
Submitted:
21 May 2023
Posted:
23 May 2023
You are already at the latest version
Abstract
Multiple sclerosis (MS) is a heterogeneous disease of the central nervous system that is governed by neural tissue loss and dystrophy during its progressive phase, with complex reactive pathological cellular changes. The immune-mediated mechanisms that promulgate the demyelinating lesions during the relapses of acute episodes are not characteristic of chronic lesions during progressive MS. This has limited our capacity to target the disease effectively as it evolves within the central nervous system white and gray matter, thereby leaving neurologists without effective options to manage individuals as they transition to a secondary progressive phase. The current review highlights the molecular and cellular sequelae that have been identified to cooperate and/or contribute to neurodegeneration that identifies individuals with progressive forms of MS. We emphasize the need for appropriate monitoring via known and novel molecular and imaging biomarkers that can accurately detect and predict progression for the purposes of newly designed clinical trials that may demonstrate efficacy of neuroprotection and potentially neurorepair. To achieve neurorepair, we focus on the modifications required in the reactive cellular and extracellular milieu, in order to enable endogenous cell growth as well as transplanted cells that can integrate and/or renew the degenerative MS plaque.
Keywords:
multiple sclerosis
; oligodendrocyte
; myelination
; inflammation
; microglia
; macrophage
; bi-omarkers
; imaging diagnostics
1. Introduction
Multiple sclerosis (MS) pathology presents as several multifocal lesions characterized by inflammation and demyelination within the central nervous system (CNS) [1]. These pathological hallmarks reported during initial stages of the disease are often accompanied by the clinical manifestation of functional relapses followed by remission, also known as relapsing-remitting multiple sclerosis (RRMS). Hence, the heterogeneity of this disease governs the course and severity of the neurological outcomes in patients with MS [2,3]. Although the exact cause is unknown, the infiltration of peripheral inflammatory lymphocytes and myeloid cells degenerate the myelin sheath along axons [4,5,6,7]. The destruction of myelin, deposits biological debris in the extracellular milieu within the CNS, further resulting in axonal dystrophy, synaptic injury, and gliosis, as observed in patients who transition into the progressive stage of MS [1,8,9,10].
The severity and frequency of relapses during the RRMS phase can be alleviated to some extent by currently available disease-modifying treatments (DMTs) such as fingolimod that modulate immune cell trafficking. Despite the significant therapeutic impact of DMTs in improving the symptoms of RRMS, the conversion to secondary progressive MS (SPMS) remains a prognostic outcome, with further neurological progression governed by the lack of treatment options. Therefore, treatment for progressive MS remains a major unmet medical need [11,12,13,14].
The urgent need for novel and/or repurposed therapeutics has been highlighted by a recent retrospective study conducted in Iran that predicted 93% of RRMS patients would transition into SPMS within a span of 30 years despite receiving early intensive DMTs or escalation treatment [15]. Another clinical study conducted by Kalincik et al. showed a smaller proportion of RRMS patients advancing to the progressive stage with the administration of DMTs compared to the control group, with no significant effect by DMTs in progressive MS patients [16]. Therefore, to address the gap in the treatment of progressive MS, potential therapies that attempt to limit demyelination of axons and restore axonal function may have a positive therapeutic outcome in ameliorating MS chronic disease progression.
In this review, we discuss the comprehensive cellular and molecular mechanisms involved in the progressive stages of MS, with particular focus on the role of phagocytosis in promoting remyelination and axonal regeneration within the CNS. Moreover, we highlight the benefits of using cellular delivery strategies, such as genetically modified hematopoietic stem cells (HSCs) that can express potential therapeutic proteins, capable of crossing the blood-brain barrier (BBB) to repair the CNS environment during progressive MS. Furthermore, we address the lack of cellular and molecular biomarkers used in MS diagnosis and in the assessment of progression, by exploring novel potential biomarkers as a means of monitoring neuroreparative strategies designed for clinical translation during trials of recruited individuals living with SPMS.
Pathogenesis
Alterations in the blood-brain barrier during MS
Structurally, the BBB is a tightly regulated biophysical cellular barrier consisting of cerebral endothelial cells, pericytes, and a basement membrane that interacts with astrocyte end-feet [For review see [17]]. This barrier separates the CNS from systemic circulation and can selectively restrict molecules and cells from passively entering the CNS environment [For review see [17]]. As such, a key feature required when designing drug delivery into the CNS is to overcome the restrictive BBB. In RRMS, abnormalities in tight junctions located in the blood vessels of active lesions can cause a temporary disruption to the BBB [18,19]. This alteration to the BBB is accompanied by modulation of the vascular endothelial cytoskeleton and the tight junctions, attributed to the release and accumulation of pro-inflammatory cytokines secreted from differentiated T cells and activated macrophages [20]. Additionally, the interaction between endothelial cells and monocytes, produce reactive oxygen species (ROS) which further contribute to decreased BBB integrity. Consequently, making it more susceptible to increased migration and infiltration of inflammatory cell-trafficking into the CNS [21,22] and potentially promulgating axonal and neuronal damage [23].
Other pathogenic factors that are upregulated within the extracellular milieu include matrix metalloproteinases (MMPs), regulating the cleavage of the extracellular matrix (ECM) proteins, penetrating and mobilizing innate and adaptive leukocytes throughout the CNS tissue [24]. The importance of these findings of the pathogenic involvement of MMPs during inflammatory demyelination relates to the propagation of perivascular cells and microglia expanding neuroinflammatory lesions [24,25].
Throughout the neuroinflammatory lesions, the cytokines generated by differentiated T cells, that can drive MMP activity within the pathogenic milieu can include tumor necrosis factor-alpha (TNF-α) and interleukin (IL)-17, which can stimulate MMP-9 transcription to degrade the ECM [26]. This would imply that a mutual promotion of MMP activity and recruitment of immune cells exists [26]. Intriguingly, Kanesaka et al. previously reported that MMP-3 serum levels were higher during the relapsing stage of MS than in remission [27], implicating MMP-3 as a molecular biomarker for the acute phase of inflammatory demyelination.
The relationship of MMP activity during lesion formation in active MS demonstrates a dysregulation of MMP-1, -2, -3, -7, and -9 expression by demyelinating macrophages. When these lesions progress to the chronic state, macrophages display a downregulation of MMP expression [28,29]. Alexander et al. found that the decrease in MMP-8 and MMP-9 serum levels correlated with a reduction in the number of gadolinium-enhancing magnetic resonance imaging (MRI) lesions [30], suggesting that the identification of reduced levels of these MMPs may be an appropriate marker that defines neurodegenerative change during progression. Consequently, cellular-mediated alterations of the BBB may provide clues in identifying the principal cells driving MS pathology and, therefore, may assist in developing cell-based therapeutic vehicles to limit BBB permeability and immune cell infiltration.
Immune cell infiltration across the BBB may well be the primary target for future therapeutics to limit pathogenic T cell subsets from perpetuating the cycle of neuroinflammation. Recent evidence has implicated the dual immunoglobulin domain containing cell adhesion molecule (DICAM) as a prominent receptor expressed on invading T helper (Th) cell 17+ lymphocytes during RRMS and progressive MS [31]. Importantly these investigators identified the ligand for DICAM, the αvβ3 integrin, to be expressed in the BBB endothelial cells during inflammatory disease activity, in MS demyelinating lesions identified from archival tissue. DICAM is a member of the CTX family of adhesion proteins of which the extracellular Ig domain 2 that was unrelated to the Arginyl-Glycyl-Aspartate (RGD) binding domain of the αvβ3 integrin [32]. Binding of DICAM expressed on CD4+ T cells to the αvβ3 integrin expressed on endothelial cells at the BBB can promote inhibition of Akt signaling leading to integrin β3/Focal Adhesion Kinase (FAK) activity with resultant actin cytoskeletal rearrangement [33], to transiently open up the tight junctions allowing for transendothelial cell migration of the Th17+ pathogenic lymphocytes [31]. Indeed, by antagonizing DICAM interaction with endothelial v3 integrin, it was demonstrated that the clinical course of experimental autoimmune encephalomyelitis (EAE) could be reduced in severity that correlated with a reduction in the transendothelial cell migration across the BBB [31]. The data suggest that DICAM plays an integral role in the trafficking of pathogenic Th17 cells across the BBB during active inflammatory demyelinating lesions in MS.
Outside-in vs inside-out hypotheses
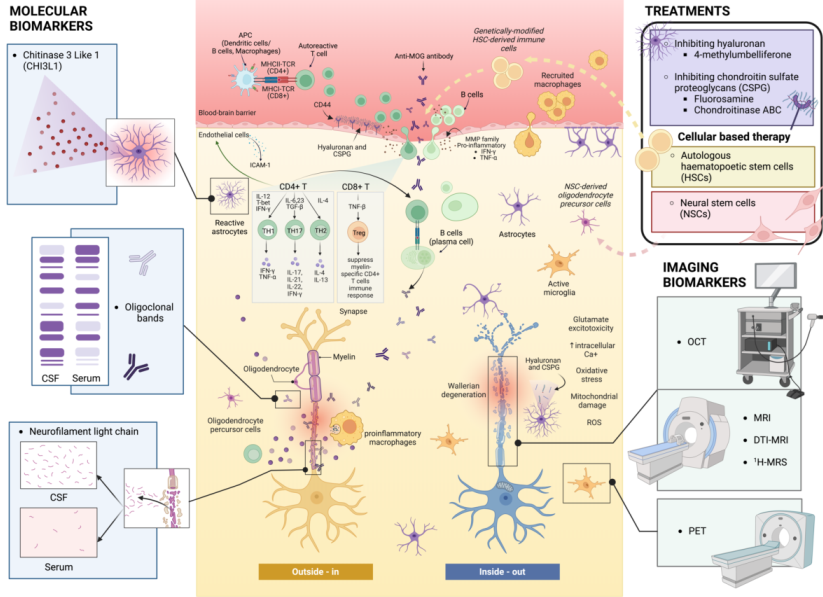
Currently, there are two competing hypotheses that explain the etiopathogenesis of MS: the inside-out and outside-in models that manifest similar clinical presentations [For review see [34]]. These models operate simultaneously in MS patients, to form inflammatory demyelinating lesions (Figure 1). The outside-in model can be described as dysregulation of peripheral immune cells that result in an autoimmune attack against myelin within the CNS [35,36,37]. Classically, myelin antigen-activated immune cells such as circulating T lymphocytes, B lymphocytes and activated monocytic cells, traverse the disrupted BBB and infiltrate into the CNS to target putative myelin epitopes [For review see [38]]. Although this hypothesis highlights the prominent role of immune cells promulgating inflammation and demyelination in MS, it fails to explain an underlying cause that initiates the autoimmune response [2]. Investigational inference may be derived from a recent genome-wide analysis mapping the X chromosome from 47,429 MS patients, which demonstrated that MS variants were enriched in human microglia, along with peripheral immune cells [39]. This study suggests that both the adaptive immune response, incorporating resident glial cells, play a combined role in MS etiopathogenesis. Therefore, the outside-in model that primarily supports the role of the adaptive immune system in propagating ongoing inflammation cannot be the sole explanation for the heterogeneous pathogenesis that manifests in MS. In contrast, the inside-out hypothesis maintains that the pathology of MS is initiated, and importantly, progresses as a result of the degeneration of oligodendrocytes in the CNS governed by altered signaling of microglia and astrocytes, responsible for innate immunity [40,41]. The slow degradation of oligodendrocytes may cause antigenic myelin proteins that are citrullinated to be released into the circulation over time, which in turn activates T and B lymphocytic responses that perpetuate an inflammatory cycle [42,43,44].
Recent data by Bjornevik et al. provided evidence that EBV infection may be a leading cause of MS, but the exact mechanism for disease initiation is still unclear [45]. Possible mechanisms may include the activation of autoreactive B cells and molecular mimicry, in which CD4+ T cells are able to recognize both EBV and myelin peptides [46,47,48]. However, these mechanisms are still not well-defined during MS pathogenesis. Serafini et al. highlighted that EBV infection was evident in the B cells and plasma cells infiltrating into the brain of MS patients but the cause of the migration of infected B cells to the site of injury in the CNS was not explored [49]. Furthermore, Bjornevik et al. showed that the median time from EBV seroconversion to MS clinical manifestations was 7.5 years [45]. The studies suggest that EBV may not be the primary cause of MS and there is another cofactor that triggers the initiation of the disease.
Ermin is a component of myelin that contributes to the integrity of myelin sheaths and its expression has been shown to be downregulated in mouse brains during cuprizone-mediated demyelination as well as mutations identified from isolated peripheral immune cells of individuals from one family that exhibited RRMS [40,50,51]. Ziaei et al. described the loss of myelin sheath integrity in 5-month-old Ermin knockout (KO) mice and axonal damage in 3-month-old Ermin KO mice [40]. Microgliosis, astrogliosis, oligodendrocytes loss, and upregulation of inflammatory response genes were also observed in 8-month-old Ermin KO mice [40]. In addition, induction of EAE in Ermin KO mice resulted in a higher number of CD45HI infiltrating monocytes in the CNS compared to EAE-induced wildtype (WT) mice [40], providing compelling evidence for inside-out paradigm of MS etiopathogenesis. However, the relationship between Ermin and MS etiopathogenesis has not been thoroughly explored to establish causal relationships with oligodendrocyte-myelin dysfunction.
The role of macrophages and microglia in driving neurodegeneration in MS
Macrophages and microglia, arising from hematogenous and endogenous precursors, are important respondents in MS immunopathogenesis [52]. Microglial cell precursors are established prior to birth and can undergo self-proliferation in situ [53]. A study by Ajami et al. showed that blood monocytes gave rise to infiltrating macrophages within the CNS but not microglia, and these infiltrating monocytes were associated with the progression of EAE [54], implying that the endogenous microglia and monocyte-derived macrophages are two separate populations. Furthermore, the infiltrating monocytic-derived macrophages at the peak of EAE were present transiently in the CNS whereas proliferating microglia were still detected three months later [54]. Mildner et al. described peripheral Ly-6ChiCCR2+ monocytes infiltrated into the CNS and differentiated into resident microglia but only when the brain and spinal cord of cuprizone or healthy mice were irradiated, highlighting the need for brain conditioning and the BBB disruption before engraftment [55].
Human monocytes can be divided into CD14+CD16- classical, CD14+CD16dim intermediate, and CD14dimCD16+ non-classical monocytes [56]. In mice, the CCR2+CD62L+CX3CR1-EGFPloLy6C+ monocytes correspond to human classical monocytes and CCR2−CD62L−CX3CR1-EGFPhiLy6Clo monocytes correspond to human non-classical monocytes [57]. A fate mapping analysis of the monocyte origin revealed that classical Ly6C+CX3CR1int monocytes from bone marrow and blood give rise to nonclassical Ly6C-CX3CR1hi monocytes in both compartments [58]. However, CD43 and Ly6c were substantiated to be better monocyte markers in CX3CR1+/EGFP mice because the green fluorescent protein (GFP) level did not accurately reflect the actual CX3CR1 expression [59]. In the CNS, CX3CL1 is mostly expressed in neurons while CX3CR1 expression is detected in the microglia [60,61]. The deficiency of CX3CR1 in cuprizone-fed mice was shown to lower TREM2 and CD11c expression in microglia, leading to lower phagocytic activity and clearance of myelin debris [62].
Similar to T lymphocytes, different cytokines and chemokines can induce macrophages and microglia to release either pro-inflammatory cytokines, TNF-α and IL-1β, to promote a pro-inflammatory environment, or anti-inflammatory cytokines, IL-10 and transforming growth factor (TGF)-β, to stimulate regeneration and repair [63,64]. Interestingly, in active demyelinating white matter lesions in MS-diagnosed individuals, macrophages are observed to co-express the proinflammatory marker CD40 and anti-inflammatory marker CD206, indicating an intermediate activation status of macrophages [65]. However, in chronic-active lesions, macrophages and microglia in slow expanding edges, co-expressed CD40 and anti-inflammatory marker CD163 [65]. This depicts the heterogeneity of macrophages and microglial cell polarization and highlights the complex classification of microglia and macrophage phenotypes in MS lesions at different stages of the pathogenic pathway.
During inflammatory disease, macrophages and microglia attempt to maintain compartmentalization of homeostasis through plasma membrane polarization to expedite phagocytosis of accumulated myelin debris and apoptotic cells within the extracellular milieu, a pathogenic mechanism that results in physiological inhibition to promote neurorepair during MS [62,66,67]. Under the controlled neuroinflammatory environment of EAE, Epstein et al. demonstrated that myelin uptake is dependent on receptor-mediated endocytosis, with evidence of myelin lamellae binding to the coated pits of macrophages, where a high concentration of ligand-receptor binding interaction is prevalent prior to endocytosis [68]. During the pathogenesis of MS, several receptors are expressed on macrophages/microglia that may be involved in the uptake of myelin, namely Fc receptors, complement receptors (CR), and scavenger receptors (SR) [69,70,71,72]. A pioneering study by Ulvestad et al. demonstrated that phagocytic cells in the parenchyma and perivascular region of active MS lesions strongly expressed Fc receptors (FcR), FcRI, FcRII, and FcRIII, whereas microglia expressed less FcR in normal-appearing white matter (NAWM) [73]. The uptake of myelin is also based on the opsonization and epitope recognition by antibodies [74]. However, myelin-specific antibodies are not only found in MS patients but also present in the circulation of healthy subjects [75,76]. Another receptor responsible for myelin internalization is CR, as confirmed by Loveless et al., who discovered several phagocytic cells expressing CR in progressive MS lesions [77]. An active subtype, CR3, was observed to facilitate approximately 80% of myelin clearance, however without the presence of active complement, the myelin clearance rate dropped to 55-60% [72]. These results highlight how overactivated-CR3 can contribute to myelin clearance. Additionally, in a study that induced EAE in SR-A-/- mice, demyelination in the CNS and disease severity were significantly reduced compared to the wild-type control [78]. In the rim of chronic-active MS lesions, SR-A1/II was also found in foamy phagocytes and ramified microglia, suggesting receptor involvement in the early phase of myelin uptake and demyelination [71]. Therefore, understanding the function of specific microglial receptors during various stages of the disease may enable the modification of these receptors to be used as therapeutic strategy for increasing myelin debris clearance and promoting anti-inflammatory environment in the lesion sites.
Another receptor, MER tyrosine-protein kinase, MERTK, is a part of the TAM family of receptors and can regulate myelin phagocytosis in human monocyte-derived macrophages and microglia [79]. The TAM receptors consist of TYRO3, AXL, and MERTK with their known ligands, growth arrest-specific 6 (GAS6) and protein S [80,81]. The TAM family of receptor tyrosine kinases has been shown to play a role in cell proliferation and survival, regulation of the immune system, and phagocytosis of cells [82]. In a study by Binder et al., cuprizone-induced demyelination in GAS6-/- mice was more severe compared to wild-type mice [83]. Additionally, Weinger et al. identified that levels of soluble MERTK were higher in chronic-active MS lesions, whereas in chronic silent MS lesions, the level of soluble AXL was elevated compared to healthy controls [84]. Furthermore, elevated levels of soluble AXL and MERTK receptors were accompanied by low levels of GAS6 in MS lesions, resulting in the dysregulation of GAS6/TAM signaling and possibly, prolonged lesion activity [84]. These studies also imply that polymorphism in the genes of TAM receptors or their ligands may be associated with an increased risk of MS. In a candidate gene study conducted by Ma et al., 12 single nucleotide polymorphisms (SNPs) were found in the MERTK gene, which is associated with MS susceptibility [82]. In a supporting study, Shen et al. established that MERTK was required for activation of microglia, microglial phagocytosis, and remyelination [85]. A recent study showed that triggering receptors expressed on myeloid cells 2 (TREM2) was expressed in MS lesions and TREM2 on microglia facilitated myelin debris clearance in cuprizone-fed mice [86]. TREM2 activates downstream spleen tyrosine kinase (SYK) via phosphorylation of DNAX-activating protein of 12 kDa (DAP12) to promote microglia activation and phagocytosis of cellular debris [[87], For review see [88]]. Therefore, phagocytic activity may indeed regulate the effectiveness of myelin clearance to enable newly formed myelin to repair denuded axons.
An important transmembrane protein TMEM119 along with the purinergic receptor P2RY12 have been successfully used as markers to differentiate resident microglia from peripheral macrophages [89,90,91]. TMEM119 and P2RY12 are expressed in the population of homeostatic microglia but expression of the genes variably decrease at brain lesion sites of archival tissue from individuals that lived with MS or AD [92,93]. Moreover, Zrzavy et al. found a reduction in the microglial expression of P2RY12 in the NAWM but the gene was depleted in the active MS lesions, whereas the expression of TMEM119 decreased in NAWM and more notably as the lesion progressed, indicating there is a reduction of homeostatic signatures in microglia or alternately, lower numbers of microglia are present in brain lesions [93].
In the gray matter, the numbers of P2RY12+ TMEM119+ microglia in demyelinating lesions were similar to the normal-appearing gray matter (NAGM), possibly due to less stimulation from locally-generated cytokines, a consequence of fewer infiltrating lymphocytes as compared to inflammatory demyelinating white matter [94]. However, it was proposed that the morphological differences exhibited by microglial subtypes can be used to differentiate their unique characteristics at specific brain regions. In the white matter, the microglia displayed amoeboid and ramified phenotypes, whereas, in the gray matter, some microglia were rod-shaped [94]. The function of rod-shaped microglia remains elusive but synaptic stripping has been proposed [95,96], which may be one mechanism that drives the rate of demyelination throughout the gray matter. Since the white matter and gray matter microglia may express distinguishable phenotypes throughout brain lesions of individuals with MS, identifying specific microglial cell populations and their respective pathogenic roles during the disease course are important to determine potential targets for disease chronicity and progression.
In support of this rationale, transcriptomic analysis of microglia has revealed genes that were not only expressed at region-specific sites but also that were disease-specific [97]. The microglia isolated from the gray matter demonstrated elevated expression profiles of genes associated with the type I interferon response whereas white matter microglia had a higher expression of genes related to the nuclear factor kappa B (NF-κB) pathway [97]. These data suggest that there exist two separate immune regulatory mechanisms operative among these two microglial cell subtypes. Furthermore, microglia that reside in the NAWM of individuals that lived with MS were enriched with genes related to lipid metabolism, differentiation of foam cells, lysosomal, and other signaling pathways (ABHD2, LPL, ASAH1, CTSD, SCARB2). Whereas, microglia from NAGM were enriched with genes associated with glycolysis and metal ion homeostasis (ABCB6, SDC1, CCR2, LPAR6, SLC25A37) [97]. Interestingly, the homeostatic genes of microglia in MS NAWM and NAGM were not affected [97]. The findings imply lipid processing and iron metabolism pathways are disrupted early in microglia throughout NAWM and NAGM during MS pathogenesis. These data provide insights into which therapeutic targets could provide efficacy to limit ongoing slow-burning demyelinating lesions during MS progression.
Astrocyte activity in the evolution of the MS plaque
Astrocytes give rise to extensive branches which develop as fibrous foot processes attaching to the blood vessels or shape the uniform globule located around axons and synapses of neural cells [For review see [98]]. Given the distribution of astrocytes within the CNS, astrocytes play a prominent role in orchestrating the connection between the vascular system and neural function, which are associated with enhanced neuronal survival and promote synaptic plasticity by regulating neuronal circuit activity in response to metabolic and structural support [99,100]. Intriguingly, studies have shown that astrocytes are not only neuroprotective but can also be deleterious in certain neurological disorders [101,102]. Abnormal astrocytes have been found in abundance in post-mortem brain tissue from patients with MS, Alzheimer’s disease, Parkinson’s disease [102,103,104]. These studies suggest that astrocytes alter their function in response to neuropathological insults, especially under inflammatory conditions, which can transform neuroprotective “resting astrocytes” into neurotoxic “reactive astrocytes” [105].
It has been identified that astrocytic responses are modulated by canonical signaling pathways, such as IKK/NF-κB, a classical mechanism implicated in the neuroinflammation [106,107,108,109]. The NF-κB signaling pathway in astrocytes can be stimulated by various factors including pathogenic extracellular or cellular debris, reactive oxygen species (ROS), and pro-inflammatory cytokines such as TNF-α, IL-1β and IL-17 secreted from peripheral immune cells and resident microglia by activating on their toll-like receptors (TLRs) [108,110]. To expand these findings, Wheeler et al. found that the astrocytes of EAE-induced mice and MS patients had a reduced nuclear factor erythroid 2–related factor 2 (NRF2) expression and a higher MAFG transcription factor level, which promoted DNA methylation, inflammation in the CNS, and limits anti-inflammatory activity [111]. They also suggested that granulocyte–macrophage colony-stimulating factor (GM-CSF) secreted by pathogenic T cells might promote pro-inflammatory activity of astrocytes by amplifying the MAFG/MAT2α signaling pathway in EAE-induced mice and in individual living with MS [111]. In addition, previous studies indicated that reactive astrocyte toxicity was mediated by secreted proteins, including SPARC, C3, and lipocalin-2 reactive markers [102,112,113]. Surprisingly, these neurotoxic factors did not cause the apoptosis of oligodendrocytes within the inflammatory environment. This finding indicated that the fundamental toxic agent resulting in myelinated cell apoptosis and axonal injury had not been found [114]. However, the enrichment of apolipoprotein (APO)-E and APO-J in reactive astrocytes suggests that an altered lipid metabolism in astrocytes may mediate cell apoptosis during inflammation [114].
Astrogliosis-mediated synaptic phagocytosis could be a compensatory mechanism independent of microgliosis-dominant engulfment for maintaining CNS homeostasis [115,116]. Synaptic elimination can be achieved via multiple epithelial growth factors (EGF)-like domains 10 (MEGF10)/MERTK phagocytic signaling pathway in astrocytes. MEGF10/MERTK-mediated astrocytes have been observed to trim synapses, thus, promoting the precise structure of neural circuits and synaptic plasticity [115]. Moreover, in MEGF10-/- mouse models, elevated levels of neuronal apoptosis and a reduced level of astrocyte phagocytosis were observed, which suggest that astrocyte phagocytotic function can be modulated by the complement component 1q (C1q)/MEGF10 signaling pathway [115].
The development of single cell (sc)-RNA sequencing techniques, have uncovered significant diversity in astrocyte populations, with spatial and temporal differences under physiological and pathological stimuli, throughout the CNS [111,117]. Despite this technical advancement, several challenges have been identified in studies addressing the heterogeneity of astrocytes in health, aging and disease. One of the major hurdles is that only limited numbers of neuropathogenic astrocytes can be collected from CNS tissues for downstream cell signaling analysis. This is primarily due to the lack of reliable surface markers to distinguish astrocyte subpopulations, thereby, preventing any comprehensive exploration of astrocyte diversity. For example, glial fibrillary acidic protein (GFAP) which is considered as a classic marker of astrocytes has not been useful in identifying neurotoxic astrocytes isolated from brain and spinal cord in MS-like animal models, such as EAE [111]. Recent studies have focused on investigating the molecular characteristics of astrocytes at the level of DNA and mRNA, which may provide an alternative avenue to differentiate cell populations of interest during the course of neuroinflammatory and neurodegenerative diseases.
Recently, Clark and colleagues identified that the upregulation of the transcription factor X-box binding protein 1 (XBP1) can promote the frequency of astrocytic cell-derived proinflammatory mechanisms exhibited during EAE and MS [118,119]. XBP1 activation is involved in processes that lead to its mRNA splicing unconventionally when potentiated by the endonuclease inositol-requiring enzyme 1 (IRE1), expressing the potential to serve as an mRNA marker for pathogenic astrocytes in MS. However, XBP1 levels determined by 3’-prime based RNA sequencing techniques showed inconsistencies, highlighting the need to address technical issue of sc-RNA sequencing in regard to low sensitivities of the detection of potential genetic and transcriptomic markers. Improving the read depth and enriching targeted reads during RNA sequencing may be the approach to enhance the sensitivity. Clark et al. have established the FIND-seq protocol which enriches the population of rare astrocyte subtypes by specific DNA barcoded beads and captured by microfluidic encapsulation [118]. This innovative strategy significantly improves the detection of gene diversity of pathogenic astrocytes, in comparison of scDrop-seq [120] and Probe-seq techniques [121].
Types of MS lesions
Neuroinflammation damages the BBB and creates macroscopic plaques whereas neurodegeneration causes injury to neurons and their axonal extensions [1,122]. Mononuclear perivenular cuffing on the lesion and the infiltration into the adjacent white matter are also observed [24,123]. The infiltration of immune cells and activated phagocytic cells is often associated with the formation of active lesions. The activated microglial cells are commonly found at the edge of demyelinating lesions, periplaque white matter and NAWM whereas, macrophages are found in the center of active lesions [2,124]. This type of lesion is more common in patients suffering from acute or RRMS [125]. A large portion of these macrophages appears to exhibit a ‘foamy’ appearance due to their myelin-loaded cytoplasm [126]. Furthermore, some of these active lesions exhibited myelinating activity, with the presence of macrophages containing myelin degradation in their cytoplasm [127].
As individuals living with MS progresses through the disease, the frequency of lesions with mixed morphology of active and inactive characteristics increases. This heterogeneity, also known as slowly expanding lesions, has centers containing an inactive demyelinated site filled with myelin debris, surrounded by activated macrophage and microglia around the rim and axonal injury observed in the active rim [128,129]. The slow expansion on these rims reflects ongoing demyelinating activity [65], whilst in patients with disease duration of more than 15 years or who have been diagnosed with progressive MS, inactive lesions are dominant [125]. In chronic lesions, demyelination, reactive gliosis, and the presence of dense fibrillary scar tissue can be observed between the transected axon space [103,130]. Furthermore, ongoing axonal damage can be identified within inactive lesions, highlighted by the disruption of the axonal transport [131]. Remyelination plaques are observed throughout all stages of MS, deemed shadow plaques, whereby axons are wrapped with new myelin sheaths. However, in chronic stages of MS, even though new myelin is present, these axons are still prone to damage due to variations of thicknesses between the inner and outer sheaths, specifically the thinner inner sheaths [132,133,134].
Interrogation of archived brain tissue derived from individuals who lived with SPMS has revealed the presence of B cell-like follicles in the meninges and the perivascular space, suggesting the possibility of trapped immune cells within the CNS after MS relapses, in transition into progressive stages [135]. Compartmentalized inflammation in the progressive stage of MS is associated with cortical demyelination, slow expanding white matter lesions, diffuse injury in NAMW, and gray matter demyelination [[125,135,136,137], for review see [138]]. These data may suggest that during progressive stages of MS, a requirement for future therapeutics, is to reach inflammatory sites located behind the repaired BBB at an appropriate dose, to resolve inflammation within the CNS.
Biomarkers of MS
Currently, there are limited biomarkers available to predict MS progression. One of the most highly researched areas of MS diagnostics need to include the elucidation of novel biomarkers that can clearly identify MS progression early for clinical management and to inform therapeutic efficacy [139,140,141,142].
Current and developing molecular biomarkers
Oligoclonal bands
In MS patients, oligoclonal bands (OCBs) are used as molecular biomarkers for diagnosis and prognosis [For review see [143]]. OCBs consist of immunoglobulin G (IgG) and immunoglobulin M (IgM) produced intrathecally by plasma cells in the CNS [For review see [144]]. Their identification in cerebrospinal fluid (CSF) samples accompanied with paired blood sera is conducted to demonstrate intrathecal antibody production from differentiated B lymphocytes [145,146]. Although CSF-specific OCBs can be detected in more than 95% of MS patients [For review see [147]], the presence of OCBs in the CSF is often correlated with the conversion from clinically isolated syndrome (CIS) to the onset of MS [148]. Furthermore, CSF OCBs are not unique to MS and the diagnosis still requires exclusion of other infectious and autoimmune diseases such as polyneuritis and optic neuritis [149,150]. Thus, CSF is the best representation of intrathecal CNS integrity but to obtain CSF, an invasive lumbar puncture is needed to be carried out [151,152]. Hence, improved diagnostic biomarkers with clinical assaying as well as advanced specificity are urgently required.
Neurofilament light chain
Neurofilaments are integral structural components of the neuronal cytoskeleton, composed of three subunits: heavy chain (NfH), medium chain (NfM), and light chain (NfL) [For review see [153]]. They are found in axons, especially in long projection axons, and they contribute to the axonal volume and mechanical strength [154,155,156]. Both NfL and NfH levels were shown to be elevated in the CSF of RRMS and progressive patients [157,158,159]. However, the role of NfH as a biomarker for MS progression is underrepresented in biomarkers studies than NfL which has a higher sensitivity in distinguishing between control and MS patients than NfH [160,161]. Recently, investigators have assessed the potential of neurofilament light chain (NfL) as a potential diagnostic and prognostic biomarker for MS. NfL is the most abundant subunit, it is released from injured axons and becomes soluble in the CSF and serum [For review see [162]]. Neurofilaments are also released into the circulation during normal aging [163] but when there is axonal injury, a larger quantity of NfL is released into the CSF and blood [For review see [164]]. The extraction of CSF for NfL quantification requires invasive lumbar puncture but with the development of a highly sensitive immunoassay such as the Simoa® assay, the detection of NfL at femtomolar levels in the serum of MS patients is made possible and may assist in the clinical interpretation of MS progression [165,166,167].
Despite controversial relevance in neurological progression, recent clinical studies reported higher serum NfL levels in MS patients than in healthy individuals in relation to disease progression potentially highlighting the detection of NfL levels as an ancillary diagnostic tool for MRI-detected lesions [168,169]. The increase in serum NfL was also shown to be associated with the loss of brain and spinal cord volume [168]. Experimentally, NfL levels are a robust detection marker of ascending paralysis at 18 days post-EAE immunization, whereby the NfL level increased 100-fold higher than the baseline level of healthy mice [170]. Malmeström et al. observed the highest level of NfL during acute relapses in RRMS patients but the level declined within three months [158]. Furthermore, Salzer et al. discovered that RRMS patients with CSF NfL levels higher than 386 ng/L were more likely to convert to the secondary progressive phase of the disease compared to patients with NfL levels lower than 60 ng/L [171]. However, the change in the level of NfL and its association with disease progression has been inconsistent [For review see [172]]. In some studies, the NfL level of progressive MS patients is higher compared to RRMS patients [159,169,173] whereas others reported that the NfL level of progressive MS patients is lower than RRMS [174,175]. Most of the studies found that there was no significant difference in NfL levels between RRMS and progressive MS groups [141,176,177]. Therefore, more studies are required to examine the change in NfL levels in terms of MS progression.
Further experimental evidence identifying the potential clinical activity for NfL levels during therapeutic intervention included the DMTs, glatiramer acetate, which resulted in a decrease of serum NfL levels by 81% compared to untreated EAE-induced mice [170]. These results indicate that NfL levels may serve as a prognostic marker during therapeutic intervention. However, Aharoni et al. detected that EAE-induced by myelin proteolipid protein (PLP)-immunization compared to myelin oligodendrocyte glycoprotein (MOG)35-55 displayed lower NfL levels at the same time point of clinical progression [170], suggesting that different myelin peptides induce variable neurodegenerative change, potentially providing difficulty to set NfL limits for different MS histopathologically characterized lesions.
NfL can be safely, easily, and objectively measured, it is sensitive to neuroaxonal injury, and the level changes depending on the severity of the disease, making it suitable as a biomarker for neurodegenerative process [139,178]. However, a major clinical disadvantage of using serum NfL levels as a biomarker is that the levels do not distinguish MS from other neurodegenerative diseases such as amyotrophic lateral sclerosis (ALS) and Alzheimer’s disease, which also exhibit elevated NfL serum and CSF levels [179,180,181]. Moreover, increases in CSF NfL levels can also be present in healthy subjects with increasing age as shown by several clinical studies [163,182]. Indeed healthy participants enrolled in a study to assess NfL levels between the ages of 18-70 years old displayed increased levels at a rate of around 2.2% per year of age [169]. Therefore, a better standardization, specific to people living with MS that demonstrate neuronal tissue loss, (taking into consideration age, sex, and other inclusion criteria), requires reform to validate serum NfL and CSF NfL over the course of disease progression. Controversially, these criteria also need to take into account that some studies observing NfL level ranges during MS often overlap with the ranges of NfL concentration in the control groups assessed [For review see [183]], suggesting that there may exist a limited window of predictive efficacy for this biomarker.
Chitinase-3-like-1
Chitinase-3-like-1 (CHI3L1) protein has also emerged as a potential biomarker for MS and its expression is detected in active demyelinating lesions [184,185]. It is expressed mainly by reactive astrocytes in the CNS, with its expression upregulated during inflammation with gliosis [142]. The induction of its expression has been suggested to result from hyper-activated macrophages and microglia that produce inflammatory mediators that heighten CHI3L1 expression of astrocytes and further stimulate triggering receptors expressed on myeloid cells 2 (TREM2) [186]. An in vitro study utilizing the administration of CHI3L1 to cortical neurons exhibited neuronal function impairment, thus, suggesting its neurotoxic properties [187]. The exact role of CHI3L1 requires further elucidation, but it is undeniably expressed within inflammatory events throughout the CNS, and thus could be considered as a surrogate biomarker that is indicative of MS microglia activity upon neuroinflammation in MS.
Elevated levels of CHI3L1 in CSF have been observed in CIS, RRMS, and progressive patients [142,186,188]. Patients progressing from CIS to RRMS experienced an increase in levels of CHI3L1 present in the CSF [142,189]. In RRMS, the expression of CHI3L1 correlated with loss of brain volume and advancement of disease activity [190]. However, another study indicated the elevated level of CHI3L1 is significantly related to the reduced cervical spinal cord volume but not to brain volume [188]. The controversy still surrounds whether CHI3L1 levels could be detected either in CSF or serum to best reflect the disease course. The levels of CHI3L1 in MS patients were usually increased in the CSF but another study observed the increased serum levels of CHI3L1 in progressive MS patients [191]. This discrepancy could be explained by the different assays used to measure these levels [142,191]. Surprisingly, in the study by Cantó et al., there was no significant difference between detected CHI3L1 plasma levels in the remission and relapsing phase [191]. Nonetheless, studies have observed a correlation between CHI3L1 levels and NfL levels in the CSF, which were stronger in RRMS patients compared to SPMS and primary progressive MS (PPMS), further contributing to the debate whether CHI3L1 is a suitable biomarker for progressive MS [192]. This study by Gil-Perotin et al. indicated increased values of CHI3L1 were more prominent in progressive MS patients, compared to NfL which was more prominent in relapsing MS patients [192].
However, utilizing CHI3L1 still requires a lumbar puncture, which is invasive to the patient and limits its clinical utility. Its expression like NfL, has also been detected in other diseases such as neuromyelitis optica [193] and Alzheimer’s disease [194], therefore it would not be suitable as a stand-alone biomarker, rather one that can be used alongside MRI to assess microstructural changes and diagnose the ongoing neurodegeneration of MS in patients. Further study is required to assess the role of CHI3L1 in chronic stages of MS to support the current promising results indicating the potential of CHI3L1 as a biomarker for neuroinflammation in MS.
Imaging diagnostics as biomarkers
Magnetic resonance imaging
MRI is considered the gold standard for imaging diagnostics biomarkers in MS and a staple in diagnosing and identifying MS progression. The most clinically advantageous diagnostic measure for using MRI is the visualization of brain atrophy and neural tissue loss, commonly utilized to assess progression in MS patients. However, brain atrophy is not just limited to lesioned areas but is also visible in regions of NAWM [195,196]. An effective measurement to assess brain atrophy is the ventricular CSF (vCSF), which reflects the change in the overall volume of the brain [197]. It provides robust data as vCSF is more commonly utilized across different MRI protocols and thus could possibly be the universal indicator of brain pathology in the clinical assessment of patients [197]. Nonetheless, brain atrophy changes have been observed to have a strong correlation with increased disability through the assessment of the objective expanded disability status scale (EDSS). Eijlers et al. assessed the annual deep gray matter and cortical atrophy rates in individuals with MS and found a strong correlation between brain atrophy and cognitive decline [198]. However, there are some factors that need to be considered that could affect brain atrophy measurements within the MS patient. For instance, the increase in brain volume leading to increase atrophy also occurs as the result of edema during inflammation [199,200]. Consideration must also be made where brain atrophy can be affected by factors such as age [201,202].
Although advanced MRI techniques such as diffusion tensor imaging-MRI (DTI-MRI) and magnetization transfer-MRI diagnosis are increasingly being used in MS research, they are still rarely employed in clinical practice to diagnose MS [143,203,204]. Fluid-attenuated inversion recovery (FLAIR), T2-weighted MRI, and post-gadolinium T1-weighted scanning are the current mainstream diagnostic tools for MS [205,206,207]. T2-hyperintense lesions in MS patients are normally found in periventricular, juxtacortical, infratentorial, or spinal cord regions [208]. However, T2-hyperintense lesions lack specificity to demonstrate the severity that incorporate the pathologic processes occurring in the lesions such as inflammation, de/remyelination, gliosis, or axonal damage [For review see [209]]. Furthermore, T2 lesions show a weak correlation with clinical status as measured by the EDSS [210,211,212]. Nevertheless, T2-weighted MRI could be a useful tool to reflect drug efficacy in clinical trials [213,214,215]. For example, Radue et al. identified that treating patients with fingolimod significantly decreased their T2 lesion volume compared to baseline [213].
In the T1-weighted pulse sequence, lipid-predominant structures such as myelin are displayed as bright spots whereas water-predominant structures such as cortex are shown as dark anatomical regions. Indeed it has been recently demonstrated that demyelination and axonal degeneration reduced lipid content and increased the water content, resulting in the formation of hypointense signal areas on the T1 images [216]. Gadolinium-enhancing lesions are often associated with T1 hypo-intensity or “black holes”, which may indicate the combination of edema and demyelination [217,218,219]. Within 6 to 12 months, acute T1-hypointense lesions associated with gadolinium-enhancement either convert back to T1-isointense lesions or remain as chronic black holes [220,221,222]. DMTs such as fingolimod and glatiramer acetate have been shown to slow down the rate of disease development and repress the conversion from acute lesions to chronic black holes [223,224]. Compared to the progressive form of MS, gadolinium enhancement is less frequently seen in RRMS, that may correlate with the changeable immunoregulation of the innate and adaptive immune responses during the disease course [225].
However, progression maybe best monitored by the accumulation of extracellular iron. Dal-Bianco et al. suggested that gadolinium enhancement may not be able to reflect the characteristics of lesions robustly during both acute and chronic periods of MS [124]. Instead, utilizing iron imaging with 7-T MRI could be a feasible approach that may provide a more accurate depiction of particular lesions. From observation, there was reduced iron visibility in areas surrounding NAWM compared to early active lesions, indicating the stage where gadolinium enhancement is visible. Subsequently, iron accumulation in the CNS led to the formation of nodular iron spheroids, finally developing into FLAIR-hyperintense iron rims of microglia and macrophages in smoldering lesions, where gadolinium enhancement is barely detectable [226,227]. Iron-rimmed lesions were deemed more destructive and indicative of neurodegenerative and disease progression, as evidenced by increasing T1 hypointensity compared to non-iron-rimed lesions and histological quantification of axonal damage through axonal spheroids, microglia activation and Wallerian degeneration on areas correlating to these FLAIR-hyperintense regions [124]. In this longitudinal study of 33 MS patients up to 7 years, RRMS patients had significantly higher iron-rimmed lesions (17.8%) than SPMS (7.2%) [124]. Interestingly, there are studies that showed contrasting results as the consequence of variable clinical characteristics of patients, potential therapeutics that the patient was on and whether this was done in vivo or conducted on post-mortem samples [125,228]. However, utilizing iron imaging with 7-T MRI to observe disease progression still requires more validation, especially with a more consistent and frequent follow-up on patients.
Diffusion tensor imaging
DTI-MRI is principally based on tracking the movement of water within the CNS tissue and providing connectomics and network analysis of neural fibers. The main DTI parameters are fractional anisotropy (FA), axial diffusivity (AD), radial diffusivity (RD), mean diffusivity (MD), and apparent diffusion coefficient (ADC) [For review see [229]]. In MS patients, usually, the FA and AD are decreased whereas the RD and MD are increased compared to healthy controls [For review see [229]]. This is related to water mobility which is negatively correlated with compact tissue integrity such as the myelin [For review see [229]].
Axons facilitate longitudinal movements of water with upon injury suggested to cause a decrease in AD [230]. Nishioka et al. discovered that AD was reduced in optic nerves of EAE-induced mice 4-8 weeks after the induction of the disease, along with reduced FA and increased RD [231]. Interestingly, a study by Naismith et al. presented evidence of decreased AD in individuals with acute optic neuritis, however after a one year follow-up assessment, AD increased as retinal ganglion cells possibly demonstrated recovery or repair [232]. Nevertheless, Budde et al. indicated that AD is a more specific marker of axonal damage in the EAE-induced mouse spinal cord compared to FA metrics [233]. However, Andersen et al. also found that in the corpus callosum body of secondary progressive MS patients, there was a reduction in FA and an increase in RD [234]. The discrepancy in the change of DTI parameters has been attributed to the variable array of tissue samples used.
Thus, to identify whether there is a correlation between DTI-MRI metrics and another promising biomarker NfL, Saraste et al. indicated an increase in serum NfL level accompanied by the variation in DTI-MRI metrics, where a decrease in FA was observed along with an increase in RD in NAWM in MS patients [181]. DTI-MRI techniques can also describe 3D neural fiber tracts by tomography, which along with quantitative analysis of these DTI measurements, greatly enriched the interpretation of microstructural white matter damage. Moreover, DTI-MRI in combination with serum NfL level analysis could be a valuable monitoring tool in assessing the degree of the developing neurodegenerative processes during MS.
Proton magnetic resonance spectroscopy
Proton magnetic resonance spectroscopy (1H-MRS) is often used to investigate neurological disease and has a similar data acquisition process to conventional MRI with only a few additional steps incorporated during the pre-scan [For review see [235]]. These pre-steps include improving the homogeneity in the magnetic field or “shimming”, suppressing the water signal, and choosing the appropriate MRS parameters or techniques [For review see [236]]. The principle underlying 1H-MRS is the signal detected from hydrogen protons utilized to measure the concentration of the metabolites in the CNS tissues of interest [For review see [235]]. In MS, the three metabolites of interest are creatine (Crn), N-acetyl aspartate (NAA), and choline (Cho). Crn is the marker of energy metabolism in the brain and because of its stability, other metabolites are often shown as a ratio relative to Crn [237,238]. However, altered Crn levels in MS lesions have been detected by 1H-MRS [239,240,241,242]. Consequently, expressing other metabolites as a ratio relative to Crn may introduce more variability into the obtained measurements if the level of Crn is not stable [243,244]. In the MR spectrum, the peak of NAA can be used to analyze axonal integrity while the peak of choline can be used to assess the cell-membrane metabolism [[10], for review see [245]]. A lower peak of NAA in white matter signifies axonal damage whereas a higher Cho peak is interpreted as higher membrane turnover, suggesting the occurrence of gliosis, demyelination and remyelination events [10,246].
A decrease in the ratio of NAA/Crn in a given region of the brain indicates disrupted integrity of the tissue, thus, has been suggested as a potential marker for neuroaxonal injury [247,248]. Aboul-Enein et al. observed a significantly reduced NAA/Crn ratio through 1H-MRS in patients with SPMS compared to RRMS patients in NAWM [249]. However, interestingly, this study observed no significant changes in NAA levels of RRMS patients compared to healthy individuals. In contrast, other studies have observed a decrease in this same parameter in NAWM and throughout the whole brain [250,251]. In addition, increases in Cho/Crn ratios in lesions from patients with RRMS and SPMS have been observed [252,253,254]. However, some studies refute this, observing a decrease in Cho/Crn ratio [255,256]. The conflicting studies indicate that the different stages of MS and different regions being measured may affect the level of metabolites detected using 1H-MRS. Furthermore, the detection of limited metabolites through MRS does not reflect the full heterogeneity of MS lesions, thus, could be utilized in support of other imaging biomarkers [249]. Additionally, when performing MRS, tissue or adjacent tissue with high susceptibility differences may result in the appearance of artifacts due to an non-uniform field [For review see [235]].
Optical coherence tomography
The vulnerability of the retinal ganglion cells and axons in MS leads to impairment of vision as a common symptom exhibited in MS patients. The onset of these visual symptoms could manifest as a result of optic neuritis (ON), with 20% of these patients going on to develop MS, or as a result of lesions in their visual pathway [For review see [257]]. Although the exact mechanisms that bring about these degenerative outcomes require further elucidation, it is evident that there are morphological changes in retinal ganglion cells from the visual pathway as MS progresses [258,259]. These neurons and thin axons can be visualized through optical coherence tomography (OCT) imaging which utilizes infrared light to create cross-sections to form a 3D image of the retinal layers. It is widely used to quantify the peripapillary retinal nerve fiber layer (pRNFL) which comprises ganglion cell axons before they coalesce to form the optic nerve [260]. Another measurement utilized clinically is the ganglion-cell-internal plexiform layer (GCIP), which is the combination of the ganglion cell layer and the inner plexiform layer but is difficult to distinguish via imaging [261]. The accelerated rate of GCIP thinning was evident in early MS patients with ON, making GCIP a suitable marker for prognosis [262].
As a part of the CNS, the retina has the unique anatomical characteristic of its axons commencing from the anterior retinal nerve fiber layer being unmyelinated, allowing visualization of axonal degeneration without factoring in the myelin membrane disruption [263,264]. The thinning of pRNFL and GCIP has been associated with neurodegeneration and reduction in ganglion cells compared to a healthy person or during normal aging [102]. Studies have identified a decrease in pRNFL layer thickness in MS patients with or without ON, compared to healthy individuals [265,266,267]. In patients with no pre-existing ON, there was a progressive thickness decline in the pRNFL layer of 6.7% compared to 0.5% in healthy controls for a 3-year follow-up [268]. Similarly, Garcia-Martin et al. performed a 5-year follow-up of pRNFL thickness in RRMS patients with and without history of ON and observed an annual decrease in the mean thickness of 1.64 μm of pRNFL, as opposed to the annual decrease of 0.32 μm measured in healthy controls, depicting that pRNFL in MS patients decreased on average 5-times faster than the healthy individual [269]. While in the same individuals GCIP thickness decreased twice as fast in the MS patients compared to the healthy control [269]. These studies were limited largely to only include RRMS patients, with a limited number of studies looking at OCT as an imaging biomarker in progressive MS patients. Hence, further investigations in a randomized control design should be explored.
Although OCT in a non-invasive manner can measure and monitor the axonal injury, there are some considerations that need to be clarified. Firstly, these studies have been conducted on defined populations and cannot be extrapolated to other ethnicities due to their differences in pRNFL levels and levels of thinning [270]. This could result from the prevalence of MS in different ethnicities, but further research is required to understand how epidemiological factors affect their morphological differences. Another factor with OCT is the variability from different software algorithms as there are different versions of OCT imaging. Older studies mainly used time-domain OCT which assesses the thickness of RNFL while current studies utilize spectral-domain which offers higher resolution and allows the use of automated software algorithms to separate the layers of the retina [271,272,273]. Recently, more studies have used OCT-angiography which assesses the density of the retinal microvasculature [274,275], reducing the variability generated by technical errors. This suggests that the clinical use of OCT could be paired with other measures such as MRI assessments of brain atrophy and volume, visual acuity tests, or in correlation with EDSS score for disease progression. However, the association of pRNFL with these factors requires further extrapolation as studies show no correlation between these factors [276]. pRNFLs decrease in thickness is also observed in other neurodegenerative diseases such as Alzheimer’s and Parkinson’s disease [277,278,279], therefore it may be insufficient to be a specific diagnostic biomarker for MS but can be used as one to track neurodegeneration and monitor the disease progression with treatment.
Positron emission tomography scan
Positron emission tomography (PET) imaging allows for non-invasive assessment of MS pathological activities using radioligands that target the tissue or molecules driving lesional expansion. PET may be combined with tomography imaging in the presence of the 18 kDa translocator protein (TSPO) biomarker to detect microglial activation in MS, which provides an avenue to explore the pathophysiological outcomes of slow-burning lesions [280,281]. TSPO is an outer mitochondrial membrane protein and high expression of TSPO is correlated with neuroinflammation and density of activated microglia [225,282,283]. The radioligands that have been used to target TSPO are [11C]PK11195 [284], [11C]PBR28 [285], [18F]FEPPA [286], and [11C]ER176 [287].
In a study conducted by Rissanen et al., an increase in binding of [11C]PK11195 in lesions and NAWM of SPMS patients was reported, which is associated with ongoing microglial activity [288]. However, [11C]PK11195 has poor BBB permeability and high non-specific binding while other tracers displayed the heterogeneous binding to TSPO [For review see [289]]. Consequently, specific targets that can bind to the radiotracers need to be investigated. Examples of other targets currently under investigational trials include the cannabinoid receptor 2, purinergic P2X7 receptor, and MerTK [For review see [290]]. Another limitation is that TSPO can also be expressed in activated astrocytes and endothelial cells [283], which decreases the specificity of evolving microglial activity. Furthermore, Nutma et al. discovered that in brain tissue from patients with MS, the increase in TSPO signal is associated with a higher density of microglia and astrocytes [280] but not the activation state of these cells as seen in the rodent studies [225,291]. This means the interpretation of PET signals using TSPO depends on the design of the studies.
Thioflavin T derivatives, such as Pittsburgh Compound-B (PiB), have also been used in PET imaging to detect amyloid pathology in Alzheimer's patients due to its binding affinity for myelin, making such tracers potentially useful in assessing demyelination and even remyelination in MS [292,293]. Stankoff et al. presented evidence that the uptake of [11C]PiB was higher in NAWM compared to gray matter and there was a lack of [11C]PiB uptake in the lesion sites of RRMS patients [294]. Similarly, Bodini et al. demonstrated dynamic changes of [11C]PiB binding in MS lesions over time using PET imaging, suggesting it may demonstrate remyelination within MS lesions [293]. However, the tracers are derivatives modified from Aβ peptide tracers, where Aβ trafficking can influence the PET signals in white matter, thus influencing these measurements [295,296]. Pietroboni et al. suggested that these signals may not be derived from within white matter but from Aβ present in the CSF [296].
Potential MS treatments
The current unmet medical need in treating progressive MS is limited due to CNS-specific pathological lesions, separated in time and space with low efficacy of targeted agents to cross the BBB, especially during the secondary progressive phase whereby the BBB reseals. Once, therapeutics can reach the CNS compartment with appropriate bioavailability, they must achieve efficacy by either limiting pathogenetic mechanisms that propagate neurodegeneration or potentiate neurorepair. As such, phagocytosis of myelin debris which may contain inhibitory factors to remyelination could be key for improving neurorepair and limiting neurodegeneration during progressive MS. With the development of cellular therapies, the transplantable cells may remodel the inhibitory and inflammatory endogenous environment that ensues during MS. These novel therapeutic strategies may be designed to target ECM deposited during the evolution of pathogenic lesions or alternatively to cellular-based therapies targeting immune cells, glial cells and neuronal responses that may initiate neurorepair.
Bruton’s Tyrosine Kinase Inhibitors: An exciting new development in clinical trials for people living with progressive MS
Recent developments in neurotherapeutic outcomes during secondary and primary progressive MS have emanated out of efficacy studies using Bruton’s tyrosine kinase (BTK) inhibitors to limit B cell development and signaling [297,298]. The clinical rationale for utilizing BTK inhibitors in MS therapeutics relates to the changing conceptual focus in MS pathogenesis over the last decade, whereby B cells associated with intrathecal follicle-like structures, may govern the brain atrophy associated with progressive MS [299]. Moreover, the efficacious clinical use in CD20 monoclonal antibody biologicals such as ocrelizumab and rituximab that demonstrate B cell reduction may limit MS progression [300,301], suggesting that B cells may propagate neurodegenerative changes and are central to MS pathogenesis.
There exists a complexity in the innate and adaptive immune interplay particularly in the CNS during chronic inflammation [For review see [302]]. B cells have a unique capacity to signal a cycle of chronic inflammation through unique cytokine and chemokine mechanisms that can involve B lymphocyte associated factor (BAFF) and a proliferation-inducing ligand (APRIL) to regulate astrocytic responsiveness [303], or alternatively/simultaneously through the activation (constitutively or induced) of the BTK enzyme, regulate microglial cell-specific Fc receptor activation, critical for innate immune system demyelinating outcomes [304]. New generation of BTK inhibitors such as tolebrutinib have been identified in phase 2b safety and efficacy studies to regulate the activity of gadolinium-enhancing lesions over a 12-week treatment period in a cross-over trial design [298] clearly demonstrating reduction in acute inflammation during relapse in MS. However, there has been some development with the possible clinical management of progressive MS whereby tolebrutinib is currently being assessed over a 12-week period for PPMS when compared with ocrelizumab treatment (Clinical Trial Identifier NCT04544449) or a more protracted 6-month period in both primary and secondary progressive MS when compared to placebo (NCT04458051 and NCT04411641 respectively). Primary and secondary outcome measures do include brain volume imaging and neurodegenerative molecular biomarkers from baseline up to the end of study and may provide insights into pathogenic mechanisms that drive the microglial expanding lesion with interactions of the active intrathecal B cell-like follicles, or indeed if this is totally independent of lymphocyte activity during demyelination [305].
Hyaluronan and chondroitin sulfate proteoglycans
The ECM has been shown to play an important role in leukocyte activation and infiltration into the CNS. The increase in the production of hyaluronan in the ECM has been observed in both acute and chronic inflammatory sites, especially in the demyelinated lesions of MS and EAE [306]. Winkler et al. identified that hyaluronan binds to its receptor, CD44 on CNS endothelial cells to facilitate the migration of T lymphocytes into the CNS during EAE pathogenesis [307]. In support of this evidence, Kuipers et al. found that treatment of EAE-induced mice with 4-methylumbelliferone (4-MU), an inhibitor of hyaluronan production, limited T lymphocyte migration into the CNS parenchyma and reduced astrogliosis associated with disease progression [308]. They also demonstrated that 4-MU administration decreased the severity of EAE and promoted the differentiation of T lymphocytes to a Th2 phenotype and forkhead box P3 (FOXP3)+ regulatory T lymphocytes (Tregs) [308]. In addition to facilitating leukocyte migration, a high molecular weight (HMW) form of hyaluronan was produced by astrocytes in chronic demyelinated lesions of EAE-induced mice, and both HWM hyaluronan and hyaluronan fragments inhibited the maturation of oligodendrocyte progenitor cells (OPCs) into myelinated oligodendrocytes in the lysolecithin (a neurotoxicant)-induced demyelinated sites [306,309]. Therefore, inhibiting the synthesis of hyaluronan and bioactive hyaluronan fragments may limit lymphocyte-mediated inflammation and promote remyelination in MS.
Another component of the ECM includes chondroitin sulfate proteoglycans (CSPGs), which play a central role in the formation of the glial scars, can regulate lymphocyte migratory responses and remyelination potential with profound effects on axonal regeneration [310,311,312]. CSPG has been observed to be expressed in brain sections of MS patients and the EAE-induced animal model [312]. In a study conducted by Stephenson et al., CSPG expression was found to be elevated in the perivascular spaces of spinal cords during EAE, whilst, decreased production of CSPG with fluorosamine treatment in this animal model led to inhibited leukocyte infiltration [312]. One of the degradation products of CSPG cleaved through the activity of chondroitinase ABC (chABC), is chondroitin sulfate proteoglycans-disaccharide (CSPG-DS). This cleaved product has also been shown by [313] to limit T cell migration and cytokine production during the course of EAE. Additionally, Zhou et al. also found that CSPG-DS prevented EAE onset and limited the disease progression [314]. These studies showed that reducing the production of CSPG using fluorosamine or degrading CSPG using chABC prevented T lymphocyte infiltration into the brain parenchyma, which reduced the inflammation in the CNS [314,315]. Furthermore, treatment with chABC reduced the misdirected growth of axons allowing for regeneration in rats following nerve transection [316]. In this rat model of spinal cord injury (SCI), degrading chondroitin sulfate glycosaminoglycan chain with chABC facilitated the regeneration of the descending corticospinal tract axons with functional recovery observed [317]. This functional recovery was also witnessed in a primate model of SCI treated with chondroitinase, where Rosenzweig et al. noted induced corticospinal axon growth in the gray matter [318].
Additionally, CPSGs have been shown to negatively influence the differentiation of OPCs in pathological conditions and limit remyelination during inflammatory demyelination. Siebert and Osterhout discovered that CSPG inhibited neurite outgrowth along with the differentiation of OPCs in vitro but treatment with chABC reversed the inhibition [319]. In support of these findings, Lau et al. showed that decreasing the CSPG production with xyloside promoted remyelination in lysolecithin-treated mice [311]. Therefore, the inhibition of CSPG could attenuate the inflammatory environment to promote remyelination in an animal model of MS. However, clinically translating the use of chABC may present some challenges, such as its thermal sensitivity for its enzymatic activity that has been shown to quickly decrease within three to five days at 37 °C [320]. Consequently, this has led to repeated delivery of chABC in animal models of SCI to the lesion sites to reach the deep regions of the spinal cord to observe therapeutic effects [321]. To try to overcome the thermal sensitivity, Lee et al. employed another method through thermostabilized chABC and a hydrogel-microtube scaffold delivery system to provide sustained release of chABC locally in vivo in a rat model of SCI [320]. More studies need to be performed to investigate effective methods of blocking CSPG production as it can provide future therapeutic benefits for MS patients.
In progressive MS patients, the most common type of lesion is the slowly expanding lesion with a hypocellular demyelinated center [134]. The glial scar and the loss of brain volume need to be replaced with cells, which can be transplanted or sourced from endogenous cells. However, aging affects the proliferation and differentiation capability of stem cells [322,323]. Since the majority of individuals living with progressive MS are usually of old age and only a few cells can be derived from endogenous stem cells, transplantation of inducible pluripotent stem cells (iPSCs) would be preferred. However, the glial scar that made up the lesion needs to be broken down first. Hyaluronan and CSPG are present in the glial scar as inhibitory factors. Thus, removal of CPSG and inhibition of hyaluronan, especially the high molecular weight form, can ameliorate scar formation by rendering the ECM more responsive to neurorepair and remyelination.
Cellular-based therapeutic strategies
Cell-based therapies may be a promising approach to support the ongoing efforts of overcoming the lack of effectiveness of DMTs in patients with progressive MS. The concept of replacement of autoreactive and pathogenic cells and related output on signaling pathway regulation, are of increasing interest in the research of progressive MS, to eliminate autoreactive immune responses and enhance neurological recovery. Neural stem cells (NSCs) and autologous HSC-based transplantation has recently reached the clinical trial phase, opening the possibility of using cellular replacement as a regimen for MS patients.
Neural stem cells
NSCs distribute in neurogenic stem cell niches, specifically enriched in the subventricular zone (SVZ) adjacent to the lateral ventricle in the forebrain and the subgranular zone (SGZ) of the dentate gyrus (DG) interface in the hippocampus [For review see [324]]. As mentioned earlier, remyelination in anatomical regions of the brain undergoing neurodegeneration is central in the treatment of MS, and this process requires the participation of endogenous NSCs, which can migrate to specific regions and differentiate into mature oligodendrocytes, restoring impaired neural function [325,326]. NSCs may treat MS through the modification of the endogenous microenvironment converting from a neurotoxic to neurotrophic phenotype [327,328]. Moreover, transplanted NSCs may limit further damage to the site of injury by promoting cell replacement, immune regulation, nutritional support, and stimulating the differentiation of neural progenitor cells, alongside maintaining the CNS homeostasis and optimizing the nervous system [329,330].
A major problem in achieving neurorepair through NSC transplantation during MS is to resolve the pro-inflammatory microenvironment and repopulate the parenchymal functional cells at the lesion site. However, excessive and disorganized ECM, apoptotic cell debris, and pro-inflammatory cytokines can affect the viability, differentiation, and migration ability of NSCs to the lesion site [331,332,333]. At present, several studies have confirmed that different in vitro induction methods can enhance the effect of NSC transplantation in MS. Moore et al. identified that estrogen receptor beta (ERβ) agonists can be used to enhance oligodendrocyte differentiation in EAE and to improve the CNS myelin repair in mice along with improved clinical outcomes [334]. However, Imamura et al. showed in recent studies that Donepezil, an approved treatment for AD, induce the expression of myelin-related genes, and further stimulate the differentiation of NSC-derived from iPSCs into oligodendrocytes through the ER signaling pathway, thus further improving myelin regeneration in the CNS [335]. In addition, some metabolites found in the human body also regulate the effect of NSC transplantation. In vivo experiments also demonstrated that transplanted NSCs exerted anti-inflammatory action by scavenging succinate through the SUCNR1 signaling pathway, leading to the production of prostaglandin E2 [336]. Moreover, succinate has been shown to activate the SUCNR1/GPR91 signaling pathway in macrophages, promoting the polarization of macrophages to a pro-inflammatory phenotype and production of pro-inflammatory IL-1β [337]. Consequently, the uptake of succinate by NSCs resulted in the induction of prostaglandin E2-dependent anti-inflammatory effects and less succinate available to activate SUCNR1/GPR91 signaling pathway in macrophages [336]. When EAE-induced mice were transplanted with Sucnr1-/- NSCs, microglia failed to convert to an anti-inflammatory phenotype, and only a slight recovery of behavioral outcomes was observed [336].
Bone marrow-derived NSCs and those derived from the SVZ have been shown to exert almost the same therapeutic effects in the EAE preclinical models, and interestingly, the BM-derived NSCs have similar morphological characteristics and similar capability of differentiating into neurons and glial cells to SVZ-derived NSCs [338]. Xie et al. injected bone marrow-derived NSC-transfected with TGF-β1 into mice with EAE via the tail vein, and transduced bone marrow-derived NSC inhibited Th1 and Th17 populations, promoting the production of immunosuppression through Treg cells and cytokine IL-10 from the periphery, thereby transforming microglia from a classical to alternative pathway [339].
These results indicated that genetically modifying NSCs can be more effective in inhibiting clinical severity, inflammation, and demyelination in the CNS of mice. In addition, these investigations reported that the total number of neurons and oligodendrocytes in the CNS was significantly increased in the TGF-β1-transfected NSC-transplantation group compared with the control group injected with normal saline [339]. However, there was no significant difference between the two groups treated with non-transfected NSCs when compared with the transfected NSC-transplantation group. This suggests that TGF-β1 does not alter the proliferation and differentiation of NSCs, and thus the more indicative markers for genetic modification of stem cells should be further identified.
Demonstration of remyelination of the CNS in EAE-induced male mice and an increased number of CD4+CD25+FoxP3+ Treg were observed, following transplantation of human NSCs into the mice at the chronic stage of the disease [340]. Compared with the control group of mice induced with EAE, the neuroinflammatory response of mice treated with human NSC transplantation was significantly reduced [340]. Harris et al. evaluated the safety and tolerability of autologous bone marrow derived NSCs for the treatment of 20 patients with MS in a Phase I clinical trial [341]. In the follow-up, 24 months post-transplantation of 20 participants, no new lesions were found on the T2 MRI and no severe adverse events were reported, as the evidence of the safety and tolerability of transplanted autologous bone marrow-derived NSC transplantation for MS in the short term [341].
Autologous hematopoietic stem cell therapy (AHSCT)
HSC transplantation has been shown as a potential treatment for ameliorating neurological deficits by promoting neural regeneration and functional recovery [342,343]. The current methodologies for transplant include AHSC populations extracted from patients and reconstituted outside of patients' bodies, characterized by high mobilized capability and low autoreactivity. Recently, a randomized-controlled study (NCT00273364) reported the significant effect of nonmyeloablative HSCT on extending the time to disease progression in patients with RRMS, compared with conventional DMTs [344]. More importantly, no death occurred and no adverse events over non-hematopoietic toxicity grade 4 were observed, confirming the safety, feasibility, and durability of AHSCT on MS patients [344]. The low incidence of transplant-related adverse events may be contributed by the more specific candidate inclusion criteria. In the aging population, due to the concern of less effectiveness of HSCs with functional decline (decreased capability of self-renewal and pluripotency) and the high risk of mortality or complications resulting from AHSCT, MS participants under 60 years old and less than 5-year relapsing-remitting stage duration, are recruited in most ongoing AHSCT clinical trials.
Gene modification techniques applied to cells (especially stem cells) before cellular-based transplantation is an ideal strategy that enhances functional cell survival and promotes CNS regeneration in the model of neurodegenerative diseases [345,346,347]. Currently, lentivirus (LV)-modified HSCT has been examined in several clinical trials majorly targeting immune, neurological and genetic diseases such as human immunodeficiency virus (HIV) infection (NCT00002221), cerebral adrenoleukodystrophy (ALD) (NCT01896102), Krabbe Disease (NCT04693598), adenosine deaminase (ADA) deficiency (NCT01380990), X-linked severe combined immunodeficiency (SCID) (NCT03601286), and sickle cell disease (NCT02140554). Some debates continue about mutagenesis resulting from virus-carried genes integrated into HSCs. However, in the recent clinical trial that utilised by using gene therapy with HSCT for ALD, 88% of patients receiving genetically modified HSCT demonstrated stable long-term hematopoietic reconstitution with modified HSCT maintained in proportion to the patient's original immune lineage [348]. Additionally, X-linked SCID patients transplanted with autologous LV-transduced HSCs showed immune reconstitution and the treatment appeared to be safe [349]. Besides using viral vectors to genetically modify the HSCs, CRISPR-Cas9 is another gene-editing technology that was reported to be a safer alternative [350].
A signaling cascade that may govern neurodegenerative change within the CNS has been well-established to involve the inhibitory signaling cascade induced by myelin-associated inhibitory factors (MAIFs). These MAIFs include Nogo-A which has the strongest inhibiting effect on CNS neuronal and myelinated oligodendroglial lineage cells through binding to Nogo receptor 1 (NgR1) [For review see [351]]. NgR1 and its coreceptors transmit downstream signaling that involves RhoA/Rho-associated coiled-coil-forming kinases (ROCK) and CRMP2, that elicit profound inhibitory neurite outgrowth, axonal growth and can thereby limit synaptic plasticity [352,353]. Accordingly, the NgR ectodomain can be used as a decoy to recognize and bind to myelin debris that harbors the target antigen such as Nogo-A on their surfaces and further reduce the activation of the inhibitory downstream pathways related to axonal degeneration. NgR(310)ecto-Fc, the soluble decoy fusion protein, is capable of binding to MAIFs and driving the therapeutic effect on animal models of glaucoma and SCI [354,355]. Therefore, the NgR(310)ecto-Fc fusion decoy protein may be a plausible self-activating vector transduced in HSCs to re-establish the immune system, and could be expected to become a novel cell-based therapeutic for patients with immune-related neurodegenerative diseases.
HSCs can differentiate into various immune cells such as T cells, B cells, and macrophage [For review see [356]] and HSC-derived immune cells are capable of crossing into the CNS [357]. Using gene editing technology, HSCs can then be utilized as vehicles to deliver the NgR(310)ecto-Fc decoy protein from the periphery to the target lesions in the CNS. As mentioned previously, macrophages and microglia are capable of phagocytosing myelin debris but there seems to be insufficient clearance of this debris in patients with MS [358]. This myelin debris is well studied to be inhibitory to axonal repair and differentiation of OPCs to mature oligodendrocytes, which remyelinate the axons [359,360]. NgR(310)ecto-Fc may bind to Nogo-A concentrated in myelin debris and the Fc portion of the fusion protein can bind to the Fc receptor localised on the cell membranes of macrophages/microglia, facilitating the clearance of inhibitory myelin debris. Furthermore, NgR(310)ecto-Fc can also inhibit myelin-mediated axonal degeneration by blocking Nogo-A/NgR signalling [359]. Our recent data has demonstrated significant remyelination and axonal repair during EAE following transplantation with NgR(310)ecto-Fc-transduced HSCs [361].
2. Conclusion
The major cellular players in MS consist of T cells, B cells, macrophages, astrocytes, microglia and oligodendrocytes that undergo reactive changes when being exposed to pathological conditions in the CNS. Although diverse immunomodulatory DMTs are being investigated, they mainly target the T and B cells and aim to resolve inflammation during the acute stage of RRMS. Moreover, there are only a few approved DMTs for patients with progressive MS who suffered from permanent neuronal and behavioral dysfunction due to extensive demyelination and neurodegeneration. Many studies focus on the clearance of myelin debris and the removal of inhibitory substrates in the glial scar to promote neuroregeneration, prompting the adaptive immunity- and glia-mediated response to facilitate the neural repair process.
Histopathologically, acute demyelinating inflammatory lesions substantially developed to chronic-active and chronic-inactive plaques, and these chronic lesions are typically observed in the post-mortem tissue sections of SPMS patients. The distribution of immune and glial cell populations within chronic plaques in progressives MS is vastly different from acute lesions in RRMS. The presence of demyelinated axons and reactive gliosis from activated astrocytic and microglial interactions contribute to the formation of glial scars, which are observed in chronic MS plaques. Classical MS-like disease models including EAE and cuprizone toxin models have similar immunopathology and glial pathology with MS and these models are being used to investigate the complexity of cellular responses during neurodegeneration. Nonetheless, several limitations such as the insufficient manifestation of MS progression and pathophysiological hallmarks in EAE and cuprizone toxin models are still existing. Hence, a newly developed animal model needs to be investigated, particularly linking “inside-out” and “outside-in” mechanisms together, to outline a more comprehensive profile of MS cellular pathology and pathogenesis. A recent study using a newly developed MS-like model, defined as cuprizone autoimmune encephalitis (CAE), reported that both endogenous and peripheral immune responses can be activated during lesion formation and demyelination [362,363]. This finding provides evidence for the “inside-out” mechanism in progressive MS that subclinical demyelination triggers the activation of endogenous immune cells in the CNS and adaptive immune response, thus, contributing to further axonal degeneration. Moreover, this animal model may provide explanation on why DMTs are ineffective against the progressive stage of MS as DMTs focus less on repairing the damage elicited by peripheral inflammatory cells and endogenous glial cells in the CNS.
One issue in translational research of MS is that there are limited molecular and cellular biomarkers available for monitoring the disease severity and examining the effectiveness of the therapies over the course of MS. As the consequence of inconsistent and unpredictable disease progression in MS patients, it is difficult to find a biomarker with well-evaluated validity and clinical relevance. From the visualisation perspective, advanced MRI techniques provide several imaging biomarkers through the assessment of brain volume and the thickness of the cortical cortex, which have helped to establish the microstructural changes of CNS for MS patients. However, fluctuations in parameters obtained from MRI techniques in different MS patients highlight the potential risk of results that is rarely reproducible. The potential strategy of combining molecular biomarkers with imaging techniques to investigate either new therapeutics or disease progression monitoring provides a feasible way to get a more accurate analysis.
Another important consideration to improve the clinical outcomes of MS patients is to investigate potential therapeutics. Stem cell transplantation combined with genetic modification techniques has become a promising option for treating autoimmune diseases and immunodeficiency disorders. This therapeutic strategy is not only replacing the pathogenic immune cell populations with healthy cells but also producing therapeutic proteins by genetic editing techniques on transplanted cells. The delivery of decoy fusion protein NgR(310)ecto-Fc via genetically modified HSCs directly into the lesions can inhibit neurodegeneration and improve neurorepair, potentially offering long-term neuroprotection after the progressive stage of the disease. The repair can also be assessed using existing molecular and imaging biomarkers. In the future, genetically modifying HSCs with CRISPR-Cas9 to deliver NgR(310)ecto-Fc may improve the safety of the treatment and possibly, offer a new therapeutic option for progressive MS patients.
Author Contributions
Conceptualization: SP; methodology: OE, SY, DN, and SP; software: OE, SY, DN; validation: OE, SY, DN, and SP; formal analysis: OE, SY, DN, and SP; investigation: OE, SY, DN; resources: CM; data curation: OE, SY, DN; writing-original draft preparation: OE, SY, DN; writing-review and editing, OE, SY, DN, MD, MP, EO, PT, NG, SP; visualization: OE, SY, DN, SP; supervision: SP; project administration: SP; funding acquisition: SP. All authors have read and agreed to the published version of the manuscript.
Funding
SP was funded by MS Australia Project Grant (ID#212-058). DN was funded by MS Australia Postgraduate Scholarship (ID#22-3-058).
Ethics approval and consent to participate
NA
Consent for publication
Not applicable.
Availability of data and material
Not applicable.
Acknowledgments
Figure 1 were created with Biorender.com.
Conflicts of Interest
The authors declare that they have no competing interests.
References
- Trapp, B.D.; Peterson, J.; Ransohoff, R.M.; Rudick, R.; Mörk, S.; Bö, L. Axonal Transection in the Lesions of Multiple Sclerosis. New Engl. J. Med. 1998, 338, 278–285. [CrossRef]
- Lucchinetti C, Brück W, Parisi J, Scheithauer B, Rodriguez M, Lassmann H. Heterogeneity of multiple sclerosis lesions: Implications for the pathogenesis of demyelination. Ann Neurol. 2000;47(6):707-17. [CrossRef]
- Lublin FD, Reingold SC, Cohen JA, Cutter GR, Sørensen PS, Thompson AJ; et al. Defining the clinical course of multiple sclerosis: The 2013 revisions. Neurology. 2014;83(3):278-86. [CrossRef]
- Hauser, S.L.; Bhan, A.K.; Gilles, F.; Kemp, M.; Kerr, C.; Weiner, H.L. Immunohistochemical analysis of the cellular infiltrate in multiple sclerosis lesions. Ann. Neurol. 1986, 19, 578–587. [CrossRef]
- Olsson, T.; Zhi, W.W.; Höjeberg, B.; Kostulas, V.; Jiang, Y.P.; Anderson, G.; Ekre, H.P.; Link, H. Autoreactive T lymphocytes in multiple sclerosis determined by antigen-induced secretion of interferon-gamma.. J. Clin. Investig. 1990, 86, 981–985. [CrossRef]
- Ota, K.; Matsui, M.; Milford, E.L.; Mackin, G.A.; Weiner, H.L.; Hafler, D.A. T-cell recognition of an immuno-dominant myelin basic protein epitope in multiple sclerosis. Nature 1990, 346, 183–187. [CrossRef]
- Brück, W.; Sommermeier, N.; Bergmann, M.; Zettl, U.; Goebel, H.H.; Kretzschmar, H.A.; Lassmann, H. CHAPTER 14: Macrophages in Multiple Sclerosis. Immunobiology 1996, 195, 588–600. [CrossRef]
- Papadopoulos, D.; Dukes, S.; Patel, R.; Nicholas, R.; Vora, A.; Reynolds, R. Substantial Archaeocortical Atrophy and Neuronal Loss in Multiple Sclerosis. Brain Pathol. 2009, 19, 238–253. [CrossRef]
- Wegner, C.; Esiri, M.M.; Chance, S.A.; Palace, J.; Matthews, P.M. Neocortical neuronal, synaptic, and glial loss in multiple sclerosis. Neurology 2006, 67, 960–967. [CrossRef]
- Bitsch, A.; Bruhn, H.; Vougioukas, V.; Stringaris, A.; Lassmann, H.; Frahm, J.; Brück, W. Inflammatory CNS Demyelination: Histopathologic Correlation with In Vivo Quantitative Proton MR Spectroscopy. 1999, 20, 1619–1627.
- Brown, J.W.L.; Coles, A.; Horakova, D.; Havrdova, E.; Izquierdo, G.; Prat, A.; Girard, M.; Duquette, P.; Trojano, M.; Lugaresi, A.; et al. Association of Initial Disease-Modifying Therapy With Later Conversion to Secondary Progressive Multiple Sclerosis. JAMA 2019, 321, 175–187. [CrossRef]
- Andersen, O.; Elovaara, I.; Färkkilä, M.; Hansen, H.J.; I Mellgren, S.; Myhr, K.-M.; Sandberg-Wollheim, M.; Sørensen, P.S. Multicentre, randomised, double blind, placebo controlled, phase III study of weekly, low dose, subcutaneous interferon beta-1a in secondary progressive multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2004, 75, 706–710. [CrossRef]
- Wolinsky, J.S.; Narayana, P.A.; O'Connor, P.; Coyle, P.K.; Ford, C.; Johnson, K.; Miller, A.; Pardo, L.; Kadosh, S.; Ladkani, D.; et al. Glatiramer acetate in primary progressive multiple sclerosis: Results of a multinational, multicenter, double-blind, placebo-controlled trial. Ann. Neurol. 2007, 61, 14–24. [CrossRef]
- Hawker, K.; O'Connor, P.; Freedman, M.S.; Calabresi, P.A.; Antel, J.; Simon, J.; Hauser, S.; Waubant, E.; Vollmer, T.; Panitch, H.; et al. Rituximab in patients with primary progressive multiple sclerosis: Results of a randomized double-blind placebo-controlled multicenter trial. Ann. Neurol. 2009, 66, 460–471. [CrossRef]
- Barzegar, M.; Najdaghi, S.; Afshari-Safavi, A.; Nehzat, N.; Mirmosayyeb, O.; Shaygannejad, V. Early predictors of conversion to secondary progressive multiple sclerosis. Mult. Scler. Relat. Disord. 2021, 54, 103115. [CrossRef]
- Kalincik, T.; Diouf, I.; Sharmin, S.; Malpas, C.; Spelman, T.; Horakova, D.; Havrdova, E.K.; Trojano, M.; Izquierdo, G.; Lugaresi, A.; et al. Effect of Disease-Modifying Therapy on Disability in Relapsing-Remitting Multiple Sclerosis Over 15 Years. Neurology 2020, 96, e783–e797. [CrossRef]
- Abbott NJ, Rönnbäck L, Hansson E. Astrocyte–endothelial interactions at the blood–brain barrier. Nature Reviews Neuroscience. 2006;7(1):41-53. [CrossRef]
- Plumb, J.; McQuaid, S.; Mirakhur, M.; Kirk, J. Abnormal Endothelial Tight Junctions in Active Lesions and Normal-appearing White Matter in Multiple Sclerosis. Brain Pathol. 2002, 12, 154–169. [CrossRef]
- Kirk, J.; Plumb, J.; Mirakhur, M.; McQuaid, S. Tight junctional abnormality in multiple sclerosis white matter affects all calibres of vessel and is associated with blood–brain barrier leakage and active demyelination. J. Pathol. 2003, 201, 319–327. [CrossRef]
- Sheikh, M.H.; Henson, S.M.; Loiola, R.A.; Mercurio, S.; Colamatteo, A.; Maniscalco, G.T.; De Rosa, V.; McArthur, S.; Solito, E. Immuno-metabolic impact of the multiple sclerosis patients’ sera on endothelial cells of the blood-brain barrier. J. Neuroinflammation 2020, 17, 153. [CrossRef]
- Schreibelt, G.; Musters, R.J.P.; Reijerkerk, A.; de Groot, L.R.; van der Pol, S.M.A.; Hendrikx, E.M.L.; Döpp, E.D.; Dijkstra, C.D.; Drukarch, B.; de Vries, H.E. Lipoic Acid Affects Cellular Migration into the Central Nervous System and Stabilizes Blood-Brain Barrier Integrity. J. Immunol. 2006, 177, 2630–2637. [CrossRef]
- Goes, A.; Wouters, D.; Pol, S.M.A.; Huizinga, R.; Ronken, E.; Adamson, P.; Greenwood, J.; Dijkstra, C.D.; Vries, H.E. Reactive oxygen species enhance the migration of monocytes across the blood-brain barrier in vitro. FASEB J. 2001, 15, 1852–1854. [CrossRef]
- Gray, E.; Thomas, T.L.; Betmouni, S.; Scolding, N.; Love, S. Elevated myeloperoxidase activity in white matter in multiple sclerosis. Neurosci. Lett. 2008, 444, 195–198. [CrossRef]
- Agrawal, S.M.; Williamson, J.; Sharma, R.; Kebir, H.; Patel, K.; Prat, A.; Yong, V.W. Extracellular matrix metalloproteinase inducer shows active perivascular cuffs in multiple sclerosis. Brain 2013, 136, 1760–1777. [CrossRef]
- Bar-Or, A.; Nuttall, R.K.; Duddy, M.; Alter, A.; Kim, H.J.; Ifergan, I.; Pennington, C.J.; Bourgoin, P.; Edwards, D.R.; Yong, V.W. Analyses of all matrix metalloproteinase members in leukocytes emphasize monocytes as major inflammatory mediators in multiple sclerosis. Brain 2003, 126, 2738–2749. [CrossRef]
- Song, J.; Wu, C.; Korpos, E.; Zhang, X.; Agrawal, S.M.; Wang, Y.; Faber, C.; Schäfers, M.; Körner, H.; Opdenakker, G.; et al. Focal MMP-2 and MMP-9 Activity at the Blood-Brain Barrier Promotes Chemokine-Induced Leukocyte Migration. Cell Rep. 2015, 10, 1040–1054. [CrossRef]
- Kanesaka, T.; Mori, M.; Hattori, T.; Oki, T.; Kuwabara, S. Serum matrix metalloproteinase-3 levels correlate with disease activity in relapsing-remitting multiple sclerosis. J. Neurol. Neurosurg. Psychiatry 2006, 77, 185–188. [CrossRef]
- Cossins, J.A.; Clements, J.M.; Ford, J.; Miller, K.M.; Pigott, R.; Vos, W.; Van Der Valk, P.; De Groot, C.J.A. Enhanced expression of MMP-7 and MMP-9 in demyelinating multiple sclerosis lesions. Acta Neuropathol. 1997, 94, 590–598. [CrossRef]
- Maeda, A.; Sobel, R.A. Matrix Metalloproteinases in the Normal Human Central Nervous System, Microglial Nodules, and Multiple Sclerosis Lesions. J. Neuropathol. Exp. Neurol. 1996, 55, 300–309. [CrossRef]
- Alexander JS, Harris MK, Wells SR, Mills G, Chalamidas K, Ganta VC; et al. Alterations in serum MMP-8, MMP-9, IL-12p40 and IL-23 in multiple sclerosis patients treated with interferon-beta1b. Mult Scler. 2010;16(7):801-9. [CrossRef]
- Charabati, M.; Grasmuck, C.; Ghannam, S.; Bourbonnière, L.; Fournier, A.P.; Lécuyer, M.-A.; Tastet, O.; Kebir, H.; Rébillard, R.-M.; Hoornaert, C.; et al. DICAM promotes T H 17 lymphocyte trafficking across the blood-brain barrier during autoimmune neuroinflammation. Sci. Transl. Med. 2022, 14, eabj0473. [CrossRef]
- Jung YK, Jin JS, Jeong JH, Kim HN, Park NR, Choi JY. DICAM, a novel dual immunoglobulin domain containing cell adhesion molecule interacts with alphavbeta3 integrin. J Cell Physiol. 2008;216(3):603-14. [CrossRef]
- Han, S.-W.; Jung, Y.-K.; Lee, E.-J.; Park, H.-R.; Kim, G.-W.; Jeong, J.-H.; Han, M.-S.; Choi, J.-Y. DICAM inhibits angiogenesis via suppression of AKT and p38 MAP kinase signalling. Cardiovasc. Res. 2013, 98, 73–82. [CrossRef]
- Sen MK, Almuslehi MSM, Shortland PJ, Coorssen JR, Mahns DA. Revisiting the Pathoetiology of Multiple Sclerosis: Has the Tail Been Wagging the Mouse? Front Immunol. 2020;11:572186. [CrossRef]
- Huseby, E.S.; Liggitt, D.; Brabb, T.; Schnabel, B.; Öhlén, C.; Goverman, J. A Pathogenic Role for Myelin-Specific Cd8+ T Cells in a Model for Multiple Sclerosis. J. Exp. Med. 2001, 194, 669–676. [CrossRef]
- Viglietta, V.; Baecher-Allan, C.; Weiner, H.L.; Hafler, D.A. Loss of Functional Suppression by CD4+CD25+ Regulatory T Cells in Patients with Multiple Sclerosis. J. Exp. Med. 2004, 199, 971–979. [CrossRef]
- Jelcic I, Al Nimer F, Wang J, Lentsch V, Planas R, Jelcic I; et al. Memory B Cells Activate Brain-Homing, Autoreactive CD4(+) T Cells in Multiple Sclerosis. Cell. 2018;175(1):85-100.e23. [CrossRef]
- Titus HE, Chen Y, Podojil JR, Robinson AP, Balabanov R, Popko B; et al. Pre-clinical and Clinical Implications of “Inside-Out” vs. “Outside-In” Paradigms in Multiple Sclerosis Etiopathogenesis. Frontiers in Cellular Neuroscience. 2020;14. [CrossRef]
- Patsopoulos NA, Baranzini SE, Santaniello A, Shoostari P, Cotsapas C, Wong G; et al. Multiple sclerosis genomic map implicates peripheral immune cells and microglia in susceptibility. Science. 2019;365(6460):eaav7188. [CrossRef]
- Ziaei, A.; Garcia-Miralles, M.; Radulescu, C.I.; Sidik, H.; Silvin, A.; Bae, H.; Bonnard, C.; Yusof, N.A.B.M.; Bardile, C.F.; Tan, L.J.; et al. Ermin deficiency leads to compromised myelin, inflammatory milieu, and susceptibility to demyelinating insult. Brain Pathol. 2022, 32, e13064. [CrossRef]
- Barnett, M.H.; Prineas, J.W. Relapsing and remitting multiple sclerosis: Pathology of the newly forming lesion. Ann. Neurol. 2004, 55, 458–468. [CrossRef]
- Kerlero de Rosbo N, Milo R, Lees MB, Burger D, Bernard CC, Ben-Nun A. Reactivity to myelin antigens in multiple sclerosis. Peripheral blood lymphocytes respond predominantly to myelin oligodendrocyte glycoprotein. J Clin Invest. 1993;92(6):2602-8. [CrossRef]
- Reindl, M.; Linington, C.; Brehm, U.; Egg, R.; Dilitz, E.; Deisenhammer, F.; Poewe, W.; Berger, T. Antibodies against the myelin oligodendrocyte glycoprotein and the myelin basic protein in multiple sclerosis and other neurological diseases: A comparative study. Brain 1999, 122, 2047–2056. [CrossRef]
- Gardinier, M.V.; Amiguet, P.; Linington, C.; Matthieu, J. Myelin/oligodendrocyte glycoprotein is a unique member of the immunoglobulin superfamily. J. Neurosci. Res. 1992, 33, 177–187. [CrossRef]
- Bjornevik K, Cortese M, Healy BC, Kuhle J, Mina MJ, Leng Y; et al. Longitudinal analysis reveals high prevalence of Epstein-Barr virus associated with multiple sclerosis. Science. 2022;375(6578):296-301. [CrossRef]
- Lang, H.L.; Jacobsen, H.; Ikemizu, S.; Andersson, C.; Harlos, K.; Madsen, L.; Hjorth, P.; Sondergaard, L.; Svejgaard, A.; Wucherpfennig, K.; et al. A functional and structural basis for TCR cross-reactivity in multiple sclerosis. Nat. Immunol. 2002, 3, 940–943. [CrossRef]
- Holmøy, T.; Kvale, E..; Vartdal, F. Cerebrospinal fluid CD4+T cells from a multiple sclerosis patient cross-recognize Epstein-Barr virus and myelin basic protein. J. NeuroVirology 2004, 10, 278–283. [CrossRef]
- Garzelli, C.; E Taub, F.; E Scharff, J.; Prabhakar, B.S.; Ginsberg-Fellner, F.; Notkins, A.L. Epstein-Barr virus-transformed lymphocytes produce monoclonal autoantibodies that react with antigens in multiple organs. J. Virol. 1984, 52, 722–725. [CrossRef]
- Serafini, B.; Rosicarelli, B.; Franciotta, D.; Magliozzi, R.; Reynolds, R.; Cinque, P.; Andreoni, L.; Trivedi, P.; Salvetti, M.; Faggioni, A.; et al. Dysregulated Epstein-Barr virus infection in the multiple sclerosis brain. J. Exp. Med. 2007, 204, 2899–2912. [CrossRef]
- Esfahani, B.S.; Gharesouran, J.; Ghafouri-Fard, S.; Talebian, S.; Arsang-Jang, S.; Omrani, M.D.; Taheri, M.; Rezazadeh, M. Down-regulation of ERMN expression in relapsing remitting multiple sclerosis. Metab. Brain Dis. 2019, 34, 1261–1266. [CrossRef]
- Oveland, E.; Ahmad, I.; Lereim, R.R.; Kroksveen, A.C.; Barsnes, H.; Guldbrandsen, A.; Myhr, K.-M.; Bø, L.; Berven, F.S.; Wergeland, S. Cuprizone and EAE mouse frontal cortex proteomics revealed proteins altered in multiple sclerosis. Sci. Rep. 2021, 11, 1–16. [CrossRef]
- Schirmer, L.; Velmeshev, D.; Holmqvist, S.; Kaufmann, M.; Werneburg, S.; Jung, D.; Vistnes, S.; Stockley, J.H.; Young, A.; Steindel, M.; et al. Neuronal vulnerability and multilineage diversity in multiple sclerosis. Nature 2019, 573, 75–82. [CrossRef]
- Alliot F, Godin I, Pessac B. Microglia derive from progenitors, originating from the yolk sac, and which proliferate in the brain. Brain Res Dev Brain Res. 1999;117(2):145-52. [CrossRef]
- Ajami, B.; Bennett, J.L.; Krieger, C.; McNagny, K.M.; Rossi, F.M.V. Infiltrating monocytes trigger EAE progression, but do not contribute to the resident microglia pool. Nat. Neurosci. 2011, 14, 1142–1149. [CrossRef]
- Mildner, A.; Schmidt, H.; Nitsche, M.; Merkler, D.; Hanisch, U.-K.; Mack, M.; Heikenwalder, M.; Brück, W.; Priller, J.; Prinz, M. Microglia in the adult brain arise from Ly-6ChiCCR2+ monocytes only under defined host conditions. Nat. Neurosci. 2007, 10, 1544–1553. [CrossRef]
- Ziegler-Heitbrock, L.; Ancuta, P.; Crowe, S.; Dalod, M.; Grau, V.; Hart, D.N.; Leenen, P.J.M.; Liu, Y.-J.; MacPherson, G.; Randolph, G.J.; et al. Nomenclature of monocytes and dendritic cells in blood. Blood 2010, 116, e74–e80. [CrossRef]
- Geissmann, F.; Jung, S.; Littman, D.R. Blood Monocytes Consist of Two Principal Subsets with Distinct Migratory Properties. Immunity 2003, 19, 71–82. [CrossRef]
- Yona, S.; Kim, K.-W.; Wolf, Y.; Mildner, A.; Varol, D.; Breker, M.; Strauss-Ayali, D.; Viukov, S.; Guilliams, M.; Misharin, A.; et al. Fate Mapping Reveals Origins and Dynamics of Monocytes and Tissue Macrophages under Homeostasis. Immunity 2013, 38, 79–91. [CrossRef]
- Meghraoui-Kheddar A, Barthelemy S, Boissonnas A, Combadière C. Revising CX3CR1 Expression on Murine Classical and Non-classical Monocytes. Front Immunol. 2020;11:1117. [CrossRef]
- Nishiyori A, Minami M, Ohtani Y, Takami S, Yamamoto J, Kawaguchi N; et al. Localization of fractalkine and CX3CR1 mRNAs in rat brain: Does fractalkine play a role in signaling from neuron to microglia? FEBS Lett. 1998;429(2):167-72. [CrossRef]
- Harrison, J.K.; Jiang, Y.; Chen, S.; Xia, Y.; Maciejewski, D.; McNamara, R.K.; Streit, W.J.; Salafranca, M.N.; Adhikari, S.; Thompson, D.A.; et al. Role for neuronally derived fractalkine in mediating interactions between neurons and CX3CR1-expressing microglia. Proc. Natl. Acad. Sci. USA 1998, 95, 10896–10901. [CrossRef]
- Lampron, A.; Larochelle, A.; Laflamme, N.; Préfontaine, P.; Plante, M.-M.; Sánchez, M.G.; Yong, V.W.; Stys, P.K.; Tremblay, M.; Rivest, S. Inefficient clearance of myelin debris by microglia impairs remyelinating processes. J. Exp. Med. 2015, 212, 481–495. [CrossRef]
- Jing, X.; Yao, Y.; Wu, D.; Hong, H.; Feng, X.; Xu, N.; Liu, Y.; Liang, H. IFP35 family proteins promote neuroinflammation and multiple sclerosis. Proc. Natl. Acad. Sci. 2021, 118. [CrossRef]
- Peferoen, L.A.; Vogel, D.Y.; Ummenthum, K.; Breur, M.; Heijnen, P.D.; Gerritsen, W.H.; Peferoen-Baert, R.M.; van der Valk, P.; Dijkstra, C.D.; Amor, S. Activation Status of Human Microglia Is Dependent on Lesion Formation Stage and Remyelination in Multiple Sclerosis. J. Neuropathol. Exp. Neurol. 2015, 74, 48–63. [CrossRef]
- Jäckle, K.; Zeis, T.; Schaeren-Wiemers, N.; Junker, A.; van der Meer, F.; Kramann, N.; Stadelmann, C.; Brück, W. Molecular signature of slowly expanding lesions in progressive multiple sclerosis. Brain 2020, 143, 2073–2088. [CrossRef]
- Grajchen, E.; Wouters, E.; van de Haterd, B.; Haidar, M.; Hardonnière, K.; Dierckx, T.; Van Broeckhoven, J.; Erens, C.; Hendrix, S.; Kerdine-Römer, S.; et al. CD36-mediated uptake of myelin debris by macrophages and microglia reduces neuroinflammation. J. Neuroinflammation 2020, 17, 1–14. [CrossRef]
- Grajchen, E.; Hendriks, J.J.A.; Bogie, J.F.J. The physiology of foamy phagocytes in multiple sclerosis. Acta Neuropathol. Commun. 2018, 6, 1–21. [CrossRef]
- Epstein, L.; Prineas, J.; Raine, C. Attachment of myelin to coated pits on macrophages in experimental allergic encephalomyelitis. J. Neurol. Sci. 1983, 61, 341–348. [CrossRef]
- Marta, C.B.; Bansal, R.; Pfeiffer, S.E. Microglial Fc receptors mediate physiological changes resulting from antibody cross-linking of myelin oligodendrocyte glycoprotein. J. Neuroimmunol. 2008, 196, 35–40. [CrossRef]
- Melief, J.; Schuurman, K.G.; van de Garde, M.D.B.; Smolders, J.; van Eijk, M.; Hamann, J.; Huitinga, I. Microglia in normal appearing white matter of multiple sclerosis are alerted but immunosuppressed. Glia 2013, 61, 1848–1861. [CrossRef]
- Hendrickx, D.A.; Koning, N.; Schuurman, K.G.; van Strien, M.E.; van Eden, C.G.; Hamann, J.; Huitinga, I. Selective Upregulation of Scavenger Receptors in and Around Demyelinating Areas in Multiple Sclerosis. J. Neuropathol. Exp. Neurol. 2013, 72, 106–118. [CrossRef]
- Reichert, F.; Rotshenker, S. Complement-receptor-3 and scavenger-receptor-AI/II mediated myelin phagocytosis in microglia and macrophages. Neurobiol. Dis. 2003, 12, 65–72. [CrossRef]
- Ulvestad, E.; Williams, K.; Vedeler, C.; Antel, J.; Nyland, H.; Mørk, S.; Matre, R. Reactive microglia in multiple sclerosis lesions have an increased expression of receptors for the Fc part of IgG. J. Neurol. Sci. 1994, 121, 125–131. [CrossRef]
- Van der Goes, A.; Kortekaas, M.; Hoekstra, K.; Dijkstra, C.D.; Amor, S. The role of anti-myelin (auto)-antibodies in the phagocytosis of myelin by macrophages. J. Neuroimmunol. 1999, 101, 61–67. [CrossRef]
- Karni, A.; Bakimer-Kleiner, R.; Abramsky, O.; Ben-Nun, A. Elevated levels of antibody to myelin oligodendrocyte glycoprotein is not specific for patients with multiple sclerosis.. Arch. Neurol. 1999, 56, 311–315. [CrossRef]
- Lampasona, V.; Franciotta, D.; Furlan, R.; Zanaboni, S.; Fazio, R.; Bonifacio, E.; Comi, G.; Martino, G. Similar low frequency of anti-MOG IgG and IgM in MS patients and healthy subjects. Neurology 2004, 62, 2092–2094. [CrossRef]
- Loveless, S.; Neal, J.W.; Howell, O.W.; Harding, K.E.; Sarkies, P.; Evans, R.; Bevan, R.J.; Hakobyan, S.; Harris, C.L.; Robertson, N.P.; et al. Tissue microarray methodology identifies complement pathway activation and dysregulation in progressive multiple sclerosis. Brain Pathol. 2017, 28, 507–520. [CrossRef]
- Levy-Barazany, H.; Frenkel, D. Expression of Scavenger receptor A on antigen presenting cells is important for CD4+ T-cells proliferation in EAE mouse model. J. Neuroinflammation 2012, 9, 120–120. [CrossRef]
- Healy, L.M.; Perron, G.; Won, S.-Y.; Michell-Robinson, M.A.; Rezk, A.; Ludwin, S.K.; Moore, C.S.; Hall, J.A.; Bar-Or, A.; Antel, J.P. MerTK Is a Functional Regulator of Myelin Phagocytosis by Human Myeloid Cells. J. Immunol. 2016, 196, 3375–3384. [CrossRef]
- Nagata, K.; Ohashi, K.; Nakano, T.; Arita, H.; Zong, C.; Hanafusa, H.; Mizuno, K. Identification of the Product of Growth Arrest-specific Gene 6 as a Common Ligand for Axl, Sky, and Mer Receptor Tyrosine Kinases. J. Biol. Chem. 1996, 271, 30022–30027. [CrossRef]
- Stitt TN, Conn G, Gore M, Lai C, Bruno J, Radziejewski C; et al. The anticoagulation factor protein S and its relative, Gas6, are ligands for the Tyro 3/Axl family of receptor tyrosine kinases. Cell. 1995;80(4):661-70. [CrossRef]
- Ma, G.Z.M.; Stankovich, J.; Kilpatrick, T.J.; Binder, M.D.; Field, J.; The Australia and New Zealand Multiple Sclerosis Genetics Consortium (ANZgene) , Polymorphisms in the Receptor Tyrosine Kinase MERTK Gene Are Associated with Multiple Sclerosis Susceptibility. PLoS ONE 2011, 6, e16964. [CrossRef]
- Binder, M.D.; Cate, H.S.; Prieto, A.L.; Kemper, D.; Butzkueven, H.; Gresle, M.M.; Cipriani, T.; Jokubaitis, V.G.; Carmeliet, P.; Kilpatrick, T.J. Gas6 Deficiency Increases Oligodendrocyte Loss and Microglial Activation in Response to Cuprizone-Induced Demyelination. J. Neurosci. 2008, 28, 5195–5206. [CrossRef]
- Weinger, J.G.; Omari, K.M.; Marsden, K.; Raine, C.S.; Shafit-Zagardo, B. Up-Regulation of Soluble Axl and Mer Receptor Tyrosine Kinases Negatively Correlates with Gas6 in Established Multiple Sclerosis Lesions. Am. J. Pathol. 2009, 175, 283–293. [CrossRef]
- Shen, K.; Reichelt, M.; Kyauk, R.V.; Ngu, H.; Shen, Y.-A.A.; Foreman, O.; Modrusan, Z.; Friedman, B.A.; Sheng, M.; Yuen, T.J. Multiple sclerosis risk gene Mertk is required for microglial activation and subsequent remyelination. Cell Rep. 2021, 34, 108835. [CrossRef]
- Cignarella, F.; Filipello, F.; Bollman, B.; Cantoni, C.; Locca, A.; Mikesell, R.; Manis, M.; Ibrahim, A.; Deng, L.; Benitez, B.A.; et al. TREM2 activation on microglia promotes myelin debris clearance and remyelination in a model of multiple sclerosis. Acta Neuropathol. 2020, 140, 513–534. [CrossRef]
- Ennerfelt, H.; Frost, E.L.; Shapiro, D.A.; Holliday, C.; Zengeler, K.E.; Voithofer, G.; Bolte, A.C.; Lammert, C.R.; Kulas, J.A.; Ulland, T.K.; et al. SYK coordinates neuroprotective microglial responses in neurodegenerative disease. Cell 2022, 185, 4135–4152.e22. [CrossRef]
- Yeh FL, Hansen DV, Sheng M. TREM2, Microglia, and Neurodegenerative Diseases. Trends in Molecular Medicine. 2017;23(6):512-33. [CrossRef]
- Bennett, M.L.; Bennett, F.C.; Liddelow, S.A.; Ajami, B.; Zamanian, J.L.; Fernhoff, N.B.; Mulinyawe, S.B.; Bohlen, C.J.; Adil, A.; Tucker, A.; et al. New tools for studying microglia in the mouse and human CNS. Proc. Natl. Acad. Sci. USA 2016, 113, E1738–E1746. [CrossRef]
- Satoh, J.; Kino, Y.; Asahina, N.; Takitani, M.; Miyoshi, J.; Ishida, T.; Saito, Y. TMEM119 marks a subset of microglia in the human brain. Neuropathology 2015, 36, 39–49. [CrossRef]
- Butovsky, O.; Jedrychowski, M.P.; Moore, C.S.; Cialic, R.; Lanser, A.J.; Gabriely, G.; Koeglsperger, T.; Dake, B.; Wu, P.M.; E Doykan, C.; et al. Identification of a unique TGF-β–dependent molecular and functional signature in microglia. Nat. Neurosci. 2013, 17, 131–143. [CrossRef]
- Kenkhuis, B.; Somarakis, A.; Kleindouwel, L.R.; van Roon-Mom, W.M.; Höllt, T.; van der Weerd, L. Co-expression patterns of microglia markers Iba1, TMEM119 and P2RY12 in Alzheimer's disease. Neurobiol. Dis. 2022, 167, 105684. [CrossRef]
- Zrzavy, T.; Hametner, S.; Wimmer, I.; Butovsky, O.; Weiner, H.L.; Lassmann, H. Loss of ‘homeostatic’ microglia and patterns of their activation in active multiple sclerosis. Brain 2017, 140, 1900–1913. [CrossRef]
- van Wageningen TA, Vlaar E, Kooij G, Jongenelen CAM, Geurts JJG, van Dam AM. Regulation of microglial TMEM119 and P2RY12 immunoreactivity in multiple sclerosis white and grey matter lesions is dependent on their inflammatory environment. Acta Neuropathol Commun. 2019;7(1):206. [CrossRef]
- Ziebell, J.M.; E Taylor, S.; Cao, T.; Harrison, J.L.; Lifshitz, J. Rod microglia: Elongation, alignment, and coupling to form trains across the somatosensory cortex after experimental diffuse brain injury. J. Neuroinflammation 2012, 9, 247–247. [CrossRef]
- Trapp BD, Wujek JR, Criste GA, Jalabi W, Yin X, Kidd GJ; et al. Evidence for synaptic stripping by cortical microglia. Glia. 2007;55(4):360-8. [CrossRef]
- van der Poel M, Ulas T, Mizee MR, Hsiao C-C, Miedema SSM, Adelia; et al. Transcriptional profiling of human microglia reveals grey–white matter heterogeneity and multiple sclerosis-associated changes. Nature Communications. 2019;10(1):1139. [CrossRef]
- Sofroniew, M.V.; Vinters, H.V. Astrocytes: Biology and pathology. Acta Neuropathol. 2010, 119, 7–35. [CrossRef]
- Ioannou, M.S.; Jackson, J.; Sheu, S.-H.; Chang, C.-L.; Weigel, A.V.; Liu, H.; Pasolli, H.A.; Xu, C.S.; Pang, S.; Matthies, D.; et al. Neuron-Astrocyte Metabolic Coupling Protects against Activity-Induced Fatty Acid Toxicity. Cell 2019, 177, 1522–1535.e14. [CrossRef]
- Pellerin, L.; Magistretti, P.J. Glutamate uptake into astrocytes stimulates aerobic glycolysis: A mechanism coupling neuronal activity to glucose utilization.. Proc. Natl. Acad. Sci. USA 1994, 91, 10625–10629. [CrossRef]
- Qi, G.; Mi, Y.; Shi, X.; Gu, H.; Brinton, R.D.; Yin, F. ApoE4 Impairs Neuron-Astrocyte Coupling of Fatty Acid Metabolism. Cell Rep. 2021, 34, 108572–108572. [CrossRef]
- Liddelow, S.A.; Guttenplan, K.A.; Clarke, L.E.; Bennett, F.C.; Bohlen, C.J.; Schirmer, L.; Bennett, M.L.; Münch, A.E.; Chung, W.-S.; Peterson, T.C.; et al. Neurotoxic reactive astrocytes are induced by activated microglia. Nature 2017, 541, 481–487. [CrossRef]
- Holley, J.E.; Gveric, D.; Newcombe, J.; Cuzner, M.L.; Gutowski, N.J. Astrocyte characterization in the multiple sclerosis glial scar. Neuropathol. Appl. Neurobiol. 2003, 29, 434–444. [CrossRef]
- Simpson, J.E.; Ince, P.G.; Lace, G.; Forster, G.; Shaw, P.J.; Matthews, F.; Savva, G.; Brayne, C.; Wharton, S.B. Astrocyte Phenotype in Relation to Alzheimer-Type Pathology in the Ageing Brain. Neurobiol. Aging 2010, 31, 578–590. [CrossRef]
- Diaz-Castro, B.; Bernstein, A.M.; Coppola, G.; Sofroniew, M.V.; Khakh, B.S. Molecular and functional properties of cortical astrocytes during peripherally induced neuroinflammation. Cell Rep. 2021, 36, 109508. [CrossRef]
- Ponath, G.; Lincoln, M.R.; Levine-Ritterman, M.; Park, C.; Dahlawi, S.; Mubarak, M.; Sumida, T.; Airas, L.; Zhang, S.; Isitan, C.; et al. Enhanced astrocyte responses are driven by a genetic risk allele associated with multiple sclerosis. Nat. Commun. 2018, 9, 5337. [CrossRef]
- Brambilla R, Bracchi-Ricard V, Hu WH, Frydel B, Bramwell A, Karmally S; et al. Inhibition of astroglial nuclear factor kappaB reduces inflammation and improves functional recovery after spinal cord injury. J Exp Med. 2005;202(1):145-56. [CrossRef]
- Brambilla R, Persaud T, Hu X, Karmally S, Shestopalov VI, Dvoriantchikova G; et al. Transgenic inhibition of astroglial NF-kappa B improves functional outcome in experimental autoimmune encephalomyelitis by suppressing chronic central nervous system inflammation. Journal of immunology (Baltimore, Md : 1950). 2009;182(5):2628-40. [CrossRef]
- Kirkley KS, Popichak KA, Hammond SL, Davies C, Hunt L, Tjalkens RB. Genetic suppression of IKK2/NF-κB in astrocytes inhibits neuroinflammation and reduces neuronal loss in the MPTP-Probenecid model of Parkinson's disease. Neurobiol Dis. 2019;127:193-209. [CrossRef]
- Kang, Z.; Altuntas, C.Z.; Gulen, M.F.; Liu, C.; Giltiay, N.; Qin, H.; Liu, L.; Qian, W.; Ransohoff, R.M.; Bergmann, C.; et al. Astrocyte-Restricted Ablation of Interleukin-17-Induced Act1-Mediated Signaling Ameliorates Autoimmune Encephalomyelitis. Immunity 2010, 32, 414–425. [CrossRef]
- Wheeler, M.A.; Clark, I.C.; Tjon, E.C.; Li, Z.; Zandee, S.E.J.; Couturier, C.P.; Watson, B.R.; Scalisi, G.; Alkwai, S.; Rothhammer, V.; et al. MAFG-driven astrocytes promote CNS inflammation. Nature 2020, 578, 593–599. [CrossRef]
- Bi, F.; Huang, C.; Tong, J.; Qiu, G.; Huang, B.; Wu, Q.; Li, F.; Xu, Z.; Bowser, R.; Xia, X.-G.; et al. Reactive astrocytes secrete lcn2 to promote neuron death. Proc. Natl. Acad. Sci. 2013, 110, 4069–4074. [CrossRef]
- Jones, E.V.; Bernardinelli, Y.; Zarruk, J.G.; Chierzi, S.; Murai, K.K. SPARC and GluA1-Containing AMPA Receptors Promote Neuronal Health Following CNS Injury. Front. Cell. Neurosci. 2018, 12, 22. [CrossRef]
- Guttenplan, K.A.; Weigel, M.K.; Prakash, P.; Wijewardhane, P.R.; Hasel, P.; Rufen-Blanchette, U.; Münch, A.E.; Blum, J.A.; Fine, J.; Neal, M.C.; et al. Neurotoxic reactive astrocytes induce cell death via saturated lipids. Nature 2021, 599, 102–107. [CrossRef]
- Chung, W.-S.; Clarke, L.E.; Wang, G.X.; Stafford, B.K.; Sher, A.; Chakraborty, C.; Joung, J.; Foo, L.C.; Thompson, A.; Chen, C.; et al. Astrocytes mediate synapse elimination through MEGF10 and MERTK pathways. Nature 2013, 504, 394–400. [CrossRef]
- Konishi, H.; Okamoto, T.; Hara, Y.; Komine, O.; Tamada, H.; Maeda, M.; Osako, F.; Kobayashi, M.; Nishiyama, A.; Kataoka, Y.; et al. Astrocytic phagocytosis is a compensatory mechanism for microglial dysfunction. EMBO J. 2020, 39, e104464. [CrossRef]
- Batiuk, M.Y.; Martirosyan, A.; Wahis, J.; de Vin, F.; Marneffe, C.; Kusserow, C.; Koeppen, J.; Viana, J.F.; Oliveira, J.F.; Voet, T.; et al. Identification of region-specific astrocyte subtypes at single cell resolution. Nat. Commun. 2020, 11, 1–15. [CrossRef]
- Clark, I.C.; Wheeler, M.A.; Lee, H.-G.; Li, Z.; Sanmarco, L.M.; Thaploo, S.; Polonio, C.M.; Shin, S.W.; Scalisi, G.; Henry, A.R.; et al. Identification of astrocyte regulators by nucleic acid cytometry. Nature 2023, 614, 326–333. [CrossRef]
- Wheeler, M.A.; Jaronen, M.; Covacu, R.; Zandee, S.E.; Scalisi, G.; Rothhammer, V.; Tjon, E.C.; Chao, C.-C.; Kenison, J.E.; Blain, M.; et al. Environmental Control of Astrocyte Pathogenic Activities in CNS Inflammation. Cell 2019, 176, 581–596.e18. [CrossRef]
- Macosko, E.Z.; Basu, A.; Satija, R.; Nemesh, J.; Shekhar, K.; Goldman, M.; Tirosh, I.; Bialas, A.R.; Kamitaki, N.; Martersteck, E.M.; et al. Highly Parallel Genome-wide Expression Profiling of Individual Cells Using Nanoliter Droplets. Cell 2015, 161, 1202–1214. [CrossRef]
- Amamoto R, Garcia MD, West ER, Choi J, Lapan SW, Lane EA; et al. Probe-Seq enables transcriptional profiling of specific cell types from heterogeneous tissue by RNA-based isolation. Elife. 2019;8. [CrossRef]
- Niu J, Tsai HH, Hoi KK, Huang N, Yu G, Kim K; et al. Aberrant oligodendroglial-vascular interactions disrupt the blood-brain barrier, triggering CNS inflammation. Nat Neurosci. 2019;22(5):709-18. [CrossRef]
- Tanaka, R.; Iwasaki, Y.; Koprowski, H. Ultrastructural studies of perivascular cuffing cells in multiple sclerosis brain.. 1975, 81, 467–78.
- Dal-Bianco, A.; Grabner, G.; Kronnerwetter, C.; Weber, M.; Kornek, B.; Kasprian, G.; Berger, T.; Leutmezer, F.; Rommer, P.S.; Trattnig, S.; et al. Long-term evolution of multiple sclerosis iron rim lesions in 7 T MRI. Brain 2021, 144, 833–847. [CrossRef]
- Frischer, J.M.; Weigand, S.D.; Guo, Y.; Kale, N.; Parisi, J.E.; Pirko, I.; Mandrekar, J.; Bramow, S.; Metz, I.; Brück, W.; et al. Clinical and pathological insights into the dynamic nature of the white matter multiple sclerosis plaque. Ann. Neurol. 2015, 78, 710–721. [CrossRef]
- Bosch, A.v.D.; Fransen, N.; Mason, M.; Rozemuller, A.J.; Teunissen, C.; Smolders, J.; Huitinga, I. Neurofilament Light Chain Levels in Multiple Sclerosis Correlate With Lesions Containing Foamy Macrophages and With Acute Axonal Damage. Neurol. - Neuroimmunol. Neuroinflammation 2022, 9. [CrossRef]
- Raine, C.S.; Wu, E. Multiple sclerosis: Remyelination in acute lesions.. 1993, 52, 199–204.
- Prineas, J.W.; Kwon, E.E.; Cho, E.; Sharer, L.R.; Barnett, M.H.; Oleszak, E.L.; Hoffman, B.; Morgan, B.P. Immunopathology of secondary-progressive multiple sclerosis. Ann. Neurol. 2001, 50, 646–657. [CrossRef]
- Kuhlmann, T.; Ludwin, S.; Prat, A.; Antel, J.; Brück, W.; Lassmann, H. An updated histological classification system for multiple sclerosis lesions. Acta Neuropathol. 2016, 133, 13–24. [CrossRef]
- Sobel, R.A.; Ahmed, A.S. White Matter Extracellular Matrix Chondroitin Sulfate/Dermatan Sulfate Proteoglycans in Multiple Sclerosis. J. Neuropathol. Exp. Neurol. 2001, 60, 1198–1207. [CrossRef]
- Kornek, B.; Storch, M.K.; Weissert, R.; Wallstroem, E.; Stefferl, A.; Olsson, T.; Linington, C.; Schmidbauer, M.; Lassmann, H. Multiple Sclerosis and Chronic Autoimmune Encephalomyelitis: A Comparative Quantitative Study of Axonal Injury in Active, Inactive, and Remyelinated Lesions. Am. J. Pathol. 2000, 157, 267–276. [CrossRef]
- Prineas JW, Connell F. Remyelination in multiple sclerosis. Ann Neurol. 1979;5(1):22-31. [CrossRef]
- Prineas, J.W.; Barnard, R.O.; Kwon, E.E.; Sharer, L.R.; Cho, E. Multiple sclerosis: Remyelination of nascent lesions: Remyelination of nascent lesions. Ann. Neurol. 1993, 33, 137–151. [CrossRef]
- Bramow, S.; Frischer, J.M.; Lassmann, H.; Koch-Henriksen, N.; Lucchinetti, C.F.; Sørensen, P.S.; Laursen, H. Demyelination versus remyelination in progressive multiple sclerosis. Brain 2010, 133, 2983–2998. [CrossRef]
- Magliozzi, R.; Howell, O.; Vora, A.; Serafini, B.; Nicholas, R.; Puopolo, M.; Reynolds, R.; Aloisi, F. Meningeal B-cell follicles in secondary progressive multiple sclerosis associate with early onset of disease and severe cortical pathology. Brain 2006, 130, 1089–1104. [CrossRef]
- Serafini, B.; Rosicarelli, B.; Magliozzi, R.; Stigliano, E.; Aloisi, F. Detection of Ectopic B-cell Follicles with Germinal Centers in the Meninges of Patients with Secondary Progressive Multiple Sclerosis. Brain Pathol. 2004, 14, 164–174. [CrossRef]
- Hochmeister, S.; Grundtner, R.; Bauer, J.; Engelhardt, B.; Lyck, R.; Gordon, G.; Korosec, T.; Kutzelnigg, A.; Berger, J.J.; Bradl, M.; et al. Dysferlin Is a New Marker for Leaky Brain Blood Vessels in Multiple Sclerosis. J. Neuropathol. Exp. Neurol. 2006, 65, 855–865. [CrossRef]
- Lassmann, H. Targets of therapy in progressive MS. Mult. Scler. J. 2017, 23, 1593–1599. [CrossRef]
- Kuhle, J.; Kropshofer, H.; Haering, D.A.; Kundu, U.; Meinert, R.; Barro, C.; Dahlke, F.; Tomic, D.; Leppert, D.; Kappos, L. Blood neurofilament light chain as a biomarker of MS disease activity and treatment response. Neurology 2019, 92, e1007–e1015. [CrossRef]
- Novakova L, Zetterberg H, Sundström P, Axelsson M, Khademi M, Gunnarsson M; et al. Monitoring disease activity in multiple sclerosis using serum neurofilament light protein. Neurology. 2017;89(22):2230-7. [CrossRef]
- Abdelhak, A.; Huss, A.; Kassubek, J.; Tumani, H.; Otto, M. Serum GFAP as a biomarker for disease severity in multiple sclerosis. Sci. Rep. 2018, 8, 14798. [CrossRef]
- Hinsinger, G.; Galéotti, N.; Nabholz, N.; Urbach, S.; Rigau, V.; Demattei, C.; Lehmann, S.; Camu, W.; Labauge, P.; Castelnovo, G.; et al. Chitinase 3-like proteins as diagnostic and prognostic biomarkers of multiple sclerosis. Mult. Scler. J. 2015, 21, 1251–1261. [CrossRef]
- Thompson, A.J.; Banwell, B.L.; Barkhof, F.; Carroll, W.M.; Coetzee, T.; Comi, G.; Correale, J.; Fazekas, F.; Filippi, M.; Freedman, M.S.; et al. Diagnosis of multiple sclerosis: 2017 revisions of the McDonald criteria. Lancet Neurol. 2018, 17, 162–173. [CrossRef]
- Ziemssen, T.; Akgün, K.; Brück, W. Molecular biomarkers in multiple sclerosis. J. Neuroinflamm. 2019, 16, 272. [CrossRef]
- Lebrun-Frénay, C.; Rollot, F.; Mondot, L.; Zephir, H.; Louapre, C.; Le Page, E.; Durand-Dubief, F.; Labauge, P.; Bensa, C.; Thouvenot, E.; et al. Risk Factors and Time to Clinical Symptoms of Multiple Sclerosis Among Patients With Radiologically Isolated Syndrome. JAMA Netw. Open 2021, 4, e2128271–e2128271. [CrossRef]
- Lebrun-Frenay, C.; Kantarci, O.; Siva, A.; Sormani, M.P.; Pelletier, D.; Okuda, D.T.; 10-year RISC study group on behalf of SFSEP, OFSEP Radiologically Isolated Syndrome: 10-Year Risk Estimate of a Clinical Event. Ann. Neurol. 2020, 88, 407–417. [CrossRef]
- Naseri, A.; Nasiri, E.; Sahraian, M.A.; Daneshvar, S.; Talebi, M. Clinical Features of Late-Onset Multiple Sclerosis: A Systematic Review and Meta-analysis. Mult. Scler. Relat. Disord. 2021, 50, 102816. [CrossRef]
- Kuhle, J.; Disanto, G.; Dobson, R.; Adiutori, R.; Bianchi, L.; Topping, J.; Bestwick, J.; Meier, U.-C.; Marta, M.; Costa, G.D.; et al. Conversion from clinically isolated syndrome to multiple sclerosis: A large multicentre study. Mult. Scler. J. 2015, 21, 1013–1024. [CrossRef]
- Kostulas VK, Link H, Lefvert AK. Oligoclonal IgG bands in cerebrospinal fluid. Principles for demonstration and interpretation based on findings in 1114 neurological patients. Arch Neurol. 1987;44(10):1041-4. [CrossRef]
- Chu, A.B.; Sever, J.L.; Madden, D.L.; Iivanainen, M.; Leon, M.; Wallen, W.; Brooks, B.R.; Lee, Y.J.; Houff, S. Oligoclonal IgG bands in cerebrospinal fluid in various neurological diseases. Ann. Neurol. 1983, 13, 434–439. [CrossRef]
- Simonsen, C.S.; Flemmen, H..; Lauritzen, T.; Berg-Hansen, P.; Moen, S.M.; Celius, E.G. The diagnostic value of IgG index versus oligoclonal bands in cerebrospinal fluid of patients with multiple sclerosis. Mult. Scler. J. - Exp. Transl. Clin. 2020, 6. [CrossRef]
- Mermelstein M, Naftali J, Wilf-Yarkoni A, Lotan I, Hellmann MA, Steiner I. Repeated lumbar puncture in search of oligoclonal bands – What is the yield? Journal of the Neurological Sciences. 2022;439:120298. [CrossRef]
- Lee, M.K.; Cleveland, D.W. Neurofilament function and dysfunction: Involvement in axonal growth and neuronal disease. Curr. Opin. Cell Biol. 1994, 6, 34–40. [CrossRef]
- Hoffman, P.N.; Cleveland, D.W.; Griffin, J.W.; Landes, P.W.; Cowan, N.J.; Price, D.L. Neurofilament gene expression: A major determinant of axonal caliber.. Proc. Natl. Acad. Sci. USA 1987, 84, 3472–3476. [CrossRef]
- Friede, R.L.; Samorajski, T. Axon caliber related to neurofilaments and microtubules in sciatic nerve fibers of rats and mice. Anat. Rec. 1970, 167, 379–387. [CrossRef]
- Yuan, A.; Sasaki, T.; Rao, M.V.; Kumar, A.; Kanumuri, V.; Dunlop, D.S.; Liem, R.K.; Nixon, R.A. Neurofilaments Form a Highly Stable Stationary Cytoskeleton after Reaching a Critical Level in Axons. J. Neurosci. 2009, 29, 11316–11329. [CrossRef]
- Kuhle, J.; Leppert, D.; Petzold, A.; Regeniter, A.; Schindler, C.; Mehling, M.; Anthony, D.; Kappos, L.; Lindberg, R. Neurofilament heavy chain in CSF correlates with relapses and disability in multiple sclerosis. Neurology 2011, 76, 1206–1213. [CrossRef]
- Malmeström, C.; Haghighi, S.; Rosengren, L.; Andersen, O.; Lycke, J. Neurofilament light protein and glial fibrillary acidic protein as biological markers in MS. Neurology 2003, 61, 1720–1725. [CrossRef]
- Semra, Y.; Seidi, O.; Sharief, M. Heightened intrathecal release of axonal cytoskeletal proteins in multiple sclerosis is associated with progressive disease and clinical disability. J. Neuroimmunol. 2002, 122, 132–139. [CrossRef]
- Kuhle, J.; Malmeström, C.; Axelsson, M.; Plattner, K.; Yaldizli, .; Derfuss, T.; Giovannoni, G.; Kappos, L.; Lycke, J. Neurofilament light and heavy subunits compared as therapeutic biomarkers in multiple sclerosis. Acta Neurol. Scand. 2013, 128, e33–e36. [CrossRef]
- Kuhle, J.; Plattner, K.; Bestwick, J.P.; Lindberg, R.L.; Ramagopalan, S.V.; Norgren, N.; Nissim, A.; Malaspina, A.; Leppert, D.; Giovannoni, G.; et al. A comparative study of CSF neurofilament light and heavy chain protein in MS. Mult. Scler. J. 2013, 19, 1597–1603. [CrossRef]
- Ferreira-Atuesta, C.; Reyes, S.; Giovanonni, G.; Gnanapavan, S. The Evolution of Neurofilament Light Chain in Multiple Sclerosis. Front. Neurosci. 2021, 15. [CrossRef]
- Khalil, M.; Pirpamer, L.; Hofer, E.; Voortman, M.M.; Barro, C.; Leppert, D.; Benkert, P.; Ropele, S.; Enzinger, C.; Fazekas, F.; et al. Serum neurofilament light levels in normal aging and their association with morphologic brain changes. Nat. Commun. 2020, 11, 1–9. [CrossRef]
- Gaetani, L.; Blennow, K.; Calabresi, P.; Di Filippo, M.; Parnetti, L.; Zetterberg, H. Neurofilament light chain as a biomarker in neurological disorders. J. Neurol. Neurosurg. Psychiatry 2019, 90, 870–881. [CrossRef]
- Engelborghs, S.; Niemantsverdriet, E.; Struyfs, H.; Blennow, K.; Brouns, R.; Comabella, M.; Dujmovic, I.; Van Der Flier, W.; Frölich, L.; Galimberti, D.; et al. Consensus guidelines for lumbar puncture in patients with neurological diseases. Alzheimer’s Dement.: Diagn. Assess. Dis. Monit. 2017, 8, 111–126. [CrossRef]
- Kuhle, J.; Barro, C.; Andreasson, U.; Derfuss, T.; Lindberg, R.; Sandelius, .; Liman, V.; Norgren, N.; Blennow, K.; Zetterberg, H. Comparison of three analytical platforms for quantification of the neurofilament light chain in blood samples: ELISA, electrochemiluminescence immunoassay and Simoa. cclm 2016, 54, 1655–1661. [CrossRef]
- Rissin, D.M.; Kan, C.W.; Campbell, T.G.; Howes, S.C.; Fournier, D.R.; Song, L.; Piech, T.; Patel, P.P.; Chang, L.; Rivnak, A.J.; et al. Single-molecule enzyme-linked immunosorbent assay detects serum proteins at subfemtomolar concentrations. Nat. Biotechnol. 2010, 28, 595–599. [CrossRef]
- Barro, C.; Benkert, P.; Disanto, G.; Tsagkas, C.; Amann, M.; Naegelin, Y.; Leppert, D.; Gobbi, C.; Granziera, C.; Yaldizli, .; et al. Serum neurofilament as a predictor of disease worsening and brain and spinal cord atrophy in multiple sclerosis. Brain 2018, 141, 2382–2391. [CrossRef]
- Disanto, G.; Barro, C.; Benkert, P.; Naegelin, Y.; Schädelin, S.; Giardiello, A.; Zecca, C.; Blennow, K.; Zetterberg, H.; Leppert, D.; et al. Serum Neurofilament light: A biomarker of neuronal damage in multiple sclerosis. Ann. Neurol. 2017, 81, 857–870. [CrossRef]
- Aharoni, R.; Eilam, R.; Lerner, S.; Shavit-Stein, E.; Dori, A.; Chapman, J.; Arnon, R. Neuroprotective Effect of Glatiramer Acetate on Neurofilament Light Chain Leakage and Glutamate Excess in an Animal Model of Multiple Sclerosis. Int. J. Mol. Sci. 2021, 22, 13419. [CrossRef]
- Salzer J, Svenningsson A, Sundström P. Neurofilament light as a prognostic marker in multiple sclerosis. Mult Scler. 2010;16(3):287-92. [CrossRef]
- Williams, T.; Zetterberg, H.; Chataway, J. Neurofilaments in progressive multiple sclerosis: A systematic review. J. Neurol. 2020, 268, 1–11. [CrossRef]
- Ferraro, D.; Guicciardi, C.; De Biasi, S.; Pinti, M.; Bedin, R.; Camera, V.; Vitetta, F.; Nasi, M.; Meletti, S.; Sola, P. Plasma neurofilaments correlate with disability in progressive multiple sclerosis patients. Acta Neurol. Scand. 2019, 141, 16–21. [CrossRef]
- Mañé-Martínez, M.; Olsson, B.; Bau, L.; Matas, E.; Cobo-Calvo, .; Andreasson, U.; Blennow, K.; Romero-Pinel, L.; Martínez-Yélamos, S.; Zetterberg, H. Glial and neuronal markers in cerebrospinal fluid in different types of multiple sclerosis. J. Neuroimmunol. 2016, 299, 112–117. [CrossRef]
- Novakova, L.; Axelsson, M.; Malmeström, C.; Imberg, H.; Elias, O.; Zetterberg, H.; Nerman, O.; Lycke, J. Searching for neurodegeneration in multiple sclerosis at clinical onset: Diagnostic value of biomarkers. PLoS ONE 2018, 13, e0194828. [CrossRef]
- Burman, J.; Zetterberg, H.; Fransson, M.; Loskog, A.S.; Raininko, R.; Fagius, J. Assessing tissue damage in multiple sclerosis: A biomarker approach. Acta Neurol. Scand. 2014, 130, 81–89. [CrossRef]
- Chatterjee, M.; Koel-Simmelink, M.J.; Verberk, I.M.; Killestein, J.; Vrenken, H.; Enzinger, C.; Ropele, S.; Fazekas, F.; Khalil, M.; E Teunissen, C. Contactin-1 and contactin-2 in cerebrospinal fluid as potential biomarkers for axonal domain dysfunction in multiple sclerosis. Mult. Scler. J. - Exp. Transl. Clin. 2018, 4. [CrossRef]
- Hendricks, R.; Baker, D.; Brumm, J.; Davancaze, T.; Harp, C.; Herman, A.; Von Büdingen, H.-C.; Townsend, M.; Fischer, S.K. Establishment of neurofilament light chain Simoa assay in cerebrospinal fluid and blood. Bioanalysis 2019, 11, 1405–1418. [CrossRef]
- Dhiman K, Gupta VB, Villemagne VL, Eratne D, Graham PL, Fowler C; et al. Cerebrospinal fluid neurofilament light concentration predicts brain atrophy and cognition in Alzheimer's disease. Alzheimer's & Dementia: Diagnosis, Assessment & Disease Monitoring. 2020;12(1):e12005. [CrossRef]
- Rosengren LE, Karlsson JE, Karlsson JO, Persson LI, Wikkelsø C. Patients with amyotrophic lateral sclerosis and other neurodegenerative diseases have increased levels of neurofilament protein in CSF. J Neurochem. 1996;67(5):2013-8. [CrossRef]
- Saraste, M.; Bezukladova, S.; Matilainen, M.; Tuisku, J.; Rissanen, E.; Sucksdorff, M.; Laaksonen, S.; Vuorimaa, A.; Kuhle, J.; Leppert, D.; et al. High serum neurofilament associates with diffuse white matter damage in MS. Neurol. - Neuroimmunol. Neuroinflammation 2021, 8. [CrossRef]
- Meeker, K.L.; Butt, O.H.; Gordon, B.A.; Fagan, A.M.; Schindler, S.E.; Morris, J.C.; Benzinger, T.L.; Ances, B.M. Cerebrospinal fluid neurofilament light chain is a marker of aging and white matter damage. Neurobiol. Dis. 2022, 166, 105662–105662. [CrossRef]
- Bridel C, van Wieringen WN, Zetterberg H, Tijms BM, Teunissen CE, Alvarez-Cermeño JC; et al. Diagnostic Value of Cerebrospinal Fluid Neurofilament Light Protein in Neurology: A Systematic Review and Meta-analysis. JAMA Neurol. 2019;76(9):1035-48. [CrossRef]
- Pérez-Miralles, F.; Prefasi, D.; García-Merino, A.; Gascón-Giménez, F.; Medrano, N.; Castillo-Villalba, J.; Cubas, L.; Alcalá, C.; Gil-Perotín, S.; Gómez-Ballesteros, R.; et al. CSF chitinase 3-like-1 association with disability of primary progressive MS. Neurol. - Neuroimmunol. Neuroinflammation 2020, 7. [CrossRef]
- Malmeström C, Axelsson M, Lycke J, Zetterberg H, Blennow K, Olsson B. CSF levels of YKL-40 are increased in MS and replaces with immunosuppressive treatment. J Neuroimmunol. 2014;269(1-2):87-9. [CrossRef]
- Kušnierová, P.; Zeman, D.; Hradílek, P.; Zapletalová, O.; Stejskal, D. Determination of chitinase 3-like 1 in cerebrospinal fluid in multiple sclerosis and other neurological diseases. PLoS ONE 2020, 15, e0233519. [CrossRef]
- Matute-Blanch, C.; Calvo-Barreiro, L.; Carballo-Carbajal, I.; Gonzalo, R.; Sanchez, A.; Vila, M.; Montalban, X.; Comabella, M. Chitinase 3-like 1 is neurotoxic in primary cultured neurons. Sci. Rep. 2020, 10, 7118. [CrossRef]
- Schneider, R.; Bellenberg, B.; Gisevius, B.; Hirschberg, S.; Sankowski, R.; Prinz, M.; Gold, R.; Lukas, C.; Haghikia, A. Chitinase 3–like 1 and neurofilament light chain in CSF and CNS atrophy in MS. Neurol. - Neuroimmunol. Neuroinflammation 2021, 8. [CrossRef]
- Cantó, E.; Tintoré, M.; Villar, L.M.; Costa, C.; Nurtdinov, R.; Álvarez-Cermeño, J.C.; Arrambide, G.; Reverter, F.; Deisenhammer, F.; Hegen, H.; et al. Chitinase 3-like 1: Prognostic biomarker in clinically isolated syndromes. Brain 2015, 138, 918–931. [CrossRef]
- Håkansson, I.; Tisell, A.; Cassel, P.; Blennow, K.; Zetterberg, H.; Lundberg, P.; Dahle, C.; Vrethem, M.; Ernerudh, J. Neurofilament levels, disease activity and brain volume during follow-up in multiple sclerosis. J. Neuroinflammation 2018, 15, 1–10. [CrossRef]
- Cantó, E.; Reverter, F.; Morcillo-Suárez, C.; Matesanz, F.; Fernández, O.; Izquierdo, G.; Vandenbroeck, K.; Rodríguez-Antigüedad, A.; Urcelay, E.; Arroyo, R.; et al. Chitinase 3-like 1 plasma levels are increased in patients with progressive forms of multiple sclerosis. Mult. Scler. J. 2011, 18, 983–990. [CrossRef]
- Gil-Perotin, S.; Castillo-Villalba, J.; Cubas-Nuñez, L.; Gasque, R.; Hervas, D.; Gomez-Mateu, J.; Alcala, C.; Perez-Miralles, F.; Gascon, F.; Dominguez, J.A.; et al. Combined Cerebrospinal Fluid Neurofilament Light Chain Protein and Chitinase-3 Like-1 Levels in Defining Disease Course and Prognosis in Multiple Sclerosis. Front. Neurol. 2019, 10, 1008. [CrossRef]
- Correale, J.; Fiol, M. Chitinase effects on immune cell response in neuromyelitis optica and multiple sclerosis. Mult. Scler. J. 2010, 17, 521–531. [CrossRef]
- Wang, Z.; Wang, R.; Li, Y.; Li, M.; Zhang, Y.; Jiang, L.; Fan, J.; Wang, Q.; Yang, D. Plasma Neurofilament Light Chain as a Predictive Biomarker for Post-stroke Cognitive Impairment: A Prospective Cohort Study. Front. Aging Neurosci. 2021, 13. [CrossRef]
- Evangelou N, Esiri MM, Smith S, Palace J, Matthews PM. Quantitative pathological evidence for axonal loss in normal appearing white matter in multiple sclerosis. Ann Neurol. 2000;47(3):391-5.
- Filippi, M.; Campi, A.; Dousset, V.; Baratti, C.; Martinelli, V.; Canal, N.; Scotti, G.; Comi, G. A Magnetization Transfer Imaging Study of Normal-Appearing White Matter in Multiple Sclerosis. Neurology 1995, 45, 478–482. [CrossRef]
- Zivadinov, R.; Uher, T.; Hagemeier, J.; Vaneckova, M.; Ramasamy, D.P.; Tyblova, M.; Bergsland, N.; Seidl, Z.; Dwyer, M.G.; Krasensky, J.; et al. A serial 10-year follow-up study of brain atrophy and disability progression in RRMS patients. Mult. Scler. J. 2016, 22, 1709–1718. [CrossRef]
- Eijlers, A.J.; Dekker, I.; Steenwijk, M.D.; Meijer, K.A.; Hulst, H.E.; Pouwels, P.J.; Uitdehaag, B.M.; Barkhof, F.; Vrenken, H.; Schoonheim, M.M.; et al. Cortical atrophy accelerates as cognitive decline worsens in multiple sclerosis. Neurology 2019, 93, e1348–e1359. [CrossRef]
- Warntjes, J.; Tisell, A.; Håkansson, I.; Lundberg, P.; Ernerudh, J. Improved Precision of Automatic Brain Volume Measurements in Patients with Clinically Isolated Syndrome and Multiple Sclerosis Using Edema Correction. Am. J. Neuroradiol. 2017, 39, 296–302. [CrossRef]
- Cheriyan, J.; Kim, S.; Wolansky, L.J.; Cook, S.D.; Cadavid, D. Impact of Inflammation on Brain Volume in Multiple Sclerosis. Arch. Neurol. 2012, 69, 82. [CrossRef]
- Scahill, R.I.; Frost, C.; Jenkins, R.; Whitwell, J.L.; Rossor, M.N.; Fox, N.C. A Longitudinal Study of Brain Volume Changes in Normal Aging Using Serial Registered Magnetic Resonance Imaging. Arch. Neurol. 2003, 60, 989–94. [CrossRef]
- Ghione, E.; Bergsland, N.; Dwyer, M.G.; Hagemeier, J.; Jakimovski, D.; Paunkoski, I.; Ramasamy, D.P.; Carl, E.; Hojnacki, D.; Kolb, C.; et al. Aging and Brain Atrophy in Multiple Sclerosis. J. Neuroimaging 2019, 29, 527–535. [CrossRef]
- Filippi, M.; Cercignani, M.; Inglese, M.; Horsfield, M.; Comi, G. Diffusion tensor magnetic resonance imaging in multiple sclerosis. Neurology 2001, 56, 304–311. [CrossRef]
- de Sitter A, Steenwijk MD, Ruet A, Versteeg A, Liu Y, van Schijndel RA; et al. Performance of five research-domain automated WM lesion segmentation methods in a multi-center MS study. Neuroimage. 2017;163:106-14. [CrossRef]
- van Walderveen MA, Lycklama ANGJ, Adèr HJ, Jongen PJ, Polman CH, Castelijns JA; et al. Hypointense lesions on T1-weighted spin-echo magnetic resonance imaging: Relation to clinical characteristics in subgroups of patients with multiple sclerosis. Arch Neurol. 2001;58(1):76-81. [CrossRef]
- Fisniku, L.K.; Brex, P.A.; Altmann, D.R.; Miszkiel, K.A.; Benton, C.E.; Lanyon, R.; Thompson, A.J.; Miller, D.H. Disability and T2 MRI lesions: A 20-year follow-up of patients with relapse onset of multiple sclerosis. Brain 2008, 131, 808–817. [CrossRef]
- Klistorner, S.; Barnett, M.H.; Yiannikas, C.; Barton, J.; Parratt, J.; You, Y.; Graham, S.L.; Klistorner, A. Expansion of chronic lesions is linked to disease progression in relapsing–remitting multiple sclerosis patients. Mult. Scler. J. 2020, 27, 1533–1542. [CrossRef]
- Polman, C.H.; Reingold, S.C.; Banwell, B.; Clanet, M.; Cohen, J.A.; Filippi, M.; Fujihara, K.; Havrdova, E.; Hutchinson, M.; Kappos, L.; et al. Diagnostic criteria for multiple sclerosis: 2010 Revisions to the McDonald criteria. Ann. Neurol. 2011, 69, 292–302. [CrossRef]
- Tillema, J.-M.; Pirko, I. Neuroradiological evaluation of demyelinating disease. Ther. Adv. Neurol. Disord. 2013, 6, 249–268. [CrossRef]
- Li DK, Held U, Petkau J, Daumer M, Barkhof F, Fazekas F; et al. MRI T2 lesion burden in multiple sclerosis: A plateauing relationship with clinical disability. Neurology. 2006;66(9):1384-9. [CrossRef]
- Mostert, J.P.; Koch, M.W.; Steen, C.; Heersema, D.J.; De Groot, J.C.; De Keyser, J. T2 lesions and rate of progression of disability in multiple sclerosis. Eur. J. Neurol. 2010, 17, 1471–1475. [CrossRef]
- Ciccarelli, O.; Brex, P.A.; Thompson, A.J.; Miller, D.H. Disability and lesion load in MS: A reassessment with MS functional composite score and 3D fast FLAIR.. J. Neurol. 2002, 249, 18–24. [CrossRef]
- Radue, E.-W.; O’connor, P.; Polman, C.H.; Hohlfeld, R.; Calabresi, P.; Selmaj, K.; Mueller-Lenke, N.; Agoropoulou, C.; Holdbrook, F.; de Vera, A.; et al. Impact of Fingolimod Therapy on Magnetic Resonance Imaging Outcomes in Patients With Multiple Sclerosis. Arch. Neurol. 2012, 69, 1259–1269. [CrossRef]
- Comi, G.; Filippi, M.; Wolinsky, J.S. European/Canadian multicenter, double-blind, randomized, placebo-controlled study of the effects of glatiramer acetate on magnetic resonance imaging--measured disease activity and burden in patients with relapsing multiple sclerosis. European/Canadian Glatiramer Acetate Study Group.. 2001, 49, 290–7. [CrossRef]
- Ebers, G.C. Randomised double-blind placebo-controlled study of interferon β-1a in relapsing/remitting multiple sclerosis. Lancet 1998, 352, 1498–1504. [CrossRef]
- Elliott, C.; Belachew, S.; Wolinsky, J.S.; Hauser, S.L.; Kappos, L.; Barkhof, F.; Bernasconi, C.; Fecker, J.; Model, F.; Wei, W.; et al. Chronic white matter lesion activity predicts clinical progression in primary progressive multiple sclerosis. Brain 2019, 142, 2787–2799. [CrossRef]
- Kocsis, K.; Szabó, N.; Tóth, E.; Király, A.; Faragó, P.; Kincses, B.; Veréb, D.; Bozsik, B.; Boross, K.; Katona, M.; et al. Two Classes of T1 Hypointense Lesions in Multiple Sclerosis With Different Clinical Relevance. Front. Neurol. 2021, 12. [CrossRef]
- Truyen, L.; van Waesberghe, J.H.; van Walderveen, M.; van Oosten, B.W.; Polman, C.H.; Hommes, O.R.; Ader, H.J.; Barkhof, F. Accumulation of hypointense lesions ("black holes") on T 1 spin-echo MRI correlates with disease progression in multiple sclerosis. Neurology 1996, 47, 1469–1476. [CrossRef]
- Bagnato, F.; Jeffries, N.; Richert, N.D.; Stone, R.D.; Ohayon, J.M.; McFarland, H.F.; Frank, J.A. Evolution of T1 black holes in patients with multiple sclerosis imaged monthly for 4 years. Brain 2003, 126, 1782–1789. [CrossRef]
- Andermatt, S.; Papadopoulou, A.; Radue, E.-W.; Sprenger, T.; Cattin, P. Tracking the Evolution of Cerebral Gadolinium-Enhancing Lesions to Persistent T1 Black Holes in Multiple Sclerosis: Validation of a Semiautomated Pipeline. J. Neuroimaging 2017, 27, 469–475. [CrossRef]
- Elskamp, I.v.D.; Lembcke, J.; Dattola, V.; Beckmann, K.; Pohl, C.; Hong, W.; Sandbrink, R.; Wagner, K.; Knol, D.; Uitdehaag, B.; et al. Persistent T1 hypointensity as an MRI marker for treatment efficacy in multiple sclerosis. Mult. Scler. J. 2008, 14, 764–769. [CrossRef]
- van Waesberghe JH, van Walderveen MA, Castelijns JA, Scheltens P, Lycklama à Nijeholt GJ, Polman CH; et al. Patterns of lesion development in multiple sclerosis: Longitudinal observations with T1-weighted spin-echo and magnetization transfer MR. AJNR Am J Neuroradiol. 1998;19(4):675-83.
- Filippi, M.; Rovaris, M.; Rocca, M.A.; Sormani, M.P.; Wolinsky, J.S.; Comi, G. Glatiramer acetate reduces the proportion of new MS lesions evolving into "black holes". Neurology 2001, 57, 731–733. [CrossRef]
- Oommen VV, Tauhid S, Healy BC, Chua AS, Malik MT, Diaz-Cruz C; et al. The Effect of Fingolimod on Conversion of Acute Gadolinium-Enhancing Lesions to Chronic T1 Hypointensities in Multiple Sclerosis. Journal of neuroimaging : Official journal of the American Society of Neuroimaging. 2016;26(2):184-7. [CrossRef]
- Beckers, L.; Ory, D.; Geric, I.; Declercq, L.; Koole, M.; Kassiou, M.; Bormans, G.; Baes, M. Increased Expression of Translocator Protein (TSPO) Marks Pro-inflammatory Microglia but Does Not Predict Neurodegeneration. Mol. Imaging Biol. 2017, 20, 94–102. [CrossRef]
- Sadigh G, Saindane AM, Waldman AD, Lava NS, Hu R. Comparison of Unenhanced and Gadolinium-Enhanced Imaging in Multiple Sclerosis: Is Contrast Needed for Routine Follow-Up MRI? AJNR Am J Neuroradiol. 2019;40(9):1476-80.
- Bruschi, N.; Boffa, G.; Inglese, M. Ultra-high-field 7-T MRI in multiple sclerosis and other demyelinating diseases: From pathology to clinical practice. Eur. Radiol. Exp. 2020, 4, 1–13. [CrossRef]
- Luchetti, S.; Fransen, N.L.; van Eden, C.G.; Ramaglia, V.; Mason, M.; Huitinga, I. Progressive multiple sclerosis patients show substantial lesion activity that correlates with clinical disease severity and sex: A retrospective autopsy cohort analysis. Acta Neuropathol. 2018, 135, 511–528. [CrossRef]
- Sbardella, E.; Tona, F.; Petsas, N.; Pantano, P. DTI Measurements in Multiple Sclerosis: Evaluation of Brain Damage and Clinical Implications. Mult. Scler. Int. 2013, 2013, 1–11. [CrossRef]
- Budde, M.D.; Kim, J.H.; Liang, H.; Russell, J.H.; Cross, A.H.; Song, S. Axonal injury detected by in vivo diffusion tensor imaging correlates with neurological disability in a mouse model of multiple sclerosis. NMR Biomed. 2007, 21, 589–597. [CrossRef]
- Nishioka, C.; Liang, H.-F.; Barsamian, B.; Sun, S.-W. Sequential phases of RGC axonal and somatic injury in EAE mice examined using DTI and OCT. Mult. Scler. Relat. Disord. 2018, 27, 315–323. [CrossRef]
- Naismith, R.T.; Xu, J.; Tutlam, N.T.; Snyder, A.; Benzinger, T.; Shimony, J.; Shepherd, J.; Trinkaus, K.; Cross, A.H.; Song, S.-K. Disability in optic neuritis correlates with diffusion tensor-derived directional diffusivities. Neurology 2009, 72, 589–594. [CrossRef]
- Budde, M.D.; Xie, M.; Cross, A.H.; Song, S.-K. Axial Diffusivity Is the Primary Correlate of Axonal Injury in the Experimental Autoimmune Encephalomyelitis Spinal Cord: A Quantitative Pixelwise Analysis. J. Neurosci. 2009, 29, 2805–2813. [CrossRef]
- Andersen, O.; Hildeman, A.; Longfils, M.; Tedeholm, H.; Skoog, B.; Tian, W.; Zhong, J.; Ekholm, S.; Novakova, L.; Runmarker, B.; et al. Diffusion tensor imaging in multiple sclerosis at different final outcomes. Acta Neurol. Scand. 2017, 137, 165–173. [CrossRef]
- Gujar SK, Maheshwari S, Björkman-Burtscher I, Sundgren PC. Magnetic resonance spectroscopy. J Neuroophthalmol. 2005;25(3):217-26.
- Tognarelli, J.M.; Dawood, M.; Shariff, M.I.; Grover, V.P.; Crossey, M.M.; Cox, I.J.; Taylor-Robinson, S.D.; McPhail, M.J. Magnetic Resonance Spectroscopy: Principles and Techniques: Lessons for Clinicians. J. Clin. Exp. Hepatol. 2015, 5, 320–328. [CrossRef]
- De Stefano, N.; Narayanan, S.; Francis, S.J.; Smith, S.; Mortilla, M.; Tartaglia, M.C.; Bartolozzi, M.L.; Guidi, L.; Federico, A.; Arnold, D.L. Diffuse Axonal and Tissue Injury in Patients With Multiple Sclerosis With Low Cerebral Lesion Load and No Disability. Arch. Neurol. 2002, 59, 1565–1571. [CrossRef]
- Tartaglia, M.C.; Narayanan, S.; De Stefano, N.; Arnaoutelis, R.; Antel, S.B.; Francis, S.J.; Santos, A.C.; Lapierre, Y.; Arnold, D.L. Choline is increased in pre-lesional normal appearing white matter in multiple sclerosis. J. Neurol. 2002, 249, 1382–1390. [CrossRef]
- Suhy J, Rooney WD, Goodkin DE, Capizzano AA, Soher BJ, Maudsley AA; et al. 1H MRSI comparison of white matter and lesions in primary progressive and relapsing-remitting MS. Mult Scler. 2000;6(3):148-55. [CrossRef]
- Hannoun S, Bagory M, Durand-Dubief F, Ibarrola D, Comte JC, Confavreux C; et al. Correlation of diffusion and metabolic alterations in different clinical forms of multiple sclerosis. PLoS ONE. 2012;7(3):e32525. [CrossRef]
- Inglese, M.; Li, B.S.; Rusinek, H.; Babb, J.S.; Grossman, R.I.; Gonen, O. Diffusely elevated cerebral choline and creatine in relapsing-remitting multiple sclerosis. Magn. Reson. Med. 2003, 50, 190–195. [CrossRef]
- Vrenken, H.; Barkhof, F.; Uitdehaag, B.; Castelijns, J.; Polman, C.; Pouwels, P. MR spectroscopic evidence for glial increase but not for neuro-axonal damage in MS normal-appearing white matter. Magn. Reson. Med. 2005, 53, 256–266. [CrossRef]
- Li, B.S.; Wang, H.; Gonen, O. Metabolite ratios to assumed stable creatine level may confound the quantification of proton brain MR spectroscopy. Magn. Reson. Imaging 2003, 21, 923–928. [CrossRef]
- Bagory, M.; Durand-Dubief, F.; Ibarrola, D.; Confavreux, C.; Sappey-Marinier, D. "Absolute" quantification in Magnetic Resonance Spectroscopy: Validation of a clinical protocol in multiple sclerosis. 2007 29th Annual International Conference of the IEEE Engineering in Medicine and Biology Society. LOCATION OF CONFERENCE, FranceDATE OF CONFERENCE; pp. 3458–3461.
- Narayana PA. Magnetic resonance spectroscopy in the monitoring of multiple sclerosis. Journal of neuroimaging : Official journal of the American Society of Neuroimaging. 2005;15(4 Suppl):46S-57S. [CrossRef]
- Larsson, H.B.W.; Christiansen, P.; Jensen, M.; Frederiksen, J.; Heltberg, A.; Olesen, J.; Henriksen, O. Localized in vivo proton spectroscopy in the brain of patients with multiple sclerosis. Magn. Reson. Med. 1991, 22, 23–31. [CrossRef]
- De Stefano, N.; Narayanan, S.; Francis, G.S.; Arnaoutelis, R.; Tartaglia, M.C.; Antel, J.P.; Matthews, P.M.; Arnold, D.L. Evidence of Axonal Damage in the Early Stages of Multiple Sclerosis and Its Relevance to Disability. Arch. Neurol. 2001, 58, 65–70. [CrossRef]
- Simone, I.; Tortorella, C.; Federico, F.; Liguori, M.; Lucivero, V.; Giannini, P.; Carrara, D.; Bellacosa, A.; Livrea, P. Axonal damage in multiple sclerosis plaques: A combined magnetic resonance imaging and 1H-magnetic resonance spectroscopy study. J. Neurol. Sci. 2001, 182, 143–150. [CrossRef]
- Aboul-Enein, F.; Krššák, M.; Höftberger, R.; Prayer, D.; Kristoferitsch, W. Reduced NAA-Levels in the NAWM of Patients with MS Is a Feature of Progression. A Study with Quantitative Magnetic Resonance Spectroscopy at 3 Tesla. PLoS ONE 2010, 5, e11625. [CrossRef]
- Rigotti DJ, Inglese M, Kirov, II, Gorynski E, Perry NN, Babb JS; et al. Two-year serial whole-brain N-acetyl-L-aspartate in patients with relapsing-remitting multiple sclerosis. Neurology. 2012;78(18):1383-9. [CrossRef]
- Sun, J.; Song, H.; Yang, Y.; Zhang, K.; Gao, X.; Li, X.; Ni, L.; Lin, P.; Niu, C. Metabolic changes in normal appearing white matter in multiple sclerosis patients using multivoxel magnetic resonance spectroscopy imaging. Medicine 2017, 96, e6534. [CrossRef]
- Tourbah, A.; Stievenart, J.; Gout, O.; Fontaine, B.; Liblau, R.; Lubetzki, C.; Cabanis, E.; Lyon-Caen, O. Localized proton magnetic resonance spectroscopy in relapsing remitting versus secondary progressive multiple sclerosis. Neurology 1999, 53, 1091–1091. [CrossRef]
- Tedeschi, G.; Bonavita, S.; McFarland, H.; Richert, N.; Duyn, J.; Frank, J. Proton MR spectroscopic imaging in multiple sclerosis. Neuroradiology 2002, 44, 37–42. [CrossRef]
- Cucurella MG, Rovira A, Río J, Pedraza S, Tintoré MM, Montalbán X; et al. Proton magnetic resonance spectroscopy in primary and secondary progressive multiple sclerosis. NMR Biomed. 2000;13(2):57-63. [CrossRef]
- Ruiz-Peña, J.L.; Piñero, P.; Sellers, G.; Argente, J.; Casado, A.; Foronda, J.; Uclés, A.; Izquierdo, G. Magnetic resonance spectroscopy of normal appearing white matter in early relapsing-remitting multiple sclerosis: Correlations between disability and spectroscopy. BMC Neurol. 2004, 4, 8–8. [CrossRef]
- Wu, X.; Hanson, L.G.; Skimminge, A.; Sorensen, P.S.; Paulson, O.B.; Mathiesen, H.K.; Blinkenberg, M. CorticalN-acetyl aspartate is a predictor of long-term clinical disability in multiple sclerosis. Neurol. Res. 2014, 36, 701–708. [CrossRef]
- Britze, J.; Frederiksen, J.L. Optical coherence tomography in multiple sclerosis. Eye 2018, 32, 884–888. [CrossRef]
- Mehmood A, Ali W, Song S, Din ZU, Guo RY, Shah W; et al. Optical coherence tomography monitoring and diagnosing retinal changes in multiple sclerosis. Brain Behav. 2021;11(10):e2302. [CrossRef]
- Toussaint, D.; Périer, O.; Verstappen, A.; Bervoets, S. Clinicopathological study of the visual pathways, eyes, and cerebral hemispheres in 32 cases of disseminated sclerosis.. 1983, 3, 211–20.
- Cruz-Herranz, A.; Balk, L.J.; Oberwahrenbrock, T.; Saidha, S.; Martinez-Lapiscina, E.H.; Lagreze, W.A.; Schuman, J.S.; Villoslada, P.; Calabresi, P.; Balcer, L.; et al. The APOSTEL recommendations for reporting quantitative optical coherence tomography studies. Neurology 2016, 86, 2303–2309. [CrossRef]
- Straatsma BR, Foos RY, Heckenlively JR, Taylor GN. Myelinated Retinal Nerve Fibers. American Journal of Ophthalmology. 1981;91(1):25-38.
- Ratchford, J.N.; Saidha, S.; Sotirchos, E.S.; Oh, J.A.; Seigo, M.A.; Eckstein, C.; Durbin, M.K.; Oakley, J.D.; Meyer, S.A.; Conger, A.; et al. Active MS is associated with accelerated retinal ganglion cell/inner plexiform layer thinning. Neurology 2013, 80, 47–54. [CrossRef]
- Klistorner, A.; Sriram, P.; Vootakuru, N.; Wang, C.; Barnett, M.H.; Garrick, R.; Parratt, J.; Levin, N.; Raz, N.; Van der Walt, A.; et al. Axonal loss of retinal neurons in multiple sclerosis associated with optic radiation lesions. Neurology 2014, 82, 2165–2172. [CrossRef]
- Shen, J.; Yang, Q.; Yu, D.; Wu, J.; Zhu, Y.; Guo, W. Vulnerability study of myelinated and unmyelinated nerve fibers in acute ocular hypertension in rabbit. Mol. Med. Rep. 2017, 16, 6794–6802. [CrossRef]
- Albrecht, P.; Ringelstein, M.; Müller, A.; Keser, N.; Dietlein, T.; Lappas, A.; Foerster, A.; Hartung, H.; Aktas, O.; Methner, A. Degeneration of retinal layers in multiple sclerosis subtypes quantified by optical coherence tomography. Mult. Scler. J. 2012, 18, 1422–1429. [CrossRef]
- Davies, E.C.; Galetta, K.M.; Sackel, D.J.; Talman, L.S.; Frohman, E.M.; A Calabresi, P.; Galetta, S.L.; Balcer, L.J. Retinal Ganglion Cell Layer Volumetric Assessment by Spectral-Domain Optical Coherence Tomography in Multiple Sclerosis: Application of a High-Precision Manual Estimation Technique. J. Neuro-Ophthalmology 2011, 31, 260–264. [CrossRef]
- Walter, S.D.; Ishikawa, H.; Galetta, K.M.; Sakai, R.E.; Feller, D.J.; Henderson, S.B.; Wilson, J.A.; Maguire, M.G.; Galetta, S.L.; Frohman, E.; et al. Ganglion Cell Loss in Relation to Visual Disability in Multiple Sclerosis. Ophthalmology 2012, 119, 1250–1257. [CrossRef]
- Talman, L.S.; Bisker, E.R.; Sackel, D.J.; Long, D.A.; Galetta, K.M.; Ratchford, J.N.; Lile, D.J.; Farrell, S.K.; Loguidice, M.J.; Remington, G.; et al. Longitudinal study of vision and retinal nerve fiber layer thickness in multiple sclerosis. Ann. Neurol. 2010, 67, 749–760. [CrossRef]
- Garcia-Martin E, Ara JR, Martin J, Almarcegui C, Dolz I, Vilades E; et al. Retinal and Optic Nerve Degeneration in Patients with Multiple Sclerosis Followed up for 5 Years. Ophthalmology. 2017;124(5):688-96. [CrossRef]
- Paul, F.; Calabresi, P.A.; Barkhof, F.; Green, A.J.; Kardon, R.; Sastre-Garriga, J.; Schippling, S.; Vermersch, P.; Saidha, S.; Gerendas, B.S.; et al. Optical coherence tomography in multiple sclerosis: A 3-year prospective multicenter study. Ann. Clin. Transl. Neurol. 2021, 8, 2235–2251. [CrossRef]
- Bock, M.; Brandt, A.U.; Dörr, J.; Pfueller, C.F.; Ohlraun, S.; Zipp, F.; Paul, F. Time domain and spectral domain optical coherence tomography in multiple sclerosis: A comparative cross-sectional study. Mult. Scler. J. 2010, 16, 893–896. [CrossRef]
- Behbehani, R.; Abu Al-Hassan, A.; Al-Salahat, A.; Sriraman, D.; Oakley, J.D.; Alroughani, R. Optical coherence tomography segmentation analysis in relapsing remitting versus progressive multiple sclerosis. PLoS ONE 2017, 12, e0172120. [CrossRef]
- Garcia-Martin, E.; Polo, V.; Larrosa, J.M.; Marques, M.L.; Herrero, R.; Martin, J.; Ara, J.R.; Fernandez, J.; Pablo, L.E. Retinal Layer Segmentation in Patients with Multiple Sclerosis Using Spectral Domain Optical Coherence Tomography. Ophthalmology 2014, 121, 573–579. [CrossRef]
- Cordon, B.; Vilades, E.; Orduna, E.; Satue, M.; Perez-Velilla, J.; Sebastian, B.; Polo, V.; Larrosa, J.M.; Pablo, L.E.; Garcia-Martin, E. Angiography with optical coherence tomography as a biomarker in multiple sclerosis. PLoS ONE 2020, 15, e0243236. [CrossRef]
- Ulusoy, M.O.; Horasanlı, B.; Işık-Ulusoy, S. Optical coherence tomography angiography findings of multiple sclerosis with or without optic neuritis. Neurol. Res. 2020, 42, 319–326. [CrossRef]
- Giovannoni, G.; Lai, M.; Thorpe, J.; Kidd, D.; Chamoun, V.; Thompson, A.J.; Miller, D.H.; Feldmann, M.; Thompson, E.J. Longitudinal study of soluble adhesion molecules in multiple sclerosis. Neurology 1997, 48, 1557–1565. [CrossRef]
- Kirbas, S.; Turkyilmaz, K.; Anlar, O.; Tufekci, A.; Durmus, M. Retinal Nerve Fiber Layer Thickness in Patients With Alzheimer Disease. J. Neuro-Ophthalmology 2013, 33, 58–61. [CrossRef]
- Moreno-Ramos T, Benito-León J, Villarejo A, Bermejo-Pareja F. Retinal nerve fiber layer thinning in dementia associated with Parkinson's disease, dementia with Lewy bodies, and Alzheimer's disease. J Alzheimers Dis. 2013;34(3):659-64. [CrossRef]
- Cipollini V, Abdolrahimzadeh S, Troili F, De Carolis A, Calafiore S, Scuderi L; et al. Neurocognitive Assessment and Retinal Thickness Alterations in Alzheimer Disease: Is There a Correlation? J Neuroophthalmol. 2020;40(3):370-7. [CrossRef]
- Nutma, E.; Gebro, E.; Marzin, M.C.; van der Valk, P.; Matthews, P.M.; Owen, D.R.; Amor, S. Activated microglia do not increase 18 kDa translocator protein (TSPO) expression in the multiple sclerosis brain. Glia 2021, 69, 2447–2458. [CrossRef]
- Bezukladova, S.; Tuisku, J.; Matilainen, M.; Vuorimaa, A.; Nylund, M.; Smith, S.; Sucksdorff, M.; Mohammadian, M.; Saunavaara, V.; Laaksonen, S.; et al. Insights into disseminated MS brain pathology with multimodal diffusion tensor and PET imaging. Neurol. - Neuroimmunol. Neuroinflammation 2020, 7. [CrossRef]
- Banati RB, Newcombe J, Gunn RN, Cagnin A, Turkheimer F, Heppner F; et al. The peripheral benzodiazepine binding site in the brain in multiple sclerosis: Quantitative in vivo imaging of microglia as a measure of disease activity. Brain. 2000;123(11):2321-37. [CrossRef]
- Nutma, E.; A Stephenson, J.; Gorter, R.P.; de Bruin, J.; Boucherie, D.M.; Donat, C.K.; Breur, M.; van der Valk, P.; Matthews, P.M.; Owen, D.R.; et al. A quantitative neuropathological assessment of translocator protein expression in multiple sclerosis. Brain 2019, 142, 3440–3455. [CrossRef]
- Debruyne, J.C.; Versijpt, J.; Van Laere, K.J.; De Vos, F.; Keppens, J.; Strijckmans, K.; Achten, E.; Slegers, G.; Dierckx, R.A.; Korf, J.; et al. PET visualization of microglia in multiple sclerosis patients using [11C]PK11195. Eur. J. Neurol. 2003, 10, 257–264. [CrossRef]
- Datta G, Colasanti A, Kalk N, Owen D, Scott G, Rabiner EA; et al. (11)C-PBR28 and (18)F-PBR111 Detect White Matter Inflammatory Heterogeneity in Multiple Sclerosis. J Nucl Med. 2017;58(9):1477-82. [CrossRef]
- Vignal, N.; Cisternino, S.; Rizzo-Padoin, N.; San, C.; Hontonnou, F.; Gelé, T.; Declèves, X.; Sarda-Mantel, L.; Hosten, B. [18F]FEPPA a TSPO Radioligand: Optimized Radiosynthesis and Evaluation as a PET Radiotracer for Brain Inflammation in a Peripheral LPS-Injected Mouse Model. Molecules 2018, 23, 1375. [CrossRef]
- Ikawa, M.; Lohith, T.G.; Shrestha, S.; Telu, S.; Zoghbi, S.S.; Castellano, S.; Taliani, S.; Da Settimo, F.; Fujita, M.; Pike, V.W.; et al. 11C-ER176, a Radioligand for 18-kDa Translocator Protein, Has Adequate Sensitivity to Robustly Image All Three Affinity Genotypes in Human Brain. J. Nucl. Med. 2017, 58, 320–325. [CrossRef]
- Rissanen, E.; Tuisku, J.; Rokka, J.; Paavilainen, T.; Parkkola, R.; Rinne, J.O.; Airas, L. In Vivo Detection of Diffuse Inflammation in Secondary Progressive Multiple Sclerosis Using PET Imaging and the Radioligand 11C-PK11195. J. Nucl. Med. 2014, 55, 939–944. [CrossRef]
- Ching, A.S.C.; Kuhnast, B.; Damont, A.; Roeda, D.; Tavitian, B.; Dollé, F. Current paradigm of the 18-kDa translocator protein (TSPO) as a molecular target for PET imaging in neuroinflammation and neurodegenerative diseases. Insights into Imaging 2011, 3, 111–119. [CrossRef]
- Narayanaswami, V.; Dahl, K.; Bernard-Gauthier, V.; Josephson, L.; Cumming, P.; Vasdev, N. Emerging PET Radiotracers and Targets for Imaging of Neuroinflammation in Neurodegenerative Diseases: Outlook Beyond TSPO. Mol. Imaging 2018, 17. [CrossRef]
- Owen, D.R.; Narayan, N.; Wells, L.; Healy, L.; Smyth, E.; A Rabiner, E.; Galloway, D.; Williams, J.B.; Lehr, J.; Mandhair, H.; et al. Pro-inflammatory activation of primary microglia and macrophages increases 18 kDa translocator protein expression in rodents but not humans. J. Cereb. Blood Flow Metab. 2017, 37, 2679–2690. [CrossRef]
- Driscoll I, Troncoso JC, Rudow G, Sojkova J, Pletnikova O, Zhou Y; et al. Correspondence between in vivo (11)C-PiB-PET amyloid imaging and postmortem, region-matched assessment of plaques. Acta Neuropathol. 2012;124(6):823-31. [CrossRef]
- Bodini, B.; Veronese, M.; García-Lorenzo, D.; Battaglini, M.; Poirion, E.; Chardain, A.; Freeman, L.; Louapre, C.; Tchikviladze, M.; Papeix, C.; et al. Dynamic Imaging of Individual Remyelination Profiles in Multiple Sclerosis. Ann. Neurol. 2016, 79, 726–738. [CrossRef]
- Stankoff B, Freeman L, Aigrot MS, Chardain A, Dollé F, Williams A; et al. Imaging central nervous system myelin by positron emission tomography in multiple sclerosis using [methyl-¹¹C]-2-(4'-methylaminophenyl)- 6-hydroxybenzothiazole. Ann Neurol. 2011;69(4):673-80. [CrossRef]
- Zeydan, B.; Lowe, V.J.; Schwarz, C.G.; A Przybelski, S.; Tosakulwong, N.; Zuk, S.M.; Senjem, M.L.; Gunter, J.L.; O Roberts, R.; Mielke, M.M.; et al. Pittsburgh compound-B PET white matter imaging and cognitive function in late multiple sclerosis. Mult. Scler. J. 2017, 24, 739–749. [CrossRef]
- Pietroboni, A.M.; Carandini, T.; Colombi, A.; Mercurio, M.; Ghezzi, L.; Giulietti, G.; Scarioni, M.; Arighi, A.; Fenoglio, C.; De Riz, M.A.; et al. Amyloid PET as a marker of normal-appearing white matter early damage in multiple sclerosis: Correlation with CSF β-amyloid levels and brain volumes. Eur. J. Nucl. Med. 2018, 46, 280–287. [CrossRef]
- Montalban, X.; Arnold, D.L.; Weber, M.S.; Staikov, I.; Piasecka-Stryczynska, K.; Willmer, J.; Martin, E.C.; Dangond, F.; Syed, S.; Wolinsky, J.S.; et al. Placebo-Controlled Trial of an Oral BTK Inhibitor in Multiple Sclerosis. New Engl. J. Med. 2019, 380, 2406–2417. [CrossRef]
- Reich, D.S.; Arnold, D.L.; Vermersch, P.; Bar-Or, A.; Fox, R.J.; Matta, A.; Turner, T.; Wallström, E.; Zhang, X.; Mareš, M.; et al. Safety and efficacy of tolebrutinib, an oral brain-penetrant BTK inhibitor, in relapsing multiple sclerosis: A phase 2b, randomised, double-blind, placebo-controlled trial. Lancet Neurol. 2021, 20, 729–738. [CrossRef]
- Magliozzi, R.; Howell, O.W.; Reeves, C.; Roncaroli, F.; Nicholas, R.; Serafini, B.; Aloisi, F.; Reynolds, R. A Gradient of neuronal loss and meningeal inflammation in multiple sclerosis. Ann. Neurol. 2010, 68, 477–493. [CrossRef]
- Gibiansky, E.; Petry, C.; Mercier, F.; Günther, A.; Herman, A.; Kappos, L.; Hauser, S.; Yamamoto, Y.; Wang, Q.; Model, F.; et al. Ocrelizumab in relapsing and primary progressive multiple sclerosis: Pharmacokinetic and pharmacodynamic analyses of OPERA I, OPERA II and ORATORIO. Br. J. Clin. Pharmacol. 2020, 87, 2511–2520. [CrossRef]
- Hauser, S.L.; Waubant, E.; Arnold, D.L.; Vollmer, T.; Antel, J.; Fox, R.J.; Bar-Or, A.; Panzara, M.; Sarkar, N.; Agarwal, S.; et al. B-Cell Depletion with Rituximab in Relapsing–Remitting Multiple Sclerosis. N. Engl. J. Med. 2008, 358, 676–688. [CrossRef]
- Baecher-Allan, C.; Kaskow, B.J.; Weiner, H.L. Multiple Sclerosis: Mechanisms and Immunotherapy. Neuron 2018, 97, 742–768. [CrossRef]
- Baert L, Benkhoucha M, Popa N, Ahmed MC, Manfroi B, Boutonnat J; et al. A proliferation-inducing ligand-mediated anti-inflammatory response of astrocytes in multiple sclerosis. Ann Neurol. 2019;85(3):406-20. [CrossRef]
- Pellerin, K.; Rubino, S.J.; Burns, J.C.; A Smith, B.; McCarl, C.-A.; Zhu, J.; Jandreski, L.; Cullen, P.; Carlile, T.M.; Li, A.; et al. MOG autoantibodies trigger a tightly-controlled FcR and BTK-driven microglia proliferative response. Brain 2021, 144, 2361–2374. [CrossRef]
- Martin, E.; Aigrot, M.-S.; Grenningloh, R.; Stankoff, B.; Lubetzki, C.; Boschert, U.; Zalc, B. Bruton’s Tyrosine Kinase Inhibition Promotes Myelin Repair. Brain Plast. 2020, 5, 123–133. [CrossRef]
- A Back, S.; Tuohy, T.M.F.; Chen, H.; Wallingford, N.; Craig, A.; Struve, J.; Luo, N.L.; Banine, F.; Liu, Y.; Chang, A.; et al. Hyaluronan accumulates in demyelinated lesions and inhibits oligodendrocyte progenitor maturation. Nat. Med. 2005, 11, 966–972. [CrossRef]
- Winkler, C.W.; Foster, S.C.; Matsumoto, S.G.; Preston, M.A.; Xing, R.; Bebo, B.F.; Banine, F.; Berny-Lang, M.A.; Itakura, A.; McCarty, O.J.T.; et al. Hyaluronan Anchored to Activated CD44 on Central Nervous System Vascular Endothelial Cells Promotes Lymphocyte Extravasation in Experimental Autoimmune Encephalomyelitis. J. Biol. Chem. 2012, 287, 33237–33251. [CrossRef]
- Kuipers HF, Rieck M, Gurevich I, Nagy N, Butte MJ, Negrin RS; et al. Hyaluronan synthesis is necessary for autoreactive T-cell trafficking, activation, and Th1 polarization. Proceedings of the National Academy of Sciences of the United States of America. 2016;113(5):1339-44. [CrossRef]
- Preston, M.; Gong, X.; Su, W.; Matsumoto, S.G.; Banine, F.; Winkler, C.; Foster, S.; Xing, R.; Struve, J.; Dean, J.; et al. Digestion products of the PH20 hyaluronidase inhibit remyelination. Ann. Neurol. 2013, 73, 266–280. [CrossRef]
- Asher, R.A.; Morgenstern, D.A.; Fidler, P.S.; Adcock, K.H.; Oohira, A.; Braistead, J.E.; Levine, J.M.; Margolis, R.U.; Rogers, J.H.; Fawcett, J.W. Neurocan Is Upregulated in Injured Brain and in Cytokine-Treated Astrocytes. J. Neurosci. 2000, 20, 2427–2438. [CrossRef]
- Lau, L.W.; Keough, M.B.; Haylock-Jacobs, S.; Cua, R.; Döring, A.; Sloka, S.; Stirling, D.P.; Rivest, S.; Yong, V.W. Chondroitin sulfate proteoglycans in demyelinated lesions impair remyelination. Ann. Neurol. 2012, 72, 419–432. [CrossRef]
- Stephenson, E.L.; Mishra, M.K.; Moussienko, D.; Laflamme, N.; Rivest, S.; Ling, C.-C.; Yong, V.W. Chondroitin sulfate proteoglycans as novel drivers of leucocyte infiltration in multiple sclerosis. Brain 2018, 141, 1094–1110. [CrossRef]
- Rolls, A.; Cahalon, L.; Bakalash, S.; Avidan, H.; Lider, O.; Schwartz, M. A sulfated disaccharide derived from chondroitin sulfate proteoglycan protects against inflammation-associated neurodegeneration. FASEB J. 2006, 20, 547–549. [CrossRef]
- Zhou, J.; Nagarkatti, P.; Zhong, Y.; Nagarkatti, M. Immune modulation by chondroitin sulfate and its degraded disaccharide product in the development of an experimental model of multiple sclerosis. J. Neuroimmunol. 2010, 223, 55–64. [CrossRef]
- Keough, M.B.; Rogers, J.A.; Zhang, P.; Jensen, S.K.; Stephenson, E.L.; Chen, T.; Hurlbert, M.G.; Lau, L.W.; Rawji, K.S.; Plemel, J.R.; et al. An inhibitor of chondroitin sulfate proteoglycan synthesis promotes central nervous system remyelination. Nat. Commun. 2016, 7, 11312–11312. [CrossRef]
- Graham, J.B.; Neubauer, D.; Xue, Q.-S.; Muir, D. Chondroitinase applied to peripheral nerve repair averts retrograde axonal regeneration. Exp. Neurol. 2007, 203, 185–195. [CrossRef]
- Bradbury, E.J.; Moon, L.D.F.; Popat, R.J.; King, V.R.; Bennett, G.S.; Patel, P.N.; Fawcett, J.W.; McMahon, S.B. Chondroitinase ABC promotes functional recovery after spinal cord injury. Nature 2002, 416, 636–640. [CrossRef]
- Rosenzweig, E.S.; Salegio, E.A.; Liang, J.J.; Weber, J.L.; Weinholtz, C.A.; Brock, J.H.; Moseanko, R.; Hawbecker, S.; Pender, R.; Cruzen, C.L.; et al. Chondroitinase improves anatomical and functional outcomes after primate spinal cord injury. Nat. Neurosci. 2019, 22, 1269–1275. [CrossRef]
- Siebert JR, Osterhout DJ. The inhibitory effects of chondroitin sulfate proteoglycans on oligodendrocytes. J Neurochem. 2011;119(1):176-88. [CrossRef]
- Lee, H.; McKeon, R.J.; Bellamkonda, R.V. Sustained delivery of thermostabilized chABC enhances axonal sprouting and functional recovery after spinal cord injury. Proc. Natl. Acad. Sci. USA 2009, 107, 3340–3345. [CrossRef]
- Führmann, T.; Anandakumaran, P.N.; Payne, S.L.; Pakulska, M.M.; Varga, B.V.; Nagy, A.; Tator, C.; Shoichet, M.S. Combined delivery of chondroitinase ABC and human induced pluripotent stem cell-derived neuroepithelial cells promote tissue repair in an animal model of spinal cord injury. Biomed. Mater. 2017, 13, 024103. [CrossRef]
- Kalamakis, G.; Brüne, D.; Ravichandran, S.; Bolz, J.; Fan, W.; Ziebell, F.; Stiehl, T.; Catalá-Martinez, F.; Kupke, J.; Zhao, S.; et al. Quiescence Modulates Stem Cell Maintenance and Regenerative Capacity in the Aging Brain. Cell 2019, 176, 1407–1419.e14. [CrossRef]
- Khacho, M.; Clark, A.; Svoboda, D.S.; Azzi, J.; MacLaurin, J.G.; Meghaizel, C.; Sesaki, H.; Lagace, D.C.; Germain, M.; Harper, M.-E.; et al. Mitochondrial Dynamics Impacts Stem Cell Identity and Fate Decisions by Regulating a Nuclear Transcriptional Program. Cell Stem Cell 2016, 19, 232–247. [CrossRef]
- Mimeault M, Batra SK. Great Promise of Tissue-Resident Adult Stem/Progenitor Cells in Transplantation and Cancer Therapies. In: López-Larrea C, López-Vázquez A, Suárez-Álvarez B, editors. Stem Cell Transplantation. New York, NY: Springer US; 2012. p. 171-86.
- Snethen, H.; Love, S.; Scolding, N. Disease-responsive neural precursor cells are present in multiple sclerosis lesions. Regen. Med. 2008, 3, 835–847. [CrossRef]
- Xing, Y.L.; Röth, P.T.; Stratton, J.A.S.; Chuang, B.H.; Danne, J.; Ellis, S.L.; Ng, S.W.; Kilpatrick, T.J.; Merson, T.D. Adult Neural Precursor Cells from the Subventricular Zone Contribute Significantly to Oligodendrocyte Regeneration and Remyelination. J. Neurosci. 2014, 34, 14128–14146. [CrossRef]
- Brown, C.; McKee, C.; Halassy, S.; Kojan, S.; Feinstein, D.L.; Chaudhry, G.R. Neural stem cells derived from primitive mesenchymal stem cells reversed disease symptoms and promoted neurogenesis in an experimental autoimmune encephalomyelitis mouse model of multiple sclerosis. Stem Cell Res. Ther. 2021, 12, 1–21. [CrossRef]
- Yang, J.; Jiang, Z.; Fitzgerald, D.C.; Ma, C.; Yu, S.; Li, H.; Zhao, Z.; Li, Y.; Ciric, B.; Curtis, M.; et al. Adult neural stem cells expressing IL-10 confer potent immunomodulation and remyelination in experimental autoimmune encephalitis. J. Clin. Investig. 2009, 119, 3678–3691. [CrossRef]
- Einstein, O.; Karussis, D.; Grigoriadis, N.; Mizrachi-Kol, R.; Reinhartz, E.; Abramsky, O.; Ben-Hur, T. Intraventricular transplantation of neural precursor cell spheres attenuates acute experimental allergic encephalomyelitis. Mol. Cell. Neurosci. 2003, 24, 1074–1082. [CrossRef]
- Aharonowiz, M.; Einstein, O.; Fainstein, N.; Lassmann, H.; Reubinoff, B.; Ben-Hur, T. Neuroprotective Effect of Transplanted Human Embryonic Stem Cell-Derived Neural Precursors in an Animal Model of Multiple Sclerosis. PLoS ONE 2008, 3, e3145. [CrossRef]
- Guan Y, Jiang Z, Ciric B, Rostami AM, Zhang GX. Upregulation of chemokine receptor expression by IL-10/IL-4 in adult neural stem cells. Exp Mol Pathol. 2008;85(3):232-6. [CrossRef]
- Yang, J.; Yan, Y.; Ma, C.-G.; Kang, T.; Zhang, N.; Gran, B.; Xu, H.; Li, K.; Ciric, B.; Zangaladze, A.; et al. Accelerated and enhanced effect of CCR5-transduced bone marrow neural stem cells on autoimmune encephalomyelitis. Acta Neuropathol. 2012, 124, 491–503. [CrossRef]
- Sher, F.; Amor, S.; Gerritsen, W.; Baker, D.; Jackson, S.L.; Boddeke, E.; Copray, S. Intraventricularly Injected Olig2-NSCs Attenuate Established Relapsing–Remitting EAE in Mice. Cell Transplant. 2012, 21, 1883–1897. [CrossRef]
- Moore, C.S.; Cui, Q.-L.; Warsi, N.M.; Durafourt, B.A.; Zorko, N.; Owen, D.R.; Antel, J.P.; Bar-Or, A. Direct and Indirect Effects of Immune and Central Nervous System–Resident Cells on Human Oligodendrocyte Progenitor Cell Differentiation. J. Immunol. 2015, 194, 761–772. [CrossRef]
- Imamura, O.; Arai, M.; Dateki, M.; Oishi, K.; Takishima, K. Donepezil-induced oligodendrocyte differentiation is mediated through estrogen receptors. J. Neurochem. 2019, 155, 494–507. [CrossRef]
- Peruzzotti-Jametti L, Bernstock JD, Vicario N, Costa ASH, Kwok CK, Leonardi T; et al. Macrophage-Derived Extracellular Succinate Licenses Neural Stem Cells to Suppress Chronic Neuroinflammation. Cell Stem Cell. 2018;22(3):355-68.e13. [CrossRef]
- Littlewood-Evans, A.; Sarret, S.; Apfel, V.; Loesle, P.; Dawson, J.; Zhang, J.; Muller, A.; Tigani, B.; Kneuer, R.; Patel, S.; et al. GPR91 senses extracellular succinate released from inflammatory macrophages and exacerbates rheumatoid arthritis. J. Exp. Med. 2016, 213, 1655–1662. [CrossRef]
- Yang, J.; Yan, Y.; Ciric, B.; Yu, S.; Guan, Y.; Xu, H.; Rostami, A.; Zhang, G.-X. Evaluation of Bone Marrow- and Brain-Derived Neural Stem Cells in Therapy of Central Nervous System Autoimmunity. Am. J. Pathol. 2010, 177, 1989–2001. [CrossRef]
- Xie, C.; Li, X.; Zhou, X.; Li, Z.; Zhang, Y.; Zhao, L.; Hao, Y.; Zhang, G.-X.; Guan, Y. TGFβ1 transduction enhances immunomodulatory capacity of neural stem cells in experimental autoimmune encephalomyelitis. Brain, Behav. Immun. 2018, 69, 283–295. [CrossRef]
- McIntyre, L.L.; Greilach, S.A.; Othy, S.; Sears-Kraxberger, I.; Wi, B.; Ayala-Angulo, J.; Vu, E.; Pham, Q.; Silva, J.; Dang, K.; et al. Regulatory T cells promote remyelination in the murine experimental autoimmune encephalomyelitis model of multiple sclerosis following human neural stem cell transplant. Neurobiol. Dis. 2020, 140, 104868–104868. [CrossRef]
- Harris, V.K.; Stark, J.; Vyshkina, T.; Blackshear, L.; Joo, G.; Stefanova, V.; Sara, G.; Sadiq, S.A. Phase I Trial of Intrathecal Mesenchymal Stem Cell-derived Neural Progenitors in Progressive Multiple Sclerosis. EBioMedicine 2018, 29, 23–30. [CrossRef]
- Aigrot, M.; Barthelemy, C.; Moyon, S.; Dufayet-Chaffaud, G.; Izagirre-Urizar, L.; Gillet-Legrand, B.; Tada, S.; Bayón-Cordero, L.; Chara, J.; Matute, C.; et al. Genetically modified macrophages accelerate myelin repair. EMBO Mol. Med. 2022, 14, e14759. [CrossRef]
- Atkins, H.L.; Bowman, M.; Allan, D.; Anstee, G.; Arnold, D.L.; Bar-Or, A.; Bence-Bruckler, I.; Birch, P.; Bredeson, C.; Chen, J.; et al. Immunoablation and autologous haemopoietic stem-cell transplantation for aggressive multiple sclerosis: A multicentre single-group phase 2 trial. Lancet 2016, 388, 576–585. [CrossRef]
- Burt RK, Balabanov R, Burman J, Sharrack B, Snowden JA, Oliveira MC; et al. Effect of Nonmyeloablative Hematopoietic Stem Cell Transplantation vs Continued Disease-Modifying Therapy on Disease Progression in Patients With Relapsing-Remitting Multiple Sclerosis: A Randomized Clinical Trial. JAMA. 2019;321(2):165-74. [CrossRef]
- Marin-Bañasco, C.; Marin-Bañasco, C.; Benabdellah, K.; Benabdellah, K.; Melero-Jerez, C.; Melero-Jerez, C.; Oliver, B.; Oliver, B.; Pinto-Medel, M.J.; Pinto-Medel, M.J.; et al. Gene therapy with mesenchymal stem cells expressing IFN-ß ameliorates neuroinflammation in experimental models of multiple sclerosis. Br. J. Pharmacol. 2017, 174, 238–253. [CrossRef]
- Blurton-Jones, M.; Spencer, B.; Michael, S.; A Castello, N.; A Agazaryan, A.; Davis, J.L.; Müller, F.-J.; Loring, J.F.; Masliah, E.; LaFerla, F.M. Neural stem cells genetically-modified to express neprilysin reduce pathology in Alzheimer transgenic models. Stem Cell Res. Ther. 2014, 5, 46–46. [CrossRef]
- Suzuki, M.; McHugh, J.; Tork, C.; Shelley, B.; Hayes, A.; Bellantuono, I.; Aebischer, P.; Svendsen, C.N. Direct Muscle Delivery of GDNF With Human Mesenchymal Stem Cells Improves Motor Neuron Survival and Function in a Rat Model of Familial ALS. Mol. Ther. 2008, 16, 2002–2010. [CrossRef]
- Eichler, F.; Duncan, C.; Musolino, P.L.; Orchard, P.J.; De Oliveira, S.; Thrasher, A.J.; Armant, M.; Dansereau, C.; Lund, T.C.; Miller, W.P.; et al. Hematopoietic Stem-Cell Gene Therapy for Cerebral Adrenoleukodystrophy. New Engl. J. Med. 2017, 377, 1630–1638. [CrossRef]
- De Ravin, S.S.; Wu, X.; Moir, S.; Kardava, L.; Anaya-O’brien, S.; Kwatemaa, N.; Littel, P.; Theobald, N.; Choi, U.; Su, L.; et al. Lentiviral hematopoietic stem cell gene therapy for X-linked severe combined immunodeficiency. Sci. Transl. Med. 2016, 8, 335ra57–335ra57. [CrossRef]
- Bak, R.O.; Dever, D.P.; Porteus, M.H. CRISPR/Cas9 genome editing in human hematopoietic stem cells. Nat. Protoc. 2018, 13, 358–376. [CrossRef]
- Walmsley, A.R.; Mir, A.K. Targeting the Nogo-A Signalling Pathway to Promote Recovery Following Acute CNS Injury. Curr. Pharm. Des. 2007, 13, 2470–2484. [CrossRef]
- Petratos, S.; Ozturk, E.; Azari, M.F.; Kenny, R.; Lee, J.Y.; Magee, K.A.; Harvey, A.R.; McDonald, C.; Taghian, K.; Moussa, L.; et al. Limiting multiple sclerosis related axonopathy by blocking Nogo receptor and CRMP-2 phosphorylation. Brain 2012, 135, 1794–1818. [CrossRef]
- Niederöst, B.; Oertle, T.; Fritsche, J.; McKinney, R.A.; Bandtlow, C.E. Nogo-A and Myelin-Associated Glycoprotein Mediate Neurite Growth Inhibition by Antagonistic Regulation of RhoA and Rac1. 2002, 22, 10368–10376. [CrossRef]
- Wang, X.; Ba, K.W.B.; Basso, D.M.; Strittmatter, S.M. Delayed Nogo receptor therapy improves recovery from spinal cord contusion. Ann. Neurol. 2006, 60, 540–549. [CrossRef]
- Wang X, Lin J, Arzeno A, Choi JY, Boccio J, Frieden E; et al. Intravitreal delivery of human NgR-Fc decoy protein regenerates axons after optic nerve crush and protects ganglion cells in glaucoma models. Invest Ophthalmol Vis Sci. 2015;56(2):1357-66. [CrossRef]
- Seita, J.; Weissman, I.L. Hematopoietic stem cell: Self-renewal versus differentiation. Wiley Interdiscip. Rev. Syst. Biol. Med. 2010, 2, 640–653. [CrossRef]
- Peterson, C.W.; Adair, J.E.; Wohlfahrt, M.E.; Deleage, C.; Radtke, S.; Rust, B.; Norman, K.K.; Norgaard, Z.K.; Schefter, L.E.; Sghia-Hughes, G.M.; et al. Autologous, Gene-Modified Hematopoietic Stem and Progenitor Cells Repopulate the Central Nervous System with Distinct Clonal Variants. Stem Cell Rep. 2019, 13, 91–104. [CrossRef]
- Ruckh, J.M.; Zhao, J.-W.; Shadrach, J.L.; van Wijngaarden, P.; Rao, T.N.; Wagers, A.J.; Franklin, R.J. Rejuvenation of Regeneration in the Aging Central Nervous System. Cell Stem Cell 2012, 10, 96–103. [CrossRef]
- Fournier, A.E.; Gould, G.C.; Liu, B.P.; Strittmatter, S.M. Truncated Soluble Nogo Receptor Binds Nogo-66 and Blocks Inhibition of Axon Growth by Myelin. 2002, 22, 8876–8883. [CrossRef]
- Kotter, M.R.; Li, W.-W.; Zhao, C.; Franklin, R.J.M. Myelin Impairs CNS Remyelination by Inhibiting Oligodendrocyte Precursor Cell Differentiation. J. Neurosci. 2006, 26, 328–332. [CrossRef]
- Ye S, Theotokis P, Lee JY, Kim MJ, Nheu D, Ellen O; et al. Nogo receptor-Fc delivered by hematopoietic cells enhances neurorepair in a multiple sclerosis model. Brain Communications. 2023. [CrossRef]
- Rüther, B.J.; Scheld, M.; Dreymueller, D.; Clarner, T.; Kress, E.; Brandenburg, L.; Swartenbroekx, T.; Hoornaert, C.; Ponsaerts, P.; Fallier-Becker, P.; et al. Combination of cuprizone and experimental autoimmune encephalomyelitis to study inflammatory brain lesion formation and progression. Glia 2017, 65, 1900–1913. [CrossRef]
- Scheld, M.; Rüther, B.J.; Große-Veldmann, R.; Ohl, K.; Tenbrock, K.; Dreymüller, D.; Fallier-Becker, P.; Zendedel, A.; Beyer, C.; Clarner, T.; et al. Neurodegeneration Triggers Peripheral Immune Cell Recruitment into the Forebrain. J. Neurosci. 2016, 36, 1410–1415. [CrossRef]
Figure 1.
Outside-in and inside-out mechanisms during the pathogenesis of MS. The outside-in mechanism illustrates the infiltration of reactive CD4+ and CD8+ T cells, along with B cells, that travel from the periphery, across the BBB, and into the CNS. These cell types target and attack myelin-associated epitopes on myelinated axons, secreting a myriad of pro-inflammatory cytokines which lead to neural cell dystrophy, and glial reactive changes to promulgate neurodegeneration. Conversely, the inside-out mechanism employs the concept of Wallerian degeneration, axonal and oligodendrocyte dystrophy, whereby remyelination failure in MS is mediated by astrocytes and a peripheral/resident immune cell responses through slowly progressive lesions. CSF: cerebrospinal fluid; APC: antigen-presenting cell; TCR: T-cell receptor; MOG: myelin oligodendrocyte glycoprotein; MMP: matrix metalloproteinase; ICAM: intercellular adhesion molecule; ROS: reactive oxygen species; OCT: optical coherence tomography; MRI: magnetic resonance imaging; DTI: diffusion tensor imaging; 1H-MRS: proton magnetic resonance spectroscopy; PET: positron emission tomography.
Figure 1.
Outside-in and inside-out mechanisms during the pathogenesis of MS. The outside-in mechanism illustrates the infiltration of reactive CD4+ and CD8+ T cells, along with B cells, that travel from the periphery, across the BBB, and into the CNS. These cell types target and attack myelin-associated epitopes on myelinated axons, secreting a myriad of pro-inflammatory cytokines which lead to neural cell dystrophy, and glial reactive changes to promulgate neurodegeneration. Conversely, the inside-out mechanism employs the concept of Wallerian degeneration, axonal and oligodendrocyte dystrophy, whereby remyelination failure in MS is mediated by astrocytes and a peripheral/resident immune cell responses through slowly progressive lesions. CSF: cerebrospinal fluid; APC: antigen-presenting cell; TCR: T-cell receptor; MOG: myelin oligodendrocyte glycoprotein; MMP: matrix metalloproteinase; ICAM: intercellular adhesion molecule; ROS: reactive oxygen species; OCT: optical coherence tomography; MRI: magnetic resonance imaging; DTI: diffusion tensor imaging; 1H-MRS: proton magnetic resonance spectroscopy; PET: positron emission tomography.
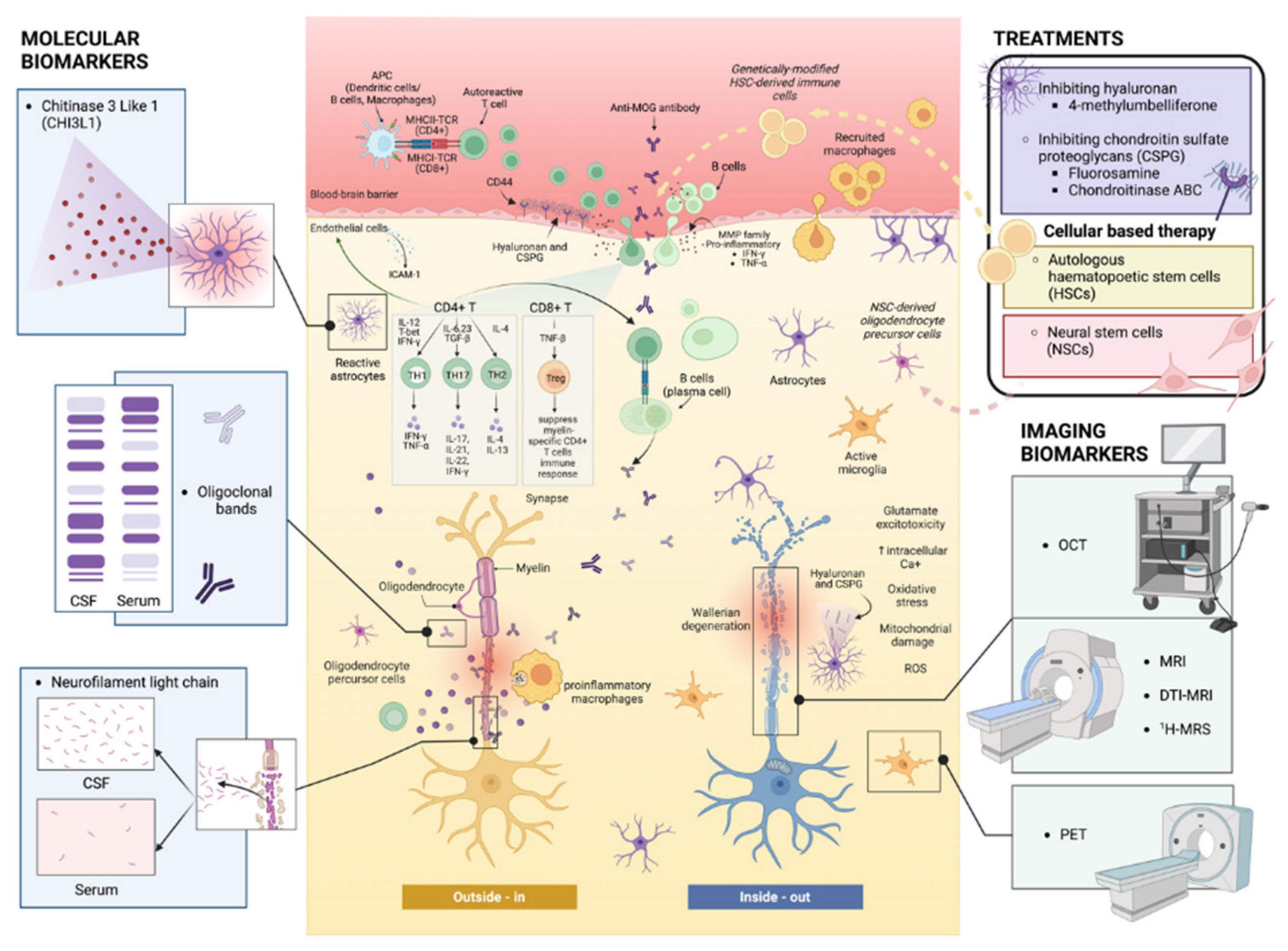
Disclaimer/Publisher’s Note: The statements, opinions and data contained in all publications are solely those of the individual author(s) and contributor(s) and not of MDPI and/or the editor(s). MDPI and/or the editor(s) disclaim responsibility for any injury to people or property resulting from any ideas, methods, instructions or products referred to in the content. |
© 2023 by the authors. Licensee MDPI, Basel, Switzerland. This article is an open access article distributed under the terms and conditions of the Creative Commons Attribution (CC BY) license (http://creativecommons.org/licenses/by/4.0/).
Copyright: This open access article is published under a Creative Commons CC BY 4.0 license, which permit the free download, distribution, and reuse, provided that the author and preprint are cited in any reuse.



