
Submitted:
12 May 2023
Posted:
15 May 2023
You are already at the latest version
Abstract
Currently, ovarian cancer (OC) is a target of intense biomarkers research because of its frequent late diagnosis and poor prognosis. Serum determination of Human epididymis protein 4 (HE4) is a very important early detection test. Most interestingly, HE4 plays a unique role in OC as it has been implicated not only in OC diagnosis but also in the prognosis and recurrence of this lethal neoplasm, actually acting as a clinical biomarker. There are several evidence about the predictive power of HE4 clinically, conversely less has been described concerning its role in OC oncogenesis. Based on these considerations, the main goal of this review is to clarify the role of HE4 in OC proliferation, angiogenesis, metastatization, immune response and also in the development of targeted therapy. Through a deeper understanding of its functions as a key molecule in the oncogenetic processes underlying OC, HE4 could be possibly considered as an essential resource not only for diagnosis but also for prognosis and therapy choice.
Keywords:
Ovarian cancer
; HE4
; oncogenesis
; target therapy
1. Introduction
Ovarian cancer (OC) is the eighth most common and the fifth deadliest cancer in women worldwide with a survival rate of just 30%. Symptoms are few and nonspecific, thus about 70 % of the cases are diagnosed in the advanced stages [1]. Ninety per cent of advanced ovarian cancer patients manifest malignant ascites ascribed to the progress of peritoneal carcinomatosis: progressive OC is characterized by metastases in the peritoneal cavity and-or in the retroperitoneal lymph nodes, supporting extensive disease spread beyond the abdomen [2,3].
Currently, OC is often first identified by transvaginal ultrasound (TVU) after a clinical examination. Several ultrasound features have been recognized to predict a malignancy, but the diagnostic precision still needs to be improved [4]. Serum biomarkers are an easily accessible, cost-effective, and non-invasive tool for a timely detection of OC. However, the heterogeneity of OC is a great obstacle in discovering reliable biomarkers to aid early diagnosis.
Gynecologic neoplasms comprise lesions of different origin such as epithelial, mesenchymal, sex cord-stromal, and germ cell. Of these categories, 75% is represented by high-grade serous ovarian carcinoma (HGSOC), with a poor survival [5,6]. Comparative transcriptomic and genomic studies of mouse models and organoids suggest that extracellular matrix in HGSOC, despite its name, originates from both the fallopian tube epithelium and the ovarian surface epithelium [7].
One of the major issues in uncovering the pathogenesis of the OC is the heterogeneous nature of the disease, comprising various histologic types (only 10% of OC are non-epithelial ones) with different behaviors and characteristics [8,9,10,11].
The four most common types of OC are actually epithelial ones: serous, clear-cell, endometrioid, and mucinous tumor: they are furtherly categorized into sub-types according to their biological features and response to treatment [12].
To date two different subtypes of epithelial ovarian carcinogenesis are recognized, Type I and Type II, diverging in epidemiology, etiology, and therapeutic approach. Invasive epithelial OC (Type I), genetically stable and asymptomatic, is generally detectable in low-grade serous, endometrioid, clear cell, and mucinous OCs: they typically proliferate slowly, can be diagnosed early and may have a good rate of prognosis. Conversely, Type II OCs are classified as high-grade tumors and are commonly diagnosed at advanced stages: they have a more aggressive progression and an extreme rate of proliferation. Moreover, Type II OCs are genetically unstable with p53 mutations peculiar to high-grade serous tumors [6].
OC specific risk depends on many factors including age and genetic predisposition; it has been well assessed that Hereditary Ovarian Cancers (HOC) is related to germline mutations in the BRCA gene, revealing that genetic testing for BRCA1/2 mutation carriers is a key point in the risk evaluation and clinical management of OC [13,14]. Although it is known that some lower penetrance genes may represent additional cancer risk factors, further studies are required to fully define their role in OC development. It’s generally recognized that these rare mutations (less than 1% in the general population) are related to 20% of the extra-familial risk factor [15,16]. Moreover, ethnic backgrounds have also been revealed as genetic risk for the onset of the disease (i.e., Jewish, French Canadian, Dutch, and those of Icelandic descent) [17].
Several investigations described an increased risk of OC in women with a high number of ovulatory cycles, as a consequence of the pro-inflammatory response of the distal fallopian tubes that occurs during ovulation [18].
Twenty-one percent of epithelial ovarian cancers are linked to lifestyle and other risk factors, (such as alcohol, obesity, smoking, talc use, diet). Minor studies have shown a link between dietary fiber eating and its correlation with the prevalence of OC. Furthermore, low levels of vitamin D have been related with an increased risk of this malignancy [19]. Whereas oral contraceptive pill (OCP) use, pregnancy, breastfeeding, and tubal ligation are well-established defensive factors [20].
Finally, also endometriosis could be considered a risk factor since endometriosis-associated epithelial OCs have been frequently observed in younger women, luckily with a better overall prognosis [21].
2. HE4 as a Multipurpose Biomarker in OC
Currently, OC is a target of intense biomarkers research because it is often diagnosed in late stages (III or IV) when the survival rate is less than 20%: efforts have therefore focused on diagnosing early-stage or low-volume disease through accurate tumour markers [22].
In this context serum determination the biomarker Human epididymis protein 4 (HE4) is one of the most promising early detection test [22]. At present there are several methods available to measure HE4 serum levels: Enzyme-linked immunosorbent assay (ELISA), Radioimmunoassay (RIA), Chemiluminiscence immunoassay (CLIA) and Electrochemiluminesce immunoassay (ECLIA). Automated CLIA and ECLIA technologies have high reproducibility and are more sensitive compared to other tests [23].
HE4 is encoded as a protein of approximately 50 amino acids by the WFDC2 (whey acidic protein four-disulfide core domain protein 2) gene localized on chromosome 20q12-13.1. The Whey Acidic Protein domain, known also as WAP Signature motif, retains an evolutionarily highly conserved motif characterized by eight cysteines forming four disulfide bonds at the core of the protein that is peculiars to all family members [24].
HE4 is secreted extracellularly as glycoprotein into the bloodstream and acts as a protease inhibitor, inhibiting serine, aspartyl and cysteine proteases; however, its exact function remains unknown. [25].
It was firstly identified as a transcript exclusively expressed in distal epididymis epithelium by researchers at the Pacific Northwestern Research Institute in Seattle. Due to its localization, it was proposed as a specific tissue marker for the same [25].
Later studies demonstrated that HE4 was expressed in several epithelia such as the oral cavity, respiratory tract, female genital tract, distal renal tubules and in the colonic mucosa but interestingly it was not found in normal ovarian surface epithelium [26]. The first report on the possible use of HE4 as a tumor marker in ovarian cancer was published by Hellstrom et al. in 2003 [27]. As mentioned before HE4 expression in ovarian tumors depends on the histological subtype: HE4 is expressed mainly in serous and endometrial ovarian tumors which constitute the majority of OCs, and rarely in mucinous epithelial and germinal cancers [23]. As a clinical biomarker, HE4 is considered an early detection method: some studies suggest increased serum HE4 expression in nearly 92% of patients with OC, showing similar sensitivity and increased specificity to CA125, the current gold standard biomarker of this malignancy [30]. Compared to the more established CA125, HE4 is in fact less frequently increased in benign gynecological conditions such as endometriosis, adenomyosis, uterine fibroids or even menstruation, and thus these do not compromise its specificity [28,29]. HE4 was also shown to have a higher sensitivity than CA125 in detecting early stages of OC [30]. In 2009, the US Food and Drug Administration (FDA) agreed to use HE4 to diagnose and monitor OC [31]. Later in 2011, it also approved its use in combination with the marker CA125 as a part of the Risk of Ovarian Malignancy Algorithm (ROMA) for the OC diagnosis, especially in the presence of adnexal masses [32]. ROMA is a logistic regression algorithm that combines HE4 and Ca125 values and patient’s menopausal status to categorize women into high- and low-risk chances that a tumour will be diagnosed in a female subject with a pelvic mass.
In spite of elevated sensitivity and negative predictive value (NPV) (respectively 94% and 99%) ROMA demonstrated a specificity of 75% for predicting OC in women with a pelvic mass: therefore, the algoritm has been considered less reliable than the biomarker HE4 alone [33]. Some studies suggest increased serum HE4 expression in nearly 92% OC patients, showing similar sensitivity and increased specificity to the CA125 marker [33]. Most interestingly, HE4 plays a unique role in OC as it has been implicated not only in OC diagnosis, but it may have also prognostic and predictive potential: several studies investigated HE4 importance for OC early detection, follow-up period, remission monitoring and therapy response. HE4 is in fact potentially able to identify patients that are at high risk for primary platinum resistance [22,32]. High HE4 expression correlates closely with poor survival of OC and may display an important role in early prediction of OC recurrence when compared to CA125 [33,34]. HE4 combined with CA125 seems to have a more rigorous prognostic for malignancy than either alone and as it has been recently reported that combining both biomarkers rapidity is more effective than either marker solely [35]. Notably, a different expression of HE4 was reported between BRCA1/2 mutated and sporadic OC patients: high levels of HE4 were predominantly observed in wild type patients. Moreover, in these patients, HE4 increased levels have been correlated to micronodular carcinomatosis and to a poor prognosis [14,36]. Indeed, recent evidence focused on the HE4 involvement in cellular proliferation, tumor growth, metastatic ability, chemoresistance and immune response suppression [2,3,14,23,37]. Based on these observations, the main goal of this review is to clarify the role of HE4 as a key molecule in the oncogenetic processes underlying OC so that HE4 could be possibly considered as an essential resource not only for diagnosis but also for prognosis and therapy choice (Figure 1).
3. HE4 in Cell Proliferation and Tumor Growth
In the last decade HE4 has been the subject of extensive investigations given its importance in OC growth and proliferation. This evidence was strengthened by several studies, demonstrating that gene expression profiles were altered in response to HE4 overexpression [37,38].
HE4 has a pivotal role in several signaling pathways of OC pathogenesis, summarized in Table 1.
The importance of HE4 in tumor progression has been investigated in vitro and in vivo, affirming its role in promoting proliferation through cell cycle regulation [39]. To this regard, HE4 silencing experiments performed in cell line SKOV3 showed cell cycle arrest in G0/G1 phase, preventing the entry into S phase. In contrast, stimulation with recombinant HE4 promotes the switch to G2/M phase [38,40]. Furthermore, in vivo studies demonstrated that HE4 knockout mice show a decrease in OC growth [41].
Among them, some reports showed that HE4 silencing experiments performed in OC cell line SKOV3, downregulated ERK pathway, significantly reducing cell proliferation, whereas overexpression of HE4 leads to ERK activation [39,42,43].
Another mechanism in which HE4 is involved is EGF/EGFR pathways. The binding of EGF to its membrane-bound receptor EGFR, leads to activation of the MAPK/ERK pathway [37,39,44]. There are two mechanisms by which HE4 interacts with the EGF/EGFR pathway: direct one through the binding to EGFR; indirect following EGF treatment that increases HE4 expression and nuclear translocation [45]. To confirm these results, recent findings demonstrated that HE4 knockdown significantly lowered ERK and EGFR phosphorylation levels, inhibiting SKOV3 cell line growth [37,39].
PI3K/AKT signaling pathway is generally overexpressed during cancerogenesis, since AKT has been established as a strong tumorigenesis promoter [37]. Several studies showed that HE4 overexpression induced AKT increase promoting cell growth, whereas HE4 knockdown has a reverse effect [37,42].
The histone deacetylase 3 (HDAC3) and HE4 are both present in the nucleus and cytosol of cellular fraction and is known that HDAC3 promotes proliferation, invasion and migration in ovarian cancer cells. Indeed, it has been reported that the interaction between HDAC3 and HE4 activates the PI3K/AKT signaling pathway. Moreover, HE4 expression is directly affected by HDAC3 attendance [46].
4. HE4 and Angiogenesis
In the tumor microenvironment, HE4 has the potential to alter signaling pathways to modify the expression of related genes. Since HE4 is a secretory protein, it can function intracellularly via autocrine or paracrine mechanisms [47].
Tumor progression and angiogenesis are usually influenced by hypoxia, a condition mediated by hypoxia-inducible factor 1-alpha (HIF1α) that, when associated with hypoxic condition, can modulate VEGF, which is essential for neovascularization [48]. The angiogenic function of HE4 in OC is promoted by VEGF jointly with epidermal growth factor (EGF) and insulin: it has also been demonstrated that VEGF synthesis is promoted by IL-1α which is directly proportional to HE4 concentration [49-51]. Another evidence supporting the pivotal role of HE4 in OC oncogenesis is that it is able to activate STAT3 protein, a multifunctional transcription factor involved in multiple biological processes [52].
The activation of STAT3 mediated by HE4 promotes transcription of pro-angiogenic factors such as IL-8 and HIF1α: IL-8 leads to persistent neutrophil recruitment in tumor tissue stimulating neoangiogenesis whereas HE4-HIF1α interaction has to be better characterized yet [53,54].
HIF1α is a key mediator of cellular adaptation to hypoxia through the activation of signaling and metabolic pathways that promote cell survival [55,56]. In vitro experiments performed by inhibiting HIF1α function, showed a significant decrease in HE4 levels [37,45,57]. Moreover, the physical interaction between HIF1α and HE4 gene promoter regions increases HE4 protein synthesis [58-60].
The alteration of these pathways and in particular of IL8 and HIF1α is described in HGSOC as an unfavorable prognosis factor [61,62].
It has also been reported that STAT3 inhibitors are able to block HE4-mediated endothelium cavity formation by reducing IL-8 and HIF1α [63].
Supporting the role of HE4 in OC microvascular invasion, there are evidences claiming that HE4 serum levels are positively related to an increased microvascular density in OC tissue [47].
Tumor angiogenesis is also regulated by programmed cell death-1 (PD-1), which suppresses the antitumor function of CD8+ T cells [64].
HE4 has also been shown to be involved in the regulation of other proteins that are responsible for angiogenesis such as metalloproteases, AKT, and annexin II (ANXA2) [42,43,65,66]. As described in literature, HE4 and ANXA2 (a neoangiogenic inducing factor), were both CD147 interacting proteins: HE4 could promote the invasion and metastasis of OC by regulating the expression of CD147. Also, this mechanism has been suggested as an intriguing therapeutic target of OC [67].
5. HE4 and Metastatic Process
Metastasization is a process finely tuned by several interactions that generally occurs between tumor cells and surrounding microenvironment (Tumor Micro Environment-TME) [68].
The bi-directional crosstalk between tumor cells and surrounding TME can promote the acquisition of epithelial mesenchymal transition (EMT) phenotype consequently driving tumor progression.
In this scenario, HE4 role has been debated for a long time: previous studies on the functional role of HE4 in multiple cellular processes indicated a potential defensive role of HE4 in OC progression [69].
However, with the progress of molecular techniques, scientists reached a different point of view on the HE4 role in OC tumorigenesis [70].
In 2019 Wang et al. performing HE4 knockout experiments, defined several functions of this protein: they reported that the reduction of HE4 expression inhibits cell proliferation switching on the apoptotic way by activating caspase-3, cleaved caspase-3 and reverting EMT. This effect is confirmed by western blot analysis showing the increasing of E-cadherin protein and the reduction of N-cadherin and Snail levels [52]. Finally, the expression of metalloproteinases 2 and 9 is also inhibited by HE4 downregulation [70].
Most of these mechanisms are strictly connected with the JAK/STAT3 activation pathway which, in the absence of HE4, is strongly impaired. To this regard, HE4 knockdown experiments performed in vitro showed a suppression of the malignant progression by inhibiting the JAK/STAT3 pathway [52].
Interestingly, in OC cells high levels of HE4 fucosylated antigens such as Lewis y antigen were detected. Studies performed on this antigen showed that when Lewis y antigen is highly expressed on HE4 surface, it ascribes a highly metastatic phenotype to OC cells [69-71]. The possibility to hide and block Lewis y antigen by using a specific antibody, could be a feasible method for the therapeutic treatment of OC [71].
6. HE4 and Immune Response
HE4 was initially suggested to have a potential role in innate immune defense of multiple epithelia, and recently few studies have been conducted to better understand HE4 function in tumor immunity [72].
Several lines of evidence suggest that during cancer proliferation, TME creates the conditions for which the immune system is no longer able to recognize and destroy cancer cells. In fact, during tumor progression, while the immune system tries to defend the body, the tumor produces molecules that reduce the effectiveness of the immune response [73].
Among them, the most attractive one is Programmed Cell Death Ligand 1 (PD-L1), a trans-membrane protein considered a co-inhibitory factor of the immune response. PD-L1 is a protein expressed at low levels in different cell types functioning as a modulator of excessive or unwanted immune responses. Recent studies reported that HE4 overexpression increases PD-L1 expression on both tumor cells and macrophages through a novel post transcriptional mechanism [74].
As discussed before, a positive correlation between HE4 serum levels and IL-8 has been described in patients with microvascular ovarian cancer, affecting trafficking of cytotoxic T lymphocyte; the trip of these cells into the tumor tissue is dysregulated and suppressed as a consequence of HE4 increase [75].
The biological meaning of HE4 overexpression has also been studied in OC tumor immune microenvironment by comparing syngeneic model of rat ovarian cancer with human patient data. In this model, it has been observed that in malignant ascites, HE4 overexpression supports M2 macrophages recruitment and at the same time reduces the recall of activated CTL and NK. To this regard, further studies highlighted a particularly aggressive molecular subtype of HGSOC, suggesting that patients with this histotype having a higher antigen-presenting cell infiltration and PD-1/PDL-1 expression, can benefit from a specific immunotherapy [74].
It has also been revealed a significant positive correlation between Regulatory T cells (Tregs) subpopulations and HE4: Tregs are usually enriched in OC, and their immunosuppressive function plays a key role in tumorigenesis and progression [76].
Additionally, some recent studies have shown that HE4 is involved in promoting ovarian tumor immune evasion, through influencing expression of two proteins, osteopontin (OPN) and dual specificity phosphatase 6 (DUSP6): consequently, through targeting of HE4, it may be possible to downregulate molecular mechanisms that promote tumorigenesis and to restore a normal tumor immune response too [77].
7. HE4 and OC Therapy
The first-line standard care of patients with OC is extensive debulking surgery combined with taxane compounds (such as paclitaxel) and platinum-based agents (such as carboplatin). It has been shown a negative predictive value of about 80% for HE4 for optimal cytoreductive surgery [78]. It has also been demonstrated that the combination of CA125, HE4, and computed tomography is more effective at predicting the presence of residual tumours post-neoadjuvant chemotherapy [79]. More than 25% of patients with relapse have a poor prognosis due to a platinum-resistant or platinum-refractory disease. Thus, angiogenic inhibitor (such as bevacizumab), immune checkpoint inhibitors, poly ADP-ribose polymerase (PARP) inhibitors, estrogen receptor inhibitors, and various inhibitors of intrinsic tumor signaling pathways are being used as potential therapeutic agents for OC patients [80].
HE4 and ROMA scores are more sensitive predictors of platinum response than CA125 alone [45].
Angioli et al. reported that serum HE4 levels predict platinum-resistant versus sensitive disease at the third chemotherapy cycle with 100 % sensitivity and 85 % specificity [81]. Moore et al. demonstrated that patients resistant to first-line chemotherapy have increased HE4 serum levels.
Furthermore, higher HE4 levels inversely correlate with clinical outcome, optimal cytoreduction and overall survival inversely correlate with increased HE4 levels: the latter can also be considered as an independent prognostic factor for progression free survival [33].
Additionally, HE4 overexpression enhances concomitant resistance to cisplatin and paclitaxel, and this chemoresistance can in part be reversed downregulating HE4: it can be speculated that small molecules or antibodies targeting HE4 may enhance the efficacy of first- or second-line therapeutics and reduce the development of resistance [43].
In an interesting study it has been revealed that in the BRCA WT patients, HE4 performed as a predictive marker of chemosensitivity with a sensibility of 80% and a specificity of 100%; in BRCA mutated women, HE4 performed as a predictive marker of chemosensitivity in all patients: the ability to detect platinum-resistant patients before tumor relapse probably could open new therapeutic scenarios [36].
Many successful OC regimens are combination therapies that produce higher response rates and lower resistance rates compared with monotherapies [82].
Numerous scientific studies are being conducted to obtain new methods of treatment that will enable better patient survival and at the same time there is a constant effort to find biomarkers as new therapeutic targets. With an increasing understanding of OC progression mechanisms, selective molecular targeted therapies are emerging as innovative and promising therapeutic strategies: in this novel scenario biomarkers assume greater importance in the clinical management of OC.
Taken together, all the findings reported in the previous paragraphs highlight the key role played by HE4 in OC progression and metastasis, thus suggesting this biomolecule as a novel therapeutic target for the malignancy.
Figure 2 Summarizes the HE4 interplays with different routes driving OC oncogenesis.
8. Conclusions
Diagnostic, prognostic and predictive biomarkers of elevated sensitivity and specificity could allow an early diagnosis, risk stratification and consequentily a better survival rate for women affected by OC, currently the most frequently fatal gynecologic neoplasm [83].
Considering the recent updates from literature, we can define HE4 not only as a diagnostic, prognostic and predictive circulating biomarker, but we can refer to HE4 as a biological agent effectively involved in many of OC tumorigenesis mechanisms. Indeed, there are several OC oncogenic pathways in which HE4 plays an important role: in the light of this new perspective, we can consider this protein as a valuable tool in aiding the current transition towards “personalized oncology”.
With advancements in precision therapeutic strategies, detecting clinically relevant predictive tumor biomarkers, and subsequently ideal candidates for these treatments, become fundamental [84].
Further studies better elucidating the exact mechanisms in which HE4 drives OC pathogenesis will ultimately provide evidence as to whether HE4 should be recommended as a therapeutic target for this lethal disease.
Acknowledgments
We are thankful to Giuseppina Gennarini and Valentina Viggiani, for their technical assistance, to Prof. Daniel Kanton, for providing language help.
References
- Momenimovahed:, Z. : Tiznobaik, A.; Taheri, S.; Salehiniya, H. Ovarian cancer in the world: epidemiology and risk factors. Int J Womens Health 2019, 11, 287–299. [Google Scholar] [CrossRef] [PubMed]
- Jiang, Y.; Wang, C.; Zhou, S. Targeting tumor microenvironment in ovarian cancer: Premise and promise. Biochim Biophys Acta Rev Cancer 2020, 1873, 188361. [Google Scholar] [CrossRef] [PubMed]
- Morand, S.; Devanaboyina, M.; Staats, H.; Stanbery, L.; Nemunaitis, J. Ovarian Cancer Immunotherapy and Personalized Medicine. Int J Mol Sci 2021, 22. [Google Scholar] [CrossRef] [PubMed]
- Schoutrop, E.; Moyano-Galceran, L.; Lheureux, S.; Mattsson, J.; Lehti, K.; Dahlstrand, H.; Magalhaes, I. Molecular, cellular and systemic aspects of epithelial ovarian cancer and its tumor microenvironment. Semin Cancer Biol 2022, 86, 207–223. [Google Scholar] [CrossRef] [PubMed]
- Goyal, A. Role of Fine Needle Aspiration Cytology in the Diagnosis of Gynecologic Tumors. Acta Cytol 2023, 67, 195–212. [Google Scholar] [CrossRef] [PubMed]
- Menon, U.; Karpinskyj, C.; Gentry-Maharaj, A. Ovarian Cancer Prevention and Screening. Obstet Gynecol 2018, 131, 909–927. [Google Scholar] [CrossRef] [PubMed]
- Brown, Y.; Hua, S.; Tanwar, P.S. Extracellular matrix in high-grade serous ovarian cancer: Advances in understanding of carcinogenesis and cancer biology. Matrix Biol 2023, 118, 16–46. [Google Scholar] [CrossRef]
- Rice, M.S.; Murphy, M.A.; Vitonis, A.F.; Cramer, D.W.; Titus, L.J.; Tworoger, S.S.; Terry, K.L. Tubal ligation, hysterectomy and epithelial ovarian cancer in the New England Case-Control Study. Int J Cancer 2013, 133, 2415–2421. [Google Scholar] [CrossRef]
- Karnezis, A.N.; Cho, K.R.; Gilks, C.B.; Pearce, C.L.; Huntsman, D.G. The disparate origins of ovarian cancers: pathogenesis and prevention strategies. Nat Rev Cancer 2017, 17, 65–74. [Google Scholar] [CrossRef]
- Seidman, J.D.; Yemelyanova, A.; Zaino, R.J.; Kurman, R.J. The fallopian tube-peritoneal junction: a potential site of carcinogenesis. Int J Gynecol Pathol 2011, 30, 4–11. [Google Scholar] [CrossRef]
- Budiana, I.N.G.; Angelina, M.; Pemayun, T.G.A. Ovarian cancer: Pathogenesis and current recommendations for prophylactic surgery. J Turk Ger Gynecol Assoc 2019, 20, 47–54. [Google Scholar] [CrossRef] [PubMed]
- Zamwar, U.M.; Anjankar, A.P. Aetiology, Epidemiology, Histopathology, Classification, Detailed Evaluation, and Treatment of Ovarian Cancer. Cureus 2022, 14, e30561. [Google Scholar] [CrossRef] [PubMed]
- Stewart, C.; Ralyea, C.; Lockwood, S. Ovarian Cancer: An Integrated Review. Semin Oncol Nurs 2019, 35, 151–156. [Google Scholar] [CrossRef] [PubMed]
- Manganaro, L.; Celli, V.; Viggiani, V.; Berardelli, E.; Granato, T.; Tartaglione, S.; Farina, A.; Catalano, C.; Angeloni, A.; Anastasi, E. CT imaging phenotypes linked to CA125 and HE4 biomarkers are highly predictive in discriminating between hereditary and sporadic ovarian cancer patients. Tumour Biol 2022, 44, 171–185. [Google Scholar] [CrossRef] [PubMed]
- Ramus, S.J.; Song, H.; Dicks, E.; Tyrer, J.P.; Rosenthal, A.N.; Intermaggio, M.P.; Fraser, L.; Gentry-Maharaj, A.; Hayward, J.; Philpott, S.; et al. Germline Mutations in the BRIP1, BARD1, PALB2, and NBN Genes in Women With Ovarian Cancer. J Natl Cancer Inst 2015, 107. [Google Scholar] [CrossRef] [PubMed]
- Dicks, E.; Song, H.; Ramus, S.J.; Oudenhove, E.V.; Tyrer, J.P.; Intermaggio, M.P.; Kar, S.; Harrington, P.; Bowtell, D.D.; Group, A.S.; et al. Germline whole exome sequencing and large-scale replication identifies. Oncotarget 2017, 8, 50930–50940. [Google Scholar] [CrossRef] [PubMed]
- National Cancer Institute. Surveillance, Epidemiology, and End Results Program. Cancer stat facts: ovarian cancer. Available online: https://seer.cancer.gov/statfacts/ html/ovary.
- Walker, J.L.; Powell, C.B.; Chen, L.M.; Carter, J.; Bae Jump, V.L.; Parker, L.P.; Borowsky, M.E.; Gibb, R.K. Society of Gynecologic Oncology recommendations for the prevention of ovarian cancer. Cancer 2015, 121, 2108–2120. [Google Scholar] [CrossRef] [PubMed]
- Huang, X.; Wang, X.; Shang, J.; Lin, Y.; Yang, Y.; Song, Y.; Yu, S. Association between dietary fiber intake and risk of ovarian cancer: a meta-analysis of observational studies. J Int Med Res 2018, 46, 3995–4005. [Google Scholar] [CrossRef]
- Cancer Research, UK. Ovarian cancer risk factors. Available online: https://www.cancerresearchuk.
- Schenken, R.S. Endometriosis: Pathogenesis, epidemiology, and clinical impact. Available online: https://www.uptodate.
- Angeloni, A.; De Vito, C.; Farina, A.; Terracciano, D.; Cennamo, M.; Passerini, R.; Bottari, F.; Schirinzi, A.; Vettori, R.; Steffan, A.; et al. New Analytical Approach for the Alignment of Different HE4 Automated Immunometric Systems: An Italian Multicentric Study. J Clin Med 2022, 11. [Google Scholar] [CrossRef]
- Chudecka-Głaz, A.; Strojna, A.; Michalczyk, K.; Wieder-Huszla, S.; Safranow, K.; Skwirczyńska, E.; Jurczak, A. Evaluation of He4 Use in the Diagnosis of Ovarian Cancer: First and Second Recurrence, and an Analysis of HE4 Concentration during Second- and Third-Line Chemotherapy. Diagnostics (Basel) 2023, 13. [Google Scholar] [CrossRef]
- Zalfa, F.; Perrone, M.G.; Ferorelli, S.; Laera, L.; Pierri, C.L.; Tolomeo, A.; Dimiccoli, V.; Perrone, G.; De Grassi, A.; Scilimati, A. Genome-Wide Identification and Validation of Gene Expression Biomarkers in the Diagnosis of Ovarian Serous Cystadenocarcinoma. Cancers (Basel) 2022, 14. [Google Scholar] [CrossRef] [PubMed]
- Kirchhoff, C.; Habben, I.; Ivell, R.; Krull, N. A major human epididymis-specific cDNA encodes a protein with sequence homology to extracellular proteinase inhibitors. Biol Reprod 1991, 45, 350–357. [Google Scholar] [CrossRef] [PubMed]
- Qing, X.; Liu, L.; Mao, X. A Clinical Diagnostic Value Analysis of Serum CA125, CA199, and HE4 in Women with Early Ovarian Cancer: Systematic Review and Meta-Analysis. Comput Math Methods Med 2022, 2022, 9339325. [Google Scholar] [CrossRef] [PubMed]
- Hellström, I.; Raycraft, J.; Hayden-Ledbetter, M.; Ledbetter, J.A.; Schummer, M.; McIntosh, M.; Drescher, C.; Urban, N.; Hellström, K.E. The HE4 (WFDC2) protein is a biomarker for ovarian carcinoma. Cancer Res 2003, 63, 3695–3700. [Google Scholar] [PubMed]
- Granato, T.; Porpora, M.G.; Longo, F.; Angeloni, A.; Manganaro, L.; Anastasi, E. HE4 in the differential diagnosis of ovarian masses. Clin Chim Acta 2015, 446, 147–155. [Google Scholar] [CrossRef] [PubMed]
- Anastasi, E.; Granato, T.; Marchei, G.G.; Viggiani, V.; Colaprisca, B.; Comploj, S.; Reale, M.G.; Frati, L.; Midulla, C. Ovarian tumor marker HE4 is differently expressed during the phases of the menstrual cycle in healthy young women. Tumour Biol 2010, 31, 411–415. [Google Scholar] [CrossRef] [PubMed]
- Hamed, E.O.; Ahmed, H.; Sedeek, O.B.; Mohammed, A.M.; Abd-Alla, A.A.; Abdel Ghaffar, H.M. Significance of HE4 estimation in comparison with CA125 in diagnosis of ovarian cancer and assessment of treatment response. Diagn Pathol 2013, 8, 11. [Google Scholar] [CrossRef]
- Moore, R.G.; McMeekin, D.S.; Brown, A.K.; DiSilvestro, P.; Miller, M.C.; Allard, W.J.; Gajewski, W.; Kurman, R.; Bast, R.C.; Skates, S.J. A novel multiple marker bioassay utilizing HE4 and CA125 for the prediction of ovarian cancer in patients with a pelvic mass. Gynecol Oncol 2009, 112, 40–46. [Google Scholar] [CrossRef]
- Cviič, D.; Jagarlamudi, K.; Meglič, L.; Škof, E.; Zore, A.; Lukanović, D.; Eriksson, S.; Osredkar, J. A Dual Biomarker TK1 Protein and CA125 or HE4-Based Algorithm as a Better Diagnostic Tool than ROMA Index in Early Detection of Ovarian Cancer. Cancers (Basel) 2023, 15. [Google Scholar] [CrossRef]
- Manganaro, L.; Anastasi, E.; Porpora, M.G.; Vinci, V.; Saldari, M.; Bernardo, S.; Ballesio, L.; Sollazzo, P.; Pecorella, I.; Recchia, N.; et al. Biparametric Magnetic Resonance Imaging as an Adjunct to CA125 and HE4 to Improve Characterization of Large Ovarian Masses. Anticancer Res 2015, 35, 6341–6351. [Google Scholar]
- Cao, H.; You, D.; Lan, Z.; Ye, H.; Hou, M.; Xi, M. Prognostic value of serum and tissue HE4 expression in ovarian cancer: a systematic review with meta-analysis of 90 studies. Expert Rev Mol Diagn 2018, 18, 371–383. [Google Scholar] [CrossRef] [PubMed]
- Samborski, A.; Miller, M.C.; Blackman, A.; MacLaughlan-David, S.; Jackson, A.; Lambert-Messerlian, G.; Rowswell-Turner, R.; Moore, R.G. HE4 and CA125 serum biomarker monitoring in women with epithelial ovarian cancer. Tumour Biol 2022, 44, 205–213. [Google Scholar] [CrossRef] [PubMed]
- Plotti, F.; Terranova, C.; Guzzo, F.; De Cicco Nardone, C.; Luvero, D.; Bartolone, M.; Dionisi, C.; Benvenuto, D.; Fabris, S.; Ciccozzi, M.; et al. Role of BRCA Mutation and HE4 in Predicting Chemotherapy Response in Ovarian Cancer: A Retrospective Pilot Study. Biomedicines 2021, 9. [Google Scholar] [CrossRef] [PubMed]
- James, N.E.; Chichester, C.; Ribeiro, J.R. Beyond the Biomarker: Understanding the Diverse Roles of Human Epididymis Protein 4 in the Pathogenesis of Epithelial Ovarian Cancer. Front Oncol 2018, 8, 124. [Google Scholar] [CrossRef] [PubMed]
- Zhu, L.; Zhuang, H.; Wang, H.; Tan, M.; Schwab, C.L.; Deng, L.; Gao, J.; Hao, Y.; Li, X.; Gao, S.; et al. Overexpression of HE4 (human epididymis protein 4) enhances proliferation, invasion and metastasis of ovarian cancer. Oncotarget 2016, 7, 729–744. [Google Scholar] [CrossRef] [PubMed]
- Zhu, Y.F.; Gao, G.L.; Tang, S.B.; Zhang, Z.D.; Huang, Q.S. Effect of WFDC 2 silencing on the proliferation, motility and invasion of human serous ovarian cancer cells in vitro. Asian Pac J Trop Med 2013, 6, 265–272. [Google Scholar] [CrossRef] [PubMed]
- Wang, H.; Zhu, L.; Gao, J.; Hu, Z.; Lin, B. Promotive role of recombinant HE4 protein in proliferation and carboplatin resistance in ovarian cancer cells. Oncol Rep 2015, 33, 403–412. [Google Scholar] [CrossRef] [PubMed]
- Lu, R.; Sun, X.; Xiao, R.; Zhou, L.; Gao, X.; Guo, L. Human epididymis protein 4 (HE4) plays a key role in ovarian cancer cell adhesion and motility. Biochem Biophys Res Commun 2012, 419, 274–280. [Google Scholar] [CrossRef]
- Lee, S.; Choi, S.; Lee, Y.; Chung, D.; Hong, S.; Park, N. Role of human epididymis protein 4 in chemoresistance and prognosis of epithelial ovarian cancer. J Obstet Gynaecol Res 2017, 43, 220–227. [Google Scholar] [CrossRef]
- Ribeiro, J.R.; Schorl, C.; Yano, N.; Romano, N.; Kim, K.K.; Singh, R.K.; Moore, R.G. HE4 promotes collateral resistance to cisplatin and paclitaxel in ovarian cancer cells. J Ovarian Res 2016, 9, 28. [Google Scholar] [CrossRef]
- Gao, J.; Li, J.; Ma, L. Regulation of EGF-induced ERK/MAPK activation and EGFR internalization by G protein-coupled receptor kinase 2. Acta Biochim Biophys Sin (Shanghai) 2005, 37, 525–531. [Google Scholar] [CrossRef] [PubMed]
- Moore, R.G.; Hill, E.K.; Horan, T.; Yano, N.; Kim, K.; MacLaughlan, S.; Lambert-Messerlian, G.; Tseng, Y.D.; Padbury, J.F.; Miller, M.C.; et al. HE4 (WFDC2) gene overexpression promotes ovarian tumor growth. Sci Rep 2014, 4, 3574. [Google Scholar] [CrossRef] [PubMed]
- Lou, T.; Zhuang, H.; Liu, C.; Zhang, Z. HDAC3 positively regulates HE4 expression to promote ovarian carcinoma progression. Arch Biochem Biophys 2019, 675, 108044. [Google Scholar] [CrossRef] [PubMed]
- James, N.E.; Emerson, J.B.; Borgstadt, A.D.; Beffa, L.; Oliver, M.T.; Hovanesian, V.; Urh, A.; Singh, R.K.; Rowswell-Turner, R.; DiSilvestro, P.A.; et al. The biomarker HE4 (WFDC2) promotes a pro-angiogenic and immunosuppressive tumor microenvironment via regulation of STAT3 target genes. Sci Rep 2020, 10, 8558. [Google Scholar] [CrossRef] [PubMed]
- Tam, S.; Fu, S.; Xu, L.; Krause, K.J.; Lairson, D.R.; Miao, H.; Sturgis, E.M.; Dahlstrom, K.R. The epidemiology of oral human papillomavirus infection in healthy populations: A systematic review and meta-analysis. Oral Oncol 2018, 82, 91–99. [Google Scholar] [CrossRef] [PubMed]
- Poddar, A.; Aranha, R.R.; K Muthukaliannan, G.; Nachimuthu, R.; Jayaraj, R. Head and neck cancer risk factors in India: protocol for systematic review and meta-analysis. BMJ Open 2018, 8, e020014. [Google Scholar] [CrossRef]
- Karna, H.; Gonzalez, J.; Radia, H.S.; Sedghizadeh, P.P.; Enciso, R. Risk-reductive dental strategies for medication related osteonecrosis of the jaw among cancer patients: A systematic review with meta-analyses. Oral Oncol 2018, 85, 15–23. [Google Scholar] [CrossRef]
- Dabkeviciene, D.; Sasnauskiene, A.; Leman, E.; Kvietkauskaite, R.; Daugelaviciene, N.; Stankevicius, V.; Jurgelevicius, V.; Juodka, B.; Kirveliene, V. mTHPC-mediated photodynamic treatment up-regulates the cytokines VEGF and IL-1alpha. Photochem Photobiol 2012, 88, 432–439. [Google Scholar] [CrossRef]
- Wang, A.; Jin, C.; Tian, X.; Wang, Y.; Li, H. Knockdown of HE4 suppresses aggressive cell growth and malignant progression of ovarian cancer by inhibiting the JAK/STAT3 pathway. Biol Open 2019, 8. [Google Scholar] [CrossRef]
- Fu, H.; Ma, Y.; Yang, M.; Zhang, C.; Huang, H.; Xia, Y.; Lu, L.; Jin, W.; Cui, D. Persisting and Increasing Neutrophil Infiltration Associates with Gastric Carcinogenesis and E-cadherin Downregulation. Sci Rep 2016, 6, 29762. [Google Scholar] [CrossRef]
- Bekes, E.M.; Schweighofer, B.; Kupriyanova, T.A.; Zajac, E.; Ardi, V.C.; Quigley, J.P.; Deryugina, E.I. Tumor-recruited neutrophils and neutrophil TIMP-free MMP-9 regulate coordinately the levels of tumor angiogenesis and efficiency of malignant cell intravasation. Am J Pathol 2011, 179, 1455–1470. [Google Scholar] [CrossRef] [PubMed]
- Shao, J.; Liu, S.; Zhang, M.; Chen, S.; Gan, S.; Chen, C.; Chen, W.; Li, L.; Zhu, Z. A dual role of HIF1α in regulating osteogenesis-angiogenesis coupling. Stem Cell Res Ther 2022, 13, 59. [Google Scholar] [CrossRef] [PubMed]
- Pugh, C.W.; Ratcliffe, P.J. Regulation of angiogenesis by hypoxia: role of the HIF system. Nat Med 2003, 9, 677–684. [Google Scholar] [CrossRef] [PubMed]
- Scortegagna, M.; Cataisson, C.; Martin, R.J.; Hicklin, D.J.; Schreiber, R.D.; Yuspa, S.H.; Arbeit, J.M. HIF-1alpha regulates epithelial inflammation by cell autonomous NFkappaB activation and paracrine stromal remodeling. Blood 2008, 111, 3343–3354. [Google Scholar] [CrossRef] [PubMed]
- Peng, C.; Liu, G.; Huang, K.; Zheng, Q.; Li, Y.; Yu, C. Hypoxia-Induced Upregulation of HE4 Is Responsible for Resistance to Radiation Therapy of Gastric Cancer. Mol Ther Oncolytics 2019, 12, 49–55. [Google Scholar] [CrossRef] [PubMed]
- Maxwell, P.H.; Wiesener, M.S.; Chang, G.W.; Clifford, S.C.; Vaux, E.C.; Cockman, M.E.; Wykoff, C.C.; Pugh, C.W.; Maher, E.R.; Ratcliffe, P.J. The tumour suppressor protein VHL targets hypoxia-inducible factors for oxygen-dependent proteolysis. Nature 1999, 399, 271–275. [Google Scholar] [CrossRef]
- Dang, C.V.; Semenza, G.L. Oncogenic alterations of metabolism. Trends Biochem Sci 1999, 24, 68–72. [Google Scholar] [CrossRef]
- Amer, H.; Kartikasari, A.E.R.; Plebanski, M. Elevated Interleukin-6 Levels in the Circulation and Peritoneal Fluid of Patients with Ovarian Cancer as a Potential Diagnostic Biomarker: A Systematic Review and Meta-Analysis. J Pers Med 2021, 11. [Google Scholar] [CrossRef]
- Sanguinete, M.M.M.; Oliveira, P.H.; Martins-Filho, A.; Micheli, D.C.; Tavares-Murta, B.M.; Murta, E.F.C.; Nomelini, R.S. Serum IL-6 and IL-8 Correlate with Prognostic Factors in Ovarian Cancer. Immunol Invest 2017, 46, 677–688. [Google Scholar] [CrossRef]
- Zhang, T.; Long, H.; Li, J.; Chen, Z.; Wang, F.; Jiang, S.W. WFDC2 gene deletion in mouse led to severe dyspnea and type-I alveolar cell apoptosis. Biochem Biophys Res Commun 2020, 522, 456–462. [Google Scholar] [CrossRef]
- Zhang, G.; Liu, C.; Bai, H.; Cao, G.; Cui, R.; Zhang, Z. Combinatorial therapy of immune checkpoint and cancer pathways provides a novel perspective on ovarian cancer treatment. Oncol Lett 2019, 17, 2583–2591. [Google Scholar] [CrossRef] [PubMed]
- Będkowska, G.E.; Piskór, B.; Gacuta, E.; Zajkowska, M.; Osada, J.; Szmitkowski, M.; Dąbrowska, M.; Ławicki, S. Diagnostic Power of Selected Cytokines, MMPs and TIMPs in Ovarian Cancer Patients - ROC Analysis. Anticancer Res 2019, 39, 2575–2582. [Google Scholar] [CrossRef] [PubMed]
- Sun, M.L.; Yang, Z.Y.; Wu, Q.J.; Li, Y.Z.; Li, X.Y.; Liu, F.H.; Wei, Y.F.; Wen, Z.Y.; Lin, B.; Gong, T.T. The Role of Human Epididymis Protein 4 in the Diagnosis and Prognosis of Diseases: An Umbrella Review of Systematic Reviews and Meta-Analyses of Observational Studies. Front Med (Lausanne) 2022, 9, 842002. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Nie, X.; Gou, R.; Qi, Y.; Liu, J.; Lin, B. Interaction of CD147 and human epididymis protein 4 promotes invasion and metastasis of ovarian cancer. J Cancer 2021, 12, 7422–7435. [Google Scholar] [CrossRef] [PubMed]
- Garcia-Gomez, A.; Rodríguez-Ubreva, J.; Ballestar, E. Epigenetic interplay between immune, stromal and cancer cells in the tumor microenvironment. Clin Immunol 2018, 196, 64–71. [Google Scholar] [CrossRef] [PubMed]
- Gao, L.; Cheng, H.Y.; Dong, L.; Ye, X.; Liu, Y.N.; Chang, X.H.; Cheng, Y.X.; Chen, J.; Ma, R.Q.; Cui, H. The role of HE4 in ovarian cancer: inhibiting tumour cell proliferation and metastasis. J Int Med Res 2011, 39, 1645–1660. [Google Scholar] [CrossRef]
- Espiau Romera, A.; Cuesta Guardiola, T.; Benito Vielba, M.; De Bonrostro Torralba, C.; Coronado Martín, P.J.; Baquedano Mainar, L. HE4 tumor marker as a predictive factor for lymphatic metastasis in endometrial cancer. Int J Gynaecol Obstet 2020, 149, 265–268. [Google Scholar] [CrossRef]
- Zhuang, H.; Hu, Z.; Tan, M.; Zhu, L.; Liu, J.; Liu, D.; Yan, L.; Lin, B. Overexpression of Lewis y antigen promotes human epididymis protein 4-mediated invasion and metastasis of ovarian cancer cells. Biochimie 2014, 105, 91–98. [Google Scholar] [CrossRef]
- Bingle, L.; Cross, S.S.; High, A.S.; Wallace, W.A.; Rassl, D.; Yuan, G.; Hellstrom, I.; Campos, M.A.; Bingle, C.D. WFDC2 (HE4): a potential role in the innate immunity of the oral cavity and respiratory tract and the development of adenocarcinomas of the lung. Respir Res 2006, 7, 61. [Google Scholar] [CrossRef]
- Labani-Motlagh, A.; Ashja-Mahdavi, M.; Loskog, A. The Tumor Microenvironment: A Milieu Hindering and Obstructing Antitumor Immune Responses. Front Immunol 2020, 11, 940. [Google Scholar] [CrossRef]
- Rowswell-Turner, R.B.; Singh, R.K.; Urh, A.; Yano, N.; Kim, K.K.; Khazan, N.; Pandita, R.; Sivagnanalingam, U.; Hovanesian, V.; James, N.E.; et al. HE4 Overexpression by Ovarian Cancer Promotes a Suppressive Tumor Immune Microenvironment and Enhanced Tumor and Macrophage PD-L1 Expression. J Immunol 2021, 206, 2478–2488. [Google Scholar] [CrossRef] [PubMed]
- Dubey, H.; Modi, M.; Verma, S.; Sinha, R.; Goel, H.; Ranjan, A.; Tanwar, P.; Chopra, A.; Rahul, E.; Ranjan, L.; et al. Role of Human Epididymis Protein 4 in Tumour Angiogenesis. Recent Advances, New Perspectives and Applications in the Treatment of Ovarian Cancer.
- Li, R.; Xu, J.; Wu, M.; Liu, S.; Fu, X.; Shang, W.; Wang, T.; Jia, X.; Wang, F. Circulating CD4. Medicina (Kaunas) 2023, 59. [Google Scholar] [CrossRef]
- Liu, P.; Chen, R.; Zhang, X.; Fu, R.; Tao, L.; Jia, W. Combined PD-1/PD-L1 and tumor-infiltrating immune cells redefined a unique molecular subtype of high-grade serous ovarian carcinoma. BMC Genomics 2022, 23, 51. [Google Scholar] [CrossRef] [PubMed]
- Saffarieh, E.; Nassiri, S.; Mirmohammadkhani, M. Predicting value of HE4 and CA125 markers for optimal cytoreductive surgery in ovarian cancer patients. Eur J Transl Myol 2022, 32. [Google Scholar] [CrossRef] [PubMed]
- Chakraborty, S.; Shenoy, P.S.; Mehrotra, M.; Phadte, P.; Singh, P.; Rekhi, B.; Ray, P. Through the Looking Glass: Updated Insights on Ovarian Cancer Diagnostics. Diagnostics (Basel) 2023, 13. [Google Scholar] [CrossRef] [PubMed]
- Yoon, H.; Kim, A.; Jang, H. Immunotherapeutic Approaches in Ovarian Cancer. Curr Issues Mol Biol 2023, 45, 1233–1249. [Google Scholar] [CrossRef] [PubMed]
- Angioli, R.; Capriglione, S.; Aloisi, A.; Guzzo, F.; Luvero, D.; Miranda, A.; Damiani, P.; Montera, R.; Terranova, C.; Plotti, F. Can HE4 predict platinum response during first-line chemotherapy in ovarian cancer? Tumour Biol 2014, 35, 7009–7015. [Google Scholar] [CrossRef]
- Vetter, M.H.; Hays, J.L. Use of Targeted Therapeutics in Epithelial Ovarian Cancer: A Review of Current Literature and Future Directions. Clin Ther 2018, 40, 361–371. [Google Scholar] [CrossRef]
- Lisio, M.A.; Fu, L.; Goyeneche, A.; Gao, Z.H.; Telleria, C. High-Grade Serous Ovarian Cancer: Basic Sciences, Clinical and Therapeutic Standpoints. Int J Mol Sci 2019, 20. [Google Scholar] [CrossRef]
- Algethami, M.; Kulkarni, S.; Sadiq, M.T.; Tang, H.K.C.; Brownlie, J.; Jeyapalan, J.N.; Mongan, N.P.; Rakha, E.A.; Madhusudan, S. Towards Personalized Management of Ovarian Cancer. Cancer Manag Res 2022, 14, 3469–3483. [Google Scholar] [CrossRef]
Figure 1.
HE4 as a disease checkpoint. After the appearance of symptoms, HE4 is a biomarker of crucial importance since it can lead to a correct and tempestive diagnosis.
Figure 1.
HE4 as a disease checkpoint. After the appearance of symptoms, HE4 is a biomarker of crucial importance since it can lead to a correct and tempestive diagnosis.
Figure 2.
Schematic representation of HE4 interaction network in OC oncogenesis. HE4 is involved in cellular pathways of neoplastic proliferation and immunological evasion. Intracellular signaling and interaction with microenvironment can increase aggressive phenotypes that underlie angiogenesis and metastatic dissemination. Drugs that can interfere with each pathway shown in figure. STAT3, HIF 1α, HDAC3, OPN, DUSP6, LEWIS Y and CD147 may represent possible target of OC therapy (represented by dotted line), still under investigation.
Figure 2.
Schematic representation of HE4 interaction network in OC oncogenesis. HE4 is involved in cellular pathways of neoplastic proliferation and immunological evasion. Intracellular signaling and interaction with microenvironment can increase aggressive phenotypes that underlie angiogenesis and metastatic dissemination. Drugs that can interfere with each pathway shown in figure. STAT3, HIF 1α, HDAC3, OPN, DUSP6, LEWIS Y and CD147 may represent possible target of OC therapy (represented by dotted line), still under investigation.
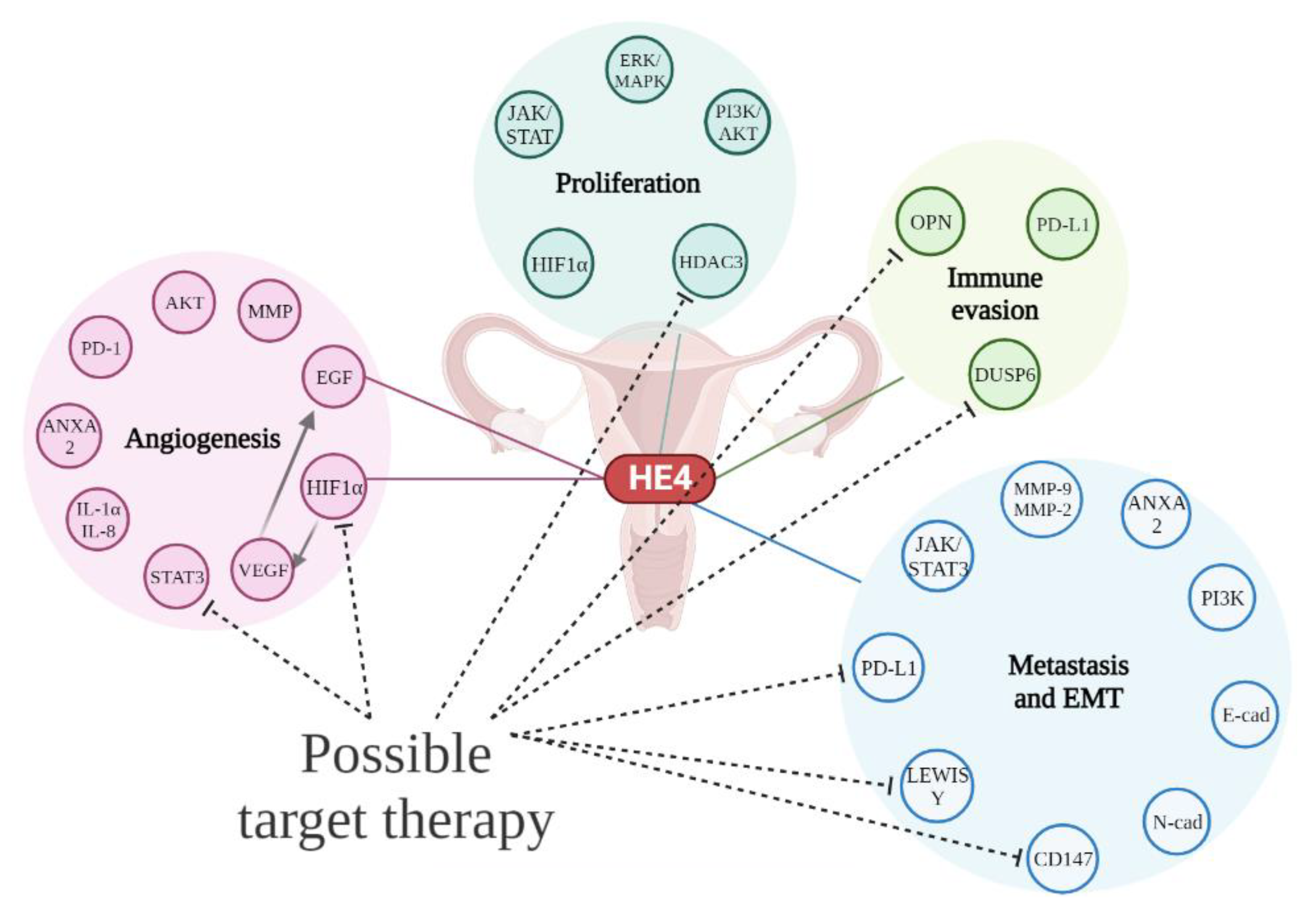

Table 1.
Summary table of the main pathways involved. Functions of signaling pathways and the influence of HE4 are described.
Table 1.
Summary table of the main pathways involved. Functions of signaling pathways and the influence of HE4 are described.
| Pathway |
Description and functions | HE4 influence |
|---|---|---|
|
ERK/MAPK (extracellular signal-regulated kinases/ mitogen-activated protein kinase) |
▪ pathway usually activated by EGF. ▪ phosphorylation of neighboring proteins by ERK ("on" or "off" switch) ▪ ERK required for activation of genes for entry into the cell cycle. ▪ pathway mutated in many cancers |
▪ regulation of proliferation and invasion of SOC cells ▪ ERK activation with HE4 overexpression ▪ decrease in proliferation when HE4 was silenced in SKOV3 cells. ▪ activation of ERK/MAPK pathway by interaction of HE4 with EGF/EGFR |
|
PI3K/AKT (phosphoinositide 3- kinases/ Protein kinase B) |
▪ PI3K indirectly activates AKT after phosphorylation of phosphatidyl inositol 4,5 bisphosphate (PIP2) and phosphatidyl inositol 3,4,5 trisphosphate (PIP3) ▪ phosphorylation of protein substrates by AKT ▪ activation of biochemical pathways leading to cell growth and resistance to apoptosis ▪ mTOR protein involved in angiogenesis and increase of membrane glucose transporters. |
▪ AKT increase and subsequent cell growth in OVCAR3 cells when HE4 is overexpressed. ▪ AKT decrease and subsequent reduced cell growth in OVCAR3 cells when there is HE4 knockout. |
|
HDAC3 (histone deacetylase 3) |
▪ role in S phase progression, DNA damage control, genomic stability maintenance |
▪ HDAC3 expression or knockdown lead to a corresponding increase or decrease in HE4 expression. ▪ HE4 and HDAC3 binding activates the PI3K/AKT signaling pathway. ▪ inhibition of the interaction between HDAC3 and HE4 may have potential therapeutic value |
|
HIF1α (hypoxia-inducible factor 1-alpha) |
▪ key mediator of cellular adaptation to hypoxia ▪ Involved in processes of proliferation, survival and angiogenesis. ▪ modulated by hydroxylation, acetylation, and phosphorylation. |
▪ HE4-HIF1α interaction is yet not well understood. ▪ decrease in HE4 levels in SKOV3 cells treated with HIF1α siRNA or with HIF1α inhibitors |
|
JAK/STAT (Janus kinases/signal transducer and activator of transcription proteins) |
▪ pathway activated by cytokines and growth factors. ▪ intracellular response triggered by the action of the activated STAT proteins. ▪ alteration of gene expression of proteins involved in proliferation, differentiation and apoptosis |
▪ HE4 knockdown inhibits the activity of the JAK/STAT3 pathway in vitro and in vivo. ▪ HE4 knockdown suppresses cell proliferation and malignant progression of ovarian cancer |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



