Randall, S.; Berry, C.R. Dynamic computed tomography of the normal feline hypophysis cerebri (Glandula pituitaria). Vet Radiol Ultrasound 2005, 46, 33–38. [Google Scholar] [CrossRef]
- Wallack, S.T.; Wisner, E.R.; Feldman, E.C. Mensuration of the pituitary gland from magnetic resonance images in 17 cats. Vet Radiol Ultrasound 2003, 44, 278–282. [Google Scholar] [CrossRef]
- Nadimi, S.; Molazem, M.; Jarolmasjed, S.; Esmaili Nejad, M.R. Volumetric evaluation of pituitary gland in dog and cat using computed tomography. Vet Res Forum 2018, 9, 337–341. [Google Scholar] [CrossRef]
- Häußler, T.C.; von Pückler, K.H.; Thiel, C.; Enderlein, S.; Failing, K.; Ondreka, N.; Kramer, M.; Schmidt, M.J. Measurement of the normal feline pituitary gland in brachycephalic and mesocephalic cats. J Feline Med Surg 2018, 20, 578–586. [Google Scholar] [CrossRef]
- Kooistra, H.S.; Voorhout, G.; Mol, J.A.; Rijnberk, A. Correlation between impairment of glucocorticoid feedback and the size of the pituitary gland in dogs with pituitary-dependent hyperadrenocorticism. J Endocrinol 1997, 152, 387–394. [Google Scholar] [CrossRef] [PubMed]
- Costanza, D.; Coluccia, P.; Castiello, E.; Greco, A.; Meomartino, L. Description of a low-cost picture archiving and communication system based on network-attached storage. Vet Radiol Ultrasound 2022, 63, 249–253. [Google Scholar] [CrossRef] [PubMed]
- Friedrichs, K.R.; Harr, K.E.; Freeman, K.P.; Szladovits, B.; Walton, R.M.; Barnhart, K.F.; Blanco-Chavez, J. ASVCP reference interval guidelines: determination of de novo reference intervals in veterinary species and other related topics. Vet Clin Pathol 2012, 41, 441–453. [Google Scholar] [CrossRef] [PubMed]
- Reed, A.H.; Henry, R.J.; Mason, W.B. Influence of statistical method used on the resulting estimate of normal range. Clin Chem 1971, 17, 275–284. [Google Scholar] [CrossRef] [PubMed]
- CLSI. Defining, Establishing and Verifying Reference Intervals in the Clinical Laboratory; Approved Guideline - Third Edition. CLSI document EP28-A3c 2008.
- Koo, T.K.; Li, M.Y. A Guideline of Selecting and Reporting Intraclass Correlation Coefficients for Reliability Research. J Chiropr Med 2016, 15, 155–163. [Google Scholar] [CrossRef] [PubMed]
- Geffré, A.; Concordet, D.; Braun, J.-P.; Trumel, C. Reference Value Advisor: a new freeware set of macroinstructions to calculate reference intervals with Microsoft Excel. Veterinary Clinical Pathology 2011, 40, 107–112. [Google Scholar] [CrossRef] [PubMed]
- Hecht, S.; Adams, W.H. MRI of brain disease in veterinary patients part 1: Basic principles and congenital brain disorders. Vet Clin North Am Small Anim Pract 2010, 40, 21–38. [Google Scholar] [CrossRef]
- Verdun, F.R.; Racine, D.; Ott, J.G.; Tapiovaara, M.J.; Toroi, P.; Bochud, F.O.; Veldkamp, W.J.H.; Schegerer, A.; Bouwman, R.W.; Giron, I.H.; et al. Image quality in CT: From physical measurements to model observers. Physica Medica 2015, 31, 823–843. [Google Scholar] [CrossRef]
- Faby, S.; Flohr, T. Multidetector-Row CT Basics, Technological Evolution, and Current Technology. In Body MDCT in Small Animals: Basic Principles, Technology, and Clinical Applications, Bertolini, G., Ed.; Springer International Publishing: Cham, 2017; pp. 3–33. [Google Scholar] [CrossRef]
- Bertolini, G. Basic Principles of MDCT Angiography. In Body MDCT in Small Animals: Basic Principles, Technology, and Clinical Applications, Bertolini, G., Ed.; Springer International Publishing: Cham, 2017; pp. 37–51. [Google Scholar] [CrossRef]
- Schwarz, T.; O'Brien, R. CT Acquisition Principles. In Veterinary Computed Tomography; 2011; pp. 9-27. [CrossRef]
- Vandenbroucke, J.P.; von Elm, E.; Altman, D.G.; Gøtzsche, P.C.; Mulrow, C.D.; Pocock, S.J.; Poole, C.; Schlesselman, J.J.; Egger, M. Strengthening the Reporting of Observational Studies in Epidemiology (STROBE): explanation and elaboration. Epidemiology 2007, 18, 805–835. [Google Scholar] [CrossRef]
- Argyropoulou, M.; Perignon, F.; Brunelle, F.; Brauner, R.; Rappaport, R. Height of normal pituitary gland as a function of age evaluated by magnetic resonance imaging in children. Pediatric Radiology 1991, 21, 247–249. [Google Scholar] [CrossRef] [PubMed]
- Sari, S.; Sari, E.; Akgun, V.; Ozcan, E.; Ince, S.; Saldir, M.; Babacan, O.; Acikel, C.; Basbozkurt, G.; Ozenc, S.; et al. Measures of pituitary gland and stalk: from neonate to adolescence. Journal of Pediatric Endocrinology and Metabolism 2014, 27, 1071–1076. [Google Scholar] [CrossRef] [PubMed]
- Lurie, S.N.; Doraiswamy, P.M.; Husain, M.M.; Boyko, O.B.; Ellinwood, E.H., Jr.; Figiel, G.S.; Krishnan, K.R. In vivo assessment of pituitary gland volume with magnetic resonance imaging: the effect of age. J Clin Endocrinol Metab 1990, 71, 505–508. [Google Scholar] [CrossRef] [PubMed]
- van der Vlugt-Meijer, R.H.; Meij, B.P.; Voorhout, G. Intraobserver and interobserver agreement, reproducibility, and accuracy of computed tomographic measurements of pituitary gland dimensions in healthy dogs. Am J Vet Res 2006, 67, 1750–1755. [Google Scholar] [CrossRef]
- Van Hoe, L.; Haven, F.; Bellon, E.; Baert, A.L.; Bosmans, H.; Feron, M.; Suetens, P.; Marchal, G. Factors influencing the accuracy of volume measurements in spiral CT: a phantom study. J Comput Assist Tomogr 1997, 21, 332–338. [Google Scholar] [CrossRef]
Figure 1.
(A, C, D) Transverse and (B) sagittal soft tissue algorithm postcontrast CT images of the skull of a twelve-month-old DSH cat. (A) Pituitary height (blue line) measured on the transverse plane (PHT) at the level of the pituitary fossa, perpendicular to the basisphenoid bone. (B) Pituitary height (blue line) measured on the sagittal plane (PHS) perpendicular to the basisphenoid bone and pituitary length (PL, red line) measured where the maximal length of the pituitary gland was visible and parallel to the basisphenoid bone. (C) Pituitary width (red line) measured on the transverse plane (PW) at the point of maximal width of the gland. (D) Brain area (BA, green line) measured on the transverse plane, at the same level of the PTH using an automated region of interest tool. (A, B, C) manually windowed to WW = 455, WL = 234; (D) manually windowed to WW = 2000, WL = 800. Abbreviations: Ca: Caudal; L: Left; R: Right; Ro: Rostral.
Figure 1.
(A, C, D) Transverse and (B) sagittal soft tissue algorithm postcontrast CT images of the skull of a twelve-month-old DSH cat. (A) Pituitary height (blue line) measured on the transverse plane (PHT) at the level of the pituitary fossa, perpendicular to the basisphenoid bone. (B) Pituitary height (blue line) measured on the sagittal plane (PHS) perpendicular to the basisphenoid bone and pituitary length (PL, red line) measured where the maximal length of the pituitary gland was visible and parallel to the basisphenoid bone. (C) Pituitary width (red line) measured on the transverse plane (PW) at the point of maximal width of the gland. (D) Brain area (BA, green line) measured on the transverse plane, at the same level of the PTH using an automated region of interest tool. (A, B, C) manually windowed to WW = 455, WL = 234; (D) manually windowed to WW = 2000, WL = 800. Abbreviations: Ca: Caudal; L: Left; R: Right; Ro: Rostral.
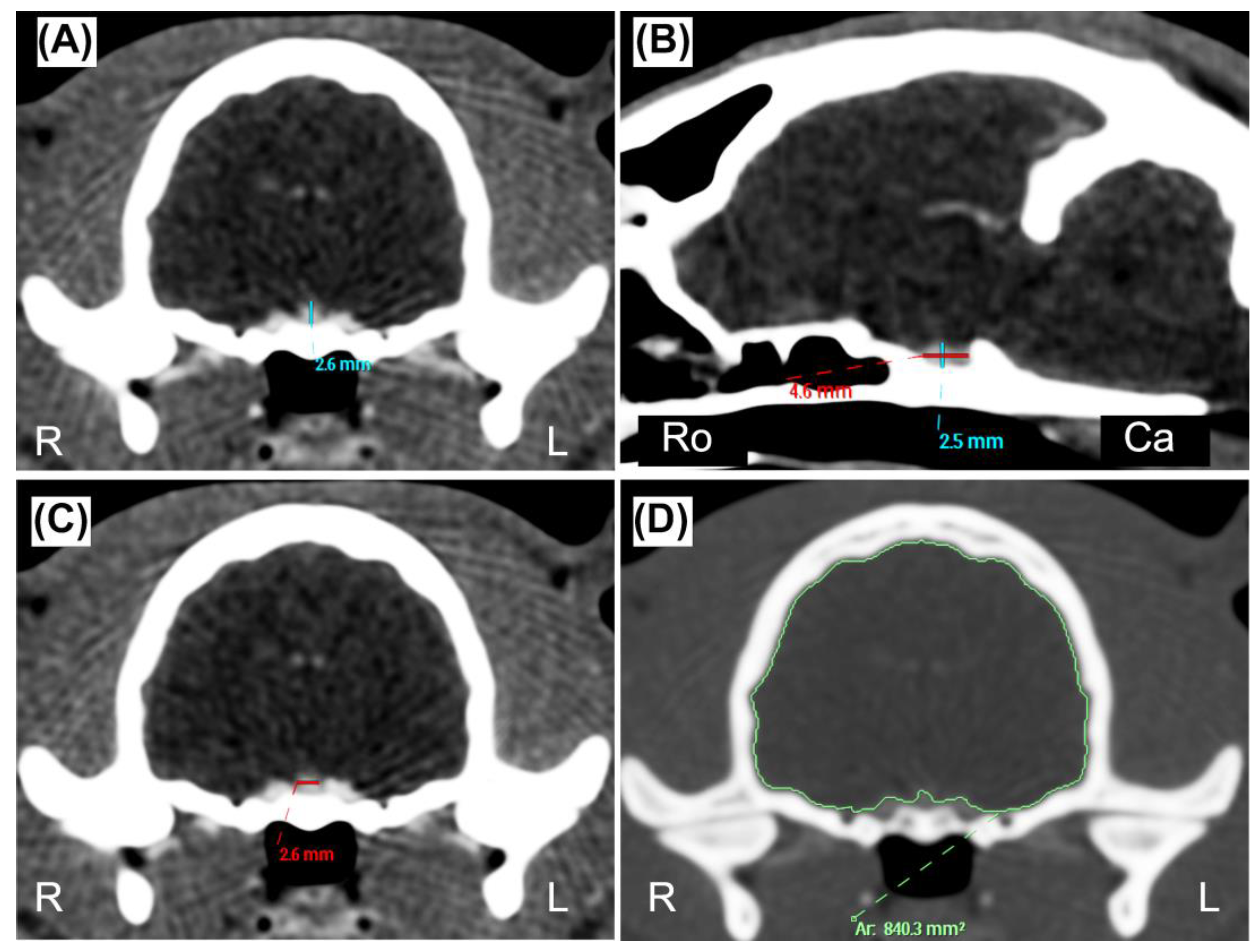
Figure 2.
Bland-Altman plot comparing measurements of the pituitary gland height measured in the transverse (PHT) and sagittal (PHS) plane. The y-axis shows the difference between the two measurements, and the x-axis shows the average. The blue dotted lines represent the 95% confidence intervals, and the red dotted line represents the bias.
Figure 2.
Bland-Altman plot comparing measurements of the pituitary gland height measured in the transverse (PHT) and sagittal (PHS) plane. The y-axis shows the difference between the two measurements, and the x-axis shows the average. The blue dotted lines represent the 95% confidence intervals, and the red dotted line represents the bias.
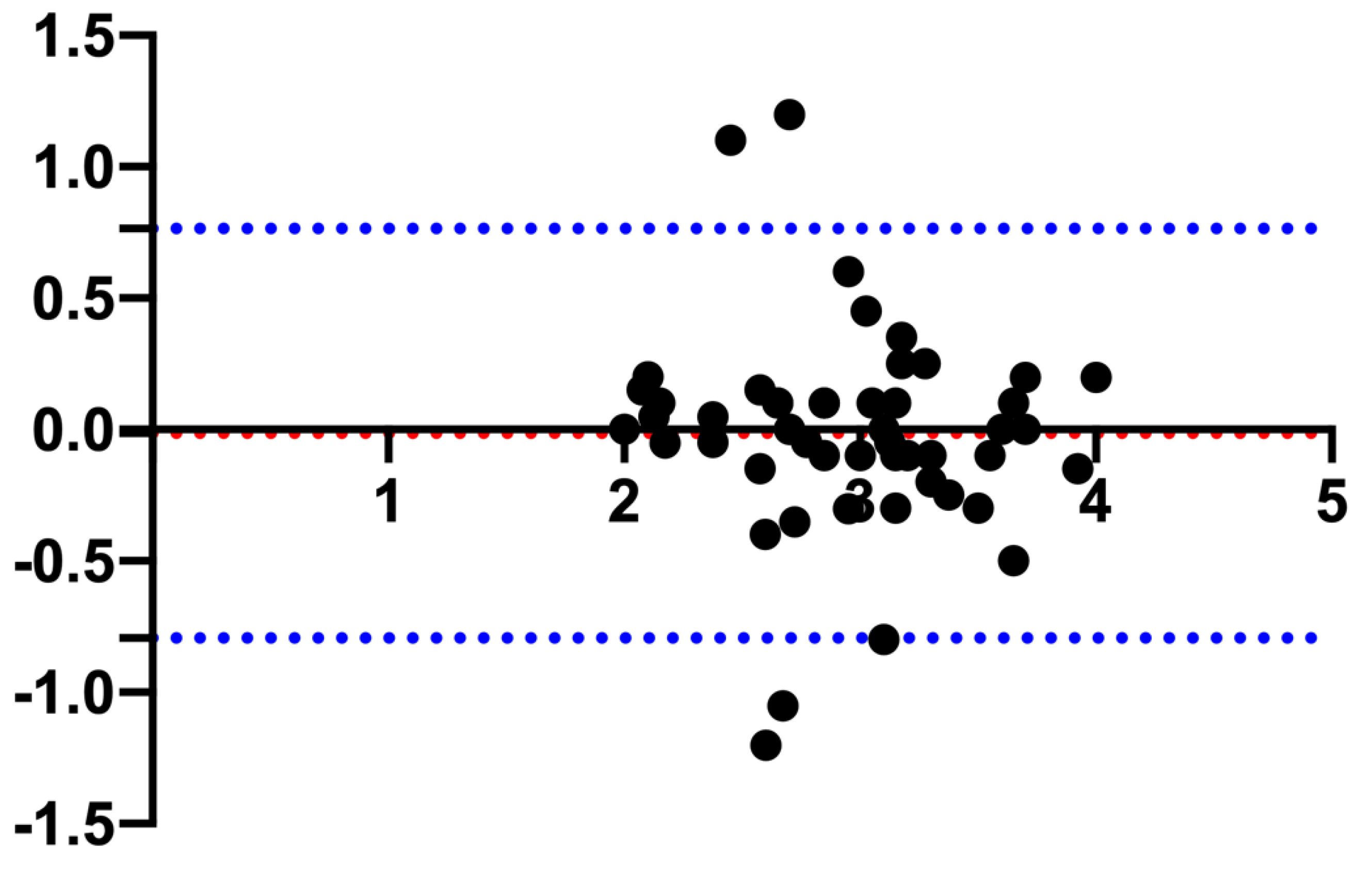

Table 1.
Mean ± standard deviation, upper and lower limits of the reference value (and corresponding 90% CI) of the pituitary gland linear measurements, brain area and pituitary-to-brain ratio.
Table 1.
Mean ± standard deviation, upper and lower limits of the reference value (and corresponding 90% CI) of the pituitary gland linear measurements, brain area and pituitary-to-brain ratio.
| Measurement | Mean (±SD) | Range (Min–Max) |
Lower Limit (90% CI) |
Upper Limit (90% CI |
|---|---|---|---|---|
| PHT (mm) | 2.94 (± 0.52) | 2.0 – 4.1 | 1.88 (1.68 – 2.10) |
4.01 (3.81 – 4.20) |
| PHS (mm) | 2.95 (± 0.55) | 1.9 – 4.0 | 1.84 (1.63 – 2.08) |
4.10 (3.89 – 4.27) |
| PL (mm) | 3.17 (± 0.52) | 2.0 – 4.4 | 2.13 (1.92 – 2.37) |
4.23 (4.03 – 4.42) |
| PW (mm) | 3.24 (± 0.61) | 2.1 – 4.8 | 1.92 (1.66 – 2.15) |
4.41 (4.12 – 4.71) |
| BA (mm2) | 789.02 (± 61.85) | 647.87 – 962.85 | 659.51 (634.51 – 687.61) |
910.96 (883 – 938.01) |
| P:B ratio | 0.37 (± 0.06) | 0.25 – 0.48 | 0.25 (0.23 – 0.28) |
0.49 (0.47 – 0.51) |
Abbreviations: CI, confidence interval; BA, brain area; Max, maximum; Min, minimum; P:B ratio, pituitary gland height to brain area ratio; PHS, maximal pituitary height on the sagittal plane; PHT, maximal pituitary height on the transverse plane; PL: pituitary length; PW: pituitary width; SD, standard deviation.
Table 2.
Mean ± standard deviation, upper and lower limits of the reference value (and corresponding 90% CI) of the pituitary gland linear measurements, brain area and pituitary-to-brain ratio.
Table 2.
Mean ± standard deviation, upper and lower limits of the reference value (and corresponding 90% CI) of the pituitary gland linear measurements, brain area and pituitary-to-brain ratio.
| Measurement | Body weight | p-value | Age | p-value |
|---|---|---|---|---|
| PHT (mm) | r = 0.39 | 0.004 | rs = 0.22 | 0.12 |
| PHS (mm) | r = 0.30 | 0.032 | rs = 0.35 | 0.012 |
| PL (mm) | r = 0.28 | 0.044 | rs = 0.36 | 0.009 |
| PW (mm) | r = 0.35 | 0.011 | rs = 0.12 | 0.39 |
| BA (mm2) | r = 0.29 | 0.036 | rs = 0.17 | 0.24 |
| P:B ratio | r = 0.29 | 0.038 | rs = 0.14 | 0.33 |
Abbreviations: CI, confidence interval; BA, brain area; P:B ratio, pituitary gland height to brain area ratio; PHS, maximal pituitary height on the sagittal plane; PHT, maximal pituitary height on the transverse plane; PL: pituitary length; PW: pituitary width; r: Pearson’s correlation coefficient; rs: Spearman’s rank correlation coefficient.
Table 3.
Intraclass correlation coefficients (ICC), relative 95% confidence intervals and p-values for the inter-observer reliability test.
Table 3.
Intraclass correlation coefficients (ICC), relative 95% confidence intervals and p-values for the inter-observer reliability test.
| Measurement | ICC | 95% CI | p-value |
|---|---|---|---|
| PHT | 0.69 | 0.38 – 0.84 | < 0.0001 |
| PHS | 0.58 | 0.37 – 0.74 | < 0.0001 |
| PL | 0.58 | 0.36 – 0.73 | < 0.0001 |
| PW | 0.66 | 0.46 – 0.79 | < 0.0001 |
| BA | 0.81 | 0.50 – 0.91 | < 0.0001 |
Abbreviations: CI, confidence interval; BA, brain area; ICC, intraclass correlation coefficients; PHT: pituitary height in the transverse plane; PHS: pituitary height in the sagittal plane; PL: pituitary length; PW: pituitary width.
Table 4.
Intraclass correlation coefficients (ICC), relative 95% confidence intervals and p-values for the intra-observer reliability test.
Table 4.
Intraclass correlation coefficients (ICC), relative 95% confidence intervals and p-values for the intra-observer reliability test.
| Measurement | Operator 1 | Operator 2 | ||||
|---|---|---|---|---|---|---|
| ICC | 95% CI | p-value | ICC | 95% CI | p-value | |
| PHT | 0.81 | 0.63 – 0.91 | < 0.0001 | 0.66 | 0.17 – 0.86 | <0.0001 |
| PHS | 0.87 | 0.71 – 0.94 | < 0.0001 | 0.60 | -0.04 – 0.85 | <0.0001 |
| PL | 0.51 | 0.19 – 0.73 | 0.001 | 0.70 | 0.10 – 0.89 | <0.0001 |
| PW | 0.78 | 0.59 – 0.89 | < 0.0001 | 0.60 | 0.08 – 0.83 | <0.0001 |
| BA | 0.82 | 0.66 – 0.91 | < 0.0001 | 0.92 | 0.84 – 0.96 | <0.0001 |
Abbreviations: CI, confidence interval; BA, brain area; ICC, intraclass correlation coefficient; PHS, maximal pituitary height on the sagittal plane; PHT, maximal pituitary height on the transverse plane; PL: pituitary length; PW: pituitary width.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



