Submitted:
19 May 2023
Posted:
22 May 2023
You are already at the latest version
Abstract
We present a case of neglected atypical high grade prostatic stromal sarcoma (PSS) at the transitional zone , invading the peripheral zone, prostatic capsule & peri prostatic fat reaching to pelvic side wall, it showed T2WI hyperintense signal (compared to typical cases of PSS showing T2WI hypointense signal) corresponding to developing on top of pre-existing nodular hyperplasia.
Careful reviewing of prostatic central / transitional zone lesions is mandatory especially at T2WI, diffusion & contrast images to exclude malignancy which can be easily missed due to multiple signal patterns described. Most common tumors at transitional zone is stromal sarcoma which could be typical showing T2 hypointense signal or atypical showing T2 hyperintense signal intensity.
Keywords:
prostatic carcinoma
; MRI prostate
; MRI prostate stromal sarcoma
Figures:
Figure 1.
Axial T2WI at: A: upper part of the gland,, B &C: at mid part of the gland,, D: at lower part of the gland showing: -RT. lobe at both zones (TZ & PZ) [mainly at mid and lower parts of the gland] shows large area of heterogeneous mixed signals hypo & hyperintense signals suggesting hemorrhage as a post biopsy changes ( patient did biopsy in another hospital 3 weeks ago with no histopathology provided from that biopsy) . -LT. lobe at all parts of the gland (mainly mid & lower parts) shows large bi-zonal mass (mainly central zone) invading the left posterior part of the peripheral zone at mid gland (arrows at B) , prostatic capsule & regional peri prostatic fat (arrow at C), showing small numerous areas of cystic necrosis. Regional small L.Ns are also shown (double arrow heads at E image). -Note :peripheral zone showing hyperplastic nodule (arrow head at D image) which could explain the hyperintense signal of the tumor at T2WI as developing on top of benign hyperplastic nodules. ((Typical cases of TZ prostatic cancer appear at T2WI as a focal, homogeneous hypointensity against a background of the high-signal-intensity glandular tissue with ill-defined margins (“erased charcoal sign”), lenticular shape with no peripheral zone or capsule invasion. [12,13])) ((Atypical cases of TZ prostatic cancer appear at T2WI as a hypointense or slightly hyperintense lesion showing irregular margins . T2-hyperintense signal likely due to oedema or mucin or arising on top of benign prostatic hyperplastic nodules.[14,15,16] )).
Figure 1.
Axial T2WI at: A: upper part of the gland,, B &C: at mid part of the gland,, D: at lower part of the gland showing: -RT. lobe at both zones (TZ & PZ) [mainly at mid and lower parts of the gland] shows large area of heterogeneous mixed signals hypo & hyperintense signals suggesting hemorrhage as a post biopsy changes ( patient did biopsy in another hospital 3 weeks ago with no histopathology provided from that biopsy) . -LT. lobe at all parts of the gland (mainly mid & lower parts) shows large bi-zonal mass (mainly central zone) invading the left posterior part of the peripheral zone at mid gland (arrows at B) , prostatic capsule & regional peri prostatic fat (arrow at C), showing small numerous areas of cystic necrosis. Regional small L.Ns are also shown (double arrow heads at E image). -Note :peripheral zone showing hyperplastic nodule (arrow head at D image) which could explain the hyperintense signal of the tumor at T2WI as developing on top of benign hyperplastic nodules. ((Typical cases of TZ prostatic cancer appear at T2WI as a focal, homogeneous hypointensity against a background of the high-signal-intensity glandular tissue with ill-defined margins (“erased charcoal sign”), lenticular shape with no peripheral zone or capsule invasion. [12,13])) ((Atypical cases of TZ prostatic cancer appear at T2WI as a hypointense or slightly hyperintense lesion showing irregular margins . T2-hyperintense signal likely due to oedema or mucin or arising on top of benign prostatic hyperplastic nodules.[14,15,16] )).
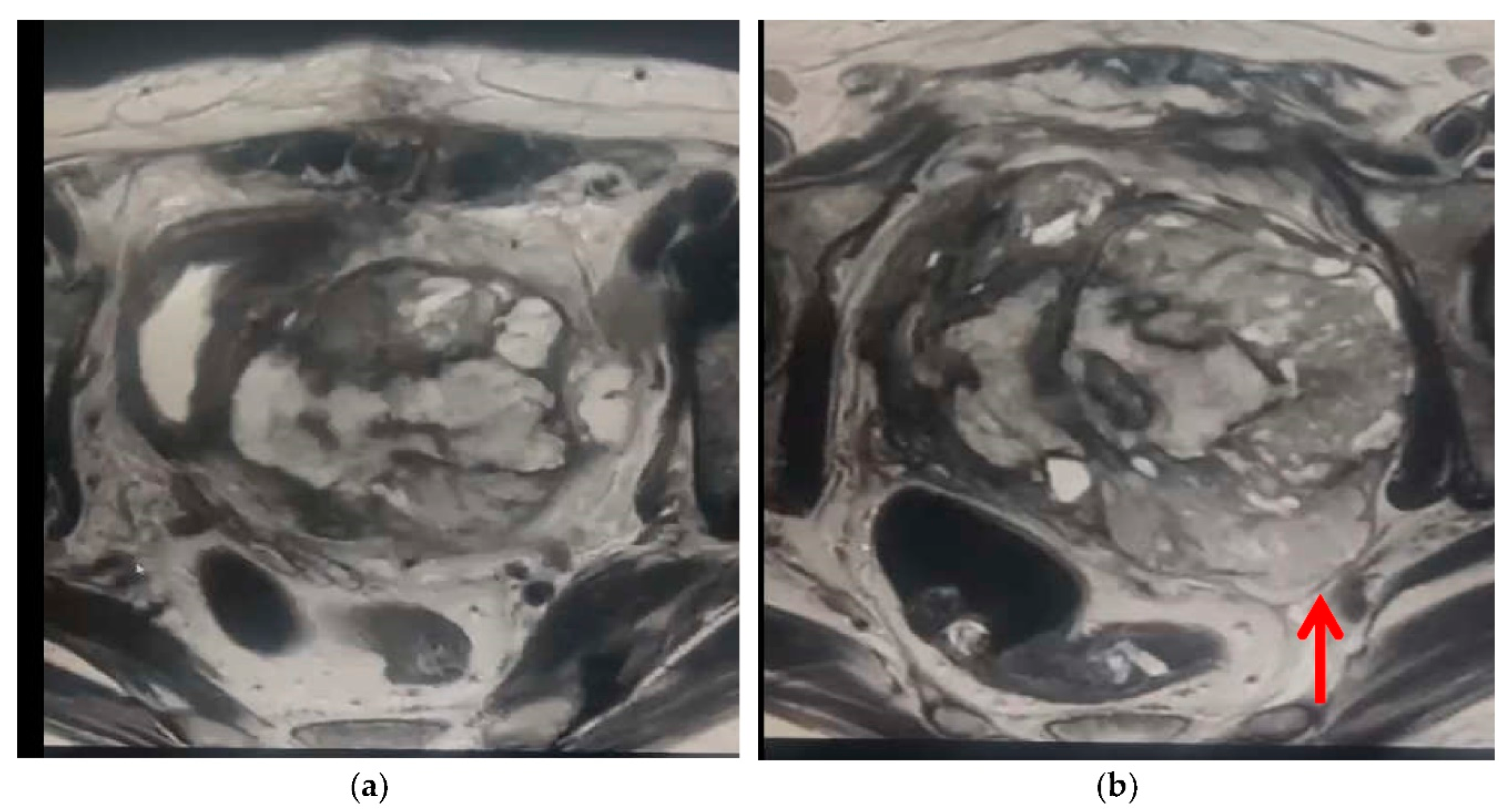
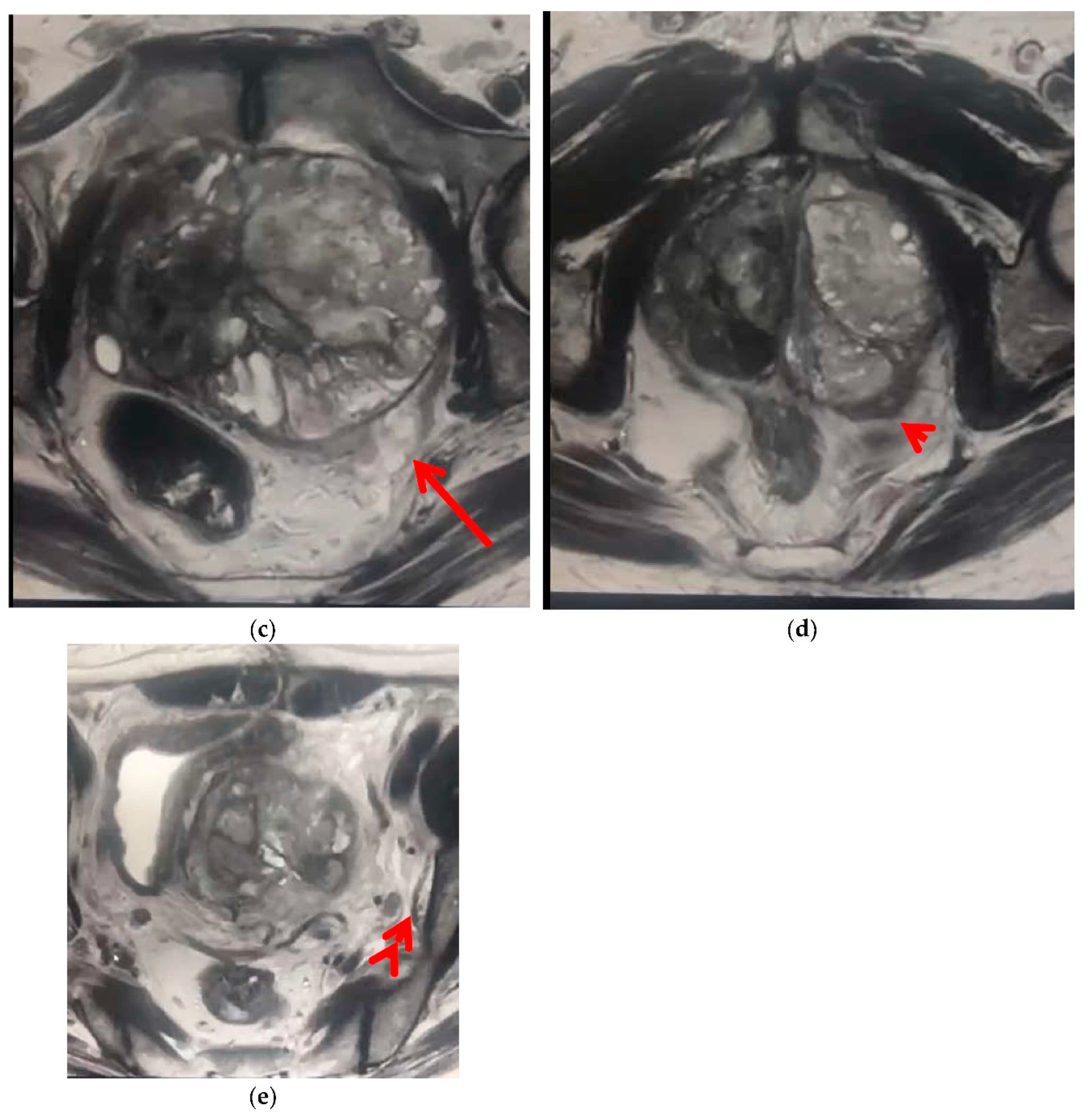
Figure 2.
Axial T1WI : A image at upper part of the gland, B:at mid part of the gland and C at lower part of the gland. RT.lobe: shows irregular area of mixed signals ( mainly hyperintense signal ) extending to central area …late sub acute & chronic hematoma of post biopsy changes. LT.lobe: showing Large central mass of hypointense signal ,extending to the LT. postero-lateral aspect of peripheral zone & peri-prostatic fat,, non separable from mesorectal fascia (arrow at C image). Preserved peri rectal fat.
Figure 2.
Axial T1WI : A image at upper part of the gland, B:at mid part of the gland and C at lower part of the gland. RT.lobe: shows irregular area of mixed signals ( mainly hyperintense signal ) extending to central area …late sub acute & chronic hematoma of post biopsy changes. LT.lobe: showing Large central mass of hypointense signal ,extending to the LT. postero-lateral aspect of peripheral zone & peri-prostatic fat,, non separable from mesorectal fascia (arrow at C image). Preserved peri rectal fat.
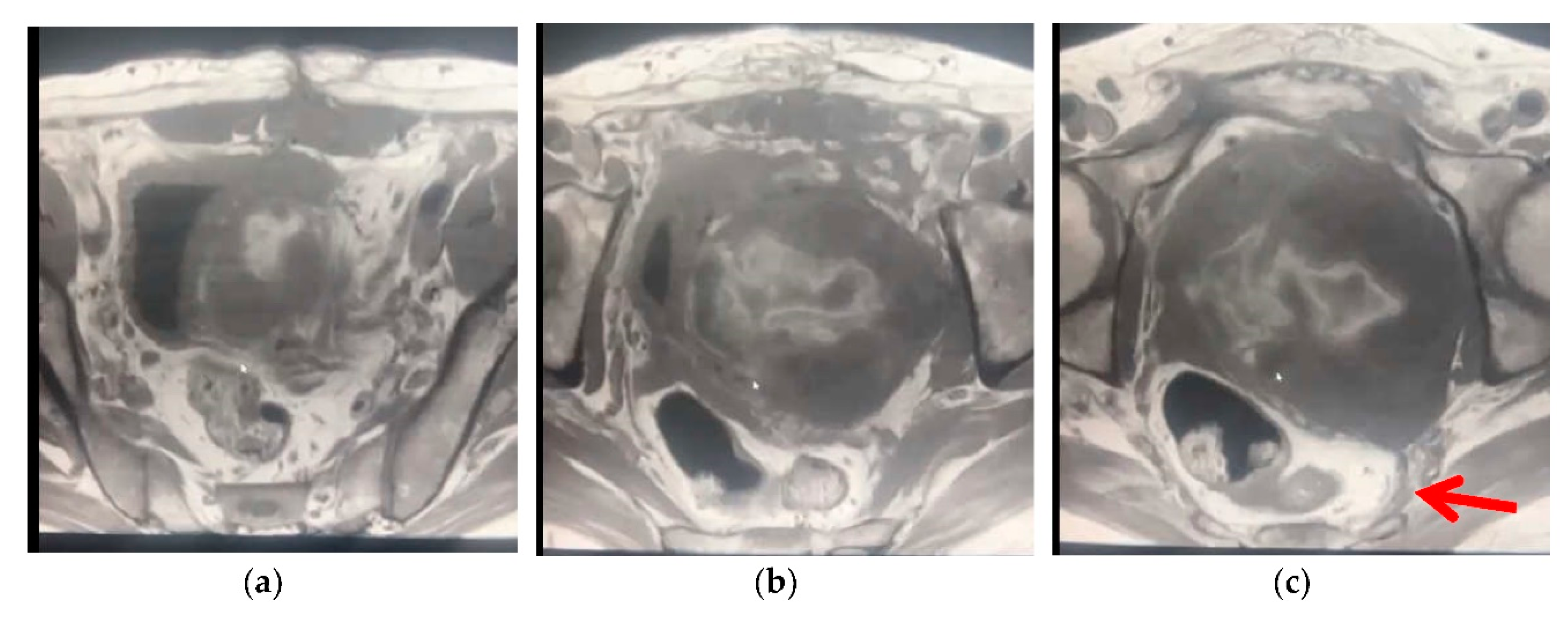
Figure 3.
Diffusion images:A & B: diffusion images at different levels at b 800,, C :ADC map. RT.side of the gland at the sites of old hematoma of post biopsy changes shows significant diffusion restriction: hyperintense signal at A & B images with hypointense signal at C. LT.side: A & B show hyperintense signal with mild hypointense signal at C…..mild diffusion restriction of the tumor at left side of the gland.
Figure 3.
Diffusion images:A & B: diffusion images at different levels at b 800,, C :ADC map. RT.side of the gland at the sites of old hematoma of post biopsy changes shows significant diffusion restriction: hyperintense signal at A & B images with hypointense signal at C. LT.side: A & B show hyperintense signal with mild hypointense signal at C…..mild diffusion restriction of the tumor at left side of the gland.
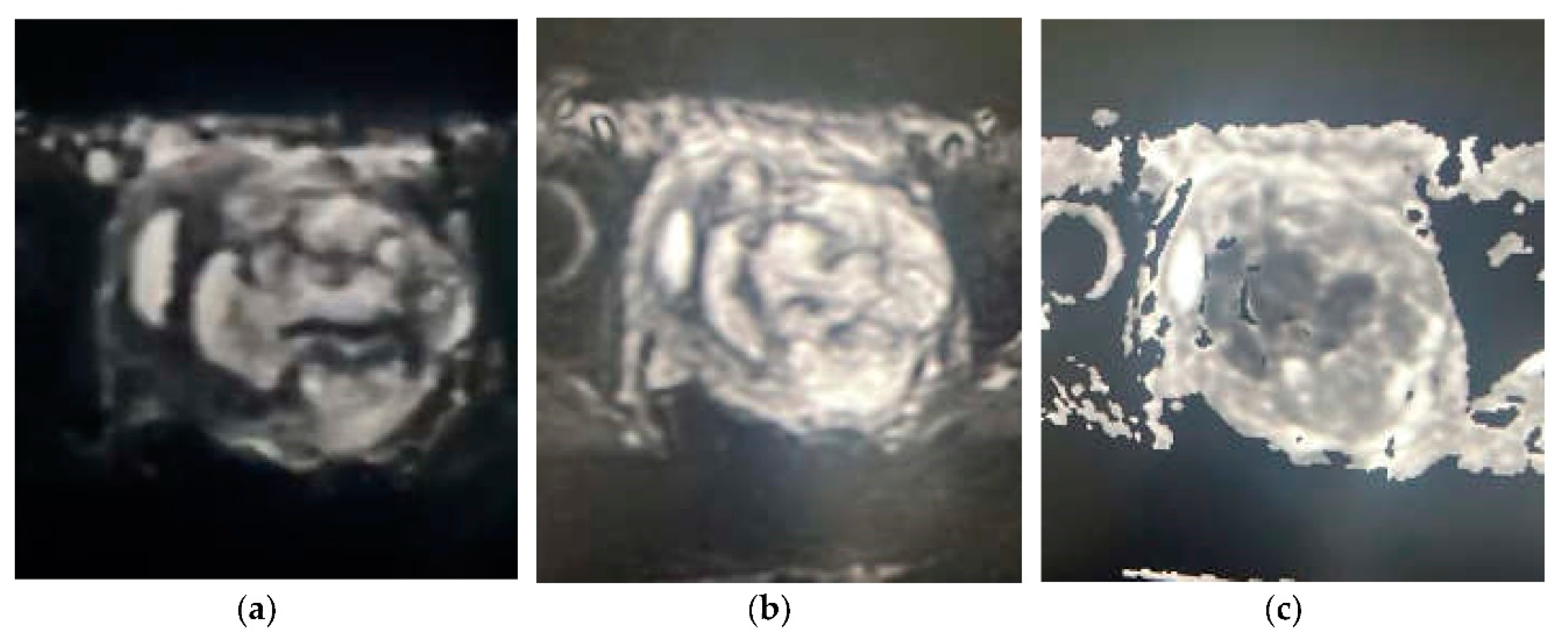
Figure 4.
post contrast T1WI fat sat images :A at upper gland, B&C at mid gland and D at lower gland. -RT.side of the gland: marginally enhancing area corresponding to post biopsy old hermatoma. LT.side of the gland: Shows large prostatic bi-zonal heterogeneous mass: mainly central zone , moderately enhancing, showing areas of no enhancement corresponding to cystic necrosis. Extension of the mass to the LT. posterolateral part of the peripheral zone ,prostatic capsule, periprostatic fat ,mesorectal fascia & postero- lateral pelvis wall , no rectal wall invasion arrow at C image.
Figure 4.
post contrast T1WI fat sat images :A at upper gland, B&C at mid gland and D at lower gland. -RT.side of the gland: marginally enhancing area corresponding to post biopsy old hermatoma. LT.side of the gland: Shows large prostatic bi-zonal heterogeneous mass: mainly central zone , moderately enhancing, showing areas of no enhancement corresponding to cystic necrosis. Extension of the mass to the LT. posterolateral part of the peripheral zone ,prostatic capsule, periprostatic fat ,mesorectal fascia & postero- lateral pelvis wall , no rectal wall invasion arrow at C image.
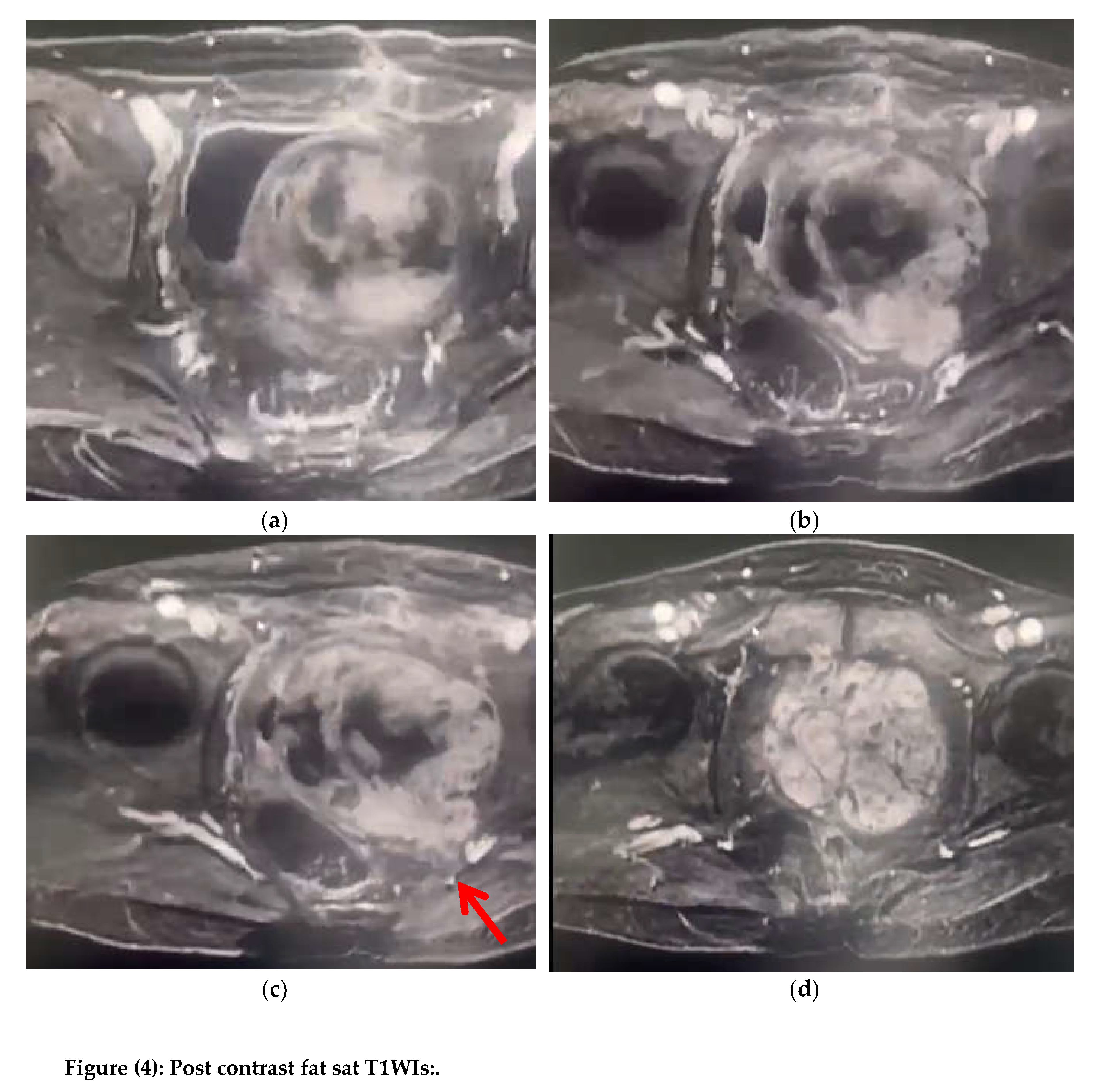
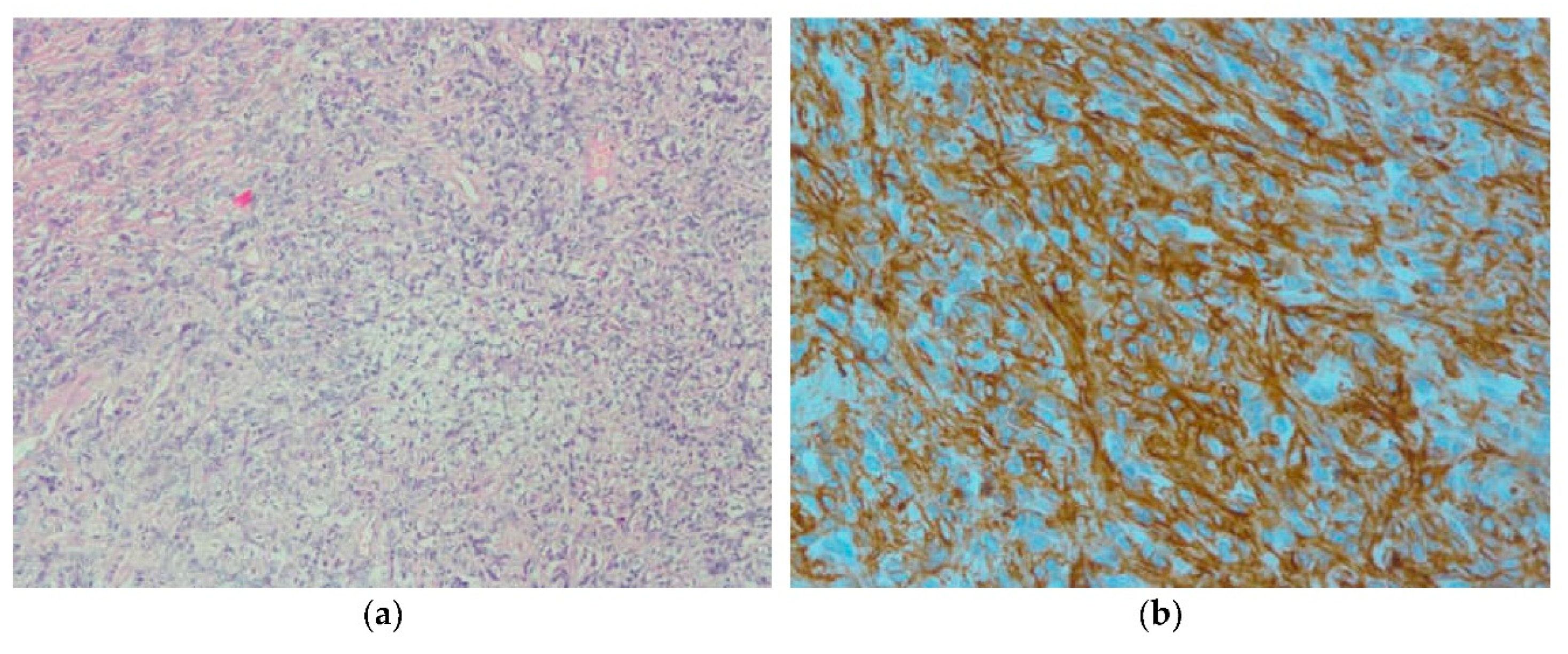
Figure 5.
Histopathology of the tumor: Hypercellular tumor with storiform pattern. B:The tumor cells are positive for CD34. ((solid hyper-cellular tumor with infiltrative margins composed of spindle to oval cells with mild to moderate nuclear atypia. Foci of necrosis and mitotic figures noted. The tumor cells are positive for CD34 and progesterone receptors while negative for PSA,SMA,Desmine,h-Caldesmon,ER,S-100, CK, AE1/AE3 ,EMA, CD31, Chromogranin, Synaptophysin,CD56,CD117,LCA and CD10 immunosatins)).
Figure 5.
Histopathology of the tumor: Hypercellular tumor with storiform pattern. B:The tumor cells are positive for CD34. ((solid hyper-cellular tumor with infiltrative margins composed of spindle to oval cells with mild to moderate nuclear atypia. Foci of necrosis and mitotic figures noted. The tumor cells are positive for CD34 and progesterone receptors while negative for PSA,SMA,Desmine,h-Caldesmon,ER,S-100, CK, AE1/AE3 ,EMA, CD31, Chromogranin, Synaptophysin,CD56,CD117,LCA and CD10 immunosatins)).
Author Contributions
All authors (J.A.M, KH A.A. & G.B.) have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Institutional Review Board Statement
Ethical review and approval were waived for this study, due to it is a retrospective case report, which did not impact the management of the patient.
Informed Consent Statement
Written informed consent has been obtained from the patient to publish this paper.
Conflicts of Interest
The authors declare no conflict of interest.
Abbreviations
PSS: prostatic stromal sarcoma. PSA: Prostatic specific antigen. PCa; prostatic cancer. CZ: Central zone. PZ: peripheral zone. TZ: transitional zone. KSA: Kingdom of Saudi Arabia.
References
- Jeremy Jones: prostatic sarcoma: Radiopaedia (2021). 20 Sep .
- Weiping Yang, MB, Ailian Liu, MD∗, Jingjun Wu, MMed, Miao Niu, MB: Prostatic stromal sarcoma A case report and literature review .Medicine (2018) 97:18(e0495).
- Hansel DE, Herawi M, Montgomery E, EpsteinJI. :Spindle cell lesions of the adult prostate. Pathol 2007; 20:148–158.
- Linda C. Chu, Hillary M. Ross,Tamara L. Lotan & Katarzyna J. Macura: Prostatic Stromal Neoplasms: Differential Diagnosis of Cystic and Solid Prostatic and Periprostatic Masses. AJR:200, June 2013 W571.
- Herawi M, Epstein JI. Specialized stromal tumors of the prostate: a clinic-pathologic study of 50 cases. Am J Surg Pathol 2006; 30:694–704.
- Andrea Molinari: Prostatic cancer, radiopaedia (2022) on 03 December.
- Rhiannon Van Loenhout, Frank Zijta, Robin Smithuis and Ivo Schoots: Prostatic cancer. . PI-RADS, version 2 .Radiology assistant.
- David Bonekamp, MD, PhD • Michael A. Jacobs, PhD • Riham El-Khouli, MD • Dan Stoianovici, PhD • Katarzyna J. Macura, MD, PhD: Advancements in MR Imaging of the Prostate: From Diagnosis to Interventions. Radiographics, (2011), May-Jume. Volume 31 Number 3.
- JINXING YU, MD, ANN S FULCHER, MD, SARAH G WINKS, MD, MARY A TURNER, MD, RYAN D CLAYTON, MD, MICHAEL BROOKS, MD and SEAN LI, MD: Diagnosis of typical and atypical transition zone prostate cancer and its mimics at multiparametric prostate MRI.BJR (2017),February.
- Haas GP, Sakr WA. Epidemiology of prostate cancer. CA Cancer J Clin 1997; 47: 273–87.
- Kitzing YX, Prando A, Varol C, Karczmar GS, Maclean F, Oto A. Benign conditions that mimic prostate carcinoma: MR imaging features with histopathologic correlation. Radiographics 2016; 36: 162–75.
- Akin O, Sala E, Moskowitz CS. Transition zone prostate cancers: features, detection, localization, and staging at endorectal MR imaging. Radiology 2006; 239: 784–92.
- American College of Radiology. MR prostate imaging reporting and data system version 2.0, 2015 [Cited 20 July 2015].
- Ren FY, Lu JP, Wang J, Ye JJ, Shao CW, Wang MJ. Adult prostate sarcoma: radiological-clinical correlation. Clin Radiol 2009; 64:171–177.
- Bittencourt LK, Barentsz JO, de Miranda LC, Gasparetto EL. Prostate MRI: diffusion weighted imaging at 1.5T correlates better with prostatectomy Gleason grades than TRUS-guided biopsies in peripheral zone tumours. Eur Radiol 2012; 22: 468–75. doi:.
- Li H, Sugimura K, Kaji Y. Conventional MRI capabilities in the diagnosis of prostate cancer in the transition zone. AJR Am J Roentgenol 2006; 186: 729–42.
- Quick CM, Gokden N, Sangoi AR, BrooksJD, McKenney JK. The distribution of PAX-2 Immune-reactivity in the prostate gland, seminal vesicle, and ejaculatory duct: comparison with prostatic adenocarcinoma and discussion of prostatic zonal embryogenesis. Hum Pathol 2010; 41: 1145–9.
- Herawi M, Epstein JI. Specialized stromal tumors of the prostate: a clinicopathologic study of 50 cases. Am J Surg Pathol 2006; 30:694–704.
- Hansel DE, Herawi M, Montgomery E, Epstein JI. Spindle cell lesions of the adult prostate. Mod Pathol 2007; 20:148–158.
- Gaudin PB, Rosai J, Epstein JI. Sarcomas and related proliferative lesions of specialized prostatic stroma: a clinicopathologic study of 22 cases. Am J Surg Pathol 1998; 22:148–162.
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



