Submitted:
10 May 2023
Posted:
11 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Identifying the psychological impacts of the COVID-19 pandemic on the general population can help with planning and preparing for future pandemics. The main objective of the current study was to examine the psychological impacts of the COVID-19 pandemic among Iranian citizens in 2021. The current study used an online cross-sectional survey via web-based questionnaires among Iranian citizens. Perceived feelings during the COVID-19 pandemic were measured by the validated self-reported inventory by Reynolds et al, 2007. The collected data were analyzed using descriptive statistics, including percent, mean, and standard deviation, as well as inferential statistics, including, correlation, chi-square, independent t-test, and analysis of variances (ANOVA) by SPSS.22. The average age of the respondents was 34.62 (±11.86). The most frequent feelings experienced by Iranian citizens were boredom (44.0%), nostalgia (40.6%), anxiety (35.3%), and nervousness (34.1%). Female participants, younger respondents, unemployed, single individuals, and those living in the urban areas experienced significantly higher levels of the negative feelings. The results of the study showed the high prevalence of the psychological effects of the COVID-19 pandemic in Iranian citizens, particularly among women, single, and unemployed people. Therefore, we need to develop more supportive and consultative packages for future pandemics as well as implement psychological rehabilitation after the crises.
Keywords:
COVID-19 Pandemic
; Emotions
; Iran
; National Survey
; Online Study
; Psychological Impact
Introduction
After years of controlling viral and infectious diseases, 27 cases of a pneumonia-like disease with unknown etiology were identified in late 2019 (December 31) in Wuhan, China. Afterward, the number of patients increased, and on January 9, 2020, a novel coronavirus (2019-nCoV) was introduced as the causing agent for this type of pneumonia. The infection rate of the disease was high, creating many concerns, especially for the vulnerable population since the first case of death due to this disease was a 61-year-old Chinese elderly person (1). On March 23, 2020, the COVID-19 virus spread globally, infecting many all around the world. As a result, countries introduced several scenarios for combating this virus. The symptoms of COVID-19 were variable, ranging from mild symptoms to acute sickness. The common symptoms include headaches, losing the sense of smell and the sense of taste, nasal congestion and a runny nose, coughing, muscular pain, sore throat, fever, diarrhea, and breathing difficulties (2). At the moment, i.e., March 5, 2023, three years after the first incidence, 680,610,521 people around the world have contracted the virus, and 6,805,012 people died as a result. Multiple waves of this pandemic have been experienced in different countries, and new cases are still being diagnosed in some countries (3).
With the spread of the COVID-19 virus, WHO emphasized the importance of quarantining and keeping social distance, resulting in a significant reduction in public, sports, and social activities. These changes impacted all age groups, including children, young adults, and the elderly (4). As a consequence, the spread of the COVID-19 virus, as a global problem, and its consequences, including the necessity to follow quarantining rules for the general public, created a new phenomenon in the everyday life of all individuals in the community. Moreover, the behaviors of individuals during this pandemic, in terms of physical and mental health, have directly or indirectly impacted access to food, social activities, occupational activities, and financial security (5).
Many behavioral changes, such as avoiding presence in public and participating in antiviral treatments, have had some positive impacts in different countries. However, it should be noted that while these changes have impacted physical health, they were not able to mitigate the mental consequences of COVID-19 and the quarantine. Similarly, the continuation of the pandemic and the related strategies, such as long-term quarantining in some countries, have resulted in harmful mental outcomes, including PTSD, confusion and anger, despair, fatigue, financial losses, and stigma for people. Accordingly, it should be noted that such diseases and the strategies used to combat them have harmful mental consequences that can lead to more significant psychological problems if neglected (6).
Previous studies done on the mental and social consequences of COVID-19 shows that a wide range of mental and social problems have been reported in different countries. The mental consequences of COVID-19, including stress and anxiety, PTSD, boredom, obsession, symptoms of prolonged grief, and sleeping problems (7–11), and its social consequences, including loneliness and isolation, household violence, suicide, drug abuse, stigma and discrimination, reduced social support, and increased financial problems, have been mentioned in the findings for different populations and age groups (12–17). The findings of a meta-analysis study among adults and children showed that the total prevalence rates of depression and anxiety were 25.2 and 20.5 percent, respectively. These symptoms were more pronounced among women and the older adults (18). In addition, symptoms of anxiety were more frequent among patients (39.6%) than among the general public. Furthermore, symptoms of anxiety were more frequently reported in the general public living in Africa (61.8%) than those living in America (34.9%), European countries (30.7%), and Asian countries (24.5%) (19). In addition to depression and anxiety, irritability and anger were also highly prevalent among the studied population (20).
According to the theories of health promotion and health behaviors, such as the protection motivation theory, the health belief model, and the theory of planned behavior, the nature of pandemics, the way news and/or rumors about pandemics is spread in social media, the focus on the main prevention protocols, such as quarantining (which goes back to the Spanish influenza of 1919 and SARS in 2003 (21,22), and the level of acceptance of the regulations by the citizens can lead to psychological consequences. Demographic variables, such as gender, age, ethnicity, education level, marital status, and occupational status, can impact the level of psychological consequences in individuals (23).
After China, Iran was one of the first countries that had to deal with the COVID-19 virus. So far, 7,569,769 infection cases and 144,878 deaths have been recorded in Iran. With the spread of COVID-19 in Iran, the lifestyle of people in the community changed, and at the beginning of the pandemic, social distancing followed by forced quarantines that were suggested as the main preventive measures against COVID-19 infection. Therefore, the COVID-19 pandemic had numerous physical and psycho-social consequences not only for patients but also for the general public. The important point is that the short-term effects of these consequences became long-term effects that still impact people in this country (24). However, the main focus during the pandemic was on physical health and the effectiveness of the vaccines, while psychological outcomes and interventions for vulnerable groups and the general public were mainly neglected. As a result, identifying the consequences of the COVID-19 pandemic at the national level can help with planning for controlling negative impact of future pandemics. The main objective of the current study was to examine the psychological impacts of the COVID-19 pandemic on the general population of Iran.
Material and Methods
The current study used an online cross-sectional survey via questionnaires among Iranian citizens. The study consisted of the following steps:
1. Developing an online web-based questionnaire by a team of experts,
2. Conducting a pilot study to evaluate the questions, the accuracy of the data, and the feasibility of the main study,
3. Distributing the online questionnaire throughout the country with the help of a representative selected from each province of the country,
4. Continuous monitoring of the online questionnaire to resolve any problems,
5. Keeping the online questionnaire open for two weeks,
6. Extracting and cleaning the received responses, and
7. Closing down the online questionnaire after collecting the required data.
The Sampling Method and the Sample Size
The convenient sampling method was used in the current study. To properly distribute the questionnaire, a representative from each province of the country who was familiar with the characteristics of the province was selected. Then, the representatives distributed the questionnaires online and in social groups.
To determine the size of the sample, Cochran’s formula, shown below, was utilized.
Cochran’s formula: Considering the diversity in the prevalence rate of the psychological symptoms of COVID-19, a prevalence rate of 50 percent was selected. Considering a confidence level of 95 percent and a precision of 97 percent in the formula, the size of the sample was obtained as 1067. Since the sampling process was not randomized, the obtained value was multiplied by 1.5. Then, considering a share of 10 percent for defective questionnaires, the final size of the sample was set at 1760. In total, 1827 questionnaires were completed; however, 92 questionnaires were rejected because of defects. Finally, data from 1735 completed questionnaires were analyzed.
Data Collection Tools
The online questionnaire included the following sections:
1. Demographic characteristics, including gender, age, stratum, level of education, marital status, and employment status
2. Perceived feelings during the COVID-19 pandemic were measured using the validated self-reported inventory by Reynolds, Garay (22). The self-reported inventory of feelings forward translated from English to Persian, then five experts consisting of psychologists and psychiatrics evaluated the relevancy of translated feelings for the Iranian context during the covid-19 pandemic. Also the feeling was presented to the ten lay people to confirm the clarity of feeling. These feelings included anger, annoyance, fear, guilt, happiness, helplessness, loneliness, nervousness, sadness, upset, agitation, boredom, nostalgia, worry, and relief.
The data for this study were collected from 1827 questionnaires completed from April 21 to June 21, 2021. About 57 percent of the questionnaires were completed during the first half of this period while 35 percent were completed during the second half.
The representative from each province shared a link to the questionnaire on social media networks while also asking the respondents to send the link to their friends and family members living in the same province as them. The questionnaire was designed in such a way that the respondents could refrain from answering any of the questions they didn’t want to answer. To keep the information of the respondents confident, the IPs for all questionnaires were deleted after managing the data. Since online studies do not allow providing oral explanations about the study and obtaining consent forms, after explaining the objectives of the study in detail in the questionnaire, some explanations were provided telling the respondents that participation was voluntary and that their information would remain strictly confidential. The study conducted after approving by the research ethics committee of the University of Social welfare and Rehabilitation Sciences (IR.USWR.REC.1400.145)
Data Analysis
The data were evaluated to identify missing data and outliers. Then, descriptive statistics, including percent, mean, and standard deviation, were used as well as inferential statistics, including chi-square, independent t-test, and analysis of variances (ANOVA) by SPSS.22.
Results
The average age of the respondents was 34.62 years with a standard deviation of 11.86. About 77 percent of the respondents were female, and the majority of the participants (38%) had a bachelor’s degree. Approximately 60 percent of the participants were married. The demographic characteristics of the respondents are presented in Table 1.
The Feelings of the Respondents during the COVID-19 Pandemic
The most frequent feeling experienced by the respondents during the covid-19 pandemic was boredom (44.0%), followed by nostalgia (40.6%), worry (35.3%), nervousness (34.1%), and fear (33.3%). Moreover, 8.2 percent of the participants had experienced relief and 9.3 percent had experienced happiness (Table 2).
Table 2. presents the feelings of the respondents during the covid-19 pandemic according to sex. The results from the chi-square test showed a significant relationship between gender and the level of perceived feelings. wherein, women experienced fear, sadness, nostalgia, nervousness, helplessness, and upset more significantly than men.
Figure 1.
Feelings of the respondents during the Covid-19 pandemic.
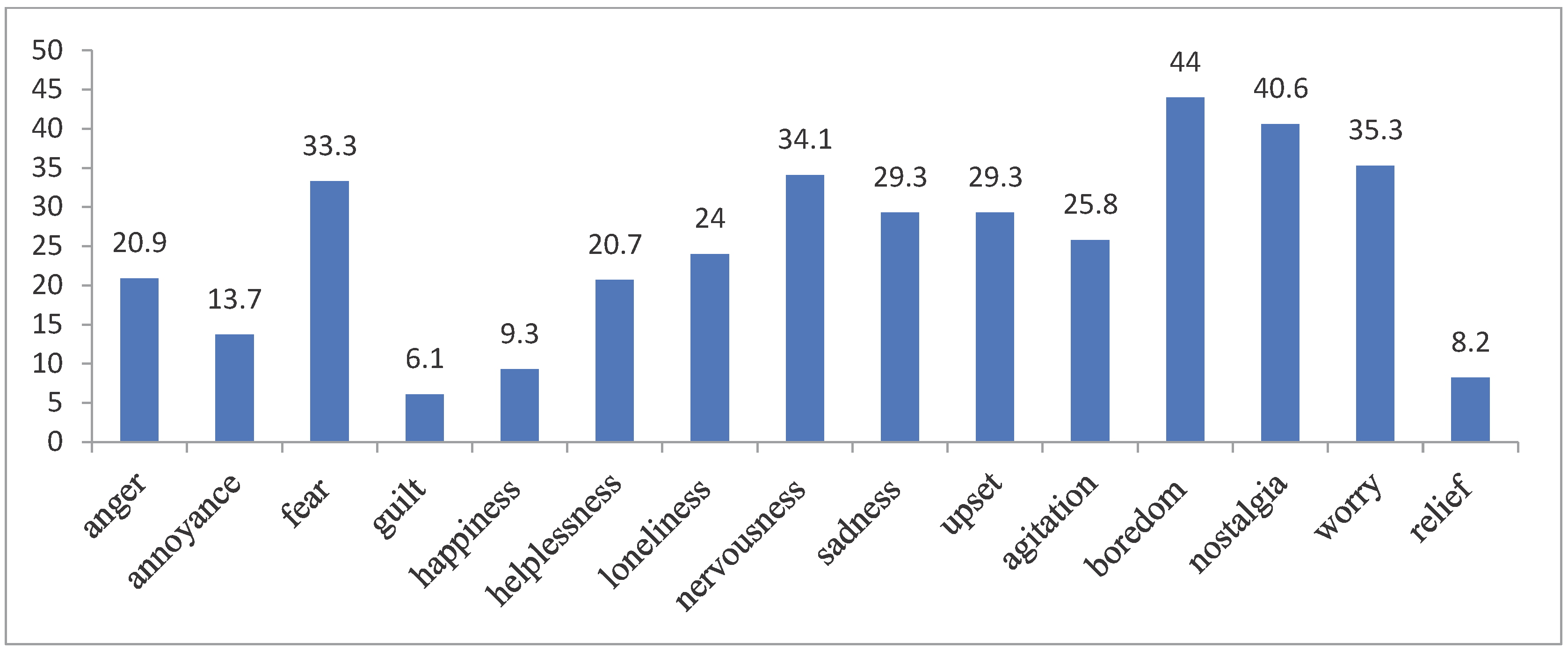
Table 3. shows the average age of the respondents according to their perceived feelings during the covid-19 pandemic. To evaluate the age difference between individuals experiencing the feelings and those not experiencing these feelings, an independent t-test was used. As shown in the table, participants with a higher average age experienced significantly lower levels of anger, annoyance, fear, guilt, happiness, helplessness, loneliness, nervousness, sadness, upset, agitation, boredom, and nostalgia.
Table 4. shows the perceived feelings of the respondents during the covid-19 pandemic based on their educational level. A series of chi-square tests were used to determine the relationship between the level of education and perceived feelings. The results revealed that there is a significant relationship between the level of education and feelings of annoyance, guilt, happiness, helplessness, agitation, and worry.
Table 5. shows the perceived feelings of the respondents during the covid-19 pandemic according to their employment status. The results from chi-square tests showed that employed individuals, compared to unemployed respondents, experienced significantly lower levels of anger, annoyance, guilt, happiness, loneliness, nervousness, sadness, upset, agitation, boredom, and nostalgia.
Table 6. shows the perceived feelings of the respondents during the covid-19 pandemic according to the stratum. The results from chi-square tests showed that those living in the city, compared to those living in rural areas, experienced significantly higher levels of anger, helplessness, sadness, upset, agitation, nostalgia, worry, and relief.
Table 7. shows the perceived feelings of the respondents during the stratum based on marital status. As can be seen from this table, the results of the chi-square tests show that married individuals, compared to single participants, experienced significantly lower levels of anger, annoyance, guilt, happiness, helplessness, loneliness, nervousness, sadness, upset, agitation, boredom, and nostalgia.
Discussion
While the focus at the global level was more on clinical symptoms and the physical effects of COVID-19 as well as the development of different vaccines, the psychological effects of this virus are also significant since they may remain for a long time or create changes in the lifestyle of the general population. As a result, the main objective of the current study was to evaluate and explore the prevalence rate of psychological effects among Iranian citizens. Based on the findings of the current study, the most frequent feelings experienced by the respondents during the covid-19 pandemic included boredom, nostalgia, and worry, respectively. Other studies performed in Asian countries, including India, the Philippines, and China, using online surveys have reported different figures for the prevalence rates of psychological problems. In these three countries, the rates of depression were reported as approximately 10, 13, and 37 percent, respectively, while the rates of anxiety were reported as approximately 29, 8, and 29 percent, respectively (25–27). In Asian countries where the infection rate of COVID-19 was lower, such as Saudi Arabia, about 24 percent of individuals reported mild to acute psychological problems. The difference in the prevalence rate stems from the differences in the time of the studies and the type of measurement tools utilized by these studies. However, a common point in the majority of studies is the increase in the level of negative feelings and emotions, especially anxiety. While in the current study, depression and anxiety were not evaluated using screening tools, reporting feelings such as helplessness and sadness can be a symptom of depression and anxiety, which is in line with the findings of other studies (25,26,28).
In addition to the fatal nature of COVID-19 and the fear of the infection, the spread of negative emotions, especially anxiety, can be the result of lower participation in society and the spread of numerous true and false news items about this virus in mass media and social media. During the pandemic, people were more focused on related news, which resulted in higher levels of fear and worry (29). However, it should be noted that a meta-analysis of longitudinal studies concluded that the effects of the quarantine during the COVID-19 pandemic on anxiety and depression were negligible, while they did not have a significant impact on positive emotions either (30). It seems that it is necessary to investigate the findings related to the spread of diseases like depression through more precise studies that consider individuals with a history of the disease, the prevalence of psychological disorders in the selected country before the COVID-19 pandemic, and the changes in emotions during different waves of the COVID-19 pandemic.
Some studies have reported that some participants experienced positive emotions during the quarantine as well, resulting in better relationships with family members (26). In the current study, experiencing feelings of happiness and relief was not frequently observed; however, it was reported more significantly among individuals with lower education levels. This is perhaps because of the possibility of spending more time with family. Nonetheless, this very group of individuals with lower levels of education reported higher levels of annoyance. While spending more time with family can be accompanied by feelings of happiness and relief, the lower capacity for resolving issues encountered in family discussions can result in higher levels of annoyance among spouses or parents and their children.
While people with higher education reported experiencing higher levels of relief, which can be the result of more financial security than other groups, they also reported higher levels of agitation, which can be due to fewer opportunities to be present in society and engage with everyday work activities. Moreover, the findings showed that those working during the pandemic reported lower levels of negative emotions. The COVID-19 pandemic resulted in the closure of many businesses, and unemployed individuals reported a higher prevalence of negative emotions and feelings, which can have long-term effects on these people since they need welfare support from the government to be able to return to their jobs.
In the current study, women had significantly higher levels of fear, sadness, and helplessness compared to men, which is in line with other studies (27,29) and can be due to the reduced level of social interactions and emotional support for women during the pandemic. The interesting finding that is in line with some studies (27) and at odds with some other studies (31) is that as age increases, the reported levels of negative emotions decreased. This can be because increased age is accompanied by the increased experience of going through different events, having financial security and stability, and having lower levels of fear of death. It should be noted that only the reported level of feeling worried was similar for different age groups, showing no significant difference. In general, contracting the COVID-19 virus can be worrisome for an individual and/or his or her loved ones.
In line with other studies, the findings of the current study showed that married individuals report lower levels of negative emotions compared to single individuals, emphasizing the buffering effect of social support from the family during crises (28). Before the COVID-19 pandemic, single individuals were experiencing higher levels of negative emotions and feelings, such as loneliness, and the pandemic had more significant impacts on this vulnerable group, which requires psychological interventions after the pandemic to prevent the continuation and/or exacerbation of these emotions. Furthermore, the findings of the study showed that people living in cities experienced more negative emotions and feelings compared to those living in rural areas because COVID-19 spread more heavily in cities because of the concentration of the population.
The spread of psychological problems has been more significant in the COVID-19 pandemic compared to previous pandemics, such as SARS and MERS, because of the higher possibility of suffering from acute infection, debilitating effects, and fatality in the COVID-19 pandemic. This necessitates a more serious focus on psychological interventions and rehabilitation (32,33). Some studies have claimed that people with better health information or better health status reported lower levels of anxiety during the COVID-19 pandemic. This can be a basis for policymaking for future pandemics, especially for vulnerable groups such as women.
In general, in addition to its clinical aspects, the COVID-19 virus created a challenge in the field of mental health around the world. Problems such as depression, fear, anxiety, and stress afflicted the general public along with health workers. Mental problems can lead to more severe conditions and problems, such as suicide since 90 percent of suicides are rooted in psychological problems. In individuals with a history of mental diseases and among unemployed people, such a pandemic can act as a mediatory variable between suicide ideation and suicide attempt (34). Moreover, with the spread of the COVID-19 virus and a higher focus on quarantining vulnerable groups, the consequent mental problems can result in physical problems such as cardiovascular diseases based on the embodiment approach. Therefore, it is necessary to consider the macro and micro aspects of the COVID-19 virus in society when setting healthcare policies.
Conclusions
Considering the prevalence of the psychological effects of the COVID-19 pandemic in many countries, particularly among vulnerable groups such as women, single, and unemployed people, we need to develop more supportive and consultative packages during pandemics as well as implement psychological rehabilitation after the crises. Moreover, at a global level, crises such as the COVID-19 pandemic can create more pressures and problems in countries like Iran which are suffering from economic sanctions because of problems in access to services and medicines. Therefore, it is necessary to consider plans and interventions for increasing resiliency and social support at local and national levels for future pandemics. Finally, considering the limitations of the current study because of using an online cross-sectional survey, it is recommended for future studies to perform longitudinal studies to analyze the remaining long-term psychological problems. Moreover, qualitative studies can more deeply explore the causes of these problems.
Author Contributions
Conceptualization, Y.M. and N.Z. Formal analysis, Y.M.; Methodology, Y.M.; Writing—review and editing, Y.M., N.Z., A.D., M.F. All authors have read and agreed to the published version of the manuscript.
Funding
No other funding has been provided for this work.
Conflicts of Interest
The authors have no competing interests to declare.
References
- Commission WMH. Wuhan Municipal Health Commission on the current situation of pneumonia in our city. Available online: http://wjw wuhan gov cn/front/web/showDetail/2019123108989 (accessed on 26 February 2020).
- Kaeuffer, C.; Le Hyaric, C.; Fabacher, T.; Mootien, J.; Dervieux, B.; Ruch, Y.; Hugerot, A.; Zhu, Y.-J.; Pointurier, V.; Clere-Jehl, R.; et al. Clinical characteristics and risk factors associated with severe COVID-19: prospective analysis of 1,045 hospitalised cases in North-Eastern France, March 2020. Eurosurveillance 2020, 25, 2000895. [Google Scholar] [CrossRef] [PubMed]
- COVID-19 CORONAVIRUS PANDEMIC 2022 [updated , 2022; cited 2022 ]. Available from: https://www.worldometers.info/coronavirus/. 10 December.
- Bentlage, E.; Ammar, A.; How, D.; Ahmed, M.; Trabelsi, K.; Chtourou, H.; Brach, M. Practical Recommendations for Maintaining Active Lifestyle during the COVID-19 Pandemic: A Systematic Literature Review. Int. J. Environ. Res. Public Heal. 2020, 17, 6265. [Google Scholar] [CrossRef] [PubMed]
- Di Renzo, L.; Gualtieri, P.; Pivari, F.; Soldati, L.; Attinà, A.; Cinelli, G.; Leggeri, C.; Caparello, G.; Barrea, L.; Scerbo, F.; et al. Eating habits and lifestyle changes during COVID-19 lockdown: an Italian survey. J. Transl. Med. 2020, 18, 229. [Google Scholar] [CrossRef] [PubMed]
- Jiang, W.; Hou, G.; Li, J.; Peng, C.; Wang, S.; Liu, S.; Zhuang, Q.; Chen, J.; Liu, H. Prevalence of H7N9 subtype avian influenza viruses in poultry in China, 2013–2018. Transbound. Emerg. Dis. 2019, 66, 1758–1761. [Google Scholar] [CrossRef] [PubMed]
- Sharma, P.; Sharma, R. Impact of covid-19 on mental health and aging. Saudi J. Biol. Sci. 2021, 28, 7046–7053. [Google Scholar] [CrossRef] [PubMed]
- Viner R, Russell S, Saulle R, Croker H, Stansfield C, Packer J, et al. School Closures during Social Lockdown and Mental Health, Health Behaviors, and Well-being among Children and Adolescents during the First COVID-19 Wave: A Systematic Review. JAMA Pediatrics. 2022.
- Yan, Y.; Du, X.; Lai, L.; Ren, Z.; Li, H. Prevalence of depressive and anxiety symptoms among Chinese older adults during the COVID-19 pandemic: A systematic review and meta-analysis. J. Geriatr. Psychiatry Neurol. 2022, 35, 182–195. [Google Scholar] [CrossRef] [PubMed]
- Yunitri, N.; Chu, H.; Kang, X.L.; Jen, H.-J.; Pien, L.-C.; Tsai, H.-T.; Kamil, A.R.; Chou, K.-R. Global prevalence and associated risk factors of posttraumatic stress disorder during COVID-19 pandemic: A meta-analysis. Int. J. Nurs. Stud. 2021, 126, 104136–104136. [Google Scholar] [CrossRef] [PubMed]
- Zhang, X.; Shi, X.; Wang, Y.; Jing, H.; Zhai, Q.; Li, K.; Zhao, D.; Zhong, S.; Song, Y.; Zhang, F.; et al. Risk Factors of Psychological Responses of Chinese University Students During the COVID-19 Outbreak: Cross-sectional Web-Based Survey Study. J. Med Internet Res. 2021, 23, e29312. [Google Scholar] [CrossRef]
- Mohamadi, M.; Goodarzi, A.; Aryannejad, A.; Fattahi, N.; Alizadeh-Khoei, M.; Miri, S.; Hekmat, H.; Payab, M.; Bodaghabadi, M. Geriatric challenges in the new coronavirus disease-19 (COVID-19) pandemic: A systematic review. Med J. Islam. Repub. Iran 2020. [Google Scholar] [CrossRef]
- Sen, K.; Prybutok, G.; Prybutok, V. The use of digital technology for social wellbeing reduces social isolation in older adults: A systematic review. SSM—Popul. Heal. 2021, 17, 101020. [Google Scholar] [CrossRef]
- Sepúlveda-Loyola, W.; Sepúlveda-Loyola, W.; Rodríguez-Sánchez, I.; Rodríguez-Sánchez, I.; Pérez-Rodríguez, P.; Pérez-Rodríguez, P.; Ganz, F.; Ganz, F.; Torralba, R.; Torralba, R.; et al. Impact of Social Isolation Due to COVID-19 on Health in Older People: Mental and Physical Effects and Recommendations. J. Nutr. Heal. Aging 2020, 24, 938–947. [Google Scholar] [CrossRef]
- Wan Mohd Yunus WMA, Kauhanen L, Sourander A, Brown JSL, Peltonen K, Mishina K, et al. Registered psychiatric service use, self-harm and suicides of children and young people aged 0–24 before and during the COVID-19 pandemic: a systematic review. Child and Adolescent Psychiatry and Mental Health. 2022;16(1). [CrossRef]
- Wang X, Wong YD, Yuen KF. Rise of ‘Lonely’ Consumers in the Post-COVID-19 Era: A Synthesised Review on Psychological, Commercial and Social Implications. International journal of environmental research and public health. 2021;18(2). [CrossRef]
- Yang, X.; Yip, B.H.K.; Mak, A.D.P.; Zhang, D.; Lee, E.K.P.; Wong, S.Y.S. The Differential Effects of Social Media on Depressive Symptoms and Suicidal Ideation Among the Younger and Older Adult Population in Hong Kong During the COVID-19 Pandemic: Population-Based Cross-sectional Survey Study. Psychopharmacol. 2021, 7, e24623. [Google Scholar] [CrossRef]
- Racine N, McArthur BA, Cooke JE, Eirich R, Zhu J, Madigan S. Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19: A Meta-analysis. JAMA Pediatrics. 2021;175(11):1142-50. [CrossRef]
- Kan, F.P.; Raoofi, S.; Rafiei, S.; Khani, S.; Hosseinifard, H.; Tajik, F.; Raoofi, N.; Ahmadi, S.; Aghalou, S.; Torabi, F.; et al. A Systematic Review of the Prevalence of Anxiety among the General Population during the COVID-19 Pandemic. J. Affect. Disord. 2021, 293, 391–398. [Google Scholar]
- Panchal, U.; de Pablo, G.S.; Franco, M.; Moreno, C.; Parellada, M.; Arango, C.; Fusar-Poli, P. The impact of COVID-19 lockdown on child and adolescent mental health: systematic review. Eur. Child Adolesc. Psychiatry 2021, 32, 1151–1177. [Google Scholar] [CrossRef] [PubMed]
- Bass, S.B.; Ruzek, S.B.; Ward, L.; Gordon, T.F.; Hanlon, A.; Hausman, A.J.; Hagen, M. If You Ask Them, Will They Come? Predictors of Quarantine Compliance During a Hypothetical Avian Influenza Pandemic: Results From a Statewide Survey. Disaster Med. Public Heal. Prep. 2010, 4, 135–144. [Google Scholar] [CrossRef] [PubMed]
- Reynolds, D.L.; Garay, J.R.; Deamond, S.L.; Moran, M.K.; Gold, W.; Styra, R. Understanding, compliance and psychological impact of the SARS quarantine experience. Epidemiology Infect. 2007, 136, 997–1007. [Google Scholar] [CrossRef]
- Carlucci, L.; D’ambrosio, I.; Balsamo, M. Demographic and Attitudinal Factors of Adherence to Quarantine Guidelines During COVID-19: The Italian Model. Front. Psychol. 2020, 11, 559288. [Google Scholar] [CrossRef]
- Shanbehzadeh, S.; Tavahomi, M.; Zanjari, N.; Ebrahimi-Takamjani, I.; Amiri-Arimi, S. Physical and mental health complications post-COVID-19: Scoping review. J. Psychosom. Res. 2021, 147, 110525–110525. [Google Scholar] [CrossRef]
- Ahmed, M.Z.; Ahmed, O.; Aibao, Z.; Hanbin, S.; Siyu, L.; Ahmad, A. Epidemic of COVID-19 in China and associated Psychological Problems. Asian J. Psychiatry 2020, 51, 102092. [Google Scholar] [CrossRef]
- Grover S, Sahoo S, Mehra A, Avasthi A, Tripathi A, Subramanyan A, et al. Psychological impact of COVID-19 lockdown: An online survey from India. Indian Journal of Psychiatry. 2020;62(4).
- Tee, M.L.; Tee, C.A.; Anlacan, J.P.; Aligam, K.J.G.; Reyes, P.W.C.; Kuruchittham, V.; Ho, R.C. Psychological impact of COVID-19 pandemic in the Philippines. J. Affect. Disord. 2020, 277, 379–391. [Google Scholar] [CrossRef]
- Serafini, G.; Parmigiani, B.; Amerio, A.; Aguglia, A.; Sher, L.; Amore, M. The psychological impact of COVID-19 on the mental health in the general population. Qjm: Int. J. Med. 2020, 113, 531–537. [Google Scholar] [CrossRef] [PubMed]
- Moghanibashi-Mansourieh, A. Assessing the anxiety level of Iranian general population during COVID-19 outbreak. Asian J. Psychiatry 2020, 51, 102076–102076. [Google Scholar] [CrossRef] [PubMed]
- Prati, G.; Mancini, A.D. The psychological impact of COVID-19 pandemic lockdowns: a review and meta-analysis of longitudinal studies and natural experiments. Psychol. Med. 2021, 51, 201–211. [Google Scholar] [CrossRef] [PubMed]
- Jassim, G.; Jameel, M.; Brennan, E.; Yusuf, M.A.; Hasan, N.; Alwatani, Y. Psychological Impact of COVID-19, Isolation, and Quarantine: A Cross-Sectional Study. Neuropsychiatr. Dis. Treat. 2021, ume 17, 1413–1421. [Google Scholar] [CrossRef]
- Data NAPT-L. From RSV F Vaccine Phase 1 Clinical Trial in Pediatrics| NovavaxInc.. Novavax. Retrieved 2020-12-11.
- Kunz, R.; Minder, M. COVID-19 pandemic: palliative care for elderly and frail patients at home and in residential and nursing homes. Swiss Med Wkly. 2020, 150, w20235. [Google Scholar] [CrossRef]
- Mamun MA, Ullah I. COVID-19 suicides in Pakistan, dying off not COVID-19 fear but poverty?–The forthcoming economic challenges for a developing country. J Brain, behavior, immunity. 2020;87:163. [CrossRef]

Table 1.
Demographic characteristics of the respondents.
| Variable | Category | frequency | % |
|---|---|---|---|
| Sex | Female | 1337 | 77.1 |
| Male | 398 | 22.9 | |
| Stratum | Urban | 1629 | 93.9 |
| Rural | 106 | 6.1 | |
| Level of Education | Primary | 27 | 1.6 |
| Secondary | 37 | 2.1 | |
| High school | 64 | 3.7 | |
| Diploma | 433 | 25.0 | |
| Bachler | 660 | 38.0 | |
| Master | 327 | 18.8 | |
| PhD | 187 | 10.8 | |
| Marital status | Single | 653 | 37.6 |
| Married | 1031 | 59.4 | |
| Divorced | 30 | 1.7 | |
| Widow | 21 | 1.3 | |
| Employment status | Employed | 871 | 50.2 |
| Unemployed | 864 | 49.8 |
The Feelings of the Respondents during the COVID-19 Pandemic
Table 2.
Feelings of the respondents during the Covid-19 pandemic by Sex.
| Feelings | Female | Male | Χ² | P-Value | ||
| N | % | N | % | |||
| anger | 286 | 21.4 | 77 | 19.3 | 0.78 | 0.379 |
| annoyance | 179 | 13.4 | 59 | 14.8 | 0.53 | 0.465 |
| fear | 476 | 35.6 | 101 | 25.4 | 14.45 | 0.001 |
| guilt | 84 | 6.3 | 21 | 5.3 | 0.55 | 0.46 |
| happiness | 116 | 8.7 | 46 | 11.6 | 3.01 | 0.083 |
| helplessness | 295 | 22.1 | 65 | 16.3 | 6.13 | 0.013 |
| loneliness | 344 | 25.7 | 72 | 18.1 | 9.82 | 0.002 |
| nervousness | 478 | 35.8 | 113 | 28.4 | 7.4 | 0.007 |
| sadness | 420 | 31.4 | 89 | 22.4 | 12.12 | 0.001 |
| upset | 410 | 30.7 | 98 | 24.6 | 5.41 | 0.02 |
| agitation | 345 | 25.8 | 102 | 25.6 | 0.01 | 0.944 |
| boredom | 605 | 45.3 | 159 | 39.9 | 3.5 | 0.061 |
| nostalgia | 581 | 43.5 | 123 | 30.9 | 20.04 | 0.001 |
| worry | 497 | 37.2 | 116 | 29.1 | 8.65 | 0.003 |
| relief | 110 | 8.2 | 33 | 8.3 | 0.01 | 0.967 |
Table 3.
The Mean age of the respondents by perceived Feeling during the Covid-19 pandemic.
| Feelings | No | Yes | t | P-Value | ||||
| N | M | SD | N | M | SD | |||
| anger | 1357 | 35.80 | 11.92 | 361 | 30.26 | 10.52 | 8.64 | 0.001 |
| annoyance | 1481 | 35.16 | 11.70 | 237 | 31.39 | 12.33 | 4.56 | 0.001 |
| fear | 1144 | 35.35 | 12.26 | 574 | 33.21 | 10.88 | 3.55 | 0.001 |
| guilt | 1614 | 35.07 | 11.82 | 104 | 27.96 | 10.39 | 5.99 | 0.001 |
| happiness | 1556 | 35.17 | 11.73 | 162 | 29.53 | 11.90 | 5.82 | 0.001 |
| helplessness | 1361 | 35.65 | 12.22 | 357 | 30.77 | 9.43 | 7.02 | 0.001 |
| loneliness | 1304 | 35.49 | 11.58 | 414 | 31.94 | 12.32 | 5.35 | 0.001 |
| nervousness | 1130 | 36.24 | 12.14 | 588 | 31.56 | 10.65 | 8.22 | 0.001 |
| sadness | 1209 | 35.74 | 11.96 | 509 | 32.01 | 11.17 | 6.03 | 0.001 |
| upset | 1211 | 36.30 | 11.89 | 507 | 30.67 | 10.79 | 9.55 | 0.001 |
| agitation | 1272 | 35.78 | 11.91 | 446 | 31.37 | 11.06 | 6.84 | 0.001 |
| boredom | 957 | 36.78 | 12.20 | 761 | 31.94 | 10.82 | 8.70 | 0.001 |
| nostalgia | 1018 | 35.46 | 11.71 | 700 | 33.43 | 11.97 | 3.50 | 0.001 |
| worry | 1110 | 34.94 | 12.27 | 608 | 34.08 | 11.05 | 1.49 | 0.137 |
| relief | 1575 | 34.68 | 11.83 | 143 | 34.11 | 12.15 | 0.55 | 0.580 |
Table 4.
Feeling of the respondents during Covid-19 pandemic by level of education.
| Feelings | Low Education | Diploma | Bachelor | Master/PhD | Χ² | P-Value | ||||
| N | % | N | % | N | % | N | % | |||
| anger | 24 | 18.8 | 96 | 22.2 | 122 | 18.5 | 121 | 23.5 | 5.27 | 0.153 |
| annoyance | 20 | 15.6 | 68 | 15.7 | 71 | 10.8 | 79 | 15.4 | 7.91 | 0.048 |
| fear | 38 | 29.7 | 128 | 29.6 | 225 | 34.1 | 186 | 36.2 | 5.59 | 0.133 |
| guilt | 10 | 7.8 | 36 | 8.3 | 29 | 4.4 | 30 | 5.8 | 7.83 | 0.050 |
| happiness | 17 | 13.3 | 49 | 11.3 | 46 | 7 | 50 | 9.7 | 8.82 | 0.032 |
| helplessness | 11 | 8.6 | 83 | 19.2 | 130 | 19.7 | 136 | 26.5 | 22.8 | 0.001 |
| loneliness | 33 | 25.8 | 114 | 26.3 | 156 | 23.6 | 113 | 22 | 2.7 | 0.440 |
| nervousness | 37 | 28.9 | 155 | 35.8 | 210 | 31.8 | 189 | 36.8 | 5.25 | 0.154 |
| sadness | 31 | 24.2 | 140 | 32.3 | 178 | 27 | 160 | 31.1 | 6.07 | 0.108 |
| upset | 41 | 32 | 134 | 30.9 | 186 | 28.2 | 147 | 28.6 | 1.55 | 0.671 |
| agitation | 31 | 24.2 | 134 | 30.9 | 148 | 22.4 | 134 | 26.1 | 10.12 | 0.018 |
| boredom | 48 | 37.5 | 200 | 46.2 | 288 | 43.6 | 228 | 44.4 | 3.1 | 0.377 |
| nostalgia | 42 | 32.8 | 175 | 40.4 | 290 | 43.9 | 197 | 38.3 | 7.38 | 0.061 |
| worry | 25 | 19.5 | 140 | 32.3 | 251 | 38 | 197 | 38.3 | 19.81 | 0.000 |
| relief | 7 | 5.5 | 35 | 8.1 | 46 | 7 | 55 | 10.7 | 6.84 | 0.077 |
Table 5.
Feeling of the respondents during Covid-19 pandemic by employment status.
| Feelings | Employed | Unemployed | Χ² | P-Value | ||
| N | % | N | % | |||
| anger | 151 | 17.3 | 212 | 24.5 | 13.59 | 0.001 |
| annoyance | 99 | 11.4 | 139 | 16.1 | 8.17 | 0.004 |
| fear | 296 | 34 | 281 | 32.5 | 0.42 | 0.518 |
| guilt | 38 | 4.4 | 67 | 7.8 | 8.78 | 0.003 |
| happiness | 65 | 7.5 | 97 | 11.2 | 7.26 | 0.007 |
| helplessness | 166 | 19.1 | 194 | 22.5 | 3.04 | 0.081 |
| loneliness | 170 | 19.5 | 246 | 28.5 | 19.08 | 0.001 |
| nervousness | 257 | 29.5 | 334 | 38.7 | 16.17 | 0.001 |
| sadness | 232 | 26.6 | 277 | 32.1 | 6.16 | 0.013 |
| upset | 213 | 24.5 | 295 | 34.1 | 19.66 | 0.001 |
| agitation | 190 | 21.8 | 257 | 29.7 | 14.27 | 0.001 |
| boredom | 357 | 41 | 407 | 47.1 | 6.59 | 0.001 |
| nostalgia | 311 | 35.7 | 393 | 45.5 | 17.21 | 0.001 |
| worry | 315 | 36.2 | 298 | 34.5 | 0.53 | 0.466 |
| relief | 74 | 8.5 | 69 | 8.0 | 0.15 | 0.699 |
Table 6.
Feeling of the respondents during Covid-19 pandemic by stratum.
| Feelings | Urban | Rural | Χ² | P-Value | ||
| N | % | N | % | |||
| anger | 352 | 21.6 | 11 | 10.4 | 7.59 | 0.006 |
| annoyance | 228 | 14 | 10 | 9.4 | 1.75 | 0.186 |
| fear | 541 | 33.2 | 36 | 34 | 0.03 | 0.874 |
| guilt | 100 | 6.1 | 5 | 4.7 | 0.35 | 0.552 |
| happiness | 151 | 9.3 | 11 | 10.4 | 0.14 | 0.704 |
| helplessness | 349 | 21.4 | 11 | 10.4 | 7.39 | 0.007 |
| loneliness | 398 | 24.4 | 18 | 17 | 3.03 | 0.082 |
| nervousness | 563 | 34.6 | 28 | 26.4 | 2.94 | 0.086 |
| sadness | 489 | 30 | 20 | 18.9 | 5.97 | 0.015 |
| upset | 487 | 29.9 | 21 | 19.8 | 4.89 | 0.027 |
| agitation | 430 | 26.4 | 17 | 16 | 5.58 | 0.018 |
| boredom | 727 | 44.6 | 37 | 34.9 | 3.82 | 0.050 |
| Nostalgia | 676 | 41.5 | 28 | 26.4 | 9.39 | 0.002 |
| worry | 589 | 36.2 | 24 | 22.6 | 7.96 | 0.005 |
| relief | 141 | 8.7 | 2 | 1.9 | 6.03 | 0.014 |
Table 7.
Feeling of the respondents during Covid-19 pandemic by marital status.
| Feelings | Unmarried | Married | Χ² | P-Value | ||
| N | % | N | % | |||
| anger | 194 | 27.6 | 169 | 16.4 | 31.52 | 0.001 |
| annoyance | 130 | 18.5 | 108 | 10.5 | 22.57 | 0.001 |
| fear | 245 | 34.8 | 332 | 32.2 | 1.27 | 0.259 |
| guilt | 69 | 9.8 | 36 | 3.5 | 29.29 | 0.001 |
| happiness | 92 | 13.1 | 70 | 6.8 | 19.48 | 0.001 |
| helplessness | 198 | 28.1 | 162 | 15.7 | 47.53 | 0.001 |
| loneliness | 229 | 32.5 | 187 | 18.1 | 47.53 | 0.001 |
| nervousness | 275 | 39.1 | 316 | 30.6 | 13.18 | 0.001 |
| sadness | 252 | 35.8 | 257 | 24.9 | 23.84 | 0.001 |
| upset | 255 | 36.2 | 253 | 24.5 | 27.57 | 0.001 |
| agitation | 225 | 32 | 222 | 21.5 | 23.78 | 0.001 |
| boredom | 367 | 52.1 | 397 | 38.5 | 31.51 | 0.001 |
| nostalgia | 308 | 43.8 | 396 | 38.4 | 4.95 | 0.026 |
| worry | 257 | 36.5 | 356 | 34.5 | 0.72 | 0.398 |
| relief | 64 | 9.1 | 79 | 7.7 | 1.13 | 0.288 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



