Submitted:
12 May 2023
Posted:
19 May 2023
You are already at the latest version
Abstract
Background: Significant national and global costs were incurred from recent emerging infectious disease outbreaks, notably H1N1 highly pathogenic influenza, Zika and Severe Acute Respiratory Disease (SARS), both in the medical sphere and within the socioeconomic context around it. With forecasts expecting an increase in direct and indirect burden of novel infectious disease events, costs of future outbreak events are likely to be exacerbated. In this scope, it is critical for countries to identify this trend and work towards minimizing costs while continuing to improve prevention, treatment and mitigation. Objectives: The impacts of the West Africa Ebola crisis have largely focused on the response to the outbreak abroad. The aim of this paper was to determine the direct and indirect domestic costs of the Ebola Virus Disease (EVD) introduction into the United States (U.S.), compare the economic consequences of the epidemic with other disease outbreaks and identify the primary drivers of such costs to leverage more global health preparation to prevent, prepare for, and respond to disease threats more effectively. Methods: I conducted a literature review of 1) EVD cases documented by the U.S. Centers for Disease Control and Prevention (CDC) and the World Health Organization (WHO), 2) scientific articles identifying the costs of Ebola for the U.S. and countries around the world and 3) grey literature on treatments and public reactions. Extrapolating data from these sources, I then performed a cost-analysis of direct costs (preparation, treatment and contact tracing) and indirect costs (loss of productivity owing to disease, death, and risk avoidance behaviors) of the disease. Findings: The country spent between $300-$700 million in direct costs. Additionally, roughly $200-$340 million were forgone as results of loss of productivity from to disease, death or social risk avoidance behaviors. The cost-per-case for the United States was vastly higher than for any other country. Conclusions: High direct costs suggest that either the United States took disproportionate preparative measures to mitigate a potential American outbreak or were unprepared for a potential outbreak of this magnitude. The significant risk avoidance behavior estimates hint that forces having the ability to shape social attitudes and norms – namely traditional and online media – played a significant role in driving social behavior towards fear of exposure to others. The findings reinforce that outbreaks occurring in a single part of the world can have dramatic economic effects globally, even in areas with existing public health capacity and other preventive measures, highlighting the need for change in global health systems to shift from a passive responder and incorporate other societal actors to effectively reduce the ever-increasing costs of disease threats.
Keywords:
Ebola
; EVD
; cost-analysis
; cost-benefit analysis
Introduction
The economics of emerging infectious diseases are becoming increasingly relevant in global policymaking [1,2]. With a rising burden of emerging infectious diseases in the past two decades, as evidenced by the appearance of epidemics like SARS, H1N1, dengue fever, the Zika virus and the Ebola Virus Disease (EVD), the cost implications of these outbreaks extend far beyond traditional health sectors [3]. In a world recognizing these trends, efforts have emphasized the need for a better integrated global approach to health security by targeting identification and mitigation of newly-emerging infectious disease threats before they reach human populations and responding rapidly to diseases once detected to curb their spread [4,5].
Yet, at this stage, global health models are based on episodic, acute care models primarily concentrated on treating sick populations [5,6]. This was particularly evident during the 11 cases of EVD in the United States. Declared a public health event of international concern by the World Health Organization (WHO) in July 2014, the outbreak was primarily concentrated in the West African nations of Guinea, Liberia and Sierra Leone, where it manifested in 28,616 confirmed cases[7]. Partially due to poor health system capacity, skilled international healthcare workers were deployed to help mitigate the crisis. Amongst the American staff to participate, several were repatriated home after contracting EVD. Others were only identified as ill after arriving within the country, hence opening the possibility of a domestic EVD outbreak [8].
With the first confirmed case of Ebola identified in the United States in late September 2014, the nation engaged in preparative efforts to mitigate the threat of an epidemic. The Department of Health and Human Services (HHS), along with the Office of the Assistant Secretary for Preparedness and Response (ASPR), and the Office of Emergency Management’s Division of National Healthcare Preparedness Programs (OEMDNHPP), identified a cohesive response framework [9]. A collaboration between the private health care system, federal officials and public institutions culminated in the division of national health facilities into four primary response units. 4,845 frontline health care facilities were identified for first-response duties, isolation and diagnosis and eventual discharge or transfer. 217 Ebola assessment hospitals and 63 Ebola treatment centers (ETCs), specialized as buffer zones, had the isolative capacity to treat high volumes of patients. Lastly, 10 regional EVD hospitals were organized to be ready to receive domestically diagnosed patients with confirmed Ebola from their region, or a patient medically repatriated, within 8 hours. In total, 11 patients were diagnosed with Ebola in the U.S., including domestic healthcare-acquired infections. The cost implications of implementing the response framework and domestic transmission has not been estimated to date.
As such, this paper offers an analysis of domestic costs of EVD borne by the United States. Firstly, I estimated the costs of preparation, treatment, and contact tracing efforts as a response to the 11 domestic cases of EVD. Secondly, I explored the indirect costs of the disease associated with the societal behaviors of Americans during the domestic crisis.
Literature Review
Several studies examined the socio-economic impacts of the Ebola crisis in West Africa. The World Bank estimates $2.8 billion in GDP growth projection was lost in Sierra Leone, Guinea and Liberia in 2015 [10], from lower investments and decrease in private sector growth, increased food insecurity and rising commodity prices. The United Nations assessed it cost the three West-African nations roughly $290.6 million in direct costs to control the epidemic [11,12]. A study calculating the costs of responding to an Ebola cluster varied from $113,000 to $1.8 million, primarily driven by travel and personnel costs [12].
Compared to estimates of costs incurred for response in West Africa, the scientific literature on the costs of EVD preparedness and response for domestic cases within the United States is limited. Deploying a phone survey with 222 hospitals, a study finds the mean costs of overtime, training and supply combined was circa $80,000 per acute care hospital [13]. For Ebola Treatment Centers (ETCs), a hospital spent roughly 1.2 million dollars [14], which includes initial training of staff, construction and modifications. A recent study states the United States spent $3.3 billion in direct costs, contributing to a cost amounting to $53 billion incurred globally [11].
The costs of potentially producing 27 million vaccinations in the United States was estimated at $73 million [15]. Depending on the relative transmissibility of isolated individuals, the cost and incidence of the EVD outbreak yielded between 4 and 5 billion dollars. In the “best case” scenario, the forecast still amounted to 1-2 billion dollars.
Internationally, the costs of preparedness and response to EVD in the Dutch health system equaled €12.6 million ($13.9 million), with a range of €6.7 to €22.5 million ($7.3 – $24.7 million) for 13 evaluated and 1 confirmed case [16]. This includes the amount of time dedicated to preparation and treatment of Dutch healthcare professionals, the cost of equipment, cleaning, patient hospitalization and monitoring. Using a cost of illness method to calculate future non-health gross domestic product (NHGDP) losses associated with EVD deaths in five West-African nations, a study found that for 11,234 deaths, the discounted value of future NHGDP loss amounted to $155.6 million, a cost borne primarily by Guinea, Sierra Leone and Liberia [17]. In Nigeria, where 20 cases were seen, the costs of running awareness campaigns, purchasing prevention materials and training staff about EVD over a four months period amounted to 1.2 billion naira, or approximately US$2.85 million [18]. These efforts extended to 4,000 schools, 253 hospitals and 451 hotels, from July 20 to November 20, 2014.
In the U.S, former President Barack Obama made a 6.2 billion dollars funding request named FY2015 Emergency Ebola Appropriation, later approved by Congress for 5.4 billion dollars [19]. As no literature details the exact distribution of these funds to domestic uses, versus international response efforts, I was unable to determine whether the costs found in our study related to U.S.- based cases had been covered by the FY2015 EEA (i.e., whether hospitals and public health departments were fully reimbursed by federal funding). In addition to real-time outbreak response in West Africa and screening at ports of entry, a portion of the Ebola Appropriation funds supported post-Ebola recovery in the form of laboratory and other public health system strengthening abroad; additionally, a portion of the funds was redirected to Zika virus response in Latin America. In order to avoid double-counting of costs, I elected to omit this funding package from our calculations. I recognize the importance, however, of factoring this budget into the broader analysis of the total economic impact of EVD globally and, more generally, the economics of newly-emerging infectious diseases.
Methods
The calculations of direct and indirect costs in the U.S. reflect the period January – December 2014, during which 11 cases were diagnosed, with three of those infected within the U.S. (i.e., localized/domestic transmission) from imported cases (infections acquired abroad). Direct costs are understood in this paper as the monetary amount applied to prevention, treatment and response. Indirect costs, meanwhile, refer to the cascading costs resulting from societal behavior. In other words, indirect costs embody the market opportunity costs of populations reacting to the news of disease and adopting specific risk avoidance behaviors.
Health care facility costs
As the mean cost per ETC was already calculated by a previous study [14], including construction/facility modification, personal protective equipment (PPE) supplies, staff training, unit planning, laboratory equipment and non-PPE laboratory equipment, I scaled the figure to match the number of ETCs and find the cost-estimate of preparation for these facilities.
𝐴 = 𝑥 × 63
A = Total preparation costs of ETCs
x = average costs of preparation per ETC
To find the costs of preparation for acute-care hospitals, I extrapolated the findings in the study by Smit et al. [13] at the national level by considering the mean average costs of preparation and multiplying it by the number of facility type (excluding ETCs). I assumed all hospitals in the nation were classified in a tier as per the response framework detailed above and had prepared in some capacity for the potential eventuality of an EVD epidemic. This gave a representative figure of the costs of preparation for non-specialized hospitals.
𝐵𝑡𝑦𝑝𝑒 = (𝑧𝑡𝑦𝑝𝑒 × ℎ)
Btype = total preparation costs for hospital type
ztype = average cost of preparation per hospital type
h = type of hospital
Treatment costs
I used grey literature to estimate the treatment costs for the 11 cases. Chancellor Jeffrey Gold of the University of Nebraska Medical Center stated in a testimony that it cost $30,000 a day to treat an Ebola patient[20]. I contrasted this figure with the $18 to $24 thousand per day cost stated by Professor Anderson at John Hopkins University’s Bloomberg School of Public Health to estimate a range of cost of treatment [21]. Using these figures, I calculated the cost per patient based on the number of days in hospital for each person using 24 thousand as the mean estimate, 18 as minimum and 30 as maximum costs.
𝐶𝑝 = 24,000 × 𝑑𝑝
Cp = cost of treatment for an individual patient
p = patient name
dp = number of days in hospital per patient
Outbreak investigation/contact tracing costs
I calculated the composition of contact tracing teams (also commonly referred to as Follow-Up teams) for the three domestically-infected and diagnosed patients by combining a benchmark case study of a contact tracing team in Senegal composed by the U.S. CDC [22] and WHO guidelines[23]. Contact tracers were deployed to stop the chain of disease transmission by monitoring, detecting, and isolating any new infections stemming from those who had contact with infected individuals, with follow-up time based on the roughly three-week window for development of infections. The analysis is based on the following assumptions that drive the scale of wage costs:
- The CDC deployed 4 health workers to trace 74 contacts in Senegal. To calculate salary costs, I assumed the 4 workers were social workers, whom are best positioned to understand social relationships, build trust with at-risk patients and retrace contacts.
- There was at least 1 head epidemiologist and 1 field epidemiologist per team. It is likely the actual teams featured more roles. However, without the necessary data, I assumed there to be only 1 of each for our costs calculations.
- There was at least 1 data entry keyer per team. The reasoning for this assumption follows that of the epidemiologists.
- The rest of the team was comprised of nurses and/or supervisors.
As the CDC allocated 4 health workers for 74 contacts in Senegal, I used the average of 18.5 contacts traced per worker.
HWcity = health worker per city
TCcity = total contacts identified per city
ACcity = average number of contacts per health worker
I found the following for the three U.S. cities with EVD cases, estimating approximately 23 health workers involved in outbreak investigation/contact tracing:
To determine the minimum number of nurses per contact-tracing team as part of the Follow-Up teams, I assumed they worked 9 hours daily, slightly over the national average of 8.4 hours [24] and performed a consultation every 20 minutes (rounded up from the mean time for a doctor’s visit of 17.4 minutes [25]). This approximated roughly 3 patients per hour. From this, I determined that a nurse could consult 27 patients a day.

C = number of patients a single nurse can care for per day
As each contact was obligated to two daily checkups, I determined the number of nurses per contact tracing team by doubling the number of contacts traced per city and dividing by C.
A similar approach was used to calculate the number of supervisors per team. Assuming 1 supervisor was required for 3 nurses yielded the following:
The final composition of contact tracing teams can be found in Table 1.
Productivity Losses
The loss of productivity was calculated using the loss of productivity owing to EVD, both to cases (including for the two deaths that ensued) and to the general public that enacted disease avoidance measures, derived from existing literature using Weintraub’s equations for disease impacts and can be found in Table 3 [26].
The variables averaging daily wage, daily benefits and average cost per hire were pulled from the Bureau of Labor Statistics. The number of cases and contacts, prevalence, morbidity and mortality rates, and days lost were taken from CDC case studies. Lastly, the staff numbers were extracted from the findings.
With a population sample consisting of infected patients and contacts traced, the sample is unrepresentative of the entire American population. However, the findings can still be interpreted as a starting point for further research. As the two EVD deaths in the U.S. were of people in the medical profession, I assumed the two replacements did not require work- specific training and would be ‘productive from day one’. However, I considered that there may be environment-specific training and workshops for context familiarization and team-building. I assumed both replacements would receive at a minimum the equivalent of one week of familiarization that had to be discounted in our analysis (42 hours, in 5 days a week full-time).
The avoidance behavior analysis was based on a study performed by the analytics firm Gallup [27,28]. They compared Americans’ avoidance behavior tendencies by contrasting the fear Americans had of contracting H1N1 at the heart of the epidemic in 2009 and the fear they had of being infected with EVD in 2014, relative to the total number of domestic cases. The results show 22% of Americans were afraid to contract EVD, an identical figure to Americans’ fear of getting H1N1 in 2009, despite a disproportionate difference in number of domestic cases (11 EVD cases compared to 60 million influenza cases domestically [29]). In comparison, 90% of Americans thought they were unlikely to contract Zika virus [30]. From these findings, we reasonably inferred that Americans had at a minimum employed similar avoidance behavior to H1N1 during the EVD outbreak and therefore used previous avoidance findings for H1N1 in the U.S. to inform our calculations.
A study found that on average people spent an additional 22 minutes per day at home during the peak period of H1N1 [31]. I extrapolated this number to match EVD’s peak period of 65 days, ranging from the first to the last reported domestic case of EVD and two incubation periods [32].
𝑇𝐿𝑃𝑝𝑒𝑟𝑠𝑜𝑛 = (𝑇𝐻mn 𝑑𝑎𝑦𝑠 × 𝑊𝑐𝑖𝑡𝑦 ) − (𝑇𝐻𝐿mn 𝑑𝑎𝑦𝑠 × 𝑊𝑐𝑖𝑡𝑦 )
TLPperson = total lost productivity per person over 65 days
TH65 = total hours worked per person employed full time over 65 days
THL65 = total hours of work lost per person to social avoidance behaviors over 65 days
Wcity = median hourly wage for the cities
With this figure, I used the mean hourly wage [24] for NYC, Dallas and Cleveland’s metropolitan areas and their average populations [33] to determine the loss of productivity from avoidance behaviors, assuming they affected work activities (e.g. late or missed work because of panic, whether rational or irrational, of coming into contact with the virus) in the three cities over EVD’s peak period.
𝑇𝐿𝑃𝑐𝑖𝑡𝑦 = 𝑇𝐿𝑃𝑝𝑒𝑟𝑠𝑜𝑛 × 𝑃𝑐𝑖𝑡𝑦
TLPcity = total lost productivity for city
Pcity = Population of city
I was able to estimate the indirect costs from having to isolate EVD patients incurred by the four hospitals by subtracting the calculated cost of treatment for the first case of Ebola introduction into the U.S. from the total costs incurred by Texas Presbyterian as estimated by the hospital’s CEO at $500,000 [21]. The patient, Thomas Eric Duncan, was stated to be uninsured.

ICTexas Presb./Duncan = indirect costs for Texas Presbyterian hospital for Thomas Duncan
CDuncan = the costs of treatment for Thomas Duncan
dduncan = days in hospital for Thomas Duncan
From this, I then estimated the individual indirect costs of hospitals for the 11 cases.
𝑇𝐼𝐶ℎ = 𝐼𝐶𝑇𝑒𝑥𝑎𝑠 𝑃𝑟𝑒𝑠𝑏./D𝑢𝑛𝑐𝑎𝑛 × 𝑑𝑝
TICh = Total indirect costs for hospitals
dp = days in hospital per patient
Results
I estimated the 11 domestic cases of Ebola Virus Disease cost the American economy from $700 million to $1 billion for hospital facility upgrades, contact tracing for disease investigation, treatment, and lost wages in the form of illness, death, and disease avoidance. Table 4 illustrates the results.
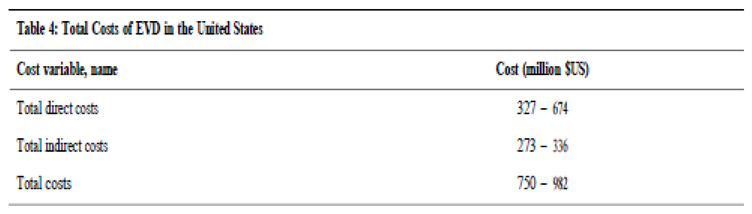
Figure 1 shows the breakdown of direct and indirect costs as follows:
Direct costs
Displayed in Table 5 are the direct costs associated with EVD for the period January 2015 – March 2015. 1 to 11% were preventive costs incurred by the 63 Ebola Treatment Centers, approximating 75.6 million dollars. A further 75 to 83% of total direct costs are represented by the preparation costs of American community hospitals. The costs arising from this preparation can be generalized to between $273 million and $505 million. The regional hospitals and Ebola assessment hospitals incurred mean costs of $0.8 million and $17.4 million respectively.
Treatment costs varied between $0.32 and $1.40 million, but never represented more than 1% of total direct costs. Lastly, $45 million were spent by the American government for emergency repatriation for 9 American patients infected abroad (patients in addition to the 11 diagnosed in the U.S.).
I estimated a cost of approximately $2 million (0.02% of total costs) were necessary to organize the contact tracing teams and follow-up for the three patients infected domestically.

Table 6.
Costs of Contact-Tracing and Follow-Up (in $US).
| Role | New York | Dallas | Cleveland | Total | |||
| Social worker | |||||||
| Cost/hour | 174 | 243 | 223 | 641 | |||
| Cost/week | 1,566 | 2,187 | 2,016 | 5,769 | |||
| Cost/65 days | 101,790 | 142,155 | 131,030 | 374,985 | |||
| Nurses | |||||||
| Cost/hour | 360 | 490 | 455 | 1,305 | |||
| Cost/week | 22,680 | 48,020 | 41,405 | 112,105 | |||
| Cost/65 days | 210,600 | 445,900 | 384,475 | 1,040,975 | |||
| Epidemiologists | |||||||
| Cost/day | 756 | 666 | 630 | 2,052 | |||
| Cost/week | 5,292 | 4,662 | 4,410 | 14,364 | |||
| Cost/65 days | 49,140 | 43,290 | 40,950 | 133,380 | |||
| Data entry | |||||||
| Cost/day | 15 | 144 | 135 | 432 | |||
| Cost/week | 1,071 | 1,008 | 945 | 3,024 | |||
| Cost/65 days | 9,945 | 9,360 | 8,775 | 28,080 | |||
| Supervisor | |||||||
| Cost/day | 1,080 | 1,575 | 1,260 | 3,915 | |||
| Cost/week | 7,560 | 11,025 | 8,820 | 27,405 | |||
| Cost/65 days | 70,200 | 102,275 | 81,900 | 254,475 | |||
| Total/week | 197,281 | ||||||
| Total/65 days | 1,831,895 | ||||||
Indirect costs
The findings for indirect costs are found in Table 7:
Unsurprisingly, the highest costs occurred at the risk-avoidance level. Extrapolating the data for communities living within the greater urban areas of the three major cities, I found that people staying at home an extra 22 minutes represents a significant loss in productivity. This is further compounded by the loss of productivity due to illness and death for the 11 patients. There is also a high indirect cost for hospitals hosting the 11 patients because of the mandatory isolation which dramatically reduced the hospitals’ total patient capacity, as detailed in Table 8.
Discussion
The calculations of this study estimate that the mean cost per Ebola patient diagnosed in the United States (i.e., total costs divided by 11 patients) ranges from $47.5 to 80 million (direct and indirect costs) depending on severity of cases, sample population size for behavioral computations and magnitude of investment for response interventions. As expected, the major driver of cost per case was preparation and treatment, but estimated losses from behavioral adaptation to avoid disease were much more significant than anticipated as a portion of total costs.
A key challenge of comparing these findings to existing literature is the difference in methodologies and locations used to calculate costs-per-case. A study estimated a single Ebola case in West Africa cost between $480 and $18,929, but their calculations exclude indirect costs borne by hospitals[34]. Estimates from the United Nations claim direct costs (to control the epidemic) for Sierra Leone, Guinea and Liberia to have amounted to $290.6 million [11]. These estimates are significantly lower than our findings and may be due to differences in level of economic development, cost of healthcare, technological and regulatory differences and extensiveness of preparation.
The total costs of $522 to $880 million are significantly less than estimated by a study that found EVD to have generated costs of at least $53.2 billion globally, with the United States spending at least $3.32 billion in direct funding [11]. Differences in findings may be explained by methodological variance (e.g. using standardized costs scales across counties that are less precise than our national and sub-national estimates), and the likely inclusion of the Congressional budget for Ebola for response costs abroad in their estimations. Additionally, their study used broad-scale predictive modeling to determine the costs of Ebola sequelae, the cost of death of healthcare workers on non-EVD illnesses, and long-term social factors (death of both parents, food insecurity, education) - calculations I omitted due to a lack of long-term validated data on these circumstances and their relevance to the U.S. The World Bank’s reported cost of the outbreak on the three West African nations was $2.8 billion ($600 million for Guinea, $300 million for Liberia and $1.9 billion for Sierra Leone) although a significant part of these results is declines in economic growth, investment, production and consumption as well as a severe drop in commodity prices[10].
The findings appear at odds with other single-case cost estimates for existing infectious diseases (as opposed to newly-emerging infectious diseases). The average cost of a single measles case was estimated at $369-$451 [35], although the study does not include loss of productivity. An outbreak of malaria among children in Ghana, Tanzania, and Kenya ranged from $6 to $334 per patient [36] (in 2014 USD). The average cost per person with cholera in the WHO African region is a reported as $771 (discounted to 2014 USD) [37]. The drastic differences in costs could be explained by the location of the studies (African nations versus the United States) and the well-documented scientific literature around the treatment processes of these diseases, including vaccinations or effective medication. Additionally, I believe investments to treat these diseases may have been incorporated within national public health policies to develop the entire healthcare system and thus are not reflected in these calculations. Additionally, most disease impact accounting to date has focused solely on direct medical costs, rather than the wider societal impacts incurred that our study incorporated via indirect costs.
The results are also inconsistent with several cost estimates for other recent emerging infectious diseases, namely H1N1, Zika and dengue fever. A study determined H1N1 cost China roughly $3.84 billion [38], but their findings include investments in the educational system, self-medication expenses and medical expenses for non-hospitalized self-diagnosed patients. Adjusting for the calculations not included in our own study, the total amounts to $875 million for 128,000 confirmed cases, or roughly $6,836 per case. In Mexico, the World Bank calculated the Zika epidemic cost roughly $744 million for approximately 60,000 cases [39], including $80 million in foregone income from reductions economic growth, or roughly $12,400 per confirmed case. A study on the economic burden of dengue fever in Colombia, Vietnam and Thailand determined the cost per case ranged from $141 to $385 for inpatient and $40 to $158 for outpatient [40]. Different income per capita leading to drastic differences in loss of productivity estimates, severity of the diseases and differing levels of investment in healthcare prior to the outbreaks could potentially explain the high discrepancies with our findings. However, our findings match trends seen with Severe Acute Respiratory Disease (approximately $30-45 billion for ~9,000 cases globally).
In general, this study aims to approximate conservative costs of EVD in the United States. The total costs appear insignificant when placed within the broader national context ($880 million would only be 0.025% of the federal U.S. government spending on healthcare in 2017 [41]). However, the disproportionate cost-per-case when contrasted to other recent outbreaks globally suggests two hypotheses. Firstly, that both the American government and people reacted disproportionately to the threat of an EVD epidemic. It is difficult to determine whether the federal response was excessive, as the threat was averted successfully and comparisons with previous case studies would require significant data and resources. Furthermore, it is likely that some investments into specialized equipment will have trickle-down benefits into research and development, rather than solely ad-hoc and limited-term utility, and will reduce costs of response to future potential outbreaks (however, certain resources, such as stockpiled PPE, may have a short window of use or not be allocated for optimal preparedness for future). Lastly, certain benefits extracted from such costs (e.g. training, experience) are unquantifiable yet may have long-lasting impacts.
The findings on indirect costs, including the magnitude of avoidance behaviors which are not routinely estimated for disease impacts, are remarkable and contributed significantly to overall costs. One could argue losses in productivity due to risk avoidance behaviors were disproportionately high (especially within the scope of our conservative estimates), or at least could have been substantially reduced through better management. I suspect the sensationalist media coverage [42,43] – including the strong presence of misleading information about the outbreak circulated on social media [44,45] – contributed to the promotion of reactionary, panic-fueled attitudes geared towards avoiding other people. More research on the psychology of graphic images and online news portrayal of disease risk on society is needed to better understand their role as cost drivers.
Secondly, there is a lack of a global integrated response to emerging infectious diseases that leads to high country-borne costs of preparation and response. The findings suggest the American health system was inadequately prepared to mitigate an emerging pandemic threat introduced into the U.S. from over 6,000 miles away and was constrained to invest in large-scale renovation projects in a short period of time. Better collaboration not only between governments but also between health sectors (e.g. human, animal and environmental health professionals) could perhaps have had an impact on reducing singular preparative costs related to initial emergence of the disease; similarly, preventive measures for reducing spread are needed for a suite of known and unknown emerging infections. To-date, efforts largely remain concentrated around reactionary practices taken after determination of a risk as opposed to identification and prevention occurring further up the process of transmission [5], as highlighted by the drafting of a Congressional budget after confirmation of a case on U.S. soil. The Global Health Security Agenda, which the U.S. is part of and has expanded investments in following the West Africa Ebola epidemic, recognizes the health and financial risks of emerging diseases and the benefits of stopping diseases at their source. Despite a complex global health system relying on formal and informal networks [4], recent outbreaks of Ebola, Zika, dengue, H1N1, and Middle East Respiratory Syndrome (MERS) and looming threat of anti- microbial resistance illustrate a necessity to act in a more synergetic fashion and to create better linkages between the various levels of government, the traditional health sector and its contemporary subsidiaries to mitigate economic impacts of disease events.
This study has several limitations. Due to a lack of primary data, literature and methodology, several key assumptions were made that may not fully capture the reality of costs of EVD for the United States. The composition of the contact tracing teams may be inaccurate - a lack of sufficient documentation did not allow for a more accurate estimate. Similarly, estimated wages were taken from the Bureau of Labor Statistics, but reflect a mean and may not be precise for the actual populations affected. Contact tracing was calculated for the three areas, but there may have been significantly more efforts around other parts of the country. The analysis assumes that the contact tracing staff was pulled away from their day-to-day activities to lead the tracing efforts - the opportunity cost of their absences was not factored into the calculations.
The direct costs were primarily extracted from existing literature. Whilst they encompass a significant portion of the costs, they remain estimates and it is likely other costs were omitted, such as national and state public health system alerts, rumor investigation, and possibly testing costs if additional suspected cases were screened. Treatment and indirect costs to hospitals were drawn directly from interviews. More data would have allowed for more precise and validated calculations. The loss of productivity and loss of workforce owing to the disease for indirect costs were extracted from pre-existing equations that I adapted to in this study – drafting my own equations may have been more representative of our sample of interest and the specific disease context for EVD. The behavioral avoidance cost calculations only display staying an additional 22 minutes at home for the entire duration of the local outbreak. They do not include the costs borne by the entertainment industry (such as avoiding going to the movies or restaurants), the public transportation companies, possible avoidance of healthcare treatment for other diseases as seen in West Africa due to concern of being infected with EVD, or the subsequent loss of productivity to companies from taking days off from work. Due to a lack of literature, the behavioral analysis is based on the American population’s behavioral reactions to the H1N1 virus - there is a strong possibility that people reacted significantly differently to EVD; the two are spread via different transmission routes (airborne vs. bodily fluids), with influenza being far more transmissible; however, lack of familiarity with Ebola and its depiction in the media may have resulted in disproportionate and irrational fear.
Conclusion
These findings demonstrate that the estimated costs of the 2015 Ebola virus introduction into the U.S. represent both medical and wider societal impacts. While I do not make a judgment on whether resources were applied effectively in the response to the 11 cases, this study provides a basis for further research into the costs and cost drivers of EVD for the United States. Additionally, it illustrates that even at a basic analytical level, disease outbreaks primarily occurring at a regional scale far from the country can have substantial global economic impact via our increasingly mobile societies. While drastic global health system reforms to ensure global preparedness are unlikely in the short-run, there may be opportunities to optimize resources and take stock of lessons learned from this event. In between epidemics, organizing cost-effective preparedness and mitigation techniques such as media sensitization may contribute to reduced potential for misinformation propagation through the media landscape. Similarly, studying the role of social media in promoting particular social attitudes is key to reducing indirect costs. Creating a disaster preparedness protocol incorporating various key actors within and around the medical sphere would likely help mitigate confusion around response and proactively create allies in the media with effective information dissemination. Although these solutions have limitations of their own and may require some level of upfront investment, it is essential to draw viable strategies to adapt to the rising threat of future epidemics. In the long-run, changes in the fundamental manner in which the public health and medical sectors operate will be necessary to reduce disease transmission and by extension, associated costs.
Acknowledgements
This research was supported by my supervisors Catherine Machalaba, Research Scientist, and Yasha Feferholtz, Economist, who have provided me the invaluable guidance for me to succeed in this academic and professional goal. I am also grateful to William Karesh, Executive Vice President for Health and Policy at EcoHealth Alliance, for giving me the opportunity and space to undertake this research. I must also thank my father, Franck Berthe, Senior Livestock Specialist in the Agriculture Global Practice of the World Bank, for his comments on earlier versions of the manuscript and his continuous support in this endeavor.
References
- Machalaba, C., et al., Climate Change and Health: Transcending Silos to Find Solutions. Ann Glob Health, 2015. 81(3): p. 445-58. [CrossRef]
- Machalaba, C., et al., One Health Economics to confront disease threats. Trans R Soc Trop Med Hyg, 2017. 111(6): p. 235-237. [CrossRef]
- Smith, K.M., et al., Infectious disease and economics: The case for considering multi-sectoral impacts. One Health, 2019. 7: p. 100080. [CrossRef]
- Bloom, D.E. and Cadarette, D., Infectious Disease Threats in the Twenty-First Century: Strengthening the Global Response. Front Immunol, 2019. 10: p. 549. [CrossRef]
- Sagner, M., et al., The P4 Health Spectrum - A Predictive, Preventive, Personalized and Participatory Continuum for Promoting Healthspan. Prog Cardiovasc Dis, 2017. 59(5): p. 506-521. [CrossRef]
- MaRS Discovery District, Current state: A reactive “sick” care system based on an episodic, acute care model, in Transforming Health Market Insights Series. 2019.
- World Health Organization. Ebola outbreak 2014-2016. Emergencies preparedness, response 2019.
- U.S. Department of State. The U.S. Government Response to the Ebola Outbreak. 2014.
- U.S. Department of Health and Human Services Office of the Assistant Secretary for Preparedness and Response, Regional Treatment Network for Ebola and Other Special Pathogens. 2017.
- World Bank Group, 2014-2015 West Africa Ebola Crisis: Impact Update. 2016. 1(1).
- Huber, C., Finelli, L., and Stevens, W., The Economic and Social Burden of the 2014 Ebola Outbreak in West Africa. J Infect Dis, 2018. 218(suppl_5): p. S698-S704. [CrossRef]
- Carias, C., et al., Resources needed for US CDC's support to the response to post-epidemic clusters of Ebola in West Africa, 2016. Infect Dis Poverty, 2018. 7(1): p. 113. [CrossRef]
- Smit, M.A., et al., Ebola Preparedness Resources for Acute-Care Hospitals in the United States: A Cross-Sectional Study of Costs, Benefits, and Challenges. [CrossRef]
- Herstein, J.J., et al., Initial Costs of Ebola Treatment Centers in the United States, in Emerg Infect Dis. 2016. p. 350-2. [CrossRef]
- Rosado, R.M., Charles-Smith, L., and Daniel, D., Control and Cost-benefit Analysis of Fast Spreading Diseases: The case of Ebola, in Online J Public Health Inform. 2017. [CrossRef]
- Suijkerbuijk, A.W.M., et al., Ebola in the Netherlands, 2014-2015: costs of preparedness and response. Eur J Health Econ, 2018. 19(7): p. 935-943.
- Kirigia, J.M., et al., Indirect costs associated with deaths from the Ebola virus disease in West Africa. Infect Dis Poverty, 2015. 4: p. 45. [CrossRef]
- Olugasa, B.O., Oshinowo, O.Y., and Odigie, E.A., Preventive and social cost implications of Ebola Virus Disease (EVD) outbreak on selected organizations in Lagos state, Nigeria. Pan Afr Med J, 2015. 22 Suppl 1(Suppl 1): p. 20.
- Kates, J., The U.S. Response to Ebola: Status of the FY2015 Emergency Ebola Appropriation. 2015, Kaiser Fund Foundation.
- Sun, L.H., Cost to treat Ebola in the U.S.: $1.16 million for 2 patients, in Washington Post. 2014.
- Williams, K.B., The Friday Dive: The disease that costs hospitals $1,000 an hour, in Healthcare Dive. 2014: HD.
- Mirkovic, K., Rapid Containment of Ebola Using Contact Tracing Following an Imported Case of Ebola Virus Disease – Senegal, 2014. 2015, Center for Disease Control.
- World Health Organization, Implementation and management of contact tracing for Ebola virus disease, Center for Disease Control, Editor. 2015, WHO: WHO.
- United States Department of Labor - Bureau of Labor Statistics. Overview of BLS Wage Data by Area and Occupation. 2018.
- Tai-Seale, M., McGuire, T.G., and Zhang, W., Time allocation in primary care office visits. Health Serv Res, 2007. 42(5): p. 1871-94. [CrossRef]
- Weintraub, W.S., Cardiovascular Health Care Economics. Humana Press. p. XIII, 436.
- Dugan, A., One-Fifth of Americans Worry About Getting Ebola. 2014, Gallup. p. 1.
- McCarthy, J., Ebola Debuts on Americans' List of Top U.S. Problems, in Gallup. 2014.
- Center for Disease Control, CDC Estimates of 2009 H1N1 Influenza Cases, Hospitalizations and Deaths in the United States, in H1N1 flu - General Info. 2019.
- Swift, A. and Ander, S.. Zika Virus Not a Worry to Americans. Well-Being 2017.
- Bayham, J., et al., Measured voluntary avoidance behaviour during the 2009 A/H1N1 epidemic. Proc Biol Sci, 2015. 282(1818): p. 20150814. [CrossRef]
- World Health Organization. Frequently Asked Questions on Ebola virus disease. Diseases 2019.
- United States Census Bureau. Quick Facts. Population Data 2019.
- Bartsch, S., Gorham, K., and Lee, B., The cost of an Ebola case. Pathogens and global health, 2015. 109(1): p. 4-9.
- Carabin H, et al., The average cost of measles cases and adverse events following vaccination in industrialised countries. BMC Public Health, 2002. 2: p. 22. [CrossRef]
- Sicuri E, et al., The economic costs of malaria in children in three sub-Saharan countries: Ghana, Tanzania and Kenya. Malar J, 2013. 12(307). [CrossRef]
- Kirigia, J.M., et al., Economic burden of cholera in the WHO African region. BMC Int Health Hum Rights, 2009. 9(8): p. 8. [CrossRef]
- Xue, L., et al., Cost-Benefit Analysis for China’s Influenza A (H1N1) Prevention and Control., in A Comprehensive Evaluation on Emergency Response in China. 2019, Research Series on the Chinese Dream and China’s Development Path. p. 45-177.
- World Bank Group, The short-term economic costs of Zika in Latin America and the Caribbean (LCR). 2016, World Bank.
- Lee, J.S., et al., A multi-country study of the economic burden of dengue fever: Vietnam, Thailand, and Colombia. PLoS Negl Trop Dis, 2017. 11(10): p. e0006037. [CrossRef]
- Centers for Medicaid and Medicare Services, National Health Expenditures 2017 Highlights 2017, Centers for Medicaid and Medicare Services (CMS).
- Brooks, M. , Is Ebola the real ‘World War Z?’ (Spoiler alert: It’s not). Reuters, 2014.
- Caldwell, L.A., Senator: Ebola as serious as ISIS, in CNN. 2014: CNN.
- Goldberg, R., How the feds block Ebola cures. New York Post, 2014.
- Holan, A.D. and A. Sharockman, PolitiFact names its 2014 Lie of the Year, in PolitiFact. 2014.
Figure 1.
Mapping the Total Costs of EVD for the United States (in million $US).
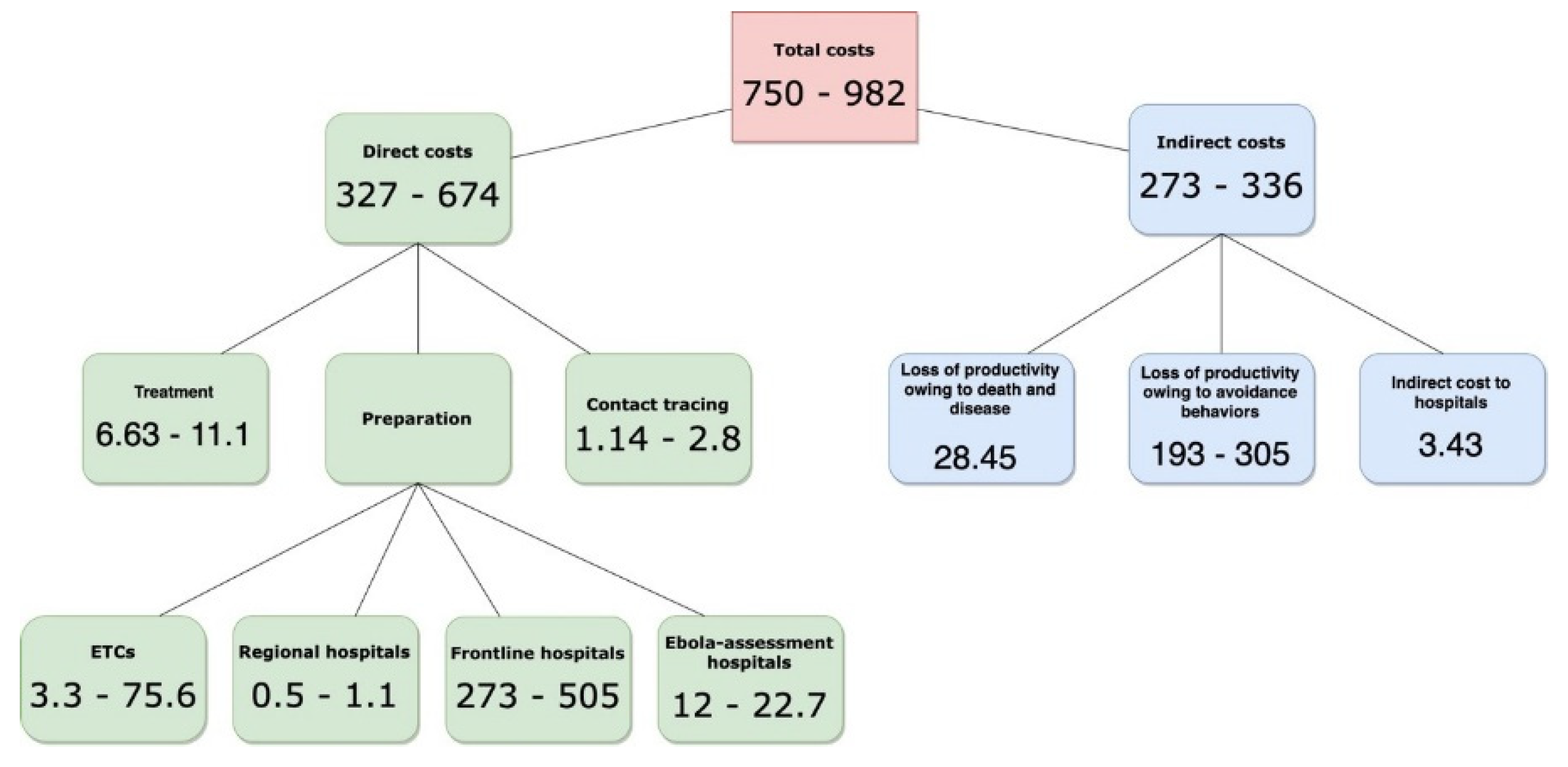
Table 1.
Contact-Tracing Teams Composition (members per team).
| Worker | New-York | Dallas | Cleveland |
| Health Social Workers | 6 | 9 | 8 |
| Nurses | 9 | 14 | 13 |
| Head epidemiologist | 1 | 1 | 1 |
| Field epidemiologist | 1 | 1 | 1 |
| Data entry keyer | 1 | 1 | 1 |
| Supervisors | 3 | 5 | 4 |
Table 2.
Contact-Tracing Team Hourly Wages (in $US).
| Worker | New-York | Cleveland | Dallas |
| Health Social Worker | 29.00 | 27.00 | 28.00 |
| Nurse | 40.00 | 35.00 | 35.00 |
| Head epidemiologist | 42.00 | 37.00 | 35.00 |
| Field epidemiologist | 42.00 | 37.00 | 35.00 |
| Data entry keyer | 17.00 | 16.00 | 15.00 |
| Supervisors | 40.00 | 35.00 | 35.00 |
Table 3.
Weintraub’s Equations and Legend Key.
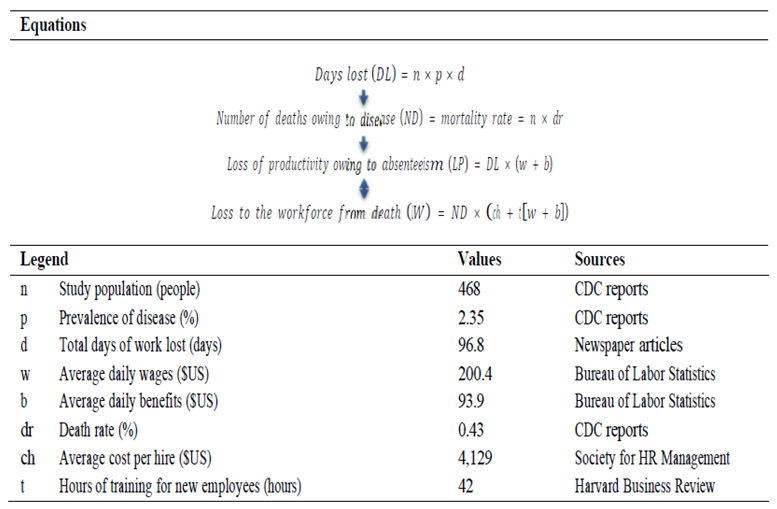 |
Table 5.
Summary Statistics of Direct Costs of EVD For the United States (in million $US).
| Type of cost | Mean | Low | High | % of direct cost |
| Preparation | ||||
| 63 Ebola Treatment Centers | 63 | 3.3 | 75.6 | 1.0 – 11 |
| 4845 frontline hospitals | 361 | 273.8 | 505.9 | 75 - 83 |
| 10 regional hospitals | 0.8 | 0.5 | 1.1 | 0.15 – 0.16 |
| 217 Ebola Assessment hospitals | 17.4 | 12.3 | 22.7 | 3.4 – 3.7 |
| Treatment | ||||
| Thomas Duncan | 0.32 | 0.24 | 0.4 | 0.05 – 0.07 |
| Nina Pham | 0.56 | 0.42 | 0.7 | 0.1 – 0.12 |
| Amber Vinson | 0.36 | 0.27 | 0.45 | 0.07 – 0.082 |
| Craig Spencer | 0.76 | 0.57 | 0.95 | 0.14 – 0.17 |
| Kent Brantly | 0.72 | 0.54 | 0.9 | 0.13 – 0.16 |
| Nancy Writebol | 0.72 | 0.54 | 0.9 | 0.13 – 0.16 |
| Rick Sacra | 0.84 | 0.63 | 1.05 | 0.16 – 0.19 |
| Ian Crozier | 1.40 | 1.05 | 1.75 | 0.25 – 0.32 |
| Ashoka Mukpo | 0.76 | 0.57 | 0.95 | 0.14 – 0.17 |
| Unknown patient | 1.20 | 0.9 | 1.50 | 0.22 – 0.27 |
| Martin Salia | 1.20 | 0.9 | 1.50 | 0.22 – 0.27 |
| Contact tracing | ||||
| New York City Area | 0.44 | 0.3 | 0.65 | 0.1 – 0.11 |
| Dallas Area | 0.74 | 0.44 | 1.12 | 0.13 – 0.16 |
| Cleveland Area | 0.64 | 0.40 | 1.03 | 0.12 – 0.15 |
| Repatriation | ||||
| 9 Americans | 45 | 30 | 55 | 8.2 – 9.2 |
| Total | 497.9 | 327.7 | 674.2 | 100 |
Table 7.
Summary Statistics of Indirect Costs of EVD for the United States (in million $US).
| Indirect cost variable, name | Cost | % of cost | |
| Loss of productivity for EVD patients | |||
| Loss of productivity owing to disease | 28.49 | 4.7 | |
| Loss of workforce owing to death | 1.07 | 0.17 | |
| Loss of productivity for population (in million $US) | Population (millions) | Cost over 65 days | % of cost |
| New York City | 8.5 | 84.36 | 43.6 |
| Dallas City | 7.1 | 65 | 21.2 |
| Cleveland City | 2.1 | 14.48 | 7.5 |
| Greater New York City | 17 | 167.96 | 55.1 |
| Greater Dallas | 11 | 79.9 | 26.2 |
| Greater Cleveland | 4 | 27.8 | 9.1 |
| Total metropolitan areas | 17.7 | 193.4 | 100 |
| Total greater areas | 32 | 305.26 | 100 |
Table 8.
The Indirect Costs of EVD for American Hospitals (in million $US).
| Indirect cost to hospitals | Number of patients | Number of days in hospital | Mean | % of cost |
| Texas Presbyterian Hospital | 1 | 8 | 0.14 | 4.1 |
| Bethesda National Institute of Health | 2 | 44 | 0.78 | 22.7 |
| Emory Hospital | 4 | 80 | 1.42 | 41.4 |
| Bellevue Hospital Center | 1 | 19 | 0.34 | 9.9 |
| Nebraska Medical Center | 3 | 42 | 0.75 | 21.9 |
| Total | 11 | 193 | 3.43 | 100 |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



