Submitted:
08 May 2023
Posted:
09 May 2023
You are already at the latest version
Abstract
Excessive intake of fluoride, one of the trace elements to maintain health, leads to liver injury. Tetramethylpyrazine (TMP) is a kind of traditional Chinese medicine monomer with good antioxidant and hepatoprotective function. The aim of this study was to investigate the effect of TMP on liver injury induced by acute fluorosis. A total of 60 1-month-old male Institute of Cancer Research mice without carriage of pathogenic bacteria were selected. All mice were fed adaptively for one week, and then randomly divided into 5 groups: control (K) group, model (F) group, low-dose (LT) group, medium-dose (MT) group and high-dose (HT) group. The control and model group were given distilled water, while 40 mg/kg (LT), 80 mg/kg (MT) and 160 mg/kg (HT) TMP were fed by gavage for two weeks with the maximum gavage volume of mice is 0.2ml/10g/d. Except for the control group, all groups were given fluoride (35 mg/kg) by intraperitoneal injection on the last day of the experiment. The results of this study showed that compared with the model group, TMP alleviated the pathological changes of liver induced by fluoride and improved the ultrastructure of liver cells; TMP significantly decreased the levels of ALT, AST and MDA (P <0.05), and increased the levels of T-AOC, T-SOD and GSH (P <0.05). The results of mRNA detection showed that TMP significantly increased the mRNA expression levels of Nrf2, HO-1, CAT, GSH-Px and SOD in liver compared with model group (P <0.05). In conclusion, TMP can inhibit oxidative stress by activating Nrf2 pathway and alleviate liver injury induced by fluoride.
Keywords:
acute fluorosis
; tetramethylpyrazine
; liver
; oxidative damage
; Nrf2
1. Introduction
Fluorine (F) is a nonmetal element in nature, which has been recognized a strong oxidant because of its unique chemical structure [1]. Fluoride is a salted compound of fluorine, which maintains physiological homeostasis and is an essential component for bone mineralization and enamel formation [2,3]. It has been reported that appropriate intake of fluoride helps with skeletal formation, prevention of dental caries, promotion of the neuron conduction, and anti-aging [4]. Supplement of fluoride in drinking waters has been used extensively worldwide for disinfection and prevention of dental diseases [5,6,7]. However, the concentration of fluoride in drinking water for prevention of dental caries should not exceed 0.7 mg/L [8]. Fluoride is a double-edged sword, given a low dose of fluoride ingestion in drinking water helps to prevent dental caries, but ingestion of fluoride in drinking water in excess of the doses described above can cause fluorosis and threaten human life health. Fluorosis leads to skeletal disorders and arthrosis, which result in deformity. Chronic fluorosis has been reported to cause encephalopathy, leading to impaired central nervous system function [9]. It has been known that fluorosis is an irreversible and a major public health threat in China [4]. There are three potential resources to get exposed with fluoride, including drinking water, coal-burning, and drinking tea [10]. Fluorosis becomes an endemic disease in China because of the habits of drinking tea and uncontrolled coal-burning [11]. Recently, the studies in regard to the molecular mechanism of action of fluorosis and explore a traditional Chinese medication to intervene fluorosis has become popular [12].
It has been recognized recently that Nrf2/ARE pathway plays a key role to mitigate oxidative stress during inflammation [13]. Liver has been known an important organ to regulate or initiate Nrf2/ARE pathway [14,15]. Furthermore, it has been shown that Nrf2 pathway is activated during fluoride induced hepatopathy to alleviate oxidative stress [16]. Therefore, one of the aims of this study is to explore the mechanism of action and the role of Nrf 2 pathway during fluoride-induced hepatopathy.
Over the past few decades, several studies have demonstrated the benefits of using natural products to counter oxidative stress via the Nrf2/ARE pathway[13]. Tetramethylpyrazine (TMP) is an active ingredient extracted from Ligusticum chuanxiong Hort (Ligusticum wallichii) [17], which has been proven that to be an effective component with anti-inflammatory and antioxidant properties [18]. It has been reported that the antioxidant effect of TMP is mainly by activating Nrf2/HO-1 pathway in liver, which scavenges free radicals, inhibits NF-κB, enhances the expressions of glutathione peroxidase (GSH-Px), superoxide dismutase (SOD) and other associated antioxidants, and promotes the antioxidant capacity of hepatocytes [19,20]. Use of traditional Chinese herb extractions, such as Longyanshen polysaccharide, Astragalus membranaceus, stilbene glycoside, gastrodin, resveratrol, and so on, to intervene fluorosis has been studied extensively [21]. Therefore, the second purpose of this study is to clarify the clinical effects and the mechanism of actions of TPM in treating fluoride-induced hepatopathy.
2. Materials and Methods
2.1. Chemicals
Sodium fluoride (NaF), sodium pentobarbital (C11H17N2NaO3), TMP, alanine aminotransferase (ALT, C009-2-1), aspartate aminotransferase (AST, C010-2-1), malondialdehyde (MDA, A003-1-2), reduced glutathione (GSH, A006-2-1), total superoxide dismutase (T-SOD, A001-1-2), and total antioxidant Capacity (T-AOC, A015-3-1) were purchased from Jiancheng Bioengineering Institute, Nanjing, China. (Kit name: PrimeScriptTM RT Reagent KitRR086A). SYBR R Premix Ex TaqTM II (cat no. RR920A) and RNAiso Plus (cat no. 9178) were provided by Takara Biotech-nology Co., Ltd. (Dalian, Liaoning, China).
2.2. Experimental Animals and Methods
The use of animals was approved by Animal Protection and Use Committee of Sichuan Agricultural University (Approval No.: dyy - 20203012). Sixty four-week-old male ICR mice with body weight from 18 to 22g were used in this study (Pegatron Biotech Co., Ltd., Chengdu, China; Animal License No.:SCXK [chuang] 2020-030). Mice were housed in a standard SPF facility with controlled room temperature at 25±2℃ under a 12-hour light-dark cycle, and fed with standard pellet diet and water ad libitum. Subjects were randomly divided into 5 groups (n = 12 in each group): (1) control group (CON); (2) model group (F), (3) low dose TMP group (LT): 40mg/kg of TMP; (4) medium dose TMP group (MT): 80mg/kg of TMP; (5) high dose TMP group (HT): 160mg/kg of TMP. TMP was dissolved in distilled water and administered to mice by gastric tube for 14 days in three TMP groups. Mice in the control and model groups were administered the same volume of distilled water for 14 days. After the last administration, mice in model group and TMP group were given NaF dissolved in distilled water (35 mg/kg body weight)[22] after the last treatment to induce acute hepatopathy; the same volume of distilled water was administered intragastrically to the control group. After 24 hours of Fluoride challenge, the mice were euthanized by administration of 80 mg/kg 2% pentobarbital sodium intraperitoneally, followed by cervical dislocation. Blood samples were collected from the Orbital venous plexus of the mice. Serum alanine aminotransferase (ALT), aspartate am-inotransferase (AST) and biomarkers of oxidative stress were measured. Livers were harvested, weighed, and stored for further histopathological and biochemical analysis, including histopathological changes, ultrastructural changes, biomarkers of oxidative stress, and gene expressions.
2.3. Body Weight, Organ Index and liver Index
Body weights were measured and recorded weekly. At the end of the experiment, brain, heart, liver, kidney, lungs, and spleen of each subject were collected, weighed and photographed. Organ index is calculated by the following formula[23]:
Organ index (%)= Organ weight (mg)/body weight (g) × 100%
2.4. Detection of Serum Levels of ALT and AST
Blood samples were collected from the mice and stored at 4℃ for 2 hours, then centrifuged at 3000 rpm for 10 min. Serum alanine aminotransferase (ALT) and aspartate aminotransferase (AST) levels were measured according to the user’s manual from the manufacture (Nanjing Jiancheng Bioengineering Institute, Nanjing, China).
2.5. Detection of Serum Levels of Oxidative Stress Biomarkers
Blood samples were collected from the mice and left to stand at 4°C for 2 hours, followed by centrifuged at 3000 rpm for 10min to obtain serum. Total superoxide dismutase (T-SOD) activity, total antioxidant capacity (T-AOC), glutathione (GSH) and malondialdehyde (MDA) content were measured by a biochemical reagent kit provided by China Jiancheng Bioengineering Institute (Nanjing, China).
2.6. Detection of Hepatic Oxidative Stress Biomarkers
Liver tissues were rinsed in isotonic saline solution at 4℃, weighed and homogenized in ice-cold isotonic saline solution at a ratio of 1:9 (w/v), followed by centrifugation (3500 rpm, 10 min at 4℃). The suspension was collected for measurement of the concentration of total protein by Bradford protein assay. The hepatic levels of T-SOD, T-AOC, GSH and MDA were detected by a biochemical reagent kit provided by China Jiancheng Bioengineering Institute (Nanjing, China).
2.7. Hepatic Histopathological Changes
The remaining liver tissues were prepared for histopathological examination. The liver tissue was repaired and rinsed with water for 4 h, Alcohol gradient dehydration was performed, and the dissolved paraffin was infiltrated into the tissue blocks, which became hard wax blocks after cooling. The wax blocks were placed on a slicer (Leica, Heidelberg, Germany), cut into 5-μm slices, and transferred to slides. The wax blocks were placed in a temperature box at 60 °C for 2 h and dried, Paraffin sections were immersed in hematoxylin for 5 min, followed by eosin for 2 min, and slides were dehydrated and sealed with neutral resin. Leica DM1000 microscope (Leica, Heidelberg, Germany) was used to observe histopathological changes [24].
2.8. Ultrastructural Changes of Hepatocytes
Samples of liver preserved in glutaraldehyde were taken and ultrathin sections were made according to standard protocols, and for ultrastructural changes examination by a JEM-1400-FLASH Transmission Electron Microscope (Jeol, Japan).
2.9. RNA Extraction and qRT-PCR
Liver samples were stored at -80℃ for RNA extraction. Total liver RNA was extracted by RNAiso Plus (9108, Takara, Otsu, Japan) followed the manufacturer ‘s instructions. cDNA was synthesized simultaneously using 1 ug of RNA with the Prim-Script. TM. RT Reagent Kit (9108, Takara, Japan) and the SYBR Premix Ex Taq. TM. II Kit (9108A, Takara, Japan). The expressions of Nrf2, HO-1, CAT, GSH-Px, and SOD-1 were detected by Real-Time quantitative PCR (Bio-Rad, USA). β-actin was applied as a housekeeping gene for normalization. RNA expression levels were calculated by 2-△△CT method [25]. Primers used in this study were designed by PREMIER 5 (PREMIER Biosoft International, Palo Alto, Calif.) and shown in Table 1.
2.10. Data Statistics and Analysis
All data were analyzed using SPSS 27.0 (SPSS Inc., Chicago, IL, USA). One-way analysis of variance (ANOVA) was used to determine overall differences among groups. All parameters were expressed as mean ± standard deviation. Significance was recognized when P < 0.05.
3. Results
3.1. Body Weight and Liver Index
There were no significant differences of body among groups (P > 0.05). Overall, there were no significant differences of organ indices (P > 0.05) except for liver. The organ index of liver increased significantly in groups of F, LT, and MT (P < 0.05) compared to the control group; however, the organ index of liver in HT group decreased significantly (P < 0.05) compared to group F. The results of body weight and organ indices are shown in Figure 1.
3.2. Serum Levels of ALT and AST
Figure 2 shows the results of serum levels of ALT and AST. The serum levels of ALT and AST in group F were significantly higher compared to the control group (P < 0.05). The serum levels of ALT and AST showed a decreasing trend among treatment groups compared to the group F. The serum levels of ALT and AST decreased significantly in HT group compared to group F (P < 0.05).
3.3. Serum Antioxidant Biomarkers
The results of serum antioxidant biomarkers are shown in Figure 3. The serum levels of T-AOC, T-SOD, and GSH decreased significantly in group F compared to the control group; however, the content of serum MDA significantly increased compared to the control group (P <0.05). Nonetheless, the serum levels of T-SOD and GSH increased significantly in groups of HT and MT, whereas the content of MDA significantly decreased compared to group F (P < 0.05).
3.4. Hepatic Antioxidant Indicators
The results of hepatic antioxidant indicators are shown in Figure 4. The hepatic levels of T-AOC, T-SOD, and GSH in group F decreased significantly compared to the control group; however, the MDA content in group F significantly increased compared to the control group (P < 0.05). The hepatic levels of T-AOC, TSOD, and GSH in groups of MT and HT significantly increased, whereas the contents of MDA significantly decreased compared to group F (P < 0.05).
3.5. Hepatic Histopathological Changes
Figure 5 presents hepatic histopathological changes in this study. The hepatocytes in the control group were found mild degeneration without significant histopathological changes. (Figure 5A,B). In group F, dilatations of the central veins and hepatic sinusoids, disoriented hepatic cordsfatty changes and necrosis with descent amount of inflammatory cells infiltration were observed (Figure 5C,D). The histopathological changes indicate a successful fluoride-induced hepatopathy. The histopathological changes were found alleviated in treatment groups, especially in groups MT and HT (FIG. 5 G-J).
3.6. Hepatic Ultrastructural Changes
Hepatic ultrastructural changes are shown in Figure 6. In the control group, the nuclei of hepatocytes were complete without nuclear deformation and nuclear rupture. Organelles, including mitochondria, ribosomes, endoplasmic reticulum, and lysosomes were intact within the cytoplasm. The rough endoplasmic reticulum (RER) affirmed in layers. There no evidences of mitochondrial swelling or rupture (Figure 6A). In group F, hepatocytes showed significant pathological changes, such as deformed or ruptured nuclei, lipid droplets deposited within the cytoplasm, mitochondria swelling, sharp fracture, dissolution, whitish areas, and increased lysosomes (Figure 6B). However, the pathological changes were mitigated all TPM treatment groups, especially in HT group (Figure 6C–E).
3.7. mRNA Expressions
The effects of TMP treatment on Nrf2 expressions are shown in Figure 7. The expressions of CAT, GSH-Px, and SOD decreased significantly in group F compared to the control group (P < 0.05). The expressions of Nrf2, HO-1, CAT, GSH-Px, and SOD in groups of MT and HT were significantly higher than that of group F (P < 0.05).
4. Discussion
Fluorine is a nature element in the environment and fluoride has been used extensively in daily life, such as sewage treatment. However, excessive exposure to fluoride lead to fluorosis, resulting in severe hepatopathy. Fluorosis-induced hepatopathy has been reported associate with reactive oxygen species (ROS) activate oxidative stress. Excess ROS cause cellular damage due to oxidative stress reactions [26]. TMP is an active ingredient of a traditional Chinese medicine, extracted from chuanxiong, which has been reported to be an effective antioxidant and anti-inflammatory agent. TMP has been used to treat liver issues, such as ischemia-reperfusion injury, hepatic fibrosis, septic liver injury, and so on [19,20,27].
The results of the current study revealed that overdose of fluoride induced liver damages. The serum levels of alanine aminotransferase (ALT) and aspartate aminotransferase (AST) are two important intracellular biomarkers to assess liver function [25]. The serum levels of ALT and AST increase during hepatocytes injuries due to increased permeability of cell membrane [28,29]. T-SOD is an antioxidant which effectively scavenges free radicals and alleviates cellular oxidative damages. GSH is another antioxidant synthesized in low-molecular-weight cells which inhibits the production of free radicals. Nonetheless, MDA is an indicator of lipid peroxidation and indirectly reflects the increase in contents of free radicals during oxidative stress. Furthermore, T-AOC represents the total antioxidant capacity of the body [30,31]. When oxidative stress is in progress, reactive oxygen species (ROS) activate the chain reactions of antioxidants, leading to elevation of the amount T-SOD and GSA, and reduction of the level of T-AOC. Meanwhile, the serum content of MDA increased. The results of this study are in line with the ROS-triggered antioxidant chain reactions after fluoride-challenged hepatopathy. After fluoride challenged, the serum levels of ALT, AST, and MDA increased significantly; however, the serum levels of T-SOD, GSH, and T-AOC decreased significantly, which in accordance with previous studies [14,30,32]. Among treatment groups, especially in groups of MT and HT, the levels of T-SOD, GSH, and T-AOC increased; whereas the content of MDA decreased, which suggested that the intervention of TMP alleviated the fluoride-induced oxidative stress and hepatic injury.
Histopathological changes directly reflect the cellular damages, which is helpful to evaluate the severity of organ damages. The severity of hepatocytes damages predisposes the progress of ROS associated damages. The results of this study showed that fluoride induced hepatopathy because of significant observation of hepatocyte vacuolation and swollen mitochondria, indicating severe ongoing oxidative stress after fluoride challenges. The findings in this study are consistent with previous reports [23,33,34]. The interventions of different dosages of TMP alleviated the severity of hepatocytes damages in the current study, especially in groups of MT and HT. The morphologies of hepatocytes, including mitochondria, in these groups were relatively normal compared to group F, indicating the potential protection of TPM on fluoride-induced hepatopathy.
Nuclear factor E2-related factor 2 (Nrf2) is ubiquitous in mammalian cells, which combines to antioxidant counter-response factors and triggers the transcription and expression of antioxidant enzymes such as SOD, GSH-Px, etc.; however, which is inhibited during oxidative stress. Nrf2 has been reported involvement in regulating oxidation balance and protecting antioxidant and phase II detoxification reactions in organisms [35]. The expressions of Heme oxygenase-1 (HO-1) is regulated by Nrf2, which promotes heme degradation. Physiologically, the expression of Nrf2 is regulated Keap1 protein in cytoplasm; however, Nrf2 is uncoupled from Keap1 and rapidly translocated to nucleus when oxidative stress occurs, in terms of Nrf2-dependent cellular defense mechanism which activates the transcriptions of HO-1, SOD, CAT, and GSH-Px in order to enhance cellular antioxidant capacities. Nrf2/HO-1 signaling pathway is critical in improving the capability of organisms to defense oxidative stress induced cellular damages, which has been recognized a most important endogenous antioxidant signaling pathway in mammalians [36]. The results of the current study showed that the hepatic mRNA expressions of Nrf2 and HO-1 increased concurrently with decreased expressions of SOD and CAT decreased in group F, suggesting that acute excessive fluoride intake led to oxidative stress and compromise the ability to scavenge free radicals. Previous studies have shown that fluorosis activates Keap1-Nrf2 signaling pathway to prevent oxidative stress induced hepatic or renal injuries in chronic fluorosis rats [1,14]; Nevertheless, fluoride-induced oxidative stress promotes the expressions of intracellular ROS, inducing peroxiredox-dependent unfolded protein response and triggering the autophosphorylation of Nrf2 [37], which reduces the expression of downstream genes of Nrf2 pathway and exacerbates oxidative stress induced hepatopathy. According to the results of this study, the expressions of genes associated with Nrf2 pathway in the liver are enhanced by the TMP, suggesting that TMP is effective to promotes the expressions of the Nrf2 pathway associated genes by activating the Nrf2/HO-1 signal pathway and facilitate elimination of excessive ROS in fluoride-induced hepatopathy mice. The finding is consistent with previous studies [19,20,38,39]. Furthermore, it has been reported that TMP improves the expressions of Nrf2 pathway associated genes in Nrf2 gene knockout mice [40].
5. Conclusions
In conclusion, TMP ameliorates fluoride-induced hepatopathy in male ICR mice by promoting the expressions of Nrf2 pathway, enhancing the hepatic levels of SOD and GSH, and reducing the hepatic level of MDA; the intervention of TMP overall enhances hepatic antioxidant capacity. The result of the current study helps to understand the pathophysiological changes of fluoride-induced hepatopathy and the basic mechanism of actions of TMP in alleviating fluoride-induced hepatopathy. However, the detailed mechanism of actions of TMP in treating fluoride-induced hepatopathy needs to be explored further.
References
- Zou J. Alteration of liver oxidative stress injury and Keap1-Nrf2 signaling pathway in rats with chronic fluorosis and screening of antioxidant activity of botanical extracts[D]. Guizhou Medical University, 2022.
- Kerdoun M A, Mekhloufi S, Adjaine O, et al. Fluoride concentrations in drinking water and health risk assessment in the south of Algeria[J]. Regul Toxicol Pharmacol, 2022, 128, 105086. [CrossRef]
- Srivastava S, Flora S. Fluoride in Drinking Water and Skeletal Fluorosis: a Review of the Global Impact[J]. Curr Environ Health Rep, 2020, 1, 140-146. [CrossRef]
- Patil M M, Lakhkar B B, Patil S S. Curse of Fluorosis[J]. Indian J Pediatr, 2018, 1, 375-383. [CrossRef]
- Boone J S, Vigo C, Boone T, et al. Per- and polyfluoroalkyl substances in source and treated drinking waters of the United States[J]. Sci Total Environ, 2019, 653, 359-369. [CrossRef]
- Kabore H A, Vo D S, Munoz G, et al. Worldwide drinking water occurrence and levels of newly-identified perfluoroalkyl and polyfluoroalkyl substances[J]. Sci Total Environ, 2018,616-617:1089-1100. [CrossRef]
- Riddell J K, Malin A J, McCague H, et al. Urinary Fluoride Levels among Canadians with and without Community Water Fluoridation[J]. Int J Environ Res Public Health, 2021,18(12). doi: 10.3390/ijerph18126203.
- U.S. Public Health Service Recommendation for Fluoride Concentration in Drinking Water for the Prevention of Dental Caries. Public Health Reports. 2015, 1, 318-331. [CrossRef]
- Ren C, Li H H, Zhang C Y, et al. Effects of chronic fluorosis on the brain[J]. Ecotoxicol Environ Saf, 2022, 244, 114021. [CrossRef]
- Kan P.J., Yao X.W., Wang W. Overview of research on drugs for the treatment of endemic fluorosis[J]. Endemic disease control in China, 2022, 1, 385-386.
- Gong Y, Zheng D, Chen FP, et al. Current status of endemic fluorosis and forensic identification[J]. China Forensic Identification, 2022(02):35-40.
- Chen QX, Jiang SH, Zhu J. Current status of research on the therapeutic effects of Chinese medicine on endemic fluorosis[J]. Endemic disease control in China, 2021, 1, 215-216.
- Wang L, Wei W, Xiao Q, et al. Farrerol Ameliorates APAP-induced Hepatotoxicity via Activation of Nrf2 and Autophagy[J]. Int J Biol Sci, 2019, 1, 788-799. [CrossRef]
- Wang D, Yin K, Zhang Y, et al. Novel pathways of fluoride-induced hepatotoxicity: P53-dependent ferroptosis induced by the SIRT1/FOXOs pathway and Nrf2/HO-1 pathway[J]. Comp Biochem Physiol C Toxicol Pharmacol, 2023, 264, 109526.
- Yang R, Zhao YQ, Zhang Q. Research progress of fluorosis on liver system damage[J]. China Endemic Disease Control, 2022, 1, 198-199.
- Tian X L , Feng J , Dong N S , et al. Subchronic exposure to fluoride and arsenite induces oxidative stress and activates the Nrf2 signaling pathway in the kidneys of rat offspring[J]. Science of The Total Environment, 2019, 686. [CrossRef]
- Zhou X, Sun XY, Jia LY, et al. Research progress on the application and mechanism of the Chinese medicine monomer Tetramethylpyrazine in the treatment of diseases[J]. Shaanxi TCM, 2022, 1, 541-544.
- AlKreathy H M, Alghamdi M K, Esmat A. Tetramethylpyrazine ameliorates indomethacin-induced gastric ulcer in rats: Impact on oxidative, inflammatory, and angiogenic machineries[J]. Saudi Pharm J, 2020, 1, 916-926. [CrossRef]
- Xiao L, Mei GC, Wu LH, et al. Study on the protective effect of Danshen TMP injection on acute liver injury in young rats with sepsis[J]. Chinese Traditional Chinese Medicine Emergency, 2019, 1, 1585-1589.
- Feng L, Zhao J. Effect of Tetramethylpyrazine hydrochloride injection on hepatic ischemia-reperfusion injury through Nrf2/HO-1 pathway[J]. Modern Drugs and Clinics, 2023, 1, 22-28.
- Wang w.y., Gui c.z., Guan z.z.. Research progress of antagonists for fluorosis[J]. Occupational and Health, 2021, 1, 2433-2435.
- Zhou HJ, Li JS, Sun YM. Effects of acute fluorosis on nitric oxide synthase protein expression in mouse cerebral cortex[J]. Journal of Environment and Health, 2008(05):445-446.
- Li X, Yang J, Liang C, et al. Potential Protective Effect of Riboflavin Against Pathological Changes in the Main Organs of Male Mice Induced by Fluoride Exposure[J]. Biol Trace Elem Res, 2022, 1, 1262-1273. [CrossRef]
- Li Y, WANG Z, LI J, et al. Sodium Butyrate Ameliorates Fluorosis-Induced Neurotoxicity by Regulating Hippocampal Glycolysis In Vivo[J]. Biological Trace Element Reserch, 2023. [CrossRef]
- Kong D, Chen L, Huang W, et al. Combined therapy with ligustrazine and paeonol mitigates hepatic fibrosis through destroying mitochondrial integrity of stellate cell[J]. Am J Transl Res, 2020, 1, 1255-1266.
- Zhao Y, Wang J, Zhang J, et al. Fluoride exposure induces mitochondrial damage and mitophagy via activation of the IL-17A pathway in hepatocytes[J]. Sci Total Environ, 2022, 804, 150184. [CrossRef]
- Yang Y, Xu QY, Huang M, et al. The relationship between TNFR2 and immune liver injury in trichloroethylene sensitized mice[J]. Journal of Anhui Medical University, 2021, 1, 602-607.
- Lehmann-Werman R, Magenheim J, Moss J, et al. Monitoring liver damage using hepatocyte-specific methylation markers in cell-free circulating DNA[J]. JCI Insight, 2018,3(12). [CrossRef]
- Wang G W, Zhang X L, Wu Q H, et al. The hepatoprotective effects of Sedum sarmentosum extract and its isolated major constituent through Nrf2 activation and NF-kappaB inhibition[J]. Phytomedicine, 2019, 53, 263-273. [CrossRef]
- Obradovic D, Andjelic T, Ninkovic M, et al. Superoxide dismutase (SOD), advanced oxidation protein products (AOPP), and disease-modifying treatment are related to better relapse recovery after corticosteroid treatment in multiple sclerosis[J]. Neurol Sci, 2021, 1, 3241-3247. [CrossRef]
- Wang L. Effect of different doses of calcium on liver injury in fluorosis rats[D]. Shanxi Agricultural University, 2019. [CrossRef]
- Chen WJ, Wu LW, Peng JY, et al. Protective effect of Xiao Chai Hu Tang on liver injury caused by chronic fluorosis in rats[J]. China Hospital Drug Evaluation and Analysis, 2022, 1, 277-280.
- Zhang Z, Zhou B, Wang H, et al. Maize purple plant pigment protects against fluoride-induced oxidative damage of liver and kidney in rats[J]. Int J Environ Res Public Health, 2014, 1, 1020-1033. [CrossRef]
- Zhou B H, Wei S S, Jia L S, et al. Drp1/Mff signaling pathway is involved in fluoride-induced abnormal fission of hepatocyte mitochondria in mice[J]. Sci Total Environ, 2020, 725, 138192. [CrossRef]
- Chan B, Elmasry M, Forootan S S, et al. Pharmacological Activation of Nrf2 Enhances Functional Liver Regeneration[J]. Hepatology, 2021, 1, 973-986. [CrossRef]
- Zhang XQ, Yang H, Zhang XH. Study of Nrf2/HO-1 signaling pathway in chronic liver disease[J]. Chinese Journal of Liver Disease (Electronic Version), 2017, 1, 36-39.
- Jiang L, Rui YJ, Dai JQ, et al. Effects of tanshinone IIA on hydrogen peroxide-induced apoptosis and oxidative stress in human lens epithelial cells[J]. New Advances in Ophthalmology, 2021, 1, 838-842. [CrossRef]
- Lu C, Xu W, Shao J, et al. Nrf2 Activation Is Required for Ligustrazine to Inhibit Hepatic Steatosis in Alcohol-Preferring Mice and Hepatocytes[J]. Toxicol Sci, 2017, 1, 432-443. [CrossRef]
- Chen JQ, Zhao L, Ding XH, et al.Ligustrazine inhibits high glucose-induced neutrophil extracellular capture network formation by regulating NRF2/HO-1 pathway [J].Journal of Army Medical University, 2022, 44 (21):2157-2164.
- Lu C, Xu W, Zhang F, et al. Nrf2 knockdown attenuates the ameliorative effects of ligustrazine on hepatic fibrosis by targeting hepatic stellate cell transdifferentiation[J]. Toxicology, 2016, 365, 35-47. [CrossRef]
Figure 1.
Body weight and organ indices. (A) Body weight of mice; (B) Organ indices; (C) Organ index of liver. Data are presented as mean ± SD. Different alphabets indicate statistically significant differences among groups (P < 0.05). K: control group; F: model group; LT, low-dose TMP group; MT, medium-dose TMP group; HT, high dose TMP group.
Figure 1.
Body weight and organ indices. (A) Body weight of mice; (B) Organ indices; (C) Organ index of liver. Data are presented as mean ± SD. Different alphabets indicate statistically significant differences among groups (P < 0.05). K: control group; F: model group; LT, low-dose TMP group; MT, medium-dose TMP group; HT, high dose TMP group.
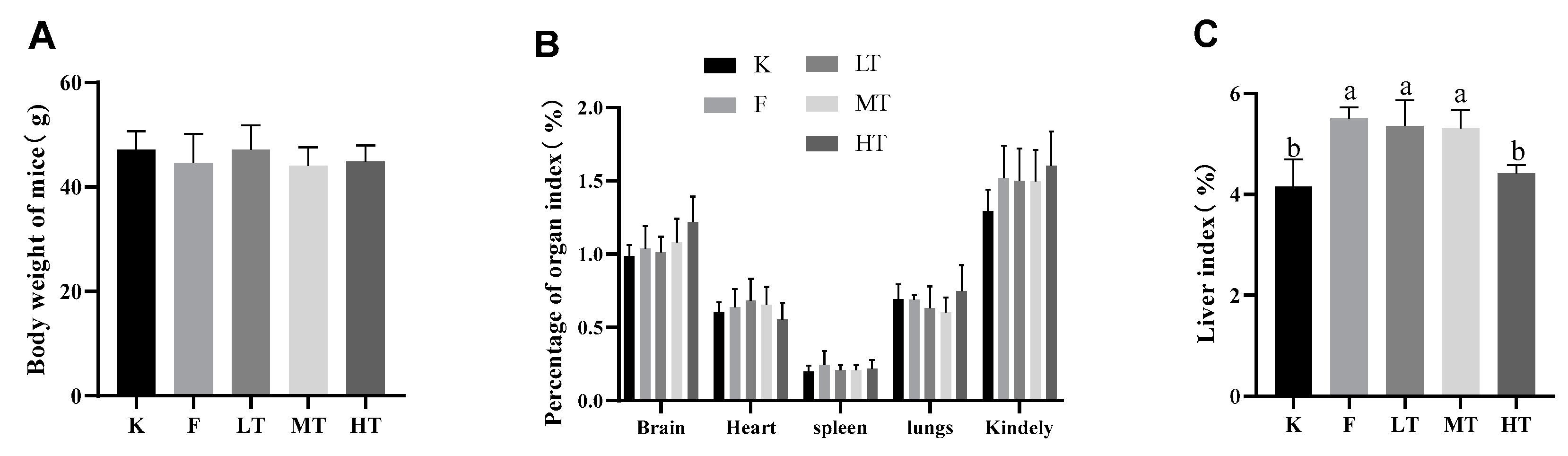
Figure 2.
| Serum levels of ALT and AST. (A) serum level of ALT; (B) serum level of AST. Different alphabets indicate statistically significant differences among groups (P < 0.05).
Figure 2.
| Serum levels of ALT and AST. (A) serum level of ALT; (B) serum level of AST. Different alphabets indicate statistically significant differences among groups (P < 0.05).
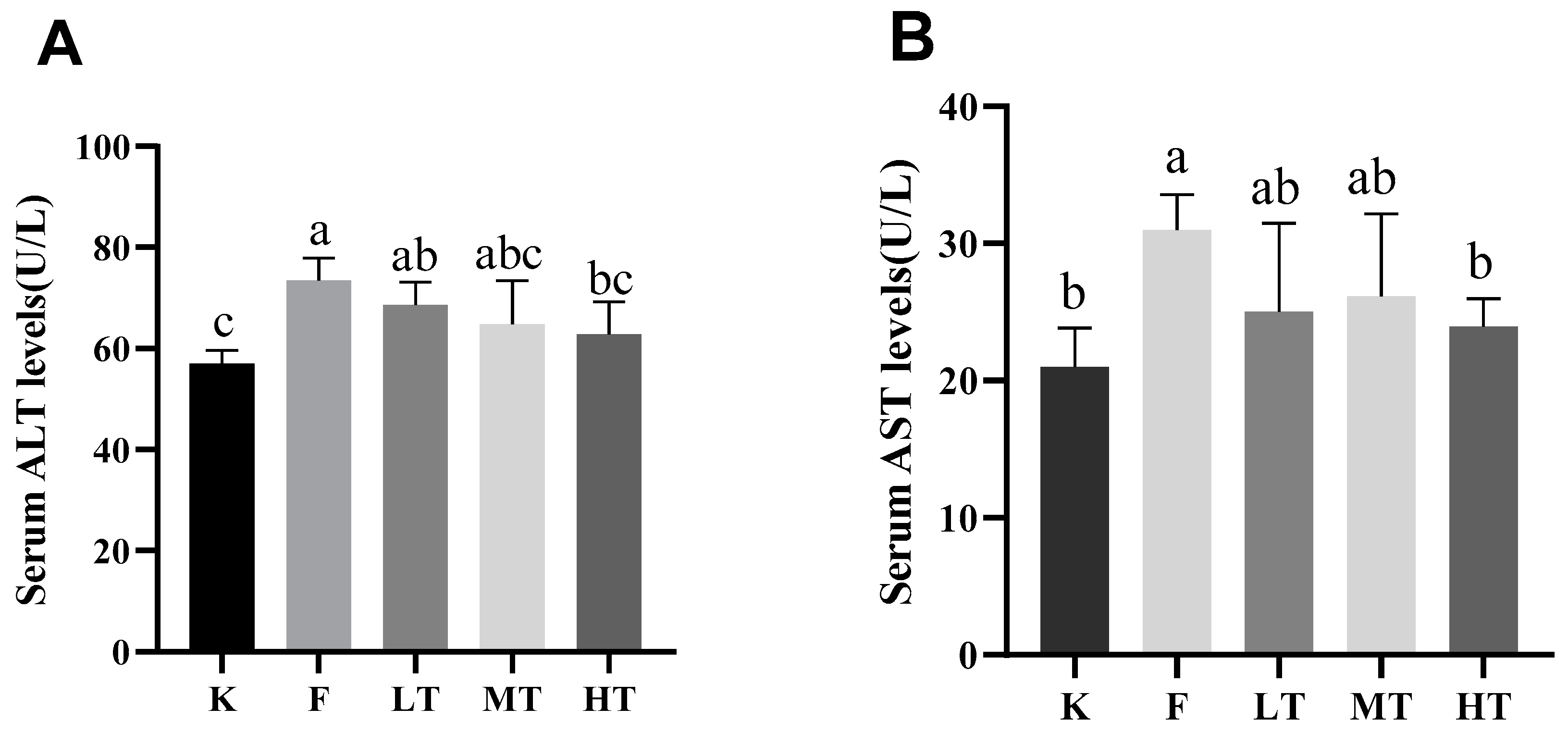
Figure 3.
Serum antioxidant enzyme activity and oxidative concentration. (A) total antioxidant capacity T-AOC; (B) superoxide dismutase T-SOD; (C) Glutathione (GSH); (D) Malondialdehyde (MDA). Different alphabets indicate statistically significant differences among groups (P < 0.05).
Figure 3.
Serum antioxidant enzyme activity and oxidative concentration. (A) total antioxidant capacity T-AOC; (B) superoxide dismutase T-SOD; (C) Glutathione (GSH); (D) Malondialdehyde (MDA). Different alphabets indicate statistically significant differences among groups (P < 0.05).
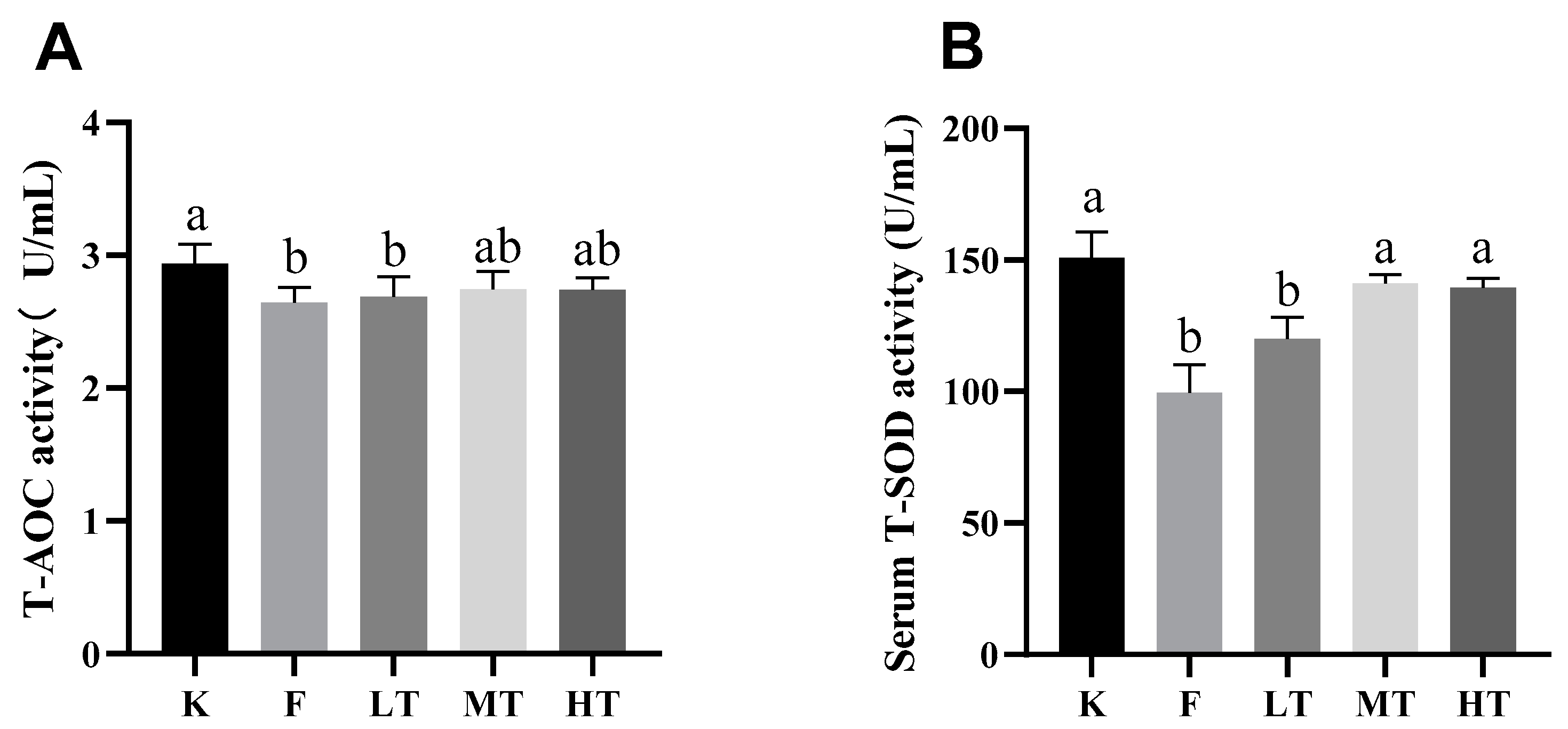
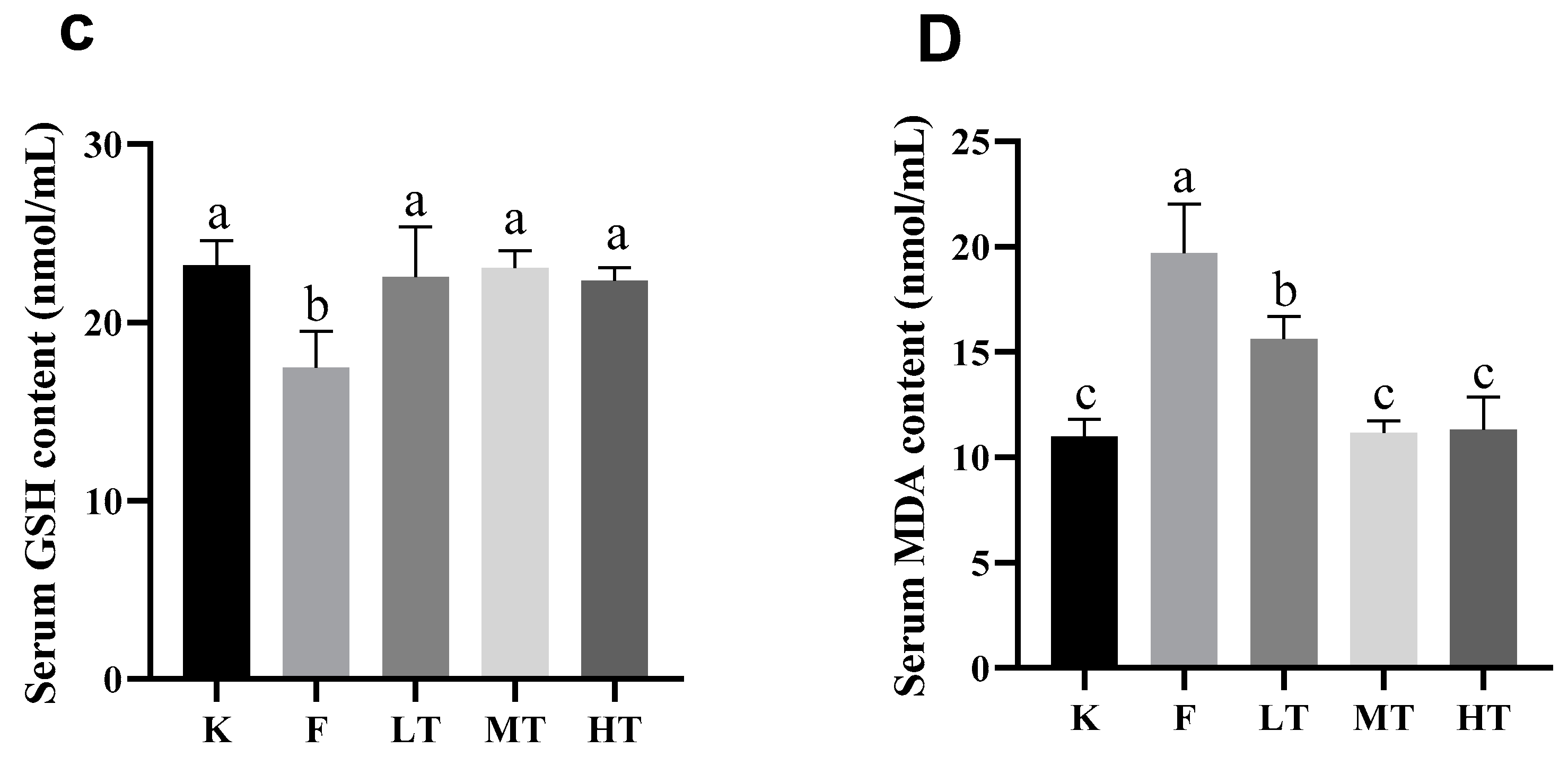
Figure 4.
Liver antioxidant index results. (A) total antioxidant capacity T-AOC; (B) superoxide dismutase T-SOD; (C) glutathione GSH; (D) MDA. Different alphabets indicate statistically significant differences among groups (P < 0.05).
Figure 4.
Liver antioxidant index results. (A) total antioxidant capacity T-AOC; (B) superoxide dismutase T-SOD; (C) glutathione GSH; (D) MDA. Different alphabets indicate statistically significant differences among groups (P < 0.05).
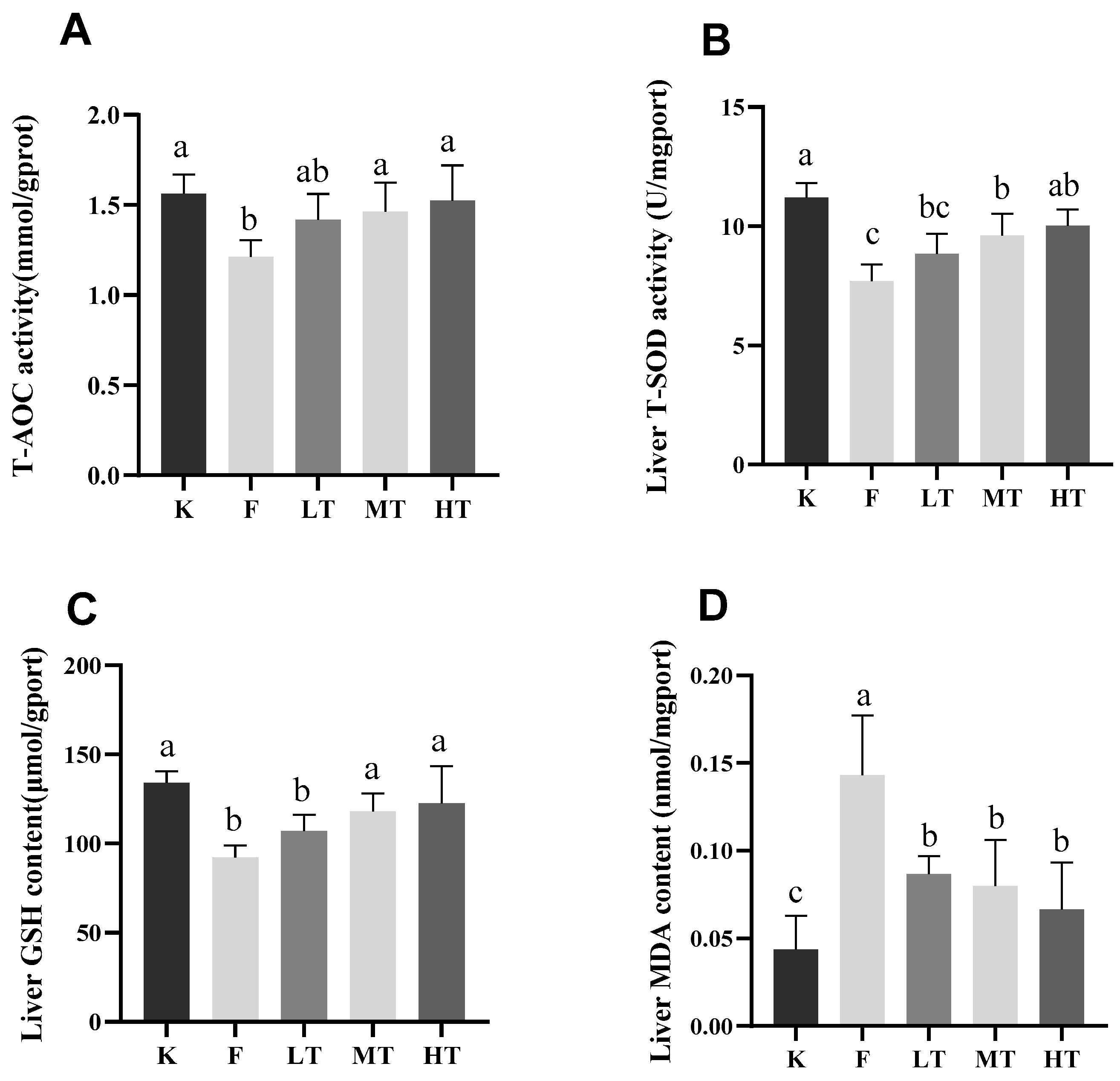
Figure 5.
Liver morphology, left magnification: 50 µ m, 200×;Right magnification: 20 µ m, 400 ×. (A, B) is the liver degeneration of the control group. (C, D) shows the changes in the liver of the model group. (E, F) indicates the changes of liver in low dose TMP group. (G, H) represents the changes of liver in the middle dose TMP group. (I, J) indicates the liver changes in high-dose TMP group. Black arrow: nuclear pyknosis; Blue snip: nuclear lysis; Yellow arrow: indicates neutrophil infiltration.
Figure 5.
Liver morphology, left magnification: 50 µ m, 200×;Right magnification: 20 µ m, 400 ×. (A, B) is the liver degeneration of the control group. (C, D) shows the changes in the liver of the model group. (E, F) indicates the changes of liver in low dose TMP group. (G, H) represents the changes of liver in the middle dose TMP group. (I, J) indicates the liver changes in high-dose TMP group. Black arrow: nuclear pyknosis; Blue snip: nuclear lysis; Yellow arrow: indicates neutrophil infiltration.
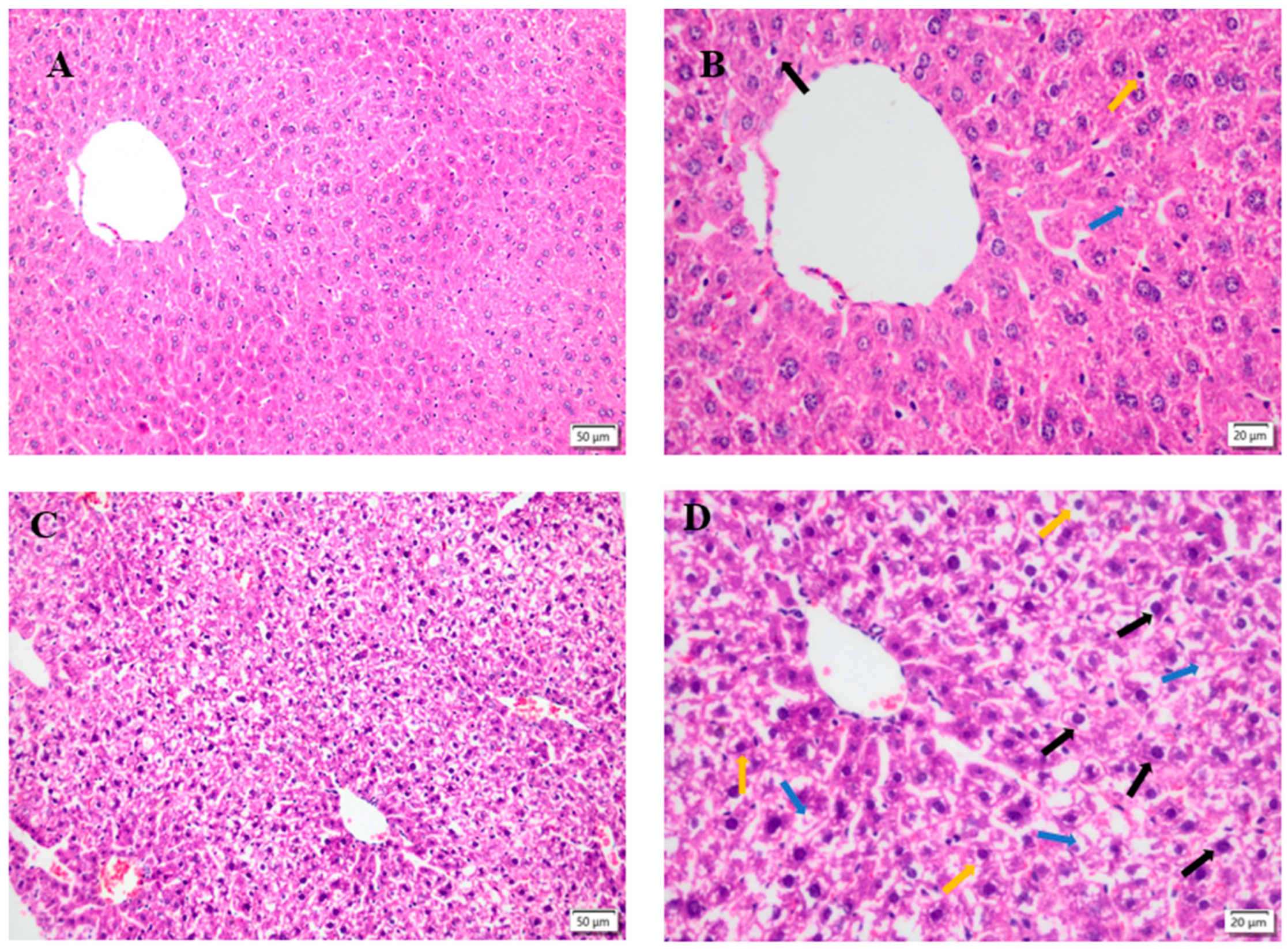
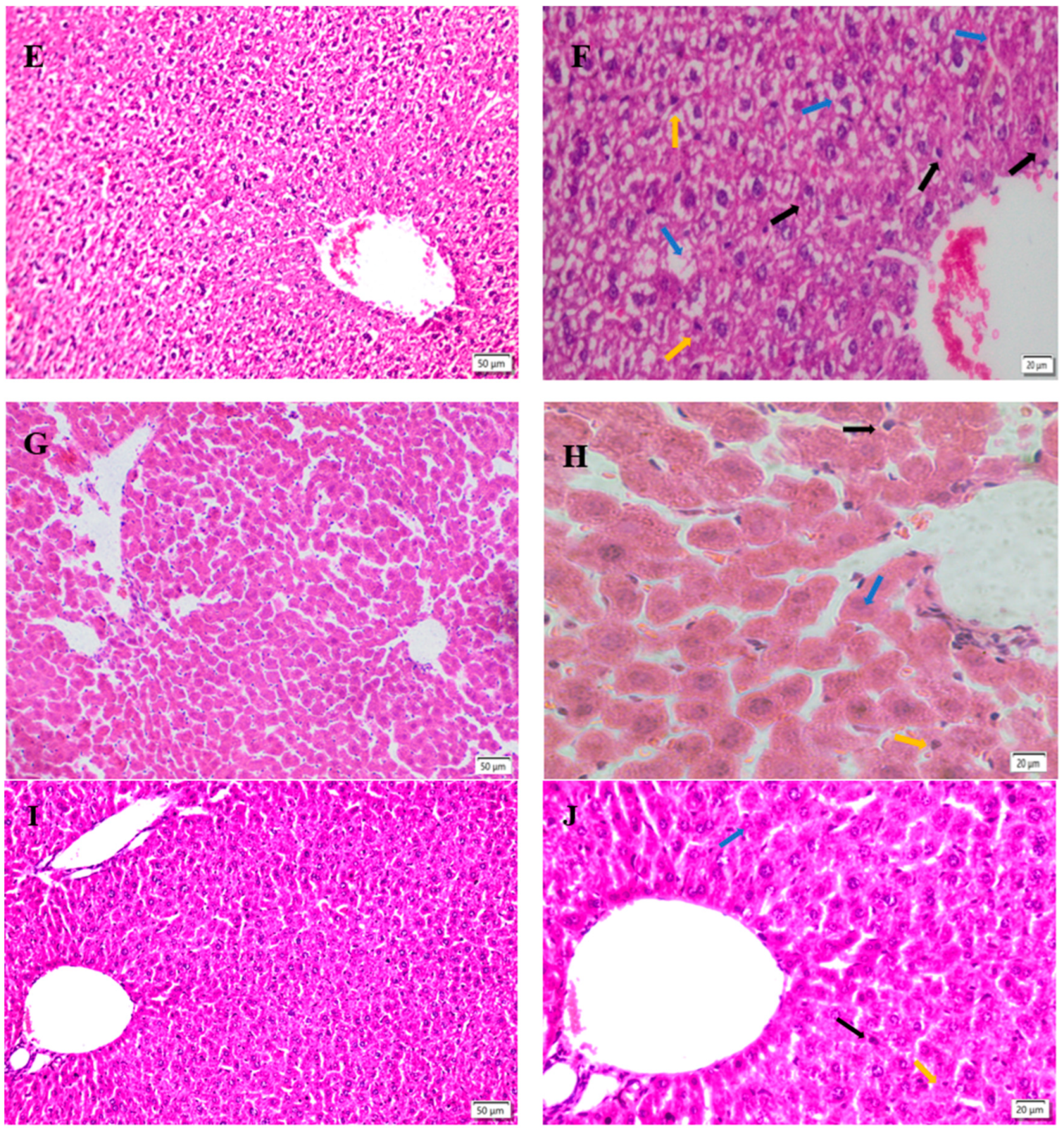
Figure 6.
Ultrastructural image of liver, magnification: 1 µm, 15000X. MC: mitochondria; CRN: nucleus; REN: rough endoplasmic reticulum; LYS: Lysosomes. (A) is that structure of hepatocyte in the control group. (B) It shows the structure of hepatocytes in model group. (C) It is the structure of liver cells in low dose TMP group. (D) It represents the structure of liver cells in middle dose TMP group. (E) The structure of liver cells in high dose TMP group.
Figure 6.
Ultrastructural image of liver, magnification: 1 µm, 15000X. MC: mitochondria; CRN: nucleus; REN: rough endoplasmic reticulum; LYS: Lysosomes. (A) is that structure of hepatocyte in the control group. (B) It shows the structure of hepatocytes in model group. (C) It is the structure of liver cells in low dose TMP group. (D) It represents the structure of liver cells in middle dose TMP group. (E) The structure of liver cells in high dose TMP group.
Figure 7.
The relative expression of Nrf2, HO-1, CAT, GSH-Px, SOD mRNA in the liver was measured. (A) Nrf2, (B) HO-1, (C) CAT, (D) GSH-Px, (E) SOD. Different alphabets indicate statistically significant differences among groups (P < 0.05).
Figure 7.
The relative expression of Nrf2, HO-1, CAT, GSH-Px, SOD mRNA in the liver was measured. (A) Nrf2, (B) HO-1, (C) CAT, (D) GSH-Px, (E) SOD. Different alphabets indicate statistically significant differences among groups (P < 0.05).
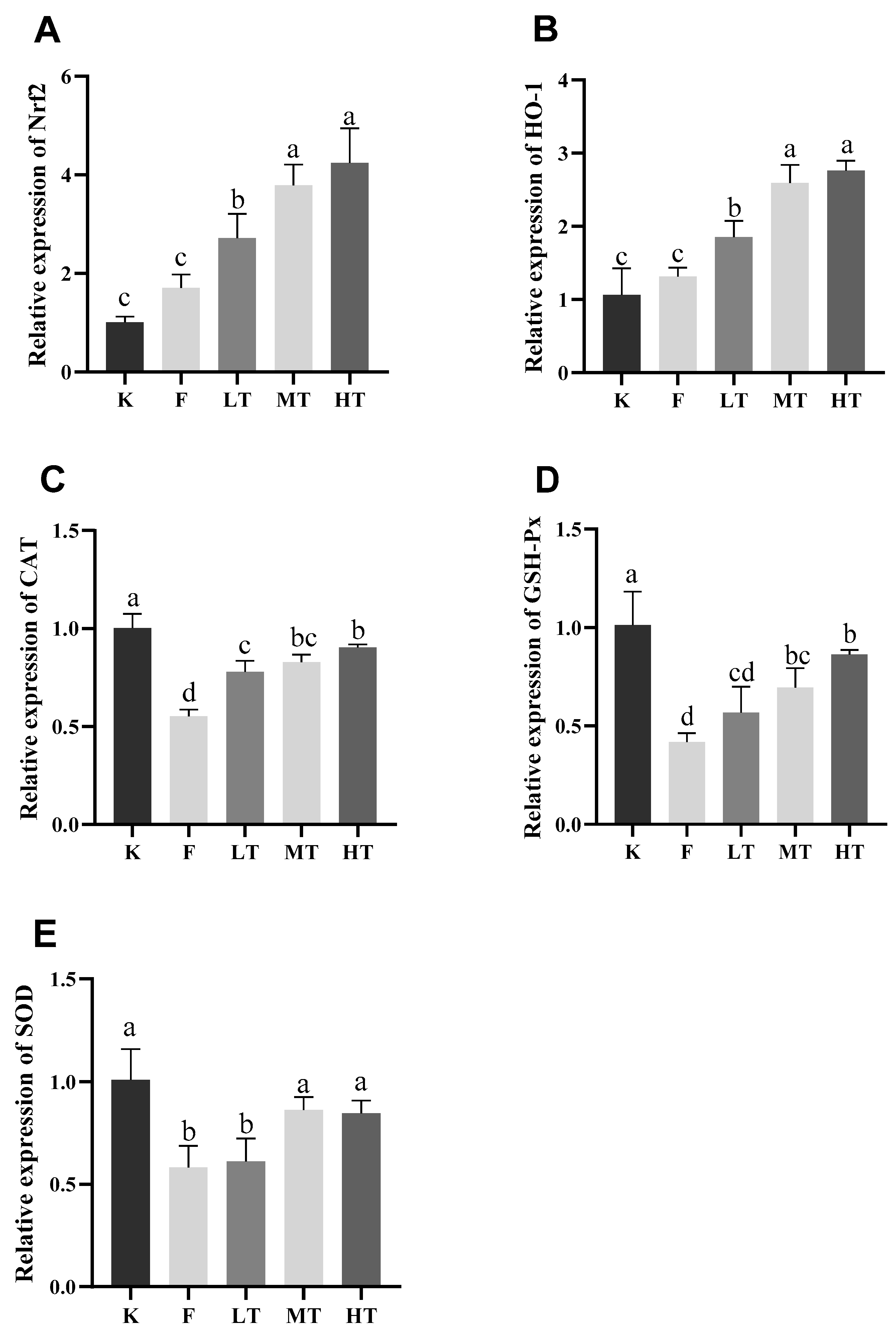

Table 1.
qRT-PCR Primer Sequence Listing.
| Gene | Accession number | Primer sequence (5′-3′) | Product length(bp) |
|---|---|---|---|
| Nrf2 | NM-010902.4 | F: AGCGGTAGTATCAGCCAR: GCCCAGTCCCTCAATAGC | 150 |
| HO-1 | NM-010442.2 | F: TGTTGCGCTCTATCTCCR: GTACACATCCAAGCCGAG | 136 |
| CAT | NM-009804.2 | F: TTCCTGAGCAAGCCTTCR: CACATGAATGGCTATGGATCACA | 138 |
| GSH-Px | NM-008160.6 | F: TCTCTTCATTCTTGCCATR: GACTACACCGAGATGAACGA | 112 |
| SOD1 | NM-011434.2 | F: CACCTTTGCCCAAGTCAR: TCCATTGAAGATCGTGT | 97 |
| β-Actin | NM-007393 | F: CGCTCGTTGCCAATAGTGR: GCTGTGCTATGTTGCTCTAG | 117 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



