
Submitted:
18 May 2023
Posted:
19 May 2023
You are already at the latest version
Abstract
It is believed that fetal hemoglobin (HbF) expression in adults is largely genetically regulated. The increased expression of HbF in pregnancy has been reported in a small number of articles. Different mechanisms have been proposed, but the description of HbF expression during pregnancy remains unclear. The objectives of this study were to document HbF expression during peri and postpartum periods, confirm its maternal origin, and assess clinical and biochemical parameters potentially associated with HbF modulation. In this observational prospective study, 345 pregnant women were followed. At baseline, 169 had HbF expression (≥1% of total hemoglobin) and 176 did not have HbF expression. Women were followed at the obstetric clinic during their pregnancy. Clinical and biochemical parameters were measured at each visit. Analyses were made to determine which parameters had a significant correlation to HbF expression. Results show that HbF expression of ≥ 1% during peri and postpartum periods in pregnant women without influencing comorbidities is at its highest peak during the first trimester. In all women, it was proven that HbF was of maternal origin. A significant positive correlation between HbF expression, β-HCG, and HbA1C was present. A significant negative association between HbF expression and total hemoglobin was found. HbF expression induction during pregnancy is probably associated with increase in β-HCG and HbA1C, and decrease of total hemoglobin, which could temporarily reactivate the fetal erythropoietic system.
Keywords:
Fetal hemoglobin
; pregnancy
; glycosylated hemoglobin
; HbA1C
; β-HCG
1. Introduction
In human adults, fetal hemoglobin (HbF) normally represents approximately 1% of total hemoglobin. The switch from fetal hemoglobin forms (α2 Gγ2 and α2 Aγ2) to adult HbA and minor HbA2 forms happens in utero in the last weeks of pregnancy. The precise mechanism of this switch is still misunderstood. One proposed mechanism relates to a change in the gene expression of a single population of stem cells [1]. Another implies silencing of the γ-globin gene in reticulocytes. Orneal and al suggested that the gradual decrease of the γ-globin gene during the fetal period seems to be independent of this silencing [2]. However, there is a temporal relationship between birth and the silencing of the γ-globin gene. Indeed, there is an abrupt postnatal increase in the amount of gene-silenced γ-globin reticulocytes which is presumed to be triggered by an event related to birth, possibly normoxic respiration.
The percentage of HbF in adults can be higher in some hematologic pathologies, such as β-thalassemia, sickle cell disease, and aplastic anemia [3]. In these conditions, the persistence of fetal hemoglobin production in adult erythrocytes (F-cells) can have protective properties. It is believed that the HbF and F-cells percentage in adults is substantially genetically regulated [1]. However, HbF synthesis regulation mechanisms in adults remain misunderstood despite the underlying therapeutic potential for hemoglobinopathies. Pregnancy is the only known non-pathological condition in which HbF level can transiently increase in adults, either by feoto-maternal transfusion or by physiologic expression. It has been observed that this increase during pregnancy happens both in normal pregnancies and pregnancies of women with hemoglobinopathies [4,5]. The maternal origin of the HbF at the beginning of pregnancy has been reported in many studies. Several hypotheses have been put forward to explain this expression. Among those, pregnancy expression of HbF has been linked to an increase in variable hormones (human chorionic gonadotropin, medroxyprogesterone acetate, and prolactin), erythropoiesis and expansion of maternal erythrocytes mass, and stress-induced temporary reactivation of fetal erythropoietic system [5,6,7,8,9]. However, some of these observations have been denied by others [10,11]. The number of articles and the associated sample sizes that have reported this phenomenon are quite small. Therefore, the description of HbF expression during pregnancy remains unclear. These premises motivated this study, which was conducted in women followed during pregnancy in order to describe and analyze their level of HbF hemoglobin. The objectives of this study were the following: to document HbF expression during peri and postpartum periods, to confirm its maternal origin, and to assess clinical and biochemical parameters potentially associated with HbF modulation.
2. Materials and Methods
2.1. Parturients selection
This study is an observational single-institution prospective study. Inclusion criteria are defined as followed: to be a woman of 18 years old or more, to be pregnant in the first trimester of pregnancy (as shown by a fetal heartbeat on ultrasound or a positive urine dipstick β-HCG test), and to be followed at the obstetric clinic of Hôpital St-Luc of the CHUM (Centre hospitalier de l’Université de Montréal). Exclusion criteria are defined as the presence of an abnormal form of hemoglobin (HbC, HbS, HbH or β-thalassemia minor, major or intermedia) as determined by high-performance liquid chromatography (HPLC), patients with type 1 diabetes, patients with myeloproliferative or myelodysplastic syndromes, use of immune suppressors (tacrolimus, azathioprine, cyclosporine or mercaptopurine), creatinine > 140 μmol/L and hepatic disease. 879 pregnant women were screened to participate from March 2014 to January 2016. The sampling continued until approximately 150 HbF positive women were listed. Approximately 150 of the first HbF negative parturients during the sampling were followed during the whole pregnancy in order to have a sufficient comparator sample size. Overall, at the first visit, a total of 169 women had HbF expression and 176 women did not have HbF expression. Negative total HbF expression was defined as a <1% HbF level of total hemoglobin and positive total HbF expression was defined as ≥1% HbF level of total hemoglobin.
2.2. Study procedures
Women were followed during four visits at the obstetric clinic. The three first visits were at each trimester (8-12, 24-28, and 36th gestational weeks) and HbF positive women had an additional 6 weeks post-partum visit to assess for hereditary persistence of HbF (HPFH). Consent and information forms were presented and signed by the parturients at the first visit. Clinical characteristics were identified at the first and consecutive visits: age, weight (kg), date of latest menstruation, smoking history, primiparous or multiparous status, presence of multiple pregnancy, hypertension history, and history of a fertility clinic consultation. The level of creatinine was only measured at the first visit. At each following visit, the following data were also noted: gestational week, presence or absence of active hypertension, diabetes, eclampsia or preeclampsia, and use of progesterone. The baby’s weight (kg) was also measured. Gestational age was determined by the date of the latest menstruation and first-trimester fetal ultrasound. Hypertension was defined as a systolic pressure > 140 mm Hg or a diastolic pressure > 90 mm Hg. Preeclampsia was defined as the presence of hypertension with proteinuria of > 0.3 g in a 24-hour urine collection after 20 weeks of gestation. Eclampsia was defined as generalized seizures or coma in a pregnant woman with diagnosed preeclampsia, in the absence of another cause. Type II diabetes was diagnosed if women had a fasting blood glucose > 7 mmol/L or blood glucose > 11 mmol/L after a 2-hour glucose challenge test. Gestational diabetes was diagnosed if parturients had at least two of the following criteria: a fasting blood glucose of > 5.3 mmol/L, blood glucose of > 10 mmol/L 1 hour after a glucose challenge test, blood glucose of > 8.6 mmol/L 2 hours after a glucose challenge test or blood glucose of > 7.8 mmol/L 3 hours after a glucose challenge test. Using specialized questionnaires created for the study, an obstetric nurse at the follow-up clinic collected the data.
Laboratory evaluations and measurement of hemoglobin components
The following laboratory results were measured at each visit: hemoglobin, hematocrit (Ht), red blood cells level (RBC), red cell distribution width (RDW), mean corpuscular volume (MCV), mean corpuscular hemoglobin concentration (MCHC), mean corpuscular hemoglobin (MCH), reticulocyte count, ferritin, β-HCG level, erythropoietin level (EPO) and glycosylated hemoglobin (HbA1C). At each visit, blood samples were analyzed by high-performance liquid chromatography (HPLC) to detect HbF, HbA, HbA2, and to quantify HbA1C. The percentage of HbF was measured and defined by negative (<1%) or positive (≥1%) at every visit. The samples that were HbF positive were analyzed by flux cytometry to determine the origin of the HbF (fetal versus maternal) and to quantify the percentage of erythrocytes containing HbF (F-cells). For HPLC, we used the automated analyzer Bio-Rad Variant II, with the double program HbA2/HbA1C. During the procedure, the time of retention of the hemoglobins as well as the total area of the hemoglobin curves, with target values between 1 and 3.5 million, were monitored. The device pressure was maintained between 35-40 kg/cm and the temperature at 28 °C. The cartridges were calibrated every 250 injections and replaced after every 500 injections. Regarding flux cytometry, we used intracellular labeling with anti-HbF monoclonal antibody (MHFH05, Caltage Laboratories). Initially, 2.5 x 107 peripheral blood cells were fixed with 1 ml of 15% glutaraldehyde solution for 10 minutes at room air temperature. This preparation was cleaned thrice with a Phosphate Buffered Saline solution with Bovin Serum Albumin (PBS-BSA) 1%. It was then suspended in 0.5 ml of Triton X-100 solution and incubated 3-5 minutes at room temperature. The sample was cleaned once again and suspended in 0.5 ml of PBS-BSA 1%. After, 10 μL of this suspension were added to 5 μL of antibody and 10 μL of PBS-BSA 0.1%. The marked red blood cells were stored in 0.5 ml of 1% formaldehyde, then stored in the dark before being analyzed by the cytometer.
2.3. Statistics
Descriptive statistics were used to present the characteristics of HbF positive and negative women. The comparisons were made at first, second, and third visits, and at any time, assessing the proportions of positive and negative cases. Means were calculated on all demographic values and blood parameters. Multiple analyses of covariance (ANCOVA) were performed between each of the following parameters and demographic and medical data: HbF %, F-cells %, HbA1C, total hemoglobin, EPO and β-hCG levels. Both HbF positive and negative groups were included in those analyzes. For the HbF positive group, Pearson correlations were made to predict the HbF %, based on F-cells %, HbA1C %, EPO and β-hCG level, total hemoglobin, and multiple blood parameters (reticulocytes, Ht, RBC, MCHC, MCH, RDW, MCV, and ferritin). The bilateral p-value significance was set between 0.01 and 0.05, depending on the correlation studied. Student t-tests were performed on significant correlations to determine if a significant difference was present between the pregnancy periods (at each of the four visits). Additional t-tests were performed on parameters strongly correlated with the expression of HbF, to compare the mean level of the parameter in the HbF positive and HbF negative groups. Among the Pearson correlations with significant results, multivariate analyses were made using linear regressions.
3. Results
3.1. Descriptive statistics
Among all pregnant women screened (n=879), 22.07% (n = 194) had positive HbF expression. Among those HbF positive women, 18 were non-eligible. Thus, among screened women, 20.02% (n = 176) filled the inclusion criteria. The total number of women included in the comparative study was 345: 51.01% (n=176) were HbF positive women and 48.99% (n=169) were HbF negative initially. Including the women who became HbF positive at the second follow-up visit among the women who were initially HbF negative, 22.53% (n=198) of 879 screened women were HbF positive. Analyzed at the time of the second visit, of the 345 women included, 57.39% were HbF positive. Therefore, 13.02% of the 169 initially HbF negative women became HbF positive at the second visit. At the time of analysis, 155 HbF positive and 147 HbF negative women had completed follow-up for a total of 302 women (Table 1).
The median HbF percentage of HbF positive women was 1.2% at the first visit, 1.0% at the second visit, 0.8% at the third visit, and 0.7% at the fourth visit. For all visits, the median HbF % of positive women was 1.0% (Table 2). Among the 176 originally HbF positive women, 155 completed the fourth visit follow up. At this visit, 113 out of 155 HbF positive women (72.9%) showed a post-partum decrease of HbF < 1%. The means of demographic values and blood parameters are presented in Table 3 and Table 4.
3.2. F-cells percentage
F-cells analyses confirmed the maternal origin of HbF in all cases. At the first visit, the mean F-cells percentage in HbF positive women was 13.89%. Other means were 13.48% at the second visit, 12.22% at the third visit, and 11.48% at the fourth visit. For all visits, the mean F-cells percentage was 13.3% (standard deviation=5.38%) when total HbF was ≥ 1% during pregnancy (Table 5).
3.3. Pearson Correlations and t-tests
Many independent t-tests and Pearson correlations showed that the link between multiple demographic data and the HbF % at the first visit was not significant (Table 6). However, for all parturients included, significant variables linked with HbF expression were β-HCG, MCH, RDW, HbA1C, and ferritin. For the HbF positive group, the results show a significant positive association between HbF expression and β-HCG, HbA1C, MCH, and RDW, as well as a significant negative association between HbF expression and total hemoglobin (Table 7, Figure 1 and Figure 2). Those results had a p-value of 0.00001.
4. Discussion
The objectives of this study were met to document HbF expression during peri and postpartum periods, to confirm its maternal origin, and to assess clinical and biochemical parameters potentially associated with HbF modulation. To our knowledge, this study depicts the largest cohort description of the expression of HbF in pregnant women. Indeed, the sample size and the number of characteristics studied are sufficient to adequately describe the prevalence and duration of this biologic behavior. Moreover, this study also represents the longest longitudinal evaluation of HbF expression during peri and postpartum periods in the literature. It is also the first study reporting the physiologic expression of HbF in pregnancy studied by HPLC. The current study has wide applicability to pregnant women without comorbid conditions as defined in the exclusion criteria.
The results show that at the first-trimester visit, 176/879 (20.02%) screened women were HbF positive. At any time during total evaluation, 198/879 (22.53%) screened women were HbF positive. At the postpartum visit, 72.9% of HbF positive women showed a decrease of HbF < 1%. This observation allows us to exclude hereditary persistence of fetal hemoglobin syndrome as the cause of higher HbF percentage in participating parturients. Additionnally, flux cytometry confirmed the maternal origin of HbF in all cases as expected because HbF is not expressed at this time in pregnancy in the fetus. For all visits, the mean of erythrocytes expressing fetal hemoglobin was 13.3% (representing mean F-cells percentage). Given the considerable sample size, these results are likely to represent the reality regarding HbF expression in pregnant women and serve as a reference for the future.
The results evidence that 20.02% of pregnant women express HbF. This proportion is higher than the expected 1/8 based on previous reports in the literature [5,6,8,9]. It is even more striking since the selection criteria excluded women with hemoglobinopathies and type 1 diabetes, known populations that have a higher proportion of women with an HbF percentage of ≥ 1% [12].
The data also provides evidence that there is a significant positive association between HbF expression in pregnant women and β-HCG, HbA1C, MCH, and RDW. However, there is a significant negative association between HbF expression and total hemoglobin. The association between β-HCG and HbF has already been described in other reviews. Indeed, Popat established a temporal relationship between β-HCG and HbF rise in pregnancies with and without HCG injections [6]. Similarly, Lee showed that the peaks of β-HCG and HbF, between 9 and 12 weeks of gestation, were concordant [11]. The results of this study present the same pattern, with a spike of β-HCG and HbF during the first trimester in HbF positive women, declining thereafter. However, other studies have not observed this phenomenon. For example, the β-HCG pattern was identical between pregnant women who showed an increase in HbF expression and those who did not in a study by Pembrey and colleagues [10]. Their sample size was only 54 women and HbF measurement was executed with a modified alkaline denaturation method. Noteworthy to be highlighted is the temporality of the HbF rise. Like Pembrey [10] and Kristoffersen [13], the results of this study show that the maximal expression of HbF was during the first trimester. In Popat [6] and Rucknagel’s [9] studies, this peak was rather in the second trimester, and in Boyer’s [14], it was between the 23rd and 31st gestational weeks. In Lee’s study [11], in addition to the first-trimester major HbF peak, two minor peaks (between weeks 16-20 and 22-24) were demonstrated. Therefore, the timing of the maximal HbF spike seems inconsistent. One reason that could explain this variation is the differing inclusion and exclusion criteria between the studies and the distinct HbF measurement methods used. The results suggest that β-HCG may induce HbF synthesis during pregnancy, but the precise mechanism remains unknown. A bystander effect is possible, but a hormone-responsive rise in HbF is certainly a preferred possible mechanism in pregnancy.
The negative relationship between total hemoglobin and HbF expression could be related to the suggested mechanism by Rucknagel and Chernoff of fetal erythropoietic reactivation during pregnancy [9]. They linked this reactivation with the various stressors associated with the beginning of pregnancy, for example, the abrupt rise of β-HCG. A hypothesis for the subsequent gradual decline after the early rise of HbF during pregnancy was the accustoming of the woman’s body to these changes. Various studies have proved the reactivation of HbF synthesis in situations of abrupt expansion of erythropoiesis, like iron deficiency anemia, hemolytic anemia, and acute bleeding [15], [16]. All of these situations correspond to an inverse relationship between HbF expression and total hemoglobin. In an acute phase of erythrocyte repopulation secondary to anemia, it is proposed that the more immature erythrocyte precursors, the Erythroid Burst-Forming Unit (BFU), are temporarily mobilized to enter directly into terminal maturation until the size of the Erythroid Colony-Forming Unit (CFU), the more mature precursors, increase. It was demonstrated in vitro that the presence of BFU is associated with a transient increase in HbF [17,18]. It is thought that the difference in HbF production between BFU and CFU is due to a difference in HbF produced by the F-cells [19]. Anemia is a frequent phenomenon in pregnancy; it is thus possible that the increase in HbF expression in pregnant women is caused by alike mechanisms. However, anemia is usually more pronounced during the third trimester in which expression of HbF is usually not as marked in the results presented here.
A significant positive association between HbF expression and HbA1C was also found in the results. The link between insulin via insulin growth factor 1 (IGF-1) and erythropoiesis has already been well established by previous studies, both in vitro and in vivo [20]. It is believed that IGF-1 acts as an erythropoiesis-inducing hormone via EPO dependant and independent pathways, as shown on in vitro human erythroid colony formation. This hypothesis is supported by the demonstration of erythropoiesis induction by IGF-1 both in the presence and absence of EPO [21,22]. Regarding in vitro human studies, Miyagawa and colleagues observed that IGF-1 stimulated erythropoiesis from the terminal stage of BFU to the stage of CFU [23]. They suggested that insulin and IGF-1 could act as a burst-promoting activity on BFU. In parallel, various authors have already shown the correlation between higher HbF percentage and diabetes, particularly in type 1 diabetes. Koskinen measured that in a population of 1104 patients with type 1 or 2 diabetes, among adults, 6.5% of them had an HbF > 1% 13. Some characteristics, such as younger age, type 1 diabetes, and treatment with insulin, seem to be more strongly associated with HbF expression. Pardini and Wise also established the association between insulin and a higher HbF expression [24,25]. Perrine and colleagues suggested that insulin as well as other growth factors like EPO could cause a change in the production sequence of β-globin gene chains. The finding that the production of β-chains is delayed in newborns of diabetic mothers supports this hypothesis. Indeed, it suggests the persistence of γ-chain production synthesis in a context of hyperinsulinism [26]. Interestingly enough, the only non-experimental treatment currently used for gestational diabetes besides lifestyle changes is insulin. The relation between gestational diabetes and HbF expression has been less reported than the one with type 1 and 2 diabetes. The study shows that there is a significant relation between HbF expression and HbA1C in pregnant women, which could be linked to the regulatory effect of insulin and IGF-1 on human erythropoiesis, as described before. However, to our knowledge, there has not been any research that studied the specific mechanism of IGF-1 during pregnancy yet.
This study is associated with some limitations, but the difference in results compared with previous studies is balanced by the large sample size of the current demonstration. However, one source of variability compared to previous reports concerns the use of HPLC. One study has shown that HbF levels determined by HPLC were inaccurate in the presence of increased HbA1C in 41% of diabetic patients tested [27]. The risk of false positives was greater if the HbA1C % was higher, especially in severe cases with HbA1C measuring between 11.1 and 19.8%. The authors found that this false rise could be predicted by an HbF retention time of over 1.15 minutes. However, this source of error should not have greatly influenced this study’s results since the HbA1C % of the parturients was between 3.7 and 6.4%.
The cause of HbF synthesis induction during pregnancy probably lies within a mix of different factors. β-HCG, acute anemia, and elevated HbA1C are probably some of those associated with the modulation of fetal hemoglobin synthesis. This points to polymorphism in genes associated with HbF production, either directly or indirectly. These could be hormone receptors as well as proteins affected by anemia. Future genetic analyzes with the sequencing of multiple genes of different HbF loci will help to elucidate these mechanisms.
5. Conclusions
In summary, this study showed that HbF expression of ≥ 1% during peri and postpartum periods in pregnant women without influencing comorbidities is at its highest peak during the first trimester. At any time in the study, the highest percentage of HbF positive (≥1%) women among included parturients was 22.53%. The HbF percentage decreased below 1% in 72.9% of positive women in the postpartum period, therefore excluding hereditary persistence of fetal hemoglobin. In all women, it was proven that HbF was of maternal origin. The results show a significant positive correlation between HbF expression and β-HCG as well as HbA1C, and a significant negative association with total hemoglobin . Fetal hemoglobin expression induction during pregnancy is probably associated with these elements, which could temporarily reactivate the fetal erythropoietic system. To our knowledge, this study has the largest sample size and longitudinal evaluation that has ever been reported on fetal hemoglobin expression during pregnancy as of today. Therefore, it provides important reference data. Further investigations are warranted to propose mechanisms leading to physiologic expression of fetal hemoglobin during pregnancy. Mild fetal hemoglobin induction is common in normal pregnancies and should not be a reason for concern. However, it may be associated with anemia and increased risk of diabetes. Since these conditions are already systematically screened for during peripartum care, we do not suggest modifying the management of pregnant women with mild HbF induction at this moment.
Author Contributions
Conceptualization, Denis Soulières and Pierre-Olivier Gaudreau; methodology, Denis Soulières, Pierre-Olivier Gaudreau and Xiaoduan Weng; software, Christian Watier; validation, Denis Soulières, Pierre-Olivier Gaudreau and Michael Newmarch; formal analysis, Christian Watier, Pierre-Olivier Gaudreau, Laurence Blain and Xiaoduan Weng; investigation, Andre Masse, Marie-Josée Bédard, Nazila Bettache, Florence Weber, Michele Mahone and Vincent-Philippe Lavallée; resources, Christian Watier and Xiaoduan Weng; data curation, Christian Watier; writing-original draft preparation, Laurence Blain; writing-review and editing, Laurence Blain, Stéphanie Forte and Denis Soulières; visualization, Laurence Blain and Pierre-Olivier Gaudreau; supervision, Denis Soulières; project administration, Denis Soulières; funding acquisition, Denis Soulières and Pierre-Olivier Gaudreau. All authors have read and agreed to the published version of the manuscript.
Funding
This research was funded by the CHUM (Centre Hospitalier de l’Université de Montréal) hematology-oncology teaching fund.
Institutional Review Board Statement
The study was conducted in accordance with the Declaration of Helsinki, and approved by Ethics Committee of the CHUM (Centre Hospitalier de l’Université de Montréal) (May 6 2013).
Informed Consent Statement
Informed consent was obtained from all subjects involved in the study. Written informed consent has been obtained from patients to publish this paper within the initial consent form.
Data Availability Statement
The data presented in this study are available in Prospective Evaluation of Fetal Hemoglobin Expression in Maternal Erythrocytes: an Analysis of a Cohort of 345 Parturients, Blain Laurence, Soulières Denis and Al.
Conflicts of Interest
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript; or in the decision to publish the results.
References
- Manca, L.; Masala, B. Disorders of the synthesis of human fetal hemoglobin. IUBMB Life 2008, 60, 94–111. [Google Scholar] [CrossRef] [PubMed]
- Orneal, P.S.; Gantt, N.M.; Schwartz, J.D.; Bhanu, N.V.; Lee, Y.T.; Moroney, J.W.; Reed, C.H.; Schechter, A.N.; Luban, N.L.C.; Miller, J.L. Fetal haemoglobin silencing in humans. Blood 2006, 108, 2081–2086. [Google Scholar] [CrossRef] [PubMed]
- Clarke, G.M.; Higgins, T.N. Laboratory investigation of hemoglobinopathies and thalassemias : review and update. Clinical Chemistry 2000, 46, 1284–1290. [Google Scholar] [CrossRef] [PubMed]
- Schuman, J.E.; Tanser, C.L.; Péloquin, R.; de Leeuw, N.K.M. The erythropoietic response to pregnancy in β-thalassemia minor. British Journal of Haematology 1973, 25, 249–260. [Google Scholar] [CrossRef]
- Dunn, D.T.; Poddar, D.; Serjeant, B.E.; Serjeant, G.R. Fetal haemoglobin and pregnancy in homozygous sickle cell disease. British Journal of Haematology 1989, 72, 434–438. [Google Scholar] [CrossRef]
- Popat, N.; Wood, W.G.; Weatherall, D.J.; Turnbull, A.C. Pattern of maternal F-cell production during pregnancy. Lancet 1977, 2, 377–379. [Google Scholar] [CrossRef]
- De Ceulaer, K.; Hayes, R.; Gruber, C.; Serjeant, G.R. Medroxyprogesterone acetate and homozygous sickle-cell disease. Lancet 1982, ii, 229–231. [Google Scholar] [CrossRef]
- Weatherall, D.J.; Clegg, J.B. The thalassemia syndromes. 3rd edition; Blackwell Scientific: Oxford, 1981; pp. 76–77. [Google Scholar]
- Rucknagel, D.L.; Chernoff, A.I. Immunologic studies of hemoglobins. III. Fetal haemoglobin changes in the circulation of pregnant women. Blood 1955, 10, 1092. [Google Scholar] [CrossRef]
- Pembrey, M.E.; Weatherall, D.J.; Clegg, J.B. Maternal synthesis of haemoglobin F in pregnancy. Lancet 1973, 1, 1350–1354. [Google Scholar] [CrossRef]
- Lee, J.C.; Hayashi, R.H.; Shepard, M.K. Fetal hemoglobin in women with normal and with hydatidiform molar pregnancy. American Journal of Hematology 1982, 13, 131–139. [Google Scholar]
- Koskinen, L.K.; Lahtela, J.T.; Koivula, T.A. Fetal hemoglobin in diabetic patients. Diabetes Care 1994, 17, 828–831. [Google Scholar] [CrossRef] [PubMed]
- Kristoffersen, K. FOETAL HAEMOGLOBIN IN MATERNAL BLOOD DURING PREGNANCY AND DELIVERY. Acta Obstet Gynecol Scand. 1964, 42, 74–77. [Google Scholar] [CrossRef]
- Boyer, S.H.; Belding, T.K.; Margolet, L.; Noyes, A.N.; Burke, P.J.; Bell, W.R. Variations in the frequency of fetal haemoglobin-bearing erythrocytes (F-cell) in well adults, pregnant women, and adult leukemics. The John Hopkins Medical Journal 1975, 137, 105–115. [Google Scholar]
- Dover, G.J.; Boyer, S.H.; Zinkham, W.H. Production of erythrocytes that contain fetal haemoglobin in anemia. Journal of Clinical Investigations 1979, 63, 173–176. [Google Scholar] [CrossRef] [PubMed]
- Blau, C.; Constantoulakis, P.; Al-Khatti, A.; Spadacino, E.; Goldwasser, E.; Papayannopoulos, T.; Stamatoyannopoulos, G. Fetal hemoglobin in acute and chronic states of erythroid expansion. Blood 1993, 812, 227–233. [Google Scholar] [CrossRef]
- Ishikawa, Y.; Ito, T. Kinetics of hemopoietic stem cells in a hypoxic culture. European Journal of Haematology 1988, 40, 126–129. [Google Scholar] [CrossRef] [PubMed]
- Lu, L.; Broxmeyer, H.E. Comparative influences of phytohemagglutinin-stimulated leukocyte conditioned medium, hemin, prostaglandin E, and low oxygen tension on colony formation of erythroid precursor cells in normal human bone marrow. Experimental Hematology 1985, 13, 989–993. [Google Scholar]
- Dover, G.J.; Chan, T.; Sieber, F. Fetal haemoglobin production in cultures of primitive and mature human erythroid progenitors: differentiation affects the quantity of fetal haemoglobin produced per fetal-hemoglobin-containing cell. Blood 1983, 61, 1242–1246. [Google Scholar] [CrossRef]
- Halvorsen, S.; Bechensteen, A.G. Physiology of erythropoietin during mammalian development. Acta Paediatr Suppl. 2002, 91, 17–26. [Google Scholar] [CrossRef]
- Kurtz, A.; Jelkmann, W.; Bauer, C. A new candidate for the regulation of erythropoiesis. Insulin-like growth factor I. FEBS Lett 1982, 149, 105–108. [Google Scholar] [CrossRef]
- Correa, P.N.; Axelrad, A.A. Productio n of erythropoieti c bursts by progenitor cells from adult human peripheral blood in an improved serum-free medium: role of insulinlike growth factor 1. Blood 1991, 78, 2823–2833. [Google Scholar] [CrossRef] [PubMed]
- Miyagawa, S.; Kobayashi, M.; Konishi, N.; Sato, T.; Ueda, K. Insulin and insulin-like growth factor I support the proliferation of erythroid progenitor cells in bone marrow through the sharing of receptors. Br J Haematol 2000, 109, 555–562. [Google Scholar] [CrossRef] [PubMed]
- Pardini, V.C.; Victória, I.M.; Pieroni, F.B.; Milagres, G.; Nascimento, P.D.; Velho, G.; Purisch, S.; Pardini, H. Fetal hemoglobin levels are related to metabolic control in diabetic subjects. Braz J Med Biol Res. 1999, 32, 695–701. [Google Scholar] [CrossRef] [PubMed]
- Wise, J.E.; Sauder, S.E.; Weiss, A.E. Increased fetal hemoglobin production in a child with congenital hyperinsulinism. Journal of Pediatry 1987, 110, 912–914. [Google Scholar] [CrossRef]
- Perrine, S.P.; Greene, M.F.; Faller, D.V. Delay in the fetal globin switch in infants of diabetic mothers. New England Journal of Medicine 1985, 312, 334–338. [Google Scholar] [CrossRef]
- Grey, V.; Wilkinson, M.; Phelan, L.; Hughes, C.; Bain, B.J. Inaccuracy of high-performance liquid chromatography estimation of haemoglobin F in the presence of increased haemoglobin A1C. International Journal of Laboratory 2007, 29, 42–44. [Google Scholar] [CrossRef]
Figure 1.
HbF percentagle by HPLC for HbF positive parturients.
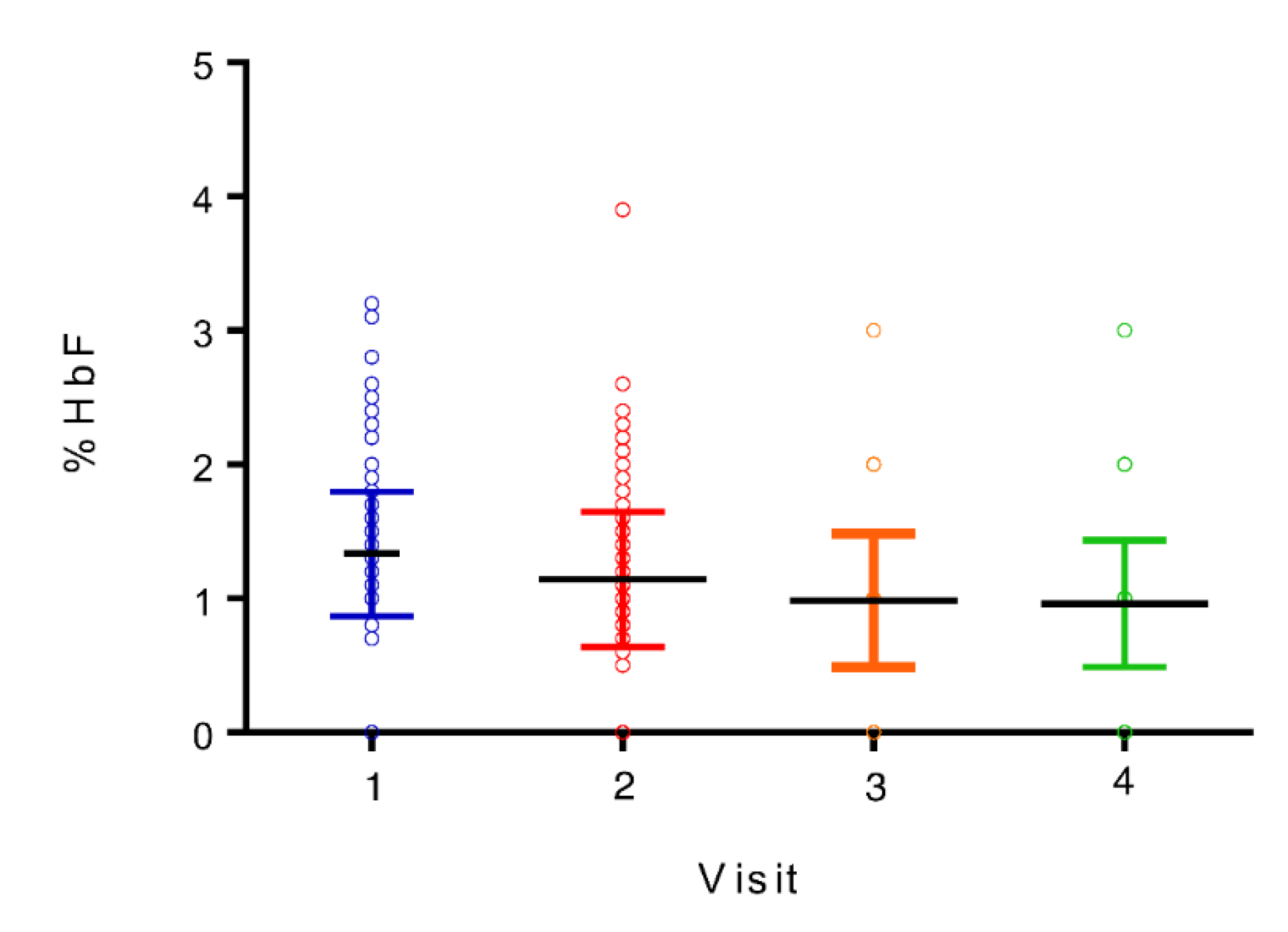
Figure 2.
β -HCG per visit for HbF positive parturients.
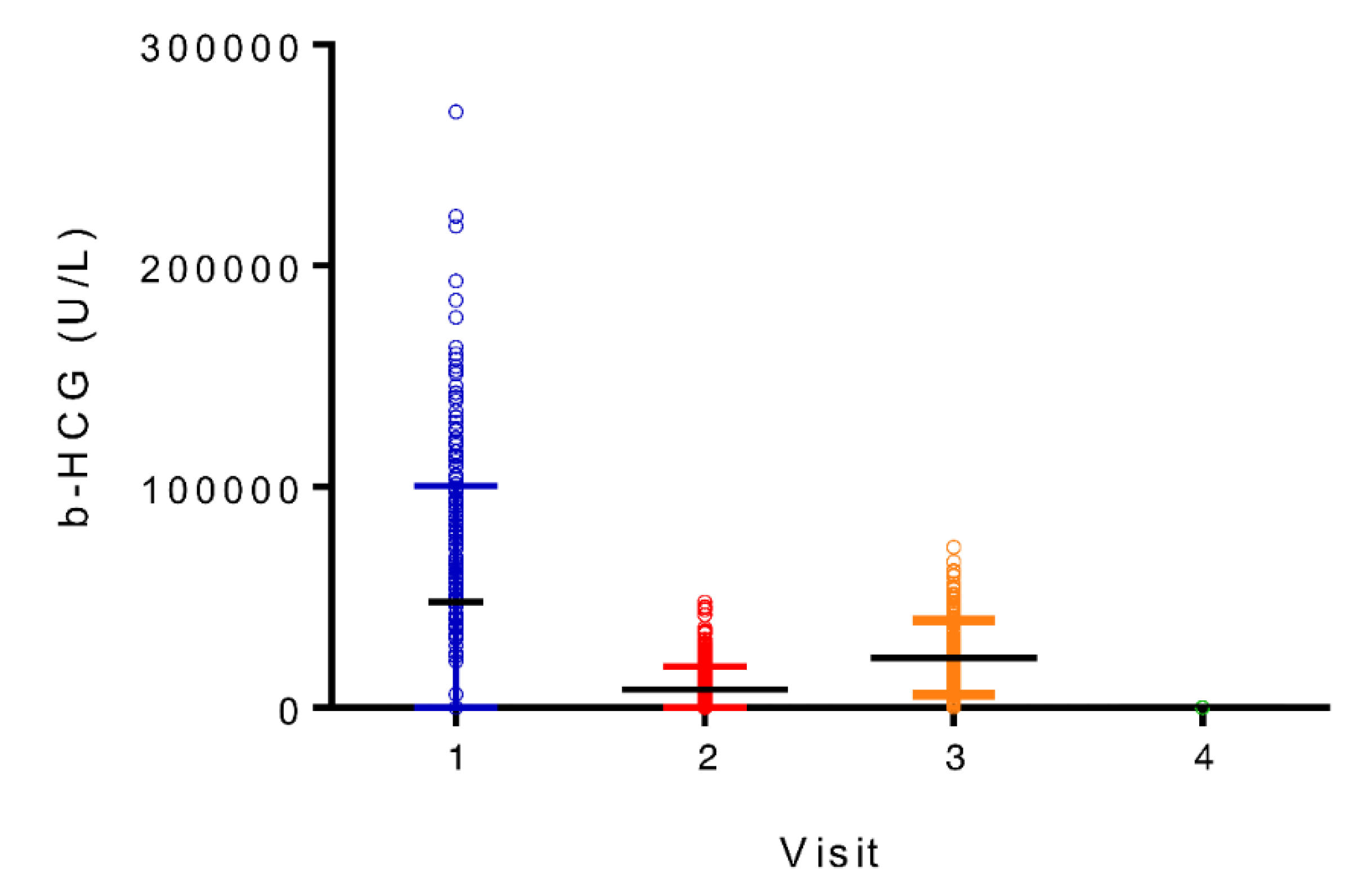

Table 1.
demographic values.
| Demographic value | Detail | Number (%) SD |
|---|---|---|
| Age | Mean | 32.29 (NA) 4.11 |
| Minimum | 20 (NA) | |
| Maximum | 44 (NA) | |
| More than 35 years old | 255/345 (73.9) | |
| Less than 35 years old | 90/345 (26.09) | |
| History of smoking | Number of parturients | 124/345 (35.94) |
| Mean of years of smoking in parturients with smoking history | 3.28 (NA) 5.62 |
|
| Mean of number of pregnancies | 2.00 (NA) 1.20 |
|
| Mean of parity | 0.57 (NA) 0.72 |
|
| Multiple pregnancy | 2/345 (0.58) | |
| History of anterior fertility clinic consultation | 41/345 (11.88) | |
| History of hypertension | 10/345 (2.90) | |
| Parturients with hypertension at first visit | 3/345 (0.87) | |
| Parturients with active preeclampsia at first visit | 0/345 (0) | |
| Parturients with gestational diabetes at first visit | 1/345 (0.29) | |
| History of type 2 diabetes | 0/345 (0) | |
| Use of progesterone before visit 1 | 23/345 (6.67) | |
NA: non applicable; SD: standard deviation.
Table 2.
Descriptive statistics of the study.
| Value | n |
|---|---|
| Number of women screened | 879 |
| Number of women included in the study | 345 |
| Number of HbF negative women at first visit selected for comparator group | 169 |
| Number of HbF negative women who completed follow-up at time of analysis | 147 |
| Number of HbF positive women at first visit | 176 |
| Number of HbF positive women at anytime during evaluation | 198 |
| Number of HbF positive women who completed follow-up at time of analysis | 155 |
Table 3.
Median HbF percentage in HbF positive women.
| Visit | Median Hb F percentage (%) | Range (%) |
|---|---|---|
| 1 (weeks 8-12) | 1.2 | 0-3.2 |
| 2 (weeks 24-28) | 1.0 | 0-3.9 |
| 3 (week 36) | 0.8 | 0-3.2 |
| 4 (6 weeks postpartum) | 0.7 | 0-2.9 |
Table 4.
Means of blood parameters.
| Value | Visit 1 Mean (SD) |
Visit 2 Mean (SD) |
Visit 3 Mean (SD) |
Visit 4 Mean (SD) |
|---|---|---|---|---|
| Hemoglobin (g/L) |
126.2 (8.3) |
117.4 (8.0) |
120.2 (10.1) |
132.2 (8.0) |
| Hematocrit (L/L) |
0.367 (0.022) |
0.349 (0.022) |
0.356 (0.026) |
0.397 (0.022) |
| RBC (*1012/L) |
4.15 (0.30) |
3.82 (0.28) |
3.95 (0.30) |
4.43 (0.30) |
| MCV (fL) |
88.8 (3.4) |
91.7 (3.7) |
90.5 (4.4) |
89.9 (3.9) |
| RDW (%) |
12.9 (0,7) |
13.3 (0.6) |
13.5 (0.8) |
13.2 (1.6) |
| MCHC (g/L) |
343.6 (7.9) |
336.4 (7.7) |
337.4 (9.2) |
332.7 (9.2) |
| MCH (pg) |
30.5 (1.3) |
30.8 (1.5) |
30.5 (1.9) |
29.9 (1.6) |
| Reticulocytes (*109/L) |
70.8 (20.7) |
82.9 (20.7) |
88.5 (19.0) |
55.5 (17.3) |
| Ferritin (ng/ml) |
72.2 (48.9) |
29.9 (81.2) |
20.7 (14.8) |
66.8 (47.5) |
| β -HCG (mUI/ml) |
86344 (41388) |
15151 (10549) |
22916 (17840) |
225 (2831) |
| EPO (UI/L) |
9.1 (3.5) |
18.9 (11.4) |
26.6 (31.1) |
7.8 (3.9) |
| HbA1C (%) |
5.095 (2.99) |
4.911 (3.482) |
5.192 (3.934) |
5.318 (3.809) |
RBC: red blood cells count / MCV: mean corpuscular volume / RDW: red cell distribution width / MCHC: mean corpuscular hemoglobin concentration / MCH: mean corpuscular hemoglobin/ β -HCG: beta human chorionic gonadotropin / EPO: Erythropoietin / ; HbA1C: glycosylated hemoglobin/ SD: standard deviation.
Table 5.
F-cells percentage in HbF positive women.
| Visit | Minimum (%) | Maximum (%) | Range (%) | Mean (%) |
|---|---|---|---|---|
| 1 (weeks 8-12) | 4.0 | 32.8 | 28.8 | 13.89 |
| 2 (weeks 24-28) | 4.0 | 30.2 | 26.2 | 13.48 |
| 3 (week 36) | 5.2 | 26.9 | 21.7 | 12.22 |
| 4 (6 weeks postpartum) | 4.8 | 22.8 | 18.0 | 11.48 |
| All visits | 4.0 | 32.8 | 28.8 | 13.30 |
Table 6.
Independent t-tests and Pearson correlations between demographic data and HbF % at the first visit.
Table 6.
Independent t-tests and Pearson correlations between demographic data and HbF % at the first visit.
| T-tests relation | t value | p-value |
|---|---|---|
| HbF Positive/Negative women and total hemoglobin | NA | NS |
| Age (above or below 35 years-old) and HbF % | -0.114144 | 0.909190 |
| Smoking status and HbF % | 1.787341 | 0.074770 |
| Fertility clinic consultation and HbF % | 1.189824 | 0.234939 |
| Hypertension history and HbF % | -0.451676 | 0.651788 |
| Use of progesterone and HbF % | 0.916958 | 0.359809 |
| Pearson correlations relation | p-value | |
| Weight and HbF % | 0.05 | |
| Number of years of smoking and HbF % | 0.05 | |
| Number of pregnancies and HbF % | 0.05 | |
NS : non-significant; NA: non applicable.
Table 7.
Correlation coefficients of multivariate analyses between HbF, F-Cells percentage and various variables.
Table 7.
Correlation coefficients of multivariate analyses between HbF, F-Cells percentage and various variables.
| Ascending stepwise regression variables (all visits) | p-value | Adjusted correlation coefficient (R2) |
|---|---|---|
| All parturients and all variables to predict HbF % | 0.0041 | 62.20% |
| All parturients and significant variables to predict HbF % | 0.0010 | 58.44% |
| All parturients and all variables to predict F-cells % | 0.0539 | 76.49% |
| All parturients and significant variables to predict F-cells % | 0.1139 | 68.29% |
| All parturients and all variables to predict F-cells intensity | 0.0141 | 64.99% |
| All parturients and significant variables to predict F-cells intensity | 0.0141 | 64.99% |
| HbF positive parturients and all variables to predict HbF | 0.0013 | 16.14% |
| HbF positive parturients and significant variables to predict HbF | 0.0000 | 15.18% |
| HbF positive parturients and all variables to predict F-cells % | 0.0567 | 76.53% |
| HbF positive parturients and significant variables to predict F-cells % | 0.9977 | 75.87% |
| HbF positive parturients and all variables to predict F-cells intensity | 0.0140 | 64.98% |
| HbF positive parturients and significant variables to predict F-cells intensity | 0.0140 | 64.98% |
All variables: b-HCG, MCV, RBC, HbA1C, EPO, MCHC, Hb, Ferritin, EPO; Significant variables: b-HCG, MCV, HbA1C, MCHC, Hb.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



