
Submitted:
14 May 2023
Posted:
15 May 2023
You are already at the latest version
Abstract
In this review we look at the developments in the field of artificial intelligence (A.I) and their current impact as well as future implications in the field of cardiology, we as physicians and cardiologists have tried to put our perspective on the rapidly evolving field, In light of the fact that many of the healthcare workers and professionals across the world still find the concept of A.I quite complicated, elusive and somewhat paradoxical, we have tried to simplify the concept of artificial intelligence and make it easy for everyone to understand from all walks of life. The Databases utilized for our review are PubMed, PubMed Central, Google Scholar. The Keywords used for our Data Search are “Artificial Intelligence”, “A.I Cardiology”, “A.I in Cardiovascular Medicine”, “Machine Learning in Cardiology”. We screened all relevant since inception till March 25th and included 44 relevant articles after careful consideration into our paper. We have discussed the implementation of and scope of artificial intelligence across a broad spectrum of applications including cardiovascular imaging and diagnostics like electrocardiograms, echocardiograms, cardiac CT/MRIs to novel cardiac monitoring devices, CRISPR gene editing in cardiology and implementation of artificial intelligence in the field of Cardiovascular Bioprinting. This is the initial review in a series of reviews regarding A.I in Cardiology.
Keywords:
Artificial Intelligence
; A.I Cardiology
; A.I in Cardiovascular Medicine
; Machine Learning in Cardiology
Introduction & Background
The field of artificial intelligence (A.I) within medicine has witnessed a remarkable surge in publications. However, quantifying the clinical advantages of incorporating AI-assisted tools in patient care remained elusive until recently [1]. A.I, characterized by its capacity to discern meaningful patterns from data sets and make decisions based on these patterns, offers valuable support in clinical decision-making processes [2]. Machine learning (ML), an A.I subdomain, utilizes algorithms to empirically learn data patterns [3]. Unlike conventional statistics, ML algorithms detect non-linear relationships, high-order interactions among multiple variables, and more subtle patterns [3]. A.I, often perceived as human-like intelligence exhibited by a machine, encompasses systems based on ML, expert systems, and robotics. ML, in contrast, comprises a set of algorithms enabling a computer to learn a specific task through numerous examples.
Machine learning algorithms have their foundation in traditional statistics [4]. The most basic ML model can utilize logistic regression [4]. Nevertheless, more sophisticated methods, such as decision trees, support vector machines, random forests, or neural networks, provide the capability to handle intricate and non-linear relationships within data, circumventing improper dichotomization [5]. Recently developed techniques encompass deep neural networks, commonly referred to as deep learning. These algorithms facilitate rapid advancements in image recognition, natural language processing, speech recognition, and are extensively employed in cutting-edge medical research [6,7]. Deep learning (DL) has evolved, necessitating large datasets and recent enhancements in computational power to make efficient decisions on intricate data [3]. ML and DL have demonstrated success across diverse disciplines, including language processing, gaming, computer vision, engineering, industrial, and scientific fields, showcasing promise at multiple levels [3].
Neural networks, artificial computational models designed to mimic biological neural networks, hierarchically transmit data through nodes in each layer [8]. These networks have proven effective in pattern recognition tasks and can be implemented in various decision-making phases, delivering information, diagnoses, and even comprehensive clinical assessments based on medical history, clinical findings, laboratory results, and other relevant factors [9,10,11,12,13,14,15]. Diverse data types can serve as input; however, human observational data may introduce interobserver variability, potentially reducing accuracy, particularly when utilized outside the system's development setting [9]. Networks directly accepting data inputs, such as electrocardiographic signals, maintain higher accuracy since they provide the same precise data regardless of location [10,11,12,13]. Furthermore, Bio-signal data-based A.I tools are more prevalent than those based on clinical data [1].
The increasing availability of digital health data and recent advancements in A.I technology (particularly in machine learning and deep neural networks) have enabled the rapid and accurate processing and analysis of vast data volumes, paving the way for A.I applications in cardiology. Additionally, cardiology represents a research-intensive, rapidly advancing, and dynamic discipline, with cardiologists, regularly making high-risk, high-reward decisions, thereby suggesting that A.I will play a crucial role in cardiology's future. With this context in mind, this review aims to examine the literature reporting the latest developments and implications of A.I in cardiovascular medicine.
Review
Artificial intelligence: A brief overview
Prior to delving into the various applications of artificial intelligence in cardiovascular medicine, this paper aims to provide clarity on technical terms that may be unfamiliar to readers within the context of A.I.
A.I definition and subfields:
There are several types of learning models, each with its own strengths and weaknesses, and suited to different types of tasks and datasets. Figure 1.
EKG - Electrocardiogram
CAD - Coronary Artery Disease
EMR - Electronic Medical Record
Image Credits - Dr. Vijaya Durga Pradeep Ganipineni and Dr. Sai Dheeraj Gutlapalli
I) Supervised learning models:
These models are trained using labeled data, where the input data is paired with corresponding output or target values. Examples of supervised learning models include linear regression model, logistic regression, decision trees, random forests, support vector machines (SVMs), and artificial neural networks (ANNs) [16,17,18,19].
II) Unsupervised learning models:
These models are used when the data does not have any predefined labels or targets. The goal of these models is to identify patterns and relationships within the data. Examples of unsupervised learning models include clustering algorithms, such as K-means clustering, and dimensionality reduction techniques, such as principal component analysis (PCA) [16,17,18,19].
III) Semi-supervised learning models:
These models are used when only a small portion of the data is labeled. The goal is to use the labeled data to guide the learning of the model on the unlabeled data. Examples of semi-supervised learning models include generative models, such as variational autoencoders (VAEs), and self-training algorithms [16,17,18,19].
IV) Reinforcement learning models:
These models are used to train agents to make decisions based on a series of actions and rewards. The goal is to learn a policy that maximizes the cumulative reward over time. Examples of reinforcement learning models include Q-learning and deep reinforcement learning algorithms [16,17,18,19].
A model can be used to make predictions, classify data, or generate new data based on the patterns and relationships learned from a given dataset [20,21].
The goal of building a model is to create a generalizable representation of the underlying process or system that can be used to make predictions or decisions in real-world applications. The performance of a model is typically evaluated using metrics such as accuracy, precision, recall, and F1 score [22].
The parameters in a deep learning model determine the multiple weights and biases of the connections between the layers of the network, allowing it to learn complex features and patterns in the input data [22]. The use of large amounts of parametric data is a key feature of deep learning, as it enables the models to learn and generalize to new data [23,24].
Healthcare data:
The application of A.I in cardiovascular medicine has been fueled by the rapid growth and availability of healthcare data [5]. Electronic health records (EHRs) are a valuable source of information, providing structured and unstructured data on patients' demographics, medical histories, diagnoses, treatments, and outcomes [25]. The widespread adoption of EHRs has resulted in the generation of vast amounts of data that can be analyzed to improve patient care [26].
Imaging data plays a critical role in cardiovascular medicine, including modalities such as echocardiography, magnetic resonance imaging (MRI), and computed tomography (CT) scans [27]. These imaging techniques generate a plethora of data that can be used to identify disease patterns, monitor disease progression, and guide treatment decisions [28]. A.I algorithms, particularly deep learning methods, have demonstrated remarkable success in interpreting and analyzing medical imaging data, enabling more accurate and faster diagnosis of cardiovascular diseases [6].
Wearable devices and mobile health (mHealth) technologies have further expanded the available data for cardiovascular medicine [29]. These devices continuously monitor physiological parameters such as heart rate, blood pressure, and physical activity, generating large volumes of real-time data [30]. By incorporating this data into A.I algorithms, it is possible to create personalized treatment plans, predict disease progression, and improve patient outcomes [18].
Omics data, including genomics, transcriptomics, proteomics, and metabolomics, have also been increasingly integrated into cardiovascular medicine [31]. By leveraging A.I techniques to analyze these complex datasets, researchers have identified novel biomarkers, therapeutic targets, and insights into the underlying mechanisms of cardiovascular diseases [32].
Raw health data once selected for input undergoes signal preprocessing and feature engineering to transform it into a analyzable format that can be used to develop machine learning models for various healthcare applications, such as disease diagnosis, personalized treatment, and health monitoring [8]. Signal preprocessing involves filtering, noise removal, normalization, and other techniques to enhance the quality of the data, while feature engineering involves selecting and extracting relevant features or characteristics from the data to represent important aspects of the health condition or process being studied [8]. These steps are crucial for ensuring the accuracy and reliability of the results obtained from machine learning algorithms trained on health data Figure 2.
Despite the potential benefits of A.I in cardiovascular medicine, challenges remain in utilizing healthcare data effectively. Data privacy, security, and interoperability are key concerns that must to be addressed to ensure the safe and efficient use of healthcare data in A.I applications [33]. Additionally, the quality and representativeness of healthcare data are crucial for ensuring that A.I models are accurate and unbiased [34].
The assertion by John McCarthy who coined the term "artificial intelligence" that the quality of the input determines the effectiveness of A.I serves as a basis for an in-depth analysis of the crucial role played by robust data feeding and validation processes in the development of A.I systems and the associated limitations.
Methods of A.I application in cardiology:
Although the concept of A.I was first proposed in the 1950s, its application in the healthcare sector has only recently expanded. This expansion is due to A.I's ability to process a significant volume of data, making it useful for risk prediction, cardiovascular imaging, and electrophysiology in cardiology. In the near future, A.I is expected to have a tremendous impact on the diagnosis and management of cardiovascular diseases, leading to a paradigm shift. However, it is crucial to note that as powerful as A.I techniques can be, they must be motivated by clinical problems and applied to assist clinical practice ultimately [17,19,35].
I) Clinical Practice:
Artificial intelligence algorithms are being employed to improve the accuracy and efficiency of cardiovascular disease diagnosis and treatment selection. Machine learning models are utilized to analyze medical data such as ECGs, echocardiograms, and medical imaging for early diagnosis and risk stratification [5]. By incorporating patient-specific data, including medical history, genetic information, and lifestyle factors, AI can assist clinicians in tailoring treatment strategies to optimize patient response and minimize adverse effects [5].
II) Research and Development:
AI-powered drug discovery is being used to accelerate the identification and development of novel therapeutic agents for cardiovascular diseases. Machine learning algorithms analyze large datasets of molecular structures, biological targets, and drug interactions to identify potential drug candidates more efficiently than traditional methods [14]. Precision disease stratification enables healthcare professionals to identify patient-specific risk factors, understand disease progression, and predict response to therapy [5]. A.I has the potential to integrate multi-omic data, including genomics, transcriptomics, proteomics, and metabolomics, to provide a comprehensive understanding of disease mechanisms and identify potential therapeutic targets [5].
III) Population Health:
A.I can assist healthcare providers and policymakers in allocating resources more effectively by identifying areas of greatest need and predicting the demand for healthcare services. AI-driven tools can augment physician decision-making by providing real-time clinical decision support and reducing the cognitive load on healthcare professionals. AI-powered remote monitoring technologies, such as wearable devices and telemedicine platforms, can enable continuous patient monitoring outside of the clinical setting, facilitating early detection of cardiovascular events and empowering patients to take a more proactive role in managing their health [5].
Challenges and limitations of A.I in cardiology:
Despite the many benefits of A.I in cardiology, limitations exist. One significant concern revolves around the "black box" problem where A.I systems mechanisms and processes are not readily understood by observers or users [3,8,21]. This issue restricts the technology's usefulness in research and innovation since understanding how models generate their outcomes is challenging and critical in refining or improving them.
Explainability, Uncertainty, Robustness in A.I:
Explainability, also known as interpretability, is a crucial aspect of artificial intelligence applications in cardiovascular medicine. As A.I models become more complex, it becomes increasingly challenging to understand the rationale behind their predictions and decisions [36]. Explainable A.I (XAI) aims to provide insights into the inner workings of A.I models, facilitating the understanding of the relationships between input features and output predictions [37]. This is particularly important in healthcare, where clinicians must trust the A.I models' recommendations to make informed treatment decisions. Incorporating XAI techniques, such as LIME (Local Interpretable Model-agnostic Explanations) and SHAP (SHapley Additive exPlanations), helps to bridge the gap between model predictions and clinical decision-making, ensuring transparency and fostering trust in AI solutions [38].
Uncertainty quantification is another critical aspect of A.I applications in cardiovascular medicine. Inherent uncertainty in healthcare data and the stochastic nature of A.I models can lead to predictions with varying degrees of confidence [39]. Estimating and conveying this uncertainty is essential for clinicians to gauge the reliability of A.I model predictions and make informed decisions [40]. Bayesian methods, such as Monte Carlo Dropout and Bayesian Neural Networks, provide a principled way to estimate uncertainty in A.I models, allowing clinicians to better understand the limitations of A.I-based predictions and avoid overreliance on potentially erroneous recommendations [41].
Robustness is the ability of A.I models to maintain their performance in the face of perturbations, such as noisy data, missing values, or adversarial attacks [42]. In the context of cardiovascular medicine, A.I models must be robust to variations in data quality, acquisition protocols, and patient populations to ensure accurate and reliable predictions across diverse clinical settings [43]. Techniques such as data augmentation, transfer learning, and adversarial training help improve the robustness of A.I models, making them more resilient to changes in input data and potential attacks [44]. Ensuring robustness in A.I applications is crucial to maintain patient safety and enable the widespread adoption of A.I solutions in cardiovascular medicine.
In decision-making areas within cardiology, such as the diagnosis and treatment of patients, A.I can assist physicians in making more informed choices. However, legal, and ethical challenges emerge when A.I is used to make decisions that affect patients lives. In such cases, the workings of A.I systems must be fully transparent and accountable individuals can assess these systems fairness and accuracy. Another limitation to A.I in cardiology is the interpretability of complex models. Although such models can predict patient outcomes effectively, they can be difficult to explain to physicians or patients. This interpretability concern may hinder the commitment to and acceptance of A.I in cardiology. Furthermore, A.I's reliance on large data sets can also serve as hurdles in smaller, resource-limited clinical settings. A.I models that necessitate extensive amounts of data to produce accurate predictions would be insignificant in such settings.
Addressing these limitations will prove critical in fully realizing the potential of A.I in cardiology. Researchers and technicians concerted effort in promoting transparency, explainability, and interpretability of A.I algorithms can help advance the understanding of how A.I systems work and allow for more accurate predictions and better patient care.
Future directions of A.I in cardiology:
The future implications of A.I in cardiology are vast and promising. One of the most significant benefits is the potential to accelerate cardiovascular research. With the ability to process extremely large amounts of data much more quickly than humans can, A.I can analyze patient and population data to identify new patterns in medication and drug interactions. This process could lead to the development of more effective treatments and drug therapies. A.I also has implications for CRISPR models, where it can facilitate the prediction of gene targeting and increase the accuracy of gene editing. Bioprinting, another emerging field in cardiology, could be made even more precise with the use of A.I. By integrating biomechanics with A.I, we could produce custom-made, semisynthetic heart valves that mimic the function of natural valves more closely.
Athletes could benefit from A.I-based cardiac bio-enhancement technology, which would help detect and track cardiac function changes and optimize training programs. A.I technology can help predict stent longevity, and improve the placement and deployment of these devices. In addition, A.I could be used to develop nanoparticle-mediated thrombolysis and removal of plaques in a targeted and efficient manner. Another important development would be identifying novel biomarkers that can help with the very early detection and diagnosis of cardiovascular disease. Finally, in the future, robotic PCI could become more advanced with the use of A.I, making cardiac surgery safer and more precise.
The potential for using A.I in cardiac electrophysiology is still being studied. Further research is needed to explore how A.I can be used to investigate genomic and proteomic data, histological characterization, and drug discovery for treating arrhythmia.One significant advantage of A.I is that it can combine different types of patient data to develop more accurate diagnoses. Currently, most A.I research uses data independently collected from institutions, which makes it difficult to combine data across different centers. Collecting, labeling, and standardizing clinical data and outcomes would make it easier to generate more reliable and meaningful results. Making harmonized data accessible in public repositories, such as the EKG databases available from PhysioNet, would make it easier to develop AI for cardiac electrophysiology. However, there is still a significant need to increase accessibility to various other types of essential data [3].The next challenge is developing a framework for incorporating A.I into clinical practice while considering patient safety, privacy, data transfer, and access. Clinical and technical experts must partner to validate prospective clinical studies to ensure the reliability and benefit of A.I. Additionally, commercial establishment, FDA approval, and reimbursement mechanisms must be addressed when implementing A.I into clinical practice [3]. Overall, the future looks very bright for A.I in cardiology, and its potential applications could have a significant impact on the clinical diagnosis, treatment, and prevention of cardiovascular disease.
Conclusions
Recent advancements in A.I have shown significant potential for improving cardiology by enhancing diagnostics, predictions, and evaluations of various cardiac diseases and conditions. The integration of A.I in medical imaging and the use of machine learning algorithms have demonstrated a marked increase in accuracy and efficiency. However, several challenges and limitations must be addressed to fully realize the potential of A.I in cardiology. These include the "black box" problem, explainability, uncertainty, robustness, legal and ethical issues, and data accessibility. Future directions of AI in cardiology encompass accelerating cardiovascular research, developing more effective treatments and drug therapies, and advancing CRISPR models, bioprinting, and robotic PCI. A.I can also benefit athletes through cardiac bio-enhancement technology, improve stent longevity, and enable targeted nanoparticle-mediated thrombolysis. Additionally, A.I can facilitate the identification of novel biomarkers and enhance the precision of cardiac interventions. The ongoing exploration of A.I's applications in cardiac electrophysiology calls for further research and access to harmonized data in public repositories. Developing a framework that incorporates A.I into clinical practice while addressing patient safety, privacy, data transfer, and access is a critical next step. Collaboration between clinical and technical experts, commercial establishment, FDA approval, and reimbursement mechanisms will be essential in implementing A.I in cardiology. Ultimately, A.I holds immense promise for revolutionizing the diagnosis, treatment, and prevention of cardiovascular disease, paving the way for a brighter future in cardiology.
Author Contributions
1st Author - GV, 2nd Author - GSD, 3rd Author - PJ, 4th Author - OI, 5th Author - UD, 6th Author - FM, 7th Author - FD, 8th Author - KT, 9th Author - PG, 10th Author - IASK, 11th Author - AZ, 12th Author - AM, 13th Author - GS, 14th Author - NJ, 15th Author – RF. Concept, design and writing of the abstract was done by FD & OI and reviewed by GSD, GV, GS, RF & NJ. The Concept of the study and the overall structure and framework of the paper was concieved by GSD, GS, GV, NJ and discussed with and approved by AM, AZ, IASK, FD, OI, PJ, KT, & UD. The General discussion was structured and written by PJ,KT,AZ & AM and was edited and finalized by GSD, GS, GV & NJ. The Conclusion was written by PG & UD. The conclusion was screened by all of the authors as well chiefly GSD, GS, GV, NJ and final approval was based on unanimous consensus. Images and Figures - GSD, GV and Edited by FM, DS, OI, PJ, KT, UD, AM, IASK. Each of the authors has made substantial contributions to the concept, design, analysis and worked with the data. They have drafted and revised the article and put in their own intellectual inputs, each of them have approved the final form of the manuscript for Publication
Funding
Not Applicable.
Institutional Review Board Statement
Not Applicable.
Informed Consent Statement
Not Applicable.
Data Availability Statement
All of the Data is publicly available and can be gathered from PubMed and Google Scholar.
Acknowledgments
None
Conflicts of Interest
The authors declare no conflict of interest.
References
- Lam TYT, Cheung MFK, Munro YL, Lim KM, Shung D, Sung JJY: Randomized controlled trials of artificial intelligence in clinical practice: systematic review. J Med Internet Res. 2022, 24:37188. [CrossRef]
- Bonderman D: Artificial intelligence in cardiology. Wien Klin Wochenschr. 2017, 129:866-868. [CrossRef]
- Feeny AK, Chung MK, Madabhushi A, et al.: Artificial intelligence and machine learning in arrhythmias and cardiac electrophysiology. Circ Arrhythm Electrophysiol. 2020, 13:007952. [CrossRef]
- Pieszko K, Hiczkiewicz J, Budzianowski J, et al.: Clinical applications of artificial intelligence in cardiology on the verge of the decade. Cardiol J. 2021, 28:460-472. [CrossRef]
- Johnson KW, Torres Soto J, Glicksberg BS, et al.: Artificial intelligence in cardiology. J Am Coll Cardiol. 2018, 71:2668-2679. [CrossRef]
- Rajkomar A, Dean J, Kohane I: Machine learning in medicine.. N Engl J Med. 2019, 380:1347-1358. [CrossRef]
- Litjens G, Ciompi F, Wolterink JM, et al.: State-of-the-art deep learning in cardiovascular image analysis. JACC Cardiovasc Imaging. 2019, 12:1549-1565. [CrossRef]
- Nagarajan VD, Lee SL, Robertus JL, Nienaber CA, Trayanova NA, Ernst S: Artificial intelligence in the diagnosis and management of arrhythmias. Eur Heart J. 2021, 42:3904-3916. [CrossRef]
- Hedén B, Edenbrandt L, Haisty WK, Pahlm O: Artificial neural networks for the electrocardiographic diagnosis of healed myocardial infarction. Am J Cardiol. 1994, 74:5-8. 1. [CrossRef]
- Dassen WR m., Mulleneers RG a., Dulk KD, et al.: An artificial neural network to localize atrioventricular accessory pathways in patients suffering from the wolff-parkinson-white syndrome. Pacing Clin Electrophysiol. 1990, 13:1792-1796. [CrossRef]
- Bortolan G, Degani R, Willems JL: Neural networks for ECG classification . Proceedings Computers in Cardiology. . 1990, 269-272. [CrossRef]
- L E, B D, Pw M: Neural networks for classification of ECG ST-T segments. J Electrocardiol. 1992, 25:. [CrossRef]
- Edenbrandt L, Devine B, Macfarlane PW: Classification of electrocardiographic ST-T segments--human expert vs artificial neural network. Eur Heart J. 1993, 14:464-468. [CrossRef]
- Baxt WG: Use of an artificial neural network for the diagnosis of myocardial infarction. Ann Intern Med. 1991, 115:843-848. [CrossRef]
- Asada N, Doi K, MacMahon H, et al.: Potential usefulness of an artificial neural network for differential diagnosis of interstitial lung diseases: pilot study. Radiology. 1990, 177:857-860. [CrossRef]
- Watson X, D’Souza J, Cooper D, Markham R: Artificial intelligence in cardiology: fundamentals and applications. Intern Med J. 2022, 52:912-920. [CrossRef]
- Lopez-Jimenez F, Attia Z, Arruda-Olson AM, et al.: Artificial Intelligence in cardiology: present and future. Mayo Clin Proc. 2020, 95:1015-1039. [CrossRef]
- Krittanawong C, Johnson KW, Rosenson RS, et al.: Deep learning for cardiovascular medicine: a practical primer. Eur Heart J. 2019, 40:2058-2073. [CrossRef]
- Jiang F, Jiang Y, Zhi H, et al.: Artificial intelligence in healthcare: past, present and future. Stroke Vasc Neurol. 2017, 2:230-243. [CrossRef]
- Miller RJH, Huang C, Liang JX, Slomka PJ: Artificial intelligence for disease diagnosis and risk prediction in nuclear cardiology. J Nucl Cardiol Off Publ Am Soc Nucl Cardiol. 2022, 29:1754-1762. [CrossRef]
- Itchhaporia D: Artificial intelligence in cardiology. Trends Cardiovasc Med. 2022, 32:34-41. [CrossRef]
- Attia ZI, Harmon DM, Behr ER, Friedman PA: Application of artificial intelligence to the electrocardiogram. Eur Heart J. 2021, 42:4717-4730. [CrossRef]
- Dorado-Díaz PI, Sampedro-Gómez J, Vicente-Palacios V, Sánchez PL: Applications of artificial intelligence in cardiology. The future is already here. Rev Espanola Cardiol Engl Ed. 2019, 72:1065-1075. [CrossRef]
- Sanders WE, Khedraki R, Rabbat M, et al.: Machine learning algorithms. JACC Adv. 2023, 2:100166. [CrossRef]
- Adler-Milstein J, Jha AK: HITECH act drove large gains in hospital electronic health record adoption. Health Aff (Millwood). 2017, 36:1416-1422. [CrossRef]
- Raghupathi W, Raghupathi V: Big data analytics in healthcare: promise and potential. Health Inf Sci Syst. 2014, 2:3. [CrossRef]
- Panayides AS, Amini A, Filipovic ND, et al.: AI in medical imaging informatics: current challenges and future directions. IEEE J Biomed Health Inform. 2020, 24:1837-1857. [CrossRef]
- Narula S, Shameer K, Salem Omar AM, Dudley JT, Sengupta PP: Machine-learning algorithms to automate morphological and functional assessments in 2D echocardiography. J Am Coll Cardiol. 2016, 68:2287-2295. [CrossRef]
- Walsh JA, Topol EJ, Steinhubl SR: Novel wireless devices for cardiac monitoring. Circulation. 2014, 130:573-581. [CrossRef]
- Piwek L, Ellis DA, Andrews S, Joinson A: The rise of consumer health wearables: promises and barriers. PLoS Med. 2016, 13:e1001953. [CrossRef]
- Shah SH, Arnett D, Houser SR, et al.: Opportunities for the cardiovascular community in the precision medicine initiative. Circulation. 2016, 133:226-231. [CrossRef]
- Tolani P, Gupta S, Yadav K, Aggarwal S, Yadav AK: Big data, integrative omics and network biology. Adv Protein Chem Struct Biol. 2021, 127:127-160. [CrossRef]
- Yue X, Wang H, Jin D, Li M, Jiang W: Healthcare data gateways: found healthcare intelligence on blockchain with novel privacy risk control. . J Med Syst. 2016, 40:218. [CrossRef]
- Gianfrancesco MA, Tamang S, Yazdany J, Schmajuk G: Potential biases in machine learning algorithms using electronic health record data. JAMA Intern Med. 2018, 178:1544-1547. [CrossRef]
- Gupta MD, Kunal S, Girish MP, Gupta A, Yadav R: Artificial intelligence in cardiology: The past, present and future. Indian Heart J. 2022, 74:265-269. [CrossRef]
- Adadi A, Berrada M: Peeking inside the black-box: A survey on explainable artificial intelligence (XAI). IEEE Access. 2018, 6:52138-52160. [CrossRef]
- Goebel R, Chander A, Holzinger K, et al.: Explainable AI: the new 42? In: machine learning and knowledge extraction: second IFIP TC 5, TC 8/WG 8.4, 8.9, TC 12/WG 12.9. International Cross-Domain Conference, CD-MAKE. 2018273020182018, 295-303. [CrossRef]
- Lundberg SM, Lee SI: A unified approach to interpreting model predictions. ArXiv. 2017, May:.
- Gal Y, Ghahramani Z: Dropout as a bayesian approximation: representing model uncertainty in deep learning. Proceedings of The 33rd International Conference on Machine Learning. PMLR. 2016, 1050-1059.
- Cai X, Perez-Concha O, Coiera E, et al.: Real-time prediction of mortality, readmission, and length of stay using electronic health record data. J Am Med Inform Assoc JAMIA. 2016, 23:553-561. [CrossRef]
- Blundell C, Cornebise J, Kavukcuoglu K, Wierstra D: Weight uncertainty in neural networks. arXiv. 2015, May:. [CrossRef]
- Goodfellow IJ, Shlens J, Szegedy C: Explaining and harnessing adversarial examples. arXiv. 2015, March:. [CrossRef]
- Shorten C, Khoshgoftaar TM: A survey on image data augmentation for deep learning.. J Big Data. 2019, 6:60. [CrossRef]
- Weimann K, Conrad TOF: Transfer learning for ECG classification. Sci Rep. 2021, 11:5251. [CrossRef]
Figure 1.
Outline of the training process of an A.I system.
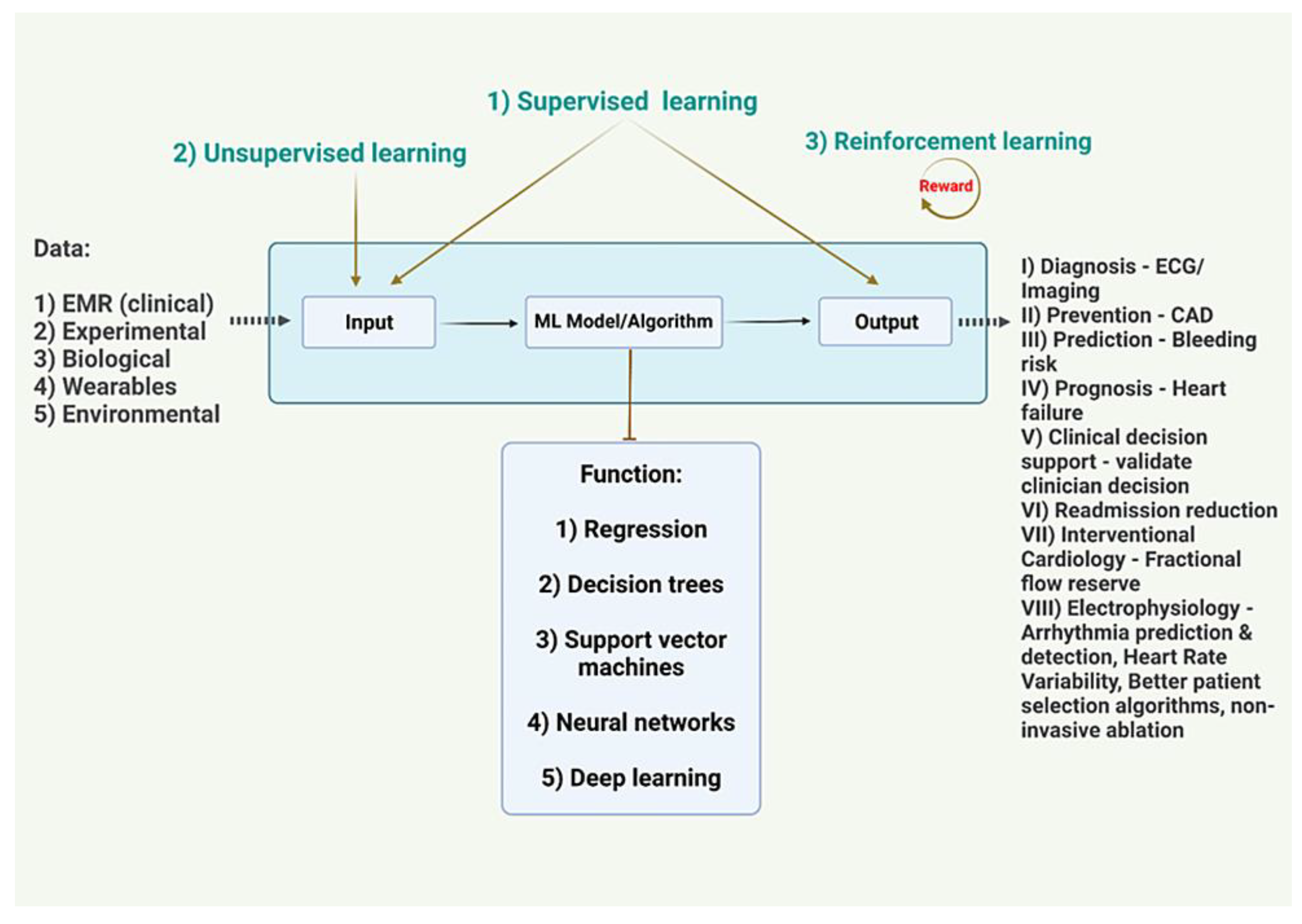
Figure 2.
Summary of data processing before feeding it to the A.I. Image Credits: Dr. Vijaya Durga Pradeep Ganipineni and Dr. Sai Dheeraj Gutlapalli.
Figure 2.
Summary of data processing before feeding it to the A.I. Image Credits: Dr. Vijaya Durga Pradeep Ganipineni and Dr. Sai Dheeraj Gutlapalli.
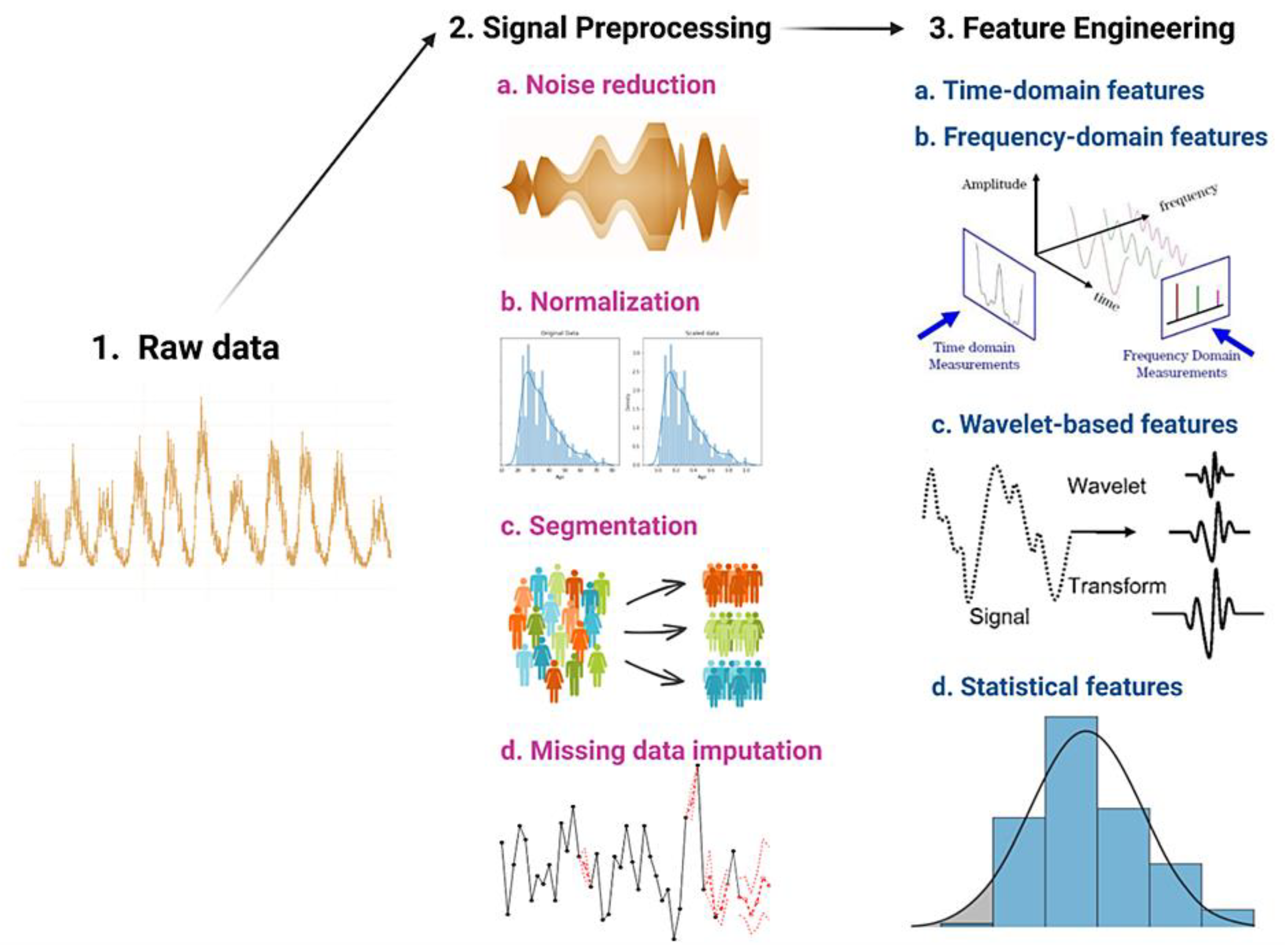

Table 1.
Fundamentals of A.I: An Elaboration of Basic Terminology.
| Input data: Input refers to the data that is fed into a model or an algorithm in order to obtain a specific output. Input data can come in many forms, such as text, images, audio, or numerical data, and can be either raw data or pre-processed data. Output basically refers to the result or the prediction that is generated by the model or the algorithm based on the input data [1,2,3,4,5,6,7,8,9,10]. |
| Output data/labels/target: The output can also take many different forms, depending on the type of problem being solved. For example, in a classification task, the output might be a label that indicates the class or category to which a particular input belongs. In a regression task, the output might be a numerical value that predicts a specific quantity or value [1,2,3,4,5,6,7,8,9,10]. |
| Dataset: consists of input-output pairs, also known as training data on which a model is trained on [1,2,3,4,5,6,7,8,9,10]. |
| Parameter: a variable used in the mathematical functions of a model [1,2,3,4,5,6,7,8,9,10]. |
| Function: defined by a set of parameters to generate a simple mathematical function. The function created by the model defines how the input is transformed to generate the output, and the model's parameters are the variables that are adjusted during the training process to optimize the accuracy of the function [1,2,3,4,5,6,7,8,9,10]. |
| Model/Algorithm: model is a set of functions to perform an operation. A simple model can perform a single/few tasks. If a model is trained using large amounts of parametric data, it’s called deep learning which is very versatile in performing tasks. It typically consists of a set of interconnected nodes or layers that perform mathematical operations on the input data to produce an output. The specific architecture of the model and the parameters used in the operations are determined during the training process, where the model learns to minimize the difference between the output predicted and the actual output [1,2,3,4,5,6,7,8,9,10]. |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



