
Submitted:
16 May 2023
Posted:
17 May 2023
You are already at the latest version
Abstract
Appropriate nutrition during pregnancy and the post-partum period is vital to both the parent and their offspring. Both under- and over-nourished status may have important microbial implications on the parental and infant gut microbiomes. Alterations to the microbiome can have implications for a person’s risk of obesity and metabolic diseases. In this review, we examine alterations in the parental gut, vaginal, placental, and milk microbiomes in the context of pre-pregnancy BMI, gestational weight gain, body composition, gestational diabetes, and parental diet. We also investigate how the infant gut microbiome may be altered by these different parameters. Many of the microbial changes seen in under- and over-nourished states in birthing parents may result in long-term implications to the health of offspring. Differences in diet appear to be a major driver of the parental, and subsequently milk and offspring microbiomes. Further prospective longitudinal cohort studies are needed examining nutrition and the microbiome to better understand its implications. Additionally, trials involving dietary interventions in child-bearing age adults should be explored to improve the parent and child’s risks for metabolic diseases.
Keywords:
Parental nutrition
; Obesity
; Pregnancy
; Microbiome
INTRODUCTION
The pregnancy and post-partum periods are times of significant metabolic and microbial change for the birthing parent and their offspring. There are increased energy requirements to support the growth of the uterus, breast tissue, placenta, and fetal tissues.[1] The gut microbiome facilitates nutrient absorption, gut defense barrier, and immune development. There is an increase during pregnancy in gut Akkermansia, Bifidobacterium, and Firmicutes bacteria, likely to facilitate energy storage.[2] There is also an increased abundance of gut bacteria Proteobacteria and Actinobacteria which are believed to protect against inflammation.[2] The nutritional status of the pregnant person is important in regulating these microbial shifts necessary in pregnancy and the post-partum period.
Both excessive and inadequate nutrition can have remarkable consequences to the parent during pregnancy (Table 1). Obesity, excessive gestational weight gain, gestational diabetes, and hypertension have been associated with increased future risk for obesity, cardiovascular disease, and type 2 diabetes.[1] In contrast, inadequate nutrition in pregnancy has been associated with increased risk of life-threatening hemorrhage, obstructed labor, sepsis, and all-cause mortality. [3,4,5]
Excessive and inadequate nutrition can also have consequences to the offspring (Table 2). The effects of parental nutritional status on infant outcomes may be mediated through several pathways including dietary intake, milk composition, and parental microbiome (Figure 1). Infants of parents with gestational diabetes and/or pre-pregnancy obesity have increased risk of increased fetal growth, large for gestational age status at birth, and later metabolic syndrome.[6] Inadequate nutrition during pregnancy alters placental histomorphology and function [7] and can lead to epigenetic changes regarding nutrient utilization, as well as a higher risk of fetal growth restriction, small for gestational age status, and later metabolic syndrome.[7] Additionally, human milk oligosaccharides (HMOs) can be altered by nutritional status[8,9] and are pre-biotics for milk and gut bacteria. Thus, HMOs may alter the milk microbiome and shape the infant gut microbiome.[10,11,12]
Alterations in the microbiome have been associated with inappropriate nutrition in pregnancy. Both obesity and undernutrition in pregnancy have been associated with decreased gut microbial diversity and shifts in microbial abundance.[13] However, changes in diet can modify the microbiome of the mother and offspring. In this review, we will explore the impact of different markers of metabolic health and diet on the parental and infant microbiome in pregnancy and postpartum period.
PRE-PREGNANCY BMI AND ITS ROLE IN MICROBIAL CHANGES
OVERWEIGHT/OBESITY
Increases in pre-pregnancy body mass index (BMI) have been associated with alterations to the parental gut microbiome. In the first trimester, pregnant parents who were obese prior to pregnancy were found to have a higher relative abundance of Firmicutes and a lower relative abundance of Proteobacteria compared to their normal body weight counterparts.[14] A high abundance of Firmicutes has been found in multiple studies of adults with obesity, with evidence suggesting that Firmicutes increase the efficiency of energy extraction and promote the absorption of calories.[15] In the third trimester, overweight pregnant parents compared to normal BMI parents were found to have increased Bacteroides,[16] Clostridium,[16] Biolphila,[17] Roseburia,[17] Dialster,[17] and S. aureus [16] and decreased Phascolarctobacterium compared to normal BMI parents.[17] S. aureus have been found in the presence of intestinal inflammation secondary to adipocyte hyperplasia [15]. However, these changes are inconsistent across studies- one study found no changes in genus-level composition between those with an elevated BMI compared to those with a normal BMI.[18] Similarly, some studies have found decreased diversity with obesity [13] while others have not.[17]
Obesity also has been associated with alterations to the parental vaginal and placental microbiomes. Alterations in the vaginal and placental microbiome have been associated with preterm birth.[19] Women with normal weight have with increased diversity in the vaginal microbiome in the introitus and post-fornix compared to those with obesity.[20] Another study in Caucasian parents found pre-pregnancy BMI was associated with an elevated Nugent score, a score concerning for vaginal dysbiosis[21]. The role of obesity versus gestational weight gain on the placental microbiome has been controversial. Parental obesity is believed to contribute to placental dysfunction. In a pig model of obesity in pregnancy, the obese group had increased oxidative damage with increased reactive oxygen species protein[22]. These reactive oxidative species and interleukins were correlated with relative abundance of Christensenellacaea_R-7 and decreased norank_f_Bacteroidales_S24-7_group, members of Firmicutes phyla. These findings suggest that placental inflammation may be secondary to microbial changes and could contribute to risk for preterm birth. However, when examining placentas of parents who delivered preterm, there was no clustering of microbial communities by obesity.[23] In contrast, a study in term parents found the placental microbiome of obese pre-pregnant parents to have less diversity, less microbial richness, and less abundance of taxa[24].
HMOs are considered a pre-biotic for infant gut bacteria, and thus altered composition could impact the gut microbiome. The milk microbiome and HMOs may be altered in the setting of obesity. In general, parents with elevated BMI have been found to have a less diverse milk bacterial community.[25] An elevated BMI has been associated with a higher relative abundance of Staphylococcus,[26,27,28] Akkermansia,[25,26] Corneybacterium,[28] Granulicatella,[28,29] and low abundance of Lactobacillus,[26,27] Bacteroidetes,[29] Bifidobacterium,[25,26] and Streptococcus[27] in the milk microbiome. However, there are some studies which have found no relationship between BMI and milk microbial composition.[30,31] One study found obese parents were more likely to be non-secretors (those who cannot produce fucosylated HMOs), and among non-secretors, there was increased sialyl-lacto-N-tetraose b (LSTb) and fucosyl-disialyl-lacto-N-hexaose (FDSLNH) in overweight parents compared to normal weight parents.[32] Lacto-N-pentose II/III, and lacto-N-fucopentose I were associated with parent pre-pregnancy BMI.[31] Fucosylated HMOs are an important energy source for infant gut Bifidobacterium and may impact the development of the infant gut.[33]
Parental overweight/obesity status has also been associated with alterations to the infant gut microbiome. One study found meconium samples of infants born to parents who were obese pre-pregnancy, had less Firmicutes and increased Proteobacteria compared to infants born to parents with normal pre-pregnancy BMI.[14] When examining infants of overweight parents up to 12 months, diversity indices of the gut microbiome were increased in the overweight group compared to the normal weight group.[34] However, the evidence of changes in infant gut bacterial abundance are mixed. In a study examining infant gut bacterial abundance at the genus level, infants from overweight parents had greater abundance of Salmonella, Serratia and Coprobacillus; however, significance was only achieved with unadjusted p-values.[34] Another study found mode of delivery altered the findings. There were no associations of pre-pregnancy BMI and the infant gut microbiome in the Cesarean-delivered infants, but in the vaginal birth delivered group, there was increased Bacteroides fragilis, Escherichia coli, Veillonella dispar, Staphylococcus, and Enterococcus.[35] Infants of overweight parents had less butyric acid-producing bacteria compared to normal-weight parents.[34] These findings suggest infants of overweight/obese parents begin with pathogenic bacteria with less butyrate production. Butyrate has been considered the optimal energy source for colonocytes, and limited source of this could impact intestinal health.[36]
UNDERWEIGHT
The effects of parental underweight on the parental and infant microbiome are less well-defined than that of obesity and overweight. There is animal data to suggest that parental undernutrition alters the microbiome. A study of pregnant cattle demonstrated decreased placental microbial diversity in the setting of feed restriction in late gestation.[37] Furthermore, feed restriction of pregnant ewes results in an altered relative abundance of gut microbial communities.[38] Feed restriction of ewes additionally results in decreased colonic microbiome diversity and increased relative abundance of Peptococcaceae and decreased relative abundance of Ruminococcus.[39] Peptococcacea has been associated with higher high-density lipoprotein cholesterol,[40] whereas Ruminoccocus plays a key role in complex carboydrate degradation[41] and may be important to maintaining colonic health as decreased abundance of Ruminococcaceae has been implicated in inflammatory bowel diseases[42,43] and antibiotic associated diarrhea.[44]
Evidence from individuals with anorexia has demonstrated decreased alpha diversity[45] and lower amounts of total bacteria and obligate anaerobes in fecal samples when compared to well-nourished individuals.[38] Reduction of energy-balance and nutrient load in the diet results in an increase in Firmicutes and a decrease in Bacteroidetes; similar to obese adults.[46] This could be plausible as these bacteria facilitate energy usage, and in a starved state this is critical.
Additionally, evidence from young children with severe undernutrition demonstrates less mature gut microbiomes that may promote excessive weight loss.[47] Children with malnutrition have lower richness and increased abundance of Proteobacteria, including pathogenic Klebsiella and Escherichia and lower abundance of Bacteroidetes when compared to healthy children.[48] Reduced diversity and increased relative abundance of Acidaminococcus is also reported among children with undernutrition.[49] Taken together, it is plausible and likely that undernutrition in pregnancy results in distinct changes to the parental microbiome which will affect offspring, though additional studies focusing on the microbiome of undernourished individuals are needed.
GESTATIONAL WEIGHT GAIN
The role of gestational weight gain in pregnancy on the parental gut microbiome has been controversial. United States Preventative Task Force has differing recommendations of weight gain depending on pre-pregnancy BMI with less weight gain (11 to 20 lb) for obese pregnant parents and more weight gain (28 to 40 lb) for underweight pregnant parents.[50] The recommended amount of weight gain in pregnancy was associated with increased Bifidobacterium compared to those with excessive weight gain.[16] However, when controlling for pre-pregnancy BMI, there were no differences in diversity with excess gestational weight gain,[17,51]. There have been changes in bacterial abundance with excess gestational weight gain. Increased gestational weight gain was associated with decreased Prevotella and Dialister in the third trimester.[17] Dialister has been associated with insulin sensitivity.[16] For those with normal pre-pregnancy BMI, when they had excessive gestational weight gain, there was an increased in Firmicutes and Bacteroidetes phyla,[51] but in those who were obese prior to pregnancy who had excessive weight gain, there was an increase only in Bacteroidetes.[51] This could be due to preexistence of high quantities of Firmicutes in the context of obesity.
The milk and placental microbiome also appear to be altered by gestational weight gain in pregnancy. Multiple studies have found that with increased gestational weight gain there was an increase in milk microbiome alpha-diversity.[52,53] Independent of parental obesity, increased gestational weight gain has been associated with increased abundance of Staphylococcus,[25,26,27] decreased Streptococcus,[53] and decreased Bifidobacterium.[26,53] Staphylococcus has been associated with the pro-inflammatory state of obesity,[54] and may contribute to the infant’s risk for future metabolic diseases. Additionally, the placental microbiome in parents who deliver preterm clusters by excess gestational weight gain.[23] For those with excessive gestational weight gain, there are decreased species richness, decreased Proteobacteria, increased Actinobacteria, increased Firmicutes, and increased Cyanobacteria.[23] These findings are thought-provoking, as excessive gestational weight gain and decreased placental species richness have both been associated with increased risk of preterm birth,[55] and thus provide a potential mechanism that could be amenable to intervention.
Increased gestational weight gain in pregnancy has been associated with changes in the offspring microbiome from the neonatal period to adulthood. Gestational weight gain has been associated with decreased Akkermansia abundance at 1 month[34], increased diversity at 6 months[34], increased enrichment of microbial glucose and glycogen degradation pathways, and increased microbial phenylalanine, cysteine/serine, folate, thiamin, biotin, and pyridoxine synthesis pathways at 8 months.[56] These studies suggest gestational weight gain impacts the infant’s gut bacterial role in energy storage, which could have implications on their risk for obesity and metabolic syndrome. Another study examining women 19 to 44 years old whose parents demonstrated excess gestational weight gain, found those who exposed to excess gestational weight gain had increased visceral adiposity and increased fecal Acidaminooccus, a bacteria associated with adiposity, in adulthood.[57] These findings suggest that adiposity even in adulthood may have fetal and microbial origins.
BODY COMPOSITION
Given pre-pregnancy BMI is a flawed proxy for adiposity,[58] nutritional scientists are moving toward the use of body composition. Body composition examines fat-mass (brown, subcutaneous, visceral fat) versus fat-free mass (muscle, organs, or bone), or skeletal muscle mass. Body composition can be studied using various technologies that vary in cost and resolution. Increased white visceral adipose tissue in pregnancy releases pro-inflammatory cytokines and free fatty acids which can alter the epigenome of fetus’ muscle, liver, and adipose tissue.[49] These adaptations can increase the child’s risk of metabolic syndrome and nonalcoholic fatty liver disease. As mentioned previously, parents with increased BMI have also been found to have significant differences in the human milk oligosaccharide profile,[8,34] but no studies have directly examined the relationship between parental body composition and human milk oligosaccharide concentrations.
Given the release of free fatty acids and the changes in mother’s own milk human milk oligosaccharide composition, there are likely alterations in the parental and infant microbiome. However, this has not been well-studied. In a study examining adults with type 2 diabetes, adults with a greater lean tissue index (lean tissue mass divided by height squared) had a higher ratio of Firmicutes to Bacteroidetes phylum.[59] In a rat model giving a high protein diet versus a fat and sucrose diet, a high protein diet was associated with decreased fat mass, increased alpha-diversity, increased abundance of Lactobacillacea and Bifidobacterium in the parent.[60] In the offspring of the high protein mice, they found decreased fat mass in both male and female mice, but sex-dependent differences in the microbiome.[60] Both male and female offspring had differences in beta-diversity, but in males there was also increased alpha-diversity, increased Bifidobacterium, increased Muribaculaceae, and decreased Lachnospiraceae.[60] In an observational study examining 140 pregnant parents, increased fat mass in pregnancy was positively associated with increased Akkermansia, Blautia, and Bilophila.[17] Bilophila is a bile-resistant bacillus that expands in the presence of dietary fats and has been associated with increased intestinal inflammation in a mouse model.[61] There have been no other studies to date examining parental body composition in pregnancy and the microbiome, and further research is needed to define the role of body composition on the microbiome and better understand the microbial mechanisms for parental and neonatal metabolic changes.
GESTATIONAL DIABETES
Gestational diabetes is a hyperglycemic state that occurs during pregnancy. Gestational diabetes is one of the most common complications in pregnancy that has been increasing in prevalence alongside both the obesity epidemic and increasing parental age at time of conception.[62] To meet the demands of the developing fetus, a state of transient hyperinsulinism is necessary to store energy; however, some parents are unable to compensate for hyperinsulinism and develop hyperglycemia due to pancreatic beta-cell dysfunction.[63] There is evidence that an altered microbiome with decreased short-chain fatty acid producing bacteria, decreased amino acid degrading bacteria, increased Firmicutes to Bacteroidetes ratio, and increased gram-negative bacteria lead to gut inflammation, gut permeability, increased dyslipidemia, and insulin resistance.[64] Additionally, a Western diet (low fruits and vegetables, high sodium and fat) was associated with increased risk of gestational diabetes where as a Mediterranean diet (higher bread, cereal, legume, fish, and olive oil diet) was associated with a decreased risk of gestational diabetes.[65]
The parental microbiome is altered in the setting of gestational diabetes. One study found that the vaginal, oral, and intestinal microbiomes were distinctly different from the non-diabetic microbiome on Bray-Curtis distance analyses comparing compositional similarity.[66] They found the oral cavity had more Proteobaceria and less Firmicutes in gestational diabetes, but no significant abundance differences in the intestinal or vaginal microbiome.[66] In contrast, one study examining 502 pregnant parents’s vaginal microbiomes found gestational diabetes was associated with vaginal dysbiosis.[67] In regards to the gut microbiome, some experts argue that the origins of gestational diabetes are microbial.[59,61,62,63] When comparing the gut microbiota of pregnant parents in the first trimester, those who developed gestational diabetes had increased Ruminococcaceae family,[68] butyrate-producing bacteria Faecalibacterium[69] and Eubacterium.[69] In the third trimester of pregnancy, gestational diabetes is associated with increased gut Bacteroides,[70] Streptococcus and Enterobacteriaceae family.[69] All of these bacteria are associated with gut inflammation.[71] Further studies are necessary to determine whether altered gut bacteria in the third trimester predict gestational diabetes earlier than the glucose tolerance test in the second trimester.
Gestational diabetes also alters the microbial signatures of infants of affected parents. In one study, Chinese infants of parents with gestational diabetes and normal BMI were found to have decreased alpha diversity of meconium, as well as altered Firmicutes [72] and Proteobacteria at the phylum level[72]. Another study examining meconium from a similar population of parents with gestational diabetes found at the genus level altered Prevotella,[66] Streptococcus,[66] Bacteroides,[66] and Lactobacillus abundances.[66] Lactobacilus is important in amino acid synthesis de novo. [59] The decreased abundance of Lactobacillus may have implications for protein metabolism in the newborn.
It is difficult to disentangle the role of pre-pregnancy BMI and gestational diabetes on the microbiome as many studies are under-powered to adjust for BMI or do not include more nuanced assessments of body composition. However, one study comparing the parental gut microbiome in parents with gestational diabetes compared to those who were normo-glycemic controlled for pre-pregnancy BMI found decreased Clostridium and Veillonella after controlling for pre-pregnancy BMI.[73] Another study examining parental milk microbiome changes with gestational diabetes and pre-pregnancy BMI demonstrated microbial differences when adjusting for gestational diabetes.[28] Nonetheless, when examining gestational diabetes’ role on the milk microbiome for those parents without obesity, they did not find significant differences.[28] Another study examining the infant meconium microbiome of infants born to parents with gestational diabetes and healthy parents found gestational diabetes state to be a driver of Bacteroidetes, Firmicutes, and Proteobacteria after adjusting for first trimester parental BMI.[74] Alterations in Bacteroides have been associated with type 2 diabtetes [63]. Furthermore, another study found neonates of parents with gestational diabetes had decreased Lactobacillus, Flavonifractor, erysipelotrichaceae, and Gammoproteobacteria after adjusting for pre-pregnancy BMI.[75] These findings provide evidence that gestational diabetes independently alters the microbiomes of parents and infants.
PARENTAL DIET AND THE MICROBIOME
There is evidence to suggest that parental diet may play a critical role in shaping the microbiome in pregnancy and the neonate independent of parental body habitus. Parental dietary intake during pregnancy is associated with parental gut, vaginal, and milk microbiome composition.[21,76,77] Subsequently, the neonatal microbiome is influenced by parental diet. Potential mechanisms of transfer to the infant include via vaginal delivery, the placenta, or the amniotic fluid. The effects of the parental diet on the infant stool microbiome persist after delivery for at least 6 weeks[78] and have been found to be greater among infants delivered vaginally than via Cesarean section.[76] However, when examining the drivers of the infant microbiome up until 6 months, chestfeeding status was the primary driver rather than parental dietary intake.[79]
Fat intake is associated with microbial shifts in pregnancy. Saturated fatty acid intake has been positively associated with gut microbial Simpson diversity index in obese/overweight participants.[17] In normal weight subjects, increased monounsaturated and polyunsaturated fatty acids are associated with Ruminococcus and Paraprevotella abundance.[17] Ruminococcus has been previously positively associated with polyunsaturated fatty acid supplementation and plant-based diets. [16,80] In a study examining mother-infant pairs in the Mediterranean, parental lipid intake has been associated with decreased Bacteroidetes and increased Firmicutes relative abundance prior to delivery, consistent with findings in obesity.[76] In regards to the milk microbiome, increased intake of saturated fatty acids and monounsaturated fatty acids were inversely related to the relative abundance of Corneybacterium in American parents.[29] However, the study was unable to look at the lipid profiles of the milk itself to see if this impacted the milk fat composition.[17] Fat intake has also been directly associated with changes in the infant microbiome.[78] A parental diet high in total lipids, saturated fatty acids, and mono-unsaturated fatty acids has been associated with enrichment of Firmicutes phylum and depletion of Proteobacteria phylum in infant meconium.[76] Infants of parents with high fat intake during pregnancy were found to have lower Bacteroides that persisted from birth to 6 weeks of age.[78] This effect was not modified by pre-pregnancy BMI and gestational diabetes, suggesting that parental diet may be a primary parental driver of the infant microbiome.
Fruit and vegetable consumption also influences the parental microbiome. Particularly, a Mediterranean diet of higher plant and limited animal protein appears to be influential. [81,82,83] Parents who consume vegetarian diets have lower relative abundances of Collinsella, Holdemania, and Eubacterium but increased abundance of Roseburia, and Lachnospiraceae compared to their omnivore counterparts in the gut microbiome during the second trimester of pregnancy.[81] Lachnospiraceae break down polysaccharides to short chain fatty acids and have been associated with people who practice a vegetarian diet.[72,84] A study examining adherence to a Mediterranean diet throughout pregnancy in Hawaiian parents found increased parental gut microbiome diversity and increased abundance of bacteria that produce short chain fatty acids.[82] A predominantly plant/fish protein diet also alters the milk microbiome. In a primate study providing a “Mediterranean diet” compared to a “Western diet” (high animal protein, high sodium, high sugar), they found the mammary tissues had 10-fold higher abundance of Lactobacillus with the Mediterranean diet.[83] A potential mechanism for these alterations in the milk microbiome may be through the entero-mammary pathway where gut bacteria are transmitted to the mammary gland by dendritic cells.
Parental fruit and vegetable intake has been frequently associated with infant gut microbial changes. When examining infant meconium, parental dietary fiber and vegetable protein intake is negatively associated with the relative abundance of Coprococcus, Blautia, Roseburia, Ruminococcaceae, and Lachnospiraceae families.[76] This suggests a more positive microbial profile as Blautia has been associated with increased visceral adiposity in adults.[85] In a study of 39 2-month-old infants in Taiwan, parents with high fruit and vegetable consumption had a higher abundance of Propionibacteriales, Propionibacteriacea, Cutibacterium, Tannerellaceae, Parabacteroides, and Lactococcus.[86] In contrast, infants of parents who ate less fruits and vegetables had higher abundance of Prevotella, Isobaculum, Clostridia, Clostridiales, Lachospiraceae, Hungatella, Lachnoclostridium, Ruminococcacaea, flavonifractor, erysipelatoclostridium, Acidaminococcaceae, Phascolarctobacterium, Megamonas, Betaproteobacteriales, Burkholderiacea, and Suterella.[86] Cutibacterium has been found to degrade hexoses to produce propionate.[75] Propoionate consumption has been shown to be associated with less antigen presentation on dendritic cells associated with allergic disease in mouse models.[87] Another study found similar results at 6 weeks of age but found the effect of fruit intake to be modified by mode of delivery[88]; infants born by Cesarean section whose parents had a high fruit intake had increased odds of high Streptococcus and Clostridium. As the infant ages, there are more environmental drivers to the gut microbiome, but parental dietary intake appears to continue to play a role. One study found at 6 months when controlling for type of milk (mother’s own milk versus formula), solid food introduction, mode of delivery, age, parental education, and race/ethnicity, infants of parents who ate more fruits and vegetables had increased Lactobacillus.[79] Lactobacillus has been associated with cellular immunity in infants and has been utilized as a probiotic supplement in atopic diseases with some success.[89,90]
Additionally, fish and animal protein sources have been associated with changes in the parental and infant gut microbiome. Animal protein intake in pregnancy was positively associated with parental gut Shannon diversity index.[17] Low processed meat intake is positively associated with Lactobacillus abundance in the gut[79] and the vagina;[21] and total animal protein intake has been positively associated with Collinsella abundance.[17] In regards to the infant microbiome, one study found that higher parental animal protein intake is associated with higher abundance of Veillonella, Escherichia/Shigella, Klebsiellla, and Clostridium in infant meconium.[76] These bacteria have been associated with infant gut dysbiosis and inflammation in preterm infants.[91,92,93,94] Increased parental fish and seafood intake was positively associated with increased Streptococcus in six-week-old infants regardless of mode of delivery or parental BMI.[76]
Carbohydrates have also been associated with alterations in the parental and infant microbiome. Increased carbohydrates in pregnancy have been associated with increased Bacteroidetes in the parental gut microbiome prior to delivery.[76] Increased total carbohydrates and sugars in pregnancy was associated with improved vaginal health with a lower Nugent score.[21] In regard to the milk microbiome, increased total carbohydrates, disaccharides, and lactose were negatively associated with abundance of Firmicutes in lactating parents in the United States.[29] There is minimal information regarding parental diet and the milk microbiome, and further research is needed to characterize the microbial differences.
FUTURE DIRECTIONS – DIETARY AND PROBIOTIC INTERVENTIONS
Given the impacts of parental nutritional status and diet on the parental and infant gut microbiome, there have been efforts to improve parental and neonatal health outcomes through prebiotic, probiotic and dietary interventions. Unfortunately, these interventions have had varying levels of success.
Multiple randomized control trials utilizing probiotics have been conducted in overweight pregnant parents. There have been seven studies to date that have examined the use of probiotics in the prevention of gestational diabetes, and a recent meta-analysis conducted found that probiotics had no effect on the risk of gestational diabetes, cesarean section, gestational weight gain in pregnancy, or large for gestational age infants.[95] Another study providing fish oil and/or probiotic supplementation to overweight pregnant parents in early pregnancy to assess gestational weight gain and body composition found no significant differences in gestational weight gain or body composition[96], but supplementation did decrease Ureaplasma and Prevotella.[97] A recent meta-analysis found increased Ureaplasma abundance is associated with preterm rupture of membranes, preterm birth, chorioamionitis, and bronchopulmonary dysplasia, but evidence is low-quality.[98] Thus, probiotics decreasing the abundance of Ureaplasma may have benefits to pregnancy, but further large, randomized control trials are necessary.[99]To date, there is little evidence to support the use of probiotics in pregnancy.
Dietary and exercise interventions in pregnancy have been performed with variable success. In an animal model, methyl-donor nutrients (folate, vitamin B12, choline, methionine, betadine) provided in pregnancy and lactation to mice receiving a high fat diet lead to decreased cytokine expression, decreased colonic vitamin D receptor (VDR) signaling in pups.[100] VDR signaling impacts vitamin D metabolism.[81] The UPBEAT trial enrolled obese pregnant parents to participate in a low glycemic index diet plus physical activity and resulted in decreased skinfold thickness, gestational weight gain, improved metabolome in parents, and decreased infant subscapular skinfold thickness z-score at 6 months.[101] Another study examined if the use of a “HealthyMoms” smartphone app in pregnancy would improve gestational weight gain, glycemia, and insulin resistance,[102] and did not find any significant differences in clinical outcomes. However, the parents did have improved healthy eating scores post-partum.[82] Further research is needed to examine the microbial changes to the mother and neonate following nutritional interventions.
GAPS IN THE LITERATURE
Better understanding of how parental factors including BMI, body composition and diet affect the infant microbiome is needed. Longitudinal studies following from pre-pregnancy and early pregnancy through the period of exclusive chestfeeding would allow for thorough characterization of interactions between parental health, the parental microbiome, and infant health and microbiome. Multi-omic studies evaluating metabolomic and microbiome signatures would allow for a more thorough understanding of interactions between host metabolism, the microbiome and microbial metabolism. Another large gap in the literature is the effect of parental undernutrition including macronutrient and micronutrient deficiencies, low BMI, and inadequate gestational weight gain on both the parental and infant microbiome. Additionally, current methods for assessing parental diet are inadequate as 24 hour recalls, food frequency questionnaires, and other survey methods may not accurately capture dietary intake and quality. As the double burden of malnutrition continues to increase among pregnant people globally, a clear understanding of the effects of malnutrition on the microbiome and infant outcomes is necessary to identify novel targets for intervention to optimize outcomes and development among offspring.
CONCLUSIONS
Parental metabolic factors regarding adiposity, lean mass accretion, insulin resistance, gestational weight gain, and diet all have microbial implications to the mother, the milk produced, and the offspring. Dietary differences during pregnancy appear to be one of the largest drivers of the parental microbiome but are the most difficult to study reliably due to methodology utilized. There also is a paucity of literature on undernutrition's implications on the parental microbiome. Microbial shifts in the mother and their offspring can influence their risk for future metabolic diseases. Although interventions with probiotics in pregnancy have not been successful, dietary changes appear to have the most promise. Further research efforts should concentrate on multi-omic approaches and utilize dietary assessments throughout pregnancy and the lactation period, mother’s own milk composition, and the parental and neonatal microbiome in vulnerable populations to provide precise nutritional and microbiome directed interventions.
Author Contributions
Conceptualization, KMS and DTH; Writing- Original Draft Preparation, DTH and KMS.; Writing – Review & Editing, DTH and KMS.
Funding
This research received no external funding.
Acknowledgments
We would like to thank Dr. Sandra Juul and Dr. Thomas Wood for their thoughtful review of the manuscript.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Most, J.; Dervis, S.; Haman, F.; Adamo, K.B.; Redman, L.M. Energy Intake Requirements in Pregnancy. Nutrients 2019, 11. [Google Scholar] [CrossRef] [PubMed]
- Gorczyca, K.; Obuchowska, A.; Kimber-Trojnar, Ż.; Wierzchowska-Opoka, M.; Leszczyńska-Gorzelak, B. Changes in the Gut Microbiome and Pathologies in Pregnancy. Int J Environ Res Public Health 2022, 19. [Google Scholar] [CrossRef] [PubMed]
- Sikder, S.S.; Labrique, A.B.; Shamim, A.A.; Ali, H.; Mehra, S.; Wu, L.; Shaikh, S.; West, K.P.; Christian, P. Risk factors for reported obstetric complications and near misses in rural northwest Bangladesh: analysis from a prospective cohort study. BMC Pregnancy Childbirth 2014, 14, 347. [Google Scholar] [CrossRef] [PubMed]
- Rush, D. Nutrition and parental mortality in the developing world. Am. J. Clin. Nutr. 2000, 72, 212S–240S. [Google Scholar] [CrossRef]
- Brabin, B.J.; Hakimi, M.; Pelletier, D. An analysis of anemia and pregnancy-related parental mortality. J. Nutr. 2001, 131, 604S–614S, discussion 614S-615S. [Google Scholar] [CrossRef]
- Ornoy, A. Prenatal origin of obesity and their complications: Gestational diabetes, parental overweight and the paradoxical effects of fetal growth restriction and macrosomia. Reprod Toxicol 2011, 32, 205–212. [Google Scholar] [CrossRef]
- Belkacemi, L.; Nelson, D.M.; Desai, M.; Ross, M.G. Parental undernutrition influences placental-fetal development. Biol Reprod 2010, 83, 325–331. [Google Scholar] [CrossRef]
- Isganaitis, E.; Venditti, S.; Matthews, T.J.; Lerin, C.; Demerath, E.W.; Fields, D.A. Parental obesity and the human milk metabolome: associations with infant body composition and postnatal weight gain. Am J Clin Nutr 2019, 110, 111–120. [Google Scholar] [CrossRef]
- Saben, J.L.; Sims, C.R.; Abraham, A.; Bode, L.; Andres, A. Human Milk Oligosaccharide Concentrations and Infant Intakes Are Associated with Parental Overweight and Obesity and Predict Infant Growth. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Hegar, B.; Wibowo, Y.; Basrowi, R.W.; Ranuh, R.G.; Sudarmo, S.M.; Munasir, Z.; Atthiyah, A.F.; Widodo, A.D.; Supriatmo; Kadim, M.; et al. The Role of Two Human Milk Oligosaccharides, 2'-Fucosyllactose and Lacto-N-Neotetraose, in Infant Nutrition. Pediatr Gastroenterol Hepatol Nutr 2019, 22, 330–340. [Google Scholar] [CrossRef]
- Jost, T.; Lacroix, C.; Braegger, C.; Chassard, C. Impact of human milk bacteria and oligosaccharides on neonatal gut microbiota establishment and gut health. Nutr Rev 2015, 73, 426–437. [Google Scholar] [CrossRef] [PubMed]
- Bunesova, V.; Lacroix, C.; Schwab, C. Fucosyllactose and L-fucose utilization of infant Bifidobacterium longum and Bifidobacterium kashiwanohense. BMC Microbiol 2016, 16, 248. [Google Scholar] [CrossRef] [PubMed]
- Morita, C.; Tsuji, H.; Hata, T.; Gondo, M.; Takakura, S.; Kawai, K.; Yoshihara, K.; Ogata, K.; Nomoto, K.; Miyazaki, K.; et al. Gut Dysbiosis in Patients with Anorexia Nervosa. PLoS One 2015, 10, e0145274. [Google Scholar] [CrossRef] [PubMed]
- Cömert, T.K.; Akpinar, F.; Erkaya, S.; Durmaz, B.; Durmaz, R. The effect of pre-pregnancy obesity on gut and meconium microbiome and relationship with fetal growth. J Matern Fetal Neonatal Med 2022, 35, 10629–10637. [Google Scholar] [CrossRef] [PubMed]
- Krajmalnik-Brown, R.; Ilhan, Z.E.; Kang, D.W.; DiBaise, J.K. Effects of gut microbes on nutrient absorption and energy regulation. Nutr. Clin. Pract. 2012, 27, 201–214. [Google Scholar] [CrossRef] [PubMed]
- Collado, M.C.; Isolauri, E.; Laitinen, K.; Salminen, S. Distinct composition of gut microbiota during pregnancy in overweight and normal-weight women. Am. J. Clin. Nutr. 2008, 88, 894–899. [Google Scholar] [CrossRef] [PubMed]
- Ruebel, M.L.; Gilley, S.P.; Sims, C.R.; Zhong, Y.; Turner, D.; Chintapalli, S.V.; Piccolo, B.D.; Andres, A.; Shankar, K. Associations between Parental Diet, Body Composition and Gut Microbial Ecology in Pregnancy. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Griffee, M.B. An update on endodontics and other oral microbiology. J Indiana Dent Assoc 1986, 65, 27–28. [Google Scholar]
- Cao, B.; Stout, M.J.; Lee, I.; Mysorekar, I.U. Placental Microbiome and Its Role in Preterm Birth. Neoreviews 2014, 15, e537–e545. [Google Scholar] [CrossRef]
- Faucher, M.A.; Greathouse, K.L.; Hastings-Tolsma, M.; Padgett, R.N.; Sakovich, K.; Choudhury, A.; Sheikh, A.; Ajami, N.J.; Petrosino, J.F. Exploration of the Vaginal and Gut Microbiome in African American Women by Body Mass Index, Class of Obesity, and Gestational Weight Gain: A Pilot Study. Am J Perinatol 2020, 37, 1160–1172. [Google Scholar] [CrossRef]
- Dall'Asta, M.; Laghi, L.; Morselli, S.; Re, M.C.; Zagonari, S.; Patuelli, G.; Foschi, C.; Pedna, M.F.; Sambri, V.; Marangoni, A.; et al. Pre-Pregnancy Diet and Vaginal Environment in Caucasian Pregnant Women: An Exploratory Study. Front Mol Biosci 2021, 8, 702370. [Google Scholar] [CrossRef] [PubMed]
- Hu, C.; Yan, Y.; Ji, F.; Zhou, H. Parental Obesity Increases Oxidative Stress in Placenta and It Is Associated With Intestinal Microbiota. Front Cell Infect Microbiol 2021, 11, 671347. [Google Scholar] [CrossRef] [PubMed]
- Antony, K.M.; Ma, J.; Mitchell, K.B.; Racusin, D.A.; Versalovic, J.; Aagaard, K. The preterm placental microbiome varies in association with excess parental gestational weight gain. Am J Obstet Gynecol 2015, 212, 653.e651–616. [Google Scholar] [CrossRef]
- Benny, P.A.; Al-Akwaa, F.M.; Dirkx, C.; Schlueter, R.J.; Wolfgruber, T.K.; Chern, I.Y.; Hoops, S.; Knights, D.; Garmire, L.X. Placentas delivered by pre-pregnant obese women have reduced abundance and diversity in the microbiome. FASEB J 2021, 35, e21524. [Google Scholar] [CrossRef] [PubMed]
- Cabrera-Rubio, R.; Collado, M.C.; Laitinen, K.; Salminen, S.; Isolauri, E.; Mira, A. The human milk microbiome changes over lactation and is shaped by parental weight and mode of delivery. Am J Clin Nutr 2012, 96, 544–551. [Google Scholar] [CrossRef] [PubMed]
- Collado, M.C.; Laitinen, K.; Salminen, S.; Isolauri, E. Parental weight and excessive weight gain during pregnancy modify the immunomodulatory potential of breast milk. Pediatr Res 2012, 72, 77–85. [Google Scholar] [CrossRef] [PubMed]
- Ding, M.; Qi, C.; Yang, Z.; Jiang, S.; Bi, Y.; Lai, J.; Sun, J. Geographical location specific composition of cultured microbiota and Lactobacillus occurrence in human breast milk in China. Food Funct 2019, 10, 554–564. [Google Scholar] [CrossRef]
- LeMay-Nedjelski, L.; Butcher, J.; Ley, S.H.; Asbury, M.R.; Hanley, A.J.; Kiss, A.; Unger, S.; Copeland, J.K.; Wang, P.W.; Zinman, B.; et al. Examining the relationship between parental body size, gestational glucose tolerance status, mode of delivery and ethnicity on human milk microbiota at three months post-partum. BMC Microbiol 2020, 20, 219. [Google Scholar] [CrossRef]
- Williams, J.E.; Carrothers, J.M.; Lackey, K.A.; Beatty, N.F.; York, M.A.; Brooker, S.L.; Shafii, B.; Price, W.J.; Settles, M.L.; McGuire, M.A.; et al. Human Milk Microbial Community Structure Is Relatively Stable and Related to Variations in Macronutrient and Micronutrient Intakes in Healthy Lactating Women. J Nutr 2017, 147, 1739–1748. [Google Scholar] [CrossRef]
- Moossavi, S.; Sepehri, S.; Robertson, B.; Bode, L.; Goruk, S.; Field, C.J.; Lix, L.M.; de Souza, R.J.; Becker, A.B.; Mandhane, P.J.; et al. Composition and Variation of the Human Milk Microbiota Are Influenced by Parental and Early-Life Factors. Cell Host Microbe 2019, 25, 324–335.e324. [Google Scholar] [CrossRef]
- Li, S.W.; Watanabe, K.; Hsu, C.C.; Chao, S.H.; Yang, Z.H.; Lin, Y.J.; Chen, C.C.; Cao, Y.M.; Huang, H.C.; Chang, C.H.; et al. Bacterial Composition and Diversity in Breast Milk Samples from Mothers Living in Taiwan and Mainland China. Front Microbiol 2017, 8, 965. [Google Scholar] [CrossRef] [PubMed]
- Larsson, M.W.; Lind, M.V.; Laursen, R.P.; Yonemitsu, C.; Larnkjær, A.; Mølgaard, C.; Michaelsen, K.F.; Bode, L. Human Milk Oligosaccharide Composition Is Associated With Excessive Weight Gain During Exclusive Breastfeeding-An Explorative Study. Front Pediatr 2019, 7, 297. [Google Scholar] [CrossRef] [PubMed]
- Turroni, F.; Milani, C.; Duranti, S.; Ferrario, C.; Lugli, G.A.; Mancabelli, L.; van Sinderen, D.; Ventura, M. Bifidobacteria and the infant gut: an example of co-evolution and natural selection. Cell. Mol. Life Sci. 2018, 75, 103–118. [Google Scholar] [CrossRef] [PubMed]
- Gilley, S.P.; Ruebel, M.L.; Sims, C.; Zhong, Y.; Turner, D.; Lan, R.S.; Pack, L.M.; Piccolo, B.D.; Chintapalli, S.V.; Abraham, A.; et al. Associations between parental obesity and offspring gut microbiome in the first year of life. Pediatr Obes 2022, 17, e12921. [Google Scholar] [CrossRef] [PubMed]
- Singh, S.B.; Madan, J.; Coker, M.; Hoen, A.; Baker, E.R.; Karagas, M.R.; Mueller, N.T. Does birth mode modify associations of parental pre-pregnancy BMI and gestational weight gain with the infant gut microbiome? Int J Obes (Lond) 2020, 44, 23–32. [Google Scholar] [CrossRef] [PubMed]
- Miquel, S.; Martin, R.; Rossi, O.; Bermudez-Humaran, L.G.; Chatel, J.M.; Sokol, H.; Thomas, M.; Wells, J.M.; Langella, P. Faecalibacterium prausnitzii and human intestinal health. Curr. Opin. Microbiol. 2013, 16, 255–261. [Google Scholar] [CrossRef] [PubMed]
- Hummel, G.; Woodruff, K.; Austin, K.; Knuth, R.; Lake, S.; Cunningham-Hollinger, H. Late Gestation Parental Feed Restriction Decreases Microbial Diversity of the Placenta While Mineral Supplementation Improves Richness of the Fetal Gut Microbiome in Cattle. Animals (Basel) 2021, 11. [Google Scholar] [CrossRef]
- Xue, Y.; Lin, L.; Hu, F.; Zhu, W.; Mao, S. Disruption of ruminal homeostasis by malnutrition involved in systemic ruminal microbiota-host interactions in a pregnant sheep model. Microbiome 2020, 8, 138. [Google Scholar] [CrossRef]
- Xue, Y.; Hu, F.; Guo, C.; Mei, S.; Xie, F.; Zeng, H.; Mao, S. Undernutrition shifted colonic fermentation and digest-associated bacterial communities in pregnant ewes. Appl Microbiol Biotechnol 2020, 104, 5973–5984. [Google Scholar] [CrossRef]
- Villasenor-Aranguren, M.; Roses, C.; Riezu-Boj, J.I.; Lopez-Yoldi, M.; Ramos-Lopez, O.; Barcelo, A.M.; Milagro, F.I. Association of the Gut Microbiota with the Host's Health through an Analysis of Biochemical Markers, Dietary Estimation, and Microbial Composition. Nutrients 2022, 14. [Google Scholar] [CrossRef]
- Ze, X.; Duncan, S.H.; Louis, P.; Flint, H.J. Ruminococcus bromii is a keystone species for the degradation of resistant starch in the human colon. ISME J 2012, 6, 1535–1543. [Google Scholar] [CrossRef] [PubMed]
- Morgan, X.C.; Tickle, T.L.; Sokol, H.; Gevers, D.; Devaney, K.L.; Ward, D.V.; Reyes, J.A.; Shah, S.A.; LeLeiko, N.; Snapper, S.B.; et al. Dysfunction of the intestinal microbiome in inflammatory bowel disease and treatment. Genome Biol. 2012, 13, R79. [Google Scholar] [CrossRef] [PubMed]
- Joossens, M.; Huys, G.; Cnockaert, M.; De Preter, V.; Verbeke, K.; Rutgeerts, P.; Vandamme, P.; Vermeire, S. Dysbiosis of the faecal microbiota in patients with Crohn's disease and their unaffected relatives. Gut 2011, 60, 631–637. [Google Scholar] [CrossRef] [PubMed]
- Gu, X.; Sim, J.X.Y.; Lee, W.L.; Cui, L.; Chan, Y.F.Z.; Chang, E.D.; Teh, Y.E.; Zhang, A.N.; Armas, F.; Chandra, F.; et al. Gut Ruminococcaceae levels at baseline correlate with risk of antibiotic-associated diarrhea. iScience 2022, 25, 103644. [Google Scholar] [CrossRef] [PubMed]
- Mörkl, S.; Lackner, S.; Müller, W.; Gorkiewicz, G.; Kashofer, K.; Oberascher, A.; Painold, A.; Holl, A.; Holzer, P.; Meinitzer, A.; et al. Gut microbiota and body composition in anorexia nervosa inpatients in comparison to athletes, overweight, obese, and normal weight controls. Int J Eat Disord 2017, 50, 1421–1431. [Google Scholar] [CrossRef] [PubMed]
- Jumpertz, R.; Le, D.S.; Turnbaugh, P.J.; Trinidad, C.; Bogardus, C.; Gordon, J.I.; Krakoff, J. Energy-balance studies reveal associations between gut microbes, caloric load, and nutrient absorption in humans. Am J Clin Nutr 2011, 94, 58–65. [Google Scholar] [CrossRef] [PubMed]
- Smith, M.I.; Yatsunenko, T.; Manary, M.J.; Trehan, I.; Mkakosya, R.; Cheng, J.; Kau, A.L.; Rich, S.S.; Concannon, P.; Mychaleckyj, J.C.; et al. Gut microbiomes of Malawian twin pairs discordant for kwashiorkor. Science 2013, 339, 548–554. [Google Scholar] [CrossRef] [PubMed]
- Monira, S.; Nakamura, S.; Gotoh, K.; Izutsu, K.; Watanabe, H.; Alam, N.H.; Endtz, H.P.; Cravioto, A.; Ali, S.I.; Nakaya, T.; et al. Gut microbiota of healthy and malnourished children in bangladesh. Front Microbiol 2011, 2, 228. [Google Scholar] [CrossRef]
- Gough, E.K.; Stephens, D.A.; Moodie, E.E.; Prendergast, A.J.; Stoltzfus, R.J.; Humphrey, J.H.; Manges, A.R. Linear growth faltering in infants is associated with Acidaminococcus sp. and community-level changes in the gut microbiota. Microbiome 2015, 3, 24. [Google Scholar] [CrossRef]
- Force, U.S.P.S.T.; Davidson, K.W.; Barry, M.J.; Mangione, C.M.; Cabana, M.; Caughey, A.B.; Davis, E.M.; Donahue, K.E.; Doubeni, C.A.; Krist, A.H.; et al. Behavioral Counseling Interventions for Healthy Weight and Weight Gain in Pregnancy: US Preventive Services Task Force Recommendation Statement. JAMA 2021, 325, 2087–2093. [Google Scholar] [CrossRef]
- Cömert, T.K.; Akpinar, F.; Erkaya, S.; Durmaz, B.; Durmaz, R. The effect of gestational weight gain on serum total oxidative stress, total antioxidant capacity and gut microbiota. Biosci Microbiota Food Health 2022, 41, 160–167. [Google Scholar] [CrossRef] [PubMed]
- Lundgren, S.N.; Madan, J.C.; Karagas, M.R.; Morrison, H.G.; Hoen, A.G.; Christensen, B.C. Microbial Communities in Human Milk Relate to Measures of Parental Weight. Front Microbiol 2019, 10, 2886. [Google Scholar] [CrossRef] [PubMed]
- Cortés-Macías, E.; Selma-Royo, M.; Martínez-Costa, C.; Collado, M.C. Breastfeeding Practices Influence the Breast Milk Microbiota Depending on Pre-Gestational Parental BMI and Weight Gain over Pregnancy. Nutrients 2021, 13. [Google Scholar] [CrossRef] [PubMed]
- Daiy, K.; Harries, V.; Nyhan, K.; Marcinkowska, U.M. Parental weight status and the composition of the human milk microbiome: A scoping review. PLoS One 2022, 17, e0274950. [Google Scholar] [CrossRef] [PubMed]
- Aagaard, K.; Ma, J.; Antony, K.M.; Ganu, R.; Petrosino, J.; Versalovic, J. The placenta harbors a unique microbiome. Sci Transl Med 2014, 6, 237ra265. [Google Scholar] [CrossRef] [PubMed]
- Baumann-Dudenhoeffer, A.M.; D'Souza, A.W.; Tarr, P.I.; Warner, B.B.; Dantas, G. Infant diet and parental gestational weight gain predict early metabolic maturation of gut microbiomes. Nat Med 2018, 24, 1822–1829. [Google Scholar] [CrossRef]
- Freitas, R.G.B.O.; Vasques, A.C.J.; Fernandes, G.R.; Ribeiro, F.B.; Solar, I.; Barbosa, M.G.; Almeida-Pititto, B.; Geloneze, B.; Ferreira, S.R.G. Gestational weight gain and visceral adiposity in adult offspring: Is there a link with the fecal abundance of Acidaminococcus genus? Eur J Clin Nutr 2022, 76, 1705–1712. [Google Scholar] [CrossRef]
- Flegal, K.M.; Shepherd, J.A.; Looker, A.C.; Graubard, B.I.; Borrud, L.G.; Ogden, C.L.; Harris, T.B.; Everhart, J.E.; Schenker, N. Comparisons of percentage body fat, body mass index, waist circumference, and waist-stature ratio in adults. Am. J. Clin. Nutr. 2009, 89, 500–508. [Google Scholar] [CrossRef]
- Hung, W.C.; Hung, W.W.; Tsai, H.J.; Chang, C.C.; Chiu, Y.W.; Hwang, S.J.; Kuo, M.C.; Chen, S.C.; Dai, C.Y.; Tsai, Y.C. The Association of Targeted Gut Microbiota with Body Composition in Type 2 Diabetes Mellitus. Int J Med Sci 2021, 18, 511–519. [Google Scholar] [CrossRef]
- Chleilat, F.; Schick, A.; Deleemans, J.M.; Ma, K.; Alukic, E.; Wong, J.; Noye Tuplin, E.W.; Nettleton, J.E.; Reimer, R.A. Paternal high protein diet modulates body composition, insulin sensitivity, epigenetics, and gut microbiota intergenerationally in rats. FASEB J 2021, 35, e21847. [Google Scholar] [CrossRef]
- Natividad, J.M.; Lamas, B.; Pham, H.P.; Michel, M.L.; Rainteau, D.; Bridonneau, C.; da Costa, G.; van Hylckama Vlieg, J.; Sovran, B.; Chamignon, C.; et al. Bilophila wadsworthia aggravates high fat diet induced metabolic dysfunctions in mice. Nat Commun 2018, 9, 2802. [Google Scholar] [CrossRef] [PubMed]
- McIntyre, H.D.; Catalano, P.; Zhang, C.; Desoye, G.; Mathiesen, E.R.; Damm, P. Gestational diabetes mellitus. Nat Rev Dis Primers 2019, 5, 47. [Google Scholar] [CrossRef] [PubMed]
- Hasain, Z.; Mokhtar, N.M.; Kamaruddin, N.A.; Mohamed Ismail, N.A.; Razalli, N.H.; Gnanou, J.V.; Raja Ali, R.A. Gut Microbiota and Gestational Diabetes Mellitus: A Review of Host-Gut Microbiota Interactions and Their Therapeutic Potential. Front Cell Infect Microbiol 2020, 10, 188. [Google Scholar] [CrossRef] [PubMed]
- Huang, L.; Thonusin, C.; Chattipakorn, N.; Chattipakorn, S.C. Impacts of gut microbiota on gestational diabetes mellitus: a comprehensive review. Eur J Nutr 2021, 60, 2343–2360. [Google Scholar] [CrossRef] [PubMed]
- Mijatovic-Vukas, J.; Capling, L.; Cheng, S.; Stamatakis, E.; Louie, J.; Cheung, N.W.; Markovic, T.; Ross, G.; Senior, A.; Brand-Miller, J.C.; et al. Associations of Diet and Physical Activity with Risk for Gestational Diabetes Mellitus: A Systematic Review and Meta-Analysis. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Wang, J.; Zheng, J.; Shi, W.; Du, N.; Xu, X.; Zhang, Y.; Ji, P.; Zhang, F.; Jia, Z.; Wang, Y.; et al. Dysbiosis of parental and neonatal microbiota associated with gestational diabetes mellitus. Gut 2018, 67, 1614–1625. [Google Scholar] [CrossRef] [PubMed]
- Rafat, D.; Singh, S.; Nawab, T.; Khan, F.; Khan, A.U.; Khalid, S. Association of vaginal dysbiosis and gestational diabetes mellitus with adverse perinatal outcomes. Int J Gynaecol Obstet 2022, 158, 70–78. [Google Scholar] [CrossRef]
- Mokkala, K.; Houttu, N.; Vahlberg, T.; Munukka, E.; Rönnemaa, T.; Laitinen, K. Gut microbiota aberrations precede diagnosis of gestational diabetes mellitus. Acta Diabetol 2017, 54, 1147–1149. [Google Scholar] [CrossRef]
- Koren, O.; Goodrich, J.K.; Cullender, T.C.; Spor, A.; Laitinen, K.; Bäckhed, H.K.; Gonzalez, A.; Werner, J.J.; Angenent, L.T.; Knight, R.; et al. Host remodeling of the gut microbiome and metabolic changes during pregnancy. Cell 2012, 150, 470–480. [Google Scholar] [CrossRef]
- Dualib, P.M.; Taddei, C.R.; Fernandes, G.; Carvalho, C.R.S.; Sparvoli, L.G.; Silva, I.T.; Mattar, R.; Ferreira, S.R.G.; Dib, S.A.; Almeida-Pititto, B. Gut Microbiota across Normal Gestation and Gestational Diabetes Mellitus: A Cohort Analysis. Metabolites 2022, 12. [Google Scholar] [CrossRef]
- Zeng, M.Y.; Inohara, N.; Nunez, G. Mechanisms of inflammation-driven bacterial dysbiosis in the gut. Mucosal Immunol. 2017, 10, 18–26. [Google Scholar] [CrossRef] [PubMed]
- Chen, T.; Qin, Y.; Chen, M.; Zhang, Y.; Wang, X.; Dong, T.; Chen, G.; Sun, X.; Lu, T.; White, R.A.; et al. Gestational diabetes mellitus is associated with the neonatal gut microbiota and metabolome. BMC Med 2021, 19, 120. [Google Scholar] [CrossRef]
- Crusell, M.K.W.; Hansen, T.H.; Nielsen, T.; Allin, K.H.; Rühlemann, M.C.; Damm, P.; Vestergaard, H.; Rørbye, C.; Jørgensen, N.R.; Christiansen, O.B.; et al. Gestational diabetes is associated with change in the gut microbiota composition in third trimester of pregnancy and postpartum. Microbiome 2018, 6, 89. [Google Scholar] [CrossRef]
- Hu, J.; Nomura, Y.; Bashir, A.; Fernandez-Hernandez, H.; Itzkowitz, S.; Pei, Z.; Stone, J.; Loudon, H.; Peter, I. Diversified microbiota of meconium is affected by parental diabetes status. PLoS One 2013, 8, e78257. [Google Scholar] [CrossRef] [PubMed]
- Soderborg, T.K.; Carpenter, C.M.; Janssen, R.C.; Weir, T.L.; Robertson, C.E.; Ir, D.; Young, B.E.; Krebs, N.F.; Hernandez, T.L.; Barbour, L.A.; et al. Gestational Diabetes Is Uniquely Associated With Altered Early Seeding of the Infant Gut Microbiota. Front Endocrinol (Lausanne) 2020, 11, 603021. [Google Scholar] [CrossRef]
- Selma-Royo, M.; García-Mantrana, I.; Calatayud, M.; Parra-Llorca, A.; Martínez-Costa, C.; Collado, M.C. Parental diet during pregnancy and intestinal markers are associated with early gut microbiota. Eur J Nutr 2021, 60, 1429–1442. [Google Scholar] [CrossRef] [PubMed]
- Zaidi, A.Z.; Moore, S.E.; Okala, S.G. Impact of Parental Nutritional Supplementation during Pregnancy and Lactation on the Infant Gut or Breastmilk Microbiota: A Systematic Review. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Chu, D.M.; Antony, K.M.; Ma, J.; Prince, A.L.; Showalter, L.; Moller, M.; Aagaard, K.M. The early infant gut microbiome varies in association with a parental high-fat diet. Genome Med 2016, 8, 77. [Google Scholar] [CrossRef]
- Savage, J.H.; Lee-Sarwar, K.A.; Sordillo, J.E.; Lange, N.E.; Zhou, Y.; O'Connor, G.T.; Sandel, M.; Bacharier, L.B.; Zeiger, R.; Sodergren, E.; et al. Diet during Pregnancy and Infancy and the Infant Intestinal Microbiome. J Pediatr 2018, 203, 47–54.e44. [Google Scholar] [CrossRef]
- Garcia-Mantrana, I.; Selma-Royo, M.; Gonzalez, S.; Parra-Llorca, A.; Martinez-Costa, C.; Collado, M.C. Distinct parental microbiota clusters are associated with diet during pregnancy: impact on neonatal microbiota and infant growth during the first 18 months of life. Gut Microbes 2020, 11, 962–978. [Google Scholar] [CrossRef]
- Barrett, H.L.; Gomez-Arango, L.F.; Wilkinson, S.A.; McIntyre, H.D.; Callaway, L.K.; Morrison, M.; Dekker Nitert, M. A Vegetarian Diet Is a Major Determinant of Gut Microbiota Composition in Early Pregnancy. Nutrients 2018, 10. [Google Scholar] [CrossRef] [PubMed]
- Miller, C.B.; Benny, P.; Riel, J.; Boushey, C.; Perez, R.; Khadka, V.; Qin, Y.; Maunakea, A.K.; Lee, M.J. Adherence to Mediterranean diet impacts gastrointestinal microbial diversity throughout pregnancy. BMC Pregnancy Childbirth 2021, 21, 558. [Google Scholar] [CrossRef] [PubMed]
- Shively, C.A.; Register, T.C.; Appt, S.E.; Clarkson, T.B.; Uberseder, B.; Clear, K.Y.J.; Wilson, A.S.; Chiba, A.; Tooze, J.A.; Cook, K.L. Consumption of Mediterranean versus Western Diet Leads to Distinct Mammary Gland Microbiome Populations. Cell Rep 2018, 25, 47–56.e43. [Google Scholar] [CrossRef] [PubMed]
- Furet, J.P.; Firmesse, O.; Gourmelon, M.; Bridonneau, C.; Tap, J.; Mondot, S.; Dore, J.; Corthier, G. Comparative assessment of human and farm animal faecal microbiota using real-time quantitative PCR. FEMS Microbiol. Ecol. 2009, 68, 351–362. [Google Scholar] [CrossRef] [PubMed]
- Ozato, N.; Yamaguchi, T.; Mori, K.; Katashima, M.; Kumagai, M.; Murashita, K.; Katsuragi, Y.; Tamada, Y.; Kakuta, M.; Imoto, S.; et al. Two Blautia Species Associated with Visceral Fat Accumulation: A One-Year Longitudinal Study. Biology (Basel) 2022, 11. [Google Scholar] [CrossRef] [PubMed]
- Fan, H.Y.; Tung, Y.T.; Yang, Y.S.H.; Hsu, J.B.; Lee, C.Y.; Chang, T.H.; Su, E.C.; Hsieh, R.H.; Chen, Y.C. Parental Vegetable and Fruit Consumption during Pregnancy and Its Effects on Infant Gut Microbiome. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Trompette, A.; Gollwitzer, E.S.; Yadava, K.; Sichelstiel, A.K.; Sprenger, N.; Ngom-Bru, C.; Blanchard, C.; Junt, T.; Nicod, L.P.; Harris, N.L.; et al. Gut microbiota metabolism of dietary fiber influences allergic airway disease and hematopoiesis. Nat. Med. 2014, 20, 159–166. [Google Scholar] [CrossRef]
- Lundgren, S.N.; Madan, J.C.; Emond, J.A.; Morrison, H.G.; Christensen, B.C.; Karagas, M.R.; Hoen, A.G. Parental diet during pregnancy is related with the infant stool microbiome in a delivery mode-dependent manner. Microbiome 2018, 6, 109. [Google Scholar] [CrossRef]
- Won, T.J.; Kim, B.; Oh, E.S.; Bang, J.S.; Lee, Y.J.; Yoo, J.S.; Yu, H.; Yoon, J.; Hyung, K.E.; Park, S.Y.; et al. Immunomodulatory activity of Lactobacillus strains isolated from fermented vegetables and infant stool. Can. J. Physiol. Pharmacol. 2011, 89, 429–434. [Google Scholar] [CrossRef]
- Sun, M.; Luo, J.; Liu, H.; Xi, Y.; Lin, Q. Can Mixed Strains of Lactobacillus and Bifidobacterium Reduce Eczema in Infants under Three Years of Age? A Meta-Analysis. Nutrients 2021, 13. [Google Scholar] [CrossRef]
- Warner, B.B.; Deych, E.; Zhou, Y.; Hall-Moore, C.; Weinstock, G.M.; Sodergren, E.; Shaikh, N.; Hoffmann, J.A.; Linneman, L.A.; Hamvas, A.; et al. Gut bacteria dysbiosis and necrotising enterocolitis in very low birthweight infants: a prospective case-control study. Lancet 2016, 387, 1928–1936. [Google Scholar] [CrossRef] [PubMed]
- Claud, E.C.; Keegan, K.P.; Brulc, J.M.; Lu, L.; Bartels, D.; Glass, E.; Chang, E.B.; Meyer, F.; Antonopoulos, D.A. Bacterial community structure and functional contributions to emergence of health or necrotizing enterocolitis in preterm infants. Microbiome 2013, 1, 20. [Google Scholar] [CrossRef] [PubMed]
- de la Cochetiere, M.F.; Piloquet, H.; des Robert, C.; Darmaun, D.; Galmiche, J.P.; Roze, J.C. Early intestinal bacterial colonization and necrotizing enterocolitis in premature infants: the putative role of Clostridium. Pediatr. Res. 2004, 56, 366–370. [Google Scholar] [CrossRef] [PubMed]
- Heida, F.H.; Harmsen, H.J.; Timmer, A.; Kooi, E.M.; Bos, A.F.; Hulscher, J.B. Identification of bacterial invasion in necrotizing enterocolitis specimens using fluorescent in situ hybridization. J. Perinatol. 2017, 37, 67–72. [Google Scholar] [CrossRef]
- Davidson, S.J.; Barrett, H.L.; Price, S.A.; Callaway, L.K.; Dekker Nitert, M. Probiotics for preventing gestational diabetes. Cochrane Database Syst Rev 2021, 4, CD009951. [Google Scholar] [CrossRef] [PubMed]
- Pellonperä, O.; Vahlberg, T.; Mokkala, K.; Houttu, N.; Koivuniemi, E.; Tertti, K.; Rönnemaa, T.; Laitinen, K. Weight gain and body composition during pregnancy: a randomised pilot trial with probiotics and/or fish oil. Br J Nutr 2021, 126, 541–551. [Google Scholar] [CrossRef] [PubMed]
- Houttu, N.; Mokkala, K.; Saleem, W.T.; Virtanen, S.; Juhila, J.; Koivuniemi, E.; Pellonperä, O.; Tertti, K.; Luokola, P.; Sorsa, T.; et al. Potential pathobionts in vaginal microbiota are affected by fish oil and/or probiotics intervention in overweight and obese pregnant women. Biomed Pharmacother 2022, 149, 112841. [Google Scholar] [CrossRef]
- Xu, Y.P.; Hu, J.M.; Huang, Y.Q.; Shi, L.P. Parental Ureaplasma exposure during pregnancy and the risk of preterm birth and BPD: a meta-analysis. Arch. Gynecol. Obstet. 2022, 306, 1863–1872. [Google Scholar] [CrossRef]
- Dawe, J.P.; McCowan, L.M.E.; Wilson, J.; Okesene-Gafa, K.A.M.; Serlachius, A.S. Probiotics and Parental Mental Health: A Randomised Controlled Trial among Pregnant Women with Obesity. Sci Rep 2020, 10, 1291. [Google Scholar] [CrossRef]
- Teoh, C.M.; Cooper, A.; Renteria, K.M.; Lane, M.; Zhu, J.; Koh, G.Y. Supplementation of Methyl-Donor Nutrients to a High-Fat, High-Sucrose Diet during Pregnancy and Lactation Normalizes Circulating 25-Dihydroxycholecalciferol Levels and Alleviates Inflammation in Offspring. Metabolites 2022, 12. [Google Scholar] [CrossRef]
- Antoun, E.; Kitaba, N.T.; Titcombe, P.; Dalrymple, K.V.; Garratt, E.S.; Barton, S.J.; Murray, R.; Seed, P.T.; Holbrook, J.D.; Kobor, M.S.; et al. Parental dysglycaemia, changes in the infant's epigenome modified with a diet and physical activity intervention in pregnancy: Secondary analysis of a randomised control trial. PLoS Med 2020, 17, e1003229. [Google Scholar] [CrossRef] [PubMed]
- Sandborg, J.; Söderström, E.; Henriksson, P.; Bendtsen, M.; Henström, M.; Leppänen, M.H.; Maddison, R.; Migueles, J.H.; Blomberg, M.; Löf, M. Effectiveness of a Smartphone App to Promote Healthy Weight Gain, Diet, and Physical Activity During Pregnancy (HealthyMoms): Randomized Controlled Trial. JMIR Mhealth Uhealth 2021, 9, e26091. [Google Scholar] [CrossRef] [PubMed]
Figure 1.
Schematic of the pathways maternal nutrition influences the infant gut microbiome. Figure created with Biorender.com.
Figure 1.
Schematic of the pathways maternal nutrition influences the infant gut microbiome. Figure created with Biorender.com.
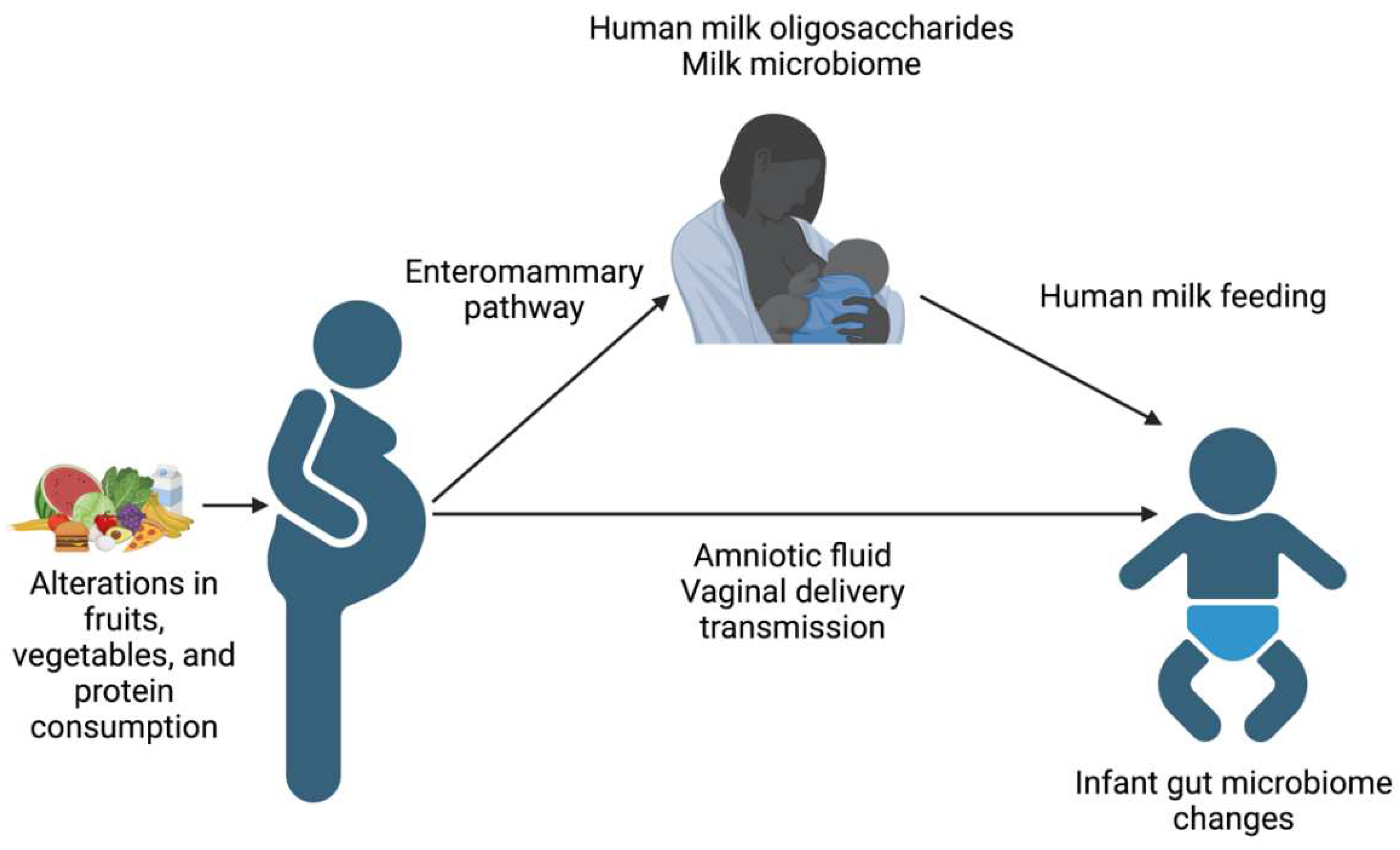

Table 1.
Maternal intestinal microbiome changes due to various anthropometric and nutritional states. References are listed in brackets.
Table 1.
Maternal intestinal microbiome changes due to various anthropometric and nutritional states. References are listed in brackets.
| Maternal Factor | Diversity | Increased Abundance | Decreased Abundance |
|---|---|---|---|
| Elevated pre-pregnancy BMI | Potentially decreased diversity [13] | Firmicutes [14], Bacteroides [16], Clostridium[16], S. aureus [16] Biolphila [17], Roseburia [17], Dialster [17], | Proteobacteria [14], Phascolarctobacterium [17] |
| Underweight | Potentially decreased [35,43,46] | Acidaminococcus [47] | Firmicutes [44], Bacteroidetes [44] |
| Excessive Gestational Weight Gain | Prevotella [17], Dialister [17], Firmicutes [49], Bacteroidetes [49] | Bifidobacterium [16] | |
| Gestational Diabetes | Ruminococcaceae family [66], Faecalibacterium [67], Eubacterium [67], Streptococcus [67], Enterobacteriaceae family [67], Bacteroides [68], | ||
| Fat Intake | Increased Simpson diversity [17] | Ruminococcus [16,17], Paraprevotella [17] | Bacteroidetes, Firmicutes [74] |
| Vegetable Intake | Roseburia [79], Lachnospiraceae [79] | Collinsella [79], Holdemania, Eubacterium [79] | |
| Animal Protein Intake | Increased Shannon diversity [17] | Collinsella [17] | |
| Carbohydrate Intake | Bacteroidetes [74] |
Table 2.
Infant gut microbiome changes due to various anthropometric and nutritional states. References are listed in brackets.
Table 2.
Infant gut microbiome changes due to various anthropometric and nutritional states. References are listed in brackets.
| Maternal Factor | Infant Gut Microbiome Diversity | Infant Gut Microbiome Increased Abundance | Infant Gut Microbiome Decreased Abundance | Infant Gut Microbiome Functional Roles |
|---|---|---|---|---|
| Elevated Pre-pregnancy BMI | Increased [34] | Proteobacteria [14] Vaginal delivery infants [35]: Bacteroides fragilis, Escherichia coli, Veillonella dispar, Staphylococcus, Enterococcus |
Firmicutes [14] | Decreased butyrate production [36] |
| Gestational Weight Gain | Increased [34] | Akkermansia [34] | Enrichment of glucose and glycogen degradation pathways, increased phenylalanine, cysteine/serine, folate, thiamin, biotin, and pyridoxine synthesis pathways [56] | |
| Gestational Diabetes | Decreased [72] | Clostridium [73], Veillonella [73], Firmicutes [72], Streptooccus [66] | Proteobacteria [72], Lactobacillus [66,75], Flavonifractor [75], Erysipelotrichaceae [75], Gammoproteobacteria [75], Bacteroides [66] | |
| Maternal Fat Intake | Firmicutes [76] | Proteobacteria [76], Bacteroides [78] | ||
| Maternal Fruit and Vegetable Intake | Lactobacillus [79], Propionibacteriales [86], Priopionibacteriaceae [86], Cutibacterium [86], Tannerellaceae [86], Parabacteroides [86], Lactococcus [86] | Coprococcus [76], Blautia [76], Roseburia [76], Rumiococcaceae [76], Lachnospiracea [76] | ||
| Maternal Animal Protein | Veillonella [76], Escherichia/Shigella [76], Klebsiella [76], and Clostridium [76] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



