
Submitted:
19 May 2023
Posted:
22 May 2023
You are already at the latest version
Abstract
The main purpose of tissue engineering is to fabricate and exploit engineered constructs suitable for the effective replacement of damaged tissues and organs, and able to perfectly integrate with the host’s organism without eliciting any adverse reaction. Ideally, autologous materials represent the best option, but they are often limited due to the low availability of compatible healthy tissues. So far, one therapeutic approach relies on the exploitation of synthetic materials: they exhibit good features in terms of impermeability, deformability and flexibility, but present chronic risks of infections and inflammations. Alternatively, biological materials, including naturally derived ones and acellular tissue matrices of human or animal origin, can be used to induce cells growth and differentiation, which are needed for tissue regeneration: however, this kind of materials lacks satisfactory mechanical resistance and reproducibility, affecting their clinical application.
In order to overcome the above-mentioned limitations, hybrid materials, which can be obtained by coupling synthetic polymers and biological materials, have been investigated with the aim to improve biological compatibility and mechanical features. Currently, the interest in these mate-rials is growing, but the ideal ones have not been found yet.
The present review aims at exploring some applications of hybrid materials, with particular mention to urological and cardiovascular fields: in the first case, the efforts to find a construct that can guarantee impermeability, mechanical resistance and patency will be herein illustrated; in the second case, the search for impermeability, hemocompatibility and adequate compliance will be been disclosed.
Keywords:
Biomaterials
; Hybrid Materials
; Tissue Engineering
; Regenerative Medicine
1. Introduction: the birth of tissue engineering and the challenging choice of adequate biomaterials
Tissue-engineering is becoming the answer to several clinical needs related to the restoration and replacement of injured tissues and organs. As formally established at a National Science Foundation workshop in 1998, tissue-engineering is “the application of principles and methods of engineering and life sciences toward the fundamental understanding of structure-function relationships in normal and pathological mammalian tissues and the development of biological substitutes to restore, maintain or improve tissue function” [1].
Consequently, the choice of the right biomaterial to use as a scaffold is of crucial importance. However, the term “biomaterial” did not receive a univocal definition: it changed over time starting from the indication of a material used for implantable devices, with the exception of drugs and soft biological tissues [2], to “a systematically, pharmacologically inert substance designed for implantation within or incorporation with a living system” [3]. In the last decades, a biomaterial was defined as “a substance (other than a drug) or combination of substances, synthetic or natural in origin, which can be used for any period of time, as a whole or as a part of a system which treats, augments, or replaces any tissue, organ, or function of the body” [4].
For tissue engineering purposes, the materials are fabricated with the aim to preserve the remaining normal tissue and to replace the diseased ones [5,6].
Therefore, the biocompatibility issue is of foremost importance in order to avoid (or at least minimize) adverse reactions after implantation: in this context, it is worthy to consider not only the “biological” compatibility, but also the overall functionality of the implantable system [7].
For these reasons, several types of biomaterials have been tested both unseeded and seeded with living cells in order to restore, maintain or enhance damaged or missing anatomical structures. From a general point of view, biomaterials for tissue-engineering can be divided into two classes: synthetic and biological. In turn, biological materials can be grouped into naturally derived ones and acellular tissue matrices.
Among a wide variety of synthetic materials, polymers such as polyglycolic acid (PGA), polylactic acid (PLA), poly-(lactic-co-glycolic) acid (PLGA), polycaprolactone (PCL), polyethylene glycol (PEG), polyvinyl alcohol (PVA) and polyurethane (PU) [8,9,10] have been tested. Major advantages of these materials are due to easy fabrication with tailored structural conformation and geometry, beyond the biodegradability rate that can be adjusted by controlling the chemical composition. Unfortunately, synthetic polymers often lack regeneration properties since they do not give cells the appropriate signals to adhere, migrate and differentiate.
Biological materials such as alginate, collagen, proteoglycans, chitosan, fibroin, agarose and gelatin, have been used to overcome these limitations [11,12,13]. In fact, natural polymers have the advantage of being biologically active and able to promote cell adhesion and growth. However, they possess weak mechanical properties, which are limited by fair reproducibility due to their inherent biological variability. Acellular matrices have been proposed as alternative types of biological materials. These matrices are produced by removing all cellular and nuclear components of the donor (which can be both human and animal), at the same time keeping the extra-cellular matrix (ECM) structure intact. The procedure for removing cellular and nuclear components is called “decellularization”: it aims at avoiding host immune response once the acellular matrices are implanted in vivo, and enhancing tissue regeneration by means of the natural growth factors that are normally present within the ECM. Moreover, appropriately decellularized matrices maintain the structural conformation and mechanical features of the original tissues, which are as much important for damaged tissue repair [14,15,16,17].
After implantation, acellular matrices provide an appropriate environment for cell adhesion and growth, and degrade over time being progressively replaced and remodeled by cells [5].
However, the main drawback of decellularized tissues is due to the high level of batch-to-batch variability, which greatly limits the repeatability of clinical outcomes.
To overcome the limitations of both synthetic and biological materials, and take advantage of their favorable features, a new approach was recently suggested, which combines biological tissues with synthetic polymers [18,19,20,21,22,23,24,25,26]. These new materials are usually termed “hybrid materials”: in the present review, the most important hybrid materials, and current applications thereof, are presented, with a specific focus on the urological and cardiovascular fields.
2. Moving toward a new concept of biocompatible materials: hybrid materials
Hybrid materials can be conveniently used in tissue engineering in order to repair and/or replace damaged or diseased tissues/organs using a combination of cells, growth factors and scaffolds.
While it is unknown where the definition of hybrid materials derived at first, organic and inorganic materials have been combined for thousands of years: for example, bright and colorful paints have been created by mixing colors with inorganic pigments. Moreover, hybrid membranes have been exploited in biotechnology for a long time, but only recently their distinctive physicochemical features have been investigated thanks to the introduction of sophisticated analytical instruments [27].
In the scientific literature, the concept of hybrid materials emerged in the 2000s, and the interest on their advantageous exploitation boosted over time. Figure 1 shows the increasing trend in the number of articles published from 2000 to 2023 concerning hybrid materials in regenerative medicine. The following words were used as keywords for searching PubMed and ScienceDirect databases: hybrid membrane, hybrid materials in tissue engineering and regenerative medicine. The words were included in articles title and abstract. Research has been performed on the PubMed and ScienceDirect databases between September 2022 and November 2022, with a total result of 28088 articles. Articles not matching the provided definition of hybrid materials and not related to urological and cardiovascular fields were excluded.
Hybrid materials can be considered a subgroup of composite materials: these latter are obtained by joining two or more constituent materials with different chemical or physical properties, which are somehow combined to get a new material with better features specifically oriented for a given application. Hybrid materials are composite materials, which are produced by coupling synthetic polymers with biological tissues. In this sense, they are “hybrid”: they merge the chemical and physical characteristics of both kinds of materials [28,29].
Combining the beneficial functionalities of each material to produce a construct with improved properties such as mechanical functionality, biocompatibility, and (bio)degradability [30], hybrid materials have the novel ability to exhibit special properties not found in any individual component. For this reason, recent efforts are addressing the idea to couple different materials in order to exploit the advantages of both by creating new constructs able to overcome the limitations of traditional materials. Table 1 summarizes the found studies published on hybrid materials and their clinical applications.
These novel materials can be made by combinations of organic-inorganic and organic-organic individual materials.
With regard to the hybrid materials based on coupling organic and inorganic components, only a selected number thereof can be correctly categorized as “hybrid”, fitting our criterion of having two or more different layers. For example, the hydroxyapatite/chitosan material was created by Zhang et al. in 2017 to regenerate bone tissue [31]. The aim of Zhang’s work was to design a biomimetic and bioactive scaffold in order to take advantage of the mechanical properties and osteoinductivity of hydroxyapatite combined with chitosan chemoattractant properties due to its structural similarity with bone glycosaminoglycans. When the product was tested in vitro, it appreciably stimulated both cell growth and mineral deposition. Hydroxyapatite was used in combination with fibroin for its excellent and intrinsic properties that are suitable in biotechnological and biomedical fields [53].
Ghosal et al. [34] used polycaprolactone/TiO2 electrospun fibers coated with collagen type I for skin tissue engineering. Nanofibers were obtained by electrospinning to get the scaffold, which was successively immersed in a collagen type I solution. The material was then dried in air and characterized from the physicochemical point of view. According to the study, biomaterials made of natural components, including collagen, demonstrated the capability to effectively coat synthetic biomaterials with nanofibers: collagen-coated nanofibers showed higher hydrophilicity than those without collagen; moreover, collagen can promote cell attachment and proliferation.
PCL has been extensively used for tissue engineering applications. In 2014, Cardoso et al. [33] proposed a new hybrid membrane based on chitosan and PCL. Vero cells were used to assess the cytocompatibility of a PCL mesh covered with chitosan. The results showed that hybrid membranes obtained by coupling PCL with chitosan gave better outcomes than PCL used alone. Thus, chitosan not only guaranteed proper biodegradation rates but also exhibited the inherent ability to act as an antibacterial agent. Moreover, it promoted cell growth, allowing the creation of a 3D hybrid structure.
In 2009, Ananta et al. [22] produced a biodegradable hybrid scaffold for tissue repair, which was made of poly(lactic acid-co-caprolactone) (PLACL) in the internal layer, and two plastically-compressed hyperhydrated collagen gels on the external sides. Neonatal (foreskin) fibroblasts (NNFs) were seeded inside and on the top of the collagen gels to mimic one interstitial, one epithelial and one composite interstitial-epithelial tissue. After 7 days, the cells seeded within the scaffold proliferated, suggesting that the construct acted as a porous and interconnected network through which oxygen and nutrients can be efficiently supplied.
In the same year, Lawrence et al. [32] proposed a multilayered scaffold with the aim to mimic small intestinal submucosa (SIS) mechanical features: this scaffold achieved a huge interest for several tissue engineering applications due to its promising properties, but its clinical exploitation is still limited because of its heterogeneity and permeability to urea, which can cause inflammation in the surrounding tissues. To overcome these limitations, the authors created a hybrid material by sandwiching a PLGA film (to provide mechanical resistance) between two external porous chitosan matrices (to get biological activity). Fibroblasts and canine bladder SMCs growth was then evaluated in vitro for 7 days, showing promising results in terms of shape, viability and functionality. Unfortunately, in vivo tests were not performed to confirm these appealing results.
Hong et al. [54] offered an example of animal-derived tissues used in combination with synthetic materials. They created a solution using decellularized ECM from pig skin that was electrospun onto a surface, which they refer to as a “biohybrid membrane”. The same technique was used to deposit a poly(ester-urethane)urea (PEUU) solution concurrently. The two components were deposited separately using a two-nozzle system. A bonding with the biodegradable PEUU, which has good mechanical properties but limited cellular infiltration and tissue integration capacity, was used in combination with the decellularized ECM from porcine skin, which presents interesting biocompatibility and bioactivity, also ensuring rapid degradation rates. The electrospinning process has been thoroughly investigated as a way to create fibrous scaffolds on micrometric and submicrometric scales that are structurally similar to ECM. This study revealed that the created structure can demonstrate rapid cellular infiltration without any sign of inflammation.
Two examples of hybrid membranes developed for cardiovascular and urological applications by coupling a polycarbonate urethane with decellularized tissues, are reported in Figure 2.
The rationale for using hybrid materials that combine polymeric materials and biological tissues is explained in Figure 3: biocompatible polymeric materials are able to guarantee mechanical resistance and impermeability to the hybrid construct; after being properly decellularized, biological tissues can be repopulated with the patient’s own circulating cells.
The above-mentioned examples demonstrate the potential of hybrid materials, which are emerging in the field of regenerative medicine for a variety of different settings, including orthopedics (e.g., bone and cartilage regeneration), skin lesion repair, urological and cardiovascular surgeries. These two areas will be covered in more detail in the following paragraphs.
3. Urological applications of hybrid materials: from urological conduits to the regeneration of the urinary bladder
Next to the general characteristics needed to obtain the ideal scaffold for implantation (i.e., biocompatibility, biodegradability, non-immunogenicity, adequate blood supply and vascularization, cell growth promotion and mechanical features similar to those of native tissue), other important characteristics have to be achieved in the urological field. First, the impermeability of the hybrid construct has to be ensured since it has to function as a barrier against urine, which is toxic for the surrounding tissues. Secondly, depending on the tissue site (i.e., a conduit such as ureter or urethra, or a whole organ such as urinary bladder), adequate mechanical resistance has to be assured [55,56]. In the case of urinary conduits, the patency is crucial to prevent stenosis that can hamper urine transport with subsequent renal damage [57]. On the other hand, urinary bladder substitution needs a functional support for an adequate dynamic mechanical and chemical resistance during both filling and emptying phases. In fact, engineered bladders have to support urine storage at low pressures, keeping contractile properties to allow physiologic voiding; consequently, an appropriate compliant muscular wall reconstruction with a highly specialized urothelium has to be obtained [58]. The epithelium serves to protect the scaffold from urine toxicity, while the muscular wall has to provide the peristaltic activity for the physiologic urine transport. For these reasons, a complete and functional repopulation of all bladder components is required during bladder regeneration [59]: a rapid urothelial repopulation and differentiation are necessary to restore the impermeable barrier against urine and to limit its leakage, which can lead to inflammatory responses and graft shrinkage [60]. At the same time, blood vessel regeneration is required to provide oxygen and nutrients and to remove wastes and damaged cells. Moreover, it is essential to regenerate the smooth muscle layers to perform bladder compliance and contractility [59].
The necessity for both impermeability and adequate scaffold porosity to promote cell ingrowth, is really challenging [55]. However, the formation of a urothelial lining is not important only for the re-establishment of barrier function from urine [61], but also for the regeneration of all bladder wall components [62].
The best scaffold for urinary applications has been sought after using a variety of strategies, including both synthetic materials (e.g., poly(glycolic acid) and poly(lactic-glycolic acid [63,64,65,66,67]) and biological ones (e.g., naturally derived polymers such as silk [68,69], alginate [70] and collagen [71,72,73,74] or acellular tissue matrices such as small intestinal submucosa (SIS) [75,76,77,78,79,80,81,82], bladder acellular matrix (BAM) [83,84], amniotic membrane (AM) [85] and dermis [86,87]).
On one side, acellular matrices offer excellent trophic factors since they are naturally provided with a wide variety of growth factors, thereby stimulating tissue regeneration and growth [88,89]. Moreover, they prevent permeation from luminal to abdominal cavities and undergo biodegradation after implantation being remodeled by usual activity of cells [90]. However, these matrices cannot shelter a high density of SMCs [91]. On the other side, synthetic polymers can be fabricated reproducibly with customized mechanical features, degradation properties and porosity [92,93]. However, synthetic materials lack biological competence due to the absence of trophic factors and natural barrier function of luminal endothelium.
Unfortunately, the individual limitations of both types of materials impaired their applications in clinics. Consequently, researchers’ attention has been focusing on hybrid materials. Indeed, synthetic materials can provide reproducible and tailored mechanical properties while biological materials provide growth factors and cytokines to promote cell ingrowth and differentiation.
One of the first studies evaluating a hybrid graft for urological purposes was published in 2007, when Kanatani et at. [37] created two types of urethral substitutes by combining a copoly(L-lactide/ε-caprolactone) [P(LA/CL)] tube with a collagen type I sponge following two different approaches: the first substitute was waved in a vascular stent style (type 1) while the second was tailored for the urethral tube (type 2). In detail, the tubes of P(LA/CL) were dipped in a collagen solution and then lyophilized to create a P(LA/CL)-collagen scaffold. Afterwards, the grafts were implanted to replace 1.5 cm urethral defects in 28 male rabbits (14 for each group). The authors found that type 2 grafts demonstrated more encouraging results compared with type 1 ones: the fibers were more tightly knitted and eventual prolapsed fibers into the lumen would have degraded without dragging the remaining fibers. This study pinpointed not only the importance of biomaterial composition for urethral tissue regeneration, but also the significance of the fabrication technique.
Soon after, Eberli et al. [18] fabricated a hybrid scaffold by bonding bladder acellular matrix (BAM) to a thick layer of PGA with threaded collagen fiber stitches. They intended to accommodate a large number of cells on one side, while the other served as a barrier against urine. Thus, urothelial cells (UCs) were seeded onto the BAM side, while bladder smooth muscle cells (SMCs) were seeded on the PGA side. Recellularized scaffolds were then implanted in mice, comparing hybrid scaffolds to BAM and PGA alone (controls groups). The authors concluded that only the hybrid scaffolds could maintain the specific organization of a normal bladder tissue. Three distinct layers were revealed: urothelial layer, dense collagen layer, and thick muscle compartment, where SMCs had begun to align and form compact muscle bundles. On the contrary, it was demonstrated that seeded BAM alone allowed the attachment of both cell types, but a thick muscular compartment was absent; seeded PGA alone allowed both cell types attachment with the development of a smooth muscle layer, but with a less distinct interface between UCs and SMCs, with UCs deeply penetrating into the muscle layer. The authors concluded that hybrid scaffolds made of BAM coupled with PGA possess the ideal features for hollow organ replacement, recognizing the superiority of hybrid material in comparison with each individual component.
Similarly, in 2012 Horst et al. [19] developed a bilayered hybrid scaffold composed by BAM and PLGA, with the aim to support various cell types growth and to provide an effective barrier for urine. BAM was chosen to improve scaffold stability, to provide barrier function and to promote the attachment of UCs; PLGA was chosen for improving structural support to cellular infiltration. In particular, PLGA microfibers were electrospun directly onto the abluminal surface of BAM. The resulting hybrid scaffold provided good support for primary bladder SMCs growth, attachment and proliferation, which was less evident in the case of cells seeded on BAM alone, reaching conclusions similar to those presented by Eberli et al. In the work by Horst et al., 4 and 8 weeks after implantation in rats for bladder reconstruction after partial cystectomy, the regeneration of bladder tissue structures consisting of urothelium, smooth muscle and collagen rich layers infiltrated with host cells and micro vessels, was evident. Moreover, hybrid scaffolds were able to maintain normal bladder capacity, whereas BAM recipients showed a significant distension of the bladder, demonstrating how this hybrid scaffold can support bladder regeneration. Afterwards, the same authors [24] performed more specific studies on the hybrid material by investigating the role of scaffold porosity on tissue ingrowth using hybrid scaffolds produced through the direct electrospinning of polymer microfibers on the external side of BAM. They compared two types of scaffolds: single-spun (SS) PLGA and more porous co-spun (CS) PLGA, which were all seeded with SMCs and implanted in rats undergoing augmentation cystoplasty. They demonstrated that SMCs penetrated into deeper regions of the CS scaffolds as compared with the SS ones. Moreover, cell distribution throughout the CS sections was more homogeneous: this suggested how scaffold porosity of scaffold can support superior cell seeding and migration. Four weeks after implantation, tissue regeneration was observed with a multilayered composition, typical of the bladder wall, in both SS and CS scaffolds. SS scaffolds exhibited significant shrinkage, whereas CS ones maintained their size after 4 weeks. Furthermore, the same research group [41] proposed a hybrid microporous scaffold obtained by co-spinning non-water-soluble polyester urethane or PLGA and water-soluble PEG directly onto the external side of BAM and tested them in rat cystoplasty model. The authors applied an innovative technique to seed SMCs and let them infiltrate into the scaffolds by using a series of centrifuges. They found better results in terms of healing and smooth muscle and urothelial regeneration on polyester urethane scaffolds after 8 weeks from surgery. Whereas the regeneration in the PLGA group decreased during time, in the case of polyester urethane the regeneration significantly increased between week 4 and 8, demonstrating the superiority of polyester urethane for bladder reconstruction.
A different type of material was proposed in 2012: Geutjes et al. [39] tested a collagen-polymer conduit as urinary diversion in the porcine model. They created a conduit (12 cm in length and 15 mm in diameter) using bovine collagen type I coupled with Vypro II synthetic polymer mesh, which was then seeded with UCs in the lumen side. In this study, Vypro II mesh was used to reinforce the fragile and easily collapsible collagenic conduit. Unfortunately, the authors noticed that Vypro II mesh was not incorporated in the tissue because of its limited biocompatibility. Moreover, there was an evident hydroureter and a hydronephrotic kidney on the urostomy side in all animals. The authors also suggested the importance of seeding other cell types like SMCs to allow peristaltic movement and prevent hydronephrosis.
The same year, Basu et al. [40] reported the successful application of a PGA-shaped tube coated with PLGA, seeded with SMCs from porcine adipose and peripheral blood into a porcine cystectomy model. The authors established the superiority of seeded constructs compared to unseeded ones in terms of muscle regeneration.
The following year, Engelhardt et al. [38] realized a collagen-poly(lactic acid-co-ε-caprolactone) (PLAC) hybrid scaffold for bladder tissue regeneration. A sterilized PLAC mesh was placed on the top of a collagen layer and then covered with a second layer of collagen: it was exposed to plastic compression to remove water excess. Human bladder SMCs and UCs were cultured on and inside the collagen-PLAC hybrid scaffold in vitro for 14 days. Both cell types were able to proliferate in and on the construct, forming dense cell layers on the top after two weeks. Afterwards, seeded scaffolds were implanted subcutaneously in the backs of nude mice: in vivo, hybrid constructs showed a lower inflammatory reaction compared to PLAC meshes alone. Moreover, the first signs of degradation were visible after six months. The authors concluded that these hybrid scaffolds have the potential to regenerate the urinary bladder, as they showed efficient cell proliferation and appropriate mechanical properties.
Differently from other studies, in 2013 Franck et al. [23] compared several groups of silk scaffolds produced by the gel spinning process: they consisted of smooth, compact multi-laminates (group 1) or rough, porous lamellar-like sheets (group 2). Both groups were assessed alone or coated with collagen type I or fibronectin in order to evaluate attachment, proliferation and differentiation of SMCs, UCs, murine embryonic stem cells (ESCs), and induced pluripotent stem (iPS) cells. The best results were achieved in the case of fibronectin-coated group 2 scaffolds, which promoted the highest levels of SMCs and UCs attachment and growth and facilitated ESCs and iPS cells differentiation toward both urothelial and smooth muscle bladder-associated lineages. For this reason, the authors concluded that fibroin-coated group 2 scaffolds represent a promising scaffold for cell-seeded bladder tissue engineering.
In the same year, Ajalloueian et al. [35] proposed an innovative approach to reduce the preparation time of the constructs by introducing minced mucosal bladder tissue as part of a hybrid material consisting of PCL-knitted mesh integrated with 2 layers of collagen that was plastically compressed. Combining PCL mesh with collagen allowed improving the mechanical properties of collagen alone, while the use of minced tissue allowed reducing the time for cells preparation and expansion by directly placing minced tissue inside the plastically-compressed collagen. This innovative seeding method resulted in optimal proliferation of UCs and epithelial cells. However, the use of autologous minced mucosal bladder tissue remains limited to non-oncologic cases, impairing its application to a wider range of patients. The following year, the same research group [25] presented a hybrid electrospun PLGA-plastically compressed (PC) collagen scaffold for bladder mucosa expansion. In particular, the authors optimized the electrospinning process in order to increase pore size and scaffold porosity with the aim of supporting neovascularization and tissue ingrowth. The PLGA was placed between two collagen gels and the minced bladder mucosa was distributed on the top, or both on the top and inside, the construct prior to plastic compression. The scaffolds were then cultured for 4 weeks. Improved mechanical properties in comparison to PC collagen alone were assessed and the strength of the hybrid PLGA-PC collagen construct was comparable to human bladder tissue. Moreover, they were able to demonstrate that cells from minced tissue migrated, expanded and re-organized to a confluent cell layer on the top of the construct after 2 weeks and formed a multilayered urothelium after 4 weeks.
Another tissue source was evaluated in 2016 by Adamowicz et al. [20], who proposed a novel material obtained by coupling frozen human amniotic membrane with two-layered membranes prepared from electrospun poly-(L-lactide-co-E-caprolactone) (PLCL) on both external and internal sides. The constructs were then implanted in rats, which underwent hemi cystectomy and bladder augmentation. The authors demonstrated the effective regeneration of urothelium and smooth muscle, achieving the requirements for a normal bladder contraction and compliance. In fact, PLCL nanofibers formed an elastic three-dimensional frame, which assured the necessary strength, shape and protection of amniotic membrane, which alone lacks adequate mechanical resistance, but it guarantees a regeneration-enhancing effect.
In 2019, a new material based on the use of a copolymer (P) with gelatin (G) was investigated by comparing two versions of the hybrid material [42]: the first group (PG) with gelatin electrospun on the electrospun copolymer, and the second one (PGP) with gelatin sandwiched between two external layers of copolymer. PG exhibited increased hydrophilic properties in comparison to PGP and copolymer alone; however, it presented lower solution stability than PGP, which has good water-resistant features.
The following year, it was proposed another innovative graft obtained by coupling graphene with amniotic membrane in order to replace the neuronal network of tissue-engineered urinary bladder [21]. The bio-composite material was created with a sandwiched structure covering the stromal side of the amniotic membrane with two layers of graphene. Scaffolds were seeded with UCs and SMCs, showing a good organization on the graphene surface, significantly increasing the electrical conductivity of the material. Moreover, the electrical stimulation applied in vitro allowed improving SMCs growth and linear arrangement.
Recently, it was proposed a different application of decellularized porcine SIS (whose application in the urological field could be limited due to permeability [82]) in combination with two commercially available polycarbonate urethanes (i.e., Chronoflex AR and Chronoflex AR-LT) [43]. Both the proposed SIS-based hybrid membranes demonstrated promising features, suitable for the creation of a tissue-engineered urinary diversion: the presence of polymers in combination with the decellularized SIS enhanced the mechanical resistance, but also significantly increased MSCs growth in vitro compared to SIS and polymers alone.
4. Hybrid materials in the cardiovascular field: a challenge for material-blood interaction.
The materials used in the cardiovascular field are mainly exploited for heart valve and vessel replacements. Regarding valve replacement, either mechanical or biological valves are currently used in clinics, but both present several drawbacks. In particular, mechanical valves significantly impact on patient quality of life since they represent long-term risk factors due to thrombosis and thromboembolism [94], thus requiring lifelong anticoagulation therapy. Moreover, both durability and functionality of current bioprosthetic heart valves are limited by their calcification potential [95,96]. The rate of calcification is inversely related with the age of the patient at the time of implantation [97,98,99]. Additionally, commercially available bioprosthetic valves are chemically fixed with glutaraldehyde to stabilize the biological tissue and mask xenogeneic epitopes to prevent immune rejection, causing possible cytotoxic effects.
Autologous vessels (e.g., radial artery or saphenous vein) are the preferred conduits for grafting in vascular surgery, but their availability is limited due to their poor quality, and their withdrawal results in donor site morbidity [100,101]. Currently, synthetic grafts are used as a feasible alternative, but they are limited by low patency rates [102]. Thrombosis is the most frequent cause of vascular graft failure, which can be also associated with intimal hyperplasia: it develops around the anastomosis and can be due to a variety of factors, such as a mismatch in vessel compliance or in the diameter between the native and grafted vessels. After one year from vascular surgery, graft failure appears to be significantly influenced by atherosclerosis, which is mostly the result of the reaction of the immune system’s cells that cause the formation of atherosclerotic plaques [103,104,105].
The main issue in the use of any material of synthetic or chemically-fixed biological origins, is that they cannot perfectly integrate with the patient and they are not able to adapt to the patient’s somatic growth, lacking remodeling and regenerative properties: this prevents their application in the pediatric population [51]. Hence, the major challenge of tissue engineering in cardiovascular tissue repair is the development of a material that can overcome the drawbacks of currently available devices.
As previously mentioned, there are two approaches for the realization of cardiovascular constructs: the use of decellularized matrices [106,107,108,109], which has the advantage of preserving anatomical architecture [110] and growth factors, and the use of bioresorbable biopolymers [111,112,113,114]. Decellularized tissues frequently lack patency, are not impermeable, and lack appropriate mechanical strength, whereas resorbable biopolymers often exhibit a degradation rate that is too fast in comparison with the time needed for tissue regeneration.
Hybrid materials have been proposed to produce a construct with the required technical features and the correct physicochemical behavior [26,115,116]. In the light of the necessity to obtain a scaffold as much as close to the native tissue in terms of both mechanical and biological functionalities, researchers have been able to adapt conventional regenerative biomaterials to maintain biological stability or functional activity by combining tissue components with polymers [5,34].
As aforementioned, synthetic materials (e.g. polytetrafluoroethylene (PTFE)) are frequently utilized in cardiovascular tissue reconstruction, however they possess a high risk of graft failure due to their potential for early development of thrombosis and intimal hyperplasia [117,118,119].
Several approaches have been investigated in order to facilitate the deposition of cells to increase the thromboresistance of implanted grafts. To this purpose, the first attempt was the direct seeding of endothelial cells to promote the growth of an endothelial layer, which is the only perfectly hemocompatible surface. However, the cells have to be isolated from the patient’s vessels several weeks before surgery, increasing the time needed for the graft preparation and preventing the use of a ready-to-use graft [120].
In order to improve hemocompatibility [121], heparin is employed in several clinical treatments and sometimes it can be covalently bound to synthetic grafts, such as polyethylene terephthalate (PET); unfortunately, it can result in the risk of heparin-induced thrombocytopenia [122,123].
Alt et al. [44] and Herrmann et al. [45] added polymers like PLA and PDLLA (poly(DL-lactide)), which are known for their biocompatibility and their suitability as scaffolding materials able to promote cell growth and proliferation, with anticoagulants. These two polymers have been used to improve the interaction of synthetic grafts with surrounding tissues and blood, like polytetrafluoroethylene (PTFE) is able to do.
The combination of polymer degradation and anticoagulant reactivation effectively reduced the formation of thrombi on the material surface, which is the reason why Heise et al. [46] decided to continue the work.
Using the dip-coating technique, a PLA containing polyethylene glycol (PEG)-hirudin/iloprost combination was applied to PTFE [45]. Anticoagulants were used to prevent thrombus formation while PLA was chosen for its biocompatibility and biodegradability [44,45]. The grafts were implanted in a pig animal model: no blockage was found; the patency was 90% and it was observed a pseudo-neointima development within the explanted grafts.
While the aforementioned groups prepared materials for vascular grafts that fit the definition of hybrid material by coupling two synthetic components, in 2009 Heidenhain et al. [47] coated a cross-linked decellularized pig aorta with PDLLA, which also contained lepirudin as anticoagulant drug. Biological tissue was decellularized to reduce immunogenicity and the ECM of the final product was cross-linked to stabilize it and limit the ECM absorption protecting it against macrophages’ fast deterioration [124].
Moreover, instead of glutaraldehyde, the 10000-times less toxic fixative genepin was used, which has a proliferative capability 5000 times higher than glutaraldehyde [125]. PDLLA-lepirudin was used to coat the decellularized and fixed tissue using a dipping method. PDLLA was used for its biocompatibility, whereas lepirudin was chosen because it has been proven to successfully reduce the thrombogenicity of vascular prostheses in vitro [45]. The major weakness of the proposed approach is due to the rapid rate of polymer degradation, especially due to PDLLA breaking via hydrolytic digestion and non-enzymatic activities [126]. Following in vivo implantation in pigs, the luminal side of each graft did develop a pseudo intima producing stenosis, which may have been caused by the rapid PDLLA degradation.
Reid et al. [48] adopted a different approach: they combined a polymer with an ECM generated from decellularized tissues (i.e., bovine heart and aorta) to create a scaffold suitable for vascular tissue engineering. Minced decellularized tissue was dissolved in a PCL solution to produce an electrospun ECM/PCL scaffold. Nevertheless, the authors refer to this material as a hybrid material, even though it does not fit our definition, which calls for the existence of two distinct layers formed of two constituents. The polymer has been employed for its favorable chemical and physical qualities, whereas decellularized tissue has been used for its favorable physical and chemical ability to sustain cells [127,128]. According to the experimental evidence, the ECM/PCL scaffold provided cell adhesion qualities superior to the control (polymeric scaffold), and cell survival assays supported this observation. Regarding the material’s mechanical characteristics, the polymer makes the scaffold stiffer and more hydrophobic.
Heydarkhan-Hagvall et al. [36] used a strategy similar to that presented by Reid et al. to create a material combining synthetic and natural materials by hybridization or bio-hybridization. This group used the electrospinning technique with natural proteins to create fibrous scaffolds for various tissue engineering applications. This method is promising since it combines natural proteins with PCL. During the manufacturing process, PCL was added to a mixture of collagen and elastin to create the electrospun scaffold. Indeed, electrospinning has a great potential for the effective and affordable creation of 3D fibrous matrices, with a high surface area to volume ratio. When the electrospun scaffold was exposed to glutaraldehyde, it intermolecularly cross-linked, enabling cell culture; however, the cross-linking process significantly decreased the porosity.
Stamm et al. [49] made further efforts to find the ideal material in terms of increased integration with surrounding tissues but with a decreased potential for thrombogenesis. They were aware that decellularized tissues cannot be directly implanted in vivo since collagen fibers, which are exposed in the decellularized tissue, are highly thrombogenic and induce platelet adhesion and activation [129]. In order to improve the mechanical properties of such a construct, the research team decided to enzymatically decellularize pig aortic valves and saturate them with biodegradable poly(hydroxybutyrate) via a stepwise solvent exchange method. According to in vitro biocompatibility tests, human blood vessel cells were found to survive and thrive on matrix/polymer hybrid tissue. Matrix/polymer patches were implanted in rabbit to assess proinflammatory activity in vivo; the sheep model was used for the functional in vivo test. Tests on rabbits gave positive results and confirmed that the material does not lead to the formation of thrombi. However, less encouraging results were obtained in the larger animal model since discrete fibrinous deposits were found on the inflamed leaflets.
Grabow et al. [50] applied the same strategy by coating a decellularized plus lyophilized aortic valve with two biopolymers: poly(4-hydroxybutyrate) (P[4HB]) and poly(3-hydroxybutyrate-co4-hydroxybutyrate) (P[3HB-co4HB]). The selected polymers are bioresorbable, and the degradation product is a naturally occurring human metabolite found in heart, brain, and several other organs [130]. These materials possess excellent pliability and elasticity, that make them very good candidates for the use in soft tissue engineering. Actually, regarding other mechanical properties, the structure had a lower resistance compared to decellularized valves, and this was likely due to the lyophilization process, which involved microscopic shrinking effects that have been thought to impair the three-dimensional tissue architecture, changing the structural characteristics of the decellularized matrix. This effect was shown during the functional tests of heart valves as well: a large transvalvular pressure gradient was observed with an important regurgitation due to restricted leaflet motion and inadequate valve function caused by lyophilization-induced leaflet shrinking.
Jahnavi et al. [51] created a heart valve made of Bio-Hybrid scaffold: it was obtained by combining polymers with decellularized bovine pericardium. In detail, the scaffold was made by electrospinning decellularized pericardium and PCL-CH (polycaprolactone - chitosan) together. The combination of these polymers exploits the biocompatibility of decellularized tissue, which has weak mechanical features and quickly degrades, and the characteristics of polymeric nanofibers. The creation of hydrogen bonds between chitosan hydroxyl groups and the ester groups of PCL can be used to explain why PCL-CH adheres to ECM of decellularized bovine pericardium. Delamination was thus prevented. Dip-coating of biological tissues with biodegradable polymers revealed higher mechanical capabilities; however, the organic solvents used to dissolve the polymer disrupted the structural integrity of the ECM, thus the authors opted for the electrospinning process [49,50,131]. Cytocompatibility direct contact tests in vitro revealed an increased cell adhesion and proliferation on Bio-Hybrid materials without any lysis or alteration in cell morphology. Meanwhile, physicochemical analyses showed that the Bio-Hybrid scaffold possessed biomechanical properties similar to those of native valve leaflets, including contact angle, fiber diameter, and mechanical resistance (tensile strength, Young’s modulus, and burst strength). In addition, the scaffold demonstrated an increased capacity to absorb water compared with the decellularized pericardium. Minimum hemolysis was experienced, thus proving a sufficient hemocompatibility level.
Pericardium has been extensively used not only for heart valve reconstruction, but also for the creation of vessel grafts, and the internal chamber of circulatory support devices, as in the case of the CARMAT TAH, the Total Artificial Heart developed by Carpentier et al. [132]. In terms of both materials and automation, this TAH holds the distinction of being a real innovative device. Commercial bioprosthetic heart valves are used to control the blood flow and a hybrid membrane separates the blood compartments of the ventricular chambers from the actuation fluid. The membrane was obtained by combining a synthetic polymer with animal pericardium chemically treated with glutaraldehyde [52]. After fixation, pericardium was immersed in polyethylene glycol (PEG) to prevent solvent reaction with water. Finally, the pericardium was coupled with the polymer (Chronoflex AR, a polyurethane carbonate supplied by AdvanceSource Biomaterials, Wilmington, MA, US) using the solution casting technique. This invention aimed at producing a fully hemocompatible material with good mechanical and sealing properties. In the CARMAT TAH, blood-contacting surfaces showed good hemocompatibility without clot formation after being exposed to human blood in vitro. However, pericardium is fixed with glutaraldehyde, which has all the previously mentioned drawbacks.
Recently, Todesco et al. [133] decided to combine decellularized pericardium with polycarbonate urethanes (Chronoflex AR and Chronoflex ARLT, AdvanSource Biomaterials) to avoid the use of glutaraldehyde [26]. These two polymers are widely used in the biomedical field, particularly in cardiovascular applications, and their biocompatibility has already undergone extensive in vitro assessment [134].
The ability to stimulate thrombin production and activate platelets has been preliminarily tested in vitro and the results demonstrated that the proposed hybrid membrane possesses good blood compatibility.
A similar approach has been used by Mudigonda et al. [115], who functionalized a pericardial matrix with a layer of polymeric nanofibers to get the mechanical strength needed for implantation in the circulatory system also improving cell homing capacity. A PCL solution was electrospun onto a decellularized pericardial core mounted on a rotating mandrel. Subsequent analyses and characterization stated an appropriate mechanical strength, associated with biocompatibility and hemocompatibility of the material.
5. Conclusions
An increasing number of studies have already acknowledged the limitations of biological and synthetic materials, taken individually, for many biomedical applications. Thus, recent efforts have been focusing on the optimization of grafts’ properties, by combining synthetic and biological materials in order to exploit the strengths and to overcome the disadvantages of both.
Differently from composite materials, which are obtained by physical combination of two or more components, this review defined hybrid materials as those in which two distinct interfaces can be distinguished, providing unique properties compared with individual materials alone. Moreover, the main advantage of hybrid constructs with respect to composites consists in the possibility to provide distinct biological and mechanical properties on the different sides of the graft.
Hybrid materials can be specifically tailored addressing the desired properties, which can be optimized for each particular application by choosing the right combination of individual materials. In this way, mechanical properties and biocompatibility can be improved in comparison with the single components, making them suitable for a wider number of medical applications by enhancing tissue regeneration and promoting cell growth and tissue formation. However, the properties of hybrid materials can be more complex than those of each individual component making necessary further research and development to fully understand their potential applications.
Moreover, some limitations of this kind of materials cannot be neglected. First, it has to be stated the complexity of hybrid material realization, which is more complicated than that of individual components: indeed, more advanced processing techniques and materials science expertise are required. Secondly, the hybrid material has to be stable over time without degrading, reducing its effectiveness and increasing the risk of adverse reactions. A further issue can be associated with long realization times, implying that the product may not be immediately available for the clinical use. Therefore, it is necessary to find an appropriate storage to provide hybrid scaffolds off-the-shelf.
The present review illustrated recent advancements in realization and optimization of hybrid materials for tissue engineering applications, with particular regard to the urological and cardiovascular fields, also discussing their strengths and also their weaknesses. Certainly, further efforts have to be made in terms of material’s choice and fabrication techniques, but promising results are suggesting the potentiality of hybrid materials in future clinical applications.
Author Contributions
Conceptualization, M.C., M.T. and A.B.; literature search and data collection, M.C. and M.T.; manuscript writing, M.C., M.T.; review and editing, all authors; supervision, C.G.F, A.M., F.D.M. and A.B. All authors have read and agreed to the published version of the manuscript.
Funding
This research received no external funding.
Data Availability Statement
no new data were created.
Conflicts of Interest
The authors declare no conflict of interest.
References
- Tissue Engineering: Proceedings of a Workshop Held at Granlibakken, Lake Tahoe, California, February 26-29, 1988; Skalak, R., Fox, C.F., Eds.; UCLA symposia on molecular and cellular biology; Liss: New York, 1988; ISBN 978-0-8451-4706-1.
- Cohen, J. Biomaterials in Orthopedic Surgery. Am. J. Surg. 1967, 114, 31–41. [Google Scholar] [CrossRef] [PubMed]
- Park, J.B. Biomaterials Science and Engineering; Springer US: Boston, MA, 1984; ISBN 978-1-4612-9710-9. [Google Scholar]
- Bergmann, C.P.; Stumpf, A. Dental Ceramics: Microstructure, Properties and Degradation; Topics in Mining, Metallurgy and Materials Engineering; Springer: Berlin Heidelberg, 2013; ISBN 978-3-642-38223-9. [Google Scholar]
- Murphy, S.V.; Atala, A. Organ Engineering--Combining Stem Cells, Biomaterials, and Bioreactors to Produce Bioengineered Organs for Transplantation. BioEssays News Rev. Mol. Cell. Dev. Biol. 2013, 35, 163–172. [Google Scholar] [CrossRef]
- Suh, H. Tissue Restoration, Tissue Engineering and Regenerative Medicine. Yonsei Med. J. 2000, 41, 681. [Google Scholar] [CrossRef] [PubMed]
- Todros, S.; Todesco, M.; Bagno, A. Biomaterials and Their Biomedical Applications: From Replacement to Regeneration. Processes 2021, 9, 1949. [Google Scholar] [CrossRef]
- Place, E.S.; George, J.H.; Williams, C.K.; Stevens, M.M. Synthetic Polymer Scaffolds for Tissue Engineering. Chem. Soc. Rev. 2009, 38, 1139–1151. [Google Scholar] [CrossRef] [PubMed]
- Liu, S.; Qin, S.; He, M.; Zhou, D.; Qin, Q.; Wang, H. Current Applications of Poly(Lactic Acid) Composites in Tissue Engineering and Drug Delivery. Compos. Part B Eng. 2020, 199, 108238. [Google Scholar] [CrossRef]
- Reddy, M.S.B.; Ponnamma, D.; Choudhary, R.; Sadasivuni, K.K. A Comparative Review of Natural and Synthetic Biopolymer Composite Scaffolds. Polymers 2021, 13, 1105. [Google Scholar] [CrossRef]
- O’Brien, F.J. Biomaterials & Scaffolds for Tissue Engineering. Mater. Today 2011, 14, 88–95. [Google Scholar] [CrossRef]
- Nikolova, M.P.; Chavali, M.S. Recent Advances in Biomaterials for 3D Scaffolds: A Review. Bioact. Mater. 2019, 4, 271–292. [Google Scholar] [CrossRef]
- Gomez-Florit, M.; Pardo, A.; Domingues, R.M.A.; Graça, A.L.; Babo, P.S.; Reis, R.L.; Gomes, M.E. Natural-Based Hydrogels for Tissue Engineering Applications. Molecules 2020, 25, 5858. [Google Scholar] [CrossRef]
- Crapo, P.M.; Gilbert, T.W.; Badylak, S.F. An Overview of Tissue and Whole Organ Decellularization Processes. Biomaterials 2011, 32, 3233–3243. [Google Scholar] [CrossRef]
- Keane, T.J.; Swinehart, I.T.; Badylak, S.F. Methods of Tissue Decellularization Used for Preparation of Biologic Scaffolds and in Vivo Relevance. Methods San Diego Calif 2015, 84, 25–34. [Google Scholar] [CrossRef]
- Mendibil, U.; Ruiz-Hernandez, R.; Retegi-Carrion, S.; Garcia-Urquia, N.; Olalde-Graells, B.; Abarrategi, A. Tissue-Specific Decellularization Methods: Rationale and Strategies to Achieve Regenerative Compounds. Int. J. Mol. Sci. 2020, 21, E5447. [Google Scholar] [CrossRef]
- Rabbani, M.; Zakian, N.; Alimoradi, N. Contribution of Physical Methods in Decellularization of Animal Tissues. J. Med. Signals Sens. 2021, 11, 1–11. [Google Scholar] [CrossRef]
- Eberli, D.; Freitas Filho, L.; Atala, A.; Yoo, J.J. Composite Scaffolds for the Engineering of Hollow Organs and Tissues. Methods San Diego Calif 2009, 47, 109–115. [Google Scholar] [CrossRef]
- Horst, M.; Madduri, S.; Milleret, V.; Sulser, T.; Gobet, R.; Eberli, D. A Bilayered Hybrid Microfibrous PLGA--Acellular Matrix Scaffold for Hollow Organ Tissue Engineering. Biomaterials 2013, 34, 1537–1545. [Google Scholar] [CrossRef]
- Adamowicz, J.; Pokrywczyńska, M.; Tworkiewicz, J.; Kowalczyk, T.; van Breda, S.V.; Tyloch, D.; Kloskowski, T.; Bodnar, M.; Skopinska-Wisniewska, J.; Marszałek, A.; et al. New Amniotic Membrane Based Biocomposite for Future Application in Reconstructive Urology. PLOS ONE 2016, 11, e0146012. [Google Scholar] [CrossRef]
- Adamowicz, J.; Pasternak, I.; Kloskowski, T.; Gniadek, M.; Van Breda, S.V.; Buhl, M.; Balcerczyk, D.; Gagat, M.; Grzanka, D.; Strupinski, W.; et al. Development of a Conductive Biocomposite Combining Graphene and Amniotic Membrane for Replacement of the Neuronal Network of Tissue-Engineered Urinary Bladder. Sci. Rep. 2020, 10, 5824. [Google Scholar] [CrossRef] [PubMed]
- Ananta, M.; Aulin, C.E.; Hilborn, J.; Aibibu, D.; Houis, S.; Brown, R.A.; Mudera, V. A Poly(Lactic Acid-Co-Caprolactone)–Collagen Hybrid for Tissue Engineering Applications. Tissue Eng. Part A 2009, 15, 1667–1675. [Google Scholar] [CrossRef]
- Franck, D.; Gil, E.S.; Adam, R.M.; Kaplan, D.L.; Chung, Y.G.; Estrada, C.R.; Mauney, J.R. Evaluation of Silk Biomaterials in Combination with Extracellular Matrix Coatings for Bladder Tissue Engineering with Primary and Pluripotent Cells. PloS One 2013, 8, e56237. [Google Scholar] [CrossRef]
- Horst, M.; Milleret, V.; Nötzli, S.; Madduri, S.; Sulser, T.; Gobet, R.; Eberli, D. Increased Porosity of Electrospun Hybrid Scaffolds Improved Bladder Tissue Regeneration: The Role of Scaffold Porosity on Tissue Ingrowth. J. Biomed. Mater. Res. A 2014, 102, 2116–2124. [Google Scholar] [CrossRef]
- Ajalloueian, F.; Zeiai, S.; Fossum, M.; Hilborn, J.G. Constructs of Electrospun PLGA, Compressed Collagen and Minced Urothelium for Minimally Manipulated Autologous Bladder Tissue Expansion. Biomaterials 2014, 35, 5741–5748. [Google Scholar] [CrossRef] [PubMed]
- Todesco, M.; Zardin, C.; Iop, L.; Palmosi, T.; Capaldo, P.; Romanato, F.; Gerosa, G.; Bagno, A. Hybrid Membranes for the Production of Blood Contacting Surfaces: Physicochemical, Structural and Biomechanical Characterization. Biomater. Res. 2021, 25, 26. [Google Scholar] [CrossRef] [PubMed]
- Hybrid Materials: Synthesis, Characterization, and Applications; Kickelbick, G. , Ed.; Wiley - VCH: Weinheim, 2007; ISBN 978-3-527-31299-3. [Google Scholar]
- Chowdhury, S.; Pal, B.; Datta, P. Composite Biomaterials for Bone Grafting and Other Biomedical Applications. In Encyclopedia of Materials: Plastics and Polymers; Elsevier, 2022; pp. 697–716 ISBN 978-0-12-823291-0.
- Knight, M.; Curliss, D. Composite Materials. In Encyclopedia of Physical Science and Technology; Elsevier, 2003; pp. 455–468 ISBN 978-0-12-227410-7.
- Coenen, A.M.J.; Bernaerts, K.V.; Harings, J.A.W.; Jockenhoevel, S.; Ghazanfari, S. Elastic Materials for Tissue Engineering Applications: Natural, Synthetic, and Hybrid Polymers. Acta Biomater. 2018, 79, 60–82. [Google Scholar] [CrossRef] [PubMed]
- Zhang, Y.; Venugopal, J.R.; El-Turki, A.; Ramakrishna, S.; Su, B.; Lim, C.T. Electrospun Biomimetic Nanocomposite Nanofibers of Hydroxyapatite/Chitosan for Bone Tissue Engineering. Biomaterials 2008, 29, 4314–4322. [Google Scholar] [CrossRef] [PubMed]
- Lawrence, B.J.; Maase, E.L.; Lin, H.; Madihally, S.V. Multilayer Composite Scaffolds with Mechanical Properties Similar to Small Intestinal Submucosa. J. Biomed. Mater. Res. A 2009, 88A, 634–643. [Google Scholar] [CrossRef]
- Cardoso, G.B.; Machado-Silva, A.B.; Sabino, M.; Santos Jr, A.R.; Zavaglia, C.A. Novel Hybrid Membrane of Chitosan/Poly (ε-Caprolactone) for Tissue Engineering. Biomatter 2014, 4, e29508. [Google Scholar] [CrossRef]
- Ghosal, K.; Thomas, S.; Kalarikkal, N.; Gnanamani, A. Collagen Coated Electrospun Polycaprolactone (PCL) with Titanium Dioxide (TiO2) from an Environmentally Benign Solvent: Preliminary Physico-Chemical Studies for Skin Substitute. J. Polym. Res. 2014, 21, 410. [Google Scholar] [CrossRef]
- Ajalloueian, F.; Zeiai, S.; Rojas, R.; Fossum, M.; Hilborn, J. One-Stage Tissue Engineering of Bladder Wall Patches for an Easy-to-Use Approach at the Surgical Table. Tissue Eng. Part C Methods 2013, 19, 688–696. [Google Scholar] [CrossRef]
- Heydarkhan-Hagvall, S.; Schenke-Layland, K.; Dhanasopon, A.P.; Rofail, F.; Smith, H.; Wu, B.M.; Shemin, R.; Beygui, R.E.; MacLellan, W.R. Three-Dimensional Electrospun ECM-Based Hybrid Scaffolds for Cardiovascular Tissue Engineering. Biomaterials 2008, 29, 2907–2914. [Google Scholar] [CrossRef]
- Kanatani, I.; Kanematsu, A.; Inatsugu, Y.; Imamura, M.; Negoro, H.; Ito, N.; Yamamoto, S.; Tabata, Y.; Ikada, Y.; Ogawa, O. Fabrication of an Optimal Urethral Graft Using Collagen-Sponge Tubes Reinforced with Copoly(L-Lactide/ε-Caprolactone) Fabric. Tissue Eng. 2007, 13, 2933–2940. [Google Scholar] [CrossRef]
- Engelhardt, E.-M.; Micol, L.A.; Houis, S.; Wurm, F.M.; Hilborn, J.; Hubbell, J.A.; Frey, P. A Collagen-Poly(Lactic Acid-Co-ɛ-Caprolactone) Hybrid Scaffold for Bladder Tissue Regeneration. Biomaterials 2011, 32, 3969–3976. [Google Scholar] [CrossRef] [PubMed]
- Geutjes, P.; Roelofs, L.; Hoogenkamp, H.; Walraven, M.; Kortmann, B.; de Gier, R.; Farag, F.; Tiemessen, D.; Sloff, M.; Oosterwijk, E.; et al. Tissue Engineered Tubular Construct for Urinary Diversion in a Preclinical Porcine Model. J. Urol. 2012, 188, 653–660. [Google Scholar] [CrossRef] [PubMed]
- Basu, J.; Jayo, M.J.; Ilagan, R.M.; Guthrie, K.I.; Sangha, N.; Genheimer, C.W.; Quinlan, S.F.; Payne, R.; Knight, T.; Rivera, E.; et al. Regeneration of Native-Like Neo-Urinary Tissue from Nonbladder Cell Sources. Tissue Eng. Part A 2012, 18, 1025–1034. [Google Scholar] [CrossRef] [PubMed]
- Horst, M.; Milleret, V.; Noetzli, S.; Gobet, R.; Sulser, T.; Eberli, D. Polyesterurethane and Acellular Matrix Based Hybrid Biomaterial for Bladder Engineering: HYBRID BIOMATERIAL FOR BLADDER ENGINEERING. J. Biomed. Mater. Res. B Appl. Biomater. 2017, 105, 658–667. [Google Scholar] [CrossRef] [PubMed]
- Azuraini, M.J.; Huong, K.-H.; Khalil, H.P.S.A.; Amirul, A.A. Fabrication and Characterization of P(3HB-Co-4HB)/Gelatine Biomimetic Nanofibrous Scaffold for Tissue Engineering Application. J. Polym. Res. 2019, 26, 257. [Google Scholar] [CrossRef]
- Casarin, M.; Todesco, M.; Sandrin, D.; Romanato, F.; Bagno, A.; Morlacco, A.; Dal Moro, F. A Novel Hybrid Membrane for Urinary Conduit Substitutes Based on Small Intestinal Submucosa Coupled with Two Synthetic Polymers. J. Funct. Biomater. 2022, 13, 222. [Google Scholar] [CrossRef]
- Alt, E.; Seliger, C. Antithrombotic Stent Coatings: Hirudin/Iloprost Combination. Semin. Interv. Cardiol. SIIC 1998, 3, 177–183. [Google Scholar]
- Herrmann, R.; Schmidmaier, G.; Märkl, B.; Resch, A.; Hähnel, I.; Stemberger, A.; Alt, E. Antithrombogenic Coating of Stents Using a Biodegradable Drug Delivery Technology. Thromb. Haemost. 1999, 82, 51–57. [Google Scholar] [CrossRef]
- Heise, M.; Schmidmaier, G.; Husmann, I.; Heidenhain, C.; Schmidt, J.; Neuhaus, P.; Settmacher, U. PEG-Hirudin/Iloprost Coating of Small Diameter EPTFE Grafts Effectively Prevents Pseudointima and Intimal Hyperplasia Development. Eur. J. Vasc. Endovasc. Surg. 2006, 32, 418–424. [Google Scholar] [CrossRef]
- Heidenhain, C.; Weichert, W.; Schmidmaier, G.; Wildemann, B.; Hein, M.; Neuhaus, P.; Heise, M. Polymer Coating of Porcine Decellularized and Cross-Linked Aortic Grafts. J. Biomed. Mater. Res. B Appl. Biomater. 2010. [Google Scholar] [CrossRef] [PubMed]
- Reid, J.A.; Callanan, A. Hybrid Cardiovascular Sourced Extracellular Matrix Scaffolds as Possible Platforms for Vascular Tissue Engineering. J. Biomed. Mater. Res. B Appl. Biomater. 2020, 108, 910–924. [Google Scholar] [CrossRef] [PubMed]
- Stamm, C.; Khosravi, A.; Grabow, N.; Schmohl, K.; Treckmann, N.; Drechsel, A.; Nan, M.; Schmitz, K.-P.; Haubold, A.; Steinhoff, G. Biomatrix/Polymer Composite Material for Heart Valve Tissue Engineering. Ann. Thorac. Surg. 2004, 78, 2084–2092. [Google Scholar] [CrossRef] [PubMed]
- Grabow, N.; Schmohl, K.; Khosravi, A.; Philipp, M.; Scharfschwerdt, M.; Graf, B.; Stamm, C.; Haubold, A.; Schmitz, K.-P.; Steinhoff, G. Mechanical and Structural Properties of a Novel Hybrid Heart Valve Scaffold for Tissue Engineering. Artif. Organs 2004, 28, 971–979. [Google Scholar] [CrossRef] [PubMed]
- Jahnavi, S.; Kumary, T.V.; Bhuvaneshwar, G.S.; Natarajan, T.S.; Verma, R.S. Engineering of a Polymer Layered Bio-Hybrid Heart Valve Scaffold. Mater. Sci. Eng. C 2015, 51, 263–273. [Google Scholar] [CrossRef] [PubMed]
- Capel, A.; Melot, M. (73) Assignee: Carmat, Velizy Villacoublay (FR ).
- Li, L.; Wei, K.-M.; Lin, F.; Kong, X.-D.; Yao, J.-M. Effect of Silicon on the Formation of Silk Fibroin/Calcium Phosphate Composite. J. Mater. Sci. Mater. Med. 2008, 19, 577–582. [Google Scholar] [CrossRef]
- Hong, Y.; Huber, A.; Takanari, K.; Amoroso, N.J.; Hashizume, R.; Badylak, S.F.; Wagner, W.R. Mechanical Properties and in Vivo Behavior of a Biodegradable Synthetic Polymer Microfiber–Extracellular Matrix Hydrogel Biohybrid Scaffold. Biomaterials 2011, 32, 3387–3394. [Google Scholar] [CrossRef]
- Casarin, M.; Morlacco, A.; Dal Moro, F. Bladder Substitution: The Role of Tissue Engineering and Biomaterials. Processes 2021, 9, 1643. [Google Scholar] [CrossRef]
- Casarin, M.; Morlacco, A.; Moro, F.D. Tissue Engineering and Regenerative Medicine in Pediatric Urology: Urethral and Urinary Bladder Reconstruction. Int J Mol Sci 2022, 26. [Google Scholar] [CrossRef]
- Kloskowski, T.; Kowalczyk, T.; Nowacki, M.; Drewa, T. Tissue Engineering and Ureter Regeneration: Is It Possible? Int. J. Artif. Organs 2013, 36, 392–405. [Google Scholar] [CrossRef]
- Serrano-Aroca, Á.; Vera-Donoso, C.D.; Moreno-Manzano, V. Bioengineering Approaches for Bladder Regeneration. Int. J. Mol. Sci. 2018, 19, E1796. [Google Scholar] [CrossRef] [PubMed]
- Lin, H.-K.; Madihally, S.V.; Palmer, B.; Frimberger, D.; Fung, K.-M.; Kropp, B.P. Biomatrices for Bladder Reconstruction. Adv. Drug Deliv. Rev. 2015, 82–83, 47–63. [Google Scholar] [CrossRef] [PubMed]
- Sievert, K.D.; Tanagho, E.A. Organ-Specific Acellular Matrix for Reconstruction of the Urinary Tract. World J. Urol. 2000, 18, 19–25. [Google Scholar] [CrossRef]
- Lavelle, J.; Meyers, S.; Ramage, R.; Bastacky, S.; Doty, D.; Apodaca, G.; Zeidel, M.L. Bladder Permeability Barrier: Recovery from Selective Injury of Surface Epithelial Cells. Am. J. Physiol. Renal Physiol. 2002, 283, F242–253. [Google Scholar] [CrossRef] [PubMed]
- Baskin, L.S.; Hayward, S.W.; Young, P.; Cunha, G.R. Role of Mesenchymal-Epithelial Interactions in Normal Bladder Development. J. Urol. 1996, 156, 1820–1827. [Google Scholar] [CrossRef] [PubMed]
- Oberpenning, F.; Meng, J.; Yoo, J.J.; Atala, A. De Novo Reconstitution of a Functional Mammalian Urinary Bladder by Tissue Engineering. Nat. Biotechnol. 1999, 17, 149–155. [Google Scholar] [CrossRef] [PubMed]
- Lai, J.-Y.; Yoon, C.Y.; Yoo, J.J.; Wulf, T.; Atala, A. Phenotypic and Functional Characterization of in Vivo Tissue Engineered Smooth Muscle from Normal and Pathological Bladders. J. Urol. 2002, 168, 1853–1857. [Google Scholar] [CrossRef]
- Nakanishi, Y.; Chen, G.; Komuro, H.; Ushida, T.; Kaneko, S.; Tateishi, T.; Kaneko, M. Tissue-Engineered Urinary Bladder Wall Using PLGA Mesh-Collagen Hybrid Scaffolds: A Comparison Study of Collagen Sponge and Gel as a Scaffold. J. Pediatr. Surg. 2003, 38, 1781–1784. [Google Scholar] [CrossRef]
- Atala, A.; Freeman, M.R.; Vacanti, J.P.; Shepard, J.; Retik, A.B. Implantation in Vivo and Retrieval of Artificial Structures Consisting of Rabbit and Human Urothelium and Human Bladder Muscle. J. Urol. 1993, 150, 608–612. [Google Scholar] [CrossRef]
- Atala, A.; Bauer, S.B.; Soker, S.; Yoo, J.J.; Retik, A.B. Tissue-Engineered Autologous Bladders for Patients Needing Cystoplasty. Lancet Lond. Engl. 2006, 367, 1241–1246. [Google Scholar] [CrossRef]
- Xie, M.; Song, L.; Wang, J.; Fan, S.; Zhang, Y.; Xu, Y. Evaluation of Stretched Electrospun Silk Fibroin Matrices Seeded with Urothelial Cells for Urethra Reconstruction. J. Surg. Res. 2013, 184, 774–781. [Google Scholar] [CrossRef]
- Algarrahi, K.; Franck, D.; Ghezzi, C.E.; Cristofaro, V.; Yang, X.; Sullivan, M.P.; Chung, Y.G.; Affas, S.; Jennings, R.; Kaplan, D.L.; et al. Acellular Bi-Layer Silk Fibroin Scaffolds Support Functional Tissue Regeneration in a Rat Model of Onlay Esophagoplasty. Biomaterials 2015, 53, 149–159. [Google Scholar] [CrossRef]
- Yang, B.; Zhang, Y.; Zhou, L.; Sun, Z.; Zheng, J.; Chen, Y.; Dai, Y. Development of a Porcine Bladder Acellular Matrix with Well-Preserved Extracellular Bioactive Factors for Tissue Engineering. Tissue Eng. Part C Methods 2010, 16, 1201–1211. [Google Scholar] [CrossRef] [PubMed]
- Micol, L.A.; Arenas da Silva, L.F.; Geutjes, P.J.; Oosterwijk, E.; Hubbell, J.A.; Feitz, W.F.J.; Frey, P. In-Vivo Performance of High-Density Collagen Gel Tubes for Urethral Regeneration in a Rabbit Model. Biomaterials 2012, 33, 7447–7455. [Google Scholar] [CrossRef] [PubMed]
- Sayeg, K.; Freitas-Filho, L.G.; Waitzberg, Â.F.L.; Arias, V.E.A.; Laks, M.; Egydio, F.M.; Oliveira, A.S. Integration of Collagen Matrices into the Urethra When Implanted as Onlay Graft. Int. Braz J Urol Off. J. Braz. Soc. Urol. 2013, 39, 414–423. [Google Scholar] [CrossRef] [PubMed]
- Pinnagoda, K.; Larsson, H.M.; Vythilingam, G.; Vardar, E.; Engelhardt, E.-M.; Thambidorai, R.C.; Hubbell, J.A.; Frey, P. Engineered Acellular Collagen Scaffold for Endogenous Cell Guidance, a Novel Approach in Urethral Regeneration. Acta Biomater. 2016, 43, 208–217. [Google Scholar] [CrossRef] [PubMed]
- Aufderklamm, S.; Vaegler, M.; Kelp, A.; Maurer, S.; Gustafsson, L.; Mundhenk, J.; Busch, S.; Daum, L.; Stenzl, A.; Amend, B.; et al. Collagen Cell Carriers Seeded with Human Urothelial Cells for Urethral Reconstructive Surgery: First Results in a Xenograft Minipig Model. World J. Urol. 2017, 35, 1125–1132. [Google Scholar] [CrossRef]
- Kropp, B.P.; Eppley, B.L.; Prevel, C.D.; Rippy, M.K.; Harruff, R.C.; Badylak, S.F.; Adams, M.C.; Rink, R.C.; Keating, M.A. Experimental Assessment of Small Intestinal Submucosa as a Bladder Wall Substitute. Urology 1995, 46, 396–400. [Google Scholar] [CrossRef]
- Kropp, B.P.; Rippy, M.K.; Badylak, S.F.; Adams, M.C.; Keating, M.A.; Rink, R.C.; Thor, K.B. Regenerative Urinary Bladder Augmentation Using Small Intestinal Submucosa: Urodynamic and Histopathologic Assessment in Long-Term Canine Bladder Augmentations. J. Urol. 1996, 155, 2098–2104. [Google Scholar] [CrossRef]
- Campodonico, F.; Benelli, R.; Michelazzi, A.; Ognio, E.; Toncini, C.; Maffezzini, M. Bladder Cell Culture on Small Intestinal Submucosa as Bioscaffold: Experimental Study on Engineered Urothelial Grafts. Eur. Urol. 2004, 46, 531–537. [Google Scholar] [CrossRef]
- Drewa, T. The Artificial Conduit for Urinary Diversion in Rats: A Preliminary Study. Transplant. Proc. 2007, 39, 1647–1651. [Google Scholar] [CrossRef]
- Ayyildiz, A.; Akgül, K.T.; Huri, E.; Nuhoğlu, B.; Kiliçoğlu, B.; Ustün, H.; Gürdal, M.; Germiyanoğlu, C. Use of Porcine Small Intestinal Submucosa in Bladder Augmentation in Rabbit: Long-Term Histological Outcome. ANZ J. Surg. 2008, 78, 82–86. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Liu, Y.; Bharadwaj, S.; Atala, A.; Zhang, Y. Human Urine-Derived Stem Cells Seeded in a Modified 3D Porous Small Intestinal Submucosa Scaffold for Urethral Tissue Engineering. Biomaterials 2011, 32, 1317–1326. [Google Scholar] [CrossRef]
- Wang, Y.; Liao, L. Histologic and Functional Outcomes of Small Intestine Submucosa-Regenerated Bladder Tissue. BMC Urol. 2014, 14, 69. [Google Scholar] [CrossRef] [PubMed]
- Casarin, M.; Fortunato, T.M.; Imran, S.; Todesco, M.; Sandrin, D.; Borile, G.; Toniolo, I.; Marchesan, M.; Gerosa, G.; Bagno, A.; et al. Porcine Small Intestinal Submucosa (SIS) as a Suitable Scaffold for the Creation of a Tissue-Engineered Urinary Conduit: Decellularization, Biomechanical and Biocompatibility Characterization Using New Approaches. Int. J. Mol. Sci. 2022, 23, 2826. [Google Scholar] [CrossRef]
- Liu, Y.; Bharadwaj, S.; Lee, S.J.; Atala, A.; Zhang, Y. Optimization of a Natural Collagen Scaffold to Aid Cell-Matrix Penetration for Urologic Tissue Engineering. Biomaterials 2009, 30, 3865–3873. [Google Scholar] [CrossRef] [PubMed]
- Liao, W.-B.; Song, C.; Li, Y.-W.; Yang, S.-X.; Meng, L.-C.; Li, X.-H. Tissue-Engineered Conduit Using Bladder Acellular Matrix and Bladder Epithelial Cells for Urinary Diversion in Rabbits. Chin. Med. J. (Engl.) 2013, 126, 335–339. [Google Scholar]
- Chen, C.; Zheng, S.; Zhang, X.; Dai, P.; Gao, Y.; Nan, L.; Zhang, Y. Transplantation of Amniotic Scaffold-Seeded Mesenchymal Stem Cells and/or Endothelial Progenitor Cells From Bone Marrow to Efficiently Repair 3-Cm Circumferential Urethral Defect in Model Dogs. Tissue Eng. Part A 2018, 24, 47–56. [Google Scholar] [CrossRef]
- Bhargava, S.; Chapple, C.R.; Bullock, A.J.; Layton, C.; MacNeil, S. Tissue-Engineered Buccal Mucosa for Substitution Urethroplasty. BJU Int. 2004, 93, 807–811. [Google Scholar] [CrossRef]
- Kimuli, M.; Eardley, I.; Southgate, J. In Vitro Assessment of Decellularized Porcine Dermis as a Matrix for Urinary Tract Reconstruction. BJU Int. 2004, 94, 859–866. [Google Scholar] [CrossRef]
- Ziats, N.P.; Miller, K.M.; Anderson, J.M. In Vitro and in Vivo Interactions of Cells with Biomaterials. Biomaterials 1988, 9, 5–13. [Google Scholar] [CrossRef] [PubMed]
- Chun, S.Y.; Lim, G.J.; Kwon, T.G.; Kwak, E.K.; Kim, B.W.; Atala, A.; Yoo, J.J. Identification and Characterization of Bioactive Factors in Bladder Submucosa Matrix. Biomaterials 2007, 28, 4251–4256. [Google Scholar] [CrossRef] [PubMed]
- Eberli, D.; Susaeta, R.; Yoo, J.J.; Atala, A. Tunica Repair with Acellular Bladder Matrix Maintains Corporal Tissue Function. Int. J. Impot. Res. 2007, 19, 602–609. [Google Scholar] [CrossRef] [PubMed]
- Atala, A. Tissue Engineering of Human Bladder. Br. Med. Bull. 2011, 97, 81–104. [Google Scholar] [CrossRef] [PubMed]
- Dong, Y.; Yong, T.; Liao, S.; Chan, C.K.; Stevens, M.M.; Ramakrishna, S. Distinctive Degradation Behaviors of Electrospun Polyglycolide, Poly(DL-Lactide-Co-Glycolide), and Poly(L-Lactide-Co-Epsilon-Caprolactone) Nanofibers Cultured with/without Porcine Smooth Muscle Cells. Tissue Eng. Part A 2010, 16, 283–298. [Google Scholar] [CrossRef] [PubMed]
- Dvir, T.; Timko, B.P.; Kohane, D.S.; Langer, R. Nanotechnological Strategies for Engineering Complex Tissues. Nat. Nanotechnol. 2011, 6, 13–22. [Google Scholar] [CrossRef] [PubMed]
- Coyan, G.N.; da Mota Silveira-Filho, L.; Matsumura, Y.; Luketich, S.K.; Katz, W.; Badhwar, V.; Wagner, W.R.; D’Amore, A. Acute In Vivo Functional Assessment of a Biodegradable Stentless Elastomeric Tricuspid Valve. J Cardiovasc. Transl. Res. 2020, 13, 796–805. [Google Scholar] [CrossRef] [PubMed]
- Grunkemeier, G.L.; Furnary, A.P.; Wu, Y.; Wang, L.; Starr, A. Durability of Pericardial versus Porcine Bioprosthetic Heart Valves. J. Thorac. Cardiovasc. Surg. 2012, 144, 1381–1386. [Google Scholar] [CrossRef] [PubMed]
- Makkar, R.R.; Fontana, G.; Jilaihawi, H.; Chakravarty, T.; Kofoed, K.F.; De Backer, O.; Asch, F.M.; Ruiz, C.E.; Olsen, N.T.; Trento, A.; et al. Possible Subclinical Leaflet Thrombosis in Bioprosthetic Aortic Valves. N. Engl. J. Med. 2015, 373, 2015–2024. [Google Scholar] [CrossRef]
- METHODS FOR DEVELOPMENT OF HYBRID TISSUE ENGINEERED VALVE WITH POLYURETHANE CORE.Pdf.
- Stephens, E.H.; de Jonge, N.; McNeill, M.P.; Durst, C.A.; Grande-Allen, K.J. Age-Related Changes in Material Behavior of Porcine Mitral and Aortic Valves and Correlation to Matrix Composition. Tissue Eng. Part A 2010, 16, 867–878. [Google Scholar] [CrossRef] [PubMed]
- Ong, S.H.; Mueller, R.; Iversen, S. Early Calcific Degeneration of a CoreValve Transcatheter Aortic Bioprosthesis. Eur. Heart J. 2012, 33, 586–586. [Google Scholar] [CrossRef] [PubMed]
- Conte, M.S. Critical Appraisal of Surgical Revascularization for Critical Limb Ischemia. J. Vasc. Surg. 2013, 57, 8S–13S. [Google Scholar] [CrossRef] [PubMed]
- Klinkert, P.; Post, P.N.; Breslau, P.J.; van Bockel, J.H. Saphenous Vein Versus PTFE for Above-Knee Femoropopliteal Bypass. A Review of the Literature. Eur. J. Vasc. Endovasc. Surg. 2004, 27, 357–362. [Google Scholar] [CrossRef] [PubMed]
- Pashneh-Tala, S.; MacNeil, S.; Claeyssens, F. The Tissue-Engineered Vascular Graft—Past, Present, and Future. Tissue Eng. Part B Rev. 2016, 22, 68–100. [Google Scholar] [CrossRef] [PubMed]
- Davies, M.G.; Hagen, P.-O. Pathophysiology of Vein Graft Failure: A Review. Eur. J. Vasc. Endovasc. Surg. 1995, 9, 7–18. [Google Scholar] [CrossRef] [PubMed]
- FitzGibbon, G.M.; Leach, A.J.; Kafka, H.P.; Keon, W.J. Coronary Bypass Graft Fate: Long-Term Angiographic Study. J. Am. Coll. Cardiol. 1991, 17, 1075–1080. [Google Scholar] [CrossRef] [PubMed]
- Vanderwal, A.; Becker, A.; Elbers, J.; Das, P. An Immunocytochemical Analysis of Rapidly Progressive Atherosclerosis in Human Vein Grafts. Eur. J. Cardiothorac. Surg. 1992, 6, 469–474. [Google Scholar] [CrossRef]
- Steinhoff, G.; Stock, U.; Karim, N.; Mertsching, H.; Timke, A.; Meliss, R.R.; Pethig, K.; Haverich, A.; Bader, A. Tissue Engineering of Pulmonary Heart Valves on Allogenic Acellular Matrix Conduits: In Vivo Restoration of Valve Tissue. Circulation 2000, 102. [Google Scholar] [CrossRef]
- Wilson, G.J.; Courtman, D.W.; Klement, P.; Michael Lee, J.; Yeger, H. Acellular Matrix: A Biomaterials Approach for Coronary Artery Bypass and Heart Valve Replacement. Ann. Thorac. Surg. 1995, 60, S353–S358. [Google Scholar] [CrossRef]
- Bader, A.; Schilling, T.; Teebken, O.E.; Brandes, G.; Herden, T.; Steinhoff, G.; Haverich, A. Tissue Engineering of Heart Valves – Human Endothelial Cell Seeding of Detergent Acellularized Porcine Valves1. Eur. J. Cardiothorac. Surg. 1998, 14, 279–284. [Google Scholar] [CrossRef]
- Mirsadraee, S.; Wilcox, H.E.; Korossis, S.A.; Kearney, J.N.; Watterson, K.G.; Fisher, J.; Ingham, E. Development and Characterization of an Acellular Human Pericardial Matrix for Tissue Engineering. Tissue Eng. 2006, 12, 763–773. [Google Scholar] [CrossRef] [PubMed]
- Bechtel, J.F.M.; Müller-Steinhardt, M.; Schmidtke, C.; Brunswik, A.; Stierle, U.; Sievers, H.-H. Evaluation of the Decellularized Pulmonary Valve Homograft (SynerGraft). J. Heart Valve Dis. 2003, 12, 734–739. [Google Scholar] [PubMed]
- Hoerstrup, S.P.; Sodian, R.; Daebritz, S.; Wang, J.; Bacha, E.A.; Martin, D.P.; Moran, A.M.; Guleserian, K.J.; Sperling, J.S.; Kaushal, S.; et al. Functional Living Trileaflet Heart Valves Grown In Vitro. Circulation 2000, 102, III–44. [Google Scholar] [CrossRef]
- Shinoka, T.; Breuer, C.K.; Tanel, R.E.; Zund, G.; Miura, T.; Ma, P.X.; Langer, R.; Vacanti, J.P.; Mayer, J.E. Tissue Engineering Heart Valves: Valve Leaflet Replacement Study in a Lamb Model. Ann. Thorac. Surg. 1995, 60, S513–S516. [Google Scholar] [CrossRef] [PubMed]
- Stock, U.A.; Nagashima, M.; Khalil, P.N.; Nollert, G.D.; Herdena, T.; Sperling, J.S.; Moran, A.; Lien, J.; Martin, D.P.; Schoen, F.J.; et al. Tissue-Engineered Valved Conduits in the Pulmonary Circulation. J. Thorac. Cardiovasc. Surg. 2000, 119, 732–740. [Google Scholar] [CrossRef]
- Sodian, R.; Loebe, M.; Hein, A.; Martin, D.P.; Hoerstrup, S.P.; Potapov, E.V.; Hausmann, H.; Lueth, T.; Hetzer, R. Application of Stereolithography for Scaffold Fabrication for Tissue Engineered Heart Valves. ASAIO J. 2002, 48, 12–16. [Google Scholar] [CrossRef]
- Mudigonda, J.; Xu, D.; Amedi, A.; Lane, B.A.; Corporan, D.; Wang, V.; Padala, M. A Biohybrid Material With Extracellular Matrix Core and Polymeric Coating as a Cell Honing Cardiovascular Tissue Substitute. Front. Cardiovasc. Med. 2022, 9, 807255. [Google Scholar] [CrossRef]
- Zheng, Z.; Eglin, D.; Alini, M.; Richards, G.R.; Qin, L.; Lai, Y. Visible Light-Induced 3D Bioprinting Technologies and Corresponding Bioink Materials for Tissue Engineering: A Review. Engineering 2021, 7, 966–978. [Google Scholar] [CrossRef]
- Goldman, M.D.; Simpson, D.; Hawker, R.J.; Norcott, H.C.; Mccollum, C.N. Aspirin and Dipyridamole Reduce Platelet Deposition on Prosthetic Femoro-Popliteal Grafts in Man: Ann. Surg. 1983, 198, 713–716. [Google Scholar] [CrossRef] [PubMed]
- Pumphrey, C.W.; Chesebro, J.H.; Dewanjee, M.K.; Wahner, H.W.; Hollier, L.H.; Pairolero, P.C.; Fuster, V. In Vivo Quantitation of Platelet Deposition on Human Peripheral Arterial Bypass Grafts Using Indium-111-Labeled Platelets. Am. J. Cardiol. 1983, 51, 796–801. [Google Scholar] [CrossRef]
- Sayers, R.D.; Raptis, S.; Berce, M.; Miller, J.H. Long-Term Results of Femorotibial Bypass with Vein or Polytetrafluoroethylene. Br. J. Surg. 2003, 85, 934–938. [Google Scholar] [CrossRef] [PubMed]
- Salacinski, H.J.; Tiwari, A.; Hamilton, G.; Seifalian, A.M. Cellular Engineering of Vascular Bypass Grafts: Role of Chemical Coatings for Enhancing Endothelial Cell Attachment. Med. Biol. Eng. Comput. 2001, 39, 609–618. [Google Scholar] [CrossRef] [PubMed]
- Kolar, M.; Mozetič, M.; Stana-Kleinschek, K.; Fröhlich, M.; Turk, B.; Vesel, A. Covalent Binding of Heparin to Functionalized PET Materials for Improved Haemocompatibility. Mater. Basel Switz. 2015, 8, 1526–1544. [Google Scholar] [CrossRef] [PubMed]
- Calaitges, J.G.; Liem, T.K.; Spadone, D.; Nichols, W.K.; Silver, D. The Role of Heparin-Associated Antiplatelet Antibodies in the Outcome of Arterial Reconstruction. J. Vasc. Surg. 1999, 29, 779–785. [Google Scholar] [CrossRef] [PubMed]
- Curi, M.A.; Skelly, C.L.; Baldwin, Z.K.; Woo, D.H.; Baron, J.M.; Desai, T.R.; Katz, D.; McKinsey, J.F.; Bassiouny, H.S.; Gewertz, B.L.; et al. Long-Term Outcome of Infrainguinal Bypass Grafting in Patients with Serologically Proven Hypercoagulability. J. Vasc. Surg. 2003, 37, 301–306. [Google Scholar] [CrossRef]
- Liang, H.-C.; Chang, Y.; Hsu, C.-K.; Lee, M.-H.; Sung, H.-W. Effects of Crosslinking Degree of an Acellular Biological Tissue on Its Tissue Regeneration Pattern. Biomaterials 2004, 25, 3541–3552. [Google Scholar] [CrossRef]
- Schmidmaier, G.; Lucke, M.; Schwabe, P.; Raschke, M.; Haas, N.P.; Wildemann, B. Collective Review: Bioactive Implants Coated with Poly(D,L-Lactide) and Growth Factors IGF-I, TGF-Β1, or BMP-2 for Stimulation of Fracture Healing. J. Long. Term Eff. Med. Implants 2006, 16, 61–69. [Google Scholar] [CrossRef]
- Tamada, J.A.; Langer, R. Erosion Kinetics of Hydrolytically Degradable Polymers. Proc. Natl. Acad. Sci. U. S. A. 1993, 90, 552–556. [Google Scholar] [CrossRef]
- Tapias, L.F.; Ott, H.C. Decellularized Scaffolds as a Platform for Bioengineered Organs. Curr. Opin. Organ Transplant. 2014, 19, 145–152. [Google Scholar] [CrossRef]
- Lu, T.-Y.; Lin, B.; Kim, J.; Sullivan, M.; Tobita, K.; Salama, G.; Yang, L. Repopulation of Decellularized Mouse Heart with Human Induced Pluripotent Stem Cell-Derived Cardiovascular Progenitor Cells. Nat. Commun. 2013, 4, 2307. [Google Scholar] [CrossRef]
- van der Meijden, P.E.J.; Munnix, I.C.A.; Auger, J.M.; Govers-Riemslag, J.W.P.; Cosemans, J.M.E.M.; Kuijpers, M.J.E.; Spronk, H.M.; Watson, S.P.; Renné, T.; Heemskerk, J.W.M. Dual Role of Collagen in Factor XII–Dependent Thrombus Formation. Blood 2009, 114, 881–890. [Google Scholar] [CrossRef] [PubMed]
- Nelson, T.; Kaufman, E.; Kline, J.; Sokoloff, L. The Extraneural Distribution of ?-Hydroxybutyrate. J. Neurochem. 1981, 37, 1345–1348. [Google Scholar] [CrossRef] [PubMed]
- Wu, S.; Liu, Y.-L.; Cui, B.; Qu, X.-H.; Chen, G.-Q. Study on Decellularized Porcine Aortic Valve/Poly (3-Hydroxybutyrate-Co-3-Hydroxyhexanoate) Hybrid Heart Valve in Sheep Model. Artif. Organs 2007, 31, 689–697. [Google Scholar] [CrossRef] [PubMed]
- Jansen, P.; van Oeveren, W.; Capel, A.; Carpentier, A. In Vitro Haemocompatibility of a Novel Bioprosthetic Total Artificial Heart. Eur. J. Cardiothorac. Surg. 2012, 41, e166–e172. [Google Scholar] [CrossRef]
- Todesco, M.; Pontara, E.; Cheng, C.; Gerosa, G.; Pengo, V.; Bagno, A. Preliminary Hemocompatibility Assessment of an Innovative Material for Blood Contacting Surfaces. J. Mater. Sci. Mater. Med. 2021, 32, 86. [Google Scholar] [CrossRef]
- Reed, A.M.; Potter, J.; Szycher, M. A Solution Grade Biostable Polyurethane Elastomer: ChronoFlex® AR. J. Biomater. Appl. 1994, 8, 210–236. [Google Scholar] [CrossRef]
Figure 1.
Articles on hybrid materials published between 2000 and 2023 (PubMed and ScienceDirect).
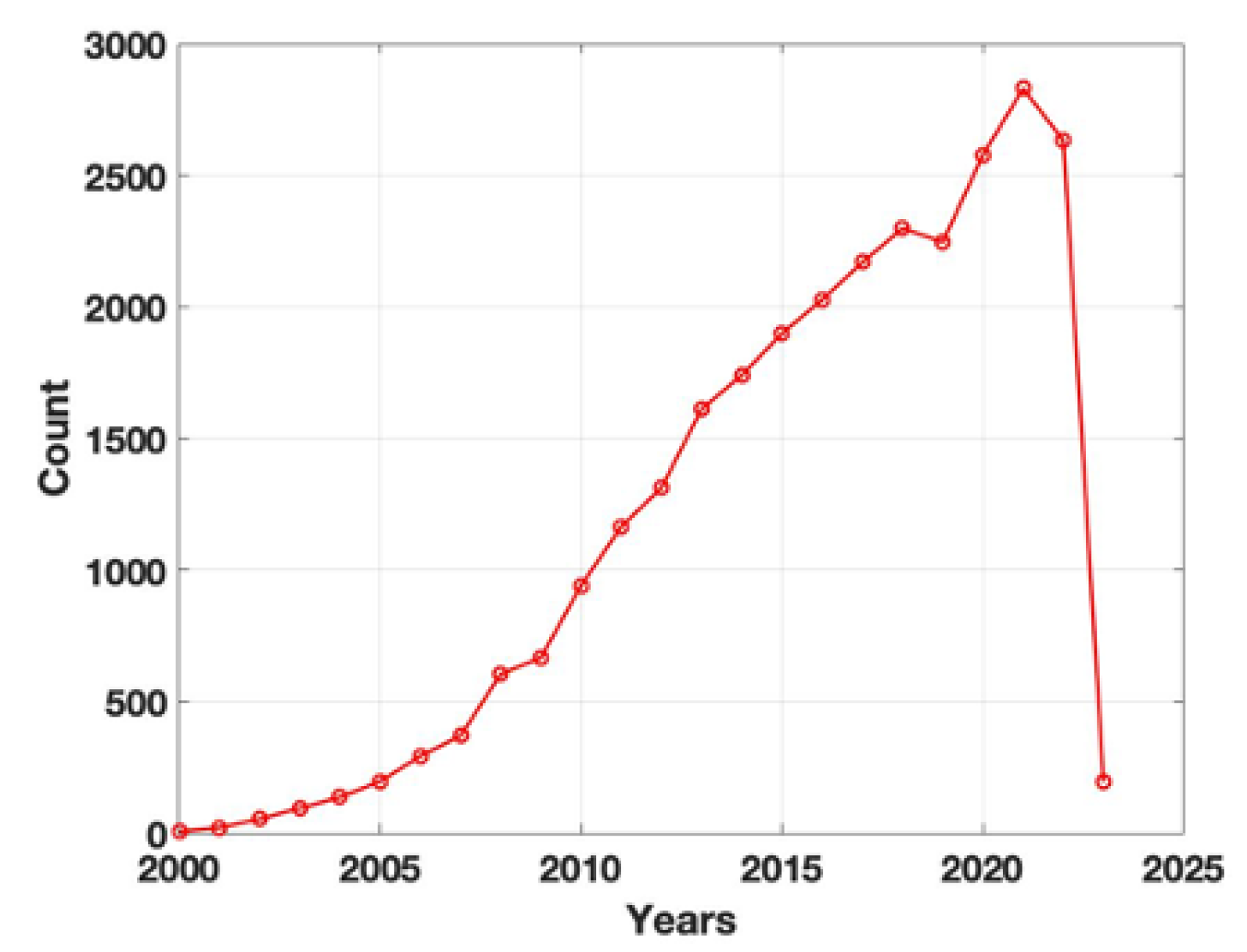
Figure 2.
Examples of the hybrid materials obtained by coupling: (A) porcine decellularized pericardium with polycarbonate urethane (Chronoflex AR) for cardiovascular tissue reconstruction; (B) porcine decellularized SIS with polycarbonate urethane (Chronoflex AR-LT) for urological applications.
Figure 2.
Examples of the hybrid materials obtained by coupling: (A) porcine decellularized pericardium with polycarbonate urethane (Chronoflex AR) for cardiovascular tissue reconstruction; (B) porcine decellularized SIS with polycarbonate urethane (Chronoflex AR-LT) for urological applications.
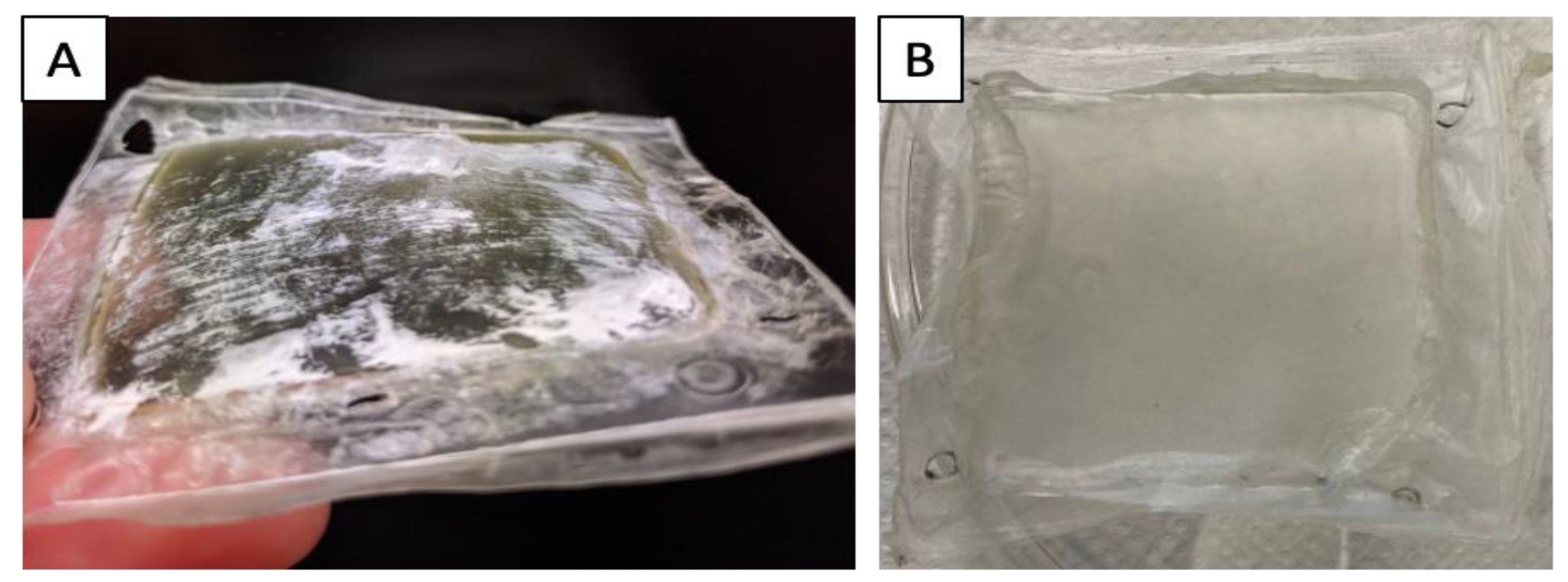
Figure 3.
Representation of the fate of a hybrid material after in vivo implantation: on the left, the schematic composition of the hybrid material made by coupling a decellularized biological tissue with a synthetic polymer: circulating cells are chemo-attracted by the acellular ECM, whose mechanical resistance is sustained by the polymer. On the right, the hybrid material is effectively repopulated with the host’s circulating cells.
Figure 3.
Representation of the fate of a hybrid material after in vivo implantation: on the left, the schematic composition of the hybrid material made by coupling a decellularized biological tissue with a synthetic polymer: circulating cells are chemo-attracted by the acellular ECM, whose mechanical resistance is sustained by the polymer. On the right, the hybrid material is effectively repopulated with the host’s circulating cells.
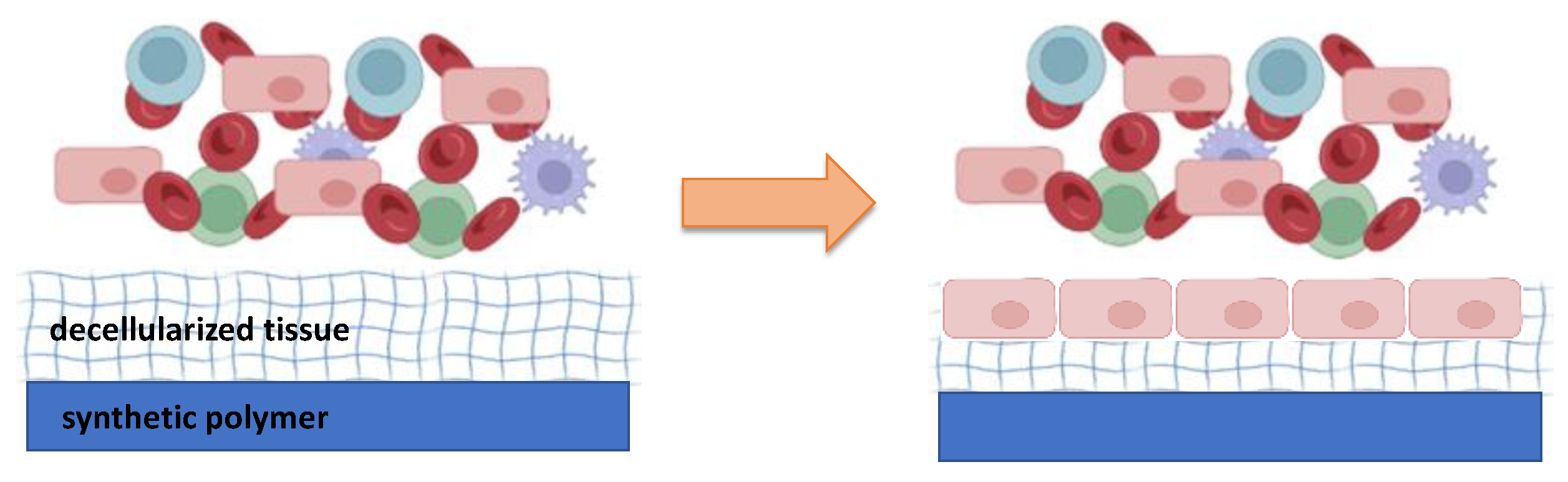

Table 1.
Summary of the main studies on hybrid materials for different clinical applications.
| Biological materials | Synthetic materials | Applications | Type of study | References |
|---|---|---|---|---|
| Hydroxyapatite + Chitosan | - | Orthopedic | in vitro | [31] |
| Chitosan | Poly lactic glycolic acid | - | in vitro | [32] |
| Chitosan | Polycaprolactone | - | in vitro | [33] |
| Collagen | Polycaprolactone + TiO2 | Dermatological | in vitro | [34] |
| Collagen | Polycaprolactone | Urological | in vitro | [35] |
| Collagen and elastin | Polycaprolactone | Cardiovascular | in vitro | [36] |
| Collagen | copoly(L-lactide/ε-caprolactone) | Urological | in vitro andin vivo | [37] |
| Collagen | poly(lactic acid-co-caprolactone) | Dermatological | in vitro | [22] |
| Collagen | poly(lactic acid-co-ε-caprolactone) | Urological | in vitro andin vivo | [38] |
| Collagen | Vypro II | Urological | in vitro andin vivo | [39] |
| Silk + collagen or fibronectin | - | Urological | in vitro | [23] |
| Collagen | Poly lactic glycolic acid | Urological | in vitro | [25] |
| - | poly glycolic acid + poly lactic glycolic acid | Urological | in vivo | [40] |
| Bladder acellular matrix + collagen | Poly glycolic acid | Urological | in vivo | [18] |
| Bladder acellular matrix | Poly lactic glycolic acid | Urological | in vitro andin vivo | [19,24] |
| - | Polyester urethane or poly lactic glycolic acid + Polyethylene glycol | Urological | in vivo | [41] |
| Human amniotic membrane | Poly-(L-lactide-co-E-caprolactone) | Urological | in vivo | [20] |
| Amniotic membrane | Graphene | Urological | in vitro | [21] |
| Gelatin | Copolymer | Urological | in vitro | [42] |
| Small intestinal submucosa | Polycarbonate urethane | Urological | in vitro | [43] |
| - | Polytetrafluoroethylene + Polylactic acid | Cardiovascular | in vitro | [44] |
| - | polytetrafluoroethylene + Poly(DL-lactide) | Cardiovascular | in vitro and in vivo | [45] |
| - | polytetrafluoroethylene + polylactic acid with Polyethylene glycol -hirudin/iloprost | Cardiovascular | in vitro and in vivo | [46] |
| Chemically fixed decellularized porcine aorta | Poly(D,L-lactide) with lepirudin | Cardiovascular | in vitro and in vivo | [47] |
| Decellularized bovine heart and aorta | Polycaprolactone | Cardiovascular | in vitro | [48] |
| Decellularized porcine aortic valve | Poly(hydroxybutyrate) | Cardiovascular | in vitro and in vivo | [49] |
| Decellularized aortic valve | Poly(4-hydroxybutyrate) (P[4HB]) or poly(3-hydroxybutyrate-co4-hydroxybutyrate) (P[3HB-co4HB]) | Cardiovascular | in vitro | [50] |
| Decellularized bovine pericardium + Chitosan | Polycaprolactone | Cardiovascular | in vitro | [51] |
| Fixed bovine pericardium | Polycarbonate urethane | Cardiovascular | in vitro | [52] |
| Bovine or porcine pericardium | Polycarbonate urethane | Cardiovascular | in vitro | [26] |
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2024 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (https://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



