
Submitted:
09 May 2023
Posted:
11 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Invasive fungal infections, notably candidemia, have been associated with COVID-19. The epidemiology of candidemia has significantly changed during the COVID-19 pandemic. We aim to identify the microbiological profile, resistance rates, and outcomes of COVID-19 associated candidemia (CAC) compared to patients with candidemia not associated with COVID-19. We retrospectively collected data on patients with candidemia admitted to the American University of Beirut Medical Center between 2004 and 2022. We compared the epidemiology of candidemia during and prior to the COVID-19 pandemic. Additionally, we compared the outcomes of critically ill patients with CAC to those with candidemia without COVID-19 from March 2020 till March 2022. Among 245 candidemia episodes, 156 occurred prior to the pandemic and 89 during the pandemic. Of the latter, 39 (43.8%) were CAC, most of which (82%) were reported from intensive care units (ICU). Non-albicans Candida (NAC) spp. were predominant throughout the study period (67.7%). Candida auris infection was the most common cause of NAC spp. in CAC. C. glabrata had decreased susceptibility rates to fluconazole and caspofungin during the pandemic period (46.1% and 38.4% respectively). Mortality rate in the overall ICU population during the pandemic was 76.6%, much higher than the previously reported mortality of candidemia from previous studies at our center. There was no significant difference in 30-day mortality between CAC and non-CAC (75.0% vs 78.1%; P =0.76). Performing ophthalmic examination (P = 0.002), CVC removal during the 48 hours following the candidemia (P = 0.008) and identifying the Candida spp. (P = 0.028) were significantly associated with a lower case-fatality rate. The epidemiology of candidemia has been significantly affected by the COVID-19 pandemic at our center. Rigorous infection control measures and proper antifungal stewardship are essential to combat highly resistant species like C. auris.
Keywords:
Candida
; Candidemia
; invasive candidiasis
; Candida auris
; non-albicans candida
; COVID-19
; antifungal susceptibility
; Lebanon
; Arab world
; EQUAL score
1. Introduction
Candida species are the fourth most commonly isolated pathogens in nosocomial bloodstream infections (BSI) in the United States and are associated with over 350,000 yearly deaths worldwide [1]. The epidemiology of candidemia varies widely around the globe. While Candida albicans is the predominant spp. in Europe and in neighboring Arab countries, accounting for 57% [2] and 22.3 to 60% [3] of episodes of candidemia respectively, studies from Lebanon show a predominance of non-albicans candida (NAC) spp. [4].
Since December 2019, the COVID-19 pandemic has triggered a global health crisis. Critically ill COVID-19 patients have been reported to be more susceptible to co-infections with other pathogens, notably multidrug-resistant (MDR) bacterial and fungal organisms [5,6]. The incidence of COVID-19 associated candidemia (CAC) has been highly variable from different reports, ranging from 0.03% to 9% [7]. Both the incidence and mortality of candidemia in patients with COVID-19 is substantially higher compared to patients without COVID-19 and may reach 75%[8]. Additionally, the onset of candidemia is earlier in patients with COVID-19 compared to patients without [9,10]. CAC also results in prolonged length of hospitalization and overall worse patients’ outcomes [10].
Although one study mentioned that there were no significant differences in the microbiological profile of candidemia in patients with COVID-19 and those without, other reports confirm that NAC spp. appear to be the most predominant in CAC [8,11,12]. The emergence of highly resistant Candida auris during the COVID-19 pandemic has been of particular concern and has been responsible for multiple outbreaks in healthcare settings, especially in intensive care units (ICU), including in health care settings that had not reported such infections previously [6,8].
The aim of this study was to describe the changing epidemiology and rates of antifungal resistance of episodes of candidemia in a tertiary care center in Lebanon before and after the COVID-19 pandemic. Additionally, we aimed to compare the outcomes of patients with CAC and those with candidemia in patients not infected with COVID-19. We also investigated the impact of compliance with the elements of the European Confederation of Medical Mycology Quality of Clinical Candidemia Management (EQUAL) Candida score on mortality in patients with CAC.
2. Research Design and Methods
2.1. Study Design and Setting
We conducted a retrospective study that included all patients admitted with candidemia to the American University of Beirut Medical Center (AUBMC), over a span of 18 years from January 2004 to March 2022, including the period of the COVID-19 pandemic in our region (March 1st, 2020, till March 30th, 2022).
AUBMC is a 420-bed academic tertiary-care center and a national and regional referral center in Beirut, Lebanon. AUBMC receives over 25,000 inpatient admissions annually. It provides specialized medical and surgical services including oncology and bone marrow transplantation services. The Clinical Microbiology Laboratory (CML) at AUBMC is accredited by the College of American Pathologists since 2004 and uses the CLSI breakpoints for antimicrobial susceptibility breakpoints.
2.2. Population and Data Collection
Using the Electronic Health Records (EHR) at AUBMC, we identified all confirmed episodes of candidemia from hospitalized patients between January 2004 and March 2022. Inclusion criteria were patients (1) aged 18 years old and above, (2) who had candidemia defined by isolation of Candida spp. in at least one blood culture. We excluded episodes of candidemia with concomitant bacteremia. Patients whose outcomes were not available at 30 days were excluded from the mortality analysis.
After determining the prevalence of each Candida species during each year and trends of antifungal susceptibility within each year, we sought to compare the outcomes of critically ill patients with CAC and those with candidemia without COVID-19. For this analysis, we included episodes of candidemia that occurred from March 2020 till March 2022. We did not include patients without COVID-19 who had candidemia prior to the onset of the pandemic to adjust to the ongoing changes of the fungal ecology at our center. The first group consisted of all episodes of candidemia that were not associated with COVID-19 (non-CAC) while the second group consisted of episodes of CAC.
Data collected included: demographics (age, sex), comorbidities (diabetes mellitus, hemodialysis), immunosuppression (malignancy, chemotherapy, or immunotherapy within the previous 30 days, hematopoietic or solid organ transplantation, neutropenia), and patient characteristics at the onset of infection (hospital unit, mechanical ventilation (MV), presence of central venous catheter (CVC), parenteral nutrition, abdominal surgery within the previous 30 days, antibiotic and antifungal history within the previous 30 days and source of candidemia). We also extracted data regarding COVID-19 clinical course and management (including acute respiratory distress (ARDS), need for MV, treatment with corticosteroids and immunomodulatory medications) for patients who were admitted between March 1st, 2020 and March 30th, 2022. We defined neutropenia as an absolute neutrophil count (ANC) < 1500 cells/mm3 which was further categorized into mild (<1500 and ≥ 1000 cells/mm3), moderate (<1000 and ≥ 500 cells/mm3) and severe (<500 cells/mm3) [13].
2.3. Microbiological Definitions
All cases of COVID-19 were confirmed using a real-time polymerase chain reaction (RT-PCR) that was performed on nasal swabs, tracheal aspirates, broncho-alveolar lavage, or other respiratory samples.
Candidemia was defined as the isolation of Candida spp. from blood culture of a peripheral or central sample. Non-albicans candidemia was defined as the isolation of a non-albicans Candida spp. (NAC) from initial blood cultures, whether it occurred individually or as co-infection with C. albicans. Blood culture bottles were incubated in a BACT/ALERT® system (Durham, NC, USA), and Candida spp. identification and antifungal susceptibility testing were performed using VITEK® 2 system (BioMérieux, Marcy L’Etoile, France). Antifungal susceptibility was reported using the Clinical and Laboratory Standards Institute breakpoints (CLSI) [14].
Candidemia was considered as CAC if the episode occurred within 42 days following the onset of COVID-19. Recurrent candidemia was defined as two episodes of candidemia occurring ≥7 days apart with clinical and microbiological resolution in the interim.
We used the National Healthcare Safety Network (NHSN) definition of central line associated bloodstream infection (CLABSI)[15]. As per the Infectious Diseases Society of America (IDSA) guidelines on the treatment of invasive candidiasis, appropriate duration of treatment was defined as 14 days of antifungal treatment after the first negative blood culture [16].
2.4. Statistical Analysis:
Data management and analysis were conducted using IBM SPSS version 28 (IBM, New York, NY, USA). Categorical data was presented using count (percent), while continuous data was presented using mean ± standard deviation (SD). Associations between categorical variables and the outcome variable (CAC vs. non-CAC) were assessed using the Chi-square test or Fisher’s exact test when 20% of expected cell counts are below 5. Associations between continuous variables and the outcome variable (CAC vs. non-CAC) were assessed using independent-samples t-test. Significance was set at < 0.05.
2.5. Ethical Considerations
The study received approval by the institutional review board (IRB) at AUBMC (Protocol number: BIO-2019-0290). Patient consent was waived, as this is a retrospective chart review. The study included all adult patients with candidemia presenting to AUBMC in the study period, with no regard to sex and ethnic background. It posed no risk to patients. The potential benefits of the study outweigh the potential risks.
3. Results
3.1. Baseline Characteristics of the Study Population
We identified 233 patients with a total of 245 episodes of candidemia between 2004 and 2022. We reported 245 episodes of candidemia of which 156 occurred prior to March 2020 and 89 during the pandemic. Among the latter, 39 (43.8%) were CAC while the remainder (56.2%) were reported from patients without COVID-19. Most episodes of CAC (82%) occurred in the intensive care unit (ICU). In patients with CAC, the median time between SARS-CoV-2 positive testing and candidemia was 24 days while median time from ICU admission to candidemia was 17.5 days.
3.2. Epidemiology of Candida Species
Over the span of 18 years, we found a predominance of NAC species (67.7%) compared to C. albicans (32.2%). NAC were predominant in both patients with and without COVID-19 (74.3% and 66.5% respectively). We noted an increase in the prevalence of NAC species between 2020 and 2022. Speciation was done for 83.3% of all isolates. For NAC species, the rate of speciation was 66.7 % between 2004 and 2008, 70% between 2009 and 2013, 79.6% between 2014 and 2019, and 76.1% between the years 2020 and 2022.
Candida glabrata was the most predominant NAC species in the pre-pandemic era (42.7%). However, during the pandemic period we observed a decrease in the incidence of C. glabrata (21.7%). We also reported the emergence of C. auris candidemia for the first time in Lebanon. After the pandemic, C. auris was responsible for 26 episodes of candidemia. Its prevalence was 32% in patients with non-CAC and 25.6% in patients with CAC (Figure 1).
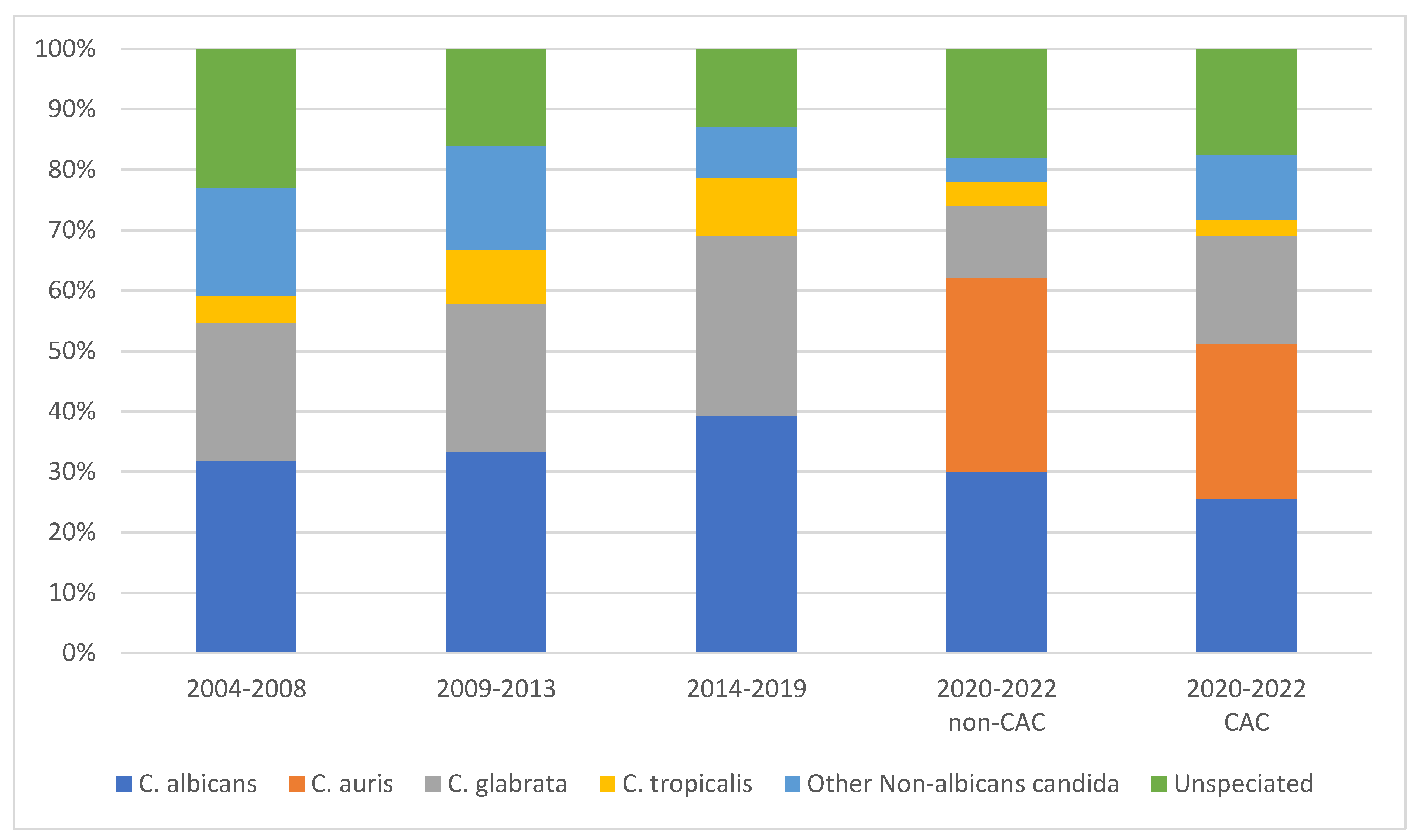
Figure 1.
Predominance of Candida spp. over 18 years at AUBMC.
3.3. Antifungal Susceptibility
Antifungal susceptibility testing was performed on 140 isolates (57.1%) including 48.7% of C. albicans and 70% of NAC.
Overall, C. albicans isolates had high susceptibility rates to fluconazole (91.7%), voriconazole (88.2%), amphotericin B (100%), and caspofungin (100%). On the other hand, C. glabrata isolates had lower rates of susceptibility to fluconazole (58%), voriconazole (84%), and caspofungin (63.6%) but were highly susceptible to amphotericin B (97.2%) (Table 1).
Susceptibility results were available for twelve isolates of C. auris all of which were found to be resistant to azoles and amphotericin B but susceptible to caspofungin.
3.4. Outcomes of CAC and non-CAC
We compared characteristics, comorbidities, management, and outcomes of CAC and non-CAC in critically ill patients between March 2020 and March 2022. All patients were admitted to the ICU. We found no significant differences in age, sex, and comorbidities between both groups (Table 2). There were also no significant differences in the percentage of episodes occurring while patients were mechanically ventilated, had CVC or had recently received antimicrobials including antifungals. We also found no significant differences in the epidemiology of Candida spp. between both groups.
We noted a 30-day mortality of 76.6% from all episodes, with no significant difference between CAC and non-CAC. Regarding the management of both groups, we noted a significantly higher rate of empirical antifungal treatment with caspofungin for CAC compared to non-CAC (83.3% vs. 37.9%; P<0.001). However, there was no statistically significant difference in empirical treatment with anidulafungin (P=0.19) or micafungin (P=0.49) between the two groups. Overall, the use of echinocandin as treatment was significantly higher in CAC compared to non-CAC (93.3% vs. 69.0%; P=0.016) (Table 3).
We found that 17% of all episodes of candidemia were treated for a duration of 14 or more days after the first negative blood culture. The median duration of treatment for CAC patients was 9.63 days and 16.06 days for non-CAC (P=0.14). Moreover, our analysis showed that 79% of patients with CAC died before the completion of 14 days of antifungal treatment.
3.5. EQUAL Score Analysis
The mean EQUAL score in the total ICU population during the pandemic was not statistically significant between survivors and non-survivors (9.92 ± 3.82 vs. 9.12 ± 3.49, P= 0.28). Similarly, no statistical difference was found in scores in the subset of patients with CVC between survivors and non-survivors (10.36 ± 3.66 vs. 9.43 ± 3.36, P=0.25).
When assessing the components of the EQUAL score individually, survival was higher with susceptibility testing (35.7%) compared to episodes when susceptibility testing was not performed (16.7%). However, this was not statistically significant (P= 0.098). Although performing echocardiography was not associated with lower mortality, survival was significantly higher when ophthalmic examination was done (63.6% vs. 15.4%; P= 0.002). Survival was also higher when a CVC, if placed at onset of infection, was removed within 48 hours (37.9% vs. 7.7%; P= 0.008), and when Candida speciation was performed (100% vs. 73.5%; P= 0.028).
Only 17% of our patient population completed the 14 days of antifungal treatment after the first negative blood culture with a significantly higher survival rate than those treated for a shorter duration (40% vs. 7.9%; P= 0.011).
4. Discussion
This study describes the changing epidemiology of candidemia over 18 years from a tertiary care center in Lebanon. It also reports the first investigation of CAC in Lebanon. Only one study has been previously reported from the Arab countries in the Middle East region [8]. We observed significant differences in the epidemiology of candidemia during the COVID-19 pandemic compared to the pre-pandemic era. Our findings revealed the emergence of new Candida spp. with higher resistance rates during the pandemic. While we did not find evidence of higher mortality among patients with CAC compared to those with non-CAC, the management strategies differed between the two groups. We also noted a higher mortality rate of patients with candidemia during the pandemic compared to the pre-pandemic period.
According to our analysis, we observed a significant change in candidemia epidemiology. In the pre-pandemic era, the microbiologic profile of candidemia at AUBMC was consistent with worldwide and Arab world observations regarding the increasing predominance of NAC [17]. Additionally, during the pre-pandemic period, C. glabrata was identified as the primary NAC species at our center [18]. However, during the pandemic period, we observed a decrease in C. glabrata incidence with the emergence of C. auris, a highly resistant species that can rapidly colonize patients and spread in the units. The COVID-19 pandemic overwhelmed the healthcare system, leading to breaches in infection control practices and measures [19]. This resulted in the transmission of C. auris and other multidrug resistant organisms (MDRO) among hospitalized patients [6,19], leading to multiple outbreaks worldwide, particularly in ICUs [20].
We did not observe any difference in Candida spp. between CAC and non-CAC, as both groups had a higher prevalence of NAC. These findings are consistent with a previous study by Machado et al., which suggests that changes in the prevalence of multi-drug resistant Candida spp. are not exclusive to COVID-19 patients, but may be linked to the increased use of antifungal medications [21]. In fact, COVID-19 affected the pattern of antifungal use in our center, with a significant increase in the use of echinocandins as first line antifungal treatment in CAC patients, probably due to the emergence of fluconazole resistant species such as C. glabrata and C. auris [22]. Such species are known to be more prevalent in COVID-19 ICU patients particularly in those with prolonged length of stay [12,23]. Additionally, as per the international guidelines, echinocandins were used as first line therapy in the management of candidemia in the ICU including in patients with septic shock, and those with liver injury [23]. The unrestricted use of antifungals during the pandemic could have contributed to the increase in resistance rates of Candida spp. in our center [24]. Susceptibility rates to fluconazole in C. glabrata isolates decreased from 73.9% before the pandemic to 46.1% during the pandemic. In addition, there are increasing reports of C. glabrata resistance to echinocandins [25,26]. Our results show a rate of resistance of C. glabrata to caspofungin of 36.4 %. Similar findings have been reported in studies from Turkey and Kuwait, which have shown an increase in the prevalence of multi-drug-resistant Candida spp. among CAC patients [9,25,26]. The increased resistance rates are of high clinical significance, as echinocandins are considered first-line agents for empiric treatment of invasive candidiasis [27]. Our results show that 34.4% of the candidemic patients had received antifungal agents in the 30 days prior to candidemia. These findings reiterate on the importance of antifungal stewardship efforts to control the evolution of antifungal resistance among Candida spp. [28]. Furthermore it reinforces the need for the One-Health approach that expands antifungal stewardship efforts beyond human medicine only [29,30].
In our study, we used the EQUAL score to assess compliance with the guidelines of invasive candidiasis during the pandemic and to identify factors that may be associated with an increased 30-day mortality. Our results show that survivors had slightly higher EQUAL scores than non-survivors (9.92 ± 3.82 vs. 9.12 ± 3.49, P= 0.28) in the overall population as well as in CVC carriers (10.36 ± 3.66 vs. 9.43 ± 3.36, P=0.25); however, the difference in scores was not statistically significant. Surprisingly, we found lower scores during the pandemic than in a previous study conducted at our center [31]. Additionally, a study by Huang et al. reported that patients with EQUAL scores above 10 had a significantly higher survival rate compared to those with scores less than 10[23]. Our findings demonstrated mean scores of 9.92 and 10.36 in survivors in the overall population and CVC carriers, respectively. These results suggest a lower adherence to management guidelines during the pandemic, which may be related to the high mortality rate observed in the overall pandemic population compared to the pre-pandemic period.
In contrast to our previous study [31], echocardiography and performing susceptibility testing were not found to be associated with lower mortality. However, ophthalmic exam, when performed, improved survival rates in our population. Although a recent systematic review suggested that universal ophthalmological examination does not improve outcomes [32], the Infectious Diseases Society of America (IDSA) and the European Confederation of Medical Mycology (ECMM) guidelines both recommend that all patients with candidemia should undergo routine dilated funduscopic exam [27,33]. These recommendations were supported by a recent meta-analysis by Phongkhun et al, which found that ocular manifestations in patients with candidemia were more common than previously reported by the American Academy of Ophthalmology (AAO) which suggested an incidence of less than 0.9% [34]. These discrepancies emphasize that further studies are needed to identify high-risk patients that would benefit the most from this intervention. Furthermore, the removal of CVCs within the first 48h of candidemia was found to be associated with higher survival rates. In fact, all guidelines recommend the removal of CVCs in patients with candidemia as a source control measure [33,35,36], however, there is no clear evidence supporting early removal of CVCs (prior to 48h post infection) [23,31,37].
In concordance with the IDSA recommendations [27] and previous studies [38], treatment with at least 14 days after the first negative blood culture was associated with higher survival rate. Another notable result of our study is that the majority of our patients with CAC had died before receiving the appropriate duration of antifungal treatment. These results may be due to a delay in the diagnosis of candidemia, especially in the early phases of COVID-19. However, it is very difficult to determine in those patients whether the cause of death was related to the COVID-19 respiratory complications versus the candidemia.
The 30-day mortality rate in the overall population reached 76.6%. Many studies from the pre-pandemic era showed a lower mortality rate of patients with candidemia ranging from 19% to 38% in European and American studies [39,40], 55.5% in our center [18], and 54% in ICU patients with candidemia from Japan [41]. Higher mortality rates found during the pandemic could be due to many factors including the emergence of the highly resistant C. auris during the pandemic period and the near collapse of healthcare systems. In addition, Lebanon experienced an economic collapse in 2019 that coincided with the COVID-19 pandemic and resulted in the exodus of health care workers. This added a significant strain on hospitals including our facility where a large number of employees were laid off. Junior staff including physicians and nurses were recruited which could have contributed to the delay in the identification and the proper management of patients with candidemia and the lack of adherence to proper infection control practices. Many studies showed a high mortality rate in patients with C. auris candidemia [42], reaching 75% in a recent study from our center [6]. Additionally, as discussed before, the adherence to guidelines in the management of candidemia was lower during the pandemic which could have predisposed to the higher mortality rate. Surprisingly, no statistical difference was found when comparing mortality between CAC and non-CAC, in contrast to other published studies [8,43]. It is possible that, with an overall mortality rate of 76.6%, it is difficult to distinguish candidemia attributable mortality from death caused by underlying diseases. Previous studies have suggested that the mortality attributed to candidemia is not significant in a population of patients with high expected mortality [44].
In this study, it was found that 80% of patients with CAC were admitted to the ICU, with a median time from ICU admission to candidemia of 17.5 days. This is consistent with previous reports demonstrating that prolonged ICU stay, regardless of COVID-19 status, can increase the risk of developing candidemia [45] and confirms that the majority of our CAC cases are healthcare-associated. Critically ill COVID-19 patients have been shown to require an average of 20.6 days of ICU admission, further increasing their predisposition to invasive candidiasis [46]. On the other hand, the median time from COVID-19 infection to the development of candidemia in our population was 24 days. Candidemia seems to occur during the second phase of COVID-19 infection which typically starts after one week of the onset of illness and is characterized by excessive inflammation [47] during which the patients often require steroids and immunomodulatory therapies such as tocilizumab [48], which further increase the risk of invasive fungal infections [45]. These findings highlight the importance of close monitoring and early detection of fungal infections in COVID-19 patients, particularly during the second phase of the COVID-19 infection.
Our study has some limitations. First, it is a retrospective single-center study that may not accurately represent the national epidemiology of candidemia. Second, because all included patients had candidemia, we lacked a comparator group of patients with COVID-19 without candidemia, limiting our assessment of COVID-19 as an independent risk factor for candidemia. We also could not clearly investigate the association between different COVID-19 treatment modalities, especially tocilizumab and CAC due to the small sample size. In addition, the management of COVID-19 was constantly evolving during the two years of the pandemic, which has led to different treatment protocols over time and may have contributed to improved outcomes.
5. Conclusion
Candidemia is associated with high morbidity and mortality even when treated adequately. The epidemiology of Candida spp. has significantly shifted during the COVID-19 pandemic with the emergence of highly resistant spp. including C. auris. This shift is alarming as it significantly impacts the management and outcomes of patients. Rigorous infection control practices in combination with antifungal stewardship are essential to contain institutional outbreaks of highly resistant Candida spp. but also to decrease the emergence of future resistance. Institutional epidemiological data is vital to optimize choices of agents for empirical antifungal therapy.
Author Contributions
Conceptualization: AEZ, SSK, Data collection: OM, JZ, SN, NEG, NO Formal Analysis: WES, HT, Writing – review and editing: OM, JZ, SN, Writing –original draft: OM, JZ, SN, Methodology: AEZ, SSK, Supervision: AEZ, SSK. All authors have read and approved the final version of the manuscript and SSK as corresponding author had full access to all of the data in this study and takes complete responsibility for the integrity of the data and the accuracy of the data analysis.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Conflicts of Interest
Declare conflicts of interest or state “The authors declare no conflict of interest.” Authors must identify and declare any personal circumstances or interest that may be perceived as inappropriately influencing the representation or interpretation of reported research results. Any role of the funders in the design of the study; in the collection, analyses or interpretation of data; in the writing of the manuscript, or in the decision to publish the results must be declared in this section. If there is no role, please state “The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results”.
References
- Wisplinghoff, H.; Bischoff, T.; Tallent, S.M.; Seifert, H.; Wenzel, R.P.; Edmond, M.B. Nosocomial Bloodstream Infections in US Hospitals: Analysis of 24,179 Cases from a Prospective Nationwide Surveillance Study. Clin. Infect. Dis. 2004, 39, 309–317. [Google Scholar] [CrossRef]
- Paiva, J.-A.; Pereira, J.M.; Tabah, A.; Mikstacki, A.; de Carvalho, F.B.; Koulenti, D.; Ruckly, S.; Çakar, N.; Misset, B.; Dimopoulos, G.; et al. Characteristics and risk factors for 28-day mortality of hospital acquired fungemias in ICUs: data from the EUROBACT study. Crit. Care 2016, 20, 1–13. [Google Scholar] [CrossRef] [PubMed]
- Kmeid, J.; Jabbour, J.-F.; Kanj, S.S. Epidemiology and burden of invasive fungal infections in the countries of the Arab League. J. Infect. Public Heal. 2019, 13, 2080–2086. [Google Scholar] [CrossRef] [PubMed]
- Zakhem, A.E., et al., Predominance of Candida glabrata among non-albicans Candida species in a 16-year study of candidemia at a tertiary care center in Lebanon. Pathogens, 2021. 10(1): p. 82. [CrossRef]
- Silva, L.N.; de Mello, T.P.; Ramos, L.d.S.; Branquinha, M.H.; Roudbary, M.; dos Santos, A.L.S. Fungal Infections in COVID-19-Positive Patients: A Lack of Optimal Treatment Options. Curr. Top. Med. Chem. 2020, 20, 1951–1957. [Google Scholar] [CrossRef]
- Allaw, F.; Haddad, S.F.; Habib, N.; Moukarzel, P.; Naji, N.S.; Kanafani, Z.A.; Ibrahim, A.; Zahreddine, N.K.; Spernovasilis, N.; Poulakou, G. COVID-19 and C. auris: A Case-Control Study from a Tertiary Care Center in Lebanon. Microorganisms 2022, 10, 1011. [Google Scholar] [CrossRef]
- Arastehfar, A.; Shaban, T.; Zarrinfar, H.; Roudbary, M.; Ghazanfari, M.; Hedayati, M.-T.; Sedaghat, A.; Ilkit, M.; Najafzadeh, M.J.; Perlin, D.S. Candidemia among Iranian Patients with Severe COVID-19 Admitted to ICUs. J. Fungi 2021, 7, 280. [Google Scholar] [CrossRef]
- Omrani, A.S.; Koleri, J.; Ben Abid, F.; Daghfel, J.; Odaippurath, T.; Peediyakkal, M.Z.; Baiou, A.; Sarsak, E.; Elayana, M.; Kaleeckal, A.; et al. Clinical characteristics and risk factors for COVID-19-associated Candidemia. Med Mycol. 2021, 59, 1262–1266. [Google Scholar] [CrossRef]
- Kayaaslan, B.; Eser, F.; Kaya Kalem, A.; Bilgic, Z.; Asilturk, D.; Hasanoglu, I.; Ayhan, M.; Tezer Tekce, Y.; Erdem, D.; Turan, S. Characteristics of candidemia in COVID-19 patients; increased incidence, earlier occurrence and higher mortality rates compared to non-COVID-19 patients. Mycoses 2021, 64, 1083–1091. [Google Scholar] [CrossRef]
- Casalini, G.; Giacomelli, A.; Ridolfo, A.; Gervasoni, C.; Antinori, S. Invasive Fungal Infections Complicating COVID-19: A Narrative Review. J. Fungi 2021, 7, 921. [Google Scholar] [CrossRef]
- Avkan-Oğuz, V.; Çelİk, M.; Eren-Kutsoylu, O.Ö.; Nazli, A.; Uğur, Y.L.; Taylan, A.; Ergan, B.; Irmak, Ç.; Duğral, E.; Özkütük, A.A. Fungal colonization and infections in patients with COVID-19 in intensive care units: A real-life experience at a tertiary-care hospital. Respiratory Medicine and Research 2022, 82, 100937. [Google Scholar] [CrossRef]
- Routsi, C.; Meletiadis, J.; Charitidou, E.; Gkoufa, A.; Kokkoris, S.; Karageorgiou, S.; Giannopoulos, C.; Koulenti, D.; Andrikogiannopoulos, P.; Perivolioti, E.; et al. Epidemiology of Candidemia and Fluconazole Resistance in an ICU before and during the COVID-19 Pandemic Era. Antibiotics 2022, 11, 771. [Google Scholar] [CrossRef]
- Boxer, L.A. How to approach neutropenia. Hematology 2010, the American Society of Hematology Education Program Book 2012, 2012, 174–182. [Google Scholar] [CrossRef]
- CLSI, C. Performance standards for antimicrobial susceptibility testing. Clinical Lab Standards Institute 2016, 35, 16–38. [Google Scholar]
- CDC, N. Bloodstream infection event (central line-associated bloodstream infection and non-central line-associated bloodstream infection). Center for Disease Control Atlanta, GA: 2017.
- Berbari, E.F.; Kanj, S.S.; Kowalski, T.J.; Darouiche, R.O.; Widmer, A.F.; Schmitt, S.K.; Hendershot, E.F.; Holtom, P.D.; Huddleston, P.M.; Petermann, G.W. 2015 infectious diseases society of America (IDSA) clinical practice guidelines for the diagnosis and treatment of native vertebral osteomyelitis in adultsa. Clinical infectious diseases 2015, 61, e26–e46. [Google Scholar] [CrossRef]
- Ghazi, S.; Rafei, R.; Osman, M.; El Safadi, D.; Mallat, H.; Papon, N.; Dabboussi, F.; Bouchara, J.-P.; Hamze, M. Ghazi, S.; Rafei, R.; Osman, M.; El Safadi, D.; Mallat, H.; Papon, N.; Dabboussi, F.; Bouchara, J.-P.; Hamze, M. The epidemiology of Candida species in the Middle East and North Africa. 2019, 29, 245–252. [CrossRef]
- Zahreddine, N.K.; Haddad, S.F.; Kerbage, A.; Kanj, S.S. Challenges of coronavirus disease 2019 (COVID-19) in Lebanon in the midst of the economic collapse. Antimicrob. Steward. Heal. Epidemiology 2022, 2, e67. [Google Scholar] [CrossRef]
- Allaw, F.; Zahreddine, N.K.; Ibrahim, A.; Tannous, J.; Taleb, H.; Bizri, A.R.; Dbaibo, G.; Kanj, S.S. First Candida auris Outbreak during a COVID-19 Pandemic in a Tertiary-Care Center in Lebanon. Pathogens 2021, 10, 157. [Google Scholar] [CrossRef]
- Escandón, P.; Chow, N.A.; Caceres, D.H.; Gade, L.; Berkow, E.L.; Armstrong, P.; Rivera, S.; Misas, E.; Duarte, C.; Moulton-Meissner, H.; et al. Molecular Epidemiology of Candida auris in Colombia Reveals a Highly Related, Countrywide Colonization With Regional Patterns in Amphotericin B Resistance. Clin. Infect. Dis. 2018, 68, 15–21. [Google Scholar] [CrossRef]
- Machado, M.; Estévez, A.; Sánchez-Carrillo, C.; Guinea, J.; Escribano, P.; Alonso, R.; Valerio, M.; Padilla, B.; Bouza, E.; Muñoz, P. Incidence of Candidemia Is Higher in COVID-19 versus Non-COVID-19 Patients, but Not Driven by Intrahospital Transmission. J. Fungi 2022, 8, 305. [Google Scholar] [CrossRef] [PubMed]
- Tsay, S.; Welsh, R.M.; Adams, E.H.; Chow, N.A.; Gade, L.; Berkow, E.L.; Poirot, E.; Lutterloh, E.; Quinn, M.; Chaturvedi, S. Notes from the field: ongoing transmission of Candida auris in health care facilities—United States, June 2016–May 2017. Morbidity and Mortality Weekly Report 2017, 66, 514. [Google Scholar] [CrossRef] [PubMed]
- Huang, H.-Y.; Lu, P.-L.; Wang, Y.-L.; Chen, T.-C.; Chang, K.; Lin, S.-Y. Usefulness of EQUAL Candida Score for predicting outcomes in patients with candidaemia: a retrospective cohort study. Clin. Microbiol. Infect. 2020, 26, 1501–1506. [Google Scholar] [CrossRef] [PubMed]
- Rahme, D.; Ayoub, M.; Shaito, K.; Saleh, N.; Assaf, S.; Lahoud, N. First trend analysis of antifungals consumption in Lebanon using the World Health Organization collaborating center for drug statistics methodology. BMC Infect. Dis. 2022, 22, 1–9. [Google Scholar] [CrossRef]
- Khan, Z.; Ahmad, S.; Al-Sweih, N.; Mokaddas, E.; Al-Banwan, K.; Alfouzan, W.; Al-Obaid, I.; Al-Obaid, K.; Varghese, S. Increasing Trends of Reduced Susceptibility to Antifungal Drugs Among ClinicalCandida glabrataIsolates in Kuwait. Microb. Drug Resist. 2020, 26, 982–990. [Google Scholar] [CrossRef]
- Habibzadeh, A.; Lankarani, K.B.; Farjam, M.; Akbari, M.; Kashani, S.M.A.; Karimimoghadam, Z.; Wang, K.; Imanieh, M.H.; Tabrizi, R.; Ahmadizar, F. Prevalence of Fungal Drug Resistance in COVID-19 Infection: a Global Meta-analysis. Curr. Fungal Infect. Rep. 2022, 16, 154–164. [Google Scholar] [CrossRef]
- Pappas, P.G.; Kauffman, C.A.; Andes, D.R.; Clancy, C.J.; Marr, K.A.; Ostrosky-Zeichner, L.; Reboli, A.C.; Schuster, M.G.; Vazquez, J.A.; Walsh, T.J. Clinical practice guideline for the management of candidiasis: 2016 update by the Infectious Diseases Society of America. Clinical Infectious Diseases 2016, 62, e1–e50. [Google Scholar] [CrossRef]
- Rizk, N.A.; Moghnieh, R.; Haddad, N.; Rebeiz, M.-C.; Zeenny, R.M.; Hindy, J.-R.; Orlando, G.; Kanj, S.S. Challenges to Antimicrobial Stewardship in the Countries of the Arab League: Concerns of Worsening Resistance during the COVID-19 Pandemic and Proposed Solutions. Antibiotics 2021, 10, 1320. [Google Scholar] [CrossRef]
- McEwen, S.A.; Collignon, P.J. Antimicrobial resistance: a one health perspective. Antimicrobial resistance in bacteria from livestock and companion animals 2018, 521–547. [Google Scholar] [CrossRef]
- Kanj, S.S.; Ramirez, P.; Rodrigues, C. Beyond the Pandemic: The Value of Antimicrobial Stewardship. Front. Public Heal. 2022, 10, 902835. [Google Scholar] [CrossRef]
- El Zakhem, A.; El Eid, R.; Istambouli, R.; Tamim, H.; Kanj, S.S. The Utility of EQUAL Candida Score in Predicting Mortality in Patients with Candidemia. J. Fungi 2022, 8, 238. [Google Scholar] [CrossRef]
- Breazzano, M.P.; Day, H.R.; Bloch, K.C.; Tanaka, S.; Cherney, E.F.; Sternberg, P.; Donahue, S.P.; Bond, J.B. Utility of ophthalmologic screening for patients with Candida bloodstream infections: a systematic review. JAMA ophthalmology 2019, 137, 698–710. [Google Scholar] [CrossRef] [PubMed]
- Cornely, O.; Bassetti, M.; Calandra, T.; Garbino, J.; Kullberg, B.; Lortholary, O.; Meersseman, W.; Akova, M.; Arendrup, M.; Arikan-Akdagli, S. ESCMID* guideline for the diagnosis and management of Candida diseases 2012: non-neutropenic adult patients. Clinical Microbiology and Infection 2012, 18, 19–37. [Google Scholar] [CrossRef] [PubMed]
- Phongkhun, K.; Pothikamjorn, T.; Srisurapanont, K.; Manothummetha, K.; Sanguankeo, A.; Thongkam, A.; Chuleerarux, N.; Leksuwankun, S.; Meejun, T.; Thanakitcharu, J.; et al. Prevalence of Ocular Candidiasis and Candida Endophthalmitis in Patients With Candidemia: A Systematic Review and Meta-Analysis. Clin. Infect. Dis. 2023, 76, 1738–1749. [Google Scholar] [CrossRef] [PubMed]
- Andes, D.R.; Safdar, N.; Baddley, J.W.; Playford, G.; Reboli, A.C.; Rex, J.H.; Sobel, J.D.; Pappas, P.G.; Kullberg, B.J. Impact of Treatment Strategy on Outcomes in Patients with Candidemia and Other Forms of Invasive Candidiasis: A Patient-Level Quantitative Review of Randomized Trials. Clin. Infect. Dis. 2012, 54, 1110–1122. [Google Scholar] [CrossRef] [PubMed]
- Deshpande, A.; Gaur, S.; Bal, A. Candidaemia in the non-neutropenic patient: A critique of the guidelines. Int. J. Antimicrob. Agents 2013, 42, 294–300. [Google Scholar] [CrossRef]
- Nucci, M.; Braga, P.R.; Nouér, S.A.; Anaissie, E. Time of catheter removal in candidemia and mortality. Braz. J. Infect. Dis. 2018, 22, 455–461. [Google Scholar] [CrossRef]
- Ashong, C.N.; Hunter, A.S.; Mansouri, M.D.; Cadle, R.M.; Hamill, R.J.; Musher, D.M. Adherence to clinical practice guidelines for the treatment of candidemia at a Veterans Affairs Medical Center. 2017, 11, 18–23.
- Koehler, P.; Stecher, M.; Cornely, O.; Vehreschild, M.; Bohlius, J.; Wisplinghoff, H.; Vehreschild, J. Morbidity and mortality of candidaemia in Europe: an epidemiologic meta-analysis. Clin. Microbiol. Infect. 2019, 25, 1200–1212. [Google Scholar] [CrossRef]
- Morgan, J.; Meltzer, M.I.; Plikaytis, B.D.; Sofair, A.N.; Huie-White, S.; Wilcox, S.; Harrison, L.H.; Seaberg, E.C.; Hajjeh, R.A.; Teutsch, S.M. Excess Mortality, Hospital Stay, and Cost Due to Candidemia: A Case-Control Study Using Data From Population-Based Candidemia Surveillance. Infect. Control. Hosp. Epidemiology 2005, 26, 540–547. [Google Scholar] [CrossRef]
- Ohki, S.; Shime, N.; Kosaka, T.; Fujita, N. Impact of host- and early treatment-related factors on mortality in ICU patients with candidemia: a bicentric retrospective observational study. J. Intensiv. Care 2020, 8, 30. [Google Scholar] [CrossRef] [PubMed]
- Osei Sekyere, J. Candida auris: A systematic review and meta-analysis of current updates on an emerging multidrug-resistant pathogen. Microbiologyopen 2018, 7, e00578. [Google Scholar] [CrossRef] [PubMed]
- E Seagle, E.; Jackson, B.R.; Lockhart, S.R.; Georgacopoulos, O.; Nunnally, N.S.; Roland, J.; Barter, D.M.; Johnston, H.L.; A Czaja, C.; Kayalioglu, H.; et al. The Landscape of Candidemia During the Coronavirus Disease 2019 (COVID-19) Pandemic. Clin. Infect. Dis. 2021, 74, 802–811. [Google Scholar] [CrossRef] [PubMed]
- I Blot, S.; Vandewoude, K.H.; A Hoste, E.; A Colardyn, F. Effects of nosocomial candidemia on outcomes of critically ill patients. Am. J. Med. 2002, 113, 480–485. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Z.; Zhu, R.; Luan, Z.; Ma, X. Risk of invasive candidiasis with prolonged duration of ICU stay: a systematic review and meta-analysis. BMJ Open 2020, 10, e036452. [Google Scholar] [CrossRef]
- Dongelmans, D.A.; Termorshuizen, F.; Brinkman, S.; Bakhshi-Raiez, F.; Arbous, M.S.; de Lange, D.W.; van Bussel, B.C.T.; de Keizer, N.F.; Verbiest, D.P.; Velde, L.F.T.; et al. Characteristics and outcome of COVID-19 patients admitted to the ICU: a nationwide cohort study on the comparison between the first and the consecutive upsurges of the second wave of the COVID-19 pandemic in the Netherlands. Ann. Intensiv. Care 2022, 12, 1–10. [Google Scholar] [CrossRef]
- Acosta, R.A.H.; Garrigos, Z.E.; Marcelin, J.R.; Vijayvargiya, P. COVID-19 Pathogenesis and Clinical Manifestations. Infect. Dis. Clin. North Am. 2022, 36, 231–249. [Google Scholar] [CrossRef]
- Alkofide, H.; Almohaizeie, A.; Almuhaini, S.; Alotaibi, B.; Alkharfy, K.M. Tocilizumab and Systemic Corticosteroids in the Management of Patients with COVID-19: A Systematic Review and Meta-Analysis. Int. J. Infect. Dis. 2021, 110, 320–329. [Google Scholar] [CrossRef]

Table 1.
Evolution of Candida spp. susceptibility in the number of tested isolates over 18 years at AUBMC.
Table 1.
Evolution of Candida spp. susceptibility in the number of tested isolates over 18 years at AUBMC.
| 2004-2008 | 2009-2013 | 2014-2019 | 2020-2022 (non-CAC) | 2020-2022 (CAC) | Total | |
|---|---|---|---|---|---|---|
| C. albicans | ||||||
| Fluconazole | 1/1 | 6/6 | 13/16 | 5/5 | 8/8 | 33/36 |
| Voriconazole | - | 3/4 | 14/17 | 5/5 | 8/8 | 30/34 |
| Amphotericin B | - | 3/3 | 17/17 | 5/5 | 8/8 | 33/33 |
| Caspofungin | - | 1/1 | 6/6 | 5/5 | 8/8 | 20/20 |
| C. tropicalis | ||||||
| Fluconazole | 2/2 | - | 3/3 | - | 1/1 | 6/6 |
| Voriconazole | - | 4/5 | 7/7 | 1/1 | 2/2 | 14/15 |
| Amphotericin B | - | 1/1 | 7/7 | 1/1 | 2/2 | 11/11 |
| Caspofungin | - | 1/1 | 1/1 | 1/1 | 2/2 | 5/5 |
| C. glabrata | ||||||
| Fluconazole | 3/4 | 3/10 | 17/23 | 2/6 | 4/7 | 29/50 |
| Voriconazole | 0/1 | 7/8 | 18/23 | 6/6 | 7/7 | 38/45 |
| Amphotericin B | - | 1/1 | 22/23 | 6/6 | 6/6 | 35/36 |
| Caspofungin | - | - | 9/9 | 3/6 | 2/7 | 14/22 |
| C. parapsilosis | ||||||
| Fluconazole | 2/2 | - | 3/3 | - | 1/1 | 6/6 |
| Voriconazole | - | - | 3/3 | - | 1/1 | 4/4 |
| Amphotericin B | - | - | 3/3 | - | 1/1 | 4/4 |
| Caspofungin | - | - | - | - | 1/1 | 1/1 |
| C. auris | ||||||
| Fluconazole | - | - | - | 0/3 | 2/9 | 2/12 |
| Voriconazole | - | - | - | 1/3 | 5/9 | 6/12 |
| Amphotericin B | - | - | - | 0/3 | 0/7 | 0/10 |
| Caspofungin | - | - | - | 8/8 | 3/3 | 11/11 |
Table 2.
Characteristics of episodes of CAC and non-CAC in critically ill patients. ESRD, end-stage renal disease; HD, hemodialysis; AKI, acute kidney injury; CVC, central venous catheter; CLABSI, central line associated bloodstream infection; UTI, urinary tract infection; GI, gastrointestinal.
Table 2.
Characteristics of episodes of CAC and non-CAC in critically ill patients. ESRD, end-stage renal disease; HD, hemodialysis; AKI, acute kidney injury; CVC, central venous catheter; CLABSI, central line associated bloodstream infection; UTI, urinary tract infection; GI, gastrointestinal.
| Total N = 64 |
CAC N = 32 (50.0%) |
Non-CAC N = 32 (50.0%) |
p-value | |
|---|---|---|---|---|
| Age* | 73 (19) | 75 (18) | 72 (18) | 0.14 |
| Male | 38 (59.4%) | 20 (62.5%) | 18 (56.3%) | 0.61 |
| Diabetes mellitus | 29 (45.3%) | 18 (56.3%) | 11 (34.4%) | 0.07 |
| ESRD on HD | 26 (40.6%) | 12 (37.5%) | 14 (43.8%) | 0.61 |
| AKI requiring HD | 2 (3.1%) | 1 (3.1%) | 1 (3.1%) | 1.00 |
| Hematologic malignancy | 8 (12.5%) | 5 (15.6%) | 3 (9.4%) | 0.70 |
| Solid organ malignancy | 16 (25.0%) | 5 (15.6%) | 11 (34.4%) | 0.08 |
| Recent chemotherapy | 14 (22.2%) | 4 (12.5%) | 10 (32.3%) | 0.05 |
| Recent immunotherapy | 4 (6.3%) | 2 (6.3%) | 2 (6.3%) | 1.00 |
| Neutropenia | 4 (6.3%) | 1 (3.1%) | 3 (9.4%) | 0.61 |
| Recent abdominal surgery** | 6 (9.4%) | 2 (6.3%) | 4 (12.5%) | 0.67 |
| Recent antibiotics** | 62 (96.9%) | 30 (93.8%) | 32 (100.0%) | 0.49 |
| Recent antifungals** | 22 (34.4%) | 12 (37.5%) | 10 (31.3%) | 0.59 |
| Mechanical ventilation | 49 (76.6%) | 26 (81.3%) | 23 (71.9%) | 0.37 |
| CVC | 55 (85.9%) | 27 (84.4%) | 28 (87.5%) | 1.00 |
| Persistent candidemia | 10 (24.4%) | 3 (15.8%) | 7 (31.8%) | 0.29 |
| Source of candidemia CLABSI UTI GI tract Unknown Others*** |
18 (28.1%) 20 (31.3%) 14 (21.9%) 15 (23.4%) 11 (17.5%) |
8 (25.0%) 12 (37.5%) 6 (18.8%) 9 (28.1%) 4 (12.9%) |
10 (31.2%) 8 (25.0%) 8 (25.0%) 6 (18.8%) 7 (21.9%) |
0.57 0.28 0.54 0.37 0.34 |
| Species C. albicans C. auris NAC other than C. auris |
17 (26.6%) 19 (29.7%) 28 (43.8%) |
9 (28.1%) 9 (28.1%) 14 (43.8%) |
8 (25.1%) 10 (31.3%) 14 (43.8%) |
0.94 |
* Median (IQR); **30 days prior to candidemia.
Table 3.
Management and outcomes of CAC and non-CAC episodes in critically-ill patients.
| Total N = 64 |
CAC N = 32 (50.0%) |
Non-CAC N = 32 (50.0%) |
p-value | |
|---|---|---|---|---|
| Speciation | 51 (79.7%) | 26 (81.3%) | 25 (78.1%) | 0.75 |
| Susceptibility testing | 28 (48.3%) | 15 (51.7%) | 13 (44.8%) | 0.59 |
| Echocardiography | 15 (24.2%) | 9 (29.0%) | 6 (19.4%) | 0.37 |
| Ophthalmic examination | 11 (17.5%) | 5 (15.6%) | 6 (19.4%) | 0.69 |
| Empiric antifungal agent | ||||
| Fluconazole | 3 (5.1%) | 2 (6.7%) | 1 (3.4%) | 1.00 |
| Caspofungin | 36 (61.0%) | 25 (83.3%) | 11 (37.9%) | <0.001 |
| Anidulafungin | 14 (23.7%) | 5 (16.7%) | 9 (31.0%) | 0.19 |
| Micafungin | 1 (1.7%) | 0 (0.0%) | 1 (3.4%) | 0.49 |
| Lipid formulation of Amphotericin B | 5 (8.5%) | 1 (3.3%) | 4 (13.8%) | 0.19 |
| Voriconazole | 7 (11.9%) | 3 (10.0%) | 4 (13.8%) | 0.71 |
| Targeted antifungal agent |
0.054 |
|||
| Fluconazole | 44 (47.3%) | 3 (23.1%) | 41 (51.2%) | |
| Voriconazole | 14 (15.1%) | 3 (23.1%) | 11 (13.8%) | |
| Caspofungin | 13 (14%) | 2 (15.4%) | 11 (13.8%) | |
| Anidulafungin | 10 (10.8%) | 4 (30.8%) | 6 (7.5%) | |
| Micafungin | 4 (4.3%) | 1 (7.7%) | 3 (3.8%) | |
| Lipid formulation of Amphotericin B | 8 (8.6%) | 0 (0.0%) | 8 (10.0%) | |
| Empirical echinocandin | 48 (81.4%) | 28 (93.3%) | 20 (69.0%) | 0.016 |
| Step-down to fluconazole | 4 (7.1%) | 1 (3.3%) | 3 (11.5%) | 0.32 |
| Daily blood culture until negative | 2 (4.2%) | 1 (4.2%) | 1 (4.2%) | 1.00 |
| Completed 14 days of antifungals | 9 (17.0%) | 4 (14.8%) | 5 (19.2%) | 0.72 |
| 30-day mortality | 49 (76.6%) | 24 (75.0%) | 25 (78.1%) | 0.76 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



