
Submitted:
16 May 2023
Posted:
17 May 2023
You are already at the latest version
Abstract
For centuries, Foeniculi fructus (F. fructus) has been used as a traditional herbal medicine in China and Europe and is widely used as a natural therapy for digestive disorders, including indigestion, flatulence, and bloating. The mechanism by which F. fructus alleviates functional dyspepsia was analyzed through network pharmacology, and its therapeutic effect on an animal model of functional dyspepsia was investigated. The compounds, targets, and related diseases of F. fructus were studied utilizing the traditional Chinese medicine systems pharmacology (TCMSP) database. Information on the target genes was classified using the UniProt database. A network was built using Cytoscape 3.9.1, and functional dyspepsia-related genes were checked using the Cytoscape string application. The efficacy of F. fructus on functional dyspepsia, including gastroparesis and gastrointestinal motility, was confirmed by treatment with its extract in a mouse model of loperamide-induced functional dyspepsia. Seven compounds targeted twelve functional dyspepsia-associated genes. In a functional dyspepsia mouse model, F. fructus significantly suppressed the symptoms when compared to that in the control group. Our animal studies showed that the mechanism of action of F. fructus is closely related to gastrointestinal motility. Based on animal experimental results, the results showed that F. fructus provides a potential means to treat functional dyspepsia, suggesting that its medical mechanism for functional dyspepsia can be described by the relationship between seven key compounds of F. fructus, including oleic acid and β-sitosterol, and 12 functional dyspepsia-related genes.
Keywords:
Foeniculi fructus
; Functional dyspepsia
; Network Pharmacology
; Traditional Medicine
; TCMSP.
1. Introduction
Functional dyspepsia is a clinical syndrome characterized by frequent or chronic complaints of discomfort or pain in the upper abdomen, without underlying organic diseases [1]. Eradication of histamine H2 receptor antagonists [2], inhibitors of proton pumps [3], and Helicobacter pylori in patients with functional dyspepsia has demonstrated few benefits [4] and the results of controlled trials were generally disappointing. Furthermore, despite their low efficacy, pharmacological agents (e.g., cisapride) carry the risk of side effects.
One attractive alternative through a natural approach is the use of herbal remedies, which are recognized to have a low risk of side effects. However, few rigorous clinical studies are available because of the insufficient standardization of herbal ingredients.
Foeniculi fructus (F. fructus) or Foeniculum vulgare, an umbelliferous plant, is native to southern Europe and the Mediterranean region, and has been used as a traditional herbal medicine in ancient times in China and Europe. It is used as a natural cure for digestive disorders, including flatulence, bloating, and indigestion, and has antipyretic, analgesic, and antioxidant properties [5,6,7]. F. fructus alleviates the symptoms of female menopausal syndrome, regulates menstruation, and increases libido [8]. It also has galactagogue and emmenagogue properties [9]. F. fructus has hepatoprotective effects and may be used in pediatric colic [10,11]. Also, in traditional Turkish medicine, F. fructus is used as a diuretic, laxative, antispasmodic, lactating stimulant, and a wound dressing [12].
Traditional herbal medicines have complex pharmacological properties, often fundamentally limiting the study of comprehensive mechanisms of action using conventional biological experimental methodologies [13,14,15,16,17,18,19,20]. To solve these difficulties, network pharmacology, an integrated research field using physics, mathematics, medicine, pharmacology, network science, and computational systems biology, is a new and effective approach [13,14,15,16,17,18,19,20]. The goal of this integrative science is to identify the mechanisms of drug activity and disease pathogenesis through interactions between biological components such as organs, tissues, cells, proteins, and genes [13,14,15,16,17,18,19,20]. To-date, network pharmacology studies have identified distinct system-level pharmacological effects, active compounds, and key therapeutic targets, as well as mechanisms (e.g., apoptosis, proliferation, oxidation, and by further confirming the therapeutic regulation of biological processes such as reduction, cell cycle regulation, insulin metabolism, and inflammation) and the multipharmacological properties of traditional herbal drugs exerted by synergistic interactions between multiple compounds and targets [13,14,15,16,17,18,19,20,21,22,23,24,25,26,27,28,29,30,31]. A schematic representation of the study protocol is shown in Figure 1. With the present network pharmacology research, we aimed to elucidate the influence of F. fructus on the molecular mechanisms underlying its digestive properties from a systems perspective.
2. Materials and Methods
2.1. Analysis of Network pharmacology
2.1.1. Identifying compounds of F. fructus
To identify the potentially active compounds in F. fructus, we used the traditional Chinese medicine systems pharmacology (TCMSP) database. We entered 'Foeniculi fructus' as a search term for herbs.
2.1.2. Target network
The target information was obtained using TCMSP [32]. Target proteins were linked to official gene names using the UniProtKB database (https://www.uniprot.org/uniprot) [33].
2.1.3. Analysis of network
The compound-target network was built using Cytoscape 3.9.1 (https://cytoscape.org) [34]. Functional dyspepsia-associated genes were collected using Cytoscape App., which organized and updated the data weekly [35].
2.1.4. Screening of Active compound
Utilizing the absorption, distribution, metabolism, and excretion (ADME) parameters for molecular weight (MW), oral bioavailability (OB), Caco-2 (Caco-2 permeability), and drug similarity (DL), physiologically active compounds in F. fructus were screened using the following criteria: OB ≥ 30%, DL ≥ 0.10, and Caco-2 ≥-0.4. Compounds corresponding to the values that met the applied criteria were selected as the active compounds.
2.2. Analysis of F. fructus
2.2.1. Instrument and Reagent
Ultra-performance liquid chromatography (UPLC) was performed using a Waters ACQUITY ultra-performance LC system (USA). Waters ACQUITYTM photodiode array detector (PDA) and HPLC column (Waters ACQUITYTM BEH C18 columns (1.7 µm, 2.1 × 100)) and the software Empower was used. The reagents used in this experiment were methanol (Junsei for HPLC), acetonitrile (JT-BAKER for HPLC), and water (tertiary distilled water). The standard preparations of this experiment were obtained from Anethole (Sigma-Aldrich, St. Louis, MO, USA), R-(a)-phellandrene (Sigma-Aldrich, St. Louis, MO, USA), 4-Methoxybenzoic acid (ChemFaces, Wuhan, China).
2.2.2. Preparation of the standard solution
Anethole, R-(a)-phellandrene, and 4-Methoxybenzoic acid were measured accurately and melted by dimethyl sulfoxide (DMSO) and methanol, and then made into a standard undiluted solution that contained 1 mg per ml. In succession, the standard undiluted solution was diluted with methanol to 12.5, 25, 50, and 100 μg per ml and they were used as standard solutions. The standard curve determination coefficient (R2) values of all the standard materials exceeded 0.999.
2.2.3. Preparation of the test liquid for quantitative analysis
A test liquid for quantitative analysis was mixed with the sample equally and exactly 0.2 grams was added to 10 mL of ethyl alcohol, and then extracted by microwave for one hour. This test liquid was filtered through a 0.22 μm membrane filter.
2.2.4. Quantitation of the F. fructus extract
UPLC was performed using a Waters ACQUITYTM ultra-performance LC system (USA) and Waters ACQUITYTM BEH C18 column (1.7 μm, 2.1×100). The temperature of the column was maintained at room temperature. For PDA analysis, 4-Methoxybenzoic acid and R-(a)-phellandrene were analyzed at 330 nm, and the anethole was analyzed at 306 nm (Table 1). The mobile phase was a mixture of acetonitrile and water containing 0.1% formic acid. The analysis conditions were as follows: the injected sample was 2 μl, flow rate was 0.4 ml/min, and the qualitative results of the analysis was observed by checking the retention time, and then quantitated by the peak area method. The F. fructus samples were deposited at the College of Korean Medicine, Daegu Hanny University (Table 2; Figure 2).
2.3. Animal testing
2.3.1. Design of Animal experiment
A total of 108 specific pathogen-free (SPF) ICR mice (male, 19–21 g, five weeks old) were purchased from a commercial animal breeder (Samtako, Gyeonggi, Korea). The mice were housed in the room of SPF facility maintained at 22 ± 2 °C and 60 ± 5% relative humidity on a 12/12 h light/dark cycle. The mice were supplied with commercial standard chow (Samtako, Gyeonggi, Korea) and tap water ad libitum. After acclimatization for one week, the mice were randomly assigned to three experimental groups; first set for small intestine motility (6 mice/group, n = 36), second set for gastric emptying test (6 mice/group, n = 36), and third set for western blot, qPCR, and histopathology (3 mice/group, n = 18). Each set was divided into six groups: control, loperamide (10 mg/kg), three doses of F. fructus (25, 50, and 100 mg/kg), and mosapride (positive control, 3 mg/kg). In general, the treatment dose of mosapride was 3.1 mg/kg in mice [36]. Foeniculi fructus and mosapride were prepared using distilled water. Each group was orally administered distilled water (control and loperamide groups), F. fructus, or mosapride for three consecutive days [37,38]. The treatment schedule is shown in Figure 6A. Experiments and animal care were performed in accordance with the guidelines issued by the Animal Care and Use Committee of the Pusan National University Animal Research Institute (PNU-2022-0160) and the guidelines for the management and use of laboratory animals at the US National Institutes of Health.
2.3.2. Assessment of gastric weight and gastric emptying by phenol red
Mice were fasted for 19 h with a free supply of tap water. The selection of the phenol red solution volume (500 µL/mouse) and the 50% delayed gastric emptying time point (30 min after intraperitoneal (IP) injection of 10 mg/kg of loperamide) was done according to earlier study protocols was referenced [39,40]. The mice were euthanized 30 min after treatment with 0.05% phenol red, their stomachs were removed immediately, and the weights were measured. Next, the stomach was treated with 5 mL of 0.1N sodium hydroxide solution to check the optical density of the phenol red remaining in the stomach; 0.5 mL of trichloroacetic acid (20% w/v). The homogenate was centrifuged at 3000 rpm for 20 min. One milliliter of the supernatant was added to 4 mL of 0.5N sodium hydroxide solution, and the optical density of this pink liquid was measured using a spectrophotometer (560 nm).
The above emission values were obtained according to the formula:
gastric emptying (%) = (1-X/Y) *100.
X: Optical density of the phenol red remaining on it.
Y: Optical density of the phenol red mixture with sodium hydroxide under test tube conditions.
2.3.3. Assessment of intestinal transit rate by Evans blue
To measure the intestinal transit rate, the Evans blue diet method was used, in which 5% Evans blue was prepared in distilled water as previously described [41]. Evans blue diet was orally administered (250 μL/20 g mouse) 30 min after IP injection of loperamide. The mice were euthanized 30 min after the Evans blue diet, and the distance traveled through the small intestine (from the pylorus to the cecum) by Evans blue was measured to determine the intestinal transit distance. The above time points were selected as per the methods of an earlier study [42].
2.3.4. Western blot analysis for check of protein level
To measure the gastric protein levels of neuronal nitric oxide synthase (nNOS), TEME16A, and TRPM7, gastric tissues were homogenized in RIPA lysis buffer. After denaturing the protein by boiling for 5 min, the proteins were separated by electrophoresis on a 10% polyacrylamide gel and transferred to a nitrocellulose (NC) membrane. After blocking in 5% skim milk for 30 min, membranes were tested overnight at 4 °C with nNOS (1:1000, ab76067), TEME16A (1:1000, a72984), TRPM7 (1:200, ab135817), or β-actin (1:5000, sc-47778). Membranes were washed and incubated with horseradish peroxidase (HRP)-conjugated rabbit antibody (1:5000 against nNOS, TEME16A, and TRPM7) or HRP-conjugated mouse antibody (1:5000 against β-actin) for 1 h at room temperature. Proteins were visualized using the Western Bright Sirius (Advansta, San Jose, CA, USA). Protein expression was observed using an ImageQuant LAS 4000 (GE Healthcare, Chicago, IL, USA). ImageJ software (NIH) was used to quantify protein expression.
2.3.5. Quantitative real-time PCR to evaluate gene expression
To identify muscle contraction-related gene expression, including 5HT4 receptor (5HT4R), ryanodine receptor 3 (RYR3), anoctamin-1 (ANO1), and smooth muscle cell myonneuron chaining kinase (smMLCK), total mRNA was extracted from the stomach tissues using Trizol reagents (Invitrogen, Waltham, MA, USA). cDNA was synthesized from the entire RNA sample (1 μg) using a cDNA reverse transcription kit (M-MLV Reverse Transcriptase, Promega, USA). qPCR was performed using iTaq Universal SYBR Green Supermix (Bio-Rad, Hercules, CA, USA) and the primers listed in Table 3. Gene expression data were analyzed using the StepOnePlus Real-Time PCR System (Applied Biosystems, Foster City, CA, USA).
3. Results
3.1. Target information derived by examining correlations between compounds and targets
We identified 45 potentially active compounds in F. fructus using the TCMSP database (Supplementary Materials Table S1). Among these, 41 compounds contained information about the target (Supplementary Materials Table S2); 41 compounds and 260 targets were found to interact with a combination of 611 components. As shown in Figure 3, acetaldehyde was linked to the most number of targets (142 genes), followed by oleic acid (48 genes), β-sitosterol (38 genes), APIOL (31 genes), stigmasterol (31 genes), anisketone (24 genes), (-)-nopinene (21 genes), and terragon (20 genes).
3.2. Twenty active compounds achieved the criteria for the applied absorption, distribution, metabolism and excretion parameters
Nine compounds were included in the active compound screening criteria (Table 4): ammidin, β-sitosterol, EIC, oleic acid, majudin, oleic acid, petroselic acid, stigmasterol, and uvadex.
3.3. Thirty-two compounds associated with gastrointestinal (GI) diseases were identified in F. fructus
We also identified compound-target-disease relationships using the TCMSP database. We noted that 32 compounds were associated with GI disease (Table 5). In particular, ammidin, β-sitosterol, EIC, isooleic acid, oleic acid, petroselic acid, and stigmasterol were revealed to be active compounds related with gastrointestinal diseases. Other compounds associated with gastrointestinal diseases, including (-)-nopinene, (1S,5S)-1-isopropyl-4-methylenebicyclo [3.1.0]hexane, (S)-(+)-alpha-phellandrene, 1,8-cineole, acetaldehyde, alpha-amyrin, anethole, anisketone, ANN, APIOL, arachic acid, butyrophenone, cis-ligustilide, D-camphene, fenchylacetate, L-limonen, moslene, myristic acid, oleanolic acid, palmitic acid, pentadecylic acid, sitogluside, skimmetin, TDA, and terragon were confirmed as non-active compounds (Figure 4).
3.4. All 31 GI disease-related compounds in F. fructus except oleanolic acid were associated with functional dyspepsia
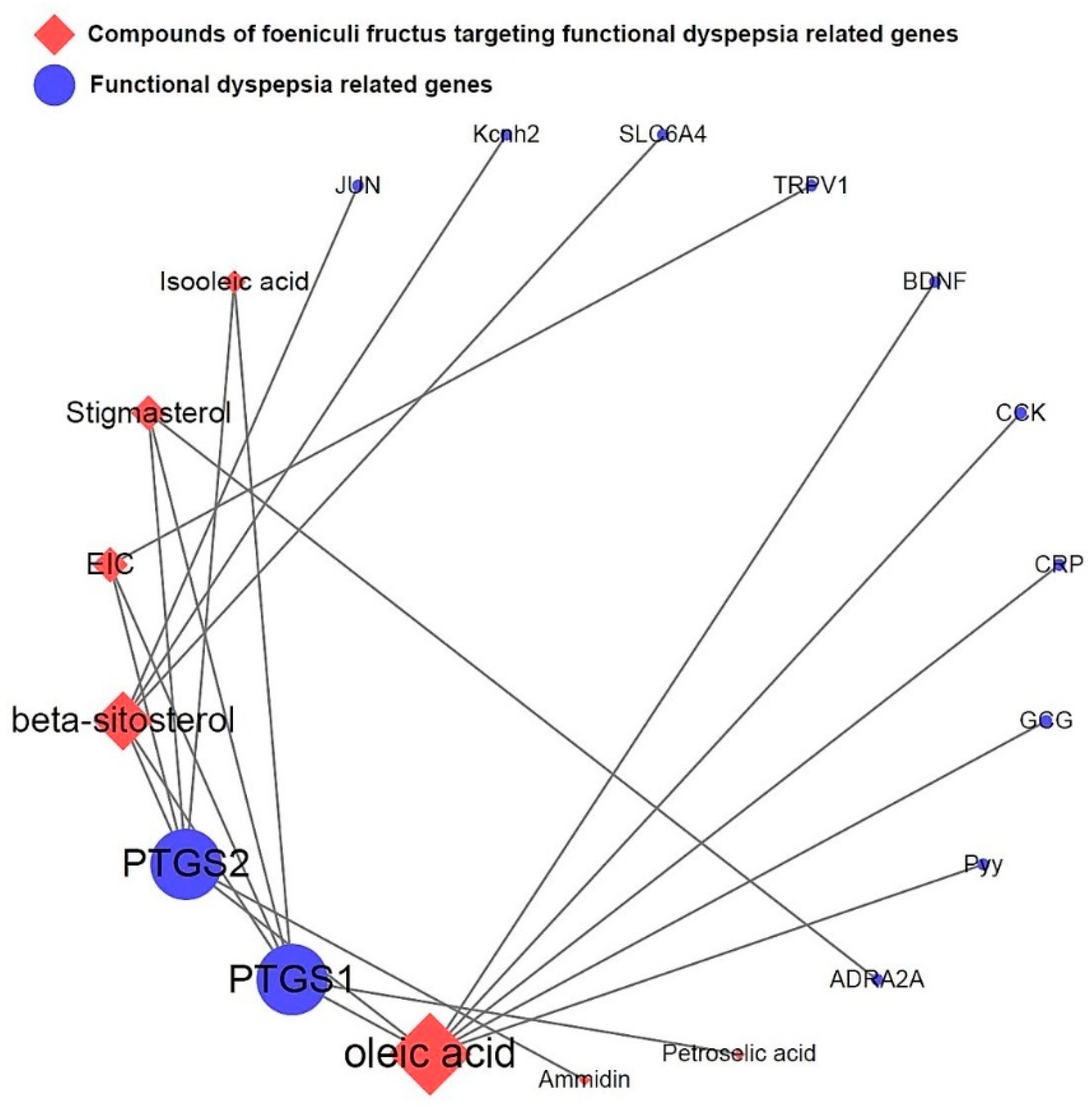
To investigate the relationship between F. fructus and functional dyspepsia, we used the Cytoscape App to determine genetic information related to functional dyspepsia. First, 100 functional dyspepsia-related genes were identified by following a confidence (score) cutoff of 0.40 and a maximum of 100 proteins (Supplementary Materials Table S3). From the results obtained, a network of functional dyspepsia-related genes and activated F. fructus compound target genes were generated (Figure 5). Fourteen genes corresponding to two gene sets were identified, and the functional dyspepsia-related genes targeted by the activated F. fructus compound were ADRA2A, BDNF, CCK, CRP, GCG, JUN, Kcnh2, PTGS1, PTGS2, Pyy, SLC6A4 and TRPV.
3.5. Network of functional dyspepsia-associated genes and compounds for identification of interesting molecules
Figure 6 shows the relationship network between activated F. fructus compounds and functional dyspepsia-associated target genes. PTGS1 and PTGS2 were most closely related to functional dyspepsia. In summary, ammidin, EIC, oleic acid, petroselic acid, stigmasterol, β-sitosterol, and oleic acid were active compounds that targeted functional dyspepsia-associated genes, suggesting that they could be potential drug candidates.
Figure 6.
Network of compounds of F. fructus and functional dyspepsia-related genes.
3.6. Mouse experiment on delayed gastric emptying
Loperamide injection induced gastric food retention, whereas pretreatment with F. fructus decreased this effect, as seen by macroscopic observation (Figure 7B). This finding was validated using quantitative analysis. The gastric weight of the F. fructus-treated group was significantly lower than that of the loperamide group (p < 0.05, Figure 7C). Pretreatment with F. fructus also significantly decreased the amount of phenol red retention in the stomach compared to that in the loperamide group (p < 0.05, Figure 7D). Pretreatment with mosapride also had similar effects as the F. fructus treatment.
3.7. Mouse experiment on molecules involved in gastrointestinal motility
Loperamide injection sharply attenuated nNOS, TEME16A, and TRPM7 protein expression in gastric tissue, whereas pretreatment with F. fructus sharply increased nNOS, TEME16A, and TRPM7 protein expression (p < 0.01, Figure 8A,B). Loperamide injection also decreased smooth muscle contraction-related gene expression, including 5HT4R, RYR3, ANO1, and smMLCK. These changes were inhibited by pretreatment with F. fructus (p < 0.05, p < 0.01, Figure 8C). Mosapride had a positive effect on nNOS, TEME16A, TRPM7 proteins and 5HT4R, RYR3, ANO1, and smMLCK gene expression.
3.8. Mouse experiment on intestinal motility
Loperamide injection sharply attenuated small intestine motility compared with that in the control group. This suppression of small intestine motility was significantly restored by pretreatment with F. fructus (p < 0.01; Figure 9A,B). Pretreatment with mosapride also sharply restored the motility of the small intestine, similar to that of F. fructus.
4. Discussion
F. fructus is widely cultivated in southern Europe and the Mediterranean region and has been used as a popular traditional herbal medicine in China and Europe for centuries. A series of studies have shown that it has antitumor, antioxidant, cytoprotective, hypoglycemic, hepatoprotective, and estrogenic activities [11,43,44,45,46] and effectively controls many infectious disorders of bacterial, fungal, mycobacterium, protozoan, and viral origin [47,48,49]. The seeds of F. fructus are known to be associated with menstrual control and alleviation of symptoms of female menopausal syndrome [8], and the aqueous extract of F. fructus has a significant antiulcer effect against ethanol-induced gastric lesions [50]. In addition, the essential oil of F. fructus regulates intestinal smooth muscle motility and reduces intestinal gas. It is also used in the treatment of spasmodic gastrointestinal disorders and indigestion caused by gastrointestinal disorders along with other plant medicines [51]. However, this has not yet been studied.
This study was performed using a combination of network-based pharmacological analysis and experimental validation to elucidate the bioactive components and therapeutic mechanisms of F. fructus. As a result of the investigation, 45 compounds, including 9 active compounds, were identified (Supplementary Materials Table S1), and 41 of the 45 compounds had target information (Supplementary Materials Table S2) and 260 target genes were identified (Supplementary Materials Table S3). FD and F. fructus-related genes included alpha-2A adrenergic receptor (ADRA2A), brain-derived neurotrophic factor (BDNF), cholecystokinin (CCK), C-reactive protein (CRP), glucagon (GCG), transcription factor Jun (JUN), hERG (Kcnh2), cyclooxygenase 1 (PTGS1), cyclooxygenase 2 (PTGS2), peptide YY (Pyy), serotonin transporter (SLC6A4), and transient receptor potential cation channel subfamily V member 1 (TRPV1) (Figure 5). These results are consistent with those of previous studies. Specifically, as shown in Figure 6, PTGS1 and PTGS2 were the targets of most of the activated FD-related compounds in F. fructus, suggesting that the compounds in F. fructus can synergistically modulate the levels of PTGS1 and PTGS2. PTGS1 is associated with dyspepsia and chronic cystitis [52] and contributes to the maintenance of the mucus barrier and mucosal blood flow in the stomach [53]. PTGS2 mediates some of the most important elements of mucosal defense, contributes significantly to resolving gastroenteritis, and plays an important role in regulating ulcer healing. PTGS2 also contributes to long-term changes in gastrointestinal function following inflammation [54]. These results indicate that the effects of F. fructus PTGS1 and PTGS2 on the treatment mechanism of functional dyspepsia are related.
Functional dyspepsia-related active compounds including ammidin, EIC, oleic acid, petroselic acid, stigmasterol, β-sitosterol, and oleic acid were identified (Figure 6). Six compounds were found to target PTGS1 and PTGS2, and oleic acid targeted BDNF, CRP, CCK, GCG, PTGS1, PTGS2, and Pyy. β-sitosterol targeted JUN, Kcnh2, PTGS1, PTGS2, and SLC6A4. Several studies have confirmed the relationship between major compounds and functional dyspepsia. Emulsions with oleic acid activate a nutrient-induced negative feedback mechanism in the small intestine, which slows gastrointestinal transit and reduces diarrhea [55]. β-Sitosterol improves antibacterial activity and DSS-induced colitis in mice [56].
In Figure 7, the multi-component multi-targeting properties of herbal medicines were confirmed by interaction with an average of approximately 15 target genes, and F. fructus was predicted to be a therapeutic agent for functional dyspepsia based on the synergy of several compounds contained in it. We investigated the therapeutic effects of F. fructus in a mouse model of functional dyspepsia. Our results showed that F. fructus has therapeutic potential for functional dyspepsia. In addition, it was found that there was a therapeutic effect on functional dyspepsia through a mechanism related to the interaction between seven major active ingredients of F. fructus, such as oleic acid and β-sitosterol, and 12 functional dyspepsia-related genes, including PTGS1 and PTGS2.
We selected a functional dyspepsia animal model using loperamide to test the pharmacological effects of F. fructus and to identify the mechanism of action. Loperamide, an agonist of the μ-opioid receptor, is used to trigger dyspepsia [57].
Loperamide injection delayed gastric emptying, as indicated by the observations of postprandial satiety, gastric weight gain, and retention of phenol red in the stomach. Pretreatment with F. fructus significantly prevented the delay in gastric emptying. (Figure 7). Delayed gastric emptying is a typical feature of functional dyspepsia observed in most clinical studies [58,59]. In our model, GI motility was significantly decreased following loperamide treatment (Figure 8). Previous studies reported a high degree of overlap (approximately 19%) between functional dyspepsia and irritable bowel syndrome (IBS) [60,61]. Postprandial satiety is a major complaint in patients with IBS and FD, in which constipation predominates [62]. The delay in GI immobility induced by loperamide was significantly alleviated by pretreatment with F. fructus extract (Figure 9).
To elucidate the mechanism of response to the therapeutic effect of F. fructus, the results of the identification of nNOS protein levels and the expression of four genes (5-HT4R, RYR3, ANO1, and smMLCK) in gastric tissue contribute to the therapeutic effect of F. fructus discussed above. NO produced by nNOS, a well-known neurotransmitter in the gastrointestinal tract, plays an important role in smooth muscle cell relaxation [63]. In addition, nNOS gene polymorphisms are associated with susceptibility to FD and pathological conditions of postprandial discomfort and epigastric pain [64]. Pretreatment with F. fructus significantly improved loperamide-induced reduction of nNOS protein levels, and smooth muscle contraction-related genes 5-HT4R, RYR3, ANO1, and smMLCK were increased by pretreatment with F. fructus (Figure 8). Both the activation of ICC and the generation of slow waves depend on the function of ANO1 to activate intracellular calcium efflux into interstitial cells of Cajal (ICC) [65,66]. The Ca2+ spark creates a slow wave and is regulated by ANO1 in the membrane of ICC and by RYR3 molecules in the endoplasmic reticulum [67,68]. A decrease in smMLCK activity in the smooth muscle in intestinal motility disorders is characterized by diminished peristalsis [69]. ANO1 and smMLCK were downregulated in an animal model of diabetic gastroparesis [70,71]. These results suggest that F. fructus has pharmacological activity that modulates ICC in the gastrointestinal tract. By modulating nNOS, F. fructus can restore normal peristalsis and activate contraction-related molecules.
5. Conclusions
In the analysis using network-based pharmacological analysis, 7 compounds and 12 genes of F. fructus were found to be associated with functional dyspepsia. Our animal studies have shown that F. fructus suppresses functional dyspepsia-like symptoms in a mouse model of functional dyspepsia. These results revealed that F. fructus has therapeutic potential for functional dyspepsia.
Supplementary Materials
The following supporting information can be downloaded at: https://www.mdpi.com/xxx/s1, Table S1: Potential active compounds of Foeniculi Fructus. Table S2: Target genes of Foeniculi Fructus. Table S3: One hundred functional dyspepsia-related genes
Author Contributions
Conceptualization, N.R.C., B.J.K. and W.G.C.; methodology, N.R.C., B.J.K. and W.G.C.; software, N.R.C., D.J., S.C.K. and J.W.P. ; validation, N.R.C., B.J.K. and W.G.C. ; formal analysis, N.R.C. and W.G.C. ; investigation, N.R.C., D.J., S.C.K. and J.W.P.; resources, D.J., S.C.K. and J.W.P.; data curation, N.R.C., B.J.K. and W.G.C.; writing—original draft preparation, B.J.K. and W.G.C.; writing—review and editing, B.J.K. and W.G.C.; visualization, N.R.C. and W.G.C.; supervision, B.J.K. and W.G.C.; project administration, B.J.K.; funding acquisition, B.J.K. All authors have read and agreed to the published version of the manuscript.
Funding
This study was supported by Basic Science Research Program through the National Research Foundation of Korea (NRF) funded by the Ministry of Education (2021R1I1A3042479).
Institutional Review Board Statement
The animal study protocol was approved by the Institutional Animal Care and Use Committee (IACUC) at Pusan National University (Busan, Korea; approval no. PNU-2022-0237).
Informed Consent Statement
Not applicable.
Data Availability Statement
The original data are available upon reasonable request to the corresponding author.
Acknowledgments
Not applicable.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Clouse, R.E.; Mayer, E.A.; Aziz, Q.; Drossman, D.A.; Dumitrascu, D.L.; Mönnikes, H.; Naliboff, B.D. Functional Abdominal Pain Syndrome. Gastroenterology 2006, 130, 1492–1497. [Google Scholar] [CrossRef]
- Talley, N.J.; McNeil, D.; Hayden, A.; Piper, D.W. Randomized, double-blind, placebo-controlled crossover trial of cimetidine and pirenzepine in nonulcer dyspepsia. Gastroenterology 1986, 91, 149–156. [Google Scholar] [CrossRef] [PubMed]
- Moayyedi, P.; Delaney, B.C.; Vakil, N.; Forman, D.; Talley, N.J. The efficacy of proton pump inhibitors in nonulcer dyspepsia: A systematic review and economic analysis. Gastroenterology 2004, 127, 1329–1337. [Google Scholar] [CrossRef] [PubMed]
- Laine, L.; Schoenfeld, P.; Fennerty, M.B. Therapy for Helicobacter pylori in Patients with Nonulcer Dyspepsia: A Meta-Analysis of Randomized, Controlled Trials. Ann. Intern. Med. 2001, 134, 361. [Google Scholar] [CrossRef] [PubMed]
- Liu, H.C.; Cheng, H.H. 2003. Genetic mapping of the chicken stem cell antigen 2 (SCA2) gene to chromosome 2 via PCR primer mutagenesis: Brief notes. Anim. Genet. 2003, 34, 158–160. [Google Scholar] [CrossRef] [PubMed]
- Choi, E.M.; Hwang, J.K. Antiinflammatory, analgesic and antioxidant activities of the fruit of Foeniculum vulgare. Fitoterapia 2004, 75, 557–565. [Google Scholar] [CrossRef] [PubMed]
- Guimarães, R.; Barros, L.; Carvalho, A.M.; Ferreira, I.C.F.R. Infusions and Decoctions of Mixed Herbs used in Folk Medicine: Synergism in Antioxidant Potential: SYNERGISM IN ANTIOXIDANT POTENTIAL OF MIXED HERBS FROM FOLK MEDICINE. Phytother. Res. 2011, 25, 1209–1214. [Google Scholar] [CrossRef]
- Albert-Puleo, M. Fennel and anise as estrogenic agents. J. Ethnopharmacol. 1980, 2, 337–344. [Google Scholar] [CrossRef]
- Ostad, S.N.; Soodi, M.; Shariffzadeh, M.; Khorshidi, N.; Marzban, H. The effect of fennel essential oil on uterine contraction as a model for dysmenorrhea, pharmacology and toxicology study. J. Ethnopharmacol. 2001, 76, 299–304. [Google Scholar] [CrossRef]
- Savino, F.; Cresi, F.; Castagno, E.; Silvestro, L.; Oggero, R. A randomized double-blind placebo-controlled trial of a standardized extract of Matricariae recutita,Foeniculum vulgare andMelissa officinalis (ColiMil®) in the treatment of breastfed colicky infants. Phytother. Res. 2005, 19, 335–340. [Google Scholar] [CrossRef]
- Özbek, H.; Uğraş, S.; Dülger, H.; Bayram, İ.; Tuncer, İ.; Öztürk, G.; Öztürk, A. Hepatoprotective effect of Foeniculum vulgare essential oil. Fitoterapia 2003, 74, 317–319. [Google Scholar] [CrossRef] [PubMed]
- Badgujar, S.B.; Patel, V.V.; Bandivdekar, A.H. Foeniculum vulgare Mill: A Review of Its Botany, Phytochemistry, Pharmacology, Contemporary Application, and Toxicology. BioMed Res. Int. 2014, 2014, 1–32. [Google Scholar] [CrossRef]
- Poornima, P.; Kumar, J.D.; Zhao, Q.; Blunder, M.; Efferth, T. Network pharmacology of cancer: From understanding of complex interactomes to the design of multi-target specific therapeutics from nature. Pharmacol. Res. 2016, 111, 290–302. [Google Scholar] [CrossRef] [PubMed]
- Lee, W.Y.; Lee, C.Y.; Kim, Y.S.; Kim, C.E. The Methodological Trends of Traditional Herbal Medicine Employing Network Pharmacology. Biomolecules 2019, 9, 362. [Google Scholar] [CrossRef] [PubMed]
- He, R.; Ou, S.; Chen, S.; Ding, S. Network Pharmacology-Based Study on the Molecular Biological Mechanism of Action for Compound Kushen Injection in Anti-Cancer Effect. Med. Sci. Monit. 2020, 26. [Google Scholar] [CrossRef]
- Mi, J.L.; Liu, C.; Xu, M.; Wang, R.S. Network Pharmacology to Uncover the Molecular Mechanisms of Action of LeiGongTeng for the Treatment of Nasopharyngeal Carcinoma. Med. Sci. Monit. 2020, 26. [Google Scholar] [CrossRef] [PubMed]
- Wang, Y.; Dong, B.; Xue, W.; Feng, Y.; Yang, C.; Liu, P.; Cao, J.; Zhu, C. Anticancer Effect of Radix Astragali on Cholangiocarcinoma In Vitro and Its Mechanism via Network Pharmacology. Med. Sci. Monit. 2020, 26. [Google Scholar] [CrossRef]
- Xu, T.; Wang, Q.; Liu, M. 2020. A Network Pharmacology Approach to Explore the Potential Mechanisms of Huangqin-Baishao Herb Pair in Treatment of Cancer. Med. Sci. Monit. 2020, 26. [Google Scholar] [CrossRef]
- Zhang, S.Q.; Xu, H.B.; Zhang, S.J.; Li, X.Y. Identification of the Active Compounds and Significant Pathways of Artemisia Annua in the Treatment of Non-Small Cell Lung Carcinoma based on Network Pharmacology. Med. Sci. Monit. 2020, 26. [Google Scholar] [CrossRef]
- Lee, H.S.; Lee, I.H.; Park, S.I.; Lee, D.Y. Network Pharmacology-Based Investigation of the System-Level Molecular Mechanisms of the Hematopoietic Activity of Samul-Tang, a Traditional Korean Herbal Formula. Evid. Based Complementary Altern. Med. 2020, 2020, 1–17. [Google Scholar] [CrossRef]
- Hu, Z.; Yang, M.; Yang, L.; Xie, C.; Gao, H.; Fu, X.; Xie, H.; Liu, Y. Network Pharmacology-Based Identification of the Mechanisms of Shen-Qi Compound Formula in Treating Diabetes Mellitus. Evid. Based Complementary Altern. Med. 2020, 2020, 1–15. [Google Scholar]
- Jiang, Y.; Zhong, M.; Long, F.; Yang, R. Deciphering the Active Ingredients and Molecular Mechanisms of Tripterygium hypoglaucum (Levl.) Hutch against Rheumatoid Arthritis Based on Network Pharmacology. Evid. Based Complementary Altern. Med. 2020, 2020, 1–9. [Google Scholar]
- Li, D.H.; Su, Y.F.; Sun, C.X.; Fan, H.F.; Gao, W.J. A Network Pharmacology-Based Identification Study on the Mechanism of Xiao-Xu-Ming Decoction for Cerebral Ischemic Stroke. Evid. Based Complementary Altern. Med. 2020, 2020, 1–8. [Google Scholar]
- Liu, W.; Fan, Y.; Tian, C.; Jin, Y.; Du, S.; Zeng, P.; Wang, A. Deciphering the Molecular Targets and Mechanisms of HGWD in the Treatment of Rheumatoid Arthritis via Network Pharmacology and Molecular Docking. Evid. Based Complementary Altern. Med. 2020, 2020, 1–13. [Google Scholar]
- Qian, H.; Jin, Q.; Liu, Y.; Wang, N.; Chu, Y.; Liu, B.; Liu, Y.; Jiang, W.; Song, Y. Study on the Multitarget Mechanism of Sanmiao Pill on Gouty Arthritis Based on Network Pharmacology. Evid. Based Complementary Altern. Med. 2020, 2020, 1–11. [Google Scholar]
- Ren, B.; Tan, L.; Xiong, Y.; Ji, W.; Mu, J.; Pei, Y.; Cheng, F.; Wang, X.; Wang, Q. Integrated Analysis of the Mechanisms of Da-Chai-Hu Decoction in Type 2 Diabetes Mellitus by a Network Pharmacology Approach. Evid. Based Complementary Altern. Med. 2020, 2020, 1–21. [Google Scholar]
- Wang, W.; Zhang, Y.; Luo, J.; Wang, R.; Tang, C.; Zhang, Y.; Borgatti, M. Virtual Screening Technique Used to Estimate the Mechanism of Adhatoda vasica Nees for the Treatment of Rheumatoid Arthritis Based on Network Pharmacology and Molecular Docking. Evid. Based Complementary Altern. Med. 2020, 2020, 1–12. [Google Scholar]
- Xiao, K.; Li, K.; Long, S.; Kong, C.; Zhu, S. 2020. Potential Molecular Mechanisms of Chaihu-Shugan-San in Treatment of Breast Cancer Based on Network Pharmacology. Evid. Based Complementary Altern. Med. 2020, 2020, 1–9. [Google Scholar]
- Yang, K.; Zeng, L.; Ge, J. Exploring the Pharmacological Mechanism of Danzhi Xiaoyao Powder on ER-Positive Breast Cancer by a Network Pharmacology Approach. Evid. Based Complementary Altern. Med. 2018, 2018, 1–20. [Google Scholar]
- Zhang, C.; Liao, Y.; Liu, L.; Sun, Y.; Lin, S.; Lan, J.; Mao, H.; Chen, H.; Zhao, Y. A Network Pharmacology Approach to Investigate the Active Compounds and Mechanisms of Musk for Ischemic Stroke. Evid. Based Complementary Altern. Med. 2020, 2020, 1–14. [Google Scholar]
- Zhou, J.; Wang, Q.; Xiang, Z.; Tong, Q.; Pan, J.; Wan, L.; Chen, J. Network Pharmacology Analysis of Traditional Chinese Medicine Formula Xiao Ke Yin Shui Treating Type 2 Diabetes Mellitus. Evid. Based Complementary Altern. Med. 2019, 2019, 1–15. [Google Scholar] [CrossRef] [PubMed]
- Ru, J.; Li, P.; Wang, J.; Zhou, W.; Li, B.; Huang, C.; Li, P.; Guo, Z.; Tao, W.; Yang, Y.; et al. TCMSP: a database of systems pharmacology for drug discovery from herbal medicines. J. Cheminform. 2014, 6, 13. [Google Scholar] [CrossRef] [PubMed]
- The UniProt Consortium. UniProt: a worldwide hub of protein knowledge. Nucleic Acids Res. 2019, 47, D506–D515. [Google Scholar] [CrossRef] [PubMed]
- Shannon, P.; Markiel, A.; Ozier, O.; Baliga, N.S.; Wang, J.T.; Ramage, D.; Amin, N.; Schwikowski, B.; Ideker, T. Cytoscape: A Software Environment for Integrated Models of Biomolecular Interaction Networks. Genome Res. 2003, 13, 2498–2504. [Google Scholar] [CrossRef] [PubMed]
- Doncheva, N.T.; Morris, J.H.; Gorodkin, J.; Jensen, L.J. Cytoscape StringApp: Network Analysis and Visualization of Proteomics Data. J. Proteome Res. 2019, 18, 623–632. [Google Scholar] [CrossRef] [PubMed]
- Reagan-Shaw, S.; Nihal, M.; Ahmad, N. Dose translation from animal to human studies revisited. FASEB J. 2008, 22, 659–661. [Google Scholar] [CrossRef] [PubMed]
- Ekor, M. The growing use of herbal medicines: issues relating to adverse reactions and challenges in monitoring safety. Front. Pharmacol. 2014, 4, 177. [Google Scholar] [CrossRef]
- Huang, W.; Zhang, J.; Moore, D.D. A traditional herbal medicine enhances bilirubin clearance by activating the nuclear receptor CAR. J. Clin. Invest. 2004, 113, 137–143. [Google Scholar] [CrossRef]
- Asano, T.; Aida, S.; Suemasu, S.; Mizushima, T. Anethole restores delayed gastric emptying and impaired gastric accommodation in rodents. Biochem. Biophys. Res. Commun. 2016, 472, 125–130. [Google Scholar] [CrossRef]
- Scarpignato, C.; Capovilla, T.; Bertaccini, G. Action of caerulein on gastric emptying of the conscious rat. Arch. Int. Pharmacodyn. Ther. 1980, 246, 286–294. [Google Scholar]
- Nunes Marona, H.R.; Bastos Lucchesi, M.B. Protocol to refine intestinal motility test in mice. Lab Anim 2004, 38, 257–260. [Google Scholar] [CrossRef] [PubMed]
- Mittelstadt, S.W.; Hemenway, C.L.; Spruell, R.D. Effects of fasting on evaluation of gastrointestinal transit with charcoal meal. J. Pharmacol. Toxicol. Methods 2005, 52, 154–158. [Google Scholar] [CrossRef] [PubMed]
- El-Soud, N.A.; El-Laithy, N.; El-Saeed, G.; Wahby, M.S.; Khalil, M.; Morsy, F.; Shaffie, N. Antidiabetic Activities of Foeniculum vulgare Mill. Essential Oil in Streptozotocin-Induced Diabetic Rats 8. Maced. J. Med. Sci. 2011, 4, 1–8. [Google Scholar]
- Malini, T.; Vanithakumari, G.; Megala, N.; Anusya, S.; Devi, K.; Elango, V. Effect of Foeniculum vulgare Mill. seed extract on the genital organs of male and female rats. Indian J. Physiol. Pharmacol. 1985, 29, 21–26. [Google Scholar] [PubMed]
- Oktay, M.; Gülçin, İ.; Küfrevioğlu, Ö.İ. Determination of in vitro antioxidant activity of fennel (Foeniculum vulgare) seed extracts. LWT - Food Sci. Technol. 2003, 36, 263–271. [Google Scholar] [CrossRef]
- Pradhan, M.; Sribhuwaneswari, S.; Karthikeyan, D.; Minz, S.; Sure, P.; Chandu, A.N.; Mishra, U.; Kamalakannan, K.; Saravanankumar, A.; Sivakumar, T. 2008. In-vitro Cytoprotection Activity of Foeniculum vulgare and Helicteres isora in Cultured Human Blood Lymphocytes and Antitumour Activity against B16F10 Melanoma Cell Line. Research J. Pharm. And Tech. 2008, 1, 450–452. [Google Scholar]
- Orhan, İl. E.; Özçeli̇K, B.; Kartal, M.; Kan, Y. 2012. Antimicrobial and antiviral effects of essential oils from selected Umbelliferae and Labiatae plants and individual essential oil components. Turk. J. Biol. 2012, 36, 239–246. [Google Scholar]
- Thaler, K.; Kaminski, A.; Chapman, A.; Langley, T.; Gartlehner, G. Bach Flower Remedies for psychological problems and pain: a systematic review. BMC Complement. Altern. Med. 2009, 9, 16. [Google Scholar] [CrossRef]
- Morales, P.; Carvalho, A.M.; Sánchez-Mata, M.C.; Cámara, M.; Molina, M.; Ferreira, I.C.F.R. 2012. Tocopherol composition and antioxidant activity of Spanish wild vegetables. Genet. Resour. Crop. Evol. 2012, 59, 851–863. [Google Scholar] [CrossRef]
- Birdane, F.M.; Cemek, M.; Birdane, Y.O.; Gülçin, I.; Büyükokuroğlu, M.E. Beneficial effects of Foeniculum vulgare on ethanol-induced acute gastric mucosal injury in rats. World J. Gastroenterol. 2007, 13, 607–611. [Google Scholar] [CrossRef]
- Chakŭrski, I.; Matev, M.; Koĭchev, A.; Angelova, I.; Stefanov, G. Treatment of chronic colitis with an herbal combination of Taraxacum officinale, Hipericum perforatum, Melissa officinaliss, Calendula officinalis and Foeniculum vulgare. Vutr. Boles 1981, 20, 51–54. [Google Scholar] [PubMed]
- Chan, F.K.; To, K.F.; Ng, Y.P.; Lee, T.L.; Cheng, A.S.; Leung, W.K.; Sung, J.J. Expression and cellular localization of COX-1 and -2 in Helicobacter pylori gastritis. Aliment. Pharmacol. Ther. 2001, 15, 187–193. [Google Scholar] [CrossRef] [PubMed]
- Vane, J.R.; Bakhle, Y.S.; Botting, R.M. Cyclooxygenases 1 and 2. Annu. Rev. Pharmacol. Toxicol. 1998, 38, 97–120. [Google Scholar] [CrossRef] [PubMed]
- Wallace, J.L.; Devchand, P.R. 2005. Emerging roles for cyclooxygenase-2 in gastrointestinal mucosal defense. Br. J. Pharmacol. 2005, 145, 275–282. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.C.; van Citters, G.W.; Heimer, F.; Bonorris, G. Slowing of gastrointestinal transit by oleic acid: a preliminary report of a novel, nutrient-based treatment in humans. Dig. Dis. Sci. 2001, 46, 223–229. [Google Scholar] [CrossRef] [PubMed]
- Ding, K.; Tan, Y.; Ding, Y.; Fang, Y.; Yang, X.; Fang, J.; Xu, D.; Zhang, H.; Lu, W.; Li, M.; et al. β-Sitosterol improves experimental colitis in mice with a target against pathogenic bacteria. J. Cell. Biochem. 2019, 120, 5687–5694. [Google Scholar] [CrossRef]
- Lee, M.C.; Ha, W.; Park, J.; Kim, J.; Jung, Y.; Kim, B.J. Effects of Lizhong Tang on gastrointestinal motility in mice. World J. Gastroenterol. 2016, 22, 7778. [Google Scholar] [CrossRef]
- Hafeez, M.; Hussain, F.; Salamat, A.; Khan, M.B. Gastric emptying scintigraphy in postprandial distress syndrome. Pak. J. Med. Sci. 2018, 34. [Google Scholar] [CrossRef]
- Quarter, A.O.; De Wit, N.J.; Lodder, A.C.; Numans, M.E.; Smout, A.J.P.M.; Hoes, A.W. Disturbed Solid-Phase Gastric Emptying in Functional Dyspepsia (A Meta-Analysis). Dig. Dis. Sci. 1998, 43, 2028–2033. [Google Scholar] [CrossRef]
- Futagami, S.; Yamawaki, H.; Shimpuku, M.; Izumi, N.; Wakabayashi, T.; Kodaka, Y.; Nagoya, H.; Shindo, T.; Kawagoe, T.; Sakamoto, C. Impact of Coexisting Irritable Bowel Syndrome and Non-erosive Reflux Disease on Postprandial Abdominal Fullness and Sleep Disorders in Functional Dyspepsia. J. Nippon. Med. Sch. 2013, 80, 362–370. [Google Scholar] [CrossRef]
- Kaji, M.; Fujiwara, Y.; Shiba, M.; Kohata, Y.; Yamagami, H.; Tanigawa, T.; Watanabe, K.; Watanabe, T.; Tominaga, K.; Arakawa, T. Prevalence of overlaps between GERD, FD and IBS and impact on health-related quality of life: Overlap of FGIDs and HR-QOL. J. Gastroenterol. Hepatol. 2010, 25, 1151–1156. [Google Scholar] [CrossRef] [PubMed]
- Choi, Y.J.; Kim, N.; Yoon, H.; Shin, C.M.; Park, Y.S.; Kim, J.W.; Kim, Y.S.; Lee, D.H.; Jung, H.C. Overlap between irritable bowel syndrome and functional dyspepsia including subtype analyses: Overlap of IBS and dyspepsia. J. Gastroenterol. Hepatol. 2017, 32, 1553–1561. [Google Scholar] [CrossRef] [PubMed]
- Terauchi, A.; Kobayashi, D.; Mashimo, H. Distinct roles of nitric oxide synthases and interstitial cells of Cajal in rectoanal relaxation. Am. J. Physiol. Gastrointest. Liver Physiol. 2005, 289, G291–G299. [Google Scholar] [CrossRef] [PubMed]
- Park, J.M.; Baeg, M.K.; Lim, C.H.; Cho, Y.K.; Choi, M.G. Nitric Oxide Synthase Gene Polymorphisms in Functional Dyspepsia. Dig. Dis. Sci. 2014, 59, 72–77. [Google Scholar] [CrossRef] [PubMed]
- Gomez-Pinilla, P.J.; Gibbons, S.J.; Bardsley, M.R.; Lorincz, A.; Pozo, M.J.; Pasricha, P.J.; de Rijn, M.V.; West, R.B.; Sarr, M.G.; Kendrick, M.L.; et al. Ano1 is a selective marker of interstitial cells of Cajal in the human and mouse gastrointestinal tract. Am. J. Physiol. Gastrointest. Liver Physiol. 2009, 296, G1370–G1381. [Google Scholar] [CrossRef]
- Sanders, K.M.; Hwang, S.J.; Ward, S.M. Neuroeffector apparatus in gastrointestinal smooth muscle organs: Neural regulation of GI smooth muscle. J. Physiol. 2010, 588, 4621–4639. [Google Scholar] [CrossRef]
- Imaizumi, Y.; Torii, Y.; Ohi, Y.; Nagano, N.; Atsuki, K.; Yamamura, H.; Muraki, K.; Watanabe, M.; Bolton, T.B. Ca2+ images and K+ current during depolarization in smooth muscle cells of the guinea-pig vas deferens and urinary bladder. J. Physiol. 1998, 510, 705–719. [Google Scholar] [CrossRef]
- Liu, H.N.; Ohya, S.; Wang, J.; Imaizumi, Y.; Nakayama, S. Involvement of ryanodine receptors in pacemaker Ca2+ oscillation in murine gastric ICC. Biochem. Biophys. Res. Commun. 2005, 328, 640–646. [Google Scholar] [CrossRef]
- He, W.; Peng, Y.; Zhang, W.; Lv, N.; Tang, J.; Chen, C.; Zhang, C.; Gao, S.; Chen, H.; Zhi, G.; et al. Myosin Light Chain Kinase Is Central to Smooth Muscle Contraction and Required for Gastrointestinal Motility in Mice. Gastroenterology 2008, 135, 610–620.e2. [Google Scholar] [CrossRef]
- Hu, W.; Feng, P. Myosin Light Chain Kinase Is Involved in the Mechanism of Gastrointestinal Dysfunction in Diabetic Rats. Dig. Dis. Sci. 2012, 57, 1197–1202. [Google Scholar] [CrossRef]
- Mazzone, A.; Bernard, C.E.; Strege, P.R.; Beyder, A.; Galietta, L.J.V.; Pasricha, P.J.; Rae, J.L.; Parkman, H.P.; Linden, D.R.; Szurszewski, J.H.; et al. Altered Expression of Ano1 Variants in Human Diabetic Gastroparesis. J. Biol. Chem. 2011, 286, 13393–13403. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
The study protocol schematic.
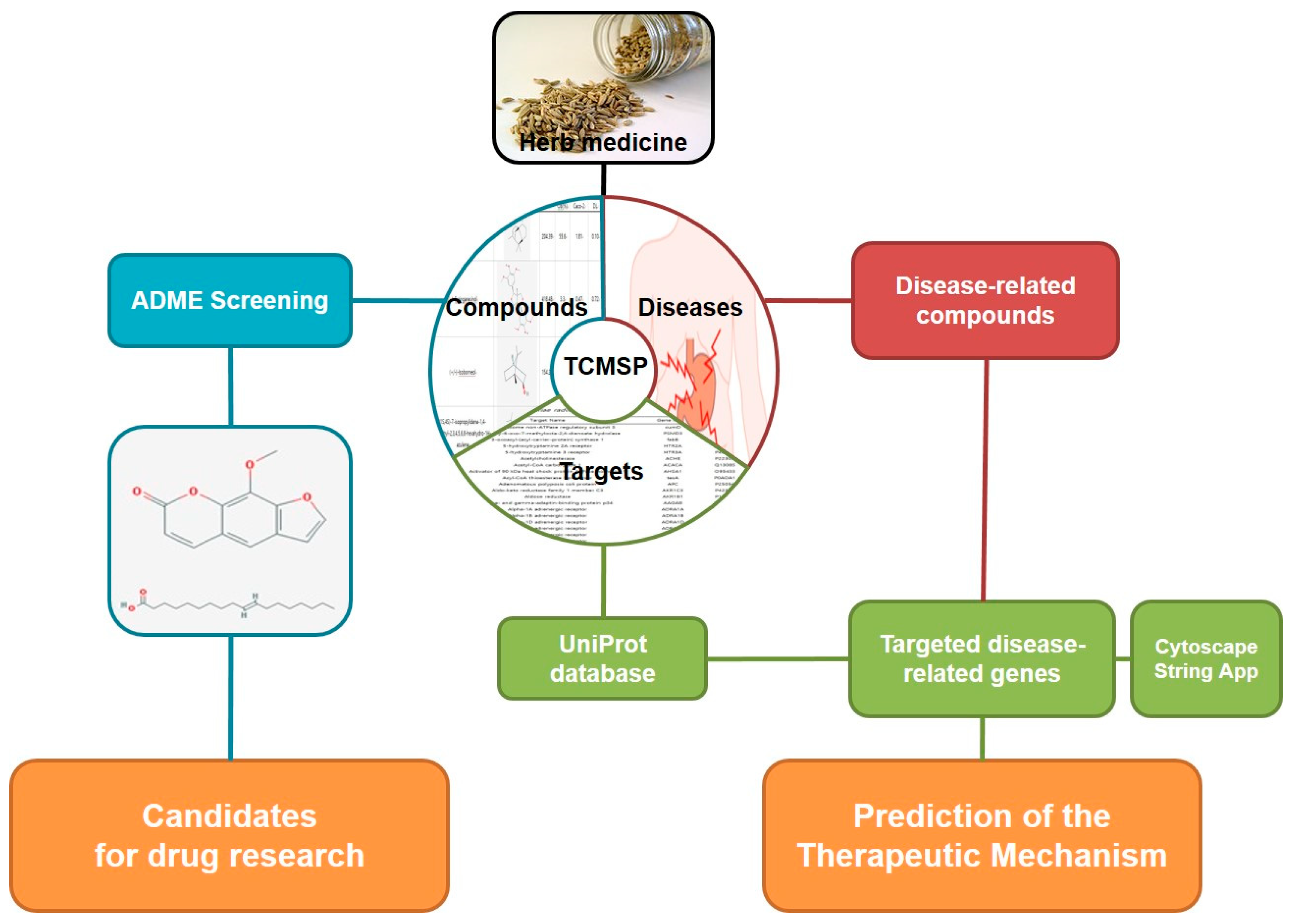
Figure 2.
UPLC profiles of 3 major compounds identified in F. fructus. (A) UPLC profile of the commercial standard compounds. (B) UPLC profile of 3 major compounds in F. fructus. 4-Methoxybenzoic acid and R-(a)-phellandrene were analyzed at 330 nm, and the anethole was analyzed at 306 nm.
Figure 2.
UPLC profiles of 3 major compounds identified in F. fructus. (A) UPLC profile of the commercial standard compounds. (B) UPLC profile of 3 major compounds in F. fructus. 4-Methoxybenzoic acid and R-(a)-phellandrene were analyzed at 330 nm, and the anethole was analyzed at 306 nm.
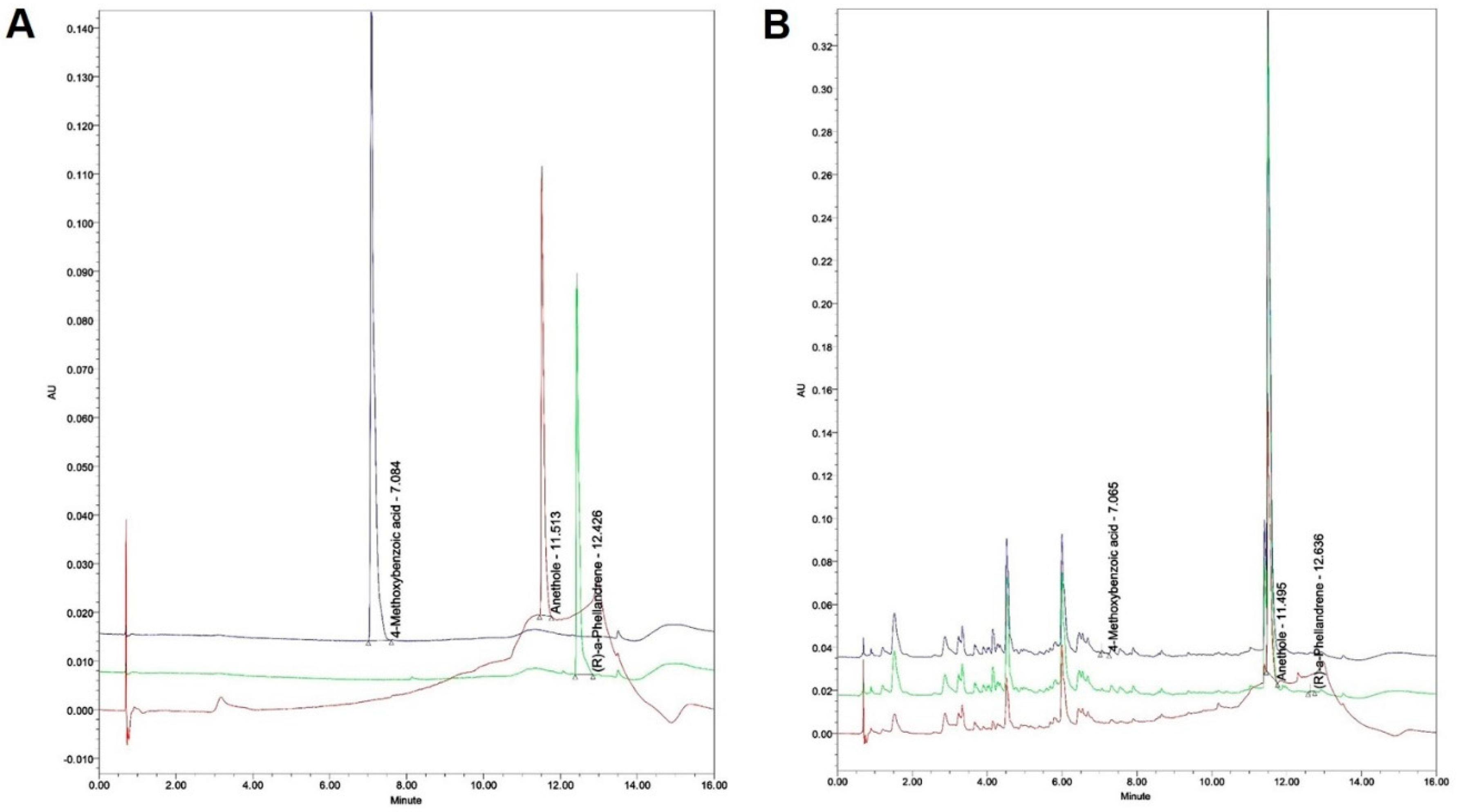
Figure 3.
Compound-target network of F. fructus. The node size depends on the number of connected edges. The compound is represented as a red square-shaped node, and the targets are represented as a blue round-shaped node.
Figure 3.
Compound-target network of F. fructus. The node size depends on the number of connected edges. The compound is represented as a red square-shaped node, and the targets are represented as a blue round-shaped node.
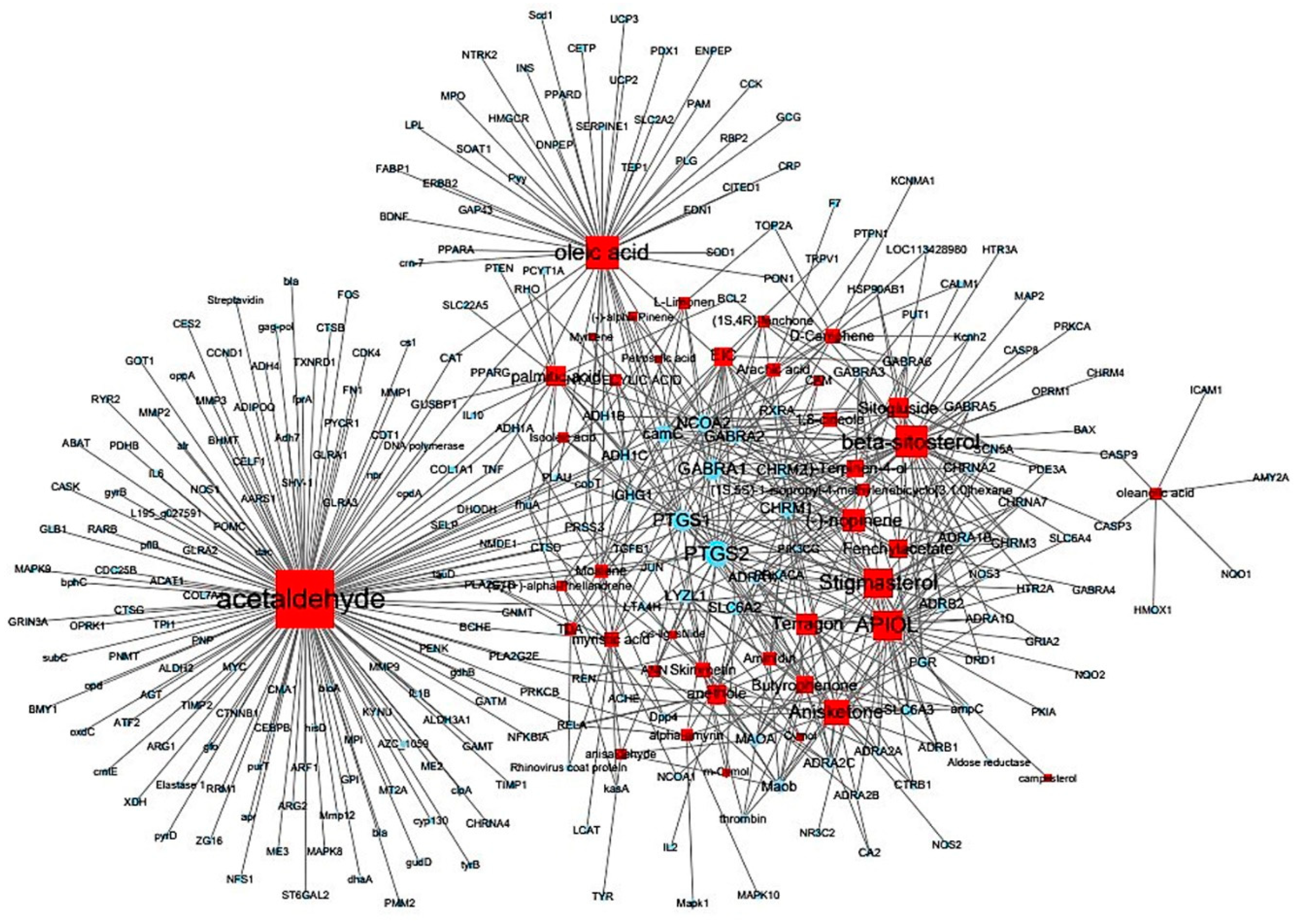
Figure 4.
The Venn diagram of active compounds and GI disease-related compounds of F. fructus.
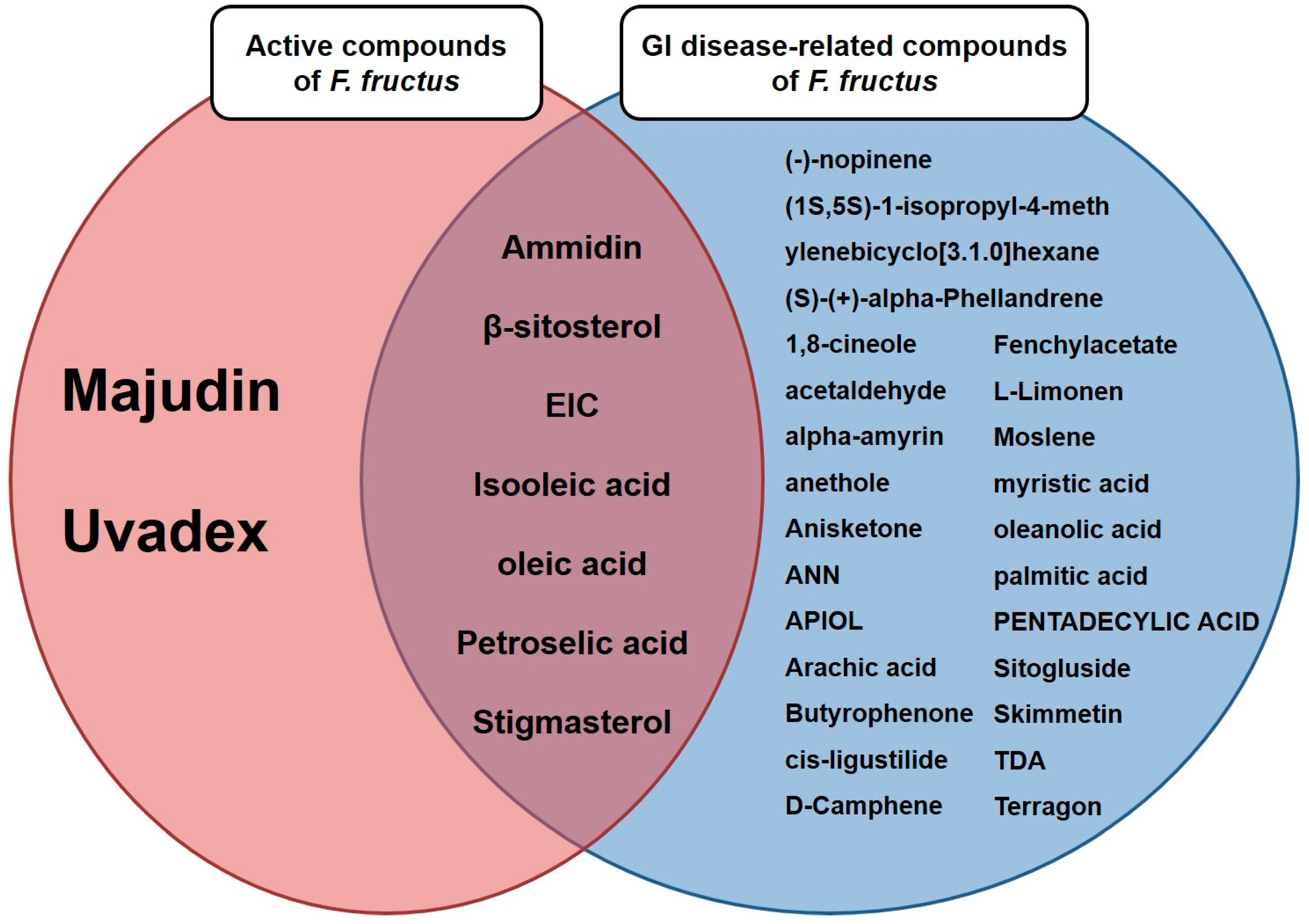
Figure 5.
Network of functional dyspepsia related genes and F. fructus target genes. The 12 genes included in both "gene related to functional dyspepsia" and "F. fructus target genes" were collected in the center.
Figure 5.
Network of functional dyspepsia related genes and F. fructus target genes. The 12 genes included in both "gene related to functional dyspepsia" and "F. fructus target genes" were collected in the center.
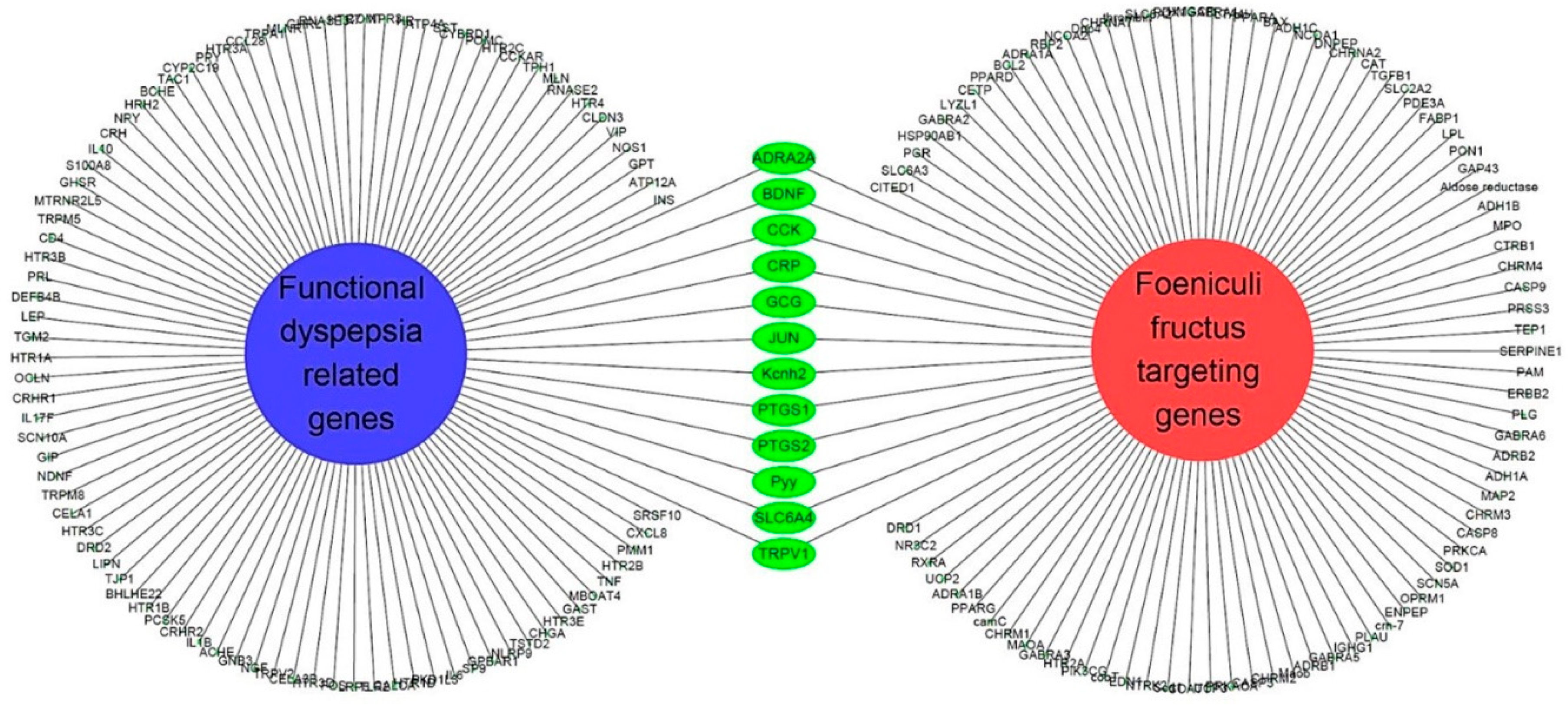
Figure 7.
Results of F. fructus (FF) on gastric emptying. The experimental schedule is summarized in (A). For 3 days, mice (n = 6/group) were treated by po with 25, 50, and 100 mg/kg of FF or 3 mg/kg of mosapride and then treated by IP injection with 10 mg/kg of loperamide. After the treatment of phenol red, results of visualization (B), weight of stomach (C), and results of gastric emptying (D) are presented. The data are organized as the mean ± SEM. *p < 0.05, **p < 0.01 for the Control group; #p < 0.05 for the loperamide group.
Figure 7.
Results of F. fructus (FF) on gastric emptying. The experimental schedule is summarized in (A). For 3 days, mice (n = 6/group) were treated by po with 25, 50, and 100 mg/kg of FF or 3 mg/kg of mosapride and then treated by IP injection with 10 mg/kg of loperamide. After the treatment of phenol red, results of visualization (B), weight of stomach (C), and results of gastric emptying (D) are presented. The data are organized as the mean ± SEM. *p < 0.05, **p < 0.01 for the Control group; #p < 0.05 for the loperamide group.
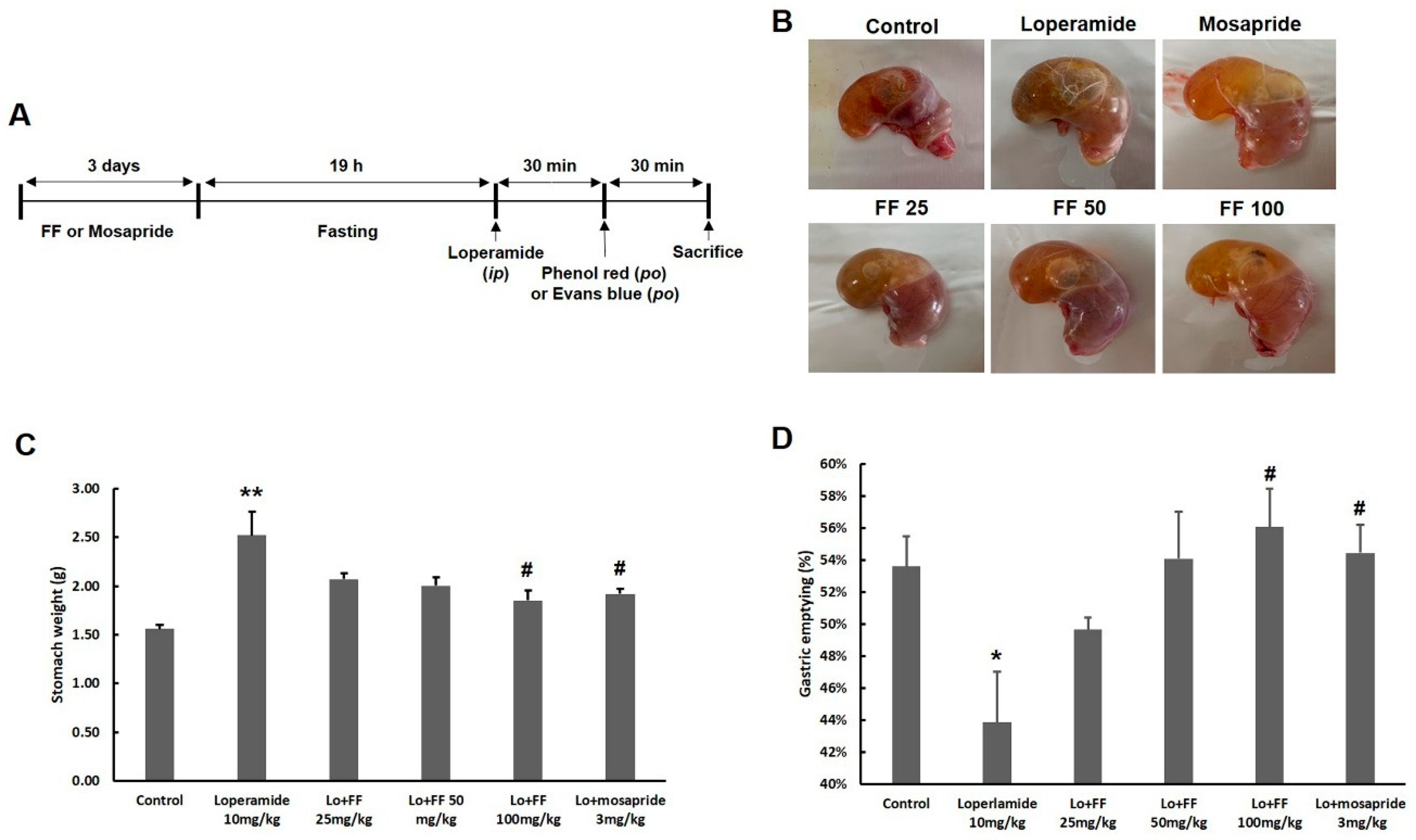
Figure 8.
Results of F. fructus (FF) on GI motility-associated molecules in stomach tissue. The analyses of western blot for nNOS, TMEM16A, and TRPM7 (A) and semi-quantifications (B) were conducted (n = 3). The analyses of mRNA expression of GI motility-associated genes were performed (C) (n = 3) in the stomach tissue. The data are organized as the mean ± SEM. *p < 0.05, ***p < 0.001 for the Control group; #p < 0.05, ##p < 0.01, ###p < 0.001 for the loperamide group.
Figure 8.
Results of F. fructus (FF) on GI motility-associated molecules in stomach tissue. The analyses of western blot for nNOS, TMEM16A, and TRPM7 (A) and semi-quantifications (B) were conducted (n = 3). The analyses of mRNA expression of GI motility-associated genes were performed (C) (n = 3) in the stomach tissue. The data are organized as the mean ± SEM. *p < 0.05, ***p < 0.001 for the Control group; #p < 0.05, ##p < 0.01, ###p < 0.001 for the loperamide group.
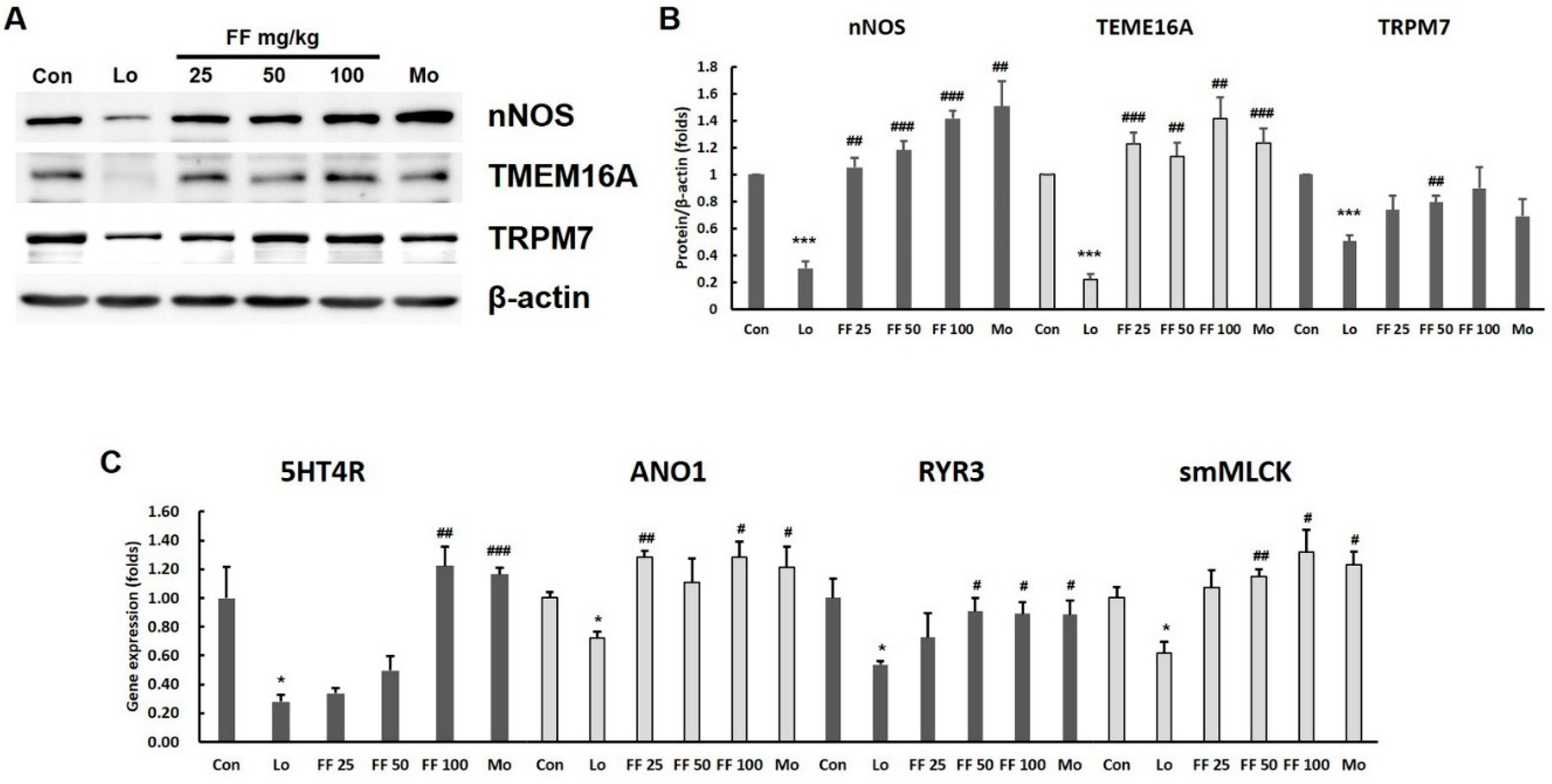
Figure 9.
Results of F. fructus (FF) on small intestinal motility. For 3 days, mice (n = 6/group) were treated by po with 25, 50, and 100 mg/kg of FF or 3 mg/kg of mosapride and then treated by IP injection with 10 mg/kg of loperamide. After 30 min of treatment with Evans blue, the distances stained were checked and quantified. The data are organized as the mean ± SEM. ***p < 0.001 for the Control group; ###p < 0.001 for the loperamide group.
Figure 9.
Results of F. fructus (FF) on small intestinal motility. For 3 days, mice (n = 6/group) were treated by po with 25, 50, and 100 mg/kg of FF or 3 mg/kg of mosapride and then treated by IP injection with 10 mg/kg of loperamide. After 30 min of treatment with Evans blue, the distances stained were checked and quantified. The data are organized as the mean ± SEM. ***p < 0.001 for the Control group; ###p < 0.001 for the loperamide group.
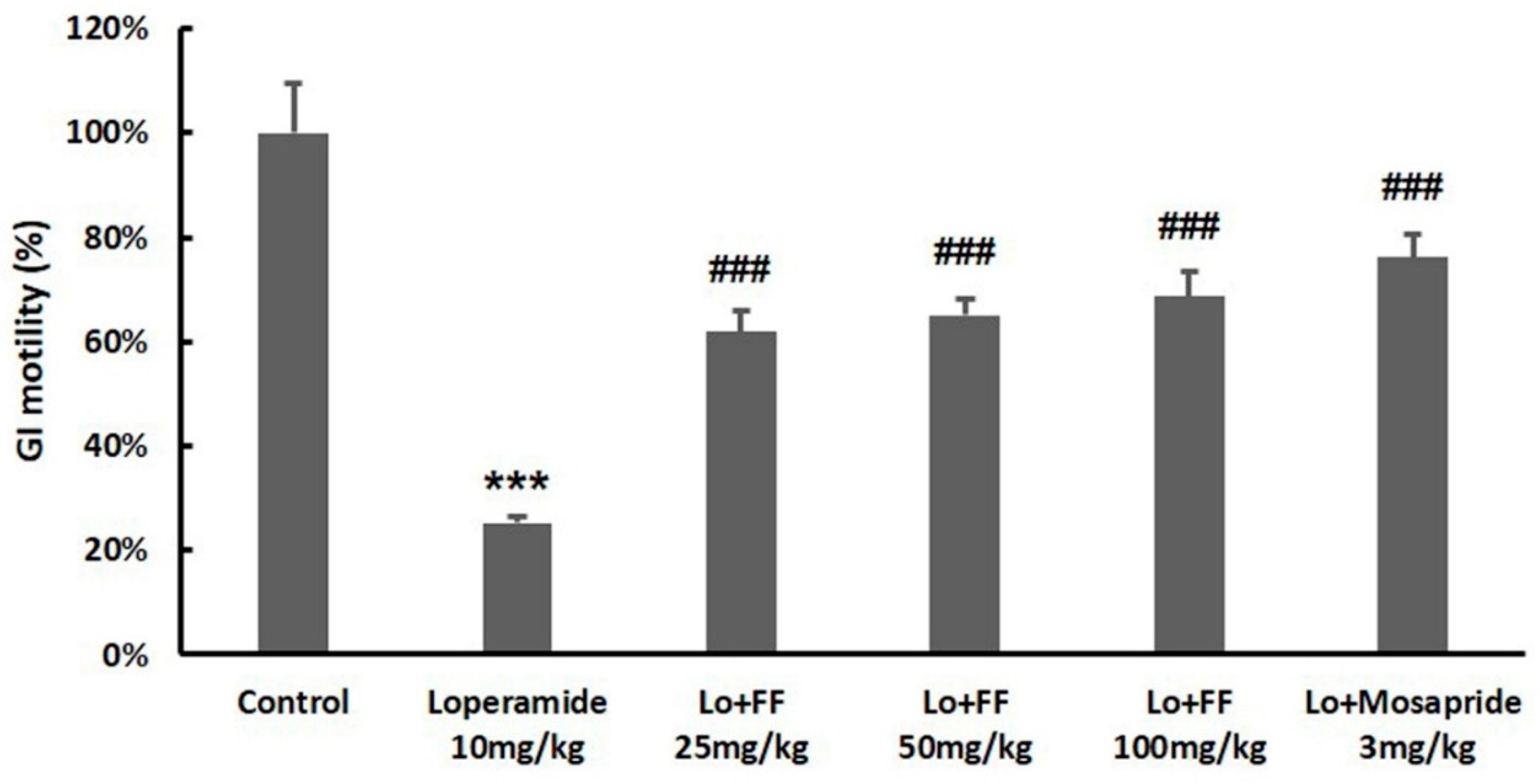

Table 1.
The analysis condition of 4-Methoxybenzoic acid, Anethole, and R-(α)-Phellandrene.
| Time (minute) | 0.1% FA/water (%) | 0.1% FA/acetonitrile (%) | Flow rate (ml/minute) |
|---|---|---|---|
| 0 | 98 | 2 | 0.40 |
| 1.0 | 98 | 2 | 0.40 |
| 3.0 | 85 | 15 | 0.40 |
| 5.0 | 75 | 25 | 0.40 |
| 6.0 | 55 | 45 | 0.40 |
| 8.0 | 50 | 50 | 0.40 |
| 9.0 | 30 | 70 | 0.40 |
| 10.0 | 10 | 90 | 0.40 |
| 12.0 | 2 | 98 | 0.40 |
| 14.0 | 98 | 2 | 0.40 |
| 16.0 | 98 | 2 | 0.40 |
Table 2.
Contents of the F. fructus marker compounds by UPLC.
| F. fructus (Unit: mg/kg) | |||
|---|---|---|---|
| 4-Methoxybenzoic acid | 0.219± 0.042 | ||
| Anethole | 63.029 ± 2.076 | ||
| R-(a)-Phellandrene | 0.792 ± 0.059 | ||
Table 3.
Summary for gene sequence.
| Gene | Primer | Sequence (5' to 3') | Product length (bp) |
|---|---|---|---|
| 5HT4R | Forward | AGTTCCAACGAGGGTTTCAGG | 92 |
| Reverse | CAGCAGGTTGCCCAAGATG | ||
| ANO1 | Forward | GGCATTTGTCATTGTCTTCCAG | 140 |
| Reverse | TCCTCACGCATAAACAGCTC | ||
| RYR3 | Forward | GGCCAAGAACATCAGAGTGACTAA | 79 |
| Reverse | TCACTTCTGCCCTGTCAGTTTC | ||
| smMLCK | Forward | AGAAGTCAAGGAGGTAAAGAATGATGT | 76 |
| Reverse | CGGGTCGCTTTTCATTGC | ||
| GAPDH | Forward | CATGGCCTTCCGTGTTCCT | 103 |
| Reverse | CCTGCTTCACCACCTTCTTGA |
Table 4.
Active compounds of F. fructus.
| Molecule Name | Structure | MW | OB(%) | Caco-2 | DL |
|---|---|---|---|---|---|
| Ammidin* | 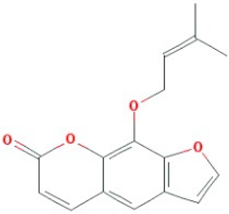 |
270.3 | 34.55 | 1.13 | 0.22 |
| beta-sitosterol | 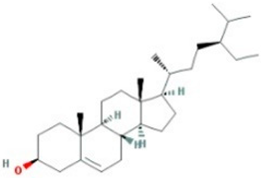 |
414.79 | 36.91 | 1.32 | 0.75 |
| EIC | 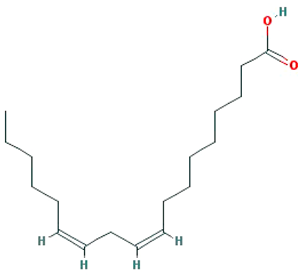 |
280.5 | 41.9 | 1.16 | 0.14 |
| Isooleic acid |  |
282.52 | 33.13 | 1.15 | 0.14 |
| Majudin |  |
216.2 | 42.21 | 0.94 | 0.13 |
| oleic acid |  |
282.52 | 33.13 | 1.17 | 0.14 |
| Petroselic acid |  |
282.52 | 33.13 | 1.17 | 0.14 |
| Stigmasterol |  |
412.77 | 43.83 | 1.44 | 0.76 |
| Uvadex |  |
216.2 | 35.3 | 1.05 | 0.13 |
Table 5.
Compounds and targets related to GI diseases.
| Molecule name | Gene name | Disease name |
|---|---|---|
| (-)-nopinene | PTGS1 | *Functional dyspepsia |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| (1S,5S)-1-isopropyl-4 -methylenebicyclo [3.1.0]hexane |
PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
| (S)-(+)-alpha-Phellandrene | ACHE | *Functional dyspepsia |
| 1,8-cineole | NOS3 | Colorectal cancer |
| PTGS2 | *Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| acetaldehyde |
BCHE | *Functional dyspepsia |
| CTNNB1 | Colorectal cancer | |
| FOS | *Functional dyspepsia | |
| IL1B | *Functional dyspepsia | |
| IL6 | *Functional dyspepsia | |
| JUN | *Functional dyspepsia | |
| LTA4H | Oesophageal cancer | |
| MAPK8 | Crohns's Disease, unspecified | |
| MAPK9 | Crohns's Disease, unspecified | |
| MMP1 |
Kaposi's Sarcoma Pancreatic Cancer |
|
| Mmp12 |
Crohns's Disease, unspecified Gastro-intestinal ulcers Ulcerative colitis |
|
| MMP2 |
Kaposi's Sarcoma Pancreatic Cancer |
|
| MMP3 | Pancreatic Cancer | |
| NOS1 | *Functional dyspepsia | |
| OPRK1 | Diarrhea | |
| POMC | *Functional dyspepsia | |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| RARB | Pancreatic Cancer | |
| RRM1 | Pancreatic Neoplasms | |
| TNF |
*Functional dyspepsia Crohns's Disease, unspecified |
|
| alpha-amyrin | PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
| Ammidin | PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
| anethole | JUN | *Functional dyspepsia |
| Anisketone | ACHE | *Functional dyspepsia |
| ADRA2A | *Functional dyspepsia | |
| CA2 | Pancreatic Cancer | |
| NOS3 | Colon cancer | |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| ANN | PTGS1 | *Functional dyspepsia |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| APIOL | ADRA2A | *Functional dyspepsia |
| LTA4H | Oesophageal cancer | |
| NOS3 | Colon cancer | |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| SLC6A4 | *Functional dyspepsia | |
| Arachic acid | HSP90AB1 | Gastrointestinal Stromal Tumors (GIST) |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| beta-sitosterol | HSP90AB1 | Gastrointestinal Stromal Tumors (GIST) |
| JUN | *Functional dyspepsia | |
| Kcnh2 | *Functional dyspepsia | |
| OPRM1 |
Diarrhea Opioid-induced bowel dysfunction |
|
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| SLC6A4 | *Functional dyspepsia | |
| Butyrophenone | CA2 | Pancreatic Cancer |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| cis-ligustilide | PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
| D-Camphene | Kcnh2 | *Functional dyspepsia |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| EIC | PTGS1 | *Functional dyspepsia |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| TRPV1 | *Functional dyspepsia | |
| Fenchylacetate | PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
| Isooleic acid |
PTGS1 | *Functional dyspepsia |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| L-Limonen | PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
| Moslene | ACHE | *Functional dyspepsia |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| myristic acid | BCHE | *Functional dyspepsia |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| oleanolic acid | AMY2A | Pancreatic disease |
| oleic acid | BDNF | *Functional dyspepsia |
| CCk | *Functional dyspepsia | |
| CRP | *Functional dyspepsia | |
| GCG | *Functional dyspepsia | |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 | *Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| Pyy | *Functional dyspepsia | |
| palmitic acid | IL10 | *Functional dyspepsia |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 |
*Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| TNF | *Functional dyspepsia Crohns's Disease, unspecified |
|
| PENTADECYLIC ACID | PTGS1 | *Functional dyspepsia |
| PTGS2 | *Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| Petroselic acid | PTGS1 | *Functional dyspepsia |
| Sitogluside | HSP90AB1 | Gastrointestinal Stromal Tumors (GIST) |
| HTR3A | *Functional dyspepsia Chemotherapy-induced nausea and vomiting Diarrhea Irritable bowel syndrome Postoperative nausea and vomiting |
|
| Kcnh2 | *Functional dyspepsia | |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 | *Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| Skimmetin | ADRA2A | *Functional dyspepsia |
| LTA4H | Oesophageal cancer | |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 | *Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| Stigmasterol | ADRA2A | *Functional dyspepsia |
| LTA4H | Oesophageal cancer | |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 | *Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
|
| TDA | PTGS1 | *Functional dyspepsia |
| Terragon | ADRA2A | *Functional dyspepsia |
| PTGS1 | *Functional dyspepsia | |
| PTGS2 | *Functional dyspepsia Colorectal cancer Oropharyngeal squamous cell carcinoma Peutz-Jeghers syndrome |
* After investigating the relationship between F. fructus and functional dyspepsia using cytoscape stringApp, genes related to functional dyspepsia were added to this table.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



