Submitted:
21 May 2023
Posted:
22 May 2023
You are already at the latest version
Abstract
Diabetes mellitus and dental caries (tooth decay) are not only common Non Communicable Diseases (NCDs) contributing to high burden of diseases but costly diseases to manage. Diabetes mellitus is a leading cause of mortality and reduced life expectancy across the globe. Early child hood dental caries (ECC) denotes a common chronic childhood disease and cariogenic dietary patterns dominated by refined sugar is one of the main causative factors. Thus, high burden of ECC could be a proxy indicator of excessive refined sugar consumption of a child. If such unhealthy dietary patterns are continued through to adolescent to adulthood, there is a high probability of an individual becoming a diabetic. Therefore, it is rational to argue high ECC burden in a country could be an indicator of future burden of diabetes. Moreover, ECC provides a critical period and a window of opportunity across life-course perspective, to intervene with cariogenic dietary patterns underpinned by common risk factor approach. This could be achieved by tailored dietary counseling for parental care givers of children with ECC. A healthy dietary pattern fostered in the childhood, most probably would continue to adulthood which may become beneficial in reducing the incidence of diabetes. Against this backdrop, we provide a perspective from Sri Lanka: a lower-middle-income country (LMIC) which records the highest prevalence of diabetes and pre-diabetes in south Asia. Our perspective will provide novel insights and innovative ideas into prevention and control of diabetes burden in LMICs, harnessing the potential of preventive dentistry.
Keywords:
Diabetes
; pre-diabetes
; early childhood dental caries
; refined sugar
; dietary counseling
; Sri Lanka
Introduction
Diabetes mellitus (DM) denotes a public health burden as the most common metabolic disease in the world. The global prevalence of diabetes among 20-79-year-olds in 2021 was estimated to be 10.5% (536.6 million people), increasing to 12.2% (783.2 million) in 2045 1. Middle income countries are expected to be more at risk, with the greatest relative increase in the prevalence between 2021 and 2045 (21.1%) compared to high (12.2%) and low-income (11.9%) countries. Global diabetes-related health expenditures is high, estimated at 966 billion USD in 2021, with the projected increase to reach 1,054 billion USD by 2045 1.
Sri Lanka as a LMIC carry a high burden of NCDs, which cause more than 75% of deaths and nearly 20% of premature deaths in the country, and DM is among top NCDS 2. Diabetes has reached epidemic proportions in low and middle income countries in South Asia attributed to a plethora of predisposing factors such as rapid urbanization, sedentary lifestyles, unhealthy dietary patterns and genetic predisposition 3. Moreover, South Asians are not only at an elevated risk of developing diabetes, but developing the disease at a younger age as well as developing diabetic complications dominated by cardiovascular, renal and eye complications 3. Previous research identified Sri Lanka as the country with the highest prevalence of diabetes in South Asia associated with urbanization and higher body mass index (BMI) as major contributory factors. Supporting this notion, a recent research based on a robust, national survey revealed 23% adult prevalence of diabetes in Sri Lanka in 2019, while the pre-diabetes prevalence was 30% thus recording significantly higher prevalence than previous estimates 4. Furthermore, as speculated by this ground breaking research, most of the increase in diabetes and pre-diabetes prevalence with BMI occurred among Sri Lankans with “normal weight” as classified by Asian cut offs stipulated by WHO 4. Sri Lanka as a LMIC, therefore, needs stringent policies and practices for preventing and controlling the diabetes burden,
Excessive free sugar intake is associated with an elevated risk of negative health consequences such as dental caries and nutritional problems among problems and an array of NCDs among adults including obesity, diabetes, cardiovascular diseases, several types of cancers and dental caries among adults 5,6. Early childhood dental caries (ECC) denotes a common chronic childhood disease with multifactorial aetiology, predominantly attributed to cariogenic dietary patterns dominated by refined sugars 7. Therefore, a high burden of ECC could be considered as a proxy indicator of excessive refined sugar consumption of a child. Thus, it could be rationally argued that if such unhealthy dietary patterns are continued, there is a high probability of child to become a diabetic adult. There is notably limited research linking dental caries with diabetes, despite both diseases share the common risk factor of high refined sugar consumption. However, a study conducted among 6-12-yer-old type 1 diabetic Saudi Arabian children revealed that there was no significant difference in dental caries prevalence in them compared to their non-diabetic counterpart 8. Nevertheless, caries risk assessments tests indicated higher caries risk among diabetic children compared to the non-diabetic children with regard to Lactobacillus counts and critical pH values (4.5-5.5) 8.
The Preventive Oral Health Unit (POHU) of National Dental Hospital (Teaching) Sri Lanka, which is one of the premier, multispecialty, tertiary care public dental hospital in the country offers a dynamic preventive oral health care model 9-14. This model incorporates life-course perspective and includes high caries risk toddlers, preschool children and diabetic patients and other target groups from socially disadvantaged and culturally diverse backgrounds, among its service recipients 9-14. Against this backdrop, we aim to provide a perspective from Sri Lanka which could provide innovative insights into tackling the future burden of diabetes via preventive oral health care approach.
Methods
In order to synthesize evidence for our perspective, we accessed the performance statistics of preventive dental clinic for 2022 and diabetic patient data base of POHU. We randomly selected data collection forms of 40 diabetic patients who received preventive oral health care from POHU in 2022. The data on age, gender, duration of having diabetes since diagnosis, fasting blood sugar (FBS) level of the most recent report and presence of comorbidities and diabetic complications were extracted from data collection forms. The data were entered and analysed using SPSS-21 statistical software package.
Results
The mean age of diabetic patients was 56.07 (95% CI) : 52.48-59.66 years, ranging from 29 to 79 years. Females dominated as 67.5%. The mean duration of being diagnosed with diabetes was 10.95 years with 95% CI of 8.97 to 12.92 years, ranging from 1 to 24 years. Most recent FBS levels demonstrated a skewed distribution with the median value of 126 mg/dl, ranging from 54.0 to 280.00 mg/dl.
Figure 1 shows prevalence of comorbidities and diabetic complications among 40 patients. Accordingly, hypertension was the most common co-morbidity followed by hypercholesterolaemia. Of diabetic complications, neuropathy, retinopathy and nephropathy were prominent.
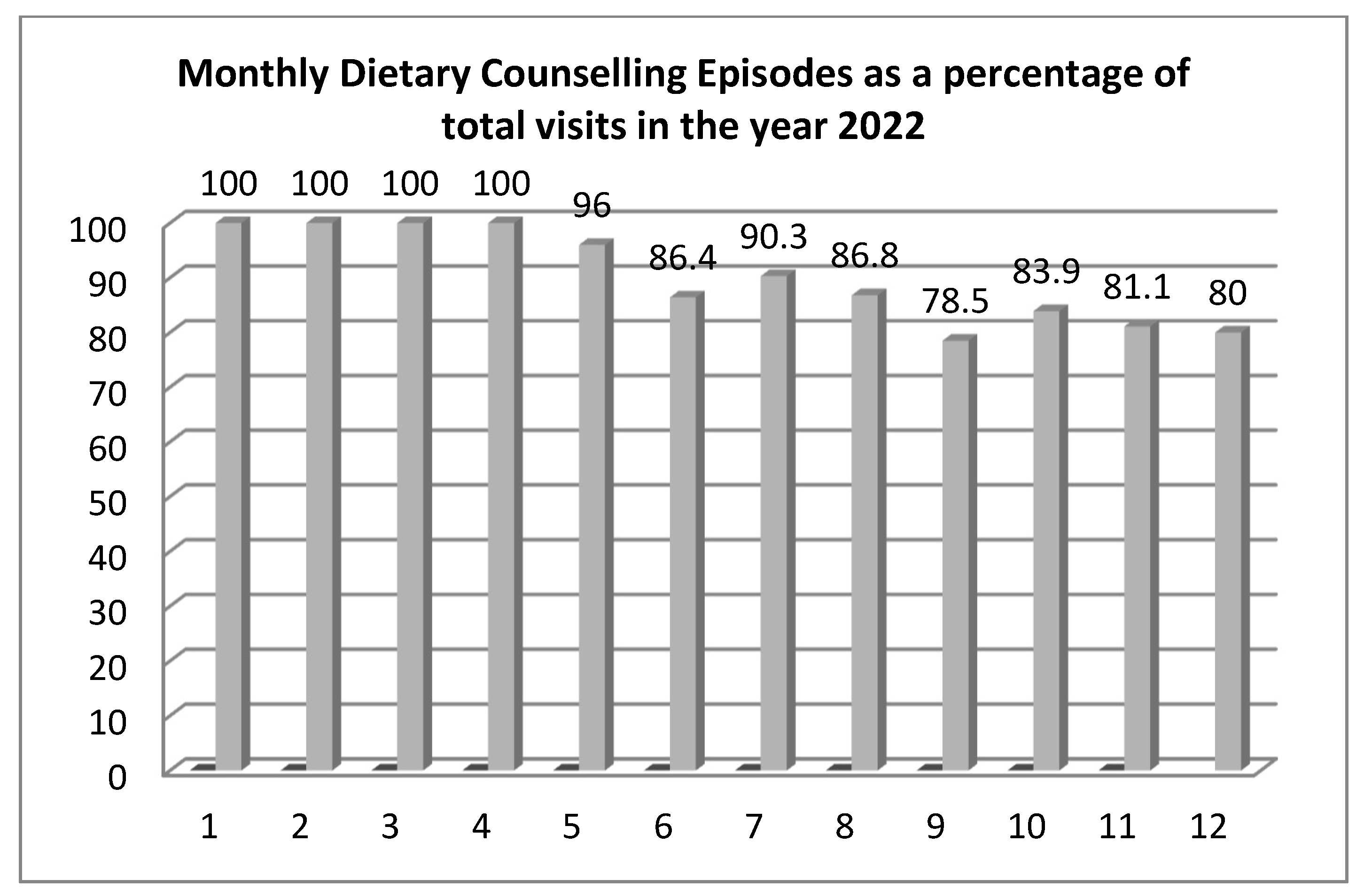
Figure 2, showcases monthly dietary counseling episodes performed in the year 2022, as a percentage of total visits. Findings reveals the high priority given for dietary counseling in managing ECC by preventive oral health care approach.
Discussion
Our rapid analysis of selected characteristics of diabetic patients received preventive oral health care painted the classical portrait of burden of diabetes in Sri Lanka which cause for concern. A two-fold increase in diabetes prevalence is evident in the country 4 compared to the estimated global prevalence 1. This becomes a major cause for concern and action. Female preponderance, occurrence of diabetes at younger ages, sub-optimal glycaemic control and presence of diabetic complications were evident from our data analysis. Those findings are in agreement with previous studies conducted among Sri Lankan diabetic patients 15. However, according to global diabetes prevalence estimates in 2021, men and women had a similar prevalence 1.
Sri Lanka is currently grappling with an unprecedented economic crisis impacting negatively on public health, availability and affordability of essential medicines and many other facets of health and well-being of people16. The negative impact is felt in public health care services to a greater extent funded by the government that offer free of charge services for all patients including diabetic patients 2. The direct and indirect costs of diabetic care are high across the globe 1. A study was conducted on economic cost of diabetic care in a rural district in Sri Lanka with high prevalence of diabetes 17. As revealed by the findings of that study, the monthly average economic cost amounted to US $87.93 per patient, of which the majority was born by family members of a diabetic patient 17. As this study was conducted prior to the economic crisis of the country it is reasonable to argue that economic cost of diabetes would be higher at present. Therefore, countries like Sri Lanka needs prioritization of reducing future burden of diabetes as a top economic and public health priority.
Preventive oral health care approach for managing ECC is underpinned by dietary counseling, oral hygiene improvements and professional use of topical fluorides 9-12. Our previous studies reported 68.2% of toddlers ≤ 3-years with ECC attended POHU, were practicing cariogenic dietary patterns which was significantly associated with their high burden of ECC 10. Similarly, preschool children attended POHU were practicing cariogenic dietary patterns underpinned by frequent consumption biscuits, buns, toffees and chocolates 11. Supporting our findings, a recent study conducted in the Colombo district of Sri Lanka revealed that among preschool children, free sugar consumption levels were extremely high 18. Moreover, the majority of children consumed more sugar than was recommended by the WHO limiting the sugar intake to less than 5% of total energy intake per day18. The daily median (IQR) free sugar intake of preschool children was estimated as 57.9 (33.2-95.8) grams/ day (approximately to 14.5 (8.3-23.9) teaspoons/day) or 21.1% (12.5-34.9%) of their daily energy requirements. Therefore, the current level was little over four-fold and 96% of children consumed higher percentage of energy from free sugar than recommended 18. Bakery products accounted for 27%, followed by biscuits (15%), and table sugar (15%) of daily sugar consumption of preschoolers. Further, increasing maternal education level significantly reduced sugar intake of preschool children, but diverse ethnicities, the habit of eating sugary food while returning from preschool or watching television and having school going siblings, significantly increased their refined sugar intake. Undoubtedly, this could be a plausible explanation for Sri Lanka to record highest prevalence of diabetes and pre-diabetes in South Asia 4. Based on their alarming findings, the authors warranted urgent action to curb excessive sugar intake among those preschool children 18 and a special quantitative food frequency questionnaire was developed and validated to ascertain free sugar intake of preschool children in Sri Lanka 19.
Therefore, supported by such compelling evidence on the timely need of intervening high sugar intake of Sri Lankan children, POHU offers an intervention package 9-12. Tailored, dietary counseling sessions are conducted to parental care givers of toddlers and children having a high burden of dental caries. Practical advice is given on cutting down food containing refined sugar from child’s diet. In each follow up visit, the improvements made by curtailing food items containing refined sugar, substituted by healthy versions are assessed. This practice is aimed at fostering healthy dietary habits among toddlers and children which is an essential prerequisite to control ECC. If a healthy dietary pattern could be established in the childhood and continued through to adolescence and adulthood, the risk of getting diabetes would be significantly reduced. Hence, as dental caries and diabetes share the common risk factor of refined sugar, ECC provides an opportunity to intervene to reduce the future burden of diabetes.
In the absence of prospective cohort studies with methodological rigour that explored the association between ECC and diabetes, further research is warranted. Ideally large-scale, population-based, prospective cohort studies are needed to explore the association between ECC and development of diabetes in adulthood, accounting to all potential confounding factors.
Conclusions
Preventive oral health care approach for ECC may provide novel insights into reducing the future burden of diabetes in LMICs like Sri Lanka. Nevertheless, further research and innovative actions are warranted in this regard.
References
- WH, Zhang P, Bommer C, Kuo S, Boyko EJ, Magliano DJ. IDF Diabetes Atlas: Global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2022 Jan;183:109119. [CrossRef]
- Rajapaksa L, De Silva P, Abeykoon A, Somatunga L, Sathasivam S, Perera S et al. Sri Lanka health system review. New Delhi: World Health Organization Regional Office for South-East Asia; 2021.
- 3. Arun Nanditha, Ronald C.W. Ma, Ambady Ramachandran, Chamukuttan Snehalatha, Juliana C.N. Chan, Kee Seng Chia, Jonathan E. Shaw, Paul Z. Zimmet; Diabetes in Asia and the Pacific: Implications for the Global Epidemic. Diabetes Care, 1 March. [CrossRef]
- Rannan-Eliya RP, Wijemunige N, Perera P, Kapuge Y, Gunawardana N, Sigera C, Jayatissa R, Herath HMM, Gamage A, Weerawardena N, Sivagnanam I, Dalpatadu S, Samarage S, Samarakoon U, Samaranayake N, Pullenayegam C, Perera B; SLHAS Collaborators. Prevalence of diabetes and pre-diabetes in Sri Lanka: a new global hotspot-estimates from the Sri Lanka Health and Ageing Survey 2018/2019. BMJ Open Diabetes Res Care. 2023 Feb;11(1):e003160. [CrossRef]
- Rippe JM, Angelopoulos TJ. Relationship between Added Sugars Consumption and Chronic Disease Risk Factors: Current Understanding. Nutrients. 2016 Nov 4;8(11):697. [CrossRef]
- Mututanthri, S. , Thoradeniya, T., Samaranayake, A. et al. Free sugar intake and associated factors among Sri Lankan preschool children. BMC Nutr 8, 137 (2022). [CrossRef]
- Folayan MO, El Tantawi M, Ramos-Gomez F, Sabbah W. Early childhood caries and its associations with sugar consumption, overweight and exclusive breastfeeding in low, middle and high-income countries: an ecological study. PeerJ. 2020 Oct 1;8:e9413. [CrossRef]
- Al-Badr AH, AlJameel AH, Halawany HS, Al-Jazairy YH, Alhadlaq MK, Al-Maflehi NS, Al-Sharif JA, Jacob V, Abraham N. Dental caries prevalence among Type 1 diabetes mellitus (T1DM) 6- to 12-year-old children in Riyadh, Kingdom of Saudi Arabia compared to non-diabetic children. Saudi Dent J. 2021 Jul;33(5):276-282. [CrossRef]
- Perera IR, Wickramaratne PWN, Liyanage NLP, Karunachandra KNN, Bollagala AD, et al. (2013) Preventive dental clinic solutions to tackle early childhood dental caries. International Conference on Public Health Innovations. National Institute of Health Sciences Sri Lanka.
- Surendra G, Perera I, Perera M, Herath C, Attanayake S. Presentation of Untreated Dental Caries for Preventive Oral Health Care and Socio-Behavioural Attributes of Toddlers Attended a Public Dental Hospital in Sri Lanka. Inter Ped Dent Open Acc J 6(3)- 2021. IPDOAJ.MS.ID.000237. [CrossRef]
- Karunachandra KNN, Bollagala AD, Perera IR, Liyanage NLP, Kottahachchi MJ, et al. (2013) Behavioural management strategies and oral health related behaviours of preschool children receiving preventive dental care. International Conference on Public Health Innovations. National Institute of Health Sciences Sri Lanka.
- Perera I, Herath C, Perera M, Dolamulla S, Jayasundara Bandara JM (2017) Service Delivery of a Preventive Oral Health Care Model to High Caries Risk Urban Children in Sri Lanka: A Retrospective, Descriptive Study. Journal of Advances in Medicine and Medical Research 20(3): 1-10. 26.
- Perera I, Siyambalapitiya S, Somasundaram N, Perera M. Screening for Oral Diseases among Diabetic Patients: The Unmet Need of Emerging Importance. Curre Res Diabetes & Obes J 2022; 16(1): 555929. [CrossRef]
- Thabrew D, Perera I, Dolamulla D, Baddage D, Perera M. Appraisal of an Oral Health Care Programme to Improve Oral Health Status of Diabetic Patients: Evidence from Sri Lanka. Curre Res Diabetes & Obes J 2022; 16(2): 555932. [CrossRef]
- Mettananda C, Chathuranga U, Rathnayaka T, Luke N, Meegodavidanage N.Glycaemic control and avenues for improvement among people with type 2 diabetes mellitus from rural Sri Lanka-a retrospective cohort study. The Lancet Regional Health South-East Asia. [CrossRef]
- Matthias AT, Jayasinghe S. Worsening economic crisis in Sri Lanka: impacts on health. Lancet Glob Health. 2022 Jul;10(7):e959. Epub 2022 May 12. PMID: 35569487; PMCID: PMC9098208. [CrossRef]
- Lebbe SMA, Rinosha KF. Economic cost of diabetes in Ampara District in Sri Lanka. Journal of Politics and Law 2018; 11(4): 147-152. [CrossRef]
- Mututanthri, S., Thoradeniya, T., & Harris, R. (2023). Development and validation of a quantitative food frequency questionnaire to assess free sugar intake among Sri Lankan preschool children. Journal of Nutritional Science, 12, E14. [CrossRef]
- Mututanthri, S., Thoradeniya, T., & Harris, R. (2023). Development and validation of a quantitative food frequency questionnaire to assess free sugar intake among Sri Lankan preschool children. Journal of Nutritional Science, 12, E14. [CrossRef]
Figure 1.
Prevalence of diabetic co-morbidities and complications.
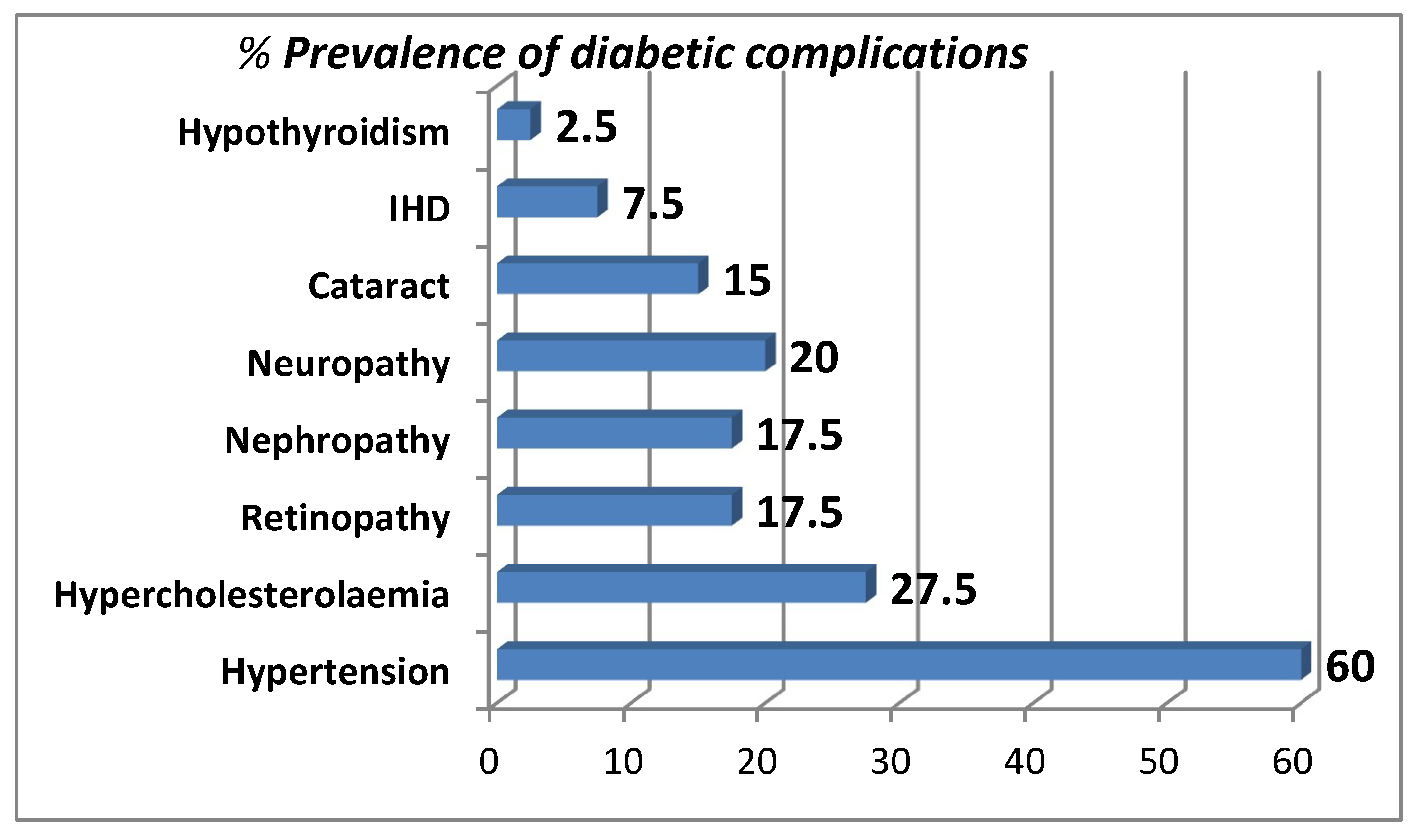
Figure 2.
Dietary counseling episodes as a percentage of total visits from January to December 2022.
Figure 2.
Dietary counseling episodes as a percentage of total visits from January to December 2022.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



