Submitted:
15 May 2023
Posted:
16 May 2023
You are already at the latest version
Abstract
Neck lymphangiomas are rare, benign congenital malformations that predominate in childhood. Most present before the age of two. There are no risk factors related to sex, ethnic origin or predominance on either side, and they can occur in any anatomical location, although the most frequent is in the head and neck. The clinical presentation depends on its location. The most frequent symptom is the existence of a painless mass that grows slowly. Available therapeutic tools include surgery, systemic treatment, and injection of sclerosing agents.
Keywords:
lymphangioma
; lymphatic malformation
; cervical mass.
1. Introduction
Neck lymphangiomas are rare, benign congenital malformations that predominate in childhood. 90% occur in children under 2 years, with an incidence of 1.2 to 2.8 per 100,000 newborns. Its presentation in adults is rare [1]. Approximately 60% are present at birth, and up to 90% are detectable by two years of age [2,3].
Approximately 47% of pediatric MVLs are found in the group of children under three years of age. Then its incidence decreases, until it is close to 3% after 16 years [4].
Although more than 90% of lymphatic malformations are clearly congenital, they may occur later as a result of trauma, infection, neoplasia or iatrogenic injury. The pathophysiology of lymphangiomas in adults is not clearly understood, but these lesions may be secondary to the induction of dormant remnants of embryonic lymphatic tissue that are stimulated to differentiate and grow [5,6]
There are no risk factors related to sex, ethnic origin or predominate on either side, but they have been associated with chromosomal abnormalities such as Turner syndrome, various trisomies and Klinefelter, Noonan and Fryns syndromes [7]
They can occur in any anatomical location. However, the most frequent location is in the neck and head. In a series of 145 patients with childhood MVL, 36.5% were located in the head and neck.
The most common location is in the posterior triangle of the neck (75% of cases) [8], after the sternocleidomastoid; 20% in the submandibular triangle, and 5% can occur in the abdomen, retroperitoneum, mediastinum, and even in multiple locations (axilla, shoulder, chest wall, abdominal wall, parotid gland, lip, floor of the mouth, tongue, tonsils, region behind the ear) [5,9,10,11].
2. Case Presentation
We present the case of a 26-year-old woman who came to the emergency room for several days presenting pain in the right laterocervical/supraclavicular region, without observing lesions at that level. She relates it to the sleeping position. In the following days there is some swelling and volume increase at that level. The pain disappeared at rest and increased when the right shoulder was mobilized. She mentioned that a week and a half earlier she had overexerted himself with his right arm playing paddle tennis, noticing slight pain in the right trapezius region in the days that followed. On examination, there was volume increase in the right supraclavicular region, with no inflammatory signs.
An ultrasound was performed, and revealed several images of a small cystic anechoic appearance, subcentimeters, with a predominantly rounded morphology and some with a tubular morphology without flow in the Doppler study, collapsing under pressure. It was associated with other vascular structures with small flow and in low number, and alteration of the echogenicity of the adjacent fat, diffuse, not defined.
The CT showed several small subcentimeter-sized nodular formations without enhancement with increased attenuation and trabeculation of adjacent fat and some small, sparse, serpingine vascular structures. The study is completed with an MRI, and the most probable diagnostic is mixed type lymphatic cystic malformation (2018 ISSVA), preferably with microcysts and some larger cystic region, with very slow flow, without nidus components, vascular disease, aneurysms or pathological veins. Thrombotic pathology was not appreciated in the nearby great vessels. The lesion seemed to extend to the left, contralateral side. On the right side, it showed changes with an inflammatory or possibly hemorrhagic appearance that justified the prominent signal difference in long TR sequences, with fat saturation, and in the late evaluation with VSD.
Figure 1.
Coronal T1 MRI with intravenous contrast, 3D, equilibrium phase.
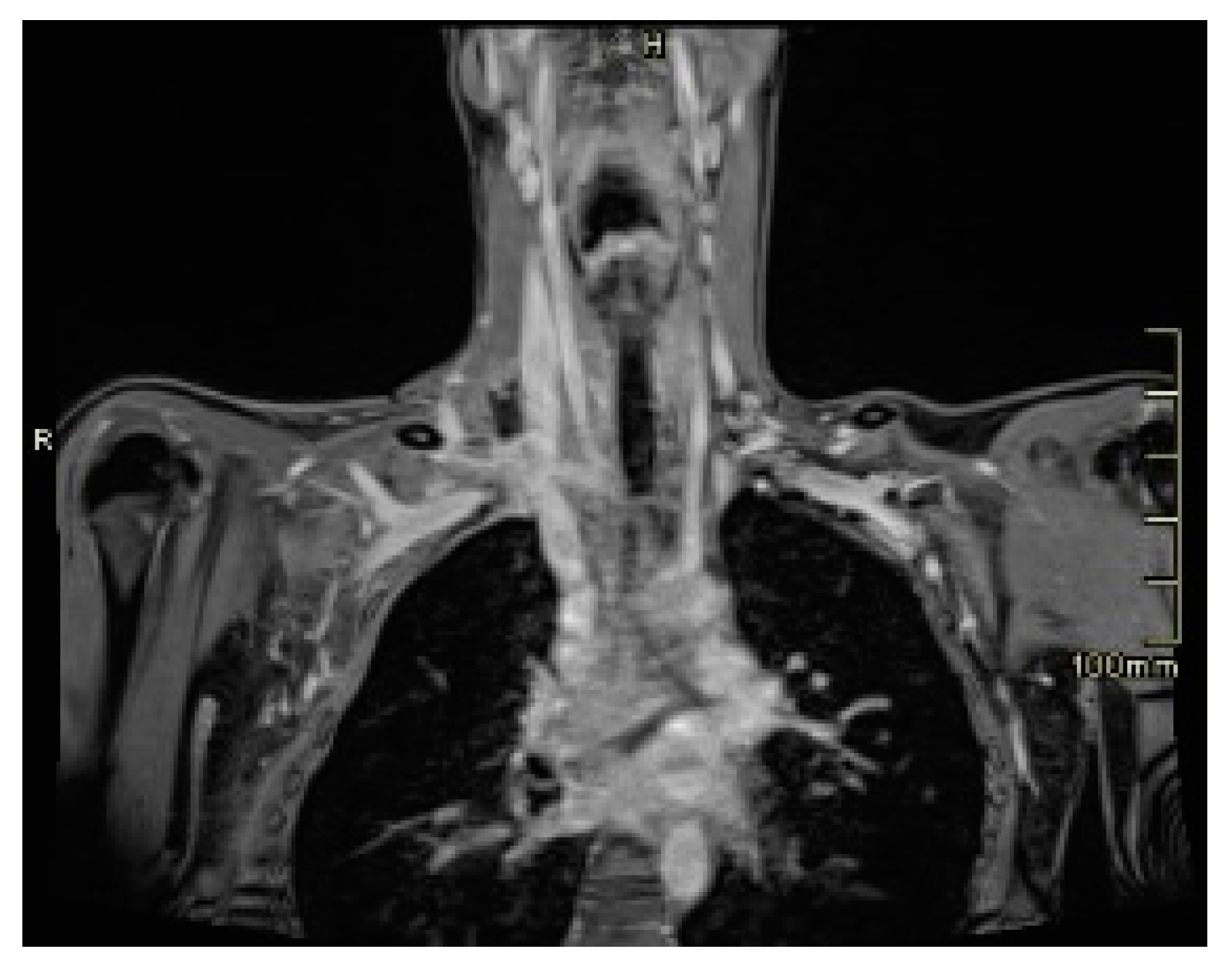
Figure 2.
4D angiographic study (temporal resolution, vascular dynamic study, early phase).
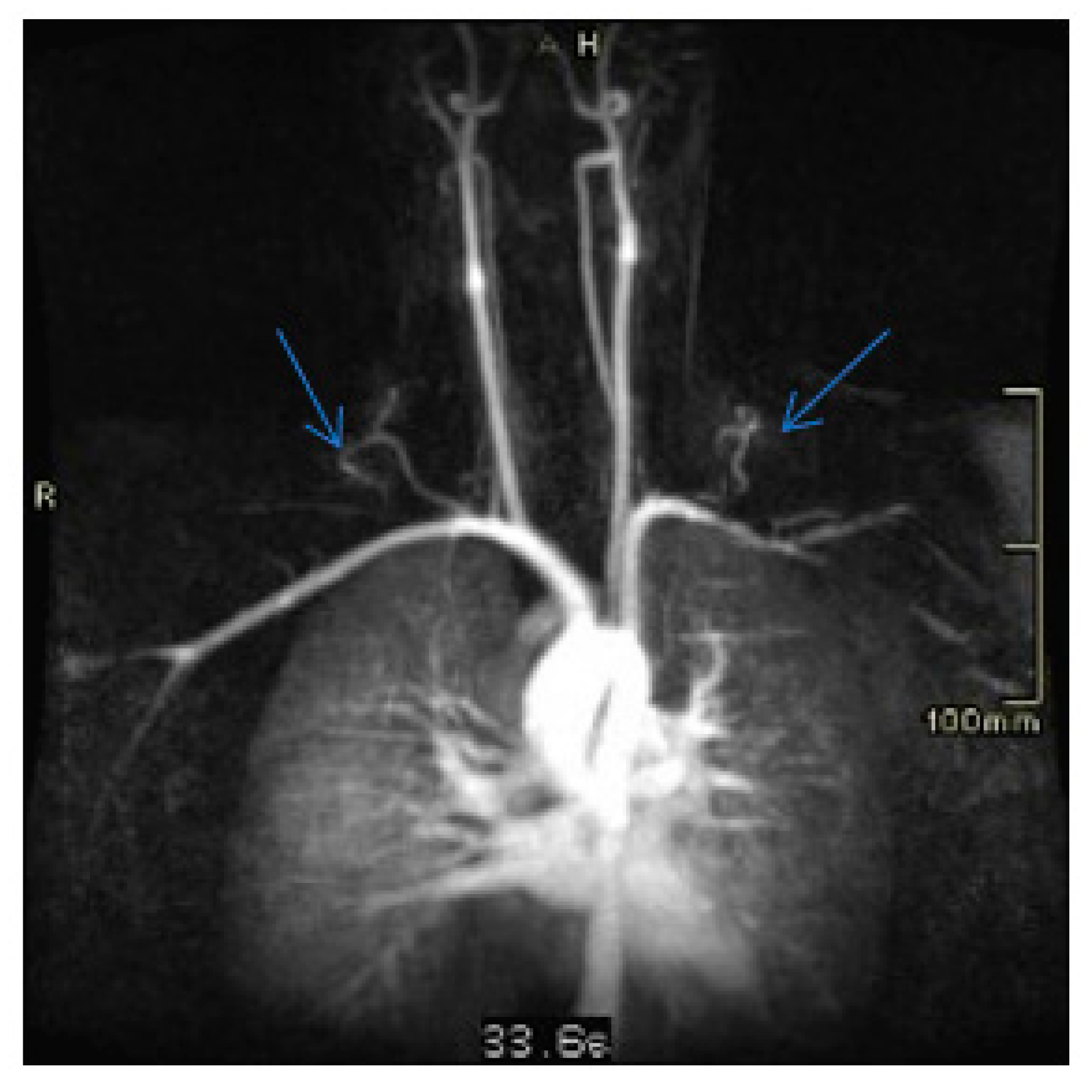
Figure 3.
4D angiographic study (temporal resolution, vascular dynamic study, intermediate phase).
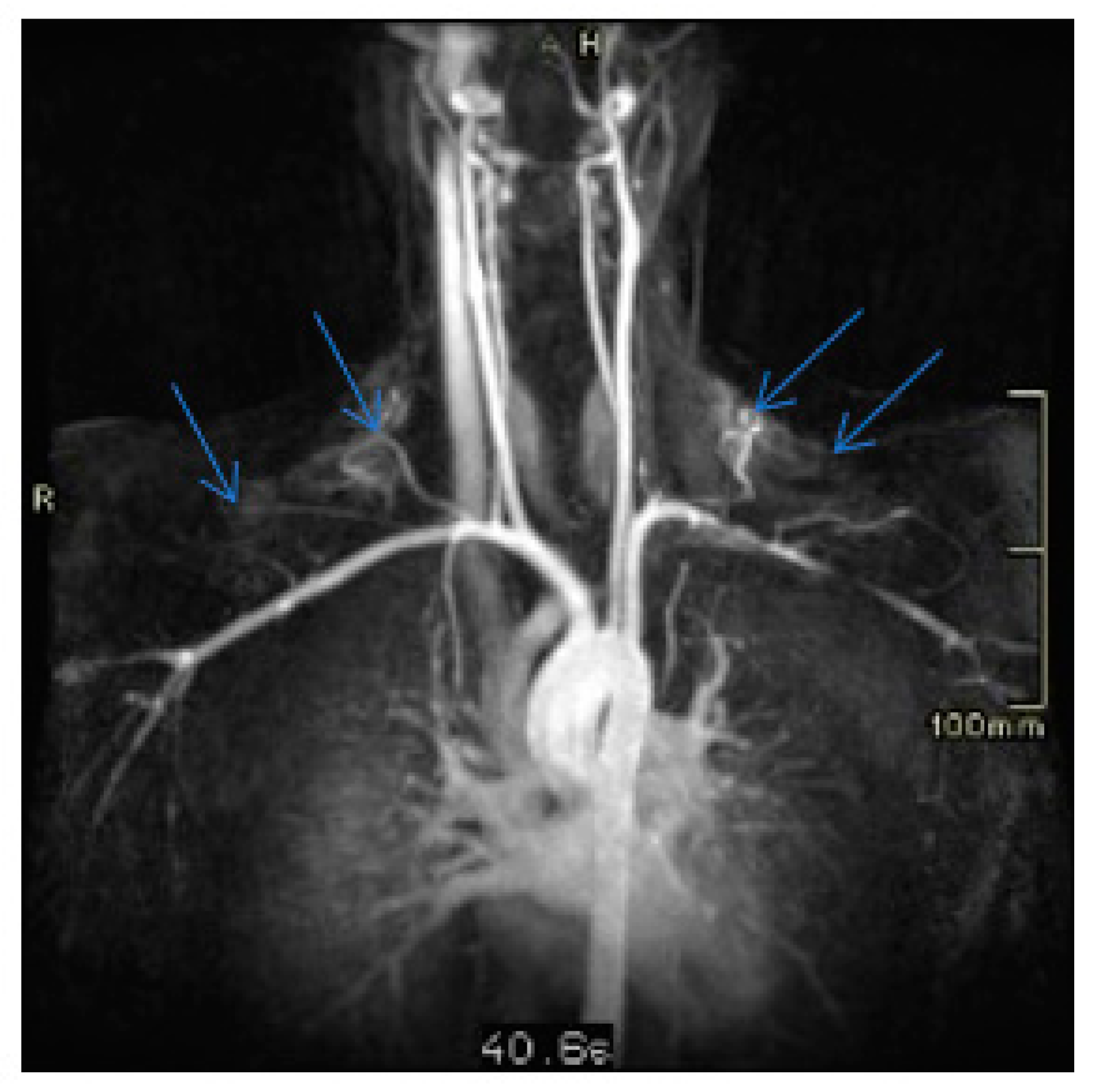
Figure 4.
4D angiographic study (temporal resolution, vascular dynamic study, venous phase).
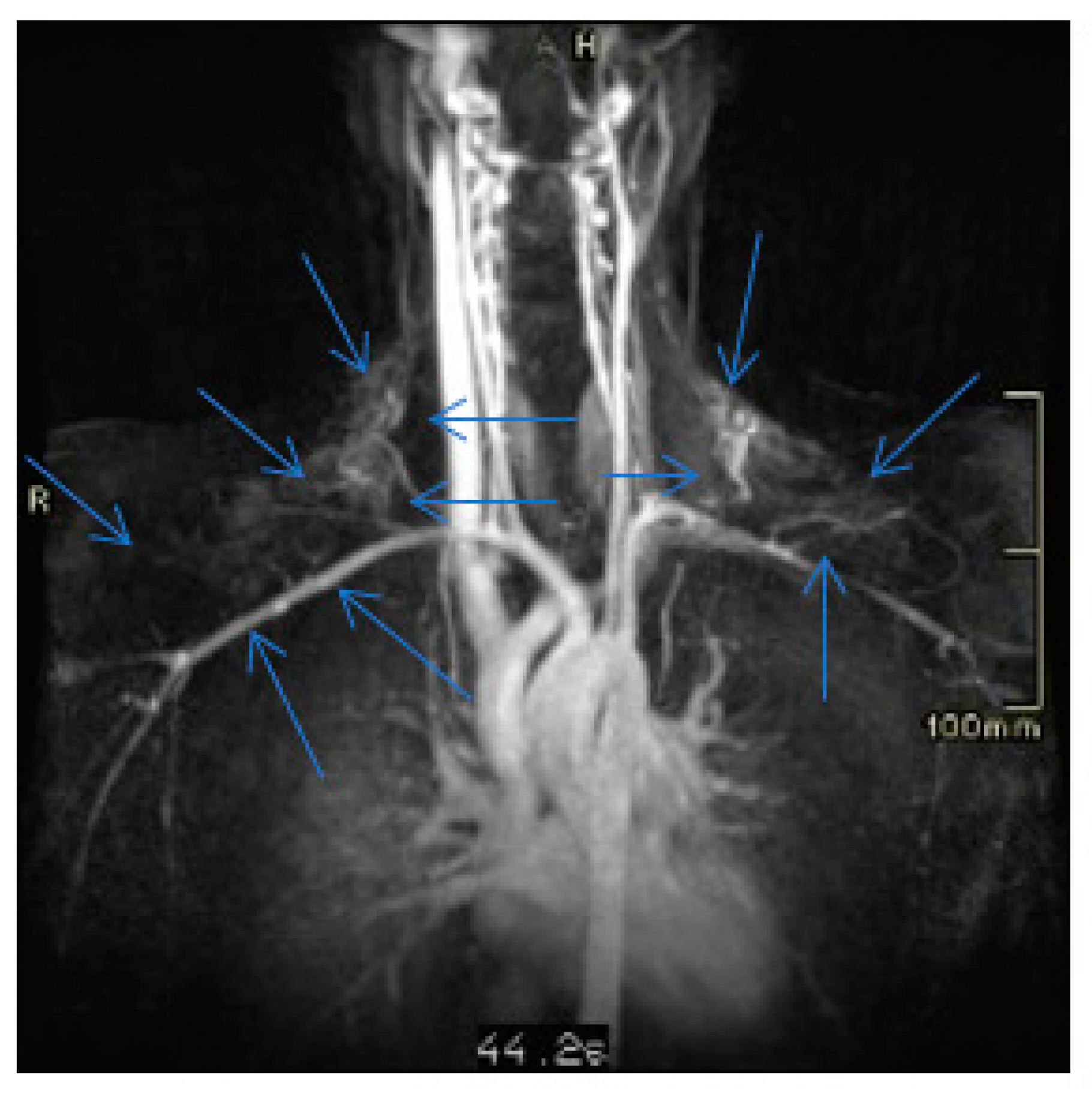
Figure 5.
Coronal MRI T2, 3D. We mark the fatty space of the thoracic outlet, where the epicenter of the lesion is located.
Figure 5.
Coronal MRI T2, 3D. We mark the fatty space of the thoracic outlet, where the epicenter of the lesion is located.
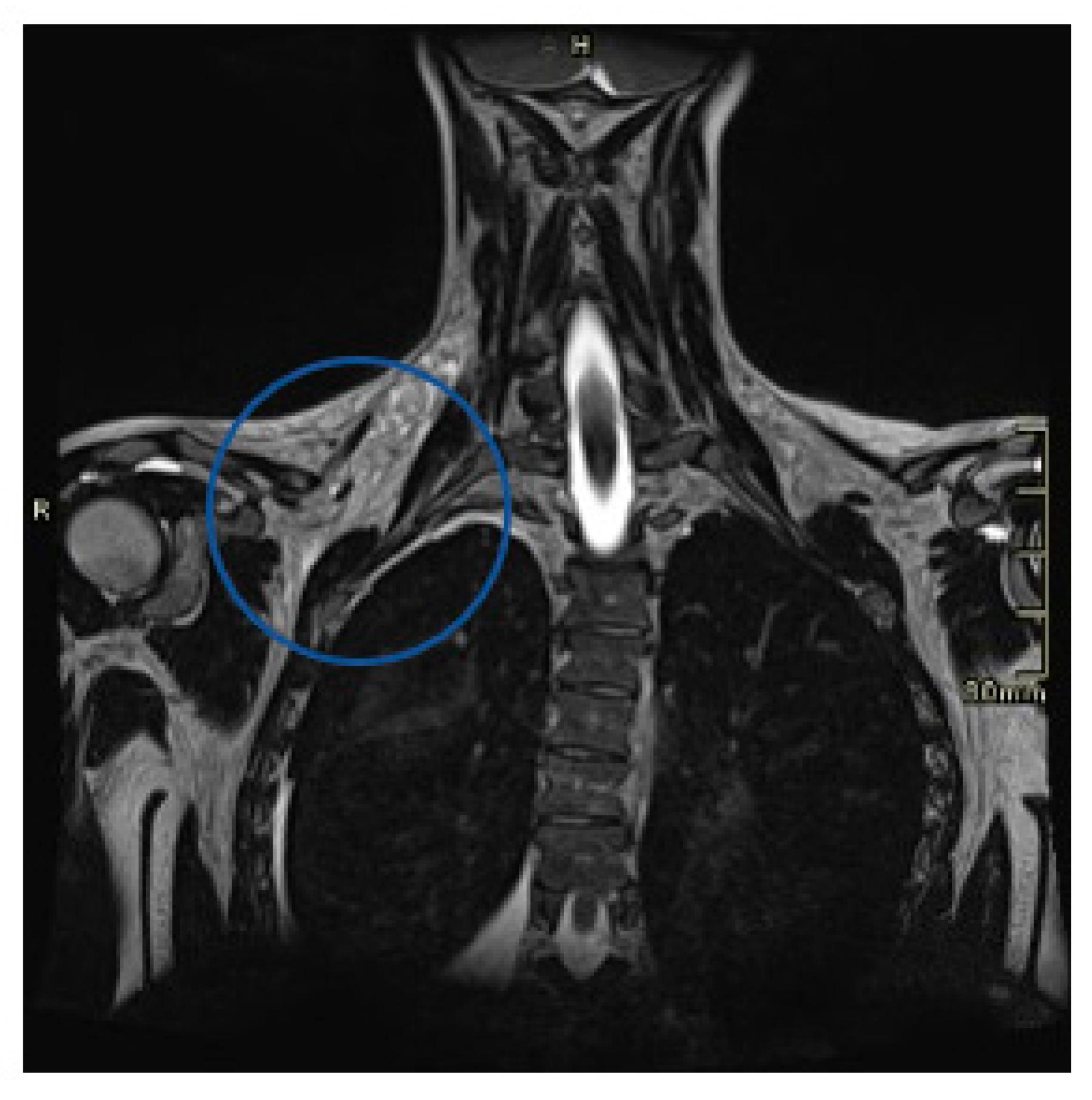
Figure 6.
Same image as in Figure 5, in a more posterior position (the aproximate limits of the lesion are marked with blue lines).
Figure 6.
Same image as in Figure 5, in a more posterior position (the aproximate limits of the lesion are marked with blue lines).
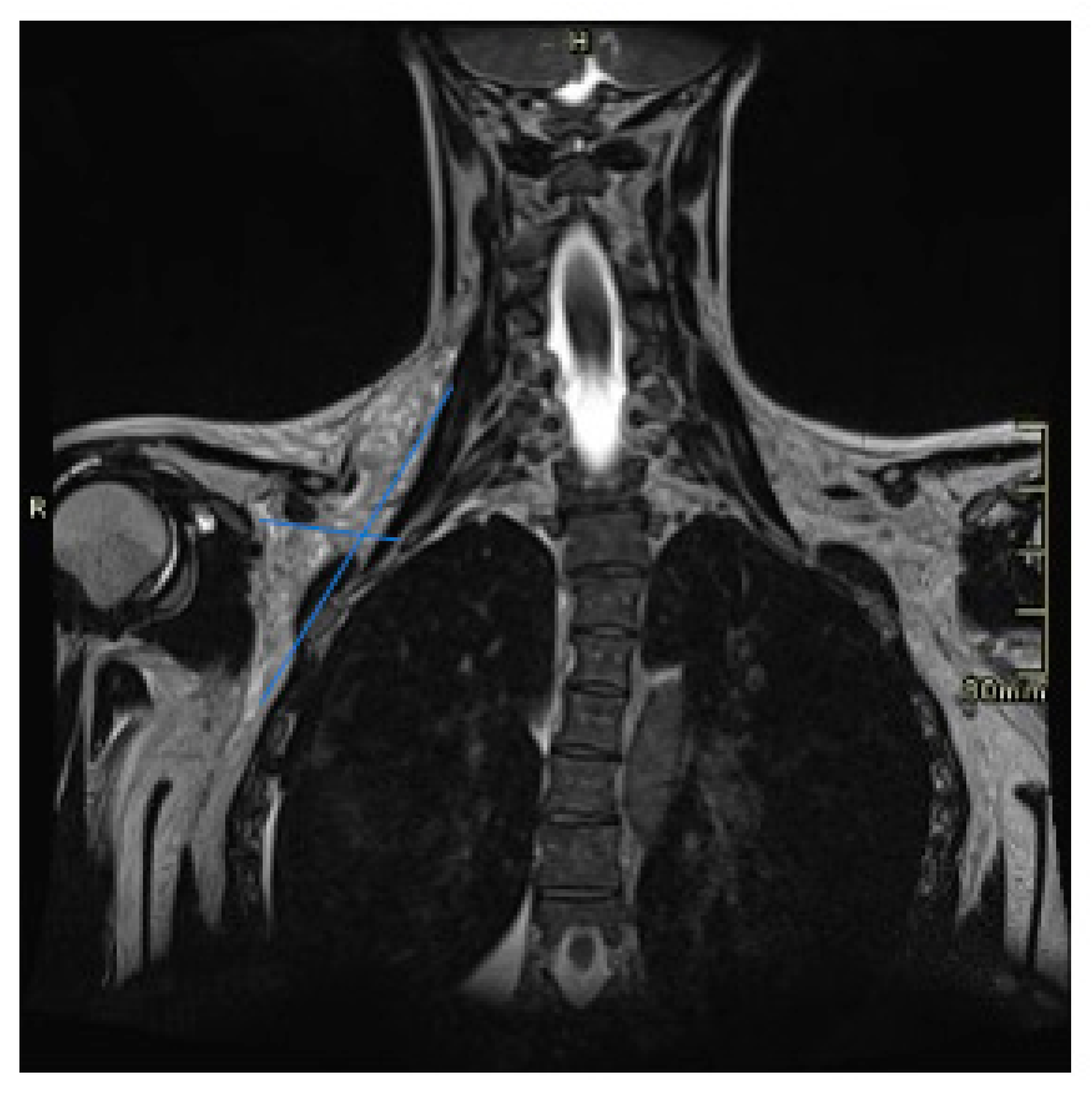
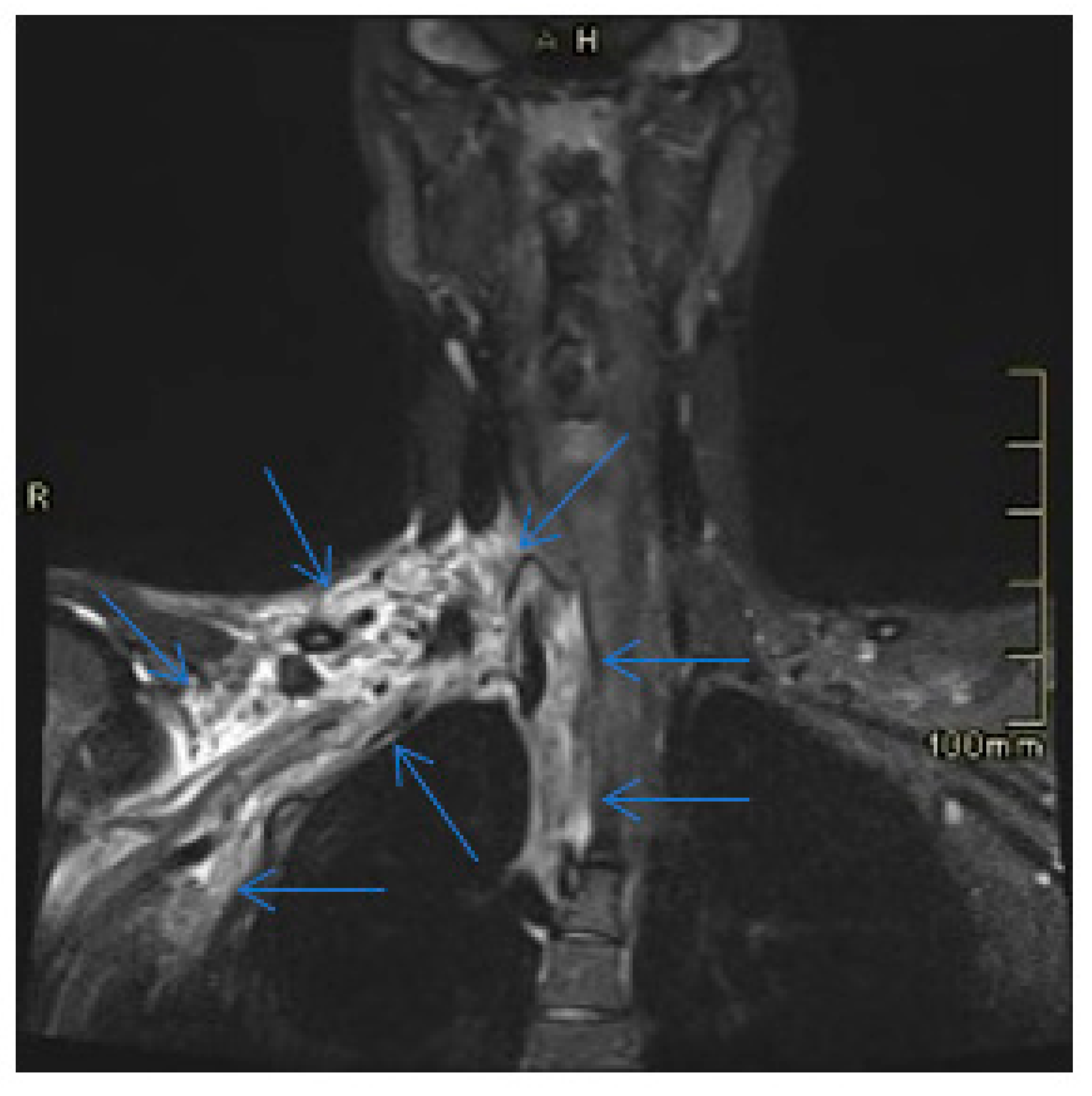
Figure 7.
Coronal T1 MRI with intravenous contrast in equilibrium phase. Bright areas show late enhancement of the lesion. The dark areas correspond to the cavernous areas of the lymphangiovenous malformation.
Figure 7.
Coronal T1 MRI with intravenous contrast in equilibrium phase. Bright areas show late enhancement of the lesion. The dark areas correspond to the cavernous areas of the lymphangiovenous malformation.
The patient evolved favorably, with improvement in pain until it disappeared and with disappearance of the swelling of the supraclavicular region, being discharged from the hospital. She is reviewed in the vascular surgery consultation after a few weeks, being asymptomatic.
3. Discussion
Several theories have been proposed to explain the origin of this anomaly. The blockage or arrest of normal growth of primitive lymphatic channels during embryogenesis. A communication defect between the lymphatic network and the lymphatic sacs or between them and the venous system. Another possibility is that during embryogenesis the lymphatic tissue is deposited in the wrong area, or there is a sequestration of the lymphatic tissue that evolves on its own. Finally, it could be a benign embryonal neoplasm with proliferative capacity of lymphatic vessels and active content (the most accepted theory in recent studies, it seems that due to an altered angiogenesis process caused by the fibroblast growth factor). [5]
It is widely accepted that they arise from the remnants of embryonic lymphatic tissue that retains the potential for proliferation. They grow as shoots and are capable of crossing anatomical limits [12].
The etiology of cervical lymphangioma acquired in adulthood is controversial. It seems to result from predisposing factors (previous theories) and precipitating factors (trauma to the area, iatrogenesis, respiratory infection, etc.) [13,14,15].
Histopathologically, there are several types, classified according to the size of the vessels involved:
- Capillary: it is made up of multiple fine lymphatic ducts, less than 1mm, located in the skin and mucous membranes. Generally located in the subcutaneous tissue.
- Cavernous: it is formed by dilated lymphatic ducts, with thin walls, with cysts smaller than 5 mm. Located on the tongue and mouth.
- Cystic: it is composed of cystic spaces lined by flat epithelium, which contain a clear liquid. They occur most often in the neck.
The most frequent type is that of cystic characteristics. However, it is very common for several types to coexist in the same tumor (lymphangiomas/mixed MVL), and are therefore considered to belong to the same pathological entity. Thus, all three types are frequently found together in the same patient, depending on the severity of the disease [16,17]. Some authors suggest that the capillary type does not really exist.
When a lymphangioma is confined to fairly dense tissue, such as the tongue, it presents as a cavernous lymphangioma, but when it develops in the relatively lax fascia of the neck, a cystic lesion occurs [5].
The clinical presentation depends on its location. Those of the neck are usually asymptomatic. The most prominent sign or symptom of all lymphangiomas is the presence of a painless mass that grows progressively. It is usually soft, painless, and poorly defined. The mass may be small and go unnoticed at birth. However, most lesions are recognized early due to their size and associated symptoms of respiratory obstruction (dyspnea when compressing the trachea) [18,19] and problems with feeding (dysphagia when compressing the esophagus), which are the second and third most common presenting symptom.
In adults, the main complaint is the cosmetic unacceptability of the mass, and the most common presentation is a painless lump in an otherwise asymptomatic patient.
Cervical lymphangiomas have not been shown to lateralize to any particular side of the neck. They can grow in a short period of time, in relation to infection, trauma or bleeding, compressing or incorporating structures such as the larynx, trachea, esophagus, brachial plexus and great vessels within the lesion [20].
Although lymphatic malformations are benign lesions, they rarely resolve spontaneously, and their infiltrative nature coupled with the difficulty in distinguishing involved vital structures of the head and neck from adjacent normal tissues makes complete surgical resection even more difficult [21]. Depending on their size and location, they can become life-threatening due to airway compromise. Some patients may even require a tracheostomy within the first hours of life to establish a secure airway [22,23,24,25].
On ultrasound, these lymphatic malformations appear as hypoechoic, multicystic, multiseptate, thin-walled masses. Those microcystic ones acquire a hyperechoic appearance. The presence of a level between two fluids of different echogenicities (fluid-fluid level) suggests internal bleeding. In the ultrasound differential diagnosis, the possibility of lipomas and bronchogenic cysts should be considered [26].
On computed tomography, they are seen as poorly defined, multilobulated, low-density lesions, usually located in the posterior triangle of the neck. Due to their infiltrative nature it is not uncommon for them to compromise other spaces in the neck [27].
Magnetic resonance imaging is the imaging test of choice. It allows a complete assessment of the extent of the lesion and how it relates to the deep neck spaces and vital structures. On T2-weighted MRI, lymphangiomas appear isointense to cerebrospinal fluid, while their intensity varies on T1-weighted images due to variable protein content [28,29].
Regarding management, observation is usually the first step for small lesions that do not expand [30]. Those that continue to grow or have obstructive symptoms should be resected [5]. Some authors propose therapeutic abstention in asymptomatic cases since complete spontaneous involution has been described in some cases of well-defined lymphangiomas [31].
Available therapeutic tools include surgery, systemic treatment, and injection of sclerosing agents [32,33]. The treatment of choice for macrocystic lymphangiomas limited to the neck is surgical removal. The appropriate age for surgery in children is a controversial issue. Some authors propose waiting until 6-9 months to reduce the risks. In adulthood, complete exeresis is less difficult and recurrences are rare [34].
Surgical removal is complex since complete removal is often not possible. This is due to the compromise of noble structures, given by the histological characteristics previously mentioned [35]. Many cases may require more than one surgical intervention. Recurrence can reach up to 30%. The orofacial location, compared to the cervical, has a significantly higher rate of recurrence. Focal microcystic lesions, with limited invasion of neighboring structures, usually have better results with surgery, when compared to macrocystic lesions.
Intraoperative complications include bleeding (which can even lead to hypovolemic shock) and pharyngeal perforation. Postoperative complications include hypovolemic shock, septic shock, surgical site infections secondary to seroma or lymphocele formation, and cranial nerve abnormalities (VII, IX, X, XI, XII). All blood vessels and nerves between the mandible and the sternoleidomastoid muscle are vulnerable to injury, specifically the mandibular branch of the facial nerve, the spinal branch of the accessory nerve, and most auricular nerves. Alterations in swallowing, chewing may occur. Venous bleeding is a possibility, but injury to the carotid sheath and its contents should be rare.
The rate of complications is variable according to the reported series, but they reach up to 35%. Among the long-term sequelae, unsatisfactory aesthetic results stand out in relation to the scar, with the consequent psychological effect [36]. There may be a long scar depending on the size of the cystic mass, but usually it should improve with time.
Wound infection is usually rare in neck surgery [37].
Another treatment modality is sclerotherapy, which is also considered the treatment of choice when surgery is difficult. However, its superiority compared to surgery has not been demonstrated. The results of sclerosing therapy vary according to the location and histological type. For an optimal result it is necessary to extract the greatest amount of fluid from the lesion prior to injection, regardless of the agent used. After the procedure the operated site must be compressed, in order to maximize contact with the sclerosing agent and reduce the risk of extravasation. Different substances have been proposed, such as bleomycin, tetracyclines, ethanol, hemostatic-sealant agents, doxycycline and OK 432. These modalities can be used either alone or in combination [38,39].
Intralesional bleomycin injection has been used for the treatment of tumors that also have great invasion of neighboring organs, the objective being to reduce the size of the tumor and thus the damage to neighboring organs. It is a cytotoxic agent that has been used in microcystic or mixed malformations [40,41].
In one study using intralesional bleomycin injection, complete reduction was reported in 47% of cases, with partial reduction in more than 50%, with morbidity of 42.9% [2].
Doxycycline is an antibiotic from the tetracycline group that has been used in lymphaticocystic malformations in various anatomical locations, including the cervico-facial region.
OK 432 (picibanil) is a lyophilisate of group A Streptococcus pyogenes (P-hemolytic) incubated with penicillin-G. It is presented as a relatively safe and effective treatment for patients of any age. Intracystic injection of OK-432 produces a local inflammatory reaction that resolves the lesion. The aesthetic appearance is excellent, since it does not leave skin lesions at the injection site, unlike other sclerosing agents. For this reason, it can be considered the treatment of choice, especially in cases in which surgical treatment can produce serious functional or aesthetic sequelae [42,43,44].
Sirolimus is an inhibitor of mTOR (mammalian target of rapamycin), whose cellular pathway has been associated with lymphangiogenesis in preclinical studies. This drug has recently been used for the management of vascular malformations in pediatric patients and, specifically, for lymphatic malformations of the head and neck in children [45,46]. In retrospective studies, it has been shown to be useful in reducing the size of malformations, particularly in macrocystic ones and in younger patients, with mucosal involvement and in cases refractory to previous therapies. Adverse effects include cellulitis, stomatitis, acne, headache, nausea, fatigue, laboratory abnormalities such as hypercholesterolemia, neutropenia, and elevated transaminases. These are related to the dose used and are transient. In 2018, a systematic review on the use of sirolimus for lymphaticocystic malformations was published. The included studies were all retrospective, with a total of 71 patients, with partial remission in 84.5% of the patients. Only 4% of patients progressed the disease despite treatment.
4. Conclusions
Cervical lymphangiomas are uncommon benign congenital malformations usually present in children, but are rare in adults. They are often large asymptomatic masses, in some cases infiltrating or adjacent to surrounding vital structures. There are some factors, including neck trauma, that have been considered as potential triggers for the development and exacerbation of lymphangiomas, as it happens in the case that we present. Observation is usually the first step for small lesions that do not expand, thoug the spontaneous regression is rarely seen, but those that continue growing or have obstructive symptoms should be resected. Sclerotherapy has been popularized and is gradually becoming an adjuvant or alternative treatment for lymphangiomas.
Limitation of sclerotherapy is that nearly all the relevant studies were performed in pediatric patients, and convincing evidence supporting the use of sclerotherapy for treating lymphangiomas in adult patients is still lacking [49].
In this case we adopted a conservative attitude, and the patient presented a favorable evolution.
Author Contributions
Conceptualization, AM.G and E.G; writing—original draft preparation,
AM.G; writing—review and editing, AM.G and E.G; supervision, E.G. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Not applicable.
Informed Consent Statement
Informed consent was obtained from the subject of the case.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Luis Hernández J, Rojas Crespo KL, Artazkoz del Toro JJ, de Serdio-Arias JL. Linfangioma cervical en un adulto (Cervical lymphangioma in an adult). Med Clin (Barc). 2014 Jun 16;142(12):e23. Spanish. [CrossRef] [PubMed]
- Basurto-Kuba EO, Hurtado-Lopez LM, Campos-Castillo C, Buitrón Garcia-Figueroa R, Figueroa-Tentori D, Pulido-Cejudo A. Linfangioma de cuello en el adulto. Reporte de 2 casos (Cervical lymphangioma in the adult. A report of 2 cases). Cir Cir. 2016 Jul-Aug;84(4):313-7. Spanish. [CrossRef] [PubMed]
- Valenzuela Martínez MJ, Santero MP, Arribas MD, Córdoba E, Martínez F. Linfangioma quístico cervical en el adulto (Cervical cystic lymphangioma in adults). Cir Esp. 2010 Feb;87(2):122-3. Spanish. [CrossRef] [PubMed]
- Peral Cagigal B, Serrat Soto A, Calero H, Verrier Hernández A. OK-432 como tratamiento del linfangioma cervicofacial en el adulto (OK-432 therapy for cervicofacial lymphangioma in adults). Acta Otorrinolaringol Esp. 2007 May;58(5):222-4. Spanish. [PubMed]
- V.T. Kandakure, G.V. Thakur, A.R. Thote, A.J. Kausar. Cervical lymphangioma in adult. Case report. Otorhinolaringology Clin Inter J, 4 (3) (2012), pp. 147-150.
- Aydin S, Demir MG, Selek A. A Giant Lymphangioma on the Neck. J Craniofac Surg. 2015 Jun;26(4):e323-5. [CrossRef] [PubMed]
- Acta Otorrinolaringológica Gallega Caso clínico Higroma quístico del adulto Adult cystic hygroma Mohamad Al Rifai Al Masri, Celia Lendoiro Otero, Socorro Tedín García, Manuel Blanco Labrador.
- Brea-Álvarez B, Roldán-Hidalgo A. Quistes en el triángulo cervical posterior en adultos (Cysts in the posterior triangle of the neck in adults). Acta Otorrinolaringol Esp. 2015 Mar-Apr;66(2):106-10. Spanish. [CrossRef] [PubMed]
- Rodríguez-Montes JA, Collantes-Bellido E, Marín-Serrano E, Prieto-Nieto I, Pérez-Robledo JP. Linfangioma esplénico. Un tumor raro. Presentación de 3 casos y revisión de la bibliografía (Splenic lymphangioma. A rare tumour. Presentation of 3 cases and a literature review). Cir Cir. 2016 Mar-Apr;84(2):154-9. Spanish. [CrossRef] [PubMed]
- García-Vico A, Cañete-Gómez J, Gómez-Sotelo AI, Parra-Membrives P. Retroperitoneal cystic lymphangioma as an incidental finding in a patient with pancreatitis symptoms. Cir Esp (Engl Ed). 2019 Dec;97(10):594. English, Spanish. [CrossRef] [PubMed]
- Palomeque Jiménez A, Herrera Fernández FA, Calzado Baeza S, Reyes Moreno M. Linfangioma quístico mesentérico gigante como hallazgo incidental en adulto joven (Giant mesenteric cystic lymphangioma as an incidental finding in a young adult). Gastroenterol Hepatol. 2014 Aug-Sep;37(7):416-7. Spanish. [CrossRef] [PubMed]
- Guruprasad, Y. , Chauhan, D.S. Cervical Cystic Hygroma. J. Maxillofac. Oral Surg. 11, 333–336 (2012). [CrossRef]
- Rev. Soc. Otorrinolaringol. Castilla Leon Cantab. La Rioja 2013 Dic. 4 (24): 194-200 Linfangioma quístico supraclavicular derecho. Presentación inusual en adulto Torres-Morientes LM et al.
- Mathew M, Dil SK. Adult lymphangioma – a rare entity: a report of two cases. Turk Patoloji Derg. 2012; 28 80-82.
- Gleason TJ, Yuh WT, Tali ET, Harris KG, Mueller DP. Traumatic cervical cystic lymphangioma in an adult. Ann Otol Rhinol Laryngol. 1993 Jul;102(7):564-6. [CrossRef] [PubMed]
- Miceli A, Stewart KM. Lymphangioma. 2022 Aug 8. In: StatPearls (Internet). Treasure Island (FL): StatPearls Publishing; 2023 Jan–. [PubMed]
- Liu X, Cheng C, Chen K, Wu Y, Wu Z. Recent Progress in Lymphangioma. Front Pediatr. 2021 Dec 15;9:735832. [CrossRef]
- Torres-Palomino G, Juárez-Domínguez G, Guerrero-Hernández M, Méndez-Sánchez L. Obstrucción de la vía aérea por higroma quístico en un recién nacido (Airway obstruction due to cystic hygroma in a newborn). Bol Med Hosp Infant Mex. 2014 Jul-Aug;71(4):233-237. Spanish. [CrossRef] [PubMed]
- Berrada O, Beghdad M, El Krimi Z, Oukessou Y, Rouadi S, LarbiAbada R, Roubal M, Mahtar M. Cervicofacial cystic lymphangiomas in 17 childrens: A case series. Ann Med Surg (Lond). 2022 May 19;78:103835. [CrossRef]
- L. Gow, R. Gulati, A. Khan, F. Mihaimeed. Adult-onset cystic hygroma: A case report and review of management. Gran Rounds, 11 (2011), pp. 5-11.
- Q. Zhou, J.W. Zheng, H.M. Mai, Q.F. Luo, X.D. Fan, L.X. Su, et al. Treatment guidelines of lymphatic malformations of the head and neck. Oral Oncol, 47 (12) (2011), pp. 1105-1109.
- 22. Lerat J, Mounayer C, Scomparin A, Orsel S, Bessede JP, Aubry K. Head and neck lymphatic malformation and treatment: Clinical study of 23 cases. Eur Ann Otorhinolaryngol Head Neck Dis 2016; 133: 393-396.
- 23. Molino J, Guillén G, Peiró J, García-Vaquero J, et al. Linfangioma quístico cervical: todavía un reto. Cir Pediatr 2010; 23: 147-152.
- 24. Tucci FM, De Vincentiis GC, Sitzia E, Giuzio L, Trozzi M, Bottero S. Head and neck vascular anomalies in children. Int J Pediatr Otorhinolaryngol 2009; 73 Suppl 1:S71-6.
- Kaira V, Kaira P, Agarawal T. Cervical Cystic Lymphangiomas in Adults: A Case Series of a Rare Entity with Literature Review. Head Neck Pathol. 2021 Jun;15(2):503-508. [CrossRef]
- López Uriarte B, Frías Vargas M, Rivera Teijido M, Montes Belloso E, García Martínez G. Linfangioma axilar en el adulto. A propósito de un caso: La ecografía clínica como herramienta de orientación diagnóstica (Axillary lymphangioma in the adult: Clinical ultrasound as a diagnostic tool). Semergen. 2021 Jul-Aug;47(5):350-352. Spanish. [CrossRef] [PubMed]
- Woo EK, Connor SE. Computed tomography and magnetic resonance imaging appearances of cystic lesions in the suprahyoid neck: a pictorial review. Dentomaxillofac Radiol. 2007 Dec;36(8):451-8. [CrossRef] [PubMed]
- 28. Gaddikeri S, Vattoth S, Gaddikeri RS, et al. Congenital cystic neck masses: embryology and imaging appearances, with clinicopathological correlation. Curr Probl Diagn Radiol 2014; 43: 55-67.
- 29. Kadom N, Lee EY. Neck masses in children: current imaging guidelines and imaging findings. Semin Roentgenol 2012; 47:7-20.
- Luján Martínez DM, Candel Arenas MF, Ruiz Marín M, Parra Baños PA, Albarracín Marín-Blázquez A. Utility of conservative treatment in cystic lymphangioma. Cir Esp. 2016 Oct;94(8):485-7. English, Spanish. [CrossRef] [PubMed]
- Díaz Rodríguez D, Benítez Del Rosario JJ, Valido Quintana M, Sánchez Tudela AT. Spontaneous regression of a cervical giant cystic lymphangioma. Acta Otorrinolaringol Esp (Engl Ed). 2021 May-Jun;72(3):195-197. English, Spanish. [CrossRef] [PubMed]
- Kennedy, T. L. , Whitaker, M., Pellitteri, P., & Wood, W. E. (2001). Cystic hygroma/lymphangioma: a rational approach to management. The laryngoscope 111(11), 1929-1937.
- Creger PE, Harper C 3rd, Curry C, Kramer A. Resection of an Asymptomatic Lymphangioma in a 76-Year-Old Male. Cureus. 2021 Jun 10;13(6):e15577. [CrossRef]
- Liu Q, Fu J, Yu Q, Gong W, Li P, Guo X. Laparoscopic surgery of intra-abdominal lymphatic malformation in children. Exp Ther Med. 2022 Jul 19;24(3):581. [CrossRef]
- Curran, A. , Malik, N., McShane, D., & Timon, C. (1996). Surgical management of lymphangiomas in adults. The Journal of Laryngology & Otology, 110 (6), 586-589. [CrossRef]
- Cirugía y Cirujanos. Volume 84, Issue 4, July–16, Pages 313-317. 20 August.
- Tamilselvi R, Tang IP, Linger S, Mohd Soffian MS. Dilemma in management of cervico-facial cystic hygroma. Med J Malaysia. 2019 Oct;74(5):450-451. [PubMed]
- 38. Perkins JA, Manning SC, Tempero RM, et al. Lymphatic malformations: review of current treatment. Otolaryngol Head Neck Surg 2010;142:795-803.
- 39. Colbert SD, Seager L, Haider F, Evans BT, Anand R, Brennan PA. Lymphatic malformations of the head and neck-current concepts in management. Br J Oral Maxillofac Surg 2013;51:98-102.
- Niramis, R. , Watanatittan, S., & Rattanasuwan, T. (2010). Treatment of cystic hygroma by intralesional bleomycin injection: experience in 70 patients. European journal of pediatric surgery 20(03), 178-182.
- Vaid, L. , Gupta, M., Gupta, N., & Singh, P. P. (2010). Bleomycin sclerotherapy in a rare case of adult-onset cervical lymphangioma. ENT: Ear, Nose & Throat Journal 89(1).
- Fasching G, Dollinger C, Spendel S, Tepeneu NF. Treatment of lymphangiomas by means of sclerotherapy with OK-432 (Picibanil®) is safe and effective - A retrospective case series. Ann Med Surg (Lond). 2022 Sep 2;81:104531. [CrossRef]
- Manzini M, Schweiger C, Manica D, Kuhl G. Response to OK-432 sclerotherapy in the treatment of cervical lymphangioma with submucosal extension to the airway. Braz J Otorhinolaryngol. 2020 Jan-Feb;86(1):127-129. [CrossRef]
- Alonso J, Barbier L, Alvarez J, Romo L, Martín JC, Arteagoitia I, Santamaría J. OK432 (picibanil) efficacy in an adult with cystic cervical lymphangioma. A case report. Med Oral Patol Oral Cir Bucal. 2005 Aug-Oct; 10(4): 362-6. English, Spanish. PMID: 16056191. [Google Scholar]
- 45. Strychowsky JE, Rahbar R, O'Hare MJ, Irace AL, Padua H, Trenor CC 3rd. Sirolimus as treatment for 19 patients with refractory cervicofacial lymphatic malformation. Laryngoscope 2018;128:269-276.
- 46. Triana P, Dore M, Cerezo VN, et al. Sirolimus in the Treatment of Vascular Anomalies. Eur J Pediatr Surg 2017;27:86-90.
- Khanwalkar A, Valika T, Maddalozzo J. Long-term symptom control following resection of cervical lymphatic malformations: a case series. J Otolaryngol Head Neck Surg. 2020 Apr 19;49(1):19. [CrossRef]
- 48. Colbert SD, Seager L, Haider F, Evans BT, Anand R, Brennan PA. Lymphatic malformations of the head and neck-current concepts in management. Br J Oral Maxillofac Surg 2013;51:98-102.
- Wang J, Yang Y, Guo J, Yao Y, Dong L, Mou Y, Zhang Y, Song X. Cervical lymphangioma in adults: A report of seven cases and review of the literature. Laryngoscope Investig Otolaryngol. 2022 Apr 22;7(3):751-756. [CrossRef]
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



