
Submitted:
10 May 2023
Posted:
11 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
All severe cases of SARS-CoV-2 infections are characterized by a high risk of disease progression towards ARDS, leading to bad outcome. Respiratory symptoms in COVID-19 patients often do not correspond to disease’s worsening. A dysregulated host response to the large viral load could play a key role in the disease progression. In our sample median age was 74 years (72-75) and 54% were men. Median period of hospitalization was 9 days. Firstly, we observed an asynchronous trend of neutrophil-to-lymphocyte ratio (NLR) and C-reactive protein (CRP) in 764 selected among 963 patients who were consecutively recruited in two hospitals (Cannizzaro, S. Marco) in Catania, Italy. NLR values in deceased patients showed an increase from baseline over time. By contrast, CRP tended to fall from baseline to median day of hospitalization in all four subgroups, but steeply increased at the end of hospitalization only in ICU-admitted patients. Then we evaluated the relationships between NLR and CRP as continuous variables with PaO2/FiO2 ratio (P/F). Finally, we made mediation and moderation analyses to determine the link between inflammation (CRP), immune system (neutrophils and lymphocytes) and respiratory failure (P/F). CRP, neutrophils and P/F are linked in the same pathogenetic chain leading to respiratory failure.
Keywords:
NLR
; CRP
; P/F
; COVID-19
; Neutrophil-to-lymphocyte ratio
; Neutrophils
; Lymphocytes
; immune system
; biomarkers
; SARS-CoV-2
; inflammation
; ICU
; lung failure
1. Introduction
Clinical features of SARS-CoV-2 infection are various, from mild to moderate symptoms, characterized by spontaneous regression, to severe cases, showing conditions leading to ICU admission or death[1,2]. Despite virus transmission and clinical presentation are well known, scanty information is available about the pathophysiology of disease worsening.
The severe respiratory failure caused by COVID-19 is primarily manifested as acute respiratory distress syndrome (ARDS). Its related pathological findings were often documented in most COVID-19 autoptic studies[3]. ARDS nosography has been substantially modified after COVID-19 pandemic, since several studies have shown that COVID-19-related ARDS is atypical, although often falling within the Berlin definition of ARDS[4,5].
As a matter of fact, inflammation plays a key role in the disease worsening, if any, of COVID-19 patients. Several studies have focused on the cytokine storm and the lymphocyte fall observed in these patients[6,7,8]. The relationship between the clinical presentation of severe cases of COVID-19 and the related immuno-inflammatory factors have not so far well understood[9].
The early identification of cases with greater clinical severity is mandatory to ensure the best possible care. The detection of laboratory bio-markers or indices representing the unbalanced innate and adaptive immune responses allows a rapid characterization of patients in a hospital-setting. Venous and arterial samplings, together with a chest computer tomography (CT) could quickly provide enough information to recognize hyper-inflammatory state and respiratory distress, to assess clinical severity and predict outcome.
Several biochemical parameters were under investigation for an early assessment of disease severity[10,11]. Among them, C-reactive protein (CRP) and Neutrophil-to-lymphocyte ratio (NLR) are rapid and widely available inflammatory indices, recently under debate as predictors of bad outcome in a large variety of pathological conditions characterized by exaggerated systemic inflammation[12,13]. In our previous study we found that both NLR and CRP are reliable prognostic predictors in COVID-19 patients. [14].
Neutrophilia, lymphopenia and high CRP levels are closely linked with the pathophysiology of COVID-19. Cytokine storm determines a massive recruitment of circulating cells resulting in a continuous activation of neutrophils, incremental consumption and negative counter-regulation of lymphocytes and a strengthened inflammatory response, with an over-production of CRP, that is a protein of acute phase.
In the present study, we aimed to evaluate the time-course of immuno-inflammatory pathways involvement in the development of respiratory failure. We especially evaluated the dynamic changes of neutrophils, lymphocytes and CRP during hospitalization. Finally, we also assessed the link between CRP, neutrophils and lymphocytes with P/F ratio, to better understand the individual role of mediators leading to respiratory failure.
2. Materials and Methods
In this retrospective, multicentre, observational study, a total of 963 patients were consecutively candidates among patients admitted to the Emergency Unit of San Marco Hospital and the COVID-19 Internal Medicine Unit at Cannizzaro Hospital, in the city of Catania, Italy, between October 2020 and September 2022. Within this cohort, 764 patients were selected, based on predefined inclusion criteria (Figure 1):
- 1)
- a reliable diagnosis of SARS-CoV2 infection obtained by RT-PCR molecular swab testing;
- 2)
- no history of pharmacological treatments responsible for alterations in the leukocyte count and/or CRP upon admission;
- 3)
- no current or past history of conditions responsible for alterations in the leukocyte count and/or CRP;
- 4)
- availability of at least three blood tests and blood gas analyses during hospitalization, and a hospitalization period not less than 48 hours.
Routine biomarkers were measured using standard techniques using auto-analyzers (Beckman Coulter DxH 800; Danaher Corporation, Miami, FL, USA, Beckman DxC 700 AU; Danaher Corporation, Miami, FL, USA).
Total and differential leukocyte count and CRP levels were measured three times: at baseline, on the median day of hospitalization, and at discharge (defined as death, transfer to the Intensive Care Unit, ICU, or routine discharge).
The severity of respiratory failure was identified using P/F ratio obtained by blood gas test reports, using PaO2/FiO2 ratio, namely the ratio between. Partial arterial pressure of oxygen/Fraction of inspired oxygen.
The neutrophil-to-lymphocyte ratio (NLR) was calculated as follows: NLR = number of neutrophils/number of lymphocytes.
Relevant information was obtained by reviewing the medical records of the participants, including their demographic and anamnestic data, clinical and laboratory characteristics, treatment regimen, as well as outcome.
Appropriate measures were taken to display information before performing statistical analysis.
The present study exclusively focused on death following SARS-CoV2 infection, so excluding those caused by any other factors.
2.1. Statistical Analysis
The statistical analysis was performed using the IBM-SPSS and R statistical software packages.
Categorical variables were described in terms of absolute frequency and percentage prevalence, while continuous variables were further divided into two groups, after performing the Kolmogorov-Smirnov test to evaluate their distribution. Continuous variables were expressed as mean ± standard deviation in presence of normal distribution and median and interquartile range in presence of non- Gaussian distribution.
The sample was initially divided into three groups, according to outcome. Differences between outcome were evaluated using the chi-square test with Fisher’s correction for categorical variables, one-way ANOVA for normally distributed continuous variables, and the Kruskal-Wallis test for non-normally distributed continuous variables.
Non-parametric tests, such as Spearman’s correlation coefficient and Kendall’s Tau, were used to assess the correlations between the variables of interest, considering their distribution.
Where appropriate, we used the z-scores for variables characterized by extreme kurtosis and asymmetry.
Firstly, to evaluate the relationship between NLR and CRP as continuous variables with Pa02/FiO2 ratio, univariate and multivariate logistic regression models were used, and odds ratios (ORs), both corrected and uncorrected, as well as 95% confidence intervals (CIs), were calculated.
All these relationships were assessed in the whole sample and also according to single outcome.
Multiple logistic and Cox regression models were also built to verify the associations between biomarkers and outcome.
Repeated measures ANOVA was performed, whenever necessary, to test the differences over time in the mean levels of variables.
Finally, to better understand the existing relationships between inflammatory biomarkers and P/F ratio, we performed a mediation analysis, to verify if these relationships resulted mediated by an external variable. A moderation analysis was also done to estimate if the effect of such variable could influence the strength and direction of these relationships, after verifying that the required assumptions were met.
3. Results
Figure 1 depicts the flow chart of patient recruitment, as well as different outcomes.
Median age of the whole sample was 74 years and 54% were men. Median period of hospitalization was 9 days.
Compared to survivors, patients deceased or admitted to ICU showed higher median levels of NLR, CRP, leukocyte and neutrophil count, lower values of lymphocyte count and P/F ratio. Regarding age, significant differences were only observed between deceased and survivors.
As regards comorbidities, no statistically differences were observed between the various outcomes. All demographic and clinical characteristics of the patients are shown in Table 1.
First, we analysed the temporal trend shown by NLR and CRP during hospitalization, and assessed the differences by repeated measure ANOVA, in the whole sample and for each subgroup (Figure 2A,B).
While whole sample, survivors and ICU-admitted patients showed a flat pattern of NLR over time, deceased patients, by contrast, showed an increase of NLR from baseline over time. At variance, CRP tended to fall from baseline to median day of hospitalization in all four subgroups, but steeply increased at the end of hospitalization only in ICU-admitted patients.
As shown in Figure 2, admission to ICU occurred within an interval corresponding to the peak of CRP, while death occurred within the interval in which the maximum peak of NLR was observed.
The correlation between NLR and P/F was not statistically significant in ICU-admitted patients (ρ = -0.03 p = 0.7203, Figure 3a), but resulted significant in deceased patients (ρ = -0.26 p = 0.0025; Figure 3b). An opposite phenomenon was observed in the correlation between CRP and P/F ratio in the two subgroups identifying the outcome (ρ = -0.24, p = 0.0129; ρ = -0.13 p = 0.865) (Figure 3c,d).
Furthermore, we analysed these relationships using multiple linear regression analysis, being P/F ratio the dependent variable, and then using univariate and multivariate logistic regression analyses with single outcomes as dependent variable (Table 2 and Table 3). All multivariate regression models were adjusted for age, sex, and comorbidities.
In the multiple linear regression model (Table 2) adjusted for age, sex, and comorbidities, NLR and CRP significantly predicted P/F in both whole population and in survivors, while only CRP predicted P/F in ICU-admitted patients; conversely, only NLR predicted P/F in deceased patients.
In Cox proportional hazard regression, NLR predicted mortality independently of CRP, which did not result statistically significant, and other confounders. ICU admission was significantly associated with both biomarkers, although CRP showed a higher HR, a more significant p value, and a more restricted confidence interval (Table 3).
Based on our results, showing that NLR and CRP are differently associated with P/F in deceased and ICU-admitted patients, we wondered whether the relationship between CRP and P/F could be mediated by another variable that could partly explains why CRP has a greater weight than NLR in influencing P/F in ICU patients, with no significant association with P/F in deceased patients.
Observing the trend of NLR over time, we used as mediating variables the two cell populations from which it is calculated, namely absolute neutrophil and lymphocyte counts. We first demonstrated by repeated measures ANOVA that the mean levels of neutrophils and lymphocytes differed significantly in the various time intervals, comparing patients grouped for outcome (Figure 4).
Finally, mediation analysis was made to examine the mediating effect of neutrophils, lymphocytes, and age on the relationship between CRP and P/F. Age, ANC, CRP and Lymphocytes significantly and directly influenced P/F, while the influence of CRP on P/F was also mediated by ANC, with no mediating effect of lymphocytes and age (Figure 5).
In Table 4 are shown details of the significant indirect effect of CRP on P/F, mediated by neutrophils (b= -0.035, p=0.001).
Furthermore, the direct effect of CRP on P/F in presence of the neutrophils as mediator was stronger (83.7 %; b = -2.849 p < 0.001), as compared to indirect effect mediated by neutrophils (16.3%; b-0.035; p=0.001). Hence, these results suggest that neutrophils partially mediated the relationship between CRP and P/F.
4. Discussion
To the best of our knowledge this is the first study evaluating the pathways of main immuno-inflammatory circulating biomarkers, as well as their direction, in COVID-19 patients. Of note, we also demonstrated the relationships between two markers we have already described as prognostic factors in COVID-19 patients[14], namely NLR and CRP, with P/F, that is in turn a marker of respiratory failure secondary to respiratory distress .
Type 1 respiratory failure in COVID-19 patients is characterized by high compliance and a lack of apparent respiratory distress, at least in the early phase, also known as silent hypoxemia[5]. This could lead to an underestimation of the disease’s severity, and could seriously impact on decision-making, so delaying ICU admission. Consequently, emergency departments are facing a sneaky clinical scenario, sometimes leading to underestimate disease severity.
Recently Sinatti et al.[15] highlighted the potential of PaO2/FiO2 in predicting pneumonia progression towards ARDS in COVID-19 patients.
Of note, the acute respiratory failure in COVID-19 is characterized by a specific pathological substrate: the primum movens is endothelial damage, as a consequence of the hyperinflammatory state, with a massive cytokine and immune cell storm. In this direction, ARDS is the first result of V/Q mismatch due to a vascular damage[16]. In this respect, recent studies have highlighted the link between inflammation, arterial stiffening, and cardiovascular events[17]. In this direction, our group [18] recently demonstrated the stiffening of elastic arteries following COVID-19 infection, followed by partial regression in survivors, in contrast to the higher brachial-ankle pulse wave velocity (PWV) shown in deceased.
Overall, mechanisms underlying the close connection between respiratory failure and systemic inflammation are still under debate. We aimed to investigate this link in order to identify the time-course and dynamics of release of inflammatory substances and activation of immune system during hospitalization, that should be considered an alarm bell.
Laboratory abnormalities have been linked to adverse outcomes in COVID-19 patients. In our previous study[14], we assessed the predictive value of inflammatory biomarkers, such as NLR and CRP, on mortality and severe COVID-19 disease by examining their trends during hospitalization. In our previous study we demonstrated the different CRP and NLR behaviour, as related to mortality and ICU admission.
In the present study we attempted to understand whether these two biomarkers are differently involved in determining outcome and to identify the relationships, if any, between both CRP and NLR with P/F ratio. We demonstrated for the first time the influence of CRP and NLR on P/F, so giving ground to the concept that a derangement in host immune-inflammatory response can influence disease severity.
CRP is a non-specific acute phase protein, induced by IL-6 in the liver, and a sensitive biomarker of inflammation, infection and tissue damage. The increase of CRP levels generally starts as early as 4-8 hours after the initiation of the inflammatory process and peaks at 48 hours, although the duration of this peak is variable, and directly proportional to the stimulus persistence, with a half-life of about 19 hours[19]. The higher CRP levels observed in COVID-19 patients requiring intensive treatment is the consequence of systemic hyper-inflammatory state occurring in severe COVID-19 cases[20]. Despite its low specificity, CRP is an helpful marker in a lot of acute conditions characterized by inflammation/infection[12], and its elevation was shown to be associated with a bad outcome in cardiovascular diseases[21,22]. It is crucial to emphasize, in this respect, the functional role of CRP in the inflammatory process, aimed at recruiting complement components, with positive feedback on inflammation, especially involving endothelium[23,24,25]. In COVID-19 patients CRP has been already described as bad outcome predictor, together with the cytokines associated with its expression (IL-6, IL-10)[26,27].
In the present study, the prominent peak in NLR (Figure 2A) should be finalized to face the disease. However, the early activation of the innate immune response (increase in neutrophils) and the subsequent fall in lymphocytes (adaptive immune response) characterizes the host response to COVID-19 infection[28].
Lowery et al. [29] described the kinetics of innate immune system, demonstrating that COVID-19 pathophysiology depends on the so-called cytokine storm, with production of cytokines and chemokines (TNF, IL-6, CXCL10, CCL2, CCL5 and IFN-II), and/or the lack of early IFN-I and IFN-III expression. The consequent prolonged activation of the innate immune system and a continuous suppression of lymphocytes release into circulation are main characteristics of COVID-19 disease. An elevated absolute neutrophil count (ANC) has been described as negative predictor of outcome in COVID-19 patients[30,31], so reflecting the hyper-activation of the innate immune response caused by both virus-triggered or cytokine-dependent mechanisms[13]. In particular, neutrophils are involved in platelet activation, over-production of inflammatory cytokines, epithelial and endothelial cells damage, especially through a process named NETsosis, that is a molecular mechanism leading to formation of neutrophil extracellular traps (NETs)[32]. As a matter of fact, an elevated expression of NETs could be associated with death and disease progression in COVID-19 patients[33].
By contrast, adaptative immune response induces a reduction of lymphocyte absolute count in COVID-19, as a consequence of extended TNF-α-induced apoptosis, peripheral consumption, direct ACE-2-cytopathic effect, or through the interaction with CD147[29,34,35,36]. Peripheral lymphopenia in COVID-19 patients has been largely described in recent literature assessing its predictive value for disease severity and mortality[37,38]. In addition, neutrophilia itself leads to a suppression of lymphocytes, through a cytotoxic indirect effect[39,40].
NLR represents the balance between innate and immune response. It readily increases as a consequence of physiological and pathophysiological response to acute stress[29]. NLR may be considered a marker of subclinical inflammation, with higher values in acute exacerbations, such as CAP, COPD, sepsis, cancer and many cardiac diseases[41,42,43,44,45]. It is strictly linked to the immune system derangement and could be used as a predictor of disease severity and mortality, especially in conditions characterized by systemic inflammation, such as COVID-19[14,46,47].
Considering that respiratory failure in COVID-19 is characterized by a strong inflammatory involvement, we sought to identify a potential link between the host response to viral load and severity degree of COVID-19 disease. Some studies have already identified an association between CRP and respiratory failure. Poggiali et al.[48] and Herold et al.[49], in two single-center studies, demonstrated that higher CRP levels are associated with lung function worsening, but data on their time-course throughout hospitalization and their correlation with outcome were lacking. On the other hand, Mueller et al.[50], in a single-center study, showed the temporal relationship between CRP and P/F, without any data referred to outcome.
In a recent study we emphasized that NLR independently predicted mortality and ICU admission in COVID-19 patients, being this prediction abolished after adjustment for P/F[14].
Here we further tested the pathways linking neutrophils, lymphocytes, age and CRP to P/F. In consideration of the differences in the time-course of NLR and CRP between ICU admitted and deceased during hospitalization (Figure 2A,B), we investigated the relationships of these biomarkers with P/F, according to outcome, and found a significant inverse correlation between NLR and P/F in deceased (Figure 3B) and a significant inverse correlation between CRP and P/F in the subgroup of ICU-admitted (Figure 3C).
Furthermore, we corroborated the robustness of these correlations by a multiple linear regression analysis, demonstrating that NLR and CRP significantly predicted P/F in the whole population, while only CRP predicted P/F in ICU-admitted patients, whereas only NLR predicted P/F in deceased patients (Table 2). These findings would imply that inflammation plays a key role in the worsening of respiratory failure, but also that a dysfunction of immune system, as shown by neutrophilia/lymphopenia, would be closely associated with decease.
Clinical implications of our findings look interesting. For each increase of 1 unit of standard deviation of NLR, the risk of mortality increased by 77% in the whole sample. As to ICU admission, NLR and CRP have both a specific weight, especially CRP, whose increment of 1 unit of standard deviation corresponded to a 70% increase in the risk of ICU admission.
Finally, we investigated the pathways and their direction influencing P/F. In this way, we demonstrated that mean levels of neutrophils and lymphocytes, whose absolute counts determine NLR, have a significantly different trend during hospitalization in ICU-admitted and deceased (Figure 4). Besutti et al. [51] have recently reported that persistent lung abnormalities had a link to inflammatory burden, especially to CRP, reflecting the intensity and the duration of inflammatory reaction. In keeping with Besutti’s data [51], we considered the potential influence of neutrophils and lymphocytes in the relationship between CRP, a marker of inflammation, and P/F, a marker of lung function.
We observed that, in the worsening of lung function, CRP had a large direct effect (83.7%) (Tab. 4) on P/F: the higher was CRP at hospital admission, the lower resulted P/F (Figure 5) (path coefficient: - 0.19; p<0.05). Neutrophils significantly mediated the deleterious effect of inflammation on lung function. In fact, neutrophils count indirectly influenced (16.3%) the relationship between CRP and P/F (Table 4, Figure 5). Taken together, these data support the notion that neutrophilia would potentiate the impact of CRP on P/F, therefore paving the way to the need for ICU admission.
To the best of our knowledge, our study is therefore the first to demonstrate some of the pathways, and their direction, involved in the pathogenetic chain of respiratory failure in COVID-19 patients. Of note, we carried out this retrospective survey involving two different centers recruiting a selected cohort of hospitalized COVID-19 patients free of confounders affecting lymphocyte and neutrophil counts and/or serum CRP values.
5. Conclusions
In conclusion, NLR and CRP, that are cheap and widely available tools, show different time-courses during hospitalization in COVID-19 patients, with a characteristic pattern depending on outcome. An imbalance between innate and adaptive immunity (increase in NLR), associated with systemic inflammation (increase in CRP), are linked to deterioration of respiratory function, with a specific prediction of outcome: NLR predicted P/F in deceased patients, whereas CRP predicted P/F only in ICU-admitted patients. The mediation analysis confirmed that CRP, neutrophils, lymphocytes and age are linked with P/F (Figure 5) in the same pathogenetic chain leading to respiratory failure.
Our study has some strengths: the ability to demonstrate in two different centres (a) the different pattern of relationships existing between NLR and CRP with P/F as related to different outcome; (b) the inverse relationship between NLR and CRP with P/F; (c) the immuno-inflammatory pathways revealing the co-participation of CRP and neutrophils in determining lower P/F values. Our study has also limitations: it is retrospective, carried out in patients with homogeneous demographic and clinical characteristics.
Further prospective multi-center studies are needed to better understand this complex pathophysiological chain and also to apply this model in other pathophysiological conditions with an immuno-inflammatory involvement.
Author Contributions
Conceptualization, L.M. and M.R. (Matteo Regolo); methodology, M.R. (Matteo Regolo), A.S. and L.M.; software, A.S.; validation, L.M., A.S. and M.R. (Matteo Regolo); formal analysis, A.S. and M.R. (Matteo Regolo); investigation, M.R. (Matteo Regolo), F.G. and D.F.; resources, L.M.; data curation, M.R. (Matteo Regolo), I.I., F.C., F.G., D.F., P.A., A.L., M.V., B.S., M.C., G.N., M.R. (Mario Russo), N.S. and M.M.; writing—original draft preparation, M.R. (Matteo Regolo) and L.M.; writing—review and editing, L.M. and M.R. (Matteo Regolo); visualization, M.R. (Matteo Regolo); supervision, L.M., P.N. and B.S.; project administration, L.M.; funding acquisition, L.M. All authors have read and agreed to the published version of the manuscript.
Funding
This study was in keeping with the objectives of the project “DEGENER action”, Department of Clinical and Experimental Medicine, University of Catania, Catania, Italy.
Institutional Review Board Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. Ethical review and approval were waived due to the type of the study that is an anonymous observational survey on dataset.
Informed Consent Statement
The study was conducted according to the guidelines of the Declaration of Helsinki. Ethical review and approval were waived due to the type of the study that is an anonymous observational survey on dataset.
Data Availability Statement
The data presented in this study are available on request from the corresponding author.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
| CRP | C-Reactive Protein |
| ICU | Intensive Care Unit |
| NLR | Neutrophil-to-lymphocyte ratio |
| P/F | PaO2/FiO2 ratio |
| CAP | COMMUNITY acquired Pneumonia |
| COPD | Chronic Obstructive Pulmonary Disease |
| V/Q | Ventilation/Perfusion |
References
- da Rosa Mesquita, R.; Francelino Silva, L. C., Jr.; Santos Santana, F. M.; Farias de Oliveira, T.; Campos Alcântara, R.; Monteiro Arnozo, G.; da Silva Filho, E. R.; Galdino dos Santos, A. G.; Oliveira da Cunha, E. J.; Salgueiro de Aquino, S. H.; Freire de Souza, C. D. Clinical manifestations of COVID-19 in the general population: systematic review. Wiener klinische Wochenschrift 2021, 133, 377-382. [CrossRef]
- Zhu, J.; Ji, P.; Pang, J.; Zhong, Z.; Li, H.; He, C.; Zhang, J.; Zhao, C. Clinical characteristics of 3062 COVID-19 patients: a meta-analysis. Journal of medical virology 2020, 92, 1902-1914. [CrossRef]
- Caramaschi, S.; Kapp, M. E.; Miller, S. E.; Eisenberg, R.; Johnson, J.; Epperly, G.; Maiorana, A.; Silvestri, G.; Giannico, G. A. Histopathological findings and clinicopathologic correlation in COVID-19: a systematic Review Modern Pathology 2021, 34(9), 1614-1633. [CrossRef]
- FORCE, ARDS Definition Task, et al. Acute respiratory distress syndrome JAMA 2012, 307(23), 2526-2533. [CrossRef]
- Gattinoni, L.; Chiumello, D.; Caironi, P.; Busana, M.; Romitti, F.; Brazzi, L.; Camporota L. COVID-19 pneumonia: different respiratory treatments for different phenotypes? Intensive Care Med 2020, 46, 1099–1102. [CrossRef]
- Hu, B.; Huang, S.; Yin, L. The cytokine storm and COVID-19. Journal of medical virology 2021, 93, 250– 256. [CrossRef]
- Vaninov, N. In the eye of the COVID-19 cytokine storm. Nat. Rev. Immunol. 2020, 20, 277. [CrossRef]
- Yang, L.; Xie, X.; Tu, Z.; Fu J.; Xu D.; Zhou Y. The signal pathways and treatment of cytokine storm in COVID-19 Sig. Transduct. Target Ther. 2021, 6, 255. [CrossRef]
- Xu, Z.; Shi L.; Wang Y.; Zhang J.; Huang L.; Zhang C.; Liu S.; Zhao P.; Liu H.; Zhu L. et al. Pathological findings of COVID-19 associated with acute respiratory distress syndrome. The Lancet respiratory medicine 2020, 8, 420-422. [CrossRef]
- Ou, M.; Zhu, J.; Ji, P.; Li, H.; Zhong, Z.; Li, B.; Pang, J.; Zhang, J.; Zheng, X. Risk factors of severe cases with COVID-19: a meta-analysis. Epidemiology and infection 2020 148, e175. [CrossRef]
- Wolff, D.; Nee, S.; Hickey, N.S.; Marschollek M. Risk factors for Covid-19 severity and fatality: a structured literature review Infection 2021, 49, 15–28. [CrossRef]
- Clyne, B.; Olshaker, J.S. The C-reactive protein. J Emerg Med. 1999, 17(6), 1019-1025. [CrossRef]
- Zahorec R. Neutrophil-to-lymphocyte ratio, past, present and future perspectives. Bratislavske lekarske listy 2021, 122(7), 474–488. [CrossRef]
- Regolo, M.; Vaccaro, M.; Sorce, A.; Stancanelli, B.; Colaci, M.; Natoli, G.; Russo, M.; Alessandria, I.; Motta, M.; Santangelo, N.; et al. Neutrophil-to-Lymphocyte Ratio (NLR) Is a Promising Predictor of Mortality and Admission to Intensive Care Unit of COVID-19 Patients. J. Clin. Med. 2022, 11, 2235. [CrossRef]
- Sinatti, G.; Santini, S.J.; Tarantino, G.; Picchi G.; Cosimini B.; Ranfone F.; Casano N.; Zingaropoli M. A.; Iapadre N.; Bianconi S.; et al. PaO2/FiO2 ratio forecasts COVID-19 patients’ outcome regardless of age: a cross-sectional, monocentric study. Intern Emerg Med 2022, 17, 665–673. [CrossRef]
- Marini, J. J.; Gattinoni, L. Management of COVID-19 respiratory distress Jama 2020 323(22), 2329-2330. [CrossRef]
- Zanoli, L.; Briet, M.; Empana, J. P.; Cunha, P. G.; Mäki-Petäjä, K. M.; Protogerou, A. D.; Tedgui, A.; Touyz, R. M.; Schiffrin, E. L.; Association for Research into Arterial Structure, Physiology (ARTERY) Society, the European Society of Hypertension (ESH) Working Group on Vascular Structure and Function, and the European Network for Noninvasive Investigation of Large Arteries; et al. Vascular consequences of inflammation: a position statement from the ESH Working Group on Vascular Structure and Function and the ARTERY Society. Journal of hypertension 2020, 38(9), 1682–1698. [CrossRef]
- Zanoli, L.; Gaudio, A.; Mikhailidis, D. P.; Katsiki, N.; Castellino, N.; Lo Cicero, L.; Geraci, G.; Sessa, C.; Fiorito, L.; Marino, F.; et al. Vascular Dysfunction of COVID-19 Is Partially Reverted in the Long-Term. Circulation research 2022, 130(9), 1276–1285. [CrossRef]
- Pepys, M.B.; Hirschfield, G.M. C-reactive protein: a critical update [published correction appears in J Clin Invest. 2003 Jul;112(2):299]. J Clin Invest. 2003,111(12),1805-1812. [CrossRef]
- Gustine, J.N.; Jones, D. Immunopathology of Hyperinflammation in COVID-19. Am J Pathol. 2021, 191(1), 4-17. [CrossRef]
- Haverkate, F.; Thompson, S.G.; Pyke, S.D.; Gallimore, J.R.; Pepys, M.B. Production of C-reactive protein and risk of coronary events in stable and unstable angina. European Concerted Action on Thrombosis and Disabilities Angina Pectoris Study Group. Lancet 1997, 349(9050), 462-466. [CrossRef]
- Ridker, P.M.; Rifai, N.; Rose, L.; Buring, J.E.; Cook, N.R. Comparison of C-reactive protein and low-density lipoprotein cholesterol levels in the prediction of first cardiovascular events. N Engl J Med. 2002, 347(20), 1557-1565. [CrossRef]
- Sproston, N.R.; Ashworth, J.J. Role of C-Reactive Protein at Sites of Inflammation and Infection. Front Immunol. 2018, 9:754. Published 2018 Apr 13. [CrossRef]
- Mold, C.; Gewurz, H.; Du Clos, T.W. Regulation of complement activation by C-reactive protein. Immunopharmacology 1999, 42(1-3), 23-30 . [CrossRef]
- Buono, C.; Come, C.E.; Witztum, J.L.; Maguire, G.F.; Connelly P.W.; Carroll, M.; Lichtman, A.H. Influence of C3 deficiency on atherosclerosis. Circulation 2002, 105(25), 3025-3031. [CrossRef]
- Ahnach, M.; Zbiri, S.; Nejjari, S.; Ousti, F.; Elkettani, C. C-reactive protein as an early predictor of COVID-19 severity Journal of medical biochemistry 2020, 39(4), 500–50. [CrossRef]
- Han, H.; Ma, Q.; Li, C.; Liu, R.; Zhao, L.; Wang, W.; Zhang, P.; Liu, X.; Gao, G.; Liu, F.; Jiang, Y.; Cheng, X.; Zhu, C.; Xia, Y. Profiling serum cytokines in COVID-19 patients reveals IL-6 and IL-10 are disease severity predictors Emerging microbes & infections 2020, 9(1), 1123–1130 . [CrossRef]
- Tirelli, C.; De Amici, M.; Albrici, C.; Mira, S.; Nalesso, G.; Re, B.; Corsico, A.G.; Mondoni, M.; Centanni, S. Exploring the Role of Immune System and Inflammatory Cytokines in SARS-CoV-2 Induced Lung Disease: A Narrative Review. Biology 2023, 12, 177. [CrossRef]
- Lowery, S. A.; Sariol, A.; Perlman, S. Innate immune and inflammatory responses to SARS-CoV-2: Implications for COVID-19. Cell Host & Microbe 2021, 29(7), 1052-1062. [CrossRef]
- Zhou, F.; Yu, T.; Du, R.; Fan, G.; Liu, Y.; Liu, Z.; Xiang, J.; Wang, Y.; Song, B.; Gu, X.; et al. Clinical course and risk factors for mortality of adult inpatients with COVID-19 in Wuhan, China: a retrospective cohort study [published correction appears in Lancet. 2020 Mar 28;395(10229):1038] [published correction appears in Lancet. 2020 Mar 28;395(10229):1038]. Lancet 2020, 395(10229), 1054-1062. [CrossRef]
- Del Valle, D. M.; Kim-Schulze, S.; Huang, H. H.; Beckmann, N. D.; Nirenberg, S.; Wang, B.; Lavin, Y.; Swartz, T. H.; Madduri, D.; Stock, A.; et al. An inflammatory cytokine signature predicts COVID-19 severity and survival. Nature medicine 2020, 26(10), 1636–1643. [CrossRef]
- Vorobjeva, N. V.; Chernyak, B. V. NETosis: molecular mechanisms, role in physiology and pathology. Biochemistry (Moscow) 2020, 85, 1178-1190. [CrossRef]
- González-Jiménez, P.; Méndez, R.; Latorre, A.; Piqueras, M.; Balaguer-Cartagena, M.N.; Moscardó, A.; Alonso, R.; Hervás, D.; Reyes, S.; Menéndez, R. Neutrophil Extracellular Traps and Platelet Activation for Identifying Severe Episodes and Clinical Trajectories in COVID-19. Int. J. Mol. Sci. 2023, 24, 6690. [CrossRef]
- Liao, Y.C.; Liang, W.G.; Chen, F.W.; Hsu, J.H.; Yang, J.J.; Chang, M.S. IL-19 induces production of IL-6 and TNF-alpha and results in cell apoptosis through TNF-alpha. Journal of Immunology (Baltimore, MD: 1950), 2002, 169(8), 4288–4297. [CrossRef]
- Xu, H.; Zhong, L.; Deng, J.; Peng, J.; Dan, H.; Zeng, X.; Li, T.; Chen, Q. High expression of ACE2 receptor of 2019-nCoV on the epithelial cells of oral mucosa. International Journal of Oral Science 2020, 12(1), 8–5. [CrossRef]
- Helal, M. A.; Shouman, S.; Abdelwaly, A.; Elmehrath, A. O.; Essawy, M.; Sayed, S. M.; Saleh, A,H.; El-Badri, N. Molecular basis of the potential interaction of SARS-CoV-2 spike protein to CD147 in COVID-19 associated-lymphopenia. Journal of Biomolecular Structure and Dynamics, 2022, 40(3), 1109-1119. [CrossRef]
- Tan, L.; Wang, Q.; Zhang, D.; Ding, J.; Huang, Q.; Tang, Y. Q.; Wang, Q.; Miao, H. Lymphopenia predicts disease severity of COVID-19: a descriptive and predictive study. Signal transduction and targeted therapy 2020, 5(1), 33. [CrossRef]
- Qin, C.; Zhou, L.; Hu, Z.; Zhang, S.; Yang, S.; Tao, Y.; Xie, C.; Ma, K.; Shang, K.; Wang, W.; Tian, D. S. Dysregulation of Immune Response in Patients with Coronavirus 2019 (COVID-19) in Wuhan, China. Clinical infectious diseases: an official publication of the Infectious Diseases Society of America, 2020 71(15), 762–768. [CrossRef]
- Petrie, H. T.; Klassen, L. W.; Kay, H. D. Inhibition of human cytotoxic T lymphocyte activity in vitro by autologous peripheral blood granulocytes. Journal of immunology (Baltimore, Md.: 1950) 1985, 134(1), 230-234. [CrossRef]
- El-Hag, A.; Clark, R. A. Immunosuppression by activated human neutrophils. Dependence on the myeloperoxidase system Journal of immunology (Baltimore, Md.: 1950), 1987, 139(7), 2406-2413. [CrossRef]
- Cataudella, E.; Giraffa, C. M.; Di Marca, S.; Pulvirenti, A.; Alaimo, S.; Pisano, M.; Terranova, V.; Corriere, T.; Ronsisvalle, M. L.; Di Quattro, R.; Stancanelli, B.; Giordano, M.; Vancheri, C.; Malatino, L. Neutrophil-To-Lymphocyte Ratio: An Emerging Marker Predicting Prognosis in Elderly Adults with Community-Acquired Pneumonia. Journal of the American Geriatrics Society 2017, 65(8), 1796–1801. [CrossRef]
- Paliogiannis, P.; Fois, A. G.; Sotgia, S.; Mangoni, A. A.; Zinellu, E.; Pirina, P.; Negri, S.; Carru, C.; Zinellu, A. Neutrophil to lymphocyte ratio and clinical outcomes in COPD: recent evidence and future perspectives. European respiratory review: an official journal of the European Respiratory Society, 2018, 27(147), 170113. [CrossRef]
- Liu, S.; Wang, X.; She, F.; Zhang, W.; Liu, H.; Zhao, X. Effects of Neutrophil-to-Lymphocyte Ratio Combined With Interleukin-6 in Predicting 28-Day Mortality in Patients With Sepsis Frontiers in immunology 2021, 12, 639735. [CrossRef]
- Cupp, M. A.; Cariolou, M.; Tzoulaki, I.; Aune, D.; Evangelou, E.; Berlanga-Taylor, A. J. Neutrophil to lymphocyte ratio and cancer prognosis: an umbrella review of systematic reviews and meta-analyses of observational studies BMC medicine 2020, 18(1), 360. [CrossRef]
- Afari, M. E.; Bhat, T. Neutrophil to lymphocyte ratio (NLR) and cardiovascular diseases: an update. Expert review of cardiovascular therapy 2016, 14(5), 573–577. [CrossRef]
- Buonacera, A.; Stancanelli, B.; Colaci, M.; Malatino, L. Neutrophil to Lymphocyte Ratio: An Emerging Marker of the Relationships between the Immune System and Diseases. Int. J. Mol. Sci. 2022, 23, 3636. [CrossRef]
- Yang, A. P.; Liu, J. P.; Tao, W. Q.; Li, H. M. The diagnostic and predictive role of NLR, d-NLR and PLR in COVID-19 patients 2020, International immunopharmacology, 84, 106504. [CrossRef]
- Poggiali, E.; Zaino, D.; Immovilli, P.; Rovero, L.; Losi, G.; Dacrema, A.; Nuccetelli, M.; Vadacca, G. B.; Guidetti, D.; Vercelli, A.; Magnacavallo, A.; Bernardini, S.; Terracciano, C. Lactate dehydrogenase and C-reactive protein as predictors of respiratory failure in CoVID-19 patients. Clinica chimica acta; international journal of clinical chemistry, 509 2020, 135–138. [CrossRef]
- Herold, T.; Jurinovic, V.; Arnreich, C.; Lipworth, B. J.; Hellmuth, J. C.; von Bergwelt-Baildon, M.; Klein, M.; Weinberger, T. Elevated levels of IL-6 and CRP predict the need for mechanical ventilation in COVID-19 The Journal of allergy and clinical immunology 2020, 146(1), 128–136.e4. [CrossRef]
- Mueller, A. A.; Tamura, T.; Crowley, C. P.; DeGrado, J. R.; Haider, H.; Jezmir, J. L.; Keras, G.; Penn, E. H.; Massaro, A. F.; Kim, E. Y. Inflammatory Biomarker Trends Predict Respiratory Decline in COVID-19 Patients Cell reports. Medicine, 2020, 1(8), 100144. [CrossRef]
- Besutti, G.; Giorgi Rossi, P.; Ottone, M.; Spaggiari, L.; Canovi, S.; Monelli, F.; Bonelli, E.; Fasano, T.; Sverzellati, N.; Caruso, A.; et al. Inflammatory burden and persistent CT lung abnormalities in COVID-19 patients Scientific reports, 2022, 12(1), 4270. [CrossRef]
Figure 1.
Flow chart of the protocol and subsets of patients divided for outcome.
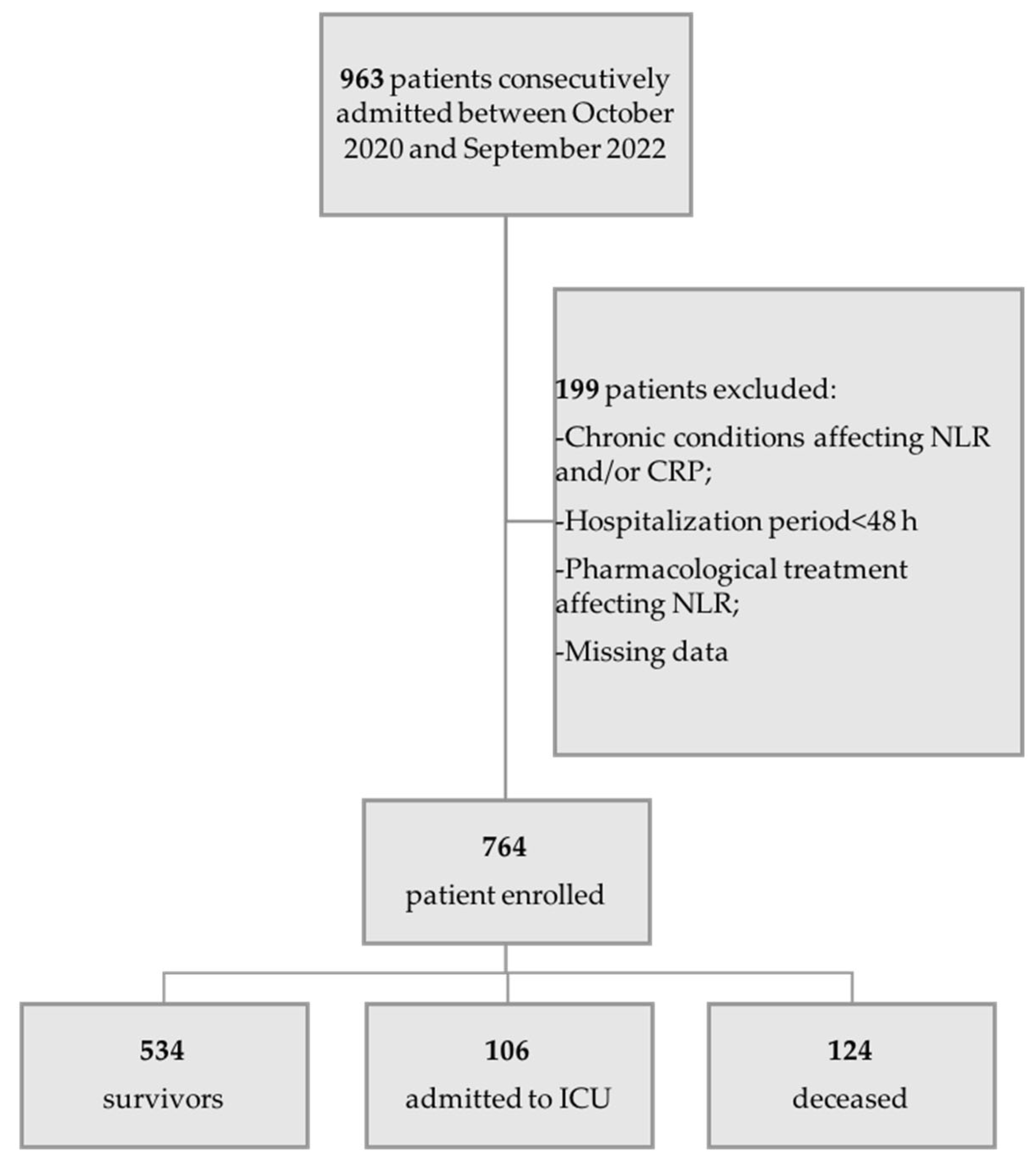
Figure 2.
Time-course of mean values of NLR (Panel A) and CRP (Panel B) in the whole sample (blue line), in survivors (orange line), deceased (yellow line) and ICU-admitted patients (grey line) during hospitalization.
Figure 2.
Time-course of mean values of NLR (Panel A) and CRP (Panel B) in the whole sample (blue line), in survivors (orange line), deceased (yellow line) and ICU-admitted patients (grey line) during hospitalization.
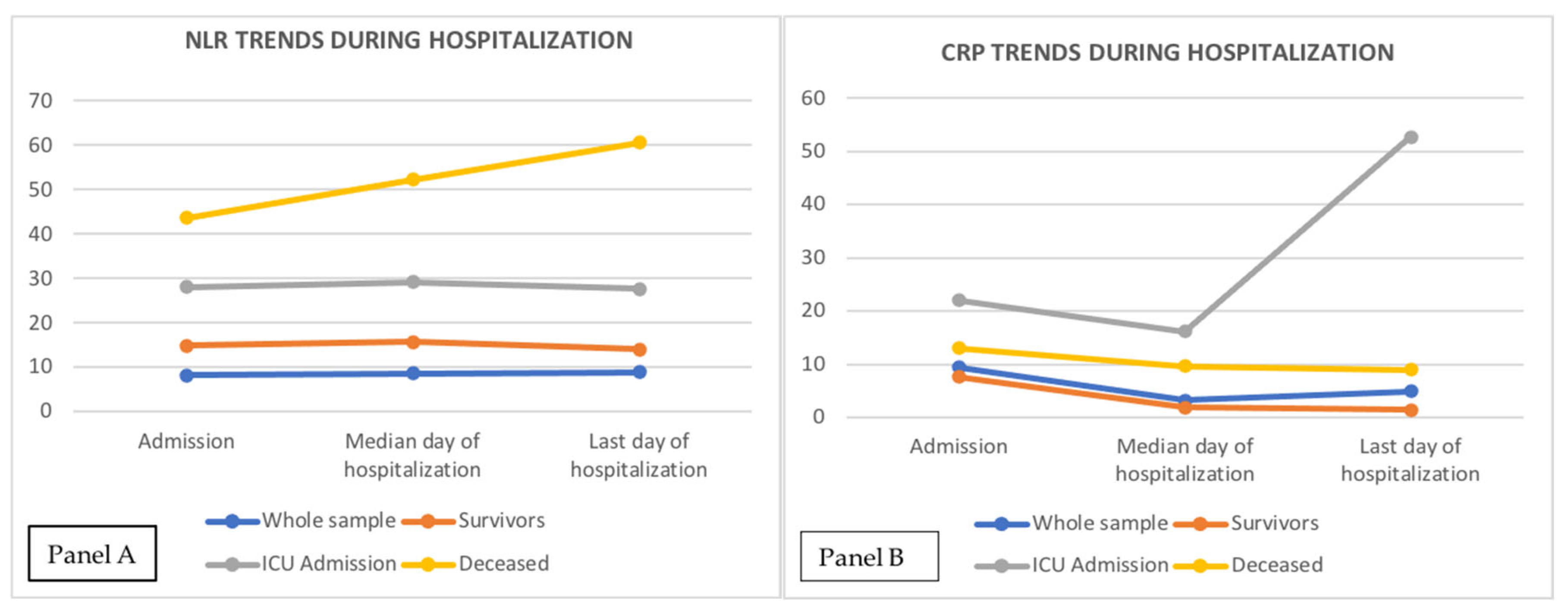
Figure 3.
Pattern of relationships between NLR and CRP and P/F with different outcome (Panel a: NLR and P/F in ICU-admitted; Panel b: NLR and P/F in deceased; Panel c: CRP and P/F in ICU-admitted; Panel d: CRP and P/F in deceased).
Figure 3.
Pattern of relationships between NLR and CRP and P/F with different outcome (Panel a: NLR and P/F in ICU-admitted; Panel b: NLR and P/F in deceased; Panel c: CRP and P/F in ICU-admitted; Panel d: CRP and P/F in deceased).
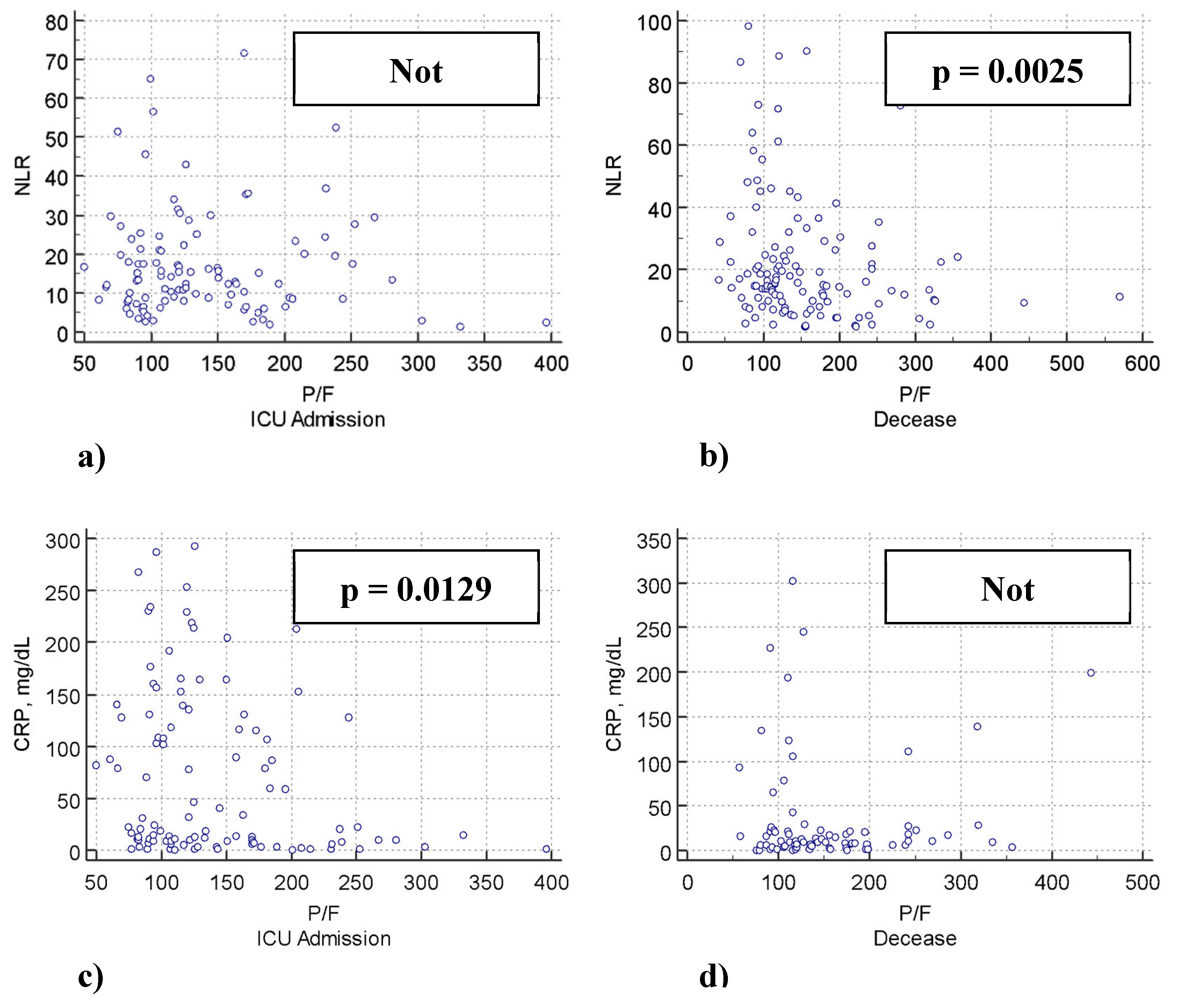
Figure 4.
Repeated measures ANOVA clustered by outcome groups. Bars represent 95% confidence intervals (CI). ANC: Absolute Neutrophil Count; T0: baseline; T1: median day; T2: last day of hospitalization. *Significant variation between groups (p<0.001).
Figure 4.
Repeated measures ANOVA clustered by outcome groups. Bars represent 95% confidence intervals (CI). ANC: Absolute Neutrophil Count; T0: baseline; T1: median day; T2: last day of hospitalization. *Significant variation between groups (p<0.001).
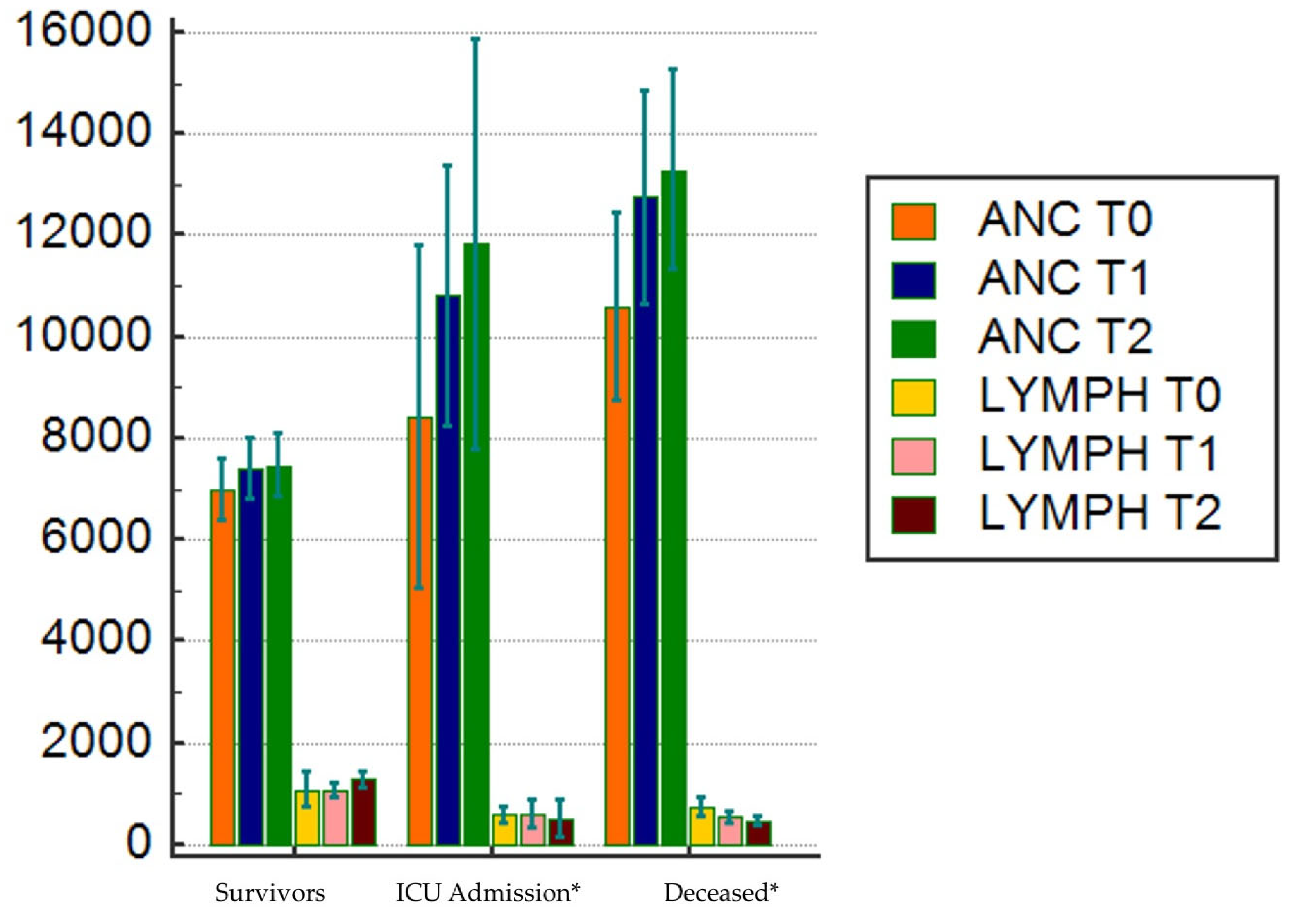
Figure 5.
Path analysis performed in 764 patients with COVID-19 using a path weighting scheme. Effect of neutrophils, lymphocytes, CRP and age on P/F ratio. Age, neutrophils, lymphocytes and CRP were included as independent variables; neutrophils, lymphocytes and age had a dual relationship as both dependent and moderator variables; P/F was the dependent variable. Significant (*p<0.05) direct effects are reported as continuous black lines; nonsignificant direct effects are reported as dotted lines. Arrows indicate the direction of the effects tested in the model. r2 indicates the variance explained by the model.
Figure 5.
Path analysis performed in 764 patients with COVID-19 using a path weighting scheme. Effect of neutrophils, lymphocytes, CRP and age on P/F ratio. Age, neutrophils, lymphocytes and CRP were included as independent variables; neutrophils, lymphocytes and age had a dual relationship as both dependent and moderator variables; P/F was the dependent variable. Significant (*p<0.05) direct effects are reported as continuous black lines; nonsignificant direct effects are reported as dotted lines. Arrows indicate the direction of the effects tested in the model. r2 indicates the variance explained by the model.
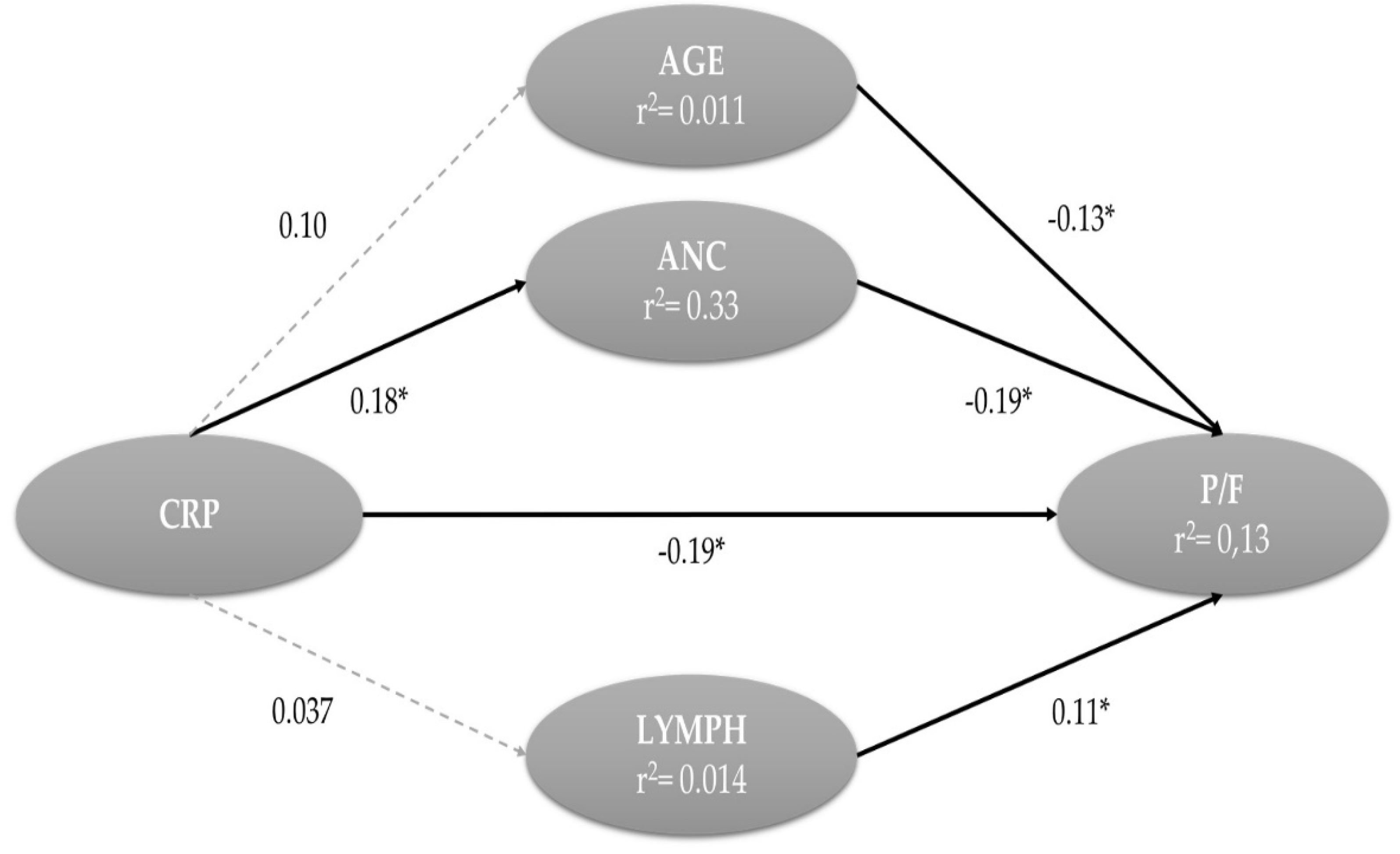

Table 1.
Main demographic and clinical features of whole sample and subsets of patients (T0=Admission; T1= Median day of hospitalization; T2= Last day of hospitalization).
Table 1.
Main demographic and clinical features of whole sample and subsets of patients (T0=Admission; T1= Median day of hospitalization; T2= Last day of hospitalization).
| TOTAL n=764 |
SURVIVORS n=534 |
ICU ADMISSION n=106 |
DECEASED n=124 |
p | |
|---|---|---|---|---|---|
| Age, years | 74 (72-75) | 71 (69-73) | 71 (67-73) | 85 (84-86) | < 0.000001 (1-2, 3) |
| Male sex, n (%) | 412 (54.1) | 282 (68.2) | 69 (16.7) | 61 (14.8) | 0.019 (1,2,3) |
| Lymph, 109/L | 800 (718 – 800) | 900 (800-900) | 581 (506-820) | 600 (500-671) | < 0.000001 (1,2) |
| Anc, 109/L | 6500 (6200-6800) | 5900 (5600-6300) | 7500 (6760-8927) | 9000 (7500-9039) | < 0.000001 (1,2,3) |
| P/F Ratio | 206 (198 – 224) | 258 (241-272) | 171(121-133) | 128 (117-146) | < 0.000001 (1,2,3) |
| NLR T0 | 8.18 (7.7 – 8.9) | 6.7 (6.2-7.3) | 13.2 (11.1-15.8) | 15.5 (13.6-18.6) | < 0.000001 (1,2) |
| NLR T1 | 8.7 (7.8 – 9.7) | 7 (6.1-7.8) | 13.5 (11-16) | 23 (17.8-31.3) | < 0.000001 (1,2,3) |
| NLR T2 | 8.9 (8.6-10.5) | 5.2 (4.5-5.3) | 13.5 (12.4-22.4) | 33 (22.6-41,7) | < 0.000001 (1,2,3) |
| CRP T0, mg/dL | 9.4 (8.4-10.6) | 7.7 (6.2-8.7) | 22 (12.8-73.8) | 13 (9.3-15.5) | < 0.000001 (1,2,3) |
| CRP T1, mg/dL | 3.3 (2.5-4.5) | 1.9 (1.4-2.4) | 16.2 (8.5-25) | 9.7 (6.9-11) | < 0.000001 (1,2,3) |
| CRP T2, mg/dL | 4.9 (3-6.6) | 1.5 (1.3-2.2) | 52.7 (22.4-101) | 10 (8.1-16.8) | < 0.000001 (1,2,3) |
| Length of stay, days | 9 (8-10) | 10 (10-11) | 4 (3-5) | 8 (7-9) | < 0.000001 (1,2,3) |
|
Comorbidities Hypertension n (%) Diabetes, n (%) CKD, n (%) COPD, n (%) CV disease, n (%) |
457 (62.5) 334 (43.9) 166 (21.7) 107 (13.8) 297 (25.7) |
306 (57) 221 (41) 105 (19) 82 (15) 198 (37) |
68 (64) 47 (44) 30 (28) 11 (10) 47 (44) |
83 (66) 66 (53) 31 (25) 14 (11) 52 (41) |
0.09 0.06 0.082 0.252 0.279 |
Outcome resulted statistically different (p < 0.01) from baseline, at median time and at the end of hospitalization.
Table 2.
Multiple linear regression adjusted for age, sex and comorbidities according to outcome.
| Dependent Variable P/F ratio | WHOLE POPULATION | SURVIVORS | ICU ADMISSION | DECEASED | ||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|
| β | r | p | β | r | p | β | r | p | β | r | p | |
| NLR | -1.91 | - 0.22 | <0.0001 | -1.68 | -0.13 | 0.002 | -0.35 | -0.007 | 0.438 | -0.84 | -2.2 | 0.023 |
| CRP | -0.5 | -0.27 | <0.0001 | -0.65 | -0.24 | <0.0001 | -0.19 | -0.23 | 0.015 | -0.15 | -1.5 | 0.134 |
Table 3.
Univariable and multivariable Cox regression models adjusted for sex, age and comorbidities. *HR obtained using NLR and CRP z-scores.
Table 3.
Univariable and multivariable Cox regression models adjusted for sex, age and comorbidities. *HR obtained using NLR and CRP z-scores.
| DEPENDENT VARIABLE: DECEASE | ||||
| HR univariable | p | HR multivariable | p | |
| NLR | 1.05 (2.01*) [1.0406 – 1.0709] |
<0.0001 | 1.04 (1.77*) [1.0295 – 1.0618] |
<0.0001 |
| CRP | 1.002 [0.9996 – 1.0058] |
0.0879 | 1.002 (1.001*) [0.9994 – 1.0063] |
0.1081 |
| DEPENDENT VARIABLE: ICU ADMISSION | ||||
| HR univariable | p | HR multivariable | p | |
| NLR | 1.02 (1.4*) [1.0127 – 1.0390] |
0.0001 | 1.02 (1.39*) [1.0117 – 1.0419] |
0.002 |
| CRP | 2.66 [2.4315 – 3.1368] |
<0.0001 | 2.4 (1.7*) [1.922 – 2.615] |
<0.0001 |
Table 4.
Joint assessment of the direct effect of CRP on P/F and the mediation of neutrophils.
| 95% Confidence Interval | |||||||||||||||
|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|---|
| Effect | Estimate | SE | Lower | Upper | Z | p | % Mediation | ||||||||
| Indirect | -0.035 | 0.174 | -0.940 | -0.251 | -3.19 | 0.001 | 16.3 | ||||||||
| Direct | -2.849 | 0.640 | -4.153 | -1.583 | -4.45 | < 0.001 | 83.7 | ||||||||
| Total | -3.404 | 0.672 | -4.678 | -2.112 | -5.07 | < 0.001 | 100.0 | ||||||||
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



