
Submitted:
08 May 2023
Posted:
09 May 2023
You are already at the latest version
Abstract
Total hip arthroplasty (THA) is one of the most successful orthopedic procedures and is highly effective in improving function and quality of life. However, after discharge patients commonly experience edema, which can lead to health consequences and lower quality of life. For these rea-sons, the aim of this study is to evaluate the effectiveness of a specific intermittent leg pneumatic compression on lower limb edema and physical outcomes in patients after total hip arthroplasty, compared to standard conservative treatment. A total of 47 patients were enrolled and randomly allocated into two groups: the pneumatic compression group (PG=24) and the control group (CG=23). We evaluated thigh and calf circumferences, knee and ankle range of motion, pain and walking autonomy. Our results showed a greater reduction in thigh and calf circumference for PG (p<0.001), while other outcomes were similar for the two groups (p>0.05). The combination of standard therapy with pneumatic leg compression was more effective in reducing lower limb edema, thigh, and calf circumferences compared to the use of standard treatment. Our results suggest that pressotherapy treatment is a valuable and efficient option for managing lower limb edema and preventing VTE after THA.
Keywords:
leg pneumatic compression
; total hip arthroplasty
; lower limb edema
1. Introduction
Total hip arthroplasty (THA) is one of the most successful orthopedic procedures and is highly effective in relieving pain and improving function and quality of life [1,2]. In Italy, THA use has increased over the last 20 years and this is mainly related to the increase in patients’ longevity (higher number of individuals candidates for surgery) and the higher expectations of patients in terms of quality of life and possibility of performing recreational activities again [3]. The complication rate for the THA is quite low, but major complications such as venous thromboembolism (VTE- incidence of 0.6-1.5%) can be highly debilitating due to increased length of stay and potentially worsened outcomes after the surgery [4]. In fact, a study by O’Reilly et al. reports that after discharge from the hospital, patients had a higher risk to develop VTE with a prevalence of 8.9% [5]. The risk factors for VTE are described by Virchow’s triad: hypercoagulable state, endothelial injury, and venous stasis, where at least two factors are generally necessary for VTE development [6]. The endothelial injury leads to edema and is inevitable in surgery but can be minimized through proper surgical techniques. The hypercoagulable state is a local and systemic inflammatory response induced by tissue injury during surgery [7,8,9]. Venous stasis could occur both during surgery, because of tourniquet use and intraoperative immobilization, and after surgery, when patients are less mobile in the postoperative period. In fact, prolonged immobility is a risk factor for the development of VTE [10]. Rapid recovery programs and early mobilization may reduce the immobilization period and complications after THA. The importance of multimodal treatment such as graduated compression stockings and pharmacologic prophylaxis against VTE by inhibiting the coagulation cascade is, therefore, evident [11,12,13]. To reduce the risk of developing VTE, with also a better prognosis related to edema resorption and physical outcomes, the introduction of other non-pharmacological interventions such as pneumatic compression (pressotherapy) could be helpful. The Cochrane review by Kakkos et al. [14] showed that a combination of intermittent pneumatic leg compression and pharmacological prophylaxis can reduce the incidence of deep vein thrombosis and pulmonary embolism compared with compression or pharmacological prophylaxis alone [14] but, remains unclear the effectiveness of combined treatments on reduce VTE development. Despite these results, all 15 randomized controlled trials included in this review, showed low reliability due to a high risk of selection and performance bias highlighting the necessity of further studies to confirm (or not) the effectiveness of combined treatments. A subsequent Cochrane review provided by Zhao et al. [15] evaluated the efficacy of different intermittent pneumatic leg compression combined with pharmacological treatment in VTE reduction without reaching significant and reliable results, underlying the lack of randomized controlled trials for this topic. In particular, several studies highlighted the persistence of edema in patients after total hip arthroplasty with a higher risk of VTE development and a decrement in functional capacity and quality of life [16,17,18]. For these reasons, the aim of this study is to evaluate the effectiveness of a specific intermittent leg pneumatic compression on lower limb edema and physical outcomes in patients after total hip arthroplasty, compared to standard conservative treatment.
2. Materials and Methods
2.1. Study design and participants
A randomized control trial using randomly sequenced blocks of variable size was conducted. For the block design elaboration, a generation of random numbers is carried out by the STATA statistical software (release 17.0, 2021, Stata Corporation, College Station, Texas, USA), using the “ralloc” command. The researchers are unaware of the block size to avoid the possibility of sequence predictability.
A total of 47 patients were enrolled from the Department of Orthopedic Surgery of the University Hospital “Istituto di Cura Città di Pavia” (Pavia, Italy), in accordance with the doctors and therapists and randomly allocated into two groups: the pneumatic compression group (PG=24) and the control group (CG=23). CG performed the standard VTE therapy: pharmacological prophylaxis, compressive stockings and electrostimulation (T-ONE Rehab, I-TECH Medical Division, Scorzè, Italy). PG combined pneumatic compression to standard VTE therapy.
The inclusion criteria were: elective total hip arthroplasty, via postero-lateral approach, age between 50 and 80 years old, both genders, and the ability to understand the study protocol and procedure. The exclusion criteria were: co-morbidity such as obesity and diabetes, orthopedic or neurological pathologies that modify the ability to walk, pathologies that modify balance (neurological and/or vestibular), contraindications to the use of the medical equipment used in the study and the inability to understand and sign the informed consent.
The study protocol and procedure were explained to the patients before their engagement in the study and written informed consent was obtained. Patients could withdraw from the study at any moment without repercussion. The study protocol was approved by the Ethical Committee of Fondazione IRCSS Policlinico San Matteo of Pavia (protocol number 0014626/22) and was performed according to the Declaration of Helsinki as revised in 2018 [19].
2.2. Anthropometric characteristics
Weight was measured barefoot and in light clothing, standing in the middle of the scale platform (Seca, Hamburg, Germany), with hands along the trunk. Standing height was measured using a Harpenden stadiometer (Holtain Ltd., Cross-Well, UK) with a fixed vertical table and an adjustable head. The measurement was carried out with the subjects in an upright standing position, without shoes, and with their head in the horizontal plane of Frankfort. Two measurements were taken for each parameter, and a third was obtained if a discrepancy of 500 g and 0.5 cm was noted between the initial measurements. Anthropometric parameters were then based on the average of the two closest measurements. Body mass index (BMI) was calculated as body weight (kilograms) divided by height squared (meters squared).
2.3. Study protocol and evaluation
All patients were enrolled by the surgeon before the THA intervention after the explanation of the study protocol procedure.
All assessments were performed by the same trained specialist 1 day after the THA surgery (T0) and at the end of the treatment, after 10 days of treatment, before the hospital discharge (T1). All the evaluations were performed in the afternoon (4–5:00 or 5–6:00 p.m.) in the same clinical setting; specifically, in a room in a clinical context with a constant temperature of 21°C.
To evaluate postoperative edema, the following measurements were performed on the operated limb:
- the circumference of the distal third of the thigh (15cm above the upper border of the patella);
- the circumference of the proximal third of the leg (20cm above the lateral malleolus);
- the knee flexion range of motion (ROM);
- the ankle dorsiflexion ROM.
The circumferences were taken with a tape measure and the ROM with a manual arthrogoniometer.
The Numeric Rating Scale (NRS), a reliable and validated scale [20,21,22], was used to assess subjective pain. Patients circle the number between 0 and 10, 0 and 20, or 0 and 100, in accordance with their pain intensity perception. Zero usually corresponds to ‘no pain at all’, instead the upper limit represents ‘the worst pain ever possible’.
The 20-meter walking test (20 mwt) was used to evaluate functional capacity. Patients had to walk in a 20-meter straight trail as fast as possible [23] without interruption. Prior to the execution of the test, the specialist explained to the patients the procedure and then showed them how to perform it. The time was taken using a chronograph to record the time (stopwatch W073, SEIKO, Tokyo, Japan), and a lower time showed better performance.
2.4. The pneumatic compression therapy
The I-Press® instrument (I-Tech Medical Division, Scorzè, Italy) was used to perform the therapy. The instrument consists of a pumping system, connected to two 4-chamber pressure leggings, which are responsible for pumping air through the tubes connected to the different chambers of the leg cuffs. The device reproduces the mechanism of controlled compression on the limbs, with a distal-proximal movement (from the periphery towards the center).
Table 1 shows the technical features of the instrument used.
The PG performed two times per day for a total of 10 days the pneumatic compression therapy; each session lasted 30 minutes. To ensure the correct use of the device, the inflatable legging was placed on the operated limb by the physiotherapist and the pressure was set at 100 mmHg.
2.5. Statistical analysis
To ensure the correctness of sample numerosity a sample size calculation was performed. Pearson's chi-square test for two independent proportions, considering an alpha error equal to 0.05, a power of 80%, and an effect size equal to 1.76 (according to Cohen's classification) was performed. All quantitative data are shown as mean ± standard deviation (SD). We tested for normality by Shapiro–Wilk tests and graphically checked for linearity. We used an independent samples t-test, a parametric Student or non-parametric Mann-Whitney as appropriate, to evaluate the differences between the pressotherapy and the control group changes. To estimate the size of the effect we used the Cohen d’ or Rank Biserial correlation as appropriate. All the significance was set at a p-value less than 0.05. Statistical analyses were performed using The Jamovi Project (2021). Jamovi Version 1.6 for Mac [Computer Software], Sydney, Australia; retrieved from https://www.jamovi.org (accessed on 5 March 2023).
3. Results
In Table 2 are reported the baseline characteristics of the 47 patients (30 females, 17 males, aged 68.20 ± 9.13 years, range 50–80) enrolled in the study.
A comparison between the PG and the CG for all outcomes is shown in Table 3. In particular, PG had a greater reduction in calf circumference (p<0.001) and in thigh circumference (p<0.001) than CG after the somministration of the combined protocol.
4. Discussion
The aim of our study was to evaluate the effectiveness of intermittent pneumatic compression of the operated lower limb combined with standard VTE treatment on edema and physical outcomes in patients after THA and compare it to standard VTE treatment alone. The results of our study showed that the combination of standard therapy with pneumatic leg compression was more effective in reducing thigh and calf circumferences (p<0.001). The two types of treatment (standard and combined treatment) did not differ in improving the range of motion (ROM) of the knee and ankle and in reducing the perceived pain (p>0.05). These results are in accordance with the findings of Fujisawa et al. [24], who demonstrated that leg pneumatic compression can decrease the swelling in the lower limbs after seven days from the THA operation. Furthermore, Westrich et al. [25] showed a greater effect of leg pneumatic compression combined with the use of aspirin in reducing lower limb edema after total knee arthroplasty compared to the only use of pharmacological treatment. The reduction of lower limb edema is an essential part of therapy after THA. Edema can cause various problems, including skin damage, increased risk of infection and impaired circulation [26], which can lead to the development of one of the three factors of Virchow’s triad (venous stasis). After the surgery, venous stasis increases the risk of developing VTE in THA patients highlighting the relevance of lower limb edema reduction. In addition, Fujisawa et al. [24] analyzed the effect of leg pneumatic compression treatment on D-dimer concentration, a direct marker for the risk of developing VTE. The study found that after seven days of leg-pneumatic compression, this treatment was effective in reducing D-dimer concentration, thus proving that leg-pneumatic compression is effective after THA to prevent VTE. The use of leg pneumatic compression also has other benefits, such as improving blood flow, reducing muscle soreness, and aiding in the recovery of injured joints. This enhances the therapy's effectiveness and helps improve THA's physical outcomes. Furthermore, we did not find any collateral effect in both groups, suggesting that leg pneumatic compression is a safe and effective technique. The time needed for pressotherapy treatment is shorter than the traditional VTE treatment leading to an efficient cure. However, it is fundamental that this device is used with the supervision of healthcare professionals that could determine the appropriate pressure level and treatment duration. To the best of our knowledge, no other studies have investigated the effects of leg pneumatic compression on ROM, NRS, and 20mwt in patients after THA. Our results did not reveal any differences in ROM which may be attributed to the area where the edema was located, being distant from the knee and ankle joints. Moreover, we did not observe any differences in 20mwt and NRS, which could suggest that the edema experienced post-THA had no influence on walking performance and without association with perceived pain.
We recognize that our study had some limitations. Firstly, we did not evaluate the effect of pressotherapy on VTE with the D-dimer blood concentration, which could provide more accurate results about VTE risk. Additionally, the duration of our study protocol was limited; we only analyzed the effect of pressotherapy after 10 days of treatment. Thus, future studies should extend the duration of the protocol and investigate the effect of pressotherapy even after months of the THA to gain a more comprehensive understanding of the effects.
5. Conclusions
The combination of standard therapy with pneumatic leg compression was more effective in reducing lower limb edema, thigh, and calf circumferences compared to the use of standard treatment. Our results suggest that pressotherapy treatment is a valuable and efficient option for managing lower limb edema and could lead to a VTE reduction after the THA. Although the use of leg pneumatic compression on physical outcomes of THA is not clear, further studies should investigate this to enhance the effectiveness of this treatment. Since it is also a safe, effective and low-cost treatment, with no adverse effects reported in the literature, it is recommended that pneumatic compression of the operated limb is included in THA's standard post-operative therapy. Furthermore, since our patients expressed satisfaction with the pneumatic compression, reporting a feeling of well-being after the treatment, future research should focus on the self-reported pleasantness of pressotherapy.
Author Contributions
Conceptualization, V.C.P., M.V., M.F. and L.M.; methodology, L.M., S.B. and P.P.; validation, M.V., M.F. and P.P.; formal analysis, A.G.; investigation, A.G. ad C.C..; data curation, C.C.; writing—original draft preparation, V.C.P, A.G., C.C., S.B. and P.P; writing—review and editing, M.V., M.F. and L.M. ; visualization, M.V..; supervision, L.M.; project administration, L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki and approved by the Institutional Review Board (or Ethics Committee) of Ethical Committee of Pavia (protocol code 0014626/22 and 15/03/2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Chang, R.W.; Pellisier, J.M.; Hazen, G.B. A Cost-Effectiveness Analysis of Total Hip Arthroplasty for Osteoarthritis of the Hip. JAMA 1996, 275, 858–865. [Google Scholar] [CrossRef] [PubMed]
- Bozic, K.J.; Kurtz, S.M.; Lau, E.; Ong, K.; Vail, T.P.; Berry, D.J. The Epidemiology of Revision Total Hip Arthroplasty in the United States. J Bone Joint Surg Am 2009, 91, 128–133. [Google Scholar] [CrossRef] [PubMed]
- benedetta Report Annuale Riap 2019 e Compendio Available online:. Available online: https://riap.iss.it/riap/it/attivita/report/2020/10/19/report-riap-2019/ (accessed on 2 May 2023).
- Santana, D.C.; Emara, A.K.; Orr, M.N.; Klika, A.K.; Higuera, C.A.; Krebs, V.E.; Molloy, R.M.; Piuzzi, N.S. An Update on Venous Thromboembolism Rates and Prophylaxis in Hip and Knee Arthroplasty in 2020. Medicina (Kaunas) 2020, 56, 416. [Google Scholar] [CrossRef] [PubMed]
- O’Reilly, R.F.; Burgess, I.A.; Zicat, B. The Prevalence of Venous Thromboembolism after Hip and Knee Replacement Surgery. Med J Aust 2005, 182, 154–159. [Google Scholar] [CrossRef] [PubMed]
- Righini, M.; Le Gal, G.; De Lucia, S.; Roy, P.-M.; Meyer, G.; Aujesky, D.; Bounameaux, H.; Perrier, A. Clinical Usefulness of D-Dimer Testing in Cancer Patients with Suspected Pulmonary Embolism. Thromb Haemost 2006, 95, 715–719. [Google Scholar] [PubMed]
- Dahl, O.E.; Harenberg, J.; Wexels, F.; Preissner, K.T. Arterial and Venous Thrombosis Following Trauma and Major Orthopedic Surgery: Molecular Mechanisms and Strategies for Intervention. Semin Thromb Hemost 2015, 41, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Albayati, M.A.; Grover, S.P.; Saha, P.; Lwaleed, B.A.; Modarai, B.; Smith, A. Postsurgical Inflammation as a Causative Mechanism of Venous Thromboembolism. Semin Thromb Hemost 2015, 41, 615–620. [Google Scholar] [CrossRef]
- Wanderling, C.; Liles, J.; Finkler, E.; Carlsgaard, P.; Hopkinson, W.; Guler, N.; Hoppensteadt, D.; Fareed, J. Dysregulation of Tissue Factor, Thrombin-Activatable Fibrinolysis Inhibitor, and Fibrinogen in Patients Undergoing Total Joint Arthroplasty. Clin Appl Thromb Hemost 2017, 23, 967–972. [Google Scholar] [CrossRef]
- Risk of and Prophylaxis for Venous Thromboembolism in Hospital Patients. Thromboembolic Risk Factors (THRIFT) Consensus Group. BMJ 1992, 305, 567–574. [CrossRef]
- Morris, G.K.; Henry, A.P.; Preston, B.J. Prevention of Deep-Vein Thrombosis by Low-Dose Heparin in Patients Undergoing Total Hip Replacement. Lancet 1974, 2, 797–800. [Google Scholar] [CrossRef]
- Agu, O.; Hamilton, G.; Baker, D. Graduated Compression Stockings in the Prevention of Venous Thromboembolism. Br J Surg 1999, 86, 992–1004. [Google Scholar] [CrossRef] [PubMed]
- Snyder, M.A.; Sympson, A.N.; Scheuerman, C.M.; Gregg, J.L.; Hussain, L.R. Efficacy in Deep Vein Thrombosis Prevention With Extended Mechanical Compression Device Therapy and Prophylactic Aspirin Following Total Knee Arthroplasty: A Randomized Control Trial. J Arthroplasty 2017, 32, 1478–1482. [Google Scholar] [CrossRef] [PubMed]
- Kakkos, S.K.; Caprini, J.A.; Geroulakos, G.; Nicolaides, A.N.; Stansby, G.; Reddy, D.J.; Ntouvas, I. Combined Intermittent Pneumatic Leg Compression and Pharmacological Prophylaxis for Prevention of Venous Thromboembolism. Cochrane Database Syst Rev 2016, 9, CD005258. [Google Scholar] [CrossRef] [PubMed]
- Zhao, J.M.; He, M.L.; Xiao, Z.M.; Li, T.S.; Wu, H.; Jiang, H. Different Types of Intermittent Pneumatic Compression Devices for Preventing Venous Thromboembolism in Patients after Total Hip Replacement. Cochrane Database Syst Rev 2012, 11, CD009543. [Google Scholar] [CrossRef] [PubMed]
- Al Thaher, Y.; Alfuqaha, O.A.; Dweidari, A. Health-Related Quality of Life and Outcome after Total Knee Replacement: Results from a Cross-Sectional Survey in Jordan. Adv Orthop 2021, 2021, 5506809. [Google Scholar] [CrossRef]
- Canovas, F.; Dagneaux, L. Quality of Life after Total Knee Arthroplasty. Orthopaedics & Traumatology: Surgery & Research 2018, 104, S41–S46. [Google Scholar] [CrossRef]
- Miller, L.K.; Jerosch-Herold, C.; Shepstone, L. Effectiveness of Edema Management Techniques for Subacute Hand Edema: A Systematic Review. Journal of Hand Therapy 2017, 30, 432–446. [Google Scholar] [CrossRef]
- World Medical Association World Medical Association Declaration of Helsinki: Ethical Principles for Medical Research Involving Human Subjects. JAMA 2013, 310, 2191–2194. [CrossRef]
- Farrar, J.T.; Young, J.P.; LaMoreaux, L.; Werth, J.L.; Poole, M.R. Clinical Importance of Changes in Chronic Pain Intensity Measured on an 11-Point Numerical Pain Rating Scale. Pain 2001, 94, 149–158. [Google Scholar] [CrossRef]
- Jensen, M.P.; Karoly, P.; Braver, S. The Measurement of Clinical Pain Intensity: A Comparison of Six Methods. Pain 1986, 27, 117–126. [Google Scholar] [CrossRef]
- Kremer, E.; Atkinson, H.J.; Ignelzi, R.J. Measurement of Pain: Patient Preference Does Not Confound Pain Measurement. Pain 1981, 10, 241–248. [Google Scholar] [CrossRef] [PubMed]
- Motyl, J.M.; Driban, J.B.; McAdams, E.; Price, L.L.; McAlindon, T.E. Test-Retest Reliability and Sensitivity of the 20-Meter Walk Test among Patients with Knee Osteoarthritis. BMC Musculoskeletal Disorders 2013, 14, 166. [Google Scholar] [CrossRef] [PubMed]
- Fujisawa, M.; Naito, M.; Asayama, I.; Kambe, T.; Koga, K. Effect of Calf-Thigh Intermittent Pneumatic Compression Device after Total Hip Arthroplasty: Comparative Analysis with Plantar Compression on the Effectiveness of Reducing Thrombogenesis and Leg Swelling. J Orthop Sci 2003, 8, 807–811. [Google Scholar] [CrossRef] [PubMed]
- Westrich, G.H.; Sculco, T.P. Prophylaxis against Deep Venous Thrombosis after Total Knee Arthroplasty. Pneumatic Plantar Compression and Aspirin Compared with Aspirin Alone. J Bone Joint Surg Am 1996, 78, 826–834. [Google Scholar] [CrossRef]
- Foldi, E.; Foldi, M.; Rockson, S. Complete decongestive physiotherapy. Lymphedema: A Concise Compendium of Therapy and Practice 2018, 403–411. [Google Scholar]
Figure 1.
Difference between PG and CG in thigh circumference. Legend: PG=pneumatic compression group; CG= control group; cm=centimeters; ***p<0.001. .
Figure 1.
Difference between PG and CG in thigh circumference. Legend: PG=pneumatic compression group; CG= control group; cm=centimeters; ***p<0.001. .
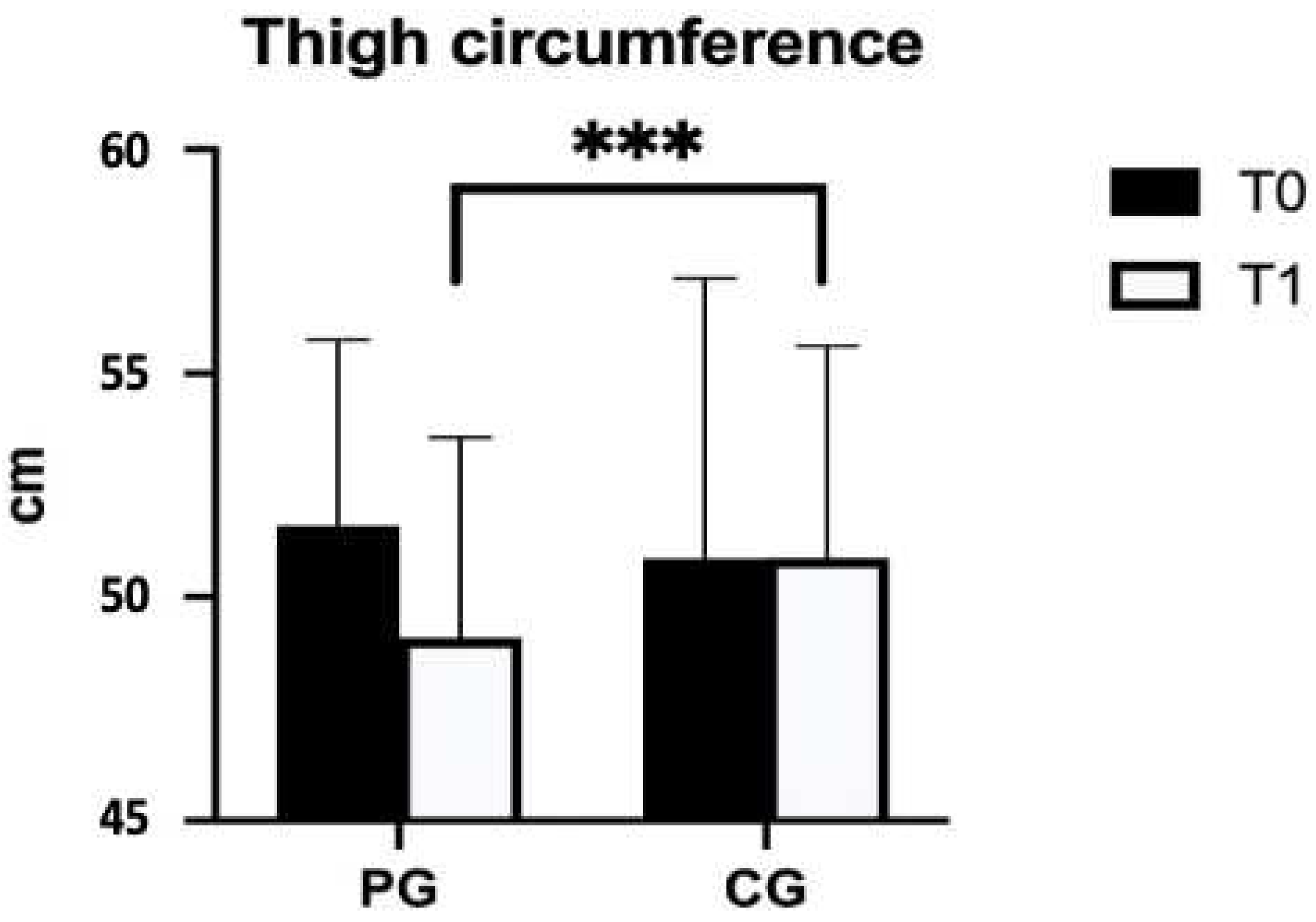
Figure 2.
Difference between PG and CG in calf circumference. Legend: PG=pneumatic compression group; CG= control group; cm=centimeters; ***p<0.001.
Figure 2.
Difference between PG and CG in calf circumference. Legend: PG=pneumatic compression group; CG= control group; cm=centimeters; ***p<0.001.
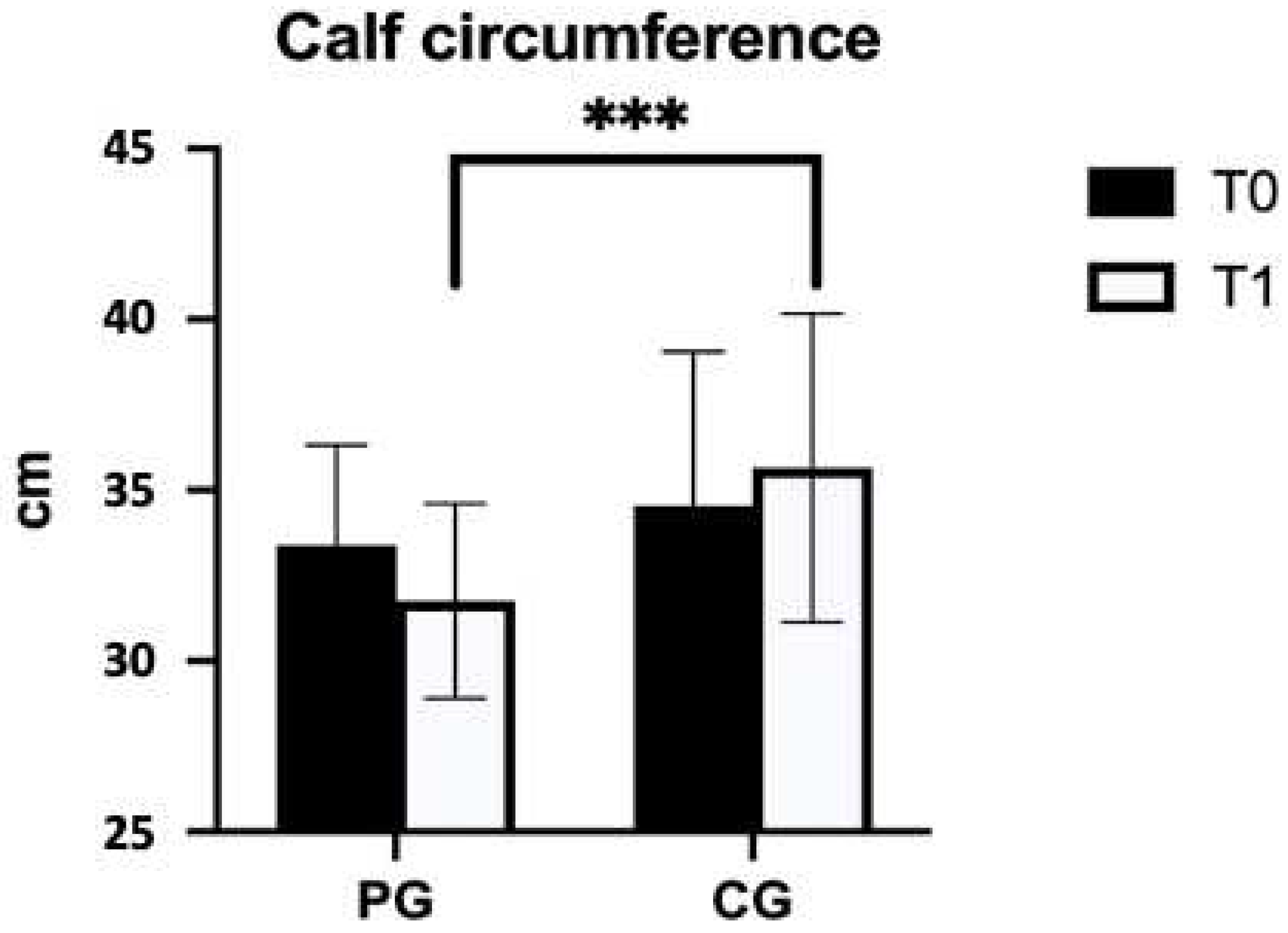

Table 1.
Instrument technical features.
| Power supply | 230V AC, 50 Hz |
| Current | 0,1 A |
| Therapy time | 0÷30 min. |
| Pressure | 200 mmHg (±20%) |
| Weight | 2 Kg |
Table 2.
Descriptive characteristics of the sample.
| PG (n=24) | CG (n=23) | |
|---|---|---|
| Male : Female | 9 : 15 | 8 : 15 |
| Age (years) | 68.38 ± 9.35 | 68.09 ± 9.11 |
| Weight (kg) | 71.71 ± 12.77 | 73.57 ± 12.28 |
| Height (m) | 1.65 ± 0.09 | 1.68 ± 0.10 |
| BMI (kg/m2) | 25.96 ± 3.14 | 25.72 ± 2.59 |
1 All data are shown as mean±SD. Legend: kg=kilograms; m=meters; BMI= body mass index.
Table 3.
Comparison of measurement changes at baseline (T0) and after the intervention (T1) in the PG and CG.
Table 3.
Comparison of measurement changes at baseline (T0) and after the intervention (T1) in the PG and CG.
| T0 | T1 | Delta (post-pre) | p-value | Effect size | ||
|---|---|---|---|---|---|---|
| Thigh circumference (cm) | PG (n=24) | 51.6 ± 4.1 | 49.1 ± 4.5 | -2.5 ± 1.6 |
<0.001*** |
0.850 |
| CG (n=23) | 50.9 ± 6.3 | 50.9 ± 4.7 | 0.0 ± 3.3 | |||
| Calf circumference (cm) | PG (n=24) | 33.4 ± 2.9 | 31.8 ± 2.9 | -1.6 ± 2.1 |
<0.001*** |
0.690 |
| CG (n=23) | 34.5 ± 4.5 | 35.7 ± 4.5 | 1.2 ± 4.2 | |||
| Knee ROM (°) | PG (n=24) | 99.38 ± 23.95 | 117.20 ± 9.97 | 16.88 ± 25.47 |
>0.05 |
// |
| CG (n=23) | 93.91 ± 23.95 | 110.57 ± 12.09 | 16.65 ± 13.66 | |||
| Ankle ROM (°) | PG (n=24) | 91.79 ± 4.37 | 95.58 ± 6.07 | 3.79 ± 5.40 |
>0.05 |
// |
| CG (n=23) | 87.96 ± 6.26 | 92.09 ± 3.90 | 4.13 ± 5.27 | |||
| NRS | PG (n=24) | 4.92 ± 2.00 | 2.46 ± 1.61 | -2.46 ± 1.74 |
>0.05 |
// |
| CG (n=23) | 6.13 ± 2.24 | 4.00 ± 1.73 | -2.13 ± 1.32 | |||
| 20 mwt (s) | PG (n=24) | 52.44 ± 22.79 | 25.27 ± 4.83 | -24.98 ± 24.95 |
>0.05 |
// |
| CG (n=23) | 58.39 ± 20.62 | 34.52 ± 10.24 | -23.87 ± 15.90 |
1 All data are shown as mean±SD. *p<0.05 and ***p<0.01 as significant values. Legend: PG= pneumatic compression group; CG= control group; cm=centimeters; °=grade; ROM= range of motion; NRS= Numeric Rating Scale; mwt= meter walking test. .
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



