
Submitted:
11 May 2023
Posted:
11 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
(1) Background: Our paper aimed to examine the ways in which the care centers for the elderly acted and adapted during the pandemic period, by taking into account the opinions of the beneficiaries, of the employees and of the managers of those centers. (2) Methods: in order to conduct the research we used a mixed-method approach. Considering the quantitative research, we applied a questionnaire to 430 institutionalized elderly from Timis county, Romania. Considering the qualitative analysis, we conducted interviews with 31 institutionalized elderly, with 7 employees and 4 managers. (3) Results: most institutionalized elderly were mainly satisfied with their life in the care centers, the main difficulties they had were: the impossibility of being close to loved ones, and the difficulty of adapting to the living conditions within the center, and the elderly were satisfied with the interactions they had with the staff of the care centers. (4) Conclusions: the research conducted provides a view on the lifestyle of the elderly from care centers during the pandemic, it highlights the struggles of the elderly and it can be used as a point of reference for the further improvement of the lifestyle of the elderly within the care centers.
Keywords:
elderly
; care centers
; COVID-19
; lifestyle
1. Introduction
The decision to institutionalize an elderly person is based on several reasons, including his advanced age, the lack or small number of children, the deterioration of the home or its inaccessibility, cognitive disorders or the absence of the spouse [1].Although the elderly avoid institutionalization, preferring as much as possible to live in the community, in their houses, the transition to a nursing home becomes an option when the state of health worsens, when physical and cognitive impairments appear and, implicitly, the needs of palliative care, specialized care. Added to these are situations in which family members cannot take care of the person in need, especially if they are also elderly or have other obligations that do not allow them to get involved [2].
For the elderly, the house is more than a residence, because they feel deeply connected to it, they feel safe, they have familiar objects and a community with common principles and values, a fact that helps them always find resources, resist more easily in the face of risks. This is also the reason why the elderly want to stay at home as much as possible and even spend their last years there [3].
In what regards the advantages, residential centers for the elderly offer them a safe and hygienic environment, medical care, food and protection from possible abuse suffered at home. On the other hand, the disadvantages consist of social exclusion, excessive sadness, the impossibility of establishing solid social relationships, the diminution or even loss of communication skills [4].
The elderly person's transition to a nursing home causes other family members to redefine their roles, control and involvement in care diminishing with this move. However, in addition to the reduction of burdens, they may also feel a sense of guilt caused by the decision to institutionalize. However, they can still monitor the care received by the elderly, provide feedback to the staff, but also effectively contribute to their care and maintain the beneficiary's connection with the outside world [2].
At the same time, this transition also associates several changes for the beneficiary, especially on the style and quality of life. Institutionalization can therefore increase the degree of vulnerability of the elderly who are prone to experience, in addition to loneliness, functional impairments or depression [1].
Although the Covid 19 pandemic affected all socio-demographic groups, scientific evidence has shown that advanced age is a risk factor associated with a higher lethality of the virus [5]. Not only did the direct contact with the virus make them more vulnerable, but also the indirect effects of social isolation, embodied in loneliness, limited access to medical services, limited social relationships and reduced accessibility to community life [6]. However, due to the comorbidities and frailty that characterize them, the institutionalized elderly represented one of the most vulnerable populations to the morbidity and mortality of the SARS COV 2 virus [2].
Among the measures adopted by residential centers for the elderly in order to limit the spread of the SARS COV 2 virus were the prohibition of group activities, the limitation of movements outside the premises and isolation in their own rooms [7], the efficient distribution of residents in space ( avoiding overcrowding), establishing hygiene measures, cleaning and disinfecting spaces and devices, control policies and management of infected people [5], canceling all social activities and restricting all visits [8]. Thus, the staff of residential centers for the elderly became solely responsible for the transmission of the virus to the residents [9].
Basically, once all the measures to prevent the spread of the virus were put in place, social relations with other residents, staff and family members, and informal care from the relatives was limited [10].
Thus, as a result of physical isolation and the impossibility of using common residential spaces, the institutionalized elderly felt the physical, psychological and cognitive consequences, exacerbating a pressing pre-existing problem, namely loneliness. Derived clinical effects consisted of weight loss, the appearance of depressive symptoms, deterioration of cognitive functions, insomnia, but also increased frailty, a consequence of the lack of mobility [5].Even though adults naturally become frailer and less mobile as they age, the excess sedentariness caused by the COVID 19 restrictions has drastically increased the rate of this decline. In addition, these restrictions constituted a barrier to leisure activities for residents. Even though occupational employment plays an important role in residential centers for the elderly in the sense that they favor the psychosocial well-being and dignity of the beneficiaries, the latter have been forced to spend passive time in their rooms with reduced opportunities for occupational stimulation [10].
Beneficiary families have tried to adopt various support strategies embodied in various ways of remote care: delivering essential items to the elderly, staying connected through technology, visiting outside with social distancing or behind a glass partition. All of these, however, have been shown to be ineffective for residents with cognitive impairments or those with vision and hearing impairments [2].
Even if they could not fully compensate for physical visits, alternative ways of contacting the family, namely phone calls, video calls, e-mails or letters, proved useful in the sense that they positively influenced the emotional well-being of residents [7]. Despite the fact that video calling may be inappropriate for elderly people with dementia, for instance, this form of digital contact has been found to reduce agitation and anxiety in these residents [10]. Another study, [11], reinforces this idea, appreciating that the frequency of communication is directly proportional to resident satisfaction. Thus, social support, embodied in the present situation in telephone or video calls, lessened the negative effects of isolation on mental health. More, the support thus received helped them in the sense that they felt listened to and protected.
Thus, in order to support the residents, employees helped them use technology, namely electronic devices, to keep in touch with their family. However, the digital gap between generations has made communication very difficult, a fact that has exacerbated feelings of isolation and loneliness [1]. Also, the reduced staff and its overload during the COVID 19 pandemic constituted a barrier to alternative means of communication, which is why, in most cases, the digital contact between the beneficiary and the family ceased after the restrictions were lifted [7].
Despite the dramatic consequences of COVID 19 and, implicitly, the restrictions imposed, the elderly were much more self-confident compared to other age groups, based on a vast life experience. Given the fact that they have experienced, in the past, stressful events and similar moments of crisis, they have developed skills that have led to an increase in the degree of resistance. Thus, if other age groups perceived the pandemic as an element of novelty, the elderly demonstrated greater adaptability [12].
According to [11], nursing home residents paid particular attention to spirituality during the COVID 19 pandemic. Religiosity and spirituality helped the elderly to remain calm and confident, being considered both resources and coping skills, with a positive impact on physical health and mental. Given the fact that the elderly are the people most involved in religious activities, spiritual resources can thus constitute a source of resilience to manage the stressful period of the pandemic [13].
Generically referred to as information disorder, misinformation and fake news have dominated the media scene during the COVID 19 pandemic. The sharing of fake content has called into question both medicine and technology. The fact that the elderly have low experience with digital media makes them more vulnerable and prevents them from detecting manipulative images, clickbait news or any other form of deception [14]. Thus, mass media or traditional media is considered more credible than social media due to the processing of information using journalistic standards, but also due to sources of information that are verifiable. During the COVID 19 pandemic, the news disseminated information related to death, dramatic aspects that generally produced panic and negative effects. On the other hand, news has given less importance to information about prevention, spread control and healthy practices [15].
The fear of infection and the lack of a specific treatment for COVID 19, but also the preconceptions related to the vaccine, caused negative emotions, stress and anxiety. Although age is a critical factor in vaccine acceptance, with older people more willing to be vaccinated, this decision was influenced by information sources. During the COVID 19 pandemic, in addition to the large amount of fake news, there were also conspiracy theories about the disease and the vaccine. Thus, misinformation presented as evidence-based could affect vaccination behavior in the sense that the elderly have a lower ability to differentiate between conventional and fake news [16].
At the same time, social media platforms have spread, in addition to misinformation about the virus, treatment schemes or simple alternative treatments, unscientific remedies and unverified drugs promoted by fake doctors, thus causing people to become negligent, refuse hospitalization and , implicitly, to spread the disease [17]. The media can thus limit government efforts to inform the population during the pandemic, having a substantial impact on subsequent behaviors [18]. Also, the promotion by the mass media of the news that the elderly are almost the only demographic group affected by COVID 19, emphasizing their weakness, created a form of stigmatization and increased the level of psychosocial suffering among them [19].
In addition to increasing care costs, aging also implies diminishing functional abilities and decreasing quality of life. In this regard, occupational therapy can play an important role in maintaining or improving the independence and, implicitly, the mobility of the elderly [20].
Cognitive decline is a problem characteristic of the elderly in the sense that it can produce dementia and, implicitly, can increase the risk of mortality. Although cognitive decline is associated with a low quality of life in the elderly, its contributing factors include hypertension, myocardial infarction, stroke, and depression. On the other hand, balanced food diets based on fruits and vegetables, as well as physical activity are associated with a lower risk of cognitive impairment [21].
At the same time, one of the expressions of aging, considered to be the most visible, is fragility. This is rather a consequence in the sense that it involves the installation of some changes in the physiological systems, the increase of vulnerability and, implicitly, the alteration of the state of health. Repeated falls, disability, dependence on long-term care, hospitalization, but also mortality, are some of the characteristics of the elderly considered to be frail [22,23].
Loneliness is also a risk factor for mortality, with older people feeling this more acutely because of the changes and functional losses associated with aging. If social loneliness refers to the lack or diminution of social relationships or social support, emotional loneliness represents the lack of closeness, of intimacy with another person. The latter is experienced, in particular, by the elderly whose partners have died, which is why they live alone and do not have reliable relationships with other people. However, regardless of its specifics, loneliness has negative consequences on both the mental and physical health of the elderly manifested in depression, increased stress level, sudden mood changes [24]. Thus, loneliness, also defined as an unpleasant subjective state of sensing a discrepancy between the desired amount of affection or emotional support and the one received, is an effect of social isolation, prevalent among the elderly population [25]. In addition to health consequences, loneliness is also associated with malnutrition, sleep disorders (nighttime insomnia and daytime sleepiness), but also with other risky behaviors such as excessive alcohol consumption and tobacco use [26,27].
Although most seniors prefer to remain in the community, in their familiar environment, institutionalization becomes imminent when functional disability or frailty occurs. The latter is defined by weight loss, exhaustion, weakness, slow walking speed and low physical activity. Thus, the chances of institutionalization are up to 5 times higher in the case of the frail elderly, the transition to an asylum can even amplify the loss of autonomy and independence of the elderly [28]. At the same time, institutionalization is a feasible alternative when the elderly person presents a severe cognitive impairment. Professional care, including medical care, can improve the resident's quality of life, on the one hand, and reduce stress and burden on caregivers, on the other [29].
Thus, the decision to institutionalize the elderly requires his relocation and acceptance of a new lifestyle, which is why it proved to be very difficult from an emotional point of view. If for some beneficiaries moving to an asylum is associated with the opportunity to socialize and make new friends, others see it as a loss of freedom and independence. Therefore, given that institutionalization is a stressful event by its nature, elderly people who overestimate their ability to care for themselves at home do not understand the need to move, do not cooperate and have difficulties adapting to the new environment [30].
Another research [31], considers malnutrition and depression to be two major problems that particularly affect the institutionalized elderly, with a prevalence of 60% and 45%, respectively. Thus, undernutrition indicates an insufficient intake of energy and nutrients, which increases the risk of complications such as infections, falls, frailty and sarcopenia. On the other hand, obesity involves an excessive accumulation of fat, both of which pose health risks [32]. Elderly people usually consume insufficient amounts of food or inappropriate food, due to reduced basal metabolic rates, low level of physical activity, difficulties in chewing and swallowing, but also due to reduced digestion capacity [33].
Therefore, the consequences of malnutrition and depression increase the degree of dependence and, implicitly, the risk of mortality. Moreover, there is also a causal relationship between the two by reference to the elderly in that depression, an increasingly common problem among the institutionalized elderly, can cause weight loss. However, very often, depression among the elderly is not diagnosed, thus remaining untreated [31].
At the same time, approximately 70% of the institutionalized elderly face a decrease in sleep quality, a fact generated by medical conditions, anxiety, stress, fear or other associated factors. Moreover, insomnia is considered to be a facilitating factor of mental disorders, in general, and of depression, in particular, hence its association with difficulties in managing emotions. However, sleep disturbances can be lessened by physical activity that helps institutionalized seniors improve their cognitive function and increase their self-esteem. Furthermore, gymnastics encourages psychosocial interactions and has positive effects on attention and memory, significantly reducing anxiety among the elderly [34]. At the same time, physical exercises can be a way to prevent and even treat the frailty of the elderly. They can improve gait, increase muscle strength, and decrease weakness [28].
The residential environment plays an important role in increasing the quality of life of the elderly. Therefore, friendly, safe and comfortable homes are directly proportional to well-being, enabling people to enjoy old age. Also, the infrastructure of the communities of which the elderly are a part (public transport, accessibility to buildings and public spaces) to which is added the promotion of a healthy lifestyle, social participation, entertainment and social services for the elderly represent some of the necessary conditions to lead an autonomous and independent living in old age. So, the physical and social facilities in the proximity of the elderly's homes (including shops, public lighting, green areas, recreational spaces, bicycle paths, medical services) are associated with the functional performance of the elderly. On the other hand, steep or uneven streets, lack of infrastructure for pedestrians, lack of street safety can constitute dangers for the elderly, restricting their participation in the community space [35].
Thus, walking among the elderly, i.e. walking in the vicinity of the home, helps them maintain their health and stay in their homes as long as possible. To this end, the elderly must benefit from enabling infrastructure, including adequate sidewalks, seating areas, and chairs or benches along their route [36].
So, physiological conditions, community design, social participation and social support strongly influence the psychological health of the elderly. However, [37] appreciates that the elderly, accustomed to living in areas with a developed infrastructure and increased security, also present greater material and spiritual demands. For this reason, dissatisfaction makes them prone to negative emotions and, implicitly, to feel an acute need for emotional support (telephone conversations, the company of family members). Thus, in order to reduce the risk of psychological problems, stress, but also feelings of loneliness and abandonment among the elderly, the younger generations must offer them emotional support.
However, elderly people living in the community are prone to frequent falls, with about one third of them experiencing this problem. In addition to the physical effects (bruises, fractures), many of the falls also have psychosocial consequences in the form of isolation, fear or even depression. Thus, falls in the elderly may require medical treatment, but in extreme cases, they may also cause the death of the elderly [38].
A high risk of falling is caused by malnutrition. Even if it has a higher prevalence among the institutionalized elderly, those in the community also face this pathology, weight loss being a predictive factor in this regard. Thus, malnourished elderly are prone to injury, long-term hospitalizations and even slower recovery from illness, thus a shorter life expectancy [39].
However, the falls of the elderly can also be caused by the number of medications they administer and, implicitly, by their adverse effects, by functional disorders or even by an inappropriately organized environment. Other predictive factors of falls among the elderly may also be certain comorbidities such as diabetes or hypertension [40].
Considering the aspects mentioned above, the purpose of our paper was to examine the ways in which the care centers for the elderly acted and adapted, mainly during the pandemic period from the perspective of the beneficiaries, the employees and the managers of those centers.
2. Materials and Methods
2.1. Purpose and objectives of the research
The purpose of this research was to study the ways in which the care centers for the elderly acted and adapted, mainly during the pandemic period from the perspective of the beneficiaries, the employees and the managers of those centers. Note: for simplification, we will call the elderly people from those centers with the term 'beneficiaries'.
Related to the purpose stated above, we also formulated a series of objectives, as follows:
O1. Measuring the general level of satisfaction of beneficiaries in specialized care centers.
O2. Identifying the main difficulties faced by the beneficiaries during the institutionalization period and during the pandemic
O3. Identification of the main medical/therapeutic services that the beneficiaries receive.
O4. Identification of the main leisure activities of the beneficiaries.
O5. Evaluation of beneficiaries' perceptions regarding the pandemic period and how their general health, mental health and personal needs were affected.
O6. Identification of the beneficiaries' proposals for improving the way of life in the care centers
O7. Identification of perceptions regarding the pandemic period from the perspective of employees and managers of the care centers
2.2. Hypotheses of the research
Hypothesis 1 (H1). The satisfaction with life in care and support centers treatment is significant different with gender, initial residence environment, the life stage and time spent in this kind of organizations.
Hypothesis 2 (H2). There are statistically significant differences in the calls of therapies in care and support centers according to the gender of respondents and to the age category.
Hypothesis 3 (H3). The biggest difficulties encountered during the pandemic were significant different with gender, residence environment, the life stage and time spent in care center.
Hypothesis 4 (H4). The more the pandemic affected the physical condition of the beneficiaries, the better was the perception of the relationship with the staff in the care centers.
2.3. Data collection method
We used for this research a mixed methods design named more precisely convergent parallel design [41] (pp.111-113). These designs refer to the implementation of quantitative and qualitative techniques at the same time, both being equally prioritized. The research was conducted between February – June 2022.
From a quantitative perspective, we applied a questionnaire to a quota sample of beneficiaries of care centers for the elderly in Timis County, Romania, and from a qualitative perspective, we applied interview guides to three target populations (beneficiaries, employees of care centers, managers of these centers).
Questionnaires and interview guides were applied in the following elderly care centers:
The socio-medical care center "St. Francis" Bacova, DGASPC Timiş – Centers 1-4, DAS Timiş, Periam Neuropsychiatric Recovery and Rehabilitation Center, Gavojdia Neuropsychiatric Recovery and Rehabilitation Center, Neuropsychiatric Recovery and Rehabilitation Center, Care and Assistance Center, Ciacova.
2.4. Sample
The sample of our research consists of retired people who live in the state or private asylums in Timis County Romania listed above. The subjects were selected by controlled quota sampling. The volume of the sample was 430 institutionalized elderly. The structure of the resulting sample was recorded thus following a series of independent variables: gender (male-49%, female-51%), initial residence environment (urban-53%, rural-47%), the life stage (adults under 64 years old [ 20%], young-old, ages 65–74 [50%], the middle-old, ages 75–84 [20%]), and the old-old, over age 85 [10%]), time spent in care and support center (up to 2 years -28%; 2-4 years -33.5%; 4 years and over 38.5%) and the type of care centers (public and private). All those quotas were established having as a model the characteristics of the research population transposed into a descriptive matrix [42]. Furthermore, considering the qualitative research, the interview was applied to 31 beneficiaries- people living in the care centers, to 7 employees and to 4 managers.
2.5. The research instruments
The questionnaire applied to the beneficiaries can be seen in Appendix 1 and we note that it is structured on a series of thematic areas as follows:
- Questions about the life in the care center/home before the covid 19 pandemic
- Questions about the life in the care center during the COVID 19 pandemic
- Identification questions
According to the objectives of the research, the questions from the questionnaire were used either for descriptive data or for stating and testing the hypotheses. Considering the qualitative research, the three interview guides used in the discussion with the beneficiaries, with employees and with managers, can be found in Appendix 2. In the interview guide applied to the beneficiaries we took into consideration dimensions such as: adjusting to the changes imposed by the move to the care center, adapting to the changes that have occurred due to the COVID-19 pandemic, changes in care mode due to the COVID-19 pandemic, the most important task they had to accomplish during the COVID-19 pandemic, contracting the virus, losing loved ones due to the COVID-19 virus, mood during the COVID-19 pandemic, solidarity at the level of the institution's employees, respondent’s greatest achievement, respondents' relationship with God. In the interview guide applied to employees we took into account dimensions such as: physical distancing measures during the COVID-19 pandemic, the greatest difficulty encountered by the beneficiaries, losing relatives, friends and/or loved ones due to the COVID-19 virus, the most important task they had to accomplish during the COVID-19 pandemic, mood during the COVID-19 pandemic, solidarity in the behavior of the institution's employees and beneficiaries, changes in the activity of the institution during the COVID-19 pandemic, care of the elderly in other institutions, respondents' relationship with God. Furthermore, in the interview guide applied to managers with measured the following the dimensions: physical distancing measures during the COVID-19 pandemic, the greatest difficulty encountered by the beneficiaries, losing beneficiaries, relatives or acquaintances due to the COVID-19 virus, the most important task they had to accomplish during the COVID-19 pandemic, mood during the COVID-19 pandemic, solidarity at the level of the institution's employees and beneficiaries, changes in the activity of the institution during the COVID-19 pandemic, changes that managers would like to make in the future, models of good practices identified in other institutions, respondents' relationship with God.
2.6. Data analysis
The data collected after applying a questionnaire in the care centers were analyzed with the 20 version of the program Statistical Package for the Social Sciences (SPSS). The analyzed variables were: a word describing the life in the care and support center, reason to be in support center, seniority in center, decision to stay in the center, Likert scale about satisfaction with the way of treatment in the center, six Likert scales about satisfaction with different services, general attitude of the staff, the biggest difficulty encountered in centers, kinds of medical/therapeutic services, main relaxation activities, communications with family members or other acquaintances/close people. For the pandemic situation the variables were: a word describing the life in the care and support center during pandemic, physical health affected by Covid 19, mental health affected by Covid 19, emotional states during the pandemic, concerns during pandemics, activities allowed during the pandemic, activities that miss the most, physical distancing measures, quality of the services in care centers, biggest difficulty encountered during the pandemic, kinds of contacts with family members, kinds of communications with family members, relationship evolution with family members, digital communications, staff attitudes during the pandemic, evaluation of relations with staff, socialization with beneficiaries, ways of socialization, emotional states during the pandemic, needs respect, suggestions for improving the way of life in the care center. To these are added the socio-demographic variables.
In our analysis we included as predictors gender, age categories, initial residence environment, the life stage and time spent in centers. In order to test the hypothesis, we used the construction of some statistical indexes, parametric Independent T Test, Kruskal-Wallis non parametric test, Chi Square test of independence, Spearman correlation.
3. Results
3.1. Results of the quantitative research
The quantitative analysis of sociological research obliges us to divide the obtained results into several large distinct chapters:
3.1.1. General evaluation of the care and support center
In accord with Objective 1 from the beginning we questioned the respondents what is the first word that comes to mind when they think about lifestyle in the care and support center? The results were presented in Figure 1.
In Figure 1 the size of each item is directly related to the frequency of appearance in the answers: good feelings (44.7%), care (7.9%), bad feelings (6%), restlessness (4.7%), serenity (4.7%) for example, but it is important to note that a high percentage fail to represent their own residence (21.4% with answer “I don’t know”). Of course, all the items were obtained after a recodification of answers. For example, the term ‘bad feelings’ refers to many aspects: maladjustment, ‘it's not like home’, regret or tendency to leave the center/asylum etc.
Regarding the main causes for which these beneficiaries arrived in that care and support center we recorded the following (Table 1):
Hypothesis 1 (H1). The satisfaction with life in care and support center treatment is significant different with gender, initial residence environment, the life stage and time spent in this kind of organizations.
For testing this hypothesis, we construct a general index of satisfaction (GIS) with all items from A6 question in the applied questionnaire. The items from these questions refers to satisfaction with offered food, entertainment opportunities, organized activities, medical care, accommodation services and spiritual assistance. The new scale GIS measuring the satisfaction with life has good reliability (with Alpha Cronbach= 0.917>0.700 for six items). The newly constructed index has the following descriptive values (Table 2).
Hypothesis 1 (H1) was divided into four other sub-hypotheses that we test in turn:
- Independent Sample T Test was conducted to decide that GIS for 208 interviewing males (M = 5.45, SD = 1.11) it is not significant different compared to the 222-interviewing female (M = 5.27, SD =1.14) for t(428) =1.626, p = 0.105. This sub-hypothesis is not confirmed.
- The 222 interviewing (that come from the urban environment) about general satisfaction with care and support center (M = 5.39, SD = 1.18) compared to the 198 interviewing (that come from the rural environment) (M = 5.30, SD =1.08) demonstrated that it does not show significant differences for t(428) = 1.62, p = 0.420. This sub-hypothesis is not confirmed.
- Kruskal-Wallis Test was conducted to examine the differences on general satisfaction with treatment according to the types of life stage. Significant differences (Chi square = 30.69, df = 3, p = 0.000) were found among the four categories of life stage (1. under 64 years old, 2. young-old, ages 65–74, 3. the middle-old, ages 75–84, 4. old-old, over age 85). A Mann-Whitney U test was conducted and observed that the adults under 64 years old are significantly more satisfied than young-old, ages 65–74 ( U= 6722, z = -3.668, p =0.000; mean ranks: 179.3>138.9), the middle-old, ages 75-84 are significantly more satisfied than the young old, ages 65-74 years (U= 5988, z = -4.993, p =0.000; mean ranks: 190.4>135.4), the middle-old, ages 75–84 are significantly more satisfied than the old-old over age 85 (U= 1346, z = -2.507, p =0.012; mean ranks: 71.2>53.5). All other comparisons were non-significant. In conclusion we cannot decide whether satisfaction increases or decreases with age.
- Kruskal-Wallis Test was conducted to examine the differences on satisfaction with time spent in care and support center. Significant differences (Chi square = 15.501, df = 2, p = 0.000) were found among the three categories of time spent in care and support center (1. Up to two years, 2. 2-4 years, 3. 4 years and over). A Mann-Whitney U test was conducted and observed that the clients who live in these centers up to two years are significantly more satisfied than clients who live over a period between 2 to 4 years (U= 6376, z = -3.676, p =0.000; mean ranks: 151.3>116.7) and significantly more satisfied than clients who live from four years and up (U= 8514, z = -2.104, p =0.03; mean ranks: 155.5>134.7). For the last two categories (2-4 years and 4 years and over) we found also significant differences (U= 10032, z = -2.451, p =0.01; mean ranks: 167>142); the people with 4 years and over are significant more satisfied than people with 2-4 years of stay. In general, we conclude that a shorter period spent in the center is more satisfactory but in the last case we found an opposite situation.
In conclusion the Hypothesis 1 (H1) is partially confirmed and in some of cases, in future research the analyses can be deepened with a qualitative methodology.
Furthermore, we asked the respondents to indicate the biggest difficulty they have encountered since they were institutionalized. The main difficulties are exposed in Table 3.
One of the main tasks of these care centers is to provide medical and therapeutic assistance to patients. The various care techniques were inserted in the questionnaire at question A9 and the needs of these patients are specific and without exception. Thus, in the last year, they have turned to the following forms of help (Table 4).
In order to have an image of the frequency with which these techniques/procedures are applied, we preferred to calculate a count type variable (which accumulates the types of activities). We conclude that 0.5% from all sample they called for all seven categories of therapy, 21% called for six of them, 35% called for five therapies, 26% called for four therapies from all of them and 17.5% called for one to three therapies. This kind of data proves the urgent needs of these people and the field research can give suggestions regarding the capacity building of the infrastructure specific to such care strategies.
Hypothesis 2 (H2). There are statistically significant differences in the calls of therapies in care and support center according to the gender of respondents and to the age category.
To test this hypothesis, we applied the Chi Square test of independence using a variable with multiple choice therapies and the two independent variables (gender and the life stage). We prefer to present the results obtained in a single table (Table 5).
The statistical analysis showed that there are statistically significant differences regarding the request for specific therapies according to the gender of the respondents (Chi Square=25.93, df=7, p=0.001) and also according to the age category of the beneficiaries (Chi Square=65. 01, df=21, p=0.000). In conclusion our hypothesis is confirmed.
The specific differences can be seen directly in the Table 5, from which we derived detailed explanations:
a. regarding the independent gender variable, it is observed that men request to a greater extent than women therapeutic massage (194>180) and medical assistance (28>20). Women request more than men recuperative gymnastics (188>174), physical therapy (178>174), assistance in basic activities (108>94), psychological assistance (92>82) and other services (2014>186).
b. regarding the independent the life stage variable we observe a concentration of the demand for therapeutic services for the elderly in the second columns (young-old, ages 65–74).
These findings can be very useful in order to improve the services offered. For example, the services offered can be diversified (considering the demand for ‘other services’ mentioned in the table below) or it can be investigating why the requests for specific therapies are so low for the other age categories (adults under 64 years old, the middle-old, ages 75–84 , and the old-old, over age 85) and dominant for the second age category (young-old, ages 65–74).
In our research we also took into consideration the leisure time of the respondents divided according to specific activities (deduced from the initial documentation in all the visited centers). The percents obtained are visible in Table 6.
In Table 6 we can observe easily the most intensively addressed activities and if we questioned the respondents again about the activity 'that makes greatest pleasure' the hierarchy in Table 6 remained identical. In other words, the relaxing activities carried out in the center correspond to the activities considered most desired by the beneficiaries. In reality, many other very diverse ones (32.7%) are added to the whole set of activities already mentioned: taking care of a green space, taking care of/playing with the animals in the center, participation in religious services, occupational therapy, playing on the piano, occupational workshops, crosswords, dish washing, drawing, painting.
3.1.2. Life, adaptation and pandemic condition
The period of pandemic was a big challenge for our questioned subjects especially in the conditions of collective living in these care and support centers, them facing problems related with some important variables: age, comorbidities, the protection strategies put into practice, etc. Moreover, The European Asylum Support Office (EASO) has published the report named COVID-19 emergency measures in asylum and reception systems (2020), in several series as an alarm signal regarding protection against Covid 19, accumulating experiences from all the EU countries.
To explain the results of quantitative research we preferred to split the presentation in some resumed chapters (in relation to the items in the questionnaire).
Personal representation and evaluation of the pandemic
Describing with a single word (or a few) the pandemic situation it was not very simple for the interviewing (Figure 2). For us it was interesting to compare this kind of definition with the representations from Figure 1.
The positive terms (adaptation-3%, good feeling-32%, safety-4, same situation-7%, silence-1%) were this time complemented by predictable negative items (bad feelings-10%, confusion-3%, isolation and restriction-12%, restlessness-3%, stress and afraid-11%). All these items can reflect a balance between the state of well-being and the panic created by the pandemic. In fact, the care centers did not have serious problems in terms of illnesses or deaths (although these do not include the emotional states of customers), and the analysis of the websites of these organizations reveals the strict measures were taken during the pandemic. This equilibrium also resulted from the descriptive analysis of questions B3 (evaluation of the health status) and B4 (evaluation of mental health) and B24 presented in Table 7.
The first impression is that these statistical data may suggest a positive background and an under control social framework. Nevertheless, we insisted on finding out the weight of some emotional states felt during the pandemic, and the results are presented in Table 8.
Regardless of the duration of these emotional states, we observed high weights (calculated for all subjects): the great majority of the questioned subjects have experienced one or many kinds of negative emotional state. By applying a Chi independence test, we found that there were no significant statistical differences according to the gender of the respondents (Chi Square=9.65, df=5, p=0.08>0.05). In other words, these negative emotional states affected the respondents equally regardless of gender.
Finally, with a count type variable, we conclude another evaluation in Table 9 about how many of the emotional states did they feel during the pandemic.
Thinking about the emotional states that the impossibility /reduced possibility of socializing with the other members of the center has created for you, most often during the pandemic you have felt: “alone” (16%). “restless” (31%), “nervous” (10%), “helpless” (9%), sad (26%).
To all these traumas it is added the concern for ‘own state of health’ (45% from respondents), for ‘the health status of the family members’ (24%), the decision to be vaccinated or not against Covid (14%) or for ‘the health of friends/acquaintances’ (3%).
Evaluation of organizational limitations generated by the pandemic
At the social problems explained before, we can add the specific organizational measure, in fact a series of limitations imposed for social distancing of which the interviewees mentioned the limitation of the number of people with access to common spaces (12%), limitation of the amount of time spent in the common spaces (17%), the ban to socialize through board games (22%), reduction of the number of roommates (30%), wearing the masks (20%).
In this situation, we expected that the staff's activity would be strongly criticized. However, the opinions about the quality of provided social services of the interviewees were significantly positive: 85 percent declared that they considered the quality of all the services offered during the pandemic being good and very good (Table 10).
The strictness of the rules applied in the care centers predictably blocked the activities that were currently taking place. Those activities have already been stipulated in Table 6, but we will repeat them here specifying the percentage of respondents in each case (percent of cases) when the specified activities were not allowed (Table 11).
In Table 11 we observed that all the limitations were accepted as such and reflect the fact that they were effective and unequivocal. Applying a Chi independence test, we found that there were no significant statistical differences regarding the perception of specific limitations according to the gender of the respondents (Chi Square=9.36, df=6, p=0.154>0.05). All the limitations were perceived the same regardless of the gender of the subject.
The data from Table 11 is suggestive in terms of the very strict restrictions generated by social distancing, a fact that triggered social isolation or negative emotional states already presented. It was also very suggestive that the respondents remembered which specific activities they missed the most (Table 12).
We notice that ‘walks outside the care center’ were felt to be the most desirable, but the possibility of leaving the center and returning already infected was definitely a credible threat. On the other hand, ‘socializing with other residents in common activities’ could also be the source of infection.
The other answers to this open question were much more diverse and even surprising. Here are the most interesting answers about desired activities: 'I want to paint' (declared a male person, 70 years, higher education, lived in the urban environment); "I want freedom" (male, 78, gymnasium, rural environment); "I wasn't allowed to scream" (female, 70, gymnasium, rural environment); "celebrations and theatre" (male, 31, gymnasium, urban environment); "to drink coffee and smoke cigarettes" (female, 70, gymnasium, urban environment) etc. Of course, this kind of answers can also be tracks for in-depth research according to the principle of serendipity (see for example Merton & Barber, 2004). Also, a starting point can be the 22 percent of those who declare that they do not know how to specify the activities they miss the most.
Finally, we initiated the item B12 from the questionnaire as a look at the problem of consequences of organizational limitations, questioning what was the biggest difficulty encountered during the pandemic in the care center. The responses are resumed in Table 13 and were the starting point in the statement of the third hypothesis.
Starting from these data in Table 13 we formulated our third hypothesis.
Hypothesis 3 (H3). The biggest difficulties encountered during the pandemic were significant different with gender, residence environment, the life stage and time spent in care center.
We divided this hypothesis into four sub-hypotheses as follows:
a. Regarding the independent gender variable the statistical analysis showed that there are not statistically significant differences in terms of perception of the biggest difficulty during pandemic with gender (Chi Square=6.92, df=5, p=0.226). There are no differences in perception according to the gender of the subjects.
b. Regarding the independent residence environment variable the statistical analysis showed that there are not statistically significant differences in terms of perception of the biggest difficulty during pandemic with environment (Chi Square=6.92, df=5, p=0.226). There are no differences in perception according to residence environment of the respondents.
c. Regarding the independent life stage and time spent in center variables we preferred to present statistical data in the same table (Table 14). The initial crosstabulation of the variables including the life stage (adults under 64 years old, young-old, ages 65–74, the middle-old, ages 75–84 and the old-old, over age 85) has generated 7 cells (29.2%) with expected count less than 5. In this situation we recoded the variable the life stage for three categories (adults under 64 years old, young-old, ages 65–74, the middle-old and old- old , ages 75 and over) but the variable ‘time spent in center’ remained the same (Table 14).
The statistical analysis showed that there are statistically significant differences regarding the perception of the biggest difficulty during pandemic with life stage (Chi Square=38.51, df=10, p=0.000) and the same statistically significant differences with time spent in center (Chi Square=28.55, df=10, p=0.001).
Some descriptive conclusions can be set. For example, “impossibility to communicate with family members / close persons” remained the dominant difficult problem for every category of the independent variables: 40.5% from the beneficiary under 64 years old; 41.6% from young-old, ages 65–74; 59.7% from the middle-old and old-old, ages 75 and over. The same situation is in the case of the categories in time spent in center variables: 42.6% from the beneficiaries who stay in centers for up to 2 years; 39.4% for those who have been staying for 2-4 years and 56.3% from those who have been 4 years and over.
The significant statistical differences come from the fact that in both cases the dominant percentages are capitalized in general by the ‘young-old, ages 65–74’ and those who have been in the centers between 2 and 4 years.
As a general conclusion we can observe that the hypothesis 3 is partially confirmed. If for gender and residence environment there are not statistically significant differences regarding the perception of the biggest difficulty during the pandemic in the case of the last two variables life stage and time spent in center there are statistically significant differences.
3.1.3. Maintaining ties with the family and methods of communication
Part of the previous questions referred to the links that the beneficiaries have with their own families. This situation comes to characterize the relations with the family starting from the specific conditions of hospitalization in a care center. In this case we could observe that 47% of the beneficiaries considered 'impossibility to communicate with family members / close persons' as one of the major difficulties (Table 13), while 22% declared that 'family members no longer had the opportunity to provide them with the necessary care' (Table 1) while "communication with family members/close people" was considered "the main difficulty encountered within care and support center" by 15.6% of respondents (Table 3).
During the pandemic period, it was expected that the difficulties with relationship would increase, but the answers were contradictory in the first phase. Thus, only 30% of the respondents declared that they maintained contact with the family to a small or very small extent, and on the opposite side, 49% declared that they managed to maintain contact to a large or very large extent. This fact was primarily due to virtual meetings and not to face to face (physical) ones. The ways to ‘keep in touch’ can be seen in Table 15.
There is a low use of video calls (14.5%), the explanations being multiple: from the difficulties of using new technologies, the lack of Internet connection or the lack of upgrades specific to modern telephony. Moreover, these figures are consistent with the results of a research on a representative sample at the level of Romania, research carried out by Metro Media Transylvania (2019) regarding the use of electronic communication services. According to that research, Romanians use mobile phones in high proportion (over 90%) but only 34% have Internet on their phone. People aged 65 and over were distinguished by the fact that: 43% stated that they do not use messaging or calling on the Internet, 63% did not download/watch videos, and 71% stated that they never downloaded/listened to music on the Internet . Regarding our sample, 64% of the interviewees declare that they rarely or very rarely use video applications on their phone to communicate with their family.
Also in Table 15, we notice that physical visits practically disappear (due to the pandemic situation). In fact, in the context of the pandemic, family visits have significantly decreased (76% of respondents stated that family members were not allowed to come to the center). Even in these conditions the respondents consider either in this context that the relations with the family remained the same (57%) or even improved (7%). Only a percentage of 12% declared that relations with the family worsened during the pandemic period.
3.1.4. Relationship with the center's staff and the assessment of its activity
The evaluation of the care staff in the respective centers by the beneficiaries proves to be particularly useful, especially in the context of the Covid pandemic. To begin with, following question B18 from the questionnaire, the beneficiaries specified that the relations with the staff in the centers were rather positive (65%), neither positive nor negative (32%) and rather negative (3%). We deduce from this a dominant positive institutional context, the relationship with the respective staff being extremely important. Moreover, the respondents specified that compared to the pre-pandemic period they felt that during the pandemic the staff gave more attention to the beneficiaries (58% of the respondents declare that). A more complex evaluation of the involvement of the staff in the centers by the beneficiaries can be outlined starting from questions B20 from the questionnaire. As can be seen B20 resides in three items as follows :
1. The employees of the care center have been more reluctant towards me during the pandemic
2. For the nurses and caregivers at the center, my needs have been a priority during the pandemic
3. Nurses and carers have socialized less with beneficiaries during the COVID 19 pandemic
Based on these three items (actually three 7 point Likert scales) we built a statistical index of the perception of staff involvement in the pandemic (variable abbreviated perstaff). The index is a summative one obtained after recoding items 1 and 3 (through inversion of scales) and with next descriptive data (Table 16).
With the help of this index we formulated the fourth statistical hypothesis:
Hypothesis 4 (H4). The more the pandemic affected the physical condition of the beneficiaries, the better was the perception of the relationship with the staff in the care centers.
To test this hypothesis, we used the previously constructed statistical index and the variable that comes from question B3. The Spearman correlation analysis gave the following result (Table 17).
3.1.5. Relationship with other residents
The relationship with the other residents is equally important for the beneficiaries of the centers, especially in the conditions of the pandemic. However, the obligatory social distancing has tinted the answers of those interviewed, as can be seen in Table 18.
We note that 50% of the respondents stated that they socialized with the other residents to a low extent (Table 18). In this context the ways of socializing were still dominated by watching TV shows in common spaces respecting the rules of physical distancing (69% of the respondents), talked on the phone with the other residents (27%) and only 4% declared that they use video calls. The emotional states felt during the pandemic contributed to a certain weakening of relations with the other beneficiaries: they felt restlessness (31%), sadness (26%), loneliness (16%), nervousness (10%) helplessness (9%).
3.1.6. General/global assessment of the center and suggestions for improving the way of life in the care centers
The beneficiaries were asked to give suggestions for improving the conditions in the care centers. The answers of the beneficiaries are presented in Table 19 (with the specification that we presented only the valid answers excluding the non-responses):
We also list a series of original proposals of the beneficiaries: “attracting sponsorships” (declared a female person, 76 years, gymnasium, lived in the urban environment); "finding jobs for beneficiaries" and "stop segregating people with disabilities” (male with health problems, 42, higher education, urban environment); “beneficiaries involved in self-management” (female, 70, gymnasium, rural environment); "establishment of a gym" (male, 72, gymnasium, rural environment); "to bring new employees" (female, 56, gymnasium, rural environment). All the proposals of the beneficiaries must be taken into account and that's why we would recommend to all the managers of these centers to make permanent consultations with the beneficiaries through opinion polls or by encouraging collaborations in order to improve the collective life of the elderly.
3.2. Results of the qualitative research
In the qualitative analysis we were interested in obtaining a more clear view on the lifestyle institutionalized elderly had in the care centers during the pandemic. The results of the qualitative analysis were analyzed according to the dimensions established in the interview guide (Table 20).

Table 20.
Analysis of the interviews applied to institutionalized elderly.
| Adjusting to the changes imposed by the move to the care centre | The majority of the respondents stated that they adjusted rather well to the changes imposed by their move. Out of the 16 women and 15 men that were interviewed as beneficiaries, one woman didn’t provide an answer, another woman mentioned both the positive aspects, as well as the negative aspects of adjusting, while six other women and six men stressed the difficulty of the adjustment. |
| Adapting to the changes that have occurred due to the COVID-19 pandemic | The main features that are associated by the respondents with the emergence of the COVID-19 pandemic are isolation and the implementation of more drastic hygiene measures. When specifically mentioned, the challenges that arose during the process of adapting to the changes determined by the pandemic were correlated with the impossibility of receiving visits from their relatives. Another respondent emphasized the fact that she had no other choice. The majority of respondents that specified the difficulty of adapting to the changes generated by the restrictions imposed during the COVID-19 pandemic didn’t explain what were its causes. Out of the respondents that were beneficiaries, ten women and three men specifically stated that it was hard to adapt to the changes that have occurred due to the COVID-19 pandemic. |
| Changes in care mode due to the COVID-19 pandemic | The interviewed beneficiaries stated that isolation and the ban on visits, outside walks and socialising where the most noticeable changes determined by the emergence of the COVID-19 pandemic. Furthermore, greater attention was paid to the beneficiaries’ hygiene and health condition. The beneficiaries had to wear surgical or N95 masks in public contexts. Social distancing and restricting the number of persons in public spaces were other measures taken by the nursing personnel. The mandatory wearing of masks, prohibition of visits and socializing, social distancing, restricting the number of people in enclosed spaces were among the measures considered by the respondents to be the most exaggerated, wrong and even abusive. |
| The most important task they had to accomplish during the COVID-19 pandemic | Taking care of their own health, respecting the rules of living in harmony, maintaining the cleanliness in their space and keeping the morale were the tasks most mentioned by the interviewed beneficiaries. 12 of the respondents mentioned their own health as being the priority. Three stated that respecting the rules of living in harmony with each other was paramount. |
| Contracting the virus | Nine of the respondents admitted that they have contracted COVID-19: six of them were women and three were men. Only one woman chose to describe her experience, stating that she had a less serious form of the disease. |
| Losing loved ones due to the COVID-19 virus | Three women and five men stated that they have lost relatives, acquaintances or loved ones. All of those that admitted losing people due to the COVID-19 virus chose not to offer other information on the topic. |
| Mood during the COVID-19 pandemic | 11 men declared that the mood during the COVID-19 pandemic was “good” or “very good”, while five men declared that the mood was “precarious” and/ or “bad”. 12 women declared that the mood was “ok” or “good”, while one woman declared that the mood was either “agitated” or “bad”. Out of the women that declared that the mood was “good”, one respondent claimed that the fact the institutionalized beneficiaries were together was an advantage for all of them. |
| Solidarity at the level of the institution's employees | The mood of the employees was generally assessed by the interviewed beneficiaries as being “acceptable”, “good” or “optimistic”. However, three respondents claimed that the employees were either “psychically exhausted”, “burned-out” or “restless”. Other three of the interviewees stated that the personnel were either “resigned”, “reserved” or “demoralised”. Generally, the effects of the COVID-19 pandemic were considered to bring at least partial changes in the consciousness and the behaviour of the respondents’ peers. For example, isolation was a consequence specifically mentioned by one of the respondents as being determined by the pandemic. Furthermore, the increased focus on improving the hygiene measures was another aspect mentioned by another of the interviewees. |
| Respondent’s greatest achievement | The achievements mentioned by the interviewed beneficiaries actually cover a plethora of areas that are difficult to sum in one category. “Children”, “freedom”, the fact that the respondents were able to survive the pandemic, “happy marriage”, “family”, their studies and “returning to Romania” are all considered by various respondents to be their greatest achievement in their life. The most frequently mentioned achievement mentioned by the beneficiaries was their “children”: ten women and three men referred to it specifically as their greatest achievement. Interestingly, two respondents stated that their greatest achievement was surviving and reaching their current age. |
| Respondents' relationship with God | When addressing their relationship with God, the majority of the respondents declared that they were believers. Ten interviewees specifically claimed that they had either a relation with God or benefited from Divine intervention in one form or another: for example, one respondent stated that he was saved from two heart attacks. Another four respondents asserted that they have a good relationship with God. One respondent specified that he would rather not answer when asked whether he has faith in God or not. Another respondent stated that she doesn’t believe in God. |
Table 21.
Analysis of the interviews applied to employees of the care centers.
| Physical distancing measures during the COVID-19 pandemic | The nursing staff respondents stated that the physical distancing measures during the pandemic entailed strict isolation of the beneficiaries. Daily information sessions on anti-COVID-19 prevention measures were organised in the elderly care centres. Wearing surgical or N95 masks and the isolation at the workplace were among the most difficult measures that were recurrently mentioned by the interviewed personnel. For example, the employees from the “St. Francisc” Centre from Brașov and those from the Adam Muller Gutenbrunn Complex stated that isolation was used as a measure to combat the COVID-19 virus. Aside from these measures the interviewed employees stated that strict compliance with hygiene regulations and distancing rules were accompanied by offsetting the schedule of all the beneficiaries. The number of activities developed in all the institutions surveyed decreased significantly: all the respondents stated that some activities were either limited or stopped altogether. |
| The greatest difficulty encountered by the beneficiaries | The respondents declared that the most difficult measures imposed on the beneficiaries was isolating them in relation to their relatives and the community, and distancing them vis-à-vis their peers. All the interviewed women stated that the quarantine subjected both the beneficiaries and themselves to increased pressure during their everyday activities. Two of the men that were interviewed asserted that the isolation was associated with limiting the rights of beneficiaries: particularly, the quarantine removed the possibility of meeting their relatives and partaking into social events. The new measures entailed by the quarantine also increased the volume of work, according to two women employed at the Adam Muller Gutenbrunn Complex for the Elderly. This meant that the employees had longer work schedules. |
| Losing relatives, friends and/or loved ones due to the COVID-19 virus | 11 out of the 29 interviewed employees declared that they have lost either relatives, friends and/or loved ones due to the COVID-19 virus. While most of those that admitted losing friends and/or loved ones didn’t offer any additional explanations, two specifically claimed that they have lost relatives. |
| The most important task they had to accomplish during the COVID-19 pandemic | The most important tasks that had to be accomplished by the employees during the COVID-19 pandemic was enforcing the new rules of conduct with an emphasis on social distancing and ensuring that the health measures decided nationwide were enforced at institutional level. Nine women and two men, which were employees during the pandemic, stated that aside from doing their job, taking care of their own health was a priority. Except for three employees, all the respondents stated that maintaining the health of the beneficiaries was a top priority. Interestingly, two of the aforementioned employees (both men) stated that social distancing was the most important task they had to accomplish. |
| Mood during the COVID-19 pandemic | The mood of the beneficiaries was characterized as being “good” by the majority of the respondents. However, ten of the employees stated that the beneficiaries were disturbed and manifested sadness, confusion, anger, frustration and even desperation due to the fact that they weren’t able to interact with their families and the community. Six of the respondents claimed that their own mood influenced by tiredness. For example, one of the women employed at the “Saint Francisc” Centre from Brașov asserted that her mood and that of her colleagues was “disturbed”. Nevertheless, the rest of the respondents specified that their mood was “good” although, as employees, they had to respect new rules, were subjected to stress and had to endure longer working hours. |
| Solidarity in the behaviour of the institution's employees and beneficiaries | 24 of the respondents claimed that they noticed a real solidarity in the behaviour of their colleagues, managers and beneficiaries after the emergence of the pandemic. Four of the employees stated that they didn’t notice any form of solidarity. Two respondents argued that while there were situations in which they noticed solidarity, there were also circumstances when it did not manifest in the various interactions between the employees, managers and beneficiaries. The responses associated with this topic tended to be quite succinct: only five of the employees offered somewhat more detailed responses. Two of them said that there were both moments of solidarity and tension. The other three claimed that everybody in their institutions helped each other. However, they didn’t provide additional details. |
| Changes in the activity of the institution during the COVID-19 pandemic | All of the employees said that there were significant changes in the consciousness and the behaviour of their colleagues, managers and beneficiaries. Though the responses offered on this topic by the employees vary considerably. The personnel from the Caritas Centre Timișoara, which were isolated at their working place, claimed that they were called daily on the phone by the management, in order to ascertain their mood and to support them morally. When asked about the most important changes noticed, the respondents stressed that the various types of documentation needed for many institutional activities were no longer submitted face-to-face. Instead, all submissions were done online. Furthermore, there were no resignations and layoffs. The employees were no longer able to carry out the social surveys face-to-face with the beneficiaries, but only by phone. The respondent from the Schwabenhause–Lenauheim Home for the Elderly emphasized that while there were no layoffs, the isolation period in the institution was difficult. One of the employees from the “Saint Nicholas” Complex for Elderly People from Lugoj emphasized the personal hygiene requirements. In the Adam Muller Gutenbrunn Home for the Elderly one of the three interviewed employees detailed the changes that have occurred in the activity and personnel scheme of the institution: unlike the other two respondents he emphasized that there were three resignations and two employments. At the Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG), one of the respondents stated that there was an outbreak of COVID-19 for two weeks at their institution. Accordingly, wearing protective equipment was a necessity, a statement confirmed by the other interviewed employee. The three employees from the Periam Neuropsychiatric Recovery and Rehabilitation Centre emphasized that in the direct activities with the beneficiaries, the activities were developed in small groups. Keeping the distance of at least 2 meters was actively enforced. At the “Saint Francisc” Centre from Brașov both respondents declared that the pandemic brought with it a change for the worse in people’s behaviour on a daily basis. One of the interviewees emphasised that there were no changes in the personnel scheme, but the activities changes dramatically and the number of restrictions increased considerably. One of the respondents from the “Inochentie Micu Klein” Home for Elderly People specified that the most important change in the behaviour of her colleagues and beneficiaries brought by the pandemic was the attainment of a greater awareness in some areas of life. Both of the employees interviewed mentioned that isolation in the workplace was the most important change in the activities undertaken at their centre. At the Support Centre for Crisis Situations, one the two respondents mentioned that (a) isolation, (b) the enforcement of wearing mandatory protective equipment, and (c) social distancing were noticeable changes. Furthermore, the employees were separated in small groups and their work schedule was changed. |
| Care of the elderly in other institutions | The interviewees answered that caring for the elderly is difficult in all contexts and the measures necessary for offering them a good standard of living are similar in all institutions. The employees from the “Inochentie Micu Klein” Home for Elderly People mentioned that they found out about the ways in which elder beneficiaries were cared for in other institutions via mass media (i.e. television, radio and newspapers). The personnel from the Ciacova Care and Assistance Centre didn’t detail their answers: only one of the respondents mentioned Internet as a means of finding out what were the actions undertaken in other institutions. When asked on this topic, 13 of the employees declined to offer any answers or stated that they didn’t know what the situation was in other centres. |
| Respondents' relationship with God | The responses regarding the employees’ relation to God were varied. They can be placed on a continuum between statements that emphasize the good relation between the interviewee and God and assertions that deny the existence of God and/or refute any relation between any form of divinity and the COVID-19 pandemic. For example, the response of one of the interviewees from the “Saint Francisc” Centre is suggestive: she answered that “I have a good relationship with God; I put all my hope in Him in these difficult times. He can cure any disease if he wants to. Everything depends on us, on how we live our lives, listening, keeping or not His commandments.” (woman, 54 years, bachelor graduate). On the other hand, another employee from the same institution stated that “faith has no influence on what man invents” (man, 31 years old, bachelor graduate). Those that mentioned their belief in God stated that their faith helped them during the pandemic. Two of the employees from the Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre replied that during the pandemic they felt closer to God (woman, 40 years old, High School graduate; man, 42 years old, master graduate). One employee from the “Saint Nicholas” Complex for Elderly People from Lugoj claimed she got through the first year of the pandemic only by having faith in God (woman, 40 years old, master graduate). |
| Other comments | The final question on the interview guide invited the respondents to add other aspects they deemed to be relevant. The interviewees’ responses cover specific topics on religious themes and mental wellbeing. For example, one of the employees from the “Saint Francisc” Centre expounded the lengthiest response at this question on religious themes, emphasizing the importance of God for people’s lives during the pandemic (woman, 54 years old, bachelor graduate). Faith and prayer were mentioned to a lesser extent by other respondents (woman, 42 years old, bachelor graduate). Another woman that works as a caregiver stated that she passed easier through the pandemic than her colleagues. She mentioned that her colleagues had to spend in isolation at their workplace three 14 days periods. Accordingly, she mentioned that the isolation marked her colleagues because they claimed to have panic attacks, fear and low morale (woman, 33 years old, master graduate). One employee from “Saint Nicholas” Complex for Elderly People stressed her hopes that the experiences associated with the pandemic will never be repeated again and the situation will revert to “normal” (woman, 40 years old, master graduate). |
Table 22.
Analysis of the interviews applied to the managers of the care centers.
| Physical distancing measures during the COVID-19 pandemic | The interviewed managers enumerated among the concrete measures taken in order to ensure physical distancing, the following actions: wearing masks/ protection equipment, limiting the number of beneficiaries in each room and separating the daily meal schedule, marking the routes with stickers in order to avoid crowding. Social distancing between beneficiaries and employees was also enforced everywhere, with one exception: in the Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre this measure was impossible to implement due to the specific activities with the beneficiaries. However, in this institution the employees used protection equipment in all their interactions. The sanitary measures imposed throughout the country were deemed as being either (a) good or (b) panic inducing, illogical and/or chaotic. For example, the manager from the Schwabenhause – Lenauheim Home for the Elderly from Timiș responded that sometimes the imposed measures were beneficial and other times they were exaggerated and made work difficult at the expense of the beneficiaries. The measures were considered to be good and/or necessary, albeit insufficient, by the managers of the following five centres: Periam Neuropsychiatric Recovery and Rehabilitation Centre, Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre, Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG), Anitaheim Varel Home for the Elderly from Lugoj, Caritas Centre Timișoara. Conversely, the chaoticity of the health measures imposed at national level was emphasized by the managers of five institutions: “Saint Francisc” Centre, “Inochentie Micu Klein” Home for Elderly People, Support Centre for Crisis Situations, Adam Muller Gutenbrunn Complex for the Elderly, “Saint Nicholas” Complex for Elderly People from Lugoj. Accordingly, it was difficult to respect all the imposed measures in order to protect the beneficiaries and the employees. Aside from the aforementioned measures, the manager from the “Inochentie Micu Klein” Home for Elderly People added also the interdiction receiving visits from the exterior and restrictions regarding existing the institution. The managers that were interviewed stated that the governmental measures imposed in Romania had generally a negative impact on the activities from their institutions. Consequently, it was very difficult for the employees to carry out their activities and to ensure that all the people involved (beneficiaries and employees) equally respected the established norms and rules. The manager from the Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG) mentioned that communication became difficult as well: the messages were hard to send and their understanding was problematic, due to the online platforms used and the lack of face-to-face interactions. The three managers from the Adam Muller Gutenbrunn Complex for the Elderly expounded that the biggest difficulties they encountered during the pandemic were associated with: the process of hospitalization of the beneficiaries, the excessive bureaucracy developed during the pandemic, the physical exhaustion and the deficit of personnel. The excessive bureaucracy was mentioned as the most difficult aspect of the pandemic by the manager from the Schwabenhause–Lenauheim Home for the Elderly as well. The manager from the Anitaheim Varel Home for the Elderly from Lugoj claimed that the biggest difficulty he was confronted with was getting access to protective equipment. The managers from the Caritas Centre Timișoara and the “Saint Nicholas” Complex for Elderly People from Lugoj responded that for them, the most difficult aspects were the compulsory isolation at their workplace and the quarantine. |
| The greatest difficulty encountered by the beneficiaries | The three managers from the Adam Muller Gutenbrunn Complex responded that the biggest difficulty encountered by the beneficiaries was associated with the fact that they were unable to understand what was happening. Accordingly, the beneficiaries tended to become frightened by the new evolutions. The rest of the interviewed managers stated that the inability to socialize, the limitations imposed on their freedom (e.g. the quarantine), the rejection of the reality outside their institutions (e.g. the number of deaths attributed to the COVID-19 pandemic) and the inability to meet their relatives were the most significant difficulties encountered by the beneficiaries. |
| Losing beneficiaries, relatives or acquaintances due to the COVID-19 virus | Six of the managers answered that they did not lose any beneficiaries, relatives or acquaintances. Nine of them responded that they have lost people belonging to at least one of the aforementioned categories. However, most of the interviewees offered single word answers on this topic. There were a few that detailed their replies. For example, the manager from the Anitaheim Varel Home for the Elderly from Lugoj claimed that he lost two of the beneficiaries for whom he was responsible due to COVID-19. He also stated that between March 2020 – March 2021 his institution was confronted with more deaths than in any other year. The reason expounded for this situation was the precarious health state of the beneficiaries from that institution (man, 74 years old, bachelor graduate). The manager from the Schwabenhause–Lenauheim Home for the Elderly mentioned that there were a few deceased beneficiaries, who were declared by the medical authorities as being infected with COVID-19. However, they had multiple associated comorbidities and/or complications (woman, 32 years old, bachelor graduate). There were also five respondents that claimed to have lost people who didn’t contract the COVID-19 virus. Death resulted due to the fact that those mentioned by the managers didn’t receive the necessary medical care in a timely manner as a result of the enforcement of anti-COVID-19 measures. Notably, the manager from the Anitaheim Varel Home for the Elderly from Lugoj stated that two of his employees and one beneficiary died as a result of not receiving medical care in time, even though they were not infected with COVID-19 man, 74 years old, bachelor graduate). |
| The most important task they had to accomplish during the COVID-19 pandemic | The managers offered a plethora of responses pertaining to this topic, which were associated with one form or another of responsibility. Their responses can be grouped into two categories. There were respondents that emphasized the importance of maintaining a veneer of “normality” in their institutions and improving the relations between beneficiaries, in institutions such as: “St. Francisc” Centre, Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG), Schwabenhause–Lenauheim Home for the Elderly. Other managers stressed the importance of protecting their employees and beneficiaries and providing them with information daily (e.g. Ciacova Care and Assistance Centre, Periam Neuropsychiatric Recovery and Rehabilitation Centre, Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre, Anitaheim Varel Home for the Elderly from Lugoj and Saint Nicholas” Complex for Elderly People from Lugoj. |
| Mood during the COVID-19 pandemic | The mood of the beneficiaries was characterized by some of the managers as being subsumed to anxiety, fear, “irritability” and irascibility. Furthermore, the employees and the managers themselves were described as being stressed and overloaded. This description was expounded by the managers of the following institutions: Support Centre for Crisis Situations, “St. Francisc” Centre from Brașov, Ciacova Care and Assistance Centre, Adam Muller Gutenbrunn Complex (i.e. one of the three managers: man, 65 years old, master graduate), Caritas Centre Timișoara (i.e. regarding the beneficiaries). However, the majority of the respondents claimed that the mood of their beneficiaries and employees was optimistic, such as the managers of the “Inochentie Micu Klein” Home for Elderly People, Periam Neuropsychiatric Recovery and Rehabilitation Centre, Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre, Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG), Adam Muller Gutenbrunn Complex (i.e. two of the three managers: (1) woman, 65 years old, master graduate; (2) woman, undisclosed age, bachelor graduate), Anitaheim Varel Home for the Elderly from Lugoj, Caritas Centre Timișoara (i.e. regarding the manager and the employees), Schwabenhause–Lenauheim Home for the Elderly, “Saint Nicholas” Complex for Elderly People from Lugoj. |
| Solidarity at the level of the institution's employees and beneficiaries | The responses of all the managers confirmed that there was a noticeable solidarity between the employees and beneficiaries. The manager from the Anitaheim Varel Home for the Elderly from Lugoj emphasized that this solidarity is the reason why both the employees and the beneficiaries were able to go through the pandemic more easily (man, 74 years old, bachelor graduate). |
| Changes in the activity of the institution during the COVID-19 pandemic | The managers from most of the institutions subjected to the study responded that the pandemic didn’t bring with it a change for the better in the consciousness of the employees and beneficiaries. Furthermore, the respondents enumerated the following changes that occurred and/or were imposed in the organization of their institutions’ activities during the pandemic: the isolation of the employees, quarantine and social distancing imposed on the beneficiaries, new sets of sanitary rules were enforced (including weekly PCR testing), the location of some activities was changed. The manager from the Periam Neuropsychiatric Recovery and Rehabilitation Centre claimed that some of the most important changes were: mandatory wearing of protective equipment and frequent disinfections. She also mentioned that there were two resignations. On the other hand, the four managers from the (1) Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre, (2) Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG), (3) Schwabenhause–Lenauheim Home for the Elderly and (4) “Saint Nicholas” Complex for Elderly People from Lugoj answered that the pandemic brought with it a change for the better, without offering any details. The latter respondent replied that she hired new employees (woman, 32 years old, bachelor graduate). The manager from the Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre stated that there were no significant changes in the organization of his institution’s activities (man, 57 years old, bachelor graduate). The three managers from the Adam Muller Gutenbrunn Complex specifically stated that they had to consider, when they organized their activities, a series of resignations. They didn’t offer any other details on this topic. The manager from Anitaheim Varel Home for the Elderly from Lugoj mentioned that the mood of the employees and beneficiaries worsened, which had an impact on the various activities. The work shifts had to be changed in order to take better care of the beneficiaries with special needs and to strengthen the relationship between employees and beneficiaries. |
| Changes that managers would like to make in the future | The managers offered a large plethora of answers on this topic. They encompass numerous directions of development associated by the respondents with the term ‘improvement’ rather than ‘change’: (1) keeping and improving discipline in the activities with beneficiaries (“Saint Francisc” Centre from Brașov); (2) improving the ties between beneficiaries and employees (“Inochentie Micu Klein” Home for Elderly People); (3) training the personnel for potential special situations that may require changes in the organization and operation of the institution (Support Centre for Crisis Situations); (4) hiring new personnel (Ciacova Care and Assistance Centre); (5) permanent improvements in various fields (Periam Neuropsychiatric Recovery and Rehabilitation Centre); (6) improvements in accordance with the changing legislation (Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre); (7) improving teamwork by integrating the beneficiaries in the team (Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG)); (8) new equipment – emphasized by two of the three managers from the Adam Muller Gutenbrunn Complex (woman, no declared age, bachelor graduate; man, 65 years old, master graduate), while the third manager stated that she didn’t want any changes for the time being (woman, 65 years old, master graduate); (9) improving the connections and the involvement of the local community as well as acquiring greater support from the authorities (Anitaheim Varel Home for the Elderly from Lugoj); (10) expanding the internment capacity and building a kitchen in the institution’s cafeteria (Schwabenhause–Lenauheim Home for the Elderly); (11) supplementing the specialist positions and modifying the regulations regarding the accessibility of the service (“Saint Nicholas” Complex for Elderly People from Lugoj). |
| Models of good practices identified in other institutions | The managers from “Saint Francisc” Centre from Brașov, “Inochentie Micu Klein” Home for Elderly People, Support Centre for Crisis Situations, Neuropsychiatric Recovery and Rehabilitation Centre (SINERSIG), Adam Muller Gutenbrunn Complex (two managers) and “Saint Nicholas” Complex for Elderly People from Lugoj offered no answer on this topic. The manager from Ciacova Care and Assistance Centre answered that the models are “identical” to the ones used in his institution. The manager from the Periam Neuropsychiatric Recovery and Rehabilitation Centre and one of the three managers from the Adam Muller Gutenbrunn Complex (woman, no declared age, bachelor degree) stated that she didn’t know models of good practices from other institutions, but she assumed that in most institutions everything possible was done in the best interest of the beneficiaries (woman, 42 years old, master graduate). The good practices from other institutions were correlated with legal norms issued by the authorities by the managers of the Gavojdia Neuropsychiatric Recovery and Rehabilitation Centre, Caritas Centre Timișoara and the Schwabenhause–Lenauheim Home for the Elderly. The manager from the Anitaheim Varel Home for the Elderly from Lugoj mentioned that social distancing remains an issue necessary and difficult to tolerate. |
| Respondents' relationship with God | With the exception of two managers (i.e. Ciacova Care and Assistance Centre, Caritas Centre Timișoara), all the interviewees mentioned that their faith in God they helped them get through the pandemic more easily. |
To all the dimensions sociodemographic variables are added: gender, age, area of residence, last level of education completed, the field in which they worked.
4. Discussion and conclusions
In our research we aimed to examine the ways in which the care centers for the elderly acted and adapted during the pandemic period, by taking into account the opinions of the beneficiaries, of the employees and of the managers of those centres. In this regard, in our research we used a mixed method approach, by applying a questionnaire to the beneficiaries of the care centers and also by conducting interviews with beneficiaries, employees and managers of the care centres.
Considering the results of the quantitative research, our research showed that the institutionalized elderly described, in general, the care centres while using positive words, and that most of the elderly were institutionalized because they remained alone, with having no other people to care for them. However, a significant number of the respondents also declared that they were institutionalized due to the fact that they had health problems which required assistance that could no longer be provided at home.
Taking into account the beneficiaries’ satisfaction with their life in the care centre, the results of the research revealed that most respondents were mainly satisfied with their life and the level of satisfaction does not differ depending on their gender or on their initial living environment (urban/rural). However, the research revealed differences depending on the age of the respondents in the sense that adults under 64 years old were significantly more satisfied than adults aged 65 to 74, but also that adults aged 75 to 84 were significantly more satisfied than those aged 65 to 74. In this regard, although the results showed differences according to age, we could conclude whether the level of satisfaction with the life in the centres increases or decreases with age. Thus, in order to clarify the matter, this issue could be also analysed from a qualitative perspective.
Moreover, the findings showed that the time spent in the care centre can influence the beneficiaries’ level of satisfaction with their life. In this regard, the results revealed that those who spent up to two years in the care centres were significantly more satisfied than adults who lived there for a period of 2 to 4 years.
Given the difficulties the elderly experienced in the care centres, the main difficulty mentioned was the impossibility of being close to loved ones, it being followed by the difficulty of adapting to the living conditions within the centre. Hence, the institutionalized elderly were affected by the fact that while being in the centre, they were away from their family and friends, and by the fact that they had to adjust to a new way of living, compared to the one they had at home. In this regard, our research is in line with a previous study [4], which emphasized the disadvantages of living in a care centre, disadvantages such as social exclusion, or the impossibility to establish solid social relationships.
Considering the type of medical services they usually receive, most respondents declared they receive therapeutic massages, that they do therapeutic gymnastics, and that they receive physical therapy. Thus, as expected, the results of the research showed that gender and age are elements that influence the type of medical help received by the beneficiaries. In this regard, men requested to a greater extent than women therapeutic massages and medical assistance, while women requested more than men recuperative gymnastics, physical therapy, or assistance in basic activities. Also, adults aged 65 to 74, were the ones who requested therapeutic services more than the other age groups categories.
Taking into account the main leisure activities carried out by the beneficiaries, the findings revealed that most respondents declared they mostly watch TV shows, that they play board games with the other residents or that the take walks in the inner courtyard of the centre.
In the context of the COVID – 19 pandemic, the beneficiaries described the period while using positive but also negative words such as isolation, restriction, stress. The respondents considered to a small extent that the pandemic influenced the process of improving their physical health, and most of them declared that their need have been met to a great extent during this period. However, most respondents stated that they have felt “alone, restless, “nervous”, “helpless” and sad, during the pandemic and the research revealed that these emotional states were not influenced by the gender of the respondents. In other words, we found no differences in the emotions felt by the elderly depending on their gender.
Given the restrictions the elderly had to comply with in the pandemic period, our research is in line with previous studies which described similar measures taken in order to assure the well-being of people, measures such as the prohibition of group activities, the limitation of movements outside the premises, isolation in their own rooms [7,10], and limiting all social activities and restricting all visits [8]. Hence, most of the respondents of our research mentioned restrictions such as: having fewer roommates, impossibility to play board games, wearing masks, limitation of the number of people who had access to common spaces and limitation of the time they were allowed to spend in the common spaces. Hence, even though we expected beneficiaries to develop negative attitudes towards the staff of the care centres in the pandemic periods, the results showed that most respondents had positive opinions, them considering the quality of the services they received to be good and very good.
Furthermore, according to the results of the research, the measures taken within the centres were quite restrictive, the beneficiaries not being allowed to watch TV shows, or take walks in the inner courtyard of the centre, or to socialize and interact with the other members of the centre. In this regard, in the pandemic period, the elderly missed the most the possibility to take walks outside the centre and the possibility to socialize with the other residents.
When being asked to state the biggest difficulty encountered during the pandemic, most of the respondents referred to the impossibility to communicate with family members / close persons, to the fact that they had to adapt to the new living conditions in the centre, that they weren’t allowed to interact with the other members of the centre, and that their feelings of loneliness increased. From this perspective, our research is in line with a previous study [6], which highlighted that the pandemic increased the elderly’s feeling of loneliness and limited their social relationships. Comparing the respondents of the elderly about difficulties encountered in general and in the COVID – 19 period in particular, we observed that those difficulties are similar in the sense they refer to the idea of adapting to a new lifestyle and to the idea that institutionalization and the pandemic both affected communication with family members or friends. Moreover, the research showed that variables such as age or living environment did not influence the opinion about the main difficulties encountered, but the opinion of the respondents was influenced by age and time spent in the care centre. In this regard, while the main difficulty mentioned referred to the impossibility to communicate with family members, the dominant percentages of the respondents who felt this difficulty was represented by adults aged 65 to 74 and by those who had been in the centre for a period of 2 to 4 years.
Considering the way beneficiaries managed to maintain communication with their family members or loved ones, the finding indicated that the communication process was mainly maintained through the usual phone calls. We expected the elderly to communicate with friends or family through video calls, but due to lack of technology skills and knowledge, most of them resorted to phone calls. From this perspective our study is in line with a previous study [43], which showed that even if they have phones, the elderly do not usually use apps that require internet.
Furthermore, face to face interaction with the family members was not possible during the pandemic, and the interesting results of our research showed that even in these conditions, most respondents declared their relationships with family members remained the same, and some of them even stated that they improved. A possible explanation for this result could be represented by the fact that, it is possible that during the pandemic the families were more concerned with the well- being of the institutionalized elderly and as a result, they may have called them more often compared to the pre-pandemic period. This idea is indirectly supported by a previous study [11], which showed that the frequency of communication influences the satisfaction of the beneficiaries, and that the social support received through the phone calls decreased the negative effects of isolation on the mental health of the patients.
Similar to the attitude towards the relationship with family members, the research revealed that the elderly were satisfied with the interactions they had with the staff of the care centres and they even mentioned that in the pandemic period, the employees paid more attention to them than before. However, when the role of the pandemic in influencing the opinion of the elderly about the interaction with employees was measured, the results showed that the more important the influence of COVID – 19 was, the more the beneficiaries tended to perceive in a negative manner the relationship with the employees.
Taking into account the suggestions of the beneficiaries regarding improving the way of life of residents of the care centres, the main suggestions mentioned referred to: developing more collective/recreational activities, offering residents more freedom of movement, improving the spaces of the centres, encouraging the employees to have more empathy and respect for the patients, offering the possibility to receive more visits from family and friends, or taking measures in order to reassure discipline and peace within the centres. Such measures should be taken into consideration by the employees and the managers of care centres and the matter should also be approached in detail in a future research.
Considering the results of the qualitative research, in the context of the perception of the beneficiaries, the results showed that: most respondents stated that they adjusted rather well to the changes imposed by their move, but they had a hard time adapting to the changes which took place due to the COVID – 19 pandemic. The results of the qualitative research are similar to the results of the quantitative research in the sense that in both types of research, the beneficiaries stated that their main difficulty was represented by the impossibility to communicate or receive visits from family and friends. Moreover, the beneficiaries described the attitude of the employees as being good or acceptable.
Given the opinions of the employees, the findings revealed that physical distancing measures during the pandemic comprised the strict isolation of the beneficiaries, that the activities developed within the centre decreased significantly, that the main measure taken referred to isolating the elderly from their families and from the community and that their work hours increased. The most important task that employees had was to make sure the beneficiaries comply with the social distancing rules, they generally tried to have a good mood in their interactions with the patients and the employees observed that the beneficiaries manifested sadness, confusion, anger, frustration and even desperation during the pandemic period. Most of them stated they experienced solidarity from their colleagues or from their managers, and significant changes took place within the centre in the pandemic period, changes such as: isolation, the need to wear masks, social distancing.
In the context of the opinions of the managers, the findings showed that managers highlighted the inconsistencies between the measures imposed by the government at national level, they emphasized the difficulty to comply with all the measures in order to protect both the health of the beneficiaries and of the employees. Other difficulties encountered were represented by bureaucracy, having access to protective equipment, or the deficit of personnel. Given the most difficulty encountered by the beneficiaries, the managers stated that the elderly had a hard time understanding what was happening, that they had difficulties due to the fact that they had to remain isolated and they no longer had the opportunity to socialize with their relative or with the other members of the centre. Considering the most important task they had, managers declared that they struggled with keeping things normal, that they had to make sure the health of the beneficiaries and of the employees is protected, and that they had to offer updated information to the beneficiaries and to the employees. Managers described their mood as being stressed and even overloaded and they perceived the beneficiaries to be anxious and afraid. Furthermore, the managers also highlighted that they observed solidarity between the employees and the beneficiaries and they mentioned a series of measure which they would like to take in the future to improve the activity of the care centre. The main measures mentioned were represented by: keeping and improving discipline in the activities with beneficiaries, improving the ties between beneficiaries and employees, training the personnel for potential special situations that may require changes in the organization, hiring new personnel, improving teamwork by integrating the beneficiaries in the team, or improving the connections and the involvement of the local community.
Hence, both the employees and the managers were aware of the difficulties encountered by the beneficiaries during the pandemic, they tried to maintain a positive mood in their interactions with the beneficiaries and they tried to protect their health and well- being by complying with the social distancing rules. Moreover, the pandemic period generated feelings of solidarity between the beneficiaries and the employees and the pandemic also made managers aware of some measures they require to take in order to improve the way the care centres function.
Therefore, considering the theoretical and practical implications of our paper, from a theoretical point of view, our research contributes to the literature on the effects of the pandemic at the level of the elderly. From a practical perspective, our research offers a view on the lifestyle and struggle of the institutionalized elderly during the pandemic, it raises awareness regarding the struggles of the beneficiaries as well as of the employees and managers of these institutions, and it offers a series of measure which could be taken in account by managers in order to improve the activity of the care centres.
4.1. Limitations and future research directions
Considering the limitations of the research, one limitation is represented by the fact that the study was conducted only in a specific area of Romania, Timis county, and thus the results can not be generalized. However, the results are relevant considering that most care centres had to comply with the same rules during the pandemic, but in order to obtain a larger view on the matter of the lifestyle of the institutionalized elderly during the pandemic, a future research should take into consideration care centre from other regions of Romania and even care centre from other countries.
Another limitation refers to the fact that we obtained only the opinion of the institutionalized elderly and a future research should considering examining the opinion of the elderly that had to stay at home during the pandemic too, in order to analyse further if the COVID -19 pandemic influenced differently the lifestyle and the mental health of the elderly who stay at home and of the institutionalized elderly.
Author Contributions
Conceptualization, C.C., C.G., and L.P.; Methodology, F.A., C.G., C.B., and M.C.B..; Software, A.N. and C.C..; Validation, C.C., M.C.B., C.B., and L.P,.; Formal Analysis, C.C., A.N..; Investigation, C.B., G.C., F.A., L.P., and D.B..; Resources, C.G., C.B., G.C.,L.P., G.C, and F.A.; Data Curation, C.C., A.N., M.C.B., C.G., C.B, F.A., and L.P.; Writing – Original draft preparation, C.B., C.G., L.P, G.C., F.A., A.N., M.B., and M.C.B.; Writing – Review & Editing, C.C., C.B., C.G., M.C.B., F.A., L.P.,G.C., A.N., M.B., and D.B.; Visualization, C.C., C.G., C.B., L.P., M.B., M.C.B., and A.N..; Supervision, C.C..; Project Administration, C.C., C.G. A.N., M.C.B.
Funding
This research received no external funding.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by the Institutional Review Board (or Ethics Committee) of The Faculty of Sociology and Communication (HCF 1929/29.01.2022).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study.
Conflicts of Interest
The authors declare no conflict of interest.
Appendix A. Questionnaire applied to the beneficiaries
A. First of all, please answer some questions referring to your life in the healthcare centre/old age home before the start of the COVID 19 pandemic.
A1. Which is the first word that comes to your mind when you think about your lifestyle in the health care and assistance centre?
……………………………………………………………………………………………………….
A2. Why are you in this centre?
- because of my poor health I need supplementary care which cannot be offered at home
- the members of my family did not have the possibility to offer me the necessary care
- I remained alone and I do not have other people to take care of my wellbeing
- other.......................
A3. Since when are you a resident of this home?
- less than 1 year
- one year
- 3 two years
- three years
- four years
- more than 5 years
A4. Concerning the decision to come to this centre, this was made:
- by the members of my family
- by my acquaintances and close friends
- by you
- by someone else
A5. On a scale of 1 to 7, how satisfied are you with the way you are treated in the healthcare centre?
1 2 3 4 5 6 7
Extremely dissatisfied
very dissatisfied
quite dissatisfied
neither satisfied nor dissatisfied
quite satisfied
very satisfied
extremely satisfied
A6. On a scale of 1 to 7, how satisfied are you with the following services of the healthcare centre?
1
Extremely dissatisfied
very dissatisfied
quite dissatisfied
neither satisfied nor dissatisfied
quite satisfied
very satisfied
extremely satisfied
- the food you are offered 1 2 3 4 5 6 7
- Entertainment opportunities 1 2 3 4 5 6 7
- the activities organised by the centre (trips, events)1 2 3 4 5 6 7
- the medical care from the staff 1 2 3 4 5 6 7
- accommodation services 1 2 3 4 5 6 7
A7. Do you consider that in general the staff’s attitude towards you is:
- rather positive
- rather negative
- neither positive/nor negative
A8. Which is, in your opinion, the biggest difficulty you have encountered since you are in this centre?
- 1.
- The impossibility to be with the loved ones
- 2.
- the communication with the members of the family/close friends
- 2.
- socialisation with the other residents of the healthcare centre
- 3.
- adjusting to the living standards within the healthcare centre
- 4.
- the enhancement of the loneliness feeling
- 5.
- the relationship with the staff
- 6.
- other.........................................................................................................................
A9. In your particular case, what kind of medical/therapeutic services do you regularly benefit from within the healthcare centre?
- 1.
- psychological assistance
- 2.
- assistance in achieving the basic activities (hygiene, moving, feeding)
- 3.
- kineto-therapy
- 4.
- therapeutic massage
- 4.
- recovering gymnastics
- 5.
- others.............................................................................................................................................
A10. The main relaxing activities that you currently do in the centre are:
- Reading
- Watching TV shows
- Walks in the centre’s yard
- Socialisation with other residents by means of society games
- Maintaining fitness by doing easy physical exercises
- Participating in music evenings
- Others....................................................................................
A11. What is the activity that you like the most within the centre?
- Reading
- Watching TV shows
- Walks in the centre’s yard
- socialisation with other residents by means of society games
- maintaining fitness by doing easy physical exercises
- participating in music evenings
- others....................................................................................
..........................................................................................................................
A12. How do you usually communicate with the members of your family or other acquaintances/close friends?
- by phone
- by means of internet / mobile applications
- when they come to visit
- other ways...................................................................................................
B. Next, I would kindly ask you to answer some questions referring to your lifestyle in the centre during the COVID 19 pandemic.
B.1 How would you describe in one word your way of living in the centre after the start of COVID 19 pandemic? .........................................................................................
B2. On a scale of 1 to 7, please express the agreement with the following statements referring to your life in general:
- 1.
- definitely disagree
- 2.
- disagree
- 3.
- slightly disagree
- 4.
- neither agree nor disagree
- 5.
- slightly agree
- 6.
- agree
- 7.
- strongly agree
- a)
- In general, my life is very close to my ideal life 1 2 3 4 5 6 7
- b)
- My life conditions are excellent 1 2 3 4 5 6 7
- c)
- I am satisfied with the life I have 1 2 3 4 5 6 7
- d)
- Until now I have obtained the important things that I have wanted in my life 1 2 3 4 5 6 7
- e)
- If I could live my life again, I would not change anything 1 2 3 4 5 6 7
B3. Having in view your state of health, in what degree do you think the COVID 19
pandemic has affected the process of maintaining/improving your physical health?
1 2 3 4 5 6 7
Extremely low degree
Very low degree
Neither low nor high degree
High degree
Very high degree
Extremely high degree
B4. To what degree do you consider the impossibility to socialise with other residents during the pandemic has affected your psychic health?
1 2 3 4 5 6 7
Extremely low degree
Very low degree
Neither low nor high degree
High degree
Very high degree
Extremely high degree
B5. What emotional states did you experience during the pandemic? (multiple answer)
- Anxiety
- Restlessness
- Fear
- Depression
- Psychic fatigue
- Irritability
- Others..........................................................................
B6. Which of these emotional states did you feel the most during the pandemic? (only one answer)
- Anxiety
- Restlessness
- Fear
- Depression
- Psychic fatigue
- Irritability
- others..........................................................................
B7. During the pandemic you were mostly preoccupied with:
- your own health
- the health of your family members
- the health of your friends/acquaintances
- I do not know/ I do not answer
B8. Having in view the relaxation activities in the centre, what kind of activities you were not allowed to do during the pandemic?
- reading in public spaces
- walking in the yard of the centre
- relating with the other residents by means of society games
- watching TV shows in the common/public spaces
- participating in music evenings
- other........................................................................................
B9. Among the relaxation activities that you were not allowed to do during the pandemic which one did you miss the most?
B10. Taking into consideration the protection measures against infection or spread of the virus, what kind of physical distancing measures were taken in the centre?
- 1
- the limitation of the number of people who have access in the communal spaces
- 2
- the limitation of the time spent in the communal spaces of the centre
- 2
- the interdiction of the socialisation by means of society games
- 3
- the diminution of the room-mates’ number
- 4
- the achievement of the communal activities with the obligation of wearing a mask
- 5
- others..........................................................................................
B11. On a scale of 1 to 7, how do you appreciate the quality of services offered by the healthcare centre in the context of COVID 19 pandemic?
1 2 3 4 5 6 7
Extremely bad
Very bad
Quite bad
Neither bad nor good
Quite good
Very good
Extremely good
B12. Which was the biggest difficulty that you have encountered during the pandemic in the centre?
1. the impossibility to socialise with the other residents
2. the impossibility to communicate with the family members/close friends
3. adjusting to the new conditions of life in the centre
4. enhancing the loneliness feeling
5. relating with the staff
6. other....................................
B13. Having in view the relation with the family members/close friends to what degree did you keep in touch with them during the COVID 19 pandemic?
1 2 3 4 5 6 7
Extremely low degree
Very low degree
Neither low nor high degree
High degree
Very high degree
Extremely high degree
B14. What way of communicating with your family members/close friends did you use mostly during the pandemic?
- phone calls
- video calls by means of mobile applications
- visits in the centre
- other............................................................................................
B15. Referring to your relationship with family members/close friends during the pandemic, do you consider that this relationship:
- improved
- worsen
- stayed the same
- I do not know/I do not answer
B16. In the context of COVID 19 pandemic, were your family members/close friends allowed to visit you in the centre?
- Yes
- No
- I do not know/ I do not answer
B17. Concerning the technology, how often did you communicate on video with the closed people outside the centre by means of mobile applications?
1 2 3 4 5 6 7
Extremely rare
Very rare
Quite rare
Neither rare nor often enough
Often
Very often
Extremely often
B18. Taking into consideration the relationship with the staff in the centre during the pandemic do you consider that the employees’ attitude towards you was:
- rather positive
- rather negative
- neither positive, nor negative
B19. As compared to the period before the pandemic, did you feel that during the pandemic the staff has given you:
- more attention
- less attention
- neither more nor less attention
B20. Next, I would kindly ask you to express the agreement with the following statements:
- 1.
- Strong disagreement
- 2.
- Disagreement
- 3.
- Rather disagreement
- 4.
- Neither disagreement nor agreement
- 5.
- Rather agreement
- 6.
- Agreement
- 7.
- Strong agreement
- 1.
- The centre employees were more reticent towards me during the pandemic 1 2 3 4 5 6 7
- 2.
- For the assistants and caretakers in the centre, my needs represented a priority during the pandemic 1 2 3 4 5 6 7
- 3.
- The assistants and caretakers socialised less with the beneficiaries during the COVID 19 pandemic 1 2 3 4 5 6 7
B21. To what degree could you socialise with the other residents of the healthcare centre during the pandemic?
1 2 3 4 5 6 7
Extremely low degree
Very low degree
Neither low nor high degree
High degree
Very high degree
Extremely high degree
B22. What are the socialising ways with other people who live in the same centre in the context of COVID 19 pandemic?
- We have watched TV shows in the communal spaces respecting the rules of physical distancing
- We have socialised by means of phone calls
- We have socialised by means of video calls with mobile applications
- others......................
B23. Thinking about the emotional states created by the impossibility/reduced possibility of socialising with other members of the centre, most often during the pandemic you felt:
- Alone
- Restless
- Nervous
- Helpless
- other ways.................................................................................................................................
B24. To what degree do you consider that your needs were respected in the context of the COVID 19 pandemic?
1 2 3 4 5 6 7
Extremely low degree
Very low degree
Neither low nor high degree
High degree
Very high degree
Extremely high degree
B25. If you were the decision maker, which were the first three measures you would implement in order to improve the lifestyle of the residents of the health care centre?
- ............................................................
- ...........................................................
- ............................................................
B26. Where did you find out what the pandemic did in the country? .............................................
B26. Whom do you trust in the most within the centre?
C. In the end, please offer us the answer to some identification questions :
C1. Your gender
- male
- female
C2. Your age
...........................................................................
C3. Do you come from the:
- Urban area
- Rural area
C4. The last graduated school
- primary school
- secondary school
- high school
- faculty
- master
- 6ther………………………………
C5. The field you worked in:
- 1.
- IT
- 2.
- Sales
- 3.
- Services
- 4.
- Health
- 5.
- Education
- f)
- Other..................................
Thank you for your answer!
Appendix B. Interview guides
B1. Interview guide - the way of life of elderly people in care centers and the changes brought about by the covid-19 pandemic
- − How did you adjust to the changes imposed on your way of life when you moved to the care center ?
- − How have you adapted to these changes after the start of the covid-19 pandemic?
- − What changes have you noticed in your grooming?
- − Which changes of this type did/do you consider exaggerated, erroneous or even abusive? How did/do you deal with them?
- − What has been the most important task you have had or still have to complete since you have been in the care facility? (To yourself, to your family or to someone else.)
- − Have you contracted covid-19? Do you want to talk to us about this fact?
- − Have you lost loved ones, relatives or acquaintances to this disease?
- − What about someone else who did not get this disease, but did not receive the necessary/timely medical care as a result of the imposition of anti-covid measures?
- − How would you characterize the current mood of downtown residents?
- − But that of the management of the institution and the care staff?
- − Do you think that the pandemic has brought with it a change for the better in the consciousness and behavior of peers? (Including you, the staff, the management of the institution).
- − What do you consider to be the greatest achievement of your life?
- − Tell us about your relationship with God.... Are you a believer?
- − Would you like to add anything else? ------------
- − Your gender is
- − Your age in years is
- − You come from the environment
- − Last school completed
- − The field in which you worked
B2. Interview guide - challenges for care staff in residential care and the changes brought about by the covid-19 pandemic
- − What concrete physical distancing measures were you able to take/respect in the care of the beneficiaries and in the usual activities in the institution?
- − How would you characterize the sanitary measures in the country imposed during this period?
- − How did these measures influence the way you did your business? What was the biggest difficulty you encountered in this regard?
- − What do you think was the biggest difficulty faced by your beneficiaries?
- − Have you lost beneficiaries, relatives or acquaintances to this disease?
- − But someone who did not get sick from this virus, but did not receive the necessary medical care / in a timely manner as a result of the imposition of anti-covid measures?
- − What has been the most important task you have had or still have to complete in relation to your own conscience and to the beneficiaries?
- − How would you characterize the current mood of downtown residents?
- − What about yours and the care staff?
- − Have you noticed a real solidarity in the behavior of the institution's employees (managers, care staff), as well as the beneficiaries after the pandemic?
- − Do you think that the pandemic has brought with it a change for the better in the consciousness and behavior of peers? (Including you, the staff, the management of the institution, the beneficiaries).
- − What changes have occurred in the activity and personnel scheme of the institution? (number/period of quarantines, resignations, layoffs, changes regarding involvement in direct activity with beneficiaries, employment, etc.)
- − How did you find out that care for the elderly would be done now in similar institutions, both in the country and abroad?
- − Tell us, if you can, about your relationship with God. How has faith influenced the realities you have experienced in the past year?
- − Would you like to add anything else?
- − Your gender is
- − Your age in years is
- − Last school completed
- − Your experience in aged care is:
- − Your job description provides care and responsibilities towards ..../ (number of) beneficiaries.
B3. Interview guide- the challenges of managers of elderly care centers during the pandemic
- − What concrete physical distancing measures were you able to take/respect in the care of the beneficiaries and in the usual activities in the institution?
- − How would you characterize the sanitary measures in the country imposed during this period?
- − How did these measures influence the way you did your business? What was the biggest difficulty you encountered in this regard?
- − What do you think was the biggest difficulty faced by your beneficiaries?
- − Have you lost beneficiaries, relatives or acquaintances to this disease?
- − But someone who did not get sick from this virus, but did not receive the necessary medical care / in a timely manner as a result of the imposition of anti-covid measures?
- − What has been the most important task you have had or still have to complete in relation to your own conscience and to the beneficiaries?
- − How would you characterize the current mood of downtown residents?
- − What about yours and the care staff?
- − Have you noticed a real solidarity in the behavior of the institution's employees and the beneficiaries after the pandemic?
- − Do you think that the pandemic has brought with it a change for the better in the consciousness and behavior of peers? (Including you, your beneficiaries, and your institution's employees.)
- − What models of good practice do you know in similar institutions, both in the country and abroad? ------------
- − What changes occurred/imposed in the organization of the institution's activities during the pandemic? (Resignations, quarantines, changes regarding involvement in direct activity with beneficiaries, employment, etc.)
- − What changes do you want to make in the future in the management of the institution?
- − Tell us, if you can, about your relationship with God. How has faith influenced the realities you have experienced in the past year?
- − Would you like to add anything else?
- − Your gender is
- − Your age in years is
- − Last school completed
- − Your experience in aged care is of
- − Your social work experience is of
References
- Rojo-Perez, F.; Rodriguez-Rodriguez, V.; Fernandez-Mayoralas, G.; Sánchez-González, D.; Perez de Arenaza Escribano, C.; Rojo-Abuin, J.-M.; Forjaz, M.J.; Molina-Martínez, M.-Á.; Rodriguez-Blazquez, C. Residential Environment Assessment by Older Adults in Nursing Homes during COVID-19 Outbreak. Int J Environ Res Public Health 2022, 19, 16354. [Google Scholar] [CrossRef] [PubMed]
- Dolberg, P.; Lev, S.; Even-Zahav, R. “Let Me Touch Him”: Perceptions and Experiences of Family Caregivers of Nursing Home Residents during the COVID-19 Outbreak in Israel. J Aging Stud 2023, 64, 101115. [Google Scholar] [CrossRef] [PubMed]
- Chen, C.-Y. Analysing the Quality of Life of Older Adults: Heterogeneity, COVID-19 Lockdown, and Residential Stability. International Journal of Environmental Research and Public Health 2022, 19, 12116. [Google Scholar] [CrossRef] [PubMed]
- Araújo, P.O. de; Freitas, M.Y.G.S.; Carvalho, E.S. de S.; Peixoto, T.M.; Servo, M.L.S.; Santana, L. da S.; Silva, J.M.D.S.; Moura, J.C.V. Institutionalized Elderly: Vulnerabilities and Strategies to Cope with Covid-19 in Brazil. Invest Educ Enferm 2021, 39, e07. [Google Scholar] [CrossRef] [PubMed]
- Rodriguez-Rodriguez, V.; Rojo-Perez, F.; Perez de Arenaza Escribano, C.; Molina-Martínez, M.-Á.; Fernandez-Mayoralas, G.; Sánchez-González, D.; Rojo-Abuin, J.-M.; Rodríguez-Blázquez, C.; Forjaz, M.J.; Martín García, S. The Impact of COVID-19 on Nursing Homes: Study Design and Population Description. Int J Environ Res Public Health 2022, 19, 16629. [Google Scholar] [CrossRef] [PubMed]
- Pascut, S.; Feruglio, S.; Crescentini, C.; Matiz, A. Predictive Factors of Anxiety, Depression, and Health-Related Quality of Life in Community-Dwelling and Institutionalized Elderly during the COVID-19 Pandemic. Int J Environ Res Public Health 2022, 19, 10913. [Google Scholar] [CrossRef] [PubMed]
- Noten, S.; Stoop, A.; De Witte, J.; Landeweer, E.; Vinckers, F.; Hovenga, N.; van Boekel, L.C.; Luijkx, K.G. “Precious Time Together Was Taken Away”: Impact of COVID-19 Restrictive Measures on Social Needs and Loneliness from the Perspective of Residents of Nursing Homes, Close Relatives, and Volunteers. International Journal of Environmental Research and Public Health 2022, 19, 3468. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Xiao, L.D.; Nan, J.; Zhao, S.; Yin, P.; Zhang, D.; Liao, L.; Li, M.; Yang, X.; Feng, H. Nursing Home Residents’ Perceptions of Challenges and Coping Strategies during COVID-19 Pandemic in China. Int J Environ Res Public Health 2023, 20, 1485. [Google Scholar] [CrossRef]
- Burgaña Agoües, A.; Serra Gallego, M.; Hernández Resa, R.; Joven Llorente, B.; Lloret Arabi, M.; Ortiz Rodriguez, J.; Puig Acebal, H.; Campos Hernández, M.; Caballero Ayala, I.; Pavón Calero, P.; et al. Risk Factors for COVID-19 Morbidity and Mortality in Institutionalised Elderly People. Int J Environ Res Public Health 2021, 18, 10221. [Google Scholar] [CrossRef]
- Richardson, G.; Cleary, R.; Usher, R. The Impact of the COVID-19 Restrictions on Nursing Home Residents: An Occupational Perspective. Journal of Occupational Science 2022, 29, 386–401. [Google Scholar] [CrossRef]
- Crespo-Martín, A.; Palacios-Ceña, D.; Huertas-Hoyas, E.; Güeita-Rodríguez, J.; Fernández-Gómez, G.; Pérez-Corrales, J. Emotional Impact and Perception of Support in Nursing Home Residents during the COVID-19 Lockdown: A Qualitative Study. Int J Environ Res Public Health 2022, 19, 15712. [Google Scholar] [CrossRef] [PubMed]
- Elaidy, A.M.; Hammoud, M.S.; N. Albatineh, A.; Ridha, F.M.; Hammoud, S.M.; Elsadek, H.M.; Rahman, M.A. Coping Strategies to Overcome Psychological Distress and Fear during COVID-19 Pandemic in Kuwait. Middle East Current Psychiatry, Ain Shams University 2023, 30, 12. [Google Scholar] [CrossRef]
- Chirico, F. Spirituality to Cope with COVID-19 Pandemic, Climate Change and Future Global Challenges. Journal of Health and Social Sciences 2021, 6, 151–158. [Google Scholar] [CrossRef]
- Oliveira, A.F.; Brites, M.J.; Cerqueira, C. Intergenerational Perspectives on Media and Fake News During Covid-19: Results From Online Intergenerational Focus Groups. Media and Communication 2022, 10, 277–288. [Google Scholar] [CrossRef]
- Giri, S.P.; Maurya, A.K. A Neglected Reality of Mass Media during COVID-19: Effect of Pandemic News on Individual’s Positive and Negative Emotion and Psychological Resilience. Pers Individ Dif 2021, 180, 110962. [Google Scholar] [CrossRef] [PubMed]
- Pakalniškienė, V.; Kairys, A.; Jurkuvėnas, V.; Mikuličiūtė, V.; Ivleva, V. Could Belief in Fake News Predict Vaccination Behavior in the Elderly? International Journal of Environmental Research and Public Health 2022, 19, 14901. [Google Scholar] [CrossRef] [PubMed]
- Anwar, K.; Adnan, M. Online Learning amid the COVID-19 Pandemic: Students Perspectives. Journal of Pedagogical Research 2020, 1, 45–51. [Google Scholar] [CrossRef]
- Ng, R.; Tan, Y.W. Media Attention toward COVID-19 across 18 Countries: The Influence of Cultural Values and Pandemic Severity. PLOS ONE 2022, 17, e0271961. [Google Scholar] [CrossRef]
- Giritli Nygren, K.; Klinga, M.; Olofsson, A.; Öhman, S. The Language of Risk and Vulnerability in Covering the COVID-19 Pandemic in Swedish Mass Media in 2020: Implications for the Sustainable Management of Elderly Care. Sustainability 2021, 13, 10533. [Google Scholar] [CrossRef]
- Steultjens, E.M.J.; Dekker, J.; Bouter, L.M.; Jellema, S.; Bakker, E.B.; van den Ende, C.H.M. Occupational Therapy for Community Dwelling Elderly People: A Systematic Review. Age Ageing 2004, 33, 453–460. [Google Scholar] [CrossRef]
- Lor, Y.-C.M.; Tsou, M.-T.; Tsai, L.-W.; Tsai, S.-Y. The Factors Associated with Cognitive Function among Community-Dwelling Older Adults in Taiwan. BMC Geriatrics 2023, 23, 116. [Google Scholar] [CrossRef] [PubMed]
- Clegg, A.; Young, J.; Iliffe, S.; Rikkert, M.O.; Rockwood, K. Frailty in Elderly People. Lancet 2013, 381, 752–762. [Google Scholar] [CrossRef]
- Nerobkova, N.; Park, Y.S.; Park, E.-C.; Shin, J. Frailty Transition and Depression among Community-Dwelling Older Adults: The Korean Longitudinal Study of Aging (2006–2020). BMC Geriatrics 2023, 23, 148. [Google Scholar] [CrossRef] [PubMed]
- Ibáñez-del Valle, V.; Corchón, S.; Zaharia, G.; Cauli, O. Social and Emotional Loneliness in Older Community Dwelling-Individuals: The Role of Socio-Demographics. International Journal of Environmental Research and Public Health 2022, 19, 16622. [Google Scholar] [CrossRef] [PubMed]
- Golden, J.; Conroy, R.M.; Bruce, I.; Denihan, A.; Greene, E.; Kirby, M.; Lawlor, B.A. Loneliness, Social Support Networks, Mood and Wellbeing in Community-Dwelling Elderly. Int J Geriatr Psychiatry 2009, 24, 694–700. [Google Scholar] [CrossRef] [PubMed]
- Crewdson, J. The Effect of Loneliness in the Elderly Population: A Review. Healthy Aging & Clinical Care in the Elderly 2016, 8, 1. [Google Scholar] [CrossRef]
- Oduro, J.K.; Okyere, J.; Nyador, J.K.M.T. Risky Health Behaviours and Chronic Conditions among Aged Persons: Analysis of SAGE Selected Countries. BMC Geriatrics 2023, 23, 145. [Google Scholar] [CrossRef]
- Kojima, G. Frailty as a Predictor of Nursing Home Placement Among Community-Dwelling Older Adults: A Systematic Review and Meta-Analysis. J Geriatr Phys Ther 2018, 41, 42–48. [Google Scholar] [CrossRef]
- Chen, P.; Cai, H.; Bai, W.; Su, Z.; Tang, Y.-L.; Ungvari, G.S.; Ng, C.H.; Zhang, Q.; Xiang, Y.-T. Global Prevalence of Mild Cognitive Impairment among Older Adults Living in Nursing Homes: A Meta-Analysis and Systematic Review of Epidemiological Surveys. Transl Psychiatry 2023, 13, 88. [Google Scholar] [CrossRef]
- Johnson, R.; Popejoy, L.L.; Radina, M.E. Older Adults’ Participation in Nursing Home Placement Decisions. Clin Nurs Res 2010, 19, 358–375. [Google Scholar] [CrossRef]
- Smoliner, C.; Norman, K.; Wagner, K.-H.; Hartig, W.; Lochs, H.; Pirlich, M. Malnutrition and Depression in the Institutionalised Elderly. Br J Nutr 2009, 102, 1663–1667. [Google Scholar] [CrossRef] [PubMed]
- Vossius, C.; Borda, M.G.; Lichtwarck, B.; Myhre, J.; Sollid, M.I.V.; Borza, T.; Feiring, I.H.; Benth, J.Š.; Bergh, S. Body Mass Index in Nursing Home Residents during the First Year after Admission. BMC Nutr 2023, 9, 50. [Google Scholar] [CrossRef] [PubMed]
- Hua, N.; Zhang, Y.; Tan, X.; Liu, L.; Mo, Y.; Yao, X.; Wang, X.; Wiley, J.; Wang, X. Nutritional Status and Sarcopenia in Nursing Home Residents: A Cross-Sectional Study. Int J Environ Res Public Health 2022, 19, 17013. [Google Scholar] [CrossRef] [PubMed]
- Effendy, E.; Prasanty, N.; Utami, N. The Effects of Brain Gym on Quality of Sleep, Anxiety in Elderly at Nursing Home Care Case Medan. Open Access Maced J Med Sci 2019, 7, 2595–2598. [Google Scholar] [CrossRef] [PubMed]
- Segura Cardona, A.; Cardona Arango, D.; Segura Cardona, A.; Robledo Marín, C.; Muñoz Rodríguez, D. Friendly Residential Environments That Generate Autonomy in Older Persons. Int J Environ Res Public Health 2023, 20, 409. [Google Scholar] [CrossRef] [PubMed]
- Wang, Z.; Shepley, M. The Relationship of Neighborhood Walking Behavior to Duration of Aging in Place—A Retrospective Cohort Study. International Journal of Environmental Research and Public Health 2022, 19, 16428. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Shen, H.; Tan, L.; Huang, Q.; Chen, Q.; Liang, M.; He, L.; Zhou, Y. Prevalence and Factors Associated with Anxiety and Depression among Community-Dwelling Older Adults in Hunan, China: A Cross-Sectional Study. BMC Psychiatry 2023, 23, 107. [Google Scholar] [CrossRef]
- Vandervelde, S.; Vlaeyen, E.; de Casterlé, B.D.; Flamaing, J.; Valy, S.; Meurrens, J.; Poels, J.; Himpe, M.; Belaen, G.; Milisen, K. Strategies to Implement Multifactorial Falls Prevention Interventions in Community-Dwelling Older Persons: A Systematic Review. Implementation Science 2023, 18, 4. [Google Scholar] [CrossRef]
- Van Offenwert, E.; Schoenmakers, B. The Predictive Value of Weight Evolution in Screening for Malnutrition in Community-Dwelling Older Persons (70+) in Antwerp. BMC Primary Care 2023, 24, 64. [Google Scholar] [CrossRef]
- Farrell, A.; Castro, T.; Nalubola, S.; Lakhi, N. Trauma-Related Falls in an Urban Geriatric Population: Predictive Risk Factors for Poorer Clinical Outcomes. Inj Epidemiol 2023, 10, 7. [Google Scholar] [CrossRef]
- Creswell, J.W.; Plano Clark, V.L. Designing and Conducting Mixed Methods Research, 2nd ed.; SAGE Publications: Los Angeles, 2011; ISBN 978-1-4129-7517-9. [Google Scholar]
- Babbie, E. Practica Cercetarii Sociale [The Practice of Social Research]; 2nd ed.; Polirom: Iasi, 2010; ISBN 978-973-46-1274-1. [Google Scholar]
- Metro Media Transilvania, Studiu cantitativ privind utilizarea serviciilor de comunicații electronice de către utilizatorii finali-persoane fizice Available online:. Available online: https://statistica.ancom.ro/sscpds/public/alldocuments/marketstudy (accessed on 21 May 2022).
Figure 1.
A single word which characterizes the life in care and support centers. Created with worditout.com.
Figure 1.
A single word which characterizes the life in care and support centers. Created with worditout.com.

Figure 2.
A single word which characterizes the life in care and support centers during the pandemic.
Figure 2.
A single word which characterizes the life in care and support centers during the pandemic.
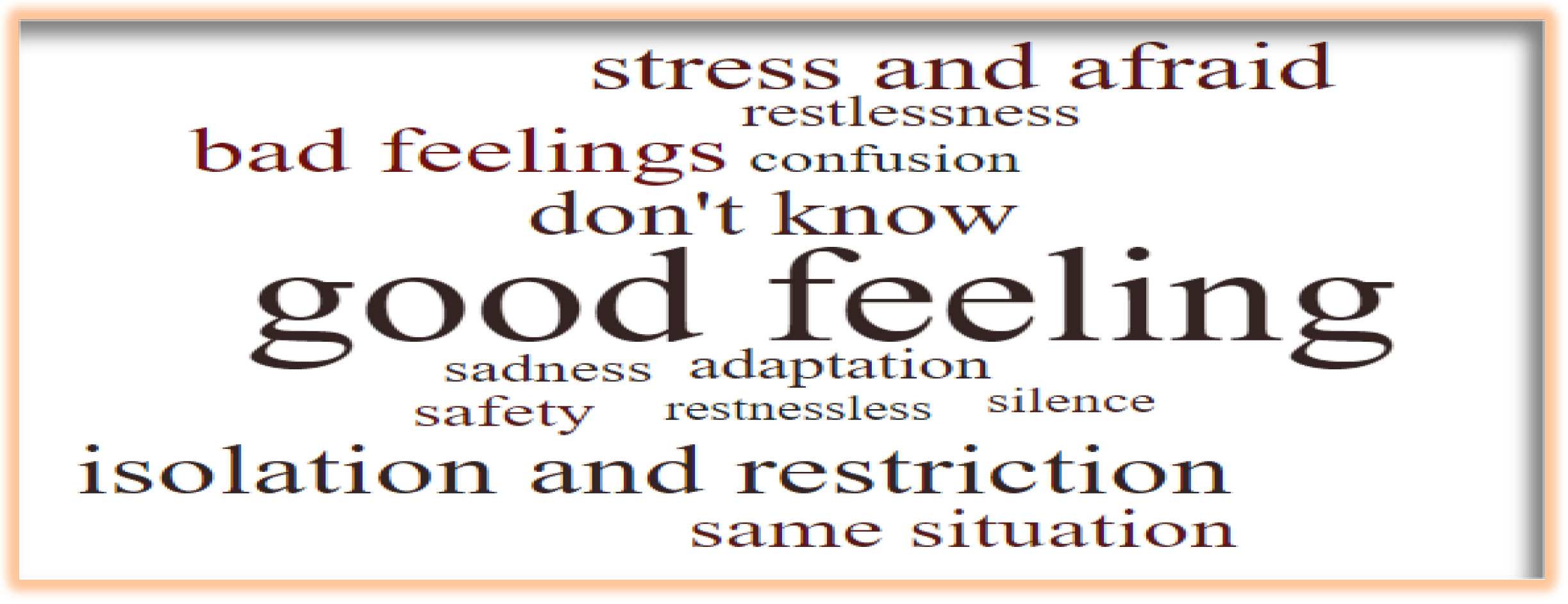
Table 1.
The main reason to be in care and support center.
| Frequency | Percent | |
|---|---|---|
| I was left alone and I have no other people to care about my well-being | 190 | 44.4% |
| Due to my health, I need additional care that cannot be provided at home | 124 | 29.0% |
| Family members no longer had the opportunity to provide me with the necessary care | 94 | 22.0% |
| Without shelter | 2 | 0.5% |
| Personal desire | 2 | 0.5% |
| Another reason | 16 | 3.7% |
Table 2.
Descriptive statistics for global index of satisfaction.
| Descriptive Statistics | |||||
|---|---|---|---|---|---|
| N | Minimum | Maximum | Mean | St. Dev. | |
| GIS | 430 | 1.00 | 7.00 | 5.36 | 1.13 |
| Valid N (listwise) | 430 | ||||
Table 3.
The principal difficulty encountered within care and support centre.
| Percent | |
|---|---|
| the impossibility of being close to loved ones | 38.3% |
| accommodation to the living conditions within the center | 16.1% |
| communication with family members/close people | 15.6% |
| increasing the feeling of loneliness | 8.1% |
| socializing with the other residents of the care center | 7.1% |
| the relationship with the staff | 6.2% |
| the impossibility of having money | 0.5% |
| difficulty of living among seniors with neuro-psychiatric conditions | 0.5% |
| I did not encounter any difficulties | 5.2% |
| another | 2.4% |
Table 4.
What kind of medical/therapeutic services do you usually receive?
| Percent | |
|---|---|
| therapeutic massage | 19.6% |
| recuperative gymnastics | 18.9% |
| physical therapy | 18.4% |
| assistance in carrying out basic activities (hygiene, travel, feeding) | 10.6% |
| psychological assistance | 9.1% |
| medical assistance (routine/ basic medical consultations) | 2.5% |
| other services | 20.9% |
Table 5.
The crosstabulation of the multiple responses’ variable therapies and independent variables gender and the life stage.
Table 5.
The crosstabulation of the multiple responses’ variable therapies and independent variables gender and the life stage.
| male | female | under 64 years old | young-old, ages 65–74 | the middle-old, ages 75–84 | old-old, over age 85 | |
|---|---|---|---|---|---|---|
| Count | Count | |||||
| therapeutic massage | 194 | 180 | 76 | 196 | 70 | 32 |
| recuperative gymnastics | 174 | 188 | 80 | 184 | 68 | 30 |
| physical therapy | 174 | 178 | 72 | 186 | 64 | 30 |
| assistance in carrying out basic activities (hygiene, travel, feeding) | 94 | 108 | 28 | 116 | 34 | 24 |
| psychological assistance | 82 | 92 | 26 | 84 | 44 | 20 |
| medical assistance (routine/ basic medical consultations) | 28 | 20 | 10 | 24 | 8 | 6 |
| other services | 186 | 214 | 82 | 198 | 80 | 40 |
| Chi Square test of independence | Chi Square=25.93, df=7, p=0.001 | Chi Square=65. 01, df=21, p=0.000 | ||||
Table 6.
Main leisure activities in the care and support center.
| Activities | Percents | |
|---|---|---|
| reading | 7.9 | |
| watching TV shows | 22 | |
| walks in the inner courtyard of the center | 12.1 | |
| socializing with other residents through board games | 15 | |
| maintaining the physical condition through light physical exercises | 6.1 | |
| participation in music evenings | 4.2 | |
| other | 32.7 | |
Table 7.
Evaluation of health, mental health status and personal needs.
| Percentages of those who declared …. | …to a small and very small extent | …neither largely nor to a small extent | …to a great and very great extent |
|---|---|---|---|
| Given your health status, to what extent do you think the COVID 19 pandemic has affected the process of improving your physical health? | 47% | 19% | 34% |
| To what extent do you think the impossibility of socializing with other residents during the pandemic has affected your mental health? | 52% | 14% | 32% |
| To what extent do you consider that your needs have been respected in the context of the COVID 19 pandemic | 9% | 16% | 75% |
Table 8.
Emotional state during the pandemic.
| During the pandemic have you been through.... | Percent of respondents |
|---|---|
| anxiety | 78 |
| restlessness | 58 |
| fear | 63 |
| depression | 84 |
| mental fatigue | 86 |
| nervousness | 75 |
Table 9.
Quantifying the number of negative emotional states.
| During the pandemic have you been through.... | Percent of respondents |
|---|---|
| all the six states | 41 |
| five of them | 30 |
| four of them | 7.5 |
| three of them | 11.5 |
| two of them | 3 |
| just one of them | 4 |
| another negative state neither one of them |
2.5 0.5 |
Table 10.
Evaluation of the services during the pandemic.
| Percentages of those who declared (valid percent) |
extremely weak and rather weak | neither good nor weak | good and very good |
|---|---|---|---|
| On a scale of 1 to 7, how do you assess the quality of the services offered by the care center in the context of the COVID 19 pandemic | 5% | 10% | 85% |
Table 11.
Activities that you were not allowed to do during the pandemic.
| Activities | Percents of respondens |
|
|---|---|---|
| reading | 83 | |
| watching TV shows | 84 | |
| walks in the inner courtyard of the center | 53 | |
| socializing with other residents through board games | 66 | |
| participation in music evenings | 71 | |
| other | 86 | |
Table 12.
During the pandemic which of the activities did you miss the most?
| Desired activities | Percents of responses |
|---|---|
| walks outside the care center | 32 |
| socializing with other residents in common activities | 15 |
| meetings with family/relatives | 9 |
| physical activities/sport | 6 |
| going to church/religious activities | 4 |
| watching TV shows | 3 |
| participation in music evenings | 3 |
| walks in the inner courtyard of the center | 1 |
| other | 5 |
| I don t know | 22 |
Table 13.
The biggest difficulty encountered during the pandemic.
| Percents of cases |
|
|---|---|
| impossibility to socialize with other residents (1) | 10.5 |
| impossibility to communicate with family members / close persons (2) | 47 |
| accommodation to the new living conditions within the center (3) | 19.5 |
| accentuating the feeling of loneliness (4) | 10 |
| understanding the truth about the pandemic and the treatment of the covid disease (5) | 11.5 |
| relations with staff (6) | 1.5 |
Table 14.
Crosstabulation of variables life stage and time spent in the center.
| Variables | n | Difficult problems* | ꭓ2 | df | p | |||||
| 1 | 2 | 3 | 4 | 5 | 6 | |||||
|
Life stage 1.under 64 years old |
74 | 8(10.8**) | 30(40.5) | 12(16.2) | 4(5.4) | 2(2.7) | 18(24.3) | 38.51 | 10 | 0.000 |
| 2.young-old, ages 65–74 | 202 | 24(11.9) | 84(41.6) | 50(24.8) | 28(13.9) | 4(2) | 12(5.9) | |||
| 3. the middle-old and old-old, ages 75 and over | 124 | 10(8.1) | 74(59.7) | 16(12.9) | 8(6.5) | 0 | 16(12.9) | |||
| Total | 400 | 42(10.5) | 188(47) | 78(19.5) | 40(10) | 6(1.5) | 46(11.5) | |||
|
time spent in center 1.Up to two years |
108 | 8(7.4) | 46(42.6) | 26(24.1) | 20(18.5) | 2(1.9) | 6(5.6) | 28.55 | 10 | 0.001 |
| 2.2-4 years | 132 | 18(13.6) | 52(39.4) | 26(19.7) | 14(10.6) | 2(1.5) | 20(15.2) | |||
| 3.4 years and over | 160 | 16(10) | 90(56.3) | 26(16.3) | 6(3.8) | 2(1.3) | 20(12.5) | |||
| Total | 400 | 42(10.5) | 188(47) | 78(19.5) | 40(10) | 6(1.5) | 46(11.5) | |||
*Codification for the variable ‘difficult problems’ are from Table 13. ** The percentages per line are specified in parentheses.
Table 15.
Way of communicating with family members/loved ones during the pandemic.
| Way of communicating | Percent of respondents |
|---|---|
| Phone calls | 76.5 |
| Video calls via mobile applications | 14.5 |
| Visits to the centre | 1 |
| Other situations | 8 |
Table 16.
Descriptive statistics for the index of the perception of the relationship with the staff.
Table 16.
Descriptive statistics for the index of the perception of the relationship with the staff.
| Descriptive Statistics | |||||
| N | Minimum | Maximum | Mean | Std. Deviation | |
| perstaff | 422 | 1.33 | 7.00 | 4.9115 | 1.22677 |
| Valid N (listwise) | 422 | ||||
Table 17.
Correlation between perstaff index and affected state of health.
| Considering your health, to what extent do you consider that the COVID 19 pandemic has affected the process of maintaining / improving physical health | perstaff | |||
| Spearman's rho | Considering your health, to what extent do you consider that the COVID 19 pandemic has affected the process of maintaining / improving physical health | Correlation Coefficient | 1.000 | -.386** |
| Sig. (2-tailed) | . | .000 | ||
| N | 428 | 420 | ||
| perstaff | Correlation Coefficient | -.386** | 1.000 | |
| Sig. (2-tailed) | .000 | . | ||
| N | 420 | 422 | ||
**. Correlation is significant at the 0.01 level (2-tailed).
Table 18.
Relationship with other residents during the pandemic.
|
Percentages of those who declared …. (valid percent) |
to an extremely small and to a small extent | neither largely nor to a small extent | to a large and extremely large extent |
| …to what extent have you been able to socialize with the other residents | 50% | 20% | 30% |
Table 19.
Suggestions for improving the way of life of care center residents.
| Proposals | Percentage |
|---|---|
| More collective/recreational activities | 17.3 |
| Freedom/freedom of movement | 10.9 |
| Arrangements of the interior/exterior space | 10.9 |
| More respect, empathy from the staff | 8.2 |
| More visits of the family members/relatives | 8.2 |
| More discipline, order, peace | 8.2 |
| The return to normality | 7.3 |
| Reducing the number of beneficiaries per room | 7.3 |
| Improving food, nutrition | 3.6 |
| Better hygiene and care conditions | 2.7 |
| Religious life | 1.8 |
| No change | 6.4 |
| Other proposal | 7.3 |
| Total | 100.0 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



