
Submitted:
17 May 2023
Posted:
18 May 2023
You are already at the latest version
Abstract
The worldwide population is undergoing a fundamental change in its age structure, which challenges the health and social services system. The need to migrate towards a more person-centered and coordinated model of care that supports the optimization of abilities and capacities for older people has to be matched. In this sense, eHealth technologies can play a fundamental role. In this paper, through a questionnaire-based data collection on 30 primary (older people) and 32 secondary (informal caregivers) end-users, we share the sustainable way to develop a product optimizing the user experience and ensuring adoption. Both older adults and caregivers consider the use of smartphone and smartwatch to be very important, but also the use of digital devices for healthcare can be helpful. Seniors care about self-monitoring of health parameters using wearable devices, regardless of their health status, and would like to be included in the process of making good health decisions, because they need to feel in control of their healthcare process. Digital solutions in health and care can support the wellbeing of older adults in many areas of their daily lives at home and in their communities, but only if such innovation is designed around the natural voice of the intended target.
Keywords:
active and healthy ageing
; intrinsic capacity
; user-centered design
; eHealth literacy
; technology-based interventions
1. Introduction
The decade 2021–2030 is the Decade of Healthy Ageing [1] that aims to improve the quality of life of older adults and support independent living also using all the opportunities offered by new technologies.
Bringing up to date the classic definition of health launched by the World Health Organization (WHO) [2], in 1948, “Health is a state of complete physical, mental and social well-being and not merely the absence of disease or infirmity”, Rowe and Kahn [3] defined successful ageing as the absence of physical impairment and chronic diseases, as well as optimal social participation and mental well-being. Afterwards, the focus shifted from defining “a state” to defining “the ability”, since health is a dynamic progress, not only a static situation or condition. In 2011, Huber et al. [4] introduced a new concept of health as: “the ability to adapt and to self-manage, in the face of social, physical and emotional challenges”.
Recent research [5] identified ten determinants related to healthy ageing, such as physical activity, diet, self-awareness, outlook/attitude, life-long learning, faith, social support, financial security, community engagement, and independence. It is a growing recognition of the influence of physical, mental/cognitive, and social well-being as determinants of healthy ageing, despite any influence of culture/customs, level of living, age, and varied geographical locations. In relation to mental/cognitive well-being the studies mention: self-awareness, viewpoint/attitude, life-long learning, and faith.
Especially the recent COVID-19 pandemic shows us how vulnerable we are, regardless of age, and why health priorities change from treatment to prevention and early detection. Megatrends show that “the better uses of data and technology are transforming health outcomes for patients and citizens and enhancing our ability to detect threats. A focus on disease prevention, rather than cure, holds promise for a healthier future” [6].
In this regard, the WHO [7] defined Healthy Ageing (HA) as “the process of developing and maintaining the functional ability that enables wellbeing in older age”. Functional Ability (FA) (i.e., the health-related attributes that enable people to be and to do what they have reason to value) is determined by Intrinsic Capacity (IC) (i.e., the composite of all the physical and mental capacities of an individual), the environment (EN) (i.e., all the factors in the extrinsic world that form the context of an individual’s life), and the interactions between the two. FA is composed of the following domains: (1) basic needs, (2) learn, grow and make decisions, (3) mobility, (4) build and maintain relationships, (5) contribute to community/society. EN also includes five domains: (1) products and technology, (2) natural and human-made environment, (3) support and relationship, (4) attitudes and (5) service, systems and policies [8]. Then, the concept of IC is designed to have a “positive” connotation, focusing on the measurement of the residual biological capacities of the organism rather than on its impairments/deficits. Five different domains describe the IC framework: (1) cognition, (2) psychological (i.e., mood and sociality), (3) sensory function (i.e., vision and hearing), (4) vitality (i.e., homeostatic regulation, or balance between energy intake and energy utilization), and (5) locomotion (i.e., muscular function). Each domain closely interacts with the others as part of a dynamically interrelated environment [9]. So, IC decline is significantly associated with increased risk of frailty, disability, falls, fractures and death.
In summary, the combination of IC, FA, and EN gives life to an innovative model proposed by the WHO that has the potential to substantially modify the way in which clinical practice is currently conducted, shifting from disease-centered toward person-centered paradigms.
1.1. Study Objectives
This study is part of the CAREUP (Integrated Care Platform Based on the Monitoring of Older Individual Intrinsic Capacity for Inclusive Health) project that is dedicated to bringing innovation and the latest achievements of digital healthcare into people’s life. The aim of the project is to develop an intervention for the continuous improvement of the quality of life of older adults, leveraging on an ICT-based solution (the CAREUP platform) oriented towards health promotion and disease prevention in later life. The CAREUP platform will be useful to slow down the decline of intrinsic capacity (the totality of all physical and mental abilities that an individual draws on during his/her lifetime), which is very important for older adults and their families or caregivers. Also, considering the healthcare process perspective as a personalized, predictive and integrative process, with a special focus on individual participation.
A major factor identified as a point of failure in the development and implementation of health information systems is the limited understanding of users, their needs, and the contexts in which the systems are used. Therefore, it is important to understand end-user needs from multiple perspectives [10,11].
Within this manuscript, we are interested in sharing the older adults’ challenges and their perceptions as an underlying factor of their involvement in the use of the new CAREUP platform. Furthermore, we work to improve their experience as senior users and develop a ready to market product, according to their needs and interests. This is why studying people attitudes and experiences before, during and after interacting with the ICT-based solutions is mandatory.
Therefore, the research objective is to understand the primary (older adults) and secondary (caregivers, family members) end users’ perspectives on the proposed CAREUP platform by inquiring their attitude to self-monitoring. This is the sustainable way to develop a product optimizing the user experience and ensuring adoption.
2. Materials and Methods
2.1. The CAREUP-based intervention
The CAREUP platform architecture is exhibiting a modular and expandable design in which interoperability and standardization are considered together with a cost-effective selection of the integrated technologies. These comprise sensors and devices for health and home monitoring, activity and sleep monitoring as well as gamification elements developed for Android platforms. Both software and hardware multiprotocol gateways are used for data collection and subsequent transfer to a central server. Data collected with different technologies and processed with AI algorithms are used to evaluate and predict the progress of the platform user in terms of IC. For this purpose, Python is used as the main programming language as it provides highly reliable libraries such as sci-kit-learn, and general-purpose efficient matrix operations libraries.
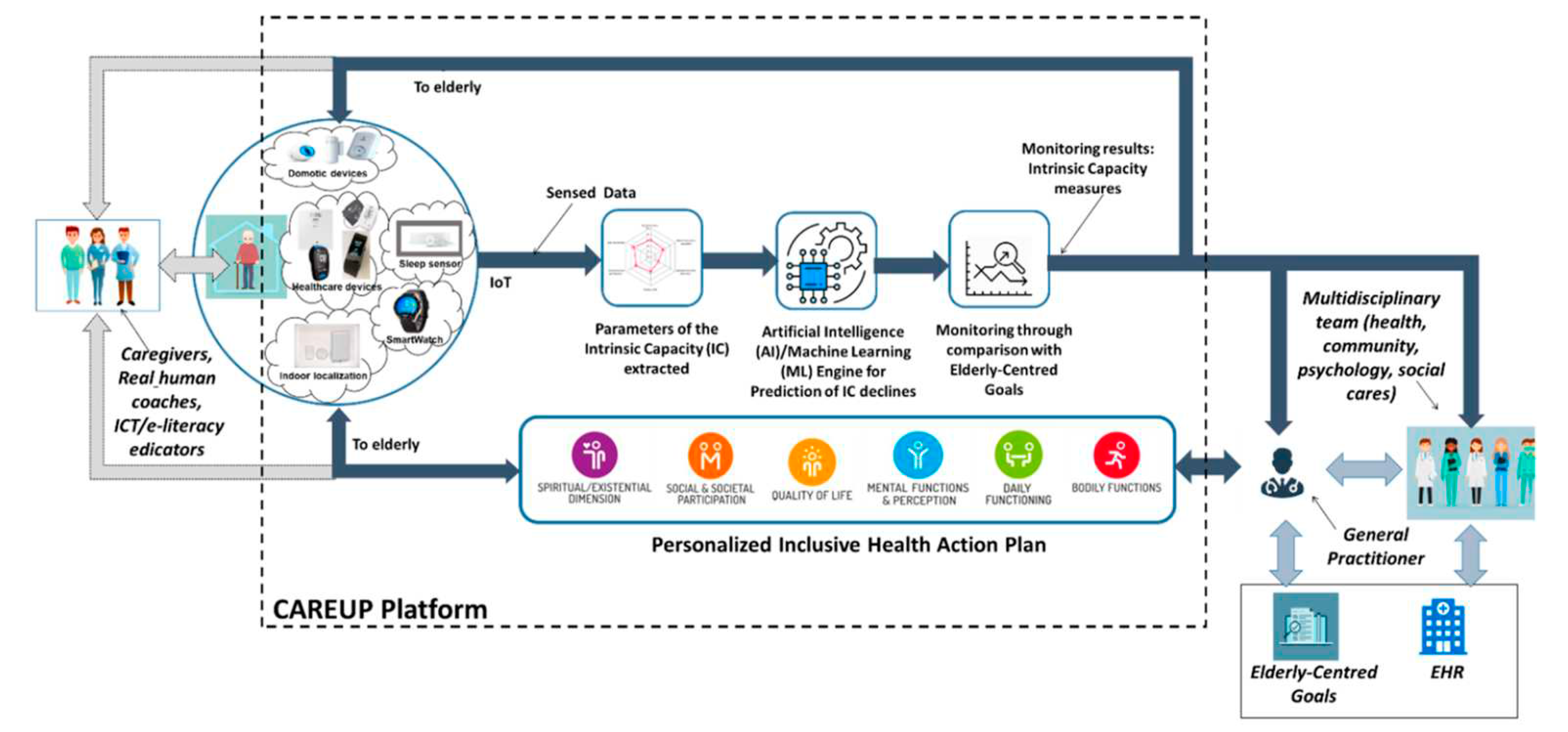
Indeed, the CAREUP platform (Figure 1) is a system integrated with devices, sensors and functionalities dedicated to assess and compensate the declines in the IC of individuals in relation with their specific environments. It is a tool for primary users (care plan performance to help to slow down IC declines), their caregivers (availability of the care plan reduces caregiver's burden) and healthcare professionals (monitoring data help in primary user's health status evaluation).
CAREUP will provide the user with a visualization of his health status in the form of an intuitively easy to interpret the IC domains. Furthermore, CAREUP will visualize changes in health status and compare these with self-defined health goals
The General Practitioner (GP) is the older individual’s first point of contact with the platform. The GP together with the Multidisciplinary team (i.e. group of persons involved in care: physicians, nurses, social care workers, etc.) and family members helps to identify the person-centered goals. Monitoring and IC evaluation results, goals and EHR data are the basis for development of the Personalized Inclusive Health Action Plan. The care planning process is focused on older individual needs, values and preferences. The plan defines activities to be performed and specifies tools to be used to compensate identified IC declines in particular PH domains. Caregivers and coaches have access to monitoring data and the plan, their role consist in monitoring progress and supporting plan implementation. The elderly person can observe his results which increases awareness about the health. The IC evaluation is carried out periodically at weekly intervals, based on the current sets of collected data.
An innovative approach in CAREUP is the gamification functionality. Specially designed gamification elements will aid in diagnosing and improving the physical and mental health of the primary users. The diagnosis part will mostly entail gamified tests (a core innovation of the project) while the mitigation part will focus on long-term adherence, the main challenge that many platforms for seniors struggle nowadays, and one that AAL calls have intensively insisted on. Unity 3D will be mostly used for developing the games. It is a versatile development platform, widely used in the game development industry.
2.2. The method
According to the User Centered Design approach [12], a dedicated phase of the CAREUP platform definition is the end users’ needs analysis reported in this study. For that purpose, a structured interview guide was used to gather information from both older adults and informal caregivers. The tool is a questionnaire with a pre-defined set of open-ended and closed-ended questions. Closed-ended questions allow a limited range of answers. Options and responses are rated with 3, 4, 5 points Linkert scale that might measure the level of agreement or their feelings regarding the topic. Open-ended response permit respondents to share their ideas and suggestions with us. Dimensions and sub-dimensions were used to build the tool for older adults and caregivers. The questionnaire designed for older adults’ requests information on: socio-demo characteristics and self-reported health status, attitude to health and integrated care from home (i.e., self-monitoring), perceived benefits, intention to use, adherence to the Care Plan. Questionnaire for caregivers’ requests information on: attitude to monitor the loved one, perceived barriers.
2.3. The end-users’ involvement and recruiting strategy
According to the CAREUP project activities, primary end-users are older adults, the ones for whom the platform is envisioned with the main aim to help them live longer and improve their life quality as they age. Secondary users are adults who directly benefit from the implementation of the platform, especially informal caregivers (family members, friends).
For this research, convenience sampling of older adults and caregivers was used. The recruitment was performed in three European countries (Austria, Italy and Romania) at the headquarter of the organizations (EURAG for Austria, INRCA for Italy and AAIF for Romania). Inclusion and exclusion criteria were defined for both groups of end-users.
The Inclusion criteria for primary end-users are: age over 65 years, living independently in their home or care facilities, having basic ICT skills, able to agree and to sign the Informed Consent. The Exclusion criteria are one of the following: failure to meet the inclusion criteria, severe cognitive impairment, severe behavioral syndromes not compensated by medications, significant visual or hearing impairment, or incapacity to give informed consent.
The Inclusion criteria for secondary end-users are: Age over 18 years old, willingness to participate voluntarily in the investigation; capacity to sign the Informed Consent. The Exclusion criteria are: failure to meet the inclusion criteria or the incapacity to give informed consent. In this research, we involved especially informal caregivers (family members, persons listed as trusted contact) who help older adults in performing daily activities, shopping, meal preparation, money management, light housework, laundry, etc.
Different recruiting strategies were used in the three centers. We first pre-selected to reach those participants who can give us valuable feedback for the purpose of our study.
In Austria, various tools were used by EURAG to recruit participants such as mailings, telephone calls, and article in the EURAG newsletter. In the calls for the study for primary users, the project idea was briefly explained, also what requirements must be met for participation (inclusion criteria), and how long the interview will take. The interested parties responded to these calls, appointments were made for the interviews (either in the office of the organization or in the homes of the participants) and queries or open questions were clarified. Interviews were held in compliance with special safety measures such as keeping distance, disinfecting hands and objects used in the study. As secondary users are quite busy, on the one hand because most of them work full-time or can't leave the person they care for alone and on the other hand with the support of their relatives, only some interviews (5) could be conducted in person, for others (7) an online questionnaire was set up and sent by email and filled in by the informal caregivers.
In Italy, 10 primary and 10 secondary users were informed of the project objectives, methods, and timing, and we underlined to them that participation in the study was completely voluntary, and that they could leave the study at any time without providing any explanation. The staff then asked participants specific screening questions to check their inclusion characteristics. Nobody refused to attend, and participants signed a written document giving their informed consent for the processing of their data, in accordance with the GDPR 2016 and national legislation on privacy and data protection. After the signature, each participant watched the slides presentation and then responded to the interview. The recruitment was performed in rural and urban context.
In Romania, most participants were recruited using an internal social network of seniors, and after that, contacting each one by phone. People were informed using social media (e.g., posts on the AAIF Facebook page, website, etc.), mailings, and person-to-person contacts. Before their enrollment, information was offered to targeted people. The features and services of the CAREUP platform were explained. People were informed about the purpose of the survey, how the interview was conducted, and how the results were collected and used.
2.3. The interview administration
In Austria, 8 interviews with seniors were conducted, including individual interviews, one of which was conducted via telephone (due to a last-minute scheduling conflict of the participant). The interviews took place in the EURAG office and participants' homes. Some of the 12 interviews with secondary users (5) took place in EURAG's premises as individual interviews and (7) responses were received via an online questionnaire (Lime Survey).
INRCA conducted only individual interviews in Italy, half performed by telephone and the other half at participants’ homes.
In Romania, AAIF conducted 12 interviews with older adults. Seniors were invited to AAIF premises, after a short description of the meeting. The CAREUP project, platform, and objectives of the meeting were explained. There were 3 groups of people, but the questionnaires were administered to each person individually by AAIF researchers.
In total, we collected responses from 30 primary end-users and 32 secondary end-users. Only one older adult is withdrawn.
3. Results
3.1. Primary Users
3.1.1. Sample description
Questionnaires were applied to 30 older adults, of which 8 were in Austria, 10 in Italy, and 12 in Romania. The distribution by age category is balanced so that we had 7 participants (a percentage of 23%) between 65 and 70 years old, 7 (23%) aged between 71 and 75 years old, 9 (30%) aged between 76 and 80 years old and 7 (23%) aged over 80 years. Respondents are primarily women, 19 females and 11 males. Most older adults (70%) are retired, and one-third (30%) are retired and still working. 63% of the respondents live in urban areas, less (36%) in rural areas, and only three individuals (10%) spend the summer in the countryside. One-third of the respondents live alone, and two-thirds live with someone else.
3.1.2. Attitude to health and the use of eHealth technology
To gain information about the attitude to health of the involved primary end users, the questionnaire contained specific items about self-assessment of the health status. The respondents are physically active people, for example, there are 12 older adults who do physical activity for 6-7 days a week. 10 seniors do physical activity for 4-5 days a week, whereas 8 respondents for less than three days a week.
On mood, out of 30 participants, 12 seniors (40%) said they have no problems with anxiety or worrying. 15 respondents (50%) declared that they feel anxious 5-6 days a week and 3 feel anxious every day. While 19 respondents (63%) said they do not experience depression, 9 seniors (30%) stated that they feel hopeless, with no interest or pleasure in doing things for 5-6 days a week. Moreover, 2 older adults (7%) said they feel down and depressed almost every day.
The participants declared they have social interactions “always” (10%) or “often” (60%), only 9 seniors interact “sometimes” (20%). Few respondents said they interact “rarely” (7%) or “never” (3%).
About the type of technology that older adults consider important to have in use, most of them (18) considered it as “extremely important” to use a smartphone or a smartwatch. Then, it is “very important” (16 seniors) to use digital devices for healthcare and “slightly important” (10) to use a tablet or other touchscreen devices. The respondents believed that it is “not important” to use virtual assistants (15 seniors) and laptop or personal computer (PC) (11).
Smartphone was best valued. More than half of the participants (18) considered it like ‘’extremely important” (60%) and 6 older adults like ‘’very important”. On the other hand, only 3 seniors said that it is ‘’slightly important” and another 3 that it is ‘’not important at all”. The breakdown by country shows broadly the same distribution, then most people in each country consider the use of smartphone/smartwatch to be extremely important or very important.
On second place at the top of the user preferences were the digital devices used in healthcare, thus 12 respondents considered their use as “extremely important” and 16 like “very important”. The least appreciated was the use of virtual assistants. The distribution by country closely follows the total distribution. So, most people in Austria (5 out of 8) and Italy (6 out of 10) considered that it is “very important” to use digital devices in healthcare, and in Romania most people (7 out of 12) said that the use of digital devices is “extremely important” or “very important”. Not a single person declared that the use of digital devices is “not at all” important in any of the considered countries. This is significant because it shows awareness of the importance of using devices for healthcare like the proposed solution (CAREUP platform).
Regarding the interest in cognitive games, out of a total of 30 people, 16 used digital devices to play games and 14 didn't use it for this purpose. Among the players, 8 seniors played boardgames (e.g., crosswords, cards, solitaire, sudoku, crosswords, Remi, monopoly, Bridge, and chess), 6 played digital games on PC, mobile phone or tablet (e.g., solitaire, sorting balls, Mhajong, Hexa Block Puzzle), and 2 played both types of games. Among those who play, the majority (11 people) said they would like to receive a score after the game, only 2 respondents said “no” and 3 “don't know”.
Most players (11) declared that “it is exciting to get a price for their performance or a token to use in future games”, only 2 said “no” and 1 “doesn't know”. Moreover, 10 players replied that “they like to receive a score and consider it exciting to get a token”. Finally, on average, they spend 1 hour and a half playing PC games.
Self-perceived health status is central to our study because the indicator has been linked to increased use of health services. Only a third of the participants said that their health is “very good” (10 people, respectively 31%) and, no one called it “excellent”. On the other hand, the respondents declared that their health is “good” (38%) or “fair” (28%), and one person assessed his/her health as “poor”.
Studying whether people are interested in self-care, we asked “would these features help you take care of your own health at home?”. About 2/3 of the respondents (70%) declared that the self-monitoring of health parameters is very important for their health. Half of them live in Romania. Only 5 seniors (17%) said that self-monitoring is moderately important, mostly in Italy, and 4 (13%) said that it is not important at all. If we analyze the attitude (or intention) to self-monitoring according to the health status, we notice that there is no strong correlation. Anyway, all people whose health is just “fair” declared that self-monitoring of health parameters is very important. So, we can assume that people care about self-monitoring of health parameters regardless of their health status. Only 10 older adults considered that the assessment of physical activity by tests is very important, mostly in Romania. On the other hand, 15 participants thought that it is moderately important, mostly in Italy. Then, 5 seniors stated that the physical assessment is not important, most of them coming from Austria. More than half of the respondents, namely 17 people, said that the assessment of mental activity and mood by questionnaires is very important. Most of them are seniors from Romania. Also, 10 participants thought that the mental assessment is moderately important and only 3 said that it is not important at all.
To evaluate intention to use the CAREUP solution, respondents were asked “Do you think you would use one of the above-mentioned functions on a digital platform, if you were offered the opportunity?”. Out of a total of 30 people, only 11 older adults (36%) intended to use the CAREUP solution independently at home, whereas 14 (47%) would have liked to use it together with a healthcare professional, mostly in Italy and Romania. Then, only 5 seniors said they don't intend to use technology even if they are offered the opportunity. In general, most people (76,6%) stated that they would agree to wear sensors to measure health parameters. The distribution by countries shows that more respondents from Italy and Romania agree on sensor technology compared to Austria, but the numbers are too small to generalise such conclusions. Out of 22 people who would agree to wear sensors, 9 said that they want to wear it during the day, 3 during the day and night, and 10 affirmed that they would wear sensors just for a quick health assessment. Out of these 22 people who agree to wear sensors and share health information and data with someone, 16 older adults would have trusted medical doctor or experts, 4 would have relied on family and medical doctor, 2 would have shared data with anyone, if the platform had been safe and transparent. So, people trust health specialists and rely on their medical guidance and advice, especially when it comes to their own health, but also assistance in monitoring or sharing health data with someone.
We then investigated the perceived benefits of the CAREUP solution in order to improve the platform in response to user expectations and needs. Also, 7 respondents considered it relevant that wearable sensors allow collecting and measuring multiple health parameters at the same time, and 16 seniors appreciated the real-time monitoring of health parameters, mostly in Romania. Majority, 22 people considered relevant the opportunity to signal and receive a message when abnormal values are recorded, especially in Austria and Italy. It would seem that older adults see benefits in using wearable devices (e.g., wristbands, smartwatches) to collect information and monitor their physical activity. So, 12 seniors said that keeping track of physical activity meets their needs, 18 appreciated especially the opportunity to monitor movement and prevent falls, and 14 considered it relevant to receive a report about their physical activity progress. Only 2 participants from Austria said that none of these features are relevant to meet their needs. The respondents considered that monitoring mental and emotional health meets their needs. 19 people best valued the activities recommended by medical professionals to maintain their emotional balance, self-control, stress management, etc., mostly in Romania and Austria. Then, 15 seniors considered that is important to keep track of mental activity and mood changes, even more than tracking physical activity. Similar, 14 seniors were interested in keeping their mental health by receiving smart games and cognitive activities designed for older adults to improve cognitive function. In summary, seniors see immediate benefits in 1) reporting and receiving a message when outliers are recorded; 2) detecting movement to prevent falls; 3) recommending to maintain emotional balance, self-control, stress management, etc.; 4) real-time monitoring health values; 5) receiving a progress report; 6) evaluating and improving cognitive function.
3.1.3. Care Plan: Decision making process, Desired and useful features, Perceived barriers
Most of the respondents (26) thought that it is very important to be included in the process of making good health decisions, because they need to feel in control of their healthcare process. However, only 2 seniors said that their involvement is moderately important and other 2 that is not important at all, both of them come from Romania. It is also true that these 2 persons self-assessed their physical health as “good” and they would not have been willing to wear body sensors. About the care plan desired features, most seniors (22) wanted to know when a quick intervention is needed by signaling a situation of risk by receiving an alarm or alert message. Also, 17 people appreciated that the intervention is personalized, based on collected health parameters and physical and mental capacities decline, and other 17 said that is relevant that the care plan allows them to know when their situation changes. Similar, 16 older adults were interested in receiving quick intervention when needed. Only 15 people appreciated that the care plan is developed by a multidisciplinary team and 11 agreed that the care plan would keep them motivated and engaged. About the care plan useful features, most respondents (28) said that they were interested in measuring their health parameters, and 26 in receiving a signal or an alert message when a decline in the IC is detected. Also, 23 people were interested in having a personalized care plan and 22 said that they want to allow the care team to send recommendations for investigations, specialist medical consultations based on health assessment, medical advices, etc. Similar, they were interested in the prevention or early detection of any medical conditions/disorders that could be based on their physical and mental capacities decline. Moreover, 20 participants were interested in having self-defined health goals according to their health status and vulnerability, and only 19 people wanted to get information about the prediction of their physical and mental capacities decline. The use of digital platform and smart sensors could be hindered by real obstacles or perceived barriers. We investigated the opinion of users regarding these difficulties to know how to develop the CAREUP platform and facilitate its adoption. First, 16 respondents considered that a poor experience in using technology could be an important barrier. The second perceived barrier was that the platform would not be easy to use (16 people). On the other hand, 9 seniors were worried about the possible doctor's refusal to work with data that he/she has not collected him/herself and does not rely on. Moreover, 6 older adults were concerned for their safety and personal data protection. Fewer participants (5) considered that the preference for traditional care and visiting the doctor's office could be a barrier. Also, 1 senior from Austria explained that “advice from GP is more trustworthy than the advice from the platform”. It is good that not one person said that the lack of confidence in the benefits of technology would be a barrier, and neither the feeling of stigma when using such a system.
3.2. Secondary Users
3.2.1. Sample description
The group of caregivers consists of 32 people, of which 12 were in Austria, 10 in Italy, and 10 in Romania. We included only informal caregivers who could help older adults by using the proposed CAREUP platform. Mostly they are very close to seniors, and they know better their needs and expectations. The majority of caregivers (26/32 individuals) are active employees, only 4 are retired, and 2 are retired and still working. 29/32 respondents live in urban areas, whereas only 3 lives in rural areas. For the two third of respondents (22/32), use a smartphone or smartwatch is considered “extremely important”, but also, the use of digital devices for healthcare (17/32) can be helpful. Only few caregivers prefer to use a laptop (8/32), tablet or other touchscreen devices and services such as virtual assistants. Half of the respondents (15/32) said that their care receiver monitors health parameters at home at least once a week, especially people from Austria, whereas Romanian older adults monitor their parameters once a month, or a few times a year, especially in Italy. Most respondents (29/32) declared that the self-monitoring of health parameters is very important for their care-receiver health. According to the respondents’ preferences, it would be relevant to assess the activities of their beloved related to social engagement and interaction (30/32), physical activity (29/32), cognitive activities (28/32) and mood changes (30/32).
3.2.2. Perspective on the CAREUP solution
Out of a total of 32 respondents, 25 caregivers said that using the CAREUP platform would help to improve the caregiving process. Two third (22/32) said that the use of the platform would lead to stress reduction and increased quality of life (19/32). The majority of caregivers, 27/32, stated that they agree to support the older adult to use the platform correctly and effectively since it will offer a lot of information and measurements that could help them better to evaluate the current health status of the older adult. Most respondents (28/32) appreciated that the system could send information on the values of health parameters and their variation over time. Indeed, caregivers believe that using the platform could have an impact on the health status of older adults, as it encourages self-care and self-monitoring (23/32), and treatment adherence (11/32), so making the care process easier. Another benefit is that caregivers could have early information on the deterioration of health and IC decline (21/32). Some respondents (12/32) mentioned that using the CAREUP platform could have positive consequences on overcoming the stigma today applied to individuals experiencing age-related decline. In terms of barriers, that might prevent them from using the technology-based solution to its maximum capacity, most caregivers (18/32) are concerned about the fact that collected data are not reliable due to different circumstances like the wrong usage of the devices. Moreover, older adults cannot be able to make the best decision for the benefit of their health, said 14 people. Also, 13 people are concerned about some emergency situations that could appear and facing older adults with life-threatening emergencies. On the other hand, using the platform could confuse the doctors in their diagnosis or put a pressure if they do not know if the collected data are reliable or not, said 10 people.
4. Discussion
To make a sustainable product optimizing the user experience and ensuring adoption, in the proposed technology-based solution we engage users throughout the development process according to the ISO standard [12]. The aim was to understand seniors’ and caregivers’ perceptions, needs, and habits, interpret the motivations behind their behaviors and uncover the barriers or frustrations face during the interaction with the system. Since for older adults, it is important to maintain a healthy lifestyle, be physically well and have a good mental status, we intend to learn and understand the reasons behind their behaviors, choices, and positive perceptions. This aims to make systems usable and useful by focusing on the users, their needs and requirements, ensuring the sustainability of the eHealth product.
Indeed, electronic health tools provide little value if the intended users lack the skills to engage usingthem effectively. Engaging with eHealth requires a skill set, or literacy, of its own. The concept of eHealth literacy is introduced and defined as the ability to seek, find, understand, and appraise health information from electronic sources and apply the knowledge gained to addressing or solving a health problem [13].
Seniors over 65 years are not a heterogeneous group, but a very diverse one regarding their health status, attitudes, and interests. There are personal limitations related to age and health problems, from diminishing physical capabilities and cognitive difficulties to the skill to use digital devices and the related self-confidence. That is exactly why older adults’ personal experiences, social interactions, and familiarity with technology are relevant. Results show that comparatively, older adults are more interested in using technology. Such use is related to the benefits they value: keeping values within normal parameters and identifying risk values, maintaining cognitive function and emotional balance, preventing injuries, etc. In general, older adults are willing to wear body sensors due to beneficial reasons for their health and are confident to share their health data with someone they trust. Some of them would use the self-monitoring techniques and technology independently, but more of them would need a piece of advice because people trust healthcare specialists and rely on their medical advice and guidance, especially regarding health technology. Older adults are aware of the many benefits that using technology has on healthy life. Still, their use in daily life depends on several factors such as immediate help or action happening without delay. Elderly users see immediate benefits in reporting and receiving a message when outliers are recorded; detecting movement to prevent falls; recommending to maintain emotional balance, self-control, stress management, etc.; real-time monitoring health values; receiving a progress report; evaluating and improving cognitive function. Easy to use is still a condition to facilitate daily usage. On the contrary, we could assume that the difficulty lies in the solution’s novelty and the need to learn a new health-related behavior. Even so, people are keen to learn, but learning needs an external “sign to action” that it is good to engage in this new behavior (e.g., training, external events, social support).
Some questions asked about health problems, personal preferences, the help they need and expect from caregivers may have been too private and intrusive. Consequently, the answers given may result from traditions and cultural biases. It can therefore be assumed that there are different situations in which older adults may have problems finding the help they need. For example, due to progressive social isolation, some seniors experience moods of anxiety and depression, often difficult to treat due to relapses and/or cognitive deterioration [14,15].
After all, for age-related reasons, older adults tend to pay more attention to physical symptoms than mental difficulties. Self-perceived health status is important, not only because it plays a key role in health, but also because it is related to adopting a lifestyle that promotes health itself [16]. This is also significant because this indicator has been related to the increased use of health services.
Many factors influence the intention of seniors to use healthcare technologies. In this study, the intention of older adults to use the CAREUP platform in their daily lives seems to be linked more to the attitude of self-confidence and the perception of control over their state of health, for example through self-monitoring of health parameters. Self-confidence and empowerment trigger positive feelings toward themselves and control over their life and/or life satisfaction [17].
The use of technology has multiple benefits confirmed over the years on the health and aging process of people. Perceived benefit refers to the perception of positive consequences caused by a specific action. In behavioral medicine, the term “perceived benefit” is often used to explain the motivations that drive an individual to perform a behavior and/or adopt an intervention or treatment. Perceived benefits have been used to measure positive perceptions because it is believed that a behavior is driven by an individual’s cognition in terms of acceptability, motives, and attitudes toward such behavior or psychology, especially if positive [18].
If seniors think that it is very easy to use a certain technology, then it is likely that they will try to use it. On the contrary, we could assume that the difficulty lies in the solution’s novelty and the need to learn something new. Indeed, the adoption of new health-related behavior is often determined by experience and personal resources, as well as social influence. However, it is likely that if people think it is worth it, they will choose to learn and adopt a new behavior [19,20].
According to Mannheim et al. [21], autonomy concerns a person’s right to make their own decisions about life independently. For seniors, this is highly associated with decision-making concerning the care, housing, social activities, and even the end of life. Including the individual in the decision-making process of good health is important. Older adults prefer to consider information that is important and/or familiar to them and prefer simpler, more personalized strategies, becoming less willing to take risks [22]. Taking an active role in their healthcare is the best way for them to adhere to healthy ageing.
Regarding the involvement of secondary users, our study shows that caregivers want to know that their loved ones are well and are available to help them use the proposed solution. Considering that people act according to their interests and beliefs, if caregivers feel that healthcare is important, then it is likely that they will promote and encourage older adults to use the CAREUP platform [23].
Moreover, the use of multiple and heterogeneous data-driven decision-making system can drive the transformation of preventive and healthcare pathways towards real needs of individuals and society. In order to drive such process ethically, it is fundamental to involve citizens in a participative process that requires the increase of health literacy, and the empowerment of citizens as data owners [24]. The increase in interconnectivity reinforce our underlying interdependence, thus Digital Cooperation across domains and across borders is critical to realize the transformational potential of digital technologies, while safeguarding against risks and unintended consequences [25].
This study confirms that the acceptance and use of technology rely on the active involvement of people and professionals, responding to the real needs of end users and building a responsible perception of positive health, prevention and integrated care [26,27]. Despite the benefits of collecting and comparing these different perspectives, the specific national centrality of Italy, Romania and Austria, as well as gender disparities in the sample size, could be seen as bias and have significant limitations that do not allow for the generalization of results. Furthermore, the sole use of a questionnaire is also a limitation: a mixed-methods approach could have guaranteed a broad understanding of thoughts. These limitations can be assumed as suggestions for future research in the field.
5. Conclusions
Digital solutions in health and care can support the well-being of older adults in many areas of their daily lives at home and in their communities. As a matter of fact, to guarantee this support, health and social services need to be re-oriented towards a more person-centered and coordinated model of care that supports the optimisation of abilities and capacities for older people. In such a scenario, empowering older adults to learn to take care of their health because it fits with and is integrated with their personal life-centred goals. Indeed, before proposing empowering and coaching, with or without eHealth devices, we still need to understand how to support all the ageing needs and changes by listening to the authentic voice of older adults facing their life every day in their community. Even if much research seems to have explored this field, nowadays, the innovative tools are still far from a huge acceptance and usage, and the silver market is still a landscape to explore. Once again, it is mandatory to underline the adoption of technical solutions and services, and finally, its commercialisation requires users’ involvement in almost every stage of development and testing. This mission is pursued by initiating and conducting collaborative, multisectoral, and transdisciplinary research as well as adapt person-centered integrated care focusing on the needs of older people.
Author Contributions
Conceptualization, M.V., V.S. and M.R., Methodology, M.V., L.S., M.D.M., investigation, M.V., V.S., M.R., E.V., writing—original draft preparation, M.V., V.S., M.R, writing—review and editing M.D.M, L.S., E.R., S.G., B.B., O.C., L.M., J.K., J.A.
All authors have read and agreed to the published version of the manuscript.
Funding
This research was co-funded by the Active and Assisted Living Program (reference no. aal-2021-8-95-CP). This study was also partially supported by Ricerca Corrente funding from the Italian Ministry of Health to IRCCS INRCA, Istituto di Ricovero e Cura a Carattere Scientifico Istituto Nazionale Ricovero e Cura per Anziani (Scientific Institute for Research, Hospitalization, andHealthcare National Institute of Health and Science on Aging).
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki.
Informed Consent Statement
Written informed consent was obtained from all subjects involved in the study.
Data Availability Statement
The data presented in this study are available in the article itself.
Acknowledgment
This work was undertaken in the context of the CAREUP aal-2021-8-95-CP project “Integrated Care Platform Based on the Monitoring of Older Individual Intrinsic Capacity for Inclusive Health (CAREUP)”. The AAL JP is partially funded by the AAL JP countries. We thank the CAREUP AAL participating NationalFunding Bodies for their support.
Conflicts of Interest
The authors declare no conflict of interest.
References
- World Health Organization. Decade of Healthy Ageing: Baseline Report; World Health Organization: Geneva, Switzerland, 2020. [Google Scholar]
- World Health Organization, Constitution. Available online: https://www.who.int/about/governance/constitution (accessed on 9 January 2023).
- Rowe, J.W.; Kahn, R.L. Human aging: Usual and successful. Science 1987, 237, 143–149. [Google Scholar] [CrossRef] [PubMed]
- Huber, M.; Knottnerus, J.A.; Green, L.; van der Horst, H.; Jadad, A.R.; Kromhout, D.; Leonard, B.; Lorig, K.; Loureiro, M.I.; van der Meer, J.W.M.; et al. How should we define health? BMJ-Brit. Med. J. 2011, 343. [Google Scholar] [CrossRef] [PubMed]
- Abud, T.; Kounidas, G.; Martin, K.R.; Werth, M.; Cooper, K.; Myint, P.K. Determinants of healthy ageing: A systematic review of contemporary literature. Aging Clin. Exp. Res. 2022, 34, 1215–1223. [Google Scholar] [CrossRef] [PubMed]
- European Commission, Shifting Health Challenges. Available online: https://knowledge4policy.ec.europa.eu/shifting-health-challenges_en (accessed on 10 January 2023).
- World Health Organization. World Report on Ageing and Health; World Health Organization: Geneva, Switzerland, 2015. [Google Scholar]
- Golino, H.; Thiyagarajan, J.A.; Sadana, R.; Teles, M.; Christensen, A.P.; Boker, S.M. Investigating the broad domains of intrinsic capacity, functional ability and environment: An exploratory graph analysis approach for improving analytical methodologies for measuring healthy aging. 2020.
- Cesari, M.; Araujo de Carvalho, I.; Thiyagarajan, J.A.; Cooper, C.; Martin, F.C.; Reginster, J.-Y.; Vellas, B.; Beard, J.R. Evidence for the domains supporting the construct of intrinsic capacity. J. Gerontol. 2018, 73, 1653–1660. [Google Scholar] [CrossRef] [PubMed]
- Schlomann, A.; Seifert, A.; Zank, S.; Woopen, C.; Rietz, C. Use of Information and Communication Technology (ICT) devices among the oldest-old: Loneliness, anomie, and autonomy. Innov. Aging 2020, 4, igz050. [Google Scholar] [CrossRef] [PubMed]
- Ienca, M.; Schneble, C.; Kressig, R.W.; Wangmo, T. Digital health interventions for healthy ageing: A qualitative user evaluation and ethical assessment. BMC Geriatr. 2021, 21, 1–10. [Google Scholar] [CrossRef] [PubMed]
- ISO 9241-210:2010, Ergonomics of Human-System Interaction—Part 210: Human-Centred Design for Interactive Systems. Available online: https://www.iso.org/standard/52075.html (accessed on 9 January 2023).
- Norman, C.D.; Skinner, H.A. eHealth literacy: Essential skills for consumer health in a networked world. J. Med. Internet Res. 2006, 8, e506. [Google Scholar] [CrossRef] [PubMed]
- Singer, C. Health effects of social isolation and loneliness. J. Aging Life Care 2018, 28, 4–8. [Google Scholar]
- Malcolm, M.; Frost, H.; Cowie, J. Loneliness and social isolation causal association with health-related life-style risk in older adults: A systematic review and meta-analysis protocol. Syst. Rev. 2019, 8, 1–8. [Google Scholar] [CrossRef]
- Zangão, M.O. Self-perceived health status. In Handbook of Research on Health Systems and Organizations for an Aging Society; Fonseca, C., Lopes, M.J., Mendes, D., Mendes, F., García-Alonso, J., Eds.; IGI Global: Hershey, PA, 2020; pp. 1–11. [Google Scholar]
- Chipps, J.; Jarvis, M.A.; Ramlall, S. The effectiveness of e-Interventions on reducing social isolation in older persons: A systematic review of systematic reviews. J. Telemed. Telecare 2017, 23, 817–827. [Google Scholar] [CrossRef]
- Leung, Y. Perceived benefits. In Encyclopedia of Behavioral Medicine; Gellman, M.D., Turner, J.R., Eds.; Springer: New York, NY, 2013; pp. 1450–1451. [Google Scholar]
- Quan-Hasse, A.; Williams, C.; Kicevski, M.; Elueze, I.; Wellman, B. Dividing the grey divide: Deconstructing myths about older adults’ online activities, skills, and attitudes. Am. Behav. Sci. 2018, 62, 1207–1228. [Google Scholar] [CrossRef]
- Schreurs, K.; Quan-Haase, A.; Martin, K. Problematizing the digital literacy paradox in the context of older adults’ ICT use. Can. J. Commun. 2017, 42, 359–377. [Google Scholar] [CrossRef]
- Mannheim, I.; Schwartz, E.; Xi, W.; Buttigieg, S.C.; McDonnell-Naughton, M.; Wouters, E.J.M.; van Zaalen, Y. Inclusion of older adults in the research and design of digital technology. Int. J. Environ. Res. Public Health 2019, 16, 3718. [Google Scholar] [CrossRef]
- Simons Foundation, How Decision-Making Changes with Age. Available online: https://www.simonsfoundation.org/2022/03/02/how-decision-making-changes-with-age (accessed on 11 January 2023).
- De Angeli, A.; Jovanovi´c, M.; McNeill, A.; Coventry, L. Desires for active ageing technology. Int. J. Hum. Comput. 2020, 138, 102412. [Google Scholar] [CrossRef]
- Mucchi, L.; Jayousi, S.; Caputo, S.; Paoletti, E.; Zoppi, P.; Geli, S.; Dioniso, P. How 6G Technology Can Change the Future Wireless Healthcare. In 2020 2nd 6G Wireless Summit (6G SUMMIT), Levi, Finland, 17-20 March 2020.
- United Nations, The Age of Digital Interdependence: Report of the UN Secretary-General's High-Level Panel on Digital Cooperation. Available online: https://digitallibrary.un.org/record/3865925 (accessed on 10 January 2023).
- Menghi, R.; Ceccacci, S.; Gullà, F.; Cavalieri, L.; Germani, M.; Bevilacqua, R. How Older People Who Have Never Used Touchscreen Technology Interact with a Tablet. In Human-Computer Interaction-INTERACT 2017, Mumbai, India, 25-29 September 2017.
- Bevilacqua, R.; Felici, E.; Marcellini, F.; Glende, S.; Klemcke, S.; Conrad, I.; Esposito, R.; Cavallo, F.; Dario, P. Robot-era Project: Preliminary Results on the System Usability. In Design, User Experience, and Usability: Interactive Experience Design, Los Angeles, CA, USA, 2-7 August 2015.
Figure 1.
The CAREUP platform.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



