Submitted:
18 May 2023
Posted:
19 May 2023
You are already at the latest version
Preprints on COVID-19 and SARS-CoV-2
Abstract
Vaccine hesitancy remains a public health challenge. It has been argued that the sources of vaccine-related information may serve as important condiments to one’s decision to be vaccinated. However, little empirical attention is given to the subject. We contribute to this debate by assessing the level of COVID-19 vaccine hesitancy and the role of information explaining hesitancy, using the Nelson Mandela Bay Municipality of South Africa as a case study. Findings confirm high level of vaccine hesitancy, representing 78.8 percent of the respondents (which is above the national level of 41%). Furthermore, findings reveal that vaccination decisions are influenced by family, which is the most trusted among all institutions in the society, especially on sensitive matters and those shrouded by myths and misinformation. Additionally, the majority trusts health care workers and mass media as sources of health-related and general information; however, the use of popular personalities to convey health information is not supported. The findings reveal key socio-demographic and institutional drivers of COVD-9 vaccine hesitancy, such as age, inadequate information on the vaccine, trust issues, conspiracy beliefs, vaccine-related factors, and perceived side effects associated with the vaccine. Recommendations based on the findings are provided.
Keywords:
Information
; Sources of information
; COVID-19
; Vaccine hesitancy
1. Introduction
To vaccinate or not has become a pertinent question related to the COVID-19 pandemic, especially as the world starts to open again [1]. Even though vaccine coverage is steadily increasing globally, hesitancy remains increasingly high in some countries, including South Africa, which has the highest record of cases in Africa. Vaccine hesitancy is defined as a delay in accepting or refusing a vaccine despite the availability of vaccination services [2,3]. Vaccination-hesitant individuals have come to be known as anti-vaxxers or vaccine deniers [4], with mobilization and identification of like-minded individuals aided by social media [5], which is known as the "echo chamber hypothesis. Conspiracies exist on both the virus and the vaccine, arguably due to the sources of or insufficient information that then affects one’s decision to be vaccinated.
Although vaccine hesitancy has existed among a small percentage of the population for centuries [6], its negative effects have become more pronounced than previously during the COVID-19 pandemic [7], and it is regarded as one of the most serious threats to global health (Robinson, Jones, and Daly 2020). COVID-19 is one of the most recent catalysts that has set off an economic shock, and the measures to contain it have undoubtedly affected the social, economic, and risk preferences of individuals and groups. Apprehension is a critical force.
Vaccine apprehension is widespread, misinformed, and contagious, and it is not limited to COVID-19 vaccination. Social media has significantly accelerated global information exchange, resulting in the viral spread of fringe opinions and misinformation [5]. As a result, instead of fighting a pandemic, we are now fighting an infodemic [3]. Vaccine apprehension is a complex and dynamic social process characterized by multiple webs of influence, meaning, and logic. People's vaccination attitudes and practices are typically the results of an ongoing engagement that is contingent on evolving personal, social circumstances and information flow [7]. Individuals' vaccination decisions frequently communicate not only what they think about vaccines but also who they are, what they value, and with whom they identify. It has been argued that the sources of vaccine-related information may serve as important condiments to one’s decision to be vaccinated. However, little empirical attention is given to the subject. We contribute to this debate by assessing the level of COVID-19 vaccine hesitancy and the role information plays in explaining hesitancy, using the Nelson Mandela Bay Municipality of South Africa as a case study. This contributes significantly to literature and shape policy direction and interventions on the management of pandemic and related crisis in the future using information as an effective tool.
2. Methods
This study seeks to assess the level of COVID-19 vaccine hesitancy and the role of information explaining hesitancy, using the Nelson Mandela Bay Municipality of South Africa as a case study. This objective and literature guide the design of the instruments (semi-structured questionnaires) on four thematic areas as follows; (1) socioeconomic characteristics; (2) sources of information and contextual influence; (3) individual and group influence; and (4) questions related to the vaccine or vaccination. Questions on these areas help elicit facts on the major drivers of willingness to be vaccinated, sources of information and the roles of information in vaccination decision. The instrument was pilot tested with few respondents in the study area to identify any weakness and enhance the overall validity.
The target population was all adults in the Nelson Mandela Bay Municipality, and the three major towns of Gqeberha, Kariega, and Despatch were considered. In 2019, the Nelson Mandela Bay Metropolitan Municipality was comprised of 375 000 households, and when using Raosoft's1 sample calculation, a minimum of 400 respondents across Gqeberha, Kariega, and Despatch are considered representative. The survey was designed and administered and interviewed conducted in these three regions of the Bay to ensure representation and to consider other demographics such as population groups, age, and gender. The composition of the households by population group consists of 62.9 percent, which is attributed to the African population group. The colored population group had a total composition of 19.6 percent (ranking second), the white population group had a total composition of 16.2 percent of the total households, and the smallest population group by households is the Asian population group, with only 1.3 percent in 2019.
Given that the three major towns of the municipality were represented and homogenous in each area, a convenience sampling technique was employed, and those who were available and willing to respond to the questionnaire participated. A convenience sample is a type of non-probability sampling method where the sample is taken from a group of people who are easy to contact, reach or available to participate. A total of 460 respondents were selected for this study in the above thematic areas. Since the study is qualitative in nature, descriptive statistics, univariate analysis, graphical presentation and thematic categorisation were used for the analysis.
3. Results
Demographics of the sample
Table 1 documents statistics of respondents in the three major towns of the municipality and their knowledge about the COVID-19 vaccine. Based on the data sample, almost 97 per cent of respondents have heard about the COVID-19 vaccine, while only 3 per cent claim to have no knowledge about the vaccine. Hearing about the vaccine is dependent on how such information is disseminated, and the strategies used to implement the vaccine rollout. The internet and social media platforms have been leveraged in distributing COVID-19 vaccine information nationwide.
All major areas within Nelson Mandela Bay have highlighted that they have heard about the COVI-19 vaccine, with 97.9 percent in Gqeberha, 93.3 percent in Kariega, and 84.6 percent in Despatch. Information about the COVID-19 vaccine has reached significant numbers across all age groups: 96.1 percent of the 18–24 age group; 96.9 percent of the 25–34 age group; 96.7 percent of the 25–54 age group; and all the 55–64 and 65+ age groups.
Other demographic characteristics of the respondent is displayed in Figure 1.
Figure 1 reveals that 28.9% of the research participants were male and 71.1% were female. The bulk of respondents were aged 25–34 (37%), followed by 18–24 (31%), 35–54 (26%), 55–64 (4.6%), and 65+ (1.3%). 45.84 percent of respondents had higher education, 42.52 percent had matriculation, 10.32 percent had elementary education, and 1.3% had no education. 75% of the people in the sample were single, 17% were married, and a few were divorced, widowed, or cohabiting. Most respondents (79%), and a few others, were Christians. Africans made up approximately 87% of the participants, followed by colored, Asian/Indian, and white.
Figure 2 reveals that most responders are from Gqeberha (59.4%), followed by Kariega (17.9%), Despatch, and others. Respondents were from average-income homes. Average income implies the same as most households, less than average means less than most households, and above means above most households. Result shows that 59.2% of families have an average income, 38% have a lower income, and a few have a higher income. About 68.6% of respondents claimed they are as attentive and responsible as others, while 28.4% said they are extra-careful, and very few stated they are not careful.
When asked if they are vaccinated, most of the participants (48.3%) responded that they are not vaccinated but are not planning to get vaccinated, while 30.51 percent said they were not vaccinated but are planning to get vaccinated much later. This shows a high level of vaccine hesitancy (78.8%) among the respondents. Only 19.5 percent reported that they were fully vaccinated, and 1.7 percent reported receiving only one vaccination (Figure 3).
Figure 4 above shows that 93.8 percent of the participants have heard about the COVID-19 vaccine, while only 6.2 percent responded "no,", meaning, they haven’t heard about the vaccine. In one question, where respondents were asked whether the government should make vaccines compulsory, bearing in mind that not all those who disagree are unvaccinated, most of the participants, representing 69.7 percent, were against it, while the participants that were in favor were 10.2 percent, the others who responded preferred not to respond, and those who did not know were 12.0 percent and 8.1 percent, respectively. This means that more people are against vaccine enforcement (compulsory vaccination), a sign of high hesitance toward the vaccine! The variable was recorded for further analysis, including the vaccine hesitance ratio. The beliefs or perceptions around the safety of the vaccine show that 47.4 percent of respondents do not believe that vaccines are safe for them, and 33.9 percent prefer not to respond, while 18.6 percent believe vaccines are safe for them. This shows that there is a greater sense of not trusting the safety of the vaccine among the respondents. The majority of respondents do not believe that vaccine is the best solution for COVID-19; this is shown by 24.2 percent who believe there is another solution than vaccination, while 59.87 percent of the sample who responded are not sure, and only 15.9 percent (less than 1 in every 5) believe that vaccine is the best solution for COVID-19.
Regarding available information on the COVID-19 vaccine, only 18.7 percent believe they have adequate information, while over a third reported not having adequate information (36.8%), 36.7% were not sure, and 7.7 percent preferred not to say. This analysis shows that most people do not have enough information regarding the COVID-19 vaccine, including those who responded that they were not sure, and this could also be the determining factor in vaccine hesitancy. It is imperative to consider the convenience of getting a vaccination. The largest proportion (27%) prefers that vaccination take place at home, followed by 19% who prefer it at the workplace (cumulatively 46%).
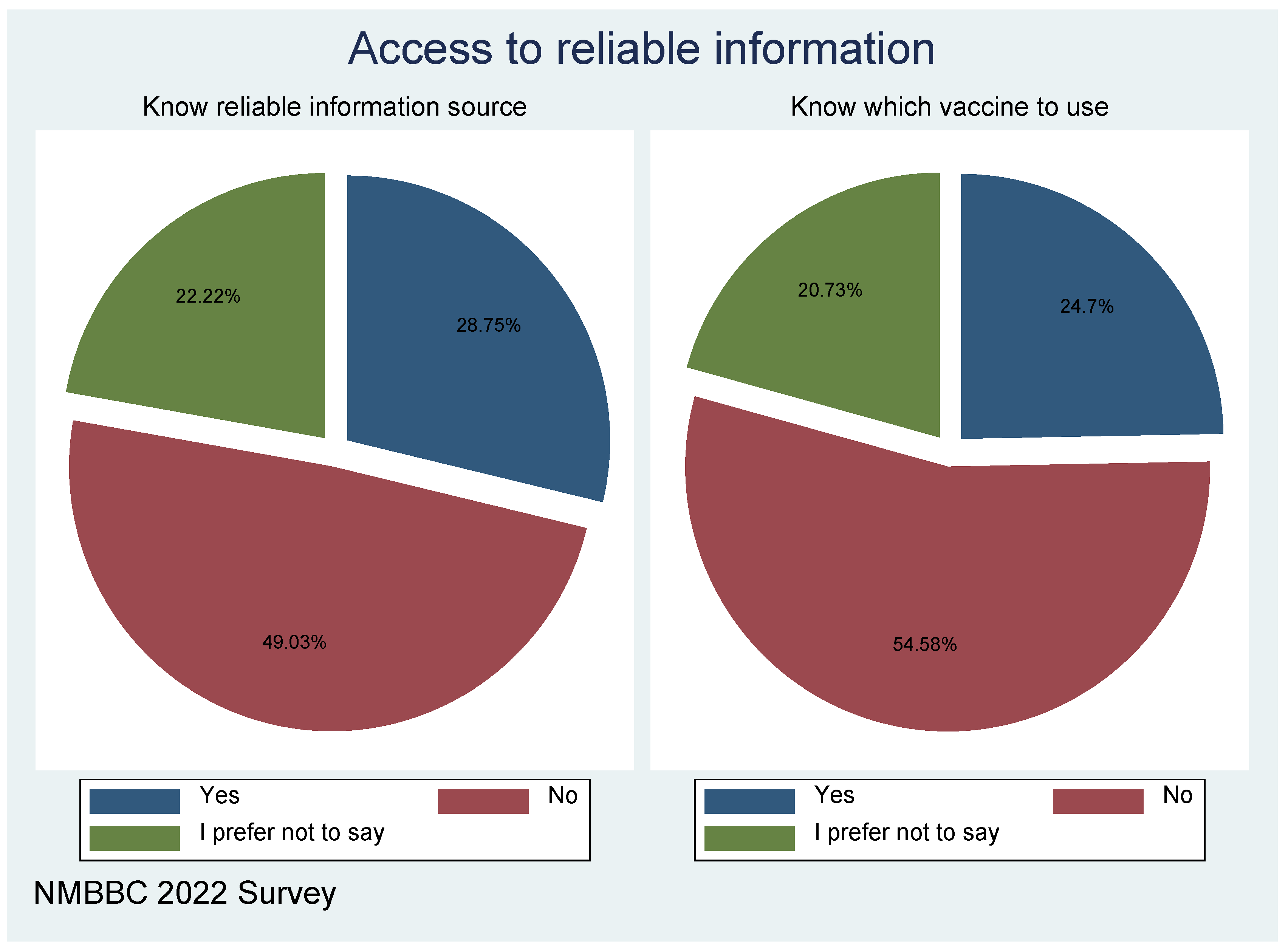
On the other hand, 49 percent reported that they do not know of a reliable source of information; only 28.8 percent are aware of such reliable sources, and 22.2 percent are not sure. The same goes for knowledge on which vaccine one needs to take; the majority, representing 54.6 percent, are not aware, only a quarter reported that they are aware, and a few respondents were not sure. This reflects a lack of adequate information, as reported also above, which creates opportunities for misinformation (to fill the knowledge gaps).
Figure 6.
Knowledge about vaccination and related source of information.
Mass media (e.g., newspapers, TV, and radio) are the most trusted sources of general information, followed by health care workers, the government, and employers. Friends and family follow, and then last is social media. On the other hand, health care workers are most trusted with health information, followed by mass media, the government, employers, family, and friends, and again, social media. It appears that social media is least trusted by most respondents as a source for either general or health information. Social media has been accused of spreading misinformation, but it is sometimes hard to verify the source.
The beliefs or perceptions around the safety of the vaccine show that 44.6 percent of respondents do not believe that vaccines are safe for them, and 21.4 percent prefer not to respond, while 33.9 percent believe vaccines are safe for them (Figure 7). This shows that there is a greater sense of not trusting the safety of the vaccine among the respondents.
Sensitive matters (such as those likely to spike unnecessary public tension, fear, and panic and those related to personal issues) and those shrouded by myths and misinformation require appropriate information management and dissemination, mainly through trusted channels. It is important to get to know trusted sources of information so that they can be utilized to dispel any misinformation.
Figure 8.
Social network and information sharing: to what extent do individuals trust different people and institutions within society. Note: The smaller the percentage (inner circle) the more trusted the individual/institution.
Figure 8.
Social network and information sharing: to what extent do individuals trust different people and institutions within society. Note: The smaller the percentage (inner circle) the more trusted the individual/institution.
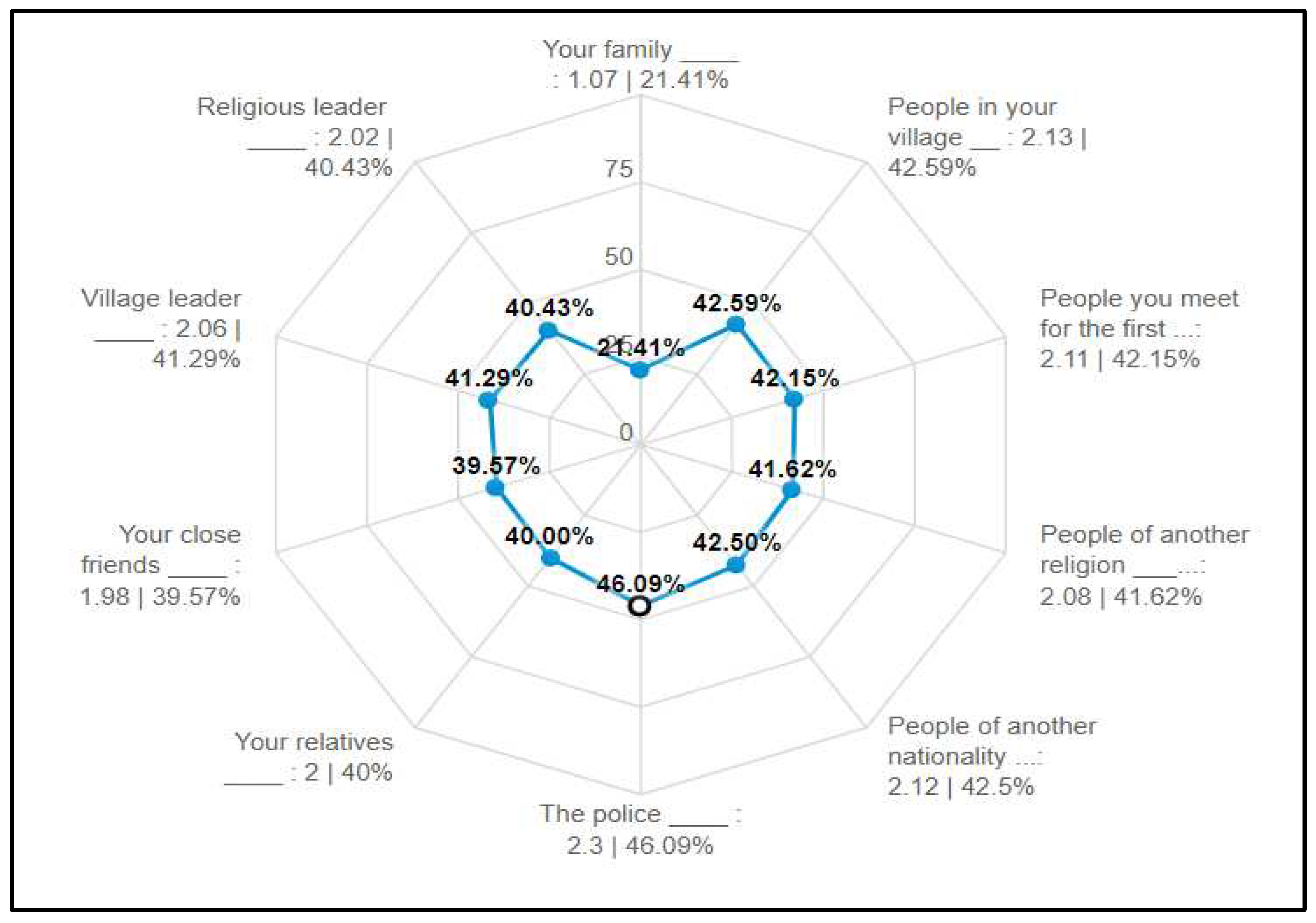
While the family is the most trusted, it has also been revealed that much discouragement for vaccination has come from family members. This implies that any efforts to increase vaccination uptake must take into account family dynamics. It is important to understand the key decision-makers within the family. With reliance on social media for information, it is always the head of the family or elders who are the key decision-makers. The youth may wield so much influence as they can easily source and share information with the rest of their family members, casting aspersions on the official information and authenticity of the vaccine. By the same token, if that generation is convinced that vaccination is the solution, then the outcome will be positive.
The most preferred mode of communication is via Television (19.5%), followed by WhatsApp and Radio both at 17.1 per cent. Mass media was also highlighted as the most trusted source of general information, and the second most trusted for heath related information (Figure 9).
4. Discussions
This section reflects on the results (causes of vaccine hesitancy and the role of information) in the preceding section and relates the findings of this study to previous research and the implications. Concerning vaccine hesitancy, some participants cited that this specific brand of vaccine was not recognized by other countries and therefore would not get vaccinated or wanted to wait for other vaccines, while others refused to receive vaccines due to beliefs about their safety and effectiveness [8]. Another reason for COVID-19 vaccination hesitancy is a lack of trust due to the belief that the vaccine moved too quickly through clinical trials, and there is a widespread belief that vaccination is extremely risky, resulting in serious health consequences [1,9]. Similarly, according to Ref. [10], participants believed that socio-political factors and pressures could lead to a rushed approval of the COVID-19 vaccine without assurances of safety and efficacy. Refs. [11,12] found, in their separate studies, that the psychological factors that affect COVID-19 vaccination hesitancy include trust in the vaccine and fear of side effects. Promoting vaccine intake requires action plan through public education, communication strategies, and tailored messaging. This action plan should be part of a trust-building strategy that focuses on relationships, transparency, justice, and participation.
Influences have been reported to emerge from lack of knowledge, personal perception of the vaccine, or influences of the social or peer environment. Ref. [13] reported that low knowledge about COVID-19 also increases vaccination hesitancy, as confirmed in this study. According to Ref. [14], due to a lack of knowledge and conspiracy theories about the COVID-19 vaccine, most people were concerned about the side effects of vaccines, which led them to refuse or postpone getting vaccinated, while other reasons included conspiracy theories and the occult [9,15,16] the results also show that respondents, due to a lack of knowledge or attitudes, have doubts about the effectiveness of the vaccination, which has led to a perception of the vaccines as being risky. Additionally, studies such as [17] identified vaccine safety, efficacy, and potential side effects, mistrust in healthcare, religious beliefs, and trust in information sources as reasons for COVID-19 vaccination hesitancy. This may have significant impacts on many aspects of life in the short and long term [18,19,20,21,22,23,24].
The study found that the family is the most trusted ‘institution’, with the least trusted being the police. This is trust in general, which, based on literature, is built over many instances through repeated interactions and observations in the communities where people live. The more that institutions and leadership are trusted, the easier it is to manage various issues within a community; that trust serves as social capital that binds the community together. A call to action is easily heeded. Where there is no trust, communities rarely flourish as individuals cannot share resources and cannot take heed of warnings of impending danger (such as floods, fire, and even the pandemic, which is the focus of this study). Concerning the above, Ref. [25] found that conspiracy beliefs negatively predicted general attitudes toward vaccines. According to Ref. [8], individuals' perceptions and attitudes play a significant role in the decision to vaccinate against COVID-19 or not. Individual barriers to vaccination include a lack of knowledge, perceptions, attitudes, and beliefs about science, vaccines, the health system, and the government. According to Amit et al. (2021), these perceptions are shaped by (mis)information exposure amplified by social media, the community, and the health system. Depending on how one feels about vaccines, one’s social network may have a positive or negative impact on vaccination uptake. As a result, interpersonal barriers, such as networks and social capital, influence health beliefs and decisions. Other studies have found that negative interactions with the healthcare system may lead to vaccine hesitancy [16,26]. Effort such as involving various community stakeholders in tailored communication through trusted family members and other strategies that can increase literacy and install trust in government.
5. Conclusion and recommendations
The study has confirmed that COVID-19 vaccine hesitancy remains high (representing 78.8 percent of the respondents which is above the national level of 41%) within Nelson Mandela Bay. Furthermore, findings reveal that vaccination decisions are influenced by family, which is the most trusted among all institutions in the society, especially on sensitive matters and those shrouded by myths and misinformation. Additionally, the majority trusts health care workers and mass media as sources of health-related and general information; however, the use of popular personalities to convey health information is not supported. The findings reveal key socio-demographic and institutional drivers of COVD-9 vaccine hesitancy, such as age, inadequate information on the vaccine, trust issues, conspiracy beliefs, vaccine-related factors, and perceived side effects associated with the vaccine.
It is pivotal to outline an action plan to build vaccine confidence and uptake. The first action plan is to promote uptake through public education, communication strategies, and tailored messaging. This action plan should be part of a trust-building strategy that focuses on relationships, transparency, justice, and participation. The action plan will mostly focus on dealing with the following factors that have been identified as drivers of vaccine hesitancy: lack of adequate information, lack of satisfaction with information provided by healthcare workers, non-tertiary population groups that find it difficult to get the right information, and lack of knowledge regarding which vaccine to take. Furthermore, engaging both online and offline platforms for clear communication about the types of vaccines and the process of deploying them
Other factors can be addressed by involving various community stakeholders in tailored communication through trusted family members and other strategies that can increase literacy, reach low-income households, and install trust in government. Another key action plan is creative communication and honest dialogue to mitigate misinformation or false information around vaccines. Innovative communication to capture youth groups that are also identified as hesitant about the vaccine would be through compelling communications methods, particularly storytelling (e.g., personal stories to which people can relate), emotion, appeals to empathy and altruism, and memes to convey essential information in engaging ways, which can flood social media in an effort to counteract misleading information.
Use all languages spoken and visual imagery from the platforms people trust, and build on local terminologies and understandings of vitality, strength, and immunity in communications about vaccination. Working together with a trusted family member, community leaders, and beyond public health online ‘influencers" to locally trusted alternative health providers and community leaders to convey information and facilitate dialogue in compelling ways. Promoting vaccine uptake and addressing vaccine hesitancy among culturally defined population groups through partnering with local religious leaders, making vaccines readily available ad accessible can also turn the tide in favor of vaccine uptake among more special religious groups.
6. Limitations
There are few limitations to this study. First, the analysis in this paper is based on the information and experience voluntarily provided by the respondents; as a result, it's possible that respondents understate or overstate the reality. Secondly, since the study used non- probability sampling technique to select the respondents for these studies, findings is not intendent for generalization to all studies. However, the large sample size used for the analysis and thematic synthesis of result respectively reflect the population and accurate.
Author Contributions
All authors contribute to the various sections of the research.
Funding
This project was funded by the German Federal Ministry for Economic Cooperation and Development (BMZ)‘s COVID-19 fund. Through a financial allocation to GIZ’s Natural Resources Stewardship Programme (NatuReS), a special project was designed together with the Nelson Mandela Bay Business Chamber (NMBBC) as a response to address the spread of the virus and its adverse impacts on economic and social development in the Nelson Mandela Bay area.
Acknowledgement
This paper would not have been possible without the support of the following institutions: the German Federal Ministry for Economic Cooperation and Development, GIZ, NatuReS, Nelson Mandela Bay Business Chamber, and Nelson Mandela University. Special acknowledgement goes to the following individuals for their invaluable contributions: Mr. Prince Matonsi, Mr. Renzo Driussi, Mr. Siyabonga Mchunu, and Ms. Khanyisa Nomda.
Conflicts of Interest
The project received ethical clearance from Nelson Mandela University, reference number H22-BES-ECO-031. The views contained herein do not necessarily represent the views of the funder, its funding partners, or Nelson Mandela University.
References
- G. Anakpo and S. Mishi, “Hesitancy of COVID-19 vaccines: Rapid systematic review of the measurement, predictors, and preventive strategies,” Human Vaccines & Immunotherapeutics, 18(5), p. 2074716, 2022. [CrossRef]
- S. Cooper, H. van Rooyen and C. S. Wiysonge, “COVID-19 vaccine hesitancy in South Africa: how can we maximize uptake of COVID-19 vaccines?,” Expert review of vaccines, vol. 20, no. 8, pp. 921-933., 2021. [CrossRef]
- W. World Health Organization, “Behavioural considerations for acceptance and uptake of COVID-19 vaccines: WHO Technical Advisory Group on Behavioural Insights and Sciences for Health, Meeting Report, 15 October 2020. 2020.,” 2020.
- S. L. Benoit and R. F. Mauldin, “The “anti-vax” movement: a quantitative report on vaccine beliefs and knowledge across social media,” BMC public health, vol. 2, no. 1, pp. 1-11, 2021. [CrossRef]
- K. Hayawi, S. Shahriar, M. A. Serhani, H. Alashwal and M. M. Masud, “Vaccine versus variants (3Vs): are the COVID-19 vaccines effective against the variants? A systematic review.,” Vaccines, vol. 9, no. 11, p. 1305, 2021. [CrossRef]
- F. Pandolfi, L. Franza, L. Todi, V. Carusi, M. Centrone, A. Buonomo, .. and E. Nucera, “The importance of complying with vaccination protocols in developed countries:“Anti-Vax” hysteria and the spread of severe preventable diseases. Current Me,” 2018.
- S. Mylan and C. Hardman, “COVID-19, cults, and the anti-vax movement,” The Lancet, vol. 397, no. 10280, p. 1181, 2021. [CrossRef]
- A. M. L. Amit, V. C. F. Pepito, L. Sumpaico-Tanchanco and M. M. Dayrit, “COVID-19 vaccine brand hesitancy and other challenges to vaccination in the Philippines,” PLOS Global Public Health, vol. 2, no. 1, p. e0000165., 2022. [CrossRef]
- B. Roberts, N. Bohler-Muller and J. Struwig, “South African Social Attitudes Survey (SASAS) (Round 17) Brief report. Summary findings: Attitudes towards vaccination.,” 2021.
- J. Khubchandani, S. Sharma, J. H. Price, M. J. Wiblishauser, M. Sharma and F. J. Webb, “COVID-19 Vaccination Hesitancy in the United States: A Rapid National Assessment,” Journal of Community Health, vol. 46, no. 2, p. 270–277, 2021. [CrossRef]
- A. Campo-Arias and J. C. Pedrozo-Pupo, “Attitude towards COVID-19 vaccines in Colombian university students: Frequency and associated variables,” Acta Bio Medica: Atenei Parmensis, vol. 92, no. 6, 2022.
- S. Neumann-Böhme, N. E. Varghese, I. Sabat, P. P. Barros, W. Brouwer, J. van Exel, ... and T. Stargardt, “Once we have it, will we use it? A European survey on willingness to be vaccinated against COVID-19,” The European Journal of Health Economics, vol. 21, pp. 977-982, 2020. [CrossRef]
- E. Paul, A. Steptoe and D. Fancourt, “Attitudes towards vaccines and intention to vaccinate against COVID-19: Implications for public health communications,” The Lancet Regional Health-Europe, vol. 100012, p. 1, 2021. [CrossRef]
- C. Runciman, K. Alexander and M. Bekker, “SA survey sheds some light on what lies behind coronavirus vaccine hesitancy. Daily Maverick [Internet].,” 2021.
- J. Khubchandani, S. Sharma, J. H. Price, M. J. Wiblishauser, M. Sharma and F. J. Webb, “COVID-19 vaccination hesitancy in the United States: a rapid national assessment,” Journal of community health, vol. 46, pp. 270-277, 2021. [CrossRef]
- P. D. Katoto, S. Parker, N. Coulson, N. Pillay, S. Cooper, A. Jaca, ... and C. S. Wiysonge, “Predictors of COVID-19 vaccine hesitancy in South African local communities: The VaxScenes Study.,” Vaccines, vol. 10, no. 3, p. 353, 2022. [CrossRef]
- M. R. Biswas, M. S. Alzubaidi, U. Shah, A. A. Abd-Alrazaq and Z. Shah, “A scoping review to find out worldwide COVID-19 vaccine hesitancy and its underlying determinants,” Vaccines, vol. 9, no. 11, p. 1243, 2022. [CrossRef]
- G. Anakpo and S. Mishi, “Business response to COVID-19 impact: Effectiveness analysis in South Africa,” The Southern African Journal of Entrepreneurship and Small Business Management, vol. 13, no. 1, p. 7, 2021. [CrossRef]
- K. Jafta, G. Anakpo and M. Syden, “Income and poverty implications of Covid-19 pandemic and coping strategies: the case of South Africa,” Africagrowth Agenda., vol. 19, no. 3, pp. 4-7, 2022.
- G. Anakpo, Z. Nqwayibana and S. Mishi, “The Impact of Work-from-Home on Employee Performance and Productivity: A Systematic Review,” Sustainability, vol. 15, no. 5, p. 4529, 2023. [CrossRef]
- G. Anakpo, F. Hlungwane and S. Mishi, “The Impact of COVID-19 And Related Policy Measures on The Livelihood Strategies in Rural South Africa,” Africagrowth Agenda, 2023.
- E. Komanisi, G. Anakpo and M. Syden, “Vulnerability to COVID-19 impacts in South Africa: analysis of the socio-economic characteristics.,” Africagrowth Agenda, , vol. 19, no. 2, pp. 10-12, 2022.
- H. Gqoboka, G. Anakpo and S. Mishi, “Challenges Facing ICT Use during COVID-19 Pandemic: The Case of Small, Medium and Micro Enterprises in South Africa,” American Journal of Industrial and Business Management, vol. 12, no. 9, pp. 1395-1401, 2022. [CrossRef]
- S. Mish, N. Tshabalala, G. Anakpo and M. Weliswa, “COVID-19 experiences and Coping strategies: The case of dif-ferently sized businesses in South Africa,” Sustainability, 2023. [CrossRef]
- M. Pivetti, S. Di Battista, F. G. Paleari and E. Hakoköngäs, “Conspiracy beliefs and attitudes toward COVID-19 vaccinations: A conceptual replication study in Finland,” Journal of Pacific Rim Psychology, 15, 18344909211039893, 2021. [CrossRef]
- R. R. Marzo, W. Sami, M. Z. Alam, S. Acharya, K. Jermsittiparsert, K. Songwathana, ... and S. Yi, “Hesitancy in COVID-19 vaccine uptake and its associated factors among the general adult population: a cross-sectional study in six Southeast Asia,” Tropical medicine and health, vol. 50, pp. 1-10, 2022. [CrossRef]
Figure 1.
Socio-demographic characteristics of study participants/ Sample characteristics and vaccine hesitancy.
Figure 1.
Socio-demographic characteristics of study participants/ Sample characteristics and vaccine hesitancy.
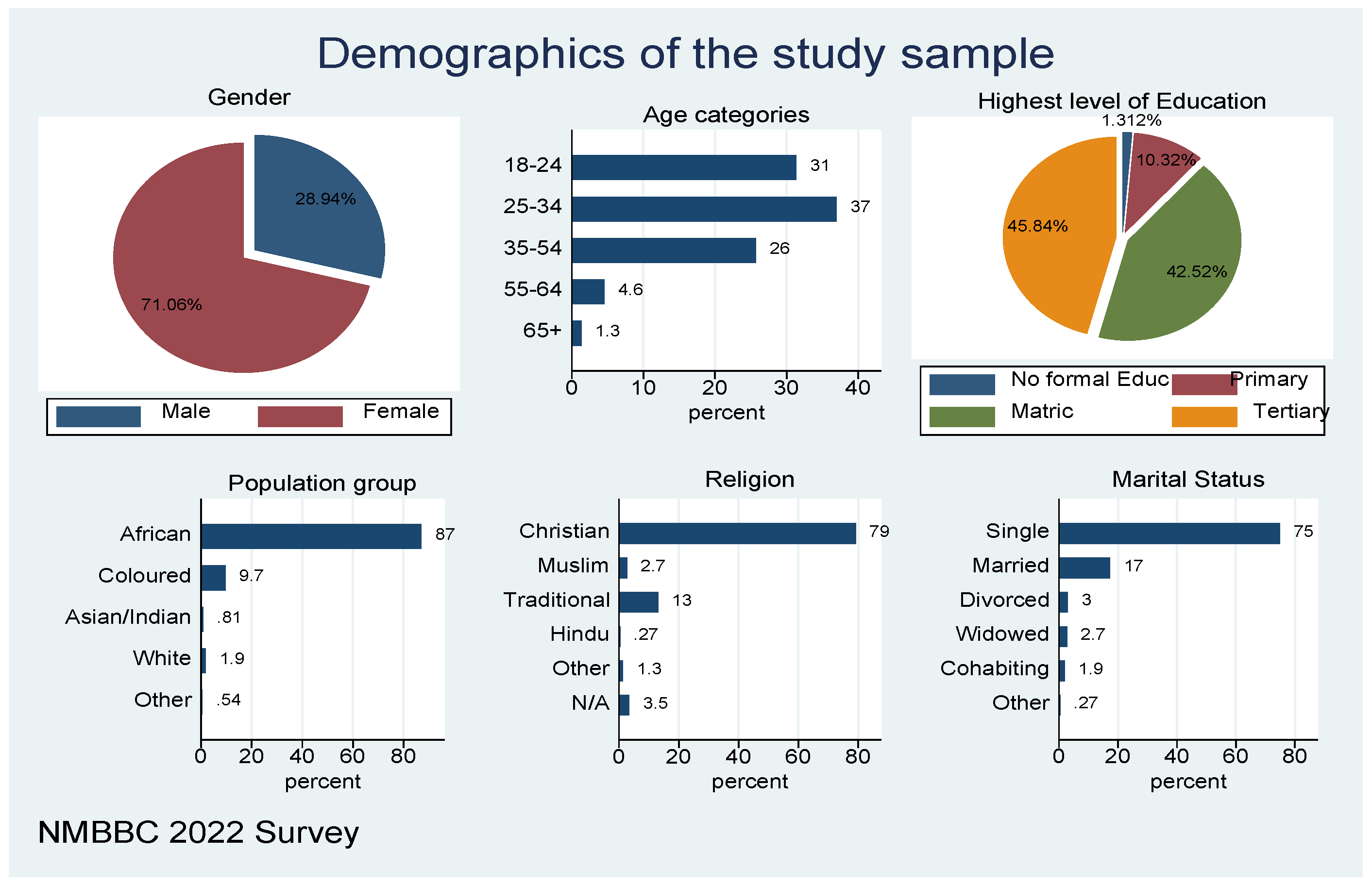
Figure 2.
Demographics and subjective wellbeing of the sample.
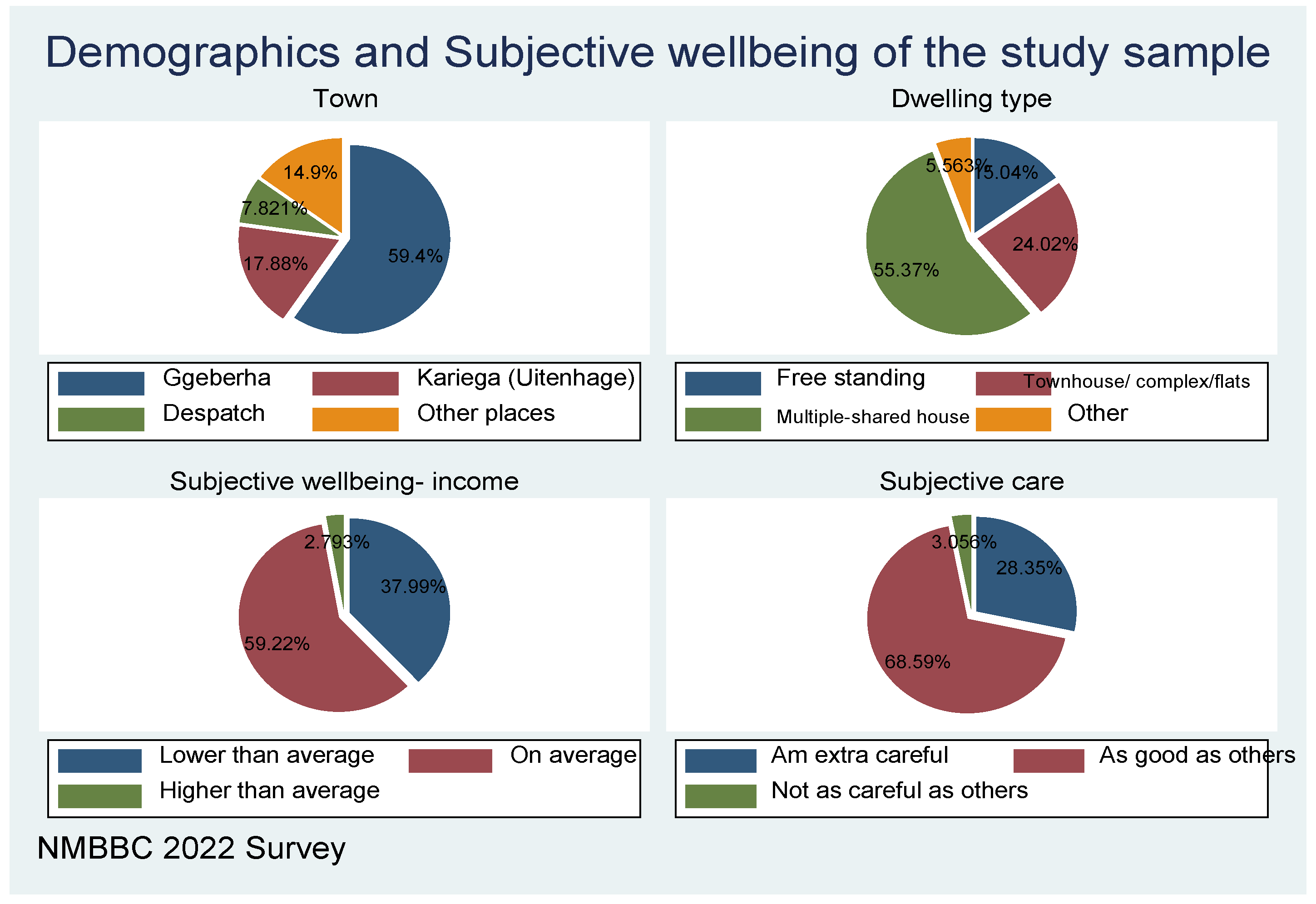
Figure 3.
COVID-19 vaccine and vaccine Hesitancy (Have you been vaccinated?).
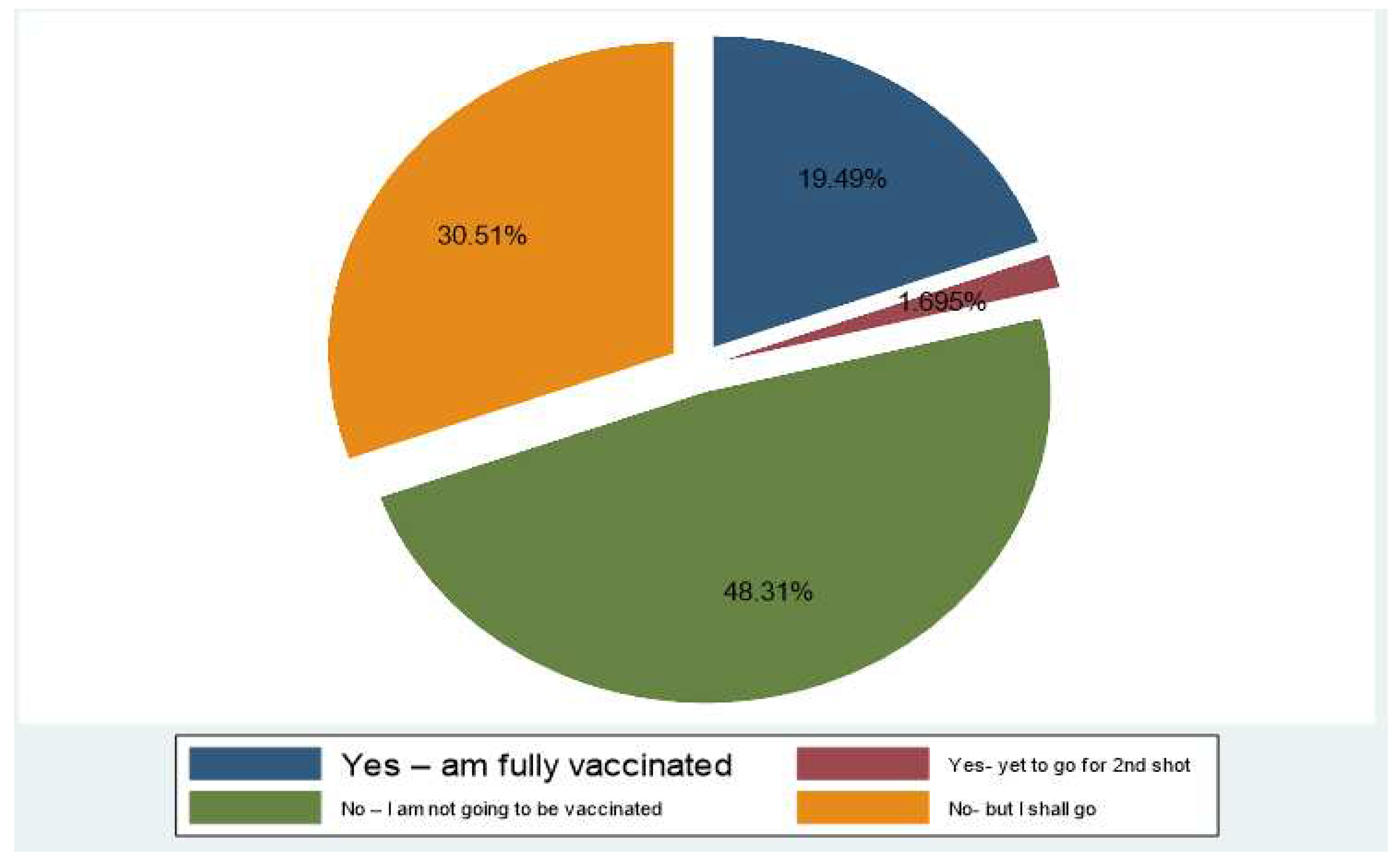
Figure 4.
Knowledge and information about COVID19 vaccine.
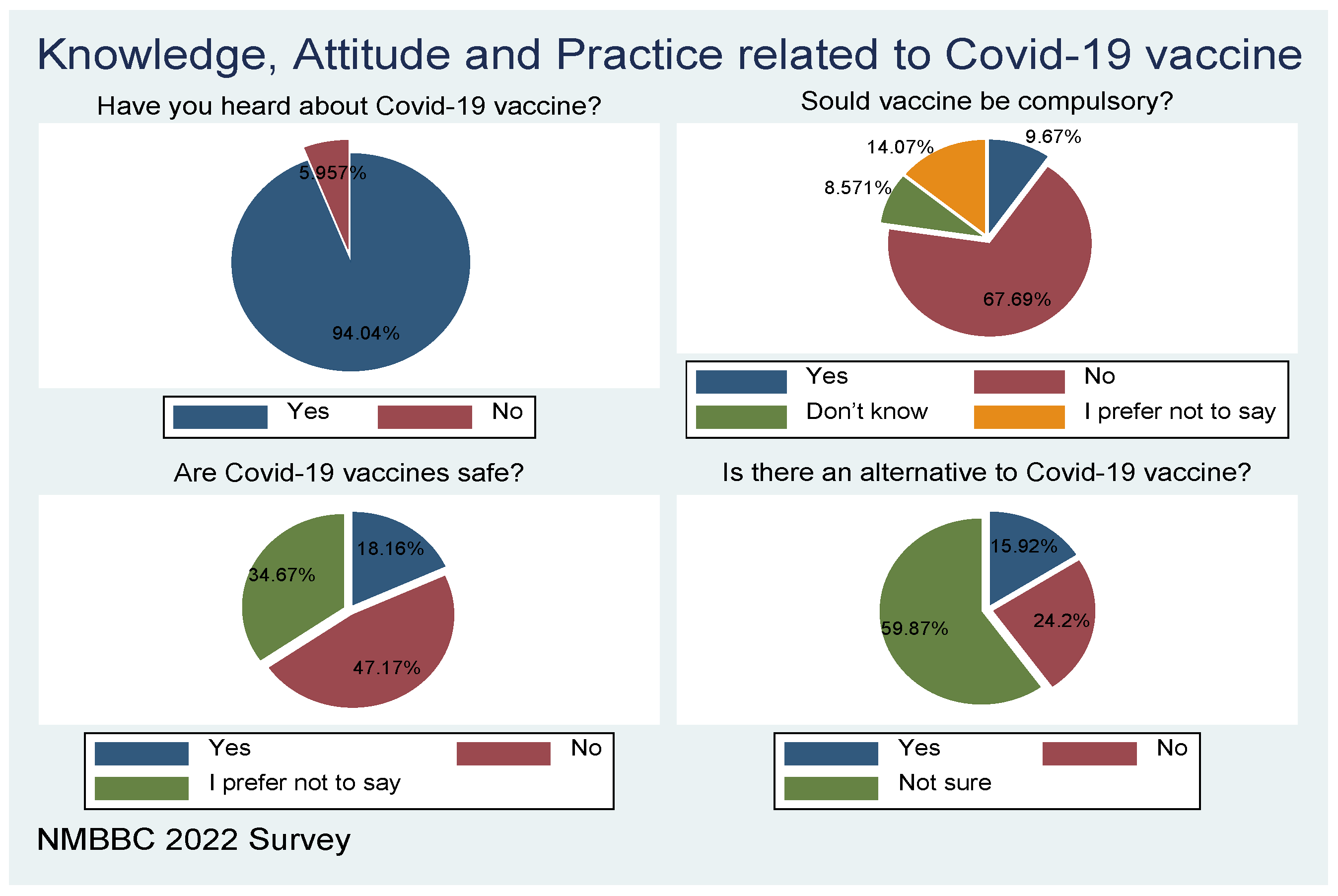
Figure 5.
Information adequacy and convenient place for vaccination uptake.
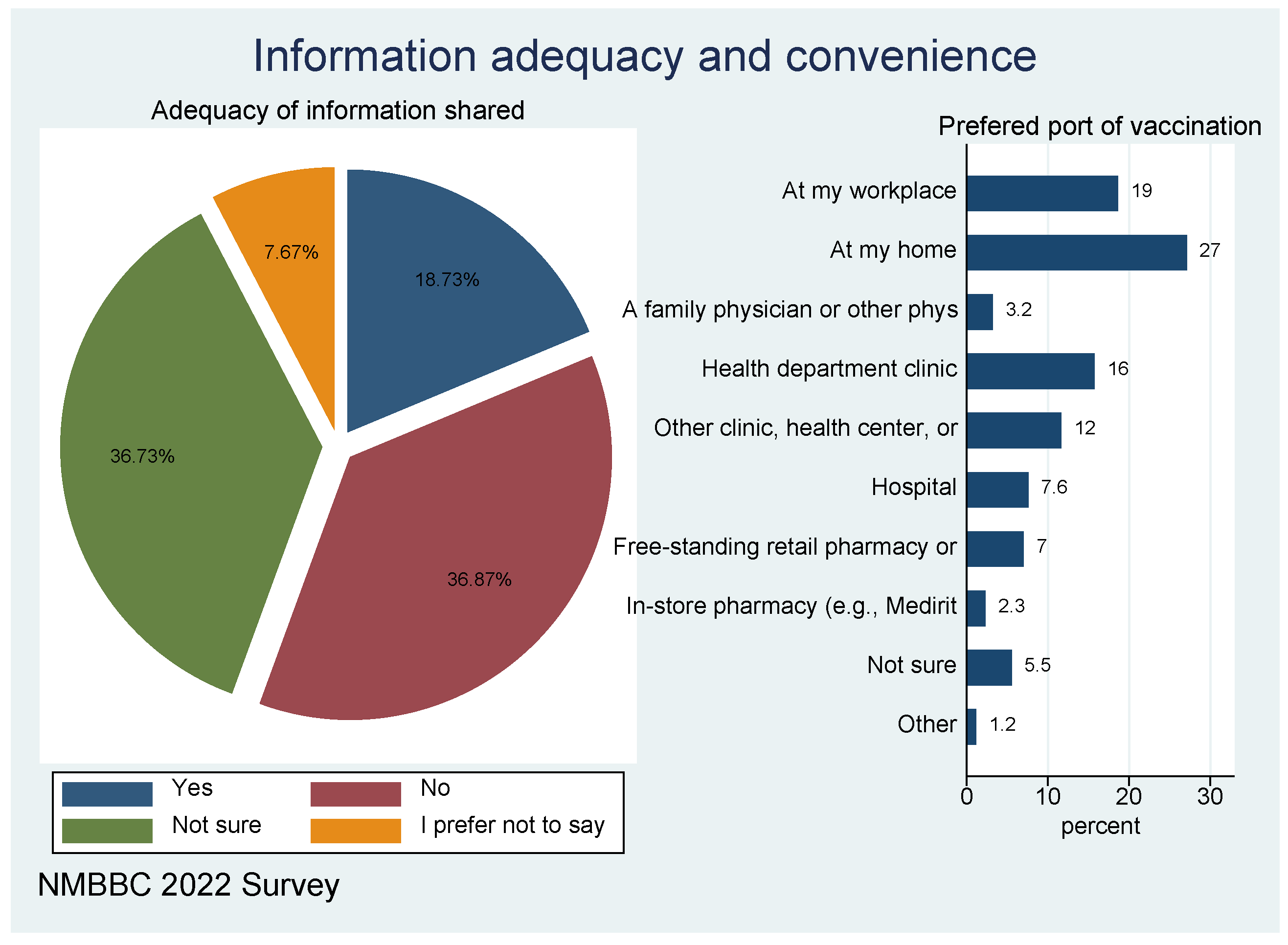
Figure 7.
Level of trust of various information sources- Health versus General (Gen) information.
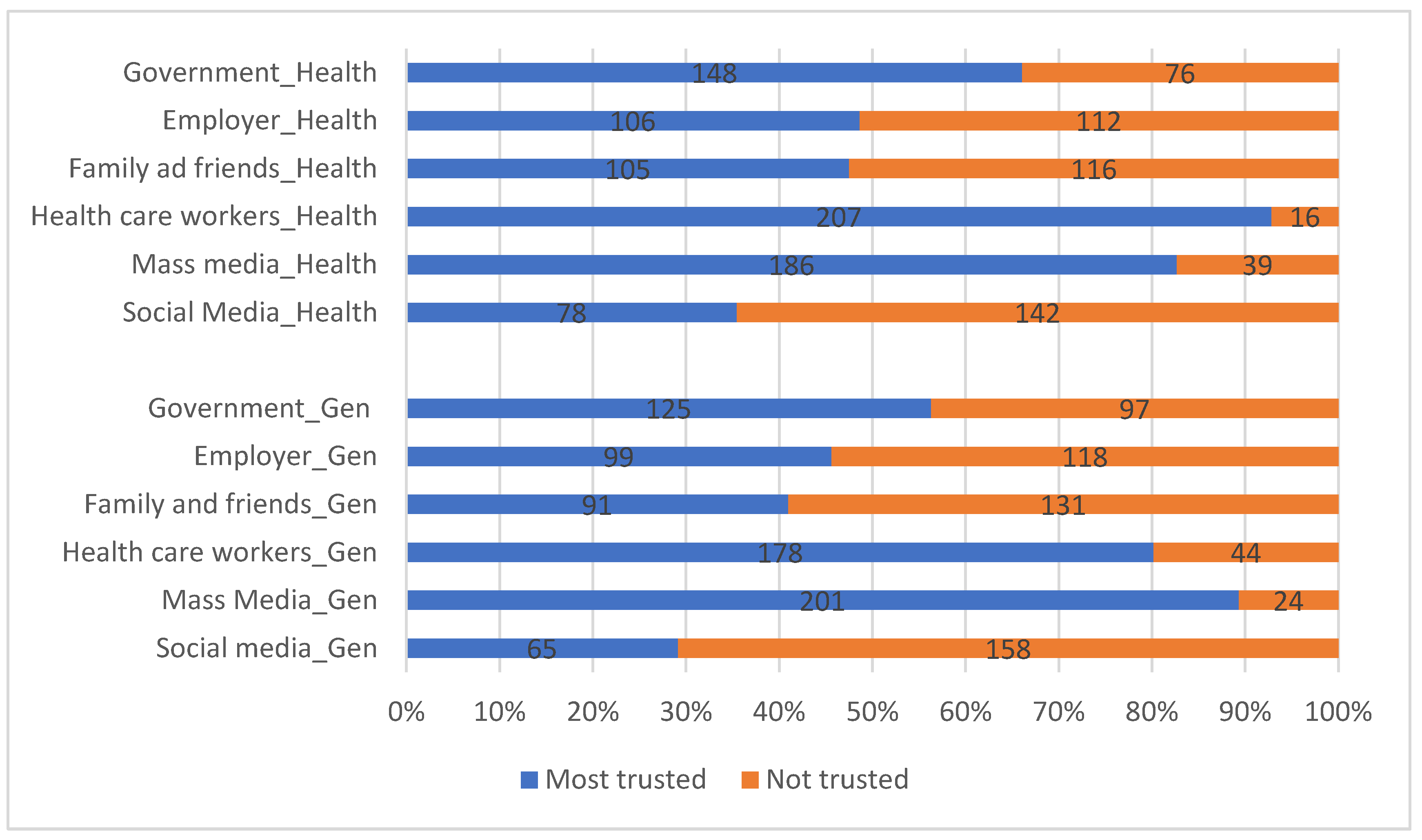
Figure 9.
Preferred source of information/ mode of communication.
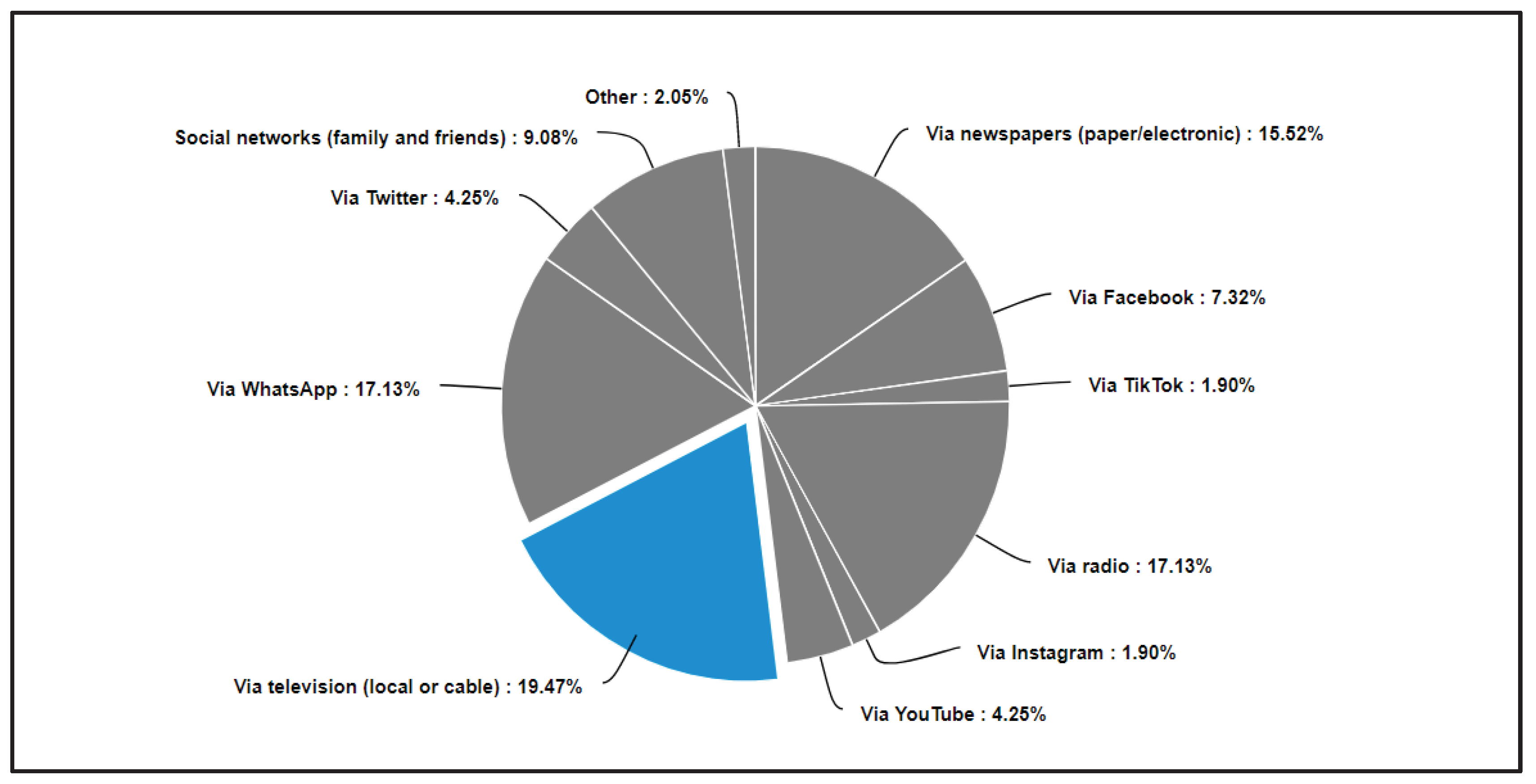

Table 1.
Number of people that have heard about the vaccine as per location.
| Have you heard about the COVID-19 vaccine | From which of the following towns do you reside? | |||
|---|---|---|---|---|
| Ggeberha | Kariega (Uitenhage) | Despatch | Total | |
| Yes | 277 | 42 | 11 | 330 |
| 84.0 | 12.7 | 3.3 | 100.0 | |
| 97.9 | 93.3 | 84.6 | 96.8 | |
| No | 6 | 3 | 2 | 11 |
| 54.6 | 27.2 | 18.2 | 100.0 | |
| 2.1 | 6.7 | 15.4 | 3.2 | |
| Total | 283 | 45 | 13 | 341 |
| 83 | 13.2 | 3.8 | 100.0 | |
| 100.0 | 100.0 | 100.0 | 100.0 | |
First row has frequencies; second row has row percentages, and third row has column percentages.
| 1 | Raosoft is a software company that primarily calculates or generates the sample size of a research or survey (Raosoft Inc., 2004).
|
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



