
Submitted:
09 May 2023
Posted:
10 May 2023
You are already at the latest version
Abstract
Background: Low-level (LLLT) and high-intensity laser therapy (HILT) can be beneficial additions to knee osteoarthritis (KOA) rehabilitation exercises; however, it is still being determined which modality is more effective. Aim: To compare the effects of LLLT and HILT as adjuncts to rehabilitation exercise (LL+EX and HL+EX) on clinical outcomes in KOA. Methods: Thirty-four adults with mild to moderate KOA were randomly allocated to either LL+EX (n = 17) or HL+EX (n = 17) groups. All participants underwent their designated laser treatment combined with rehabilitation exercises weekly for twelve consecutive weeks. The Knee Injury and Osteoarthritis Outcome Score (KOOS), Numerical Pain Rating Scale (NPRS), active knee flexion, and Timed Up-and-Go test (TUG) were assessed at baseline and immediately post-intervention. Results: Post-intervention, both groups significantly improved their KOOS, NPRS, active knee flexion, and TUG scores compared to baseline (p < 0.01). The mean difference of change in KOOS, NPRS, and active knee flexion scores for the HL+EX group surpassed the minimal clinically important difference threshold. In contrast, the LL+EX group only demonstrated clinical significance in NPRS scores. Conclusions: Incorporating HILT as an adjunct to usual KOA rehabilitation led to significantly higher improvements in pain, physical function, and knee-related disability compared to LLLT.
Keywords:
high-intensity laser
; knee osteoarthritis
; low-level laser
; pain
; photobiomodulation
; rehabilitation
1. Introduction
Knee osteoarthritis (KOA) is a global public health concern and one of the leading causes of physical impairment and disability worldwide [1,2]. As there are currently no single disease-modifying interventions for KOA [3], conservative treatments such as pharmacological therapy and rehabilitation exercises have often been complemented with physical electro-modalities to optimize treatment outcomes [4]. These include low-level (LLLT) [5,6] and high-intensity laser therapy (HILT) [7,8], therapeutic ultrasound, and transcutaneous electrical nerve stimulation [9]. In recent years, photobiomodulation therapy, specifically LLLT and HILT have emerged as the most promising modalities [4,8,10], as both can reduce pain and inflammation [6,7], augment tissue repair [11,12], increase blood circulation [13], and improve physical function and performance [6,7]. Since previous trials had predominantly evaluated either LLLT or HILT without comparing them directly [14,15], it remains unclear which modality is more effective in treating KOA [6,8,16].
Photobiomodulation therapy is a non-invasive electro-modality that utilizes therapeutic doses of light to target injured or dysfunctional tissue, activating photo-biological mechanisms for pain relief and tissue healing [11,12]. It is theorized that the laser energy (photons) is absorbed by the tissue and cells, initiating cellular mitochondrial oxidative reactions that yield adenosine triphosphate (essential for optimal cell metabolism and healing), modulate low-level reactive oxygen species, and release nitric oxide as a potent vasodilator to reduce pain and inflammation [11,12]. Low-level laser therapy (< 500 mW) was first investigated on KOA by Gur et al. (2003) [17]. High-intensity laser therapy is an advanced form of laser therapy which delivers higher energy output (greater than 500 mW), deeper tissue penetration (up to 15 cm), and is capable of inducing superficial hyperthermia (photothermic effects) [11,18]. These enhance oxidative processes and increase ATP synthesis in less time than LLLT [11,18]. Additionally, HILT with wavelengths over 1064 nm, has been demonstrated to target nerve endings directly, providing immediate pain relief [8,11]. Due to its greater anti-inflammatory, bio-stimulation, and photothermic advantages, HILT is considered more promising than LLLT for the treatment of KOA [4,11,16]. Moreover, single-treatment clinical trials (indirect comparison) and meta-analysis suggest HILT is more effective than LLLT [16]. However, a direct comparison between LLLT and HILT on KOA outcomes is lacking to support this supposition.
Kheshie et al. (2014) is one of the few studies to date that compared the effects of HILT and LLLT as an adjunct to KOA rehabilitation, concluding that HILT was more effective in improving KOA outcomes [19]. Argumentatively, the study's small sample size, which only included male participants, and the reliance solely on patient-reported outcomes (VAS and WOMAC) limit the generalizability of its findings; considering the fact that KOA is more prevalent in females [1]. Moreover, patient-reported outcome measures may be challenged due to potential subjective and biased interpretations [20]. Thus, a randomized trial using robust research methods is warranted to distinguish the clinical effects of LLLT and HILT.
To sum up, current clinical evidence for comparing the effects of LLLT and HILT in treating KOA is limited due to methodological issues such as single-treatment clinical trials, single-sex participants, reliability and validity of outcome measures, and meta-analysis. As such, this study was designed to compare the clinical effects of LLLT and HILT as adjunctive treatment to rehabilitation exercise on pain, function, and disability levels in adults with mild to moderate KOA. The findings of this study could provide a valid justification for including laser therapies as a mainstream management option for KOA and enable health professionals to select the most efficient modality (LLLT or HILT) for optimal outcomes. It was hypothesized that HILT would provide better clinical outcomes than LLLT as an adjunctive treatment for KOA.
2. Materials and Methods
2.1. Study Design
This study was a randomized, double-blinded (participants and outcomes assessor), parallel-group clinical trial.
2.2. Ethical Approval and Registration
The study protocol was approved by the Medical Research Ethics Committee of Universiti Malaya Medical Centre (MREC UMMC ID: 2020102-9129) in accordance with the Declaration of Helsinki (1975). The study protocol has been prospectively registered with the Australian New Zealand Clinical Trials Registry (ACTRN12621001694808) and the National Medical Research Register of the Ministry of Health Malaysia (NMRR-21-86-58301).
2.3. Study Population and Setting
Patients with symptomatic mild to moderate KOA were screened and recruited from the Sports Medicine Clinic of UMMC. Eligible KOA patients were invited to participate in this study based on the following inclusion and exclusion criteria.
2.3.1. Inclusion
Aged 18 years and above, diagnosed with unilateral or bilateral KOA based on the American College of Rheumatology criteria, categorised as mild to moderate KOA according to the Kellgren-Lawrence radiographic classification, and presented with knee pain; if both knees were affected, the knee with the worse symptoms was included in the outcome assessment.
2.3.2. Exclusion
(i) Recent intra-articular knee injection; less than six months, (ii) any other pathological conditions such as rheumatic disease, hip or knee joint replacements, congenital dysplasia, septic arthritis, ligament or meniscus injury, plica syndrome, and Baker's cyst, or (iii) those with comorbidities that would prevent participation in the intervention or physical evaluation.
2.4. Sample Size Calculation
The sample size was estimated using the G*Power software version 3.1.9.7. The calculation was based on a minimal clinically important difference (MCID) of 11 points for the Knee Injury and Osteoarthritis Outcome Score (KOOS) as the primary outcome [21], assuming pre-specified power of 90%, an effect size of 0.3, an alpha level of 5%, and a possible dropout rate of 15% [22,23]. Thus, the required total sample would be 34, with 17 participants per group.
2.5. Procedures
Patients with mild to moderate KOA were recruited via simple random sampling. Eligible participants received verbal and written information about the study protocol and signed their consent forms before participating. A total of 34 participants were randomly assigned in a 1:1 ratio to one of two intervention groups (LL+EX or HL+EX) using a computer-generated randomization table. The allocation concealment was achieved through sealed opaque envelopes that contained information about the treatment group. Screening, recruitment, and randomization were carried out by a researcher who was not involved in intervention implementation or outcome evaluation.
Patients in both groups received standardized knee rehabilitation exercises (usual physiotherapy treatment) weekly for twelve weeks. The knee rehabilitation exercises were structured as individual one-to-one sessions conducted by qualified physiotherapists who were unaware of the participants' group allocations. The components of the prescribed and progressed therapeutic exercises were based on recommended KOA treatment guidelines [24,25]. The usual knee rehabilitation exercises consisted of therapeutic exercises, such as manual therapy techniques (soft tissue mobilization and manipulation), mobilization, stretching, strengthening, balance, proprioception, and functional exercises [24,25]. Examples of the KOA-specific exercises included calf stretching, straight leg raise, static quadriceps, terminal knee extension, and sit-to-stand exercises [24,25,26,27].
In addition to the standardized knee rehabilitation exercise, all participants received either HILT or LLLT based on their group allocation. Laser protocols were adapted based on previous studies [19,28,29] and manufacturer's guidelines [18]. The procedures of laser treatment were identical between the two groups as follows: (i) patient position: supine with their knee flexed at 30° to allow for laser irradiation to reach the joint surfaces [19,30], (ii) treatment area: antero-medial and antero-lateral sides of the knee joint which cover approximately 20 cm2 per knee [19,30], (iii) application: the laser probe was placed vertically against the knee and slowly moved in a longitudinal and perpendicular direction [18] and (iv) treatment time: 15 minutes (5 minutes of pulse mode and 10 minutes of continuous mode) of laser treatment per knee. The interventions for both groups were administered once a week for 12 consecutive weeks. Each group received the following laser parameters:
2.5.1. Group LL+EX (n = 17)
Participants in this group received LLLT in conjunction with their knee rehabilitation exercise. The LLLT was administered using the BTL-5825SL (BTL Int) with a wavelength of 830 nm, peak power output of 400 mW, energy density of 10 to 12 J/cm2, and a total energy of 400 J (100 J pulsed and 300 J continuous mode) during each session.
2.5.2. Group HL+EX (n = 17)
Participants in this group received HILT in addition to their knee rehabilitation exercise. The HILT was administered using the BTL 6000 HIL (BTL Int) 12 Watt, with a wavelength of 1064 nm, a power output of 5 W, energy density of 19 to 150 J/cm2, and a total energy of 3190 J (190 J pulsed and 3000 J continuous mode) each session.
2.6. Standardization and Blinding
To ensure the blinding of the intervention, all laser treatment sessions (LLLT and HILT) were identical between the two groups (including laser preparation, procedures and duration of treatment). Meanwhile, all outcome measures were performed by a single assessor who was blinded to group allocation.
2.7. Outcome Measures
The outcomes of this study were the Knee Injury and Osteoarthritis Outcome Score (KOOS) for knee-related disability, Numerical Rating Pain Scale (NPRS) for pain, active knee flexion for physical function, and the Timed Up-and-Go test (TUG) for functional performance. All outcomes were assessed by the same assessor at baseline (Week 0) and immediately after completion of the intervention (Week 12).
The KOOS is a self-administered questionnaire to evaluate participants' opinions regarding their knee problems through five specific subscales: pain, symptoms, activities of daily living (ADL), sport and recreation, and quality of life (QOL) [31]. The English and Malay versions of the KOOS were employed in this study, and each item is rated on a five-point Likert scale (0 to 4). The total score for each subscale is transformed into a percentage, with 0% indicating severe knee problems or high knee-related disability and 100% indicating no knee problems or knee-related disability [32]. Validity studies have consistently demonstrated a moderate to high correlation between the KOOS subscales and the WOMAC subscales [31], with interclass correlation coefficients ranging from 0.91 to 0.99 [33] and Cronbach's alpha values ranging from 0.84 to 0.91 [32], indicating excellent test-retest reliability. Additionally, a previous study reported that the Malay version of the KOOS questionnaire demonstrated an excellent degree of goodness of fit and was found to be a valid and reliable tool for assessing Malaysian adults with KOA [34].
Meanwhile, the NPRS is a simple unidimensional measure of pain intensity that is widely used in which the participants select a whole number (0 to 10) that best reflects pain intensity that ranges from 0 (no pain) to 10 (the worst imaginable pain) [35]. It has excellent test-retest reliability, with intraclass correlation coefficients, standard measurement error, and minimal detectable change of 0.95, 0.48 and 1.33, respectively [36]. Active knee flexion was measured using a universal goniometer (2x25 cm). It was found that the universal goniometric assessment of the knee joint are both valid and reliable, with high inter- (> 0.99) and intra-rater (> 0.98) reliabilities [37].
The TUG test is a reliable and valid method for measuring functional mobility, balance, and fall risk [38,39]. It is cost-effective and time-efficient, with intra-rater reliability of 0.97 and inter-rater reliability of 0.96 [38]. The construct validity of TUG performance was correlated with the Berg Balance Scale, 10-meter gait speed test, and Bartell Index [39]. In this study, the assessor demonstrated the TUG test to the participants. Participants were instructed to sit on a standard armchair, rise from the chair, walk at a safe and comfortable pace to a marker 3 meters away (marked by a line and a cone), turn around the cone and return to sit down again. They were allowed to use walking aids and hold the armrest to sit and stand during the test. The time taken from the start of movement from the chair to sitting back on the chair was recorded, and a score of more than 14 seconds indicated a low functional mobility performance and a high risk of falls [38].
2.8. Statistical Analysis
Data were analyzed using SPSS version 25.0 (SPSS Inc., Chicago, IL, USA) based on the intention-to-treat principle, where all participants were included in the analysis, regardless of their adherence to the intervention. Descriptive statistics and cross-tabulations were used to describe participants' sociodemographic characteristics at baseline, including age, gender, body mass index, duration of illness, affected side, KOA severity, and use of mobility aid. The baseline comparison of clinical outcomes was performed using a one-way analysis of variance to assess the impact of these factors as dependent variables. The primary aim of the study was to examine the within- and between-group differences in KOOS, NPRS, active knee flexion, and TUG scores pre- and post-intervention between LL+EX and HL+EX groups, using analysis of covariance (ANCOVA). The validity and reliability of the ANCOVA analysis were ensured by conducting assumption checks for normal distribution and homogeneity of variance, which were met. To evaluate the magnitude of the difference between groups, the effect size of each variable was determined using Cohen's d, with 0.2, 0.5, and 0.8 representing small, medium, and large effects, respectively [23]. Furthermore, the MCID was considered for the KOOS, NPRS, active knee flexion range, and TUG to assess the clinical relevance of the observed changes [21,40,41]. All statistical analyses were conducted using an alpha level of 0.05 for all significance tests.
3. Results
3.1. Participants’ Characteristics
Fifty-two patients with symptomatic KOA were screened based on the study inclusion and exclusion criteria for eligibility at the Sports Medicine Clinic of UMMC. Of these, 18 were excluded for the following reasons: (i) categorized as severe/advanced KOA (n = 10), (ii) refusal to participate (n = 6), and (iii) underlying acute ligamentous knee injuries (n = 2). Thirty-four patients (76% female and 24% male) with mild to moderate symptomatic KOA agreed to participate in this study and were randomized into one of two study groups (Figure 1): LL+E (n = 17; five males and 12 females) and HL+EX (n = 17; three males and 14 females). The mean ± standard deviation (SD) for age, body mass index (BMI), and the duration of KOA in the LL+EX and HL+EX groups were 57.94 ± 10.56 years, 27.57 ± 4.47 kg/m2, and 38.35 ± 28.26 months, and 51.18 ± 9.79 years, 30.58 ± 5.43 kg/m2, and 39.88 ± 39.11 months, respectively. Additionally, about 79% (n = 27) of the participants were identified with bilateral KOA involvement, 59% (n = 20) with moderate stages, and 41% (n = 14) were mild based on the Kellgren-Lawrence classification. Furthermore, 18% (n = 6) were using mobility aids for ambulation, mostly single-point walking sticks. The baseline sociodemographic and clinical outcomes characteristics of the participants in both groups are summarized in Table 1.
3.2. Baseline Comparability Analysis
There were no significant differences in participants' sociodemographic variables (age, gender, BMI), disease characteristics (duration of illness, affected side, severity of KOA, and use of mobility aid), and outcome variables (KOOS, NPRS, active knee flexion, and TUG) between the two groups at baseline.
3.3. Evaluation of Outcomes
All participants completed the twelve intervention sessions and went through the pre-post assessments, representing an adherence rate of 100%. No adverse effects of laser therapy were reported during the study period. The mean scores of the primary and secondary outcomes with their respective standard deviations at baseline (week 0) and post-intervention (week 12) are reported in Table 2.
3.4. Changes in KOOS Scores
In terms of the main outcome (KOOS), participants in both groups showed a statistically significant within-group increase in the KOOS total score following the completion of the treatment (p < 0.001), suggesting an amelioration of KOA symptoms and enhanced participation in functional activities, thus reducing the level of knee-related disability). However, the mean differences of change for the KOOS total score were significantly higher in the HL+EX group (MD: 13.84; 95% CI: 9.83 to 17.85; p < 0.001) compared to the LL+EX (MD: 4.84; 95% CI: 1.74 to 7.94; p = 0.004) (Figure 2). Moreover, the analysis of covariance for all the KOOS subscales scores showed statistically significant mean differences of change between the two groups, favoring HL+EX (p < 0.01), with the effect size (Cohen's d) ranging from 0.14 (small) to 1.04 (large).
Abbreviations: ES, effect size; HL+EX, high-intensity laser therapy and exercise; KOOS, knee injury and osteoarthritis outcome score; LL+EX, low-level laser therapy and exercise.
3.5. Changes in NPRS, Active Knee Flexion and TUG Scores
The within-group analysis of the secondary outcomes found a statistically significant reduction in the NPRS and TUG scores (indicating a reduction in pain and improvement in functional mobility) and a significant increase in active knee flexion (denoting improvement in physical function) in both groups compared to baseline (p < 0.001). Similarly, the mean differences of change for all the secondary outcomes were higher in the HL+EX group [NPRS (MD: -3.28; 95% CI: -3.78 to -2.76; p < 0.001), active knee flexion (MD: 9.53; 95% CI: 5.57 to 13.49; p < 0.001), and TUG (MD: -0.88; 95% CI: -1.04 to -0.72; p < 0.001)] compared to the LL+EX [NPRS (MD: -1.95; 95% CI: -2.3 to -1.53; p < 0.001), active knee flexion (MD: 3.12; 95% CI: 1.56 to 4.68; p = 0.001), and TUG (MD: -0.53; 95% CI: -0.64 to -0.41; p < 0.001)] (Figure 3, Figure 4, Figure 5). Between group analysis of covariance for NPRS, active knee flexion, and TUG found statistically significant higher mean differences of change in the HL+EX group compared to LL+EX pre- and post-intervention (p < 0.01). Cohen's d analysis of effect size between the HL+EX and LL+EX groups indicated a large effect for NPRS (d = 1.05), a medium effect for active knee flexion (d = 0.61), and a small effect for TUG (d = 0.47).
4. Discussion
This study compared the effects of LLLT and HILT as adjunctive treatment to rehabilitation exercise on pain, physical function and disability levels among patients with mild to moderate KOA. The respective laser and exercise interventions for both studied groups (LL+EX and HL+EX) were administered across 12 weekly sessions, and the study outcomes were evaluated at baseline and immediately post-intervention. Results showed that both groups exhibited statistically significant reductions in knee pain and disability scores, along with improved physical function and functional mobility compared to baseline; however, the HL+EX group had significantly higher mean differences of change by 50% for NPRS, 20% for KOOS, 6% for active knee flexion, and 3% for TUG relative to the LL+EX. Crucially, the changes in KOOS, NPRS, and active knee flexion scores in the HL+EX group exceeded the MCID threshold, suggesting a clinically relevant reduction in knee-related disability and pain, along with clinically significant improvements in physical function. Conversely, only the NPRS scores of the LL+EX group reached clinical significance. While no clinically significant changes were observed for functional mobility as measured by the TUG test in either laser group. This study's clinical evidence implies that combining HILT with usual KOA rehabilitation exercises leads to more substantial positive changes in clinical outcomes, specifically in pain, physical function, and knee-related disability, compared to LLLT.
This study acknowledged Kheshie et al. (2014) and Delkhosh et al. (2018) which evaluated the effect of HILT and LLLT as adjunctive treatment to KOA rehabilitation exercise. Kheshie et al. (2014) concluded that HL+EX was more effective than LL+EX in reducing pain and knee-related disability levels in patients with mild to moderate KOA [19]. However, a few methodological issues may have confounded their findings. Kheshie et al. (2014) administered a homogenized dose of laser treatment to 1250 J per session; therefore, participants treatment times varied between LLLT (33 minutes) and HILT (15 minutes) [19], which could potentially affect the treatment blindness. The study also employed a single-blinded design which could introduce assessor bias [42]. Additionally, only male patients were recruited [19]; thus, the results may not be generalizable to females, which has a higher representation [1].
Meanwhile, Delkhosh et al. (2018) compared HL+EX and LL+EX effects on pain and knee-related disability in 45 female patients with KOA [43]. The study relied on self-reported outcomes (VAS and WOMAC), similar to Kheshie et al. (2014). The results showed that both treatments had similar effects in reducing pain and knee-related disability measured by pain VAS and WOMAC, respectively [43]. However, the study determined LLLT to be more appropriate due to its lower cost [43]. The article was only available in English as an abstract, with the rest in Persian, making accurate details on the study's design, methodology (laser intervention), and results inaccessible. Nevertheless, information on the laser intervention was accessed based on the available trial protocol registration details. The study applied ten intervention sessions within two weeks, with five sessions per week [43]. The LL+EX group received a laser output of 30 mW (830 nm of wavelength), while the HL+EX group received 3.2 W of power output (910 nm of wavelength) [43]. Unfortunately, no information was available on important details such as treatment time, mode and location of laser application, energy density, or total energy delivered per session. Therefore, a comparison between the total laser dosage delivered based on the present study and Delkhosh et al. (2018) cannot be made. However, we believe that our laser treatment delivers higher total energy compared to the study by Delkhosh et al. (2018), as we are applying 12 sessions with power output ranging from 400 mW (LLLT) to 4 W (HILT), which may justify our significant findings regarding the difference between the two laser treatments. Hence, a double-blinded (participants and outcome assessors) study design involving patients with KOA of both sexes and the combination of self-reported, clinical, and performance-based outcomes assessment could provide more reliable and valid results [23].
Based on recent studies, combining laser treatment with exercise, i.e. LL+EX [6,44] or HL+EX [8,15,29] were more effective in reducing knee pain and stiffness, and enhancing physical function among patients with KOA than rehabilitation exercise alone. These improvements were attributed to the synergistic effects of laser technology and therapeutic exercise on tissue repair at the cellular level [11,12,18]. Specifically, in this study, the higher reduction in knee pain scores in the HL+EX group compared to the LL+EX group can be attributed to the enhanced properties of high-power laser technology. These advantages include (i) a higher energy output and deeper tissue penetration than low-level laser therapy [11,18], (ii) an anti-inflammatory effect with pain modulation and impact on nerve endings for pain relief [8,11], and (iii) a scattering mode of laser radiation with therapeutic photo-thermal effects that induce localized muscle relaxation, reducing muscle spasms [13,18]. Additionally, on pain modulation and suppression of inflammation, HILT was found to induce the release of endorphins and serotonin at the peripheral nerve endings, decrease proinflammatory cytokines and other inflammatory mediators such as interleukin-1, interleukin-6, prostaglandin, C-reactive protein, and tumour necrosis factor-alpha [45]. Moreover, HILT increases local tissue temperature and blood circulation in knee joints, promoting the exchange of nutrients in cartilage, stimulating tissue regeneration, and reducing pain, oedema, and inflammation [4]. Consequently, these mechanisms lead to better outcomes following HILT than LLLT in relieving KOA pain [15,16].
Meanwhile, based on the assessments of active knee flexion range and functional mobility (TUG), the group receiving HL+EX showed a 9% increase in active knee flexion and TUG, compared to LL+EX (3% for active knee flexion and 6% for TUG). These improvements could be attributed to the established KOA rehabilitation exercises prescribed as their primary treatment, including (i) stretching exercises which are effective in increasing active joint ROM by developing greater stretch tolerance [26,27], and (ii) strengthening exercises for the quadriceps and hamstrings muscles, which serve as knee joint dynamic stabilizers, resulting in higher cadence and lower risk of falls [26,46]. Besides the prescribed rehabilitation exercises, better pain management with laser treatment can enhance physical capacity and performance [6,8], especially through HILT [16]. Furthermore, in the present study, HL+EX has been demonstrated to produce a higher reduction in knee-related disability level as measured using the KOOS (reduction in KOA pain and symptoms, increase in ADL and sports participation, and improvement of QOL) compared to LL+EX. Previous research has suggested that disability in individuals with KOA results from the intricate interactions between knee pain as the primary symptom and physical function [47,48]. Therefore, it can be expected that reducing knee pain (as evaluated by NPRS) and increasing knee joint range of motion and functional mobility (measured through active knee flexion and TUG) would be reflected through a reduction in the level of knee-related disability [47,48,49]; as indicated based on amelioration in KOA symptoms and improvement of functional activity participation as measured by the KOOS.
This double-blinded trial was conducted with a heterogeneous sample, and random group allocation was used to assign participants. The baseline comparison revealed no significant differences between the groups in terms of baseline clinical outcomes or sociodemographic factors as potential confounding variables. In addition, all participants in both groups completed their respective treatment protocols and pre-post assessments. Findings from the multi-modal assessments, including self-reported, clinician-administered, and performance-based evaluations, may provide sufficient evidence to support the integration of HILT in the management of mild to moderate KOA. However, some limitations need to be considered. First, since only pre- and post-intervention outcomes were assessed, it is not possible to evaluate long-term effects (> 4 months). Second, due to the use of self-reported measures in the evaluation of knee pain and knee-related disability, there could be a potential bias as subject perception may vary [20]. Therefore, this study suggests that future comparative research should incorporate follow-up periods to evaluate the long-term results and objective clinical measures, such as biomarkers associated with bone or cartilage for KOA.
5. Conclusions
This study found that combining LLLT or HILT with usual KOA rehabilitation exercises resulted in statistically significant improvements in knee pain, knee-related disability, physical function, and functional mobility. Interestingly, the results also indicate that combining HILT with exercise produces greater positive changes than using LLLT as an adjunctive therapy to rehabilitation exercise in patients with KOA; specifically, the improvements in knee pain, physical function, and knee-related disability surpassed clinical relevance capacity. Thus, this study supports the consideration of HILT as a more effective treatment option than LLLT in the management of KOA. These findings contribute to the growing body of evidence supporting the use of laser therapy, particularly HILT, in conjunction with rehabilitation exercises as a viable treatment approach for KOA.
Author Contributions
Conceptualization, A.Y. and M.S.A.H.; methodology, M.A.A., A.Y. and M.S.A.H.; formal analysis, M.A.A., M.M. and A.Y.; investigation, M.A.A., M.M., N.S., U.M. and N.H.; data curation, M.A.A., M.M., N.S., U.M. and N.H.; writing—original draft preparation, M.A.A. and M.M.; writing—review and editing, M.A.A., A.Y. and M.S.A.H.; visualization, M.A.A. and A.Y.; supervision, A.Y. and M.S.A.H. All authors have read and agreed to the published version of the manuscript.
Funding
This research is partially funded by institutional PPRN grant PV061-2022.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Medical Research Ethics Committee of Universiti Malaya Medical Centre (MREC UMMC ID: 2020102-9129).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The datasets analyzed during the current study are available from the corresponding author upon reasonable request. All data from the study are included in this published article.
Acknowledgments
The authors thank the participants and management of the Sports Medicine Clinic of UMMC for their participation and assistance in this study.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Peat, G.; Thomas, M.J. Osteoarthritis year in review 2020: epidemiology & therapy. Osteoarthr. Cartil. 2020, 29, 180–189. [Google Scholar] [CrossRef]
- Singh, D.K.A. , Kamsan, S. S., Ahmad, M.A., Chien-Ying, A.N., Chua, W.Q., Padzil, F.M., Hendri, E.N.M. Knee associated problems and functional mobility among adults with knee osteoarthritis. Malay. J. Health. Sci. 2018, 16, 229–230. [Google Scholar]
- Kim, H.; Seo, J.; Lee, Y.; Park, K.; Perry, T.A.; Arden, N.K.; Mobasheri, A.; Choi, H. The current state of the osteoarthritis drug development pipeline: a comprehensive narrative review of the present challenges and future opportunities. Ther. Adv. Musculoskelet. Dis. 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Wu, M.; Luan, L.; Pranata, A.; Witchalls, J.; Adams, R.; Bousie, J.; Han, J. Is high intensity laser therapy more effective than other physical therapy modalities for treating knee osteoarthritis? A systematic review and network meta-analysis. Front. Med. 2022, 9, 956188. [Google Scholar] [CrossRef] [PubMed]
- Huang, Z.; Chen, J.; Ma, J.; Shen, B.; Pei, F.; Kraus, V. Effectiveness of low-level laser therapy in patients with knee osteoarthritis: a systematic review and meta-analysis. Osteoarthr. Cartil. 2015, 23, 1437–1444. [Google Scholar] [CrossRef] [PubMed]
- Stausholm, M.B.; Naterstad, I.F.; Joensen, J.; Lopes-Martins, R. .B.; Sæbø, H.; Lund, H.; Fersum, K.V.; Bjordal, J.M. Efficacy of low-level laser therapy on pain and disability in knee osteoarthritis: systematic review and meta-analysis of randomised placebo-controlled trials. BMJ Open 2019, 9, e031142. [Google Scholar] [CrossRef] [PubMed]
- Wyszyńska, J.; Bal-Bocheńska, M. Efficacy of High-Intensity Laser Therapy in Treating Knee Osteoarthritis: A First Systematic Review. Photomed. Laser Surg. 2018, 36, 343–353. [Google Scholar] [CrossRef]
- Penberthy, W.T.; Vorwaller, C.E. Utilization of the 1064 nm Wavelength in Photobiomodulation: A Systematic Review and Meta-Analysis. J. Lasers Med Sci. 2021, 12, e86–e86. [Google Scholar] [CrossRef]
- Kim, E.-D.; Won, Y.H.; Park, S.-H.; Seo, J.-H.; Kim, D.-S.; Ko, M.-H.; Kim, G.-W. Efficacy and Safety of a Stimulator Using Low-Intensity Pulsed Ultrasound Combined with Transcutaneous Electrical Nerve Stimulation in Patients with Painful Knee Osteoarthritis. Pain Res. Manag. 2019, 2019, 1–10. [Google Scholar] [CrossRef]
- Samaan, S.S.R.R.; Sedhom, M.G.; Grace, M.O. A randomized comparative study between high-intensity laser vs low-intensity pulsed ultrasound both combined with exercises for the treatment of knee osteoarthritis. Int. J. Rheum. Dis. 2022, 25, 877–886. [Google Scholar] [CrossRef]
- White, P.F. , Alvir-Lazo, O. L., Yumul, R. Cold laser therapy for acute and chronic pain management: A comparison of low-level and high-intensity laser therapy devices. Anaesth. News. 2019, 13, 65–78. [Google Scholar]
- Kushibiki, T.; Ishihara, M. Biological Function of Low Reactive Level Laser Therapy (LLLT). In Photomedicine: Advances in Clinical Practice; Tanaka, Y., Ed.; IntechOpen: London, UK, 2017. [Google Scholar] [CrossRef]
- Kulchitskaya, D.B.; Konchugova, T.V.; E Fedorova, N. Comparative evaluation of the effects of high-intensity and low-intensity laser radiation on microcirculation among patients with knee arthritis. 2017, 826, 012015. [CrossRef]
- Jankaew, A.; You, Y.-L.; Yang, T.-H.; Chang, Y.-W.; Lin, C.-F. The effects of low-level laser therapy on muscle strength and functional outcomes in individuals with knee osteoarthritis: a double-blinded randomized controlled trial. Sci. Rep. 2023, 13, 1–9. [Google Scholar] [CrossRef]
- Siriratna, P.; Ratanasutiranont, C.; Manissorn, T.; Santiniyom, N.; Chira-Adisai, W. Short-Term Efficacy of High-Intensity Laser Therapy in Alleviating Pain in Patients with Knee Osteoarthritis: A Single-Blind Randomised Controlled Trial. Pain Res. Manag. 2022, 2022, 1–9. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.A.; Hamid, M.S.A.; Yusof, A. Effects of low-level and high-intensity laser therapy as adjunctive to rehabilitation exercise on pain, stiffness and function in knee osteoarthritis: a systematic review and meta-analysis. Physiotherapy 2021, 114, 85–95. [Google Scholar] [CrossRef] [PubMed]
- Gur, A.; Cosut, A.; Sarac, A.J.; Cevik, R.; Nas, K.; Uyar, A. Efficacy of different therapy regimes of low-power laser in painful osteoarthritis of the knee: A double-blind and randomized-controlled trial. Lasers Surg. Med. 2003, 33, 330–338. [Google Scholar] [CrossRef] [PubMed]
- BTL-Corporate. High-Intensity Laser: Painless and non-surgical management. 2023 (, 2023). Available from: www.high-intensity-laser.com. 15 February.
- Kheshie, A.R.; Alayat, M.S.M.; Ali, M.M.E. High-intensity versus low-level laser therapy in the treatment of patients with knee osteoarthritis: a randomized controlled trial. Lasers Med Sci. 2014, 29, 1371–1376. [Google Scholar] [CrossRef]
- Askim, K.; Knardahl, S. The Influence of Affective State on Subjective-Report Measurements: Evidence From Experimental Manipulations of Mood. Front. Psychol. 2021, 12. [Google Scholar] [CrossRef] [PubMed]
- Eckhard, L.; Munir, S.; Wood, D.; Talbot, S.; Brighton, R.; Walter, W.L.; Baré, J. Minimal important change and minimum clinically important difference values of the KOOS-12 after total knee arthroplasty. Knee 2021, 29, 541–546. [Google Scholar] [CrossRef]
- Alfredo, P.P.; Bjordal, J.M.; Dreyer, S.H.; Meneses, S.R.F.; Zaguetti, G.; Ovanessian, V.; Fukuda, T.Y.; Junior, W.S.; Martins, R. .B.L.; Casarotto, R.A.; et al. Efficacy of low level laser therapy associated with exercises in knee osteoarthritis: a randomized double-blind study. Clin. Rehabilitation 2011, 26, 523–533. [Google Scholar] [CrossRef]
- Serdar, C.C.; Cihan, M.; Yücel, D.; A Serdar, M. Sample size, power and effect size revisited: simplified and practical approaches in pre-clinical, clinical and laboratory studies. Biochem. Medica 2021, 31, 27–53. [Google Scholar] [CrossRef]
- Bannuru, R.R.; Osani, M.C.; Vaysbrot, E.E.; Arden, N.K.; Bennell, K.; Bierma-Zeinstra, S.M.A.; Kraus, V.B.; Lohmander, L.S.; Abbott, J.H.; Bhandari, M.; et al. OARSI guidelines for the non-surgical management of knee, hip, and polyarticular osteoarthritis. Osteoarthr. Cartil. 2019, 27, 1578–1589. [Google Scholar] [CrossRef] [PubMed]
- Collins, N.; Hart, H.; Mills, K. Osteoarthritis year in review 2018: rehabilitation and outcomes. Osteoarthr. Cartil. 2019, 27, 378–391. [Google Scholar] [CrossRef] [PubMed]
- Suzuki, Y.; Iijima, H.; Tashiro, Y.; Kajiwara, Y.; Zeidan, H.; Shimoura, K.; Nishida, Y.; Bito, T.; Nakai, K.; Tatsumi, M.; et al. Home exercise therapy to improve muscle strength and joint flexibility effectively treats pre-radiographic knee OA in community-dwelling elderly: a randomized controlled trial. Clin. Rheumatol. 2018, 38, 133–141. [Google Scholar] [CrossRef] [PubMed]
- Ponvel, P.; Singh, D.K.A.; Soon, M.S.; Kamsan, S.S.; Ahmad, M.A. Comparison of Physical Performance between Older Adult Fallers with and without Knee Osteoarthritis. J. Sains Kesihat. Malays. 2019, 17, 147–155. [Google Scholar] [CrossRef]
- Alfredo, P.P.; Bjordal, J.M.; Junior, W.S.; Lopes-Martins, R. .B.; Stausholm, M.B.; Casarotto, R.A.; Marques, A.P.; Joensen, J. Long-term results of a randomized, controlled, double-blind study of low-level laser therapy before exercises in knee osteoarthritis: laser and exercises in knee osteoarthritis. Clin. Rehabilitation 2017, 32, 173–178. [Google Scholar] [CrossRef] [PubMed]
- Nazari, A. , Moezy, A. , Nejati, P., Mazaherinezhad, A., et al. Efficacy of high-intensity laser therapy in comparison with conventional physiotherapy and exercise therapy on pain and function of patients with knee osteoarthritis: A randomised controlled trial with 12-week follow up. Lasers Med. Sci. 2019, 34, 505–516. [Google Scholar]
- Al Rashoud, A.; Abboud, R.; Wang, W.; Wigderowitz, C. Efficacy of low-level laser therapy applied at acupuncture points in knee osteoarthritis: a randomised double-blind comparative trial. Physiotherapy 2014, 100, 242–248. [Google Scholar] [CrossRef]
- Multanen, J.; Honkanen, M.; Häkkinen, A.; Kiviranta, I. Construct validity and reliability of the Finnish version of the Knee Injury and Osteoarthritis Outcome Score. BMC Musculoskelet. Disord. 2018, 19, 155. [Google Scholar] [CrossRef]
- Collins, N.J.; Misra, D.; Felson, D.T.; Crossley, K.M.; Roos, E.M. Measures of knee function: International Knee Documentation Committee (IKDC) Subjective Knee Evaluation Form, Knee Injury and Osteoarthritis Outcome Score (KOOS), Knee Injury and Osteoarthritis Outcome Score Physical Function Short Form (KOOS-PS), Knee Outcome Survey Activities of Daily Living Scale (KOS-ADL), Lysholm Knee Scoring Scale, Oxford Knee Score (OKS), Western Ontario and McMaster Universities Osteoarthritis Index (WOMAC), Activity Rating Scale (ARS), and Tegner Activity Score (TAS). Arthritis Care Res. 2011, 63, S208–S228. [Google Scholar] [CrossRef]
- Phatama, K.Y.; Aziz, A.; Bimadi, M.H.; Oktafandi, I.G.N.A.A.; Cendikiawan, F.; Mustamsir, E. Knee Injury and Osteoarthritis Outcome Score: Validity and Reliability of an Indonesian Version. Ochsner J. 2021, 21, 63–67. [Google Scholar] [CrossRef]
- Zulkifli, M. M, Kadir, A. A., Elias, A., Bea, K.C., Sadagatullah, A.N. Psychometric properties of the malay language version of knee injury and osteoarthritis outcome score (KOOS) questionnaire among knee osteoarthritis patients: a confirmatory factor analysis. Malay. Orthop. J. 2017, 11, 7–14. [Google Scholar]
- Hawker, G.A.; Mian, S.; Kendzerska, T.; French, M. Measures of adult pain: Visual Analog Scale for Pain (VAS Pain), Numeric Rating Scale for Pain (NRS Pain), McGill Pain Questionnaire (MPQ), Short-Form McGill Pain Questionnaire (SF-MPQ), Chronic Pain Grade Scale (CPGS), Short Form-36 Bodily Pain Scale (SF-36 BPS), and Measure of Intermittent and Constant Osteoarthritis Pain (ICOAP). Arthr. Care Res. 2011, 63, S240–S252. [Google Scholar] [CrossRef]
- Alghadir, A.H.; Anwer, S.; Iqbal, A.; Iqbal, Z.A. Test–retest reliability, validity, and minimum detectable change of visual analog, numerical rating, and verbal rating scales for measurement of osteoarthritic knee pain. J. Pain Res. 2018, ume 11, 851–856. [Google Scholar] [CrossRef]
- Hancock, G.E.; Hepworth, T.; Wembridge, K. Accuracy and reliability of knee goniometry methods. J. Exp. Orthop. 2018, 5, 1–6. [Google Scholar] [CrossRef] [PubMed]
- Alghadir, A.; Anwer, S.; Brismée, J.-M. The reliability and minimal detectable change of Timed Up and Go test in individuals with grade 1 – 3 knee osteoarthritis. BMC Musculoskelet. Disord. 2015, 16, 1–7. [Google Scholar] [CrossRef] [PubMed]
- Barry, D. Sarcopenia: Textbook of Natural Medicine. In. Joseph E. Pizzorno, Michael T. Murray (Fifth Edition): Churchill Livingstone 2020.
- Maldaner, N.; Sosnova, M.; Ziga, M.; Zeitlberger, A.M.; Bozinov, O.; Gautschi, O.P.; Weyerbrock, A.; Regli, L.; Stienen, M.N.M. External Validation of the Minimum Clinically Important Difference in the Timed-up-and-go Test After Surgery for Lumbar Degenerative Disc Disease. Spine 2021, 47, 337–342. [Google Scholar] [CrossRef] [PubMed]
- Salaffi, F.; Stancati, A.; Silvestri, C.A.; Ciapetti, A.; Grassi, W. Minimal clinically important changes in chronic musculoskeletal pain intensity measured on a numerical rating scale. Eur. J. Pain 2004, 8, 283–291. [Google Scholar] [CrossRef] [PubMed]
- Probst, P. , Grummich, K. , Heger, P., Zaschke, S., Knebel, P., Ulrich, A., et al. Blinding in randomised controlled trials in general and abdominal surgery: Protocol for a systematic review and empirical study. Sys. Rev. 2016, 5, 48–54. [Google Scholar]
- Delkhosh, C.T. , Fatemy, E. , Ghorbani, R., Mohammadi, R. Comparing the immediate and long-term effects of low and high power laser on the symptoms of knee osteoarthritis. J. Maz. Univ. Med. Sci. 2018, 28, 69–77. [Google Scholar]
- Braghin, R.d.M.B.; Libardi, E.C.; Junqueira, C.; Rodrigues, N.C.; Nogueira-Barbosa, M.H.; Renno, A.C.M.; de Abreu, D.C.C. The effect of low-level laser therapy and physical exercise on pain, stiffness, function, and spatiotemporal gait variables in subjects with bilateral knee osteoarthritis: a blind randomized clinical trial. Disabil. Rehabilitation 2018, 41, 3165–3172. [Google Scholar] [CrossRef]
- Wickenheisser, V.A.; Zywot, E.M.; Rabjohns, E.M.; Lee, H.H.; Lawrence, D.S.; Tarrant, T.K. Laser Light Therapy in Inflammatory, Musculoskeletal, and Autoimmune Disease. Curr. Allergy Asthma Rep. 2019, 19, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Kamsan, S.S.; Singh, D.K.A.; Tan, M.P.; Kumar, S. The knowledge and self-management educational needs of older adults with knee osteoarthritis: A qualitative study. PLOS ONE 2020, 15, e0230318. [Google Scholar] [CrossRef] [PubMed]
- Ahmad, M.A. , Singh, D. K.A., Qing, C.W., Rahman, N.N.A., Padzil, F.M. Knee osteoarthritis and its related issues: Patients’ perspective. Malay. J. Health Sci. 2018, 16, 171–177. [Google Scholar]
- Shori, G.; Kapoor, G.; Talukdar, P. Effectiveness of home-based physiotherapy on pain and disability in participants with osteoarthritis of knee: an observational study. J. Phys. Ther. Sci. 2018, 30, 1232–1236. [Google Scholar] [CrossRef]
- Turner, M.N.; Hernandez, D.O.; Cade, W.; Emerson, C.P.; Reynolds, J.M.; Best, T.M. The Role of Resistance Training Dosing on Pain and Physical Function in Individuals With Knee Osteoarthritis: A Systematic Review. Sports Heal. A Multidiscip. Approach 2019, 12, 200–206. [Google Scholar] [CrossRef]
Figure 1.
Study flowchart.
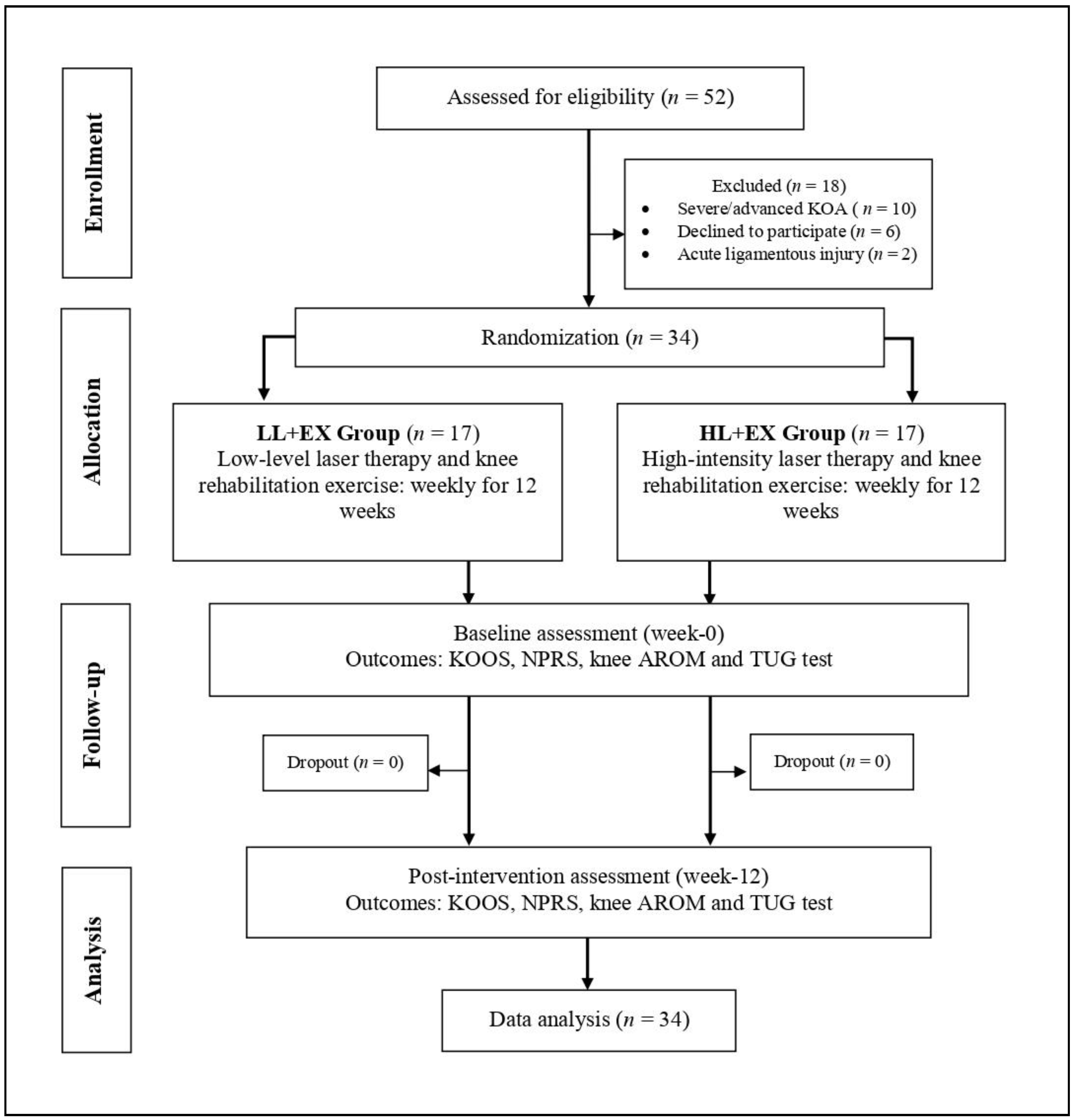
Figure 2.
Changes in the KOOS total score pre-post intervention.
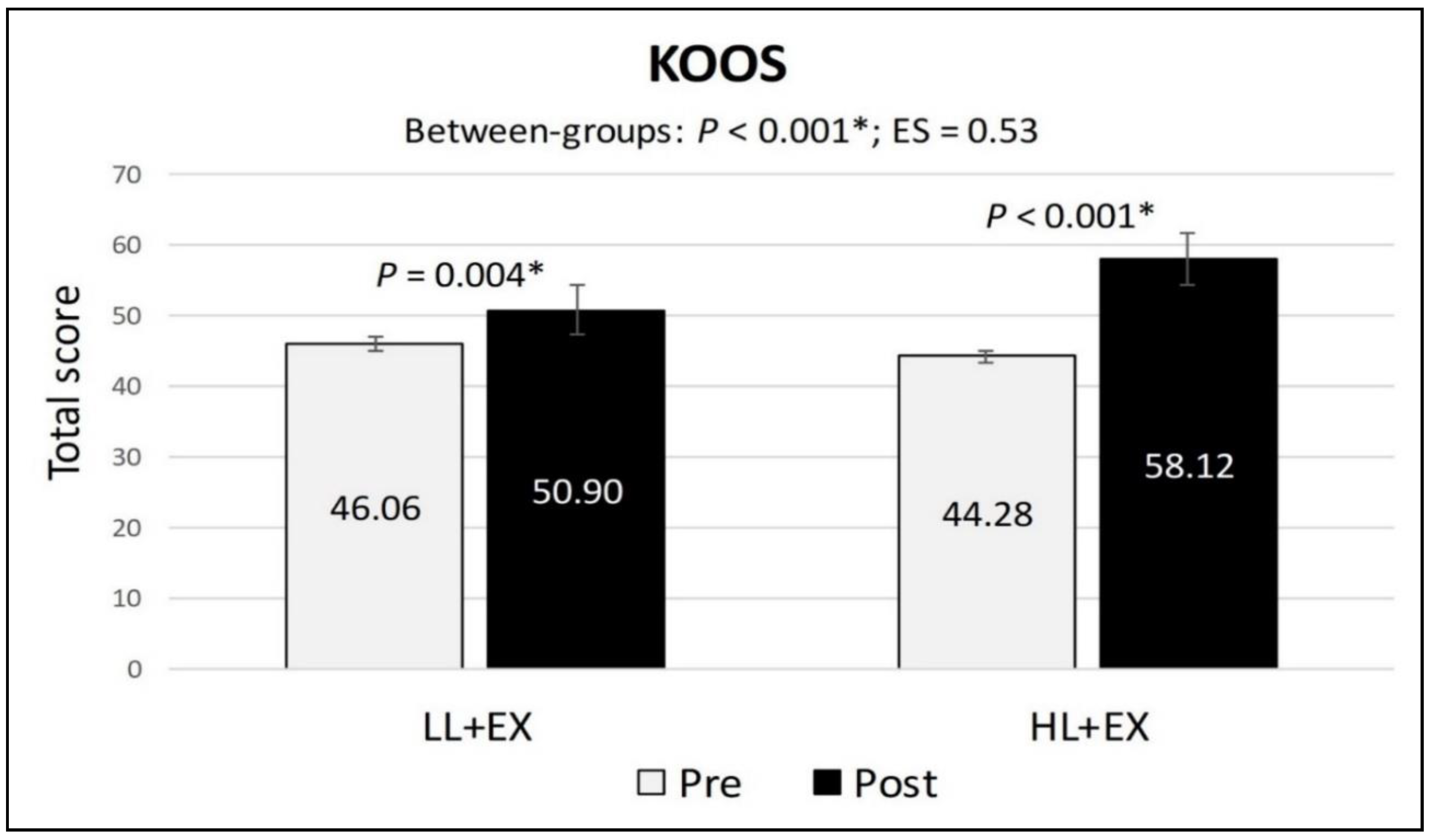
Figure 3.
Changes in the NPRS scores pre-post intervention. Abbreviations: ES, effect size; HL+EX, high-intensity laser therapy and exercise; LL+EX, low-level laser therapy and exercise; NPRS, numerical pain rating scale.
Figure 3.
Changes in the NPRS scores pre-post intervention. Abbreviations: ES, effect size; HL+EX, high-intensity laser therapy and exercise; LL+EX, low-level laser therapy and exercise; NPRS, numerical pain rating scale.
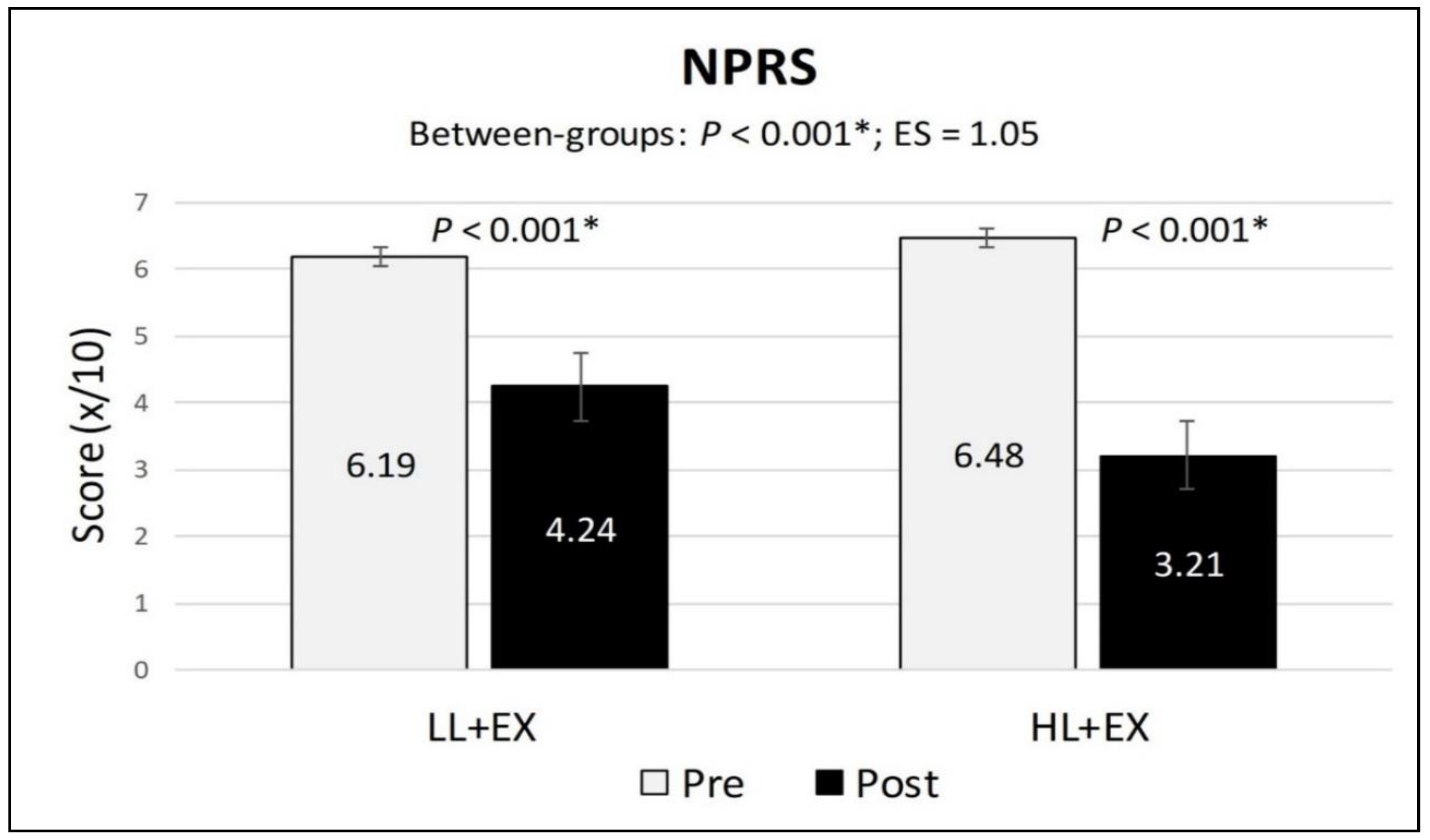
Figure 4.
Changes in the active knee flexion scores pre-post intervention. Abbreviations: ES, effect size; HL+EX, high-intensity laser therapy and exercise; LL+EX, low-level laser therapy and exercise.
Figure 4.
Changes in the active knee flexion scores pre-post intervention. Abbreviations: ES, effect size; HL+EX, high-intensity laser therapy and exercise; LL+EX, low-level laser therapy and exercise.
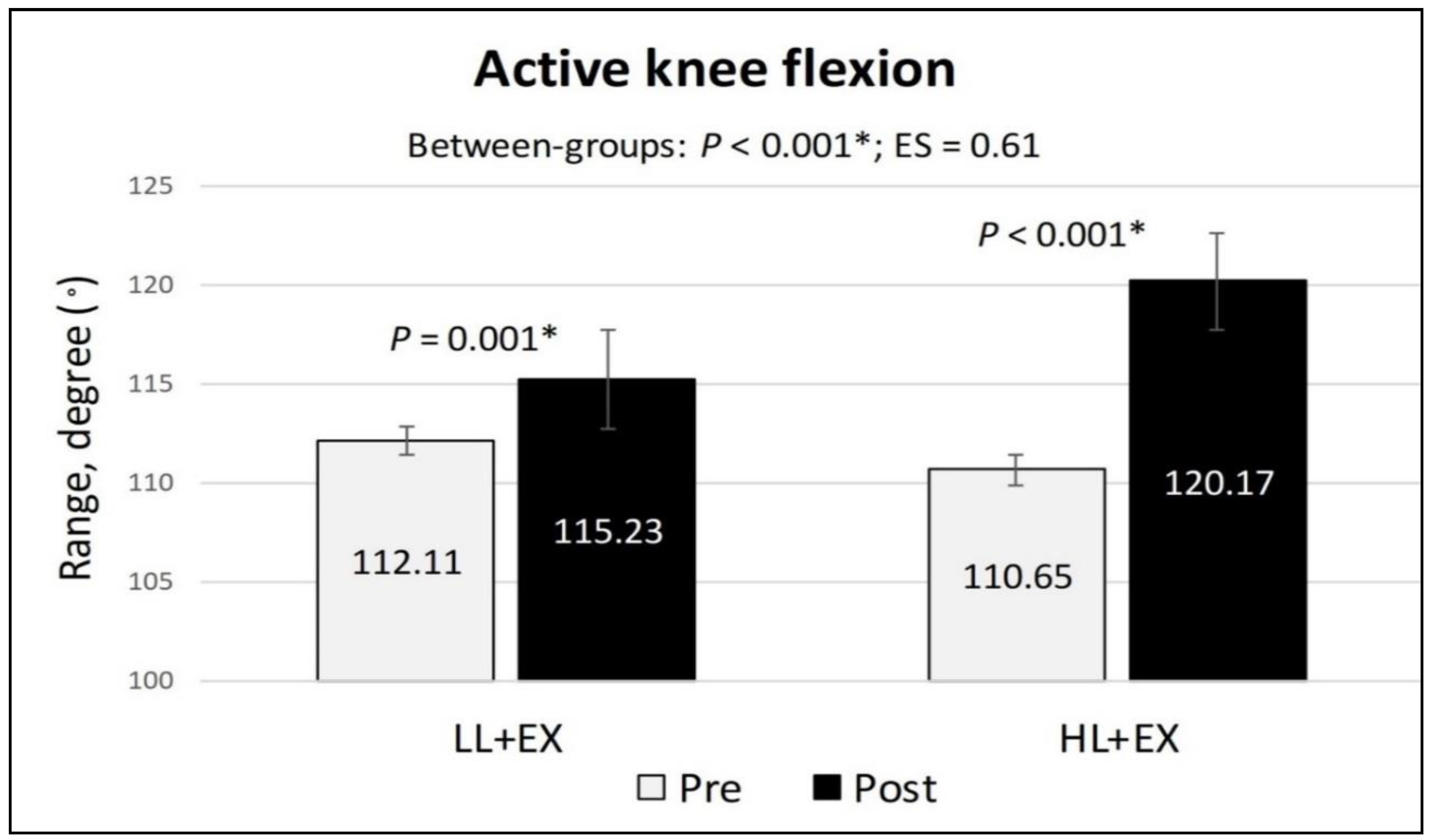
Figure 5.
Changes in the TUG scores pre-post intervention. Abbreviations: ES, effect size; HL+EX, high-intensity laser therapy and exercise; LL+EX, low-level laser therapy and exercise; TUG, timed up-and-go test.
Figure 5.
Changes in the TUG scores pre-post intervention. Abbreviations: ES, effect size; HL+EX, high-intensity laser therapy and exercise; LL+EX, low-level laser therapy and exercise; TUG, timed up-and-go test.
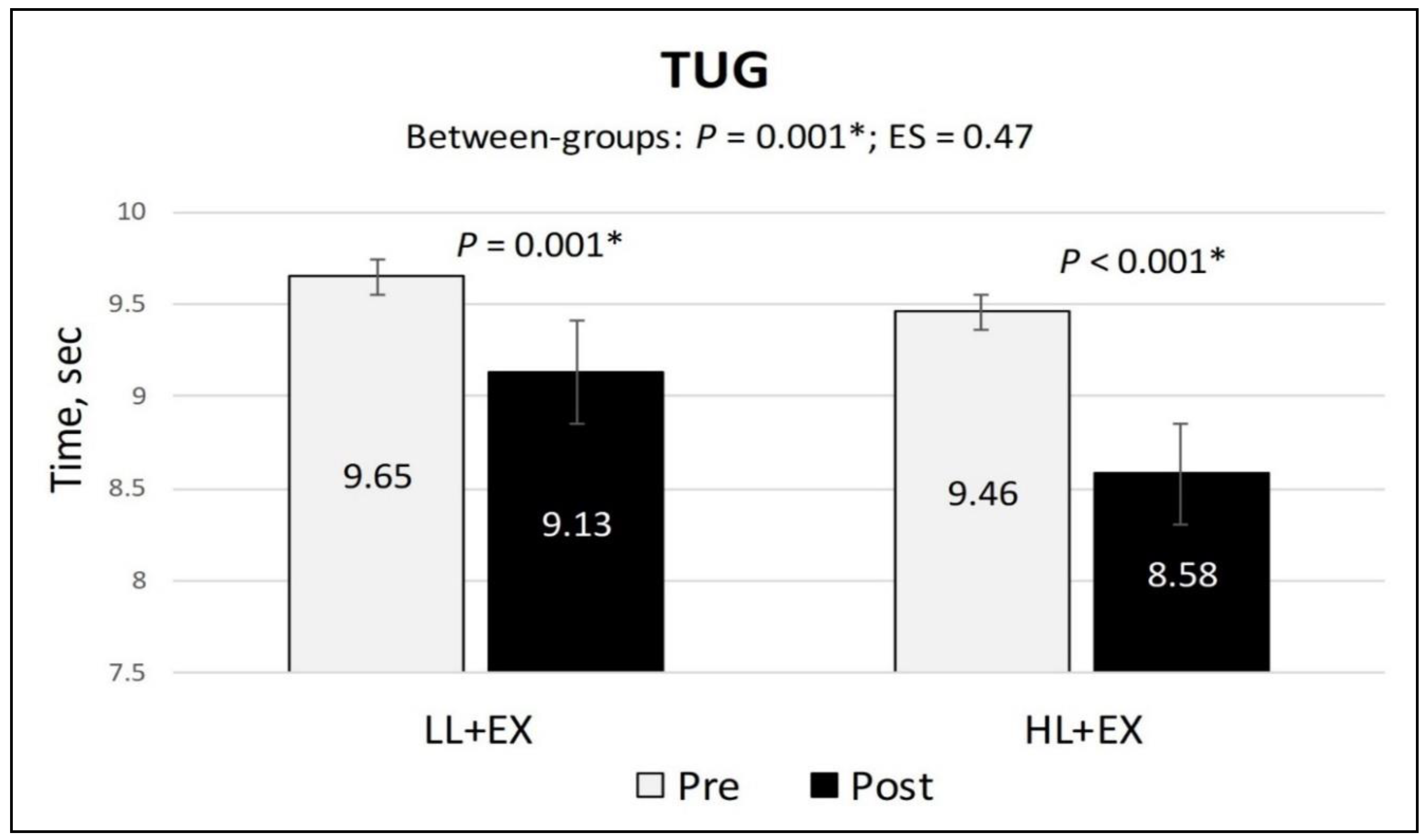

Table 1.
The demographic characteristics and clinical outcomes scores of the participants at baseline.
Table 1.
The demographic characteristics and clinical outcomes scores of the participants at baseline.
| Variables | LL+EX (n = 17) |
HL+EX (n = 17) |
p-value |
| Age (years) | 57.94 (10.56) | 51.18 (9.79) | 0.062 |
| Gender (male/female) | 5/12 | 3/14 | 0.344 |
| Body mass index (kg/m²) | 27.57 (4.47) | 30.58 (5.43) | 0.088 |
| KOA duration (months) | 38.35 (28.26) | 39.88 (39.11) | 0.897 |
| Affected side (uni/bilateral) | 5/12 | 2/15 | 0.199 |
| K-L grade (I/II/III) | 0/5/12 | 0/9/8 | 0.142 |
| Mobility aid (yes/no) | 14/3 | 14/3 | 0.672 |
| KOOS (total score) | 46.06 (9.47) | 44.28 (12.41) | 0.642 |
| NPRS (score) | 6.19 (1.45) | 6.48 (1.21) | 0.537 |
| Active knee flexion (degree) | 112.11 (11.87) | 110.65 (9.73) | 0.697 |
| TUG (time, sec) | 9.65 (1.51) | 9.46 (0.75) | 0.639 |
Abbreviations: HL+EX, high-intensity laser therapy and exercise; KOA, knee osteoarthritis; KOOS, knee injury and osteoarthritis outcome score; K-L, Kellgren-Lawrence classification; LL+EX, low-level laser therapy and exercise; NPRS, numerical pain rating scale; TUG, timed up-and-go test. Note: Values are reported as mean and standard deviation, with the exception of gender, affected side, severity, and use of mobility aids, which are presented by frequency. Categorical variables were analyzed using cross-tabulations and the Chi-square test, while one-way ANOVA was utilized to analyze continuous data. Statistically significant, p < 0.05*.
Table 2.
Changes in the KOOS, NPRS, active knee flexion, and TUG scores following twelve sessions of intervention for both groups.
Table 2.
Changes in the KOOS, NPRS, active knee flexion, and TUG scores following twelve sessions of intervention for both groups.
| Outcomes | LL+EX (n = 17) |
HL+EX (n = 17) |
Between-groups (analysis of covariance) |
||
| Mean (SD) | Mean (SD) | p-value | Effect size | ||
| KOOS (Total score) |
Pre | 46.06 (9.47) | 44.28 (12.41) | p = 0.001* | 0.53 |
| Post | 50.90 (13.92) | 58.12 (13.25) | |||
| MD; 95% CI; p | 4.84; 1.74 to 7.94; p = 0.004* | 13.84; 9.83 to 17.85; p < 0.001* | |||
| Symptoms | Pre | 10.87 (3.83) | 11.75 (2.65) | p = 0.002* | 0.14 |
| Post | 9.73 (3.83) | 8.32 (1.60) | |||
| MD; 95% CI; p | -1.12; -1.94 to -0.32; p = 0.009* | -3.43; -4.61 to -2.25; p < 0.001* | |||
| Pain | Pre | 18.32 (5.70) | 20.14 (6.38) | p < 0.001* | 1.04 |
| Post | 15.86 (5.50) | 11.09 (3.39) | |||
| MD; 95% CI; p | -2.46; -3.97 to -0.94; p = 0.003* | -9.05; -11.68 to -6.40; p < 0.001* | |||
| ADL | Pre | 36.73 (9.28) | 32.51 (11.48) | p = 0.014* | 0.26 |
| Post | 39.34 (8.33) | 41.90 (11.44) | |||
| MD; 95% CI; p | 2.60; 0.41 to 4.80; p = 0.023* | 9.40; 5.03 to 13.78; p < 0.001* | |||
| Sports | Pre | 3.92 (1.97) | 3.86 (3.31) | p < 0.001* | 0.64 |
| Post | 4.40 (2.16) | 6.55 (4.24) | |||
| MD; 95% CI; p | 0.48; 0.14 to 0.82; p = 0.007* | 2.69; 1.65 to 3.74; p < 0.001* | |||
| QOL | Pre | 4.67 (2.59) | 4.01 (2.43) | p = 0.002* | 0.66 |
| Post | 5.32 (2.88) | 7.24 (2.90) | |||
| MD; 95% CI; p | 0.65; 0.29 to 1.01; p = 0.002* | 3.24; 2.39 to 4.09; p < 0.001* | |||
| NPRS | Pre | 6.19 (1.45) | 6.48 (1.21) | p < 0.001* | 1.05 |
| Post | 4.24 (1.16) | 3.21 (0.75) | |||
| MD; 95% CI; p | -1.95; -2.3 to -1.53; p < 0.001* | -3.28; -3.78 to -2.76; p < 0.001* | |||
| Active knee flexion | Pre | 112.11 (11.87) | 110.65 (9.73) | p < 0.001* | 0.61 |
| Post | 115.23 (10.69) | 120.17 (4.26) | |||
| MD; 95% CI; p | 3.12; 1.56 to 4.68; p = 0.001* | 9.53; 5.57 to 13.49; p < 0.001* | |||
| TUG | Pre | 9.65 (1.51) | 9.46 (0.75) | p = 0.001* | 0.47 |
| Post | 9.13 (1.54) | 8.58 (0.61) | |||
| MD; 95% CI; p | -0.53; -0.64 to -0.41; p < 0.001* | -0.88; -1.04 to -0.72; p < 0.001* | |||
Abbreviations: ADL; activities of daily living; HL+EX, high-intensity laser therapy and exercise; KOOS, knee injury and osteoarthritis outcome score; LL+EX, low-level laser therapy and exercise; MD, mean difference; NPRS, numerical pain rating scale; QOL, quality of life; TUG, timed up-and-go test. Note: Values are presented as mean and standard deviation. Statistically significant, p < 0.05.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



