
Submitted:
10 May 2023
Posted:
11 May 2023
You are already at the latest version
Abstract
Shoulder pain is a serious clinical disease frequently related to absence from work. It’s characterized by pain and stiffness probably connected to the presence of an inflammatory substrate involving gleno-humeral capsule and collagen tissues. A physioterapy programme has shown to be effective for the conservative treatment of this disorder. Our aim is to assess if a manual treatment directed to fascial tissues could get better improvement regarding pain, strength, mobility and function. 94 healthcare workers with recurrent shoulder pain were recruited and then randomized in two groups: the control group (CG) underwent a physiotherapy programme; the study group (SG) underwent to 3 sessions of physiotherapy and to 2 session of Fascial Manipulation (FM) technique. At the end of the treatment phase, both groups improved every outcome. Despite few statistical differences between groups, at the follow up visit a greater percentage of subjects in SG overcame the minimal clinical important difference (MCID) in every outcome. We conclude that FM is effective for treatment of shoulder pain and further studies should better assess how to manage this treatment to get better results.
Keywords:
shoulder pain
; physiotherapy programme
; fascial manipulation
; MCID (minimal clinical important difference)
1. Introduction
Shoulder pain is an important clinical and socio-economic problem: shoulder pain and stiffness can lead to disability that affects both the working and social spheres of the individual’s life.
A feature of this clinical condition highlighted by the literature is its persistence, which involves the subjects for a very long time, influencing their activities for up to a year [1].
Analysing the literature, we find that shoulder pain, like back pain, often affects healthcare professionals and is one of the most frequent causes of absence from work, highlighting that posture-related factors or highly repetitive activities, with flexion or abduction greater than 60 degrees, are associated with this disorder.
Moreover, a causal relationship has been found between vigorous efforts, high level of static contractions, prolonged static loads and extreme postures, as well as combinations of these factors [2].
Other causes of shoulder pain may be related to: intrinsic glenohumeral joint disease, pathology in the periarticular tissues, dysfunctions related to spine and thoracic structures, or visceral dysfunctions that cause referred pain.
The clinical diagnosis of “shoulder pain” is carried out through the anamnesis, considering the type and distribution of pain, and through physical examination [3].
Chronicisation of this condition is common, especially when radiological investigations do not show structural lesions; it often establishes progressively causing functional limitations, even severe in the activities of daily life [4].
The chronicity of a painful shoulder often results in a frozen shoulder, a clinical condition that has a prevalence of 2-5% in the general population.
Many studies indicate that the onset of this pathology is due to the presence of an inflammatory substrate involving the shoulder joint capsule. This is associated with increased amounts of collagen, fibrotic growth factors such as transforming growth factor beta, and inflammatory cytokines and interleukins [5].
This histological condition causes pain and consequent immobility which, in the process of becoming chronic, is further aggravated by the very fear of pain which leads the person to further reduce their activities.
This mechanism is explained very well by the fear– avoidance model (FAM - “avoidance of movement for fear of musculoskeletal pain”), which is proposed to describe the interaction between psychological characteristics such as fear of pain and worsening of the functional activities with development of chronic musculoskeletal pain and disability [6].
Many treatments are proposed in the literature for shoulder pain; their main common goals is to restore and maintain function. Physiotherapy treatment is always present in every study.
Consequently, to define the specific physiotherapy strategy is the primary objective to prevent the aggravation of the clinical picture.
Biomedical database research has shown good levels of evidence for a program of stretching and selective strengthening exercises to positively affect the development of shoulder pain [7,8,9].
Stretching exercises are intended to prevent aggravation of joint limitation and promote a faster return to normal range; selective active exercises aim at maintaining and improving the strength of the shoulder girdle.
It is possible to start this activity by proposing isometric work within the pain-free range, for example by promoting the use of an elastic band that provides gradually increasing resistance as the range of motion increases [10].
The literature then confirmed how in consideration of the involvement of the articular and periarticular collagenous tissues and the close continuity between these and the fascia of the muscular elements involved in this clinical condition, manual treatments aimed at restoring the best functionality of the muscular fascia can affect the recovery function of the painful shoulder [11,13].
Based on these considerations, we hypothesized a clinical trial that, in addition to these physiotherapy proposals, also includes a manual treatment aimed at the peri-articular soft tissues involved in the chronicisation of pain.
2. Materials and Methods
2.1. Design of the Study
One of the objectives of our study is to highlight the importance of physiotherapy intervention for subjects suffering from chronic shoulder pain, through the administration of a targeted and continuous program of exercises to improve: pain symptoms, ROM (Range of Movement), muscle recruitment, function and quality of life in these people.
A manual technique that provides a rationale for treating specific areas of fascia is fascial manipulation® (FM).
To choose where muscular fascia needs to be treated, FM uses a twofold analysis: at first a movement verification (MoVe), and for second a palpatory verification (PaVe). MoVe is carried out with provocative tests in the involved segments in all directions along the three planes (sagittal, frontal and horizontal); PaVe is an assessment of the fascial gliding into specific fascial areas; it’s carried out with manual friction on the deep fascia: positive points are characterized by resistance in manual friction: these points are usually described as densified.
In this way the altered fascial areas are highlighted and defined by the technique as Centres of Coordination (CC) and Centres of Fusion (CF), which are potentially the site of dysfunction. The treatment consists of a manual deep friction intervention capable of heating the fascial tissues and fluidifying the sliding of the fascial planes of the deep fascia.
The mechanical and chemical effects of the FM manual treatment due to the deep manual friction and the subsequent local inflammatory tissue response, maybe able to influence the extra cellular matrix (ECM) components of the deep fascia in CC and CF areas, restoring its normal sliding and tensioning [12].
Due to the body-wide fascial tissue continuity, when stimulating a CC or a CF we can improve tensional adaptation also in segments far from the treated areas, restoring a global tensional physiological balance.
The anatomical studies named these myofascial continuities as: sequences, diagonals or spirals. They are not only a functional concept but have an anatomical substratum of fascial continuity and muscular expansions on the fascia itself [13].
Considering both the clinical involvement of the connective tissues for the onset of shoulder pain and the effectiveness of FM for the treatment of different myofascial dysfunctions, we want to verify if this manual fascial treatment in association with a physiotherapy programme could better improve shoulder pain in comparison with a physiotherapy programme alone; its will be made up of the best evidence in the literature regarding treatments for shoulder pain [14,15,16,17].
We designed a randomised, single-blind, controlled clinical trial in which the study sample was divided into two groups.
We decided to recruit the population of this study among the employees of a healthcare centre in Bergamo (ASST Bergamo Est), knowing that healthcare workers' activity is often related to recurrent pathologies of the upper limbs and the assistance activity itself can represent a chronicisation factor for pathologies affecting the scapula-humeral system [18].
The sample recruitment was carried out with an initial awareness-raising process that took place through a preliminary survey made by a questionnaire addressed to all the healthcare workers of the ASST Bergamo Est.
Interested volunteers could then contact the physiatrist in charge of evaluating the inclusion and exclusion criteria settled in the protocol for possible enrolment in research protocol [19].
We settled these inclusion criteria: age between 30 and 60 years, shoulder pain present for at least three months with 2 or more points to NRS scale, clinical positivity to at least two clinical tests among: Jobe, Neer and Hawkins.
The exclusion criteria were as follows: positive imaging (US or MRI) of a structural lesion of the glenohumeral joint; positive anamnesis of rheumatic, oncological, neurological and psychiatric diseases; previous fractures and/or trauma related to scapulohumeral girdle or cervical spine.
The subjects included in the study were divided into a Control Group (CG) and a Study Group (SG); the division into the two groups was carried out by an operator [PTA] through a computerized randomisation system using the Microsoft excel software [20].
The study was approved by the Provincial Ethics Committee of Bergamo, registration no. 697 dated 08/10/2016, clinicaltrials.gov identifier: NCT03041727.
The work protocol included a common path for CG and SG carried out in five weekly sessions, and a final follow-up session one month after the fifth appointment.
The sessions were conducted in groups of three; each group was supervised by a physiotherapist [PT B], experienced and trained in teaching the execution of the exercise protocol; each group involved GS or GC subjects separately.
In each session, all subjects were recommended to perform once a day the exercises indicated in the first session [3], with a daily commitment of approximately 25 minutes [21].
The program provided for the daily execution of no. 6 exercises; specifically, the work protocol included three stretching exercises and specific strengthening exercises [22]: see Appendix A
We based the selection of the stretching and strengthening exercises on the best available evidence [7].
The stretching exercises were directed at upper trapezius, pectoralis minor and posterior capsule; they were performed in three repetitions of thirty seconds each as indicated by the references [23].
The specific strengthening exercises concerned the activation of the shoulder external rotators, the lower trapezius, and the serratus anterior; the request was to perform three series of thirty activations each in the pain-free range using an elastic band resistance; this resistance was increased in the third week and always progressively [7].
To ease the execution of this homework protocol, the exercises were supervised by PT B in each session and each participant was provided with a DVD24 containing the videos of the same exercises [24].
To further encourage the implementation of the exercise programme, each subject was asked to keep a daily diary to be presented at each scheduled weekly meeting; this made it possible to verify the correct execution of the individual work program and, if necessary, to adapt each exercise to the needs/difficulties of each subject [24].
After the fifth meeting and until the last follow-up visit, we asked participants to suspend the execution of the exercises to verify the maintenance of the functional recovery obtained over time.
The SG subjects, in the second and fifth sessions, underwent an FM treatment instead of the exercise protocol. The treatment was performed by another physiotherapist [PT C] dedicated solely to this activity, with more than 5 years of experience in performing the FM technique.
Assuming the dynamic work of the shoulder joint and the scapular girdle, and the frequent multiplanar movements in which they are involved during daily activities, we arbitrarily decided to treat only the CFs in their diagonal or spiral organization as described by FM technique, excluding CCs because more closely related to uniplanar activities and movements [13]. See Figure A1 and Figure A2 in Appendix B
Each subject had direct live chat contact with their physiotherapist for warning of any adverse events they might have encountered during the execution of the home exercise programme.
2.2. Primary and Secondary Outcomes
We used pain as the primary outcome of our study since it is a clinical condition potentially capable of favouring the chronicisation of the clinical picture and the catastrophizing process.
We decided to standardize pain assessment using NRS scale while performing the Appley Scratch Test25.
Considering that a painful shoulder is usually affected also in its mobility, strength, and function, we decided to use these as secondary outcomes.
Active range of motion (aROM) was assessed using a bubble goniometer placed on the person's wrist, measuring the following directions of movement:
- flexion (aROM flex): individual standing in front of a square-shaped column. Shoulder flexion with elbow outstretched of the upper limb to be tested was required. The operator corrected any movement compensations (e.g. trunk movements);
- abduction (aROM abd): individual standing upright and aligned with the same column with the side not being examined; shoulder abduction with elbow extended was required. The operator paid attention to any movement compensations;
- internal and external rotation (aROM intra - aROM extra): subject prone on the couch, with pillow positioned under the chest and operator at the side to be tested. The humerus of the limb to be tested resting on the couch and the forearm in a vertical position outside with the elbow free to move; external rotation and internal rotation with flexed elbow were requested. The operator's task was to check the possible movement compensation of the articular elements of the upper limb.
- strength was measured through active muscle recruitment in flexion and abduction. The measurement was carried out by an isometric dynamometer (Sauter GmbH - FK 1K), fixed at the bottom of the wall bar by means of a fixed-length rope grasped by the hand of the limb to be tested, so as to allow a movement of less than 90° of elevation; the directions of movement considered were:
- flexion (s-Flex): The subject was positioned in an upright position facing and in contact with the back against the wall bar, requesting an elbow-stretched elevation. The operator corrected any movement compensations.
- abduction (s-Abd): the subject was positioned with the contralateral shoulder facing the wall bar, requesting abduction elevation with the elbow outstretched, with the rope tied to the dynamometer anterior to the subject's body. The operator checked that no movement compensations were performed.
The instruction was to make a progressive movement that puts the rope in tension expressing the maximum intensity for at least 5 seconds. The recorded value was deduced from the average of three successive repetitions, with a 5-second pause between them.
The operator checked that no movement compensation was performed. The instrument was previously validated through a test which involved the execution of 10 measurements with a nominal weight of 6 kg; the measurements were then performed in Newton units.
The initial, final and intra-treatment evaluations were always performed by the same operator, who was unaware of the attributions of the subjects in the two study groups, whereas the FM treatments were performed by a physiotherapist who did not carry out other treatments with the subjects of both groups.
The NRS, aROM and Strength outcome assessments were carried out at recruitment (T0), before (T1) and after (T2) the second session, before (T3) and after (T4) the fifth session and at follow-up (T5) one month after the latter. Functionality and disability outcomes measured by the DASH and Constant Murley scale were measured at T0, T4 and T5.
2.3. Statistical Analysis and Intention to Treat
Data was collected and recorded in a database by the physiotherapist who assessed all subjects without knowing which group they belonged to. The database was analysed by another operator using STATA 14 (https://www.stata.com/stata14/). Data referred to pain (NRS scale) and disability (CONSTANT MURLEY and DASH scales) assessment was treated as ordinal variable using statistical test by ranks “Mann–Whitney U test”; data referred to mobility (ARom) and strength (isometric dynamometer) assessment was treated as interval variable using “Student t-test”. Analysis between groups was conducted for each outcome. Data was also processed for the minimal clinical important difference (MCID) analysis [28,29]. NRS, Arom, Constant Murley, Dash reference values were obtained from the literature strength; reference values were obtained using the main value of all subjects at each assessment time [30].
For missing data, we used the ‘last observation carried forward’ ITT method.
2.4. Sample Size
The sample size was calculated with α = 0.05, β = 0.20 for the main objective of the study (pain assessed with NRS scale) and the expectation of a difference of 2 points and a SD of 3 points [22]. Due to these parameters, the sample size was calculated for 35 subjects for each arm of the study.
3. Results
The study began in October 2017 and was completed in October 2019.
A total of 94 subjects were recruited. In Figure 1 is displayed the flow chart of the study, showing the number of participant recruited, and how the assessments were scheduled.
9 subjects, after having signed the informed consent, did not appear at the first session and then refused further contact.
During the study, only one additional drop-out occurred, due to work-related injury not related to the activities included in the protocol. No adverse events related to the practices under study were found.
The survey carried out at T0 (shown in the table of the statistical analysis between groups), shows how all the outcome measures in the study define a homogeneity of the two study groups, with the exception of aROM flex which shows a statistically different value between the two groups; this is due to a mean value which is 150.5 (± 18.3 SD) for the SG while it is 136.9 (± 29.6 SD) for the CG. This data can be seen in Table 1, Table 2 and Table 3.
Table 1 reports T0-T4 differences for each groups in every outcomes. In the left column we have: 1st row: the mean differences of the CG; 2nd: the mean differences of the SG; 3rd: the reference MCID values; 4th: the numbers (n) of subjects of the CG which exceeded the MCID reference value; 5th: the numbers (n) of subjects of the SG which exceeded the MCID reference value; 6th: the percentage (%) of subjects of the CG which exceeded the MCID reference value; 7th: the percentage (%) of subjects of the SG which exceeded the MCID reference value.
Table 2 reports T0-T5 differences for each groups in every outcomes. In the left column we have: 1st row: the mean differences of the CG; 2nd: the mean differences of the SG; 3rd: the reference MCID values; 4th: the numbers (n) of subjects of the CG which exceeded the MCID reference value; 5th: the numbers (n) of subjects of the SG which exceeded the MCID reference value; 6th: the percentage (%) of subjects of the CG which exceeded the MCID reference value; 7th: the percentage (%) of subjects of the SG which exceeded the MCID reference value.
Table 3 reports T4-T5 differences for each groups in every outcomes. In the left column we have: 1st row: the mean differences of the CG; 2nd: the mean differences of the SG; 3rd: the reference MCID values; 4th: the numbers (n) of subjects of the CG which exceeded the MCID reference value; 5th: the numbers (n) of subjects of the SG which exceeded the MCID reference value; 6th: the percentage (%) of subjects of the CG which exceeded the MCID reference value; 7th: the percentage (%) of subjects of the SG which exceeded the MCID reference value.
MCID values are reported with literature ‘s references and data analysis of our study at different session times. Subjects exceeding the MCID values and their percentages within the reference group are reported.
With regard to the study's primary indicator - pain measured by NRS - the literature reference indicated a 2-point change as clinically significant [29,30,31].
The average difference detected between T0 and T4 in the CG and SG shows values above 2; whereas the same comparison between CG and SG between T0 and T5 shows values above 2 only in the SG. Specifically, the percentage of subjects exceeding the MCDI threshold value at T0 and T4 is 57.9% in the CG and 70.3% in the SG; between T0 and T5 it is 55.3% for the CG and 66% for the SG.
With regard to the outcome indicators of s-flexion and s-abd, we found no reference standards in the literature to use as MCIDs; in order to try to interpret the findings, we arbitrarily calculated the average value of strength gain over the entire sample of enrolled subjects who completed the study, taking this value as a reference against which to compare the results of each group.
In the survey at T4, the overall average increase in flexion force was 11.2 Newtons; compared to this value, 51.1% of the SG subjects performed better, compared to 47.4% of the CG subjects.
At T5, the average overall increase was 13.1 Newtons, a value that was exceeded by 53.2% of the SG subjects and only by 34.2% of the CG subjects.
As far as force in abduction is concerned, the overall average increase in T4 was 14.9 Newtons, a value exceeded by 57.4% of the subjects in the SG and only 44.7% of the subjects in the CG. At T5, on the other hand, compared to an overall average strength evaluation of the sample of 15.8 Newtons, we saw an improved performance for 53.2% of the subjects in the SG and only 26.3% in the CG.
A further consideration with regard to the increase in strength can be seen by observing how, while at the end of the period of active reinforcement (T4), the average strength is higher in the CG than in the SG both in flexion (11.8N compared to 10.6N) and in abduction (15, 8N versus 14.1N), the situation is reversed at follow-up (T5) when, after one month without active reinforcement, the average strength measured is significantly better in the SG than in the CG both in flexion (15.8N versus 9.9N) and in abduction (19.0N versus 11.7N).
Regarding the variation of aROM flex, the literature indicates 14° as a clinically significant variation [32].
The average measures in both groups were above this value. Specifically, at T4 72.3% of the SG subjects exceeded the reference threshold, compared with 55.3% of the CG subjects.
At follow-up, the reference value is exceeded by 68% of SG subjects and only 50% of CG subjects.
With reference to the variation of the Rom in abduction, the literature reported the MCID value to be 11°.
At the end of the training period, 85.1% of the SG subjects exceeded this increase value, but only 73.3% of the CG subjects. At follow-up, the reference value was exceeded by 80.9% of the SG subjects and only 60.5% of the CG subjects [32].
The MCDI value for internal and external rotation was indicated in the literature to be equal to 14° [30].
As far as internal rotation at T4, 63.8% of the SG subjects exceeded this value and only 50% of the CG. At T5, the percentages were 70.2% in the SG and 52.6% in the CG.
On the contrary, the change in external rotation was better at T4 for 53.2% of the SG subjects compared to 36.8% of the CG subjects. At follow-up, the percentage of subjects above baseline was 59.6% in the SG and only 28.9% in the CG [32].
In the comparison of the results referred to the Dash scale, the MCDI reported in the literature exceeds the value of 10.83. In the measure at T4 both groups have a higher mean differential value; the same is found in the measurement at follow-up.
Specifically, in the measure at T4, the percentage variation between T0 and T4 exceeded the reference value in the SG in 57.4% of the subjects, compared to 52.6% in the CG; at follow-up (T5) this variation affected 70.2% of the subjects in the SG, compared to 55.3% of the subjects in the CG.
The literature taken as a reference for the Constant Murley scale indicated an MCID value of 17 [34].
The average variation values reported between T0 and T4 are not higher than this value for either group; on the other hand, between T0 and T5, the SG exceeds the expected value, unlike the CG. In particular, it is noted that while at T4 the mean value of the SG is slightly higher than the CG (SG: 12, 25.5% and CG: 13, 34.2%), at T5 values are significantly higher (SG: 22, 46.8% and CG: 14, 36.8%); this trend reversal will be commented on in the discussion.
Table 4 reports the statistical analysis of the values obtained in this study.
Table 4 reports statistical analysis. In the 1st column are listed all the outcomes ; 2nd and 3rd columns report T0 analysis to show the homogeneity of groups; 4th and 5th column report the T0-T4 analysis; 6th and 7th column report the T0-T5 analysis; 8th and 9th column report the T4-T5 analysis. For each analysis p-value and 95% confidence interval (C.I.), if indicated, are reported.
It can be noted that between T0 and T4 there are no statistically significant differences between the two groups in any of the outcomes found; only the comparison of the ROM value in extra-rotation is statistically significant in the comparisons between T0 and T5; more significant are the differences found between T4 and T5, which appear statistically different for the outcomes of strength and again for external rotation.
4. Discussion
4.1. Results Discussion
The disorders of the shoulder girdle are multiple and complex; among these, pain is a very disabling component that over time can lead to critical dysfunctional situations, up to serious difficulties in the activities of daily living.
The importance of a physiotherapy care taking of subjects with recurrent shoulder pain, without instrumental evidence of musculoskeletal injuries is confirmed in this study.
We chose to assess pain, strength, mobility and functionality as outcome related to treatment of the shoulder joint. To assess shoulder functionality, we decided to apply the two most widely used scales in literature: DASH and Constant Murley.
In daily practice soft tissue manipulations, according to FM indications and rules, represent an approach that can offer significant improvement of pain, strength and functionality as highlighted in other papers [14,15,35]. For these reasons we associated a FM treatment to therapeutic exercise in the SG to evaluate if it could be possible to get better improvement if compared with physiotherapy exercise alone. With regard to the results of this study, it should be noted the low number of drop outs: the recruitment of subjects in the study, the organization of treatment sessions, the weekly monitoring of the suggested homework and the little time required to perform the therapeutic exercises (25 minutes a day during four weeks to perform 3 stretching and 3 strengthening selective muscle exercises), allowed the subjects to increase the compliance to the study protocol.
The exercises proposed in our protocol are the same that other studies have administered to a sample with similar clinical conditions, resulting in a good improvement in pain and DASH score [7,36].
The intervention protocol for both CG and SG did not show any dropouts or side effects; therefore, we can further state that MF treatment was well tolerated by all SG participants.
In general, all physiotherapists involved in the study gather verbal comments of good satisfaction from all people in both groups. The recruitment of subjects planned in our study allowed us to analyse a large sample of people with chronic shoulder pain and impairment; their randomisation allowed us to identify two statistically homogeneous groups.
The only outcome measure that is statistically different at T0 between the SG and CG (aROM flex) did not invalidate the global data analysis, since comparison of the averages of the two groups at T4 and T5 showed no statistically significant differences. In this study, it was arbitrarily decided to use FM through palpatory assessment and treatment of CFs only (see “materials and methods” paragraph).
Similarly, it was then agreed to administer only two FM treatments three weeks apart, instead of the standard weekly cadence typically indicated in other clinical trials related to FM [14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31,32,33,34,35,36,37].
In the last treatment session (T4) all outcome measures were also collected; this resulted in the subjects of the SG being assessed immediately after the treatment of FM. This choice has probably affected the values found for a plausible increased sensitisation of subjects due to the treatment.
Indeed, in the T0-T4 comparison not all results showed the expected clinical improvement: almost all of them overcome the MCID threshold: only the s – flex and s – abd of the SG, the aROM intra and aROM extra rotation for the CG and the Constant-Murley for both groups didn’t reach it.
In the T5 assessments only the CG shows values lower than the expected MCID with regard to s- Flex, s – Abd and aROM extra. These results confirm that the treatments carried out in T4 conditioned data collected at that time. The effectiveness of the intervention protocol of the study was confirmed by the improvement of the values of all the outcomes for both groups in the comparison between both T4 and T5 to T0.
In the comparison between T4 and T5 it is noted that SG got a greater improvement than the CG, confirming the validity of FM treatment (only aROM flex item made an exception). These better results in SG could be attributed to the ability of FM to permanently change the viscosity of the extracellular matrix, allowing a better sliding between and within fascial tissue planes even one month after last FM treatment.
Similar results, also stated in other clinical trials referred to the FM [38], are obtained due to a method that assess and treats not the only painful segment (in our study the scapular-humeral joint), but considers the anatomical continuity of fascial tissues within the clinical history of each individual. The better sliding of fascial planes would benefit the tensional homeostasis of the myofascial tissues, allowing a stable improvement over time of the results in terms of pain, mobility and strength.
With respect to the functionality, only the DASH scale showed an improvement. This difference may be related to the presence of item referred to pain in the DASH scale but not in the Constant-Murley, which contains items mainly related to mobility. In our study other pain scores improved better than mobility scores.
Inferential data analysis allows us to confirm the clinical findings.
As stated above, we think that no statistically significant difference between T0- T4 has been caused by the concurrence at T4 of the last treatment session and the final assessment. The deep fascial treatment often causes temporary soreness, and this most likely affected the assessments at T4.
In addition, the choice to include subjects with a pain value of at least 2 points on the NRS scale conditioned low average values at T0 in both groups (CG = 3.2 ± 2.5 SD; GS = 3 ± 2.3 SD); consequently, it would have been very difficult to obtain a wide reduction of this value and then a statistically significant difference in the between groups analysis.
The T0-T5 comparison shows statistically significant difference (aROM extra) and others at the limit of the significance parameters (s-Flex and s-Abd) with a better improvement of the SG: this confirms the possible interference of the FM concurrent treatment at T4, and also improvement and maintenance after 4 weeks of the above parameters.
The T4-T5 comparison shows more significant values in the same items above, confirming that the FM treatment allowed the SG to obtain stable statistically significant improvements over time with respect of CG. FM treatment permanently change the fluidity and functionality of connective tissue, as also found in other previous works [39].
4.2. Limits
The limited statistical effectiveness we found in this study could be justified on several following grounds:
- we included subjects with mild shoulder pain (at least 2 on the NRS scale); this threshold could not seriously affect mobility and functionality of the shoulder and the upper limb (the mean value of NRS at T0 in SG = 3.3 and in CG = 3.2)
- due to the randomisation criteria, the number of participants was quite different in the two groups: 47 in SG, 38 in CG. However, the two groups at T0 were statistically homogeneous in every outcome, except for the aROM flex.
- The probably most influential limit on the results of this study was the decision to treat only the CF (Centers of Fusion), as elements of integration and connection between the segmentary motor activations, excluding the CC (Center of Coordination) that are widely used in daily clinical practice.
- the usual distance between two FM session is one week: we only performed 2 FM treatments 2 weeks apart. With more and closer FM treatments, we probably could get better statistical results.
- The limited follow-up period (30 days) does not allow us a proper long-term evaluation of the effects of the treatment performed
- The aROM and strength assessment at T4 has been probably conditioned by the second FM treatment carried out at the same time. FM technique involves manual friction in the deep fascial tissues, often causing an annoying response and then potentially limiting the following active tests.
4.3. Indications for Clinical Practice
Thanks to the protocol implemented and the data collected in this study we can state that:
- a self-administered treatment with simple and easily repeatable exercises protocol, as well as a self-managed treatment diary, are elements that facilitate adherence to treatment by participants
- the treatments in the study (active exercises, stretching exercises and FM treatment) didn’t show any side effects and were well appreciated by all the subjects
- Using both CCs as well as CFs in FM treatments represent a more comprehensive treatment choice with potentially better results
- Using a weekly schedule for FM treatment and plan more than 2 FM treatments, as indicated in most clinical trials, could further improve clinical outcomes
FM treatment may adversely affect the assessments scores if collected immediately after treatment. A more truthful and reliable evaluation should be performed at least one week after the FM treatment.
This section may be divided by subheadings. It should provide a concise and precise description of the experimental results, their interpretation, as well as the experimental conclusions that can be drawn.
5. Conclusions
A physiotherapy approach is effective for the treatment of a recurrent shoulder pain. The treatment includes stretching exercises and a selective muscle reinforcement program, which are also well self-administered by subjects.
The use of a self-managed diary and the delivery of an audio-visual support (a DVD with video description of the exercises), allowed all the subjects to completely adhere to the protocol of the study.
2 FM sessions enable subjects in the SG to better improve in the short term (30 days) the active mobility and muscle strength without showing any side effects at all.
In a clinical point of view, considering MCID values, our protocol of intervention demonstrate that a specific physiotherapy program reduces pain and allows an improvement in both in active mobility and activity daily life. In the last follow up subjects in SG showed better results than CG, showing that FM treatment should be performed for non-specific shoulder pain.
Moreover, as stated above in the limit paragraph, a more faithful application of the FM technique, as indicated by the Author and applied in other studies, could further improve the outcomes in subjects with non-specific shoulder pain.
Shoulder extension targeting lower trapezius strengthening
Author Contributions
Conceptualization, Bellotti S., Busato M.; methodology, Bellotti S., Busato M.; software, Branchini M.; formal analysis, Bellotti S., Branchini M.; investigation, Bellotti S., Busato M., Cattaneo C.; data curation, Bellotti S., Busato M., Cattaneo C.; writing—original draft preparation, Bellotti S., Branchini M.; writing—review and editing, Bellotti S., Branchini M.; supervision, Branchini M.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Provincial Ethics Committee of Bergamo, registration no. 697 dated 08/10/2016, clinicaltrials.gov identifier: NCT03041727.
Informed Consent Statement
Written informed consent has been obtained from the patient(s) to publish this paper.
Data Availability Statement
The data presented in this study are available on request from the corresponding author. The data are not publicly available due to privacy reasons.
Acknowledgments
We thank the ASST Bergamo Est for the availability of the spaces and for allowing to spread our research project among its employees, allowing the recruitment of our study sample. We also thank Gabriele Fratto for his fundamental commitment as co-translator of this work.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A
The daily exercise programme
Table A1 shows the daily exercise programme for every participants. These exercises were supervised, ar-ranged and adapted for each individuals during the exercise sessions (5 for CG, 3 for SG).

Table A1.
daily exercise programme.
| Stretching exercises | ||
|---|---|---|
| Exercise 1 | Exercise 2 | Exercise 3 |
| Upper trapezius stretch | Pectoralis minor stretch | Posterior shoulder stretch |
 |
 |
 |
| Strenghtening exercises | ||
| Exercise 1 | Exercise 2 | Exercise 3 |
| Shoulder external rotation | Shoulder extension targeting lower trapezius strengthening | Shoulder protraction targeting serratus anterior strengthening |
 |
 |
 |
Appendix B
CFs location
Figure A1.
In this figure are shown CFs in the frontal aspect of the body.
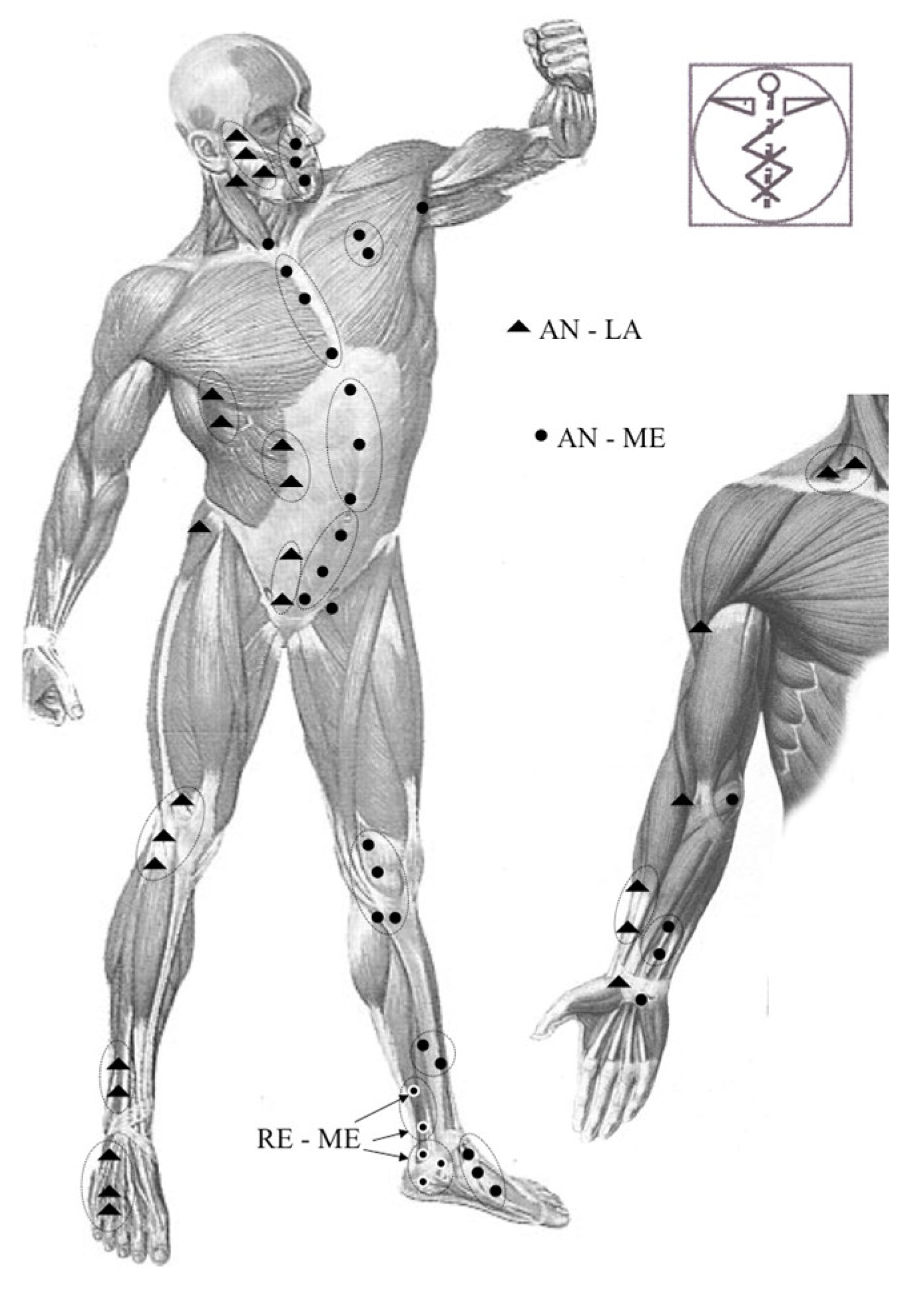
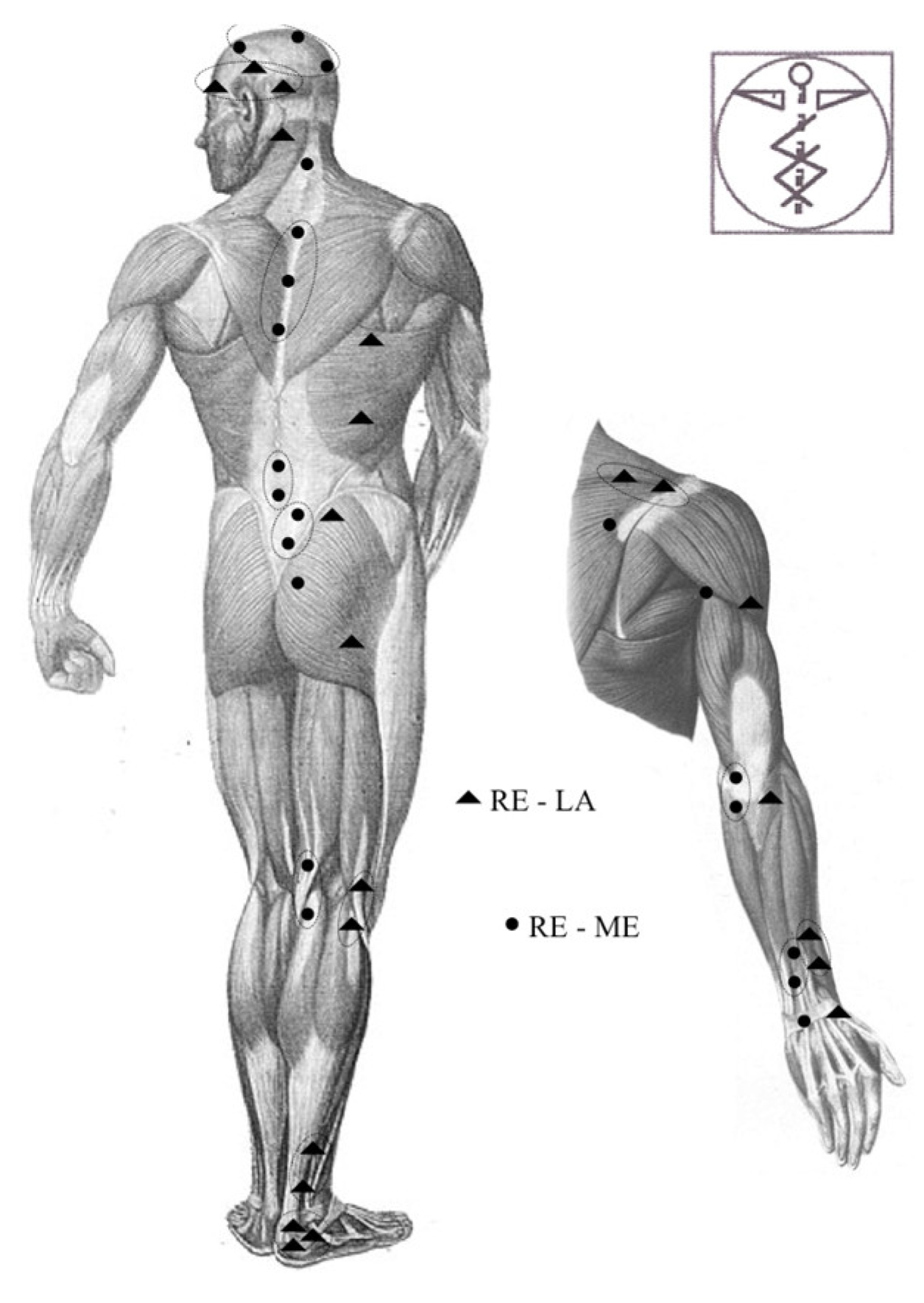
Figure A2.
In this figure are shown CFs in the posterior aspect of the body.
References
- Luime, J.J.; Koes, B.W.; Hendriksen, I.J.M.; Burdorf, A.; Verhagen, A.P.; Miedema, H.S.; Verhaar, J.A.N. Prevalence and incidence of shoulder pain in the general population; a systematic review. Scand. J. Rheumatol. 2004, 33, 73–81. [Google Scholar] [CrossRef]
- Van Rijn, R.M.; Huisstede, B.M.; Koes, B.W.; Burdorf, A. Associations between work-related factors and specific disorders of the shoulder – a systematic review of the literature. Scand. J. Work. Env. Health 2010, 36, 189–201. [Google Scholar] [CrossRef]
- Zanca, P. Shoulder pain: Involvement of the acromioclavicular joint. (Analysis of 1,000 cases). Am. J. Roentgenol. Radium Ther. Nucl. Med. 1971, 112, 493–506. [Google Scholar] [CrossRef]
- Reilingh, M.L.; Kuijpers, T.; Tanja-Harfterkamp, A.M.; van der Windt, D.A. Course and prognosis of shoulder symptoms in general practice. Rheumatology 2008, 47, 724–730. [Google Scholar] [CrossRef]
- Tamai, K.; Akutsu, M.; Yano, Y. Primary frozen shoulder: Brief review of pathology and imaging abnormalities. J. Orthop. Sci. 2014, 19, 1–5. [Google Scholar] [CrossRef]
- Lentz, T.A.; Barabas, J.A.; Day, T.; Bishop, M.D.; George, S.Z. The Relationship of Pain Intensity, Physical Impairment, and Pain-Related Fear to Function in Patients with Shoulder Pathology. J. Orthop. Sports Phys. Ther. 2009, 39, 270–277. [Google Scholar] [CrossRef]
- Camargo, P.R.; Alburquerque-Sendín, F.; Avila, M.A.; Haik, M.N.; Vieira, A.; Salvini, T.F. Effects of Stretching and Strengthening Exercises, With and Without Manual Therapy, on Scapular Kinematics, Function, and Pain in Individuals with Shoulder Impingement: A Randomized Controlled Trial. J. Orthop. Sports Phys. Ther. 2015, 45, 984–997. [Google Scholar] [CrossRef]
- Toomey, E.; Currie-Murphy, L.; Matthews, J.; Hurley, D.A. The effectiveness of physiotherapist-delivered group education and exercise interventions to promote self-management for people with osteoarthritis and chronic low back pain: A rapid review Part I. Man. Ther. 2015, 20, 265–286. [Google Scholar] [CrossRef]
- Page, M.J.; Green, S.; McBain, B.; Surace, S.J.; Deitch, J.; Lyttle, N.; Mrocki, M.A.; Buchbinder, R. Manual therapy and exercise for rotator cuff disease. Cochrane Database Syst. Rev. 2016, 2016, CD012224. [Google Scholar] [CrossRef]
- Anton, H.A. Frozen shoulder. Can. Fam. Physician 1993, 39, 1773–1778. [Google Scholar]
- Stecco, C.; Day, J.A. The Fascial Manipulation Technique and Its Biomechanical Model: A Guide to the Human Fascial System. Int. J. Ther. Massage Bodyw. 2010, 3, 38–40. [Google Scholar]
- Stecco, C.; Schleip, R. A fascia and the fascial system. J. Bodyw. Mov. Ther. 2016, 20, 139–140. [Google Scholar] [CrossRef] [PubMed]
- Day, J.A.; Stecco, C.; Stecco, A. Application of Fascial Manipulation© technique in chronic shoulder pain—Anatomical basis and clinical implications. J. Bodyw. Mov. Ther. 2009, 13, 128–135. [Google Scholar] [CrossRef] [PubMed]
- Branchini, M.; Lopopolo, F.; Andreoli, E.; Loreti, I.; Marchand, A.M.; Stecco, A. Fascial Manipulation® for chronic aspecific low back pain: A single blinded randomized controlled trial. F1000Research 2016, 4, 1208. [Google Scholar] [CrossRef] [PubMed]
- Brandolini, S.; Lugaresi, G.; Santagata, A.; Ermolao, A.; Zaccaria, M.; Marchand, A.M.; Stecco, A. Sport injury prevention in individuals with chronic ankle instability: Fascial Manipulation® versus control group: A randomized controlled trial. J. Bodyw. Mov. Ther. 2019, 23, 316–323. [Google Scholar] [CrossRef] [PubMed]
- Bennell, K.; Coburn, S.; Wee, E.; Green, S.; Harris, A.; Forbes, A.; Buchbinder, R. Efficacy and cost-effectiveness of a physiotherapy program for chronic rotator cuff pathology: A protocol for a randomised, double-blind, placebo-controlled trial. BMC Musculoskelet. Disord. 2007, 8, 86. [Google Scholar] [CrossRef] [PubMed]
- Escamilla, R.F.; Hooks, T.R.; Wilk, K. Optimal management of shoulder impingement syndrome. Open Access J. Sports Med. 2014, 5, 13–24. [Google Scholar] [CrossRef]
- Smedley, J.; Inskip, H.; Trevelyan, F.; Buckle, P.; Cooper, C.; Coggon, D. Risk factors for incident neck and shoulder pain in hospital nurses. Occup. Env. Med. 2003, 60, 864–869. [Google Scholar] [CrossRef]
- Miranda, H.; Viikari-Juntura, E.; Martikainen, R.; Takala, E.-P.; Riihimäki, H. A prospective study of work related factors and physical exercise as predictors of shoulder pain. Occup. Environ. Med. 2001, 58, 528–534. [Google Scholar] [CrossRef]
- Kallner, A. A study of simulated normal probability functions using Microsoft Excel. Accredit. Qual. Assur. 2016, 21, 271–276. [Google Scholar] [CrossRef]
- Ma, C.; Szeto, G.P.; Yan, T.; Wu, S.; Lin, C.; Li, L. Comparing Biofeedback with Active Exercise and Passive Treatment for the Management of Work-Related Neck and Shoulder Pain: A Randomized Controlled Trial. Arch. Phys. Med. Rehabil. 2011, 92, 849–858. [Google Scholar] [CrossRef] [PubMed]
- Karlsson, L.; Takala, E.-P.; Gerdle, B.; Larsson, B. Evaluation of pain and function after two home exercise programs in a clinical trial on women with chronic neck pain - with special emphasises on completers and responders. BMC Musculoskelet. Disord. 2014, 15, 6. [Google Scholar] [CrossRef] [PubMed]
- Rosa, D.P.; Borstad, J.D.; Pogetti, L.S.; Camargo, P.R. Effects of a stretching protocol for the pectoralis minor on muscle length, function, and scapular kinematics in individuals with and without shoulder pain. J. Hand Ther. 2017, 30, 20–29. [Google Scholar] [CrossRef] [PubMed]
- McLean, S.M.; Burton, M.; Bradley, L.; Littlewood, C. Interventions for enhancing adherence with physiotherapy: A systematic review. Man. Ther. 2010, 15, 514–521. [Google Scholar] [CrossRef] [PubMed]
- Woodward, T.W.; Best, T.M. The Painful Shoulder: Part I. Clinical Evaluation. Am. Fam. Physician 2000, 61, 3079–3088. [Google Scholar]
- Brindisino, F.; Pellicciari, L.; Lorusso, M.; Pennella, D.; Padua, R.; Di Bari, M. Cross-cultural adaptation, reliability, and validity of the Italian version of the Shoulder Disability Questionnaire. Musculoskelet. Sci. Pract. 2020, 46, 102123. [Google Scholar] [CrossRef]
- Carosi, M.; Galeoto, G.; Di Gennaro, S.; Berardi, A.; Valente, D.; Servadio, A. Transcultural reliability and validity of an Italian language version of the Constant–Murley Score. J. Orthop. Trauma. Rehabil. 2020, 27, 186–191. [Google Scholar] [CrossRef]
- Olsen, M.F.; Bjerre, E.; Hansen, M.D.; Tendal, B.; Hilden, J.; Hróbjartsson, A. Minimum clinically important differences in chronic pain vary considerably by baseline pain and methodological factors: Systematic review of empirical studies. J. Clin. Epidemiol. 2018, 101, 87–106. [Google Scholar] [CrossRef]
- Dabija, D.I.; Jain, N.B. Minimal Clinically Important Difference of Shoulder Outcome Measures and Diagnoses: A Systematic Review. Am. J. Phys. Med. Rehabil. 2019, 98, 671–676. [Google Scholar] [CrossRef]
- Hao, Q.; Devji, T.; Zeraatkar, D.; et al. Minimal important differences for improvement in shoulder condition patient-reported outcomes: A systematic review to inform a BMJ Rapid Recommendation. BMJ Open 2019, 9, e028777. [Google Scholar] [CrossRef]
- Tashjian, R.Z.; Deloach, J.; Porucznik, C.A.; Powell, A.P. Minimal clinically important differences (MCID) and patient acceptable symptomatic state (PASS) for visual analog scales (VAS) measuring pain in patients treated for rotator cuff disease. J. Shoulder Elb. Surg. 2009, 18, 927–932. [Google Scholar] [CrossRef] [PubMed]
- Muir, S.W.; Corea, C.L.; Beaupre, L. Evaluating change in clinical status: Reliability and measures of agreement for the assessment of glenohumeral range of motion. North. Am. J. Sports Phys. Ther. NAJSPT 2010, 5, 98–110. [Google Scholar]
- Franchignoni, F.; Vercelli, S.; Giordano, A.; Sartorio, F.; Bravini, E.; Ferriero, G. Minimal Clinically Important Difference of the Disabilities of the Arm, Shoulder and Hand Outcome Measure (DASH) and Its Shortened Version (QuickDASH). J. Orthop. Sports Phys. Ther. 2014, 44, 30–39. [Google Scholar] [CrossRef] [PubMed]
- Holmgren, T.; Öberg, B.; Adolfsson, L.; Hallgren, H.B.; Johansson, K. Minimal important changes in the Constant-Murley score in patients with subacromial pain. J. Shoulder Elb. Surg. 2014, 23, 1083–1090. [Google Scholar] [CrossRef] [PubMed]
- Busato, M.; Quagliati, C.; Magri, L.; Filippi, A.; Sanna, A.; Branchini, M.; Marchand, A.M.; Stecco, A. Fascial Manipulation Associated with Standard Care Compared to Only Standard Postsurgical Care for Total Hip Arthroplasty: A Randomized Controlled Trial. PMR 2016, 8, 1142–1150. [Google Scholar] [CrossRef] [PubMed]
- Kuhn, J.E. Exercise in the treatment of rotator cuff impingement: A systematic review and a synthesized evidence-based rehabilitation protocol. J. Shoulder Elb. Surg. 2009, 18, 138–160. [Google Scholar] [CrossRef]
- Pratelli, E.; Pintucci, M.; Cultrera, P.; et al. Conservative treatment of carpal tunnel syndrome: Comparison between laser therapy and Fascial Manipulation(®). J. Bodyw. Mov. Ther. 2015, 19, 113–118. [Google Scholar] [CrossRef]
- Stecco, A.; Meneghini, A.; Stern, R.; Stecco, C.; Imamura, M. Ultrasonography in myofascial neck pain: Randomized clinical trial for diagnosis and follow-up. Surg. Radiol. Anat. 2014, 36, 243–253. [Google Scholar] [CrossRef]
- Cotti, A.; Del Corso, M.; Diana, R.; Cornale, L.; Sudanese, A.; Stecco, A.; Branchini, M. Inter and Intra Operator Reliability of Motor and Palpation Evaluation in Fascial Manipulation in individuals with coxarthrosis. J. Man. Manip. Ther. 2020, 28, 236–245. [Google Scholar] [CrossRef]
Figure 1.
flow chart of the study: in Entry Time people were enrolled signed the informed consent and then were randomized in CG and SG; T0 represent the first assessment and the first treatment for both groups; T0-T4 represent the five treatment sessions where T2 and T4 were a FM treatment for SG; as indicated in the right column, assessments were carried out in T0 (before treatment), T4 and T5 (after treatment) visits.
Figure 1.
flow chart of the study: in Entry Time people were enrolled signed the informed consent and then were randomized in CG and SG; T0 represent the first assessment and the first treatment for both groups; T0-T4 represent the five treatment sessions where T2 and T4 were a FM treatment for SG; as indicated in the right column, assessments were carried out in T0 (before treatment), T4 and T5 (after treatment) visits.
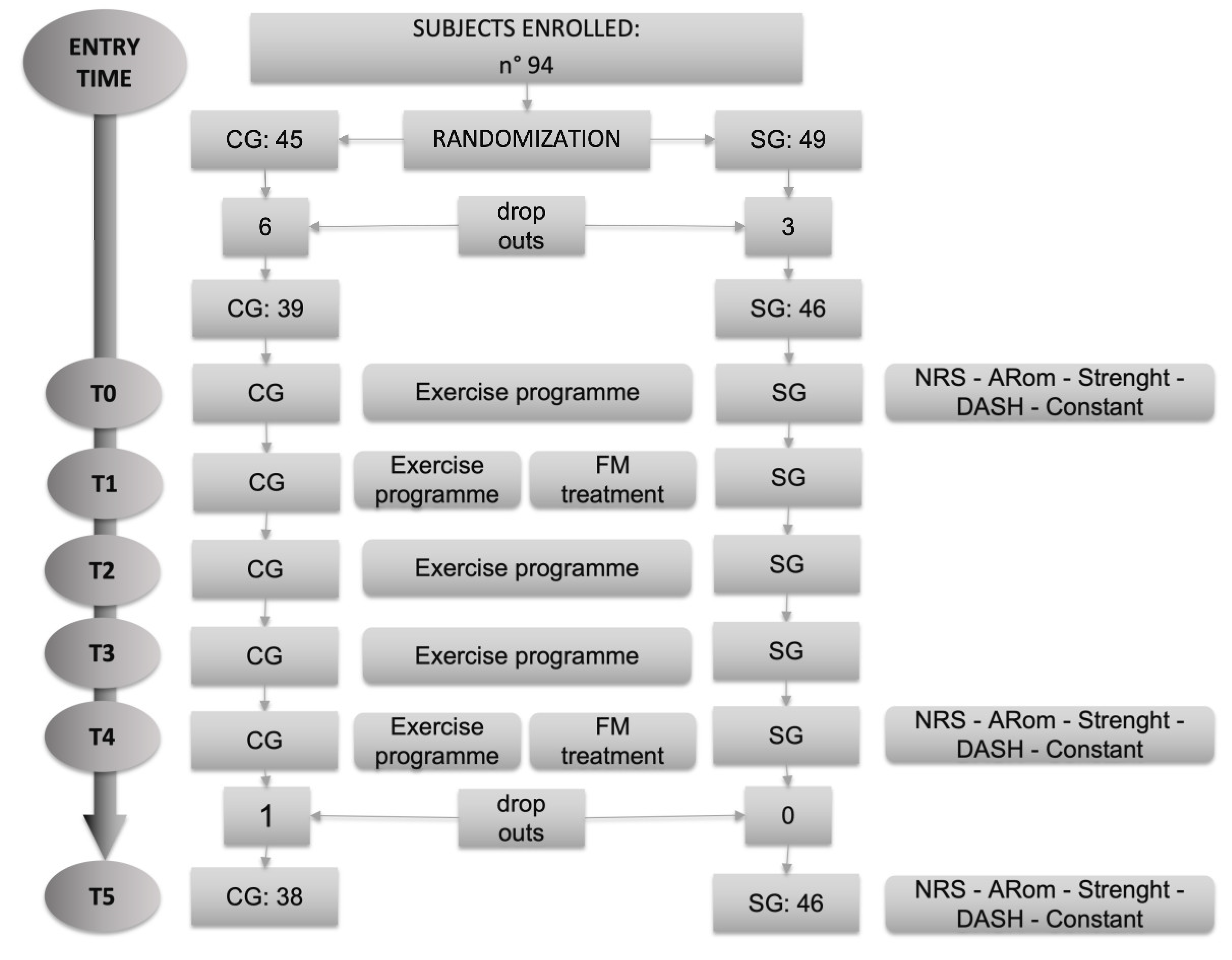
Table 1.
T0-T4 analysis.
| T0-T4 analysis | NRS | s-Flex | s-Abd | aRom Flex | aRom Abd | aRom Intra | aRom Extra | DASH | Constant Murley | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | CG | 2.2 | 11.8 | 15.8 | 22.7 | 29.4 | 12.6 | 10.0 | 13.7 | 13.6 |
| Mean | SG | 2.7 | 10.6 | 14.1 | 22.0 | 32.7 | 16.4 | 16.3 | 17.6 | 12.4 |
| MCID | 2 | 11.2 | 14.9 | 14 | 11 | 14 | 14 | 10.83 | 17 | |
| MCID (n) | CG | 22 | 18 | 17 | 21 | 28 | 19 | 14 | 20 | 13 |
| MCID (n) | SG | 33 | 24 | 27 | 34 | 40 | 30 | 25 | 27 | 12 |
| MCID (%) | CG | 57.9 | 47.4 | 44.7 | 55.3 | 73.7 | 50.0 | 36.8 | 52.6 | 34.2 |
| MCID (%) | SG | 70.2 | 51.1 | 57.4 | 72.3 | 85.1 | 63.8 | 53.2 | 57.4 | 25.5 |
Table 2.
T0-T5 analysis.
| T0-T5 analysis | NRS | s-Flex | s-Abd | aRom Flex | aRom Abd | aRom Intra | aRom Extra | DASH | Constant Murley | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | CG | 1.7 | 9.9 | 11.7 | 22.3 | 26.1 | 14.1 | 5.1 | 13.7 | 12.3 |
| Mean | SG | 2.6 | 15.8 | 19.0 | 19.4 | 34.0 | 20.9 | 18.2 | 19.3 | 13.9 |
| MCID | 2 | 13.1 | 15.8 | 14 | 11 | 14 | 14 | 10.83 | 17 | |
| MCID (n) | CG | 21 | 13 | 10 | 19 | 23 | 20 | 11 | 21 | 14 |
| MCID (n) | SG | 31 | 25 | 25 | 32 | 38 | 33 | 28 | 33 | 22 |
| MCID (%) | CG | 55.3 | 34.2 | 26.3 | 50.0 | 60.5 | 52.6 | 28.9 | 55.3 | 36.8 |
| MCID (%) | SG | 66.0 | 53.2 | 53.2 | 68.1 | 80.9 | 70.2 | 59.6 | 70.2 | 46.8 |
Table 3.
T4-T5 analysis.
| T4-T5 analysis | NRS | s-Flex | s-Abd | aRom Flex | aRom Abd | aRom Intra | aRom Extra | DASH | Constant Murley | |
|---|---|---|---|---|---|---|---|---|---|---|
| Mean | CG | -0.5 | -2.0 | -4.1 | -0.4 | -3.3 | 1.4 | -4.9 | -0.1 | -1.3 |
| Mean | SG | -0.1 | 5.2 | 4.9 | -2.5 | 1.4 | 4.5 | 2.0 | 1.7 | 1.6 |
| MCID | 2 | 2.0 | 0.9 | 14 | 11 | 14 | 14 | 10.83 | 17 | |
| MCID (n) | CG | 2 | 14 | 15 | 6 | 7 | 7 | 4 | 5 | 2 |
| MCID (n) | SG | 3 | 28 | 31 | 2 | 9 | 15 | 10 | 9 | 1 |
| MCID (%) | CG | 5.3 | 36.8 | 39.5 | 15.8 | 18.4 | 18.4 | 10.5 | 13.2 | 5.3 |
| MCID (%) | SG | 6.4 | 59.6 | 66.0 | 4.3 | 19.1 | 31.9 | 21.3 | 19.1 | 2.1 |
Table 4.
Between groups statistical analysis.
| Between group analysis | T0 | T0-T4 | T0-T5 | T4-T5 | ||||
|---|---|---|---|---|---|---|---|---|
| p-value | 95% C.I. | p-value | 95% C.I. | p-value | 95% C.I. | p-value | 95% C.I. | |
| NRS | 0.653 | ------ | 0.407 | ------ | 0.107 | ------ | 0.115 | ------ |
| s-Flex | 0.116 | -17.921 1.996 |
0.711 | -5.356 7.821 |
0.057 | -11.982 .174 |
0.001 | -11.360 -2.914 |
| s-Abd | 0.089 | -20.775 .499 |
0.656 | -5.896 9.313 |
0.052 | -14.657 .0759 |
0.001 | -14.274 -3.725 |
| aRom Flex | 0.011 | -23.971 -3.176 |
0.879 | -8.727 10.181 |
0.628 | -8.698 14.331 |
0.444 | -3.3197 .498 |
| aRom Abd | 0.235 | -23.004 .728 |
0.546 | -13.980 7.451 |
0.210 | -20.3694 .537 |
0.170 | -11.330 2.0267 |
| aRom Intra |
0.255 | -9.235 2.487 |
0.223 | -9.881 2.336 |
0.064 | -14.087 .415 |
0.298 | -8.878 2.751 |
| aRom Extra | 0.276 | -2.998 10.350 |
0.075 | -13.251 .646 |
0.001 | -21.033 -5.287 |
0.024 | -12.804 -.911 |
| DASH | 0.972 | ------ | 0.333 | ------ | 0.1398 | ------ | 0.580 | ------ |
| Constant Murley | 0.100 | ------ | 0.714 | ------ | 0.269 | ------ | 0.017 | ------ |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



