
Submitted:
06 May 2023
Posted:
10 May 2023
You are already at the latest version
Abstract
Humans have extremely variable skin pigmentation and melanin production influenced by genetics, UV exposure, and some medications. A significant number of skin illnesses that result in pigmentary abnormalities have an impact on patients’ physical appearance as well as their psychological and social well-being. Skin pigmentation can be divided into two basic categories: hyperpigmentation, where pigment appears to overflow, and hypopigmentation, where pigment is reduced. Albinism, melasma, vitiligo, Addison's disease, and post-inflammatory hyperpigmentation, which can be brought on by eczema, acne vulgaris, and drug interactions, are the most common skin pigmentation disorders in clinical practice. Anti-inflammatory medications, antioxidants, and medications that inhibit tyrosine, which prevents the production of melanin, are all possible treatments for pigmentation problems. Skin pigmentation can be treated orally and topically with medications, herbal remedies, and cosmetic products, but a doctor should always be consulted before beginning any new medicine or treatment plan. This review article explores the numerous types of pigmentation problems, their causes, and treatments, as well as the 25 plants, four marine species, and 17 topical and oral medications now on the market that have been clinically tested to treat skin diseases.
Keywords:
Skin pigmentation
; melanin
; Tyrosinase inhibitors
; hypopigmentation
; hyperpigmentation
; Vitiligo
; skin-lightening
; Depigmentation
1. Introduction
Skin pigmentation, which refers to how much melanin the body generates, determines the color of the skin. The two main types of melanin, eumelanin, and pheomelanin, are produced by melanocytes in the epidermal layer of the skin. Pheomelanin causes lighter skin tones, while eumelanin is responsible for darker skin tones. [1,2]
The skin is protected from sunburn by the dark brown pigment eumelanin (compound 1 in Figure 1), which absorbs UV rays from the sun. Darker skin tones are related to higher levels of eumelanin, while lighter skin tones are associated with lower levels. The capacity of eumelanin to prevent skin cancer is one of its additional benefits. Studies have shown that those with higher levels of eumelanin had a lower chance of developing skin cancer than people with lower levels. By absorbing solar heat and maintaining the body cool, eumelanin also helps to regulate body temperature. [3,4]
Pheomelanin, the pigment, is a lighter yellow-red tint (compound 2 in Figure 1). Because pheomelanin does not absorb UV rays as effectively as eumelanin, those with higher levels have lighter skin tones and are more prone to skin damage and sunburns. Pheomelanin does, however, have certain benefits. It helps to control body temperature and can keep the body cool in hot conditions by reflecting heat away from the body. Pheomelanin can also help prevent melanoma and other types of skin cancer. [5,6]
On chromosome 16, gene locus q24.3, the gene regulates the quantity of melanin produced for the melanocortin G-protein coupled receptor 1 (MC1R). The MC1R gene controls skin and hair color, modulates tanning (sensitivity to light exposure and sunburn), and increases melanoma risk. [7,8]
The rates of melanin synthesis vary across members of the same family and between racial groups (Figure 1). This variation (MSH) is caused by genetics, sun exposure, and certain hormones that stimulate melanocytes, such as adrenocorticotropic hormone (ACTH), lipotropin, and melanocyte-stimulating hormone. Using more melatonin results in a dirty, grayish-brown skin tone. [8,9,10]
2. Causes of Skin Pigmentation
Skin pigmentation is a common condition that can be triggered by various factors. The three leading causes of skin pigmentation are genetics, sun exposure, and particular medications. Understanding the fundamental causes of skin pigmentation will help us understand how to treat and prevent it. [2]
2.1. Genetics
Surprisingly, 125 genes can affect skin color. Genes and hormones control the melanin manufacturing process seen in Figure 1's flowchart. The skin cells' capacity to function and live and how much pheomelanin or eumelanin they generate are under a person’s control. As time passes, these factors may cause changes in skin tone [1]. Genetics is thus one of the most common causes of skin pigmentation. How many melanocytes the person has can be predetermined by genetics. It is produced by melanocytes, which are skin cells that produce melanin. However, melanosomes (the organelles that contain melanin) must be transferred and increased during hyperpigmentation and tanning, but melanosomes decrease during hypopigmentation [11]. People with darker skin tones are likelier to have higher quantities of melanin, the pigment that gives skin its color... For instance, people with darker skin tones often have more melanin than those with lighter skin tones. [12,13,14]
2.2. Sun Exposure
Sun exposure is another common factor in skin pigmentation. When exposed to UV rays from the sun, the body produces more melanin to protect itself. This can make the skin more pigmented to defend against the sun's rays. Figure 2 illustrates how those with lighter skin tones are more likely to experience enhanced skin pigmentation after prolonged sun exposure [4,14,15].
2.3. Medications
Several medications may also lighten the skin's pigment. One class of drugs, antibiotics, can boost melanin synthesis, increasing skin color. When certain medications, such as birth control pills, are taken together, skin pigmentation may also intensify. A person taking medicine should speak with his doctor to find out if the medication could impact the color of his skin. [7,16,17]
3. Types of pigmentation disorders
While ill, a person's skin tone may alter, becoming lighter (hypopigmentation), as seen in Figure 3A,B, or darker (hyperpigmentation), as seen in Figure 3C,D. Melanin, the pigment that regulates skin color, is produced less frequently by the body, which results in hypopigmentation. Hyperpigmentation, on the other hand, is an increase in melanin synthesis. [4,5,18]
3.1. Causes of hypopigmentation
Prior skin trauma, including skin sores like blisters, infections, burns, exposure to chemicals, and other wounds, is the most common cause of low melanin content. (hypopigmentation). After healing injuries, the skin is paler than the surrounding skin surfaces. [19] Other genetic diseases can result in hypopigmentation in different parts of the skin. As seen in Figure 3, hereditary disorders such as albinism, melasma, fungal infections, pityriasis versicolor, pityriasis alba, and vitiligo can result in hypopigmentation as the mechanism in Figure 4. At birth, albinism is caused by a genetic abnormality called low melanin concentration. The prevalent physical traits of albinos include a white complexion, dark blue eyes, and white hair. [20,21] The genetic melasma condition can cause brown or blue-gray spots to develop on a person's arms or face. Hormones, sun exposure, or contraceptive medication may bring it on. [22,23]
Despite the fact that the Malassezia genus is responsible for the widespread fungal infection known as tinea versicolor, also known as pityriasis versicolor, it is possible for fungi to infect humans and change the color of their skin. Small regions of discoloration are brought on by malassezia's alteration of the skin's normal melanin pigmentation. The patches on the shoulders and buttocks may be lighter or darker than the overall healthy skin tone. [25] Pityriasis alba is a skin condition that typically affects adolescents and teenagers and is characterized by oval or circular hypopigmented lesions with soft scales. Lesions on the face, upper body, and arms, which are more noticeable in those with darker skin tones, may be modestly erythematous before becoming hypopigmented. [26]
Another common hypopigmented skin disorder is depigmentation, which occurs when the skin completely loses pigment and turns white. It is exemplified by the autoimmune disease vitiligo, which is characterized by melanocyte loss, a common cause of depigmentation, and macules of a white chalky substance on the skin. Smooth, white patches develop on the skin as a result of vitiligo, as seen in cases in Figure 5A,B. Vitiligo is frequently written off as a minor issue. [27,28]
3.2. Causes of hyperpigmentation
Hyperpigmentation results from an increase in melanin production. The main causes of a rise in melanin production, such as examples C and D in Figure 3 are sun exposure, dermatological illnesses, hormones, aging, hereditary factors, skin injuries or inflammation, and acne [24].
Sun exposure is the only known cause of this pigmentation condition because it predominantly stimulates melanin synthesis. Melanin protects the skin from UV radiation, acting as a natural sunscreen. Hyperpigmentation, however, could result from extensive sun exposure. Figure 2 previously showed that early exposure to the sun could worsen dark spots by mimicking melasma, age spots, and post-inflammatory spots. [24] Two examples of hyperpigmentation brought on by hormonal factors are chloasma and melasma. It has been discovered that the female sex hormones estrogen and progesterone boost melanin synthesis when the body is exposed to sunlight, resulting in this condition, which is prevalent in women. A negative side effect of hormone replacement treatment is hyperpigmentation. [29] Melanocyte numbers decline with age, but those still around grow and specialize. These physiological changes show how aging spots in adults over 40 become more apparent. [30] Genetics has an impact on pigmentation. The development of melanocyte function, which influences skin color, requires specific genes. [31] It appears after skin inflammation or damage, as indicated by the name post-inflammatory hyperpigmentation. Some of these are Burns, wounds, psoriasis or atopic dermatitis, chemical exposure, and acne. The skin looks darker and discolored once the wound has healed. [28] The deep skin layer dermis can get infected by papules, pustules, and acne. Unusual dark patches appear when sick skin areas produce more melanin than usual. Similarly, the true causes of the hyperpigmentation problem are infections of the fatty glands and hair follicles. Typically, minor acne won't lead to hyperpigmentation. Acne pimples that have been squeezed, squashed, or punctured will likewise discolor and hyperpigmented. [32]. The following causes of hyperpigmentation: pregnancy-related birthmarks, age spots, acne scars, and several drugs, including antibiotics, birth control pills, antimalarials, and tricyclic antidepressants. Dark skin patches and impaired adrenal gland function are symptoms of Addison's disease, an uncommon ailment. Hyperpigmentation can occasionally happen as a result of laser or light therapy. [33]
4. Drugs for Treatment of Skin Pigmentation
Despite being well-recognized for many years, drugs for skin pigmentation have only recently become more widely available. Topical creams and oral pills are the primary medications for skin pigmentation. It would be best to balance the advantages and disadvantages of both medicines to choose which is most beneficial. [33,34]
4.1. Oral Medications
Oral medicine is a potential substitute for treating skin ailments and modifying skin tone. Such drugs are beneficial because they are more potent than topical creams and do not have to be applied or disposed of as frequently as topical creams. However, there are certain drawbacks to taking oral medications. They can be expensive and cause more significant side effects than topical therapies. [35]
Compound 3 in Figure 6 is tranexamic acid (Traxamac® 250 mg), one of several coagulation modifiers. In addition to eczema, melasma, other associated ailments, toxic reactions, urticaria, and its effects on erythema, itching, swelling, and other recognized symptoms, it has also been used to treat various illnesses. A plasmin inhibitor called tranexamic acid prevents the plasminogen activator from converting plasminogen to plasmin by reversibly shutting off lysine binding sites on plasminogen molecules. This reduces atypical fibrinolysis and prevents blood loss. According to recent studies, tranexamic acid helps tyrosinase untangle tangles. It might avoid and stop hyperpigmentation by reducing melanin production. It is a widely used pharmaceutical technique that is easily accessible and effective against pigment spots. Although it inhibits the effects of tyrosinase and changes the relationship between keratinocytes and melanocytes, it decreases dermal vascularity and lessens melanin production. [36,37,38,39,40]
Using tranexamic acid orally in a dosage of 250 mg twice daily for six months on 75 patients, clinical and photographic evaluation reveals an initial decline in melasma after the first month for 82.4% of patients and 94.6% in the second month. The development of pigmentation has been used to measure the treatment's success (excellent if >90%, good if >60%, fair if >30%, and poor if 30%). After six months, the overall development rate is 95.9%, with 10.8% being excellent, 54% being good, and 31.1% being fair. which is evidence that oral tranexamic acid is a safe and effective melasma treatment. [41,42]
Mexameter® was utilized to evaluate the suggest lesional melanin index (MI) ranks and the erythema index (EI) scores for 25 patients who received 1,500 mg twice daily for two months. Both of these scores fell off dramatically. Histological examination confirmed significant decreases in mast cell counts, vessels, and epidermal pigmentation. Here is an illustration of how oral tranexamic acid reversed melasma-related dermal changes, including increased vascularity, decreased mast cell populations, and decreased melasma-related epidermal pigmentation. [43,44]
In a 25-woman research, certain sides of the face received twice-daily applications of 5% topical tranexamic acid for 12 weeks as a melasma treatment. Mexameter and Melasma Area and Severity Index (MASI) results revealed a notable drop in MI and MASI scores. Additionally, for 12 weeks, 23 melasma patients applied a 2% tranexamic acid emulsion twice daily to their whole faces. With a rise in the lightness values and a decrease in the erythema values, the mMASI and chromameter results showed a significant improvement in the fourth and eighth weeks. [45,46,47]
Isotretinoin is the 13-cis retinoic acid derivative of vitamin A (Isotane® 20 mg, molecule 4 in Figure 6). [48,49,50]. In treating acne vulgaris, oral isotretinoin exerts its effects by reducing sebaceous gland activity, Propionibacterium acnes development, and inflammation. This facilitates pore cleaning and inhibits the growth of new zits. [51,52,53]
The administration of 20 mg of Accutane (isotretinoin) orally was randomly assigned to sixty patients (aged 35 to 65); 42 of the women and 18 of the males. It was administered three times a week for no more than two months, and tracking continued for months after the study was over. The 60 patients reported reductions in their wrinkles, pore thickness, and pore size. They noticed that the skin became significantly smoother and lighter in color. Both the elasticity and tone of the skin improved. Additionally, they noticed a decrease in pigmented lesions and hyperpigmentation. [54,55]
4.2. Topical Creams
Topical creams are the most common type of drug used to treat skin pigmentation. They are applied directly to the affected area and can lighten or darken the skin. The main advantage of topical creams is that they may be used at home and don't require a trip to the doctor. Additionally, they are typically less expensive than oral medications. Topical cream application, however, comes with several drawbacks. They can be messy and time-consuming to apply, and they might only sometimes be as effective as oral medications. [58,59]
Topical steroids are the most often recommended drug in dermatology. It is prescribed for various conditions, including eczema, psoriasis, atopic dermatitis, lichen simplex chronicus, intertrigo, and psoriasis, due to its immunosuppressive, anti-mitogenic, and anti-inflammatory characteristics. The dosage varies from one to three times per day. Betamethasone 0.05% (Betnovate-N®, chemical 5 in Figure 7) and clobetasol 0.05% (Dermovate®, compound 6 in Figure 7) are examples of topical steroids. NF-Kappa B inhibitors betamethasone and clobetasol are glucocorticoids that prevent neutrophil apoptosis and demarginating. Betamethasone and clobetasol are phospholipase A2 inhibitors, which also reduce the production of arachidonic acid derivatives. Additionally, glucocorticoids encourage the anti-inflammatory gene interleukin-10. [60,61,62]. a common ingredient in cream or ointment treatments. Numerous local and systemic adverse effects of topical steroids have been attributed to their continuous use. [63,64,65]
15 vitiligo patients of both sexes (F: M 1.14: 1) utilized betamethasone cream 0.05% twice daily throughout three-month research. Based on the patients' degrees of minimal pigmentation/no reaction, moderate, noticeable pigmentation, and outstanding pigmentation, the improvements of the patients were rated as (25%), (25-50%), (50-75%), and (> 75%), respectively. Compared to 40.0% of patients with limited pigmentation or no reaction, 46.7% and 13.3% showed a moderate or severe pigmentation response after therapy. [66,67]
Seven hundred thirty-one patients with moderate to severe plaque psoriasis with 3% to 20% body surface area participated in the 4-week Clobetasol Spray trial, which used two doses of clobetasol propionate spray 0.05% twice daily as treatment. The change in target plaque severity was the primary outcome measure. According to the major outcome measures scale, 80.0% of the patients in the therapy group were clear or nearly unambiguous and had a decrease in severity from the beginning. [68,69]
A topical anti-infective cream, silver sulfadiazine (Silvadene®, chemical 7 in Figure 7) is primarily used to prevent and cure burn injuries. Silver sulfadiazine solution with 1% API dissolves in water. Proteins become denaturized and enzyme activity is reduced by silver ions. Additionally, silver ions bind to proteins and surface membranes, leading to membrane proton leakage and cell death. Sulfadiazine competitively inhibits PABA, a naturally occurring bacterial substance that acts as a substrate for the dihydropteroate synthase enzyme. These organisms must carry out the blocked process to produce folic acid [70]. Silver sulfadiazine exhibits broad-spectrum action against both gram-positive and gram-negative pathogens. It has been demonstrated that it promotes wound and injury repair and has anti-infective qualities. [71,72]. Twenty-seven individuals with 2° burn injuries were randomly assigned to receive silver sulfadiazine throughout a 4-week study. After four weeks of treatment, the healing condition of 2° deep dermal burn wounds were determined to be (0–25%), (26–50%), (51–75%), and (76–100%), respectively, as poor healing, moderate healing, fast healing, and excellent healing. While 8 and 13 patients had a mild and quick recovery, six patients with 2° deep dermal burn lesions had poor healing. [73] Mixtures of creams, shampoos, powders, mouthwash, and gels contain both an anti-infective and a steroid component to treat skin or scalp infections. [74] Triamcinolone and dimethicone are ingredients in the drug (TriHeal80®; see components 8 and 9 in Figure 7). Topical corticosteroids produce similar antipruritic, anti-inflammatory, and vasoconstrictive effects. [75].
Triamcinolone is a phospholipase A2 inhibitor that acts on cell membranes to prevent the lysosomal membranes of leukocytes from rupturing. This prevents the production of arachidonic acid, which in turn lowers lipoxygenase and cyclooxygenase while inhibiting the production of prostaglandins and leukotrienes [76,77]. Dimethicone, a silicone oil, exhibits viscoelastic qualities. It has moisturizing properties, is utilized as a surfactant, antifoaming agent, and lubricant to cure skin irritation. To reduce the rate of water evaporation, dimethicone is used topically [78,79]. When used four times per day for two months and monitored for another two months, triamcinolone 0.1% mouthwash successfully treated oral lichen planus in 20 patients. All effectiveness endpoints assessed using the visual analog scale, the verbal health impact profile score, and the objective clinical score all revealed a significant improvement in the patients. [80,81,82]
Under the brand name Tri-Luma®, a triple combination cream is sold that includes the active components tretinoin, hydroquinone, and fluocinolone in concentrations of 0.01%, 4%, and 0.05%. [83]. Hydroquinone is the most often used skin-lightening or depigmenting substance (compound 10 in Figure 7). It treats dyschromic skin diseases such as melasma, chloasma, freckles, and post-inflammatory hyperpigmentation by suppressing melanin production. It stops tyrosinase from converting L-3,4-dihydroxyphenylalanine into melanin due to its structural similarity to a specific analog of melanin. [83,85] Fluocinolone (molecule 11 in Figure 8) treats symptoms, including itchiness, swelling, and redness caused by skin problems. [86,87] Retinol (compound 12 in Figure 8) cures skin aging. It was shown that it might be beneficial for concerns related to skin aging. The most remarkable feature is that treatment results manifest eight to twelve months after using the tretinoin 0.1% cream preparation. The most frequent side effects of tretinoin include very small skin irritability and a transient, mild, and clinically uncomfortable burning sensation. [85,88,89]. Sixty patients with moderate (grade 2) or severe (grade 3) melasma received treatment for eight weeks with the triple combination cream. At weeks 4, 6, and 8, the triple combination cream significantly improved the overall results, with an improvement rate of 73% (44/60). The percentage of participants who thought the triple combination cream was "excellent" as a treatment was 50%, while the most often mentioned adverse effects were erythema, burning, and desquamation. [90].
Additionally, a 12-week open-label trial was created to gauge the effectiveness and safety of applying topical retinol 0.15% twice daily. At the fourth, eighth, and twelve weeks, it was found that 39%, 77%, and 77% of patients, respectively, had significant improvement. When using topical retinol, dryness, erythema, peeling, stinging, and burning were some side effects that were tolerated.[91].
Dermatitis, eczema, rashes, and allergies are just a few of the skin conditions that TriDerm® is used to treat. The swelling, redness, and itching that are brought on by these various disorders are reduced by triamcinolone. It includes corticosteroids that range in strength from mild to potent. The mechanism of action of TriDerm is composed of betamethasone, clotrimazole, and gentamicin (compounds 13 and 14 in Figure 8), which results in the antipruritic, anti-inflammatory, and vasoconstrictive effects of betamethasone, as well as the broad-spectrum bactericidal antibiotic effect of gentamicin and the broad-spectrum antifungal effect of clotrimazole. The contents of the cell leak out when clotrimazole reacts with the fungal cell membrane. Gentamicin is an effective topical skin therapy for bacterial infections. [91,92,93,94,95]. The study included 68 patients with itchy dermatoses, including atopic dermatitis, contact dermatitis, and true eczema. 33 of the patients received a twice-daily application of a topical cream containing betamethasone, clotrimazole, and gentamicin on the affected body parts. The effectiveness of the therapy was assessed after 7, 14, and 28 days. On the seventh day of treatment, there is a reduction in the inflammatory process and subjective symptoms. Five of the 33 patients saw a scientific recovery on the fourteenth day of getting treatment. After 28 days of therapy, the patient had fully recovered medically. [96]
The main component of the topical anti-cancer drug Opzelura® is ruxolitinib (compound 15 in Figure 8). A class of drugs known as Janus kinase inhibitors, which includes roxolitinib, has an effect on the immune system. JAK inhibitors may reduce the immune system's ability to fight off infections. [97,98,99,100]. JAKs serve a variety of purposes. JAK1 and JAK3 increase lymphocyte existence and differentiation, whilst JAK2 increases the signal transduction of thrombopoietin and erythropoietin. JAKs are located in the cytoplasmic region of cytokine and growth factor receptors. JAKs are also activated and undergo cross- and tyrosine phosphorylation. Ruxolitinib has a low affinity for JAK3 but is a solid and selective inhibitor of JAK2 and JAK1. Ruxolitinib reduces plasma levels of pro-inflammatory cytokines and inhibits myeloproliferative by downregulating the JAK-STAT pathway [101,102]. The randomized controlled trials recommended using ruxolitinib 1.5% cream for treating vitiligo twice daily in various patients. It was shown to demonstrate clinically excellent repigmentation of all body areas, including the acral region, after 24 weeks, with continued improvement through week 52. It was well tolerated in patients with long-standing high contamination. [103,104].
Salicylic acid (Salvax®, compound 16 in Figure 8), podophyllum resin (Podocon-25®, compound 17 in Figure 9), and podofilox (Condylox®, compound 18 in Figure 9) are a few examples of topical keratolytic that are administered topically to the skin to soften keratin. It facilitates the peeling of skin cells. It supports the skin's capacity to retain moisture and aids in the treatment of dry skin conditions. generally used to treat skin diseases such as psoriasis, acne, warts, keratoses, and acne. [105,106]. More topical brand names for reducing skin pigmentation are included in Table 1.
Because of its keratolytic qualities, salicylic acid, a lipophilic B-hydroxy acid, is frequently used in cosmetic product formulations as a skin scaler for lightening. Arachidonic acid is reduced from converted to prostaglandins and thromboxanes by COX-1 and COX-2 inhibitors. Salicylic acid also has anti-inflammatory and antibacterial effects. [107,108]. Twenty Latin American women over the age of 18 with moderate to severe bilateral melasma participated in a small, potential randomized controlled trial to compare the efficacy of salicylic acid 20%–30% scaler every two weeks followed by up to eight weeks in combination with hydroquinone 4% twice daily for 14 weeks, versus hydroquinone 4% alone. A narrowband reflectance spectrophotometer (Mexameter MX-16) was used to quantify the degree of pigmentation on the affected and unaffected skin on each face. The Melasma Place and Severity Index (MASI) was used to assess the severity of the melasma. 33% of that 44% were regarded as having mild development and slight improvement, with 44% showing more significant progress on the peeled aspect. One patient (6%) was noted to have only slightly more growth on the unpeeled side. The peeled side had advanced more than the unpeeled side, according to 83% of the nonblinded patients (four somewhat, seven moderately, and four significantly). One patient (6%) thought the unpeeled aspect was more advanced, whereas twelve percent (12%) believed there was no difference.
5. Natural hyperpigmentation treatment
Despite the wide range of therapies available, a growing number of people are choosing plants and natural items as alternatives. Plant-based and natural remedies have been used for treating skin issues for ages, and they are gaining popularity as a secure and efficient method to treat skin hyperpigmentation. [111,112,113,114,115].
Vitamins A, B, C, and E can all be used to address skin pigmentation problems and are necessary for healthy skin. Each vitamin, which can be obtained in foods or supplements, has specific advantages. [116,117]
Niacin, Pantothenic acid, and biotin are the B vitamins most frequently found in skincare products. Niacin, also known as niacinamide, is a vitamin that is used in face creams and masks to minimize the appearance of enlarged pores, fine lines, and dullness. Pantothenic acid is also applied to dry, flaky skin as a moisturizer. Numerous hair, nail, and skin care products include biotin [118,119]. Ascorbic acid (vitamin C), an antioxidant, inhibits tyrosinase by binding to copper and suppressing the oxidative polymerization of melanin precursors, which prevents melanin synthesis in the melanogenesis pathway [120,121]. A statistically significant decrease from baseline to Week 16 was observed in a trial on 39 patients using 25% L-ascorbic acid dissolved in Nmethyl-2-pyrrolidone and dimethyl isosorbide, as indicated by MASI values and mexameter data. [122,123]. A particular kind of vitamin E is alpha-tocopheryl acetate. When fat is subjected to oxidation and during the spread of free radical reactions, vitamin E, a powerful chain-breaking antioxidant, prevents the synthesis of reactive oxygen species molecules. [124,125,126]
Artocarpus lakoocha and Glycyrrhiza glabra extracts have been reported to exhibit tyrosinase inhibitory effects and melanin pigment reduction. For the treatment of hyperpigmentation, the combination of 9:1 Artocarpus lakoocha and Glycyrrhiza glabra decreased melanin pigment by up to 53% in B16 cells by lowering the production of tyrosinase (TYR), microphthalmia-associated transcription factor (MITF), and tyrosinase-related protein-2 (TRP-2). [127,128,129]
Antioxidants and fatty acids included in oils like rosehip, jojoba, and argan oil aid in reducing inflammation and brightening the skin. Natural oils can also shield the skin from the effects of the environment, preventing further discoloration. Aloe vera also includes aloin (compound 19 in Figure 9), which has been demonstrated to lighten skin and function well as a nontoxic hyperpigmentation therapy. Sharique described aloe vera as a natural depigmenting ingredient. [130,131,132]
When used as an emollient, jojoba oil exhibits first-rate lubricity without having an oily or greasy texture in single-segment and emulsion structures. It can also contribute to the skin's effective water regulation during transpiration, reducing evaporation without obstructing the passage of gases or water vapor [133,134,135,136]. According to a study, jojoba oil (or its ozonized or hydrogenated derivatives) has emollient properties. The study discovered that a significant increase in skin surface flexibility developed within 5 minutes and persisted for hours, suggesting a potential application in solutions for dry skin [137]. Jojoba liquid wax was found to be just as effective at treating diaper rash as triamcinolone acetonide, nystatin, neomycin, and gramicidin. Jojoba oil is also an anti-inflammatory. Due to the absence of systemic adverse effects, jojoba had the benefit of being safer [138]. Additionally, it has anti-acne and anti-psoriasis qualities, which allow the dissolution of sebum deposits through the hair follicles due to its capacity to infiltrate the follicles, eliminate the comedones, and clear the skin [139].
In a research, ten women used argan oil as a bandage on their skin for 28 days. None of the women experienced itching or noticed any skin irritation or redness, demonstrating the oil's efficacy in reducing the amount of pigmentation. These women did observe a minor decrease in melanin content in the vicinity of the bandage, though, which lends credence to the idea that the oil lessens pigmentation. [140,141,142]. Licorice root extract, turmeric extract, and green tea extract are other herbal extracts high in antioxidants that help to reduce inflammation and brighten the skin.
Since ancient times, licorice root extract has been utilized for its medical benefits, particularly for skin care. It has glycyrrhizin, which has been shown to have antioxidant and anti-inflammatory properties. [143]. Given that it is thought to help enhance skin look and treat some skin disorders, these qualities make it a popular ingredient in skin care products [144]. Several research have been done to determine whether licorice root extract is effective for treating skin conditions. According to a study, licorice root extract is useful for reducing hyperpigmentation and lightening the skin [145]. Atopic dermatitis symptoms may be lessened by licorice root extract, according to a different study [146]. James M. Spencer also demonstrated in his research that licorice root extract was efficient in lessening the severity of rosacea, melasma, and acne [147]. Additionally, licorice root extract reduced the appearance of black spots and redness, as was discovered in a 2019 study by Maria Yusuf Dhariwala. [148]
Since ancient times, turmeric extract has been valued for its therapeutic benefits. It has a yellow tint and various health advantages due to the presence of the active component curcumin. when it comes to pigmentation and skin conditions. Strong anti-inflammatory qualities found in curcumin can help lessen skin inflammation brought on by a variety of skin conditions, including psoriasis and eczema [149,150,151,152]. Antioxidants included in turmeric extract reduce oxidative damage that can cause skin aging and pigmentation disorders like melasma by neutralizing free radicals [153]. Curcumin also has skin-lightening qualities. By preventing the formation of the melanin-producing enzyme tyrosinase, it can lessen hyperpigmentation and make the skin lighter. [154] Curcuminoids, which are found in turmeric, have exfoliating qualities that aid to gently remove dead skin cells and encourage skin regeneration, minimizing the appearance of hyperpigmentation and dark patches [155]. Using turmeric extract to treat skin issues was the subject of a 2018 study by Alexandra R. Vaughn. In psoriasis, eczema, and acne patients, the study found that turmeric extract was beneficial in lowering skin inflammation and enhancing skin health [156]. A topical cream with turmeric extract proved successful in lowering the severity of acne in patients after four weeks of treatment, according to a 2018 study by Penelope J. Kallis.[157]
Another organic component that has been investigated for its therapeutic advantages for the skin is green tea extract. It has a lot of polyphenols and antioxidants, as well as anti-inflammatory and skin-protective qualities [158,159,160]. Green tea extract works in a variety of ways to treat pigmentation issues and skin problems. Catechins and epigallocatechin gallate (EGCG), two antioxidants found in green tea, work to combat free radicals that can damage skin and speed up the aging process [161]. Green tea extract also has strong anti-inflammatory qualities that can help lessen skin irritation brought on by a variety of skin diseases such acne, eczema, and rosacea [162]. EGCG in green tea extract can help inhibit tyrosinase activity, reducing the production of melanin and thus lightening the skin [163]. Furthermore, green tea extract has been shown to offer some protection against UV radiation, which can cause skin damage and contribute to pigmentation disorders [164]. A clinical study has been conducted for 11 patients on the use of green tea extract for treating acne; this study found that green tea extract was effective in reducing the number of acne lesions and improving overall skin health [165]. Another published in 2017 found that green tea extract effectively reduced the appearance of fine lines and wrinkles in the skin [166].
Kojic acid (Enshine® cream 2%, compound 20 in Figure 9) has been found to be effective in treating various skin disorders and pigmentation issues due to its mechanism of action. It works by inhibiting the activity of tyrosine, which reduces the production of melanin, which can help to fade dark spots and hyperpigmentation [167,168,169]. In addition to its tyrosinase-inhibiting properties, kojic acid has antioxidant and anti-inflammatory properties; these can be particularly beneficial for individuals with acne, rosacea, and other inflammatory skin conditions [170,171,172,173]. One study published in 2016 by Peter J. Gust evaluated the efficacy of a cream containing 2% kojic acid, 10% glycolic acid, and 2% hydroquinone for treating melasma. The study involved 40 participants who applied the cream twice daily for 12 weeks. The results showed a significant reduction in the severity of melasma in the treated group compared to the control group, with no reported adverse effects [174]. In another study, Tamara Searle investigated using a cream containing 2% kojic acid, 1% arbutin, and 5% vitamin C to treat age spots. The study involved 60 participants who applied the cream twice daily for 12 weeks. The results showed a significant reduction in the number and severity of age spots in the treated group compared to the control group, with no reported adverse effects [175]. Several herbs and naturally occurring substances commonly used in skincare products for their ability to lighten skin and reduce hyperpigmentation are listed in Table 2.
Phlorotannins (compound 21 in Figure 9) from the brown algae (brown seaweed) play a crucial role in the reduction of hyperpigmented effects and the prevention of premature skin aging. They protect the skin from the sun's infrared and blue rays.
Moreover, it encourages the production of cellular energy, increasing the skin’s oxygenation. This process enhances cell innovation and decreases pigmentation and the skin’s general look. Their antioxidant activity stops the deterioration of the collagen that firms the skin [176,177,178]. Clinical trials and meta-analyses have investigated the effects of phlorotannins on skin disorders and pigmentation. A randomized, double-blind, placebo-controlled study published in 2022 found that a phlorotannin-rich Ecklonia cava (Phaeophyceae) extract improved skin hydration, elasticity, and wrinkle formation in women with dry skin. Another randomized, double-blind, placebo-controlled study found that a phlorotannin-rich extract of Ascophyllum nodosum reduced facial pigmentation and improved skin elasticity in women with age spots. [179,180]
Marine-derived chemicals from Undaria pinnatifida, Octopus vulgaris, and Sargassum polycystum, have all been investigated for their ability to enhance skin pigmentation and have antioxidant, anti-inflammatory, and immunomodulatory properties. These compounds include octaphlorethol A, fucoidan, and fucoxanthin (compounds 22-24 in Figure 9) [181,182,183,184,185,186]. Several studies have investigated the effects of octaphlorethol A on skin disorders and pigmentation. A study found that octaphlorethol A inhibited melanin production and reduced skin pigmentation in human melanoma cells. Another study found that octaphlorethol A reduced inflammation and improved skin barrier function in mice with atopic dermatitis. [187,188]. In addition, a randomized, double-blind, placebo-controlled study found that a cream containing fucoidan and marine collagen improved skin hydration, elasticity, and wrinkle formation in women with dry skin [189]. In addition, a randomized, double-blind, placebo-controlled study found that a cream containing fucoidan and marine collagen improved skin hydration, elasticity, and wrinkle formation in women with dry skin [190]. A survey of 11 randomized controlled trials found that the carotenoid pigment, fucoxanthin, supplementation was associated with a significant reduction in the severity of melasma. However, the authors noted that the quality of the inclusive studies was generally low, and more research is needed to confirm these findings [191,192,193].
6. Conclusion
Skin pigmentation refers to the color of an individual's skin, which is determined by the amount of melanin in the skin produced by melanocytes. Eumelanin and pheomelanin are the two primary forms of melanin. Dark skin tones are caused by eumelanin, which protects against skin cancer and sun damage. While pheomelanin produces lighter skin tones, which can control body temperature and offers protection from skin cancer. Some causes of skin pigmentation include genetics, sun exposure, hormonal changes, skin trauma, and certain medications. In addition, some skin pigmentation disorders, such as melasma, albinism, and vitiligo, which caused by genetic mutations.
There are two primary types of skin pigmentation; hyperpigmentation occurs when there is an overproduction of melanin, leading to areas of darker skin. This can be caused by sun exposure, hormonal changes, and certain medications. Or hypopigmentation occurs when there is a loss of melanin, leading to lighter skin areas. This can be caused by genetic conditions, skin trauma, and certain medications.
Clinical trials and meta-analysis show that oral medication by tranexamic acid and isotretinoin tablets could treat various skin illnesses, including eczema, melasma, and other related conditions. In addition, clinical trials indicate that the topical forms of betamethasone, clobetasol, silver sulfadiazine, triamcinolone, dimethicone, fluocinolone, hydroquinone, clotrimazole, ruxolitinib, salicylic acid, and tretinoin are effective in treating skin disorders. Furthermore, Natural extracts like rosehip, jojoba, argan oil, Aloe vera, Licorice root, curcumin, green tea, Kojic acid, phlorotannin,s and vitamins A, B, C, and E have potent anti-inflammatory properties that can help reduce inflammation in the skin caused by various skin conditions such as acne, eczema, and rosacea, which can be classified as a treatment for hyperpigmentation along with octaphlorethol A, fucoidan, and fucoxanthin marine extracts.
Author Contributions
A.M, A.J, D.K A.T and R.K wrote and edited the manuscript. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this review, which does not report new experimental results obtained by authors but contains a summary of already published data.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Acknowledgments
Reproduced with permission for Figure 3 that published by John Wiley and Sons 2011(A), BMJ Publishing Group Ltd, 2017 (B), Elsevier, 2017 (C,D). Reproduced with permission for figure 5 that published by JBMJ Publishing Group Ltd, 2012 (A), BMJ Publishing Group Ltd, 2021(B).
Conflicts of Interest
The authors declare no conflict of interest.
Sample Availability
Not applicable.
References
- Del Bino, S.; Duval, C.; Bernerd, F. Clinical and Biological Characterization of Skin Pigmentation Diversity and Its Consequences on UV Impact. Int. J. Mol. Sci. 2018, 19, 2668. [Google Scholar] [CrossRef] [PubMed]
- Martin, A.R.; Lin, M.; Granka, J.M.; Myrick, J.W.; Liu, X.; Sockell, A.; Atkinson, E.G.; Werely, C.J.; Möller, M.; Sandhu, M.S.; et al. An Unexpectedly Complex Architecture for Skin Pigmentation in Africans. Cell 2017, 171, 1340–1353. [Google Scholar] [CrossRef] [PubMed]
- Nasti, T.H.; Timares, L. MC1R, Eumelanin and Pheomelanin: Their Role in Determining the Susceptibility to Skin Cancer. Photochem. Photobiol. 2015, 91, 188–200. [Google Scholar] [CrossRef] [PubMed]
- Solano, F. Photoprotection and Skin Pigmentation: Melanin-Related Molecules and Some Other New Agents Obtained from Natural Sources. Molecules 2020, 25, 1537. [Google Scholar] [CrossRef] [PubMed]
- Polidori, C.; Jorge, A.; Ornosa, C. Eumelanin and pheomelanin are predominant pigments in bumblebee (Apidae:Bombus) pubescence. PeerJ 2017, 5, e3300. [Google Scholar] [CrossRef] [PubMed]
- Hu, S.; Zhai, P.; Chen, Y.; Zhao, B.; Yang, N.; Wang, M.; Xiao, Y.; Bao, G.; Wu, X. Morphological Characterization and Gene Expression Patterns for Melanin Pigmentation in Rex Rabbit. Biochem. Genet. 2019, 57, 734–744. [Google Scholar] [CrossRef]
- Baek, S.H.; Lee, S.H. Sesamol decreases melanin biosynthesis in melanocyte cells and zebrafish: Possible involvement of MITF via the intracellular cAMP and p38/JNK signalling pathways. Exp. Dermatol. 2015, 24, 761–766. [Google Scholar] [CrossRef]
- Madelaine, R.; Ngo, K.J.; Skariah, G.; Mourrain, P. Genetic deciphering of the antagonistic activities of the melanin-concentrating hormone and melanocortin pathways in skin pigmentation. PLOS Genet. 2020, 16, e1009244. [Google Scholar] [CrossRef]
- Ozdeslik, R.N.; Olinski, L.E.; Trieu, M.M.; Oprian, D.D.; Oancea, E. Human nonvisual opsin 3 regulates pigmentation of epidermal melanocytes through functional interaction with melanocortin 1 receptor. Proc. Natl. Acad. Sci. USA 2019, 116, 11508–11517. [Google Scholar] [CrossRef]
- Horrell, E.M.W.; Boulanger, M.C.; D’orazio, J.A. Melanocortin 1 Receptor: Structure, Function, and Regulation. Front. Genet. 2016, 7, 95. [Google Scholar] [CrossRef]
- Suherlan, S., Fakih, T. M., & Effendi, D. H. (2021). Uji In-Silico Aktivitas Melanogenesis Senyawa Ternatin Bunga Kembang Telang (Clitoria ternatea) terhadap Reseptor Tirosinase. Prosiding Farmasi, 849-856.
- Jablonski, N.G. The evolution of human skin pigmentation involved the interactions of genetic, environmental, and cultural variables. Pigment. Cell Melanoma Res. 2021, 34, 707–729. [Google Scholar] [CrossRef] [PubMed]
- Ainger, S.A.; Jagirdar, K.; Lee, K.J.; Soyer, H.P.; Sturm, R.A. Skin Pigmentation Genetics for the Clinic. Dermatology 2017, 233, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Feng, Y.; A McQuillan, M.; A Tishkoff, S. Evolutionary genetics of skin pigmentation in African populations. Hum. Mol. Genet. 2021, 30, R88–R97. [Google Scholar] [CrossRef] [PubMed]
- Kita, R.; Fraser, H.B. Local Adaptation of Sun-Exposure-Dependent Gene Expression Regulation in Human Skin. PLOS Genet. 2016, 12, e1006382. [Google Scholar] [CrossRef] [PubMed]
- Armenta, A.M.; Henkel, E.D.; Ahmed, A.M. Pigmentation Disorders in the Elderly. Drugs Aging 2019, 36, 235–245. [Google Scholar] [CrossRef] [PubMed]
- Adigun, C.G. Adverse Drug Reactions of the Lower Extremities. Clin. Podiatr. Med. Surg. 2016, 33, 397–408. [Google Scholar] [CrossRef] [PubMed]
- Nicolaidou, E.; Katsambas, A.D. Pigmentation disorders: hyperpigmentation and hypopigmentation. Clin. Dermatol. 2014, 32, 66–72. [Google Scholar] [CrossRef]
- Böhm, M. (2021). Disorders of Melanin Pigmentation. In Braun-Falco´ s Dermatology (pp. 1-35). Berlin, Heidelberg: Springer Berlin Heidelberg.
- Ma, E.Z.; Zhou, A.E.; Hoegler, K.M.; Khachemoune, A. Oculocutaneous albinism: epidemiology, genetics, skin manifestation, and psychosocial issues. Arch. Dermatol. Res. 2022, 315, 107–116. [Google Scholar] [CrossRef]
- Federico, J. R., & Krishnamurthy, K. (2018). Albinism.
- Lee, D.; Kim, C.; Lee, J. Trichrome vitiligo in segmental type. Photodermatol. Photoimmunol. Photomed. 2011, 27, 111–112. [Google Scholar] [CrossRef] [PubMed]
- Hill, J.P.; Batchelor, J.M. An approach to hypopigmentation. BMJ 2017, 356, i6534. [Google Scholar] [CrossRef] [PubMed]
- Silpa-Archa, N.; Kohli, I.; Chaowattanapanit, S.; Lim, H.W.; Hamzavi, I. Postinflammatory hyperpigmentation: A comprehensive overview: Epidemiology, pathogenesis, clinical presentation, and noninvasive assessment technique. J. Am. Acad. Dermatol. 2017, 77, 591–605. [Google Scholar] [CrossRef] [PubMed]
- Kallini, J.R.; Riaz, F.; Khachemoune, A. Tinea versicolor in dark-skinned individuals. Int. J. Dermatol. 2014, 53, 137–141. [Google Scholar] [CrossRef] [PubMed]
- Miazek, N., Michalek, I., Pawlowska-Kisiel, M., Olszewska, M., & Rudnicka, L. Pityriasis Alba—Common Disease, Enigmatic Entity: Up-to-Date Review of the Literature. Pediatr. Dermatol. 2015, 32, 786–791. [CrossRef]
- Jing, J.; Man, X.-Y. Vitiligo-like depigmentation in a patient treated with PD-1 antibody. BMJ 2021, 374. [Google Scholar] [CrossRef]
- McMichael, L. (2012). Skin camouflage. BMJ, 344.
- Sheth, P.; Shah, H.; Dave, J. Periorbital Hyperpigmentation: A Study of its Prevalence, Common Causative Factors and its Association with Personal Habits and Other Disorders. Indian J. Dermatol. 2014, 59, 151–157. [Google Scholar] [CrossRef]
- Choi, W.; Yin, L.; Smuda, C.; Batzer, J.; Hearing, V.J.; Kolbe, L. Molecular and histological characterization of age spots. Exp. Dermatol. 2016, 26, 242–248. [Google Scholar] [CrossRef]
- Baxter, L.L.; Pavan, W.J. The etiology and molecular genetics of human pigmentation disorders. Wiley Interdiscip. Rev. Dev. Biol. 2012, 2, 379–392. [Google Scholar] [CrossRef] [PubMed]
- Yadalla, H. K. K., & Aradhya, S. (2011). Post acne hyperpigmentation: A brief review. Our Dermatol Online, 2(4), 230-231.
- Plensdorf, S.; Livieratos, M.; Dada, N. Pigmentation Disorders: Diagnosis and Management. Am Fam Physician. 2017, 96, 797–804.
- Woolery-Lloyd, H., & Kammer, J. N. (2011, September). Treatment of hyperpigmentation. In Seminars in cutaneous medicine and surgery (Vol. 30, No. 3, pp. 171-175). WB Saunders.
- Bala, H.R.; Lee, S.; Wong, C.; Pandya, A.; Rodrigues, M. Oral Tranexamic Acid for the Treatment of Melasma: A Review. Dermatol. Surg. 2018, 44, 814–825. [Google Scholar] [CrossRef] [PubMed]
- Ali, A. A., Al-Obaidi, Z. M. J., Raauf, A. M., & Mahmood, H. S. (2020). A Comparative, Randomized, Double-Blinded, and Vehicle-Controlled Study for the Reduction in Facial Pigmentation after Treatment with both Tranexamic Acid and Tranexamic Acid Ethyl Ester. Systematic Reviews in Pharmacy, 11(6), 563-567.
- Lee, D.H.; Oh, I.Y.; Koo, K.T.; Suk, J.M.; Jung, S.W.; Park, J.O.; Kim, B.J.; Choi, Y.M. Reduction in facial hyperpigmentation after treatment with a combination of topical niacinamide and tranexamic acid: a randomized, double-blind, vehicle-controlled trial. Ski. Res. Technol. 2013, 20, 208–212. [Google Scholar] [CrossRef]
- Kaur, A., Bhalla, M., & Sarkar, R. (2020). Tranexamic acid in melasma: a review. Pigment International, 7(1), 12. [CrossRef]
- Maeda, K. Mechanism of Action of Topical Tranexamic Acid in the Treatment of Melasma and Sun-Induced Skin Hyperpigmentation. Cosmetics 2022, 9, 108. [Google Scholar] [CrossRef]
- McKesey, J.; Tovar-Garza, A.; Pandya, A.G. Melasma Treatment: An Evidence-Based Review. Am. J. Clin. Dermatol. 2019, 21, 173–225. [Google Scholar] [CrossRef]
- Grimes, P.; Ijaz, S.; Nashawati, R.; Kwak, D. New oral and topical approaches for the treatment of melasma. Int. J. Women's Dermatol. 2018, 5, 30–36. [Google Scholar] [CrossRef] [PubMed]
- Artzi, O.; Horovitz, T.; Bar-Ilan, E.; Shehadeh, W.; Koren, A.; Zusmanovitch, L.; Mehrabi, J.N.; Salameh, F.; Nelkenbaum, G.I.; Zur, E.; et al. The pathogenesis of melasma and implications for treatment. J. Cosmet. Dermatol. 2021, 20, 3432–3445. [Google Scholar] [CrossRef] [PubMed]
- Taraz, M.; Niknam, S.; Ehsani, A.H. Tranexamic acid in treatment of melasma: A comprehensive review of clinical studies. Dermatol. Ther. 2017, 30, e12465. [Google Scholar] [CrossRef]
- Tse, T.W.; Hui, E. Tranexamic acid: an important adjuvant in the treatment of melasma. J. Cosmet. Dermatol. 2013, 12, 57–66. [Google Scholar] [CrossRef] [PubMed]
- Sharma, R.; Mahajan, V.K.; Mehta, K.S.; Chauhan, P.S.; Rawat, R.; Shiny, T.N. Therapeutic efficacy and safety of oral tranexamic acid and that of tranexamic acid local infiltration with microinjections in patients with melasma: a comparative study. Clin. Exp. Dermatol. 2017, 42, 728–734. [Google Scholar] [CrossRef] [PubMed]
- Kim, S.J.; Park, J.-Y.; Shibata, T.; Fujiwara, R.; Kang, H.Y. Efficacy and possible mechanisms of topical tranexamic acid in melasma. Clin. Exp. Dermatol. 2016, 41, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Sofen, B.; Prado, G.; Emer, J. Melasma and Post Inflammatory Hyperpigmentation: Management Update and Expert Opinion. 2016, 21. [Google Scholar]
- DEMİR, B., ÇİÇEK, D., BİLİK, L., AYDOĞDU, E. G., ARTAŞ, H., DEMİRPOLAT, N., & ERGİN, C. (2017). Oral isotretinoin induced pigmentation disorder: A case report. Firat Tip Derg, 22(3).
- Mysore, V.; Mahadevappa, O.H.; Barua, S.; Majid, I.; Viswanath, V.; Bhat, R.M.; Talwar, S.; Thurakkal, S.; Aurangabadkar, S.J.; Chatterjee, M.; et al. Standard guidelines of care: Performing procedures in patients on or recently administered with isotretinoin. J. Cutan. Aesthetic Surg. 2017, 10, 186–194. [Google Scholar] [CrossRef]
- Bagatin, E., & Costa, C. S. (2020). The use of isotretinoin for acne–an update on optimal dosing, surveillance, and adverse effects. Expert review of clinical pharmacology, 13(8), 885-897. [CrossRef]
- Fallah, H.; Rademaker, M. Isotretinoin in the management of acne vulgaris: practical prescribing. Int. J. Dermatol. 2020, 60, 451–460. [Google Scholar] [CrossRef] [PubMed]
- Villani, A.; Nastro, F.; Di Vico, F.; Fabbrocini, G.; Annunziata, M.C.; Genco, L. Oral isotretinoin for acne: a complete overview. Expert Opin. Drug Saf. 2022, 21, 1027–1037. [Google Scholar] [CrossRef] [PubMed]
- pring, L. K., Krakowski, A. C., Alam, M., Bhatia, A., Brauer, J., Cohen, J., ... & Zaenglein, A. L. (2017). Isotretinoin and timing of procedural interventions: a systematic review with consensus recommendations. JAMA dermatology, 153(8), 802-809. [CrossRef]
- Chu, S.; Michelle, L.; Ekelem, C.; Sung, C.T.; Rojek, N.; Mesinkovska, N.A. Oral isotretinoin for the treatment of dermatologic conditions other than acne: a systematic review and discussion of future directions. Arch. Dermatol. Res. 2020, 313, 391–430. [Google Scholar] [CrossRef] [PubMed]
- Ye, D., Xue, H., Huang, S., He, S., Li, Y., Liu, J., ... & Zeng, W. (2022). A prospective, randomized, split-face study of concomitant administration of low-dose oral isotretinoin with 30% salicylic acid chemical peeling for the treatment of acne vulgaris in Asian population.
- Dréno, B.; Araviiskaia, E.; Kerob, D.; Andriessen, A.; Anfilova, M.; Arenbergerova, M.; Barrios, O.L.F.; Mokos, Z.B.; Haedersdal, M.; Hofmann, M.A.; et al. Nonprescription acne vulgaris treatments: Their role in our treatment armamentarium—An international panel discussion. J. Cosmet. Dermatol. 2020, 19, 2201–2211. [Google Scholar] [CrossRef] [PubMed]
- Rachmin, I.; Ostrowski, S.M.; Weng, Q.Y.; Fisher, D.E. Topical treatment strategies to manipulate human skin pigmentation. Adv. Drug Deliv. Rev. 2020, 153, 65–71. [Google Scholar] [CrossRef]
- Bose, S. K., & Ortonne, J. P. (1998). Pigmentation: dyschromia. In Textbook of cosmetic dermatology (pp. 391-415). Martin-Dunitz Ltd London.
- Yasir, M., Goyal, A., & Sonthalia, S. (2018). Corticosteroid adverse effects.
- Robert, C.; Hwu, W.-J.; Hamid, O.; Ribas, A.; Weber, J.S.; Daud, A.I.; Hodi, F.S.; Wolchok, J.D.; Mitchell, T.C.; Hersey, P.; et al. Long-term safety of pembrolizumab monotherapy and relationship with clinical outcome: A landmark analysis in patients with advanced melanoma. Eur. J. Cancer 2020, 144, 182–191. [Google Scholar] [CrossRef]
- Cho, J.H.; Bhutani, S.; Kim, C.H.; Irwin, M.R. Anti-inflammatory effects of melatonin: A systematic review and meta-analysis of clinical trials. Brain, Behav. Immun. 2021, 93, 245–253. [Google Scholar] [CrossRef] [PubMed]
- Marathe, P.; Karekar, S.; Nagarajan, V.; Khopkar, U.; Chikhalkar, S.; Desai, P.; Dongre, M. Use of topical steroids in dermatology: A questionnaire based study. Indian Dermatol. Online J. 2020, 11, 725–730. [Google Scholar] [CrossRef] [PubMed]
- Chadderdon, C., Gaston, R. G., Loeffler, B. J., & Lewis, D. (2017). Betamethasone Versus Ketorolac Injection for the Treatment of De Quervain's Tenosynovitis: A Double-Blind Randomized Clinical Trial: Level 1 Evidence. Journal of Hand Surgery, 42(9), S45-S46.
- Patel, H.K.; Barot, B.S.; Parejiya, P.B.; Shelat, P.K.; Shukla, A. Topical delivery of clobetasol propionate loaded microemulsion based gel for effective treatment of vitiligo: Ex vivo permeation and skin irritation studies. Colloids Surfaces B: Biointerfaces 2013, 102, 86–94. [Google Scholar] [CrossRef] [PubMed]
- Khaitan, B.K.; Sindhuja, T. Autoimmunity in vitiligo: Therapeutic implications and opportunities. Autoimmun. Rev. 2021, 21, 102932. [Google Scholar] [CrossRef] [PubMed]
- Eleftheriadou, V.; Atkar, R.; Batchelor, J.; McDonald, B.; Novakovic, L.; Patel, J.V.; Ravenscroft, J.; Rush, E.; Shah, D.; Shah, R.; et al. British Association of Dermatologists guidelines for the management of people with vitiligo 2021. Br. J. Dermatol. 2021, 186, 18–29. [Google Scholar] [CrossRef] [PubMed]
- A Habet, K.; Kolli, S.S.; Pona, A.; Feldman, S.R. A review of topical corticosteroid sprays for the treatment of inflammatory dermatoses. Dermatol. Online J. 2019, 25. [Google Scholar] [CrossRef]
- Gajinov, Z. Corticosteroid topical therapy range: Fluocinolone-acetonide gel. Galen. Med J. 2022, 1, 17–22. [Google Scholar] [CrossRef]
- Medici, S.; Peana, M.F.; Nurchi, V.M.; Zoroddu, M.A. Medical Uses of Silver: History, Myths, and Scientific Evidence. J. Med. Chem. 2019, 62, 5923–5943. [Google Scholar] [CrossRef]
- Bandyopadhyay, D. Topical antibacterials in dermatology. Indian J. Dermatol. 2021, 66, 117–125. [Google Scholar] [CrossRef]
- Adhya, A.; Bain, J.; Dutta, G.; Hazra, A.; Majumdar, B.; Ray, O.; Ray, S.; Adhikari, S. Healing of burn wounds by topical treatment: A randomized controlled comparison between silver sulfadiazine and nano-crystalline silver. J. Basic Clin. Pharm. 2015, 6, 29–34. [Google Scholar] [CrossRef] [PubMed]
- Nethi, S.K.; Das, S.; Patra, C.R.; Mukherjee, S. Recent advances in inorganic nanomaterials for wound-healing applications. Biomater. Sci. 2019, 7, 2652–2674. [Google Scholar] [CrossRef] [PubMed]
- Srivastava, S.; Patil, A.; Prakash, C.; Kumari, H. Comparison of Intralesional Triamcinolone Acetonide, 5-Fluorouracil, and Their Combination in Treatment of Keloids. World J. Plast. Surg. 2018, 7, 212–219. [Google Scholar] [CrossRef] [PubMed]
- A Khan, H.; Sahibzada, M.N.; Paracha, M.M. Comparison of the efficacy of intralesional bleomycin versus intralesional triamcinolone acetonide in the treatment of keloids. Dermatol. Ther. 2019, 32, e13036. [Google Scholar] [CrossRef]
- Krithika, C.L.; Anand, S.N.; Subramani, G.P. Topical Curcumin and Triamcinolone Acetonide in Recurrent Minor Aphthous Ulcers: A Pilot Trial. J. Contemp. Dent. Pr. 2020, 21, 884–890. [Google Scholar] [CrossRef]
- Kwiatkowska, D.; Wicka, M.; Bulska, E.; Kaliszewski, P. Investigation of the Excretion of Triamcinolone Acetonide and Its Metabolite. Separations 2023, 10, 164. [Google Scholar] [CrossRef]
- Mangion, S.E.; Mackenzie, L.; Roberts, M.S.; Holmes, A.M. Seborrheic dermatitis: topical therapeutics and formulation design. Eur. J. Pharm. Biopharm. 2023, 185, 148–164. [Google Scholar] [CrossRef]
- Atluri, K.; Manne, S.; Nalamothu, V.; Mantel, A.; Sharma, P.K.; Babu, R.J. Advances in Formulation and Therapeutic Strategies for the Treatment of Atopic Dermatitis. Crit. Rev. Ther. Drug Carr. Syst. 2023, 40, 1–87. [Google Scholar] [CrossRef]
- Sandhu, S.; Klein, B.A.; Al-Hadlaq, M.; Chirravur, P.; Bajonaid, A.; Xu, Y.; Intini, R.; Hussein, M.; Vacharotayangul, P.; Sroussi, H.; et al. Oral lichen planus: comparative efficacy and treatment costs—a systematic review. BMC Oral Heal. 2022, 22, 1–21. [Google Scholar] [CrossRef]
- Pakravan, F., Ghalayani, P., Emami, H., Isfahani, M. N., & Noorshargh, P. (2019). A novel formulation for radiotherapy-induced oral mucositis: Triamcinolone acetonide mucoadhesive film. Journal of research in medical sciences: the official journal of Isfahan University of Medical Sciences, 24. [CrossRef]
- Mangold, A. R., & Pittelkow, M. R. (2017). Lichen planus. Clinical and Basic Immunodermatology, 551-576.
- Nasrollahi, S.A.; Sabet, M.; Samadi, A.; Ayatollahi, A.; Yadangi, S.; Abels, C.; Firooz, A. Evaluation of the safety and efficacy of a triple combination cream (hydroquinone, tretinoin, and fluocinolone) for treatment of melasma in Middle Eastern skin. Clin. Cosmet. Investig. Dermatol. 2019, ume 12, 437–444. [Google Scholar] [CrossRef]
- Dreher, F., Draelos, Z. D., Gold, M. H., Goldman, M. P., Fabi, S. G., & Puissegur Lupo, M. L. (2013). Efficacy of hydroquinone-free skin-lightening cream for photoaging. Journal of cosmetic dermatology, 12(1), 12-17. [CrossRef]
- Banihashemi, M.; Zabolinejad, N.; Jaafari, M.R.; Salehi, M.; Jabari, A. Comparison of therapeutic effects of liposomal Tranexamic Acid and conventional Hydroquinone on melasma. J. Cosmet. Dermatol. 2015, 14, 174–177. [Google Scholar] [CrossRef] [PubMed]
- Pradhan, M.; Singh, D.; Murthy, S.N.; Singh, M.R. Design, characterization and skin permeating potential of Fluocinolone acetonide loaded nanostructured lipid carriers for topical treatment of psoriasis. Steroids 2015, 101, 56–63. [Google Scholar] [CrossRef] [PubMed]
- Treesirichod, A.; Chaithirayanon, S.; Chaikul, T.; Chansakulporn, S. The randomized trials of 10% urea cream and 0.025% tretinoin cream in the treatment of acanthosis nigricans. J. Dermatol. Treat. 2020, 32, 837–842. [Google Scholar] [CrossRef] [PubMed]
- Bagatin, E.; Gonçalves, H.D.S.; Sato, M.; Almeida, L.M.C.; Miot, H.A. Comparable efficacy of adapalene 0.3% gel and tretinoin 0.05% cream as treatment for cutaneous photoaging. Eur. J. Dermatol. 2018, 28, 343–350. [Google Scholar] [CrossRef]
- Nautiyal, A.; Wairkar, S. Management of hyperpigmentation: Current treatments and emerging therapies. Pigment. Cell Melanoma Res. 2021, 34, 1000–1014. [Google Scholar] [CrossRef]
- Ferraris, C.; Rimicci, C.; Garelli, S.; Ugazio, E.; Battaglia, L. Nanosystems in Cosmetic Products: A Brief Overview of Functional, Market, Regulatory and Safety Concerns. Pharmaceutics 2021, 13, 1408. [Google Scholar] [CrossRef]
- Usatine, R.P.; Tinitigan, M. Diagnosis and treatment of lichen planus. Am. Fam. Physician 2011, 84, 53–60. [Google Scholar]
- Korabiusz, K., Wawryków, A., Fabian-Danielewska, A., Stecko, M., Wilczyńska, A., Janik-Fuks, I., ... & Harasimowicz, J. (2019). Laser removal of tattoo-a case report. Journal of Education, Health and Sport, 9(6), 415-419.
- Doucette, K., Forster, S., & Marcus, A. (2018, April). Study to assess visual elimination of a novel otic gel (florfenicol, terbinafine, betamethasone acetate) in comparison to an otic solution (florfenicol, terbinafine, mometasone furoate) and an otic suspension (gentamicin sulfate, clotrimazole, mometasone furoate monohydrate) in dogs immediately after application to the ear canal. In BSAVA Congress Proceedings 2018 (pp. 489-489). BSAVA Library.
- Grammatikova, N. . Comparative Study of the Antimicrobial Activity of Combined Topical Medicinal Formulations of Betamethasone, Gentamicin, and Clotrimazole In Vitro. Pharm. Chem. J. 2020, 53, 971–975. [Google Scholar] [CrossRef]
- Cole, L. K., Rajala-Schultz, P. J., & Lorch, G. (2018). Conductive hearing loss in four dogs associated with the use of ointment-based otic medications. Veterinary dermatology, 29(4), 341-e120. [CrossRef]
- Hikmatovich, I. N. (2023). Evaluation of the Efficacy of External Therapy in Sick Children with Alergodermatosis. Web of Semantic: Universal Journal on Innovative Education, 2(2), 50-54.
- Harris, J.E.; Rashighi, M.; Nguyen, N.; Jabbari, A.; Ulerio, G.; Clynes, R.; Christiano, A.M.; Mackay-Wiggan, J. Rapid skin repigmentation on oral ruxolitinib in a patient with coexistent vitiligo and alopecia areata (AA). J. Am. Acad. Dermatol. 2015, 74, 370–371. [Google Scholar] [CrossRef] [PubMed]
- Rosmarin, D.; Pandya, A.G.; Lebwohl, M.; Grimes, P.; Hamzavi, I.; Gottlieb, A.B.; Butler, K.; Kuo, F.; Sun, K.; Ji, T.; et al. Ruxolitinib cream for treatment of vitiligo: a randomised, controlled, phase 2 trial. Lancet 2020, 396, 110–120. [Google Scholar] [CrossRef] [PubMed]
- Rothstein, B.; Joshipura, D.; Saraiya, A.; Abdat, R.; Ashkar, H.; Turkowski, Y.; Sheth, V.; Huang, V.; Au, S.C.; Kachuk, C.; et al. Treatment of vitiligo with the topical Janus kinase inhibitor ruxolitinib. J. Am. Acad. Dermatol. 2017, 76, 1054–1060. [Google Scholar] [CrossRef]
- Sheikh, A.; Rafique, W.; Owais, R.; Malik, F.; Ali, E. FDA approves Ruxolitinib (Opzelura) for Vitiligo Therapy: A breakthrough in the field of dermatology. Ann. Med. Surg. 2022, 81, 104499. [Google Scholar] [CrossRef]
- Shreberk-Hassidim, R.; Ramot, Y.; Zlotogorski, A. Janus kinase inhibitors in dermatology: A systematic review. J. Am. Acad. Dermatol. 2017, 76, 745–753. [Google Scholar] [CrossRef]
- Chapman, S.; Kwa, M.; Gold, L.S.; Lim, H.W. Janus kinase inhibitors in dermatology: Part I. A comprehensive review. J. Am. Acad. Dermatol. 2021, 86, 406–413. [Google Scholar] [CrossRef] [PubMed]
- Rosmarin, D.; Passeron, T.; Pandya, A.G.; Grimes, P.; Harris, J.E.; Desai, S.R.; Lebwohl, M.; Ruer-Mulard, M.; Seneschal, J.; Wolkerstorfer, A.; et al. Two Phase 3, Randomized, Controlled Trials of Ruxolitinib Cream for Vitiligo. New Engl. J. Med. 2022, 387, 1445–1455. [Google Scholar] [CrossRef] [PubMed]
- Seneschal, J.; Wolkerstorfer, A.; Desai, S.R.; Grimes, P.; Ezzedine, K.; Kornacki, D.; Wei, S.; Butler, K.; Rosmarin, D. Efficacy and safety of ruxolitinib cream for the treatment of vitiligo by patient demographics and baseline clinical characteristics: Week 52 pooled subgroup analysis from two randomized phase 3 studies. Br. J. Dermatol. 2023, 188. [Google Scholar] [CrossRef]
- Sripathi, S. K., & Lalitha, P. (2016). Keratolytic Molecule Aided Inhibition of DNA Damage and Tyrosinase Activity of a Herbal Formulation. International Journal of BioSciences & Technology, 9(2).
- Arif, T. Salicylic acid as a peeling agent: a comprehensive review. Clin. Cosmet. Investig. Dermatol. 2015, ume 8, 455–461. [Google Scholar] [CrossRef]
- Liu, J.; Jiang, R.; Zhou, J.; Xu, X.; Sun, Z.; Li, J.; Chen, X.; Li, Z.; Yan, X.; Zhao, D.; et al. Salicylic acid in ginseng root alleviates skin hyperpigmentation disorders by inhibiting melanogenesis and melanosome transport. Eur. J. Pharmacol. 2021, 910, 174458. [Google Scholar] [CrossRef] [PubMed]
- Colantonio, S.; Rivers, J.K. Botanicals With Dermatologic Properties Derived From First Nations Healing: Part 2—Plants and Algae. J. Cutan. Med. Surg. 2016, 21, 299–307. [Google Scholar] [CrossRef]
- Karnes, J.B.; Usatine, R.P. Management of external genital warts. Am. Fam. Physician 2014, 90.
- Lu, J.; Cong, T.; Wen, X.; Li, X.; Du, D.; He, G.; Jiang, X. Salicylic acid treats acne vulgaris by suppressing AMPK/SREBP1 pathway in sebocytes. Exp. Dermatol. 2019, 28, 786–794. [Google Scholar] [CrossRef]
- Yeoh, S. C., & Goh, C. F. (2021). Topical delivery of salicylates. Drug delivery and translational research, 1-21. [CrossRef]
- Ogbechie-Godec, O.A.; Elbuluk, N. Melasma: an Up-to-Date Comprehensive Review. Dermatol. Ther. 2017, 7, 305–318. [Google Scholar] [CrossRef] [PubMed]
- Kaufman, B.P.; Aman, T.; Alexis, A.F. Postinflammatory Hyperpigmentation: Epidemiology, Clinical Presentation, Pathogenesis and Treatment. Am. J. Clin. Dermatol. 2018, 19, 489–503. [Google Scholar] [CrossRef] [PubMed]
- Kanlayavattanakul, M.; Lourith, N. Plants and Natural Products for the Treatment of Skin Hyperpigmentation – A Review. Planta Medica 2018, 84, 988–1006. [Google Scholar] [CrossRef] [PubMed]
- Hollinger, J.C.; Angra, K.; Halder, R.M. Are Natural Ingredients Effective in the Management of Hyperpigmentation? A Systematic Review. J. Clin. Aesthetic Dermatol. 2018, 11, 28–37. [Google Scholar]
- Panzella, L.; Napolitano, A. Natural and Bioinspired Phenolic Compounds as Tyrosinase Inhibitors for the Treatment of Skin Hyperpigmentation: Recent Advances. Cosmetics 2019, 6, 57. [Google Scholar] [CrossRef]
- Grimes, P.; Bhawan, J.; Howell, M.; Desai, S.; Coryell, E.; Einziger, M.; Simpson, A.; Yaroshinsky, A.; McCraw, T. Histopathological Changes Induced by Malassezin: A Novel Natural Microbiome Indole for Treatment of Facial Hyperpigmentation. J. Drugs Dermatol. 2022, 21, 141–145. [Google Scholar] [CrossRef] [PubMed]
- Nautiyal, A.; Wairkar, S. Management of hyperpigmentation: Current treatments and emerging therapies. Pigment. Cell Melanoma Res. 2021, 34, 1000–1014. [Google Scholar] [CrossRef] [PubMed]
- Karadas, F.; Erdoğan, S.; Kor, D.; Oto, G.; Uluman, M. The Effects of Different Types of Antioxidants (Se, Vitamin E and Carotenoids) in Broiler Diets on the Growth Performance, Skin Pigmentation and Liver and Plasma Antioxidant Concentrations. Braz. J. Poult. Sci. 2016, 18, 101–116. [Google Scholar] [CrossRef]
- Lucock, M.D. The evolution of human skin pigmentation: A changing medley of vitamins, genetic variability, and UV radiation during human expansion. Am. J. Biol. Anthr. 2022, 180, 252–271. [Google Scholar] [CrossRef]
- Rembe, J.-D.; Fromm-Dornieden, C.; Stuermer, E.K. Effects of Vitamin B Complex and Vitamin C on Human Skin Cells: Is the Perceived Effect Measurable? Adv. Ski. Wound Care 2018, 31, 225–233. [Google Scholar] [CrossRef]
- Farzanfar, S.; Kouzekonan, G.S.; Mirjani, R.; Shekarchi, B. Vitamin B12-loaded polycaprolacton/gelatin nanofibrous scaffold as potential wound care material. Biomed. Eng. Lett. 2020, 10, 547–554. [Google Scholar] [CrossRef] [PubMed]
- Vivcharenko, V.; Wojcik, M.; Przekora, A. Cellular Response to Vitamin C-Enriched Chitosan/Agarose Film with Potential Application as Artificial Skin Substitute for Chronic Wound Treatment. Cells 2020, 9, 1185. [Google Scholar] [CrossRef] [PubMed]
- Barrios-Garay, K.; Toledano-Serrabona, J.; Gay-Escoda, C.; Sánchez-Garcés, M. Clinical effect of vitamin C supplementation on bone healing: A systematic review. Med. Oral Patol. Oral Y Cirugía Bucal 2022, 27, e205–e215. [Google Scholar] [CrossRef] [PubMed]
- Al-Niaimi, F.; Zhen Chiang, N.Y. Topical Vitamin C and the Skin: Mechanisms of Action and Clinical Applications. J. Clin. aesthetic Dermatol. 2017, 10, 14–17. [Google Scholar]
- Ravetti, S.; Clemente, C.; Brignone, S.; Hergert, L.; Allemandi, D.; Palma, S. Ascorbic Acid in Skin Health. Cosmetics 2019, 6, 58. [Google Scholar] [CrossRef]
- Ahn, K. Y., Song, H. J., & Kim, D. C. (2022). Effect of alpha-tocopheryl acetate, retinyl palmitate, and phytantriol on hair protection. Journal of Applied Biological Chemistry, 65(4), 307-312.
- Santos, J. S., Tavares, G. D., & Barradas, T. N. (2021). Vitamin E and derivatives in skin health promotion. In Vitamin E in Health and Disease-Interactions, Diseases and Health Aspects. IntechOpen.
- Putranti, A.R.; Hendradi, E.; Primaharinastiti, R. Effectivity and physicochemical stability of nanostructured lipid carrier coenzyme q10 in different ratio of lipid alfa cetyl palmitate and alpha tocopheryl acetate as carrier. Asian J. Pharm. Clin. Res. 2017, 10, 146. [Google Scholar] [CrossRef]
- Panichakul, T.; Rodboon, T.; Suwannalert, P.; Tripetch, C.; Rungruang, R.; Boohuad, N.; Youdee, P. Additive Effect of a Combination of Artocarpus lakoocha and Glycyrrhiza glabra Extracts on Tyrosinase Inhibition in Melanoma B16 Cells. Pharmaceuticals 2020, 13, 310. [Google Scholar] [CrossRef]
- Gupta, A.K.; Pathak, U.; Medhi, M.; Mastinu, A.; Sikarwar, M.S.; Mishra, P. Botanical, Chemical and Pharmacological Properties of Artocarpus lakoocha (Monkey Fruit): A Review. Agric. Rev. 2020. [Google Scholar] [CrossRef]
- Ullah, S.; Shoaib, R.; Khan, S.; Masood, A. Phytochemicals; Targeted-Based Therapeutic Approaches for Pigmentation Disorders. Open Access Indones. J. Med Rev. 2023, 3, 368–381. [Google Scholar] [CrossRef]
- Vaughn, A.R.; Clark, A.K.; Sivamani, R.K.; Shi, V.Y. Natural Oils for Skin-Barrier Repair: Ancient Compounds Now Backed by Modern Science. Am. J. Clin. Dermatol. 2018, 19, 103–117. [Google Scholar] [CrossRef] [PubMed]
- Sarkic, A.; Stappen, I. Essential Oils and Their Single Compounds in Cosmetics—A Critical Review. Cosmetics 2018, 5, 11. [Google Scholar] [CrossRef]
- Ali, S.A.; Galgut, J.M.; Choudhary, R.K. On The Novel Action of Melanolysis by a Leaf Extract of Aloe vera and Its Active Ingredient Aloin, Potent Skin Depigmenting Agents. Planta Medica 2012, 78, 767–771. [Google Scholar] [CrossRef] [PubMed]
- Gad, H.A.; Roberts, A.; Hamzi, S.H.; Gad, H.A.; Touiss, I.; Altyar, A.E.; Kensara, O.A.; Ashour, M.L. Jojoba Oil: An Updated Comprehensive Review on Chemistry, Pharmaceutical Uses, and Toxicity. Polymers 2021, 13, 1711. [Google Scholar] [CrossRef]
- Matsumoto, Y.; Ma, S.; Tominaga, T.; Yokoyama, K.; Kitatani, K.; Horikawa, K.; Suzuki, K. Acute Effects of Transdermal Administration of Jojoba Oil on Lipid Metabolism in Mice. Medicina 2019, 55, 594. [Google Scholar] [CrossRef]
- Blaak, J.; Staib, P. An updated review on efficacy and benefits of sweet almond, evening primrose and jojoba oils in skin care applications. Int. J. Cosmet. Sci. 2021, 44, 1–9. [Google Scholar] [CrossRef]
- Sturtevant, D.; Lu, S.; Zhou, Z.-W.; Shen, Y.; Wang, S.; Song, J.-M.; Zhong, J.; Burks, D.J.; Yang, Z.-Q.; Yang, Q.-Y.; et al. The genome of jojoba ( Simmondsia chinensis ): A taxonomically isolated species that directs wax ester accumulation in its seeds. Sci. Adv. 2020, 6, eaay3240. [Google Scholar] [CrossRef]
- Nasr, M., Abdel-Hamid, S., H Moftah, N., Fadel, M., & A Alyoussef, A. (2017). Jojoba oil soft colloidal nanocarrier of a synthetic retinoid: preparation, characterization and clinical efficacy in psoriatic patients. Current drug delivery, 14(3), 426-432.
- Sánchez, M.; Avhad, M.R.; Marchetti, J.M.; Martínez, M.; Aracil, J. Jojoba oil: A state of the art review and future prospects. Energy Convers. Manag. 2016, 129, 293–304. [Google Scholar] [CrossRef]
- Manoharan, S., Vishnupriya, V., & Gayathri, R. (2016). Phytochemical analysis and in vitro antioxidant activity of jojoba oil. Journal of Pharmaceutical Sciences and Research, 8(6), 512.
- Goik, U.; Goik, T.; Załęska, I. The Properties and Application of Argan Oil in Cosmetology. Eur. J. Lipid Sci. Technol. 2019, 121. [Google Scholar] [CrossRef]
- Phong, C.; Lee, V.; Yale, K.; Sung, C.; Mesinkovska, N. Coconut, Castor, and Argan Oil for Hair in Skin of Color Patients: A Systematic Review. J. Drugs Dermatol. JDD 2022, 21, 751–757. [Google Scholar] [CrossRef] [PubMed]
- Charrouf, Z.; Guillaume, D. The argan oil project: going from utopia to reality in 20 years. OCL 2018, 25, D209. [Google Scholar] [CrossRef]
- Leite, C.d.S.; Bonafé, G.A.; Santos, J.C.; Martinez, C.A.R.; Ortega, M.M.; Ribeiro, M.L. The Anti-Inflammatory Properties of Licorice (Glycyrrhiza glabra)-Derived Compounds in Intestinal Disorders. Int. J. Mol. Sci. 2022, 23, 4121. [Google Scholar] [CrossRef]
- Kwon, Y.-J.; Son, D.-H.; Chung, T.-H.; Lee, Y.-J. A Review of the Pharmacological Efficacy and Safety of Licorice Root from Corroborative Clinical Trial Findings. J. Med. Food 2020, 23, 12–20. [Google Scholar] [CrossRef]
- Mohiuddin, A. K. (2019). Skin lightening & management of hyperpigmentation. Pharma Sci Anal Res J, 2(2), 180020.
- Kimyon, R.S.; Liou, Y.L.; Schlarbaum, J.P.; Warshaw, E.M. Allergic Contact Dermatitis to Licorice Root Extract. Dermatitis® 2019, 30, 227–228. [Google Scholar] [CrossRef]
- Spencer, J.M.; Accioly, J.; Kitchen, N. Double Blind, Placebo Controlled Evaluation of a Novel Skin Lightening Agent. J. Drugs Dermatol. JDD 2018, 17, 113–115. [Google Scholar]
- Dhariwala, M.Y.; Ravikumar, P. An overview of herbal alternatives in androgenetic alopecia. J. Cosmet. Dermatol. 2019, 18, 966–975. [Google Scholar] [CrossRef]
- Kim, L., & Lio, P. (2020). Turmeric, curcumin, and curcuminoids: a dermatologic review. Clinical Focus, 38-42.
- Vo, T. S., Vo, T. T. B. C., Vo, T. T. T. N., & Lai, T. N. H. (2021). Turmeric (Curcuma longa L.): Chemical components and their effective clinical applications. Journal of the Turkish Chemical Society Section A: Chemistry, 8(3), 883-898.
- Firmansyah, D.; Sumiwi, S.A.; Saptarini, N.M.; Levita, J. Curcuma longa extract inhibits the activity of mushroom tyrosinase and the growth of murine skin cancer B16F10 cells. J. Herbmed Pharmacol. 2022, 12, 153–158. [Google Scholar] [CrossRef]
- Farooqui, R.K.; Kaurav, M.; Kumar, M.; Sudheesh, M.S.; Pandey, R.S. Permeation enhancer nanovesicles mediated topical delivery of curcumin for the treatment of hyperpigmentation. J. Liposome Res. 2022, 32, 332–339. [Google Scholar] [CrossRef] [PubMed]
- Akter, J., Islam, M. Z., Hossain, M. A., & Takara, K. (2021). Anti-tyrosinase properties of different species of turmeric and isolation of active compounds from Curcuma amada. Medicinal Chemistry Research, 30, 1669-1676.
- Rodríguez-Cid, L.; Qian, W.; Iribarra-Araya, J.; Etcheverry-Berríos. ; Martínez-Olmos, E.; Choquesillo-Lazarte, D.; Sañudo, E.C.; Roubeau, O.; López-Periago, A.M.; González-Campo, A.; et al. Broadening the scope of high structural dimensionality nanomaterials using pyridine-based curcuminoids. Dalton Trans. 2021, 50, 7056–7064. [Google Scholar] [CrossRef] [PubMed]
- Vaughn, A.R.; Clark, A.K.; Notay, M.; Sivamani, R.K. Randomized Controlled Pilot Study of Dietary Supplementation with Turmeric or Herbal Combination Tablets on Skin Barrier Function in Healthy Subjects. J. Med. Food 2018, 21, 1260–1265. [Google Scholar] [CrossRef] [PubMed]
- Kallis, P.J.; Price, A.; Dosal, J.R.; Nichols, A.J.; Keri, J. A Biologically Based Approach to Acne and Rosacea. J. Drugs Dermatol. JDD 2018, 17, 611–617. [Google Scholar]
- Song, X.-C.; Canellas, E.; Wrona, M.; Becerril, R.; Nerin, C. Comparison of two antioxidant packaging based on rosemary oleoresin and green tea extract coated on polyethylene terephthalate for extending the shelf life of minced pork meat. Food Packag. Shelf Life 2020, 26, 100588. [Google Scholar] [CrossRef]
- Bagheri, R., Rashidlamir, A., Ashtary-Larky, D., Wong, A., Alipour, M., Motevalli, M. S., ... & Zouhal, H. (2020). Does green tea extract enhance the anti-inflammatory effects of exercise on fat loss?. British journal of clinical pharmacology, 86(4), 753-762. [CrossRef]
- Gaweł-Bęben, K.; Kukula-Koch, W.; Hoian, U.; Czop, M.; Strzępek-Gomółka, M.; Antosiewicz, B. Characterization of Cistus × incanus L. and Cistus ladanifer L. Extracts as Potential Multifunctional Antioxidant Ingredients for Skin Protecting Cosmetics. Antioxidants 2020, 9, 202. [Google Scholar] [CrossRef] [PubMed]
- Tang, G.; Xu, Y.; Zhang, C.; Wang, N.; Li, H.; Feng, Y. Green Tea and Epigallocatechin Gallate (EGCG) for the Management of Nonalcoholic Fatty Liver Diseases (NAFLD): Insights into the Role of Oxidative Stress and Antioxidant Mechanism. Antioxidants 2021, 10, 1076. [Google Scholar] [CrossRef] [PubMed]
- Hodges, J.K.; Sasaki, G.Y.; Bruno, R.S. Anti-inflammatory activities of green tea catechins along the gut–liver axis in nonalcoholic fatty liver disease: lessons learned from preclinical and human studies. J. Nutr. Biochem. 2020, 85, 108478. [Google Scholar] [CrossRef] [PubMed]
- Chaikul, P.; Sripisut, T.; Chanpirom, S.; Ditthawutthikul, N. Anti-skin aging activities of green tea (Camelliasinensis (L) Kuntze) in B16F10 melanoma cells and human skin fibroblasts. Eur. J. Integr. Med. 2020, 40, 101212. [Google Scholar] [CrossRef]
- Bhattacharya, S.; Sherje, A.P. Development of resveratrol and green tea sunscreen formulation for combined photoprotective and antioxidant properties. J. Drug Deliv. Sci. Technol. 2020, 60, 102000. [Google Scholar] [CrossRef]
- Winkelman, W.J. Aromatherapy, botanicals, and essential oils in acne. Clin. Dermatol. 2018, 36, 299–305. [Google Scholar] [CrossRef] [PubMed]
- Patidar, K. (2018). Unmet Need and Challenges of Skin Aging by Herbal Anti-aging Cosmeceuticals: An Overview. Asian Journal of Pharmaceutics (AJP), 12(02).
- Phasha, V.; Senabe, J.; Ndzotoyi, P.; Okole, B.; Fouche, G.; Chuturgoon, A. Review on the Use of Kojic Acid—A Skin-Lightening Ingredient. Cosmetics 2022, 9, 64. [Google Scholar] [CrossRef]
- Saeedi, M.; Eslamifar, M.; Khezri, K. Kojic acid applications in cosmetic and pharmaceutical preparations. Biomed. Pharmacother. 2018, 110, 582–593. [Google Scholar] [CrossRef]
- Khezri, K.; Saeedi, M.; Morteza-Semnani, K.; Akbari, J.; Hedayatizadeh-Omran, A. A promising and effective platform for delivering hydrophilic depigmenting agents in the treatment of cutaneous hyperpigmentation: kojic acid nanostructured lipid carrier. Artif. Cells, Nanomedicine, Biotechnol. 2021, 49, 38–47. [Google Scholar] [CrossRef]
- Khan, A.; Park, T.J.; Ikram, M.; Ahmad, S.; Ahmad, R.; Jo, M.G.; Kim, M.O. Antioxidative and Anti-inflammatory Effects of Kojic Acid in Aβ-Induced Mouse Model of Alzheimer’s Disease. Mol. Neurobiol. 2021, 58, 5127–5140. [Google Scholar] [CrossRef] [PubMed]
- Zilles, J. C., Dos Santos, F. L., Kulkamp-Guerreiro, I. C., & Contri, R. V. (2022). Biological activities and safety data of kojic acid and its derivatives: A review. Experimental dermatology, 31(10), 1500-1521.
- Bakhouche, I.; Aliat, T.; Boubellouta, T.; Gali, L.; Şen, A.; Bellik, Y. Phenolic contents and in vitro antioxidant, anti-tyrosinase, and anti-inflammatory effects of leaves and roots extracts of the halophyte Limonium delicatulum. South Afr. J. Bot. 2021, 139, 42–49. [Google Scholar] [CrossRef]
- Li, T.-X.; Liang, J.-X.; Liu, L.-L.; Shi, F.-C.; Jia, X.-W.; Li, M.-H.; Xu, C.-P. Novel kojic acid derivatives with anti-inflammatory effects from Aspergillus versicolor. Fitoterapia 2021, 154, 105027. [Google Scholar] [CrossRef] [PubMed]
- Gust, P. J., & Luke, J. D. (2016). Kojic acid. Journal of the Dermatology Nurses' Association, 8(5), 338-340.
- Searle, T.; Al-Niaimi, F.; Ali, F.R. The top 10 cosmeceuticals for facial hyperpigmentation. Dermatol. Ther. 2020, 33, e14095. [Google Scholar] [CrossRef] [PubMed]
- Ohno, Y.; Kondo, S.; Tajima, K.; Shibata, T.; Itoh, T. Effect of Phlorotannins Isolated From Eisenia bicyclis on Melanogenesis in Mouse B16 Melanoma Cells. Nat. Prod. Commun. 2021, 16. [Google Scholar] [CrossRef]
- Phang, S.J.; Teh, H.X.; Looi, M.L.; Arumugam, B.; Fauzi, M.B.; Kuppusamy, U.R. Phlorotannins from brown algae: a review on their antioxidant mechanisms and applications in oxidative stress-mediated diseases. J. Appl. Phycol. 2023, 35, 867–892. [Google Scholar] [CrossRef]
- Jesumani, V.; Du, H.; Aslam, M.; Pei, P.; Huang, N. Potential Use of Seaweed Bioactive Compounds in Skincare—A Review. Mar. Drugs 2019, 17, 688. [Google Scholar] [CrossRef]
- Zhao, W.; Yang, A.; Wang, J.; Huang, D.; Deng, Y.; Zhang, X.; Qu, Q.; Ma, W.; Xiong, R.; Zhu, M.; et al. Potential application of natural bioactive compounds as skin-whitening agents: A review. J. Cosmet. Dermatol. 2022, 21, 6669–6687. [Google Scholar] [CrossRef]
- Kim, K.-N.; Yang, H.-M.; Kang, S.-M.; Ahn, G.; Roh, S.W.; Lee, W.; Kim, D.; Jeon, Y.-J. Whitening Effect of Octaphlorethol A Isolated from Ishige foliacea in an In Vivo Zebrafish Model. J. Microbiol. Biotechnol. 2015, 25, 448–451. [Google Scholar] [CrossRef] [PubMed]
- Lee, S.-H.; Kang, N.; Kim, E.-A.; Heo, S.-J.; Moon, S.-H.; Jeon, B.-T.; Jeon, Y.-J. Antidiabetogenic and antioxidative effects of octaphlorethol a isolated from the brown algae Ishige foliacea in streptozotocin-induced diabetic mice. Food Sci. Biotechnol. 2014, 23, 1261–1266. [Google Scholar] [CrossRef]
- Thawabteh, A.M.; Swaileh, Z.; Ammar, M.; Jaghama, W.; Yousef, M.; Karaman, R.; Bufo, S.A.; Scrano, L. Antifungal and Antibacterial Activities of Isolated Marine Compounds. Toxins 2023, 15, 93. [Google Scholar] [CrossRef] [PubMed]
- Fernando, I.P.S.; Sanjeewa, K.K.A.; Samarakoon, K.W.; Kim, H.-S.; Gunasekara, U.K.D.S.S.; Park, Y.-J.; Abeytunga, D.T.U.; Lee, W.W.; Jeon, Y.-J. The potential of fucoidans from Chnoospora minima and Sargassum polycystum in cosmetics: antioxidant, anti-inflammatory, skin-whitening, and antiwrinkle activities. J. Appl. Phycol. 2018, 30, 3223–3232. [Google Scholar] [CrossRef]
- Kok, J.M.-L.; Jee, J.-M.; Chew, L.-Y.; Wong, C.-L. The potential of the brown seaweed Sargassum polycystum against acne vulgaris. J. Appl. Phycol. 2016, 28, 3127–3133. [Google Scholar] [CrossRef]
- Lourenço-Lopes, C., Fraga-Corral, M., Soria-Lopez, A., Nuñes-Estevez, B., Barral-Martinez, M., Silva, A., ... & Prieto, M. A. (2022). Fucoxanthin’s optimization from Undaria pinnatifida using conventional heat extraction, bioactivity assays and in silico studies. Antioxidants, 11(7), 1296. [CrossRef]
- Park, E.-J.; Choi, J.-I. Melanogenesis inhibitory effect of low molecular weight fucoidan from Undaria pinnatifida. J. Appl. Phycol. 2017, 29, 2213–2217. [Google Scholar] [CrossRef]
- Lee, S.-H.; Kang, S.-M.; Ko, S.-C.; Lee, D.-H.; Jeon, Y.-J. Octaphlorethol A, a novel phenolic compound isolated from a brown alga, Ishige foliacea, increases glucose transporter 4-mediated glucose uptake in skeletal muscle cells. Biochem. Biophys. Res. Commun. 2012, 420, 576–581. [Google Scholar] [CrossRef]
- Kim, K.-N.; Yang, H.-M.; Kang, S.-M.; Ahn, G.; Roh, S.W.; Lee, W.; Kim, D.; Jeon, Y.-J. Whitening Effect of Octaphlorethol A Isolated from Ishige foliacea in an In Vivo Zebrafish Model. J. Microbiol. Biotechnol. 2015, 25, 448–451. [Google Scholar] [CrossRef]
- Lajis, A.F.B.; Ariff, A.B. Discovery of new depigmenting compounds and their efficacy to treat hyperpigmentation: Evidence from in vitro study. J. Cosmet. Dermatol. 2019, 18, 703–727. [Google Scholar] [CrossRef]
- Haggag, Y.A.; Elrahman, A.A.A.; Ulber, R.; Zayed, A. Fucoidan in Pharmaceutical Formulations: A Comprehensive Review for Smart Drug Delivery Systems. Mar. Drugs 2023, 21, 112. [Google Scholar] [CrossRef] [PubMed]
- Guan, B.; Chen, K.; Tong, Z.; Chen, L.; Chen, Q.; Su, J. Advances in Fucoxanthin Research for the Prevention and Treatment of Inflammation-Related Diseases. Nutrients 2022, 14, 4768. [Google Scholar] [CrossRef] [PubMed]
- Natsume, C.; Aoki, N.; Aoyama, T.; Senda, K.; Matsui, M.; Ikegami, A.; Tanaka, K.; Azuma, Y.-T.; Fujita, T. Fucoxanthin Ameliorates Atopic Dermatitis Symptoms by Regulating Keratinocytes and Regulatory Innate Lymphoid Cells. Int. J. Mol. Sci. 2020, 21, 2180. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Jimenez, A.; Teruel-Puche, J.A.; Berna, J.; Rodriguez-Lopez, J.N.; Tudela, J.; Garcia-Ruiz, P.A.; Garcia-Canovas, F. Characterization of the action of tyrosinase on resorcinols. Bioorganic Med. Chem. 2016, 24, 4434–4443. [Google Scholar] [CrossRef] [PubMed]
- Jin, Y.-J.; Lin, C.-C.; Lu, T.-M.; Li, J.-H.; Chen, I.-S.; Kuo, Y.-H.; Ko, H.-H. Chemical constituents derived from Artocarpus xanthocarpus as inhibitors of melanin biosynthesis. Phytochemistry 2015, 117, 424–435. [Google Scholar] [CrossRef] [PubMed]
- Yamahara, M.; Sugimura, K.; Kumagai, A.; Fuchino, H.; Kuroi, A.; Kagawa, M.; Itoh, Y.; Kawahara, H.; Nagaoka, Y.; Iida, O.; et al. Callicarpa longissima extract, carnosol-rich, potently inhibits melanogenesis in B16F10 melanoma cells. J. Nat. Med. 2015, 70, 28–35. [Google Scholar] [CrossRef] [PubMed]
- Mustapha, N.; Bzéouich, I.M.; Ghedira, K.; Hennebelle, T.; Chekir-Ghedira, L. Compounds isolated from the aerial part of Crataegus azarolus inhibit growth of B16F10 melanoma cells and exert a potent inhibition of the melanin synthesis. Biomed. Pharmacother. 2015, 69, 139–144. [Google Scholar] [CrossRef] [PubMed]
- Nam, J.H.; Nam, D.-Y.; Lee, D.-U. Valencene from the Rhizomes of Cyperus rotundus Inhibits Skin Photoaging-Related Ion Channels and UV-Induced Melanogenesis in B16F10 Melanoma Cells. J. Nat. Prod. 2016, 79, 1091–1096. [Google Scholar] [CrossRef]
- Jin, K. S., Lee, J. Y., Hyun, S. K., Kim, B. W., & Kwon, H. J. (2015). Juniperus chinensis and the functional compounds, cedrol and widdrol, ameliorate α-melanocyte stimulating hormone-induced melanin formation in B16F10 cells. Food Science and Biotechnology, 24, 611-618.
- de Freitas, M.M.; Fontes, P.R.; Souza, P.M.; William Fagg, C.; Neves Silva Guerra, E.; de Medeiros Nóbrega, Y.K.; Silveira, D.; Fonseca-Bazzo, Y.; Simeoni, L.A.; Homem-de-Mello, M.; et al. Extracts of Morus nigra L. Leaves Standardized in Chlorogenic Acid, Rutin and Isoquercitrin: Tyrosinase Inhibition and Cytotoxicity. PLoS ONE 2016, 11, e0163130. [Google Scholar] [CrossRef]
- Kanlayavattanakul, M.; Lourith, N.; Chaikul, P. Jasmine rice panicle: A safe and efficient natural ingredient for skin aging treatments. J. Ethnopharmacol. 2016, 193, 607–616. [Google Scholar] [CrossRef] [PubMed]
- Lourith, N.; Kanlayavattanakul, M.; Chingunpitak, J. Development of sunscreen products containing passion fruit seed extract. Braz. J. Pharm. Sci. 2017, 53. [Google Scholar] [CrossRef]
- Sallam, A.; Mira, A.; Ashour, A.; Shimizu, K. Acetylcholine esterase inhibitors and melanin synthesis inhibitors from Salvia officinalis. Phytomedicine 2016, 23, 1005–1011. [Google Scholar] [CrossRef] [PubMed]
- Srisayam, M.; Weerapreeyakul, N.; Barusrux, S.; Kanokmedhakul, K. Antioxidant, antimelanogenic, and skin-protective effect of sesamol. 2014, 65, 69–79. [Google Scholar]
- Diwakar, G.; Rana, J.; Saito, L.; Vredeveld, D.; Zemaitis, D.; Scholten, J. Inhibitory effect of a novel combination of Salvia hispanica (chia) seed and Punica granatum (pomegranate) fruit extracts on melanin production. Fitoterapia 2014, 97, 164–171. [Google Scholar] [CrossRef]
- Lourith, N.; Kanlayavattanakul, M.; Chaikul, P.; Chansriniyom, C.; Bunwatcharaphansakun, P. In vitro and cellular activities of the selected fruits residues for skin aging treatment. An. Da Acad. Bras. De Ciências 2017, 89, 577–589. [Google Scholar] [CrossRef]
Figure 1.
Schematic representation for melanin synthesis pathway.
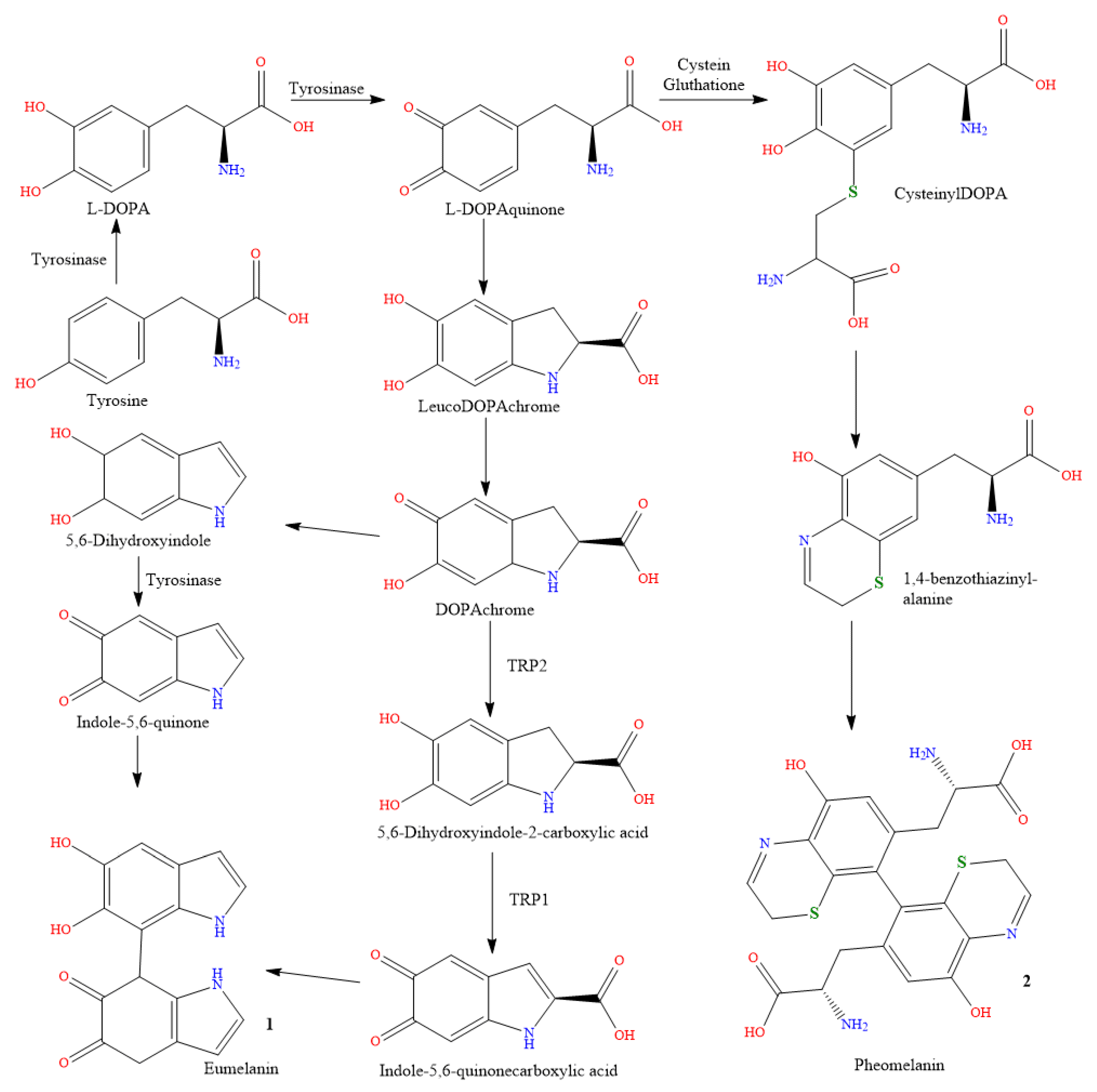
Figure 2.
(1) Ultraviolet radiation produces free radicals. (2) Free radicals and UV light both operate as biological triggers for the melanocytes, the pigment-producing cells. (3) The tyrosinase enzyme, which creates colors, is influenced by biological circumstances to manufacture more of them. (4) Tyrosine, an amino acid, is transformed into melanin pigments, which can be either red or brown in color, by the enzyme tyrosinase. (5) Melanin is transferred from melanocytes into the surrounding keratinocytes as granules to give the skin its color.
Figure 2.
(1) Ultraviolet radiation produces free radicals. (2) Free radicals and UV light both operate as biological triggers for the melanocytes, the pigment-producing cells. (3) The tyrosinase enzyme, which creates colors, is influenced by biological circumstances to manufacture more of them. (4) Tyrosine, an amino acid, is transformed into melanin pigments, which can be either red or brown in color, by the enzyme tyrosinase. (5) Melanin is transferred from melanocytes into the surrounding keratinocytes as granules to give the skin its color.
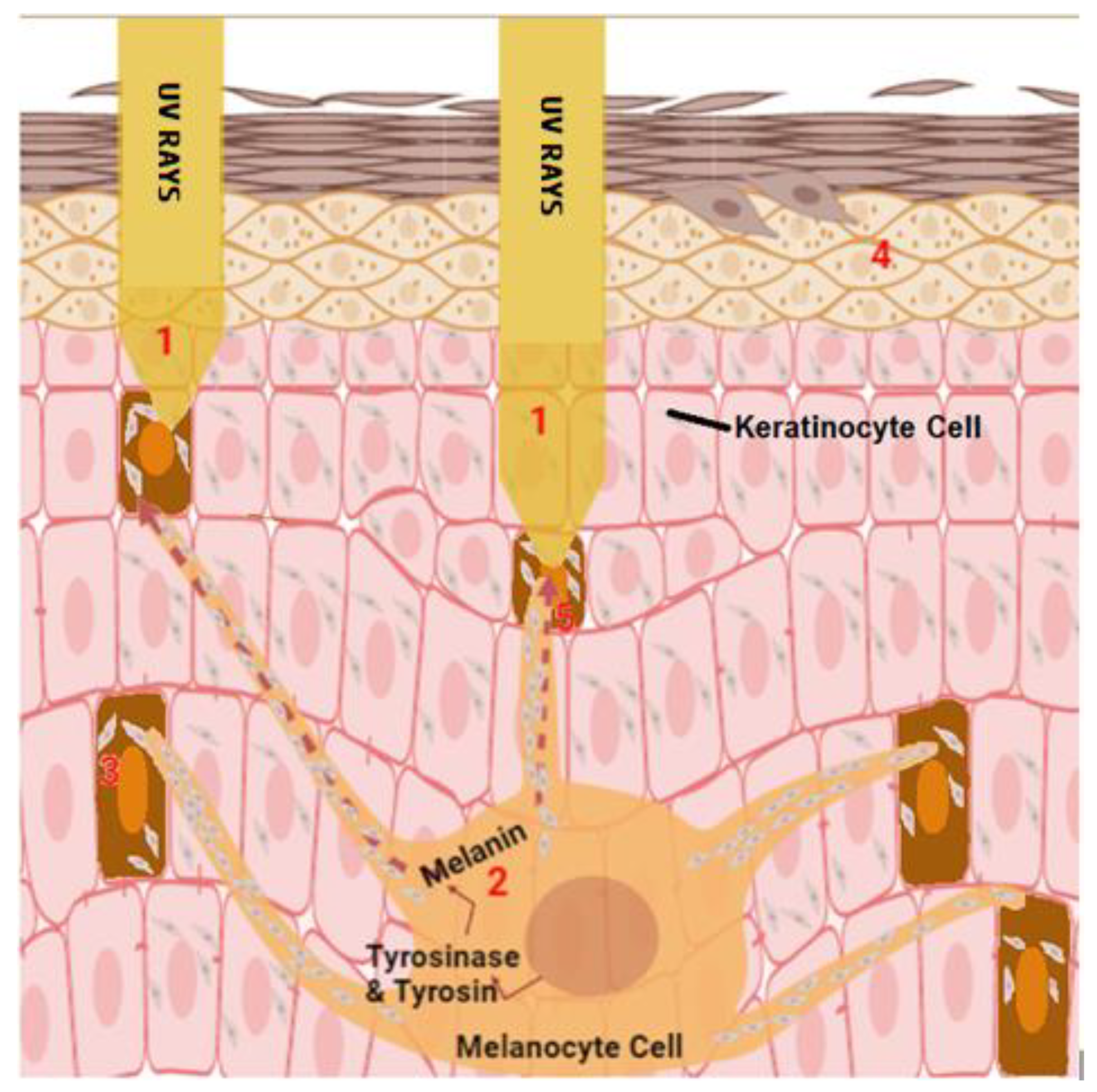
Figure 3.
hypopigmentation (A) [22], (B) [23] and hyperpigmentation (C,D) [24] cases. Figure 3A: Reproduced with permission from Joo-Heung Lee, Cho-Rok Kim, Dong-Youn Lee, Photodermatology, Photoimmunology & Photomedicine; published by John Wiley and Sons, 2011. Figure 3B: Reproduced with permission from Jeremy P Hill, Jonathan M Batchelor, The BMJ; published by BMJ Publishing Group Ltd, 2017. Figure 3C,D: Reproduced with permission from Narumol Silpa-archa, Indermeet Kohli, Suteeraporn Chaowattanapanit, Henry W. Lim, Iltefat Hamzavi, Journal of the American Academy of Dermatology; published by Elsevier, 2017.
Figure 3.
hypopigmentation (A) [22], (B) [23] and hyperpigmentation (C,D) [24] cases. Figure 3A: Reproduced with permission from Joo-Heung Lee, Cho-Rok Kim, Dong-Youn Lee, Photodermatology, Photoimmunology & Photomedicine; published by John Wiley and Sons, 2011. Figure 3B: Reproduced with permission from Jeremy P Hill, Jonathan M Batchelor, The BMJ; published by BMJ Publishing Group Ltd, 2017. Figure 3C,D: Reproduced with permission from Narumol Silpa-archa, Indermeet Kohli, Suteeraporn Chaowattanapanit, Henry W. Lim, Iltefat Hamzavi, Journal of the American Academy of Dermatology; published by Elsevier, 2017.

Figure 4.
The mechanisms involved in some types of hypopigmentation.
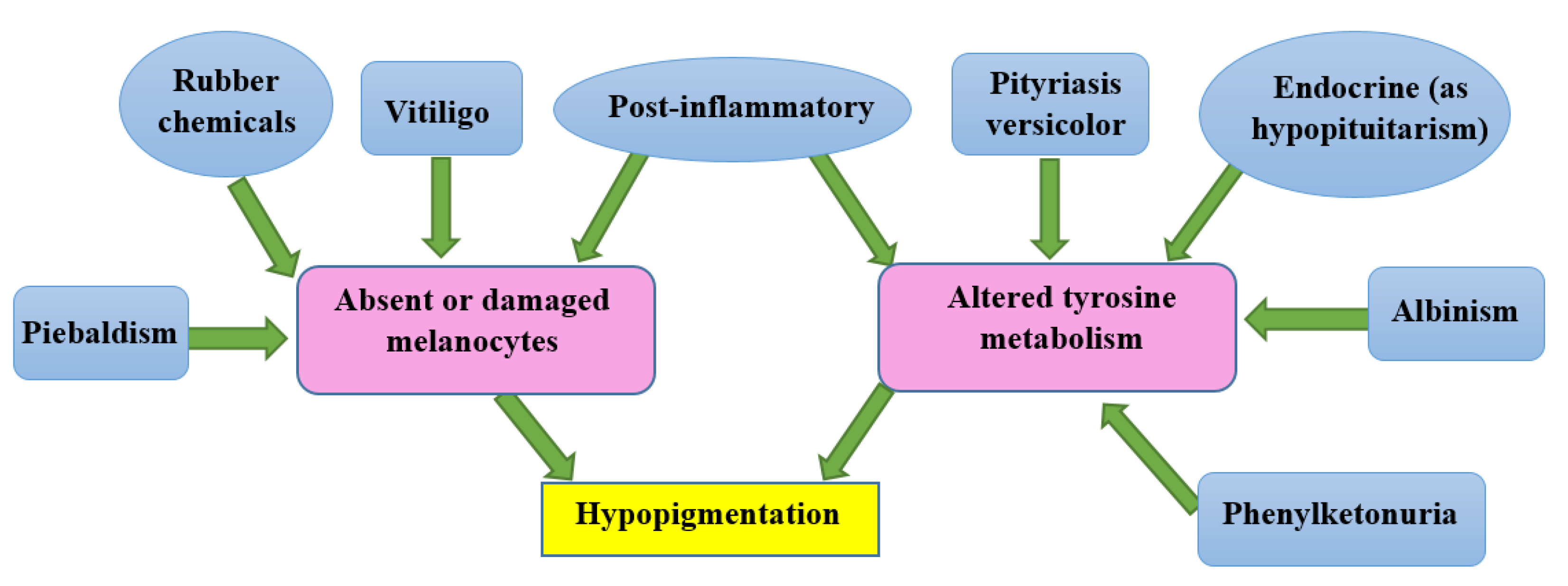
Figure 5.
Depigmentation cases [27,28]. Figure 5A: Reproduced with permission from Louise McMichael, the BMJ; published by BMJ Publishing Group Ltd, 2012. Figure 5B: Reproduced with permission from Jing Jing, Xiao-Yong Man, the BMJ; published by BMJ Publishing Group Ltd, 2021.
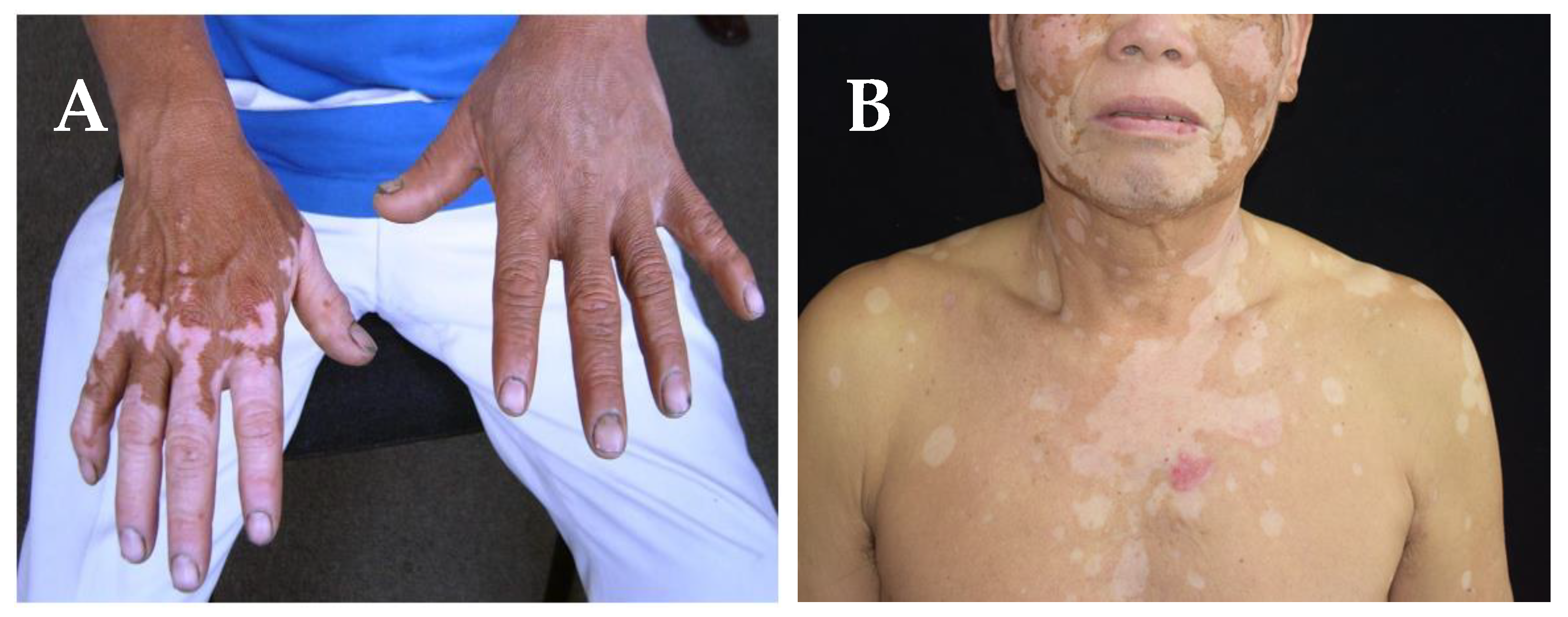
Figure 6.
Chemical structures of tranexamic acid (3), and isotretinoin (4).
Figure 7.
Chemical structures of betamethasone (5), clobetasol (6), silver sulfadiazine (7), dimethicone (8), triamcinolone (9), and hydroquinone (10).
Figure 7.
Chemical structures of betamethasone (5), clobetasol (6), silver sulfadiazine (7), dimethicone (8), triamcinolone (9), and hydroquinone (10).

Figure 8.
Chemical structures of fluocinolone (11), tretinoin (12), clotrimazole (13), gentamicin (14), ruxolitinib (15) and salicylic acid (16).
Figure 8.
Chemical structures of fluocinolone (11), tretinoin (12), clotrimazole (13), gentamicin (14), ruxolitinib (15) and salicylic acid (16).
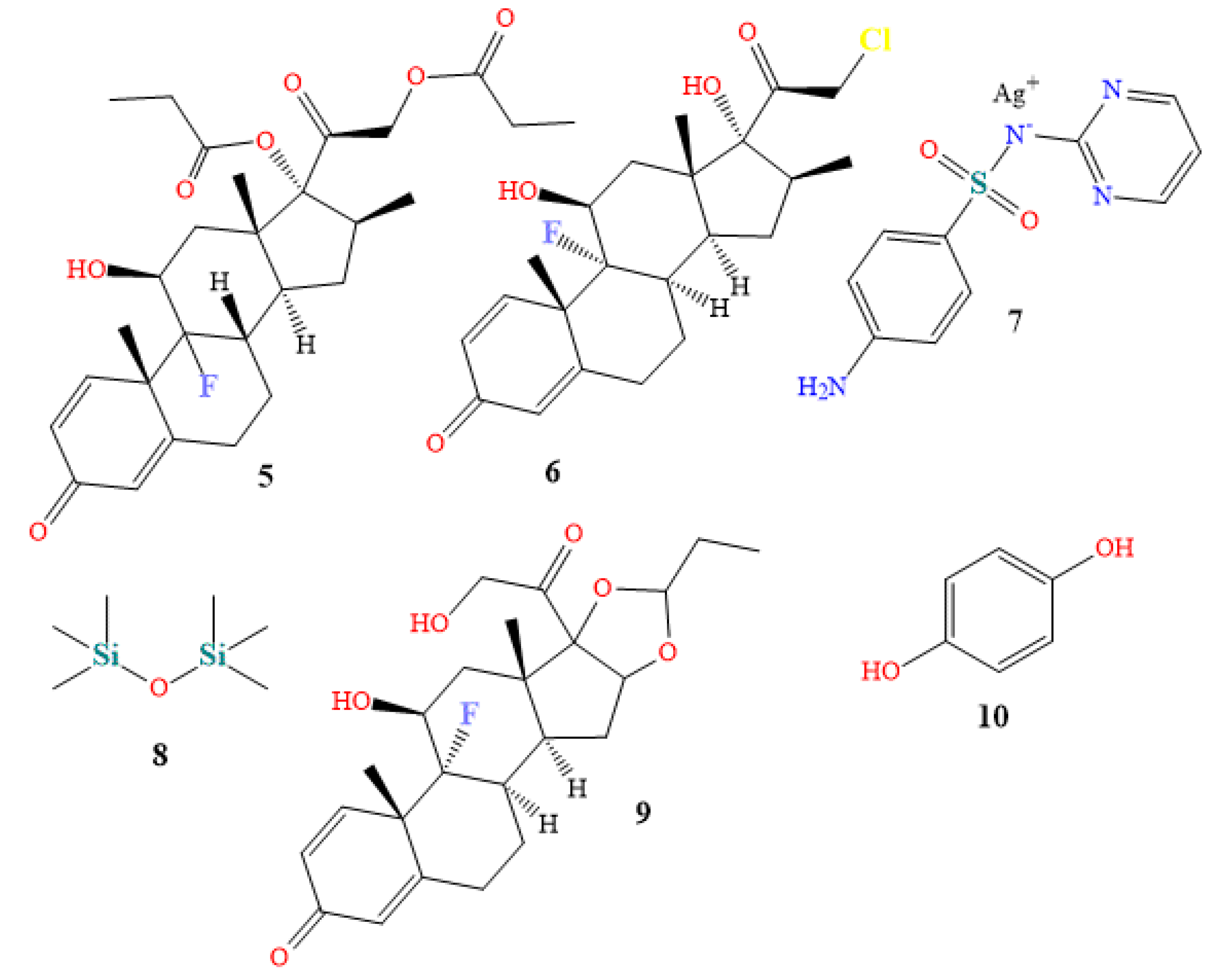
Figure 9.
Structures of podophyllum resin (17), podofilox (18), aloin (19), kojic acid (20) phlorotannins (21), octaphlorethol A (22), fucoidan (23), and fucoxanthin (24).
Figure 9.
Structures of podophyllum resin (17), podofilox (18), aloin (19), kojic acid (20) phlorotannins (21), octaphlorethol A (22), fucoidan (23), and fucoxanthin (24).
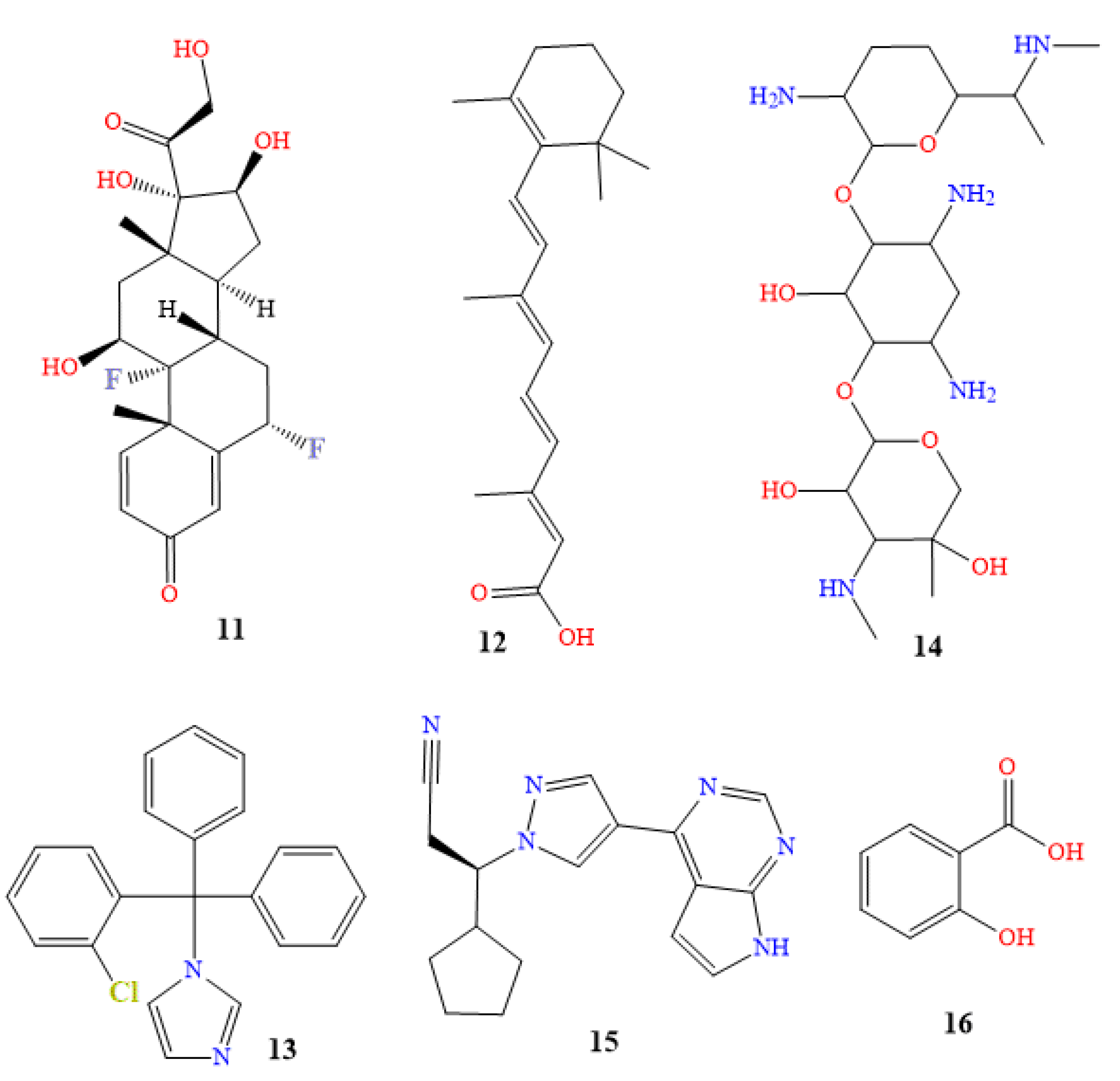

Table 1.
Topical brands drug for the treatment of skin pigmentation.
| Class | Generic name | Brand names ® | Dosage form |
|---|---|---|---|
| Topical steroids | Betamethasone | Etnovate, Diprolene, Luxiq, Beta-Val, Diprolene AF | Cream, gel, ointment, lotion |
| Clobetasol | Dermovate, Clobex, Olux, Olux-E, Temovate, Clobevate, Clodan, Cormax, Cormax Scalp, Embeline, Embeline E, Impeklo, Tovet | Solution, spray, ointment, gel, foam, lotion, cream, shampoo | |
| Triamcinolone acetonide | DermasilkRx SDS Pak, Dermasorb TA , DermaWerx SDS Pak, Kenalog , Oralone , Trianex , Triderm | Cream, ointment | |
| Topical anti-infectives | Silver topical | SilvaSorb, Aceso Ag, Solox | Cream, gel, foam |
| Topical steroids with anti-infectives | Dimethicone and triamcinolone topical | Yaliira Pak, Ellzia Pak, TriaDime-80, TriHeal-80 | Creams, shampoos, powders, gels |
| Topical depigmenting agents | Fluocinolone, hydroquinone and tretinoin topical | Tri-Luma, Triderma | Cream |
| Hydroquinone topical | Melquin HP, Alera, EpiQuin Micro, Esoterica, Hydro-Q, Melamin, Melpaque HP, Nuquin HP, AMBI Fade, Blanche, Esoterica Nighttime, Glytone, Lustra-Ultra, Melamin-C, NeoStrata HQ Skin Lightening, Olivia Quido, Fade cream, Remergent HQ | Cream | |
| Topical keratolytics | Salicylic acid topical | Bensal HP, KeralytGel, Salex, Acnex, Aliclen, DHS Salicylic Acid 3%, Durasal, Keralyt Shampoo, Stri-Dex, Akurza, DermalZone, Dr Scholl's, Fostex, Freezeone, Rayasal, Salvax, Stridex, | Liquid, soap, cream, lotion, foam |
| Podophyllum resin topical | Podocon-25, Podofin, Pododerm | Topical solution | |
| Podofilox topical | Condylox | Topical gel, topical solution |
Table 2.
Plants discovered to treat hyperpigmentation in the past ten years.
| Name of plant | Family | Growth place | Active compounds |
|---|---|---|---|
| Angelica sinensis [194] | Apiaceae | East Asia | 4-ethylresorcinol, 4-ethylphenol, 1-tetradecalnol |
| Artocarpus [195] | Moraceae | Southeast Asia | Artocarpin, cudraflavone C, artocarpanone |
| Callicarpa longissima [196] | Lamiaceae | Southeast Asia | Carnosol |
| Crataegus azarolus [197] | Rosaceae | European | Ursolic acid, hyperoside, virtexin-2″-O-rhamnoside |
| Cyperus rotundus [198] | Cyperaceae | Africa, France, Austria, southern Asia | Valencene, camphene, carryophyllene oxide |
| Juniperus chinensis [199] | Cupressaceae | China, Myanmar, Russian, Korea | Widdrol |
| Morus nigra [200] | Moraceae | Iberian Peninsula | Isoquercitrin, rutin, chlorogenic acid |
| Oryza sativa [201] | Poaceae | China | p-coumaric, ferulic |
| Passiflora edulis [202] | Passifloraceae | Brazil, Paraguay, Argentina | Piceatannol, resveratrol, quercetin |
| Salvia officinalis [203] | Lamiaceae | Mediterranean region | 7a-methoxyrosmanol, isorosmanol |
| Sesamum indicum [204] | Pedaliaceae | Africa, India | Sesamol |
| Punica granatum [205] | Lythraceae | Mediterranean | Punicalgin |
| Litchi chinensis [206] | Sapindaceae | China, India, Bangladesh, Vietnam, Thailand, Malaysia, Indonesia, Pakistan, Cambodia, Bangladesh, Himalayas | Rosmarinc acid, gallic acid |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



