
Submitted:
13 May 2023
Posted:
15 May 2023
You are already at the latest version
Abstract
Background: The most important causative agents of neoplasms in the anogenital area is the human papillomavirus (HPV). Due to the anatomical proximity of the genital and anus area and the ease with which HPV infection is transmitted, it seems that patients after treatment of HPV-related gynecological diseases may have increased risk of developing a second HPV-related neoplasm- anal cancer. The aim of the study was to determine the risk of anal intraepithelial neoplasia (AIN) and anal cancer (AC) among patients after treatment of HPV-related gynecological diseases. Methods: We conducted a comprehensive review of available literature in multiple databases. The study was performed following Cochrane Reviewers' Handbook and Preferred Reporting Items for Systematic Reviews and Meta-Analyses 2009 guidelines. Moreover, we assessed the quality of each study using QUADAS-2. Results: Twenty five studies were included in the final analysis. Patients after treatment of HPV-related gynecological diseases have a significantly higher risk of AC (mean standardized incidence ratio [SIR]= 5.387, mean incidence risk [IR]= 0.096%, mean IR per 100,000 person-years= 10.37), and AIN (mean IR= 23.683%) compared to the population risk. Conclusions: Patients with HPV-related gynecological diseases should constitute a group for which an appropriate primary and secondary screening for AC should be introduced.
Keywords:
HPV
; human papillomavirus
; anal intraepithelial neoplasia
; anal cancer
; gynecology
; cervix
; vulva
; vagina
; intraepithelial neoplasia
; cancer
1. Introduction
It is reported that only in 2020, 604,127 new cases of invasive cervical cancer (CC) were diagnosed worldwide [1]. It is a gynecological cancer, the occurrence of which is practically 100% dependent on HPV infection human papillomavirus (HPV) - the most common sexually transmitted infection [2]. Other gynecological cancers associated with HPV infection are vaginal cancer (VaC) and vulvar cancer (VC)-related with HPV infection in about 78% and 24.9% respectively [3]. These neoplasms along with corresponding pre-cancerous lesions are collectively defined as HPV-related gynecological diseases (HPV-RGD). Patients after treatment of HPV-related disease become a subgroup that requires specific control in order to prevent the development of secondary HPV-related disease.
It has been investigated that HPV has the greatest affinity for the zones where epithelium of one type merges into another of a different histological features i.e. as in cervix where the squamous epithelium joins the one-layer glandular epithelium in the transformation zone [4]. HPV integrates its genome with the DNA of epithelial cells and express the E6 and E7 genes. Afterwards, the E6 and E7 proteins are produced, which initiates inter alia the degradation of the p53 and Rb proteins. Finally, the processes characteristic for carcinogenesis are being stimulated [5].
Another histologically similar region in the human body is the anal canal, where there is transformation zone between glandular and squamous epithelium at the level of dentate line. Due to the anatomical proximity, this place seems to be particularly vulnerable to the transmission of HPV from infected gynecological organ and as a result susceptible for anal intraepithelial neoplasia (AIN) or anal cancer (AC) development. This is supported by the Hernandez et al. data, which showed, that in case of Hawaii patients with cervical HPV infection, 13% had concurrent anal HPV infection [6]. Moreover, Jacot-Guillarmod et al. showed that when cervical HPV infection was confirmed, simultaneously anal HPV infection was presented in 59,3% cases [7].
The worldwide, cumulative risk incidence of AC is 0.06 for women and 0.07 for men [1]. HIV-positive homosexual men are the group of the highest risk of developing anal cancer (the incidence rate is 77–137 per 100,000) [8,9]. However, as far as women are concerned, HIV infection is present in a relatively small percentage of AC patients. It is the chronic HPV infection which is the reason of developing nearly 90% of this neoplasms [10,11].
In the available research, HPV type 16 was responsible for infections in the perianal area and the anal canal in subgroup of HIV-negative women in the overwhelming number of cases (about 85%). The second most common was HPV type 18 followed by HPV types 31/33/45/52/58 [12]. The frequency and quality of HPV infections vary depending on whether there is a co-infection with the immunodeficiency virus (HIV). In the group of HIV positive patients, the risk of anal cancer is significantly increased. Moreover, more diverse types of HPV can be found in rectal swabs [12]. However, one of the recent studies showed that HIV-negative patients older than 45 with HPV type 16 detected in the cervix had a comparable risk of developing anal cancer as HIV- positive patients [13]. These data emphasize how substantially increased is the risk of developing AIN/AC in patients with HPV infection in the anal canal, especially with the high-oncogenic HPV types.
Considering all of the above facts, we formed a research hypothesis that patients diagnosed with HPV disease related to the gynecological organ have an increased risk of developing AIN or AC due to the facility of transmission of HPV infection into the anal canal.
The main aim of this study was to determine the risk of AIN/AC in the population of people with HPV-RGD. Secondary aim was to evaluate which of the HPV-RGD increases the risk of AIN/AC the most.
2. Materials and Methods
A systematic review of literature was performed in accordance with the criteria outlined in the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 updated guidelines [14]. A review of publications describing the risk of AC and AIN among patients treated for HPV-related gynecological diseases was carried out using: PubMed and EBSCO Discovery Service interface in order to search databases such as Medline, Cochrane Library, Web of Science, Academic Search Complete, ScienceDirect, Scopus, Nature Publishing Group, Oxford Journals, Wiley Online Library, and Clinical Key. Search strategy, included specific words and phrases, is enclosed in Supplementary Material S1.
The search included articles published from the last 30 years: from 1992 to November 2022. Only English language text were considered.
If "carcinoma in situ" (CIS) term was separately used in publications, this was considered as cervical intraepithelial neoplasia (CIN) 3, thus CIN3 and CIS were analyzed as one entity. Similarly, the term “low-grade squamous intraepithelial lesion” (LSIL) was considered equal to CIN 1 and “high-grade squamous intraepithelial lesion” (HSIL) as CIN 2 or 3. It is accordance with current terminology [15].
In most cases authors of reviewed articles used data obtained from national cancer registries. When two or more publications used the same cancer registry and the period of research was similar, for final calculation we selected data from only one of them (the most numerous), so as not to duplicate the number of patients with a given primary cancer. This was the case for the US publications where several of them analyzed data from a similar period from the National Cancer Institute Surveillance, Epidemiology, and End Results (SEER) Program. Moreover, two publications acquired date from the Finish Cancer registry and three from the Swedish Cancer Register. In these cases, for final calculation, we used data only from one publication. Also, data from Chaturvedi et al. publication were not included in final calculation, because they are based on 13 population-based cancer registries in Denmark, Finland, Norway, Sweden, and the United States - in this case the risk of duplication of patients was too high.
To determine the bias risk, each of the article was assigned to the group of low, high or unclear bias risk in accordance with the QUADAS-2 recommendations [16]. When determining the bias risk, the following factors were evaluated: patient selection, index test, reference standard and flow & timing. Moreover, the same factors were evaluated except of flow & timing in case of determining the applicability of selected researches. The exact process of determining bias risk and applicability for each of the articles is available in Supplementary Material S2. Table 1 shows the general bias risk determined for each article included in the review.
3. Results
The search resulted in 7,119 records. The first stage of screening was based on the analysis of the titles of the publication. Six thousand nine hundred fifty seven records were excluded because of being marked as not human subject, referring basic sciences, different type of research than original research, referring other malignancy than AIN/AC or being duplicated. The second stage of screening was based on the abstract review. One hundred twenty five records were excluded because: the subject of research did not concern the risk of AIN/AC or the results for different diseases were not divided or the reasons mentioned in the previous stage of screening. Finally, after reviewing full text of selected articles, we included 25 articles in our research [17-41]. The reference list of identified articles has been revived but no relevant studies has been additionally added. The process of study selection is shown in a PRISMA flowchart in Figure 1.
The study characteristics of the selected articles are presented in Table 1. There were 3 prospective cross-sectional studies and 22 retrospective population-based cohort studies. Only 4 articles determined the risk of AIN in patients with HPV-RGD, the rest of the articles (n=22) determined the risk of AC. The mean age of patients at the diagnosis of: CC was 57.7, VC was 65.5 and VaC was 81.
By summing up the number of patients reported in each of selected publications during the literature review, the total number of people diagnosed with CC was 177,984, with VC 9,572 and with VaC 2,733. In case of precancerous lesions there were 110,243 people with medical history of CIN 1, 52,151 with CIN 2, 447,739 with CIN 3, 234 with VIN 1, 16 with VIN 2, 108 with VIN 3, 104 with VaIN 1, 13 with VaIN 2 and 30 with VaIN 3. In several articles, authors did not divide the precancerous lesion into particular subcategories and therefore the total number of cases of CIN, VIN and VaIN was counted. The total number of patients with medical history of CIN was 682,991 (summed number of patients with CIN 1, 2, and 3, and the number of patients who were referred in the selected publications as CIN without specifying the degree of intraepithelial neoplasia). The total number of patients with medical history of VIN was 358 and with VaIN was 147.
Most authors of selected articles evaluated the risk of AIN/AC in people with HPV-RGD by determining the value of the standardized incidence ratio (SIR) according to the following formula: SIR= Observed cases/ Expected cases (see Supplementary Material S3 for details providing definition and interpretation of SIR). The SIR for AC in patients with a history of CC ranged from 1.63 (95% Cl: 1.21- 2.14) to 6.3 (95% Cl was not provided) with mean of 3.814. The SIR for AC in patients with a history of VC ranged from 11.7 (95% Cl: 0.15–65.51) to 17.4 (95% CI: 11.5–24.4) with mean of 14.55. The SIR for AC in patients with a history of VaC was 1.8 (95% CI: 0.2–5.3) (data from the research of Aceve-do-Fontánez et al. were not included as the authors only reported a summary SIR for VC and VaC). The SIR for AC in patients with a history of CIN 3 ranged from 2.28 (95% Cl was not provided) to 16.4 (95% CI: 13.7–19.2) with mean of 5.701. The SIR for AC in patients with a history of CIN 2 ranged from 0.89 (95% Cl: 0.09- 3.35) to 2.9 (95% Cl: 2.0–4.1) with mean of 1.895. There was no information about SIR for CIN 1, VIN or VaIN in any of the articles we have reviewed. The SIR for AC in patients with CIN without dividing into specific degree of intraepithelial neoplasia ranged from 0.89 (95% Cl: 0.09- 3.35) to 16.4 (95% CI: 13.7–19.2) with mean of 4.563. The average SIR for all HPV-RGDs is 5.387.

Table 1.
Summary of review about the risk of AIN/AC in group of patients with HPV-RGD.
| No. | Authors and year of publication | Country | Number of patients | Period of time analysed | The type of primary cancer/pre-cancer lesion | Median age of participants | Number of AIN/AC | Increased risk | Risk of bias |
|---|---|---|---|---|---|---|---|---|---|
| 1. | Acevedo-Fontánez et al. (2018) [17] | Puerto-Rico | 9,489 | 1987-2013 | 8,039 CC 1,378 VC 773 VaC |
46 CC, 70 VC, 67 VaC |
14 AC after CC 3 AC after VC 1 AC after VaC |
AC after CC: SIR= 1.8 (95% Cl: 0.9- 3.4) AC after VC & VaC: SIR= 2.9 (95% Cl: 0.8-7.5) |
L |
| 2. | Chaturvedi et al. (2007) [18] | USA | 27,466 | 1973–2001 | 27,466 CC* | 48.6 | NI | AC after CC: SIR= 3.12; 95% CI = 1.88-4.88 | L |
| 3. | Ebisch et al. (2017) [19] | Netherlands | 89,018 | 1990-2015 | 89,018 CIN 3 | 36 | 73 AC 80 AIN 3 |
AC after CIN 3: SIR= 3.85 (95% CI: 2.32-6.37) AIN 3 after CIN 3: SIR= 6.68 (95% CI: 3.64- 12.25) |
L |
| 4. | Edgren et al. (2007) [20] | Sweden | 125,292 | 1968-2004 | 125,292 CIN 3 | 35 | 131 AC | AC after CIN 3: SIR= 4.68 (95% Cl: 3.87- 5.62) | L |
| 5. | ElNaggar et al. (2013) [21] | USA | 272 | 2006-2010 | CIN 1 29 CIN 2 16 CIN 3/CIS 41 VIN 1 46 VIN 2 16 VIN 3/CIS 69 VaIN 1 34 VaIN 2 13 VaIN 3/CIS 8 =272 |
39 | 64 AIN (36 stage 1, 6 stage 2, 22 stage 3) | 48 (36.4%) had VIN, 10 (18.2%) had VaIN, and 13 (14.4%) had CIN. | H |
| 6. | Evans et al. (2003) [22] | England | 81,124 | 1960-1999 | 59,519 CIN 3 21,605 CC |
NI | 23 AC after CIN 3 18 AC after CC |
AC after CIN 3: SIR= 5.9 AC after CC: SIR= 6.3 |
L |
| 7. | Gaudet et al. (2014) [23] | Canada | 54,320 | 1985-2005 | 54,320 CIN 2 and CIN 3** |
35 | 4 AC after CIN 2 16 AC after CIN 3 |
AC after CIN 2: SIR= 0.89 (95% Cl: 0.09- 3.35) AC after CIN 3: SIR= 2.28 (95% Cl: 0.71- 5.42) |
L |
| 8. | Hemminki et al. (2001) [24] | Sweden | 17,234 | 1958-1996 | 17,234 CC | NI | 16 AC | AC after CC: SIR= 4.22 (95% Cl: 2.41-6.55) | L |
| 9. | Hemminki et al. (2000) [25] | Sweden | 135,386 | 1958-1996 | 117,830 CIN 3 17,556 CC |
NI | 68 AC after CIN 3 17 AC after CC |
AC after CIN 3: SIR= 3.75 (95% Cl: 2.91-4.69) AC after CC: SIR= 3.92 (95% Cl: 2.28-6.00) |
L |
| 10. | Heráclio et al. (2018) [26] | Brazil | 324 | 2008-2009 | 200 CIN 1, 97 CIN 2 or CIN 3, 27 CC |
33 | 37 AIN | AIN after CIN 1: IR= 7% AIN after CIN 2/3: IR= 18.5% |
L |
| 11. | Jakobsson et al. (2011) [27] | Finland | 26,876 | 1987–2006 | 26,876 CIN (unknown grade) | NI | 3 AC | AC after CIN: SIR= 3.56 (95% Cl: 0.73-10.4) | H |
| 12. | Jiménez et al. (2009) [28] | Canada | 674 | 1992-2005 | 7 CC, 3 VaC and 1 VC | 61 | 674 AC | AC after HPV-RGD: OR= 10.5 (95% CI: 3.6-30.3) AC after CC: OR= 6.84 (95% CI: 2.16-21.61) |
H |
| 13. | Kalliala et al. (2005) [29] | Finland | 7,564 | 1974-2003 | 2,446 CIN 1 1,543 CIN 2 1,334 CIN 3 2,241 CIN “not otherwise specified” |
NI | 3 AC | AC after CIN: SIR= 5.7 (95% Cl: 1.2 to 17.0) | L |
| 14. | Matsuo et al. (2018) [30] | USA | 79,050 | 1973-2013 | 79,050 CC | 63 | 49 AC | 10-, 20-, 30-year cumulative incidence for AC after CC: 0.04%, 0.16%, and 0.38% | H |
| 15. | Neumann et al. (2016) [31] | French | 4,808 | 1989-2007 | 4,234 CC 339 VC 235 VaC |
NI | 5 AC after CC 1 AC after VC 0 AC after VaC |
AC after CC: SIR= 5.42 (95% Cl: 1.75–12.64) AC after VC: SIR= 11.7 (95% Cl: 0.15–65.51) |
L |
| 16. | Pan et al. (2019) [32] | Scotland | NI | 1989-2015 | 69,714 CIN 3 | 30 | 37 AC after CIN 3 | AC after CIN 3: SIR= 2.6 (95% Cl: 1.9–3.6) | L |
| 17. | Papatla et al. (2019) [33] | USA | 21,060 | 1973-2014 | 21,060 CC | 61.73 | 17 AC | AC after CC: SIR= 2.20 (95% Cl: 1.28-3.52) | L |
| 18. | Preti et al. (2020) [34] | Italy | 3,184 | 1992-2004 | 3,184 CIN 2 or 3 | NI | 1 AC | AC after CIN 2 or 3: SIR= 1.8 (95% Cl: 0.04–10.0) | H |
| 19. | Rabkin et al. (1992) [35] | USA | 25,295 | 1935-1988 | 25,295 CC | NI | 12 AC | AC after CC: SIR= 4.6 (95% Cl: 2.4-8.1) | H |
| 20. | Saleem et al. (2011) [36] | USA | 189,206 | 1973-2007 | 124,075 CIN 3 6,792 VIN 3 1,463 VaIN 3 43,669 CC 9,950 VC 3,257 VaC |
NI | 255 AC | AC after CIN 3: SIR= 16.4 (95% CI: 13.7–19.2) AC after CC: SIR= 6.2 (95% CI: 4.1– 8.7) AC after VIN 3: SIR= 22.2 (95% CI: 16.7–28.4) AC after VC: SIR= 17.4 (95% CI: 11.5–24.4) AC after VaIN 3: SIR= 7.6 (95% CI: 2.4–15.6) AC after VaC: SIR= 1.8 (95% CI: 0.2–5.3) |
L |
| 21. | Sand et al. (2016) [37] | Denmark | 156,290 | 1978-2012 | 52,135 CIN 2 104,155 CIN 3 |
33.8 for CIN 2 34.0 for CIN 3 |
32 AC after CIN 2 125 AC after CIN 3 |
AC after CIN 2: SIR= 2.9 (2.0–4.1) AC after CIN 3: SIR= 4.2 (3.4–5.0) |
L |
| 22. | Suk et al. (2018) [38] | USA | 52,589 | 1973-2014 | 44,011 CC 6,905 VC 1,673 VaC |
63 for CC, 61 for VC, 95 for VaC |
34 AC after CC 31 AC after VC 1 AC after VaC |
AC after CC: SIR= 2.3 (95% CI: 1.6-3.2) AC after VC: SIR=13.2 (95% CI: 8.9-18.7) AC after VaC: SIR= 2.3 (95% CI: 0.1-12.8) |
L |
| 23. | Tatti et al. (2012) [39] | Argentina | 481 | 2005-2011 | 121 CIN 1 114 CIN 2/3 188 VIN 1 39 VIN 2/3 70 VaIN 1 22 VaIN 2/3 |
35 | 28 AIN 2/3 106 AIN 1 |
No info (AIN after CIN 2/3 comparted to AIN after CIN 1: OR= 1.91) |
H |
| 24. | Tomassi et al. (2018) [40] | USA | 221,511 | 2005-2015 | 1,168 CC 15,711 CIN 2/3 109,893 CIN 1 94,739 genital warts |
63.8 | 1 AC after CC 5 AC after CIN 2/3 14 AC after CIN 1 14 AC after genital wards |
AC after CC: IR= 0.09% AC after CIN 2/3: IR= 0.03% AC after CIN 1: IR= 0.01% AC after genital wards: IR= 0.01% |
H |
| 25. | Wang et al. (2020) [41] | USA | 56,127 | 2000-2015 | 46,550 CC 7,855 VC 1,722 VaC |
NI | 50 AC after CC 9 AC after VC 1 AC after VaC |
AC after CC: SIR= 1.63 (95% Cl: 1.21- 2.14) AC after VC: SIR= 1.10 (95% Cl: 0.50-2.09) AC after VaC: SIR= 0.62 (95% Cl: 0.01- 3.47) |
L |
* One out of five cancer registries divided results for AC and rectal cancer, therefore only data from US SEER program are included. **No information about separate number of CIN 2 and CIN 3. AC- anal cancer; AIN- anal intraepithelial neoplasia; CC- cervical cancer; VC- vulvar cancer; VaC- vaginal cancer; CIN- cervical intraepithelial neoplasia; VIN- vulvar intraepithelial neoplasia; VaIN- vaginal intraepithelial neoplasia; L- low risk of bias; H- high risk of bias; U- unclear risk of bias; NI- no information; SIR- standardized incidence ratio; IR- incidence risk; OR- odds ratio.
Another method of determining the risk of AIN/AC used by the authors in the reviewed articles was to provide the percentage of people with a history of a given HPV-RGD disease who were diagnosed with AIN/AC. The IR is calculated as [number of new cases of disease during specified period] / [size of population at start of period] (see Supplementary Material S4 for details providing definition and interpretation of IR). In four researches authors calculated IR [21,26,30,40]. For the remaining papers, we calculated the IR based on the data provided in the articles. Table 2 shows the results.
The IR of AC in people with history of: CC ranged from 0.06% to 0.12% with the mean IR of 0.086%; VC ranged from 0.22% to 0.295% with the mean IR of 0.265%; VaC ranged from 0.061% to 0.13% with the mean IR of 0.096%; CIN 3 ranged from 0.04% to 0.12% with the mean IR of 0.084%; CIN 2 was 0.061%; CIN 1 was 0.013%; CIN (without dividing into subcategories) ranged from 0.011% to 0.12% with the mean IR of 0.066%; VaIN 3 was 0.342%; VIN 3 was 0.810%. We have not found any study that analyzes IR of AC in people with history of VaIN 1 or 2 and VIN 1 or 2. The mean IR of AC for all HPV-RGDs is 0.096%. The IR of AIN in people with history of: CIN ranged from 14.4% to 18.5% with the mean IR of 16.45%; VIN was 36.4%; VaIN was 18.2%. The mean IR of AIN for all HPV-RGDs is 23.683%.
In publications where the authors provided information on PY, it was possible to calculate the IR per 100,000 PY according to the following formula IR per 100,000 PY = [number of new cases of disease] x 100,000 / PY (see Supplementary Material S5 for details providing definition and interpretation of IR per 100,000 PY). Table 2 shows the results. The IR per 100,000 PY of AC in case of patients with history of CC ranged from 7.6 to 12.36 with the mean of 9.73; for VC ranged from 2.1 to 65.23 with the mean of 37.98; for VaC ranged from 8.3 to 15.26 with the mean of 11.78; for CIN 3 ranged from 4.14 to 8.17 with the mean of 5.78; for CIN (1-3) ranged from 1.32 to 12.74 with the mean of 5.37. The mean IR per 100,000 of AC for all HPV-RGDs is 10.37. Only one research had sufficient data to calculate IR per 100,000 PY after AIN and that was the Ebisch et al. paper where the risk of AIN 3 in patients with a history of CIN 3 was 6.34.
Data on the risk of developing AIN after HPV-RGD were much scarcer compared to data on the risk of AC. Only four studies analyzed the risk of developing AIN after HPV-RGD and in addition all of them concentrated on patients with precancerous lesions: CIN, VIN, VaIN [18,20,25,38]. We have not found any study that analyzes the risk of AIN after HPV-related gynecological neoplasms, i.e. CC, VC and VaC. In case of only one study it was possible to determined the SIR and IR per 100,00 PY for AIN and it was 6.68 (95% CI: 3.64- 12.25) and 6.34 respectively in patients with a prior diagnosis of CIN 3 [19].
Summarized results of SIR, IR and IR per 100,000 PY of AC and AIN after primary diagnosis of specific HPV-RGD are presented in Table 3.
The obtained data indicate that the risk of developing AIN after HPV-RGD is much higher than the risk of developing AC. Taking into account only precancerous lesions, the highest risk of developing AIN concerned the history of VIN- IR=36.4%. In case of CIN history the IR was 16.45% with the IR per 100,000 of 6.34. In case of VaIN the IR was 18.2%.
4. Discussion
The results of our review shows that the HPV-RGD that increased the risk of AC the most was VC, both when using the SIR value (10.85), IR value (0.286%) and IR per 100,000 PY value (37.98). The risk of AC was lower in case of CC history (SIR = 3.629; IR= 0.084%, IR per 100,000 PY= 9.73), while the lowest risk of AC was established in case of VaC history (SIR = 1.573; IR= 0.059%, IR per 100,000 PY= 11.78). The risk of developing AC in patients with history of CIN increased with the severity of CIN. The highest was for CIN 3 (SIR = 5.637; IR = 0.075%, IR per 100,000 PY= 5.78) and the lowest for CIN 1 (SIR and IR per 100,000 PY was not obtained in any publication; IR = 0.01%). The risk of developing AC in patients with a history of CIN (without dividing into subtypes) was calculated with SIR of 4.571, IR of 0.0298% and IR per 100,000 PY of 5.37.
Although we obtained much less data on the risk of AIN in people with HPV-RGD compared to AC, it is certain that the risk of AIN in this subgroup of patients is much higher than AC. The greatest risk of AIN is in the case of previous diagnosis of VIN (36.4%), followed by VaIN (18.2%) and CIN (16.45%). The risk calculated by us is slightly higher than in the study by Santos et al, however, the authors gave the cumulative AIN risk for CIN, VIN and VaIN without separating them into individual types of precancerous lesions [42]. Moreover, Clark et al. proved that the actual prevalence of AIN may be even higher if high-resolution anoscopy (HRA) was used to detect disease, because it has the highest sensitivity in detecting precancerous anal lesions [43].
In our review study, we showed that patients with a history of HPV-related disease have a significantly increased risk of AIN and AC. This data leads to the concept that this patients, after being treated for the previous HPV-related disease, should be strictly controlled to prevent the development of another HPV-related disease. Unfortunately, currently there are no recommendations or guidelines that would clearly define how should such a control look like, how long it should last and who should be responsible for it. Recently the International Anal Neoplasia Society (IANS) assembled a Task Force in order to systematize and establish recommendations for AC screening [44].
We think that the gynecologist should be responsible for preventing the development of HPV-related disease in the a whole anogenital region. The gynecologist is the specialist to whom women regularly schedule for tests of secondary prevention of CC - cytology and/or a test for a high-risk human papillomavirus (hrHPV). The gynecologist takes a swab from the cervix. It is a quick and painless examination, which gives many benefits to patients. More importantly in the context of this divagation, it is also a perfect moment when a gynecologist can perform a similar procedure and take an additional swab from the anal canal in a group of patients with a particularly high risk of development of AC. Thus, the gynecologist will become the person responsible for detecting such changes and then referring the patient to an anorectal disease specialist in order to implement tertiary prevention.
Another important issue, that should be raised by gynecologists, in terms of prevention of other HPV-related diseases, is prophylactic vaccination against HPV. It is applicable even in people in older age, and with HPV-related disease. It was shown to be effective in older age [45,46] and in preventing recurrent CIN [47,48,49,50]. We believe that in this case it is also the gynecologist who should be responsible for disseminating knowledge and encouraging patients to be vaccinated against HPV. Currently, 9-valent, 4-valent and 2-valent HPV vaccines have been licensed and are available. They are highly effective in preventing HPV infection and following precancers and cancers of cervix, vagina, vulva, anus and probably also oropharyngeal region attributable to types of HPV targeted by the vaccines [51,52,53,54,55,56,57,58,59,60,61].
Currently, the gold standard in AC screening is HRA [62] (Figure 2). It allows the visualization of the rectal mucosa using an anoscope and the identification of macroscopic lesions that can be biopsied or locally excised and sent for histopathological examination. Due to the fact that in the anus, similarly as in the cervix, there is a transformation zone where glandular epithelium connects with squamous epithelium, tests used routinely in the screening of CC, i.e. cytology or hrHPV, may also be appropriate here. There are studies that compare the effectiveness of both methods in the context of AIN/AC diagnostics, but at the moment it has not been determined which of the tests alone or in combination with other methods, and for what population (probably for a pre-specified population at higher risk) would be ideal as an element of screening [12,43,63].
Due to rarity of AC and economic issues, the introduction of routine AC screening in case of every patient who has ever been diagnosed with HPV-related cancer or a corresponding precancerous lesion is impossible even for the richest countries. Therefore, it is important to select the subgroup of patients with the highest risk of AIN/AC and establish a cost-effective algorithms concerning AC screening. To do this, the relevant risk factors must be identified.
The major issue is the identification of people with disorders in the functioning of the immune system. Patients suffering from HIV, in immunosuppression or with congenital immunodeficiency disorders, constitute a group where HPV infection occurs more often and spreads more easily. In this particular group of patients, the time to development of AIN/AC will be much shorter than in people with a properly functioning immune system [64,65]. In programs for cervical cancer screening, patients with immunosuppression constitute a special population with distinct management a compared to general population [66,67]. In addition, there are data showing that in case of HIV-positive people the proportions of occurrence of different types of HPV in the anal canal is different compare to HIV-negative people. The frequency of infection with type 16 is decreased in favor of type 18. Moreover the frequency of infection with type 31, 33, 45, 52 and 58 is also significantly increased. This is probably due to the greater ability of type 16 to evade host immune control compared to other types. In the case of deficiency of the immune system, infection with other types of HPV is able to survive longer and thus cause precancerous lesions followed by AC [12]. Population of people living with HIV might also benefit from HPV vaccination, because its effectiveness was shown, especially those with optimal CD4 cell count [68,69,70].
Surprisingly, only 4 of the studies that we have reviewed reported the HIV status of the research participants [21,26,28,39]. The authors of this research are convinced that, due to such a distinct pathophysiology of HPV infection in HIV-positive and HIV-negative patients, this two groups should be always analyzed separately in context of subjects as discussed in this publication.
Another factor that should be mentioned is the time between the clinical disease and the onset of HPV infection. It has been proven that the risk of CC increases with increasing time since infection in the cervix. The median progression time from CIN 1 to CIN 2/3 is 2-3 years [71] and the subsequent median time to develop CC is 10–12 year [72]. Similar dependence can be found in case of the AC. Patients with long untreated active HPV infection have a higher risk of developing AIN/AC, however the specific average amount of time required to develop AC has not yet been specified. It is also important to emphasize the fact that the treatment of an HPV-related lesion in a gynecological organ, e.g. CIN, does not mean a complete treatment of HPV infection. In the case of a long-term infection of the cervix, there is a high risk of transfer of HPV to nearby anatomical regions, e.g. to the anal canal. Such a patient, even after complete treatment of gynecological intraepithelial neoplasia, may develop HPV-related disease in the anal canal in future. This is another argument for the need of AC screening in the subpopulation of people at the highest risk of developing HPV-related diseases.
Moreover, the specific type of HPV is another important issue in case of analyzing the risk of carcinogenesis process. The time needed for the development of CC in case of high-oncogenic HPV types (mostly 16 and 18, but also 31, 33, 35, 39, 45, 51, 52, 56, 58, 59, 66, and 68) is significantly shorter in comparison with low-oncogenic HPV types. In the case of perianal infection and the development of AC, the pathophysiology is probably similar. However, further research is required to isolate the HPV types with the highest risk of carcinogenesis in the anal canal.
The age of the patients is also a valid risk factor. The incidence of AC increases 2.7% per year, with pronounced increases in age groups 50 years and older [73]. The average life expectancy in the world is constantly increasing, therefore the percentage of patients who live with various chronic diseases is also increasing. In the past, such diseases did not develop enough to be a direct cause of death. With advances in medicine and better awareness of the public about their own health, such diseases have become a significant public problem. An example is AC, a disease that is more common in older people. As the age of the population increases, the mortality rate due to this cancer increases. HPV types can be detected in 80-90% of all AC cases, which make this neoplasm second after CC the closest HPV-associated cancer [74]. Due to the fact that, as in the case of CC, an appropriate amount of time must pass for the process of carcinogenesis to occur, it is young and middle-aged patients who will obtain the greatest benefits from the introduction of secondary AC prevention programs, because their potential number of years gained after treatment of detected AIN is the highest. Bearing in mind the fact that the society is constantly aging, we should already be ahead of the health problems in the society that the future will bring us.
Another major reason why the additional screening in people with HPV-related diseases is important are the problems with selection of an appropriate method of treatment in people with HPV-related extensive changes in the anogenital area. In such cases, treatment with topical cidofovir or imiquimod may be offered. Unfortunately, their effectiveness is quite low, and relatively many patients do not tolerate treatment in maximum doses [75,76]. Surgical treatment is an alternative however, it is used in limited lesions. In advanced lesions, surgery can be a mutilating procedure involving extensive operations sometimes requiring skin grafts from other areas (Figure 3).
The ANCHOR study has proven that treatment of AIN reduces the risk of future AC in people living with HIV [77]. The next step should be to determine whether such treatment is also beneficial in the HIV-negative population, i.e. in patients with HPV-RGD. However, the lack of clearly defined rules for the detection of AIN, especially in populations most at risk of developing AC constitute an obstruction. Therefore, the goal for the coming years should be to set clear, strictly defined rules of how AIN diagnostics should look like.
The strength of our study is that we performed a systematic review of all relevant publications referring to the subject of research –not only the risk of AC but also, what is unique, the risk of AIN in patients who were diagnosed and treated for gynecological HPV-related diseases. Additionally a critical evaluation of included articles was performed to provide a level of risk of bias. A summary of all available up-to-date data.
We acknowledge limitations of the study. The first is that majority of evaluated publications were based on national registries databases. This kind of research is vulnerable on bias, because of potential underreporting or misclassification of diseases and procedures is possible. The second is that AC is a rare disease. Moreover, AIN might by significantly underreported because there are no established screening programs, and HRA, as the best tool to diagnose AIN is not easily available and difficult procedure. Low numbers of both AC and AIN might have significant impact on the calculation of SIR. The smaller number of cases with the target disease, the less precise the SIR calculation is [78]. The third limitation is that interpretation of data might be biased because of a relatively long time between the diagnosis of HPV-RGD and secondary AC, which is about 13.5 years from the diagnosis of cervical cancer, based on available data [30]. Thus, a diagnosis of AIN could be the outcome, that should be considered as an end-point for future research evaluating the risk of anal HPV disease in a population of patients with HPV-RGD. Given the above mentioned fact of the relatively long period of time between cervical cancer and the diagnosis of AC, the forth obstacle should be recognized in terms of interpretation of available data. Establishing the risk of secondary AC and it’s morbidity and mortality seems more important for a subgroup of patients treated for a localized cervical cancer, because over 90% of these patients survive longer than 5 years. Contrary, only about 60% and 17% of patients with regional and distant disease respectively, live longer than 5 years [79]. Again the SIR number can be underestimated, though this issue might not be clinically useful, especially among patients with advanced, aggressive cervical carcinomas.
5. Conclusions
The risk of developing secondary AC/AIN is significantly higher in the group of people with primary HPV-RGD than in the general population. Patients who have been diagnosed with VC have the highest risk of secondary AC/AIN. The risk of AIN is much higher in people with HPV-RGD than the risk of AC. Further studies are required to determine the exact risk of AIN in the HPV-RGD subpopulation, particularly in those with CC, VC and VaIN. A targeted screening programs, including both surveillance (HRA, smears for hrHPV, cytology) and HPV vaccination, for AC/AIN should be developed for patients with HPV-RGD. The true burden of AC/AIN could be determined in prospective studies addressing these specific programs.
Supplementary Materials
The following supporting information can be downloaded at the website of this paper posted on Preprints.org.
Author Contributions
Conceptualization, M.B. and M.S.; methodology, M.B. and M.S.; validation, M.B. and M.S.; formal analysis, M.B.; investigation, M.B and M.S.; writing—original draft preparation, M.B.; writing—review and editing, M.B. and M.S.; visualization, M.B. and M.S.; supervision, M.S.; project administration, M.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Not applicable.
Data Availability Statement
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations:
| AC | anal cancer |
| AIN | anal intraepithelial neoplasia |
| CC | cervical cancer |
| CIN | cervical intraepithelial neoplasia |
| Cl | confidence level |
| HPV | human papillomavirus |
| HPV-RGD | HPV-related gynecological diseases |
| IR | incidence risk |
| OR | odds ratio |
| PY | person-years |
| SD | standard deviation |
| SIR | standardized incidence ratio |
| VaC | vaginal cancer |
| VaIN | vaginal intraepithelial neoplasia |
| VIN | vulvar intraepithelial neoplasia |
| VC | vulvar cancer |
References
- Sung, H.; Ferlay, J.; Siegel, R.L.; Laversanne, M.; Soerjomataram, I.; Jemal, A.; Bray, F. Global Cancer Statistics 2020: GLOBOCAN Estimates of Incidence and Mortality Worldwide for 36 Cancers in 185 Countries. CA. Cancer J. Clin. 2021, 71, 209–249. [Google Scholar] [CrossRef] [PubMed]
- Kreisel, K.M.; Spicknall, I.H.; Gargano, J.W.; Lewis, F.M.T.; Lewis, R.M.; Markowitz, L.E.; Roberts, H.; Johnson, A.S.; Song, R.; St Cyr, S.B.; et al. Sexually Transmitted Infections Among US Women and Men: Prevalence and Incidence Estimates, 2018. Sex. Transm. Dis. 2021, 48, 208–214. [Google Scholar] [CrossRef] [PubMed]
- de Martel, C.; Plummer, M.; Vignat, J.; Franceschi, S. Worldwide Burden of Cancer Attributable to HPV by Site, Country and HPV Type. Int. J. Cancer 2017, 141, 664–670. [Google Scholar] [CrossRef] [PubMed]
- Gheit, T. Mucosal and Cutaneous Human Papillomavirus Infections and Cancer Biology. Front. Oncol. 2019, 9, 355. [Google Scholar] [CrossRef]
- Ibeanu, O.A. Molecular Pathogenesis of Cervical Cancer. Cancer Biol. Ther. 2011, 11, 295–306. [Google Scholar] [CrossRef] [PubMed]
- Hernandez, B.Y.; McDuffie, K.; Zhu, X.; Wilkens, L.R.; Killeen, J.; Kessel, B.; Wakabayashi, M.T.; Bertram, C.C.; Easa, D.; Ning, L.; et al. Anal Human Papillomavirus Infection in Women and Its Relationship with Cervical Infection. Cancer Epidemiol. Biomark. Prev. Publ. Am. Assoc. Cancer Res. Cosponsored Am. Soc. Prev. Oncol. 2005, 14, 2550–2556. [Google Scholar] [CrossRef] [PubMed]
- Jacot-Guillarmod, M.; Balaya, V.; Mathis, J.; Hübner, M.; Grass, F.; Cavassini, M.; Sempoux, C.; Mathevet, P.; Pache, B. Women with Cervical High-Risk Human Papillomavirus: Be Aware of Your Anus! The ANGY Cross-Sectional Clinical Study. Cancers 2022, 14, 5096. [Google Scholar] [CrossRef] [PubMed]
- D’Souza, G.; Wiley, D.J.; Li, X.; Chmiel, J.S.; Margolick, J.B.; Cranston, R.D.; Jacobson, L.P. Incidence and Epidemiology of Anal Cancer in the Multicenter AIDS Cohort Study. J. Acquir. Immune Defic. Syndr. 1999 2008, 48, 491–499. [Google Scholar] [CrossRef]
- Silverberg, M.J.; Lau, B.; Justice, A.C.; Engels, E.; Gill, M.J.; Goedert, J.J.; Kirk, G.D.; D’Souza, G.; Bosch, R.J.; Brooks, J.T.; et al. Risk of Anal Cancer in HIV-Infected and HIV-Uninfected Individuals in North America. Clin. Infect. Dis. Off. Publ. Infect. Dis. Soc. Am. 2012, 54, 1026–1034. [Google Scholar] [CrossRef]
- Shiels, M.S.; Pfeiffer, R.M.; Chaturvedi, A.K.; Kreimer, A.R.; Engels, E.A. Impact of the HIV Epidemic on the Incidence Rates of Anal Cancer in the United States. J. Natl. Cancer Inst. 2012, 104, 1591–1598. [Google Scholar] [CrossRef]
- de Sanjosé, S.; Bruni, L.; Alemany, L. HPV in Genital Cancers (at the Exception of Cervical Cancer) and Anal Cancers. Presse Medicale Paris Fr. 1983 2014, 43, e423–e428. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.A.; Wentzensen, N. Strategies for Screening and Early Detection of Anal Cancers: A Narrative and Systematic Review and Meta-Analysis of Cytology, HPV Testing, and Other Biomarkers. Cancer Cytopathol. 2018, 126, 447–460. [Google Scholar] [CrossRef] [PubMed]
- Lin, C.; Slama, J.; Gonzalez, P.; Goodman, M.T.; Xia, N.; Kreimer, A.R.; Wu, T.; Hessol, N.A.; Shvetsov, Y.; Ortiz, A.P.; et al. Cervical Determinants of Anal HPV Infection and High-Grade Anal Lesions in Women: A Collaborative Pooled Analysis. Lancet Infect. Dis. 2019, 19, 880–891. [Google Scholar] [CrossRef] [PubMed]
- Page, M.J.; McKenzie, J.E.; Bossuyt, P.M.; Boutron, I.; Hoffmann, T.C.; Mulrow, C.D.; Shamseer, L.; Tetzlaff, J.M.; Akl, E.A.; Brennan, S.E.; et al. The PRISMA 2020 Statement: An Updated Guideline for Reporting Systematic Reviews. BMJ 2021, 372, n71. [Google Scholar] [CrossRef] [PubMed]
- Waxman, A.G.; Chelmow, D.; Darragh, T.M.; Lawson, H.; Moscicki, A.-B. Revised Terminology for Cervical Histopathology and Its Implications for Management of High-Grade Squamous Intraepithelial Lesions of the Cervix. Obstet. Gynecol. 2012, 120, 1465–1471. [Google Scholar] [CrossRef] [PubMed]
- Whiting, P.F.; Rutjes, A.W.S.; Westwood, M.E.; Mallett, S.; Deeks, J.J.; Reitsma, J.B.; Leeflang, M.M.G.; Sterne, J.A.C.; Bossuyt, P.M.M. QUADAS-2 Group QUADAS-2: A Revised Tool for the Quality Assessment of Diagnostic Accuracy Studies. Ann. Intern. Med. 2011, 155, 529–536. [Google Scholar] [CrossRef] [PubMed]
- Acevedo-Fontánez, A.I.; Suárez, E.; Torres Cintrón, C.R.; Ortiz, A.P. Risk of Anal Cancer in Women With a Human Papillomavirus–Related Gynecological Neoplasm: Puerto Rico 1987–2013. J. Low. Genit. Tract Dis. 2018, 22, 225–230. [Google Scholar] [CrossRef] [PubMed]
- Chaturvedi, A.K.; Engels, E.A.; Gilbert, E.S.; Chen, B.E.; Storm, H.; Lynch, C.F.; Hall, P.; Langmark, F.; Pukkala, E.; Kaijser, M.; et al. Second Cancers Among 104760 Survivors of Cervical Cancer: Evaluation of Long-Term Risk. JNCI J. Natl. Cancer Inst. 2007, 99, 1634–1643. [Google Scholar] [CrossRef]
- Ebisch, R.M.F.; Rutten, D.W.E.; IntHout, J.; Melchers, W.J.G.; Massuger, L.F.A.G.; Bulten, J.; Bekkers, R.L.M.; Siebers, A.G. Long-Lasting Increased Risk of Human Papillomavirus–Related Carcinomas and Premalignancies After Cervical Intraepithelial Neoplasia Grade 3: A Population-Based Cohort Study. J. Clin. Oncol. 2017, 35, 2542–2550. [Google Scholar] [CrossRef]
- Edgren, G.; Sparén, P. Risk of Anogenital Cancer after Diagnosis of Cervical Intraepithelial Neoplasia: A Prospective Population-Based Study. Lancet Oncol. 2007, 8, 311–316. [Google Scholar] [CrossRef]
- ElNaggar, A.C.; Santoso, J.T. Risk Factors for Anal Intraepithelial Neoplasia in Women With Genital Dysplasia. Obstet. Gynecol. 2013, 122, 218–223. [Google Scholar] [CrossRef] [PubMed]
- Evans, H.S.; Newnham, A.; Hodgson, S.V.; Møller, H. Second Primary Cancers after Cervical Intraepithelial Neoplasia III and Invasive Cervical Cancer in Southeast England. Gynecol. Oncol. 2003, 90, 131–136. [Google Scholar] [CrossRef] [PubMed]
- Gaudet, M.; Hamm, J.; Aquino-Parsons, C. Incidence of Ano-Genital and Head and Neck Malignancies in Women with a Previous Diagnosis of Cervical Intraepithelial Neoplasia. Gynecol. Oncol. 2014, 134, 523–526. [Google Scholar] [CrossRef] [PubMed]
- Hemminki, K.; Jiang, Y.; Dong, C. Second Primary Cancers after Anogenital, Skin, Oral, Esophageal and Rectal Cancers: Etiological Links? Int. J. Cancer 2001, 93, 294–298. [Google Scholar] [CrossRef] [PubMed]
- Hemminki, K.; Dong, C.; Vaittinen, P. Second Primary Cancer after in Situ and Invasive Cervical Cancer. Epidemiol. Camb. Mass 2000, 11, 457–461. [Google Scholar] [CrossRef] [PubMed]
- Heráclio, S.A.; De Souza, A.S.R.; De Souza, P.R.E.; Katz, L.; Lima Junior, S.F.; Amorim, M.M.R. Cross-Sectional Study of Anal Intraepithelial Lesions in Women with Cervical Neoplasia without HIV. Int. J. Gynecol. Obstet. 2018, 140, 233–240. [Google Scholar] [CrossRef]
- Jakobsson, M.; Pukkala, E.; Paavonen, J.; Tapper, A.; Gissler, M. Cancer Incidence among Finnish Women with Surgical Treatment for Cervical Intraepithelial Neoplasia, 1987–2006. Int. J. Cancer 2011, 128, 1187–1191. [Google Scholar] [CrossRef]
- Jiménez, W.; Paszat, L.; Kupets, R.; Wilton, A.; Tinmouth, J. Presumed Previous Human Papillomavirus (HPV) Related Gynecological Cancer in Women Diagnosed with Anal Cancer in the Province of Ontario. Gynecol. Oncol. 2009, 114, 395–398. [Google Scholar] [CrossRef]
- Kalliala, I.; Anttila, A.; Pukkala, E.; Nieminen, P. Risk of Cervical and Other Cancers after Treatment of Cervical Intraepithelial Neoplasia: Retrospective Cohort Study. BMJ 2005, 331, 1183–1185. [Google Scholar] [CrossRef]
- Matsuo, K.; Blake, E.A.; Machida, H.; Mandelbaum, R.S.; Roman, L.D.; Wright, J.D. Incidences and Risk Factors of Metachronous Vulvar, Vaginal, and Anal Cancers after Cervical Cancer Diagnosis. Gynecol. Oncol. 2018, 150, 501–508. [Google Scholar] [CrossRef]
- Neumann, F.; Jégu, J.; Mougin, C.; Prétet, J.-L.; Guizard, A.-V.; Lapôtre-Ledoux, B.; Bara, S.; Bouvier, V.; Colonna, M.; Troussard, X.; et al. Risk of Second Primary Cancer after a First Potentially-Human Papillomavirus-Related Cancer: A Population-Based Study. Prev. Med. 2016, 90, 52–58. [Google Scholar] [CrossRef] [PubMed]
- Pan, J.; Kavanagh, K.; Cuschieri, K.; Pollock, K.G.; Gilbert, D.C.; Millan, D.; Bell, S.; Graham, S.V.; Williams, A.R.W.; Cruickshank, M.E.; et al. Increased Risk of HPV-Associated Genital Cancers in Men and Women as a Consequence of Pre-Invasive Disease. Int. J. Cancer 2019, 145, 427–434. [Google Scholar] [CrossRef] [PubMed]
- Papatla, K.; Halpern, M.T.; Hernandez, E.; Brown, J.; Benrubi, D.; Houck, K.; Chu, C.; Rubin, S. Second Primary Anal and Oropharyngeal Cancers in Cervical Cancer Survivors. Am. J. Obstet. Gynecol. 2019, 221, 478.e1. [Google Scholar] [CrossRef] [PubMed]
- Preti, M.; Rosso, S.; Micheletti, L.; Libero, C.; Sobrato, I.; Giordano, L.; Busso, P.; Gallio, N.; Cosma, S.; Bevilacqua, F.; et al. Risk of HPV-Related Extra-Cervical Cancers in Women Treated for Cervical Intraepithelial Neoplasia. BMC Cancer 2020, 20, 972. [Google Scholar] [CrossRef] [PubMed]
- Rabkin, C.S.; Biggar, R.J.; Melbye, M.; Curtis, R.E. Second Primary Cancers Following Anal and Cervical Carcinoma: Evidence of Shared Etiologic Factors. Am. J. Epidemiol. 1992, 136, 54–58. [Google Scholar] [CrossRef]
- Saleem, A.M.; Paulus, J.K.; Shapter, A.P.; Baxter, N.N.; Roberts, P.L.; Ricciardi, R. Risk of Anal Cancer in a Cohort With Human Papillomavirus–Related Gynecologic Neoplasm. Obstet. Gynecol. 2011, 117, 643–649. [Google Scholar] [CrossRef]
- Sand, F.L.; Munk, C.; Jensen, S.M.; Svahn, M.F.; Frederiksen, K.; Kjær, S.K. Long-Term Risk for Noncervical Anogenital Cancer in Women with Previously Diagnosed High-Grade Cervical Intraepithelial Neoplasia: A Danish Nationwide Cohort Study. Cancer Epidemiol. Biomarkers Prev. 2016, 25, 1090–1097. [Google Scholar] [CrossRef]
- Suk, R.; Mahale, P.; Sonawane, K.; Sikora, A.G.; Chhatwal, J.; Schmeler, K.M.; Sigel, K.; Cantor, S.B.; Chiao, E.Y.; Deshmukh, A.A. Trends in Risks for Second Primary Cancers Associated With Index Human Papillomavirus–Associated Cancers. JAMA Netw. Open 2018, 1, e181999. [Google Scholar] [CrossRef]
- Tatti, S.; Suzuki, V.; Fleider, L.; Maldonado, V.; Caruso, R. Anal Intraepithelial Lesions in Women With Human PapillomavirusYRelated Disease. J Low Genit Tract Dis 2012, 16, 454–459. [Google Scholar] [CrossRef]
- Tomassi, M.J.; Abbas, M.A.; Klaristenfeld, D.D. Expectant Management Surveillance for Patients at Risk for Invasive Squamous Cell Carcinoma of the Anus: A Large US Healthcare System Experience. Int. J. Colorectal Dis. 2019, 34, 47–54. [Google Scholar] [CrossRef]
- Wang, M.; Sharma, A.; Osazuwa-Peters, N.; Simpson, M.C.; Schootman, M.; Piccirillo, J.F.; Huh, W.K.; Adjei Boakye, E. Risk of Subsequent Malignant Neoplasms after an Index Potentially-Human Papillomavirus (HPV)-Associated Cancers. Cancer Epidemiol. 2020, 64, 101649. [Google Scholar] [CrossRef] [PubMed]
- Santoso, J.T.; Long, M.; Crigger, M.; Wan, J.Y.; Haefner, H.K. Anal Intraepithelial Neoplasia in Women with Genital Intraepithelial Neoplasia. Obstet. Gynecol. 2010, 116, 578–582. [Google Scholar] [CrossRef] [PubMed]
- Clarke, M.A.; Deshmukh, A.A.; Suk, R.; Roberts, J.; Gilson, R.; Jay, N.; Stier, E.A.; Wentzensen, N. A Systematic Review and Meta-analysis of Cytology and HPV-related Biomarkers for Anal Cancer Screening among Different Risk Groups. Int. J. Cancer 2022, 151, 1889–1901. [Google Scholar] [CrossRef] [PubMed]
- IANS - IANS Committees. Available online: https://iansoc.org/IANS-Committees (accessed on 11 May 2023).
- Muñoz, N.; Manalastas, R.; Pitisuttithum, P.; Tresukosol, D.; Monsonego, J.; Ault, K.; Clavel, C.; Luna, J.; Myers, E.; Hood, S.; et al. Safety, Immunogenicity, and Efficacy of Quadrivalent Human Papillomavirus (Types 6, 11, 16, 18) Recombinant Vaccine in Women Aged 24-45 Years: A Randomised, Double-Blind Trial. Lancet Lond. Engl. 2009, 373, 1949–1957. [Google Scholar] [CrossRef] [PubMed]
- Wei, L.; Xie, X.; Liu, J.; Zhao, Y.; Chen, W.; Zhao, C.; Wang, S.; Liao, X.; Shou, Q.; Qiu, Y.; et al. Efficacy of Quadrivalent Human Papillomavirus Vaccine against Persistent Infection and Genital Disease in Chinese Women: A Randomized, Placebo-Controlled Trial with 78-Month Follow-Up. Vaccine 2019, 37, 3617–3624. [Google Scholar] [CrossRef] [PubMed]
- Bartels, H.C.; Postle, J.; Rogers, A.C.; Brennan, D. Prophylactic Human Papillomavirus Vaccination to Prevent Recurrence of Cervical Intraepithelial Neoplasia: A Meta-Analysis. Int. J. Gynecol. Cancer Off. J. Int. Gynecol. Cancer Soc. 2020, 30, 777–782. [Google Scholar] [CrossRef] [PubMed]
- Jentschke, M.; Kampers, J.; Becker, J.; Sibbertsen, P.; Hillemanns, P. Prophylactic HPV Vaccination after Conization: A Systematic Review and Meta-Analysis. Vaccine 2020, 38, 6402–6409. [Google Scholar] [CrossRef] [PubMed]
- Kechagias, K.S.; Kalliala, I.; Bowden, S.J.; Athanasiou, A.; Paraskevaidi, M.; Paraskevaidis, E.; Dillner, J.; Nieminen, P.; Strander, B.; Sasieni, P.; et al. Role of Human Papillomavirus (HPV) Vaccination on HPV Infection and Recurrence of HPV Related Disease after Local Surgical Treatment: Systematic Review and Meta-Analysis. BMJ 2022, 378, e070135. [Google Scholar] [CrossRef]
- Goodman, E.; Reuschenbach, M.; Kaminski, A.; Ronnebaum, S. Human Papillomavirus Vaccine Impact and Effectiveness in Six High-Risk Populations: A Systematic Literature Review. Vaccines 2022, 10, 1543. [Google Scholar] [CrossRef]
- Drolet, M.; Bénard, É.; Pérez, N.; Brisson, M. HPV Vaccination Impact Study Group Population-Level Impact and Herd Effects Following the Introduction of Human Papillomavirus Vaccination Programmes: Updated Systematic Review and Meta-Analysis. Lancet Lond. Engl. 2019, 394, 497–509. [Google Scholar] [CrossRef]
- Kjaer, S.K.; Nygård, M.; Sundström, K.; Dillner, J.; Tryggvadottir, L.; Munk, C.; Berger, S.; Enerly, E.; Hortlund, M.; Ágústsson, Á.I.; et al. Final Analysis of a 14-Year Long-Term Follow-up Study of the Effectiveness and Immunogenicity of the Quadrivalent Human Papillomavirus Vaccine in Women from Four Nordic Countries. EClinicalMedicine 2020, 23, 100401. [Google Scholar] [CrossRef] [PubMed]
- Olsson, S.-E.; Restrepo, J.A.; Reina, J.C.; Pitisuttithum, P.; Ulied, A.; Varman, M.; Van Damme, P.; Moreira, E.D.; Ferris, D.; Block, S.; et al. Long-Term Immunogenicity, Effectiveness, and Safety of Nine-Valent Human Papillomavirus Vaccine in Girls and Boys 9 to 15 Years of Age: Interim Analysis after 8 Years of Follow-Up. Papillomavirus Res. Amst. Neth. 2020, 10, 100203. [Google Scholar] [CrossRef] [PubMed]
- Lei, J.; Ploner, A.; Elfström, K.M.; Wang, J.; Roth, A.; Fang, F.; Sundström, K.; Dillner, J.; Sparén, P. HPV Vaccination and the Risk of Invasive Cervical Cancer. N. Engl. J. Med. 2020, 383, 1340–1348. [Google Scholar] [CrossRef] [PubMed]
- Falcaro, M.; Castañon, A.; Ndlela, B.; Checchi, M.; Soldan, K.; Lopez-Bernal, J.; Elliss-Brookes, L.; Sasieni, P. The Effects of the National HPV Vaccination Programme in England, UK, on Cervical Cancer and Grade 3 Cervical Intraepithelial Neoplasia Incidence: A Register-Based Observational Study. Lancet Lond. Engl. 2021, 398, 2084–2092. [Google Scholar] [CrossRef] [PubMed]
- Kjaer, S.K.; Dehlendorff, C.; Belmonte, F.; Baandrup, L. Real-World Effectiveness of Human Papillomavirus Vaccination Against Cervical Cancer. J. Natl. Cancer Inst. 2021, 113, 1329–1335. [Google Scholar] [CrossRef]
- Dehlendorff, C.; Baandrup, L.; Kjaer, S.K. Real-World Effectiveness of Human Papillomavirus Vaccination Against Vulvovaginal High-Grade Precancerous Lesions and Cancers. J. Natl. Cancer Inst. 2021, 113, 869–874. [Google Scholar] [CrossRef]
- Zhang, L.; Hemminki, O.; Chen, T.; Zheng, G.; Försti, A.; Sundquist, K.; Sundquist, J.; Hemminki, K. Familial Clustering, Second Primary Cancers and Causes of Death in Penile, Vulvar and Vaginal Cancers. Sci. Rep. 2019, 9, 11804. [Google Scholar] [CrossRef]
- Herrero, R.; Quint, W.; Hildesheim, A.; Gonzalez, P.; Struijk, L.; Katki, H.A.; Porras, C.; Schiffman, M.; Rodriguez, A.C.; Solomon, D.; et al. Reduced Prevalence of Oral Human Papillomavirus (HPV) 4 Years after Bivalent HPV Vaccination in a Randomized Clinical Trial in Costa Rica. PLoS ONE 2013, 8, e68329. [Google Scholar] [CrossRef]
- Lehtinen, M.; Apter, D.; Eriksson, T.; Harjula, K.; Hokkanen, M.; Lehtinen, T.; Natunen, K.; Damaso, S.; Soila, M.; Bi, D.; et al. Effectiveness of the AS04-Adjuvanted HPV-16/18 Vaccine in Reducing Oropharyngeal HPV Infections in Young Females-Results from a Community-Randomized Trial. Int. J. Cancer 2020, 147, 170–174. [Google Scholar] [CrossRef]
- Tsentemeidou, A.; Fyrmpas, G.; Stavrakas, M.; Vlachtsis, K.; Sotiriou, E.; Poutoglidis, A.; Tsetsos, N. Human Papillomavirus Vaccine to End Oropharyngeal Cancer. A Systematic Review and Meta-Analysis. Sex. Transm. Dis. 2021, 48, 700–707. [Google Scholar] [CrossRef]
- Hirsch, B.E.; McGowan, J.P.; Fine, S.M.; Vail, R.; Merrick, S.T.; Radix, A.; Hoffmann, C.J.; Gonzalez, C.J. Screening for Anal Dysplasia and Cancer in Adults With HIV; New York State Department of Health AIDS Institute Clinical Guidelines; Johns Hopkins University: Baltimore (MD), 2022. [Google Scholar]
- Leeds, I.L.; Fang, S.H. Anal Cancer and Intraepithelial Neoplasia Screening: A Review. World J. Gastrointest. Surg. 2016, 8, 41–51. [Google Scholar] [CrossRef] [PubMed]
- Kelly, H.; Chikandiwa, A.; Alemany Vilches, L.; Palefsky, J.M.; de Sanjose, S.; Mayaud, P. Association of Antiretroviral Therapy with Anal High-Risk Human Papillomavirus, Anal Intraepithelial Neoplasia, and Anal Cancer in People Living with HIV: A Systematic Review and Meta-Analysis. Lancet HIV 2020, 7, e262–e278. [Google Scholar] [CrossRef] [PubMed]
- Albuquerque, A.; Stirrup, O.; Nathan, M.; Clifford, G.M. Burden of Anal Squamous Cell Carcinoma, Squamous Intraepithelial Lesions and HPV16 Infection in Solid Organ Transplant Recipients: A Systematic Review and Meta-Analysis. Am. J. Transplant. Off. J. Am. Soc. Transplant. Am. Soc. Transpl. Surg. 2020, 20, 3520–3528. [Google Scholar] [CrossRef] [PubMed]
- Garland, S.M.; Brotherton, J.M.L.; Moscicki, A.B.; Kaufmann, A.M.; Stanley, M.; Bhatla, N.; Sankaranarayanan, R.; de Sanjosé, S.; Palefsky, J.M. ; IPVS HPV Vaccination of Immunocompromised Hosts. Papillomavirus Res. Amst. Neth. 2017, 4, 35–38. [Google Scholar] [CrossRef] [PubMed]
- Perkins, R.B.; Guido, R.S.; Castle, P.E.; Chelmow, D.; Einstein, M.H.; Garcia, F.; Huh, W.K.; Kim, J.J.; Moscicki, A.-B.; Nayar, R.; et al. 2019 ASCCP Risk-Based Management Consensus Guidelines for Abnormal Cervical Cancer Screening Tests and Cancer Precursors. J. Low. Genit. Tract Dis. 2020, 24, 102–131. [Google Scholar] [CrossRef] [PubMed]
- Mugo, N.R.; Eckert, L.; Magaret, A.S.; Cheng, A.; Mwaniki, L.; Ngure, K.; Celum, C.; Baeten, J.M.; Galloway, D.A.; Wamalwa, D.; et al. Quadrivalent HPV Vaccine in HIV-1-Infected Early Adolescent Girls and Boys in Kenya: Month 7 and 12 Post Vaccine Immunogenicity and Correlation with Immune Status. Vaccine 2018, 36, 7025–7032. [Google Scholar] [CrossRef] [PubMed]
- Mugo, N.; Eckert, L.O.; Odero, L.; Gakuo, S.; Ngure, K.; Celum, C.; Baeten, J.M.; Barnabas, R.V.; Wald, A. Antibody Responses to Prophylactic Quadrivalent Human Papillomavirus Vaccine at 48 Months among HIV-Infected Girls and Boys Ages 9-14 in Kenya, Africa. Vaccine 2021, 39, 4751–4758. [Google Scholar] [CrossRef]
- Staadegaard, L.; Rönn, M.M.; Soni, N.; Bellerose, M.E.; Bloem, P.; Brisson, M.; Maheu-Giroux, M.; Barnabas, R.V.; Drolet, M.; Mayaud, P.; et al. Immunogenicity, Safety, and Efficacy of the HPV Vaccines among People Living with HIV: A Systematic Review and Meta-Analysis. EClinicalMedicine 2022, 52, 101585. [Google Scholar] [CrossRef]
- Winer, R.L.; Kiviat, N.B.; Hughes, J.P.; Adam, D.E.; Lee, S.-K.; Kuypers, J.M.; Koutsky, L.A. Development and Duration of Human Papillomavirus Lesions, after Initial Infection. J. Infect. Dis. 2005, 191, 731–738. [Google Scholar] [CrossRef]
- Zielinski, G.D.; Snijders, P.J.; Rozendaal, L.; Voorhorst, F.J.; van der Linden, H.C.; Runsink, A.P.; de Schipper, F.A.; Meijer, C.J. HPV Presence Precedes Abnormal Cytology in Women Developing Cervical Cancer and Signals False Negative Smears. Br. J. Cancer 2001, 85, 398–404. [Google Scholar] [CrossRef]
- Deshmukh, A.A.; Suk, R.; Shiels, M.S.; Sonawane, K.; Nyitray, A.G.; Liu, Y.; Gaisa, M.M.; Palefsky, J.M.; Sigel, K. Recent Trends in Squamous Cell Carcinoma of the Anus Incidence and Mortality in the United States, 2001-2015. J. Natl. Cancer Inst. 2020, 112, 829–838. [Google Scholar] [CrossRef] [PubMed]
- Grulich, A.E.; Poynten, I.M.; Machalek, D.A.; Jin, F.; Templeton, D.J.; Hillman, R.J. The Epidemiology of Anal Cancer. Sex. Health 2012, 9, 504–508. [Google Scholar] [CrossRef] [PubMed]
- Stier, E.A.; Goldstone, S.E.; Einstein, M.H.; Jay, N.; BERRY, J.M.; Wilkin, T.; LEE, J.Y.; DARRAGH, T.M.; DA COSTA, M.; PANTHER, L.; et al. Safety and Efficacy of Topical Cidofovir to Treat High-Grade Perianal and Vulvar Intraepithelial Neoplasia in HIV-Positive Men and Women. AIDS Lond. Engl. 2013, 27, 545–551. [Google Scholar] [CrossRef]
- Tranoulis, A.; Laios, A.; Mitsopoulos, V.; Lutchman-Singh, K.; Thomakos, N. Efficacy of 5% Imiquimod for the Treatment of Vaginal Intraepithelial Neoplasia-A Systematic Review of the Literature and a Meta-Analysis. Eur. J. Obstet. Gynecol. Reprod. Biol. 2017, 218, 129–136. [Google Scholar] [CrossRef]
- Palefsky, J.M.; Lee, J.Y.; Jay, N.; Goldstone, S.E.; Darragh, T.M.; Dunlevy, H.A.; Rosa-Cunha, I.; Arons, A.; Pugliese, J.C.; Vena, D.; et al. Treatment of Anal High-Grade Squamous Intraepithelial Lesions to Prevent Anal Cancer. N. Engl. J. Med. 2022, 386, 2273–2282. [Google Scholar] [CrossRef]
- Available online: https://www.cdc.gov/nceh/cancer-environment/pdfs/standardized-incidence-ratio-fact-sheet-508.pdf (accessed on 10 May 2023).
- Cervical Cancer — Cancer Stat Facts. Available online: https://seer.cancer.gov/statfacts/html/cervix.html (accessed on 11 May 2023).
Figure 1.
PRISMA flowchart summarizing the process for the identification of eligible articles. AC- anal cancer; AIN- anal intraepithelial neoplasia.
Figure 1.
PRISMA flowchart summarizing the process for the identification of eligible articles. AC- anal cancer; AIN- anal intraepithelial neoplasia.
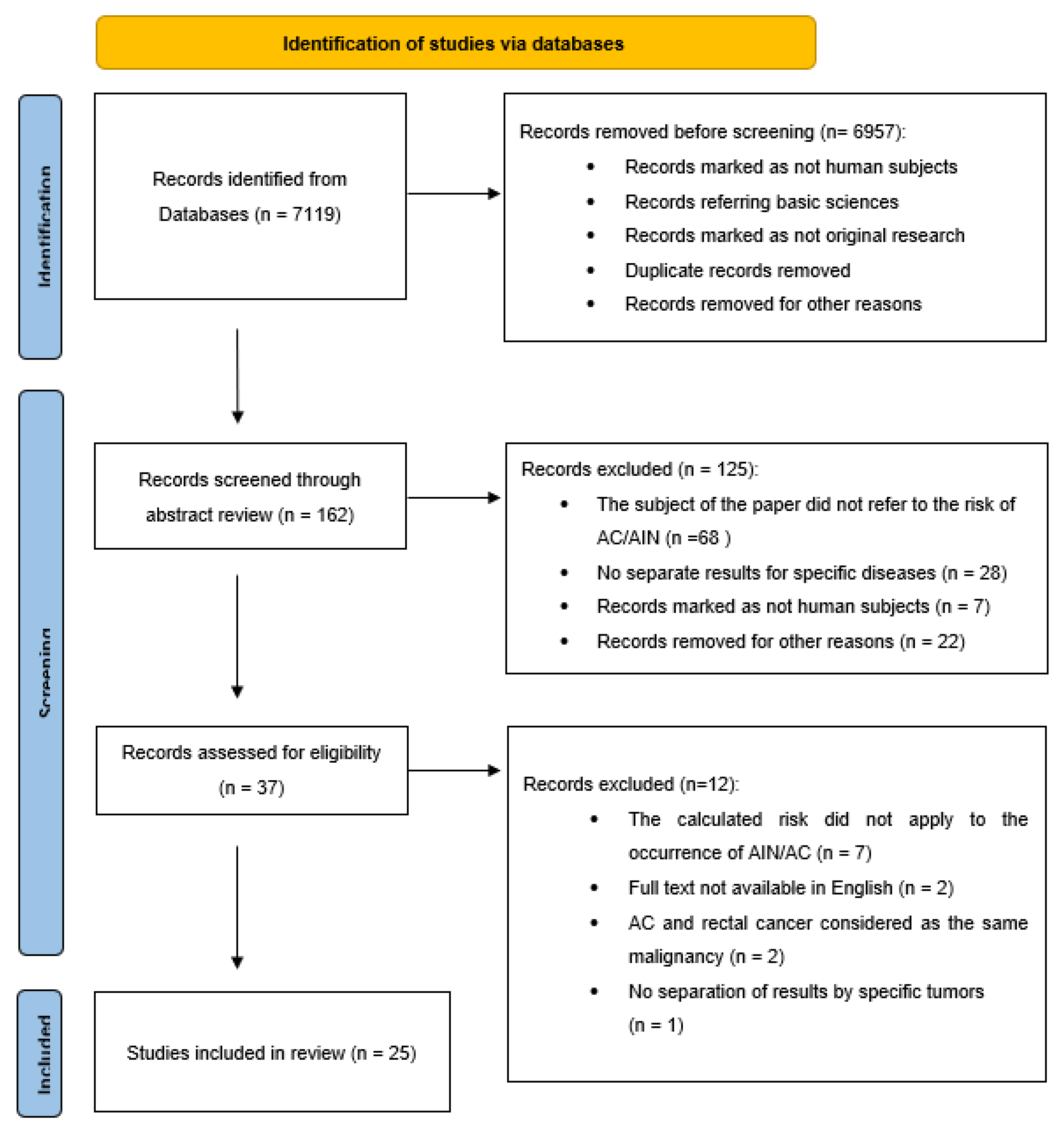
Figure 2.
Anal mucosa seen with high resolution anoscopy (HRA). Whitening of the anal mucosa after application of acetic acid indicates the probable location of anal intraepithelial neoplasia.
Figure 2.
Anal mucosa seen with high resolution anoscopy (HRA). Whitening of the anal mucosa after application of acetic acid indicates the probable location of anal intraepithelial neoplasia.
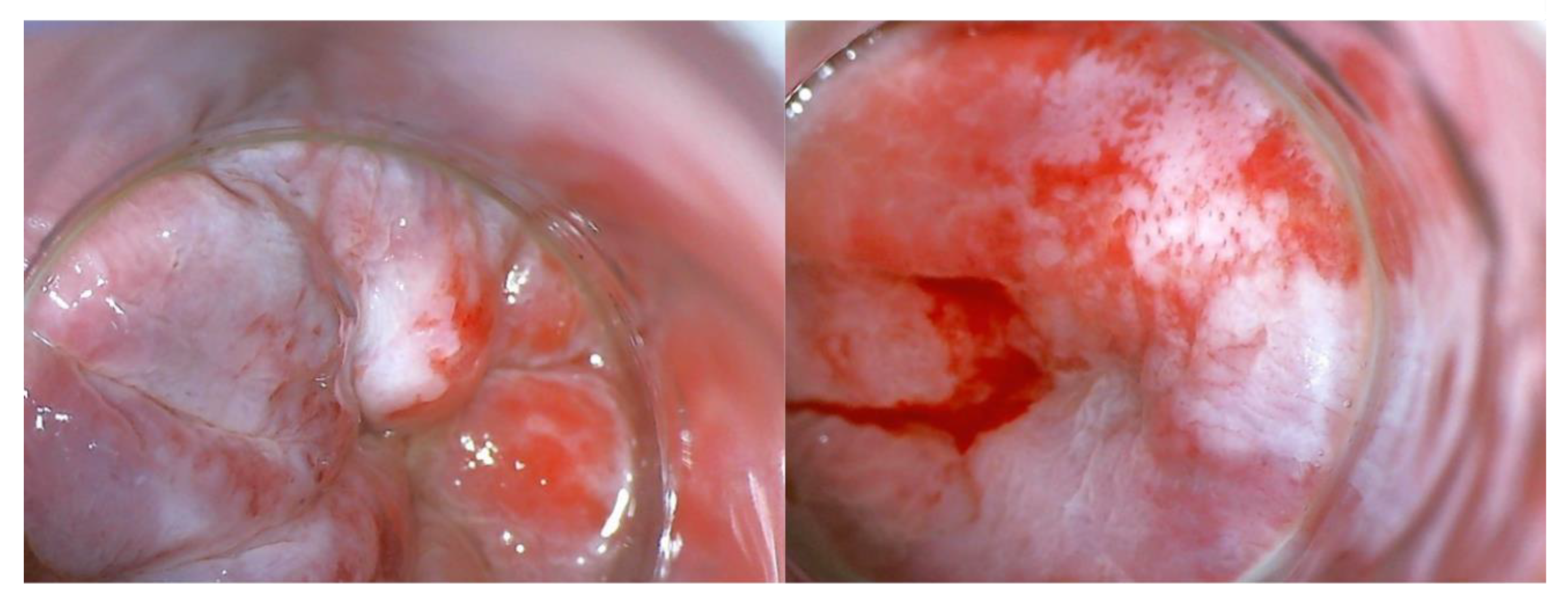
Figure 3.
Surgical treatment of HSIL(AIN3) in perianal region. A: Anal region with AIN before surgery. B: Anal region after excision of AIN . C,D: Anal region after reconstruction requiring skin grafts (Limberg flap). AIN, anal intraepithelial neoplasia.
Figure 3.
Surgical treatment of HSIL(AIN3) in perianal region. A: Anal region with AIN before surgery. B: Anal region after excision of AIN . C,D: Anal region after reconstruction requiring skin grafts (Limberg flap). AIN, anal intraepithelial neoplasia.
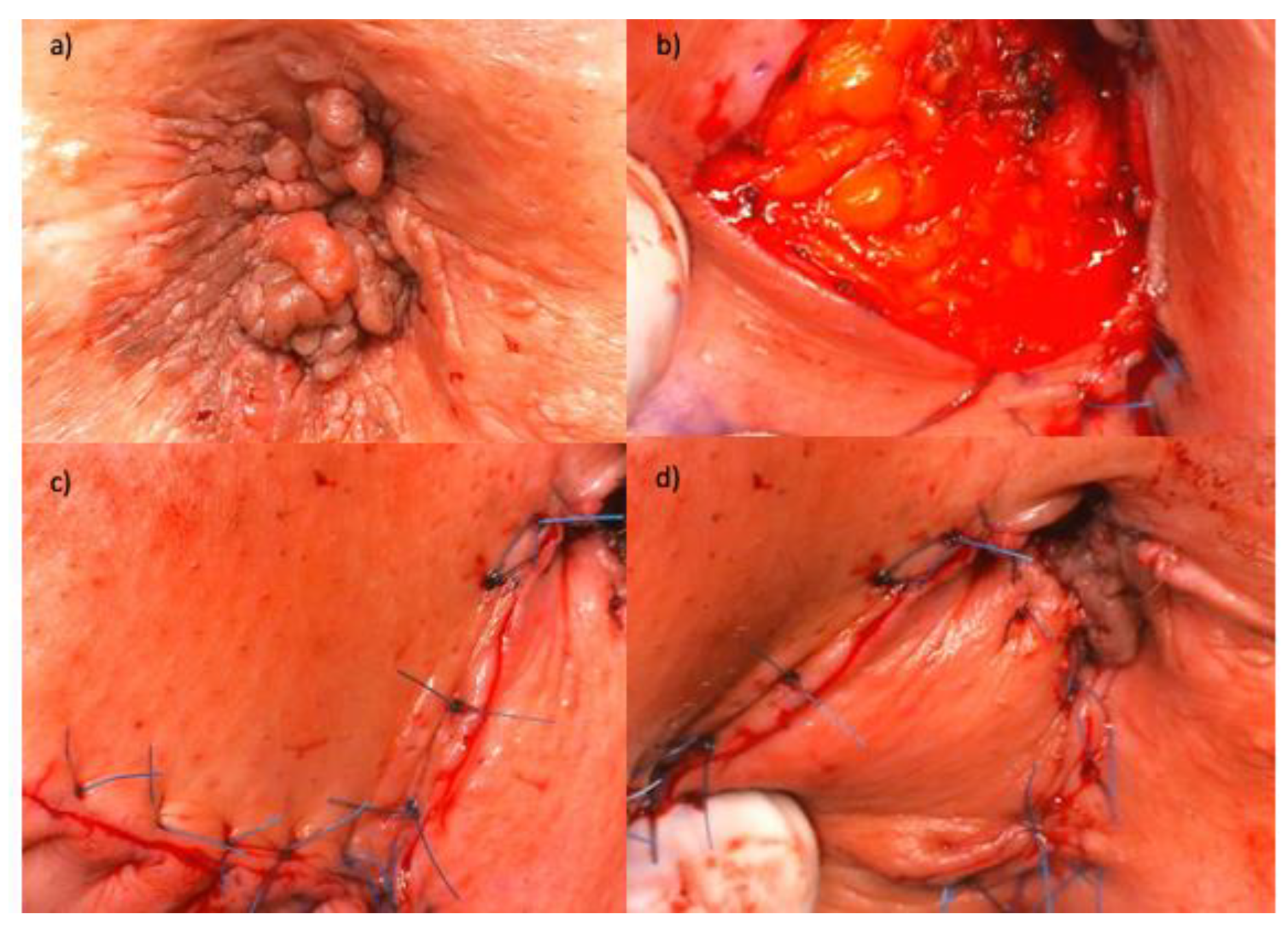
Table 2.
Incidence rate and incidence rate per 100,000 PY of anal intraepithelial neoplasia or anal cancer presented in reviewed articles or calculated on the basis of published data.
Table 2.
Incidence rate and incidence rate per 100,000 PY of anal intraepithelial neoplasia or anal cancer presented in reviewed articles or calculated on the basis of published data.
| No. | Authors and year of publication | Number of secondary AIN or AC / number of primary HPV-RGD | Person-years | Incidence rate of AIN or AC | IR per 100,000 person-years | Comment |
|---|---|---|---|---|---|---|
| 1. | Acevedo-Fontánez et al. (2018) [17] | 10 AC / 8,039 CC 3 AC / 1,378 VC 1 AC / 773 VaC |
119,617 14,631 6,554 |
0.124% 0.217% 0.129% |
8.36 20.5 15.26 |
|
| 2. | Chaturvedi et al. (2007) [18] | - | - | - | - | No information about the number of AC cases. |
| 3. | Ebisch et al. (2017) [19] | 73 AC / 89,018 CIN 3 80 AIN 3 / 89,018 CIN 3 |
1,261,804 1,261,804 |
0.082% 0.090% |
5.79 6.34 |
|
| 4. | Edgren et al. (2007) [20] | 131 AC / 125,292 CIN 3 | 2 193 409 | 0.105% | 5.97 | |
| 5. | ElNaggar et al. (2013) [21] | 13 AIN / 90 CIN 48 AIN / 132 VIN 10 AIN / 55 VaIN |
- - - |
14.4% 36.4% 18.2% |
- - - |
1 AIN out of 3 CC but not included because of to small number of cases |
| 6. | Evans et al. (2003) [22] | 23 AC / 59,519 CIN 3 18 AC / 21,605 CC |
477,069 145,621 |
0.039% 0.083% |
4.82 12.36 |
|
| 7. | Gaudet et al. (2014) [23] | 20 AC / 54,320 CIN 2 and CIN 3 | 545,945 | 0.037% | 3.66 | |
| 8. | Hemminki et al. (2001) [24] | 16 AC / 17,234 CC | - | 0.093% | - | |
| 9. | Hemminki et al. (2000) [25] | 68 AC / 117,830 CIN 3 17 AC / 17,556 CC |
- | 0.058% 0.097% |
- | |
| 10. | Heráclio et al. (2018) [26] | 14 AIN / 200 CIN 1 23 AIN / 124 CIN 2 and 3 |
- | 7% 18.5% |
- | |
| 11. | Jakobsson et al. (2011) [27] | 3 AC / 26,876 CIN | 226,510 | 0.011% | 1.32 | |
| 12. | Jiménez et al. (2009) [28] | - | - | - | - | No information about the total number of CC, VC or VaC cases. |
| 13. | Kalliala et al. (2005) [29] | 3 AC / 7,564 CIN | 97,556 | 0.040% | 3.08 | |
| 14. | Matsuo et al. (2018) [30] | 49 AC / 79,050 CC | - | 0.062% | - | |
| 15. | Neumann et al. (2016) [31] | 3 AC / 4,234 CC 1 AC / 339 VC |
28,122 1,533 |
0.071% 0.295% |
10.67 65,23 |
|
| 16. | Pan et al. (2019) [32] | 37 AC / 69,714 CIN 3 | 893,622 | 0.053% | 4.14 | |
| 17. | Papatla et al. (2019) [33] | 17 AC / 21,060 CC | - | 0.081% | - | |
| 18. | Preti et al. (2020) [34] | 1 AC / 3,184 CIN 2 and 3 | 20,022 | 0.031% | 4.99 | |
| 19. | Rabkin et al. (1992) [35] | 12 AC / 25,295 CC | 156,838 | 0.047% | 7.65 | |
| 20. | Saleem et al. (2011) [36] | 137 AC / 124,075 CIN 3 28 AC / 43,669 CC 5 AC / 1,463 VaIN 3 2 AC / 3,257 VaC 55 AC / 6,792 VIN 3 28 AC / 9,950 VC |
- | 0.110% 0.064% 0.342% 0.061% 0.810% 0.281% |
- | |
| 21. | Sand et al. (2016) [37] | 32 AC / 52,135 CIN 2 125 AC / 104,155 CIN 3 |
597,467 1,529,564 |
0.061% 0.120% |
5.36 8.17 |
|
| 22. | Suk et al. (2018) [38] | 34 AC / 44,011 CC 31 AC / 6,905 VC 1 AC / 1,673 VaC |
473,820 48,373 9,057 |
0.077% 0.449% 0.060% |
7.18 64.09 11.04 |
|
| 23. | Tatti et al. (2012) [39] | 20 AIN / 114 CIN 2 and 3 35 AIN / 121 CIN 1 18 AIN / 39 VIN 7 AIN / 22 VaIN 2 and 3 27 AIN / 70 VaIN 1 |
- | 17.544% 28.926% 46.154% 31.818% 38.571% |
- | Results without dividing AIN into HSIL (AIN 2/3) and LSIL (AIN 1). |
| 24. | Tomassi et al. (2018) [40] | 1 AC / 1,168 CC 14 AC / 109,893 CIN 1 5 AC / 15,711 CIN 2 and 3 |
10,359 708,690 114,031 |
0.086% 0.013% 0.032% |
9.65 12.74 4.38 |
|
| 25. | Wang et al. (2020) [41] | 50 AC / 46,550 CC 9 AC / 7,855 VC 1 AC / 1,722 VaC |
- - - |
0.107% 0.115% 0.058% |
7.6 2.1 8.3 |
No information about PY. IR per 100,000 PY as provided by the authors of the publication. |
AC, anal cancer; AIN, anal intraepithelial neoplasia; CC, cervical cancer; VC, vulvar cancer; VaC, vaginal cancer; CIN, cervical intraepithelial neoplasia; VIN, vulvar intraepithelial neoplasia; VaIN, vaginal intraepithelial neoplasia.
Table 3.
Standardized incidence ratio (SIR), incidence rate (IR) and incidence rate per 100,000 person-years (IR per 100,000 PY) of anal cancer (AC) and anal intraepithelial neoplasia (AIN) among patients diagnosed and treated for gynecological HPV related diseases – a summary of literature review.
Table 3.
Standardized incidence ratio (SIR), incidence rate (IR) and incidence rate per 100,000 person-years (IR per 100,000 PY) of anal cancer (AC) and anal intraepithelial neoplasia (AIN) among patients diagnosed and treated for gynecological HPV related diseases – a summary of literature review.
| Type of HPV-related gynecological disease | Risk of AC mean SIR (range)1 | Risk of AC mean IR2 | Risk of AC mean IR per 100,000 PY3 | Risk of AIN mean SIR (range)1 | Risk of AIN mean IR2 | Risk of AIN mean IR per 100,000 PY3 |
|---|---|---|---|---|---|---|
| Cervical cancer | 3.6 (1.6-6.3) | 0.084% | 9.73 | |||
| Vulvar cancer | 10.8 (1.1-17.4) | 0.286% | 37.98 | |||
| Vaginal cancer | 1.6 (0.6-2.3) | 0.059% | 11.78 | |||
| CIN 3 | 5.6 (2.3-16.4) | 0.075% | 5.78 | 6.7 (3.64- 12.25) | 6.34 | |
| CIN(1-3) | 4.6 (0.9-16.4) | 0.030% | 5.37 | 16.45% | ||
| VIN 3 | 0.810% | |||||
| VIN(1-3) | 36.4% | |||||
| VaIN 3 | 0.342% | |||||
| VaIN(1-3) | 18.2% |
1 Note: SIR data based on all reviewed literature. If SIR = 1, it means that there is no difference between population of interest (here women with specific HPV-related gynecological disease) and general population. If SIR > 1, it means that there is higher risk of the disease in the population of interest than in the general population. 2 Note: IR data based on all reviewed literature. If IR= 0.084%, it means that out of 100,000 people with specific HPV-related gynecological disease 84 will develop anal cancer/ anal intraepithelial neoplasm. 3Note: IR per 100,000 PY data based on all reviewed literature. It is a rate of newly diagnosed cases of AC/AIN in a cohort per 100,000 person years of observation time.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



